Embed Size (px)
Citation preview
Kristi Watterberg, MD
University of New Mexico
Dr. Watterberg has no financial or other conflicts of interest to disclose
She will be discussing studies of glucocorticoids in preterm infants
History – how did we get here?
Where is here? – current information
◦ Dexamethasone for BPD
◦ Hydrocortisone for BPD
◦ Hydrocortisone for early hypotension
Reasons to worry
◦ Immediate side effects
◦ Growth and development
◦ Very long term outcomes
Abstracts: early anecdotes
(„78, „80, „81)
„hastened weaning from ventilator‟
(Mammel, 6 infants; Lancet, 1983)
„striking short-term improvement‟
(Avery, 16 infants; Pediatrics, 1985)
faster weaning from IMV and O2
(Cummings, 36 infants; NEJM 1989)
“The long term effects are not clear . . . Potential complications of glucocorticoid treatment are well known [including] possibly long term neurodevelopmental compromise . . . The treatment cannot be recommended without further study of patient selection, dosage schedules, short and long-term side effects, and the mechanisms of its actions.”
--Mammel, Lancet 1983
High dose – 0.5mg/kg/day
(Prenatal: 12mg/day to mothers 0.15mg/kg)
Long-term – 42 day tapering course
(Prenatal: 2 days, ± weekly repeat)
Started earlier and earlier in life, until…
Rx works (Yeh , Pediatrics 100:(4)E3,1997)
Or it doesn‟t (Sinkin, Pediatrics 105:542, 2000)
Rx works, but dose for adverse effect
(Garland, Pediatrics, 104:91, 1999)
Study stopped for lack of efficacy and/or safety concerns
(Vt-Ox, Pediatrics 108:741, 2001)
(NICHD, NEJM 344:95, 2001)
Hyperglycemia
Hypertension, cardiac hypertrophy
Proteolysis, muscle wasting, osteopenia
Sepsis
Adrenal suppression
GI perforation
Growth failure
*Neurodevelopmental impairment*
Dex is associated with ↑CP & neurologic impairment
Meta-analysis of >1000 patients in RCTs
Barrington KJ, BMC Pediatrics 1:1, 2001
Dex is a risk factor for MDI <70 & abnormal neurologic exam
Follow up of > 1100 ELBW infants, cohort study
NICHD Neonatal Network, Pediatrics 105:1216, 2000
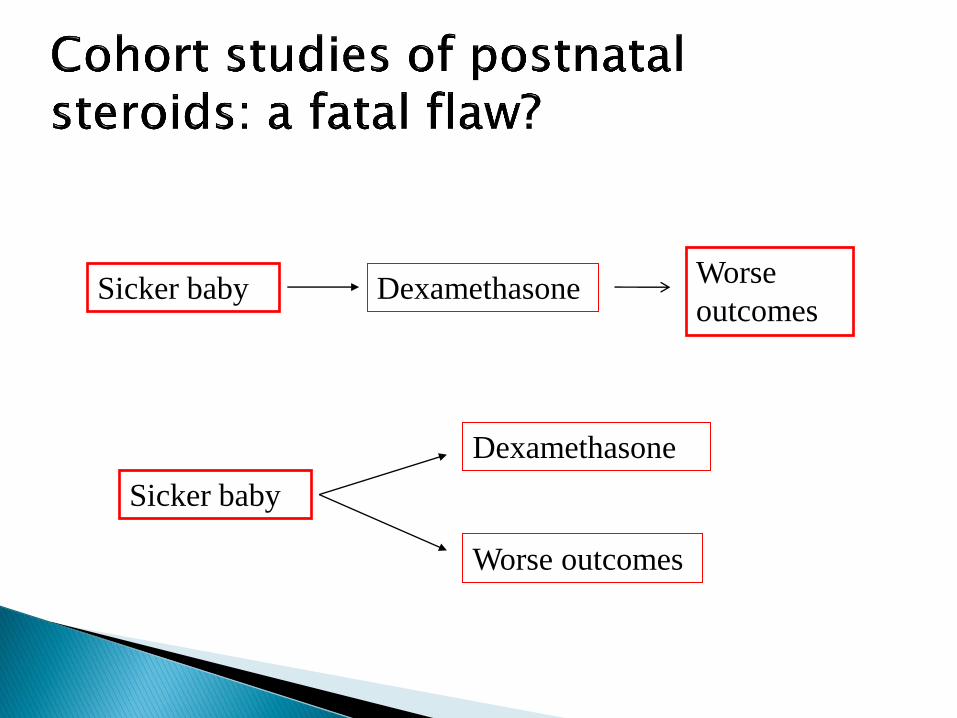
Sicker baby Dexamethasone Worse
outcomes
Sicker baby
Dexamethasone
Worse outcomes
All steroids are
bad – no babies
should get them!
Dex is good – the
more the better!
