Embed Size (px)
Citation preview

Influence of Skeletal Site of Origin and Donor Age on OsteoblasticCell Growth and Differentiation
M. E. Martı´nez,1 M. T. del Campo,1 S. Medina,1 M. Sanchez,1 M. J. Sanchez-Cabezudo,1 P. Esbrit,2 P. Martı nez,1I. Moreno,1 A. Rodrigo,1 M. V. Garces,3 L. Munuera 4
1Biochemistry Division, Hospital La Paz, Pso. de la Castellana, 261, 28046, Madrid, Spain2Metabolic Research Unit, Fundacio´n Jimenez Dıaz, Madrid, Spain3CIMBUC. Carabobo University, Valencia, Venezuela4Orthopaedic Department, Hospital La Paz, Madrid, Spain
Received: 25 March 1998 / Accepted: 1 October 1998
Abstract. Bone loss with aging may be due, at least in part,to inadequate bone formation. Moreover, the process ofbone aging is known to follow a different pattern throughoutthe skeleton. In this study, we examined the cell prolifera-tion rate (area under the cell growth curve, AUC) and thesecretion of C-terminal type I procollagen (PICP), alkalinephosphatase (ALP), and osteocalcin (OC) in primary cul-tures of osteoblastic cells from human trabecular bone. Os-teoblastic cells were obtained for 168 donors (100 womenand 68 men). Ninety-eight bone samples were obtainedfrom subjects undergoing knee arthroplastia, 52 aged 50–70years (64 ± 5) and 46 over age 70 (73 ± 2). Another 70 bonesamples were obtained from subjects undergoing hip arthro-plastia; 51 were 50–70 years old (64 ± 4) and 19 were over70 (75 ± 5). Osteoblastic cells from the older donors had alower proliferation rate and OC secretion than those fromyounger subjects. However, ALP secretion was higher inthe former subjects, whereas PICP secretion was un-changed. Osteoblastic cells from hip had a lower prolifera-tion rate than those from knee. PICP secretion was alsolower and ALP secretion was higher in the former cells. Inage-matched cell cultures, osteoblastic cells from the kneehad higher proliferation rate and PICP secretion than osteo-blastic cells from the hip. However, ALP secretion waslower in knee osteoblastic cells than those from hip only inthe younger group. With aging, ALP secretion was found toincrease in knee osteoblactic cells, whereas OC secretiondecreased in osteoblastic cell cultures from the hip. Ourfindings suggest that bone loss with aging may be accountedfor, at least in part, by a decreased osteoblastic cell prolif-eration and an increased osteoblastic maturation. In addi-tion, our data indicate that these changes with aging do notoccur similarly at different skeletal sites.
Key words: Human osteoblastic cells — Skeletal site —Aging.
Bone remodeling in adult life occurs through a process in-volving osteoclast-mediated bone resorption coupled tobone formation by osteoblasts [1]. The influence of age onbone loss is a well-known event but the underlying mecha-
nisms are still unknown [2]. Age-related osteopenia hasbeen partly accounted for by a defect in osteoblastic func-tion, based on histological findings. The sharp decrease ofbone-forming surfaces compared with bone resorption sur-faces observed in elder subjects is thought to reflect theinability of osteoblasts to reconstitute resorbed bone [3].Several mechanisms have been suggested to be involved inthis decreased bone formation with aging: a deficit of bonemarrow stromal cell populations, a lower proliferation rateof osteoblast precursors, and a decrease in osteoblasticgrowth and/or function [4]. Several animal studies supportthe first two hypotheses [5, 6]. Moreover, a histomorpho-metric analysis in aging human bone has shown a decreasednumber of osteoblast progenitors associated with a deficit ofextracellular bone matrix in resorption lacunae [7].
Human endosteal osteoblastic cell cultures are consid-ered useful for evaluating osteoblastic alterations associatedwith bone pathology and aging [8]. Human bone-derivedcells in primary culture show a dramatic decrease in theirproliferative capacity with donor age up to the second andthird decades of life, but not over 50 years of age [9, 10].However, other investigators have shown that these cellcultures from older human subjects have a reduced prolif-eration rate after stimulation with various growth factors[11]. Recently, an age-associated decline in the total contentof the bone anabolic factor, insulin-like growth factor I(IGF-I), and the bone-specific marker osteocalcin (OC), inthe femoral neck of adult humans, has been reported [12]. Inaddition, previous studies in primary cultures of human os-teoblastic cells have shown changes in the synthesis of bonematrix proteins, e.g., proteoglycans and type I collagen, butonly until the second and the third decades of life [13, 14].So far, no changes have been detected beyond this age, ineither synthesis or secretion of various osteoblastic markers(ALP, type I collagen, and OC) in osteoblastic cells fromhuman donors [10, 11, 15].
