Embed Size (px)
Citation preview
Angelo GhirarduzziResponsabile
SSD ANGIOLOGIAASMN - REGGIO EMILIA
Le TVP Distali
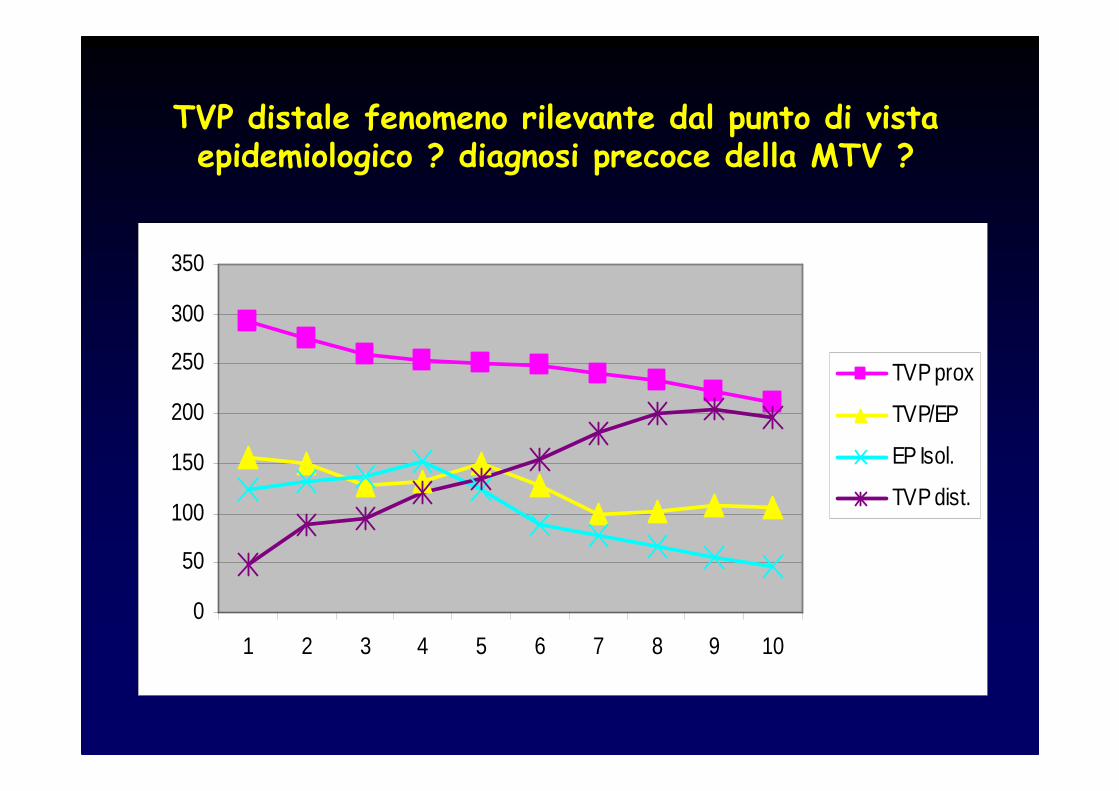
TVP distale fenomeno rilevante dal punto di vista epidemiologico ? diagnosi precoce della MTV ?
0
50
100
150
200
250
300
350
1 2 3 4 5 6 7 8 9 10
TVP prox
TVP/EP
EP Isol.
TVP dist.
E’ utile e vantaggioso ricercare la TVP DISTALE ?
SI !

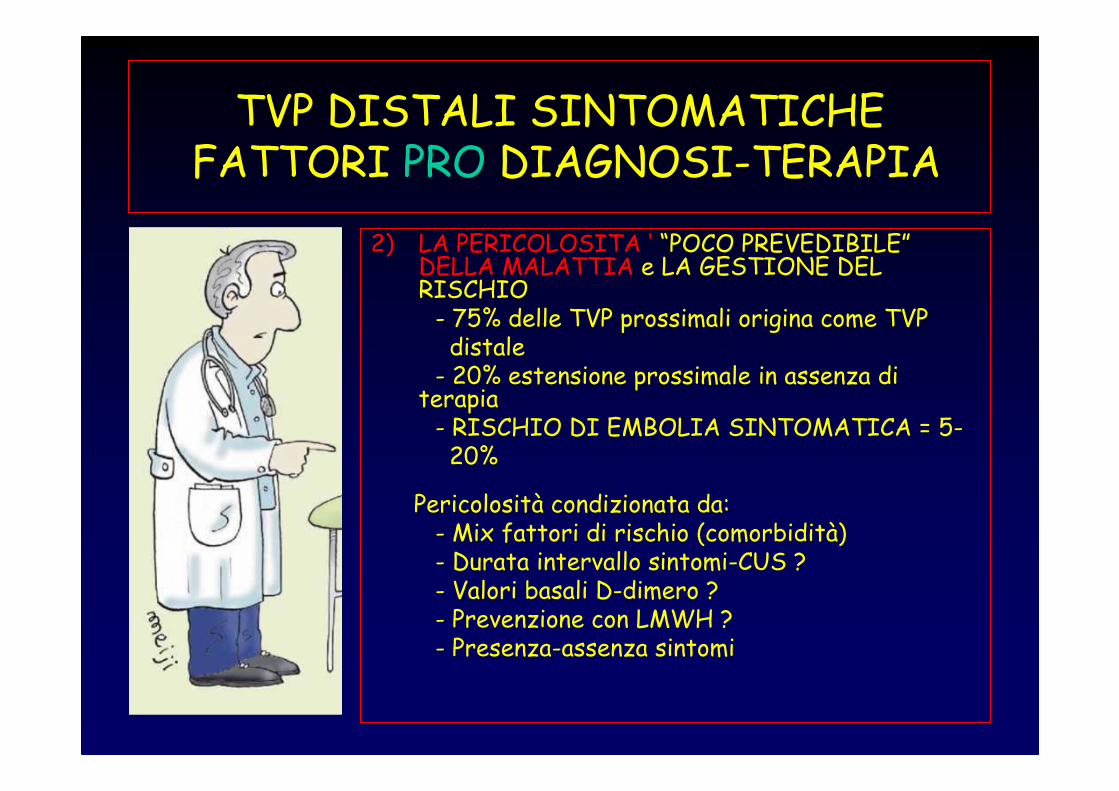
TVP DISTALI SINTOMATICHEFATTORI PRO DIAGNOSI-TERAPIA
1) I BISOGNI DEL PAZIENTE = ALLEVIARE I SINTOMI (DOLORE e IMPACCIO MOTORIO DA EDEMA). La terapia antidolorifica deve essere “patogenetica”e l’ eparina è il farmaco che risolve i sintomi da trombosi venosa nel modo più rapido e efficace.
TVP DISTALI SINTOMATICHEFATTORI PRO DIAGNOSI-TERAPIA
2) LA PERICOLOSITA ‘ “POCO PREVEDIBILE”DELLA MALATTIA e LA GESTIONE DEL RISCHIO- 75% delle TVP prossimali origina come TVP distale- 20% estensione prossimale in assenza di
terapia- RISCHIO DI EMBOLIA SINTOMATICA = 5-20%
Pericolosità condizionata da: - Mix fattori di rischio (comorbidità)- Durata intervallo sintomi-CUS ? - Valori basali D-dimero ?- Prevenzione con LMWH ?- Presenza-assenza sintomi
• TVS = terapia con LMWH per 4-6 settimane = la TVS é ± pericolosa di una TVP distale ?
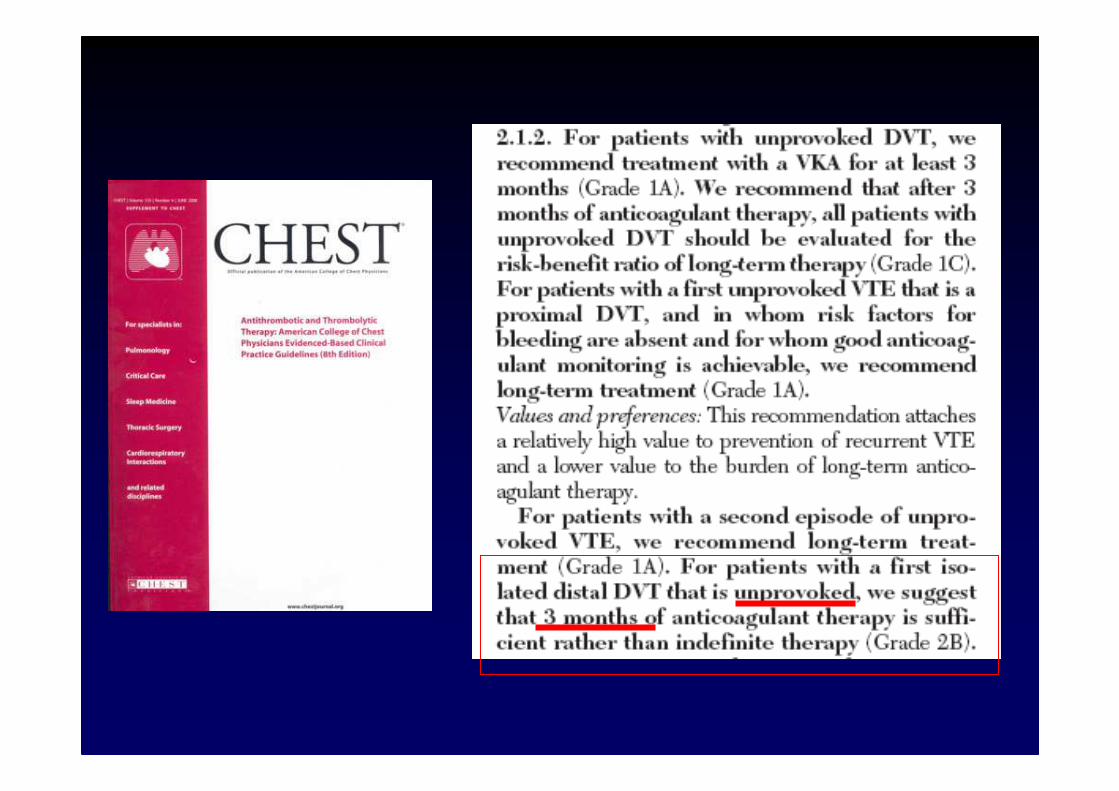
• …una volta fatta diagnosi, le TVP distali vanno trattate con warfarin per tre mesi a dosaggio pieno…..(Chest) = sono pericolose come le TVP PROSSIMALI “PROVOCATE” ?
… a volte é anche una questione dicoerenza…
