Embed Size (px)
Citation preview

JAPI • VOL. 51 • JULY 2003 695
Update Article
Insulin in Sepsis and Septic ShockUndurti N Das
AbstractNF-kB activation, and elevated concentrations of macrophage migration inhibitory factor (MIF), tumornecrosis factor-α (TNF-α), interleukin-1(IL-1), IL-6, free radicals, inducible nitric oxide (iNO), andstress hyperglycemia occurs in sepsis and this leads to systemic inflammatory response and myocardialdepression seen in sepsis and septic shock. Conversely, insulin suppresses production of MIF, TNF-α,IL-1, IL-6, and free radicals, enhances endothelial NO generation, and enhances the production of anti-inflammatory cytokines IL-4, and IL-10, corrects stress hyperglycemia and improves myocardial function.This supports my earlier proposal that insulin (with or without glucose and potassium) therapy tomaintain euglycemia suppresses the inflammatory response, improves myocardial function, and thus, isof benefit in acute myocardial infarction, sepsis and septic shock.
INTRODUCTION
Serious infections and some noninfectious disorders suchas trauma, pancreatitis, and following major abdominal
and cardiovascular surgery trigger systemic inflammatoryresponse or sepsis and when this results in hypotension andmultiorgan dysfunction, it is referred to as septic shock.1,2
Septic shock is due to inappropriate increase in innate immuneresponse by neutrophils, macrophages, and natural killer (NK)cells.
Pathobiology of sepsis and septic shock
Gram-positive and Gram-negative organisms, malarialparasite, fungi, endotoxin-containing organisms and othermicrobials proliferate and produce bacteremia and/or releasetoxins that stimulate the innate immune system, endothelialcells and other cells.1 These cells release interleukin-1 (IL-1),IL-2, IL-6, IL-8, tumor necrosis factor-α (TNF-α), plateletactivating factor (PAF), endorphins, eicosanoids, nitric oxide(NO), oxygen free radicals, high mobility group 1 (HMG1),macrophage migration inhibitory factor (MIF), andchemokines. As a result of the action of various cytokinesand chemokines, the expression of various adhesionmolecules is enhanced. ILs, TNF-α, MIF, eicosanoids, andoxygen free radicals have profound effects on thecardiovascular system, kidneys, lungs, liver, central nervoussystem, and coagulation cascade (see Fig. 1). As a resultrenal failure, myocardial dysfunction, acute respiratorydistress syndrome (ARDS), hepatic failure, and disseminated
Department of Nutrition and Surgery, SUNY Upstate MedicalUniversity Syracause, NY, USA. EFA Sciences LLC, 1420 ProvidenceHighway, Suite # 266, Norwood, MA 02062,USA.Invited ArticleReceived : 14.6.2003; Accepted :16.6.2003
intravascular coagulation occur that may result in death.1,2
Both anti-TNF monoclonal antibody and IL-1 receptorantagonist are of no benefit in sepsis (reviewed in1,3). Thissuggests that new therapeutic strategies are necessary inthe management of sepsis and septic shock.
Mediators in sepsis and septic shock
MIF, TNF-α, and ILs stimulate phospholipases inducingthe release of AA, the precursor of 2 series prostaglandins(PGs) and 4 series leukotrienes (LTs), and the production offree radicals and inducible nitric oxide (iNO), which have potentpro-inflammatory actions.1 Members of the NF-kB (nuclearfactor-(appa B) family are induced by cytokines and freeradicals, which have a significant role in sepsis and septicshock. Patients who succumb to sepsis showed increasedNF-kB activity that correlated with the APACHE-II scorecompared to those who recovered from sepsis.4-6 This led tothe suggestion that suppression of NF-kB activity may be ofbenefit in sepsis and septic shock. But, transgenic animalsexpressing degradation-resistant IkBα in hepatocytes resultsin obstruction of NF-kB activation and were unable to clearListeria monocytogenes from the liver and succumbed tosepsis and septic shock.7 On the other hand, adenosine,adenosine receptors and inosine have anti-inflammatoryactions and their use improved survival of LPS-challengedanimals.8-10 These are independent of the degradation of I-kBα and NF-kB activation. Furthermore, NF-kB, IL-6,adenosine, inosine, and adenosine receptor agonists arenecessary for the resolution of inflammation.11,12 In thiscontext, it is important to note that IL-10 and TGF-ß are anti-inflammatory cytokines that may mediate resolution ofsepsis.2,13,14 Based on this, it is suggested that normally adelicate balance exists between pro- and anti-inflammatorymolecules and when this balance is tilted more in favor of

696 JAPI • VOL. 51 • JULY 2003
pro-inflammatory molecules it results in sepsis and septicshock (Fig. 1). If so, restoring this balance is important toresolve and enhance recovery from sepsis and septic shock.
