Embed Size (px)
Citation preview
Thach Nguyen MD FACC FSCAIDirector of Cardiology St Mary Medical Center
Hobart IN USA

QUAN SÁT 1
Khi chăm sóc BN NMCT cấp, chúng ta thường quantâm đến huyết áp thấp hay phân suất tống máu thấp
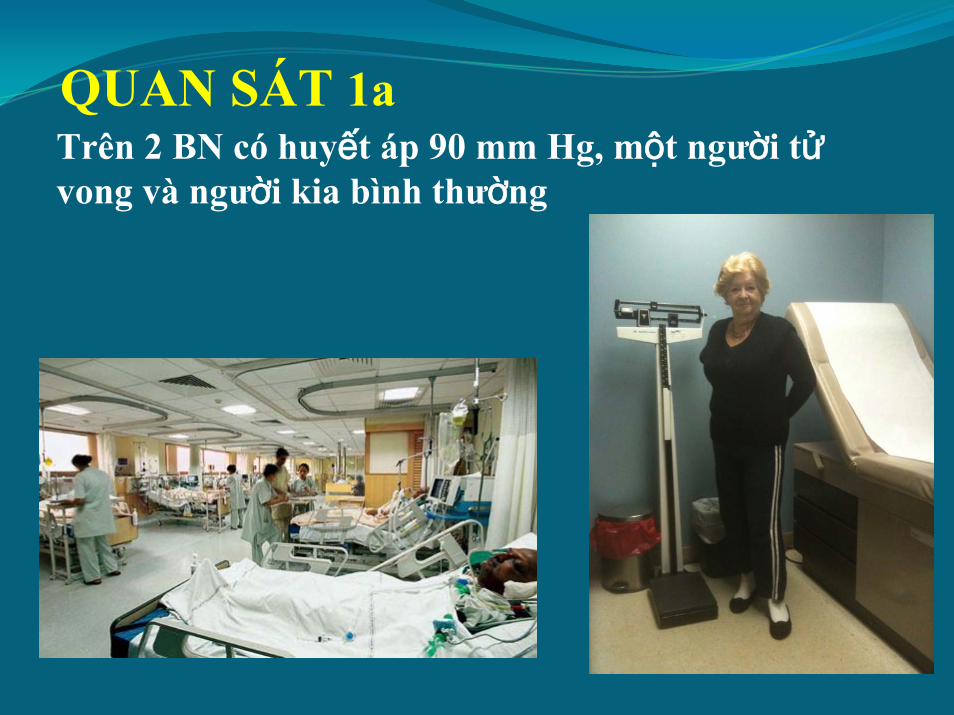
QUAN SÁT 1aTrên 2 BN có huyết áp 90 mm Hg, một người tửvong và người kia bình thường
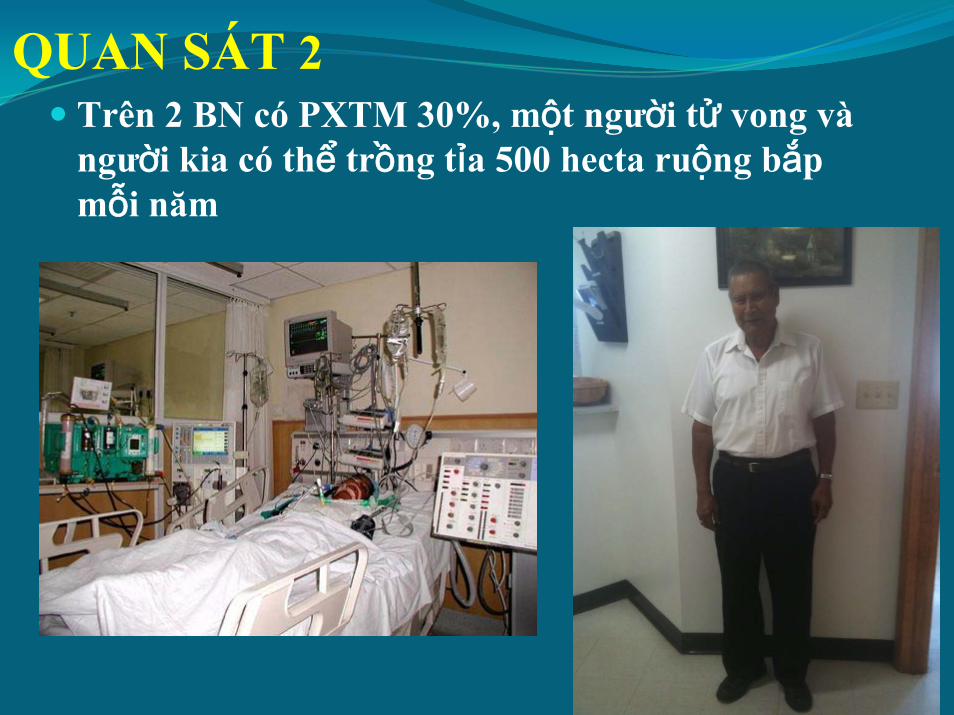
QUAN SÁT 2 Trên 2 BN có PXTM 30%, một người tử vong vàngười kia có thể trồng tỉa 500 hecta ruộng bắpmỗi năm
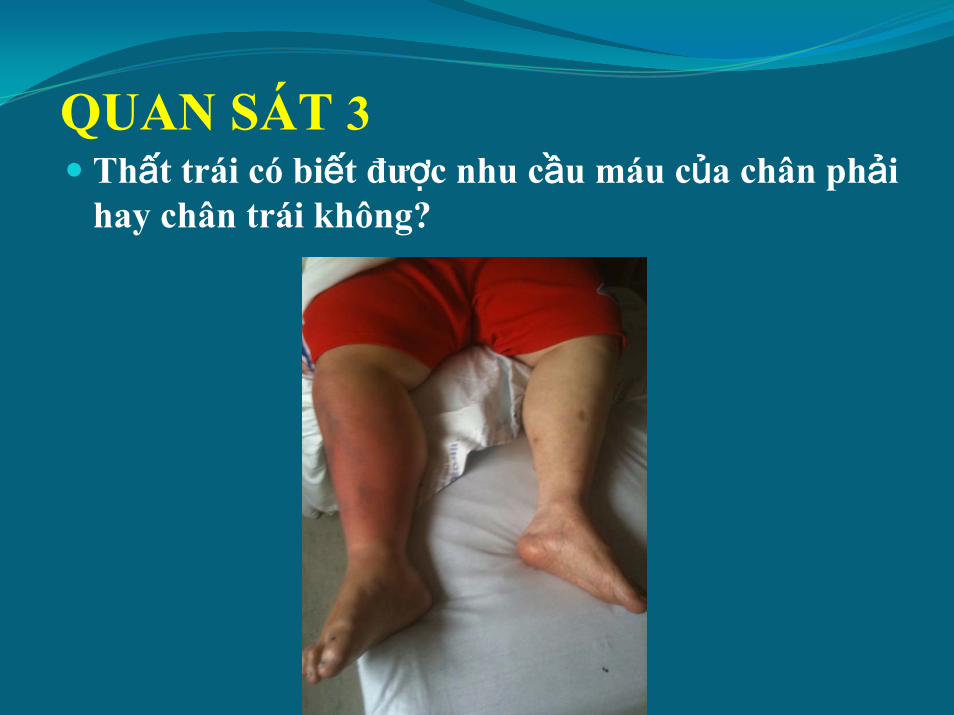
QUAN SÁT 3Thất trái có biết được nhu cầu máu của chân phảihay chân trái không?
Câu Hỏi Căn Bản
1. What is the sensing mechanism of the left ventricle?Cơ chế dẫn nhịp thất trái là gì?
