Embed Size (px)
Citation preview
‘‘Make or buy’’ decisions in the productionof health care goods and services: newinsights from institutional economics andorganizational theoryAlexander S. Preker,1 April Harding,2 & Phyllida Travis3
A central theme of recent health care reforms has been a redefinition of the roles of the state and private providers.With a view to helping governments to arrive at more rational ‘‘make or buy’’ decisions on health care goods andservices, we propose a conceptual framework in which a combination of institutional economics and organizationaltheory is used to examine the core production activities in the health sector. Empirical evidence from actual productionmodalities is also taken into consideration. We conclude that most inputs for the health sector, with the exception ofhuman resources and knowledge, can be efficiently produced by and bought from the private sector. In the healthservices of low-income countries most dispersed production forms, e.g. ambulatory care, are already provided by theprivate sector (non-profit and for-profit). These valuable resources are often ignored by the public sector. The problemsof measurability and contestability associated with expensive, complex and concentrated production forms such ashospital care require a stronger regulatory environment and skilled contracting mechanisms before governments canrely on obtaining these services from the private sector. Subsidiary activities within the production process can often beunbundled and outsourced.
Keywords: delivery of health care, methods; public sector; private sector; outcome and process assessment, healthcare; decision-making, methods; models, economic; models, organizational.
Voir page 788 le resume en francais. En la pagina 788 figura un resumen en espanol.
Public and private roles in thehealth sector
Economic theory and empirical evidence provideample justification for significant engagement by thestate (1) in tackling problems of both equity (2–6) andefficiency (7–9) in the health sector. However,experience during the past two decades has revealeda range of problems in public production (10, 11)which have parallels with well-known marketimperfections in the private sector (12–15). Theseproblems relate, among other things, to publicaccountability (16), informational asymmetry (17),abuse of monopoly power and failure of strategicpolicy formulation, and there are clear parallels inmarket failure (18).
There is an urgent need to reform inefficientand bloated bureaucracies (19–22) by exposingpublic services to competitive market forces (23),reducing the size of the public sector (24, 25) and
increasing private sector participation (26–29). Abetter match is desirable between the roles of thestate and the private sector and their respectivecapabilities (30). In most countries this meansrebalancing what is already a complex mix of publicand private roles in the health sector (31).
Using a framework based on recent develop-ments in institutional economics and organizationaltheory, we argue for greater private participation in thegeneration of inputs and the provision of healthservices (32, 33). We also stress the importance of astrong stewardship function of governments in secur-ing equity, efficiency and quality objectives throughmore effective policy-making and financing (34).
Theoretical underpinnings fora contracting framework
The current tendency is to use at least one of threeapproaches in order to deal with public sector failurein the generation of inputs and the provision of healthservices. These approaches, indicated below indescending order of strength, involve:. exit possibilities (market forces through consumer
choice);. voice (client participation);. loyalty (hierarchical sense of responsibility) (35).
1 Lead Economist, World Bank, 1818 H. Street NW, Washington,DC 20433, USA (email: [email protected]). Requests for reprintsshould be addressed to this author.2 Institutional Economist, World Bank, 1818 H. Street NW,Washington, DC 20433, USA.3 Public Health Specialist, World Health Organization,1211 Geneva 27, Switzerland.
Ref. No. 00-0606
779Bulletin of the World Health Organization, 2000, 78 (6) # World Health Organization 2000

Exit should be used unless the weaker variants haveto be employed because the goods and servicesinvolved are not marketable. Exit options can beimplemented in parallel with other public sectormanagement reforms that increase voice and loyalty.
From neoclassical economics...One of the central tenets of neoclassical economics isthat competitive forces in an optimally functioningmarket lead to a more efficient allocation of resourcesthan command economy or non-market solutions.Neoclassical economic theory shows that, if certainconditions are met, competition produces an equili-brium in which it is impossible to make someonebetter off without making someone else worse off.
The neoclassical model categorizes goods andservices as private, mixed or public. Private goodsexhibit excludability (consumption by one individualprevents consumption by another; there are nopositive or negative externalities), rivalry (there iscompetition among goods based on price), andrejectability (individuals can choose to forgo con-sumption). True public goods have significantelements of non-excludability, non-rivalry, and non-rejectability. Mixed goods have some but not all ofthe characteristics of private goods (Fig. 1).
According to neoclassical theory a breakdownoccurs in both efficiency and equity when publicgoods or services with significant externalities areallocated through competitive markets. Even publicgoods can be sold in private markets but usually thisleads to suboptimal quantity, quality or price, therebycreating a strong justification for collective action.Likewise, significant problems occur in efficiency andequity when private goods are produced or providedby a public sector monopoly (23).
The perfectly competitive Walrasian modelassumes that:. the goods involved behave like true private goods
(i.e. there is excludability, rivalry and rejectability);
. rights can be perfectly delineated;
. there are no transaction costs.
Applying this to the health sector reveals that mosthealth care goods and services have some degree ofexcludability, rivalry and rejectability. However,rights are often difficult to delineate, leaving multipleresidual claimants. Furthermore, transaction costs areoften high. Even many health activities that generatesignificant externalities, such as sanitation services,the control and prevention of communicablediseases, health promotion, research and professionaleducation, are not pure public goods. For example, avaccine given to one patient cannot simultaneouslybe consumed by another patient. Patients can choosenot to be vaccinated, and vaccination programmesmay compete for market share.
Unfortunately, consumption characteristicsalone hardly ever indicate anything about the specificproduction processes that ensure technical effi-ciency. Although the neoclassical framework pro-vides a robust test to justify the need for stewardshipand financing, it does not help us understand theoptimal organizational arrangements for serviceproduction, being essentially institution-free (36). Itdoes not help to answer the following criticalquestion facing policy-makers. When a decision hasbeen taken to finance certain items, should the publicsector make or buy them?
... to institutional economics andorganizational theoryMuch progress has been made in identifying the keyfactors causing wide variations in the performancesof organizations. The developments most relevant tounderstanding the advantages and disadvantages ofdifferent arrangements for service delivery derivefrom principal/agent theory, transaction cost eco-nomics, property rights and public choice theory.These fields, often categorized as institutionaleconomics, deal with considerations of information,motivation and innovation and the implications forthe best possible organization of productive activity.Institutional economics is directly concerned withcreating the best possible structures for organizationsthat consist of individuals pursuing multiple andoften conflicting interests (37).
Agency theory. This framework shows thatsocial and political objectives may be more readilyachieved through a series of explicit and transparentcontracts for labour and services between an agent anda principal. The agent undertakes to perform varioustasks for the principal, in exchange for a mutuallyagreed award. The principal usually needs the effortsand expertise of the agent but has limited ability tomonitor the agent’s actions or evaluate whether theoutcome is satisfactory. On such matters as paymentand monitoring arrangements, the agency literaturesurveys the range of contracts observed in theeconomy with respect to incentives and cooperationamong self-interested but interdependent individuals
Fig. 1. The nature of goods based on neoclassical economics
Special Theme – Health Systems
780 Bulletin of the World Health Organization, 2000, 78 (6)

(38). Several studies have generalized the agencyinsight from the employment context to the full rangeof relationships that make up the firm, nowconceptualized as a nexus of many contracts (39,40). The need for incentive alignment is pervasive inthe health sector: the relationships between patientand physician or governments and contractingagencies are classical examples of the principal/agentstructure.
