-
8/10/2019 Infective Arthritis - EMedWiki
1/6
6/24/14 2:nfective arthritis - eMedWiki
Page
ttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis
Figure 1: The knee joint is asynovial joint and a common
site of infective arthritis [2]
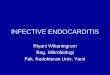
Figure 2: Common causative
agents of infective arthritis.
Adapted from [2]
Infective arthritis
From eMedWiki
nfective arthritis describes joint infections caused by
microorganisms [1]. Jointnfection is serious as it can cause rapid
destruction of articular cartilage, loss
of joint function, and diagnostic and management problems in
existing
heumatoid arthritis [3][4].
Contents
1 Classification & Aetiology2 Pathophysiology3 Risk Factors4
Clinical Manifestations
4.1 Bacterial Infections4.2 Mycobacterial/Fungal Arthritis4.3
Viral Arthritis
5Diagnosis6Treatment7Infective Arthritis &
Ageing8References
Classification& Aetiologynfective arthritis can be caused
either by direct infection of a joint space (suppurative arthritis)
or immune
esponses to systemic infections (non-suppurative arthritis) by
various microorganisms shown in Figure 2 [2]
AlthoughNeisseria gonorrhoeaeremains the most common
pathogen(75% of
ases) among younger sexually active individuals, Staph.
aureusinfection is
he main cause of bacterial arthritis in adults and in children
older than 2 years
65%) [5]. Staph. aureusis also the primary pathogen in hip
infections and in
polyarticular septic arthritis [2].
Haemophilus influenzae, a gram negative bacilli predominates in
children
under 2 years and other gram negative organisms are more common
in older or
mmunocompromised patients than in young adults [6].
While viral and fungal joint infections are rare, there have
been increasing cases of Candidainfections causi
arthritis in both native and prosthetic joints [7].
http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Mathews-5http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Referenceshttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Infective_Arthritis_.26_Ageinghttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Treatmenthttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Diagnosishttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Viral_Arthritishttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Risk_Factorshttp://php.med.unsw.edu.au/medwiki/index.php?title=File:Illu_synovial_joint.jpghttp://php.med.unsw.edu.au/medwiki/index.php?title=File:Illu_synovial_joint.jpghttp://php.med.unsw.edu.au/medwiki/index.php?title=File:Illu_synovial_joint.jpghttp://php.med.unsw.edu.au/medwiki/index.php?title=File:Illu_synovial_joint.jpghttp://php.med.unsw.edu.au/medwiki/index.php?title=File:Illu_synovial_joint.jpghttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Fungal-6http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Mathews-5http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Ross-4http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Referenceshttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Infective_Arthritis_.26_Ageinghttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Treatmenthttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Diagnosishttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Viral_Arthritishttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Mycobacterial.2FFungal_Arthritishttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Bacterial_Infectionshttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Clinical_Manifestationshttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Risk_Factorshttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Pathophysiologyhttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#Classification_.26_Aetiologyhttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Robbins-3http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-2http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=File:Classification_aetiology.jpghttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=File:Illu_synovial_joint.jpg
-
8/10/2019 Infective Arthritis - EMedWiki
2/6
6/24/14 2:nfective arthritis - eMedWiki
Page
ttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis
The rate of infection ranges from 05% to 2% for hip and knee
replacements [8]. While early-onset infections
usually the result of perioperative wound contamination, joint
infections that begin later than three months af
he joint implant are haematogenously acquired. Staph. aureusand
Streptococciare the most common causat
agents in late-onset prosthetic joint infections [2].
Pathophysiology
Bacterial arthritis is usually spread haematogenously but may
also be introduced by direct inoculation during
oint surgery or, rarely, during joint aspiration. Also, in
children, osteomyelitis may spread to adjacent joints
The bacteria enter the closed joint space and within hours,
trigger an influx of inflammatory cells. Release of
ytokines and proteases leads to cartilage degradation and
irreversible subchondral bone loss within days [2].
