Embed Size (px)
Citation preview
JHS Ebola Education Clinical Staff
2014 Mandatory Education
Please note…
Due to the dynamic nature of managing the Ebola Virus… • New information and guidelines may occur daily • The information in this learning module is based on CDC, WHO,
OSHA, and JHS policies as of October 20, 2014
Objectives
At the end of the presentation, the participant will be able to: • Explain the Ebola Virus Disease (EVD) transmission, signs and
symptoms, diagnosis, and treatment • Verbalize the risk and levels of exposure to EVD • List the process for screening, evaluating, and testing a person
under investigation for EVD • Perform correct sequence for donning on and off of personal
protective equipment (PPE) • Identify key concepts regarding EVD patient care considerations as
related to infection control for equipment, environment, specimen collection, transport, and post mortem care
Center for Disease Control (CDC) - Ebola Key Points
• The 2014 Ebola Outbreak is the largest in history • There are at least two different strands of the Ebola virus in Africa • World Health Organization (WHO) declared the current Ebola outbreak is
a Public Health Emergency of International Concern (PHEIC) • CDC and WHO are working with the affected countries to address the
Ebola outbreak • A person infected with Ebola is not contagious until symptoms appear • Healthcare providers should be alert for and evaluate any patients who
may have Ebola virus disease (EVD) • Obtaining patients’ recent travel history is mandatory for clinical staff
Evaluate all patients recent travel to West Africa within the last 21 days from symptom onset
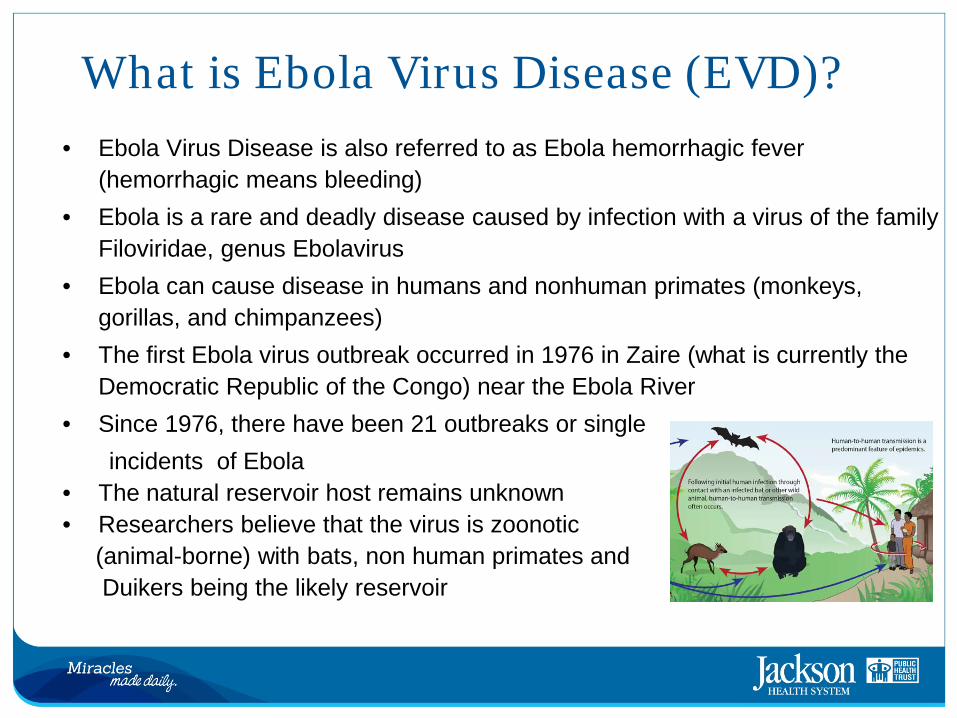
What is Ebola Virus Disease (EVD)? • Ebola Virus Disease is also referred to as Ebola hemorrhagic fever
(hemorrhagic means bleeding) • Ebola is a rare and deadly disease caused by infection with a virus of the family
Filoviridae, genus Ebolavirus • Ebola can cause disease in humans and nonhuman primates (monkeys,
gorillas, and chimpanzees) • The first Ebola virus outbreak occurred in 1976 in Zaire (what is currently the
Democratic Republic of the Congo) near the Ebola River • Since 1976, there have been 21 outbreaks or single incidents of Ebola • The natural reservoir host remains unknown • Researchers believe that the virus is zoonotic (animal-borne) with bats, non human primates and Duikers being the likely reservoir
Transmission • Disease cannot be spread until a person develops signs and/or symptoms of Ebola • Transmission has not been documents to occur in humans via food, water, or
air • Ebola can be spread by direct contact (broken skin or mucous membranes)
with: – Body fluids (blood, vomit, urine (pee), feces (poop), sweat, semen, spit,
tears, and breast milk of a person who is sick with or has died from EVD – Objects such as needles, medical equipment, linen, trash that is contaminated
with EVD – Animals infected with EVD and contact with the blood, fluids, or infected
meat of the animal – “Bushmeat” refers to meat that comes from wild animals captured in Africa
o Bushmeat is illegal in the United States o Ebola is not generally spread through food, but hunting, butchering, and
processing bush meat brings people into contact with blood/other fluids of potentially infected animals.
Signs and Symptoms • Ebola can only be spread to others after symptoms begin • Symptoms usually begin 8 to 10 days after a person has been exposed
– However, symptoms may begin anywhere from 2 to 21 days after the exposure
• Early signs and symptoms may include: – Fever (temperature greater than 101.5 F or 38.6 C) – Weakness or fatigue – Lack of appetite – Vomiting or diarrhea – Headache – Stomach pain – Joint or muscle pain
• Some people may also experience: – Chest pain – Cough or sore throat – Difficulty breathing or swallowing – Red eyes, conjunctivitis – Hiccups – Rash – Unexplained bleeding or bruising
Symptoms become increasingly severe mental confusion, bleeding inside and outside the body, shock, and multi-organ failure
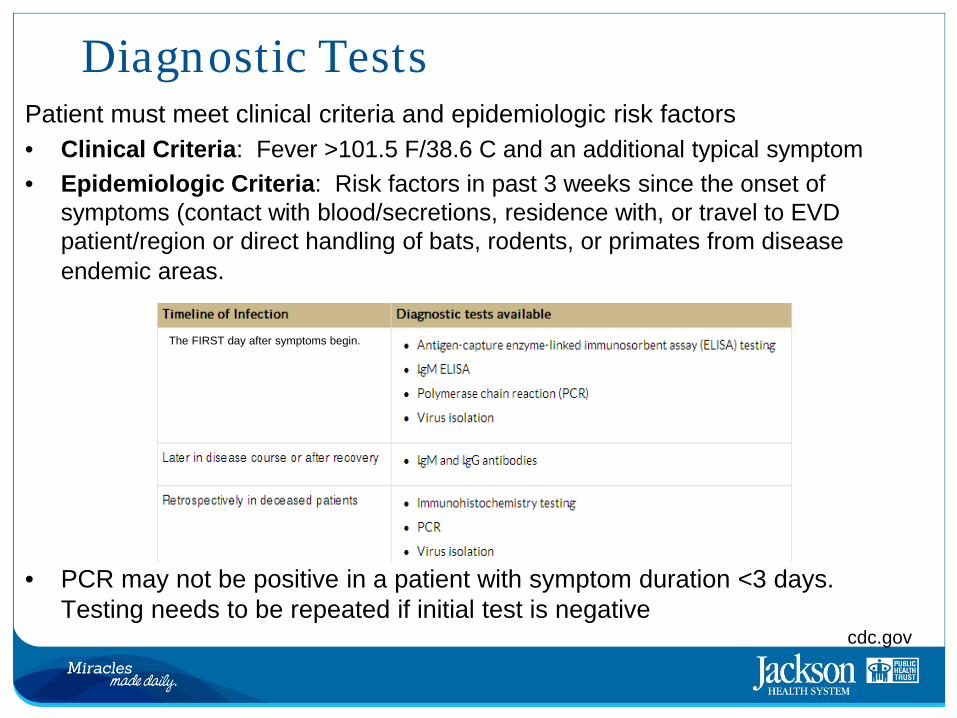
Diagnostic Tests Patient must meet clinical criteria and epidemiologic risk factors • Clinical Criteria: Fever >101.5 F/38.6 C and an additional typical symptom • Epidemiologic Criteria: Risk factors in past 3 weeks since the onset of
symptoms (contact with blood/secretions, residence with, or travel to EVD patient/region or direct handling of bats, rodents, or primates from disease endemic areas.
• PCR may not be positive in a patient with symptom duration <3 days.
Testing needs to be repeated if initial test is negative cdc.gov
The FIRST day after symptoms begin.
