-
Goce SpasovskiRaymond VanholderBruno AllolioDjillali AnnaneSteve
BallDaniel BichetGuy DecauxWiebke FenskeEwout HoornCarole
IchaiMichael JoannidisAlain SoupartRobert ZietseMaria HallerSabine
van der VeerWim Van BiesenEvi Nagler
Clinical practice guideline on diagnosisand treatment of
hyponatraemia
Received: 31 December 2013Accepted: 3 January 2014Published
online: 22 February 2014 Springer-Verlag Berlin Heidelberg andESICM
2014
Electronic supplementary materialThe online version of this
article(doi:10.1007/s00134-014-3210-2) containssupplementary
material.
G. SpasovskiState University Hospital Skopje,
Skopje,Macedonia
R. Vanholder W. Van Biesen ())Ghent University Hospital, Ghent,
Belgiume-mail: [email protected]
B. Allolio W. FenskeWurzburg University Hospital,
Wurzburg,Germany
D. AnnaneRaymond Poincare Hospital, University ofVersailles
Saint Quentin, Paris, France
S. BallNewcastle Hospitals and NewcastleUniversity, Newcastle,
UK
D. BichetConsultant Nephrologist, Sacre-CoeurHospital,
University of Montreal, Montreal,Canada
G. Decaux A. SoupartErasmus University Hospital,
Brussels,Belgium
E. Hoorn R. ZietseErasmus Medical Centre, Rotterdam,The
Netherlands
C. IchaiNice University Hospital, Nice, France
M. JoannidisInnsbruck University Hospital, Innsbruck,Austria
M. Haller S. van der Veer E. NaglerERBP Methods Support Team,
GhentUniversity Hospital, Ghent, Belgium
M. HallerKH Elisabethinen Linz, Linz, Austria
S. van der VeerCentre for informatics, Amsterdam MedicalCentre,
Amsterdam, The Netherlands
Abstract Hyponatraemia, defined asa serum sodium
concentration\135 mmol/L, is the most commondisorder of body fluid
and electrolytebalance encountered in clinical prac-tice.
Hyponatraemia is present in1520 % of emergency admissions
tohospital and occurs in up to 20 % ofcritically ill patients.
Symptomatologymay vary from subtle to severe or evenlife
threatening. Despite this, the man-agement of patients
remainsproblematic. Against this background,the European Society of
Intensive CareMedicine, the European Society ofEndocrinology and
the European RenalAssociationEuropean Dialysis andTransplant
Association, represented byEuropean Renal Best Practice
havedeveloped a Clinical Practice Guide-line on the diagnostic
approach andtreatment of hyponatraemia as a jointventure of three
societies representingspecialists with a natural interest
inhyponatraemia.
Keywords Hyponatraemia Hypotonic Guideline Diagnosis
Management
Intensive Care Med (2014) 40:320331DOI 10.1007/s00134-014-3210-2
GUIDELINES
-
1 Introduction and methodology
Hyponatraemia, defined as a serum sodium concentration\135
mmol/L, is the most common disorder of body fluidand electrolyte
balance encountered in clinical practice.Hyponatraemia is present
in 1520 % of emergencyadmissions to hospital and occurs in up to 20
% of criti-cally ill patients [1]. It can lead to a wide spectrum
ofclinical symptoms, from subtle to severe or even lifethreatening
[2, 3] and is associated with increased mortality,morbidity and
length of hospital stay in patients presentingwith a range of
conditions. Despite this, the management ofpatients remains
problematic. The prevalence of hypona-traemia in widely different
conditions and the fact thathyponatraemia is managed by clinicians
with a broad varietyof backgrounds, has fostered diverse
institution- and speci-ality-based approaches to diagnosis and
treatment.
Against this background, the European Society ofIntensive Care
Medicine (ESICM), the European Societyof Endocrinology (ESE) and
the European Renal Asso-ciationEuropean Dialysis and Transplant
Association(ERAEDTA), represented by European Renal BestPractice
(ERBP) have developed this Clinical PracticeGuideline on the
diagnostic approach and treatment ofhyponatraemia as a joint
venture of three societies rep-resenting specialists with a natural
interest inhyponatraemia. In addition to a rigorous approach
tomethodology and evaluation, we were keen to ensure thedocument
focused on patient-important outcomes and hadutility for clinicians
involved in every-day practice.
The ERBP methods support team searched TheCochrane Database of
Systematic Reviews (May 2011),DARE (May 2011), CENTRAL (May 2011)
and MED-LINE (1946 to May, week 4, 2011) for both questions
ondiagnosis and treatment. To identify limits for theincrease in
serum sodium concentration above which therisk of osmotic
demyelination starts to rise, they searchedMEDLINE from 1997
onwards under the assumption thatearlier reports would describe
more dramatic increasesand would not contribute to helping us set
an upper limit.
A member of the ERBP methods support team screenedall titles and
abstracts to discard the clearly irrelevant ones.All members of the
guideline development group completeda second screening. All
abstracts that did not meet theinclusion criteria were discarded.
Any discrepancies at thisstage were resolved by group consensus.
The methods sup-port team retrieved full texts of potentially
relevant studiesand two reviewers examined them for eligibility
indepen-dently of each other. The reviewer duos always included
onecontent specialist and a methodologist of the ERBP
methodssupport team. Any discrepancies were resolved by consen-sus.