Transaction cost economics. Transaction costeconomics emphasizes the limitations of contractsand the need for flexible means of coordinatingactivities. Principals and agents are both opportunis-tic. Agents seek to minimize aggregate productionand transaction costs and to maximize their benefits.Unless closely monitored, agents may be unreliable,engaging in behaviour such as rent-seeking, cheating,breech of contract and incomplete disclosure.Principals may try to maximize their benefits to suchan extent that the relationship could become unviablefor the agent. The degree of such opportunism variesconsiderably from country to country and from onecultural setting to another. In some settings, such asmonopolistic national health services, opportunismmay be less apparent than in other settings whereproviders are more in the habit of competing witheach other. Opportunism may appear to be relativelypronounced in some countries, e.g. Chile, India, andthe USA. In others, e.g. Costa Rica, New Zealand, theScandinavian countries, Sri Lanka, and the UnitedKingdom, there is good evidence that principal/agent relationships within the national health servicesare vulnerable to opportunistic behaviour.
This theory sheds most light on firm bound-aries and the conditions under which it is better toarrange activities within a hierarchy rather thaninteracting in a market with suppliers or othercontractors. More generally, vertically integratedorganizations, simple spot contracts, franchises orjoint ventures are interpreted as discrete structuralalternatives, each offering different advantages anddisadvantages for effective governance (41). Gov-ernance arrangements are evaluated by comparingthe patterns of costs generated for planning, adaptingand monitoring production and exchange (42, 43).
Unlike public organizations, private firms havethe flexibility, indeed the requirement, to adjust theirgovernance structure to changes in the marketenvironment. This makes them fruitful sources ofbetter practices for governance arrangements. Publicagencies that have tried adjusting public organiza-tions to changes in the market environment haveoften encountered problems with underlying incen-tive structures and their sustainability. This hashappened in relation to the formation of NationalHealth Service Trusts in the United Kingdom, theestablishment of the Hospitals Authority in HongKong, and the corporatization of publicly ownedhospitals in New Zealand. Major policy reversals inNew Zealand and the United Kingdom have addedweight to the argument that it would have been better
to privatize than to settle for the imperfect middleground of public sector corporatization.
Thus, for example, vertically integrated organi-zation, i.e. within a firm, arises as a response toproblems with market contracting. The firm sub-stitutes low-powered incentives, like salaried employ-ment, for the high-poweredmarket incentives of profitand loss. Vertical integration, i.e. unified ownership,permits details of future relations between suppliers(including employees), producers and distributors toremain unspecified; differences can be adjudicated asevents unfold. It pools the risks and rewards of variousactivities undertaken by the organization, and canfacilitate the sharing of information, the pursuit ofinnovation, and a culture of cooperation.
Notwithstanding these positive features, ver-tical integration suffers from characteristic weak-nesses as a mechanism of governance. The two mostprominent are the weakening of incentives forproductivity and the proliferation of influenceactivities (see Box 1). Weak incentives arise whenpeople obtain shrinking gains from their own effortsas rewards and losses are spread throughout anorganization. From the standpoint of transaction costeconomics, vertical integration is seen as thegovernance mechanism of last resort, even thoughthe focus is on the contracting problems thatmotivate internal organization. Even in the manyinstances where policy objectives imply that spotmarket transactions are undesirable, unified owner-ship arrangements are outperformed by contractualnetworks, virtual integration, franchising or conces-sioning.
Property rights theory. Property rights theor-ists have attempted to find out why private owner-ship appears to have strong positive incentives forefficiency. Explanations have focused on the posses-sion of residual decision rights and the allocation ofresidual returns (45). Residual rights of control are therights to make any decisions regarding an asset’s usenot explicitly contracted by law or assigned to anotherby contract. The owner of an asset usually holds these
Box 1. Influence activities
An important issue related to moral hazard and the structure oforganizations is that of influence activities and the associatedcosts, known as influence costs (44). Recent analysis has shedmuch light on the propensity of publicly owned service deliveryorganizations to capture inordinate portions of the sectorbudget, as well as their ability to influence sector policy to theirbenefit, often against the public interest.In the health sector, provider organizations try to gainadvantages by affecting decisions on the distribution ofresources or other benefits among providers. Such influenceactivities occur in all organizations, but countervailing forces areparticularly weak in public service delivery structures. Influencecosts are one of the most important costs of centralized control.Evidence of such activities in the health sector is seen in thetendency to allocate resources to tertiary and curative care at theexpense of primary, preventive and public health activities.
Production of health care goods and services
781Bulletin of the World Health Organization, 2000, 78 (6)

rights, although the owner or the law may allocatemany rights to others. The notion of ownership asresidual control is relatively clear for a simple assetlike a motor car. It gets much more complicatedwhen applied to an organization such as a firm. Largeorganizations bundle together many assets, and itmay be unclear who has specific decision rights. Inaddition to residual decision rights, owners hold therights to residual revenue flows from their assets. Inother words, owners have the right to whateverrevenue remains after all funds have been collected,and all debts, expenses and other contractualobligations have been met.
Political choice theory. This field focuses onthe self-interested behaviour of politicians, interestgroups and bureaucrats, and studies the implicationsfor effective government and the size of government.Individuals are viewed as rational utility maximizers.Bureaucrats, attempting to maximize their budgets,acquire an increasing share of national income. As aresult the state grows well beyond what is needed forthe delivery of its core functions. Powerful interestgroups capture increasing portions of resources.Institutional rigidities develop which reduce eco-nomic growth (46).
This analysis has led public choice theorists tosupport conservative political agendas which mini-mize the role of the state.
Towards a new understanding ofthe production characteristics of goodsand servicesThe principles of institutional economics lead to amuch more refined and useful understanding of thedifferent kinds institutional arrangements requiredfor the efficient and effective production of goodsand services. A model can be developed on the basisof two characteristics of goods, namely contestabilityand measurability (Box 2) (47).
The contestability and measurabilitymatrix
It is possible categorize all health care goods andservices on a matrix along a continuum ranging fromhigh contestability and high measurability to lowcontestability, low measurability and significantinformational asymmetry. The following discussionrefers mainly to curative services and public healthservices, although the analysis could be extended tosome of the broader intersectoral determinants ofgood health, such as water, sanitation, education,healthy life-style policies and good nutrition.
Production characteristics of inputs(factor markets)The contestability and measurability matrix for theproduction of inputs would be as indicated in Fig. 2.
The production of consumable items and theretailing of drugs, medical supplies and other
consumables would be the best example of highlycontestable goods where outputs are also easy tomeasure (Type I). There are usually many companiesjostling for a share of the market and few barriers toentry. The initial investment capital is modest andthere are few requirements for specialized licensing orskills. Unskilled labour also belongs in this category.
As we move across the first row in Fig. 2 anumber of factors begin contributing to increasingbarriers to entry, thereby reducing the contestabilityof the goods or services in question (Type II).Investment cost (sunk cost) and increasing technicalspecifications create moderate barriers to entry in themanufacturing of specialized equipment and sup-plies. The wholesaling of drugs, medical supplies andmedical equipment encounters some barriers to entrybecause of larger investment requirements and morelimited supply and distribution chains. The speciali-zation and licensing of pharmacists contribute tothese entry barriers. In the case of small capital stock,such as clinics and diagnostic centres, entry barriersare mainly created though certification and licensing.
On moving across to Type III activities, e.g. theproduction of pharmaceuticals and high-technologymedical equipment, barriers to entry are much greaterbecause of large initial investment costs that cannot berecovered later when assets are sold (sunk costs).These production activities are also associated withcostly and long lead times needed for research,development and the registration of new products.