BPD, extubation failure, no mortality
Many short and long-term complications
Routine use . . . is not recommended
Outside the context of a randomized trial, use of corticosteroids should be limited to exceptional clinical circumstances
Parents should be fully informed about risks
◦ Pediatrics109:330; 2002
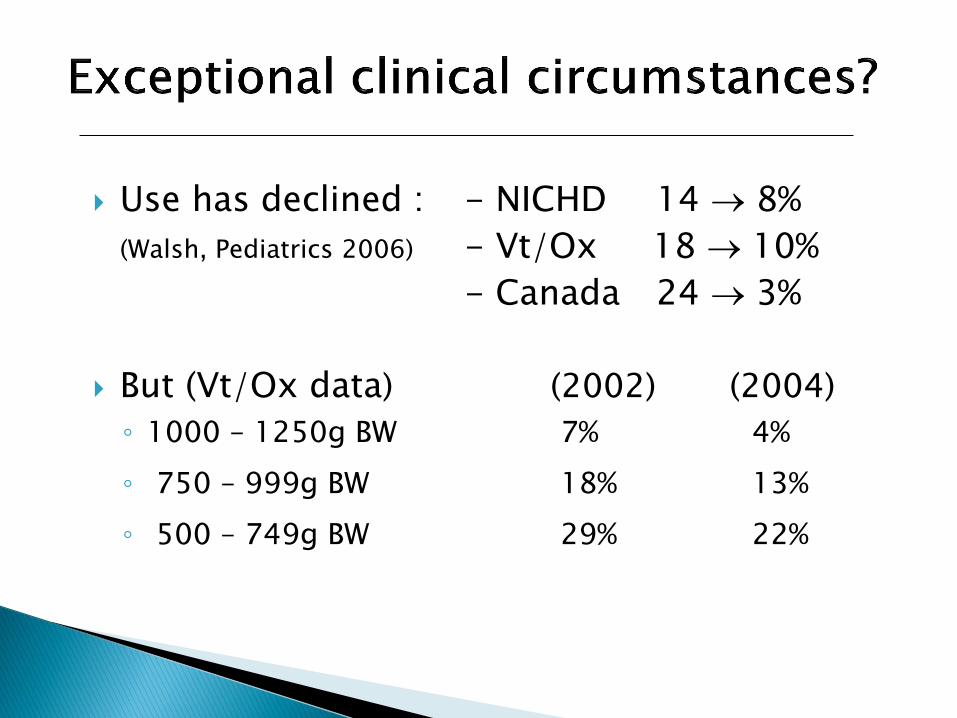
Use has declined : - NICHD 14 8%
(Walsh, Pediatrics 2006) - Vt/Ox 18 10%
- Canada 24 3%
But (Vt/Ox data) (2002) (2004)
◦ 1000 – 1250g BW 7% 4%
◦ 750 – 999g BW 18% 13%
◦ 500 – 749g BW 29% 22%
BPD may be rising in incidence and/or severity with decreasing use of PNS
◦ Population study (Israel): ↓PNS, ↑BPD
- Shinwell, Arch Dis Child 2007; 92:F30
◦ Single center cohort: ↓PNS, ↑vent dependence
- Kobaly - Pediatrics 2008;121:73
◦ Pediatrix (77,520 babies <32 weeks EGA): ↓PNS, ↑ BPD in babies <29 weeks,↑ severe BPD overall
- Yoder Pediatrics 2009; 124:673
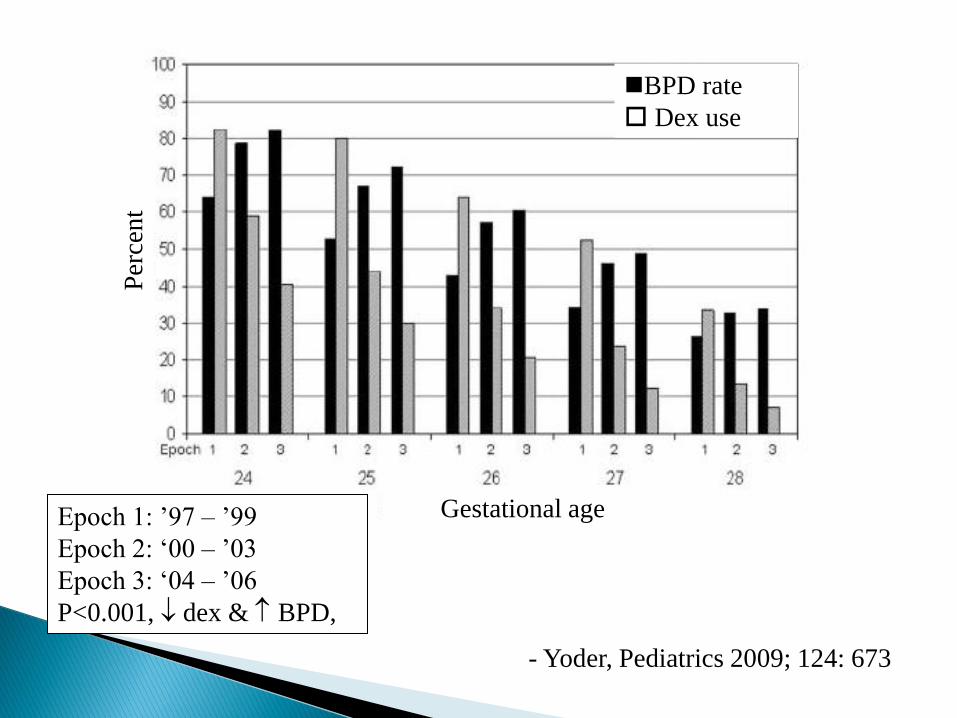
- Yoder, Pediatrics 2009; 124: 673
Epoch 1: ’97 – ’99
Epoch 2: ‘00 – ’03
Epoch 3: ‘04 – ’06
P<0.001, dex & BPD,
Gestational age
Per
cen
t
BPD rate
Dex use
BPD: ↑ incidence of Bayley MDI & PDI <70, abnormal neurologic exam
◦ (NICHD network, 1154 ELBW infants)
Balancing the risk – RCT “meta-regression”
◦ If the baseline risk for BPD in the study population
was low (35%), dex ↑ risk of death/CP
◦ If the risk was >50%, dex ↓ risk of death/CP
Doyle, Pediatrics 2005; 115:794
Decreasing the dex dose might also help
Most previous studies started with a dose of 0.5mg/kg/day
Lower doses (0.15mg/kg/day) were not associated with adverse neurodevelopmental outcomes in 2 studies
Early Rx (n=123)
Stark, EPAS 2001; 2229
Later extubation study (n = 58)
Doyle, Pediatr 2007; 119:717
But there may be another alternative…
Dexamethasone is
◦ Synthetic
◦ Contains preservative
◦ Lacks mineralocorticoid activity
◦ Suppresses endogenous cortisol synthesis
◦ Has a far longer half life than hydrocortisone
◦ Is many times more potent than cortisol
May be as much as 150x more powerful d/t amplifying effect of its prolonged half-life
Meikle, Am J Med 1977
Hydrocortisone is
◦ Identical to native cortisol
◦ Can be obtained without preservative
◦ Provides mineralocorticoid activity
◦ May suppress HPA axis at high doses, but does not do so at lower doses

First premise: at high doses ALL glucocorticoids impair growth as a natural consequence of their actions.