If no consensus could be reached, the disagreement wassettled by
group arbitrage. The evidence for outcomes ontherapeutic
interventions from included systematic reviewsand randomised
controlled trials was presented using the
Grading of Recommendations Assessment, Developmentand Evaluation
(GRADE) toolbox developed by the inter-national GRADE working group
(http://www.gradeworkinggroup.org/).
The guideline underwent external peer review
beforepublication.
This condensed version of the Clinical PracticeGuideline on
Diagnosis and Treatment of Hyponatraemiafocuses on recommendations
on diagnosis and treatmentof hyponatraemia, the full version of the
guidelines,additionally covering conflict of interest, purpose
andscope, methods of guideline development and pathophy-siology of
hyponatraemia, is available as electronicsupplemental material
(ESM).
2 Diagnosis of hyponatraemia
2.1 Classification of hyponatraemia
2.1.1 Definition of hyponatraemia based on
biochemicalseverity
We define mild hyponatraemia as a biochemicalfinding of a serum
sodium concentration between 130and 135 mmol/L as measured by ion
specific electrode.
We define moderate hyponatraemia as a biochemicalfinding of a
serum sodium concentration between 125and 129 mmol/L as measured by
ion specific electrode.
We define profound hyponatraemia as a biochemicalfinding of a
serum sodium concentration\125 mmol/Las measured by ion specific
electrode.
2.1.2 Definition of hyponatraemia based on timeof
development
We define acute hyponatraemia as hyponatraemia that isdocumented
to exist \48 h. We define chronic hyp-onatraemia as hyponatraemia
that is documented to existfor at least 48 h. If the hyponatraemia
cannot be classified,we consider it being chronic, unless there is
clinical oranamnestic evidence of the contrary (Tables 1, 2).
2.1.3 Definition of hyponatraemia based on symptoms
We define moderately symptomatic hyponatraemia asany biochemical
degree of hyponatraemia in the pre-sence of moderately severe
symptoms of hyponatraemia(Table 1).
We define severely symptomatic hyponatraemia as anybiochemical
degree of hyponatraemia in the presence ofsevere symptoms of
hyponatraemia (Table 1).
321
-
Why did we choose to set definitions?Hyponatraemia can be
classified based on different
parameters. These include serum sodium concentration,rate of
development, symptom severity, serum osmolality,and volume status.
For this guideline, we wanted theclassification to be consistent
and clear so all users wouldhave a correct understanding of the
terminology used. Wealso wanted to make the classification directly
relevant forpatient management. However, treatment strategies
can-not be adequately classified with reference to a
singlecriterion. Hence, treatment strategies have been
classifiedaccording to combinations of these criteria.
What are these definitions based on?Classification based on
serum sodium concentrationAuthors mostly use the terms mild,
moderate, and
severe [46]. We have chosen to replace severe byprofound to
avoid confusion with the classification based
on symptoms, for which we have reserved the term severe.The
definitions of mild, moderate and profound hypona-traemia in
published research are variable; especially thethreshold used to
define profound hyponatraemia for whichvalues have ranged from 110
to 125 mmol/L [7, 8]. Severalstudies report that when serum sodium
concentrations dropbelow 125 mmol/L, symptoms become more common
[1, 4,913], and the correction to normonatraemia
necessitatescareful monitoring to avoid overly rapid correction
[14].
Classification based on duration and speed
ofdevelopmentPublished research suggests using a threshold of 48 h
todistinguish acute from chronic hyponatraemia. Brainoedema seems
to occur more frequently when hypona-traemia develops in\48 h
[1518]. Experimental studiesalso suggest that the brain needs
approximately 48 h toadapt to a hypotonic environment, achieved
mainly byextruding sodium, potassium, chloride and organic os-moles
from its cells [1921]. Before adaptation, there is arisk of brain
oedema, because the lower extracellularosmolality promotes a shift
of water into the cells.However, once adaptation is completed,
brain cells canagain sustain damage if the serum sodium
concentrationincreases too rapidly. Breakdown of the myelin
sheathinsulating individual neurons can result in what is calledthe
osmotic demyelination syndrome [2225]. Conse-quently, it is
important to distinguish between acute andchronic hyponatraemia to
assess whether someone is atgreater risk of immediate brain oedema
than of osmoticdemyelination [26]. Unfortunately, in clinical
practice,the distinction between acute and chronic hyponatraemiais
often unclear, particularly for patients presenting to theemergency
room. It is often unknown when the serumsodium concentration has
started decreasing. If classify-ing hyponatraemia as acute or
chronic is not possible, wehave decided to consider the
hyponatraemia as beingchronic, unless there are reasons to assume
it is acute(Table 10). There is a good reason for this
approach.Chronic hyponatraemia is much more common than
acutehyponatraemia and should be managed accordingly toavoid
osmotic demyelination [27, 28].
Classification based on symptomsWe have divided symptoms of
hyponatraemia intomoderately severe and severe. The distinction is
basedon selected observations in acute hyponatraemia; thosewho
subsequently die more often experience what wedefine as severe
symptoms than those who live [15, 16].Moderately severe symptoms
caused by brain oedema areless frequently associated with death.
Nevertheless, theymay rapidly progress to more severe symptoms
associatedwith an adverse outcome.