Similarly, fungal arthritis can be caused by:
direct intra-articular inoculation of fungi that inhabit the
skin, causing infection in a single jointa complication of
haematogenously disseminated fungi of the Candidafamily that also
results in
monoarthritis or pauciarthritis [7]
Viral arthritis is a result of the body's immune responses to
systemic infection and the resultant presence of
proinflammatory and anti-inflammatory cytokines is what causes
inflammation and joint deformity even afte
he virus is cleared [10].
Risk Factors
Host factors that predispose to infective arthritis include age,
decreased immunocompetence seen in such
onditions as HIV AIDS, preexisting joint disease including
osteoarthritis and rheumatoid arthritis, diabetes
mellitus and intravenous drug use [2][6]. The most important
risk factor for prosthetic joint infection is revisio
arthroplasty in which the joint is surgically refashioned. This
carries a 510% risk of infection [2].
Clinical Manifestations
The knee is the site of infection in most cases of infective
arthritis and hip infections are more common in
young children [11]. Furthermore, 1020% of infections are
polyarticular, usually involving two or three join
n 50% of cases, the source of infection can be found to stem
from the skin, lungs or bladder.
Bacterial Infections
Non-gonococcal infective arthritis usually presents with the
acute onset of a single hot, swollen, and very
painful joint. Most patients are febrile, and young children in
particular may present with chills and spiking
evers. Both passive and active range of motion are limited and
cause discomfort.
http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-10http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Mathews-5http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-9http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Fungal-6http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-7
-
8/10/2019 Infective Arthritis - EMedWiki
3/6
6/24/14 2:nfective arthritis - eMedWiki
Page
ttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis
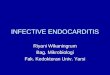
Figure 3: MRI of staphylococcal infective arthriti
of left hip, with arrows indicating fluid collection
[15]
A minority of patients (28%) with gonococcal infection will
present with a single purulent joint effusion, and
nflammation or tenderness of multiple tendons of the wrist,
ankles, and small joints [12]. Accompanying skin
esions are typically painless and pustular, and found
predominantly on fingers, hands, wrists and feet [13].
Mycobacterial/Fungal Arthritis
Two distinct clinical presentations can be observed with fungal
arthritis:
acute onset of synovial symptoms (about two thirds of patients)
with an established diagnosiswithin the first week, andindolent
presentation, with mild systemic and arthritic symptoms, and delay
in diagnosis for
months or years [7]
Viral Arthritis
Viral arthritis is associated with systemic symptoms such as
fever, and rash. Parvovirus B19 is the most
ommon viral agent and presents as a symmetric polyarticular
arthritis [14].
Diagnosis
Diagnosis of infective arthritis requires the identification
of
he microorganism present in the synovial fluid. If synovial
luid cannot be obtained with closed needle aspiration, a
econd attempt with imaging guidance is used for less
accessible joints such as the shoulders and sacroiliac
joints
6]
.
n a blood sample, elevated erythrocyte sedimentation rates,
C-reactive protein concentrations or white cell counts
>500000 per mm3) reflect an acute-phase response, and are
uggestive of infective arthritis. Although these values
alone
do not definitively diagnose for infective arthritis, the
measurements are useful in monitoring response to
reatment [16]. Bacterial infections are determined by Gram
tain or by synovial fluid culture, which is positive in 90%
of cases of non-gonococcal bacterial arthritis. Gram stainsare
positive in only 50% as clumps of stain or cellular debris
may be mistaken for bacteria. Blood cultures are positive in
5070% of patients with non-gonococcal bacterial arthritis. In
contrast, the synovial fluid Gram stain is posit
n less than 25% of patients with gonococcal arthritis, and
culture is positive in only 50%. A diagnosis of
gonococcal infection is often made based on the patient history
and examination, and a identification of
Neisseria gonorrhoeaefrom a genitourinary source [2].
http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-15http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Mathews-5http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-13http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Fungal-6http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-12http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Sharp-11http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-m2-14http://php.med.unsw.edu.au/medwiki/index.php?title=File:Mri.jpg
-
8/10/2019 Infective Arthritis - EMedWiki
4/6
6/24/14 2:nfective arthritis - eMedWiki
Page
ttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis
Figure 4: Needle aspiration of knee joint.
