Embed Size (px)
Citation preview
Diez años de avances en el tratamiento del cáncer de cabeza y cuello
Incorporación de la inmunoterapia a la estrategia de
tratamiento del cáncer de cabeza y cuello.
Ricard Mesía Instituto Catalán de Oncología - Badalona
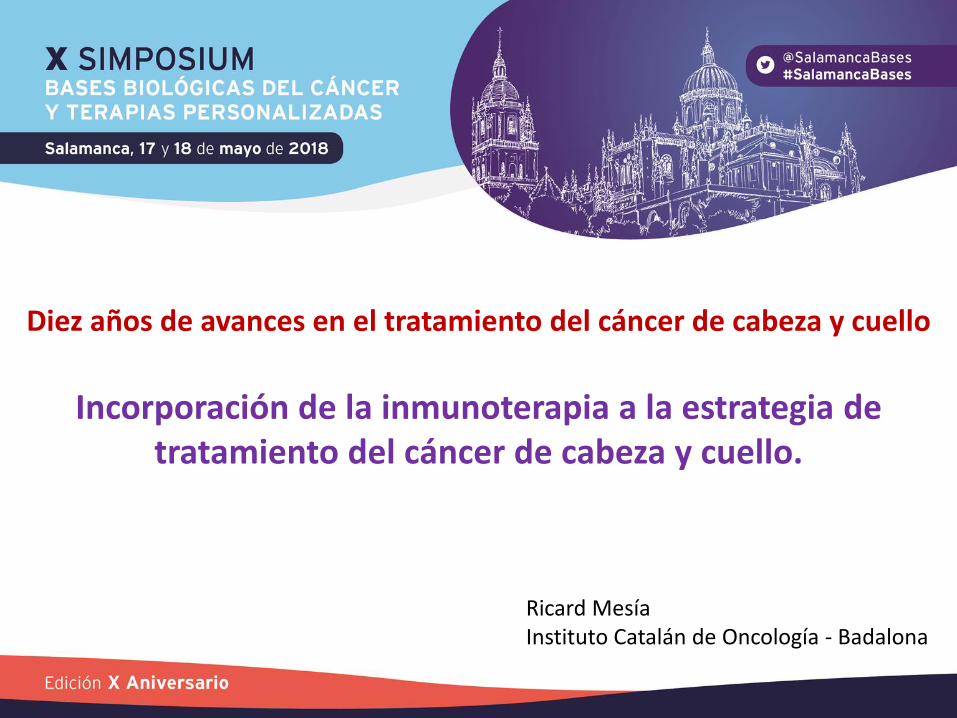
SCCHN tiene microambiente “inflamatorio”
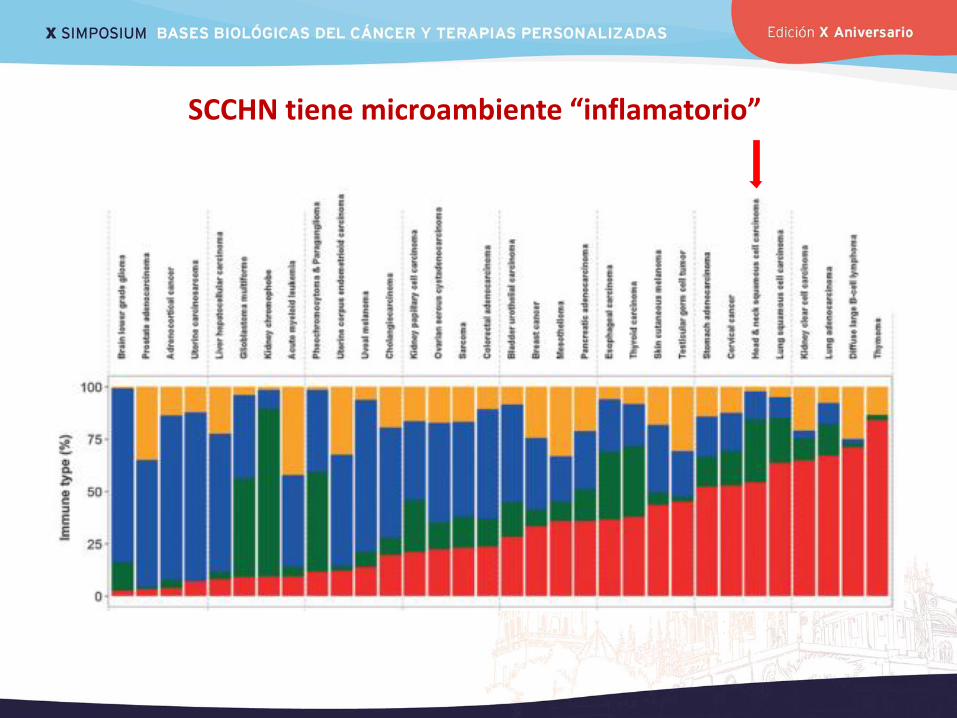
Standard of care in R/M disease
• Taxane ± platin
• Cetuximab* ± taxane
• Methotrexate
<10% 2nd line 80%
Cetuximab + platinum-based CT
Erbitax (No P candidates;
PS 2)
Cetuximab maintenance
until PD
1st line
RR: 35-40% Median SV: 10 mo
RR: <10% Median SV: 3-5 mo
3rd line
• Individualise
(slow PROG // previous RR)
• Methotrexate
RR: Anecdotic Median SV: ??
