Embed Size (px)
Citation preview

The Need to Consider Renal Health in
Transfusion Care and Research to Inform
Best Practice
Shahid Muhammad
Specialist Biomedical Scientist
Wednesday 01st February 2017
Leadership & Management

Presentation Structure • Introduction
• Objectives - Aims/ Justifications
• What is Chronic Kidney Disease (CKD)
• Clinical Factors and the Decision to Transfuse
• Strategies for Transfusion Therapy
• Assessment of Viral Hepatitis in Renal Patients/ Solid Organ Transplantation
(Table 1)
• Transfusion Risks
• Transfusion Alternatives
• Transfusion Research
• Literature Review - Design/Methods
• Literature Review – Grouping of Terms (Table 2)
• Literature Review – Explicit Number of Papers Identified via PubMed (Table 3)
• Literature Review – No. of Papers Identified via PubMed and EBSOC Host
(Table 4)
• Literature Review - Themes Derived
• Literature Review - Findings
• Concepts of Leadership and Management in Transfusion/ Care Practices
• Further Research & Interventions
• Discussion
• Conclusion
• Summary Points
• Final Message
• References
• An estimated 15 million patients in England have at least one Long-Term Condition (LTC)
or Chronic Illness (CI) (1).
• The numbers of patients with multiple LTCs/ CIs are set to rise from 1.9 million in 2008 to
2.9 million in 2018 (1).
• Already 30% of the population with LTCs/ CIs account for 70% of NHS spending (1).
• Patients with LTCs/ CIs like Chronic Kidney Disease (CKD) who have potential associated
anaemia are prescribed Erythropoiesis-Stimulating Agents (ESAs) like Erythropoietin (or
EPO) – but if in ‘crisis’ may require Red Blood Cell Transfusions (RBTs); and some cannot
receive RBTs or may refuse (because of history of antibodies or co-morbidities – thus
become 'untransfusable' patients) (2).
• There are no universally accepted treatment guidelines for managing transfusion care in
patients with LTCs/ CIs, and practice differs between hospitals, regions, and countries (2).
• There is ever more need to consider the renal health of patients who require ongoing care/
treatment, especially where renal insufficiency is evident/ can compromise the synthesis of
the hormone EPO (2).
• In addition renal health is/ should also be an important consideration for transfusion
research practices.
Introduction

Objectives – Aims/ Justifications Objectives
1) To highlight the need to consider renal health in transfusion care and
research to inform best practice and
2) To provide context of Leadership and Management in transfusion
care/ practices
Aims/ Justifications
1) To understand what further aspects of care are required for patients
with LTCs/ CIs
2) To highlight what specific practices would help in the development of
transfusion care guidelines and
3) To provide a further understanding of treatment alternatives taking
into consideration renal insufficiency from a leadership/ management
stance