TVS
TVD
TVP
LA DIAGNOSI
… a volte é anche una questione diconoscenza…
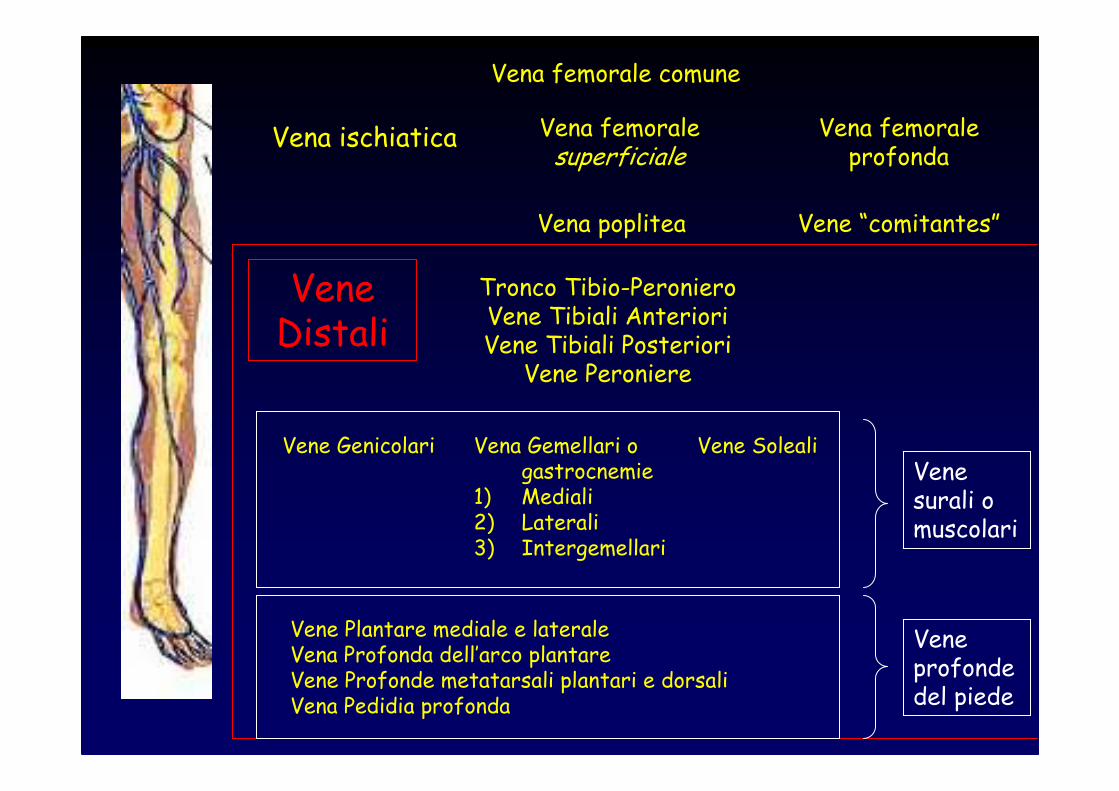
Vena femorale comune
Vena femoralesuperficiale
Vena femoraleprofonda
Vena poplitea Vene “comitantes”
Vena ischiatica
Vena Gemellari o gastrocnemie
1) Mediali2) Laterali3) Intergemellari
Vene SolealiVene Genicolari
Vene Plantare mediale e lateraleVena Profonda dell’arco plantareVene Profonde metatarsali plantari e dorsaliVena Pedidia profonda
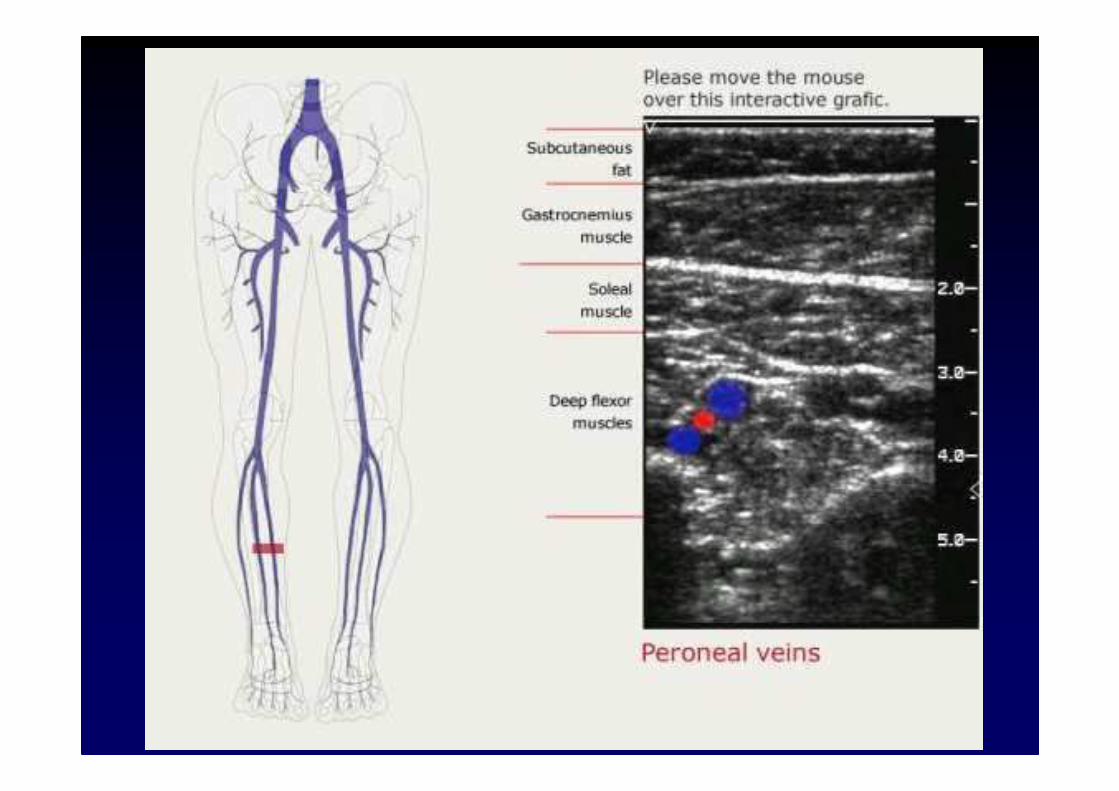
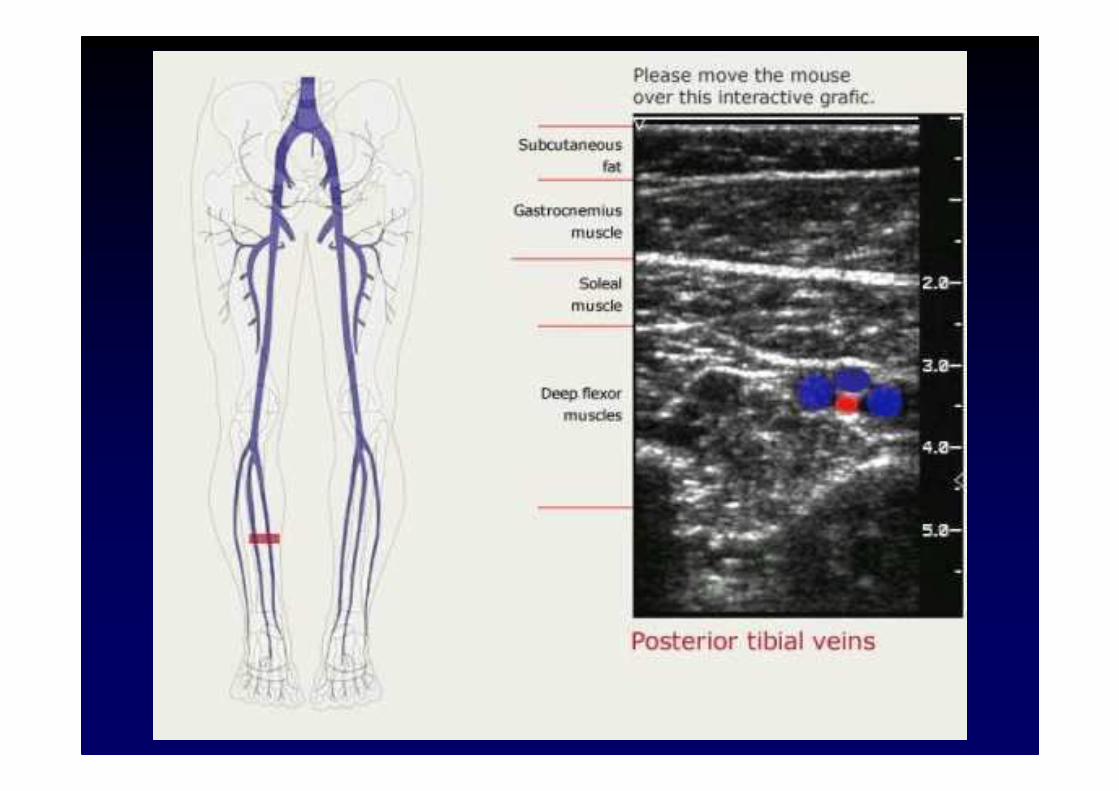
Tronco Tibio-PeronieroVene Tibiali AnterioriVene Tibiali Posteriori
Vene Peroniere
Venesurali o muscolari
VeneDistali
Veneprofondedel piede
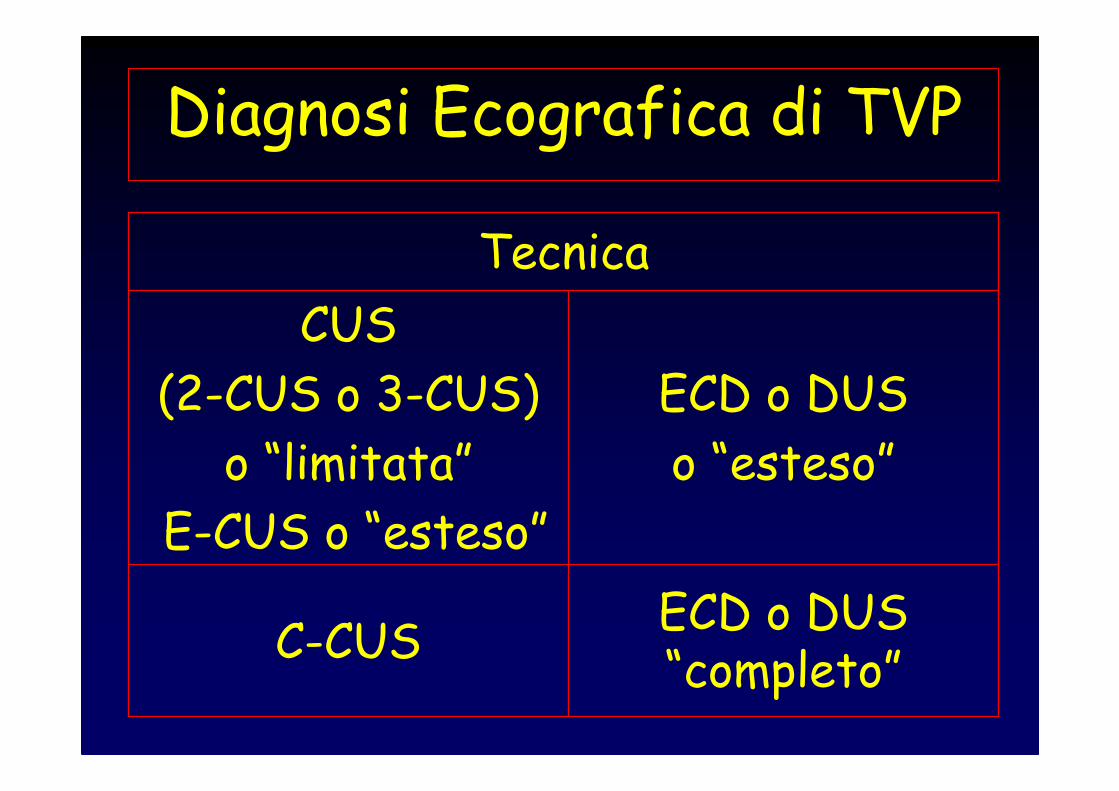
Diagnosi Ecografica di TVP
ECD o DUS “completo”
C-CUS
ECD o DUS
o “esteso”
CUS
(2-CUS o 3-CUS)
o “limitata”
E-CUS o “esteso”
Tecnica
Strategia diagnostica Ecografica nella TVP
InpatientsOutpatients
AsintomaticiSintomatici
Pazienti
Pazienti Sintomatici
TVP PROSSIMALE
CUS
o “CUS semplificata”
o 2-CUS / 3-CUS
VenaVenafemoralefemoraleprofondaprofonda
VenaVenafemoralefemorale
VenaVenagrandegrandesafenasafena
Vena Vena popliteapoplitea
DecubitoDecubitopronoprono
DecubitoDecubitosupinosupino
Legamento inguinaleLegamento inguinale
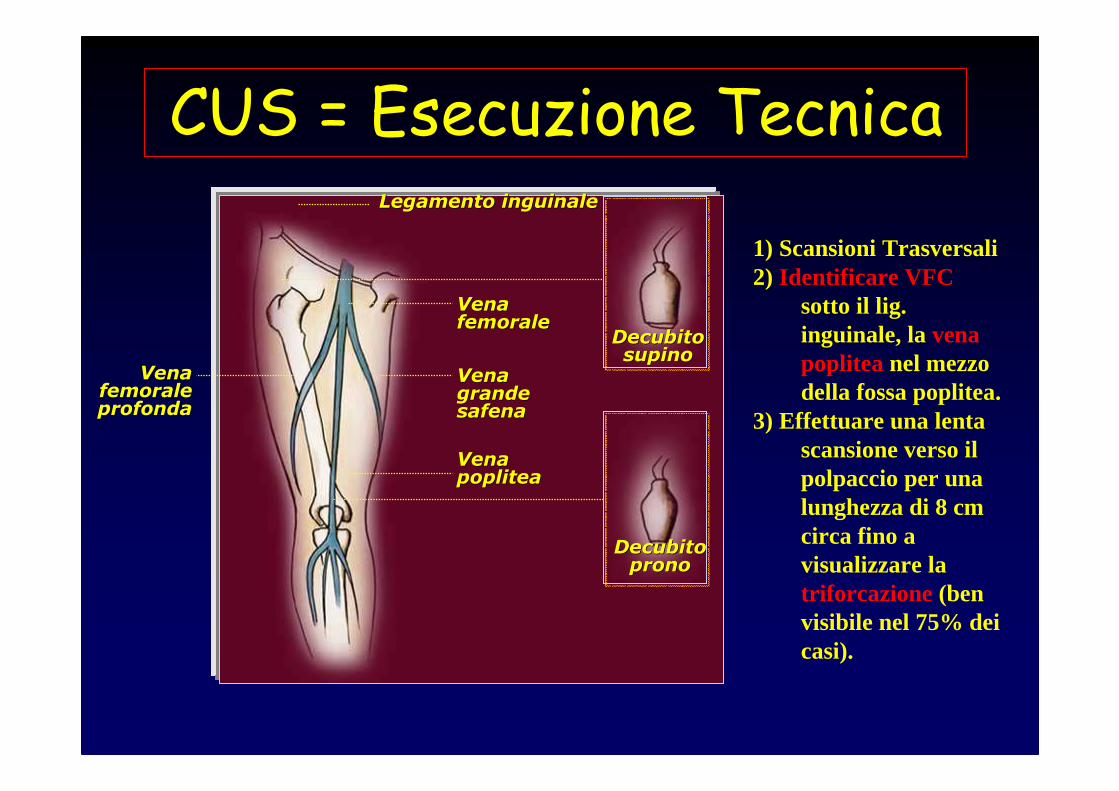
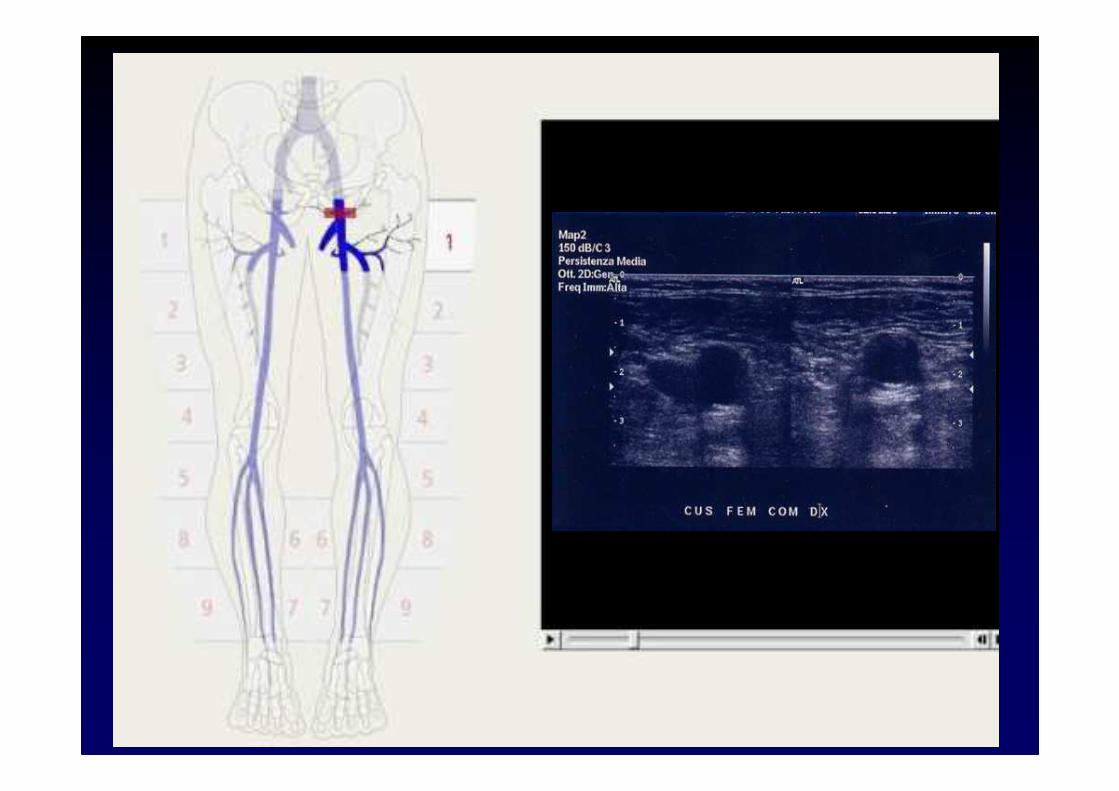
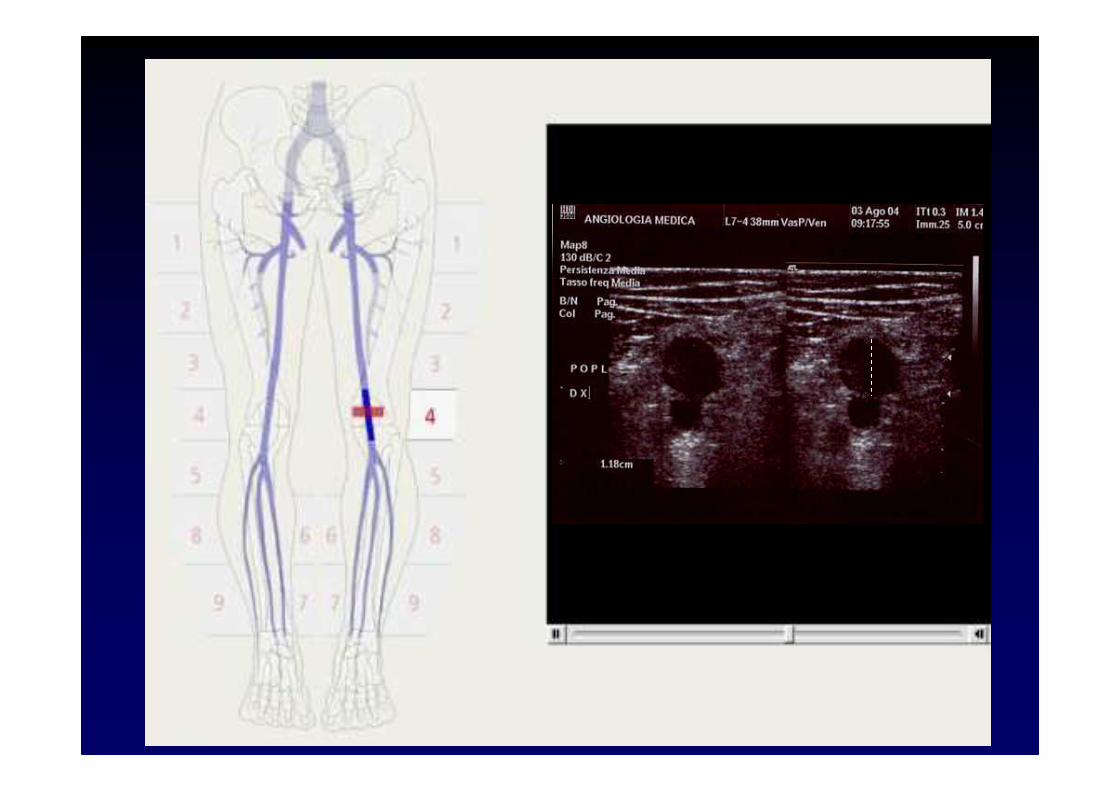
CUS = Esecuzione Tecnica
1) Scansioni Trasversali2) Identificare VFC
sotto il lig. inguinale, la vena poplitea nel mezzo della fossa poplitea.
