Embed Size (px)
Citation preview

Case ReportHumoral Hypercalcemia of Malignancy witha Parathyroid Hormone-Related Peptide-Secreting IntrahepaticCholangiocarcinoma Accompanied by a Gastric Cancer
Katsushi Takeda,1 Ryosuke Kimura,1 Nobuhiro Nishigaki,2 Shinya Sato,3 Asami Okamoto,1
KumikoWatanabe,1 and Sachie Yasui1
1Department of Endocrinology andMetabolism, Nagoya CityWest Medical Center, 1-1-1 Hirate-cho, Kita-ku, Nagoya 462-8508, Japan2Department of Gastroenterology, Nagoya City West Medical Center, 1-1-1 Hirate-cho, Kita-ku, Nagoya 462-8508, Japan3Department of Experimental Pathology andTumorBiology,NagoyaCityUniversityGraduate School ofMedical Sciences, 1 Kawasumi,Mizuho-cho, Mizuho-ku, Nagoya 467-8601, Japan
Correspondence should be addressed to Katsushi Takeda; [email protected]
Received 1 December 2016; Revised 2 March 2017; Accepted 16 April 2017; Published 10 May 2017
Academic Editor: Michael P. Kane
Copyright © 2017 Katsushi Takeda et al.This is an open access article distributed under theCreativeCommonsAttribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Humoral hypercalcemia of malignancy (HHM) is caused by the oversecretion of parathyroid hormone-related peptide (PTHrP)from malignant tumors. Although any tumor may cause HHM, that induced by intrahepatic cholangiocarcinoma (ICC) or gastriccancer (GC) is rare. We report here a 74-year-old male who displayed HHMwith both ICC and GC and showed an elevated serumPTHrP level. Treatment of the hypercalcemia with saline, furosemide, elcatonin, and zoledronic acid corrected his serum calciumlevel and improved symptoms. Because treatment of ICC should precede that of GC, we chose chemotherapy with cisplatin (CDDP)and gemcitabine (GEM). Chemotherapy reduced the size of the ICC and decreased the serumPTHrP level. One year after diagnosis,the patient was alive in the face of a poor prognosis for an ICC that produced PTHrP. Immunohistochemical staining for PTHrPwas positive for the ICC and negative for the GC, leading us to believe that the cause of the HHM was a PTHrP-secreting ICC. Inconclusion, immunohistochemical staining for PTHrP may be useful in discovering the cause of HHM in the case of two cancersaccompanied by an elevated serum PHTrP level. Chemotherapy with CDDP and GEMmay be the most appropriate treatment fora PTHrP-secreting ICC.
1. Introduction
Hypercalcemia is a well-known complication of cancer asseen in the between 20 and 30 percent of cancer patients [1].Malignant-associated hypercalcemia (MAH) is classified intofour groups: humoral hypercalcemia of malignancy (HHM),local osteolytic hypercalcemia (LOH), excess 1,25(OH)
2D
secretion, and ectopic parathyroid hormone (PTH) secre-tion. HHM is associated with 80 percent of MAHs and iscaused by the effects of the oversecretion of parathyroidhormone-related peptide (PTHrP) [1–3]. Although HHMcan essentially be caused by any tumor [1], its induction bycholangiocarcinoma or gastric cancer (GC) is rare [4, 5].In addition, to date, cases of HHM complicated by two
cancers—cholangiocarcinoma and gastric cancer—have notbeen reported.
Herein, we report the first case of HHM induced by anintrahepatic cholangiocarcinoma (ICC) that secretes PTHrP,in conjunctionwith aGC identified by immunohistochemicalstaining.
2. Case Presentation
A 74-year-old male patient was admitted for hypercalcemia.Over the preceding two months he had suffered from aloss of appetite and had a history of seborrheic keratosisand hypertension. His weight was 47.4 kg, height 153.2 cm,temperature 36.6∘C, heart rate 127 beats/minute, and blood
HindawiCase Reports in EndocrinologyVolume 2017, Article ID 7012520, 6 pageshttps://doi.org/10.1155/2017/7012520

2 Case Reports in Endocrinology
pressure 143/92mmHg. He had tenderness of the righthypochondrium, but an abdominal mass was not palpable.