Checkmate 141
Más de 100 hospitales van a indicar tratamientos sin experiencia Existe formación en manejo de afectos adversos, en los resultados del estudio Checkmate 141, pero no en indicación del tratamiento en la práctica clínica
< 15 de los 120 hospitales del TTCC tienen experiencia en ICI - CCC
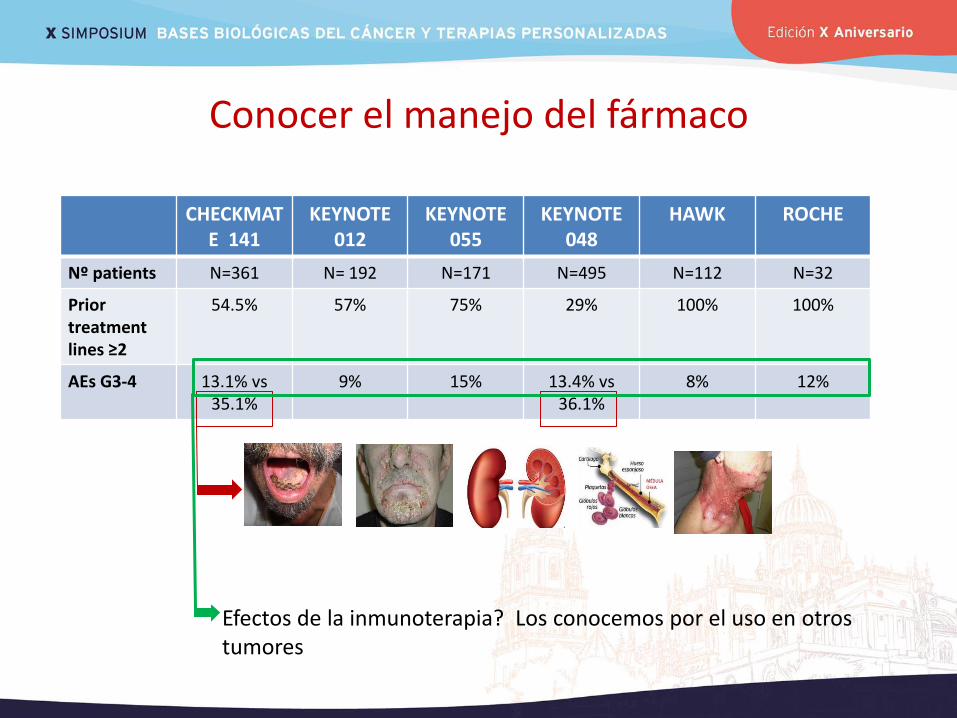
Conocer el manejo del fármaco
CHECKMATE 141
KEYNOTE 012
KEYNOTE 055
KEYNOTE 048
HAWK ROCHE
Nº patients N=361 N= 192 N=171 N=495 N=112 N=32
Prior treatment lines ≥2
54.5% 57% 75% 29% 100% 100%
AEs G3-4 13.1% vs 35.1%
9% 15% 13.4% vs 36.1%
8% 12%
Efectos de la inmunoterapia? Los conocemos por el uso en otros tumores
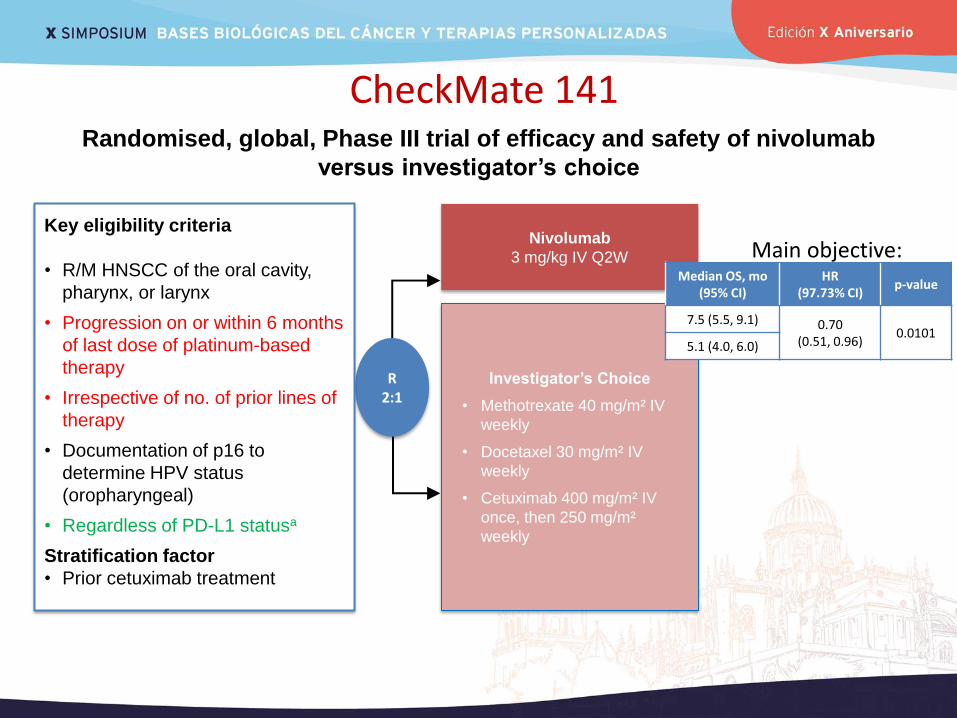
CheckMate 141
R 2:1
Nivolumab
3 mg/kg IV Q2W
Investigator’s Choice
• Methotrexate 40 mg/m² IV
weekly
• Docetaxel 30 mg/m² IV
weekly
• Cetuximab 400 mg/m² IV
once, then 250 mg/m²
weekly
Key eligibility criteria
• R/M HNSCC of the oral cavity,
pharynx, or larynx
• Progression on or within 6 months
of last dose of platinum-based
therapy
• Irrespective of no. of prior lines of
therapy
• Documentation of p16 to
determine HPV status
(oropharyngeal)
• Regardless of PD-L1 statusa
Stratification factor
• Prior cetuximab treatment
Randomised, global, Phase III trial of efficacy and safety of nivolumab
versus investigator’s choice
Ferris RL, et al. N Engl J Med 2016;375:1856–1867.
Median OS, mo (95% CI)
HR (97.73% CI)
p-value
7.5 (5.5, 9.1) 0.70 (0.51, 0.96)
0.0101 5.1 (4.0, 6.0)
Main objective:
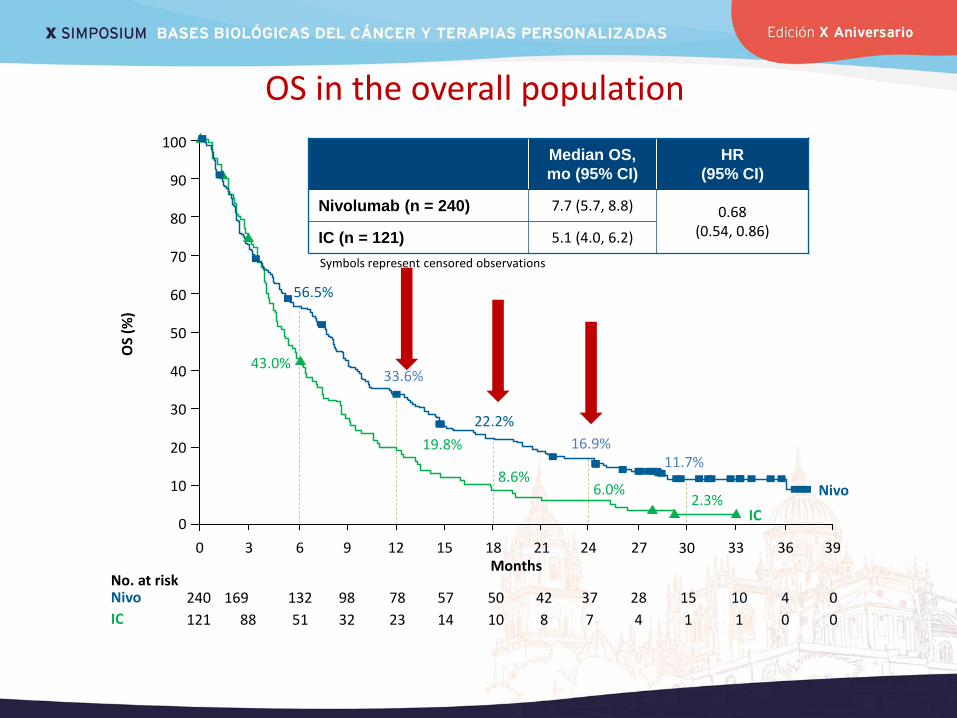
OS in the overall population
Median OS,
mo (95% CI)
HR
(95% CI)