Arthrocentesis, the draining of synovial fluid, is a
similar looking procedure [17].
dentification of microbial DNA by PCR will be most useful in
patients with partly treated or culture-negativ
bacterial arthritis and in non-suppurative arthritis.
n acute infective arthritis, radiographs are only used to detect
joint effusion and to demonstrate concurrent
osteomyelitis or arthritis. Computed tomography is used to
detect effusions and as a guide in joint aspiration
while scintigraphy and magnetic resonance imaging (MRI) allow
for differentiation between infective arthrit
and osteoarthritis [15].
Treatment
The treatment of acute infective arthritis requires antibioand
joint drainage. The initial choice of antibiotics shouldbe based on
the synovial fluid Gram stain as well as the aand risk factors of
the patient. Empirical therapy usuallyincludes broad-spectrum
parenteral antibiotics againstStaph. aureusand Streptococcidue to
their high causativrates and therapy is then modified based on the
culture an
sensitivity of the synovial fluid or blood culture [18].
Daily draining of infected joints may be necessary in
beginning stages of treatment, with arthroscopy being the
preferred method in knee or shoulder infections because
better irrigation and visualisation. If joint drainage canno
be maintained by needle aspiration or arthroscopy, open
surgical drainage is recommended [19].
n prosthetic joint infections, bacteria attach to the prosthetic
material and form a biofilm of exopolysacchari
hat protects against host phagocytes and thus contributes to
antibiotic resistance. Therefore, treatment of
nfection in prosthetic joints usually requires the surgical
removal of all bioprosthetic components. High-risk
patients or those refusing replacement arthroplasty have been
successfully treated with longterm suppressive
antimicrobial therapy [2].
Infective Arthritis & Ageing
Osteoarthritis and rheumatoid arthritis are the focus in Ageing
& Endings A, being more common in ageing
populations, affecting an estimated 1.6 million and 428,000
Australians respectively [20]. However,
osteoarthritis and rheumatoid arthritis are risk factors for the
development of infective arthritis, but can also b
differential diagnoses for the presenting symptoms of infective
arthritis. Therefore, infective arthritis remains
oncern because of its rapid progression and fatal consequences
if left undetected or untreated [2].
http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-19http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-Goldenburg-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-18http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-17http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-m2-14http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_note-16http://php.med.unsw.edu.au/medwiki/index.php?title=File:Aspi.jpg
-
8/10/2019 Infective Arthritis - EMedWiki
5/6
6/24/14 2:nfective arthritis - eMedWiki
Page
ttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis
References
1. !L. Eder, D. Zisman, M. Rozenbaum, and I. Rosner. (2005).
"Clinical features and aetiology of septic
arthritis in northern Israel",Rheumatology 44(12):1559-1563
2. !2.002.012.022.032.042.052.062.072.082.092.10Goldenburg DL.
(1998). "Septic Arthritis". The Lance
351:197-202.
3. !Russell AS & Ansell BM. (1972). "Septic
Arthritis".Annals of the Rheumatic Diseases 31:40-44.4. !Kumar, V.,
Abbas, A., Fausto, N., & Mitchell, R. (2007). Robbins Basic
Pathology (8th ed.).
Philadelphia: Saunders Elsevier.5. !Ross JJ, Saltzman CL,
Carling P, and Shapiro DS. (2003). "Pneumococcal septic arthritis:
review of
190 cases". Clinical Infectious Diseases 36:319-327
6. !6.06.16.2Mathews CJ, Kingsley G, Field M, Jones A, Weston
VC, Phillips M, Walker D, and Coakl
G. (2007). "Management of Septic Arthritis: A Systematic
Review".Annals of the Rheumatic Disease66: 440-445.