3) Effettuare una lenta scansione verso il polpaccio per una lunghezza di 8 cm circa fino a visualizzare la triforcazione (ben visibile nel 75% dei casi).
• Estensione del trombo (ricerca del limite superiore o testa e dell‘estensione distale)
• Caratterizzazione del trombo = parzialmente o totalmente occlusivo, flottante
E-CUS
Sensibilità = 96.5%
Specificità = 94.3%
Lensing NEJM 1989, Prandoni Thromb Haemost 1991, HejboerThromb Haemost 1991, Cogo BMJ 1998,
Studi di management o di accuratezza: CUS versus flebografia
Goodacre S, Sampson F, Thomas S et al. Systematic review and meta-analisys of the diagnostic accuracy of ultrasonography
for deep vein Thrombosis BMC Med imaging 2005
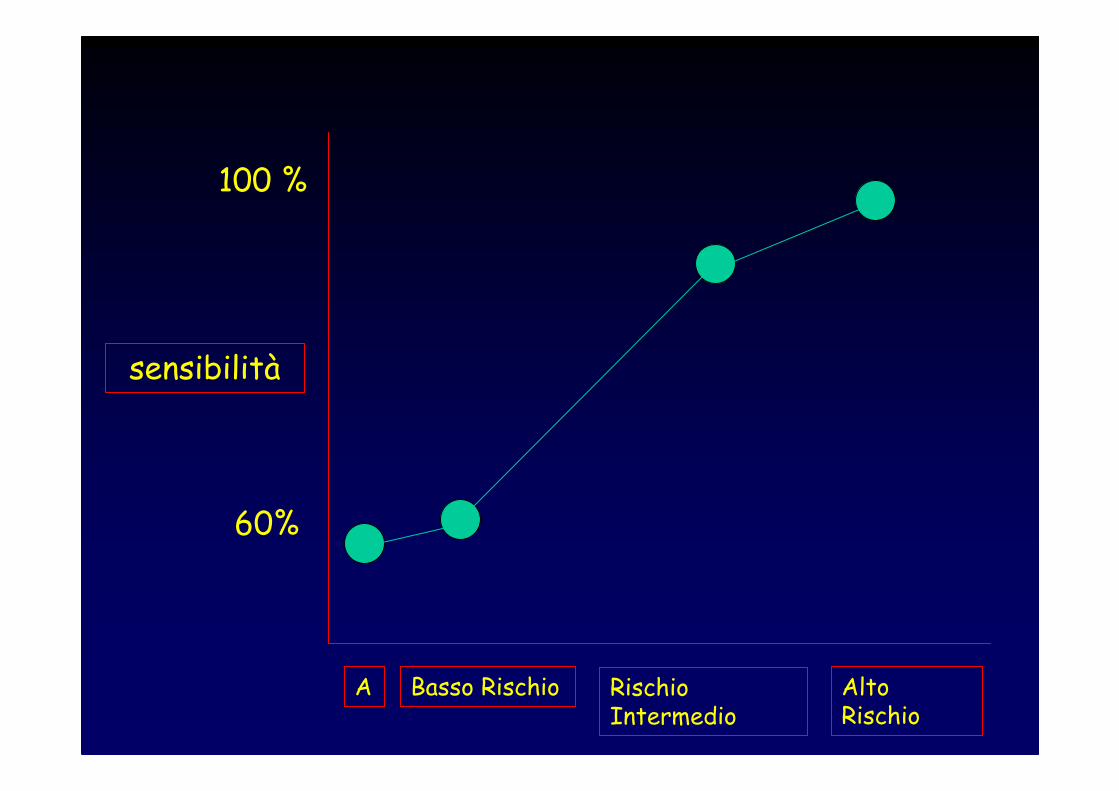
100 %
60%
sensibilità
Basso Rischio Rischio Intermedio
Alto Rischio
A
CUS e rischio di mancata visualizzazione
• Trombosi Venosa di Vaso anomalo (ex: duplicità Vena Femorale Superficiale)
• Trombosi Venosa Isolata della Femorale Profonda
• Trombosi Venosa Iliaca• TVP Distale Isolata
Gli studi di management confermano la validità della 2-CUS e 3-CUS nei casi di sospetta TVP prossimale
Kearon C Ann Intern Med 1998.
Pazienti Sintomatici
TVP DISTALE
C-CUS o “CUS completa”
o ECD “completo” ?
A single complete ultrasound investigation of the venous network for the diagnostic management of patients with a clinically suspected first episode
of deep vein thrombosis of lower limbs.
Elias E, Thromb Haemost2003
• Multicenter Study
• At 3 months no proximal DVT or PE after C-CUS
• It is safe to withhold anticoagulant therapy in patientswithclinically suspected DVT after a single, negative sonographic examination
1646 consecutive patients examined onceby a standardizedprotocol of C-CUS comprising allproximal and distalveinsas the only diagnostic test
Schellong SM.Thromb Haemost. 2003 Feb;89(2):228-34
Safety: At 3 months of follow-up, 3/1023 patientswith negative C-CUS had a symptomatic VTE episode(0.3% [95% CI 0.1%-0.8%])
Complete compression ultrasondfor the diagnosis of venous
thromboembolism. SchellongSM, Curr Opin Pulm Med2004
• The major development does not arise from technicalprogress of imaging but fromstandardizing the examination procedure.
• Interobserver variability of C-CUS resembles that of venography, as do the technical failure rates.
Specificità = 75%
Sensibilità = 76-82%
Lensing NEJM 1989, Hejboer NEJM 1993,
Wells Throm Haemost 1995
Variabilità intra ed interosservatore ?
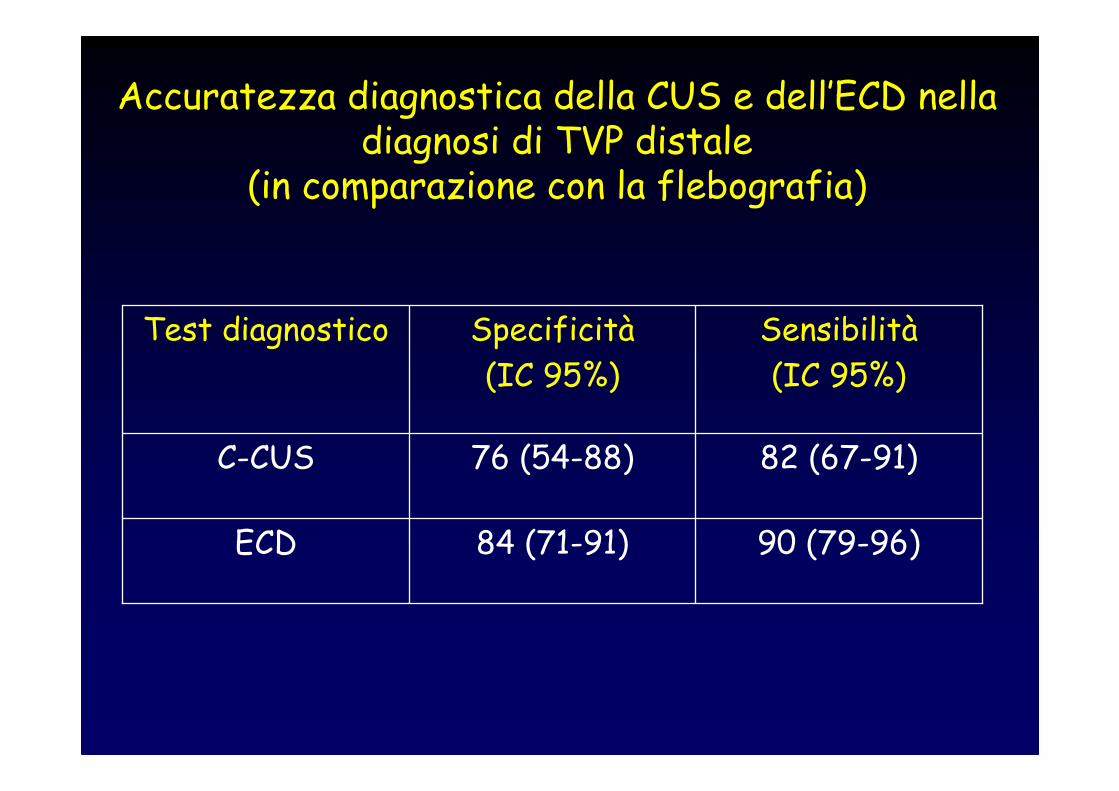
Accuratezza diagnostica della CUS e dell’ECD nelladiagnosi di TVP distale
(in comparazione con la flebografia)
90 (79-96)84 (71-91)ECD
82 (67-91)76 (54-88)C-CUS
Sensibilità
(IC 95%)
Specificità
(IC 95%)
Test diagnostico

TVP DISTALIFATTORI CONTRO DIAGNOSI
• Accuratezza diagnostica non soddisfacente
• Learning curve & expertise
Diagnosi Multimodale
DDUS
PTP
Ripetizione. Esame
•Non esiste un modello operativo universalmente valido
•E’ utile darsi regole “minime” operative comuni per poter confrontare i dati
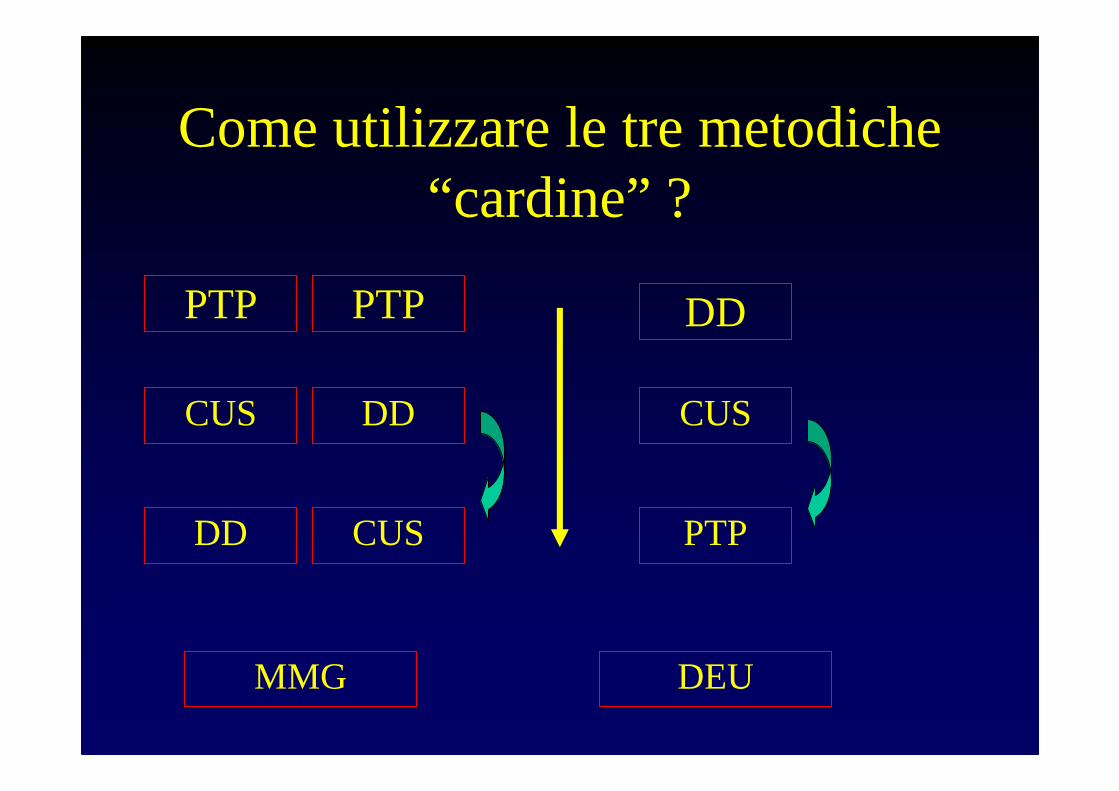
Come utilizzare le tre metodiche “cardine” ?