INSULIN RESISTANCE OCCURS IN SEPSIS AND
SEPTIC SHOCK
Insulin resistance is common in septic shock.1,15 Early
hyperglycemic and later hypoglycemic phases occur in sepsisand septic shock. In sepsis glucose utilization rate in responseto insulin infusion is decreased compared to control subjects,16
suggesting impaired insulin action in sepsis. This is due adecrease in whole-body glucose uptake with lack of responseto the elevated insulin levels. Glucose uptake is elevatedduring the euglycemic and hypoglycemic stages of sepsisand is independent of changes in glucose and insulin.17
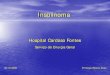
Fig. 1. Scheme showing the relationship between various mediators and inhibitors of septic shock and their relationship to insulin. The closeinteraction between various molecules shown here attests to the fact that sepsis and septic shock is a complicated process. (+) Indicates increase information/synthesis, action, or an active participant in the induction of septic shock. (-) Indicates inhibition of formation/synthesis, action or inhibition
of septic shock. ? Indicates the action is not clear. DIC = Disseminated intravascular coagulation. LPS = Lipopolysaccharide.OxPL/OxPAPC = Oxidized phospholipids. LCPUFAs= Long-chain polyunsaturated fatty acids. OX=cyclo-oxygenase

JAPI • VOL. 51 • JULY 2003 697
Insulin resistance in sepsis could be in response to elevatedconcentrations of TNF-α, IL-1, IL-2, and/or IL-6. In theeuglycemic or hypoglycemic phases of sepsis glucose uptakeis enhanced secondary to increased glucose transporterprotein-1 (GLUT-1) receptor expression that is preferentiallymetabolized to lactate.18 The elevated basal serum lactate,glucose, and insulin in the critically ill can be correlated withthe APACHE-II score.19 Further, they show increase in serumglucose, free fatty acids (FFA), glycerol, and triacylglycerol,very low-density lipoprotein, and low-density lipoprotein anda substantial decrease in high-density lipoprotein cholesterol.In those who did not survive due to sepsis also have elevatedserum lactate and free glycerol, indicators of lipolysiscompared with survivors. This suggests that glucose andlipid metabolism that is influenced by insulin, is altered insepsis. Hence, these parameters may be used as markers topredict prognosis in those with sepsis. These disturbancesin glucose and lipid metabolism are due to the developmentof insulin receptor autoantibodies, insulin-like effect ofendotoxin, perturbation by endotoxin of insulin action at thecellular level, and alterations in insulin secretion pattern. Thepresence of insulin resistance and altered insulin homeostasisin sepsis is as a result of diminished insulin-stimulatedphosphorylation of insulin receptor, insulin-receptorsubstrate-1, and mitogen-activated protein kinase byendotoxin.20 Low insulin levels seen in these patients in theearly stages of sepsis are caused by increased clearance andnot due to decreased production,21 and alterations incorticosterone levels.22