2. What activates the left ventricle?Cái gì kích hoạt thất trái?
3. What is the identity of the left ventricle?(Identity id defined as whatever makes an entity definable
and recognizable)Cái gì giúp nhận dạng thất trái?
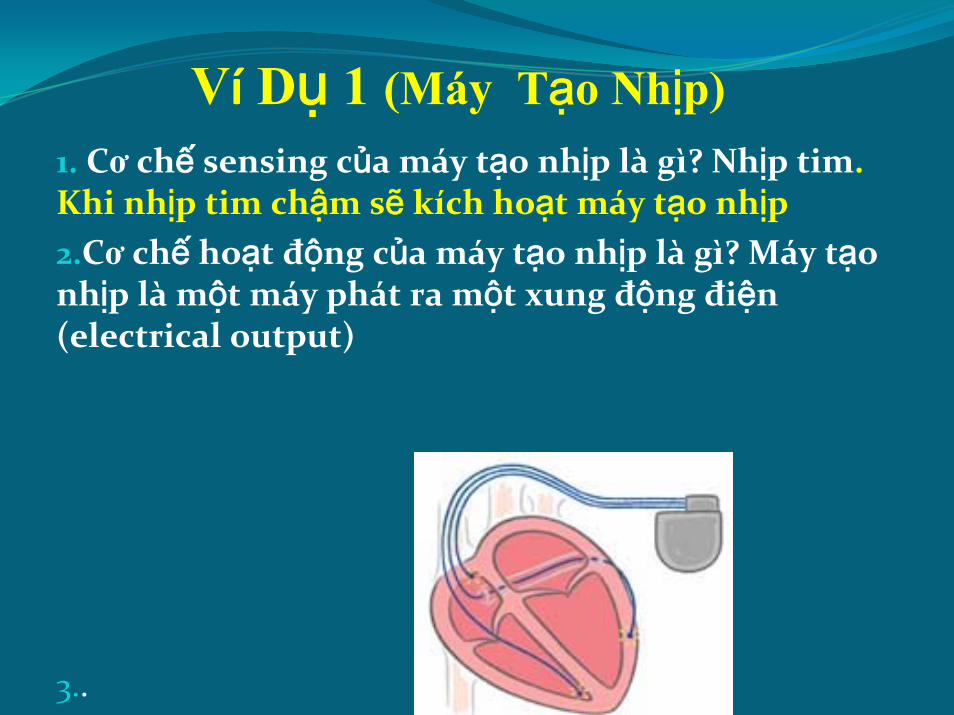
Ví Dụ 1 (Máy Tạo Nhịp)1. Cơ chế sensing của máy tạo nhịp là gì? Nhịp tim. Khi nhịp tim chậm sẽ kích hoạt máy tạo nhịp2.Cơ chế hoạt động của máy tạo nhịp là gì? Máy tạonhịp là một máy phát ra một xung động điện(electrical output)
3..
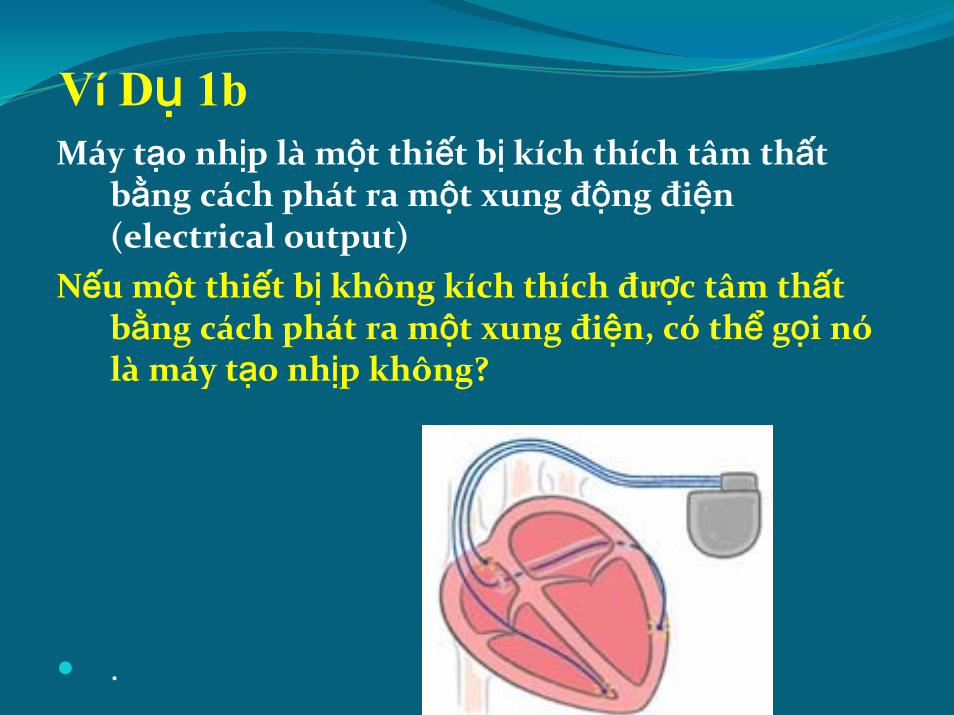
Ví Dụ 1bMáy tạo nhịp là một thiết bị kích thích tâm thất
bằng cách phát ra một xung động điện(electrical output)
Nếu một thiết bị không kích thích được tâm thấtbằng cách phát ra một xung điện, có thể gọi nólà máy tạo nhịp không?
.