PTP DD
CUS CUS
DD PTP
MMG
PTP
DD
CUS
DEU
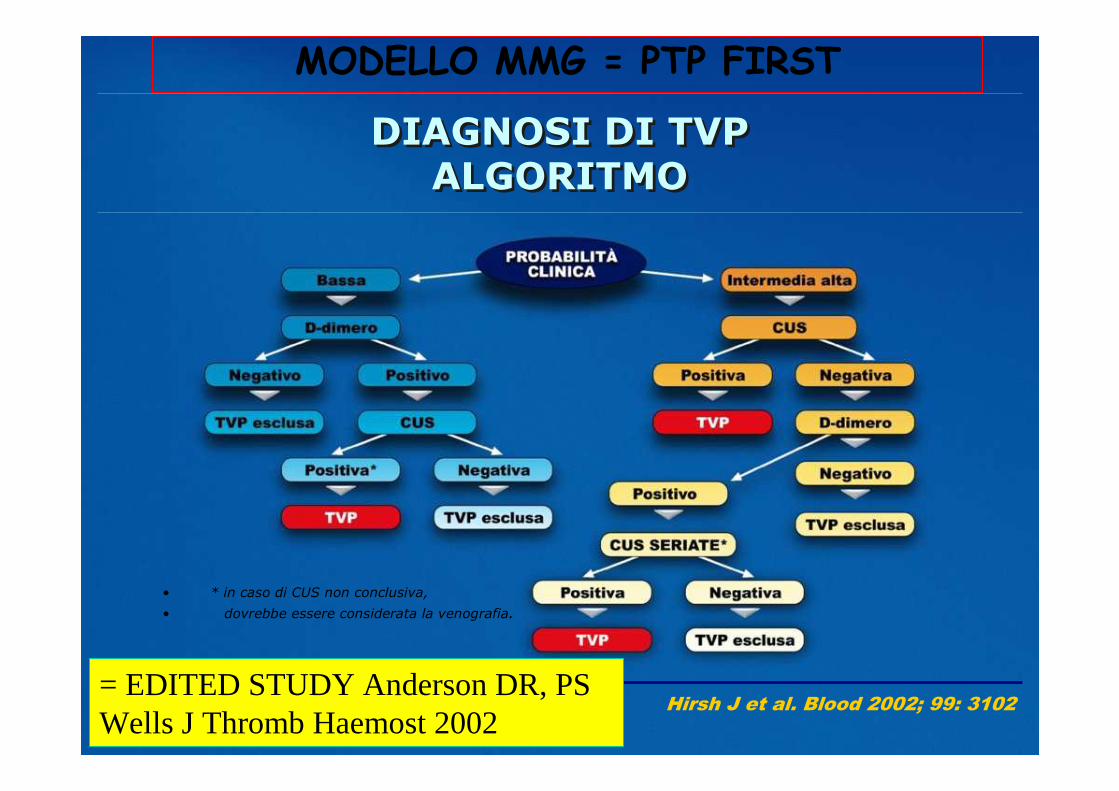
• * in caso di CUS non conclusiva,
• dovrebbe essere considerata la venografia.
Hirsh J et al. Blood 2002; 99: 3102
DIAGNOSI DI TVP
ALGORITMO
DIAGNOSI DI TVP
ALGORITMO
MODELLO MMG = PTP FIRST
= EDITED STUDY Anderson DR, PS Wells J Thromb Haemost 2002
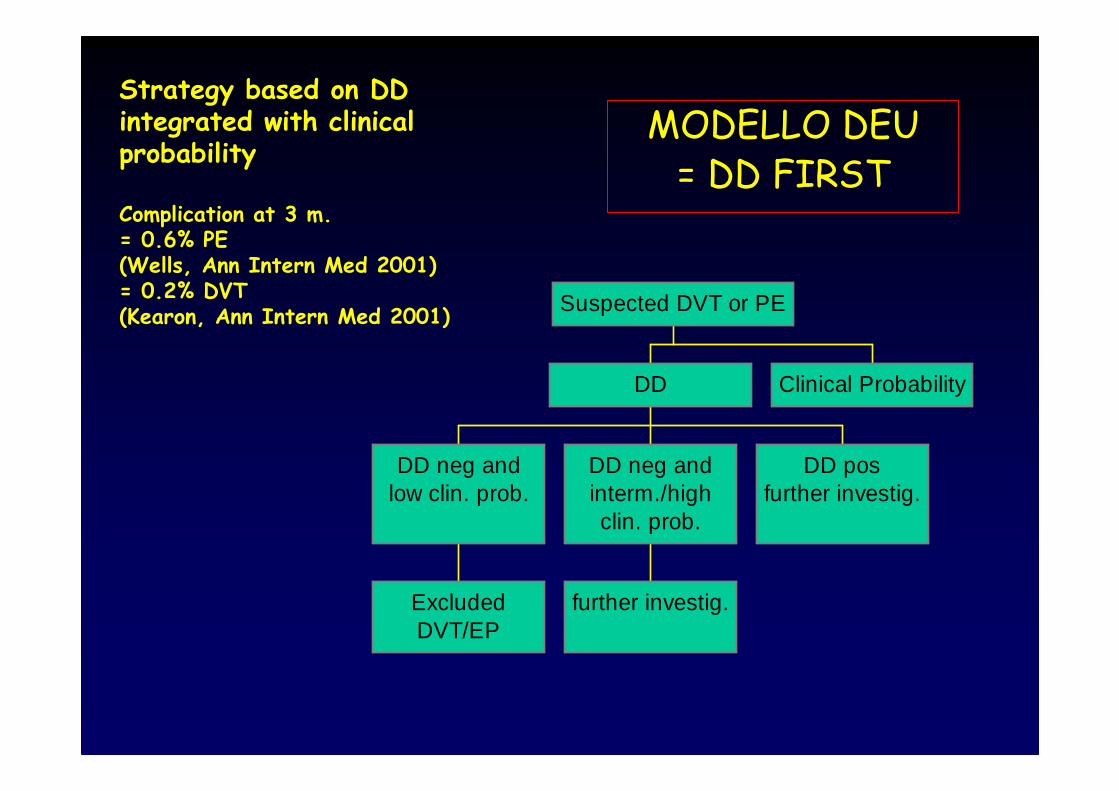
ExcludedDVT/EP
DD neg andlow clin. prob.
further investig.
DD neg andinterm./highclin. prob.
DD posfurther investig.
DD Clinical Probability
Suspected DVT or PE
Strategy based on DD integrated with clinicalprobability
Complication at 3 m.= 0.6% PE(Wells, Ann Intern Med 2001)= 0.2% DVT(Kearon, Ann Intern Med 2001)
MODELLO DEU = DD FIRST
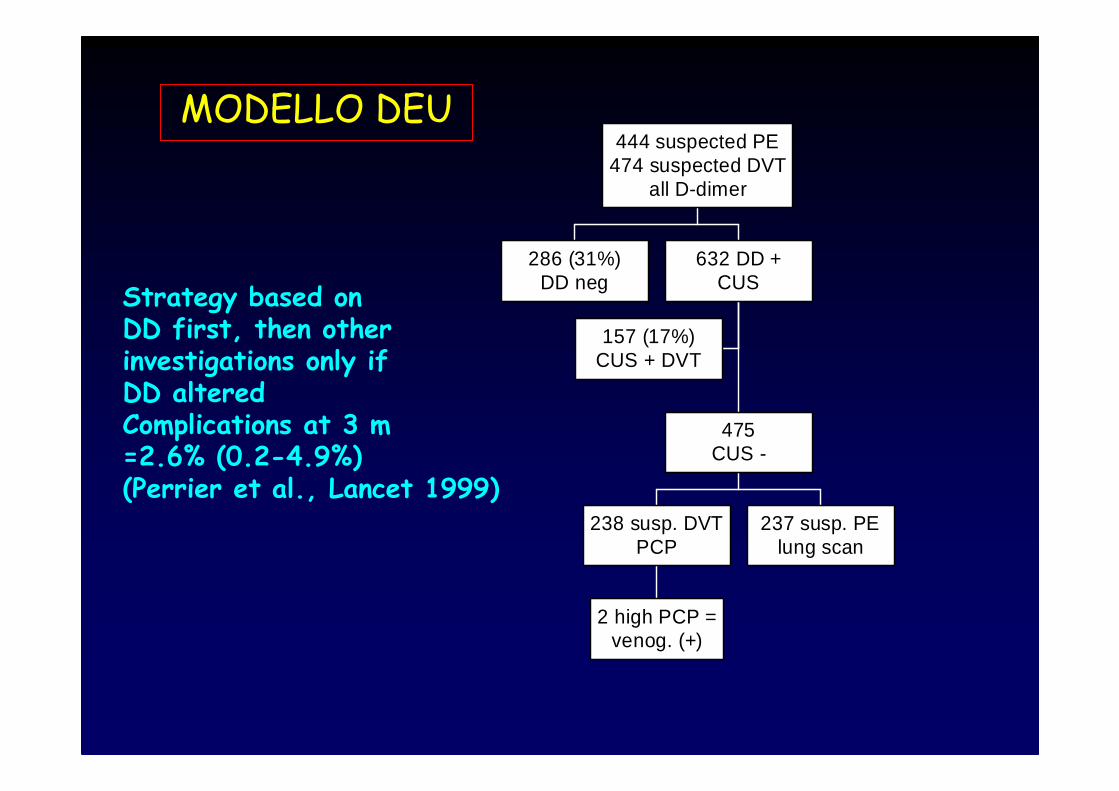
286 (31%)DD neg
157 (17%)CUS + DVT
2 high PCP =venog. (+)
238 susp. DVTPCP
237 susp. PElung scan
475CUS -
632 DD +CUS
444 suspected PE474 suspected DVT
all D-dimer
Strategy based onDD first, then otherinvestigations only if DD alteredComplications at 3 m =2.6% (0.2-4.9%)(Perrier et al., Lancet 1999)
MODELLO DEU
Come utilizzare le tre metodiche “cardine” ?
PTP
CUS
DD
Angiologia= CUS FIRST
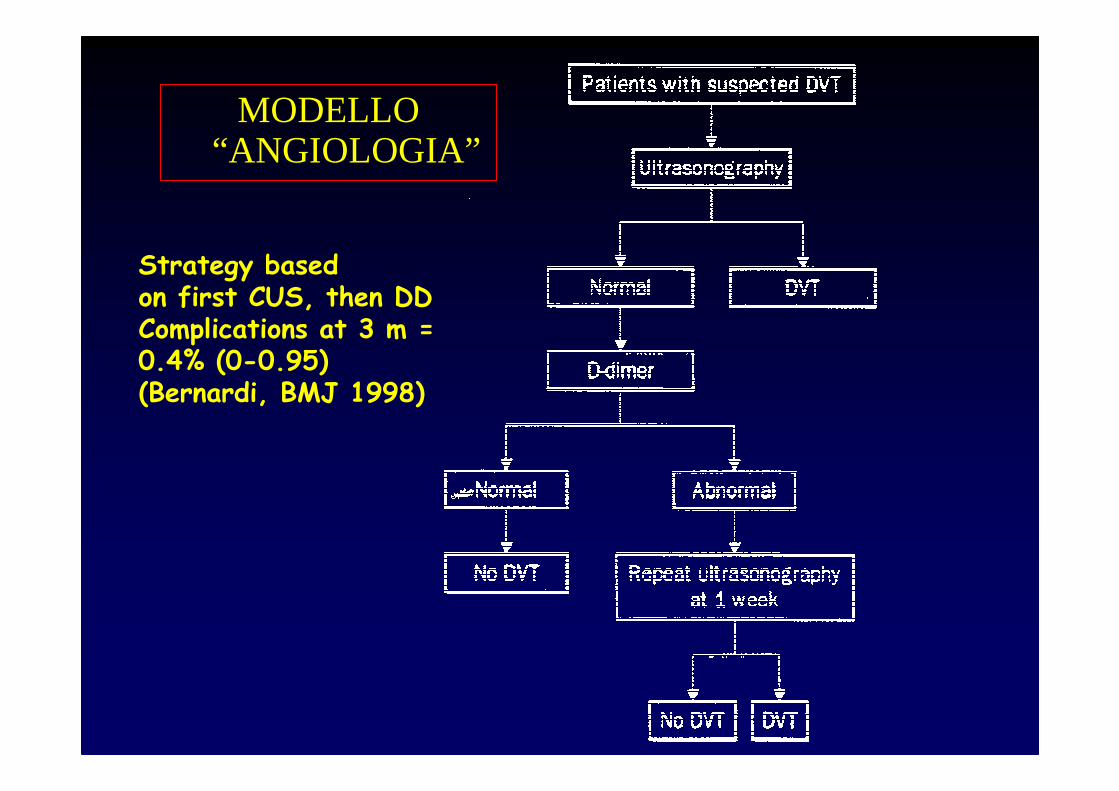
Strategy basedon first CUS, then DDComplications at 3 m =0.4% (0-0.95)(Bernardi, BMJ 1998)
MODELLO “ANGIOLOGIA”
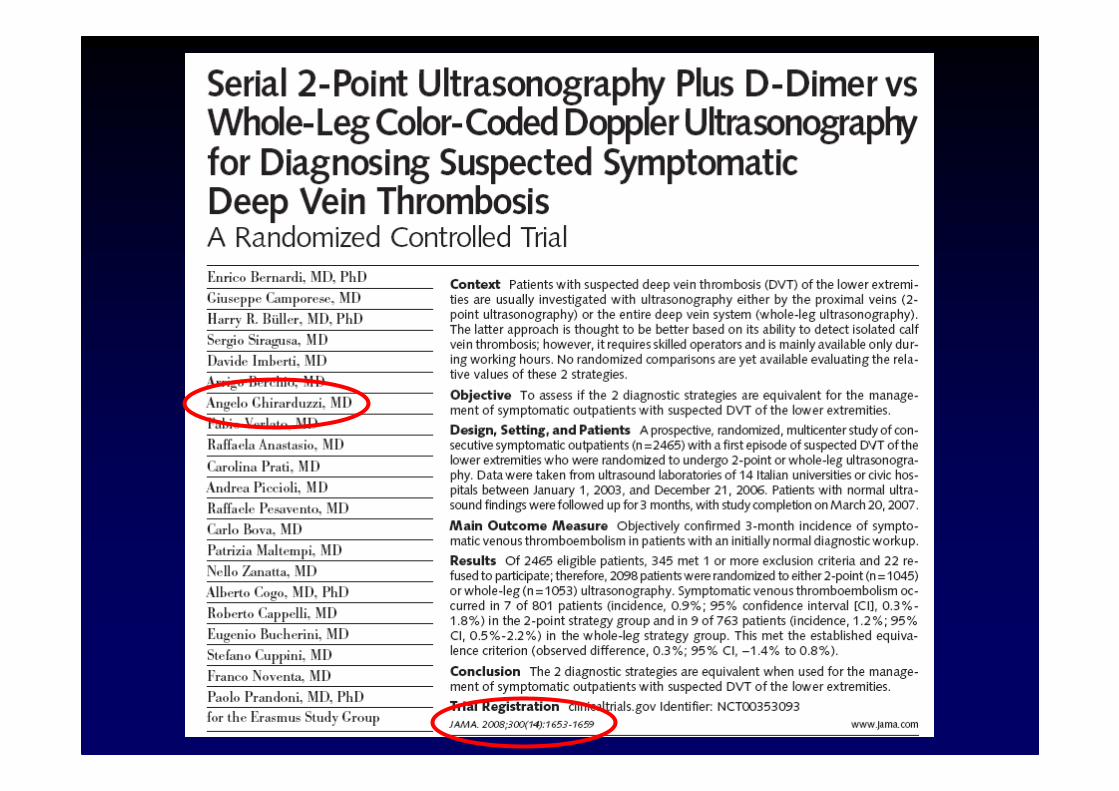
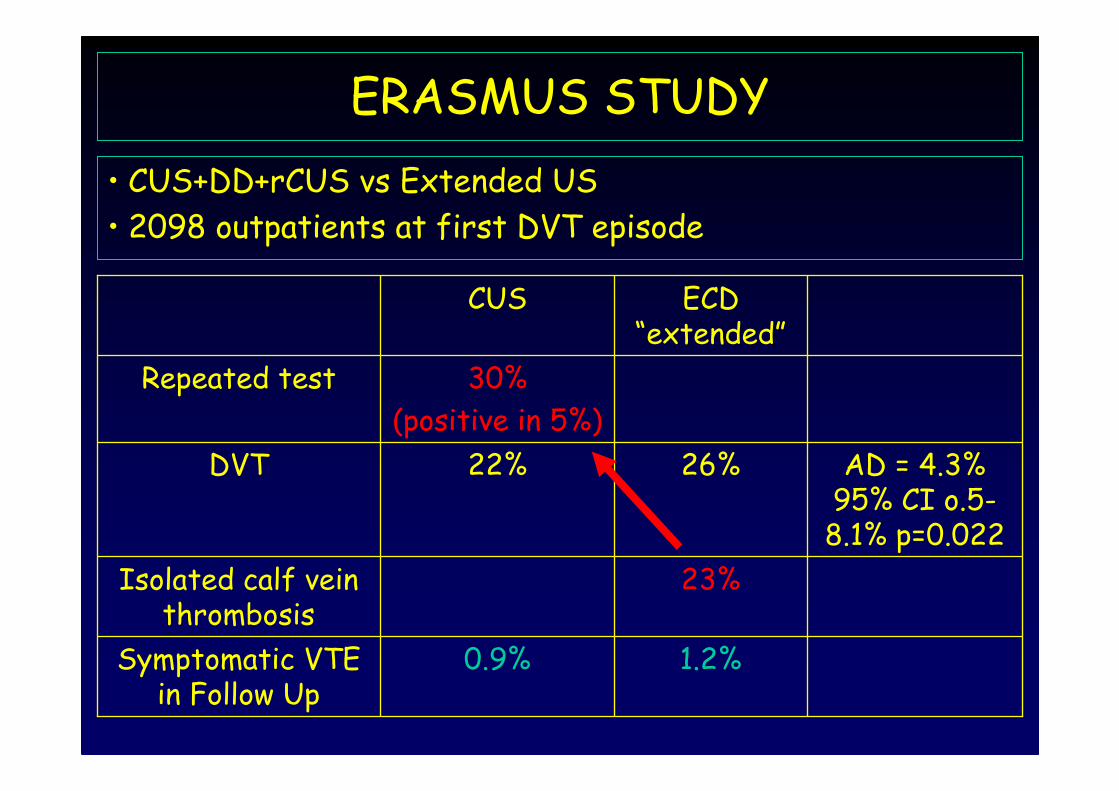
ERASMUS STUDY
• CUS+DD+rCUS vs Extended US
• 2098 outpatients at first DVT episode
1.2%0.9%Symptomatic VTE in Follow Up