Treatment
Patient must be placed on isolation: • Standard, Contact, and Airborne Precautions as per JHS Bio-
emergency Plan • Standard treatment for Ebola is still limited to supportive therapy that
consists of: – Balancing the patient’s fluids and electrolytes – Maintaining the patient’s oxygen status and blood pressure – Treating the patient for any complicating infections
• Timely treatment is important yet challenging because Ebola is difficult to diagnose clinically in the early stages due to the nonspecific signs and symptoms
• Currently vaccinations are being developed by the U.S. and Canada • Experimental drugs may be obtained with CDC/FDA approval
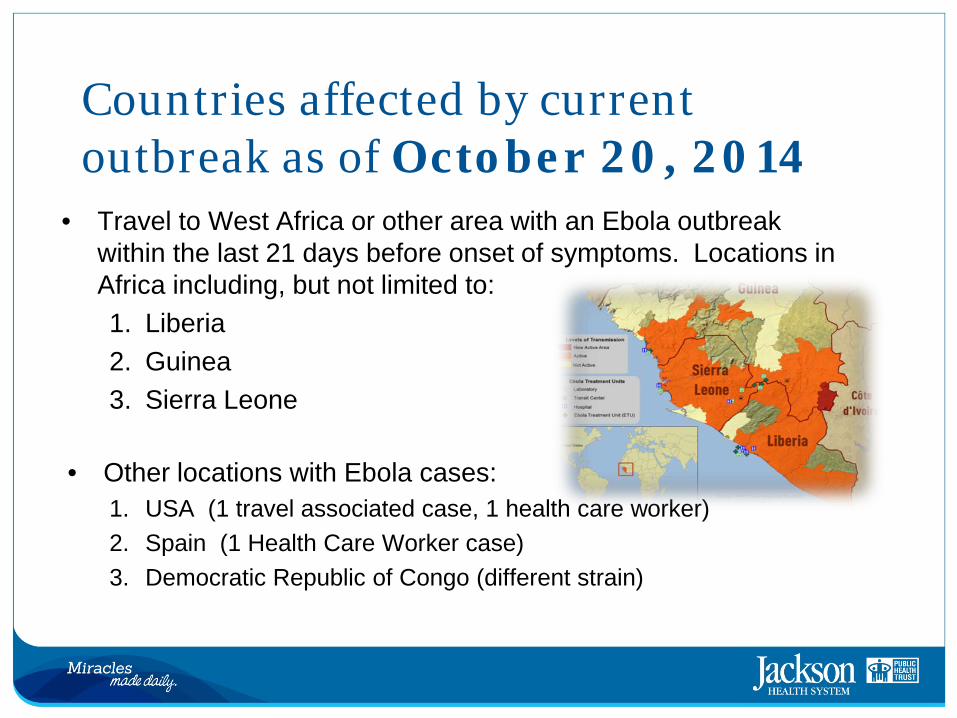
Countries affected by current outbreak as of October 20, 2014 • Travel to West Africa or other area with an Ebola outbreak
within the last 21 days before onset of symptoms. Locations in Africa including, but not limited to: 1. Liberia 2. Guinea 3. Sierra Leone
• Other locations with Ebola cases:
1. USA (1 travel associated case, 1 health care worker) 2. Spain (1 Health Care Worker case) 3. Democratic Republic of Congo (different strain)
Risk of Exposure • Healthcare providers caring for Ebola patients and the family and
friends in close contact with Ebola patients are at risk of getting sick because they may come in contact with the blood or body fluids of sick patients
• People also can become sick with Ebola after coming in contact with infected wildlife
• The likelihood of contracting Ebola is considered extremely low in the United States unless there is direct exposure to the body fluids of an infected perso • Ebola is not spread through casual contact; therefore, the risk of an outbreak in the United States is very low
Levels of Exposure Levels
• High Risk: – Needle stick or mucous membranes exposure to blood or body fluids
of a person with EVD – Direct skin contact with, or exposure to, blood or body fluids of any
person with EVD without the appropriate personal protective equipment (PPE)
– Processing blood or body fluids of a confirmed person with EVD without appropriate PPE or standard bio safety precautions
– Direct contact with the dead body without appropriate PPE in a country where an Ebola outbreak is occurring
CDC.gov
Levels of Exposure Levels
• Low Risk: – Household contact with a person with Ebola – Close contact with a person with Ebola in healthcare facilities or
community settings. – Close contact is defined as:
• Being within approximately 3 feet of the patient or within the patient's room or care area for prolonged period of time while not wearing recommended PPE
• Having direct brief contact with the person with Ebola while not wearing recommended PPE
• Brief interactions, such as walking by a person or moving through a hospital, do not constitute close contact
CDC.gov
Levels of Exposure Levels
• No Known Exposure: – Person who had residence in or traveled to Liberia, Guinea, Sierra
Leone, Lagos, or Republic of Congo WITHOUT high or low risk exposures
FDOH.org
Public Health Screening at JHS Ask every patient: 1. Have you been out of the country within the last 31 days? Yes or No 2. If so, have you traveled to or from any of the following countries: Guinea,
Liberia, Serra Leone, or Democratic Republic of Congo within the past 31 days AND do you have a fever, headache, muscle pain, vomiting, diarrhea, abdominal pain or unexplained bleeding or other symptoms? Yes or No
3. Have you recently come into contact with anyone who has traveled to or from the above countries and who has any of those symptoms? Yes or No
4. Have you had any contact with animals (bats, rodents, monkeys) from the above countries? Yes or No
If a patient answers “Yes” to any of the above, they meet the criteria for travel exposure. Patient will be escorted to a private room for further testing. A staff member will meet with you promptly to explain the next steps and answer any questions.
Evaluating Patients for Possible EVD • There are both epidemiological risk factors and clinical criteria that
must be evaluated • CDC recommendation and JHS policy is to follow JHS protocol /
FDOH algorithm / CDC check list for initial evaluation found on JHS Netportal by all health care workers: 1. Ask patients about their travel histories to determine if they have
traveled to West Africa within last 3 weeks 2. Know the signs and symptoms of Ebola. 3. Know what to do if you have a patient with Ebola symptoms
• Isolate infected/suspected patients • Follow infection control precautions to prevent spread of disease • Avoid contact with blood and body fluids of EVD patients
• CDC Checklist for Patients Being Evaluated for EVD – http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergen
cy%20Preparedness/1.%20EBOLA/04EBOLA%20checklist-patients-evaluated-us-evd%20CDC.pdf
EVD Screening as per CDC
• Emergency Department screening criteria for patient isolation/testing are likely if patient has: – Fever, headache, joint/muscle aches, fatigue, diarrhea, vomiting,
abdominal pain and lack of appetite, and in some cases, bleeding AND – Travel to West Africa (Guinea, Liberia, Nigeria, Sierra Leone, Republic of
Congo or any other countries where the EVD transmission has been reported by the World Health Organization (WHO) within the last 21 days (3 weeks) of the onset of symptoms
If BOTH criteria are met, then the patient should be moved to a negative pressure room with private bathroom and placed on Standard, Contact, & Airborne precautions followed thereafter
EVD Screening as per CDC
Immediately report Person Under Investigation (PUI) for Ebola to:
1. Immediate Supervisor
2. Hospital Leadership: AIC 305-585-2255 OR Pager #9342
3. Hospital Infection Control 305 585-6820 After hours, Weekends, & Holiday 305-996-0459
4. Security 305305-585-6111
Patient Placement/Isolation • Patients should be placed in a negative air pressure room (containing a
private bathroom or bedside commode) • Place patient on Standard, Contact, & Airborne Precautions as per JHS
Bio-emergency Plan • Wash hands with soap and water or use alcohol based sanitizer before and
after all patient contact • Restrict visitors/visitation to the EVD patient’s room/area. • Maintain a log of ALL people entering the patient's room – all staff included.
Use only a mattress and pillow with waterproof plastic or other waterproof covering. http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency%20Preparedness/1.%20EBOLA/45EbolaStaffVisitorsSurveillanceForms.pdf
• Do not place patients with suspected or confirmed EVD in carpeted rooms; remove all upholstered furniture and decorative curtains from the patient rooms before use.
• Standard Precautions – Used in the care of all patients. – Always perform hand hygiene. – Use personal protective equipment (PPE) as needed.
• Contact Precautions – In addition to standard precautions. – Put on gown and gloves before entering the patient’s room.
• Droplet Precautions – In addition to standard precautions. – Put on a surgical/procedure mask before entering the patient’s room. – Put on eye goggles/face shield when coming within 3 feet of the
patient. • Airborne Precautions
– In addition to standard precautions. – Put on an N95 respirator (you must be “fit tested” by Occupational Health prior to use, if not already done so).
Infection Control Precautions General Overview
Personal Protective Equipment
• Every suspected or actual EVD patient is to be placed on standard, contact, and airborne precautions.