The process of aging is known to occur differentlythroughout the skeleton [16]. Bone loss occurs predomi-nantly in the lumbar area in postmenopausal women and inthe hip in aging subjects [17]. These skeletal sites displaydifferences in the cortical/trabecular bone ratio, so that tra-becular bone predominates at the lumbar spine whereas cor-tical bone is predominant in the hip [18]. Histomorphomet-ric studies show differences in bone remodeling, dependingon skeletal sites [19]. Different therapeutic agents, e.g.,fluor and estrogens, increase the mass of trabecular bone,Correspondence to:M. E. Martınez
Calcif Tissue Int (1999) 64:280–286
© 1999 Springer-Verlag New York Inc.

which has a higher turnover rate compared with corticalbone, evaluated by histomorphometry [20, 21]. Based onthese findings, it has been hypothesized that differences ofosteoblastic differentiation exist at different skeletal sites.These differences might be accounted for by different me-chanical and/or biochemical factors in diverse bone micro-environments [22]. In this regard, recent studies have dem-onstrated differences in osteoblastic cell phenotypes [23]and in the osteoblastic response to dynamic mechanicalstrain [24], depending on their skeletal site of origin. On theother hand differences in the content of IGF-I and OC havebeen observed in cortical and trabecular bone within thesame skeletal site [12].
In the present study, we evaluated the influence of donorage and skeletal site of origin on cell proliferation and vari-ous osteoblastic markers in primary cultures of osteoblasticcells from human trabecular bone of adult donors over 50years old.
Materials and Methods
Subjects
Osteoblastic cells were isolated from fragments of human trabec-ular bone from 168 human donors (100 women and 68 men) un-dergoing knee or hip replacement for osteoarthritis. The studyprotocol was approved by the local Ethics Committee. Ninety-eight bone samples were obtained from subjects undergoing kneearthroplastia, 52 of these subjects were aged 50–70 years (64 ± 5),and 46 were over 70 (73 ± 2). Another 70 bone samples wereobtained from subjects during hip arthroplastia, 51 were aged 50–70 years (64 ± 4) and 19 were over 70 (75 ± 5). These subjects hadno clinical symptoms or history of bone metabolic disorders.
Cell Culture
Trabecular bone fragments from either the lower femur or uppertibia (knee) and from the upper femur (hip) that otherwise wouldbe discarded were cultured as previously described [25]. To assurethat there were no inflammatory elements influencing cell cultures,we also histologically reassessed five randomized bone samplesfrom which the cultures were raised. In all the cases, the tissuesshowed no findings, such as medullary fibrosis or mononuclearcell infiltrates, indicative of local or nearby inflammatory focuses.The samples were minced into pieces (0.3–0.5 cm of diameter),and then washed extensively with phosphate-buffered saline (PBS)to remove adherent bone marrow cells. The fragments were seededinto 25 cm2 tissue culture flasks and cultured in Dulbecco’s Modi-fied Eagle Medium (DMEM) containing 4.5 g/liter glucose, 15%fetal bovine serum (FBS), 100 IU/ml of penicillin, and 100mg/mlof streptomycin in a humidified atmosphere with 5% CO2. Themedium was changed twice weekly until confluence (4–6 weeks).Confluent cells were detached by trypsinization and seeded at adensity of 104 cell/cm2 into 24-well plates for evaluation of pro-liferation, and in 12-well plates for collecting the cell-conditionedmedium. These cells display various osteoblastic features such asALP and type I collagen secretion, 1,25(OH)2D3-stimulated OCsecretion, and parathyroid hormone-stimulated cAMP production[25, 26].
Cell Proliferation
Cells were trypsinized and counted in a Neubauer chamber on days6 and 13 after seeding. Cells from two wells were counted inquadruplicate. Cell proliferation was evaluated in cell poplulationsobtained from individual donor cultures. The area under the cellgrowth curve (AUC) was calculated by a trapezoidal method with
a kinetic analysis program (SIPHAR), using the cell number dataat days 6 and 13 after seeding [27].