Ví Dụ 2
What makes this catheter definable and recognizable and what makes it different from the others?

Ví Dụ 3What makes a cardiologist definable and recognizable and what makes him different from the other specialists

Câu Hỏi Căn Bản
1. What is the sensing mechanism of the left ventricle?Cơ chế dẫn nhịp thất trái là gì?
2. What activates the left ventricle?Cái gì kích hoạt thất trái?
3. What is the identity of the left ventricle?(Identity id defined as whatever makes an entity definable
and recognizable)Cái gì giúp nhận dạng thất trái?
Trả lời 1c
1. Cơ chế tác dụng là gì? Co bóp của thất trái đẩy rathể tích tống máu (stroke volume )
1.What is the sensing mechanism of the left ventricle?
Cái gì là cơ chế cảm biến của thất trái?
The aortic diastolic pressure (Áp lực tâm trươngtrong ĐM chủ)
Trả lời 1d
What is the identity of the left ventricle? It is a pump which provide a stroke volume to the aortic root
Định dạng của thất trái là gì? Một cái bơm tạo nênthể tích tống máu vào gốc ĐM chủ
Trả lời 1c
1. Thất trái có biết được điều gìđang xảy ra ở các động mạchngoại biên không?
2.KHÔNG
3.Now we look at the VERY SIMPLE mechanism of action of the left ventricle
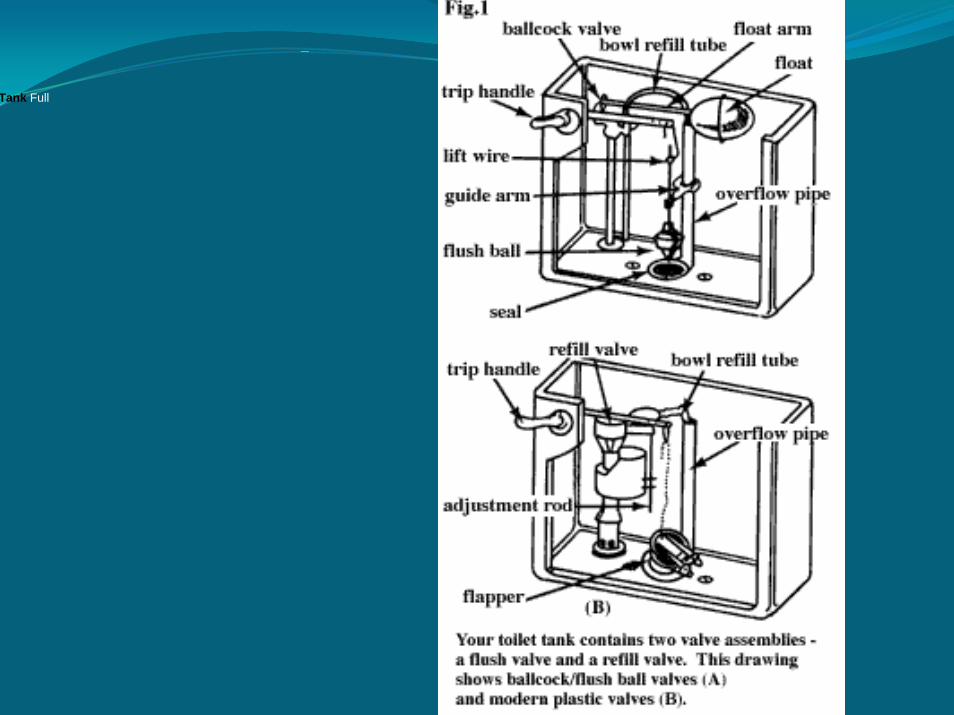
Water Tank
Tank Full
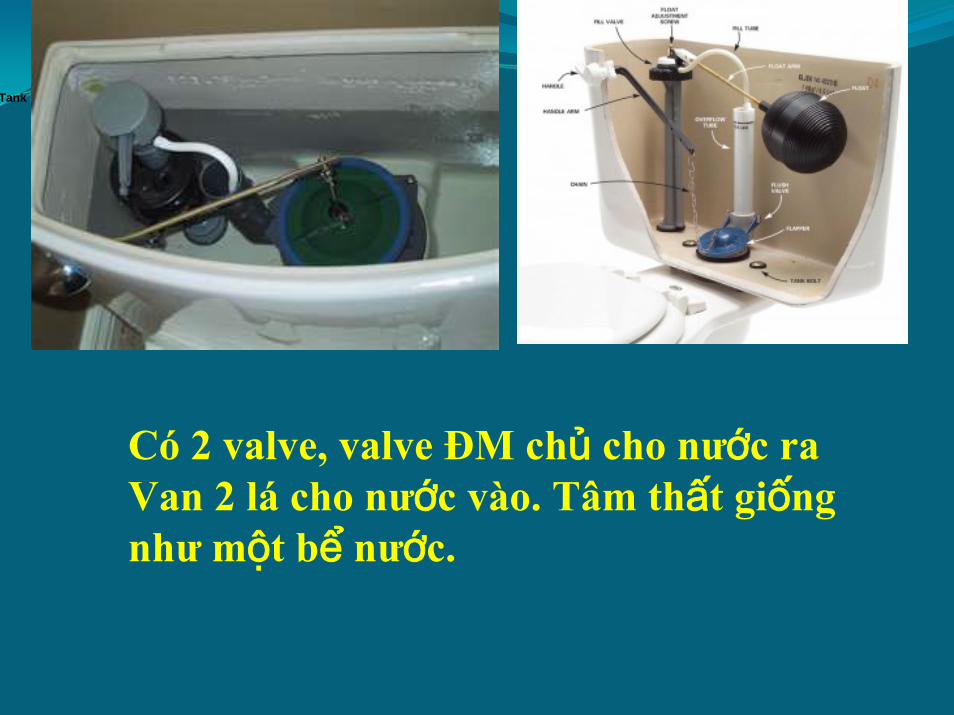
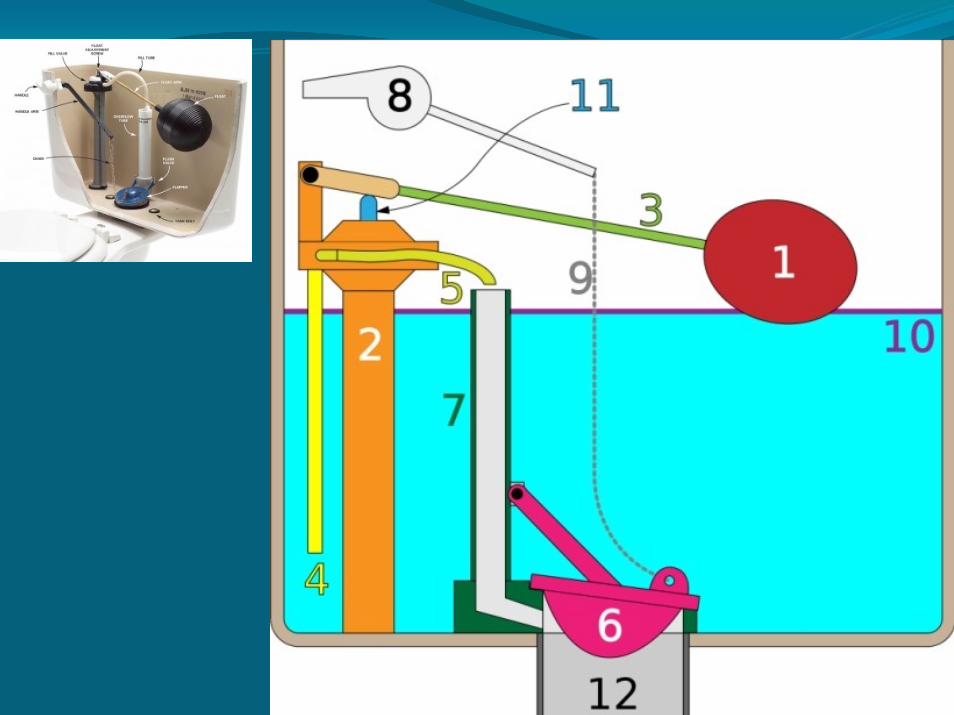
Có 2 valve, valve ĐM chủ cho nước raVan 2 lá cho nước vào. Tâm thất giốngnhư một bể nước.
Tank Full
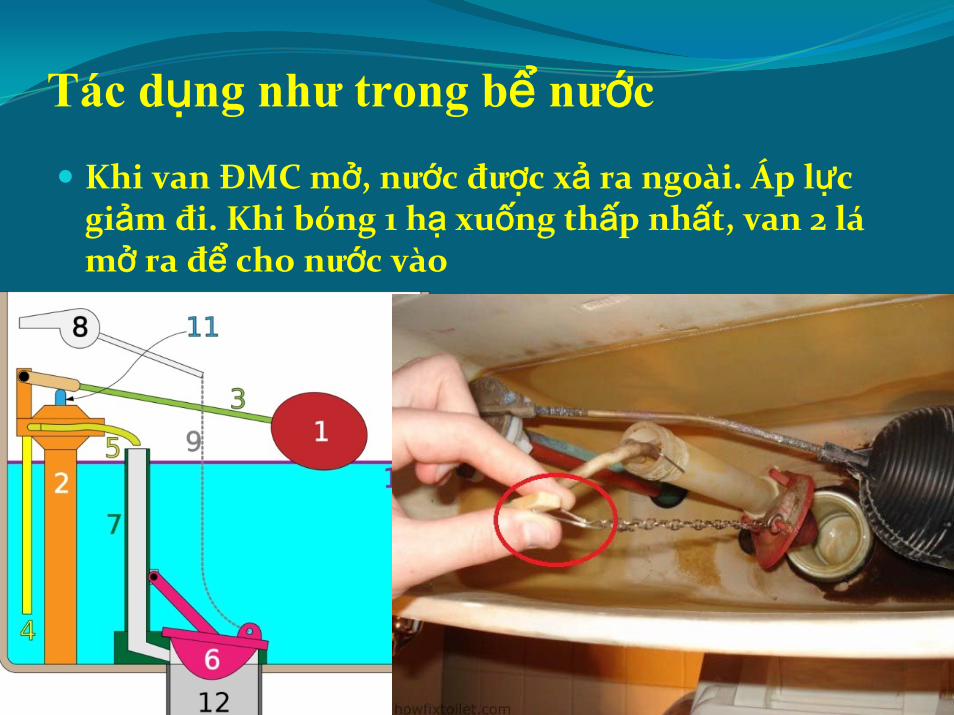
Tác dụng như trong bể nước
Khi van ĐMC mở, nước được xả ra ngoài. Áp lựcgiảm đi. Khi bóng 1 hạ xuống thấp nhất, van 2 lámở ra để cho nước vào

Tác dụng như trong bể nước
Khi muc nước xuống lam bóng 1 hạ xuống thấpnhất, van ĐMC đong lai và van 2 lá mở ra để chonước vào

How to make this process a permanent one?

