Embed Size (px)
Citation preview

143PEDIATRIC DENTAL JOURNAL 15(1): 143–146, 2005
143
Received on September 29, 2004
Accepted on January 7, 2005
Large sialolith in the submandibular gland of a child
Ikuri Konishi*1,2, Satoshi Fukumoto*2, Aya Yamada*2,Kazuaki Nonaka*2 and Taku Fujiwara*1
*1 Division of Pediatric Dentistry, Department of Developmental and Reconstructive Medicine,Nagasaki University Graduate School of Biomedical Sciences1-7-1 Sakamoto, Nagasaki 852-8588, JAPAN
*2 Section of Pediatric Dentistry, Division of Oral Health, Growth and Development,Faculty of Dental Science, Kyushu University3-1-1 Maidashi, Higashi-ku, Fukuoka 812-8582, JAPAN
Abstract Sialolithiasis is a disorder encountered by oral surgeons that israrely seen in children, although it is rather common in adults. Most sialolithfound in children are smaller than 5 mm in diameter, and the majority ofreported cases have been treated by surgically. We report a 9-year-old boy witha sialolith that measured 12�3.5�3 mm, which had developed in Wharton’sduct and was then spontaneously passed.
than 5 mm in children2,3).Children who present with sialolithiasis are
generally healthy and without systemic illness,except for symptoms of acute inflammation. Mostof their chief complaints regard intermittent andunilateral pain and swelling in the submandibularregion, usually associated with eating.
We describe here a case of submandibular glandsialolithiasis in a 9-year-old child, which resulted inthe formation of a calculus greater than 10 mm indiameter that was located in Wharton’s duct on theright side.
Case report
A 9-year-old boy was referred to our hospital withthe chief complaints of tenderness and swellingof the floor of the mouth with spontaneous pain,which had occurred over a period of 3 days. Thepatient was first seen by a general practitioner,who made a diagnosis of acute sialodochitis, andprescribed a 2-day regimen of an antibiotic (cefotiamdihydrochloride). The past medical history of thepatient was unremarkable. Physical examinationrevealed no acute distress, and body temperature,pulse, and blood pressure findings were within normalranges. Clinical examination revealed swelling in
Introduction
A sialolith is a calcareous concretion that mayoccur in the ducts of the major or minor salivaryglands, or within the glands themselves. Thesubmandibular gland is most commonly affected,in most cases, the calculus is found close to theorifice or in the anterior two-thirds of Wharton’sduct. Formation of a sialolith is considered to be theresult of calcium salt around a central nidus, whichmay consist of desquamated epithelial cells, bacterialor micro-organismal decomposition products, orforeign bodies. The high incidence of submandibularcalculi in this gland has been explained by thehigh concentration of calcium salts, pH, and mucincontent located there1). Although sialolithiasis is notuncommon in adults, only about, 3% of cases havebeen reported in children. This low frequency ofsialolithiasis in young patients is due to the longperiod required for sialolith formation, faster salivaryflow rate, lower concentrations of calcium andphosphate in saliva, and smaller orifice size forforeign body entrance. In adults, average calculussize is 6.3 mm (range, 2–30 mm), but most are less
Case Report
Key wordsChild,Sialolithiasis,Submandibular gland

144 Konishi, I., Fukumoto, S., Yamada, A. et al.
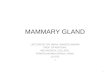
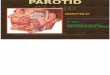
the right submandibular region, and diffuse swellingof the right submandibular gland was palpable withassociated tenderness (Fig. 1). In addition, the rightsubmandibular nodes were palpable and about thesize of the little finger, and showed mobility andsignificant pain. Trismus was not present. Intraoralexamination revealed that the left-side Wharton’sduct was normal, with clear salivary flow producedby gentle manipulation of the gland. In contrast,Wharton’s duct on the right side exhibited aprominent edema, with swelling, discharge of pus,
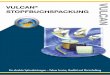
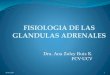
and erythema of the orifice (Fig. 2). Radiographicexamination revealed a radiopaque mass in theanterior one-third of Wharton’s duct, close to theorifice (Fig. 3). A diagnosis of submandibularacute sialodochitis caused by a sialolith was made.One day after beginning the prescribed antibiotics,a sialolith spontaneously migrated from the gland(Fig. 4). The calculus was an ash gray-colored oval,and measured approximately 12mm long and 3.5 mmin diameter.