Cell-Conditioned Medium
Cells were grown for 13 days as described above. They were thenwashed with serum-free DMEM with 1 g/liter glucose [28], andcultured for 72 hours in this medium with 10 nM vitamin K, 50mg/ml ascorbic acid, and 0.1% bovine serum albumin (BSA). Afterthis time period, the medium was removed and separated intoaliquots which were immediately frozen at −20°C. The cells werewashed in PBS and then treated with 0.1 N NaOH for 1 hour at65°C. Cell protein content in the resulting solution was determinedas described [26]. The cell-conditioned medium from two or threewells was assayed for the different markers studied, and the meanvalue from each conditioned medium was then calculated. In someexperiments, six and five cell cultures from hip and knee, respec-tively, were serum-depleted, and the treated with 10 nM1,25(OH)2D3 (kindly provided by Roche, Basel, Switzerland) [29];the conditioned medium was collected after 72 hours.
Osteocalcin Determination
OC in the cell-conditioned medium was measured in duplicate byan immunoradiometric assay (Nichols, San Juan Capistrano, CA,USA) using specific antibodies against human intact OC. Thelower detection limit of the assay is 0.6 ng/ml. The secretion of OCwas expressed as a ratio over the cell protein concentration.
C-Terminal Type I and N-Terminal Type IIIProcollagen Determination
C-terminal type I procollagen levels (PICP) are considered to be anindex of in vitro osteoblastic bone matrix formation [30]. PICP inthe cell-conditioned medium was measured using an enzyme-linked immunoassay (Metra Biosystems, Mountain View, CA,USA) [31].
N-terminal type III procollagen levels (PIIINP) were measuredin the cell-conditioned medium by radioimmunoassay (Orion Di-agnostica, Espoo, Finland) [32]. PICP and PIIINP values wereexpressed as a ratio over the cell protein concentration.
Alkaline Phosphatase Assays
ALP secretion was assayed in the cell-conditioned medium usingp-nitrophenyl phosphate as substrate [33]. The enzymatic activitywas expressed as nmol/minute (U) × mg protein.
Subconfluent hip and knee osteoblastic cell cultures in chamberslides (Nalge Nunc Int., Naperville, IL, USA) were treated with 40pM recombinant human TGFb1 and 10 nM 1,25(OH)2D3 in se-rum-free medium for 3 days, as previously described [23]. Thecells were then sequentially incubated with naphtol AS-BI and fastred violet LB diazonium salt (Sigma, St Louis, MO, USA). Thestained cells were fixed in cold ethanol and counted.
Statistical Analysis
All the data throughout the text are expressed as means ± SE,calculated from the mean values of two or three wells from eachcell culture. Differences between the values from basal and1,25(OH)2D3-treated cell cultures were analyzed by paired Wil-coxon’s test. Differences between the values of different groupswere analyzed by unpaired Student’st test.
M. E. Martınez et al.: Influence of Skeletal Origin Site and Donor Age 281

Results
Characterization of Osteoblastic Cell Cultures
We tested the response of ALP and OC to 1,25(OH)2D3, adifferentiating factor for osteoblasts [29], in our knee andhip osteoblastic cell cultures. We found that this agonistincreased ALP only in knee cultures, up to a value (60 ± 5U × mg protein) similar to that observed in nonstimulatedosteoblastic cells from the hip (71 ± 6 U × mg protein).Meanwhile, 1,25(OH)2D3 increased OC secretion in bothtypes of osteoblastic cell cultures but to a value higher inthose from knee (250 ± 40 ng/mg protein) compared withthose from hip (150 ± 30 ng/mg protein) (P < 0.05). Themajority (>70%) of cells were ALP-positive before and af-ter treatment with 10 nM 1,25(OH)2D3 and 40 pM trans-forming growth factor (TGF)b1 in both hip and knee cellcultures. In addition, PIIINP secretion, a fibroblasticmarker, was 3.2 ± 1.7 and 2.4 ± 1.1 ng/mg protein in os-teoblastic cells from either knee or hip, respectively. Thesefindings taken together indicate that osteoblastic cells arethe main cell type in our bone-derived cell cultures.
Differences in Cell Proliferation and Various OsteoblasticMarkers According to Donor Age
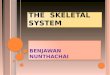
Osteoblastic cells from the older patients (>70 years old)
had a lower proliferation rate than those from the youngerpatients (50–70 years old) (Fig. 1). Furthermore, OC secre-tion by these cells was also lower in the older subjects,however, secreted ALP by osteoblastic cells was higher.PICP secretion was unchanged in osteoblastic cells fromboth age groups studied (Fig. 1).