• Use of Personal Protective Equipment (PPE) is essential. • Always use a buddy system when caring for and putting on/off
PPE • Always use correct sequence for donning/doffing PPE • Hydrate yourself and use restroom prior to starting donning
process
Personal Protective Equipment Sequence for Donning PPE
1. Remove all jewelry 2. Perform Hand hygiene 3. Put on jumpsuit 4. Put on bouffant cap 5. Put on surgical hood 6. Put on surgical gown 7. Tuck hood ties under surgical gown 8. Perform second hand hygiene 9. Put on fit-tested respirator 10. Put on face shield 11. Perform third hand hygiene 12. Put on first pair of gloves 13. Put on second pair of gloves 14. Perform a final check
Before You Begin
•You have cuts or abrasions •You feel ill •The PPE does not fit
Do not use PPE or provide care if:
1. Remove all jewelry
2. Perform hand hygiene
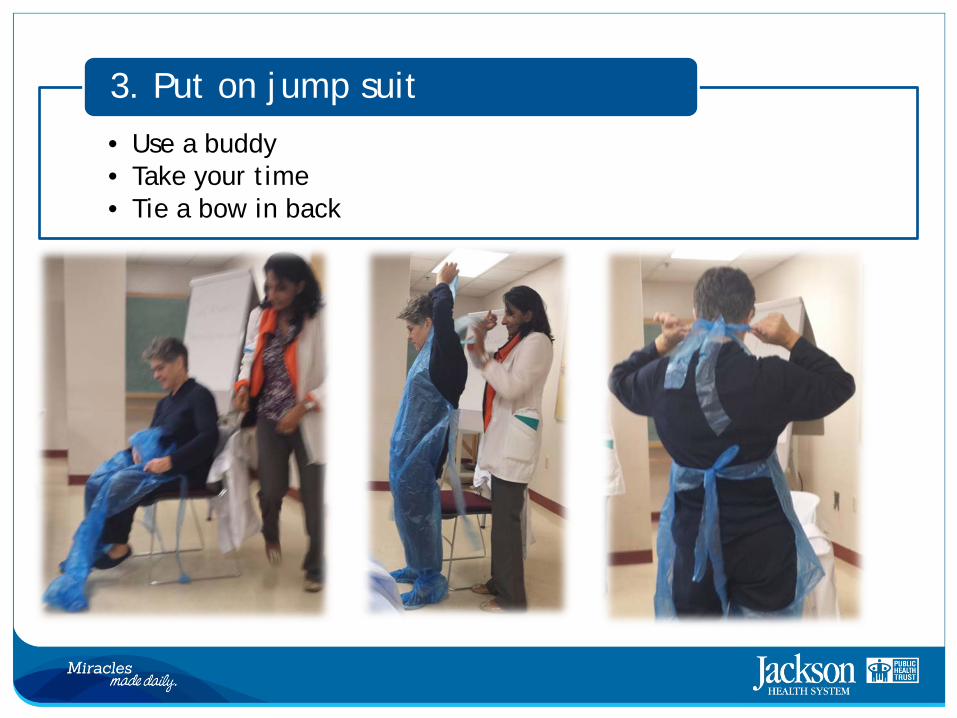
• Use a buddy • Take your time • Tie a bow in back
3. Put on jump suit
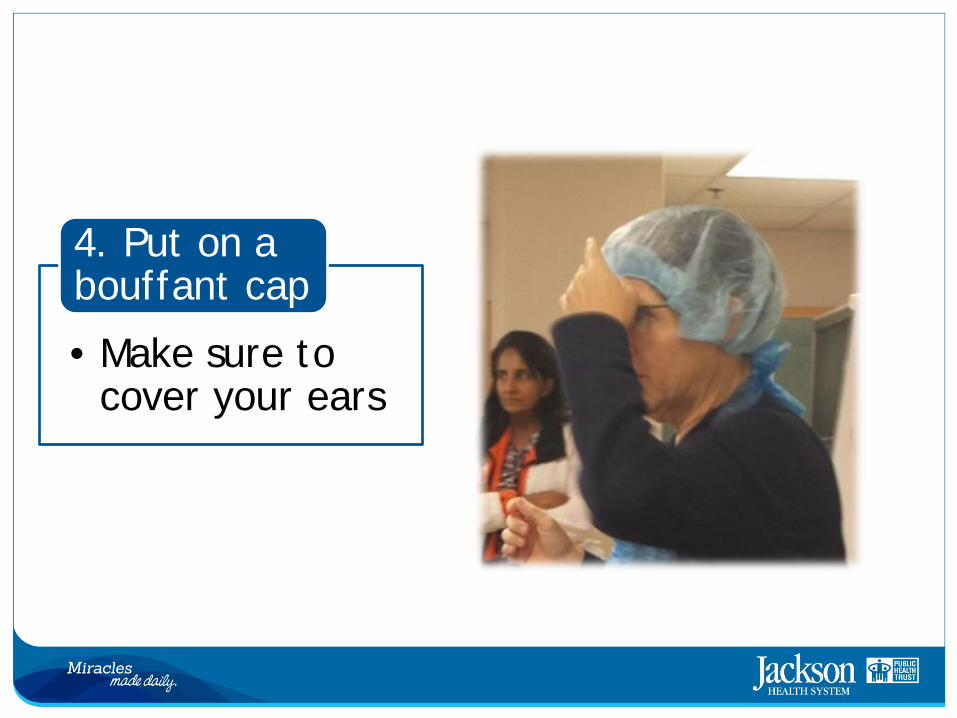
• Make sure to cover your ears
4. Put on a bouffant cap
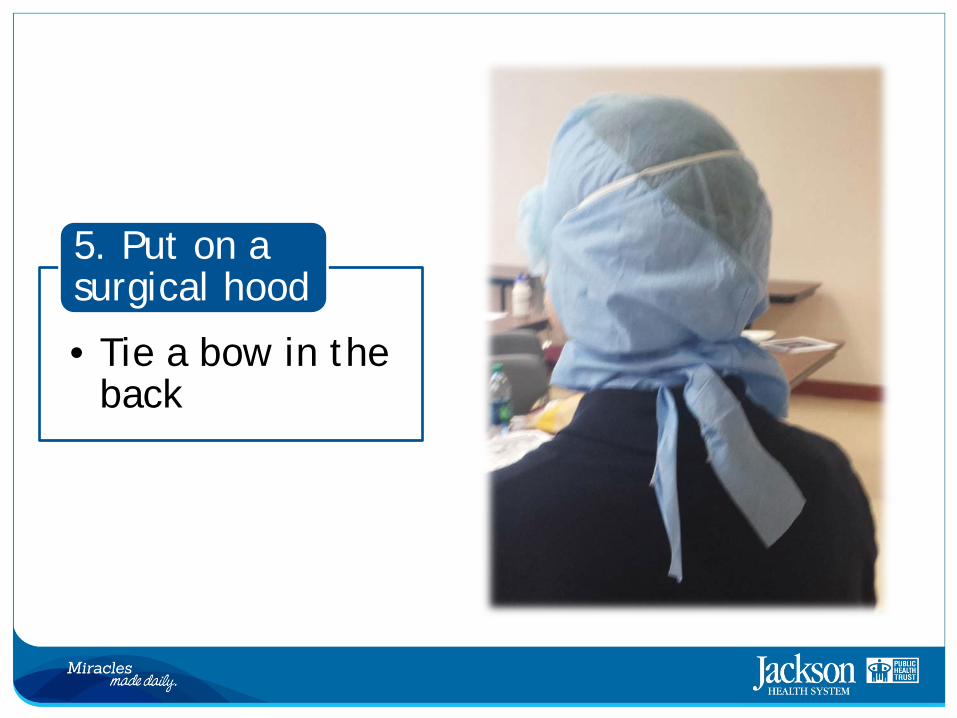
• Tie a bow in the back
5. Put on a surgical hood
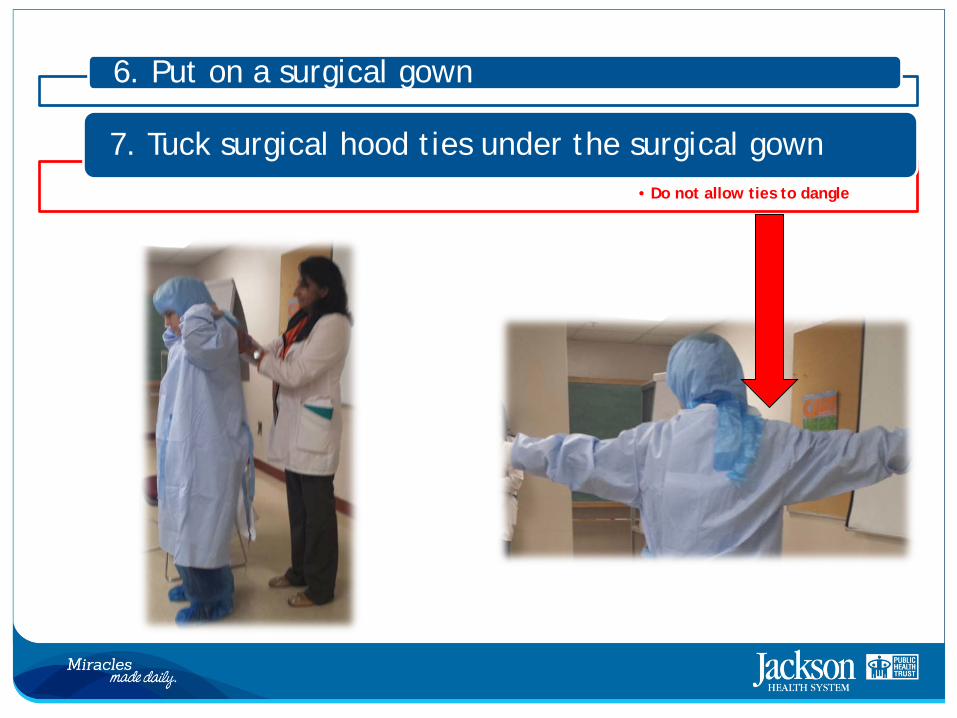
6. Put on a surgical gown
• Do not allow ties to dangle
7. Tuck surgical hood ties under the surgical gown
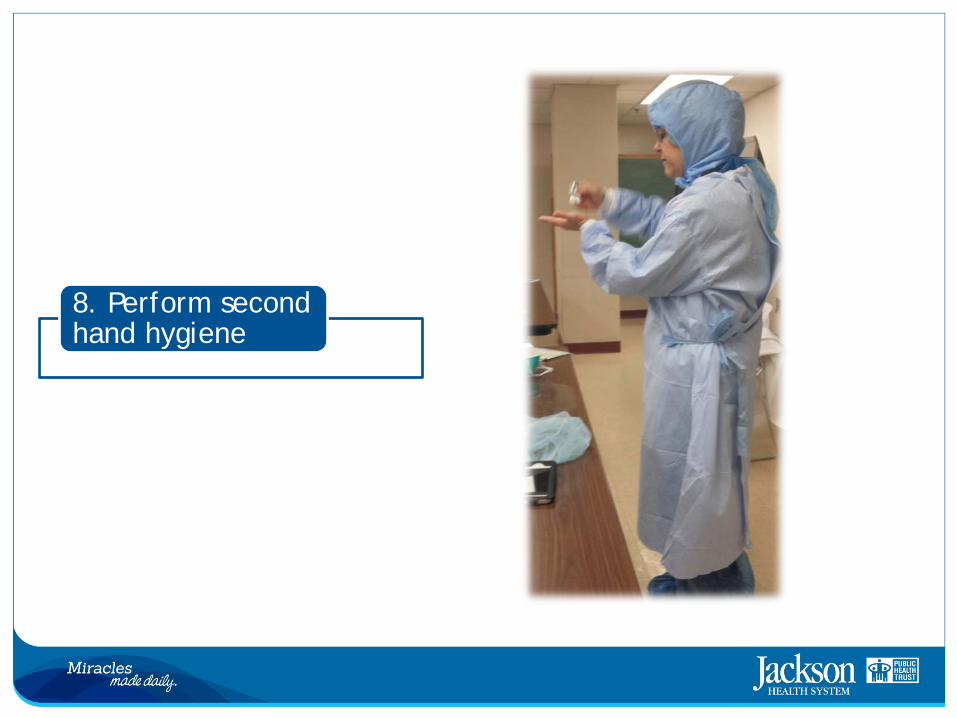
8. Perform second hand hygiene
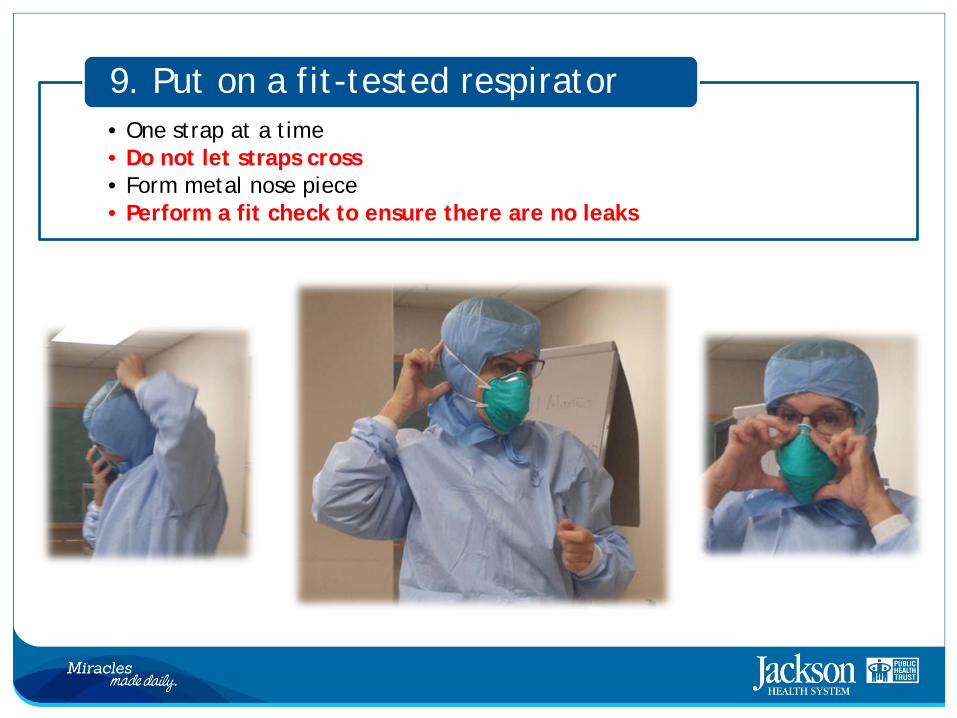