• Chronic Kidney Disease (CKD) is an LTC/ CI that can be summated as
the steady and consistent reduction in renal function over time.
• Primarily in the disease development, patients with CKD will have no
identifiable symptoms and it is thus largely a silent disease and this
has been the case for many years – CKD is an under-diagnosed CI
(1,3).
• Even in the absent of indicators, CKD adds significant burden on
cardiovascular health and can cause death acutely or over time owing
to its clinical manifestations (1,3).
• CKD is thus now increasingly being recognized as a global public
health problem and a key determinant of poor health outcomes (4,5).
• With CKD prevalence steadily increasing, scientists with clinical teams
in haematology/ transfusion and biochemistry now need to consider
further, renal health of all patients with LTCs/ CIs where RBT may be
warranted to achieve best practice.
Background
What is Chronic Kidney Disease (CKD)?
Clinical Factors and the Decision to Transfuse • Recommendations regarding optimal Hb levels in patients with LTC/ CIs like
CKD continuously evolve, and results from randomized controlled trials
(RCTs) of corrective strategies continue to be impartial (6).
• Although partial anaemia correction with EPO-stimulating formulations
provide various advantages to normalize Hb levels, there may be higher
probabilities of cardiovascular events and cancer risk (6).
• There is general agreement that RBTs are not typically indicated for Hb levels
of ≥ 100 g/L and transfusion should be considered when Hb is ≤ 70 to 80 g/L
depending on patient characteristics (7).
• As more studies (particularly RCTs) addressing RBTs are published, it will
become increasingly transparent that leaders and managers will need to
assess outcomes that may expose patients to unnecessary risks (7-8).
• The clinical importance of the RBCs storage lesion (i.e. the time-dependent
metabolic, biochemical, and molecular changes that stored cells undergo) is
still lacking. RBCs can be filtered, washed, frozen, or irradiated for specific
conditions/ indications.
Strategies for Transfusion Therapy
• A restrictive transfusion strategy is recommended for patients with
pre-existing CVD (9), and similar transfusion strategies need to be
extended in patients who are at risk of renal insufficiency and the
post renal transplant population.
• In pre-existing CVD patients, transfusion is considered when Hb
levels are ≤ 80 g/L or for symptoms such as chest pain, orthostatic
hypotension, tachycardia unresponsive to fluid resuscitation, or
congestive heart failure (9).
• This weak recommendation is based on moderate-quality evidence
due to limited clinical trial data directly addressing this population of
patients.
• Additional clinical practice guidelines exist but do not factor in
strategies for patients with renal insufficiency, more generally.