Differences in Cell Proliferation and Various OsteoblasticMarkers According to Skeletal Site of Origin
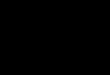
Osteoblastic cells from hip samples had a lower prolifera-tion rate than those from knee in all the subjects studied(Fig. 2). PICP secretion was also lower whereas that of ALPwas higher in the cell-conditioned medium of osteoblasticcells from the hip compared with those from the knee (Fig.2). Secreted OC was similar in osteoblastic cells from bothskeletal sites (Fig. 2). We found a significant positive cor-relation (r 4 0.308, P < 0.05) between osteoblastic cellproliferation and OC secretion in knee osteoblastic cell cul-tures.
Influence of Skeletal Site of Origin on Age-Associated Changesin Cell Proliferation and Various Osteoblastic Markers
No significant differences were observed in either cellgrowth or ALP and PICP secretion in hip osteoblastic cellsbetween both age groups studied (50–70 versus >70 years
Fig. 1. Osteoblastic growth and secretion of various osteoblasticmarkers associated with the donor age (50–70 or >70 years old) inpooled osteoblastic cultures from the hip and knee. Osteoblasticproliferation was determined as AUC calculated using the cellnumber at days 6 and 13 after seeding(A), C-terminal type I
procollagen (PICP)(B), alkaline phosphatase (ALP)(C), and os-teocalcin (OC)(D) secretion measured in conditioned medium ofosteoblastic cells in primary culture from 168 adult donors. Resultsare mean ± SE. *P < 0.05, **P < 0.001, donors aged 50–70 yearsversus >70 years, respectively.
M. E. Martınez et al.: Influence of Skeletal Origin Site and Donor Age282

old) (Table 1). However, OC secretion was significantlylower in osteoblastic cells from the hip in the older groupcompared with the younger group (Table 1).
Osteoblastic cells from the knee showed similar PICPand OC secretion in both age groups. In contrast, these cellsin the elder group had a lower proliferation rate, whereasALP secretion was significantly higher compared with theyounger group (Table 1).
In age-matched cell cultures, osteoblastic cells from thehip were found to have a lower proliferation rate and PICPsecretion than those from the knee in both age groups stud-ied (Table 1). In contrast, ALP secretion in osteoblastic cellsfrom the hip was higher in these cells from the knee in theyounger subjects. Osteoblastic cells from the older donorshad similar ALP secretion at both skeletal sites of origin(Table 1).
We found a significant correlation between osteoblasticcell growth and OC secretion (r4 0.606,P < 0.05) of kneeosteoblastic cell cultures in the younger group.
Discussion
In the present study, we found that various osteoblasticfeatures of human osteoblastic cells from donors older than50 show differences according to their skeletal site of originand donor age.
Aging is known to be associated with various changes inbone turnover. Whereas bone remodeling increases after
menopause, bone turnover gradually decreases with age inboth sexes [18]. A recent study, using electron microscopyin tibiae specimens from aging rats, has shown that age-related osteopenia is associated with a decreased number ofosteoblasts [3]. In primary cultures of human osteoblasts,cell proliferation has been shown to decrease until 30 yearsof donor age, remaining stable thereafter [9]. In addition,previous studies could not demonstrate any change in therate of DNA synthesis of human trabecular bone-derivedcells from donors between 50 and 90 years old [9, 10].However, in another study, a decreased response of thesecells to various growth factors was reported to occur withaging [11]. The bone samples from the younger donors inthe latter study were obtained from the iliac crest of womenwith breast cancer, and the other bone specimens were fromthe femoral head of patients with osteoporotic hip fracture.In the present study, using cell counting, we observed adecreased osteoblastic proliferation rate in the >70 donorsgroup. The differences observed in our study compared withthe aforementioned studies could be accounted for by thehigher accuracy of cell counting compared with [3H]thymi-dine incorporation or other colorimetric methods to assesscell proliferation. In addition, we used more subjects in thisstudy (168 specimens) compared with 20–87 samples inother studies [9–11, 15]. Moreover, our cell cultures fromhip and knee samples were from age-matched osteoarthritisdonors.
Several investigators, including us, have found a corre-lation between bone formationin vivo and osteoblastic cell
Fig. 2. Osteoblastic growth and secretion of various osteoblasticmarkers associated with the skeletal site of origin. Osteoblasticproliferation was determined as the area under the cell growthcurve (AUC) calculated using the cell number at days 6 and 13after seeding(A), C-terminal type I procollagen (PICP)(B), alka-
line phosphatase (ALP)(C), and osteocalcin (OC)(D) secretionmeasured in conditioned medium of osteoblastic cells in primaryculture from 168 adult donors. Results are mean ± SE. *P < 0.05,** P < 0.001, hip versus knee.