We have purposefully omitted the category asymp-tomatic as we
felt this might create confusion. Patientsare probably never truly
asymptomatic in the strictestsense of the word. Very limited and
subclinical signs such
Table 1 (Table 5 of the online document): classification
ofsymptoms of hyponatraemia
Severity Symptom
Moderately severe Nausea without vomitingConfusionHeadache
Severe VomitingCardio-respiratory distressAbnormal and deep
somnolenceSeizuresComa (Glasgow Coma Scale B8)
The guideline development group wants to underscore that
thesesymptoms can also be induced by other conditions. Clinical
andanamnestic data should be taken into account when assessing
thecausal relation between the hyponatraemia and a certain
symptom(i.e. to assess whether the symptom has been caused by the
hyp-onatraemia or the hyponatraemia by the underlying
condition/symptom). The less pronounced (e.g. mild) the biochemical
degreeof hyponatraemia, the more caution should be taken when
con-sidering that the hyponatraemia is the cause of the symptoms.
Thislist is not exhaustive, and all symptoms that can be signs of
cerebraloedema should be considered as severe or moderate symptoms
thatcan be caused by hyponatraemia
Table 2 (Table 8 of the online document): drugs and
conditionsassociated with acute hyponatraemia (\48 h)
Postoperative phasePost-resection of the prostate,
post-resection of endoscopic uterine
surgeryPolydipsiaExerciseRecent thiazides
prescription3,4-Methyleendioxymethamfetamine (MDMA, XTC)Colonoscopy
preparationCyclophosphamide (intravenous)OxytocinRecently started
desmopressin therapyRecently started terlipressin, vasopressin
322
-
as mild concentration deficits are seen even with
mildhyponatraemia [29].
A classification based on symptoms aims to reflect thedegree of
brain oedema and the extent of immediate danger.It allows matching
treatment to the immediate risk, withmore aggressive treatment for
symptoms that are moresevere. Nevertheless, a classification based
only on symp-tom severity has several shortcomings. First, symptoms
ofacute and chronic hyponatraemia may overlap [29]. Sec-ond,
patients with acute hyponatraemia can present withoutclear
symptoms, but go on to develop moderately severe tosevere symptoms
within hours [15]. Third, symptoms ofhyponatraemia are nonspecific.
Consequently, assessmentof symptoms needs to happen with caution.
Clinicians needto be wary that symptoms can be caused by conditions
otherthan hyponatraemia; by other conditions in combinationwith
hyponatraemia; or by conditions that cause the hyp-onatraemia. In
general, one should be particularly carefulwhen attributing
moderately severe to severe symptoms tohyponatraemia when the
biochemical degree of hypona-traemia is only mild (Table 1).
Classification based on serum osmolalityAs this guideline aimed
to cover the aspects of diagnosis
and treatment specifically of hypotonic hyponatraemia,we needed
to define what distinguishes hypotonic fromnon-hypotonic
hyponatraemia. Because this distinction isa necessary first step in
the diagnostic evaluation of anyhyponatraemia, we have devoted a
separate chapter to thistopic (chapter 8.2). For reasons of
completeness, webriefly mention it here. A measured serum
osmolality\275 mOsm/kg always indicates hypotonic hyponatra-emia,
as effective osmolality can never be higher thantotal or measured
osmolality. In contrast, if calculatedosmolality \275 mOsm/kg, the
hyponatraemia can behypotonic, isotonic or hypertonic, depending on
whichosmotically active agents are present and whether or notthey
are incorporated in the formula [30].
Classification based on volume statusPatients with hyponatraemia
may be hypovolaemic, eu-volaemic, or hypervolaemic [31]. Many
traditionaldiagnostic algorithms start with a clinical assessment
ofvolume status [32]. However, it is often not clear if vol-ume
status in this context refers to the extracellular fluidvolume, to
the effective circulating volume or to the totalbody water. In
addition, the sensitivity and specificity ofclinical assessments of
volume status are low, potentiallyleading to misclassification
early in the diagnostic tree[33, 34]. Therefore, we have used the
terms effectivecirculating volume and extracellular fluid
volumethroughout the text to reduce ambiguity.
Note of cautionWe wanted the classification of hyponatraemia to
beconsistent, easy to use and helpful for both
differentialdiagnosis and treatment. Hyponatraemia can be
classified
according to different factors, each with advantages andpitfalls
depending on the clinical setting and situation. Wehave prioritized
the criteria such that we would obtain aclassification that would
be clinically relevant and aswidely applicable as possible.
Nevertheless, the user should keep in mind that differ-ential
diagnosis of hyponatraemia is difficult and noclassification can be
100 % accurate in every situation. Weemphasize that the different
classifications of hyponatra-emia are not mutually exclusive, and
that classificationshould always occur with the clinical condition
and thepossibility of combined causes of hyponatraemia in mind.
2.2 Confirming hypotonic and excluding non-hypotonic
hyponatraemia
We recommend excluding hyperglycaemic hyponatra-emia by
measuring the serum glucose concentrationand correcting the
measured serum sodium concentra-tion for the serum glucose
concentration if the latter isincreased. (1D)
Hyponatraemia with a measured osmolality\275 mOsm/kg always
reflects hypotonic hyponatra-emia. (not graded)
Accept as hypotonic hyponatraemia a hyponatraemiawithout
evidence for causes of non-hypotonic hyp-onatraemia as listed in
Table 3. (not graded)
Advice for clinical practice
Estimates of the serum sodium concentration correctedfor the
presence of hyperglycaemia can be obtained fromthe following
equations [35]:
Corrected serum Na measured Na 2:4
Glu cos e mg=dl 100 mg=dl100 mg=dl
Corrected Na measured Na 2:4
Glu cos e mmol=L 5:5 mmol=L5:5 mmol=L
where [Na?] is the serum sodium concentration, [Glu-cose] is the
serum glucose concentration.