Physicochemical chemical analysis revealed the
Fig. 1 Diffuse swelling in the area of the right submandibulargland
Fig. 2 Image of mouth floor showing edema, swelling, pusdischarge, and erythema of Wharton’s duct orifice
Fig. 4 The calculus following passage from Wharton’s ductFig. 3 Occlusal view showing the sialolith in the anteriorportion of Wharton’s duct on the right side

145LARGE SIALOLITH IN A CHILD
calcium carbonate may provide evidence that thissialolith was made of saliva, but not other hardtissue or foreign material. Approximately 40% ofall submandibular stones are found in the distalportion of Wharton’s duct or at the orifice, andcan be removed by simple intraoral proceduresperformed under local anesthesia. For calculi thatlie in the proximal duct or gland, the treatment ofchoice has been sialoadenectomy, which is effectivein eradicating symptoms, but carries the risk of nerveinjury. Recently, several new minimally invasivetechniques have been introduced for the treatment ofsialolithiasis, such as extracorporeal sonography andintracorporeal endoscopically controlled lithotripsy,which have completely changed therapeutic methodsutilized7,8). In the case of parotid duct stones, thelong-term outcome with extracorporeal lithotripsyhas been quite satisfactory, with 50% of all patientsreported to be free of stones and 80% free ofsymptoms9). In comparison, fewer than 30% ofpatients who suffer from sialolithiasis of the sub-mandibular gland and receive lithotripsy treatmentare reported to be free of stones8,10–12). Therefore, thebenefits of a minimally invasive technique, comparedto those of other moderately invasive or otherinvasive surgical and gland-preserving techniques,must be considered for these patients.
Various techniques of sialodochotomy havebeen described in the literature, with the majorpoint of concern being the risk of injury to thelingual nerve, which passes in close proximity toWharton’s duct13–17). Surgical excision of the gland isrecommended in cases with extreme proximal stonelocalization, due to the anatomical circumstancesand the assumption that the submandibular salivarygland will not tend to exhibit improvement afteryears of obstruction and recurrent inflammation14,18).
Diagnosis is very important for correct selectionof treatment of sialolithiasis in children. As in mostcases with spontaneous passage of a sialolith, inthe present case the stone was localized in anteriorpotion of Wharton’s duct, and its passage did notdepend on its size. Preservation of gland functionin conjunction with low-level risk and minimaldiscomfort for the patient should be the primaryobjectives of treatment of sialolithiasis. Apart fromproblems such as scar formation, disturbances ofskin sensation, and injury to the gustatory nerves,transient functional disturbances of the marginalbranch of the facial nerve are most often encounteredin up to 12.5% of open gland excisions. Further,
presence of 67% calcium phosphate, 28% proteinand 5% calcium carbonate. The patient had anuncomplicated recovery and was released 1 day afterthe migration of the calculus. He was asymptomatic,and a subsequent follow-up examination 1 monthlater revealed the disappearance of submandibularswelling. Four months later, there were no signs orsymptoms of recurrence.
Discussion
Although sialolithiasis accounts for 50% of themajor salivary gland diseases localized to the headand neck region, individual reports of management ofpediatric patients with sialoadenitis or sialolithiasisare limited. In children, 80% to 90% of cases arefound in the submandibular gland, compared with5% to 10% in the parotid gland, and approximately5% in the sublingual and other minor salivaryglands3–6). The submandibular gland salivary outflowincludes large amounts of calcium and phosphorus,compared with that of the parotid gland, and includesmucin, which has a high viscosity. Further, thesubmandibular duct has an opening on the floor ofthe month that can easily retain saliva, and Wharton’sduct is longer than other sublingual ducts. Thesecharacteristics may account for the preponderanceof reports of occurrence in this gland.
Most sialoliths previously reported were removedusing a surgical procedure, while in a few cases theyspontaneously migrated out. In pediatric patientswith sialolithiasis, it is easy for the sialolith to bepassed from the duct, since most are located near theorifice of Wharton’s duct, salivary flow is faster thanthat from other salivary glands, maturation of thesialolith is generally poor, the tissues surroundingthe ducts are soft, the size of the sialolith is usuallyless than 5 mm in size, and swelling and pain aremilder than in adults. For these reasons, the firstchoice of treatment for pediatric sialolithiasis in thesubmandibular gland may be to wait for spontaneousmigration. In fact, a sialolith with a diameter greaterthan 10 mm in size passed from the duct 1 dayafter starting antibiotic treatment observed in thepresent case, to our knowledge, is the largest. Thesialolith is generally containing calcium phosphate,protein, and calcium carbonate. In adult cases, theratio of calcium phosphate is high compared withpediatric cases. In present case, the compositionof sialolith is approximately same as the previousreport in child. Additionally, the concentration of

146
permanent lesions have been reported in 7% ofthese cases19,20). In addition, unilateral excision ofthe submandibular gland also leads to substantialreduction of nonstimulated flow of saliva, whichmay significantly affect oral hygiene, risk of caries,and the development of xerostomia21). Conservativetreatment should therefore be selected for sialo-lithiasis in children.
A few reports have noted submandibular calculithat passed out of the duct spontaneously, 1–2days following stimulation. These were successfulresults of initial management protocols that includedinstructing the child to suck on a sour lemon ororange candy to stimulate salivary flow. In adultswith long-standing stones, exfoliation of the calculusthrough a perforation of the overlying mucosa hasbeen reported, but not a spontaneous passage throughthe duct. This is apparently because the orifice ofWharton’s duct is smaller than the lumen, thus itacts as a sphincter.