M. E. Martınez et al.: Influence of Skeletal Origin Site and Donor Age 283

proliferation in vitro [34–37]. To our knowledge, there areno previous studies that could find any age-related differ-ences in either synthesis or secretion of the osteoblasticmarkers ALP, type I collagen, and OC, beyond the secondand third decades of life using primary cultures of humanosteoblastic cells [10, 11, 13, 15], as reported herein. Inthese cell cultures from older (>70 years) patients we foundan increase in ALP and a decrease in OC secretion, consis-tent with a higher differentiation of osteoblastic cells.
Previous reports have demonstrated that age-relatedchanges in bone mineral content are different in severalskeletal sites [16–18]. In addition, a different effect of thera-peutic treatments on trabecular and cortical bone has beenreported in postmenopausal women with osteoporosis [18–20]. Differences in angiogenesis, mechanical strength, and/or heterogeneous cell populations associated with the typeof bone (trabecular or cortical) predominant at a particularskeletal site might account for the different bone response totreatment [38]. Recent studies have found that the expres-sion of androgenic receptors in osteoblastic cells and otherosteoblastic phenotypes depends on the skeletal site [23,39]. One of these studies [23] has shown that bone-derivedcells from mandibular and iliac crest display features con-sistent with different stages of differentiation, so that iliacosteoblastic cells exhibit higher ALP activity and lower pro-liferation rates. Furthermore, a different response to me-chanical loading [24] and a different cAMP response toPTH stimulation have been reported in primary cultures ofosteoblastic cells from different skeletal sites (iliac crest andfemoral head) [11, 23, 35].
In the present study, we found a higher proliferation rateand an increase in secreted PICP, but lower ALP secretion,in osteoblastic cells from the knee compared with these cellsfrom the hip, even in age-matched donors. We found nochanges in OC secretion between both types of cell cultures(knee and hip). OC secretion begins to occur at an interme-diate stage of osteoblastic maturation [40]. However, thefirst stages of osteoblast development,in vitro and in vivo,are associated with high proliferation, elevated type I col-lagen production, and low ALP [40]. Therefore, our find-ings are consistent with a less differentiated phenotype inosteoblastic cells from the knee than those from the hip.
Several reports support the usefulness of osteoblastic cellcultures from trabecular bone for studying bone metabolicchanges [8], mainly at the first passage [41]. We used os-teoblastic cell cultures from explants of human trabecularbone at two different skeletal sites—the hip and knee. How-ever, the trabecular/cortical bone ratio is higher in the kneecompared with the hip. Local differences in this ratio couldbe associated with the observed differences in the pheno-type of osteoblastic cells from trabecular bone at each skel-etal site. The lower ALP activity in knee osteoblastic cellcultures could be explained by the presence of a higheramount of contaminating fibroblasts in these cultures thanin hip osteoblastic cell cultures. However, this is unlikely, aswe discussed previously.
We found that osteoblastic cells from the knee had alower proliferation rate and a higher ALP secretion in theolder than in the younger donors. Thus, osteoblastic cellsfrom the knee in the younger subjects seem to display a lessmature osteoblastic phenotype than those from the olderpatients. Our findings on age-related changes in cell prolif-eration and ALP secretion support the existence of a relativeincrease of more mature osteoblasts with aging—mainly inthe knee, a predominantly trabecular type of bone.