Insulin resistance seen in sepsis can be restored tonormalcy by infusing insulin continuously. Studies revealedthat in the early phase of sepsis (i.e., first 0.5-1 hour period asstudied by using cecal ligation and puncture technique),plasma glucose levels increased, whereas plasma insulin andglucagon levels remained unchanged, but corticosteronelevels increased 2.5 fold over control values.23 At the end of20 hours, plasma glucose levels returned to normal, whereasinsulin, glucagon, and corticosterone levels increasedsignificantly, i.e., 40-fold, 6.5 fold, and 6-fold respectively.Thus the initial rise and subsequent decline in blood glucoselevels depends to a large extent on the balance between plasmainsulin and corticosterone concentrations. In view of this,continuous infusion of insulin (without inducinghypoglycemia or hypokalemia) might enhance tissue glucoseuptake, suppress lactate, FFA, glycerol production, andlipolysis, and overcome corticosterone-induced insulinresistance19,21,23 and improve tissue perfusion and recovery.1,25
This is similar to the administration of insulin for diabeticketoacidosis (DKA). Most patients with DKA are traditionallytreated by “low-dose” insulin schedules in which 8 to 10units of insulin (approximately 0.01 units/kg body weight)are infused continuously each hour. Most subjects with DKArespond adequately to this low-dose insulin regimen. Butsome patients do not respond to this regimen, presumablydue to insulin resistance, and are given 25 to 50 units ofinsulin as an intravenous bolus, followed by an infusion of
15 to 25 units an hour (0.02 to 0.05 units/kg body weight)until ketosis is reversed. This higher-dosage schedule isbelieved to saturate insulin receptors in the face of competingantibodies or other resistance factors. High concentrationsof insulin reverse diabetic ketoacidosis by acting via theinsulin-like growth factor receptor, by a mechanismindependent of the receptor. In the same fashion, even insepsis and septic shock, continuous administration of theinsulin in the form of glucose-insulin-potassium (GIK) regimenis likely to enhance tissue perfusion and glucose uptake;suppress lactate, FFA, glycerol production, and lipolysis andimprove survival1.24 The purpose of giving glucose andpotassium simultaneously with insulin is to prevent theoccurrence of hypoglycemia and hypokalemia. But, in theevent plasma glucose levels are carefully and continuouslymonitored, perhaps, continuous insulin infusion alone maybe adequate.
CARDIAC DYSFUNCTION IN SEPSIS AND ITS
REVERSAL BY INSULIN
Myocardial depression is common in sepsis and septicshock. Several studies showed that GIK regimen improvesmyocardial function during sepsis and septic shock byincreasing cardiac output, stroke volume, arterial pressure,and oxygen consumption.24,25 Cardiac dysfunction thatoccurred within 2 to 4 hours post-endotoxin was not relatedto arterial-blood glucose concentrations.25 On the other hand,intraarterial infusions of insulin at rates of 6 units/minutereversed all signs of myocardial failure and maintained normalperformance25,26 despite wide ranges in glucoseconcentrations (5-120 mg%). This suggests that it is insulinthat improves cardiac performance and that myocardialdysfunction is not due to hypoglycemia of septic or endotoxinshock. These results also suggested that the beneficial actionsof insulin on cardiac performance are due to mechanismsother than myocardial glucose transport.
Several animal and clinical studies suggested that GIKregimen preserved systolic and diastolic function in ischemiaand reperfusion27 and protects the myocardium in patientsundergoing open-heart surgery, although this is not withoutcontroversy. It is not clear why some studies showed positiveresults whereas others failed to show a benefit from the GIKregimen against myocardial dysfunction in septic shock. Ona closer examination of these studies, it was noted that thiscould be due to the different doses of glucose and insulinused in various protocols.