This translates into adding 2.4 mmol/L to the mea-sured serum
sodium concentration for every 5.5 mmol/L(100 mg/dL) incremental
rise in serum glucose concen-tration above a standard serum glucose
concentration of5.5 mmol/L (100 mg/dL).
Alternatively, the estimated value of the correctedserum sodium
concentration across a range of serumglucose concentrations can be
obtained from (ESMTable 10).
323
-
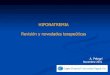
2.3 Which parameters to use for differentiating causesof
hypotonic hyponatraemia? (Fig. 1)
We recommend interpreting urine osmolality of a spoturine sample
as a first step. (1D)
If urine osmolality B100 mOsm/kg, we recommendaccepting relative
excess water intake as a cause of thehypotonic hyponatraemia.
(1D)
If urine osmolality [100 mOsm/kg, we recommendinterpreting the
urine sodium concentration on a spoturine sample taken
simultaneously with a blood sam-ple. (1D)
If urine sodium concentration B30 mmol/L, we suggestaccepting
low effective arterial volume as a cause of thehypotonic
hyponatraemia. (2D)
If urine sodium concentration[30 mmol/L, we suggestassessing
extracellular fluid status and use of diuretics tofurther
differentiate likely causes of the hyponatraemia.(2D)
We suggest against measuring vasopressin for con-firming the
diagnosis of SIADH. (2D)
Advice for clinical practice
Correct interpretation of laboratory measurementsrequires
contemporaneous collection of blood and urinespecimens.
For practical reasons, urine osmolality and sodiumconcentration
are best determined in the same urinesample.
If clinical assessment indicates the volume of extracel-lular
fluid is not overtly increased and the urine sodiumconcentration
[30 mmol/L, exclude other causes ofhypotonic hyponatraemia before
implicating SIAD.Consider using the diagnostic criteria listed in
Tables 4,5 and looking for known causes of SIAD.
Consider primary or secondary adrenal insufficiency asan
underlying cause of the hypotonic hyponatraemia.
Kidney disease complicates differential diagnosis
ofhyponatraemia. Besides possibly contributing to thehyponatraemia,
the ability of the kidneys to regulateurine osmolality and urine
sodium is often diminished,much like with the use of diuretics. As
urine osmolalityand sodium may no longer reflect the effects of
theregular hormonal axes regulating water and sodiumhomeostasis,
any diagnostic algorithm for hyponatra-emia must be used with
caution in patients with kidneydisease.
The water-loading test is generally not helpful fordifferential
diagnosis of hypotonic hyponatraemia andmay be dangerous in this
setting.
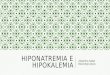
3 Treatment of hypotonic hyponatraemia
How to use the treatment recommendations
The advice provided in this chapter follows a specifichierarchy
as illustrated in Fig. 2. Individual recommen-dations and
statements can only be correctly interpretedand implemented if
considered within this structure.
The guideline development group felt that with severeor
moderately severe symptoms, the risk of brain oedemaoutweighs the
risk of osmotic demyelination syndrome.They felt it justifies
urgent treatment in these conditions,irrespective of biochemical
degree or timing (acute versuschronic) of hyponatraemia.
Conversely, the guidelinedevelopment group believed that in the
absence of severeor moderately severe symptoms, there is time for
diag-nostic assessment, and cause-specific treatment is themost
reasonable approach.
For a correct interpretation of the algorithm in Fig. 2,it is
crucial to understand that for correctly classifying
Table 3 (Table 10 of the online document): causes of
non-hypotonic hyponatraemia
Setting Serum osmolality Examples
Presence of effective osmoles that raiseserum osmolality and can
cause hyponatraemia
Isotonic or hypertonic Glucose [35]Mannitol [38]Glycine
[39]Histidinetryptophaneketoglutarate [40]Hyperosmolar
radiocontrast media [41]Maltose [42]
Presence of ineffective osmoles that raise serumosmolality but
do not cause hyponatraemia
Isotonic or hyperosmolar Urea [43]Alcohols [43]Ethylene-glycol
[43]
Presence of endogenous solutes that causepseudohyponatraemia
(laboratory artifact)
Isotonic Triglycerides [44]Cholesterol [44]Protein intravenous
immunoglobulins [45]Monoclonal gammapathies [46]
324
-
symptoms as severe or moderately severe, there mustbe sufficient
confidence that the symptoms are caused byhyponatraemia. If
hyponatraemia is mild and symptomsare severe or moderately severe
(Table 5 of the onlinedocument), the guideline development group
advises toonly accept causality in exceptional cases.
Consequently,generally, chapters 3.1, 3.2, and 3.3 are not
applicablewhen hyponatraemia is mild. It is also essential
tounderstand that the guideline development group
distinguishes between targets and limits. A target is agoal one
is aiming for; it is the change in serum sodiumconcentration that
one wishes and expects to achievewith a particular treatment. In
contrast, a limit is achange in serum sodium concentration one does
notwant to exceed and if surpassed, requires prompt
coun-ter-regulating intervention as described in chapter 9.5(ESM).
In addition, the reader should bear in mind thatthe absolute
numbers provided as targets or limits
7
Fig. 1 (Fig. 6 of the onlinedocument): algorithm for
thediagnosis of hyponatraemia
325
-
should always be interpreted in the clinical context ofthe
individual patient.