The physiological role of OC in bone is unclear [42]. Arecent study in osteocalcin-deficient mice has shown anincreased bone formation without changes in bone resorp-tion [43]. Circulating OC in serum and OC content in bothcortical and trabecular bone appear to decrease with age [12,44]. This suggests a decreased OC secretion by osteoblastsin aged subjects. However, some investigators have notbeen able to detect changes in OC secretion by primarycultures of human osteoblastic cells from older subjectscompared with younger subjects [10, 11, 15]. Changes inbasal OC secretion by osteoblastic cells in culture are dif-ficult to assess because of the lack of sensitivity of availableOC immunoassays. This requires that a large number ofsubjects must be studied to detect small changes in OCsecretion with statistical significance. In our study, OC se-cretion decreased with age in the hip osteoblastic cell cul-tures but showed no significant variation in the knee cellcultures in both age groups studied. In agreement with theseresults, a recent study has shown a decrease in OC levels
Table 1. Osteoblastic proliferation and various osteoblastic markers depending on skeletalsite of origin and donor age
AUCPICP(mg/mg protein)
ALP(U/mg protein)
OC(ng/mg protein)
Hip50–70 years 248 ± 20a 16.2 ± 1.9a 71.0 ± 7.0a 28.5 ± 3.6b
(n 4 51)>70 years 222 ± 18a 19.3 ± 4.8a 68.7 ± 13.0 17.2 ± 2.0(n 4 19)
Knee50–70 years 350 ± 24b 28.7 ± 3.7 34.8 ± 5.2b 23.6 ± 3.8(n 4 52)>70 years 285 ± 22 25.0 ± 2.0 66.8 ± 9.3 20.6 ± 4.0(n 4 46)
The cell-conditioned medium was obtained from human osteoblastic cells from differentskeletal sites (hip or knee) and donor age (50–70 years or >70 years). Results are mean ± SE.a P < 0.05, hip versus knee cultures from age-matched donors.b P < 0.05, 50–70 versus >70 years cultures, corresponding to the same skeletal site of origin.Osteoblastic proliferation was determined as the area under the cell growth curve (AUC)calculated using the cell number at days 6 and 13 after seeding. C-terminal type I procollagen(PICP), alkaline phosphatase (ALP), osteocalcin (OC)
M. E. Martınez et al.: Influence of Skeletal Origin Site and Donor Age284

with age in the aspirated blood from the hip marrow cavity,and also in the cortical and trabecular femoral neck [12].These findings, taken together, are consistent with an age-related decrease in OC secretion in hip osteoblastic cellcultures associated with a more mature osteoblastic pheno-type.
In summary, in the present study, using osteoblastic cellsfrom human trabecular bone, we observed differences incell proliferation rate and in the maturation pattern related tothe skeletal site of origin and donor age. Hence, knee os-teoblastic cells seem to display less differentiated featuresthan those from the hip in age-matched donors. In addition,we found that age-related changes in osteoblastic cells fromthe knee and hip are different. This suggests that age-relatedbone loss depends on the skeletal site, and may be due tochanges in osteoblastic differentiation. Our findings mightoffer important insights into the understanding of the basicfeatures of bone remodeling under circumstances wheretherapeutic intervention is important, such as old age-associated osteopenia and osteoporosis.
Acknowledgments.This work was supported by grants fromFondo de Investigacio´n Sanitaria (FIS 93/313, FIS 97/0307 andCYCYT 95/0249) of Spain and Fundacio´n FAES. We thank theMedical Staff from the Orthopaedic Department Surgery Room,Hospital La Paz, for providing us with the donors’ bone samples.
References
1. Parfitt AM (1983) The physiological and clinical significanceof bone histomorphometric data. In: Recker RR (ed.) Bonehistomorphometric data: techniques and interpretation. CRCPress, Boca Rato´n, pp 143–223
2. Sherman S, Gehron Robey P, Hadley EC (1995) Aging andthe human skeleton: recomendations for research. Calcif Tis-sue Int 56 (suppl 1):S3–S4
3. Roholl PJM, Blauw E, Zurcher C, Dormans JAMA, TheunsHM (1994) Evidence for a diminished maturation of preos-teoblasts into osteoblasts during aging in arts: an ultrastruc-tural analysis. J Bone Miner Res 9:355–366