• One strap at a time • Do not let straps cross • Form metal nose piece • Perform a fit check to ensure there are no leaks
9. Put on a fit-tested respirator
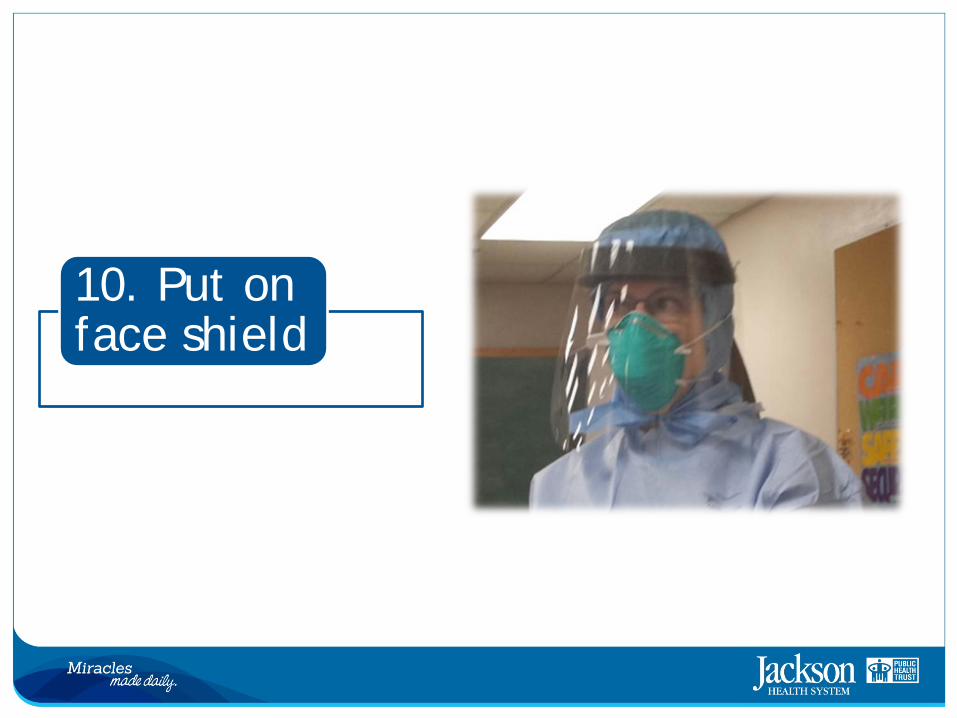
10. Put on face shield
11. Perform third hand hygiene
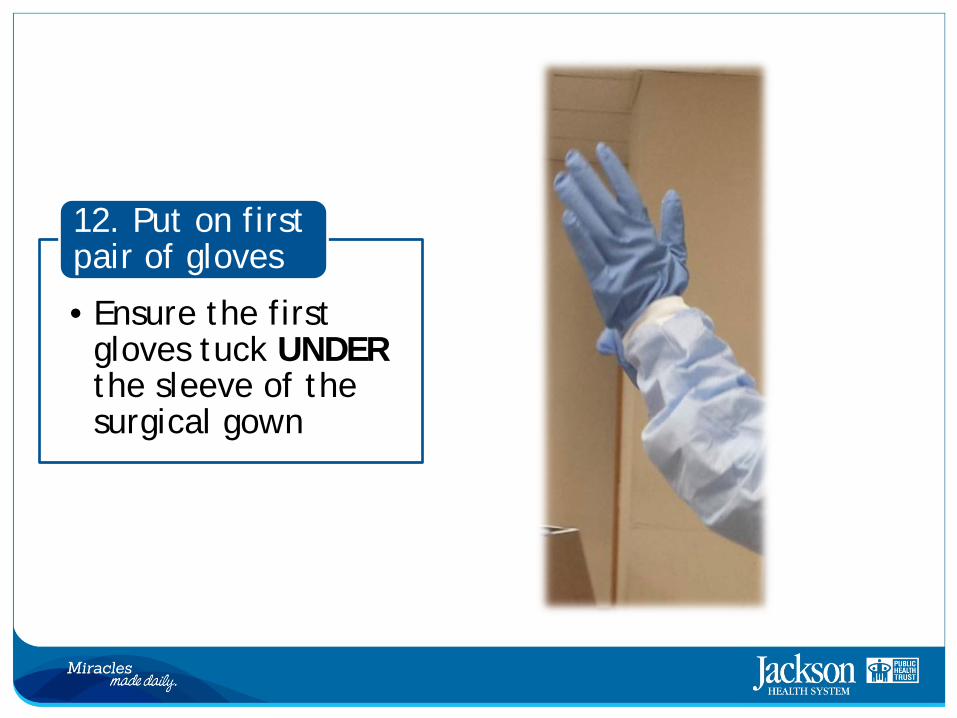
• Ensure the first gloves tuck UNDER the sleeve of the surgical gown
12. Put on first pair of gloves
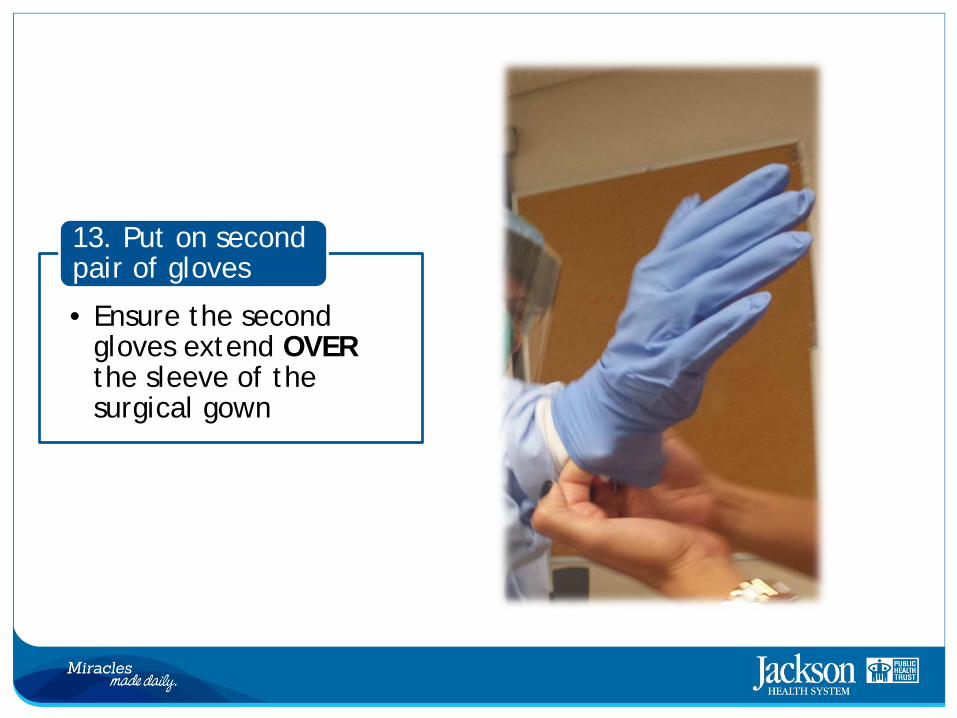
• Ensure the second gloves extend OVER the sleeve of the surgical gown
13. Put on second pair of gloves
•Both you and your buddy should confirm your PPE is correctly placed and has no rips or tears
14. Perform a final check
You are now ready to enter your patient’s room
Personal Protective Equipment • Sequence for Doffing (Removing) PPE
1. Wipe outer pair of gloves with bleach 2. Exit patient room 3. Step into designate area 4. Remove outer gloves 5. Remove face shield 6. Carefully remove surgical gown 7. Wipe inner gloves with bleach 8. Remove jumpsuit and step onto clean area 9. Remove inner gloves 10. Perform first hand hygiene 11. Put ON a pair of standard exam gloves 12. Remove respirator mask 13. Remove surgical hood 14. Remove bouffant cap 15. Wipe shoes with bleach 16. Step out of designated area 17. Ensure all PPE items have been discarded in the designated receptacle
Before You Begin
•Don’t rush •Use the buddy system •Ask for more help if you need it – never guess!