Guidelines and Frameworks
• Patients with a CKD as a co-morbidity should have their Hb
assessed (10).
• Having familiarity with the National Institute for Clinical Excellence
(NICE) (10) definitions of renal anaemia (i.e. using a threshold of
110g/L to define anaemia and the need for treatment thereof) used in
CKD and cross-reference with guidelines used by the European Best
Practice Guidelines (11) and Kidney Disease Outcomes Quality
Initiative (KDOQI) (12) is important.
• Leaders and Managers need to continue reviewing guidelines to
ensure that practices are rounded; patients with stage 3b CKD and
have Hb < 110g/L should be tested for anaemia.
• The mean Hb declines as renal function reduces in subsequent
stages of CKD and this is when anaemia then catches up with
additional clinical symptoms.
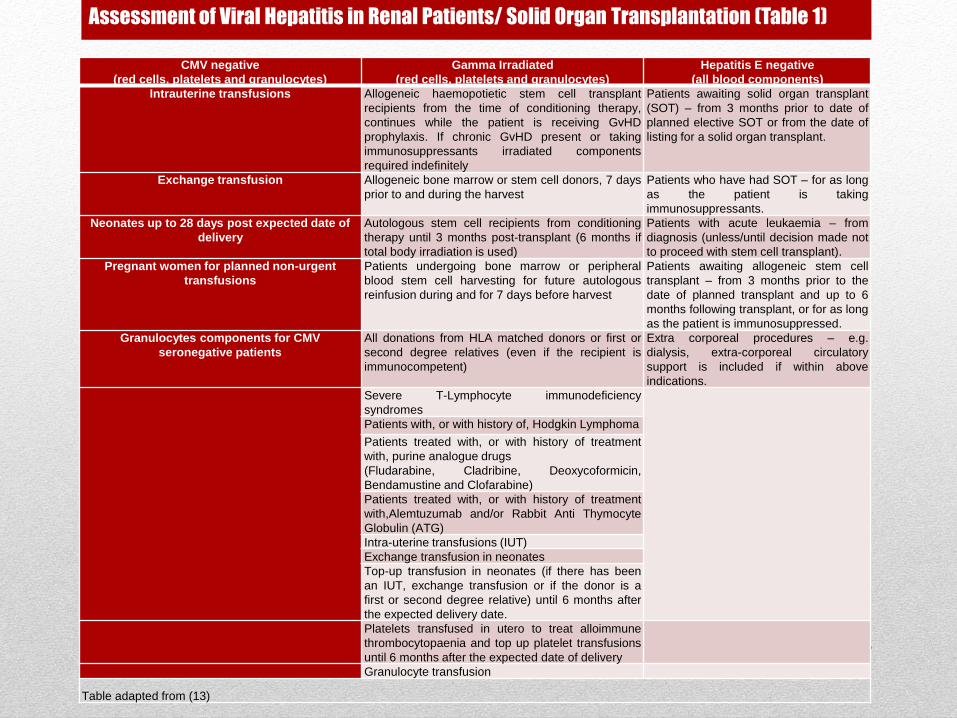
Assessment of Viral Hepatitis in Renal Patients/ Solid Organ Transplantation (Table 1)
CMV negative
(red cells, platelets and granulocytes)
Gamma Irradiated
(red cells, platelets and granulocytes)
Hepatitis E negative
(all blood components)
Intrauterine transfusions Allogeneic haemopotietic stem cell transplant
recipients from the time of conditioning therapy,
continues while the patient is receiving GvHD
prophylaxis. If chronic GvHD present or taking
immunosuppressants irradiated components
required indefinitely
Patients awaiting solid organ transplant
(SOT) – from 3 months prior to date of
planned elective SOT or from the date of
listing for a solid organ transplant.
Exchange transfusion Allogeneic bone marrow or stem cell donors, 7 days
prior to and during the harvest
Patients who have had SOT – for as long
as the patient is taking
immunosuppressants.
Neonates up to 28 days post expected date of
delivery
Autologous stem cell recipients from conditioning
therapy until 3 months post-transplant (6 months if
total body irradiation is used)
Patients with acute leukaemia – from
diagnosis (unless/until decision made not
to proceed with stem cell transplant).
Pregnant women for planned non-urgent
transfusions
Patients undergoing bone marrow or peripheral
blood stem cell harvesting for future autologous
reinfusion during and for 7 days before harvest
Patients awaiting allogeneic stem cell
transplant – from 3 months prior to the
date of planned transplant and up to 6
months following transplant, or for as long
as the patient is immunosuppressed.
Granulocytes components for CMV
seronegative patients
All donations from HLA matched donors or first or
second degree relatives (even if the recipient is
immunocompetent)
Extra corporeal procedures – e.g.
dialysis, extra-corporeal circulatory
support is included if within above
indications.
Severe T-Lymphocyte immunodeficiency
syndromes
Patients with, or with history of, Hodgkin Lymphoma
Patients treated with, or with history of treatment
with, purine analogue drugs
(Fludarabine, Cladribine, Deoxycoformicin,
Bendamustine and Clofarabine)
Patients treated with, or with history of treatment
with,Alemtuzumab and/or Rabbit Anti Thymocyte
Globulin (ATG)
Intra-uterine transfusions (IUT)
Exchange transfusion in neonates
Top-up transfusion in neonates (if there has been
an IUT, exchange transfusion or if the donor is a
first or second degree relative) until 6 months after
the expected delivery date.
Platelets transfused in utero to treat alloimmune
thrombocytopaenia and top up platelet transfusions
until 6 months after the expected date of delivery
Granulocyte transfusion
Table adapted from (13)
Transfusion Risks
• Results of a study by (Wardrop et al. 2013) elaborating on research
by (15) exploring Aprotinin (a powerful anti-fibrinolytic) in patients
undergoing heart surgery (14).
• In this observational study, 4374 patients undergoing Coronary Artery
Bypass Graft (CABG) surgery, showed doubling of the risk of renal
failure requiring HD, having an MI, or heart failure (P <0.001) and a
181% increase in the risk of stroke or encephalopathy (P=0.001)
when Aprotinin was used compared with the lysine analogues to
prevent bleeding (14).
• Evidence available for the use of anti-fibrinolytics in haematology
patients is still limited and how they may potentially have an impact
on renal function over time has not been explored (14-15).