23%Isolated calf veinthrombosis
AD = 4.3% 95% CI o.5-8.1% p=0.022
26%22%DVT
30%
(positive in 5%)
Repeated test
ECD “extended”
CUS
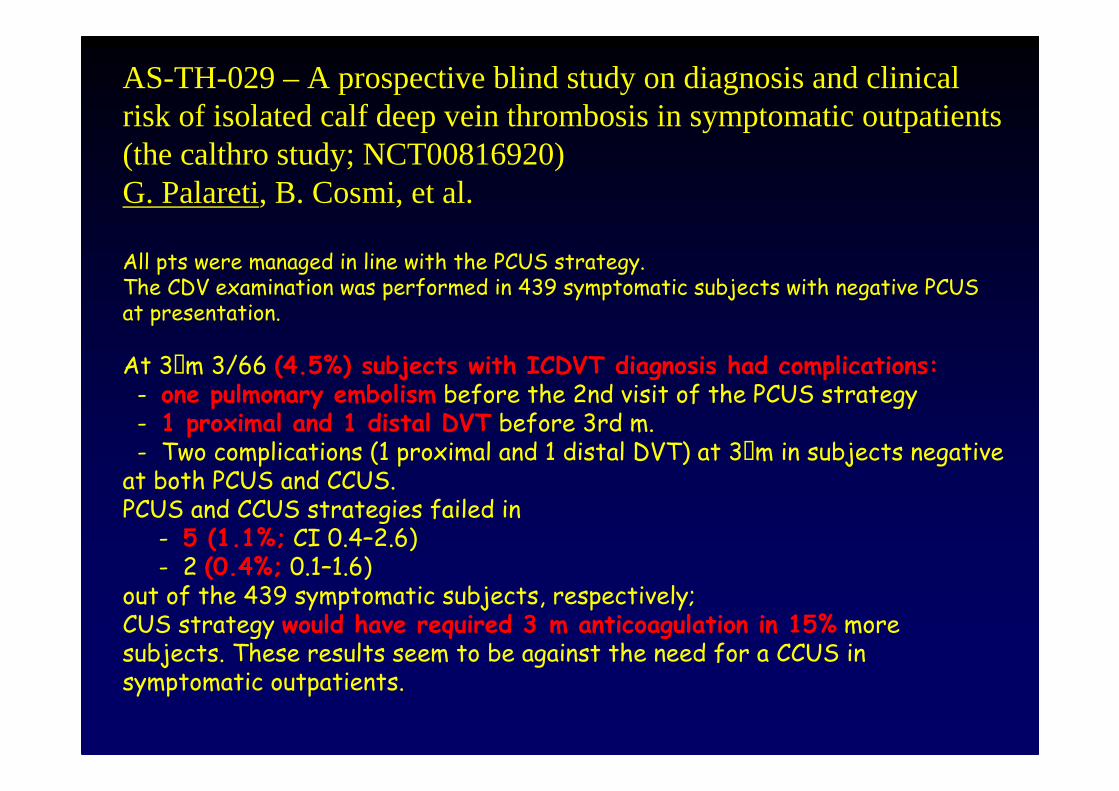
AS-TH-029 – A prospective blind study on diagnosis and clinical risk of isolated calf deep vein thrombosis in symptomatic outpatients (the calthro study; NCT00816920)G. Palareti, B. Cosmi, et al.
All pts were managed in line with the PCUS strategy. The CDV examination was performed in 439 symptomatic subjects with negative PCUS at presentation.
At 3Sm 3/66 (4.5%) subjects with ICDVT diagnosis had complications:- one pulmonary embolism before the 2nd visit of the PCUS strategy- 1 proximal and 1 distal DVT before 3rd m.- Two complications (1 proximal and 1 distal DVT) at 3Sm in subjects negative at both PCUS and CCUS. PCUS and CCUS strategies failed in
- 5 (1.1%; CI 0.4–2.6)- 2 (0.4%; 0.1–1.6)
out of the 439 symptomatic subjects, respectively; CUS strategy would have required 3Dm anticoagulation in 15% more subjects. These results seem to be against the need for a CCUS in symptomatic outpatients.
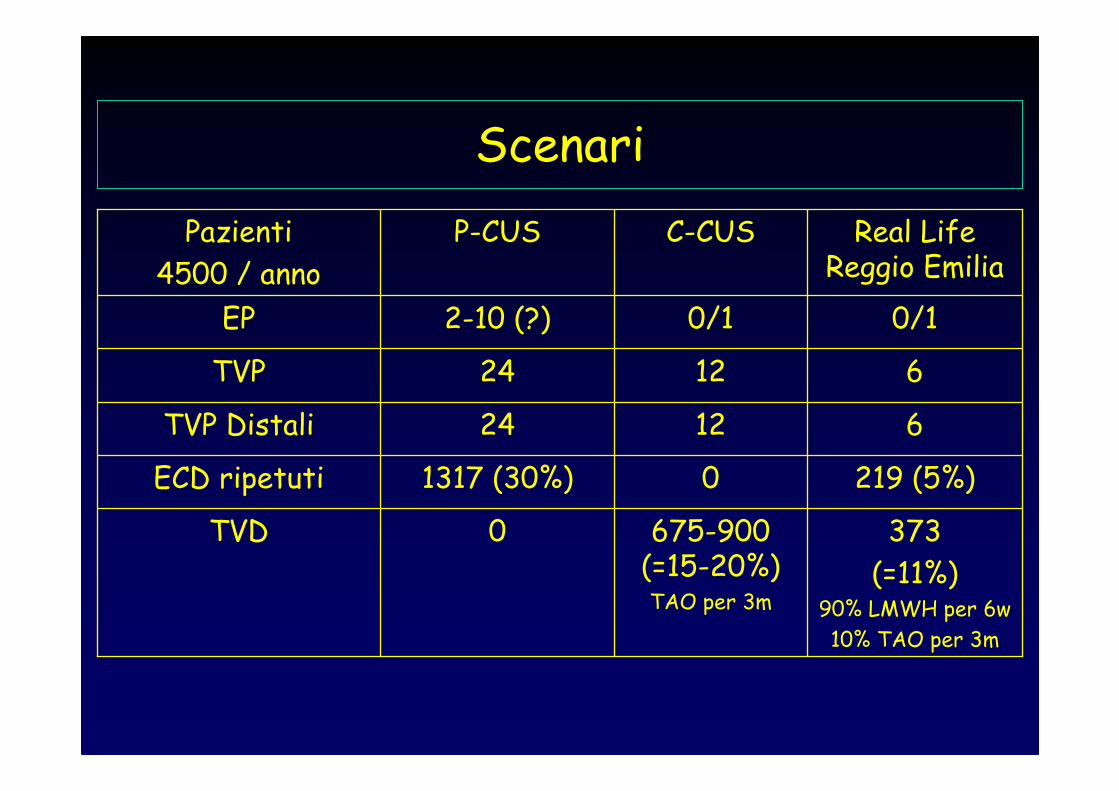
Scenari
219 (5%)01317 (30%)ECD ripetuti
373
(=11%)90% LMWH per 6w
10% TAO per 3m
675-900 (=15-20%)TAO per 3m
0TVD
61224TVP Distali
61224TVP
0/10/12-10 (?)EP
Real Life Reggio Emilia
C-CUSP-CUSPazienti
4500 / anno
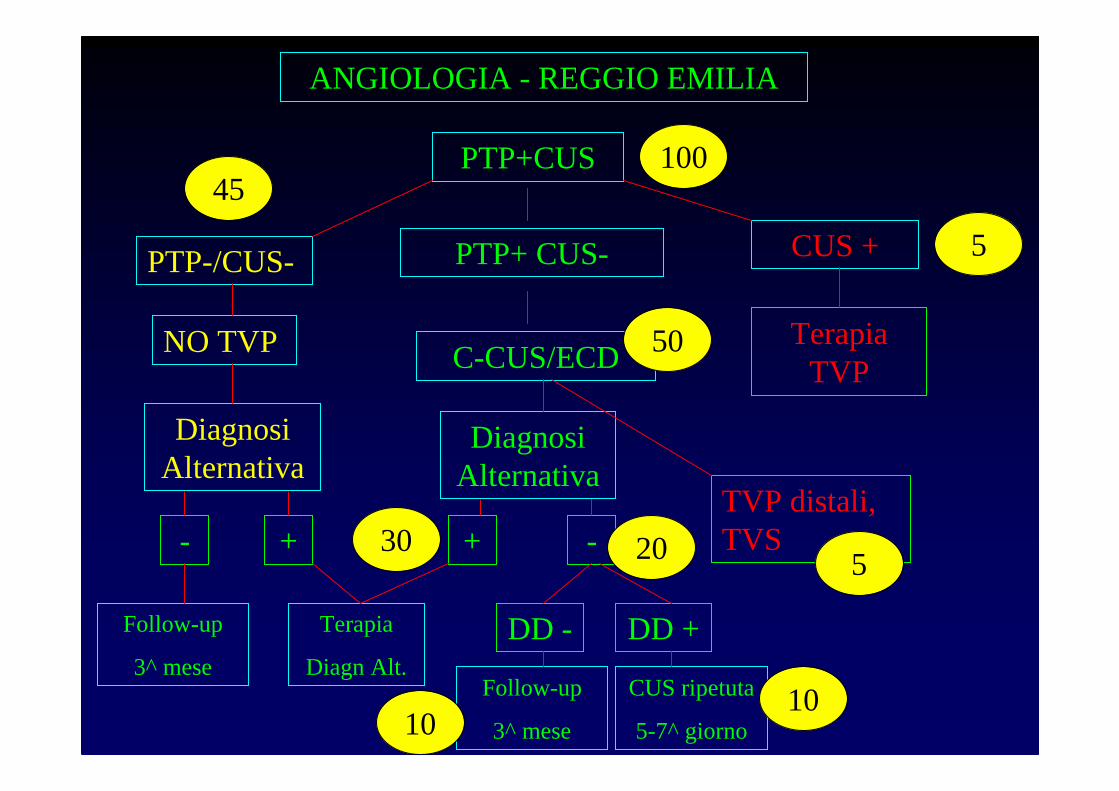
PTP+ CUS-
C-CUS/ECD
PTP-/CUS-
PTP+CUS
NO TVP
ANGIOLOGIA - REGGIO EMILIA
TVP distali, TVS
CUS +
Terapia TVP
-
Follow-up
3^ mese
Terapia
Diagn Alt.