No spontaneous passage of calculi has beenreported from Stenson’s duct. This may be becauseoccurrence is less frequent, however, becauseStenson’s duct perforates the buccinator muscle,it may be anatomically difficult for stones to passspontaneously. During treatment planning, the factthat submandibular sialoliths in children have beenreported to pass spontaneously following stimulationof salivary secretion should be taken into considera-tion, especially in cases in which the surgicalalternative is a sialadenectomy.
Finally, if the sialolith is located in the anteriorthird of Wharton’s duct, antibiotic treatment shouldbe given first to treat the acute symptoms andpossibly to stimulate a spontaneous migration outthough the duct.
References
1) Doku, H.C. and Berkman, M.: Submaxillary salivarycalculus in children. Am J Dis Child 114: 671–673,1967.
2) Kaban, L.B., Mulliken, J.B. and Murray, J.E.: Sialo-adenitis in childhood. Am J Surg 135: 570–576, 1978.
3) Lustmann, J., Regev, E. and Melamed, Y.: Sialo-lithiasis. A survey on 245 patients and a review of theliterature. Int J Oral Maxillofac Surg 19: 135–138,1990.
4) Antognini, F., Giuliani, R., Magagnoli, P.P. andRomagnoli, D.: Clinico-statistical study on sialo-lithiasis. Mondo Odontostomatol 14: 38–55, 1971.
5) Yoel, J.: Pathology and Surgery of the Salivary Glands.Charles C. Thomas, Springfield, 1975, pp.364–383,854–901, 1148.
6) Mela, F., Berrone, S. and Giordano, M.: Considera-zioni clinicostatistiche sulla scialolitiasi sottoman-dibolare. Minerva Stomatol 35: 571–573, 1986.
7) Zenk, J., Benzel, W. and Iro, H.: New modalitiesin the management of human sialolithiasis. Miniminvasive Ther 3: 275–284, 1984.
8) Iro, H., Schneider, H.T., Fodra, C. et al.: Shockwavelithotripsy of salivary duct stones. Lancet 339: 1333–1336, 1992.
9) Iro, H., Zenk, J., Waldfahrer, F., Benzel, W., Schneider,T. and Ell, C.: Extracorporeal shock wave lithotripsyof parotid stones: results of a prospective clinicaltrial. Ann Otol Rhinol Laryngol 107: 860–864, 1998.
10) Ottaviani, F., Capaccio, P., Campi, M. and Ottaviani,A.: Extracorporeal electromagnetic shockwave litho-tripsy for salivary gland stones. Laryngoscope 106:761–764, 1996.
11) Schlick, R.W., Hessling, K.H., Djamilian, M.H.,Luckey, R., Kuczyk, M. and Allhoff, E.P.: ESWL inpatients suffering from sialolithiasis. Minim invasiveTher 2: 129–133, 1993.
12) Wehrmann, T., Kater, W., Marlinghaus, E.H., Peters,J. and Gaspary, W.F.: Shock wave treatment ofsalivary duct stones: substantial progress with aminilithotripter. Clin Invest 72: 604–608, 1994.
13) Seward, G.R.: Anatomic surgery for salivary calculi,part III: calculi in the posterior part of the sub-mandibular duct. Oral Surg Oral Med Oral Pathol25: 523–531, 1968.
14) Seward, G.R.: Anatomic surgery for salivary calculi,part IV: calculi in the intraglandular part of the sub-mandibular duct. Oral Surg Oral Med Oral Pathol25: 670–678, 1968.
15) Sobol, S. and Spector, G.J.: Sialodochotomy andsialolithectomy for acute calculous submaxillarysialadenitis. Laryngoscope 89: 1864–1866, 1979.
16) Novotny, G.M.: Submandibular sialolithiasis: trans-oral excision. J Otolaryngol 18: 354–356, 1989.
17) Gross, B.D.: Sialolithiasis: diagnosis and treatment.J La Dent Assoc Summer: 9–13, 1979.
18) Beahrs, O.H. and Woolner, L.B.: Surgical treatmentof diseases of salivary glands. J Oral Surg 27: 119–128, 1969.
19) Bates, D., O’Brien, C.J., Tikaram, K. and Painter,D.M.: Parotid and submandibular sialadenitis treatedby salivary gland excision. Aust NZJ Surg 68: 120–124, 1998.
20) Hald, J. and Andreassen, U.K.: Submandibular glandexcision: short-and long-term complications. ORL JOtorhinolaryngol Relat Spec 56: 87–91, 1994.
21) Cunning, D.M., Lipke, N. and Wax, M.K.: Signifi-cance of unilateral submandibular gland excision onsalivary flow in noncancer patients. Laryngoscope108: 812–815, 1998.
Konishi, I., Fukumoto, S., Yamada, A. et al.