Transfusion Alternatives
• PBM represents an international initiative in best practice of transfusion
medicine and this policy has incorporated the key objectives of the PBM
conference: ‘The Future of Blood Transfusion’, June 2012, hosted by the
Department of Health (DH), the National Blood Transfusion Committee
(NBTC) and the NHS Blood and Transplant (NHSBT) (13).
• Autologous blood donation and EPO-based pharmacological stimulating
agents are efficacious in the pre-operative period. Intraoperatively, acute
normo-volaemic haemodilution, cell salvage, anti-fibrinolytics, specific
anaesthetic and surgical techniques, coagulation monitoring, acceptance of
minimal Hb values and artificial oxygen carriers can reduce the need for RBTs
(16).
• Alternatives to RBTs should be given strong consideration, however focused
evaluations of specific LTC/ CI patient populations and alternatives will help to
clarify best use of treatment options (17) taking into account renal function
(18-22).
Transfusion Research
• NHSBT is going to try to provide, as much as is possible,
‘bespoke’ RBTs for those who have already produced
antibodies, and to prevent those who have not from producing
antibodies in the first instance (23).
• Patients who have an LTC/ CI with potentially compromised
renal function, discussions and decisions need to be had as
to whether to transfuse or not should be envisaged with
alternative treatment modalities providing similar efficacy.
• Leaders and Managers should become more aware specific
disease states in different ethnicities to help inform routine
practices.

Literature Review - Design/ Methods
Four hundred and fifty (450) abstracts were identified between
1977-2015 (or over 38 years).
Two-hundred and seventy four (274) papers were cross-
examined using a Critical Appraisal Skills Programme (CASP
2015) and after removal of duplications, eighty-two (82) papers
were evaluated to:
1. Understand what aspects of care are required more
consideration for patients with LTCs/ CIs.
2. Understand what specific practices would help in the
development of transfusion care guidelines and
3. Provide an understanding of present indications for RBTs.

Blood Renal Leadership/ Management
Blood Transfusion Disease Leadership
Red Blood Cells Chronic Management
Blood Replacement Illness Framework
Erythropoietin Renal Guidelines
Haemoglobin Long-Term Best Practice
Anaemia Surgery Research
Haemorrhage Healthcare
Intervention Medication
Pharmacotherapy Condition
Literature Review –
General Grouping of Terms through PubMed & EBSCO Host
Database (Table 2)

Literature Review –
Explicit Number of Papers Identified through Pubmed (Table 3) Blood Renal Leadership/ Management
Basic search
A combination of Blood terms
(as listed in table 2)
This retrieved 48 articles
(1977-2015)
Basic search
A combination of renal terms inserted
(as listed in table 2)
This retrieved 24 articles
(1989-2015)
Basic search
A combination of challenges terms inserted (as
listed in table 2)
This retrieved 291 papers
(1977-2015)
Advanced search
Inserting all the words
(see table 2)
Selecting, title/ abstract, and OR search
option
This retrieved 28 articles
(1977-2015)
Advanced search
Inserting all the words
(see table 2)
Selecting, title/ abstract, and OR search option
This revealed 24 articles
(1989-2015)
Advanced search
Inserting all the words
(see table 2)
Selecting, title/ abstract, and OR search option
This revealed 388 papers
(1977-2015)
Refined search
Highlighted:
Adults
OR Search
English
Humans
Title/Abstracts
Medline and PubMed Central subsets
were also marked
This retrieved 20 articles
(1977-2015)
Refined search
Highlighted:
Adults
OR Search
English
Humans
Title/Abstracts
Medline and PubMed Central subsets were also
marked
This retrieved 22 articles
(1989-2015)
Refined search
Highlighted:
Adults
OR Search
English
Humans
Title/Abstracts
Medline and PubMed Central subsets were also
marked
This retrieved 98 abstracts
(1989-2015)