Laboratory analyses revealed that the patient’s correctedserum calcium level was elevated at 14.8mg/dL. Serumcarcinoembryonic antigen (CEA) and carbohydrate antigen(CA) 19-9werewithin normal range. Serum alpha fetoprotein(AFP) showed a normal level of 3.8 ng/mL.The serumPTHrPlevel was elevated at 26.6 pmol/L and the serum intact PTHlevel was low at 9 pg/mL (Table 1).
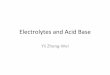
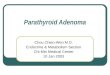
Dynamic contrast-enhanced computed tomography(CT) scans revealed a large mass, 76mm in diameter, andmultiple masses in the patient’s liver. These masses showedan enhancement of the peripheral zone in the early phase ofCT; the inside of such masses gradually became enhanced,suggesting an ICC with intrahepatic metastases (Figure 1(a)).Using fluorodeoxyglucose-positron emission tomography(FDG-PET), the patient’s liver tumor showed a SUVmax 7.1uptake value for FDG. Bone scintigraphy did not reveal anybonemetastases.Magnetic resonance imaging (MRI) showeda slightly low signal intensity on a T1-weighted image and aslightly high signal intensity on a T2-weighted image. Thesetumors showed an enhancement of the peripheral zone inthe early phase and low intake of gadolinium ethoxybenzyldiethylenetriamine pentaacetic acid- (Gd-EOB-DTPA-)enhanced MRI in the hepatobiliary phase (Figures 1(b) and1(c)). Esophagogastroduodenoscopy revealed an infiltrativeulcerative carcinoma in the anterior wall of the antrum ofthe patient’s stomach (Figure 2).
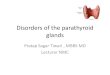
A histological examination of a biopsy specimen from thehepatic tumor revealed an ICC (Figure 3(a)). Immunohis-tochemically, ICC tumor cells were positive for cytokeratin7 and PTHrP (Figure 3(d)) and negative for cytokeratin 20,CDX2, and CA19-9. A histological examination of a biopsyspecimen from the GC revealed an adenocarcinoma (Fig-ure 3(b)). Immunohistochemically, GC tumor cells were posi-tive for cytokeratin 7, cytokeratin 20, CDX2, and CA19-9 andwere negative for PTHrP (Figure 3(e)). These findings indi-cated that this patient had two cancers, ICC and GC, and thathis HHM was induced by the oversecretion of PTHrP fromthe ICC.
After admission, the patient’s hypercalcemia was treatedwith saline, furosemide, elcatonin, and zoledronic acid. Hiscorrected serum calcium level and symptoms subsequentlyimproved.We used elcatonin only a single time on admissionand zoledronic acid five times during the five weeks afteradmission. Subsequently, his corrected calcium level was keptunder 11mg/dL without using elcatonin and bisphosphonate(Figure 4).
The patient’s prognosis was dependent on the ICC sincea prognosis for this type of cancer is generally known to bepoor and his ICCwas complicated by intrahepaticmetastasis.Therefore, we treated him with chemotherapy using cisplatin(CDDP) and gemcitabine (GEM). We started chemotherapyon the 30th day after admission, and he was dischargedon the 39th day. On the 78th day, his liver tumors werereduced (Figure 5(a)). Moreover, on the 238th day, his livertumors were smaller than tumors observed on the 78th day(Figure 5(b)). In addition, the volume of his gastric cancerwas also decreased on the 273rd day (Figure 6), suggesting
Table 1: Laboratory data on admission.