4. Hock JM, Onyia J, Bidwell J (1995) Comparisons of in vivoand in vitro models of the response of osteoblasts to hormonalregulation with aging. Calcif Tissue Int 56 (suppl 1):S44–S47
5. Inoue K, Ohgushi H, Yoshikawa T, Okumura M, Sempuku T,Tamai S, Dohi Y (1997) The effect of aging on bone forma-tion in porous hydroxyapatite: biochemical and histologicalanalysis. J Bone Miner Res 12:989–994
6. Bergman RJ, Gazit D, Kahn AJ, Gruber H, McDougall S,Hahn TJ (1996) Age-related changes in osteogenic stem cellsin mice. J Bone Miner Res 11:568–577
7. Shih MS, Cook MA, Spence CA, Palnitkar S, McElroy H,Parffit AM (1993) Relationship between bone formation rateand osteoblastic surface on different subdivisions of the end-osteal envelope in aging and osteoporosis. Bone 14:519–521
8. Marie PJ (1995) Human endosteal osteoblastic cells: relation-ship with bone formation. Calcif Tissue Int 56 (suppl 1):S13–S16
9. Shigeno Y, Ashton BA (1995) Human bone-cell proliferationin vitro decreases with human donor age. J Bone Joint Surg77B:139–142
10. Evans CE, Charles SB, Galasko B, Ward C (1990) Effect ofdonor age on the growth in vitro cells obtained from humantrabecular bone. J Orthop Res 8:234–237
11. Pfeilschifter J, Diel I, Pilz U, Brunotte K, Naumann A, ZieglerR (1993) Mitogenic responsiveness of human bone cells invitro to hormones and growth factors decreases with age. JBone Miner Res 8:707–717
12. Boonen S, Aerssens J, Dequeker J, Nicholson P, Cheng X,Lowet G, Verbeker G, Bouillon R (1997) Age-associated de-
cline in human femoral neck cortical and trabecular content ofinsulin-like growth factor I: potential implications for age-related (Type II) osteoporotic fracture occurrence. Calcif Tis-sue Int 61:173–178
13. Fedarko NS, Vetter UK, Weinstein S, Gehron Robey P (1992)Age-related changes in hyaluronan, proteoglycan, collagen,and osteonectin synthesis by human bone cells. J Cell Physiol151:215–227
14. Fedarko NS, Vetter UK, Gehron Robey P (1995) Age-relatedchanges in bone matrix structure in vitro. Calcif Tissue Int 56(suppl 1):S41–S43
15. Wong MM, Rao LG, Ly H, Hamilton L, Ish-Shalom S, Stur-tridge W, Tong J, McBroom R, Josse RG, Murray TM (1994)In vitro study of osteoblastic cells from patients with idio-pathic osteoporosis and comparison with cells from non-osteoporotic controls. Osteoporosis Int 4:21–31
16. Bonjour JP, Theintz G, Buchs B, Slosman D, Rizzoli R (1991)Critical years and stages of puberty for spinal and femoralbone mass accumulation during adolescence. J Clin Endocri-nol Metab 73:555–563
17. Davis JW, Ross PD, Wasnich RD (1994) Evidence for bothgeneralized and regional low bone mass among elderlywomen. J Bone Miner Res 9:305–309
18. Dempster DW (1992) Bone remodeling. In: Coe FL, Favus MJ(eds) Disorders of bone and mineral metabolism. Raven Press,New York, pp 355–380
19. Podenphant J, Engel U (1987) Regional variations in histo-morphometric bone dynamics from the skeleton of an osteo-porotic woman. Calcif Tissue Int 40:184–188
20. Riggs BL, Hodgson SF, O’Fallon WM (1990) Effect of fluo-ride treatment on fracture rate in postmenopausal women withosteoporosis. N Engl J Med 322:802–809
21. Lindsay R (1989) Estrogen/progesterone therapy: preventionand treatment of postmenopausal osteoporosis. Proc Soc ExpBiol Med 191:275–277
22. Heersche J, Reimers S, Denkovski P, Bellows C, Aubin J(1993) Heterogenity of osteoblasts in vivo and in vitro. In:Christiansen C, Riis B (eds) Proc 4th Int Symp Osteoporosis.Osteopress APS, Rodovre Denmark, pp 225–227
23. Kasperk C, Wergedal J, Strong D, Farley J, Wangerin K,Gropp H, Ziegler R, Baylink DJ (1995) Human bone cellphenotypes differ depending on their skeletal site of origin. JClin Endocrinol Metab 80:2511–2517
24. Rawlinson SCF, Mosley JR, Suswillo RFL, Pitsillides AA,Lanyon LE (1995) Calvarial and limb bone cells in organ andmonolayer culture do not show the same early responses todynamic mechanical strain. J Bone Miner Res 10:1225–1232
25. Martınez ME, Medina S, del Campo MT, Sa´nchez-CabezudoMJ, Sanchez M, Munuera L (1998) Effect of polyethylene onosteocalcin, alkaline phosphatase and procollagen secretion byhuman osteoblastic cells. Calcif Tissue Int 62:453–456