Literature Review – Number of Papers Identified through
both PubMed and EBSCO Host (Table 4)
Theme Papers
Theme 1
Lack of Renal Health in Transfusion Care Strategies
for Patients with LTCs/ CIs
(Carpenter 1990;Collins et al. 2014;Corry et al. 1980;Corwin et al. 1987;Corwin
2011;Corwin and Bonventre 1986;Drueke et al. 2006;Eschbach, Jr. et al.
1967;Eschbach et al. 1970;Eschbach et al. 1987;Eschbach 1994;Eschbach
2000;Eschbach 2002;Eschbach and Adamson 1985;Karkouti 2012;Macdougall and
Obrador 2013;Napolitano et al. 1999;Opelz et al. 1997;Opelz and Terasaki
1978;Whitman et al. 2013)
Theme 2
Managing Anaemia in the Chronically Ill’/
‘Untransfusable’ Patient
(Bargman 1991;Beliaev et al. 2012;Charles et al. 2006;Corwin et al.
1995;Gilbertson et al. 2013;Hebert et al. 1995;Hebert 1998;Heh-Foster et al.
2014;Karkouti et al. 2005;Karkouti et al. 2006;Karkouti et al. 2007;Karkouti et al.
2015;Karkouti and Dattilo 2006; Melmed et al. 2009;Napolitano 2004;Napolitano
2005;Shander 2004;Sherman et al. 1988;Surgenor et al. 2001)
Theme 3
Alternatives and Indications to RBTs
(Ball and Winstead 2008;Bargman 1991;Charles et al. 2006;Corwin et al.
1995;Corwin et al. 2014;Corwin and Napolitano 2014;Drews 2003;Hebert et al.
1999;Karkouti et al. 2003;Ladas et al. 2004;Lorentzen et al. 2013;Macdougall and
Obrador 2013;Madjdpour et al. 2006;Napolitano 2005;Spahn 1999;Spahn
2004;Spahn and Casutt 2000;Spence and Atabek 1994;Whitman et al. 2013)
Theme 4
The Importance of Research in Leadership and
Management to Inform Best Practice
(Blajchman and Hebert 2001;Carson 2005;Carson and Armas-Loughran
2003;Carson and Patel 2014;Corwin 1999;Corwin et al. 2003;Corwin 2005;Corwin
and Carson 2007;Goodnough and Shander 2007; Eschbach, J.W. & Adamson,
J.W. 1989;Hardy 2003;Hebert and Fergusson 2002;Karkouti et al. 2003;Klein et
al.2007;Klein et al.2015; Murphy et al. 2001; Murphy and Goodnough
2015;Napolitano et al. 1999;Napolitano 2005;Napolitano and Corwin
2004a;Napolitano and Corwin 2004b;Spahn 2004;Spahn and Casutt 2000;Spahn
and Marcucci 2004)

Literature Review - Themes Derived The themes this work uncovered include:
1) ‘Lack of Renal Health in Transfusion Care Strategies for
Patients with Chronic Illnesses’.
(20 papers)
2) ‘Managing Anaemia in the Chronically Ill’/ ‘Untransfusable’
Patient’.
(24 papers)
3) ‘Alternatives and Indications to RBTs’
(19 papers)
4) ‘The Importance of Research in Leadership and
Management to Inform Best Practice’.
(19 papers)

Literature Review - Findings Four issues were swiftly recognized
1) There were only three papers that explored RBTs and considered
renal insufficiency before 1978.
2) There have not been formal care plans to safeguard RBT requests
in the LTCs/ CI patient population for the longer term (until more
recently).
3) The alternatives and indications for RBTs in patients with a LTC/ CI
are still somewhat inconsistent universally and this makes
practices difficult to standardize.
4) There has been limited emphasis on the importance of research in
leadership and management to inform best practices.

Concepts of Leadership and Management in Transfusion/
Care Practices
• No universally accepted definitions or theories of leadership or management
actually exists.
• Scientists looking to develop their aptitudes in a specific area of practice,
there now needs to be more clarity of definitions and differentiate between
biomedical leaders and biomedical managers.
• Leadership (perhaps more so than management) is also knowing when and
how patients may benefit with alternative treatments or treatment pathways;
this also means there needs to be good examples in practice so colleagues
can gain first hand of what works and what doesn’t and this all links to
evidence-based practice.
• Scientists are needed who consider renal health more intricately in
transfusion care through research to inform best practice.