What do these 3 people have in common? s ALL they fix valve: AVR, TAVI, change the valve in the toilet tank

Independent LV

QUAN SÁT 4Thất trái có cần não chỉ huy để hoạt động không? KHÔNG .Quả tim có thể đập một cách riêng rẽnhu trong cardiac transpant
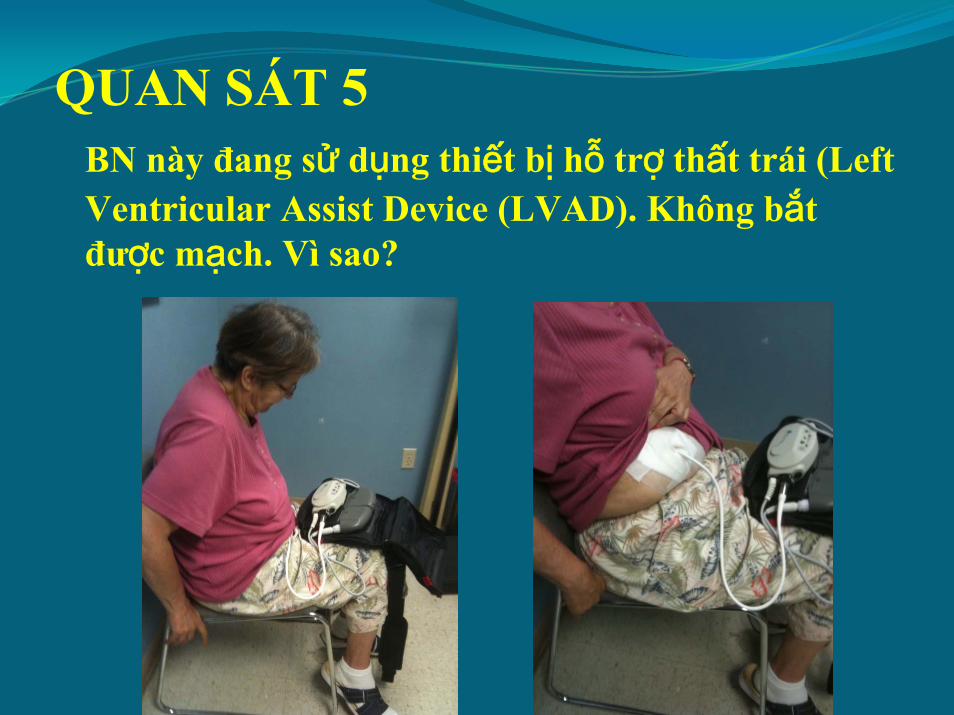
QUAN SÁT 5BN này đang sử dụng thiết bị hỗ trợ thất trái (Left Ventricular Assist Device (LVAD). Không bắtđược mạch. Vì sao?
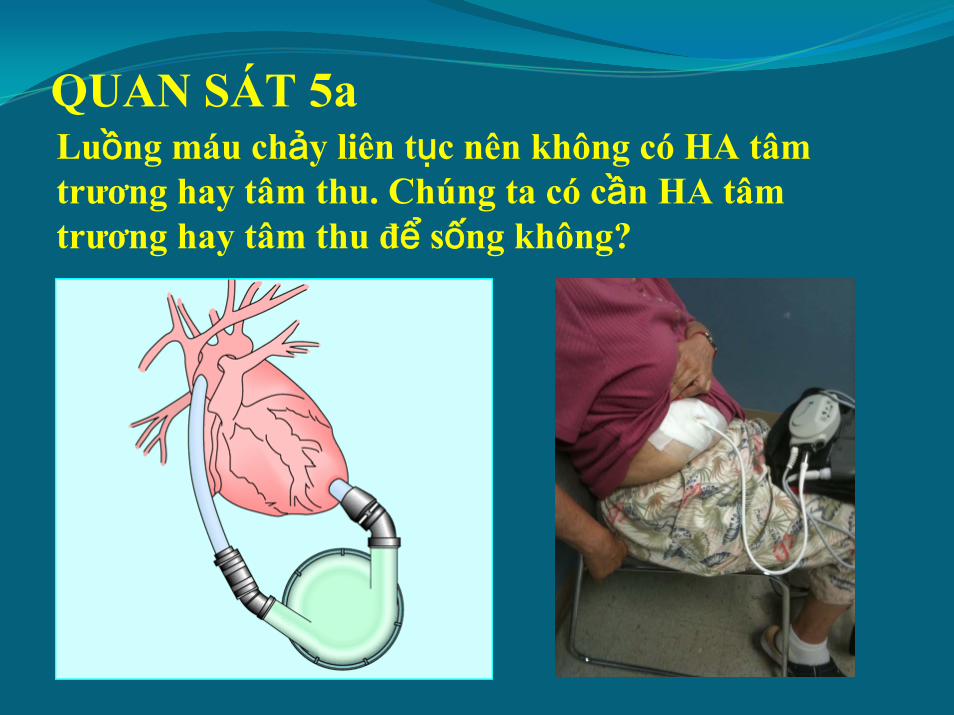
QUAN SÁT 5aLuồng máu chảy liên tục nên không có HA tâmtrương hay tâm thu. Chúng ta có cần HA tâmtrương hay tâm thu để sống không?
Irrigation System
GIẢ THIẾT
Nếu phải thiết kếmột hệ thống cấp nước cho mộtngôi làng nhỏ, trạm bơm trung tâm có cần biếttừng phút chính xác lượng nước sử dụng trong mỗibơm nhánh hay không?
Không cần thiết
Người kỹ sư chỉ cần biết số lượng nước cần bơmtrung bình mỗi ngày, với hai mức tối đa và tối thiểu
.


Áp Dụng Trong Tim Mach Học Lâm Sàng
Hệ tim mạch có thể xem nhưmột chuỗi trạmbơm. Thất trái là trạm bơm chính. Thất phải làtrạm bơm cấp nước.

Conclusion 1
Applying that principle of local control to the functioning of the heart, the role of the left ventricle is to fill up in each contraction the void in the aortic root by a stroke volume.
Trên 2 BN có PXTM 30%, một người tử vong vàngười kia có thể trồng tỉa 500 hecta ruộng bắpmỗi năm. It is not the EF. It is the stroke volume that keeps the patient alive and active