Box 2. Contestability and measurability
A market can be said to be perfectly contestable if firms canenter it freely (without any resistance from other firms) andsubsequently leave it without losing any investments, whilehaving equal access to technology (no asset specificity)(48–51 ). Contestability allows competition for the marketto substitute for competition in the market.Contestable goods are characterized by low barriers to entryand exit from the market, whereas non-contestable goods havehigh barriers such as "sunk cost", monopoly market power,geographical advantages and asset specificity. Investments inspecific assets represent a sunk cost since their value cannot berecovered elsewhere (52). Two specific assets that are ofparticular importance in the health sector are expertise andreputation. Once incumbents have invested in activities thatresult in expertise or generate trust, they enjoy a significantbarrier to entry for other potential suppliers, thereby loweringthe degree of contestability. Opportunism, on the other hand,lowers such trust or barriers to entry. The degree of suchopportunism varies from one country to another and betweendifferent cultural settings.Measurability in the health sector, as in other sectors, is theprecision with which inputs, processes, outputs and outcomesof particular goods or services can be measured. It is difficult tomeasure with precision the output and outcome of healthservices, which are characterized by informational asymmetry –the highly variable extent to which information about theperformance of a given activity is available to users,beneficiaries or contracting purchasing agencies.
Special Theme – Health Systems
782 Bulletin of the World Health Organization, 2000, 78 (6)
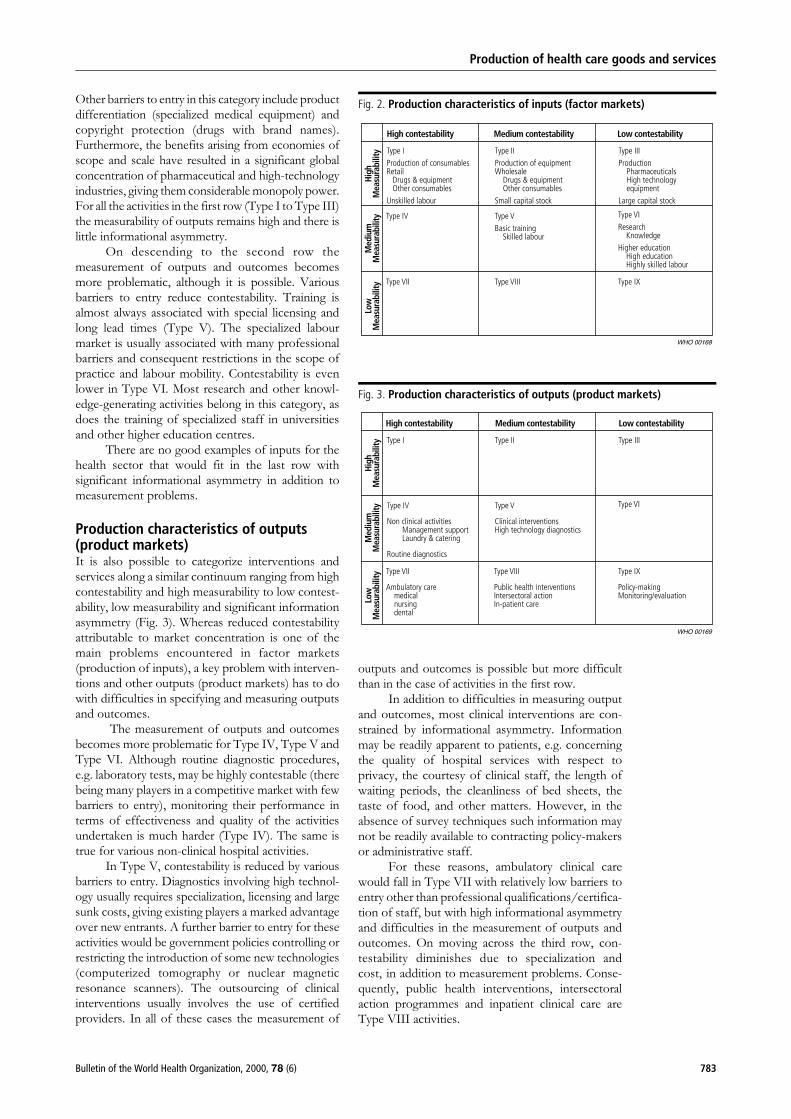
Other barriers to entry in this category include productdifferentiation (specialized medical equipment) andcopyright protection (drugs with brand names).Furthermore, the benefits arising from economies ofscope and scale have resulted in a significant globalconcentration of pharmaceutical and high-technologyindustries, giving them considerable monopoly power.For all the activities in the first row (Type I to Type III)the measurability of outputs remains high and there islittle informational asymmetry.
On descending to the second row themeasurement of outputs and outcomes becomesmore problematic, although it is possible. Variousbarriers to entry reduce contestability. Training isalmost always associated with special licensing andlong lead times (Type V). The specialized labourmarket is usually associated with many professionalbarriers and consequent restrictions in the scope ofpractice and labour mobility. Contestability is evenlower in Type VI. Most research and other knowl-edge-generating activities belong in this category, asdoes the training of specialized staff in universitiesand other higher education centres.
There are no good examples of inputs for thehealth sector that would fit in the last row withsignificant informational asymmetry in addition tomeasurement problems.
Production characteristics of outputs(product markets)It is also possible to categorize interventions andservices along a similar continuum ranging from highcontestability and high measurability to low contest-ability, low measurability and significant informationasymmetry (Fig. 3). Whereas reduced contestabilityattributable to market concentration is one of themain problems encountered in factor markets(production of inputs), a key problem with interven-tions and other outputs (product markets) has to dowith difficulties in specifying and measuring outputsand outcomes.
The measurement of outputs and outcomesbecomes more problematic for Type IV, Type V andType VI. Although routine diagnostic procedures,e.g. laboratory tests, may be highly contestable (therebeing many players in a competitive market with fewbarriers to entry), monitoring their performance interms of effectiveness and quality of the activitiesundertaken is much harder (Type IV). The same istrue for various non-clinical hospital activities.
In Type V, contestability is reduced by variousbarriers to entry. Diagnostics involving high technol-ogy usually requires specialization, licensing and largesunk costs, giving existing players a marked advantageover new entrants. A further barrier to entry for theseactivities would be government policies controlling orrestricting the introduction of some new technologies(computerized tomography or nuclear magneticresonance scanners). The outsourcing of clinicalinterventions usually involves the use of certifiedproviders. In all of these cases the measurement of
outputs and outcomes is possible but more difficultthan in the case of activities in the first row.
In addition to difficulties in measuring outputand outcomes, most clinical interventions are con-strained by informational asymmetry. Informationmay be readily apparent to patients, e.g. concerningthe quality of hospital services with respect toprivacy, the courtesy of clinical staff, the length ofwaiting periods, the cleanliness of bed sheets, thetaste of food, and other matters. However, in theabsence of survey techniques such information maynot be readily available to contracting policy-makersor administrative staff.
For these reasons, ambulatory clinical carewould fall in Type VII with relatively low barriers toentry other than professional qualifications/certifica-tion of staff, but with high informational asymmetryand difficulties in the measurement of outputs andoutcomes. On moving across the third row, con-testability diminishes due to specialization andcost, in addition to measurement problems. Conse-quently, public health interventions, intersectoralaction programmes and inpatient clinical care areType VIII activities.
Fig. 2. Production characteristics of inputs (factor markets)
Fig. 3. Production characteristics of outputs (product markets)
Production of health care goods and services
783Bulletin of the World Health Organization, 2000, 78 (6)
This leaves a few distinct activities such aspolicy-making, monitoring and evaluation in theType IX category. The contestability and measur-ability of these activities are extremely low, and theyare therefore usually retained as a core part of anintegrated bureaucracy.
‘‘Make or buy’’ decision grid
PrioritizeIn many countries, ‘‘make or buy’’ decisions are madebefore policy-makers and providers have gonethrough a process of explicit prioritization aboutthe range of interventions to be financed throughpublic resources (including preventive services) andof ensuring that public subsidies are appropriatelytargeted (e.g. on the poor and other vulnerablegroups) (53). Countries often make hasty ‘‘make orbuy’’ decisions before prioritizing interventions thatare needed and affordable. Such prioritization iscomplicated by the fact that the costs of treatingdifferent illnesses vary greatly and often bear littlerelation to the effectiveness of available interventions(54). Furthermore, there may be a range of activitiesfor which information disclosure and coordinationthrough a strong stewardship function is sufficient.