• There is still quite a gap in research and this mainly focuses on patient
management in the short-term. The question is then what should be
done better?
• This is a question that can only really be answered by conducting more
longitudinal studies that look to compare different forms of treatment
alternatives over time.
• Future research must also consult renal guidelines and the Renal
Registry (RR)/ Renal Association (RA) would be a first port of call for
Biomedical Scientists to gain more knowledge relating to what formally
constitutes renal insufficiency.
Further Research & Interventions
Discussion
• Obviously if a patient with an LTC/ CI requires an RBT and there is
no other way to treat them, then that pathway should be taken.
• However, in practice, scientists should be having tighter discussions
with medical colleagues so that they too are aware of advantages
and disadvantages in the more intricate ‘nature’ of RBTs, being more
on the forefront of practice.
• Scientists are ‘in the game’ of saving and sustaining lives – they
should not be supporting care where lives are potentially being
further compromised.

Leadership, Management and Research relating to renal health in transfusion practices are
intricate.
Biomedical Scientists with transfusion care expertise are needed where an in-depth insight on
the importance of understanding renal health and sensitivity of laboratory tests are concerned.
If transfusion services are to be effective, scientists need to Take Ownership to ensure safe
and quality assured practices. This will help to bridge gaps in transfusion practices and the
future care of patients with LTCs/ CIs.
National Blood Transfusion Committee (2014) informs: ‘Transfuse one dose of blood
component at a time, (e.g. one unit of RBTs or platelets, in non-bleeding patients and
reassess patient clinically and with further blood count to determine if further transfusion is
needed)’ and so nationally centres are now moving toward a single unit transfusion policy in 1)
keeping with PBM and 2) to reduce inappropriate RBTs (24).
Research integrated with practice is important to achieve best care/ practice, especially in
those who have/ at risk of renal insufficiency.
Conclusion – Taking Ownership!

• Frameworks/ guidelines for scientists proceeding with a RBT request, especially with regard to patients with an
LTC/ CI, are getting better.
• Literature and research practices in transfusion care need to factor in renal health more substantially so that
discourse can be re-iterated as to whether a patient ‘really needs’ to be transfused. This also means that other
forms of replacement therapies and treatments should be tried and tested.
• More research is needed to help inform whether patients who are suspect for renal insufficiency should be
provided alternative forms of therapy that may 1) support them in the longer term and 2) identify any particular
predisposition/s before a RBT is considered because a number of suspect renal insufficient patients who
receive long-term transfusions will develop allo-and/ or autoantibodies. This is going to be an issue in an ageing
population.
• Again, longitudinal studies are required to better appreciate whether there is any advantage of RBTs vs.
different EPO formulations in clinical practice with a view to assess a strategy for phenotyping and matching
patients with suspect renal insufficiency.
• A cross-sectional study would initially be helpful to understand/ appreciate how transfusion research practices
could be improved with awareness and educating medical/ clinical teams, especially those supporting the care
of patients with LTCs/ CIs, ‘untransfusable’ patients and indeed those who refuse treatment.
• There is still a need to consider renal health in transfusion care and research practices to ensure effective and
best practices are achieved across health spheres for patients with LTCs/ CIs.
• The complexity of care plans should highlight the importance of better integration across laboratory practices
and medicine in order to achieve formal consensus and help form robust guidelines.
Summary Points