26. Martınez ME, Garcı´a-Ocan˜a A, Sanchez M, Medina S, DelCampo T, Valin A, Sa´nchez-Cabezudo MJ, Esbrit P (1997)C-terminal parathyroid hormone-related protein inhibits pro-liferation and differentiation of human osteoblast-like cells. JBone Miner Res 12:778–785
27. Martınez ME, Medina S, del Campo MT, Garcı´a JA, RodrigoA, Munuera L (1998) Effect of polyethylene particles on hu-man osteoblastic cell growth. Biomaterials 19:183–187
28. Inaba M, Terada M, Koyama H, Yoshida O, Ishimura E,Kawagishi T, Okuno Y, Nishizawa Y, Otani S, Morii H(1995) Influence of high glucose on 1,25-dihydroxyvitaminD3-induced effect on human osteoblast-like MG-63 cells. JBone Miner Res 10:1050–1056
29. Owen TA, Aronow MS, Barone LM, Bettencourt B, Stein GS,Lian JB (1991) Pleiotropic effects of vitamin D on osteoblastgene expression are related to the proliferative and differen-tiated state of the bone cell phenotype: dependency upon basallevels of gene expression, duration of exposure, and bonematrix competency in normal rat osteoblast cultures. Endocri-nology 128:1496–1504
30. Kassem M, Blum W, Risteli J, Mosekilde L, Eriksen EF(1993) Growth hormone stimulates proliferation and differen-
M. E. Martınez et al.: Influence of Skeletal Origin Site and Donor Age 285

tiation of normal human osteoblast-like cells in vitro. CalcifTissue Int 52:222–226
31. Melkko J, Niemi S, Risteli L, Risteli J (1990) Radioimmuno-assay of the carboxyterminal propeptide of human type I pro-collagen. Clin Chem 36:1328–1332
32. Risteli J, Niemi S, Trivedi P, Ma¨entausta O, Mowat AP, Ris-teli L (1988) Rapid equilibrium radioimmunoassay for theamino-terminal propeptide of human type III procollagen.Clin Chem 34:715–718
33. Sabokbar A, Millett PJ, Myer B, Rushton N (1994) A rapidquantitative assay for measuring alkaline phosphatase activityin osteoblastic cells in vitro. Bone Miner 27:57–67
34. Marie PJ, Sabbagh A, De Vernejoul MC, Lomri A (1989)Osteocalcin and deoxyribonucleic acid synthesis in vitro andhistomorphometric indices of bone formation in postmeno-pausal osteoporosis. J Clin Endocrinol Metab 69:272–279
35. Marie PJ, Lomri A, De Vernejoul MC, Morieux C, GrauletAM, Gueris J, Llach F (1989) Relationships between histo-morphometric features of bone formation and bone cell char-acteristics in vitro in renal osteodystrophy. J Clin EndocrinolMetab 69:1166–1173
36. Serrano S, Marin˜oso ML, Torres A, Lorenzo V, Keysers U,Lloreta J, Nacher M, Garcı´a C, Ballester J, Dı´ez A, Aubia J(1997) Osteoblastic proliferation in bone biopsies from pa-tients with end-stage chronic renal failure. J Bone Miner Res12:191–199
37. Sanchez-Cabezudo MJ, Medina S, Selgas R, Lo´pez Barea F,
Sanchez M, Bajo MA, Del Campo MT, Martı´nez ME (1997)Osteoblastic cell growth in uremic dialysis patients. Influenceof bone turnover. Bone 20 (suppl. 4):75S
38. Ninomija JT, Tracy RP, Calore JD, Gendreau MA, Kelm RJ,Mann KG (1990) Heterogeneity of human bone. J Bone MinerRes 5:933–938
39. Kasperk C, Helmboldt A, Borcsok I, Heuthe S, Cloos O, Ni-ethard F, Ziegler R (1997) Skeletal site-dependent expressionof the androgen receptor in human osteoblastic cell popula-tions. Calcif Tissue Int 61:646–673
40. Stein GS, Lian JB, Stein JL, Van Wijnen AJ, Mortecino M(1996) Transcriptional control of osteoblast growth and dif-ferentiation. Physiol Rev 2:593–622
41. Chavassieux PM, Chenu C, Valentin-Opran A, Merle B, Del-mas PD, Hartmann DJ, Saez S, Meunier PJ (1990) Influenceof experimental conditions on osteoblast activity in humanprimary bone cell cultures. J Bone Miner Res 5:337–343
42. Calvo MS, Eyre DR, Gundberg CM (1996) Molecular basisand clinical application of biological markers of bone turn-over. Endocr Rev 17:333–368
43. Ducy P, Desbois C, Boyce B, Pinero G, Story B, Dunstan C,Smith E, Bonadio J, Goldstein S, Gundberg C, Bradley A,Karsenty G (1996) Increased bone formation in osteocalcin-deficient mice. Nature 382:448–452
44. Vanderschueren D, Gevers G, Raymaekers G, Devos P, De-queker J (1990) Sex- and age-related changes in bone andserum osteocalcin. Calcif Tissue Int 46:179–182
M. E. Martınez et al.: Influence of Skeletal Origin Site and Donor Age286