◦ They suppress cell growth and proliferation
◦ They promote differentiation, or “maturation”
◦ Therefore, high doses given to fetal or neonatal animals result in growth impairment
2 types of steroid receptors in the brain: mineralocorticoid and glucocorticoid
Both in high density in the hippocampus – an area of the brain critical to learning and memory
Under basal conditions, cortisol binds primarily to mineralocorticoid receptors
Under stressful conditions, cortisol also binds to glucocorticoid receptors
Dex suppresses cortisol production (producing a “chemical adrenalectomy”) and binds ONLY to glucocorticoid receptors
Cortisol deficiency (adrenalectomy) in adult animals leads to neuronal apoptosis in the hippocampus
Dexamethasone also leads to neuronal apoptosis in both adrenalectomized & control animals
Corticosterone (=cortisol in rats) protects animals from DEX-induced apoptosis
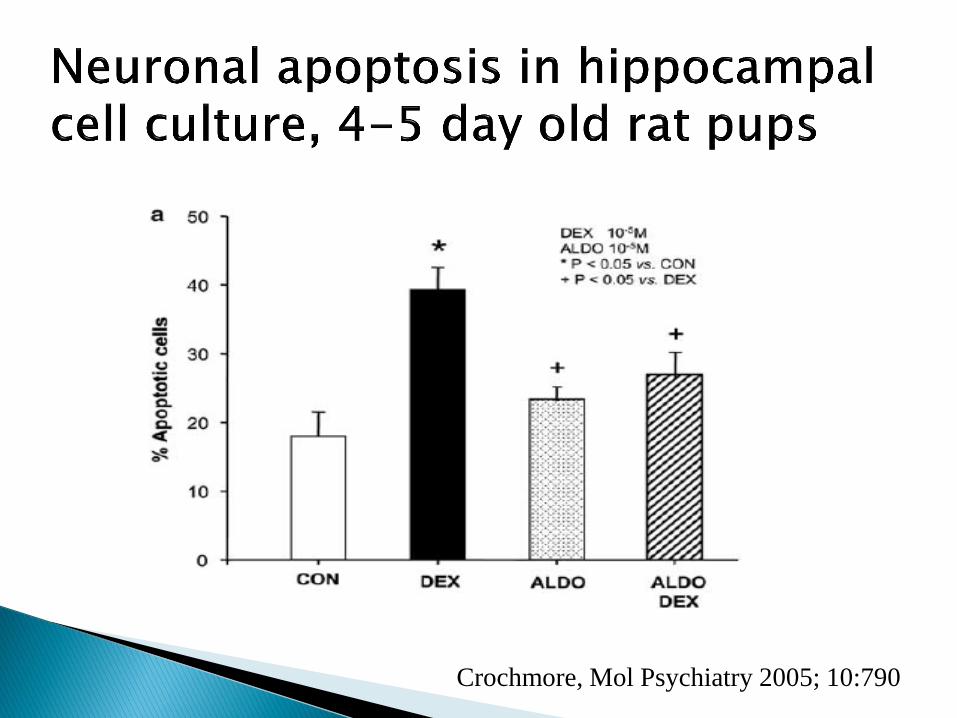
Crochmore, Mol Psychiatry 2005; 10:790
Preemies have hippocampal volume on MRI Isaacs Pediatr Res 2001; 47:713
Preemies treated with dex have hippocampal volume vs. controls (small cohort studies)
Murphy Pediatr 2001; 107:217
Parikh Pediatr 2007;119:265
Preemies treated with HC have no reduction in volume or increase in lesions vs. untreated controls (large cohort study & RCT)
Rademaker, J Pediatr 2007; 150:351
Parikh, EPAS2009; 3212.2
Intubated infants, <48o of age
HC 1–2mg/kg/day tapered over 12–15d
◦ Watterberg (n=40): survival w/o BPD
◦ Watterberg (n=360): no significant benefit
◦ Peltoniemi (n=51): 64% vs. 46% - NS
◦ Bonsante (n=50): survival w/o BPD
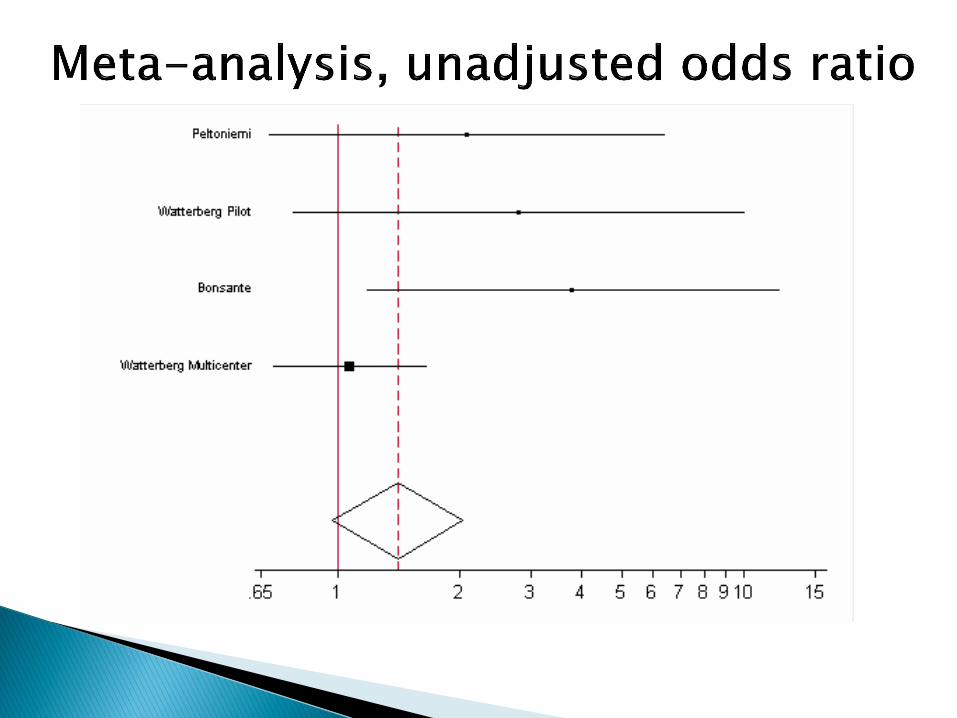
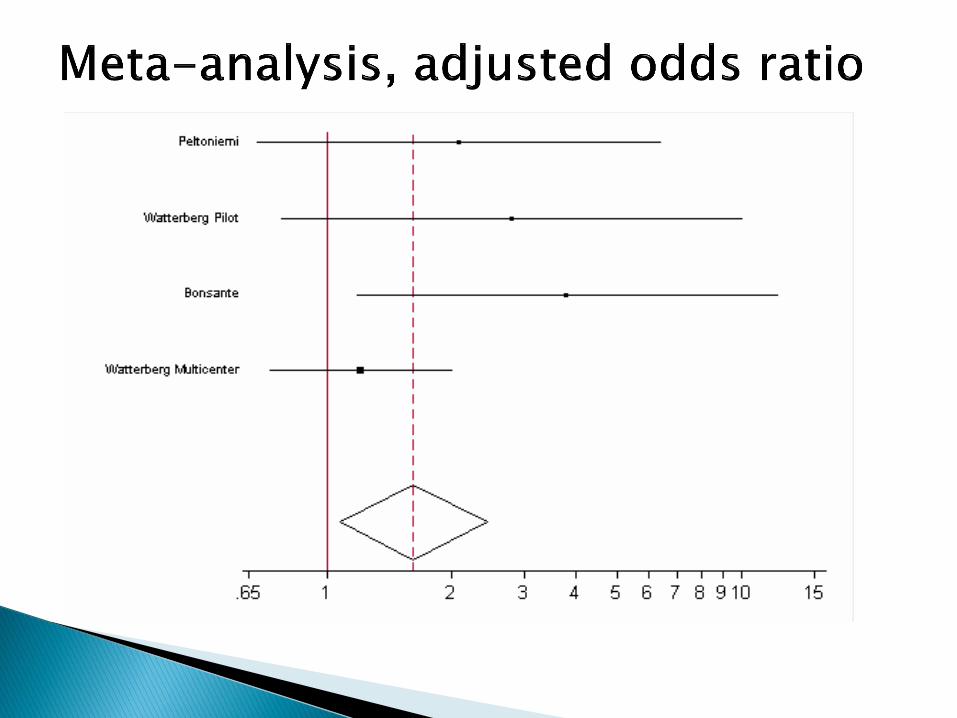
Meta-analysis (3 studies): no adverse effects
Peltoniemi, Neonatology 2009;95:240
Follow up of the multicenter trial (n=252):
◦ No adverse effects, growth or neurodevelopment
◦ Possible benefits of HC Rx:
Fewer babies with MDI <70 on Bayley II scales
More babies had attainment of object permanence –early measure of pre-frontal cortex development
Watterberg, Pediatrics 2007; 120: 40
Cohort studies of later, higher dose (5mg/kg/d tapered over 22 days)
◦ = DEX for extubation and FiO2, fewer acute adverse effects (25HC, 23dex)
Lodygensky Acta Paediatr 2003; 92:827
◦ No differences between HC-treated and larger, more mature, less sick comparison group on functional/structural outcomes at up to 8-10 years of age (62HC, 164 control)
Rademaker J Pediatr 2007; 150:351