3.1 Hyponatraemia with severe symptoms
3.1.1 First hour management, regardlessof whether hyponatraemia
is acute or chronic
We recommend prompt intravenous infusion of 150 mL3 % hypertonic
saline or equivalent over 20 min. (1D)We suggest checking the serum
sodium concentra-tion after 20 min while repeating an infusion of
150 mL3 % hypertonic saline or equivalent over the next 20
min.(2D)We suggest repeating therapeutic recommendations3.1.1.1 and
3.1.1.2 twice or until a target of 5 mmol/Lincrease in serum sodium
concentration is achieved. (2D)
Manage patients with severely symptomatic hypona-traemia in an
environment where close biochemical andclinical monitoring can be
provided. (not graded)
3.1.2 Follow up management in case of improvementof symptoms
after a 5 mmol/L increase in serumsodium concentration in the first
hour, regardlessof whether hyponatraemia is acute or chronic
We recommend stopping the infusion of hypertonicsaline. (1D)
We recommend keeping the intravenous line open byinfusing the
smallest feasible volume of 0.9 % salineuntil cause-specific
treatment is started. (1D)
We recommend starting a diagnosis specific treatmentif
available, aiming at least to stabilize sodium con-centration.
(1D)
We recommend limiting the increase in serum sodiumconcentration
to a total of 10 mmol/L during the first24 h and an additional 8
mmol/L during every 24 hthereafter until the serum sodium
concentration reaches130 mmol/L. (1D)
We suggest checking the serum sodium concentrationafter 6 and 12
h, and daily afterwards until the serumsodium concentration has
stabilised under stabletreatment. (2D)
3.1.3 Follow up management in case of no improvementof symptoms
after a 5 mmol/L increase in serumsodium concentration in the first
hour, regardlessof whether the hyponatraemia is acute or
chronic
We recommend continuing an intravenous infusion of3 % hypertonic
saline or equivalent aiming for anadditional 1 mmol/L/h increase in
serum sodium con-centration (1D).
We recommend stopping the infusion of 3 % hypertonicsaline or
equivalent when the symptoms improve, theserum sodium concentration
increases 10 mmol/L in totalor the serum sodium concentration
reaches 130 mmol/L,whichever occurs first (1D).
We recommend additional diagnostic exploration forother causes
of the symptoms than hyponatraemia (1D).
We suggest checking the serum sodium concentrationevery 4 h as
long as an intravenous infusion of 3 %hypertonic saline or
equivalent is continued (2D).
Advice for clinical practice
Prompt infusion of hypertonic saline may save lives.However,
preparing a 3 % hypertonic saline infusiontakes time and errors may
occur in calculating therequired amount of sodium chloride.
Therefore, it maybe wise for the pharmacy to store pre-prepared 150
mLbags of 3 % hypertonic saline. It ensures that solutions
Table 4 (Table 6 of the online document): diagnostic criteria
forthe syndrome of inappropriate antidiuresis
Essential criteriaEffective serum osmolality \275 mOsm/kgUrine
osmolality [100 mOsm/kg at some level of decreased
effective osmolalityClinical euvolaemiaUrine sodium
concentration[30 mmol/L with normal dietary salt
and water intakeAbsence of adrenal, thyroid, pituitary or renal
insufficiencyNo recent use of diuretic agents
Supplemental criteriaSerum uric acid \0.24 mmol/L (\4
mg/dL)Serum urea \3.6 mmol/L (\21.6 mg/dL)Failure to correct
hyponatraemia after 0.9 % saline infusionFractional sodium
excretion [0.5 %Fractional urea excretion [55 %Fractional uric acid
excretion [12 %Correction of hyponatraemia through fluid
restriction
Adapted from Schwartz et al. [36] and Janicic et al. [37]
Table 5 (Table 11 of the online document): differences
betweenSIADH and cerebral salt wasting
SIADH Cerebral salt wasting
Serum urea concentration Normallow NormalhighSerum uric acid
concentration Low LowUrine volume Normallow HighUrine sodium
concentration [30 mmol/
L[[30 mmol/L
Blood pressure Normal Normalorthostatichypotension
Central venous pressure Normal Low
Adapted from Sherlock et al. [47] and Brimioulle et al. [48]
326
-
are prepared under sterile conditions, by either thepharmacist
or the manufacturer, and are available forimmediate infusion
without having to prepare them onthe spot.
Consider using weight based (2 mL/kg) rather thanthe fixed 150
mL infusion volumes of 3 % hyper-tonic saline in case of obviously
deviant bodycomposition.
Do not expect patients with severe symptoms tocompletely recover
immediately, as it may take sometime for the brain to fully
recover. Be aware thatsometimes it may not be possible to assess
animprovement in symptoms, e.g. because the patient is
intubated and sedated. In these cases, we advise tofollow
guidance as described under 9.1.2.
Keep in mind that if hypokalaemia is present, correc-tion of the
hypokalaemia will contribute to an increasein serum sodium
concentration.
To achieve the 1 mmol/L/h increase advised in 9.1.2.1,the
formula of AdrogueMadias [32] may be used, butkeep in mind that the
actual increase may exceed thecalculated increase:
Change in serum Na infusate Na serum Na
total body water 1
7
7
7
7
7 7
7
Fig. 2 (Fig. 7 of the onlinedocument): algorithm for
themanagement of hypotonichyponatraemia (the numbers inthe yellow
boxes refer to theonline full guideline document)
327
-
Change in serum Na infusate Na infusate K serum Na
total body water 1
where [Na?] is the sodium concentration in mmol/L,[K?] is the
potassium concentration in mmol/L. Thenumerator in formula 1 is a
simplification of theexpression in formula 2, with the value
yielded by theequation in mmol/L. The estimated total body water(in
litres) is calculated as a fraction of body weight.The fraction is
0.6 in nonelderly men and 0.5 innonelderly women; and 0.5 and 0.45
in elderly menand women respectively. Normally, extracellular
andintracellular fluids account for 40 and 60 % of totalbody water
respectively.