For instance, Mauritz et al28 used glucose 70%, 1g/kg andinsulin 1.5 units/kg, whereas Bronsveld et al29 employedglucose 50%, 1g/kg and insulin 1.5 units/kg. Mauritz et alnoted that their patients did develop hyperglycemia followingGIK regimen since they used a lower dose of insulin relativeto the concentration of glucose infused compared toBronsveld et al. It is evident that studies30 in which higherconcentrations of insulin were used showed better resultsthan did those studies that employed lesser dose. Since stress

698 JAPI • VOL. 51 • JULY 2003
hyperglycemia or even mild hyperglycemia with myocardialinfarction is associated with increased mortality31 and thatintensive insulin treatment to maintain blood glucose levelsbetween 80 and 110 mg/dl is highly beneficial and reducesmorbidity and mortality among critically ill,32 the negativeresults obtained with GIK regimen can be related to the lowdose of insulin used that invariably resulted in hyperglycemia(< 110mg/dl) that is detrimental to the myocardium.33
It is common knowledge that continuous intravenousinfusion of insulin is superior to subcutaneous administrationto control hyperglycemia, especially in patients with diabetesmellitus during the preoperative and postoperative periods.34
Improved diabetic control results in fewer wound infectionsand better wound healing. Earlier, I suggested that thebeneficial effects of GIK regimen might extend beyond thecontrol of hyperglycemia alone.24,30,33,35,36 GIK infusion maysalvage myocardium, improve cardiac function, and decreasemortality by an absolute 10%, provided that hyperglycemiais prevented.37,38 This beneficial effect is independent ofglucose. A large trial32 conducted in a heterogeneous groupof 1548 critically ill patients, in which it was noted thatintensive insulin therapy to maintain blood glucose < 110mg/dl in predominantly nondiabetic patients admitted tosurgical intensive care units and receiving mechanicalventilation showed a decrease in morbidity and mortality ascompared with less intensively treated patients (blood glucosemaintained between 180 and 200 mg/dl). In this study, it wasalso observed that intensive insulin therapy was associatedwith a decrease in pro-inflammatory markers compared to thecontrol. This suggests that maintaining blood glucoseconcentrations < 110 mg/dl is critical to derive the benefits ofinsulin treatment and reverse the inflammatory process incritically ill. This is supported by the observation that cardiacdysfunction induced by endotoxin administration was notrelated to arterial blood glucose concentrations, and thatinfusions of insulin but not glucose reversed cardiac failureand maintained normal performance.25,26 American College ofCardiology and the American Heart Associationrecommended intravenous GIK be given to patients with acutemyocardial infarction (AMI), especially those who are poorcandidates for thrombolytic therapy and in whom the risk forbleeding is high,39 because the GIK regimen is beneficial intreating AMI. GIK treatment improves the integrity andfunction of myocardial cells once glucose and potassium aretransported in by insulin.
HYPERGLYCEMIA AND INSULIN IN
INFLAMMATION
Hyperglycemia increases the production of reactiveoxygen species inside cultured aortic endothelial cells.40
Superoxide anion (O2-.) inactivated both eNO and prostacyclin
(PGI2), which are potent vasodilators and platelet anti-
aggregators.41 Free radicals are cytotoxic to myocardial cellsand suppress myocardial function. Thus, free radicals induceendothelial and myocardial dysfunction. Glucose challengestimulated reactive oxygen species generation in
polymorphonuclear leukocytes and monocytes, even inotherwise normal subjects.42 High glucose concentrationsenhanced leukocyte rolling; adherence, and transmigrationwith attenuation of eNO release, and increase expression ofP-selectin on endothelial surfaces.43 Insulin not onlyattenuated these pro-inflammatory effects but also inhibitedreactive oxygen species generation, and NF-kB inmononuclear cells, and reduced soluble intercellular adhesionmolecule-1 (ICAM-1), monocyte chemoattractant protein-1(MCP-1) and plasminogen activator inhibitor-1 productionby augmenting NO generation,33,35,36,44 suggesting thathyperglycemia triggers and accentuates inflammation whereasinsulin prevents inflammation.33,45 One potential mechanismby which glucose initiated and perpetuates inflammationinclude its ability to stimulate the production of TNF-α, apotent pro-inflammatory molecule, which is capable ofactivating NADPH-dependent oxidase, and enhance NF-kBand ICAM-1 expression.33,46 These pro-inflammatory actionsof glucose could be responsible for the increased morbidityand mortality seen in patients with AMI exhibitinghyperglycemia.
On the other hand, insulin suppresses NF-kB expression,free radical generation, MIF production, IL-1, IL-6, andenhances eNO generation33,35,44,45,47 and thus, inhibitsinflammatory process. Insulin inhibited TNF-α production,48
and reversed the toxic effects of cachectin (TNF-α) in liver,lungs, kidney and spleen.49 This explains why intensive insulintherapy and GIK regimen are beneficial in critically ill, AMI,and sepsis and septic shock.