Proceed with caution!
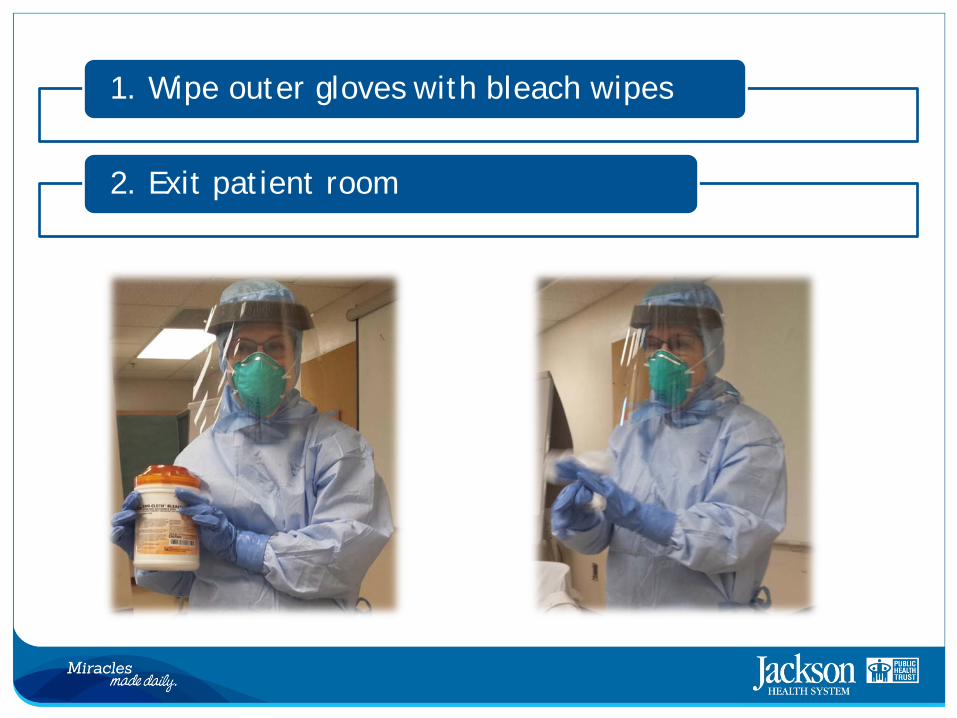
1. Wipe outer gloves with bleach wipes
2. Exit patient room
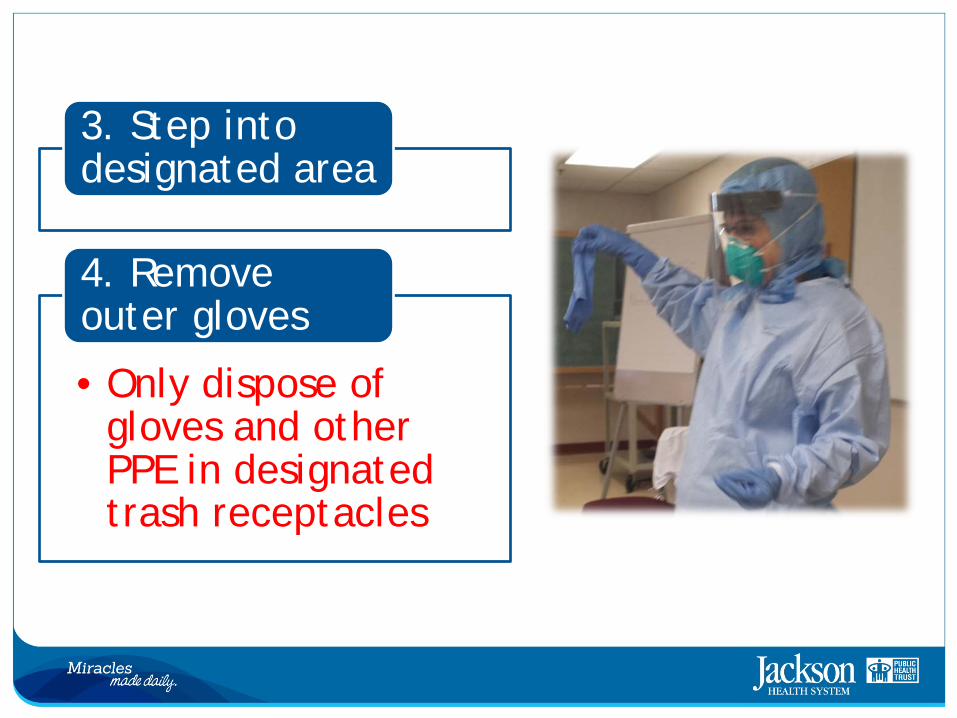
3. Step into designated area
• Only dispose of gloves and other PPE in designated trash receptacles
4. Remove outer gloves

• Remember to use designated trash receptacle
5. Remove face shield
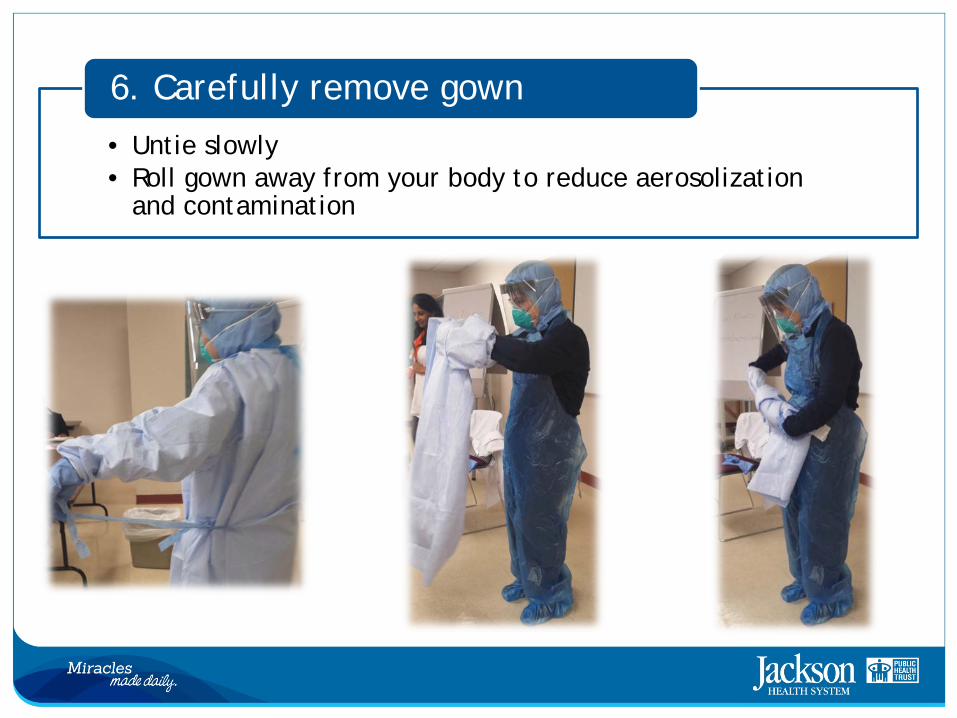
• Untie slowly • Roll gown away from your body to reduce aerosolization
and contamination