3.2 Hyponatraemia with moderately severe symptoms
We recommend starting prompt diagnostic assessment.(1D)
Stop, if possible, medications and other factors thatcan
contribute to or provoke the hyponatraemia. (notgraded)
We recommend cause-specific treatment. (1D)
We suggest immediate treatment with a single intrave-nous
infusion of 150 mL 3 % hypertonic saline orequivalent over 20 min.
(2D)
We suggest aiming for a 5 mmol/L/24 h increase inserum sodium
concentration. (2D)
We suggest limiting the increase in serum sodium con-centration
to 10 mmol/L in the first 24 h and 8 mmol/Lduring every 24 h
thereafter, until a serum sodium con-centration of 130 mmol/L is
reached. (2D)
We suggest checking the serum sodium concentrationafter one, 6
and 12 h. (2D)
We suggest additional diagnostic exploration for othercauses of
the symptoms if the symptoms do notimprove with an increase in
serum sodium concentra-tion. (2D)
We suggest considering to manage the patient as inseverely
symptomatic hyponatraemia if the serumsodium concentration further
decreases despite treatingthe underlying diagnosis. (2D)
3.3 Acute hyponatraemia without severeor moderately severe
symptoms
Make sure that the serum sodium concentration hasbeen measured
using the same technique as used forthe previous measurement and
that no administrativeerrors in sample handling have occurred. (not
graded)
If possible, stop fluids, medications and other factorsthat can
contribute to or provoke the hyponatraemia.(not graded)
We recommend starting prompt diagnostic assessment.(1D)
We recommend cause-specific treatment. (1D)
If the acute decrease in serum sodium concentrationexceeds 10
mmol/L, we suggest a single intravenousinfusion of 150 mL 3 %
hypertonic saline or equiva-lent over 20 min. (2D)
We suggest checking the serum sodium concentrationafter 4 h,
using the same technique as used for theprevious measurement.
(2D)
3.4 Chronic hyponatraemia without severeor moderately severe
symptoms
3.4.1 General management
Stop non-essential fluids, medications and other factorsthat can
contribute to or provoke the hyponatraemia.(not graded)
We recommend cause-specific treatment. (1D)
In mild hyponatraemia, we suggest against treatmentwith the sole
aim of increasing the serum sodiumconcentration. (2C)
In moderate or profound hyponatraemia, we recommendavoiding an
increase in serum sodium concentration of[10 mmol/L during the
first 24 h and[8 mmol/L duringevery 24 h thereafter. (1D)
In moderate or profound hyponatraemia, we suggestchecking the
serum sodium concentration every 6 huntil the serum sodium
concentration has stabilisedunder stable treatment. (2D)
In case of unresolved hyponatraemia, reconsider thediagnostic
algorithm and ask for expert advice. (notgraded)
328
-
3.4.2 Patients with expanded extracellular fluid
We recommend against a treatment with the sole aimof increasing
the serum sodium concentration in mildor moderate hyponatraemia.
(1C)
We suggest fluid restriction to prevent further fluidoverload.
(2D)
We recommend against vasopressin receptor antagonists. (1C)
We recommend against demeclocycline. (1D)
3.4.3 Patients with syndrome of inappropriateantidiuresis
In moderate or profound hyponatraemia, we suggestrestricting
fluid intake as first- line treatment. (2D)
In moderate or profound hyponatraemia, we suggest thefollowing
can be considered equal second line treatments:increasing solute
intake with 0.250.50 g/kg/day of ureaor a combination of low dose
loop diuretics and oralsodium chloride. (2D)
In moderate or profound hyponatraemia, we recommendagainst
lithium or demeclocycline. (1D)
In moderate hyponatraemia, we do not recommendvasopressin
receptor antagonists. (1C)
In profound hyponatraemia, we recommend againstvasopressin
receptor antagonists. (1C)
3.4.4 Patients with contracted circulating volume
We recommend restoring extracellular volume withintravenous
infusion of 0.9 % saline or a balancedcrystalloid solution at
0.51.0 mL/kg/h. (1B)
Manage patients with haemodynamic instability in anenvironment
where close biochemical and clinicalmonitoring can be provided.
(not graded)
In case of haemodynamic instability, the need for rapidfluid
resuscitation overrides the risk of an overly rapidincrease in
serum sodium concentration. (not graded)
Advice for clinical practice
A sudden increase in urine output to[100 mL/h signalsincreased
risk of overly rapid rise in serum sodiumconcentration. If
vasopressin activity is suddenly sup-pressed, as happens when
intravascular volume isrestored in hypovolaemia, free water
clearance candramatically increase, resulting in serum sodium
con-centrations rising more rapidly than expected. If urineoutput
suddenly increases, we would advise measuringthe serum sodium
concentration every 2 h until it hasstabilised under stable
treatment. The implicit advice tomonitor urine output does not
imply we advise abladder catheter solely for this purpose. Most
patientswill be able to void spontaneously and collect urine
foroutput monitoring.
As a means of increasing solute intake, we suggestdaily intake
of 0.250.50 g/kg urea can be used. Thebitter taste can be reduced
by combining it with sweettasting substances. The pharmacist may be
asked toprepare the following as sachets: urea 10 g ? NaHCO32 g ?
citric acid 1.5 g ? sucrose 200 mg, to be dis-solved in 50100 mL
water. This will result in a morepalatable, slightly sparkling
solution.