CONCLUSIONS AND THERAPEUTIC
IMPLICATIONS
Activation of NF-kB, and enhanced formation of TNF-α,MIF, and other pro-inflammatory cytokines, free radicalgeneration and iNO occurs in sepsis and septic shock. Thefailure of monoclonal anti-TNF-α antibody to show anysignificant benefit in sepsis and septic shock led to thesuggestion that there could be a major role for other moleculesin this condition. In this context, the anti-inflammatory actionsof insulin are note worthy. Many physicians are familiar withthe use of insulin. Hence, it is not difficult to extend insulintherapy to sepsis and septic shock. It is also likely that insulinalone may not be of sufficient benefit for sepsis and septicshock, partly because many mediators are involved in thisprocess. For instance, adenosine restores myocardialresponsiveness to insulin during acute endotoxin shock,50
suggesting that its co-administration along with insulin needto be considered in sepsis and septic shock. Both adenosineand insulin are not only endogenous natural molecules butare also capable of suppressing NF-k Bexpression and TNF-α production and thus, antagonizeinflammatory events. It is interesting to note that adenosineand insulin enhance wound healing.51 Hence, combined useof insulin and adenosine might be of significant benefit insepsis and septic shock.
Any one single drug or molecule is unlikely to be of

JAPI • VOL. 51 • JULY 2003 699
significant benefit in sepsis due to its complex nature. Inview of this, a combination of endogenous anti-inflammatorymolecules such as insulin, adenosine, w-3 fatty acids, andactivated protein C need to be tried for their possible use insepsis and septic shock (see Fig. 1), a condition for which nosatisfactory therapy is available at present.
REFERENCES
1. Das UN. Critical advances in septicemia and septic shock.Crit Care 2000;4:290-294.
2. Webb S. The role of mediators in septicemia resolution. AdvSepticemia 2002;2:8-14.
3. Abraham E. Why immunomodulatory therapies have notworked in septicemia? Intensive Care Med 1999;25:556-66.
4. Foulds S, Galustian C, Mansfield AO, Schachter M.Transcription factor NFêB expression and posrsurgical organdysfunction. Ann Surg 2001;233:70-8.
5. Paterson RL, Galley HF, Dhillon JK, Webster NR. Increasednuclear factor êB activation in critically ill patients who die.Crit Care Med 2000;28:1047-51.
6. Bohrer H, Qiu F, Zimmermann T, Zhang Y, Jllmer T, MannelD, Bottiger BW, Stern DM, Waldherr R, Saeger H-D, ZieglerR, Bierhaus A, Martin E, Nawroth PP. Role of NFêB in themortality of sepsis. J Clin Invest 1997;100:972-85.
7. Lavon I, Goldberg I, Amit S, Landsman L, Jung S, Tsuberi B-Z,Barshack I, Kopolovic J, Galun E, Bujard H, Ben-Neriah Y.High susceptibility to bacterial infection, but no liverdysfunction, in mice compromised for hepatocyte NF-êBactivation. Nature Med 2000;6:573-77.
8. Cronstein BN. Adenosine, an endogenous anti-inflammatoryagent. J Appl Physiol 1994;76:5-13.
9. Hasko G, Kuhel DG, Nemeth ZH, Mabley JG, StachlewitzRF, Virag L, Lohinai Z, Southan GJ, Salzman AL, Szabo C.Inosine inhibits inflammatory cytokine production by aposttranscriptional mechanism and protects againstendotoxin-induced shock. J Immunol 2000;164:1013-19.
10. Firestein GS, Boyle D, Bullough DA, Gruber HE, Sajjadi FG,Montag A, Sambol B, Mullane KM. Protective effect of anadenosine kinase inhibitor in septic shock. J Immunol1994;152:5853-59.
11. Lawrence T, Gilroy DW, Colville-Nash PR, Willoughby DA.Possible new role for NF-êB in the resolution of inflammation.Nature Med 2001;7:1291-97.
12. Gilroy DW, Colville-Nash PR, Willis D, Chivers J, Paul-ClarkMJ, Willoughby DA. Inducible cyclo-oxygenase may have anti-inflammatory properties. Nature Med 1999;5:698-701.