WBC 8900/𝜇LRBC 476 × 104/𝜇LHb 15.9 g/dLPLT 21.7 × 104/𝜇LTP 6.7 g/dLAlb 3.6 g/dLT-Bil. 0.6mg/dLD-Bil. 0.2mg/dLALP 515U/LGOT 64U/LGPT 26U/LLDH 190U/LAmy 57U/LCPK 27U/LUA 10.0mg/dLBUN 28.5mg/dLCRN 1.27mg/dLNa 138mmol/LK 3.8mmol/LCl 98mmol/LCa 14.4mg/dLCorrected Ca 14.8mg/dLI-P 2.8mg/dLMg 1.7mg/dLCRP 1.5mg/dLGlu 129mg/dLCEA 1.5 ng/mL (0.0∼5.0)∗
CA19-9 6.2U/mL (0.0∼37.0)∗
AFP 3.8 ng/mL (0.0∼10.0)∗
HBs antigen (—)HCV antibody (—)PTH intact 9 pg/mL (10∼65)∗
PTHrP 26.6 pmol/L (0∼1.1)∗∗Numbers in parentheses indicate the normal range; WBC: white bloodcells; RBC: red blood cells; Hb: hemoglobin; PLT: platelets; TP: totalprotein; Alb: albumin; T-Bil.: total bilirubin; D-Bil.: direct bilirubin; ALP:alkaline phosphatase; GOT: glutamic oxaloacetic transaminase; GPT: glu-tamic pyruvic transaminase; LDH: lactate dehydrogenase; Amy: amylase;CPK: creatine phosphokinase; UA: uric acid; BUN: blood urea nitrogen;CRN: creatinine; Na: sodium; K: potassium; Cl: chlorine; Ca: calcium; I-P: inorganic phosphate; Mg: magnesium; CRP: C-reactive protein; Glu:glucose; CEA: carcinoembryonic antigen; CA: carbohydrate antigen; AFP:alpha fetoprotein; HBs: hepatitis B surface; HCV: hepatitis C virus; PTH:parathyroid hormone; PTHrP: parathyroid hormone-related peptide.
that chemotherapy with CDDP and GEM was also effectivefor his gastric cancer.His serumPTHrP level had improved to4.9 pmol/L by the 101st day. A year after diagnosis, the patientwas alive.
3. Discussion
HHM is usually caused by the oversecretion of PTHrP bya malignant tumor. Typical tumors causing HHM include

Case Reports in Endocrinology 3
(a) (b) (c)
Figure 1:Dynamic contrast-enhanced computed tomography (CT) scans showedmultiplemasses in the patient’s liver, suggesting intrahepaticcholangiocarcinoma (ICC; (a), arrow). His liver tumors showed an enhancement of the peripheral zone in the early phase ((b), arrow) anda low intake in the hepatobiliary phase ((c), arrow) in a gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid- (Gd-EOB-DTPA-)enhanced magnetic resonance imaging (MRI).
Figure 2: Esophagogastroduodenoscopy revealed an infiltrativeulcerative carcinoma (arrow) in the anterior wall of the antrum ofthe patient’s stomach.
various squamous cell carcinomas, renal cancer, ovarian can-cer, endometrial cancer, human T-cell lymphotropic virus-(HTLV-) associated lymphoma and breast cancer [1]. Thesymptoms of HHM are often mild and nonspecific. Never-theless, HHM is associated with substantial mortality, withabout 50% of cancer patients who show hypercalcemia dyingwithin 30 days [2, 6]. Therefore, the early treatment of HHMand control of the serum calcium level are important.
PTHrP has been purified from a human lung cancercell line [7] and has significant sequence homology with theamino-terminal end of PTH [3, 7–9]. PTHrP is normallysynthesized by various tissues and has important physio-logical roles. For example, in cartilage PTHrP regulates itsproliferation and differentiation [10]. It is also produced inthe placenta, where it regulates the fetal serum calcium level[11]. However, it is known as a factor responsible for HHMsince it enhances the renal retention of calcium and increases
bone resorption [1]. In addition, it has also been recognized asone of the causes of adipose browning and cachexia recentlyand new treatments of PTHrP may be developed to improvethe prognosis of cancer patients in the future [12–14]
ICC accounts for 4.4 percent of primary liver cancers inJapan, so it is relatively rare [15]. ICC is frequently clinicallysilent in its early stages and is, therefore, often only diagnosedwhen it develops into an advanced cancer; this is a leadingreason for its poor prognosis.
Cholangiocarcinoma is a malignant neoplasm arisingfrom the biliary epithelium and can be anatomically classifiedinto intrahepatic, perihilar, and distal extrahepatic tumors[16]. Surgical resection is the only curative treatment forcholangiocarcinoma; however, most patients with this tumorare not operative candidates [4, 16]. Chemotherapy forcholangiocarcinoma is administered to those patients whoare not operative and results have been largely disappointing,especially for cholangiocarcinoma that produces PTHrP [4,16]. To the best of our knowledge, patients diagnosed witha PTHrP-secreting cholangiocarcinoma who lived for morethan six months have been reported in only four instances,including the present case (Table 2) [4, 17, 18]; chemotherapywas performed for each case but surgical resection was not.This suggests the possibility that chemotherapy is one ofthe effective treatments for a PTHrP-secreting cholangio-carcinoma, like a non-PTHrP-secreting cholangiocarcinoma.However, further reports are needed in order to decide thebest therapy for these types of tumors.