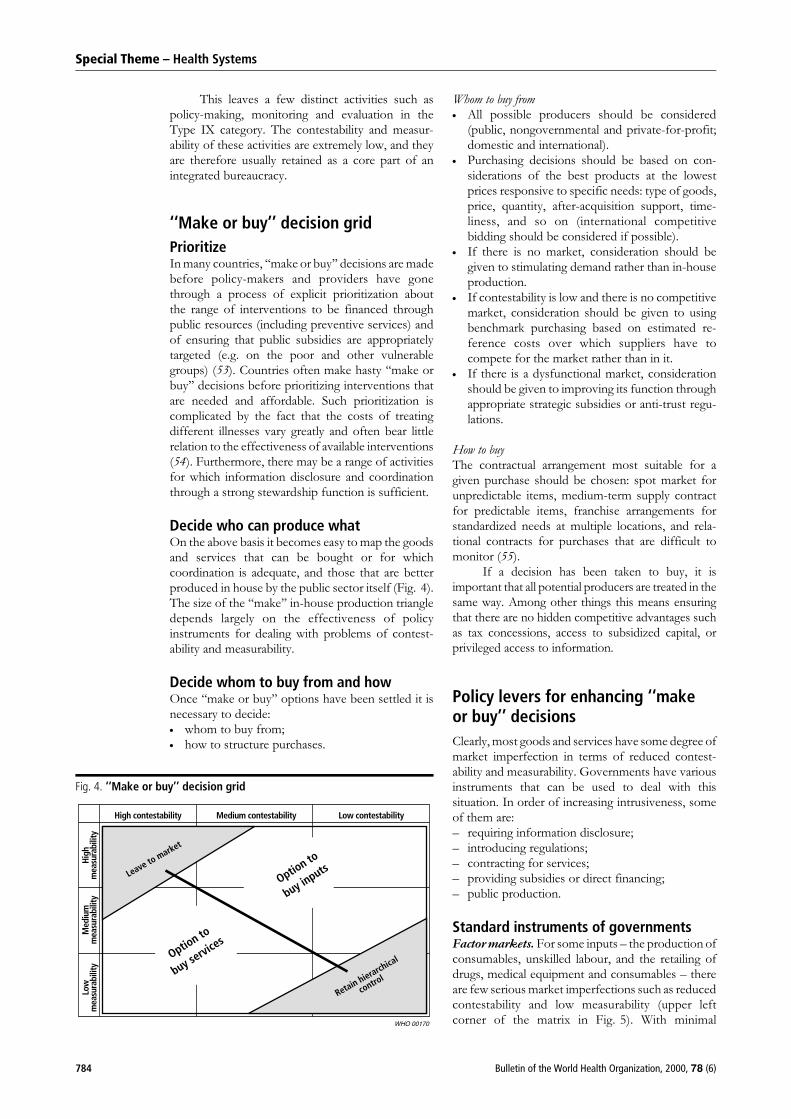
Decide who can produce whatOn the above basis it becomes easy to map the goodsand services that can be bought or for whichcoordination is adequate, and those that are betterproduced in house by the public sector itself (Fig. 4).The size of the ‘‘make’’ in-house production triangledepends largely on the effectiveness of policyinstruments for dealing with problems of contest-ability and measurability.
Decide whom to buy from and howOnce ‘‘make or buy’’ options have been settled it isnecessary to decide:. whom to buy from;. how to structure purchases.
Whom to buy from. All possible producers should be considered
(public, nongovernmental and private-for-profit;domestic and international).
. Purchasing decisions should be based on con-siderations of the best products at the lowestprices responsive to specific needs: type of goods,price, quantity, after-acquisition support, time-liness, and so on (international competitivebidding should be considered if possible).
. If there is no market, consideration should begiven to stimulating demand rather than in-houseproduction.
. If contestability is low and there is no competitivemarket, consideration should be given to usingbenchmark purchasing based on estimated re-ference costs over which suppliers have tocompete for the market rather than in it.
. If there is a dysfunctional market, considerationshould be given to improving its function throughappropriate strategic subsidies or anti-trust regu-lations.
How to buy
The contractual arrangement most suitable for agiven purchase should be chosen: spot market forunpredictable items, medium-term supply contractfor predictable items, franchise arrangements forstandardized needs at multiple locations, and rela-tional contracts for purchases that are difficult tomonitor (55).
If a decision has been taken to buy, it isimportant that all potential producers are treated in thesame way. Among other things this means ensuringthat there are no hidden competitive advantages suchas tax concessions, access to subsidized capital, orprivileged access to information.
Policy levers for enhancing ‘‘makeor buy’’ decisions
Clearly, most goods and services have some degree ofmarket imperfection in terms of reduced contest-ability and measurability. Governments have variousinstruments that can be used to deal with thissituation. In order of increasing intrusiveness, someof them are:– requiring information disclosure;– introducing regulations;– contracting for services;– providing subsidies or direct financing;– public production.
Standard instruments of governmentsFactor markets. For some inputs – the production ofconsumables, unskilled labour, and the retailing ofdrugs, medical equipment and consumables – thereare few serious market imperfections such as reducedcontestability and low measurability (upper leftcorner of the matrix in Fig. 5). With minimal
Fig. 4. ‘‘Make or buy’’ decision grid
Special Theme – Health Systems
784 Bulletin of the World Health Organization, 2000, 78 (6)
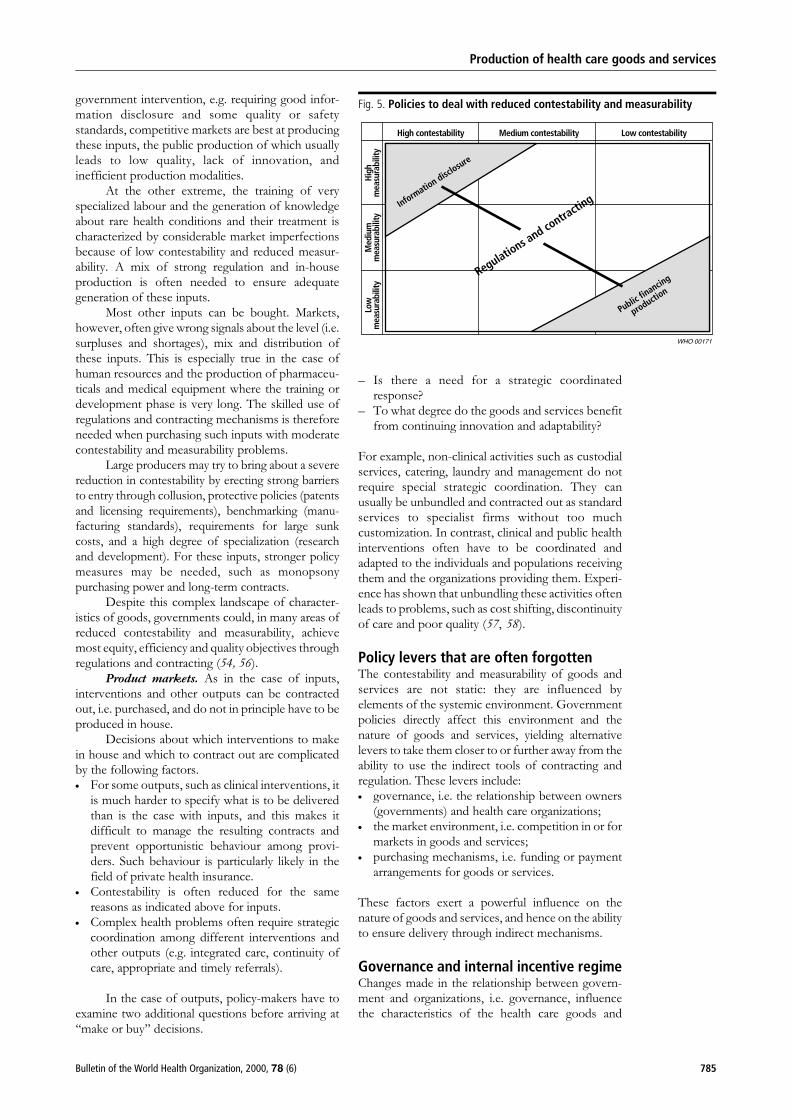
government intervention, e.g. requiring good infor-mation disclosure and some quality or safetystandards, competitive markets are best at producingthese inputs, the public production of which usuallyleads to low quality, lack of innovation, andinefficient production modalities.