Diagnosi Alternativa
Diagnosi Alternativa
-
DD - DD +
+ +
Follow-up
3^ mese
CUS ripetuta
5-7^ giorno
100
5
45
50
530 20
1010
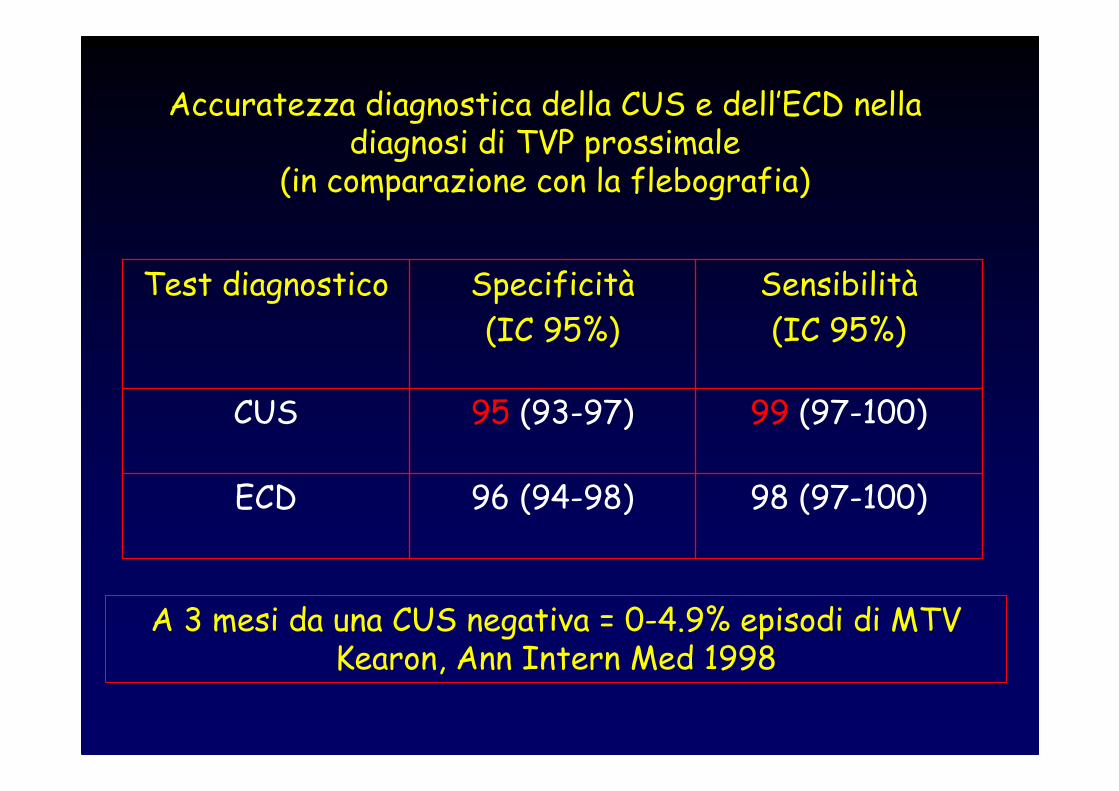
Accuratezza diagnostica della CUS e dell’ECD nelladiagnosi di TVP prossimale
(in comparazione con la flebografia)
98 (97-100)96 (94-98)ECD
99 (97-100)95 (93-97)CUS
Sensibilità
(IC 95%)
Specificità
(IC 95%)
Test diagnostico
A 3 mesi da una CUS negativa = 0-4.9% episodi di MTVKearon, Ann Intern Med 1998
COSA DANNO IN PIU’ LE METODICHE ECOCOLOR – DOPPLER NELLO STUDIO
PROSSIMALE ?
• Rapido repere arterie/vene• Studio vene iliache• Rapido riconoscimento anomalie vascolari• Esclusione fistole a-v• Valutazione flussi arteriosi ed esclusione concomitante PAD
Vantaggio “marginale” ma con perdita modesta di tempo.
Burn, ClinRadiol 1997

LA TERAPIA
TVP DISTALIFATTORI CONTRO DIAGNOSI-TERAPIA
•30% lisi spontanea•50% ricanalizzazione incompleta in polpaccio•Rischio di anticoagulare pazienti con basso rischio trombotico•Effetti nella gestione complessiva del paziente con MTV = ex. come considerare le TVP distali se secondo episodio dopo una TVP prox. ?, Studio Trombofilie ? ….
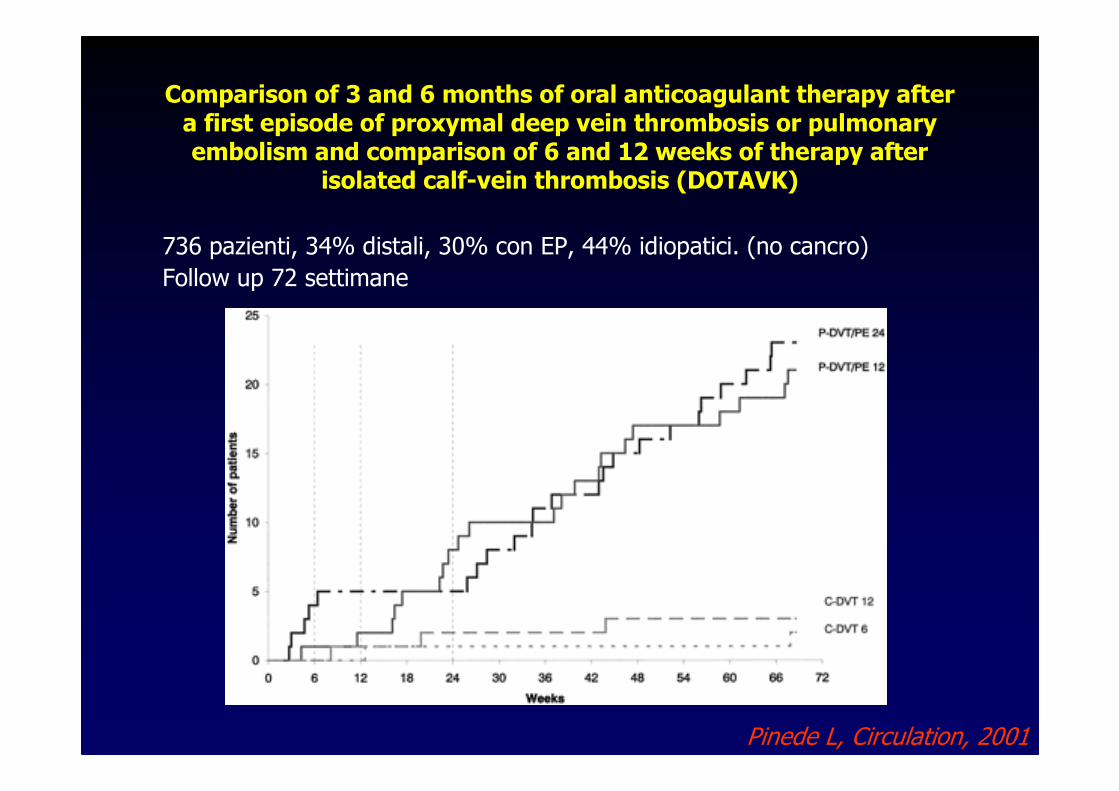
Comparison of 3 and 6 months of oral anticoagulant therapy after a first episode of proxymal deep vein thrombosis or pulmonaryembolism and comparison of 6 and 12 weeks of therapy after
isolated calf-vein thrombosis (DOTAVK)
736 pazienti, 34% distali, 30% con EP, 44% idiopatici. (no cancro)
Follow up 72 settimane
Pinede L, Circulation, 2001
Therapy of Isolated Calf Muscle Vein Thrombosis with Low-Molecular-Weight heparin:
Prospective, Randomized Study.Schwarz T, Schellong S – Dresden, Germany
• 107 pts• Nadroparin 10 days therapeutic doses vs compression therapy
alone• PE=0, Major Bleeding=0, Thrombus Progression=3.7% (hep),
3.7% (no hep)CONCLUSIONS: • severe complications rareeven if anticoagulants is not
applicated
No adverse outcome on a 3-month follow-up of patientswithDUS diagnosed CVT who did not receive anticoagulation alsoin Gottlieb Study (Radiology 1999)
AS-TH-029 – AIsolated distal deep vein thrombosis: efficacy and safety of a protocol of treatment. Treatment of Isolated Calf Thrombosis (TICT) Study.Parisi R, Visonà A, Camporese G, Verlato F, Lessiani G, Antignani PL , Palareti G.
TREATMENTtwice-daily subcutaneous administrationof a full dose of weight-adjusted LMWH for one week + a half dose of LMWH administered once-daily for another threeweeks.
171 outpatients. Sixty-one patients (36.6%) presentedan unprovoked ID-DVT. Complications during treatment period = 10/171 patients (5.8%)Extension proximal to the knee = 5/171 (2.9%) all with anunprovoked ID-DVTMinor Bleeding = 3/171 (1.7%). No major bleeding.
Complications during F-UP period = 5/171four patients showed a proximal DVT (3 with a previous unprovoked ID-DVT, 1 with a previous ID-DVT secondary to a traumatic leg fracture, with persistent difficulty of deambulation); one, with a previous secondary thrombosis, showed a ID-DVT.
CONCLUSIONS: In our study only 2.9% of patients with ID-DVT showed a progression of thrombosis to proximal deep veins; the majority of thrombus progression, during the treatment period, was observed in patients with unprovoked ID-DVT. Our results supportthe usefulness of a prolongedtreatment in unprovoked ID-DVT.
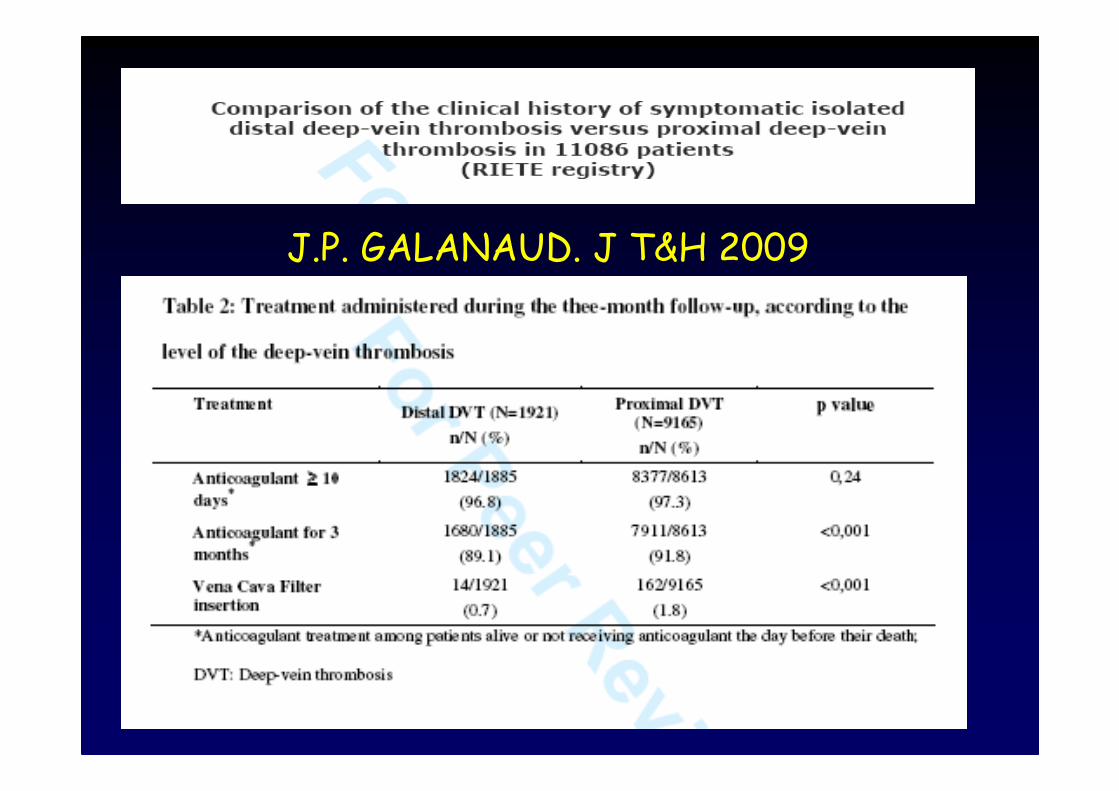
J.P. GALANAUD. J T&H 2009
Results: 11086 patients with symptomatic DVT, but without pulmonary embolism, were included between 2001 and 2008. 1921 (17.3%) exhibited isolated distal DVT. 89.1% (1680/1885) of isolated distal DVT and 91.8% (7911/8613) of proximal DVT patients were under anticoagulant treatment during the whole follow-up.
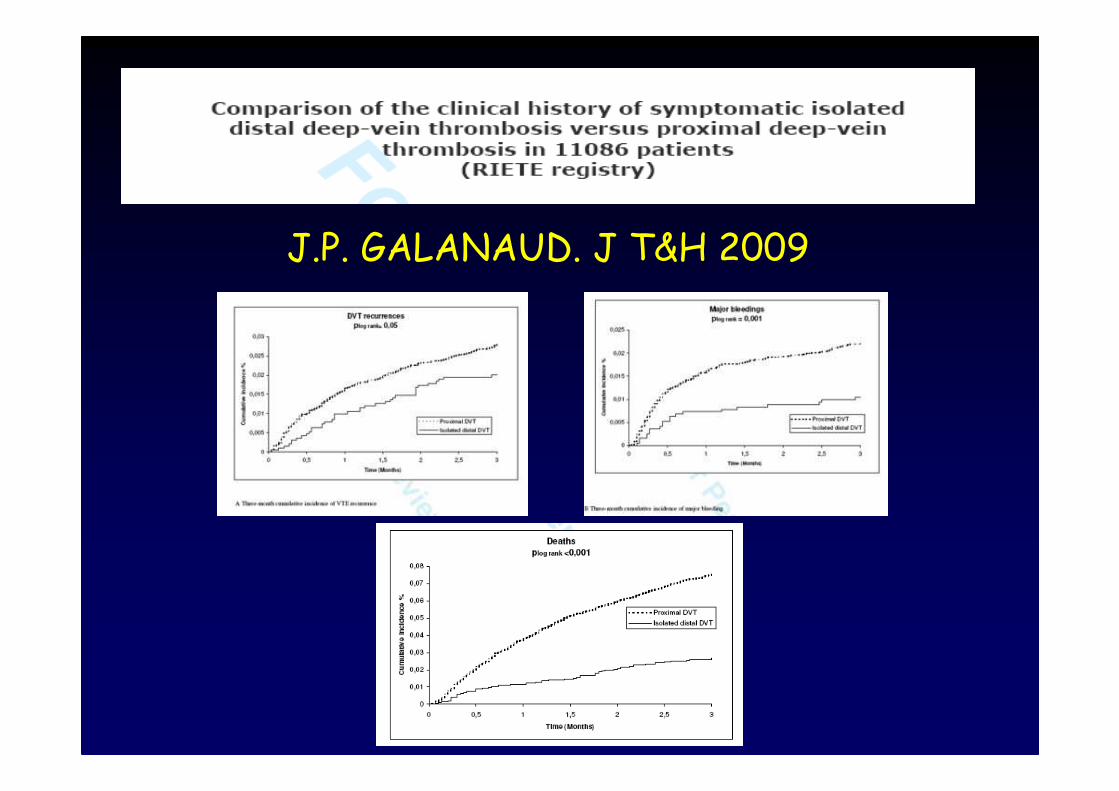
Isolated distal DVT 1) more associated with transient risk factors (recent travel, hospitalisation,
recent surgery)2) at three months, major bleeding rate was lower in patients with isolated
distal DVT (1.0% vs 2.2%, p<0.01),3) VTE recurrence rate was equivalent (2.0%vs 2.7%, p=0.07).4) The mortality rate was lower in patients with isolated distal DVT (2.7% versus
7.5%; p<0.001); this was mainly due to a lower rate of non-VTE-related deaths (2.2%versus 6.3%; p<0.001).
5) Active cancer was the main predictive factor of death in patients with isolated distal DVT.
J.P. GALANAUD. J T&H 2009
J.P. GALANAUD. J T&H 2009
J.P. GALANAUD. J T&H 2009
Conclusions: Proximal and isolated distal DVT patients differ in terms of risk factors and clinical outcomes suggesting different populations. In the short term the life expectancy of patients with isolated distal DVT depended chiefly on their cancer status.