Nivolumab (n = 240) 7.7 (5.7, 8.8) 0.68 (0.54, 0.86) IC (n = 121) 5.1 (4.0, 6.2)
OS
(%)
10
20
30
40
50
60
70
80
100
90
0
56.5%
43.0%
19.8%
33.6%
22.2%
8.6%
IC
16.9% 11.7%
6.0% 2.3%
Months 27 0 3 6 9 12 15 18 21 24 30 33 36 39
240 169 132 98 78 57 50 42 37 28
121 88 51 32 23 14 10 8 7 4
Nivo
IC
No. at risk 15
1
10
1
4
0
0
0
Nivo
Symbols represent censored observations
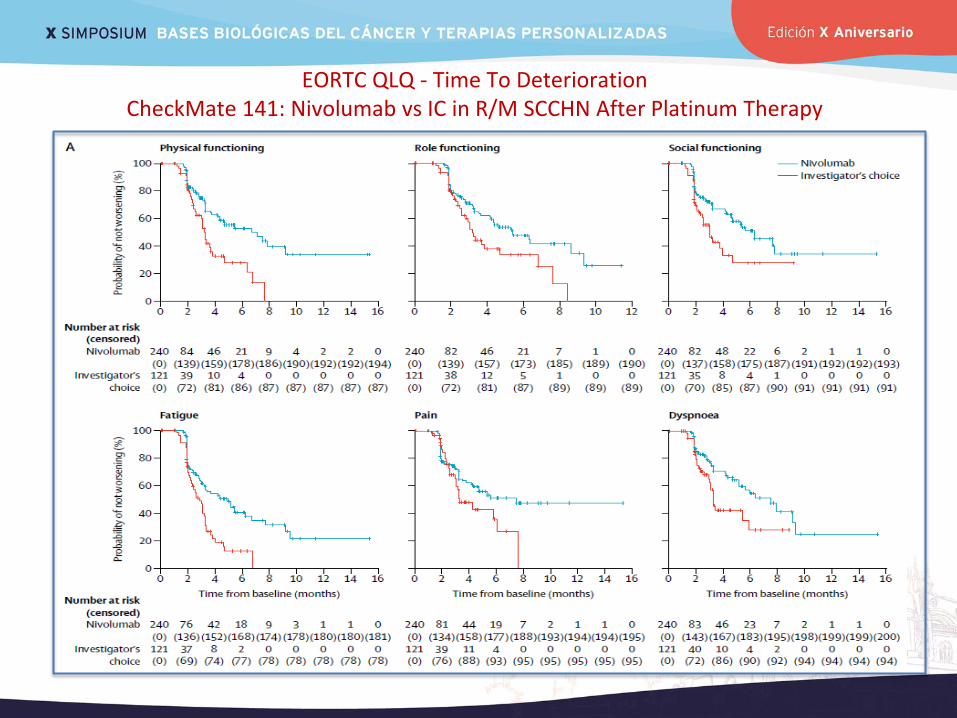
EORTC QLQ - Time To Deterioration CheckMate 141: Nivolumab vs IC in R/M SCCHN After Platinum Therapy
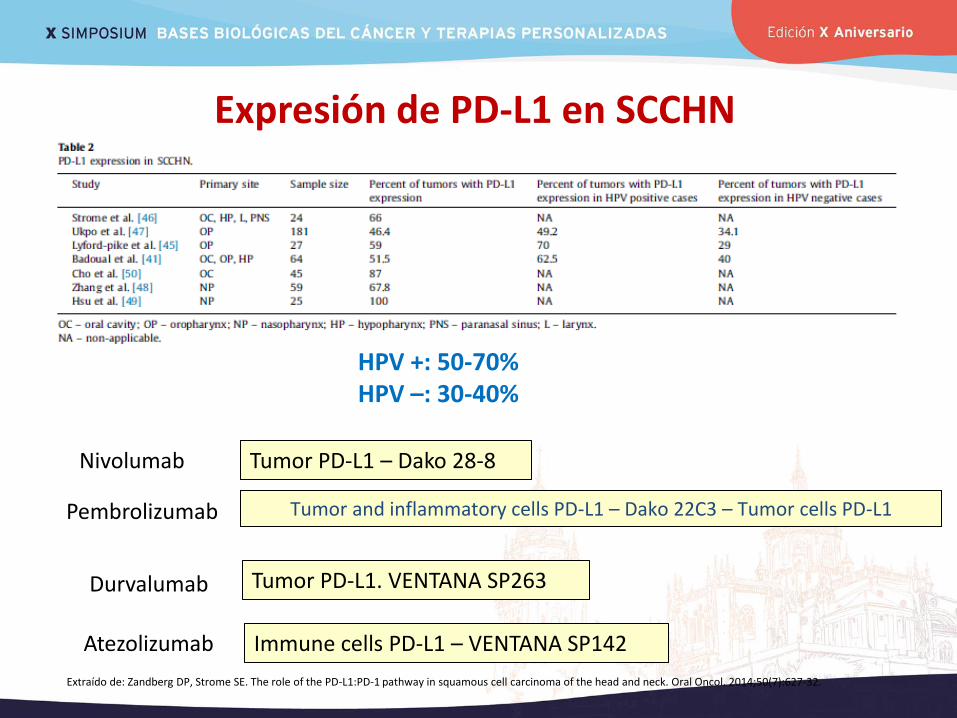
HPV +: 50-70% HPV –: 30-40%
Extraído de: Zandberg DP, Strome SE. The role of the PD-L1:PD-1 pathway in squamous cell carcinoma of the head and neck. Oral Oncol. 2014;50(7):627-32.
Tumor PD-L1 – Dako 28-8 Nivolumab
Tumor and inflammatory cells PD-L1 – Dako 22C3 – Tumor cells PD-L1 Pembrolizumab
Tumor PD-L1. VENTANA SP263 Durvalumab
Immune cells PD-L1 – VENTANA SP142 Atezolizumab
Expresión de PD-L1 en SCCHN

Overall survival according to PD-L1 expression
HR (95% CI)
0.55 (0.36, 0.83)
Ove
rall s
urv
iva
l (%
of
pa
tie
nts
)
Nivolumab (n = 88)
IC (n = 61)
Months
0 3 6 9 12 15 18
0
10
20
30
40
50
60
70
80
90
100 PD-L1 ≥1%
Nivolumab
IC
No. at risk
88 67 44 18 6 0
61 42 20 6 2 0
Ove
rall s
urv
iva
l (%
of
pa
tie
nts
)
PD-L1 <1%
Nivolumab (n = 73)
IC (n = 38)
Months
0 3 6 9 12 15 18
0
10
20
30
40
50
60
70
80
90
100
73 52 33 17 3
38 29 14 6
8
2 0
0
0
HR (95% CI)
0.89 (0.54, 1.45)
Ferris RL, et al. N Engl J Med 2016;375:1856–1867. CI, confidence interval; HR, hazard ratio;
IC, investigator’s choice; PD-L1, programmed death-ligand 1.