Infants enrolled at10 – 21 postnatal days
◦ Intubated, mechanically ventilated
◦ Respiratory index score (MAP x FiO2) >2
HC: 3mg/kg/day tapered over 7 days
No mandatory extubation specified
Survival w/o severe BPD: 3/31(10%) vs 5/33(16%)
Volumetric MRI – no adverse effect of HC
Parikh (abstract, PAS 2009)
“the benefits…especially dex, may not outweigh the risks” ◦ Facilitates extubation, BPD, but adverse effects
GI perforation
Hyperglycemia, hypertension
Hypertrophic cardiomyopathy
Growth failure
Increased cerebral palsy, abnormal neurologic exam
“a compelling need for long term follow up”
HC – few positive or negative effects
Halliday/Ehrenkranz/Doyle, Cochrane review 2009
High dose DEX (0.5mg/kg/day) associated with numerous adverse effects
There is no basis for postulating that such high doses confer additional benefit over lower dose therapy
Meta-analysis concluded cumulative dose may BPD w/o adverse neurodevelopment
Onland, Pediatrics 2009; 123:367
But: RCTs comparing higher/lower daily doses have not shown benefit from higher doses
This therapy cannot be recommended
Lower dose DEX (<0.2mg/kg/day) may facilitate extubation
Limited data suggest short- and long-term adverse effects vs. higher dose
Additional RCTs that include long-term assessment of neurodevelopmental outcomes are warranted
Pending additional data, Rx cannot be clearly recommended
RCTs: Early HC may survival w/o BPD
Cohort data: later therapy may extubation
Long-term neurodevelopmental outcomes are reassuring
Further RCTs of both early and later HC are warranted, to
◦ Target populations that may derive most benefit
◦ the incidence of spontaneous GI perforation
◦ Assess the efficacy of later HC therapy to facilitate extubation
Awaiting further studies, clinicians must balance
◦ the known adverse effects of BPD with
◦ the potential adverse effects of treatments
“it appears prudent to reserve the use of late corticosteroids to infants who cannot be weaned from mechanical ventilation and to minimize the dose and duration of any course of treatment”
Halliday/Ehrenkranz/Doyle, Cochrane Database 2009
After discussing with the parents
Based on the limited available evidence, the clinician might consider the lowest dose and shortest course of DEX shown to be efficacious, or a similar course of HC, e.g.
◦ 0.15mg/kg/day DX (Doyle Pediatr 2006; 117:75)
◦ 4 – 6 mg/kg/day HC
◦ tapered over 10 days
What are we trying to achieve?