In Sintesi…..
• LMWH 1 settimana a dosaggio pieno + 3 settimane a dosaggio dimezzato = efficacica scarsa ma rischio emorragicoaccettabile = 1% di minor bleedings)
• TAO per tre mesi = efficacia elevata ma rischio emorragico sproporzionato a basso rischio
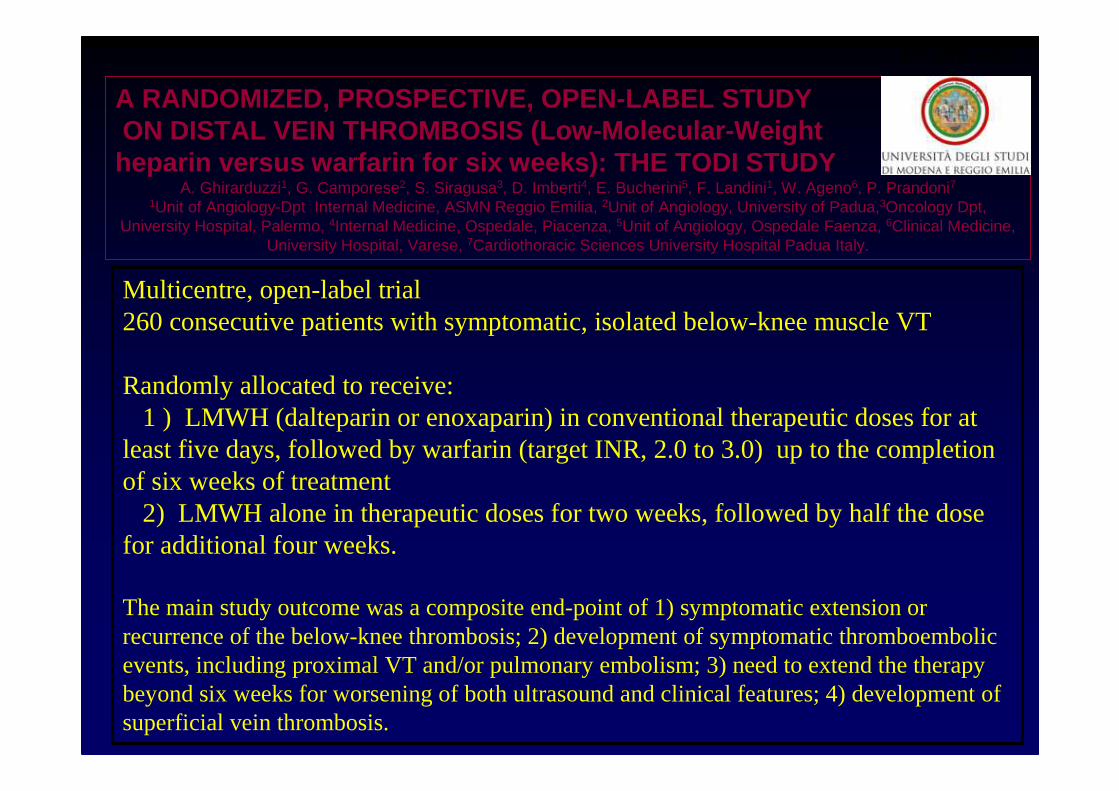
A RANDOMIZED, PROSPECTIVE, OPEN-LABEL STUDYON DISTAL VEIN THROMBOSIS (Low-Molecular-Weightheparin versus warfarin for six weeks): THE TODI STUDY
A. Ghirarduzzi1, G. Camporese2, S. Siragusa3, D. Imberti4, E. Bucherini5, F. Landini1, W. Ageno6, P. Prandoni71Unit of Angiology-Dpt Internal Medicine, ASMN Reggio Emilia, 2Unit of Angiology, University of Padua,3Oncology Dpt,
University Hospital, Palermo, 4Internal Medicine, Ospedale, Piacenza, 5Unit of Angiology, Ospedale Faenza, 6Clinical Medicine, University Hospital, Varese, 7Cardiothoracic Sciences University Hospital Padua Italy.
Multicentre, open-label trial260 consecutive patients with symptomatic, isolated below-knee muscle VT
Randomly allocated to receive:1 ) LMWH (dalteparin or enoxaparin) in conventional therapeutic doses for at
least five days, followed by warfarin (target INR, 2.0 to 3.0) up to the completion of six weeks of treatment
2) LMWH alone in therapeutic doses for two weeks, followed by half the dosefor additional four weeks.
The main study outcome was a composite end-point of 1) symptomatic extension or recurrence of the below-knee thrombosis; 2) development of symptomatic thromboembolicevents, including proximal VT and/or pulmonary embolism; 3) need to extend the therapy beyond six weeks for worsening of both ultrasound and clinical features; 4) development of superficial vein thrombosis.
PP-WE-403
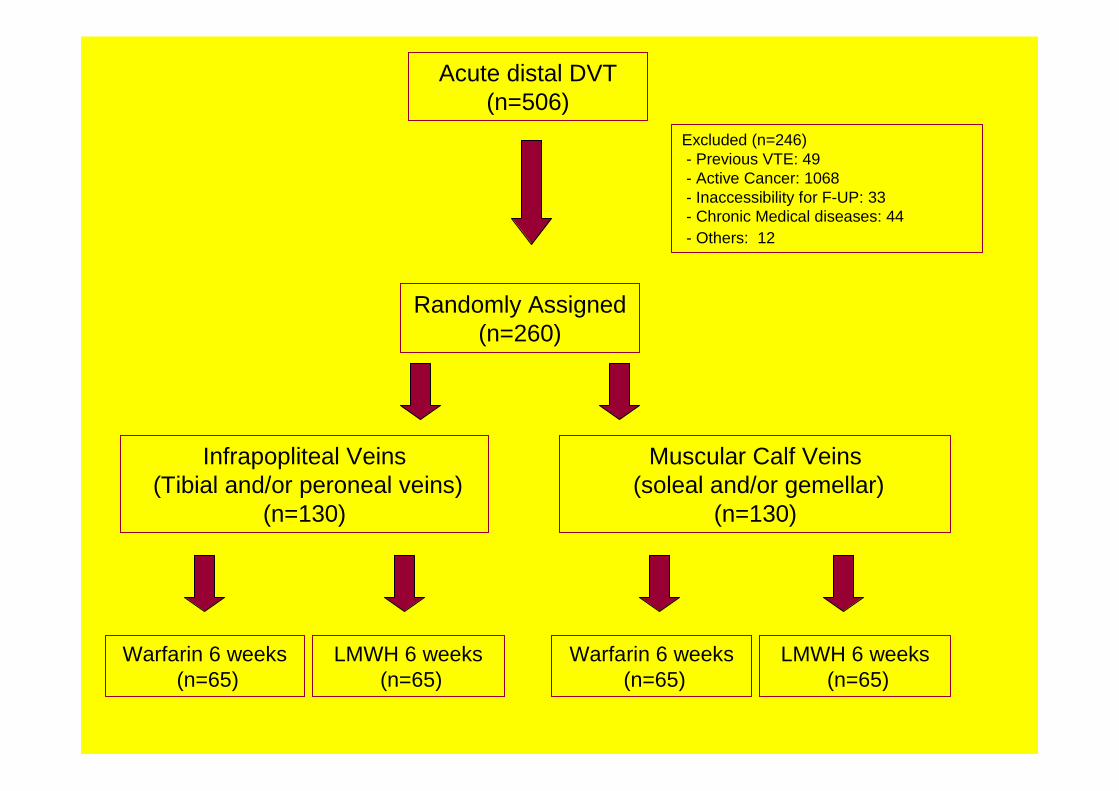
Acute distal DVT (n=506)
Excluded (n=246)- Previous VTE: 49 - Active Cancer: 1068- Inaccessibility for F-UP: 33- Chronic Medical diseases: 44- Others: 12
Randomly Assigned (n=260)
Infrapopliteal Veins(Tibial and/or peroneal veins)
(n=130)
Warfarin 6 weeks(n=65)
LMWH 6 weeks(n=65)
Muscular Calf Veins(soleal and/or gemellar)
(n=130)
Warfarin 6 weeks(n=65)
LMWH 6 weeks(n=65)
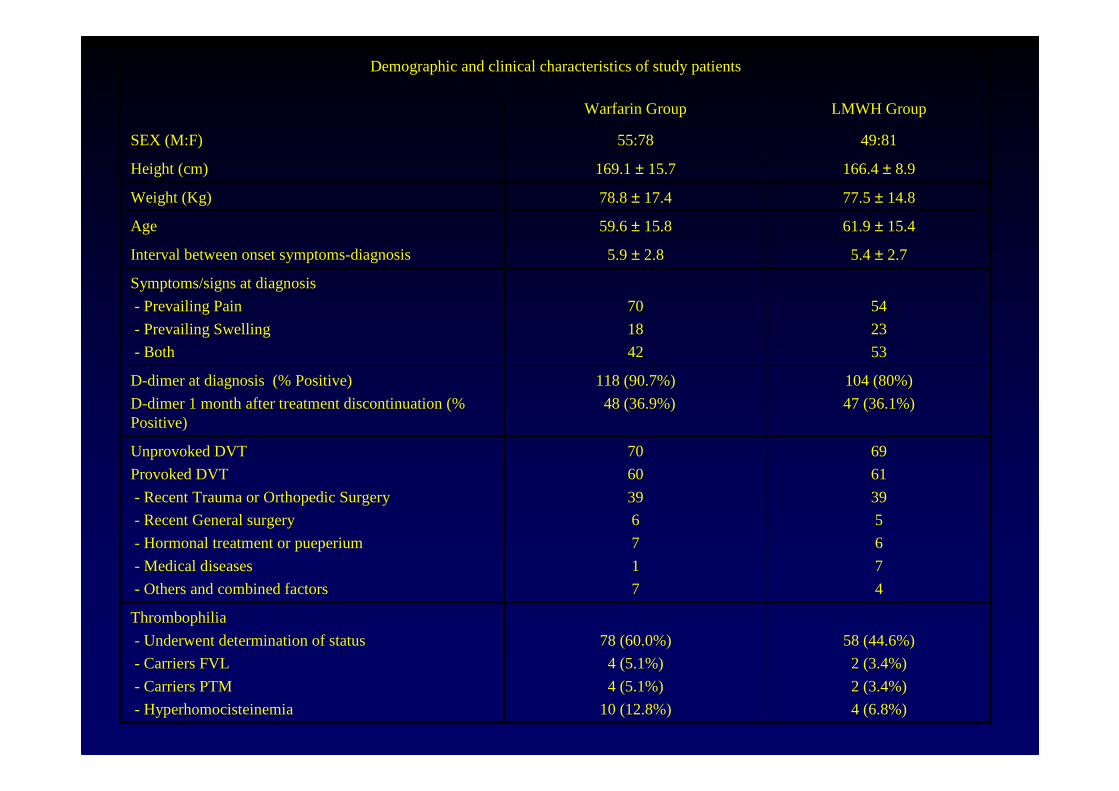
104 (80%)
47 (36.1%)
118 (90.7%)
48 (36.9%)
D-dimer at diagnosis (% Positive)
D-dimer 1 month after treatment discontinuation (% Positive)
69
61
39
5
6
7
4
70
60
39
6
7
1
7
Unprovoked DVT
Provoked DVT
- Recent Trauma or Orthopedic Surgery
- Recent General surgery
- Hormonal treatment or pueperium
- Medical diseases
- Others and combined factors
54
23
53
70
18
42
Symptoms/signs at diagnosis
- Prevailing Pain
- Prevailing Swelling
- Both
49:8155:78SEX (M:F)
Demographic and clinical characteristics of study patients
166.4 ± 8.9169.1 ± 15.7 Height (cm)
77.5 ± 14.878.8 ± 17.4Weight (Kg)
58 (44.6%)
2 (3.4%)
2 (3.4%)
4 (6.8%)
78 (60.0%)
4 (5.1%)
4 (5.1%)
10 (12.8%)
Thrombophilia
- Underwent determination of status
- Carriers FVL
- Carriers PTM
- Hyperhomocisteinemia
5.4 ± 2.75.9 ± 2.8Interval between onset symptoms-diagnosis