Deberemos decidir a qué pacientes no lo damos
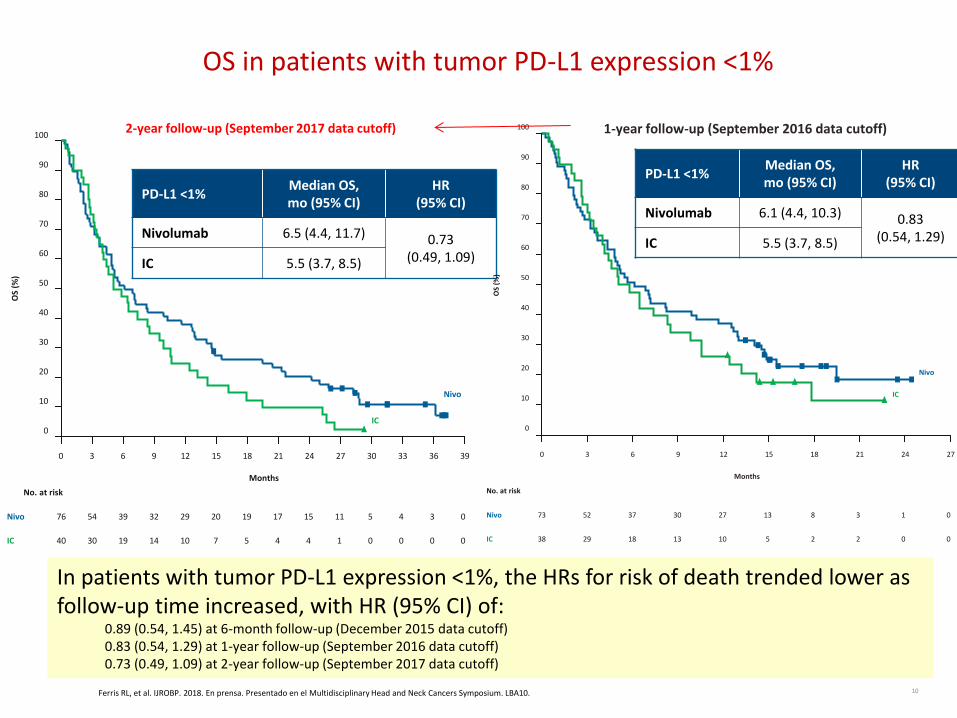
PD-L1 <1% Median OS, mo (95% CI)
HR (95% CI)
Nivolumab 6.5 (4.4, 11.7) 0.73 (0.49, 1.09) IC 5.5 (3.7, 8.5)
OS in patients with tumor PD-L1 expression <1%
2-year follow-up (September 2017 data cutoff)
0 3 6 9 12 21 15 18 24 27 30 33 36 39
Months
0
10
20
30
40
50
60
70
80
90
100
OS
(%)
Nivo
IC
76 54 39 32 29 20 19 17 15 11
40 30 19 14 10 7 5 4 4 1
Nivo
IC
No. at risk
5
0
4
0
3
0
0
0
1-year follow-up (September 2016 data cutoff)
0 3 6 9 12 21 15 18 24 27
Nivo
IC
73 52 37 30 27 13 8 3 1
38 29 18 13 10 5 2 2 0
Nivo
IC
No. at risk
0
0
0
10
20
30
40
50
60
70
80
90
100
OS
(%)
Months
PD-L1 <1% Median OS, mo (95% CI)
HR (95% CI)
Nivolumab 6.1 (4.4, 10.3) 0.83 (0.54, 1.29) IC 5.5 (3.7, 8.5)
10 Ferris RL, et al. IJROBP. 2018. En prensa. Presentado en el Multidisciplinary Head and Neck Cancers Symposium. LBA10.
In patients with tumor PD-L1 expression <1%, the HRs for risk of death trended lower as follow-up time increased, with HR (95% CI) of:
0.89 (0.54, 1.45) at 6-month follow-up (December 2015 data cutoff) 0.83 (0.54, 1.29) at 1-year follow-up (September 2016 data cutoff) 0.73 (0.49, 1.09) at 2-year follow-up (September 2017 data cutoff)

Overall Survival by Tumor PD-L1 Expression and PD-L1+ TAIC Abundance
Tumor PD-L1 ≥1% & PD-L1+ TAIC Abundance Tumor PD-L1 <1% & PD-L1+ TAIC Abundance
• Tumor PD-L1 ≥1% and rare PD-L1+ TAICs: mOS increased with NIVO vs IC (6.7 vs 4.9 months, HR 0.89 [0.44, 1.80]) • Tumor PD-L1 <1% and rare PD-L1+ TAICs: no difference mOS with NIVO vs IC (3.7 vs 4.9 months, HR 1.09 [0.50, 2.36])