◦ Treatment of relative adrenal insufficiency
- Defined as cortisol values inappropriately low for the degree of stress/illness, together with cardiovascular dysfunction/shock
◦ Or, possibly, a pharmacologic effect of HC on cardiovascular system
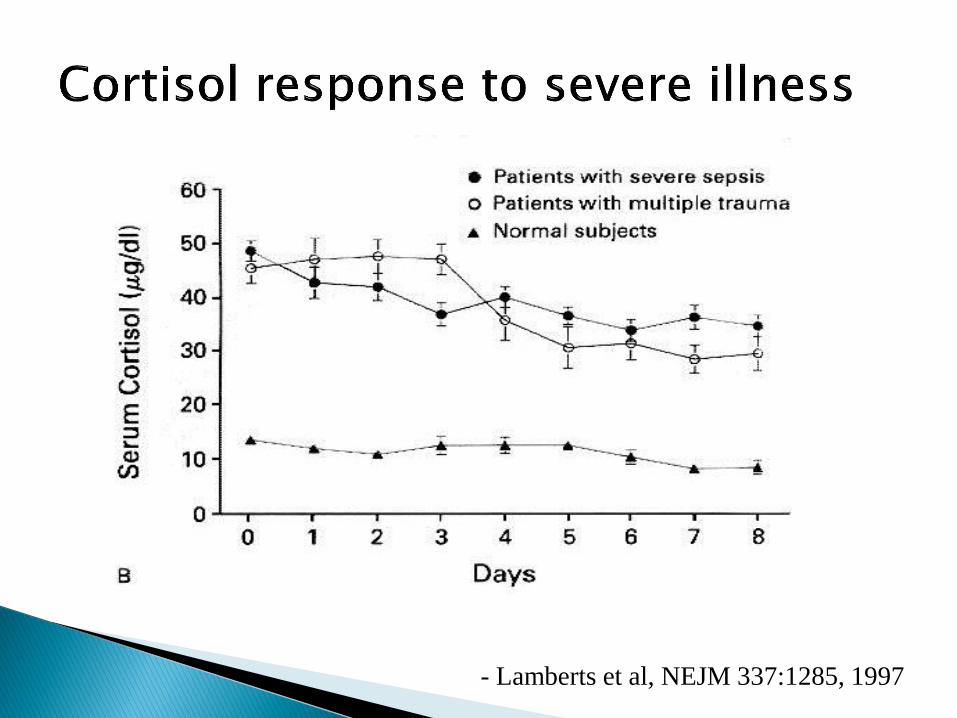
- Lamberts et al, NEJM 337:1285, 1997
820 gram 26 week EGA infant
Initially did well on low ventilator settings after surfactant, extubated to CPAP day 3
Deteriorated day 8, re-intubated, dx PDA
Indomethacin Rx x 2, failed, ligated D14
Post-op: hypotension, poor perfusion, decreased urine output
Cortisol 6.2g/dl – responded to HC Rx
Infants on dopamine have ↓basal and stimulated cortisol
Scott & Watterberg, Pediatr Res 37:112, 1995
Ng et al Arch Dis Child 89:F119, 2004
Arterial BP correlates with cortisol production
Arnold et al, Pediatric Res 44: 876, 1998
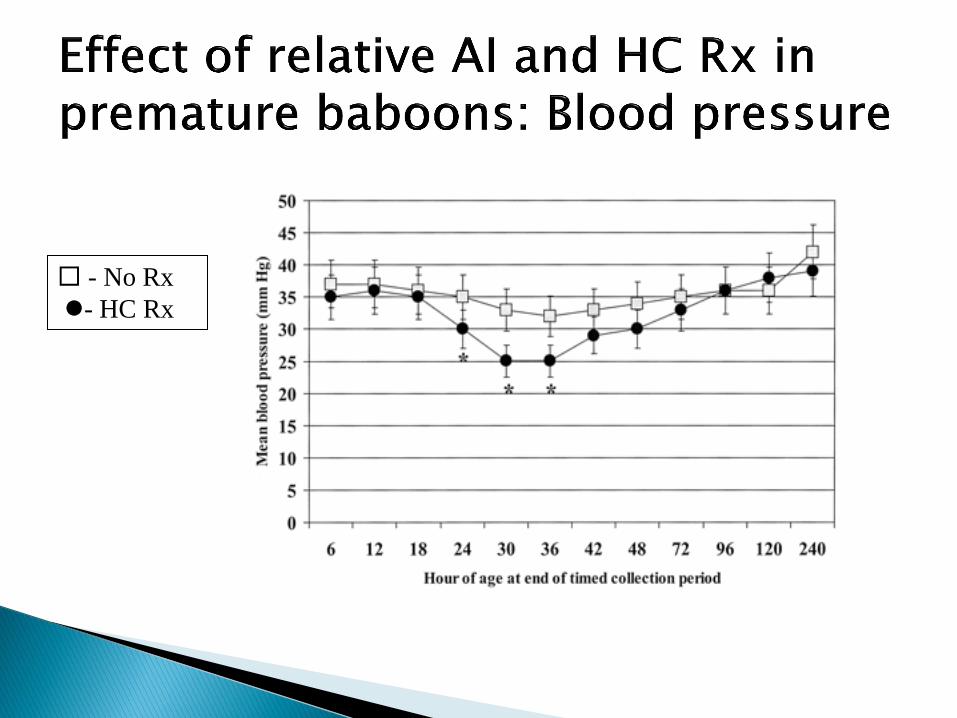
↓ cortisol production correlates with poor CV function in premature baboons
Yoder et al, Pediatr Res 51:426, 2002
San Antonio group – 125d baboons have “impaired CV function early in life”
~ 2/3 given volume & inotropic support
Some are refractory, but respond to HC
They decided to study cortisol production and CV function
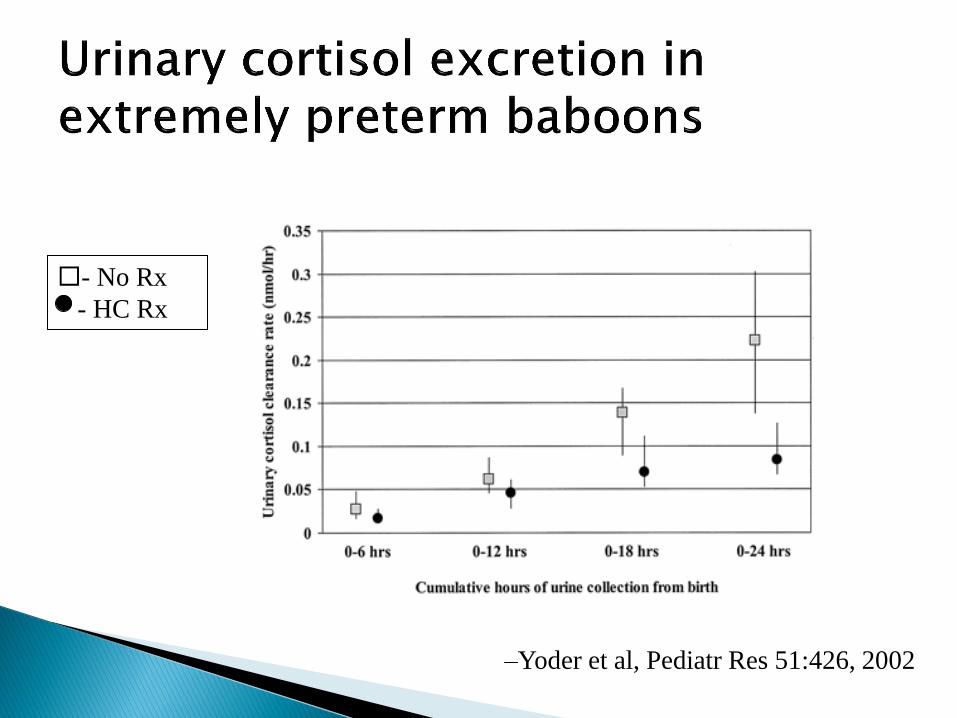