Trên BN hở van ĐMC mãn tính, HA tâmtrương thấp nên thờigian và lượng máubơm vào gốc ĐMC nhiều hơn, nên thểtích tống máu cũnglớn hơn
Conclusion 2
The aorta and peripheral arteries decide how much blood they can receive from the left ventricle. The stroke volume cannot be higher than the run-off volume from the aorta and peripheral arteries
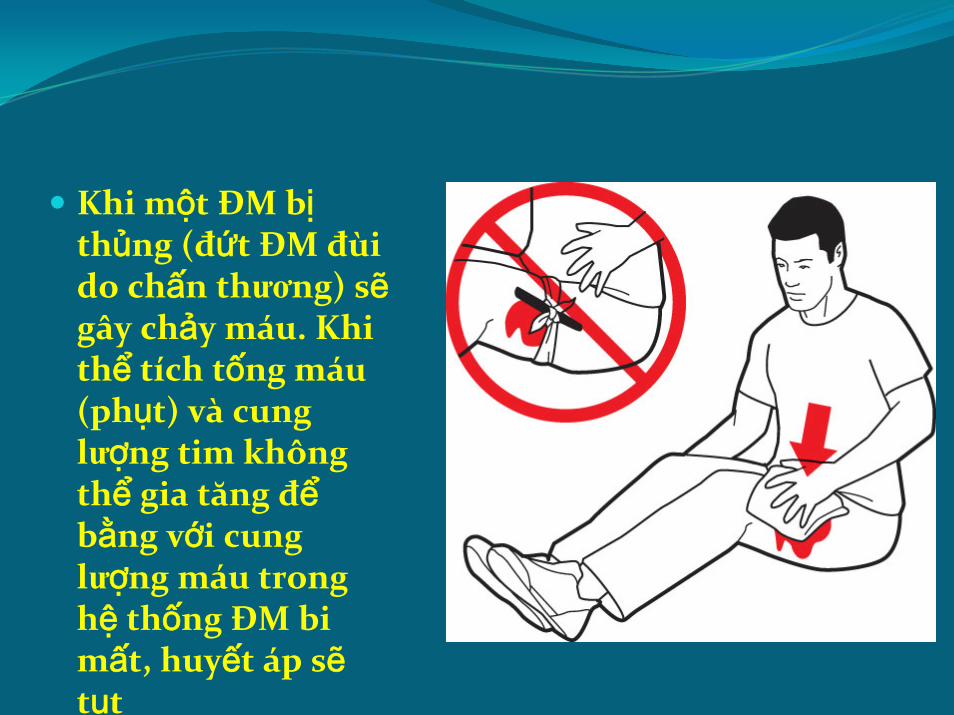
Khi một ĐM bịthủng (đứt ĐM đùido chấn thương) sẽgây chảy máu. Khithể tích tống máu(phụt) và cunglượng tim khôngthể gia tăng đểbằng với cunglượng máu tronghệ thống ĐM bi mất, huyết áp sẽtụt
3rd V
Conclusion 3
The aorta and the peripheral arterial system are and behave as a THIRD VENTRICLE. The function, action is the same as the left ventricle. The only difference is its shape
Conclusion 4
When there is low blood pressure, the stroke volume from the LV is inadequate to fill up the demand from the aorta. The output of the aorta is higher than the stroke volume
Low blood pressure is a form of heart failure
Conclusion 5
Syncope is caused by low blood pressure so syncope is a form of heart failure (or the inability of the LV to raise the stroke volume in response of the need of the aorta)
BB
Conclusion 6:
Beneficial effect
Tác dụng của chẹn beta: làm chậm nhịp tim và co mạchngoại biên. Nhịp tim chậm làm tâm trương kéo dài, máu ở lâu hơn trong mao mạch, cung cấp nhiều oxy vàdưỡng chất hơn
IWMI vs AWMI
Conclusion 7
Why is the mortality of patient with IWMI lower than the patient with AWMI?
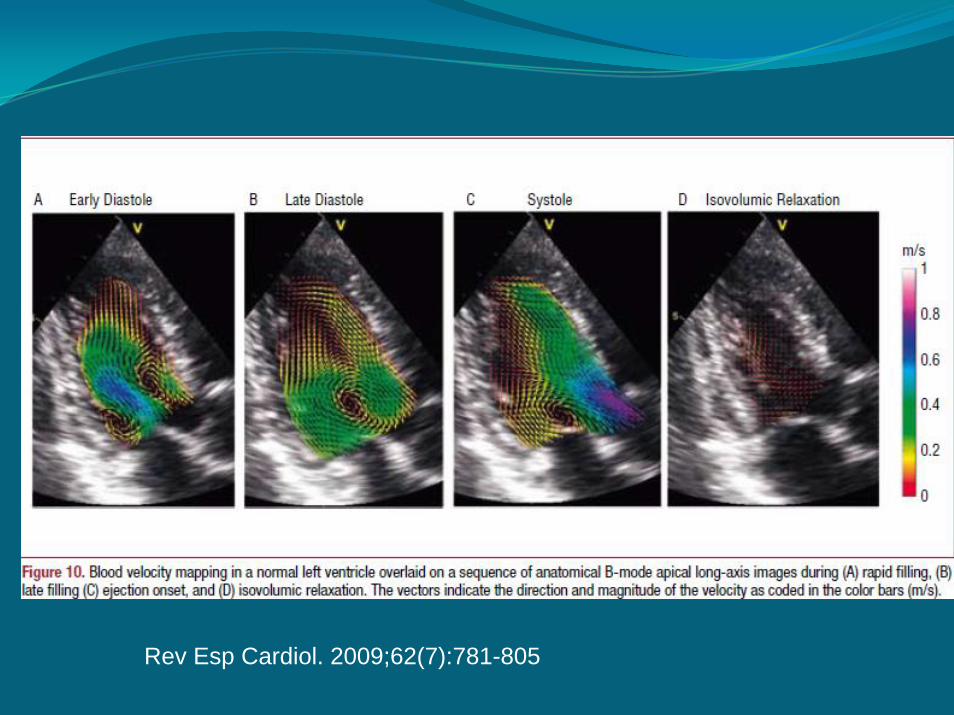
Rev Esp Cardiol. 2009;62(7):781-805