6. Carefully remove gown
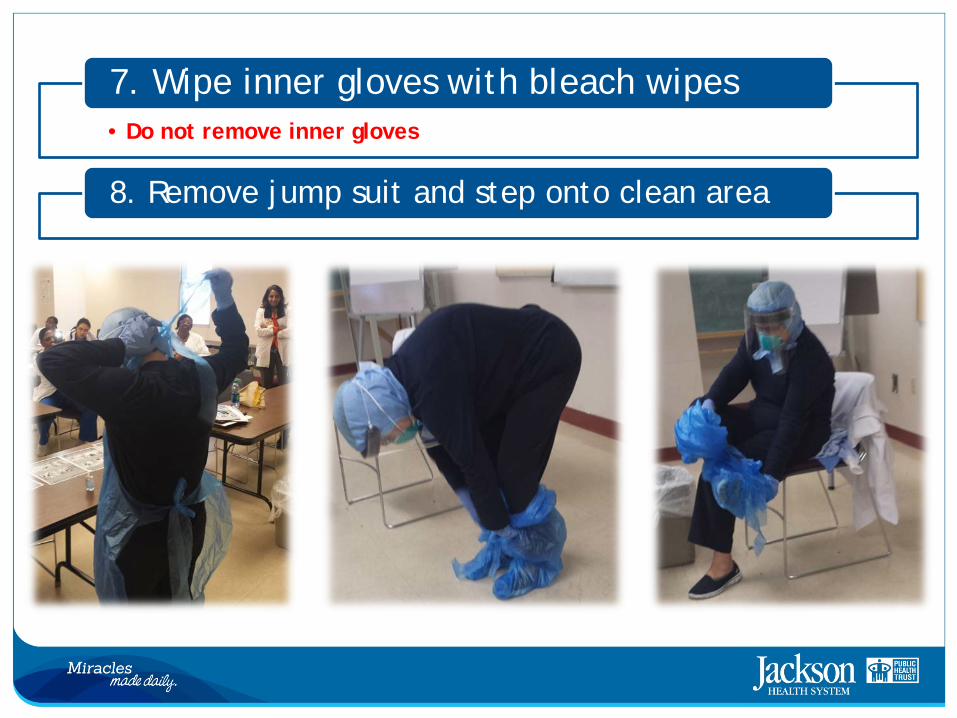
• Do not remove inner gloves
7. Wipe inner gloves with bleach wipes
8. Remove jump suit and step onto clean area
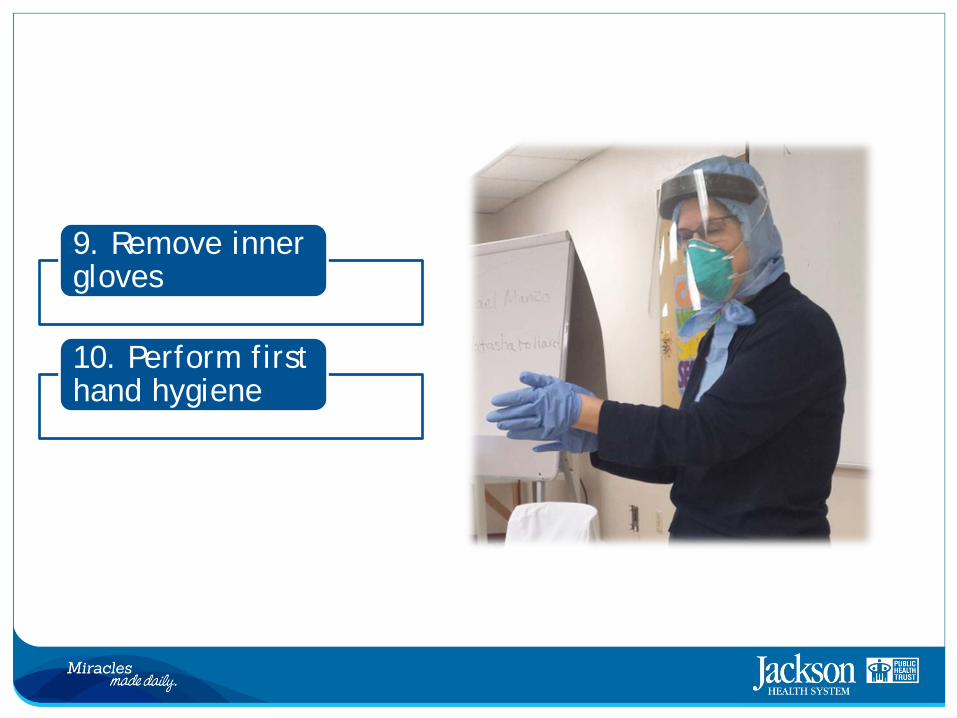
9. Remove inner gloves
10. Perform first hand hygiene
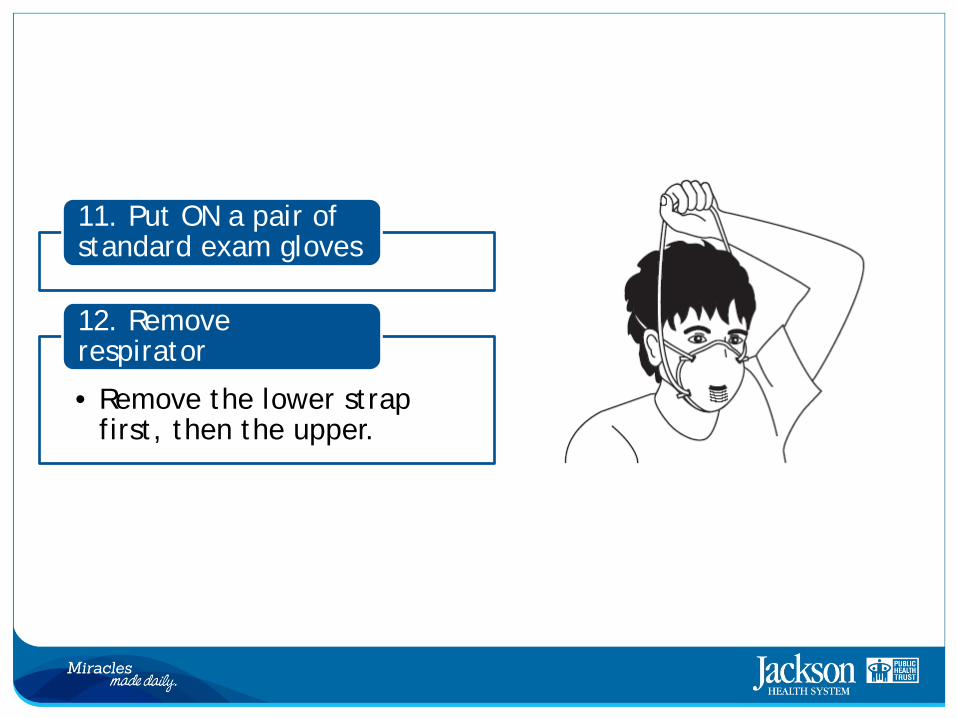
11. Put ON a pair of standard exam gloves
• Remove the lower strap first, then the upper.
12. Remove respirator
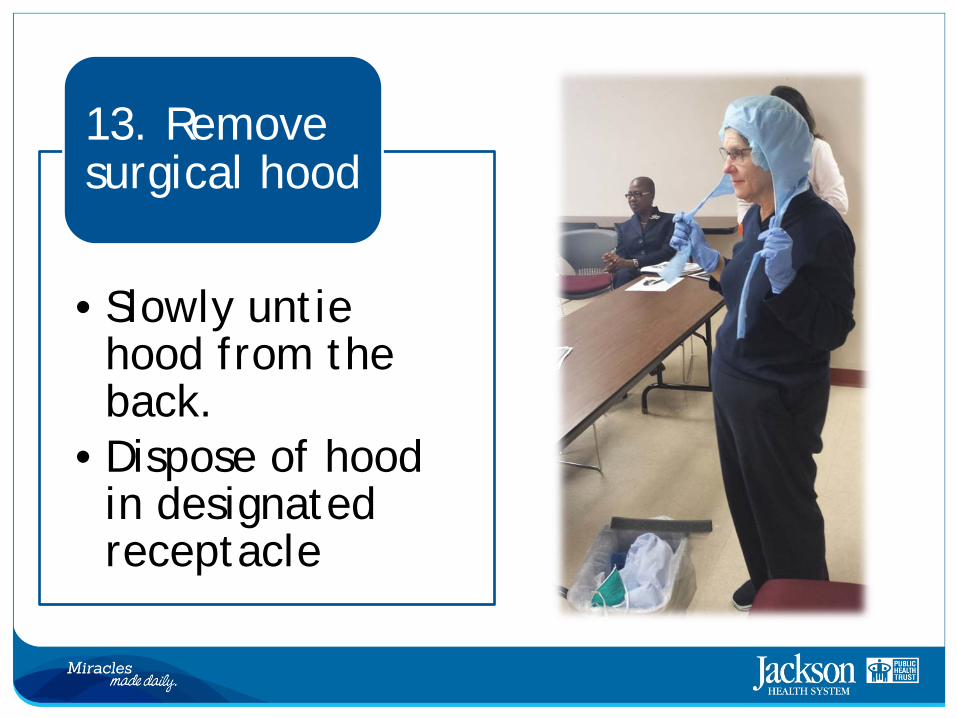
•Slowly untie hood from the back.