1.0
0.8
0.2
0.0
0.6
0.4
Surv
ival
pro
bab
ility
5 10 0 20 25 15 Months
29 22 43 2 0 11
15 8 25 1 4
NIVO
IC
Patients at risk
mOS IC: 4.60 (95% CI: 3.81, 6.24)
mOS NIVO: 9.10 (95% CI: 7.03, 11.56)
HR: 0.43 (0.28, 0.67)
mOS NIVO: 11.73 (95% CI: 5.16, 15.57)
mOS IC: 6.51 (95% CI: 4.01, 10.61)
HR: 0.67 (0.38, 1.18)
1.0
0.8
0.2
0.0
0.6
0.4
Surv
ival
pro
bab
ility
5 10 0 20 25 15 Months
41 25 61 6 0 14
21 6 47 0 2
NIVO
IC
Patients at risk
0
[Tumor PD-L1 ≥1% HR: 0.55 (0.37, 0.77)] [Tumor PD-L1 <1% HR: 0.83 (0.54, 1.29)]
Ferris et al. AACR 2017
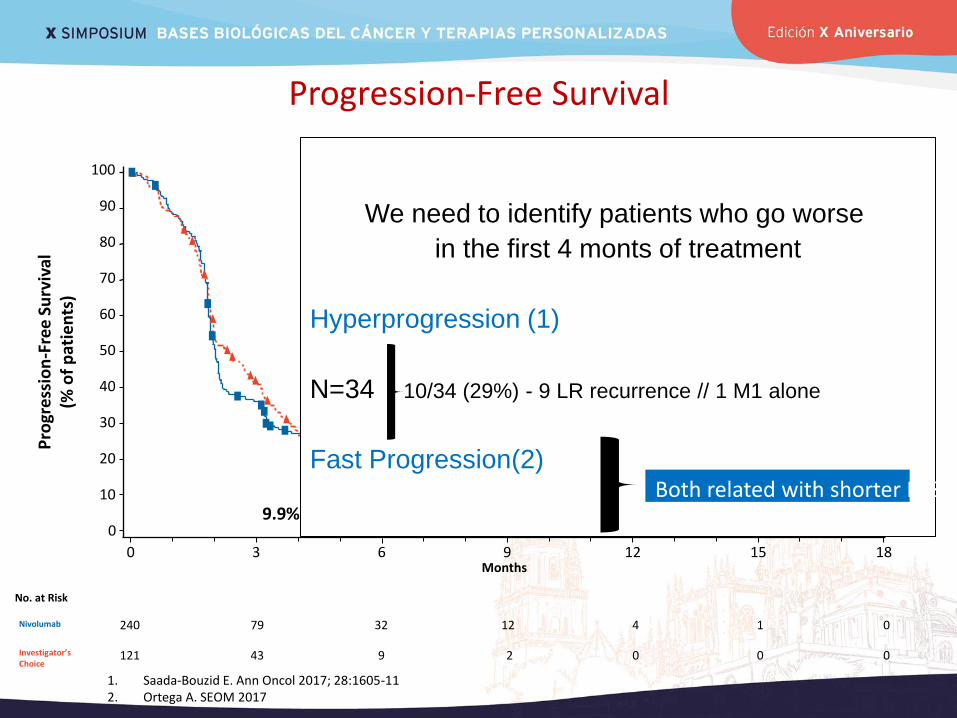
Progression-Free Survival
0 3 6 9 12 15 18 Months
Nivolumab 240 79 32 12 4 1 0
Investigator’s Choice
121 43 9 2 0 0
No. at Risk
0
0
10
20
30
40
50
60
70
80
90
100
Pro
gre
ssio
n-F
ree
Su
rviv
al
(% o
f p
atie
nts
)
Median PFS, mo (95% CI)
HR (95% CI)
P-value
Nivolumab (n = 240) 2.0 (1.9, 2.1) 0.89
(0.70, 1.1) 0.3236 Investigator’s Choice (n =
121) 2.3 (1.9, 3.1)
6-month PFS rate (95% CI) 19.7% (14.6, 25.4)
9.9% (5.0, 16.9)
We need to identify patients who go worse
in the first 4 monts of treatment
Hyperprogression (1)
N=34 10/34 (29%) - 9 LR recurrence // 1 M1 alone
Fast Progression(2)
1. Saada-Bouzid E. Ann Oncol 2017; 28:1605-11 2. Ortega A. SEOM 2017
Both related with shorter PFS

Hiperprogresión
1. Saada-Bouzid E. Ann Oncol 2017; 28:1605-11
Sangrado Ahogo Disfagia Infección
Fast progressors (FP)
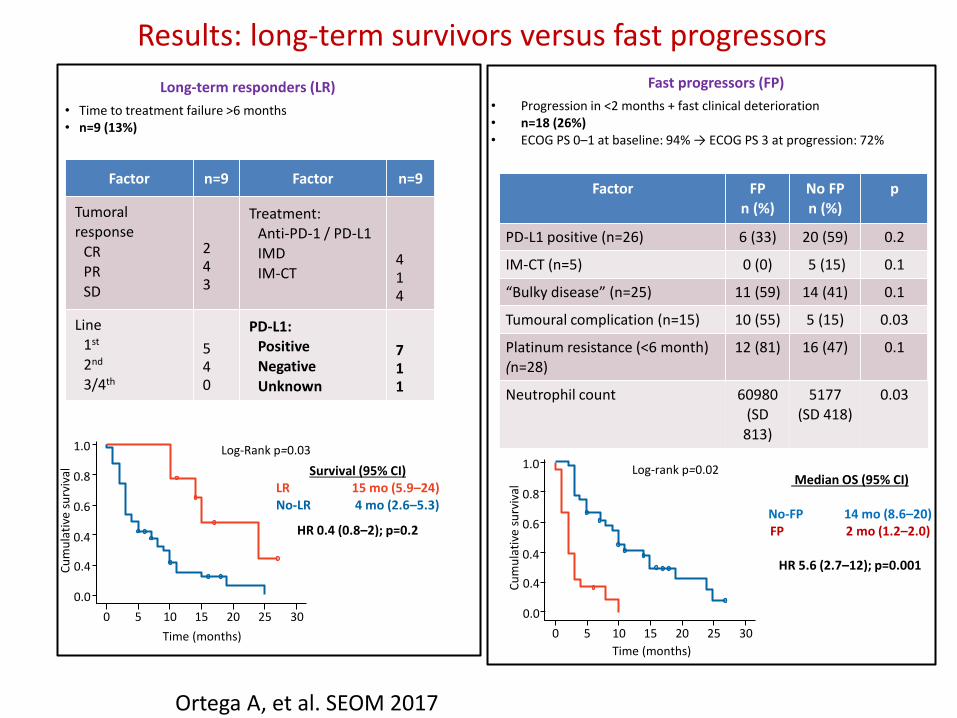
• Progression in <2 months + fast clinical deterioration • n=18 (26%) • ECOG PS 0–1 at baseline: 94% → ECOG PS 3 at progression: 72%
Long-term responders (LR)