3.5 What to do in case hyponatraemia is corrected
toorapidly?
We recommend prompt intervention for re-loweringthe serum sodium
concentration if it increases[10 mmol/L during the first 24 h or [8
mmol/L inany 24 h thereafter. (1D)
We recommend discontinuing the on-going activetreatment.
(1D)
We recommend consulting an expert to discuss if it isappropriate
to start an infusion of 10 mL/kg body weight ofelectrolyte-free
water (e.g. glucose solutions) over 1 h understrict monitoring of
urine output and fluid balance. (1D)
We recommend consulting an expert to discuss if it isappropriate
to add intravenous desmopressin 2 lg, withthe understanding that
this should not be repeated morefrequently than every 8 h. (1D)
References
1. Funk GC, Lindner G, Druml W et al(2010) Incidence and
prognosis ofdysnatremias present on ICUadmission. Intens Care
Med36:304311
2. Beukhof CM, Hoorn EJ, Lindemans J,Zietse R (2007) Novel risk
factors forhospital-acquired hyponatraemia: amatched case-control
study. ClinEndocrinol 66:367372
3. Upadhyay A, Jaber BL, Madias NE(2009) Epidemiology of
hyponatremia.Semin Nephrol 29:227238
329
-
4. Hoorn EJ, Lindemans J, Zietse R (2006)Development of severe
hyponatraemiain hospitalized patients: treatment-related risk
factors and inadequatemanagement. Nephrol Dial Transpl21:7076
5. Waikar SS, Mount DB, Curhan GC(2009) Mortality after
hospitalizationwith mild, moderate, and severehyponatremia. Am J
Med 122:857865
6. Doshi SM, Shah P, Lei X, Lahoti A,Salahudeen AK (2012)
Hyponatremiain hospitalized cancer patients and itsimpact on
clinical outcomes. Am JKidney Dis 59:222228
7. Sterns RH (1987) Severe symptomatichyponatremia: treatment
and outcome.A study of 64 cases. Ann Intern Med107:656664
8. Gill G, Huda B, Boyd A et al (2006)Characteristics and
mortality of severehyponatraemiaa hospital-based study.Clin
Endocrinol 65:246249
9. Arieff AI, Llach F, Massry SG (1976)Neurological
manifestations andmorbidity of hyponatremia: correlationwith brain
water and electrolytes.Medicine 55:121129
10. Halberthal M, Halperin ML, Bohn D(2001) Lesson of the week:
acutehyponatraemia in children admitted tohospital: retrospective
analysis offactors contributing to its developmentand resolution.
BMJ 322:780782
11. Darmon M, Diconne E, Souweine Bet al (2013) Prognostic
consequences ofborderline dysnatremia: pay attention tominimal
serum sodium change. CritCare 17:R12
12. Sakr Y, Rother S, Ferreira AMP et al(2013) Fluctuations in
serum sodiumlevel are associated with an increasedrisk of death in
surgical ICU patients.Crit Care Med 41:133142
13. Stelfox HT, Ahmed SB, Khandwala F,Zygun D, Shahpori R,
Laupland K(2008) The epidemiology of intensivecare unit-acquired
hyponatraemia andhypernatraemia in medical-surgicalintensive care
units. Crit Care 12:R162
14. Pirzada NA, Ali II (2001) Centralpontine myelinolysis. Mayo
Clin Proc76:559562
15. Arieff AI (1986) Hyponatremia,convulsions, respiratory
arrest, andpermanent brain damage after electivesurgery in healthy
women. N Engl JMed 314:15291535
16. Ayus JC, Wheeler JM, Arieff AI (1992)Postoperative
hyponatremicencephalopathy in menstruant women.Ann Intern Med
117:891897
17. Nzerue CM, Baffoe-Bonnie H, You W,Falana B, Dai S (2003)
Predictors ofoutcome in hospitalized patients withsevere
hyponatremia. J Natl Med Assoc95:335343
18. Arieff AI, Ayus JC, Fraser CL (1992)Hyponatraemia and death
or permanentbrain damage in healthy children. BMJ304:12181222
19. Verbalis JG, Drutarosky MD, Ertel RJ,Vollmer RR (1989)
Adaptive responsesto sustained volume expansion inhyponatraemic
rats. J Endocrinol122:421431
20. Verbalis JG, Gullans SR (1991)Hyponatremia causes large
sustainedreductions in brain content of multipleorganic osmolytes
in rats. Brain Res567:274282
21. Sterns RH, Silver SM (2006) Brainvolume regulation in
response to hypo-osmolality and its correction. Am J
Med119:S12S16
22. Melton JE, Patlak CS, Pettigrew KD,Cserr HF (1987) Volume
regulatoryloss of Na, Cl, and K from rat brainduring acute
hyponatremia. Am JPhysiol 252:F661F669
23. Sterns RH, Thomas DJ, Herndon RM(1989) Brain dehydration
andneurologic deterioration after rapidcorrection of hyponatremia.
Kidney Int35:6975
24. Verbalis JG, Martinez AJ (1991)Neurological and
neuropathologicalsequelae of correction of chronichyponatremia.