•Dispose of hood in designated receptacle
13. Remove surgical hood
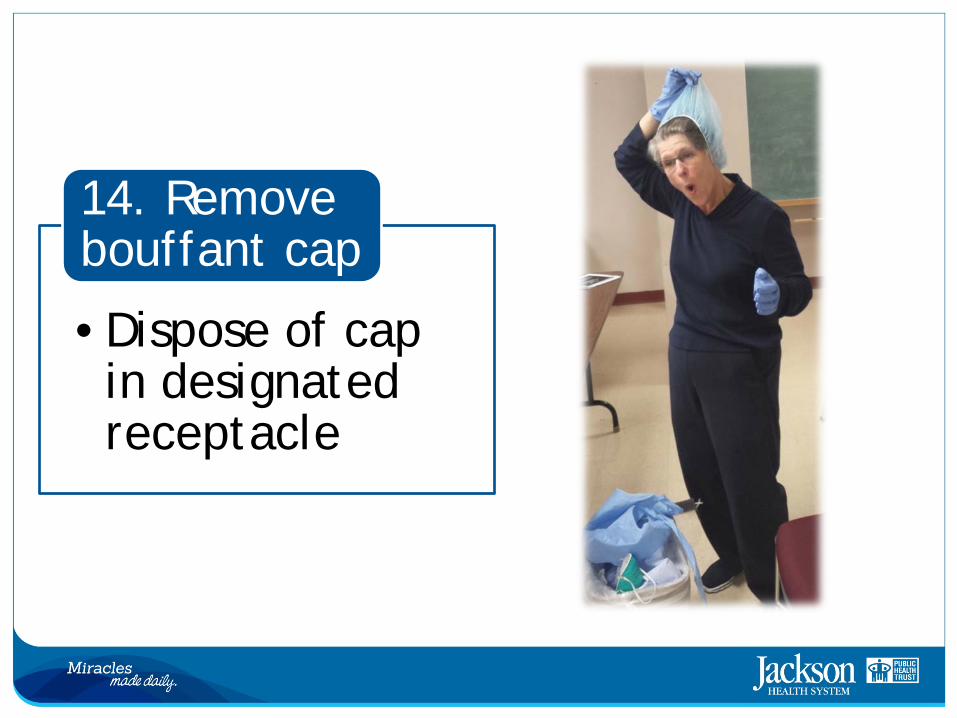
•Dispose of cap in designated receptacle
14. Remove bouffant cap
15. Wipe shoes with bleach wipes
16. Step out of designated area
17. Ensure all PPE items have been discarded in the designated receptacle
18. Remove gloves
19. Perform second hand hygiene
You are now ready to resume work safely
Personal Protective Equipment Reminders • Always use the buddy system • Never guess • Get more help if needed • Use safe work practices to protect self and limit spread of
contamination • Keep hands away from face • Limit surfaces touched • Change gloves when torn or heavily contaminated • Perform strict hand hygiene
Patient Care Considerations • Minimal number of Healthcare Worker/Staff should enter the room of
suspected or confirmed EBV • Limit the use of needles and other sharps as much as possible • Limit phlebotomy, procedures, and lab testing to the minimal necessary
for essential diagnostic evaluation and medical care • Handle all needles with extreme caution and dispose in dedicated
puncture-proof, sealed sharps container • Avoid aerosol generating procedures, as much as possible:
– BiPAP machine – Bronchoscopy – Open suctioning of airway – Sputum induction – Intubation/extubation
• Implement environmental infection control measures, equipment sterilization, etc.
Patient Care Equipment
• Dedicated medical equipment (preferably disposable, when possible) should be used to provide patient care
• All non-dedicated equipment, non-disposable medical equipment used for patient care should be cleaned and disinfected according to the manufacturer instructions and/or infection control hospital policies
Environmental Infection Control
• Daily cleaning and disinfection of hard, non-porous surfaces should be done using a US Environmental Protection Agency (EPA)-registered hospital disinfectant with a label clean for a non-enveloped virus.
• Healthcare providers performing environmental cleaning and disinfection should wear recommended PPE and consider use of additional barriers (shoe/leg coverings), if needed.
• Eye protection (face shield/goggles) and N95 Respirator should be worn when performing task, such as liquid waste disposal, that can generate splashes.
Environmental Infection Control
• Patients’ liquid waste must be “treated" by environmental care service before the disposal of liquid waste.
• Toilet seat cover should be down before flushing treated liquid waste flushing.
• If toilet bowl does not have seat cover then use a proper size disposable bed pan to cover the seat before flushing treated liquid waste and then dispose of the bedpan as EBOLA infectious waste.
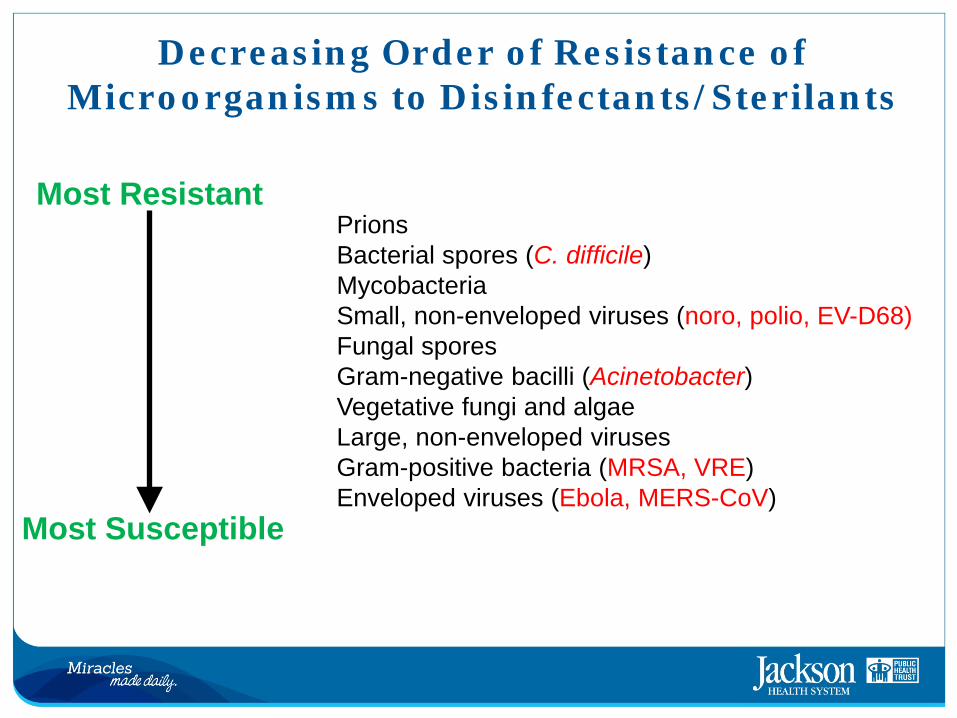
Decreasing Order of Resistance of Microorganisms to Disinfectants/Sterilants
Prions Bacterial spores (C. difficile) Mycobacteria Small, non-enveloped viruses (noro, polio, EV-D68) Fungal spores Gram-negative bacilli (Acinetobacter) Vegetative fungi and algae Large, non-enveloped viruses Gram-positive bacteria (MRSA, VRE) Enveloped viruses (Ebola, MERS-CoV)
Most Resistant
Most Susceptible

Hospital Approved Surface Disinfectants
Additional Recommendations Infection control recommendations:
• Standard, contact & airborne precautions, including gloves, fluid-resistant gowns, eye protection, face mask; additional PPE may be required.
• Single patient, negative air room with private bathroom, door closed; restrict visitors • Avoid aerosol-generating procedures. • Implement environmental infection control measures.
Testing recommendations: • Conduct only essential laboratory testing, and take appropriate precautions according to
laboratory recommendations. • Include malaria diagnostics in initial testing as it is the most common cause of febrile illness
in asymptomatic persons with travel history to affected countries. • Collect two lavender top tubes of blood; do not use pneumatic tube system for transport;
contact DOH to determine the proper category for shipment.
Follow-up recommendations for persons when EVD testing is not indicated: • Self-monitor twice daily for fever and other symptoms for 21 days from last exposure. • Seek medical evaluation at first sign of illness.