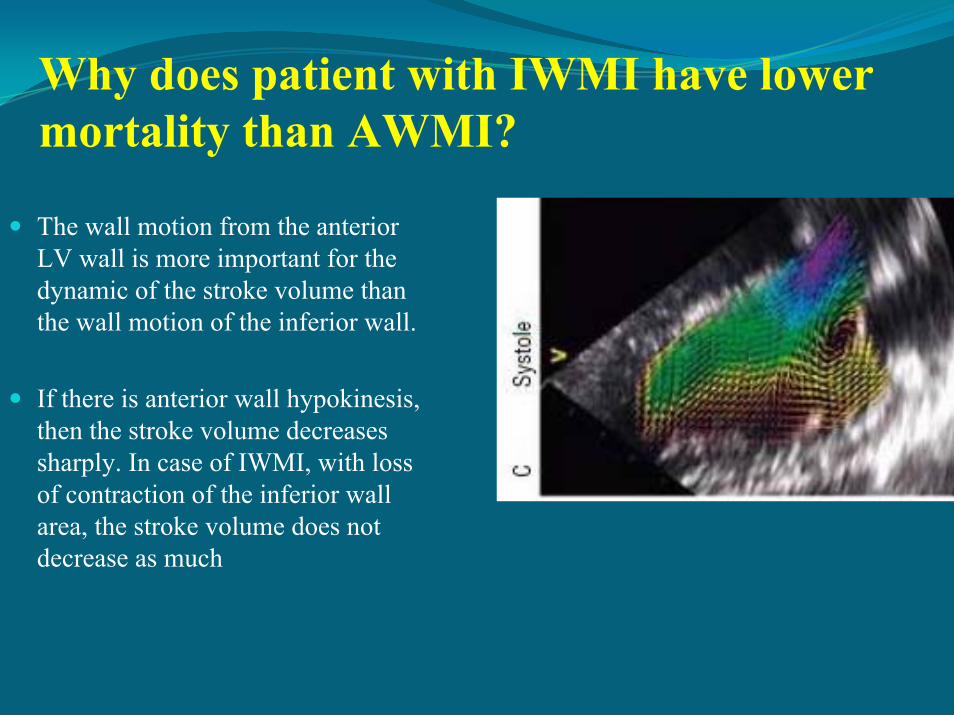
Why does patient with IWMI have lower mortality than AWMI?
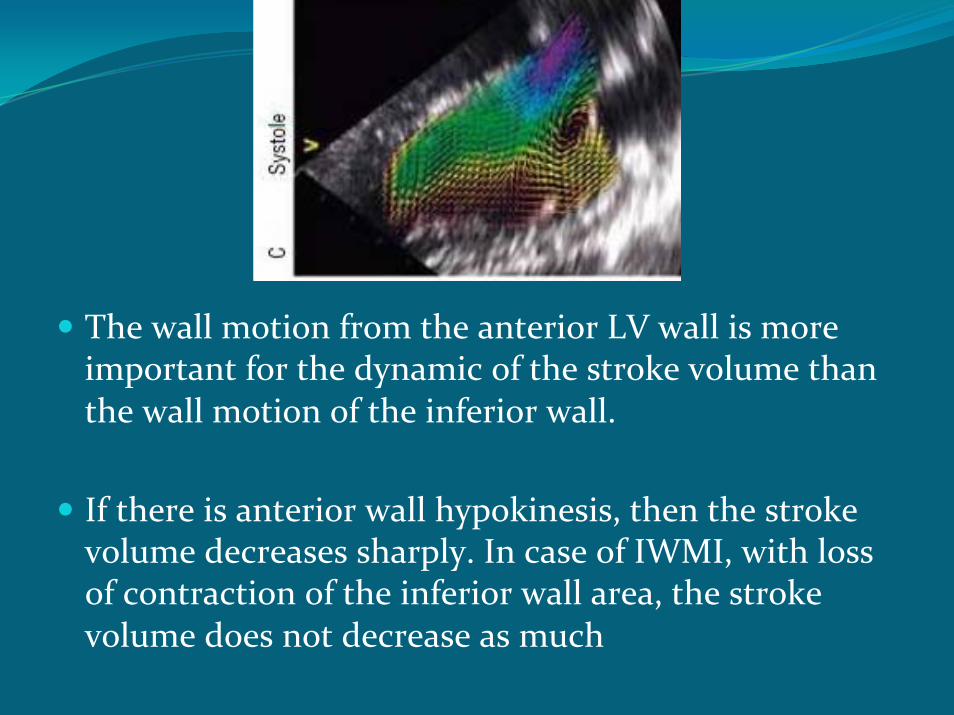
The wall motion from the anterior LV wall is more important for the dynamic of the stroke volume than the wall motion of the inferior wall.
If there is anterior wall hypokinesis, then the stroke volume decreases sharply. In case of IWMI, with loss of contraction of the inferior wall area, the stroke volume does not decrease as much
The wall motion from the anterior LV wall is more important for the dynamic of the stroke volume than the wall motion of the inferior wall.
If there is anterior wall hypokinesis, then the stroke volume decreases sharply. In case of IWMI, with loss of contraction of the inferior wall area, the stroke volume does not decrease as much
MR
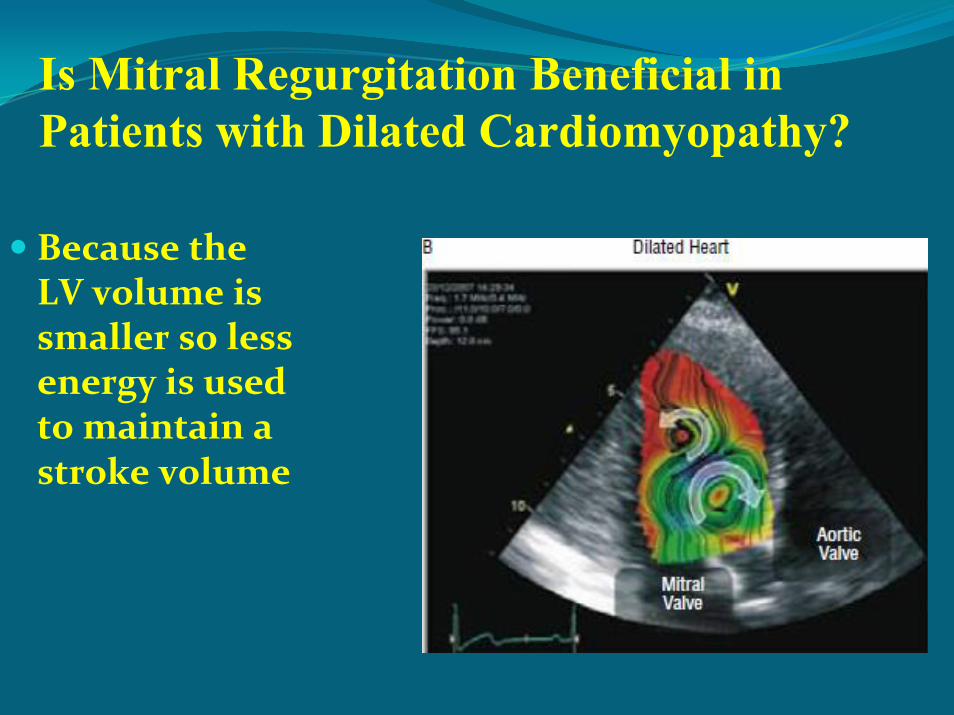
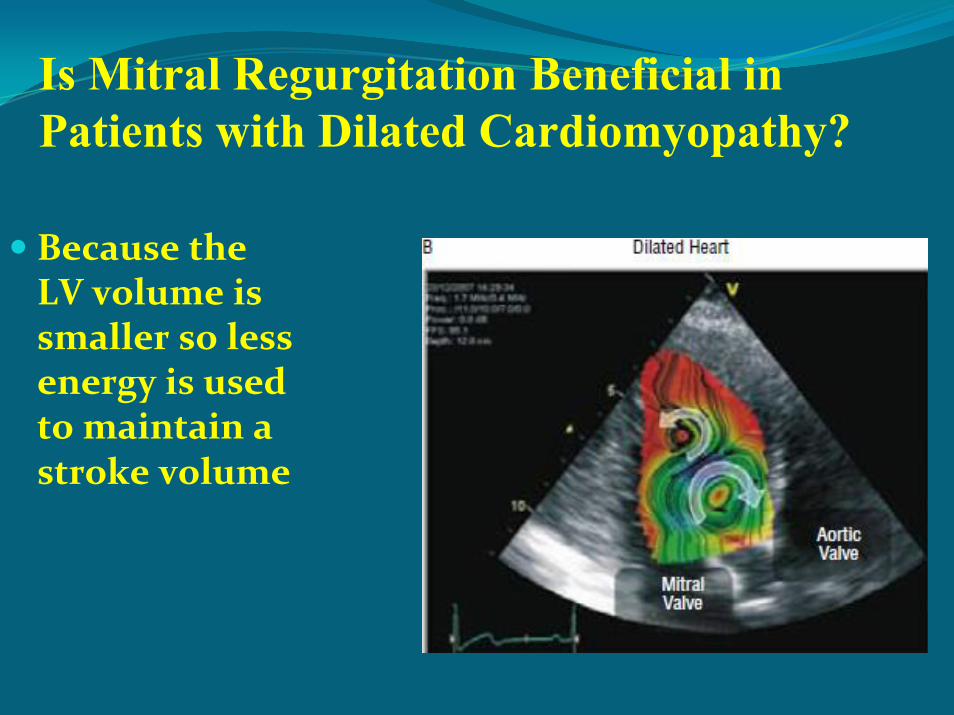
Is Mitral Regurgitation Beneficial in Patients with Dilated Cardiomyopathy?
Because the LV volume is smaller so less energy is used to maintain a stroke volume
Application The wall motion from the anterior LV wall is more important for the dynamic of the cardiac output of the inferior wall. If there is anterior wall hypokinesis, then the stroke volume decreases sharply. In case of IWMI, with loss of contraction of the inferior wall area, the stroke volume does not decrease as much
New Questions
New Question 1
Is positive remodeling good or bad for patient with AMI?
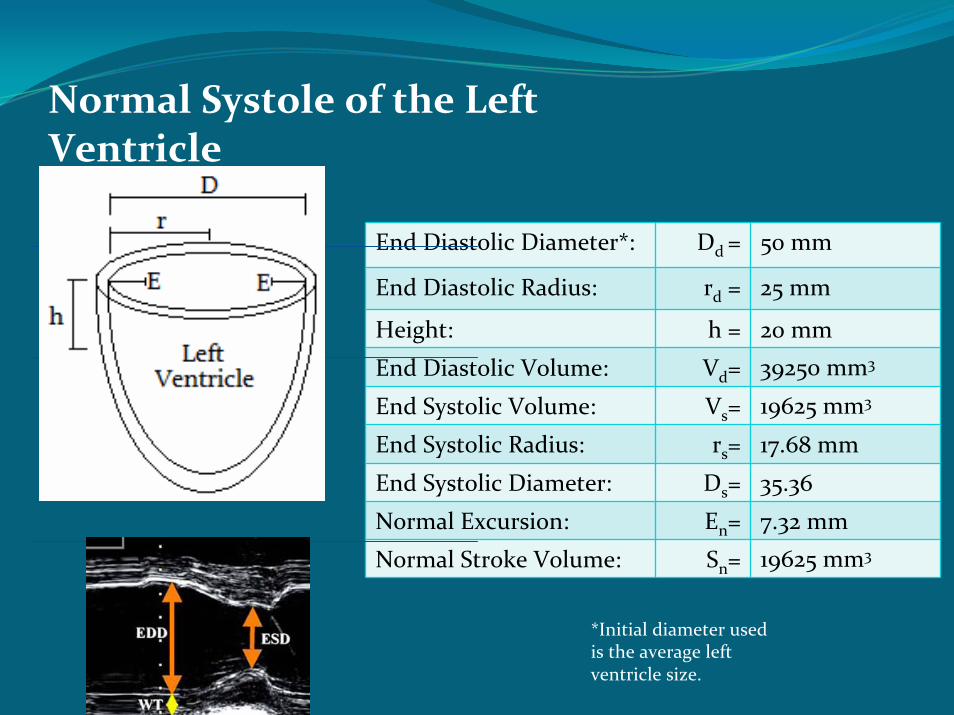
Normal Systole of the Left Ventricle
End Diastolic Diameter*: Dd = 50 mm
End Diastolic Radius: rd = 25 mm
Height: h = 20 mm
End Diastolic Volume: Vd= 39250 mm3
End Systolic Volume: Vs= 19625 mm3
End Systolic Radius: rs= 17.68 mm
End Systolic Diameter: Ds= 35.36
Normal Excursion: En= 7.32 mm
Normal Stroke Volume: Sn= 19625 mm3
*Initial diameter used is the average left ventricle size.