Kidney Int39:12741282
25. Videen JS, Michaelis T, Pinto P, RossBD (1995) Human
cerebral osmolytesduring chronic hyponatremia. A protonmagnetic
resonance spectroscopy study.J Clin Invest 95:788793
26. Hoorn EJ, Zietse R (2008)Hyponatremia revisited:
translatingphysiology to practice. Nephron Physiol108:4659
27. Hsu Y-J, Chiu J-S, Lu K-C, Chau T, LinS-H (2005) Biochemical
and etiologicalcharacteristics of acute hyponatremia inthe
emergency department. J EmergMed 29:369374
28. Sterns RH (1994) Treatinghyponatremia: why haste makes
waste.South Med J 87:12831287
29. Renneboog B, Musch W, VandemergelX, Manto MU, Decaux G
(2006)Mild chronic hyponatremia isassociated with falls,
unsteadiness, andattention deficits. Am J Med119(71):e71e78
30. Fazekas AS, Funk G-C, Klobassa DSet al (2012) Evaluation of
36formulas for calculating plasmaosmolality. Intens Care
Med39:302308
31. Adrogue HJ, Madias NE (2000)Hyponatremia. N Engl J
Med342:15811589
32. Hoorn EJ, Halperin ML, Zietse R(2005) Diagnostic approach to
a patientwith hyponatraemia: traditional versusphysiology-based
options. Q J Med98:529540
33. Chung HM, Kluge R, Schrier RW,Anderson RJ (1987)
Clinicalassessment of extracellular fluid volumein hyponatremia. Am
J Med83:905908
34. McGee S, Abernethy WB 3rd, SimelDL (1999) The rational
clinicalexamination. Is this patienthypovolemic? JAMA
281:10221029
35. Hillier TA, Abbott RD, Barrett EJ(1999) Hyponatremia:
evaluating thecorrection factor for hyperglycemia.Am J Med
106:399403
36. Schwartz WB, Bennett W, Curelop S,Bartter FC (1957) A
syndrome of renalsodium loss and hyponatremia probablyresulting
from inappropriate secretionof antidiuretic hormone. Am J
Med23:529542
37. Janicic N, Verbalis JG (2003)Evaluation and management of
hypo-osmolality in hospitalized patients.Endocrinol Metab Clin N
Am32:459481 vii
38. Aviram A, Pfau A, Czaczkes JW,Ullmann TD (1967)
Hyperosmolalitywith hyponatremia, caused byinappropriate
administration ofmannitol. Am J Med 42:648650
39. Desmond J (1970) Serum osmolalityand plasma electrolytes in
patients whodevelop dilutional hyponatremia duringtransurethral
resection. Can J Surg13:116121
40. Lindner G, Zapletal B, Schwarz C,Wisser W, Hiesmayr M,
Lassnigg A(2012) Acute hyponatremia aftercardioplegia by
histidinetryptophaneketoglutaratea retrospective study.J
Cardiothorac Surg 7:52
41. Sirken G, Raja R, Garces J, Bloom E,Fumo P (2004)
Contrast-inducedtranslocational hyponatremia andhyperkalemia in
advanced kidneydisease. Am J Kidney Dis 43:e31e35
42. Palevsky PM, Rendulic D, Diven WF(1993) Maltose-induced
hyponatremia.Ann Intern Med 118:526528
43. Oster JR, Singer I (1999)Hyponatremia, hyposmolality,
andhypotonicity: tables and fables. ArchIntern Med 159:333336
44. Lai M-Y, Lin C-C, Chung S-L, WuC-H, Yang W-C, Tseng Y-T
(2009)Milky plasma, diabetes, and severehyponatremia. Kidney Int
75:996
45. Lawn N, Wijdicks EF, Burritt MF(1998) Intravenous immune
globulinand pseudohyponatremia. N Engl J Med339:632
330
-
46. Vaswani SK, Sprague R (1993)Pseudohyponatremia in
multiplemyeloma. South Med J 86:251252
47. Sherlock M, OSullivan E, Agha A et al(2006) The incidence
andpathophysiology of hyponatraemia aftersubarachnoid haemorrhage.
ClinEndocrinol 64:250254
48. Brimioulle S, Orellana-Jimenez C,Aminian A, Vincent JL
(2008)Hyponatremia in neurological patients:cerebral salt wasting
versusinappropriate antidiuretic hormonesecretion. Intensive Care
Med34:125131
331
Clinical practice guideline on diagnosis and treatment of
hyponatraemiaAbstractIntroduction and methodologyDiagnosis of
hyponatraemiaClassification of hyponatraemiaDefinition of
hyponatraemia based on biochemical severityDefinition of
hyponatraemia based on time of developmentDefinition of
hyponatraemia based on symptoms
Confirming hypotonic and excluding non-hypotonic
hyponatraemiaWhich parameters to use for differentiating causes of
hypotonic hyponatraemia? (Fig. 1)
Treatment of hypotonic hyponatraemiaHyponatraemia with severe
symptomsFirst hour management, regardless of whether hyponatraemia
is acute or chronicFollow up management in case of improvement of
symptoms after a 5 mmol/L increase in serum sodium concentration in
the first hour, regardless of whether hyponatraemia is acute or
chronicFollow up management in case of no improvement of symptoms
after a 5 mmol/L increase in serum sodium concentration in the
first hour, regardless of whether the hyponatraemia is acute or
chronic
Hyponatraemia with moderately severe symptomsAcute hyponatraemia
without severe or moderately severe symptomsChronic hyponatraemia
without severe or moderately severe symptomsGeneral
managementPatients with expanded extracellular fluidPatients with
syndrome of inappropriate antidiuresisPatients with contracted
circulating volume
What to do in case hyponatraemia is corrected too rapidly?
References