At the other extreme, the training of veryspecialized labour and the generation of knowledgeabout rare health conditions and their treatment ischaracterized by considerable market imperfectionsbecause of low contestability and reduced measur-ability. A mix of strong regulation and in-houseproduction is often needed to ensure adequategeneration of these inputs.
Most other inputs can be bought. Markets,however, often give wrong signals about the level (i.e.surpluses and shortages), mix and distribution ofthese inputs. This is especially true in the case ofhuman resources and the production of pharmaceu-ticals and medical equipment where the training ordevelopment phase is very long. The skilled use ofregulations and contracting mechanisms is thereforeneeded when purchasing such inputs with moderatecontestability and measurability problems.
Large producers may try to bring about a severereduction in contestability by erecting strong barriersto entry through collusion, protective policies (patentsand licensing requirements), benchmarking (manu-facturing standards), requirements for large sunkcosts, and a high degree of specialization (researchand development). For these inputs, stronger policymeasures may be needed, such as monopsonypurchasing power and long-term contracts.
Despite this complex landscape of character-istics of goods, governments could, in many areas ofreduced contestability and measurability, achievemost equity, efficiency and quality objectives throughregulations and contracting (54, 56).
Product markets. As in the case of inputs,interventions and other outputs can be contractedout, i.e. purchased, and do not in principle have to beproduced in house.
Decisions about which interventions to makein house and which to contract out are complicatedby the following factors.. For some outputs, such as clinical interventions, it
is much harder to specify what is to be deliveredthan is the case with inputs, and this makes itdifficult to manage the resulting contracts andprevent opportunistic behaviour among provi-ders. Such behaviour is particularly likely in thefield of private health insurance.
. Contestability is often reduced for the samereasons as indicated above for inputs.
. Complex health problems often require strategiccoordination among different interventions andother outputs (e.g. integrated care, continuity ofcare, appropriate and timely referrals).
In the case of outputs, policy-makers have toexamine two additional questions before arriving at‘‘make or buy’’ decisions.
– Is there a need for a strategic coordinatedresponse?
– To what degree do the goods and services benefitfrom continuing innovation and adaptability?
For example, non-clinical activities such as custodialservices, catering, laundry and management do notrequire special strategic coordination. They canusually be unbundled and contracted out as standardservices to specialist firms without too muchcustomization. In contrast, clinical and public healthinterventions often have to be coordinated andadapted to the individuals and populations receivingthem and the organizations providing them. Experi-ence has shown that unbundling these activities oftenleads to problems, such as cost shifting, discontinuityof care and poor quality (57, 58).
Policy levers that are often forgottenThe contestability and measurability of goods andservices are not static: they are influenced byelements of the systemic environment. Governmentpolicies directly affect this environment and thenature of goods and services, yielding alternativelevers to take them closer to or further away from theability to use the indirect tools of contracting andregulation. These levers include:. governance, i.e. the relationship between owners
(governments) and health care organizations;. the market environment, i.e. competition in or for
markets in goods and services;. purchasing mechanisms, i.e. funding or payment
arrangements for goods or services.
These factors exert a powerful influence on thenature of goods and services, and hence on the abilityto ensure delivery through indirect mechanisms.
Governance and internal incentive regimeChanges made in the relationship between govern-ment and organizations, i.e. governance, influencethe characteristics of the health care goods and
Fig. 5. Policies to deal with reduced contestability and measurability
Production of health care goods and services
785Bulletin of the World Health Organization, 2000, 78 (6)

services in question. This relationship can bemodified substantially in five dimensions:– the rights given to managers to make decisions;– the residual claimant status;– the degree of market exposure;– accountability arrangements;– the adequacy of subsidies to cover social
functions (59).
Contestability may be enhanced by:– unbundling large bureaucratic structures (modi-
fication in governance);– outsourcing other functions to specialized provi-
ders (modification in payment system);– exposing all public and private actors to the same
potential benefits and losses attributable to marketexposure (modification in governance and pay-ment system);
– decreasing barriers to entry caused by politicalinterference or unwarranted trust in publicproduction (modification in market structure);
– explicitly separating contestable commercial func-tions and non-commercial social objectives (modi-fication in governance and stewardship).
Measurability may be enhanced by:– relying on quantifiable results (output or outcome
measures) for accountability and performancetargets rather than process (inputs and bureau-cratic procedures) (modification in governanceand payment system);
– shifting from difficult-to-define long-term rela-tionships (employment or service arrangements)to shorter-term, more specific contractual ar-rangements (modification in payment system);
– using quantifiable monetary incentives rather thannon-monetary incentives, e.g. involving consid-erations of ethics, ethos and status, which aremore difficult to track (modification in paymentsystem);
– tightening reporting, monitoring and account-ability mechanisms (modification in governanceand payment system).
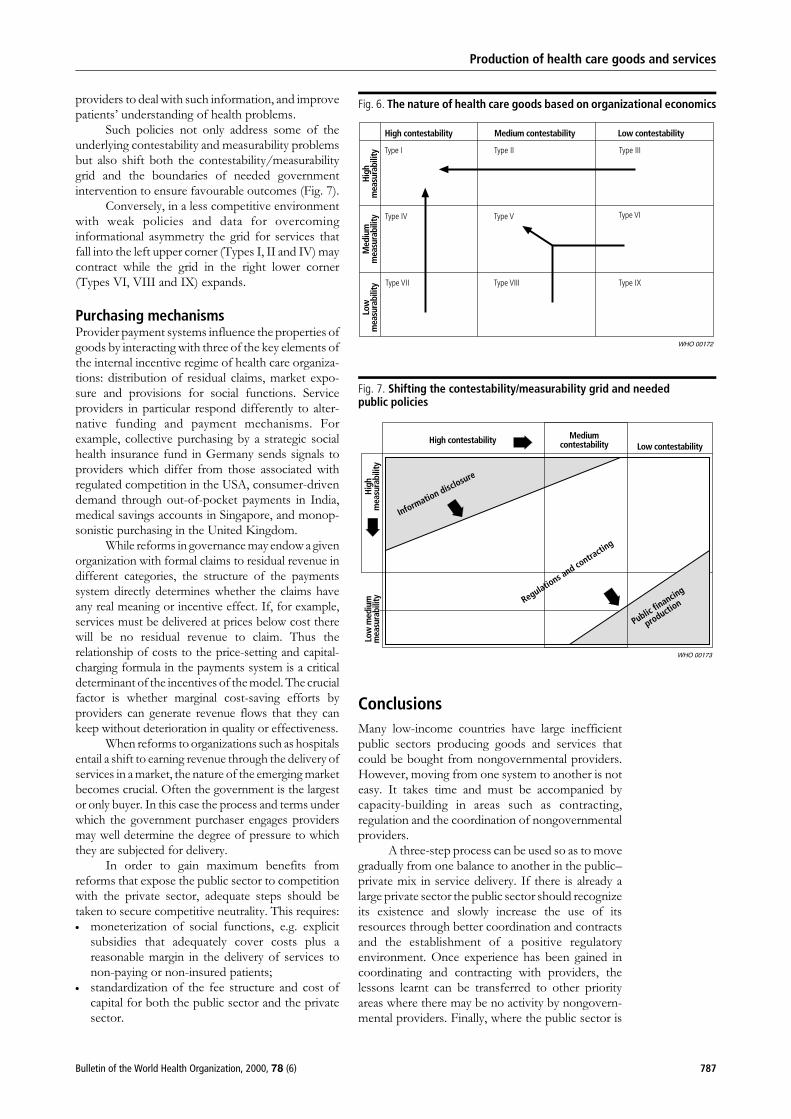
For example, by removing restrictive governmentmonopolies from vaccination services (governance/market), programmes could be shifted into a Type IIor even a Type I position. It is easy to measure thenumber of children vaccinated or contracting a givendisease, and to have moderately low barriers to entryfor firms that want to provide such services on behalfof government. Similar action applied to otherservices could shift many of them from the lowerright corner of the grid towards the upper left corner(Fig. 6).
