Embed Size (px)
Citation preview

Fungal corneal ulcer
By Glin Luckose Fernandez
The incidence of fungal corneal ulcer has increased during the recent years due to injudicious use of antibiotics and steroids
Contents • Etiology• Modes of infection • Role of antibiotics and steroids • Clinical features• Diagnosis• Treatment
Etiology Filamentous fungi : eg :: Septate : Aspergillus , Penicillium, Fusarium :: Aseptate : Mucor , Rizopus• Yeast : eg :: Candida , Cryptococcus• Dimorphic fungi : eg :: Histoplasma , Coccidioides , Blastomyces
Most commonly mycotic corneal uncler is caused by : Aspergillus , Candida , Fusarium
Modes of Infection• Injury by vegetative material : corp
leaf , branch of tree , straw , hay- commonly affects field workers especially during harvesting seasons.
• Injury by animal tail • Secondary fungal ulcers: common in
immunosupresed ,in patients with dry eye , herpetic ulcer , bullous keratopathy or post operative cases of keratoplasty
Role of antibiotics and steroids
• Antibiotics disturbs the symbiosis between bacteria and fungi and steroids make fungi facultative pathogen.
• Excessive use of them predisposes the patients to fungal infection
Clinical features
• Symptoms : *Pain , foreign body sensation – due to
mechanical effects of lids and chemical effects of toxins on exposed nerve ending
*Watering of eyes – due to reflex lacrimation * Photophobia – intolerance to light due to
stimulation of nerve ending * Blurred vision – due to corneal haze * Redness – congession of circumcorneal vessels
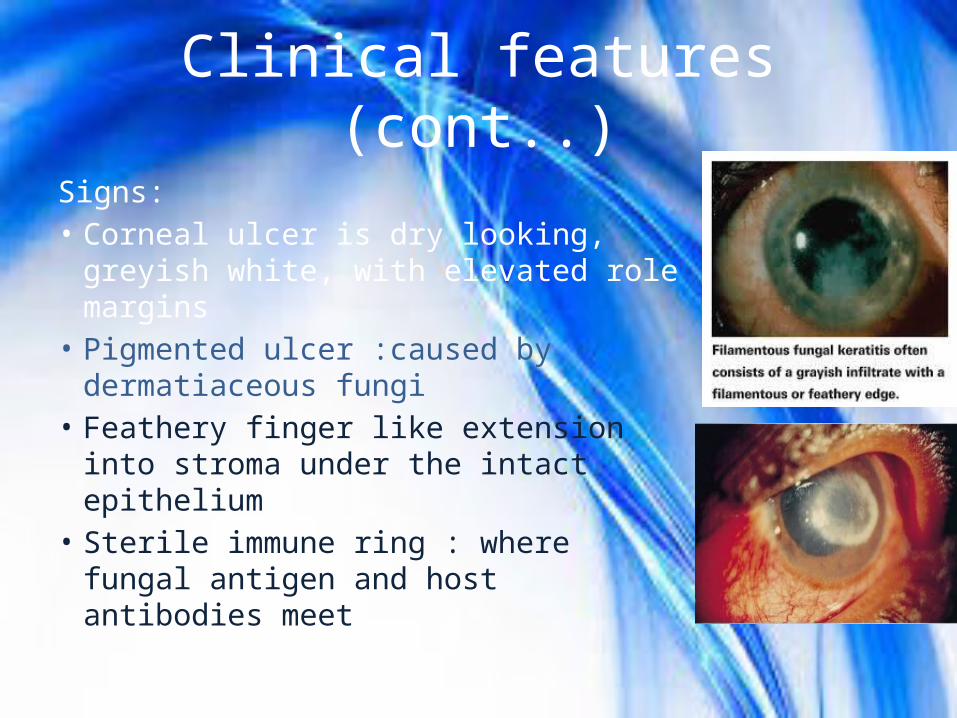
Clinical features (cont..)Signs:• Corneal ulcer is dry looking, greyish
white, with elevated role margins• Pigmented ulcer :caused by
dermatiaceous fungi• Feathery finger like extension into
stroma under the intact epithelium• Sterile immune ring : where fungal
antigen and host antibodies meet
Clinical features (cont..)Signs( cont..)• Multiple small satellite lesions around
the ulcer• Big hypopion – not sterile ( fungi can
penetrate into the anterior chamber)• Endothelial plague – composed of fibrin and
leucocytes , under stromal lesion• Perforation ( rare)• Corneal vascularization is absent
Diagnosis• By typical clinical manifestation with history of injury by
vegetative material• Chronic ulcer worsen with most effective treatment –
suspicion of mycotic involvement• Lab Diagnosis : Wet KOH, Colcoflour
white, Grams stain , Culture on Sabourauds agar media• Confocal microscopic examination • PCR Sample Collection :Corneal scraping – from base and edgeAnterior chamber parancentesisCorneal biopsy
Treatment• Specific Treatment: * Topical antifungal eye drops -for 6 to 8
week- Natamycin (5%), Amphotericin B( 0.1% to 3%)- for every 1 hr initially then tapered over 6 to 8 weeks; Nystatin (3.5%) eye ointment 5 times a day.
* Intracorneal or intrastromal administration- of voriconazole in cases intraocular extension or anterior chamber .
* Systemic antifungal – in sever cases of deeper fungal keratitis- tablet fluconazole or ketoconazole for 2 -3 weeks
Treatment ( cont..)• Nonspecific : * Cycloplegic drugs : 1% atropin , homatropine 2% - to reduce pain from cilliary spasm - to prevent posterior scynechiae from secondary
iridoclyclitis. - Increace blood supply to relieve pressure and bring
more antibodies in aqueous humour - reduce exudation by decreasing hyperemia and
vascular permeabily * Systemic analgesics and anti inflammatory – paracetamol and
ibuprofen
• Therapeutic penatrating keratoplasty - for nonresponsive cases

For