–Yoder et al, Pediatr Res 51:426, 2002
- No Rx
- HC Rx
- No Rx
- HC Rx
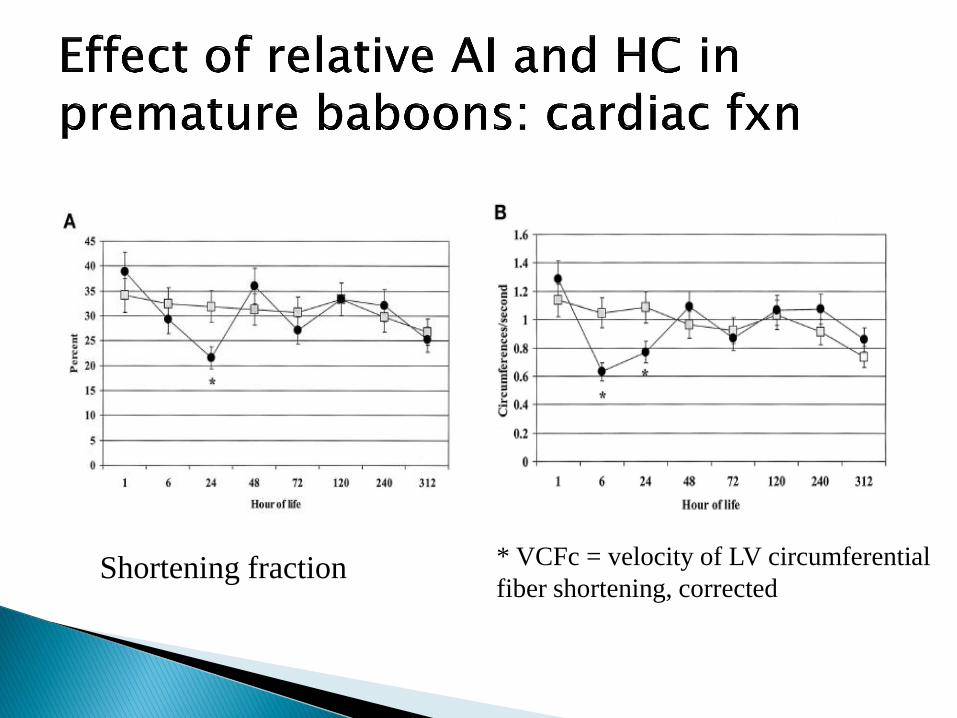
* VCFc = velocity of LV circumferential
fiber shortening, corrected Shortening fraction
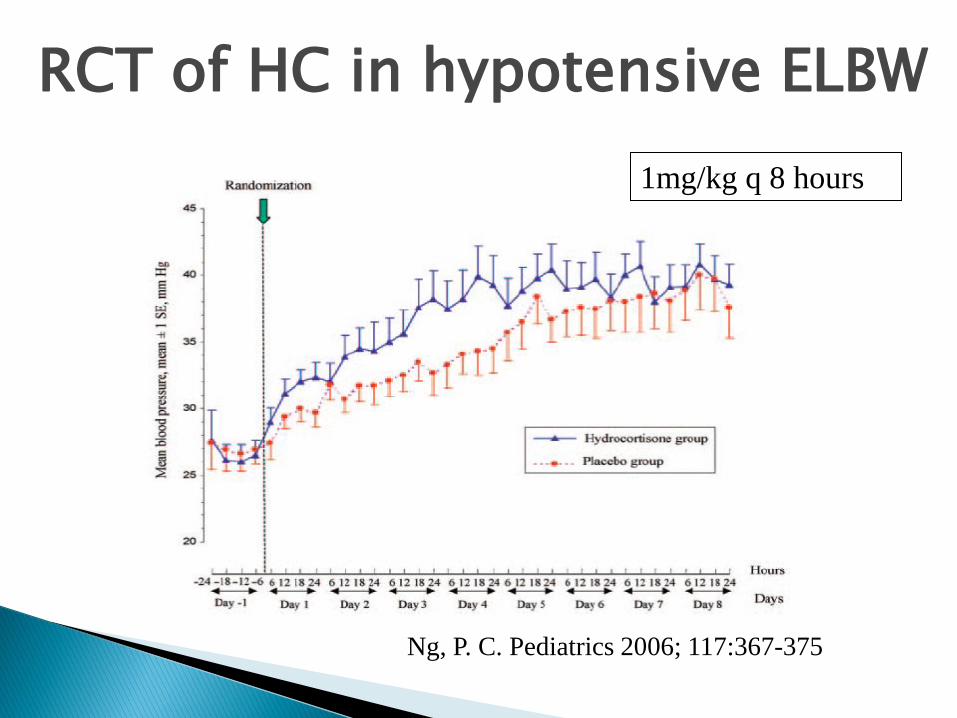
Ng, P. C. Pediatrics 2006; 117:367-375
RCT of HC in hypotensive ELBW
1mg/kg q 8 hours
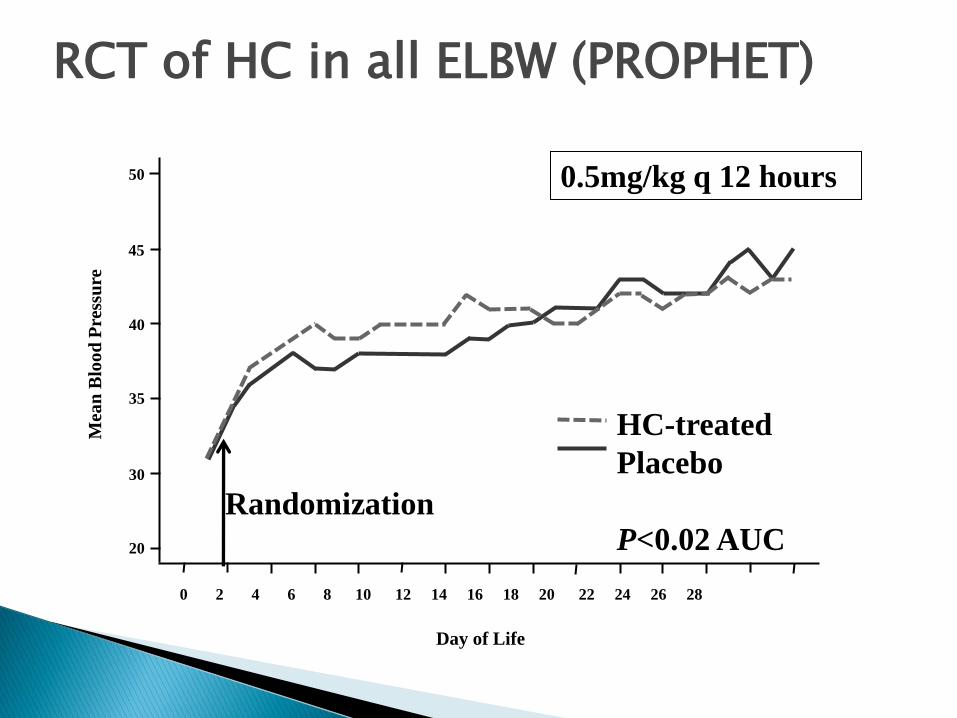
RCT of HC in all ELBW (PROPHET)
50
45
40
35
30
20
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Mea
n B
loo
d P
ress
ure
Day of Life
HC-treated
Placebo
P<0.02 AUC Randomization
0.5mg/kg q 12 hours
Low values seen in critically ill patients
Associated with cardiovascular dysfunction
◦ But…
Concern about short and long term effects of prematurely elevated cortisol values
Interaction with other drugs – indomethacin
“Need additional studies”
HC may be more appropriate for relative AI than high dose vasopressors, but…
◦ Very prolonged half-life
(adults, <2 hours; ELBW infants, mean 8-13 hours)
◦ Doses of 3 – 6 mg/kg/day may lead to very high serum levels
Perhaps, draw a cortisol level, then
◦ Try a test dose of 1 mg/kg
◦ Dose of 0.5mg/kg q 12 hours (~8-10mg/m2/d)
◦ Evaluate CV effects
“Fetal” origins of adult disease
Perinatal origins of adult disease