61.9 ± 15.459.6 ± 15.8Age
LMWH GroupWarfarin Group
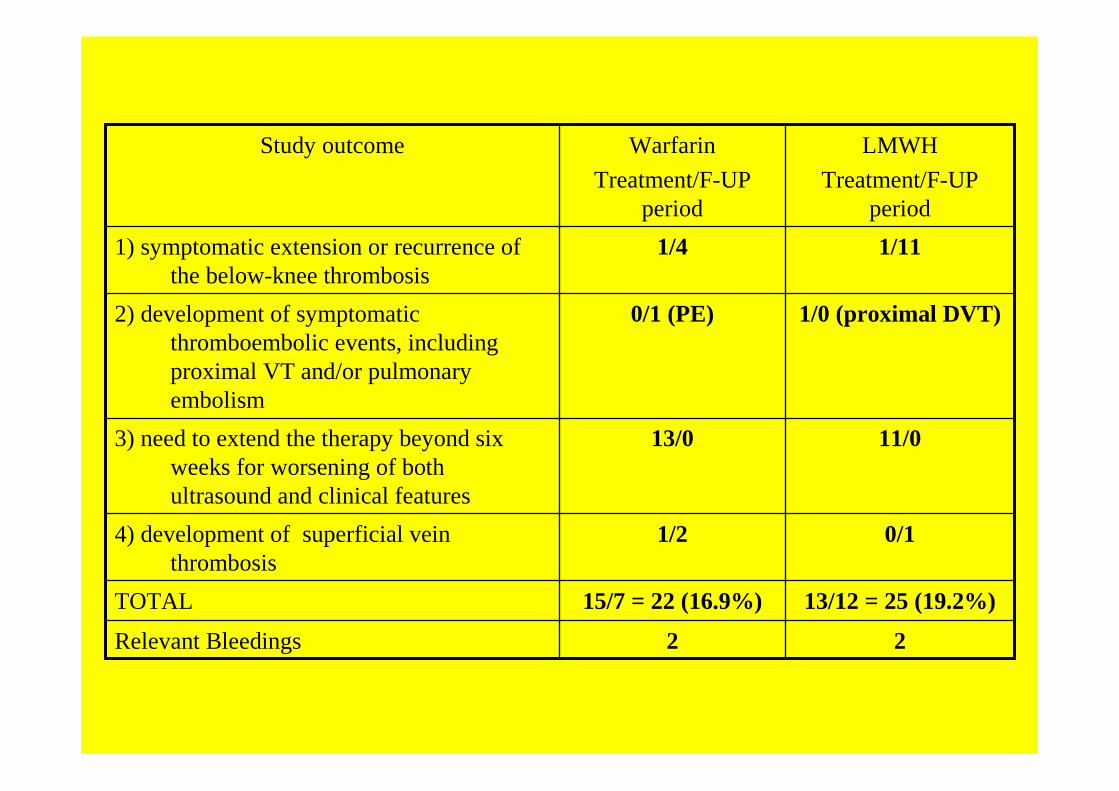
22Relevant Bleedings
13/12 = 25 (19.2%)15/7 = 22 (16.9%)TOTAL
0/11/24) development of superficial vein thrombosis
11/013/03) need to extend the therapy beyond six weeks for worsening of both ultrasound and clinical features
1/0 (proximal DVT)0/1 (PE)2) development of symptomatic thromboembolic events, including proximal VT and/or pulmonary embolism
1/111/41) symptomatic extension or recurrence of the below-knee thrombosis
LMWH
Treatment/F-UP period
Warfarin
Treatment/F-UP period
Study outcome
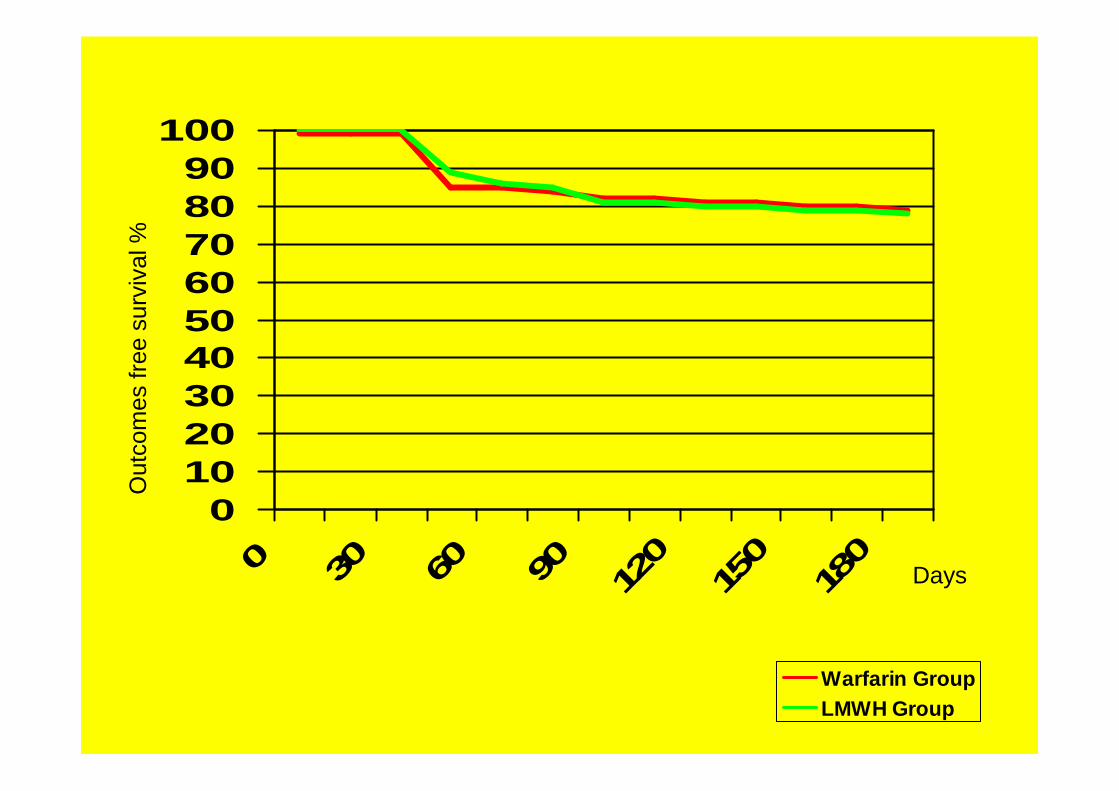
0102030405060708090
100
0 30 60 90 120
150
180
Out
com
es fr
ee s
urvi
val %
Days
Warfarin GroupLMWH Group
Pazienti Asintomatici per TVP
2-CUS/E-CUS/C-CUS/EECD/EECD
Test eseguito come sostitutivo di flebografia in pazienti ad alto rischio
Ex:
• Pazienti ad alto rischio di MTV che non possono effettuare profilassi antitrombotica (paz. con emorragia cerebrale)…
• Studi di profilassi in medicina interna o chirurgia (in PREVENT, EXCLAIM =E-CUS)
• Pazienti con EP ad arti asintomatici
• La prevalenza della trombosi venosa distale (del 5-12% nei pazienti sintomatici) diventa del 15-45% nei pazienti post-chirurgici
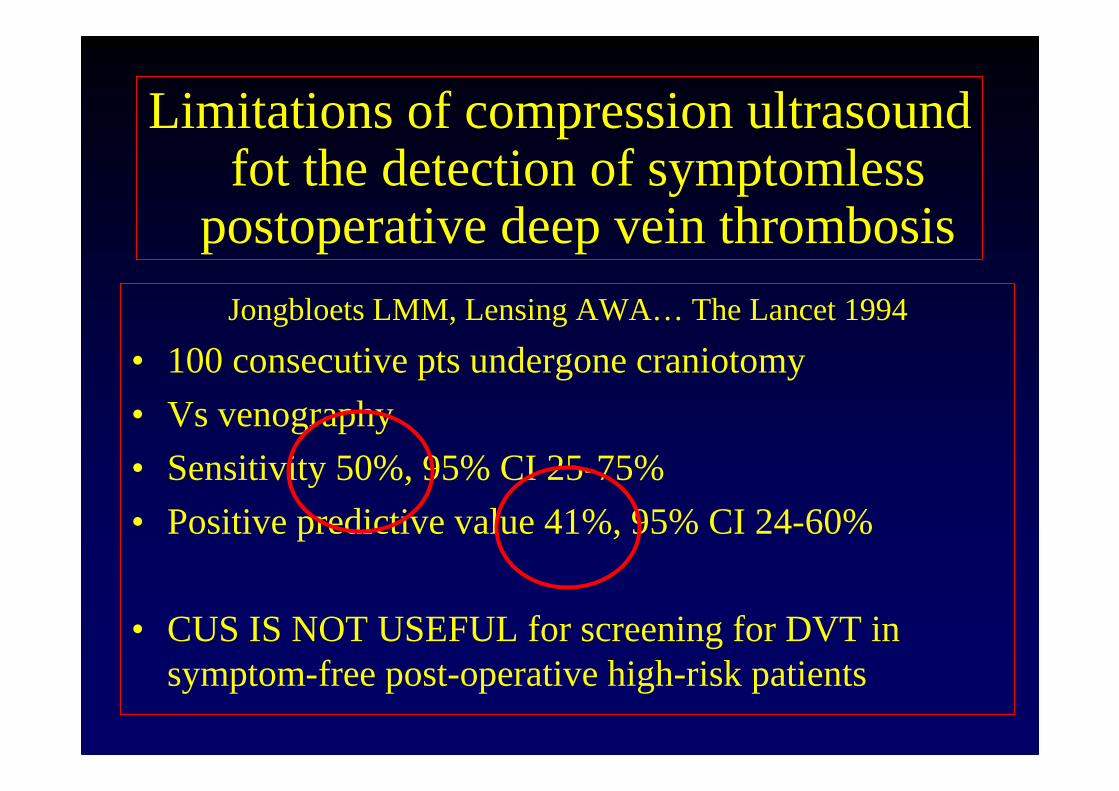
Limitations of compression ultrasound fot the detection of symptomless
postoperative deep vein thrombosis
Jongbloets LMM, Lensing AWA… The Lancet 1994
• 100 consecutive pts undergone craniotomy
• Vs venography
• Sensitivity 50%, 95% CI 25-75%
• Positive predictive value 41%, 95% CI 24-60%
• CUS IS NOT USEFUL for screening for DVT in symptom-free post-operative high-risk patients
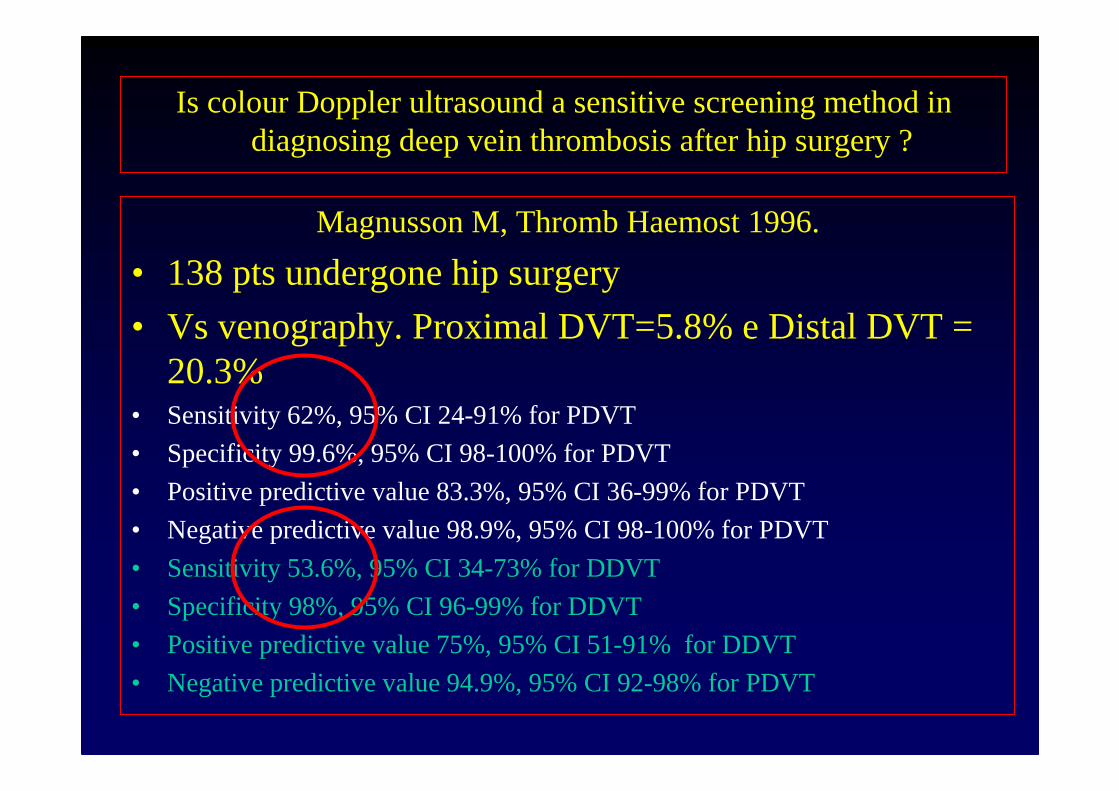
Is colour Doppler ultrasound a sensitive screening method in diagnosing deep vein thrombosis after hip surgery ?
Magnusson M, Thromb Haemost 1996.
• 138 pts undergone hip surgery
• Vs venography. Proximal DVT=5.8% e Distal DVT = 20.3%
• Sensitivity 62%, 95% CI 24-91% for PDVT
• Specificity 99.6%, 95% CI 98-100% for PDVT
• Positive predictive value 83.3%, 95% CI 36-99% for PDVT
• Negative predictive value 98.9%, 95% CI 98-100% for PDVT
• Sensitivity 53.6%, 95% CI 34-73% for DDVT
• Specificity 98%, 95% CI 96-99% for DDVT
• Positive predictive value 75%, 95% CI 51-91% for DDVT
• Negative predictive value 94.9%, 95% CI 92-98% for PDVT
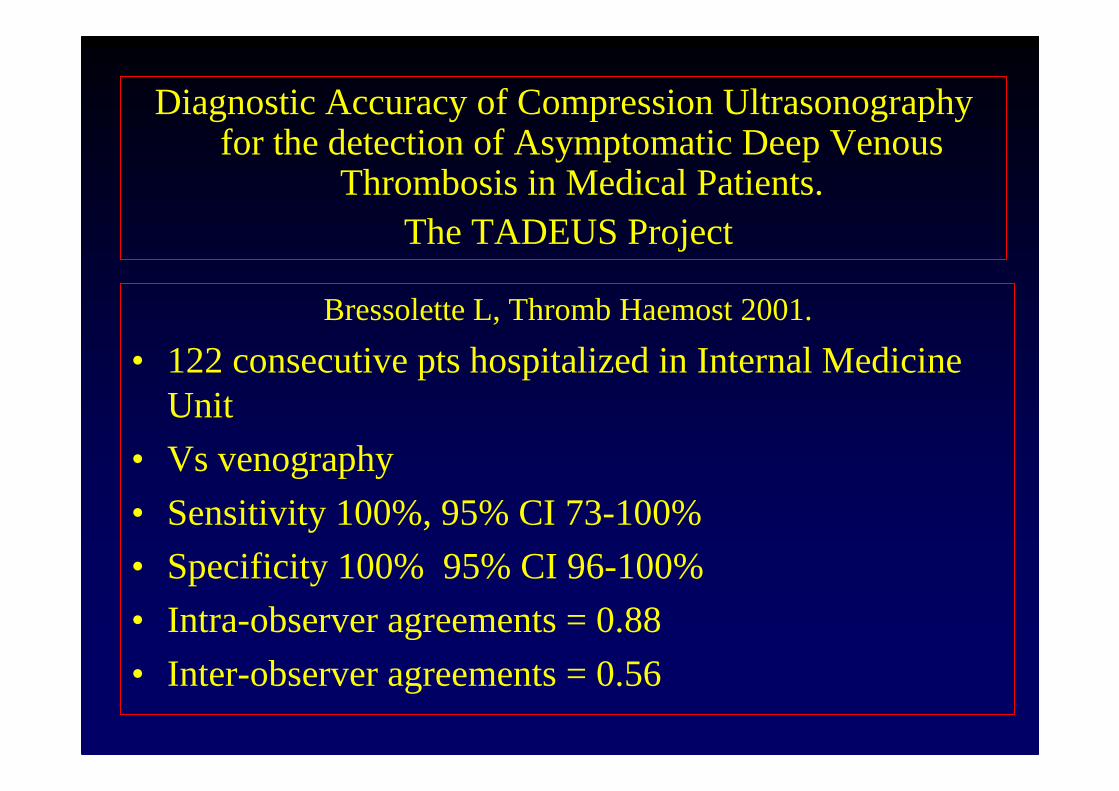
Diagnostic Accuracy of Compression Ultrasonographyfor the detection of Asymptomatic Deep Venous
Thrombosis in Medical Patients.The TADEUS Project
Bressolette L, Thromb Haemost 2001.
• 122 consecutive pts hospitalized in Internal Medicine Unit
• Vs venography
• Sensitivity 100%, 95% CI 73-100%
• Specificity 100% 95% CI 96-100%
• Intra-observer agreements = 0.88
• Inter-observer agreements = 0.56

Morena
Novella
Fiorella
SaraTiziana
Federica
Margherita
MatteoAntonia Laura
MariaLuisaCarmelo
Antonella
Manuela
Grazie per l’attenzione – [email protected]





