Immunohistochemical staining is a widely used tech-nique that demonstrates the expression and distribution ofa specific antigen by antigen-antibody immunoreaction. It isoften used not only in research, but also in clinical practice,for example, in pathological diagnosis and the determinationof molecular-targeted therapy. However, immunohistochem-ical staining for PTHrP is still uncommon.There are opinionsthat antibodies for PTHrP may be considered nonspecific.

4 Case Reports in Endocrinology
(a) (b) (c)
(d) (e) (f)
Figure 3: Histological examination of an ICC (a, d), gastric cancer (GC; (b, e)), and normal hepatocyte (c, f). Hematoxylin and eosin staining(×400) of an ICC (a), an adenocarcinoma suggesting GC (b), and normal hepatocyte (c). Immunohistochemical staining by anti-PTHrPantibody (H-137; Santa Cruz Biotechnology) in an ICC (d), GC (e), and normal hepatocyte (f).
30 60 90 120 150 180 210 240 270 300 330 360 3900Days a�er admission
Zoledronic acid 4mg
6789
10111213141516
Cor
rect
ed se
rum
Ca l
evel
(mg/
dL)
CDDP + GEM
Elcatonin 40 units
Figure 4:The corrected serumCa level was stable without bisphosphonate after the patient commenced chemotherapywith cisplatin (CDDP)and gemcitabine (GEM).
However, an antibody for PTHrP (H-137; SantaCruz Biotech-nology) is negative for normal hepatocyte which wewere ableto get whenwe performed the biopsy (Figure 3(f)), suggestingthat this antibody has the specificity for PTHrP. Therefore,our case suggests that immunohistochemical staining by an
anti-PTHrP antibody may be useful in the search for thecause of HHM in the case of two cancers accompanied byan elevated serum PTHrP level. Because of an aging society,the occurrence of two cancers together is no longer rare.Therefore, the incidence of HHM with two cancers is also

Case Reports in Endocrinology 5
(a) (b)
Figure 5: CT scans showed that the patient’s liver tumors (arrows) were reduced by the 78th (a) and 238th day (b) of admission afterchemotherapy with CDDP and GEM.
Table 2: Reported cases of cholangiocarcinoma secreting PTHrP who are alive for more than half a year.
Number Authors Age Reportedyear Sex Ca
level PTHrP Therapy Prognosis
(1) Davis et al. [17] 54 1994 Male 16.4 5.2 FUDR + 5-FU Survival (for 6 months)
(2) Yamada et al. [4] 43 2009 Male 14.4 5.0 TAE + PTPE + GEM + S-1 +Radiation Died (after 14 months)
(3) Lim et al. [18] 63 2013 Male �12.1 n6.7 CAP + CDDP + Radiation,second-line GEM
Died (after almost 1year)
(4) Our case 74 2016 Male �14.8 26.6 CDDP + GEM Survival (after 1 year)FUDR: floxuridine; 5-FU: 5-fluorouracil; GEM: gemcitabine; CAP: capecitabine; CDDP: cisplatin; TAE: transcatheter arterial embolization; PTPE:percutaneous transhepatic portal embolization; nPTHrP reported by Lim et al. was measured 9 months after an ICC diagnosis; �Ca level means corrected Ca.
Figure 6: Esophagogastroduodenoscopy showed that the patient’sgastric cancer (arrow) was reduced on the 273rd day.
expected to increase. The identification of a cancer secretingPTHrP by using immunohistochemical staining will allowthe correct prediction of fluctuation of serum calcium level.
In conclusion, we have reported the first case of a patientwith a PTHrP-secreting ICC accompanied by GC.
Disclosure
An earlier version of this manuscript was presented as aposter presentation at the 89th annual meeting of the JapanEndocrine Society (April, 2016).
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper.
References
[1] A. F. Stewart, “Hypercalcemia associated with cancer,”The NewEngland Journal of Medicine, vol. 352, no. 4, pp. 373–379, 2005.
[2] J. D. Wright, A. I. Tergas, C. V. Ananth et al., “Quality andOutcomes of Treatment of Hypercalcemia of Malignancy,”Cancer Investigation, vol. 33, no. 8, pp. 331–339, 2015.