Many developmental events occur during a specific window of opportunity
Changing the environment in that window may permanently change outcomes.
Low birth weight in term infants has been linked to a variety of adult diseases
Cardiovascular – hypertension, MI, stroke
Metabolic syndrome, Type II diabetes
Polycystic ovary syndrome
End-stage renal disease
Depression
The „thrifty gene‟ hypothesis:
◦ malnutrition in utero changes in gene expression to adapt to relative starvation
◦ adaptive in utero, maladaptive when food is plentiful
◦ may be analogous to exposure of subsistence cultures to modern abundance of food
Linked with fetal exposure to excess cortisol
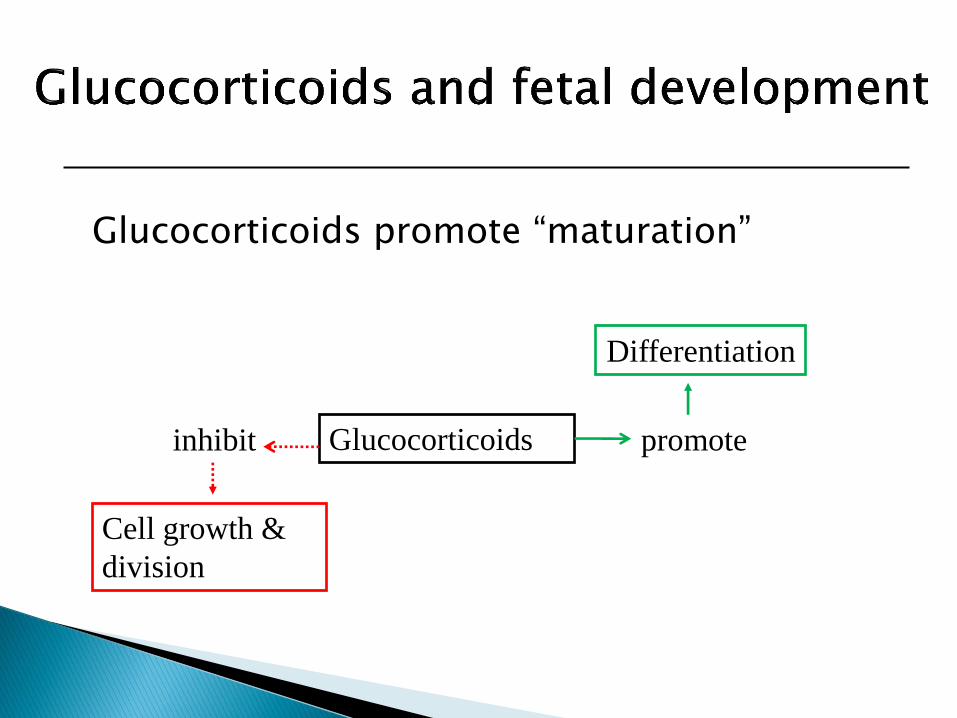
Glucocorticoids promote “maturation”
Cell growth &
division
Differentiation
Glucocorticoids inhibit promote
In animal models, fetal exposure to high dose steroids results in:
◦ Decreased brain weight
◦ Decreased organ weights
◦ Decreased total body weight
Postnatal exposure to high-dose dexamethasone in premature infants results in:
◦ Decreased weight gain
◦ Decreased head growth
◦ Decreased height at school-age
“The ex-utero fetus”
They have no choice – increased cortisol is necessary to survive under stress
And cortisol is necessary to control inflammation.