Likewise, through better information on out-come and policies favouring clearly defined con-tracts, performance benchmarks, and a tightening ofreporting, monitoring and accountability mechan-isms, it would be possible to shift tertiary andquaternary care provided in universities from a lowcontestability/measurability position to a medium
position. The same would be true for public healthservices and public health activities that are often partof the responsibility of ambulatory care providers,e.g. vaccination.
Several factors may also alter the goodscharacteristics of pharmaceuticals, medical equip-ment and consumable supplies. Medical equipmentor drugs that were highly specialized and veryexpensive due to development costs, patent protec-tion, and a small market share (Type III goods) onlyten years ago, may now behave as ordinary goods(Type I or Type II). Examples include the productionof generic drugs by many companies once patentprotection expires or the rapid increase in the use ofsigmoidoscopes and/or transcutaneous surgical in-struments once the technology is no longer new andprices have dropped.
Changes in the characteristics of goods do notoccur in only one direction. The properties of goodsmay become less contestable and more difficult tomeasure. Organizational reforms do not always leadto increased decision rights, residual claimant status,market exposure, accountability arrangements andexplicit subsidies to cover social functions. Manynational health systems that were introduced thoughthe nationalization of ownership and productionduring the past 50 years deliberately shifted goodsand services in the opposite direction.
Market imperfections may increase rather thanreduce barriers to entry. Doctors, dentists andpharmacists collude to restrict entry by potentialcompetitors. Hospitals have a natural monopoly fortheir services for patients living nearby, and can createmonopoly power through relations with otherhospitals and referring doctors. Local medicalequipment distributors that represent some of thebiggest international companies can easily mono-polize domestic markets. Pharmaceutical retailers cancontrol mark-ups through professional cartels. Thepublic and nongovernmental sectors have a compe-titive advantage over the private sector because oftheir access to subsidized or free capital fromdomestic and foreign donors.
Market environmentOne of the central arguments in favour of exposingproviders to market forces is that, in a functioningmarket, competitive forces lead to a more efficientallocation of resources than is the case withcommand economy or non-market solutions. Thestructure of the market to which organizations areexposed, therefore, has a critical influence on theirbehaviour. It may directly determine the strategies tobe adopted for the generation of increased revenue.
Policies that influence the competitive envi-ronment through regulations or contracting cansignificantly alter the contestability of health caregoods and services. Likewise, informational asym-metry can be reduced by policies that increase theavailability of good information on health services,enhance the institutional capacity of health care
Special Theme – Health Systems
786 Bulletin of the World Health Organization, 2000, 78 (6)
providers to deal with such information, and improvepatients’ understanding of health problems.
Such policies not only address some of theunderlying contestability and measurability problemsbut also shift both the contestability/measurabilitygrid and the boundaries of needed governmentintervention to ensure favourable outcomes (Fig. 7).
Conversely, in a less competitive environmentwith weak policies and data for overcominginformational asymmetry the grid for services thatfall into the left upper corner (Types I, II and IV) maycontract while the grid in the right lower corner(Types VI, VIII and IX) expands.
Purchasing mechanismsProvider payment systems influence the properties ofgoods by interacting with three of the key elements ofthe internal incentive regime of health care organiza-tions: distribution of residual claims, market expo-sure and provisions for social functions. Serviceproviders in particular respond differently to alter-native funding and payment mechanisms. Forexample, collective purchasing by a strategic socialhealth insurance fund in Germany sends signals toproviders which differ from those associated withregulated competition in the USA, consumer-drivendemand through out-of-pocket payments in India,medical savings accounts in Singapore, and monop-sonistic purchasing in the United Kingdom.
While reforms in governancemay endow a givenorganization with formal claims to residual revenue indifferent categories, the structure of the paymentssystem directly determines whether the claims haveany real meaning or incentive effect. If, for example,services must be delivered at prices below cost therewill be no residual revenue to claim. Thus therelationship of costs to the price-setting and capital-charging formula in the payments system is a criticaldeterminant of the incentives of themodel. The crucialfactor is whether marginal cost-saving efforts byproviders can generate revenue flows that they cankeep without deterioration in quality or effectiveness.
When reforms to organizations such as hospitalsentail a shift to earning revenue through the delivery ofservices in a market, the nature of the emerging marketbecomes crucial. Often the government is the largestor only buyer. In this case the process and terms underwhich the government purchaser engages providersmay well determine the degree of pressure to whichthey are subjected for delivery.
In order to gain maximum benefits fromreforms that expose the public sector to competitionwith the private sector, adequate steps should betaken to secure competitive neutrality. This requires:. moneterization of social functions, e.g. explicit
subsidies that adequately cover costs plus areasonable margin in the delivery of services tonon-paying or non-insured patients;
. standardization of the fee structure and cost ofcapital for both the public sector and the privatesector.
Conclusions
Many low-income countries have large inefficientpublic sectors producing goods and services thatcould be bought from nongovernmental providers.However, moving from one system to another is noteasy. It takes time and must be accompanied bycapacity-building in areas such as contracting,regulation and the coordination of nongovernmentalproviders.
A three-step process can be used so as to movegradually from one balance to another in the public–private mix in service delivery. If there is already alarge private sector the public sector should recognizeits existence and slowly increase the use of itsresources through better coordination and contractsand the establishment of a positive regulatoryenvironment. Once experience has been gained incoordinating and contracting with providers, thelessons learnt can be transferred to other priorityareas where there may be no activity by nongovern-mental providers. Finally, where the public sector is
Fig. 6. The nature of health care goods based on organizational economics
Fig. 7. Shifting the contestability/measurability grid and neededpublic policies
Production of health care goods and services
787Bulletin of the World Health Organization, 2000, 78 (6)

clearly engaged in inefficient activities, as is the casewith the production of many inputs, they can beconverted through outright privatization and subse-quently bought from the private sector (56).
However, the public sector may not beinvolved in areas of strategic importance, such asthe collective financing of health services. Conse-
quently, in parallel with moving out of the area ofproduction of goods and services, in many low-income and middle-income countries it may bedesirable to have a more integrated approach andgreater public sector involvement in health carefinancing, knowledge generation and the provision ofhuman resources. n
Resume
Decisions relatives a la sous-traitance des produits et services de sante : nouveauxenseignements de l’economie institutionnelle et de la theorie de l’organisationLes systemes de sante ont quatre fonctions centrales :generer des apports (connaissances, ressources humai-nes, produits pharmaceutiques, materiel et produitsmedicaux) ; assurer un financement (mobilisation desressources, mise en commun des risques et servicesd’achat) ; fournir des services (sante publique, soinsambulatoires et soins hospitaliers) ; et s’occuper del’administration generale (elaboration des politiques,supervision, coordination, reglementation, surveillanceet evaluation). Les systemes de sante de bon nombre depays a revenu faible ou moyen ne fonctionnent pas bien,parfois a cause du developpement inegal de cesfonctions et parfois a cause de desequilibres entre lerole joue par l’Etat et celui joue par le marche.