Normal Systole of the Left Ventricle
Diastolic Volume (Vd) calculated using:Vd = h π ri2Vd = 20mm (3.14) (25mm)2Vd = 39250 mm3
Systolic Volume (Vs) calculated using:Vs = h π rs2 = ½Vi @ 50% =Ejection Fraction Vs = 19625 mm3
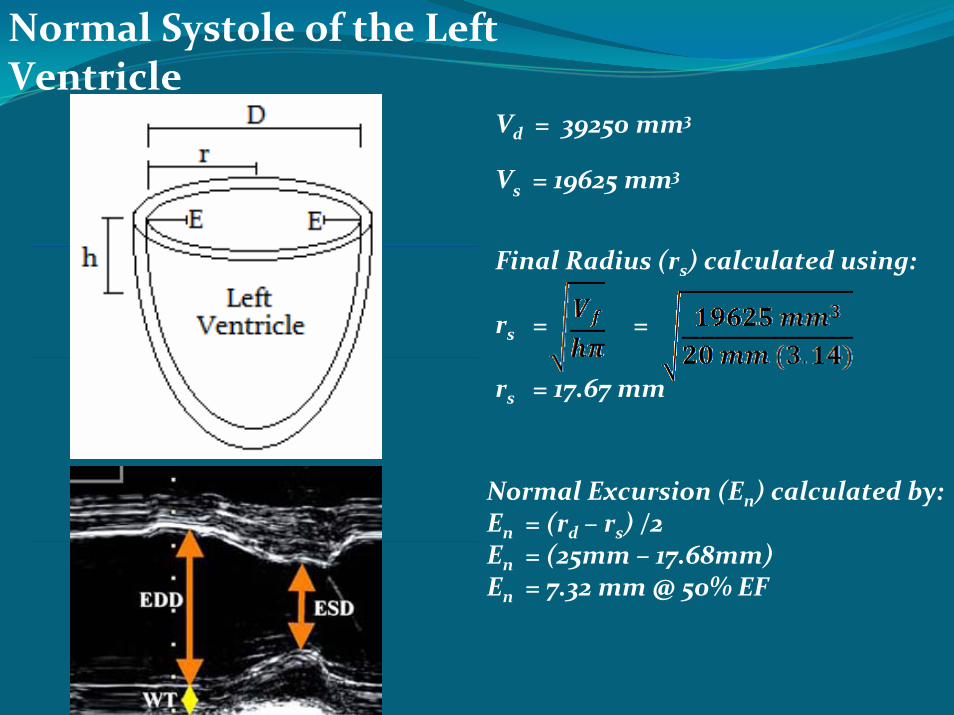
Normal Systole of the Left Ventricle
Vs = 19625 mm3
Final Radius (rs) calculated using:
rs = =
rs = 17.67 mm
Vd = 39250 mm3
Normal Excursion (En) calculated by:En = (rd – rs) /2En = (25mm – 17.68mm)En = 7.32 mm @ 50% EF
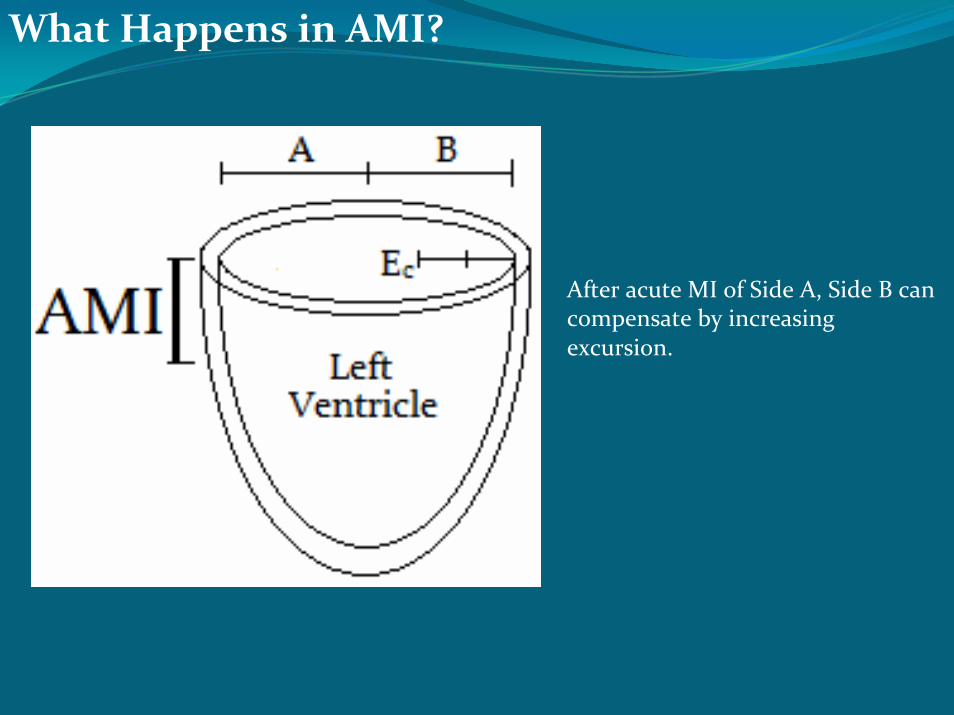
What Happens in AMI?
After acute MI of Side A, Side B can compensate by increasing excursion.
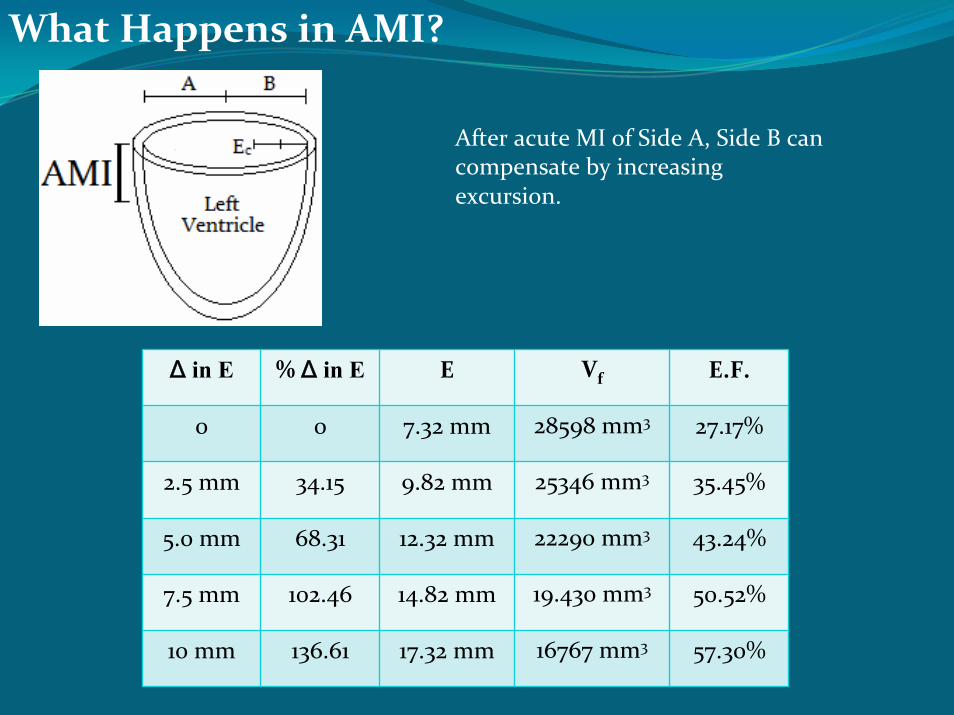
What Happens in AMI?
After acute MI of Side A, Side B can compensate by increasing excursion.
Δ in E % Δ in E E Vf E.F.
0 0 7.32 mm 28598 mm3 27.17%
2.5 mm 34.15 9.82 mm 25346 mm3 35.45%
5.0 mm 68.31 12.32 mm 22290 mm3 43.24%
7.5 mm 102.46 14.82 mm 19.430 mm3 50.52%
10 mm 136.61 17.32 mm 16767 mm3 57.30%