But . . . could increased exposure to cortisol contribute to some of their long-term adverse outcomes?
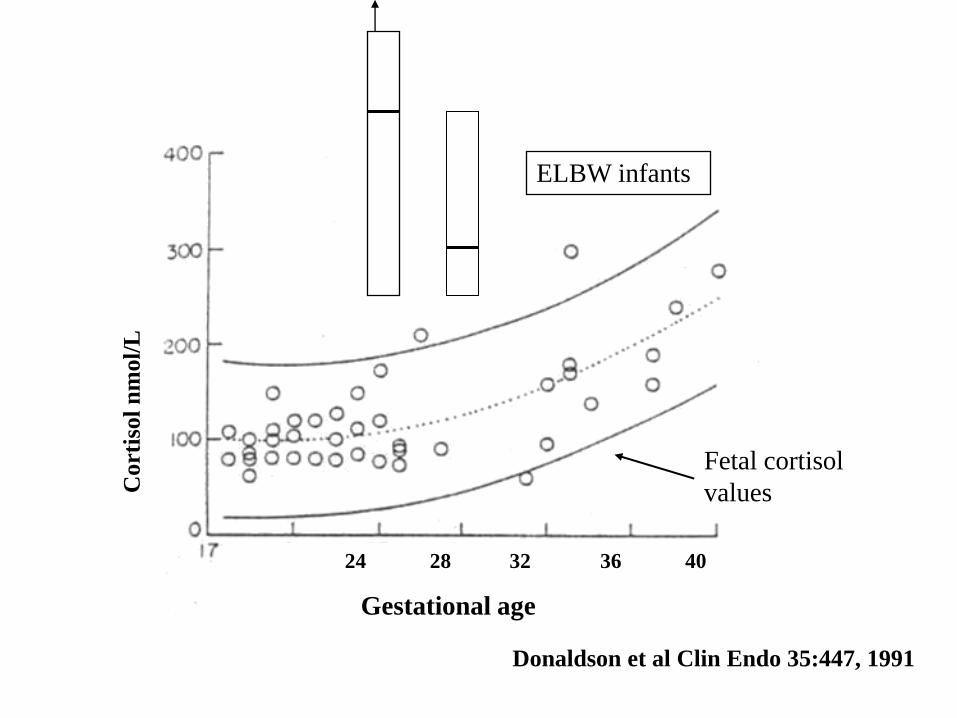
Donaldson et al Clin Endo 35:447, 1991
Cort
isol
nm
ol/
L
ELBW infants
Fetal cortisol
values
24 28 32 36 40
Gestational age
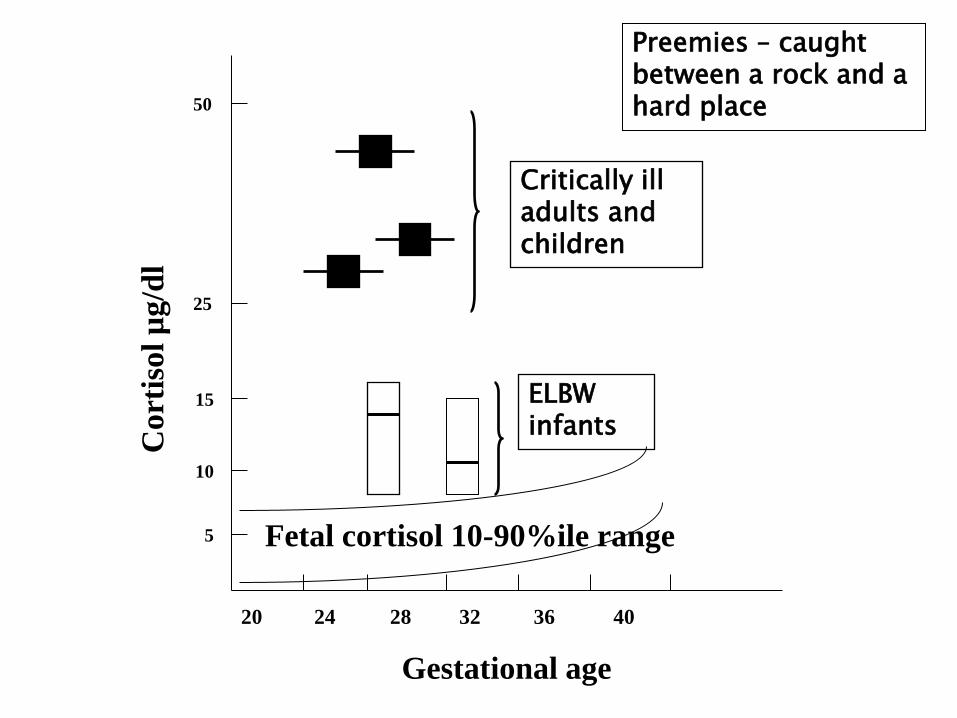
Cort
isol
µg/d
l
20 24 28 32 36 40
Gestational age
5
50
25
10
15
Critically ill adults and children
ELBW infants
Fetal cortisol 10-90%ile range
Preemies – caught between a rock and a hard place
Short stature
head circumference & brain volume
neurodevelopmental difficulties
blood pressure
Other adverse outcomes in adulthood?
◦ Little work done so far, but…
50 children tested at 4 – 10 years of age
Born at ≤ 32 weeks (38 AGA, 12 SGA)
Insulin sensitivity (x10-4/min-
1[mU/liter])
◦ term AGA infants: 21.6
◦ term SGA infants: 15.1
◦ Preterm AGA/SGA: 14.2/12.9 (p<0.01 vs control)
◦ Hofman et al, NEJM 351:2179, 2004
Exogenous glucocorticoid:
◦ Strong medicine
◦ Powerful side effects
◦ Randomized trials with long term follow-up are essential to assess risk/benefit
Endogenous glucocorticoid:
◦ Preterm infants have exposure vs. fetus
◦ May affect long term outcomes
◦ Could decreasing stress in the nursery improve outcomes?