• Time to treatment failure >6 months • n=9 (13%)
Factor FP n (%)
No FP n (%)
p
PD-L1 positive (n=26) 6 (33) 20 (59) 0.2
IM-CT (n=5) 0 (0) 5 (15) 0.1
“Bulky disease” (n=25) 11 (59) 14 (41) 0.1
Tumoural complication (n=15) 10 (55) 5 (15) 0.03
Platinum resistance (<6 month) (n=28)
12 (81) 16 (47) 0.1
Neutrophil count 60980 (SD
813)
5177 (SD 418)
0.03
Factor n=9 Factor n=9
Tumoral response
CR PR SD
2 4 3
Treatment: Anti-PD-1 / PD-L1 IMD
IM-CT
4 1 4
Line 1st
2nd
3/4th
5 4 0
PD-L1: Positive
Negative Unknown
7 1 1
Survival (95% CI) LR 15 mo (5.9–24) No-LR 4 mo (2.6–5.3)
HR 0.4 (0.8–2); p=0.2
Log-Rank p=0.03
1.0
0.8
0.6
0.4
0.4
0.0
Cu
mu
lati
ve s
urv
ival
0 5 10 15 20 25 30
Time (months)
Median OS (95% CI)
No-FP 14 mo (8.6–20) FP 2 mo (1.2–2.0)
HR 5.6 (2.7–12); p=0.001
Log-rank p=0.02
1.0
0.8
0.6
0.4
0.4
0.0
Cu
mu
lati
ve s
urv
ival
0 5 10 15 20 25 30
Time (months)
Results: long-term survivors versus fast progressors
Ortega A, et al. SEOM 2017
100
Ch
ange
Fro
m B
ase
line
in
Sum
of
Targ
et
Lesi
on
s (%
)
75
50
25
0
-25
-50
-75
-100
Weeks
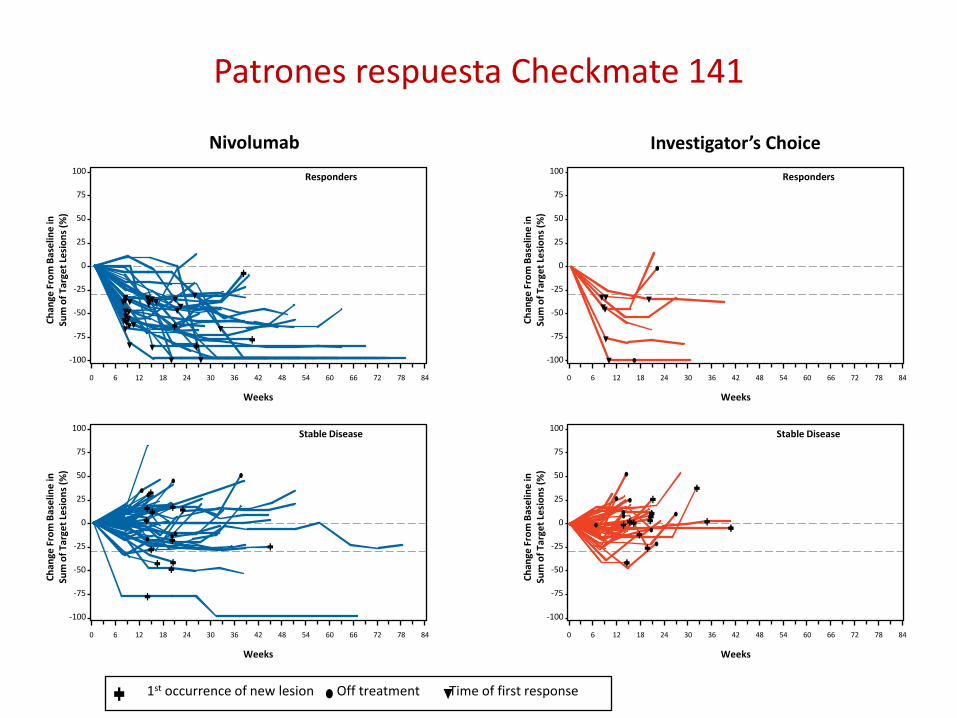
Responders
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
100
Ch
ange
Fro
m B
ase
line
in
Sum
of
Targ
et
Lesi
on
s (%
)
75
50
25
0
-25
-50
-75
-100
Weeks
Stable Disease
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
100
Ch
ange
Fro
m B
ase
line
in
Sum
of
Targ
et
Lesi
on
s (%
)
75
50
25
0
-25
-50
-75
-100
Weeks
Responders
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
100
Ch
ange
Fro
m B
ase
line
in
Sum
of
Targ
et
Lesi
on
s (%
)
75
50
25
0
-25
-50
-75
-100
Weeks
Stable Disease
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