13. Marchant A, Deviere J, Byl B, DeGroote D, Vincent JL,Goldman M. Interleukin-10 production during septicemia.Lancet 1994;343:707-8.
14. Das UN. Transforming growth factor-beta: Is it anendogenous cardioprotector? Med Sci Res 1993;21:373-5.
15. Lang CH, Dobrescu C. In vivo insulin resistance duringnonlethal hypermatebolic sepsis. Circ Shock 1989;28:165-78.
16. Chambrier C, Laville M, Rhzioual Berrada K, Odeon M,Bouletreau P, Beylot M. Insulin sensitivity of glucose and fatmetabolism in severe sepsis. Clin Sci (Colch) 2000;99:321-8.
17. Maitra SR, Wojnar MM, Lang CH. Alterations in tissue glucoseuptake during the hyperglycemic and hypoglycemic phases ofsepsis. Shock 2000;13:379-85.
18. Vary TC, Drnevich D, Jurasinski C, Brennan WA Jr.
Mechanisms regulating skeletal muscle glucose metabolismin sepsis. Shock 1995;3:403-10.
19. Lind L, Lithell H. Impaired glucose and lipid metabolism seenin intensive care patients is related to severity of illness andsurvival. Clin Intensive Care 1994;5:100-5.
20. Fan J, Li YH, Wojnar MM, Lang CH. Endotoxin-inducedalterations in insulin-stimulated phosphorylation of insulinreceptor, IRS-1, and MAP kinase in skeletal muscle. Shock1996;6:164-70.
21. Dahn MS, Lange MP, Mitchell RA, Lobdell K, Wilson RF.Insulin production following injury and sepsis. J Trauma1987;27:1031-38.
22. Raymond RM, Harkema JM, Emerson TE Jr. In vivo skeletalmuscle insulin resistance during E coli endotoxin shock inthe dog. Circ Shock 1981;8:425-33.
23. Maitra SR, Wang S, Baithwaite CE, El-Maghrabi MR.Alterations in glucose-6-phosphatase gene expression insepsis. J Trauma 2000;49:38-42.
24. Das UN. Possible beneficial action(s) of glucose-insulin-potassium regimen in acute myocardial infarction andinflammatory conditions: a hypothesis. Diabetologia2000;43:1081-82.
25. Hinshaw LB, Archer LT, Benjamin B, Bridges C. Effects ofglucose or insulin on myocardial performance in endotoxinshock. Proc Soc Exp Biol Med 1976;152:529-34.
26. Archer LT, Beller BK, Drake JK, Whitsett TL, Hinshaw LB.Reversal of myocardial dysfunction in endotoxin shock withinsulin. Can J Physiol Pharmacol 1978;56:132-8.
27. Zhu P, Lu L, Xu Y, Greyson C, Schwartz GG. Glucose-insulin-potassium preserves systolic and diastolic function inischemia and reperfusion in pigs. Am J Physiol Heart Circ Physiol2000;278:H595-603.
28. Mauritz W, Schindler I, Zadrobilek E, Sporn P. Glucose-potassium-insulin in hypodynamic septic shock. Anaesthetist1986;35:623-27.
29. Bronsveld W, van den Bos GC, Thijs LG. Use of glucose-insulin-potassium (GIK) in human septic shock. Crit Care Med1985;13:566-70.
30. Das UN. Insulin: an endogenous cardioprotector. CurrentOpinion in Critical Care, in press.
31. Capes SE, Hunt D, Malmberg K, Gerstein HC. Stresshyperglycemia and increased risk of death after myocardialinfarction in patients with and without diabetes: a systematicoverview. Lancet 2000;355:773-8.
32. Van den Berghe G, Wouters P, Weekers F, Verwaest C,Bruyninckx F, Schetz M, Vlasselaers D, Ferdinade P, LauwersP, Buillon R. Intensive insulin therapy in critically ill. N Engl JMed 2001;345:1359-67.
33. Das UN. Is insulin an endogenous cardioprotector? Crit Care2002;6:389-93.
34. Christiansen CL, Schurizek BA, Malling B, Knudsen L, AlertiKG, Hermansen K. Insulin treatment of the insulin-dependentdiabetic patient undergoing minor surgery. Continuousintravenous infusion compared with subcutaneousadministration. Anaesthesia 1988;43:533-7.