7. !7.07.17.2Cuella ML, Silveira LH, and Espinoza LR. (1992).
"Fungal Arthritis".Annals of the
Rheumatic Diseases, 51: 690-697.
8. !Brause B. (2005). "Infections with prostheses in bones and
joints". Principles and Practices ofInfectious Diseases,
1332-1337
9. !Kaandorp CJ, Dinant HJ, van de Laar MA, Moens HJ, Prins AP,
and Dijkmans BA.(1997). "Inciden
and sources of native and prosthetic joint infection: a
community based prospective survey".Annals ofthe Rheumatic
Diseases, 56:470-475
10. !Reimold, A. (2010). "Viruses and Arthritis: New Challenges
in Diagnosis, Therapy, and
Immunization".American Journal of Medical Science,
339(6):549556.11. !Goldenburg DL. (1998). "Infectious Arthritis
Complicating Rheumatoid Arthritis and Other Chronic
Rheumatic Disorders".Arthritis and Rheumatism, 32(4):496-502.12.
!Sharp JT, Lidsky MD, Duffy J, and Duncan MW. (1979). "Infectious
Arthritis".Archives of Interna
Medicine 139:1125-113013. !Bardin T. (2003). "Gonococcal
arthritis".Best Practice and Research Clinical Rheumatology
17:201
20814. !Woolf AD, Campion GV, and Chishick A. (1989). "Clinical
manifestations of human parvovirus B1
in adults".Archives of Internal Medicine, 149:1153-6.
15. !15.015.1Mathews CJ, Weston VC, Jones A, Field M, and
Coakley G. (2010). "Bacterial Septic Arthr
in Adults". The Lancet, 375:846-85516. !Li SF, Henderson J,
Dickman E, and Darzynkiewicz R. (2004). "Laboratory tests in adults
with
monoarticular arthritis: can they rule out a septic
joint?".Academic Emergency Medicine, 11: 27628017. !McNeill P.
(2011). "Arthritis 1 - Rheumatoid Arthritis [Lecture Notes].
Sydney, Australia: Universit
of New South Wales.18. !Siva C, Velazquez C, Mody A, and
Brasington R. (2003). "Diagnosing acute monoarthritis in adults
practical approach for the family physician".American Family
Physician, 68:83-9019. !Ohl C. (2005). "Infectious arthritis of
native joints". Principles and Practice of Infectious Diseases,
1311-132220. !Australian Institute of Health and Welfare (AIHW).
(2010). "A snapshot of Arthritis in Australia 20
Arthritis series no. 13. Cat. no. PHE 126. Canberra: AIHW.
http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-19http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-18http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-17http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-16http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-15http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-m2_14-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-m2_14-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-13http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-12http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Sharp_11-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-10http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-9http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-8http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-7http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Fungal_6-2http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Fungal_6-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Fungal_6-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Mathews_5-2http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Mathews_5-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Mathews_5-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Ross_4-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Robbins_3-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-2http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-10http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-9http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-8http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-7http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-6http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-5http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-4http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-3http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-2http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-1http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-Goldenburg_1-0http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis#cite_ref-0
-
8/10/2019 Infective Arthritis - EMedWiki
6/6
6/24/14 2:nfective arthritis - eMedWiki
Page
ttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis
Retrieved from
"http://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis&oldid=16660"
Categories: Ageing and Endings A Ageing & Endings A 2011
http://php.med.unsw.edu.au/medwiki/index.php?title=Special:Categorieshttp://php.med.unsw.edu.au/medwiki/index.php?title=Infective_arthritis&oldid=16660http://php.med.unsw.edu.au/medwiki/index.php?title=Category:Ageing_%26_Endings_A_2011http://php.med.unsw.edu.au/medwiki/index.php?title=Category:Ageing_and_Endings_A