Patrones respuesta Checkmate 141
Nivolumab Investigator’s Choice
1st occurrence of new lesion Off treatment Time of first response
16
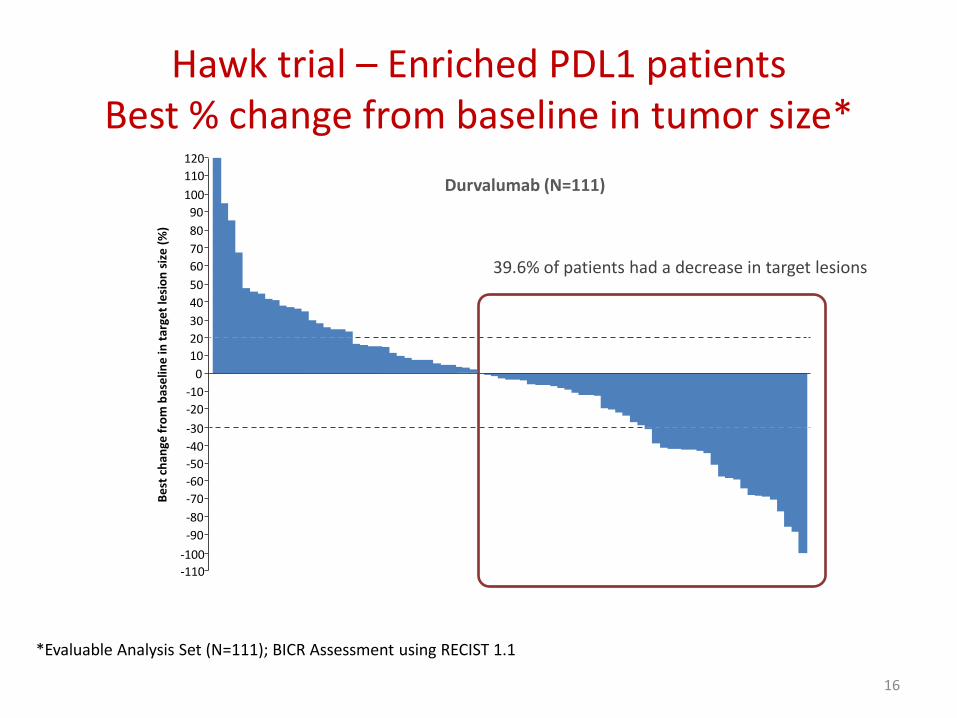
*Evaluable Analysis Set (N=111); BICR Assessment using RECIST 1.1
Durvalumab (N=111)
-110
-100
-90
-80
-70
-60
-50
-40
-30
-20
-10
0
10
20
30
40
50
60
70
80
90
100
110
120 B
est
ch
ange
fro
m b
ase
line
in t
arge
t le
sio
n s
ize
(%
)
39.6% of patients had a decrease in target lesions
Hawk trial – Enriched PDL1 patients Best % change from baseline in tumor size*
17
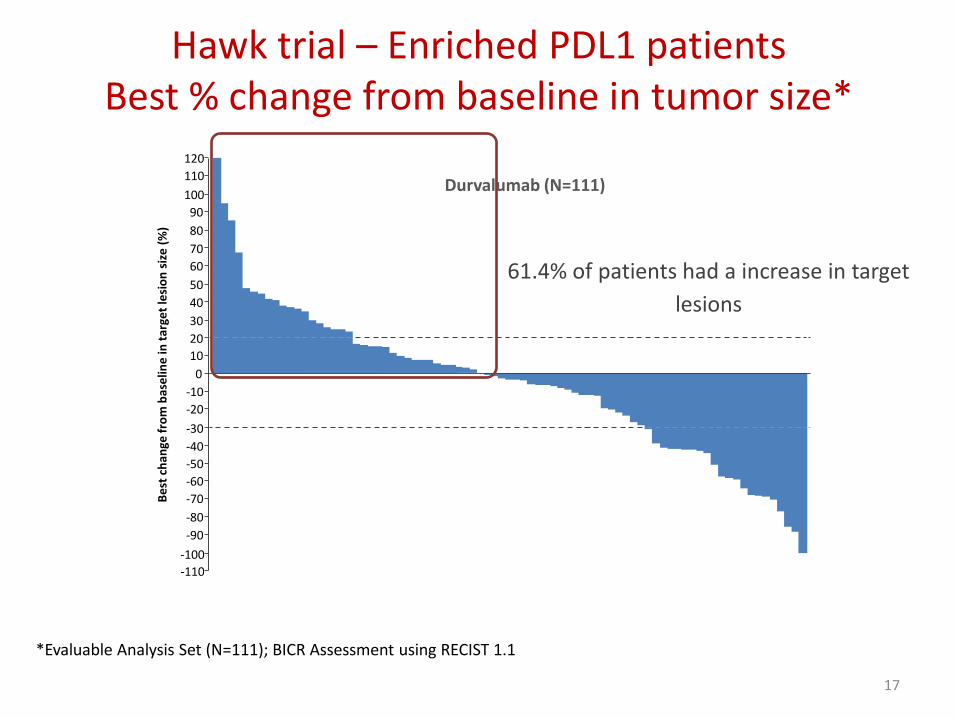
*Evaluable Analysis Set (N=111); BICR Assessment using RECIST 1.1
Hawk trial – Enriched PDL1 patients Best % change from baseline in tumor size*
Durvalumab (N=111)
-110
-100
-90
-80
-70
-60
-50
-40
-30
-20
-10
0
10
20
30
40
50
60
70
80
90
100
110
120 B
est
ch
ange
fro
m b
ase
line
in t
arge
t le
sio
n s
ize
(%
)
61.4% of patients had a increase in target
lesions
18
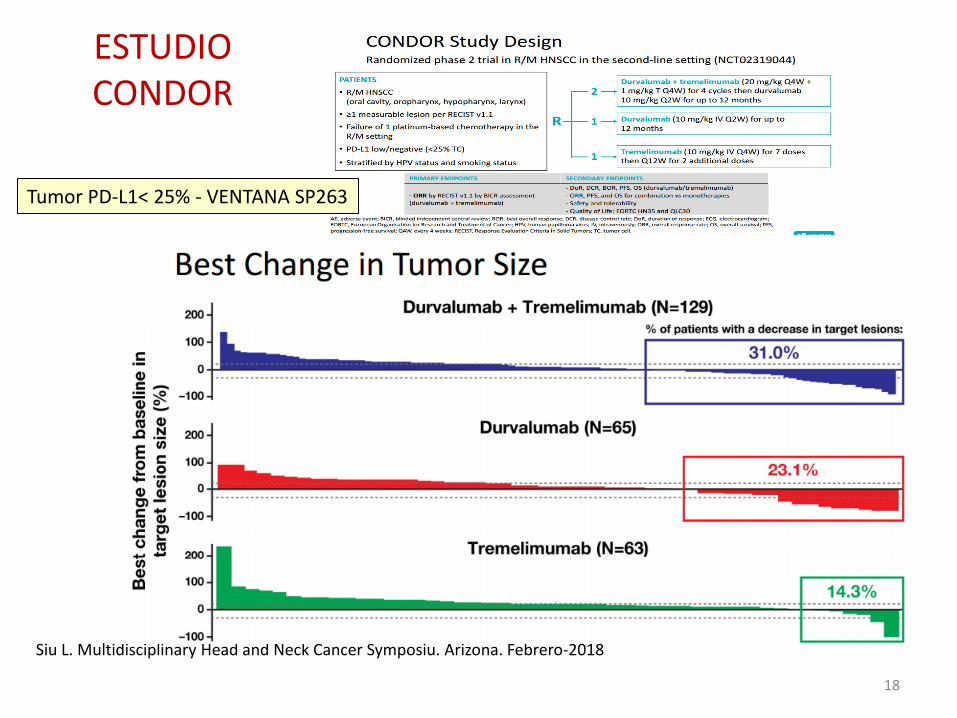
Siu L. Multidisciplinary Head and Neck Cancer Symposiu. Arizona. Febrero-2018
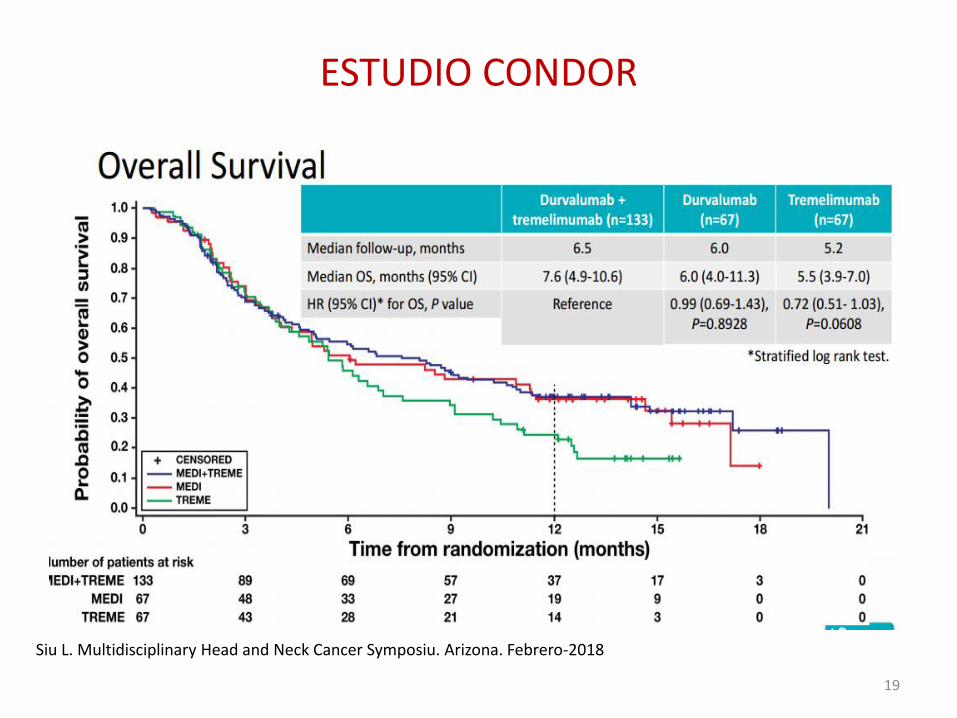
ESTUDIO CONDOR
Tumor PD-L1< 25% - VENTANA SP263
19
ESTUDIO CONDOR
Siu L. Multidisciplinary Head and Neck Cancer Symposiu. Arizona. Febrero-2018
20
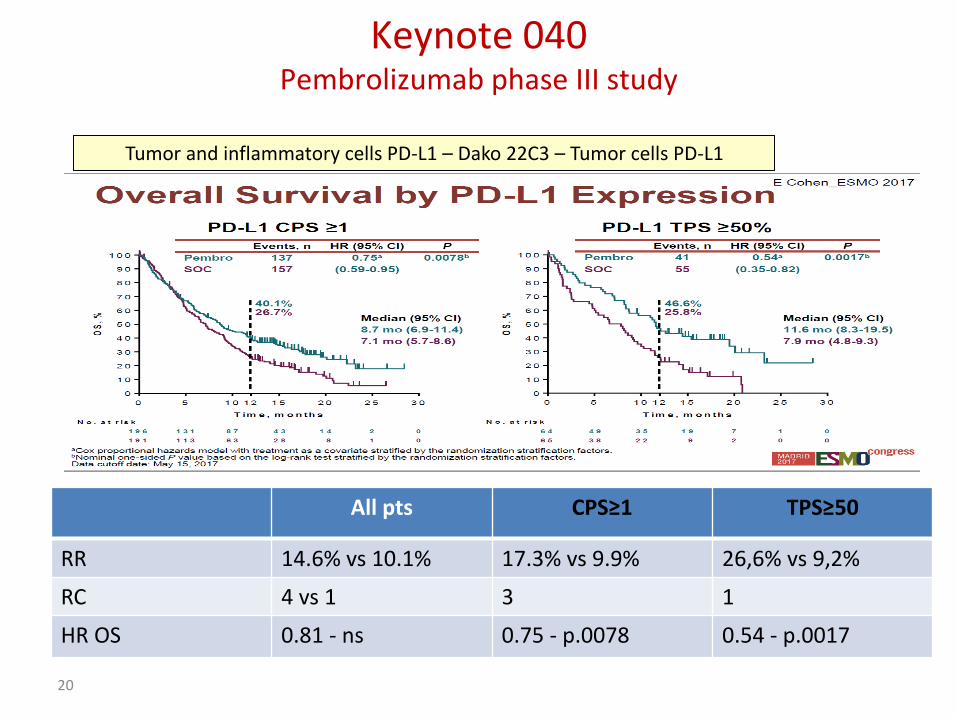
Tumor and inflammatory cells PD-L1 – Dako 22C3 – Tumor cells PD-L1
Keynote 040 Pembrolizumab phase III study
All pts CPS≥1 TPS≥50
RR 14.6% vs 10.1% 17.3% vs 9.9% 26,6% vs 9,2%
RC 4 vs 1 3 1
HR OS 0.81 - ns 0.75 - p.0078 0.54 - p.0017
Indicación
Seguiremos ficha técnica o ampliaremos indicaciones?