Specimen Collection • Clinical laboratories can safely do routine laboratory testing such as traditional chemistry, hematology, or other laboratory testing used to support and treat patients • Specimen should be obtained when a symptomatic patient reports or is
suspected of having EBV • Strictly adhere to CDC’s recommendations and hospital/infection control
guidelines • The Clinical team should contact the JMH Clinical Laboratory via telephone at
305-585-6521 and ask for the “Person in Charge” to coordinate testing. • If not already available, kits will be sent to the clinical team containing the
appropriate blood collection tubes and materials • The clinical laboratory and teams will coordinate pickup and transport of blood
specimens, so they are to be picked up by someone from the JMH Clinical Laboratory
Specimen Collection
• The following tests are indicated for laboratory evaluation of suspected EVD patients who have met clinical and travel/exposure criteria: – Complete Blood Count (CBC) - one lavender-top (EDTA) tube
• All standard laboratory CBC indices will be reported. This test will be performed on the standard laboratory hematology analyzer, which is a closed testing system
– Complete Metabolic Profile (CMP) - one green-top (lithium heparin) tube. Testing will be performed on a device dedicated to EVD patients and blood must be tested within one hour of blood collection
• The following analytes will be reported: Sodium, Potassium, Chloride, Total carbon dioxide, Calcium, Glucose, Total protein, Total Bilirubin, Alkaline Phosphatase (ALP), Alanine aminotransferase (ALT), Aspartate aminotransferase (AST)
Specimen Collection • Additional central laboratory testing for suspected EVD patients:
– Rapid malaria* test (BinxNOW - Alere). One lavender-top (EDTA) tube. **A positive malaria test does not exclude the possibility of EVD, since co-infection in EVD patients has been reported
• Any person collecting specimens from a patient with suspected EVD
should minimally wear: – Gloves – Water resistant gowns – Full face shield/goggles and N95 respirator to cover all of nose and mouth
• NOTE: It may take up to 3 days after the onset of symptoms for the
virus to reach detectable levels in the blood. If the onset of symptoms is <3 days after potential exposure, a subsequent specimen will be required in order to rule out Ebola.
Specimen Collection
• Specimens other than blood may be submitted upon consult with the CDC
• To reduce the risk of breakage or leaks, do not use any pneumatic tube system for transporting suspected Ebola virus disease specimens. DO NOT send to lab via pneumatic tube system
• In compliance with 29 CFR 1910.1030, specimens should be placed in a durable, leak-proof secondary container for transport within a facility
Specimen Collection for the CDC
• The requested test needs to be identified only on the requisition and CDC specimen submission forms – Instructions for Submitting Diagnostic Specimens to CDC’s Viral Special
Pathogens Branch • http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and
%20Emergency%20Preparedness/1.%20EBOLA/19EBOLA%20CDC%20Form%20LabSpecimenSubmissionForm1.pdf
– CDC Specimen Submission Form: Specimens Of Human Origin
• http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency%20Preparedness/1.%20EBOLA/20LapSpecimenSubmissionForm2CDCForm50-34.pdf
See link for more information regarding Specimen Collection http://www.cdc.gov/vhf/ebola/pdf/ebola-lab-guidance.pdf
Point of Care Testing
Tests available at the patient beside (Point-of-care), if indicated: 1) Standard urinalysis, by dipstick method 2) Finger-prick glucose (glucometer) level 3) INR (International Normalized Ration) coagulation test on the iStat
portable analyzer** 4) In patients with respiratory issues, the iStat portable analyzer will
be made available. 5) The CG8+ provides the following results: pH, PCO2, TCO2 , BE,
Na, Cl, K, Anion Gap, BUN, Glu, Hct, Hgb
Blood Transfusion
• Transfusion requirements for suspected EVD patients: – Pre-transfusion testing (e.g. type and screen, crossmatch, etc.)
requires open testing systems and is unsafe for laboratory personnel in the context of suspected EVD patients.
– Consequently, suspected EVD patients will receive uncrossmatched group O-negative red blood cells and group AB plasma (FFP)
• Do not send blood specimens to the clinical laboratory or transfusion laboratory
• Clinical requests for blood products will proceed as they would for emergency trauma patients
Transport • All healthcare providers must wear the following PPE to transport/transfer a suspected or actual EVD patient within the hospital:
– Gloves – Gown (fluid resistant or impermeable) – Eye protection (goggles or face shield) – N95 Respirator
• The patient should have a surgical/procedural mask, if tolerated.
Additional PPE might be required in certain situations (e.g., copious amounts of blood, other body fluids, vomit, or feces present in the environment), including but not limited to:
– Double gloving – Disposable shoe covers – Leg coverings
Post Mortem Care of EVD Patients • Use appropriate PPE • Post Mortem Care involves:
– Preparation of the body – Surface decontamination – Transport
• Preparing the body: – Wrap in a plastic shroud; wrapping the body should be done in a way that prevents
contamination of the outside of the shroud – Change gloves or gown if they become heavily contaminated with blood or body fluids. – Leave any IV lines or endotracheal tubes that may be present in place – Avoid washing or cleaning the body – After wrapping, body should be immediately placed in a “leakage proof” plastic bag not
less than 150 µm thick and zippered closed • “Leakage proof” bag is a bag that is puncture-resistant and sealed in a manner so as to contain
all the contents and prevent leakage of fluids during handling, transport, or shipping – The bagged body should then be placed in another leakage proof plastic bag not less
than 150 µm thick and zippered closed before being transported
Post Mortem Care of EVD Patients • Surface decontamination:
– Prior to transport, perform service decontamination of the corpse-containing body bags by removing visible soil on outer bag surfaces with EPA-registered disinfectants.
– Follow product label instructions, infection control and hospital guidelines.
– Once the visible soil has been removed, reapply the disinfectant to the entire bag surface and allowed to air dry
– Following the removal of the body, the patient room should be cleaned and disinfected as per Infection Control, CDC, and hospital guidelines
• Transport: – Transport of patient should be according to CDC and organizational
guidelines – For more information, see CDC website
http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency%20Preparedness/1.%20EBOLA/24EBOLA%20CDC%20Autopsy%2008%2025%2014.pdf
Accessing Information • From the JHS Intranet, click on Content Directory Disaster
and Emergency Preparedness Ebola
Intranet Links
• Ebola Fact Sheet – http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency
%20Preparedness/1.%20EBOLA/01Ebola-FactSheet%2007%2029%2014.pdf
• JHS Protocol/Brief Statements – http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency
%20Preparedness/1.%20EBOLA/03EBOLA%20Brief%20Statement%20for%20Departments(2).docx
• CDC Checklist for Patients Being Evaluated for EVD – http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency
%20Preparedness/1.%20EBOLA/04EBOLA%20checklist-patients-evaluated-us-evd%20CDC.pdf
• FDOH Ebola Testing Algorithm – http://jet/sitecol/DIVISION/008/000624/Shared%20Documents/Disaster%20and%20Emergency
%20Preparedness/1.%20EBOLA/05EBOLA%20FDOH%20AlgorithmforTesting%20of%20SuspectedEVD%20update.pdf
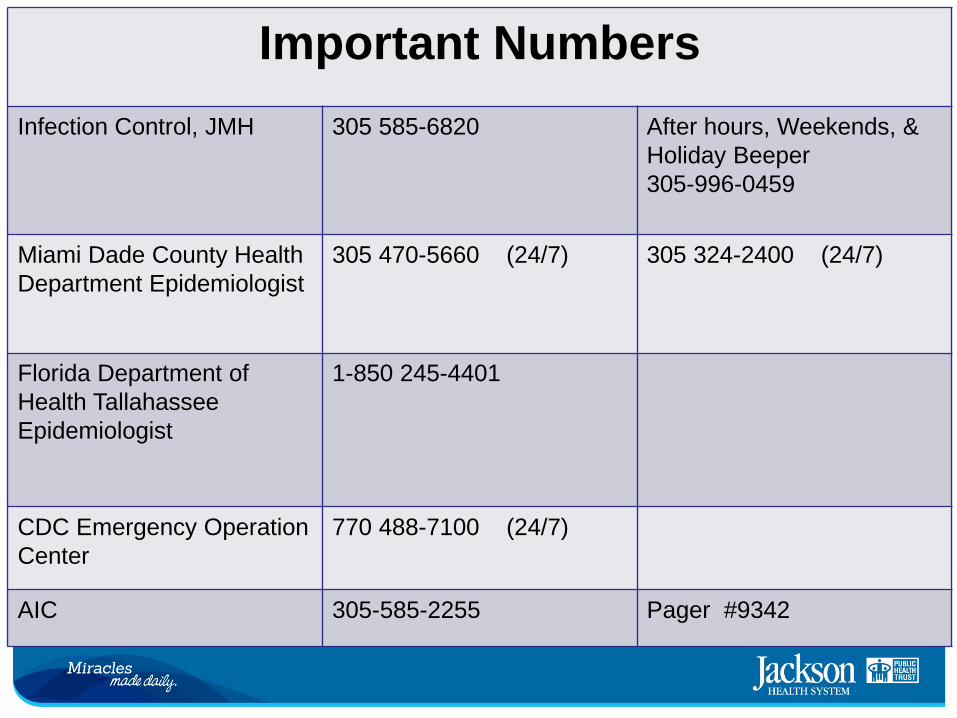
Important Numbers Infection Control, JMH
305 585-6820
After hours, Weekends, & Holiday Beeper 305-996-0459
Miami Dade County Health Department Epidemiologist
305 470-5660 (24/7)
305 324-2400 (24/7)
Florida Department of Health Tallahassee Epidemiologist
1-850 245-4401
CDC Emergency Operation Center
770 488-7100 (24/7)
AIC 305-585-2255 Pager #9342
References
• CDC website: http://www.cdc.gov/vhf/ebola/index.html • OSHA website: https://www.osha.gov/Publications/OSHA_FS-
3756.pdf • WHO website: http://www.who.int/csr/disease/ebola/en/
Education and Development October 2014
![Slide sem título - Inicial — UFRGS | Universidade Federal do Rio … · PPT file · Web view2015-06-30 · Tratamento ... fever, rash, vomiting, diarrhea, low lymphocyte counts,[5]](https://img.pdfslide.tips/doc/110x75/5be4ca5c09d3f2857c8b47e3/slide-sem-titulo-inicial-ufrgs-universidade-federal-do-rio-ppt-file.jpg)