Final Message………….. “Biomedical science professionals are encouraged, and have a
professional responsibility, to offer advice and expertise to
individuals, teams, committees or working groups where their
input can contribute positively to a service or project outcome”
Ref: Institute of Biomedical Sciences, Good Professional Practice - Benchmark Series (IBMS, 2015)
References 1. Department of Health (2012), Long Term Conditions Compendium of Information, 3rd ed. London: Department of Health. (Available at
www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_134486.pdf) (accessed June 2015)
2. Hebert, P.C., Wells, G., Blajchman, M.A., Marshall, J., Martin, C., Pagliarello, G., Tweeddale, M., Schweitzer, I., & Yetisir, E. (1999). A
multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care
Investigators, Canadian Critical Care Trials Group. N.Engl.J.Med., 340, (6) 409-417
3. World Health Organization (2005). Preventing chronic diseases: a vital statement. Switzerland: World Health Organization.
(www.who.int/chp/chronic_disease_report/en/) (accessed March 2015)
4. Aviles-Gomez, R., Luquin-Arellano, V.H., Garcia-Garcia, G., Ibarra-Hernandez, M., & Briseno-Renteria, G. (2006). Is renal replacement therapy
for all possible in developing countries? Ethn.Dis., 16, (2 Suppl 2) S2
5. Garcia-Garcia, G. and Jha, V. (2014). Chronic kidney disease in disadvantaged populations. Pediatr.Nephrol.
6. Bargman, J.M. (1991). Erythropoietin: a hormone finds a purpose. J.Rheumatol., 18, (8) 1121-1123
7. Dunbar, N.M. & Szczepiorkowski, Z.M. (2015). How do we utilize a transfusion safety officer? Transfusion
8. Beliaev, A.M., Marshall, R.J., Smith, W., & Windsor, J.A. (2012). Mortality risk stratification in severely anaemic Jehovah's Witness patients.
Intern.Med.J., 42, (3) e1-e3
9. Macdougall, I.C. & Obrador, G.T. (2013). How important is transfusion avoidance in 2013? Nephrol.Dial.Transplant., 28, (5) 1092-1099
10. Anaemia management in chronic kidney disease (2011). NICE Clinical Guideline 39: (available at http://www.nice.org.uk/Guidance/CG39)
(accessed June 2015)
11. Locatelli F, Aljama P, Ba´ra´ny P et al (2004). Revised European best practice guidelines for the management of anaemia in patients with chronic
renal failure. Nephrol Dial Transpl; 19 (Suppl 2): 1–47
12. KDOQI Clinical practice guidelines and clinical practice recommendations for anaemia in chronic kidney disease (2006). Am J Kidney Dis; 47:
S1–S145
13. The Royal Devon and Exeter (RD&E) policy for the requirement of CMV negative, Irradiated and HEV negative blood components (2016). Blood
Transfusion Guidelines, Edition 3, 25/04/2016
14. Wardrop, D., Estcourt, L.J., Brunskill, S.J., Doree, C., Trivella, M., Stanworth, S., & Murphy, M.F. (2013). Antifibrinolytics (lysine analogues) for
the prevention of bleeding in patients with haematological disorders. Cochrane.Database.Syst.Rev., 7, CD009733
15. Lien, M. & Milbrandt, E.B. (2006). A disheartening story: aprotinin in cardiac surgery. Crit Care, 10, (6) 317
16. Goodnough, L.T. & Shander, A. (2007). Blood management. Arch.Pathol.Lab Med., 131, (5) 695-701
17. The Joint UKBTS Professional Advisory Committee (JPAC) (2011) (available at http://www.transfusionguidelines.org.uk/) (accessed June 2015)
18. Blajchman, M.A. (2000). Reducing the risk of bacterial contamination of cellular blood components. Dev.Biol.(Basel), 102, 183-193
19. Blajchman, M.A. & Hebert, P.C. (2001). Red blood cell transfusion strategies. Transfus.Clin.Biol., 8, (3) 207-210
20. Spahn, D.R. (1999). Blood substitutes. Crit Care, 3, (5) R91-R92
21. Spahn, D.R. (2004). Strategies for transfusion therapy. Best.Pract.Res.Clin.Anaesthesiol., 18, (4) 661-673
22. Spahn, D.R. & Casutt, M. (2000). Eliminating blood transfusions: new aspects and perspectives. Anesthesiology, 93, (1) 242-255
23. The Institute of Biomedical Sciences (IBMS) Congress (2015), Transfusion Notes
24. National Blood Transfusion Committee (2014) Patient Blood Management, An evidence-based approach to patient care. (available at
http://www.transfusionguidelines.org/uk-transfusion-committees/national-blood-transfusion-committee/patient-blood-management) (Accessed
February 2016)

Questions – Thank you





