[3] K. Nakajima, M. Tamai, S. Okaniwa et al., “Humoral hypercal-cemia associated with gastric carcinoma secreting parathyroidhormone: a case report and review of the literature,” EndocrineJournal, vol. 60, no. 5, pp. 557–562, 2013.
[4] M. Yamada, H. Shiroeda, S. Shiroeda, K. Sato, T. Arisawa,andM. Tsutsumi, “Cholangiocarcinoma producing parathyroid

6 Case Reports in Endocrinology
hormone-related peptide treated with chemoradiation usinggemcitabine and S-1,” Internal Medicine, vol. 48, no. 24, pp.2097–2100, 2009.
[5] C. Iino, T. Shimoyama, Y. Akemoto et al., “Humoral hypercal-cemia due to gastric carcinoma secreting parathyroid hormone-related protein during chemotherapy: a case report,” ClinicalJournal of Gastroenterology, vol. 9, no. 2, pp. 68–72, 2016.
[6] S. H. Ralston, S. J. Gallacher, U. Patel, J. Campbell, and I.T. Boyle, “Cancer-associated hypercalcemia: morbidity andmortality—clinical experience in 126 treated patients,” Annalsof Internal Medicine, vol. 112, no. 7, pp. 499–504, 1990.
[7] J.M.Moseley,M. Kubota, H. Diefenbach-Jagger et al., “Parathy-roid hormone-related protein purified from a human lungcancer cell line,” Proceedings of the National Academy of Sciencesof the United States of America, vol. 84, no. 14, pp. 5048–5052,1987.
[8] L. J. Suva, G. A. Winslow, R. E. H. Wettenhall et al., “Aparathyroid hormone-related protein implicated in malignanthypercalcemia: cloning and expression,” Science, vol. 237, no.4817, pp. 893–896, 1987.
[9] A. E. Broadus, M. Mangin, K. Ikeda et al., “Humoral hypercal-cemia of cancer: identification of a novel parathyroid hormone-like peptide,”TheNew England Journal of Medicine, vol. 319, no.9, pp. 556–563, 1988.
[10] A. C. Karaplis, A. Luz, J. Glowacki et al., “Lethal skeletaldysplasia from targeted disruption of the parathyroid hormone-related peptide gene,” Genes and Development, vol. 8, no. 3, pp.277–289, 1994.
[11] C. P. Rodda, M. Kubota, J. A. Heath et al., “Evidence for a novelparathyroid hormone-related protein in fetal lamb parathyroidglands and sheep placenta: comparisons with a similar proteinimplicated in humoral hypercalcaemia of malignancy,” Journalof Endocrinology, vol. 117, no. 2, pp. 261–271, 1988.
[12] S. Kir andB.M. Spiegelman, “Cachexia and brown fat: a burningissue in cancer,”Trends in Cancer, vol. 2, no. 9, pp. 461–463, 2016.
[13] S. Kir, J. P. White, S. Kleiner et al., “Tumour-derived PTH-related protein triggers adipose tissue browning and cancercachexia,” Nature, vol. 513, no. 7516, pp. 100–104, 2014.
[14] A. R. Guntur, C. R. Doucette, and C. J. Rosen, “PTHrp comesfull circle in cancer biology,” BoneKEy Reports, vol. 4, no. 621,2015.
[15] M. Kudo, N. Izumi, T. Ichida et al., “Report of the 19th follow-upsurvey of primary liver cancer in Japan,” Hepatology Research,vol. 46, no. 5, pp. 372–390, 2016.
[16] M. J. Olnes and R. Erlich, “A review and update on cholangio-carcinoma,” Oncology, vol. 66, no. 3, pp. 167–179, 2004.
[17] J. M. Davis, R. Sadasivan, T. Dwyer, and P. V. Veldhuizen, “Casereport: cholangiocarcinoma and hypercalcemia,”The AmericanJournal of theMedical Sciences, vol. 307, no. 5, pp. 350–352, 1994.
[18] S. Lim, J. Han, K. H. Park et al., “Two cases of humoral hyper-calcemia of malignancy in metastatic cholangiocarcinoma,”Cancer Research and Treatment, vol. 45, no. 2, pp. 145–149, 2013.

Submit your manuscripts athttps://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com