35. Das UN. Is insulin an anti-inflammatory molecule? Nutrition2001;17:409-413.
36. Das UN. Insulin and the critically ill. Crit Care 2002;6:262-3.37. Diaz R, Paolasso EA, Piegas LS, Tajer CD, Moreno MG,
Corvalan R, Isea JE, Romero G. Metabolic modulation ofacute myocardial infarction. The ECLA (Estudios

700 JAPI • VOL. 51 • JULY 2003
Cardiologicos Latinoamerica) Collaborative Group. Circulation1998;98:2227-34.
38. Van Campen CMC, Klein LJ, Visser FC. Glucose-insulin-potassium imaging: the past and the future? Heart Metabol2001;12:14-18.
39. Ryan TJ, Antman EM, Brooks NH, Califf RM, Hillis LD, HiratzkaLF, Rapaport E, Riegel B, Russell RO, Smith EE III, WeaverWD, Gibbons RJ, Alpert JS, Eagle KA, Garner TJ, Garson AJr, Gregoratos G, Smith SC Jr. 1999 update: ACC/AHAGuidelines for the Management of Patients with AcuteMyocardial Infarction: Executive Summary andRecommendations: A report of the American College ofCardiology/American Heart Association Task Force onPractice Guidelines (Committee on Management of AcuteMyocardial Infarction). Circulation 1999;100:1016-30.
40. Giardino I, Edelstein D, Brownlee M. BCL-2 expression orantioxidants prevent hyperglycemia-induced formation ofintracellular advanced glycation end products in bovineendothelial cells. J Clin Invest 1996;97:1422-28.
41. Das UN. Free radicals, cytokines and nitric oxide in cardiacfailure and myocardial infarction. Mol Cell Biochem2000;215:145-52.
42. Mohanty P, Hamouda W, Garg R, Aljada A, Ghanim H,Dandona P. Glucose challenge stimulates reactive oxygenspecies (ROS) generation by leukocytes. J Clin Endocrinol Metab2000;85:2970-73.
43. Booth G, Stalker TJ, Lefer AM, Scalia R. Elevated ambientglucose induces acute inflammatory events in the
microvasculature: effects of insulin. Am J Physiol 2001;280:E848-56.
44. Aljada A, Ghanim H, Saadesh R, Dandona P. Insulin inhibitsNFkB and MCP-1 expression in human aortic endothelialcells. J Clin Endocrinol Metab 2001;86:450-3.
45. Das UN. Insulin and inflammation: further evidence anddiscussion. Nutrition 2002;18:526-7.
46. Guzik TJ, Mussa S, Gastaldi D, Sadowski J, Ratnatunga C,Pillai R, Channon KM. Mechanisms of increased vascularsuperoxide production in human diabetes mellitus. Circulation2002;105:1656-62.
47. Eschke MG, Einspanier R, Klein D, Jauch K-W. Insulinattenuates the systemic inflammatory response to thermaltrauma. Mol Medicine 2002;8:443-50.
48. Satomi N, Sakurai A, Haranaka K. Relationship ofhypoglycemia to tumor necrosis factor production andantitumor activity: role of glucose, insulin, and macrophages.J Natl Cancer Inst 1985;74:1255-60.
49. Fraker DL, Merino MJ, Norton JA. Reversal of the toxiceffects of cachectin by concurrent insulin administration. AmJ Physiol 1989;256(6 Pt 1):E725-31.
50. Law WR, McLane MP, Raymond RM. Adenosine restoresmyocardial responsiveness to insulin during acute endotoxinshock in vivo. Circ Shock 1989;28:333-45.
51. Montesinos MC, Gadangi P, Longaker M, Sung J, Levine J,Nilsen D, Reibman J, Li M, Jinag C-K, Hirschhorn R, RechtPA, Ostad E, Levin RI, Cronstein BN. Wound healing isaccelerated by agonists if adenosine A2 (Gas-linked)receptors. J Exp Med 1997;186:1615-20.