Le present article propose un cadre conceptuelvisant a aider les gouvernements a parvenir a desdecisions plus rationnelles en matiere de sous-traitancepour ce qui est de la production de produits et de servicesde sante. Par exemple, concernant les travaux nonqualifies et la vente au detail de medicaments, defournitures et de produits medicaux, les rendements sontfaciles a mesurer et les fournisseurs sont en generalnombreux. Dans la plupart des pays, ces activites sontlaissees au secteur prive et l’engagement de l’Etat y estminimal. Une participation plus importante de l’Etat estsouvent necessaire sous la forme de reglementations etde sous-traitance strategique visant a assurer desresultats optimaux pour ce qui est de la fabrication demateriel et de fournitures et de la vente en gros desmedicaments, des fournitures et du materiel medicaux.La production de substances pharmaceutiques et demateriel medical complexe est associee a un investisse-ment initial important et a une concentration du marche,qui limitent la concurrence. Cependant, meme dans cecas, la reglementation en matiere de qualite, les mesuresantitrust et les achats en situation de monopole sontpreferables a une production publique qui, en general, sesolde par la fabrication de produits de mauvaise qualite,une absence d’innovation, une technologie depassee etdes modalites de production inefficaces.
Tandis que la reduction de la concurrenceimputable a la concentration du marche est l’un desprincipaux problemes rencontres dans la productiond’apports dans ce domaine, le probleme essentiel auquelse heurte l’offre des services de sante publique et desservices curatifs n’est pas sans rapport avec les difficultesqui se posent pour preciser et observer les produits et lesresultats obtenus. Dans beaucoup de pays, les soinsambulatoires sont deja assures par le secteur prive (a butlucratif ou non) par le biais d’un financement public(sous-traitance) ou par paiement direct dans le secteurinformel. Les soins hospitaliers et les services de santepublique exigent des mecanismes de sous-traitance pluselabores et un environnement reglementaire plus solideavant que les pouvoirs publics puissent les confier ausecteur prive. Toutefois, meme en pareilles circonstan-ces, des activites auxiliaires telles que les services degestion et de soutien non clinique peuvent souvent etredissociees et externalisees.
L’assurance-maladie presente un tableau diffe-rent. Si beaucoup de fournisseurs et de produitsobservables (couverture de l’assurance) plaident enfaveur de solutions obeissant aux lois du marche,l’assurance medicale privee est, dans la pratique,associee a une grave carence du marche et a une pertede protection financiere generale de la population contrele cout de la maladie. Pour des raisons strategiques, laplupart des pays choisissent de conserver cette fonctiondans le secteur public.
Tout milite en faveur d’une plus grande participa-tion du secteur prive aux apports et a la fourniture desservices de sante parallelement a l’engagement plusimportant des pouvoirs publics en faveur des objectifsd’equite, d’efficacite et de qualite, lie au mandatd’administration generale et de financement qui est leleur. Malheureusement, bon nombre de pays a revenufaible et moyen consacrent une grande partie des fondspublics a la production, laissant peu de ressources pourl’achat strategique de services aupres d’organisationsnon gouvernementales et de dispensateurs prives.
Resumen
Decisiones relativas a la subcontratacion de productos y servicios de salud:nuevas ensenanzas de la economıa institucional y la teorıa de la organizacionLos sistemas de salud tienen cuatro funciones basicas:generacion de insumos (conocimientos, recursos huma-nos, productos farmaceuticos, equipo medico y material
fungible); financiacion (movilizacion de recursos, man-comunacion de riesgos y compra de servicios); prestacionde servicios (salud publica, atencion ambulatoria y
Special Theme – Health Systems
788 Bulletin of the World Health Organization, 2000, 78 (6)

atencion hospitalaria); y rectorıa (elaboracion depolıticas, supervision, coordinacion, reglamentacion,vigilancia y evaluacion). Los sistemas de salud demuchos paıses de ingresos bajos y medios no funcionanadecuadamente, a veces a causa del desarrollodesparejo de esas funciones y a veces de losdesequilibrios entre la funcion del Estado y la delmercado.
En el presente artıculo se propone un marcoconceptual para ayudar a los gobiernos a adoptardecisiones mas racionales por lo que respecta a lasubcontrata durante la produccion de bienes y serviciosde atencion de salud. Por ejemplo, en lo concerniente a laproduccion de personal no calificado y la venta al pormenor de medicamentos, suministros medicos y otrosbienes fungibles, los resultados son faciles de medir y porlo general hay muchos proveedores. En muchos paıses,estas actividades se dejan en manos del sector privado yla participacion del Estado es mınima. A menudo, esnecesaria una mayor participacion del Estado en formade reglamentaciones y contratos estrategicos para lograrresultados optimos en la fabricacion de equipo ysuministros y en la venta al por mayor de medicamentos,suministros y equipo medicos. La produccion depreparaciones farmaceuticas y equipo medico complejorequiere una inversion inicial y una concentracion delmercado considerables, y esos dos factores limitan lacompetencia. Incluso en este caso, sin embargo, lareglamentacion de la calidad, las medidas antimonopolioy la compra en regimen de monopsonio son preferibles ala produccion publica, que por lo general implicaproductos de baja calidad, falta de innovacion,tecnologıa obsoleta y modos de produccion ineficaces.
Mientras que la reduccion de la competenciaatribuible a la concentracion del mercado es uno de losproblemas principales con que se tropieza en laproduccion de insumos, el problema fundamental en la
produccion de servicios de salud publica y servicioscurativos tiene que ver con las dificultades que planteanla especificacion y la observacion de los productos y losresultados. En muchos paıses, la atencion ambulatoria yala presta el sector privado (con o sin fines de lucro)mediante financiacion publica sobre una base con-tractual o mediante financiacion directa en el sectorinformal. La atencion hospitalaria y los servicios de saludpublica requieren mecanismos mas cualificados decontratacion y un entorno normativo mas estricto paraque los gobiernos puedan adquirir esos servicios al sectorprivado. Aun en estas circunstancias, las actividadessubsidiarias, como la gestion y los servicios de apoyo noclınicos, a menudo se pueden disociar y confiar aterceros.
Ahora bien, el panorama es diferente en lo tocanteal seguro de enfermedad. Aunque son numerosos losproveedores y los resultados observables (coberturamediante seguro) que hacen preferibles las solucionesbasadas en el mercado, el seguro de enfermedadprivado, en la practica, esta asociado a fallos graves delmercado y a una perdida de la proteccion financierageneral de la poblacion contra los gastos de enfermedad.Por razones estrategicas, la mayorıa de los paısesprefieren mantener esta funcion dentro del sectorpublico.
Hay solidos argumentos en favor de una mayorparticipacion del sector privado en la generacion deinsumos y la prestacion de servicios de salud, que seacompane paralelamente de un mayor empeno delgobierno en conseguir los objetivos de equidad,eficiencia y calidad mediante la funcion de rectorıa y lafinanciacion. Lamentablemente, muchos paıses deingresos bajos y medios dedican una gran parte de losfondos publicos a la produccion, dejando pocos recursospara la compra estrategica de servicios a organizacionesno gubernamentales y proveedores privados.
References
1. Arrow K. Arrow’s theorem: the paradox of social choice.New Haven, CT, Yale University Press, 1980.
2. Evans RG. Strained mercy. Toronto, Butterworth, 1984.3. Rice T. The economics of health reconsidered. Chicago, IL,
Health Administration Press, 1998.4. Bator, F. The anatomy of market failure. Quarterly Journal
of Economics, 1958, 72: (3): 351–379.5. Atkinson AB, Stiglitz JE. Lectures on public economics.