- Nasofaringe?
- Senos maxilares, glándulas salivares?
- PS 2?
- Unfit para CDDP?
21
No existe evidencia para ninguna de ellas!!!

Soportar el gasto qué supone
Algunos cánceres Nuevos fármacos Inmunoterapia Combinaciones inmuno
Otras enfermedades
Mama Pertuzumab Inh. Ciclinas Everolimus,...
Neurológicas
Colon Avastin, antiEGFR Cardivasculares
Próstata Abiraterona Reumatológicas
Pulmón AntiEGFR, antiALK, Ros,...
+++ En estudio Infecciosas
Urológicos Sutent,... ++ En estudio
Melanoma Anti BRAF + Utilizadas
Hematológicos Multitud ++ En estudio
Ca CyC Cetuximab + En estudio
Ovario Inh. Ciclinas Avastin
Prevención Asistencia 1aria
22
Sistema sanitario finito y equitativo
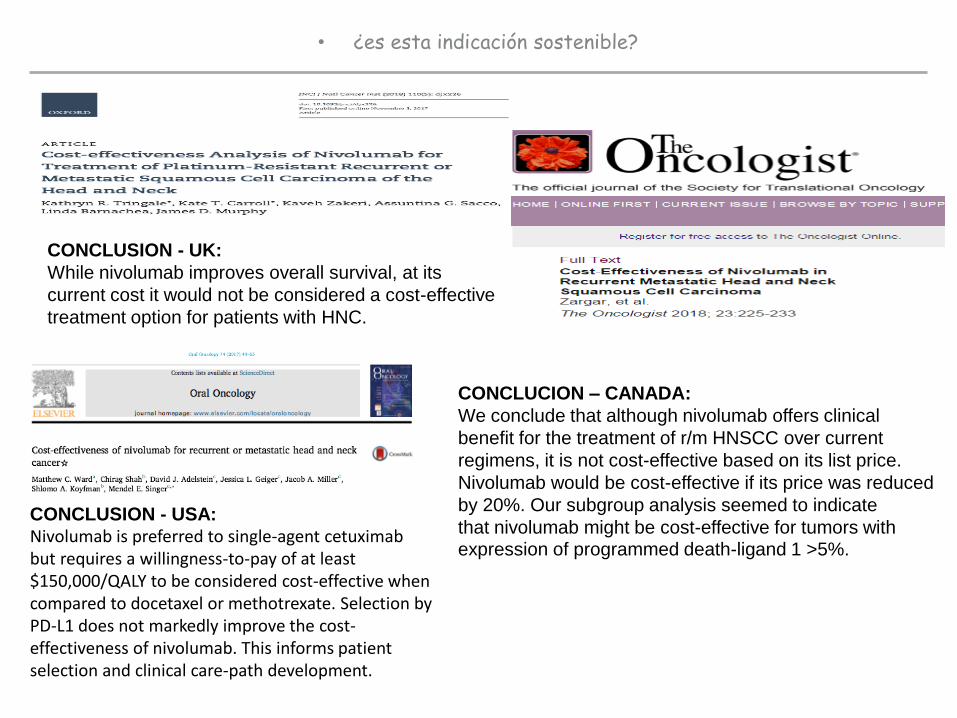
• ¿es esta indicación sostenible?
CONCLUSION - UK:
While nivolumab improves overall survival, at its
current cost it would not be considered a cost-effective
treatment option for patients with HNC.
CONCLUSION - USA: Nivolumab is preferred to single-agent cetuximab but requires a willingness-to-pay of at least $150,000/QALY to be considered cost-effective when compared to docetaxel or methotrexate. Selection by PD-L1 does not markedly improve the cost-effectiveness of nivolumab. This informs patient selection and clinical care-path development.
CONCLUCION – CANADA:
We conclude that although nivolumab offers clinical
benefit for the treatment of r/m HNSCC over current
regimens, it is not cost-effective based on its list price.
Nivolumab would be cost-effective if its price was reduced
by 20%. Our subgroup analysis seemed to indicate
that nivolumab might be cost-effective for tumors with expression of programmed death-ligand 1 >5%.
Conclusiones
• Existe una base racional para el desarrollo de inmunoterapia en CCC.
• Nivolumab ha sido el primer IO aprobado en la patología.
• Simplemente estamos empezando, y hemos de tomar conciencia de a qué pacientes beneficiamos, pero también de que podemos perjudicar.
• Precisaremos de una fuerte base traslacional para acertar en el desarrollo clínico.
• El precio del fármaco puede afectar a su incorporación a la clínica.

http://ico.gencat.cat
@ICOnoticies www.facebook.com/ICOnoticies
Institut Català d’Oncologia
ICO l’Hospitalet Hospital Duran i Reynals Av. Granvia de L’Hospitalet, 199-203 08908 L’Hospitalet de Llobregat
ICO Badalona Hospital Germans Trias i Pujol Ctra. del Canyet s/n 08916 Badalona
ICO Girona Hospital Doctor Trueta Av. França s/n 17007 Girona
ICO Camp de Tarragona i Terres de l’Ebre Hospital Joan XXIII C. Dr. Mallafrè Guasch, 4 43005 Tarragona Hospital Verge de la Cinta C. de les Esplanetes, 14 43500 Tortosa
ICO-Badalona, servei d’Oncologia Mèdica
![Agnostic evaluation of ipilimumab and nivolumab association ......Marchetti et al. J Transl Med Page 2 of 7advantageinmelanomapatients,whencomparedtoa gp100vaccineorchemotherapy[3].Nivolumab,target-ingPD-1](https://img.pdfslide.tips/doc/110x75/60ca64bf0dfb543e4a37fd17/agnostic-evaluation-of-ipilimumab-and-nivolumab-association-marchetti-et.jpg)











![[Table Main] - TIANYANCHAstock.tianyancha.com/ResearchReport/eastmoney/94cfbc7ba0cd6687e9bbc5ef... · Opdivo Nivolumab BMS PD -1 2014 U8¨3V,Z=M E4ü7 6ð, =6ô, =MC }H$ *,Z= jN¾,](https://img.pdfslide.tips/doc/110x75/5e6e60040307152ebb18e9fb/table-main-opdivo-nivolumab-bms-pd-1-2014-u83vzm-e47-6-6-mc-h.jpg)