Maidenhead, McGraw-Hill, 1980.6. Musgrave RA, Musgrave PB. Public finance in theory
and practice. 4th edition. New York, McGraw-Hill, 1984.7. Barer ML et al, eds. Health, health care and health
economics: perspectives on distribution. Chichester, John Wiley& Sons, 1998.
8. van Doorslaer E, Wagstaff A, Rutten F, eds. Equity inthe finance and delivery of health care: an internationalperspective. Oxford, Oxford Medical Publications, 1993.
9. Arrow KW. Uncertainty and the welfare economics of medicalcare. American Economics Review, 1963, 53 (5): 940–973.
10. Barr N, ed. Labor markets and social policy in central andEastern Europe. New York,Oxford University Press for TheWorld Bank, 1994.
11. Investing in people and growth. In: World development report1996: from plan to market. New York, Oxford University Pressfor The World Bank, 1996: 123–132.
12. Wolf CJ. A theory of non-market failure. Journal of Lawand Economics, 1979, 22 (1): 107–139.
13. Peacock A. On the anatomy of collective failure. Public Finance,1980, 35 (1): 33–43.
14. Weimer DL, Vining AR. Policy analysis: concept and practice.Englewood Cliffs, NJ, Prentice Hill, 1989.
15. Vining AR, Weimer DL. Government supply and governmentproduction failure: a framework based on contestability. Journalof Public Policy, 1990, 10 (1): 1–22.
16. Moore M. Creating public value. Cambridge, MA, HarvardUniversity Press, 1995.
17. Fama EF, Jensen MC. Agency problems and residual claims.Journal of Law and Economics, 1983, 26 (2): 327–349.
18. Preker AS, Harding A, Girishankar N. The economicsof private participation in health care: new insights frominstitutional economics. Geneva, International LabourOrganization, 2000.
19. World Bank. World development report 1993: investingin health. New York, Oxford University Press for The World Bank,1993.
Production of health care goods and services
789Bulletin of the World Health Organization, 2000, 78 (6)

20. World Bank. Sector strategy: health, nutrition, and population.Washington, DC, The World Bank, 1997.
21. World Bank. World development report 1997: the state ina changing world. New York, Oxford University Press for TheWorld Bank, 1997.
22. World health report 1999–Making a difference. Geneva, WorldHealth Organization, 1999.
23. Preker AS, Feachem RGA. Market mechanisms and thehealth sector in Central and Eastern Europe. Washington, DC,The World Bank, 1996 (Technical Paper Series, No. 293).
24. Young P. Privatization around the globe: lessons fromthe Reagan Administration. Houston, TX, National Center forPolicy Analysis, 1986.
25. Vickers JS, Yarrow GK. Privatization: an economic analysis.Cambridge, MA, MIT Press, 1992.
26. Enthoven A. Consumer choice health plan. New England Journalof Medicine, 1978, 298 (12): 650–658; 298 (13); 709–720.
27. Enthoven A. Theory and practice of managed competitionin health care finance. Netherlands, North-Holland, 1988.
28. Wilson JQ. Bureaucracy. New York, Basic Books, 1989.29. Donahue JD. The privatization decision: public ends, private
means. New York, Basic Books, 1989.30. Osborne D, Gaebler T. Reinventing government. New York,
Plume, 1993.31. Saltman RB, Figueras J. European health care reforms: analysis
of current strategies. Copenhagen, World Health OrganizationRegional Office for Europe, 1997 (WHO Regional Publications,European Series, No. 72).
32. Musgrove P. Public and private roles in health: theoryand financing patterns. Washington, DC, The World Bank, 1996(World Bank Discussion Paper No. 339).
33. Schieber G, ed. Innovations in health financing. Washington,DC, The World Bank, 1996.
34. The world health report 2000–Health systems: improvingperformance. Geneva, World Health Organization, 2000.
35. Hirschman A. Exit, voice, and loyalty: responses to declinein firms, organizations, and states. Cambridge, MA, HarvardUniversity Press, 1970.
36. Robinson J. Physician-hospital integration and economic theoryof the firm. Medical Care Research and Review, 1997, 54: 1.
37. Regulatory reform, privatisation and competition policy. Paris,Organisation for Economic Co-operation and Development,1992: 17.
38. Sappington DE. Incentives in principal-agent relationships.Journal of Economic Perspectives, 1991, 5 (2): 45–66.
39. Fama EF. Agency problems and the theory of the firm. Journalof Political Economy, 1980, 88 (2): 288–307.
40. Jensen MC, Meckling WH. Theory of the firm: managerialbehavior, agency costs and ownership structure. Journalof Financial Economics, 1976, 3: 305–360.
41. Williamson O. Comparative economic organization: the analysisof discrete structural alternatives. Administrative ScienceQuarterly, 1991, 36: 69–296.
42. Williamson O. The economic institutions of capitalism: firms,markets and relational contracting. NewYork, Free Press, 1985.
43. Williamson O. Transaction cost economics. In: Schmalensee R,Willig R, eds. Handbook of industrial organization. New York,North-Holland, 1989.
44. Milgrom P, Roberts J. Bargaining costs, influence costs, andthe organization of economic activity. In: Alt J, Shepsle K, eds.Perspectives on positive political economy. New York, CambridgeUniversity Press, 1990: 57–89.
45. Milgrom P, Roberts J., Economics of organization andmanagement, Englewood Cliffs, NJ, Prentice-Hall, 1992.
46. Olson M. The rise and decline of nations: economic growth,stagflation and social rigidities. New Haven, Yale University Press,1982.
47. Girishankar N. Reforming institutions for service delivery:a framework for development assistance with an applicationto the HNP portfolio. Washington, DC, The World Bank, 1999(Policy Research Working Paper 2039).
48. Baumol WJ, Panzar JC, Willing RD. Contestable marketsand the theory of industrial structure. New York, Harcourt BraceJovanovich, 1982.
49. Baumol WJ Towards a theory of public enterprise. AtlanticEconomic Journal, 1984, 12 (1): 3–20.
50. Shepherd WG. Contestability vs. competition – once more.Land Economics, 1995, 71 (3): 299–309.
51. Shepherd WG. Contestability vs. competition. AmericanEconomic Review, 1984, 74 (4): 572–587.
52. Klein B, Crawford RG, Alchian AA. Vertical integration,appropriable rents and the competitive contracting process.Journal of Law and Economics, 1978, 21 (2): 297–226.
53. Ham C. Priority setting in health care: learning from internationalexperience. Health Policy, 1997, 42 (1): 49–66.
54. Musgrove P. Public spending on health care: how are differentcriteria related? Health Policy, 1999, 47: 207–223.
55. Harding A, Preker AS, eds. Private participation toolkit,Washington, DC, The World Bank, 2000 (forthcoming).
56. Herzlinger RE. Market driven health care: who wins, wholoses in the transformation of America’s largest service industry?Reading, MA, Perseus Books, 1997.
57. Manning N. Unbundling the state: autonomous agenciesand service delivery. Washington, DC, The World Bank, 1998(draft discussion paper).
58. Bennett S, McPake B, Mills A, eds. Private health providersin developing countries: serving the public interest? London,Zed Books, 1997.
59. Harding A, Preker AS. Conceptual frameworkfor organizational reform in the hospital sector In: Preker AS,Harding A, eds. Innovations in health service delivery:corporatization in the hospital sector. Baltimore, MD,Johns Hopkins University Press, 2000 (forthcoming).
Special Theme – Health Systems
790 Bulletin of the World Health Organization, 2000, 78 (6)