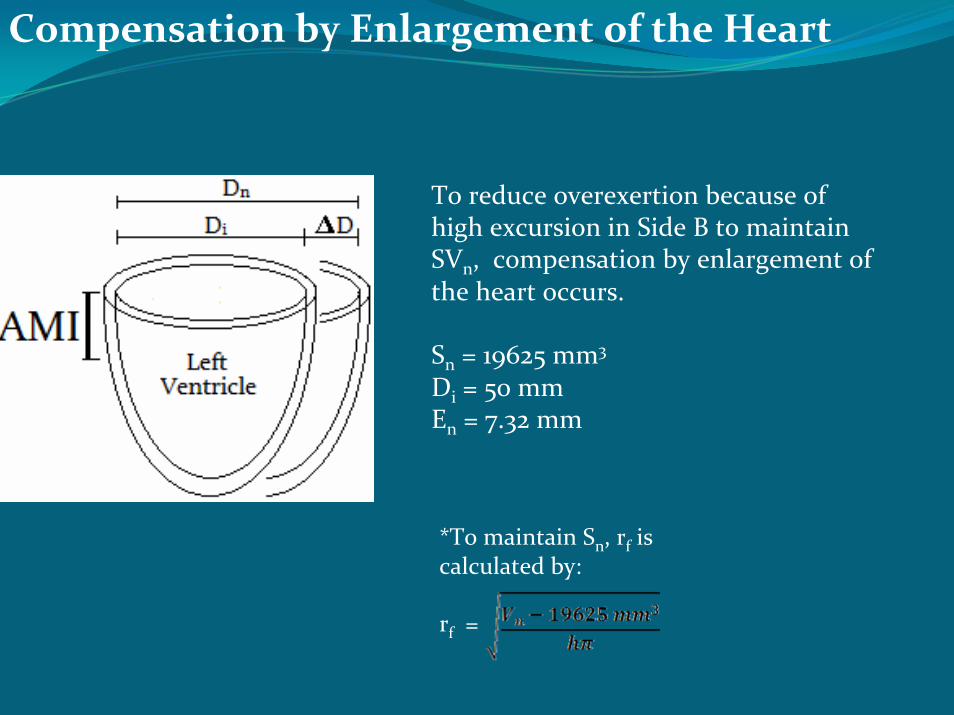
Compensation by Enlargement of the Heart
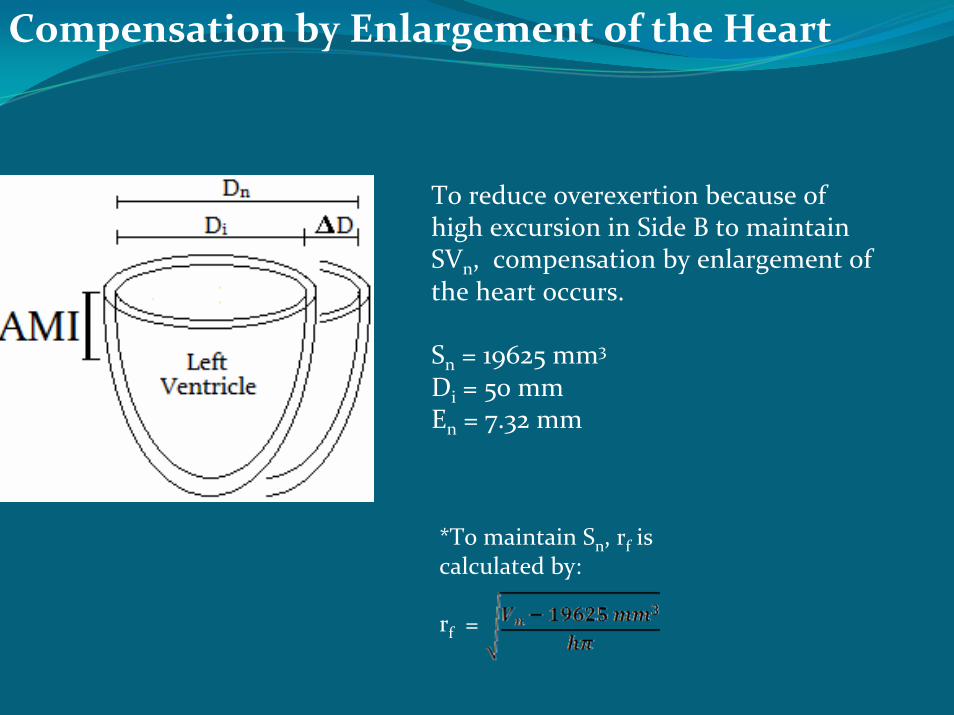
To reduce overexertion because of high excursion in Side B to maintain SVn, compensation by enlargement of the heart occurs.
Sn = 19625 mm3
Di = 50 mmEn = 7.32 mm
*To maintain Sn, rf is calculated by:
rf =
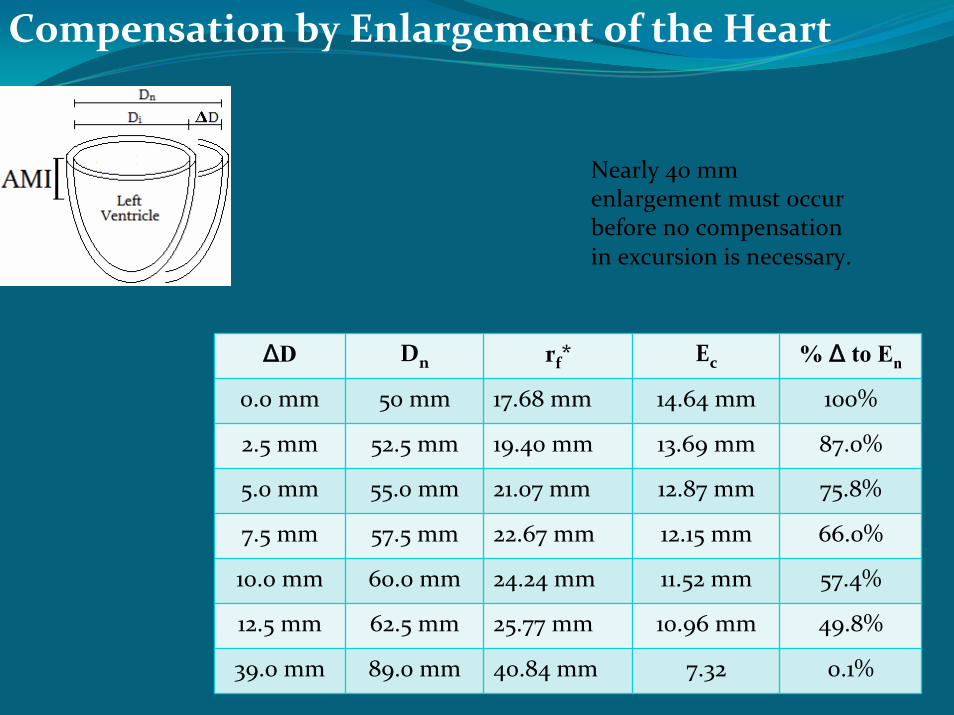
Compensation by Enlargement of the Heart
ΔD Dn rf* Ec % Δ to En
0.0 mm 50 mm 17.68 mm 14.64 mm 100%
2.5 mm 52.5 mm 19.40 mm 13.69 mm 87.0%
5.0 mm 55.0 mm 21.07 mm 12.87 mm 75.8%
7.5 mm 57.5 mm 22.67 mm 12.15 mm 66.0%
10.0 mm 60.0 mm 24.24 mm 11.52 mm 57.4%
12.5 mm 62.5 mm 25.77 mm 10.96 mm 49.8%
39.0 mm 89.0 mm 40.84 mm 7.32 0.1%
Nearly 40 mm enlargement must occur before no compensation in excursion is necessary.
Is positive remodeling good for patient with AMI?


QUAN SÁT 1
Khi chăm sóc BN NMCT cấp, chúng ta thường quan tâm đến huyết áp thấp hay phân suất tống máu thấp
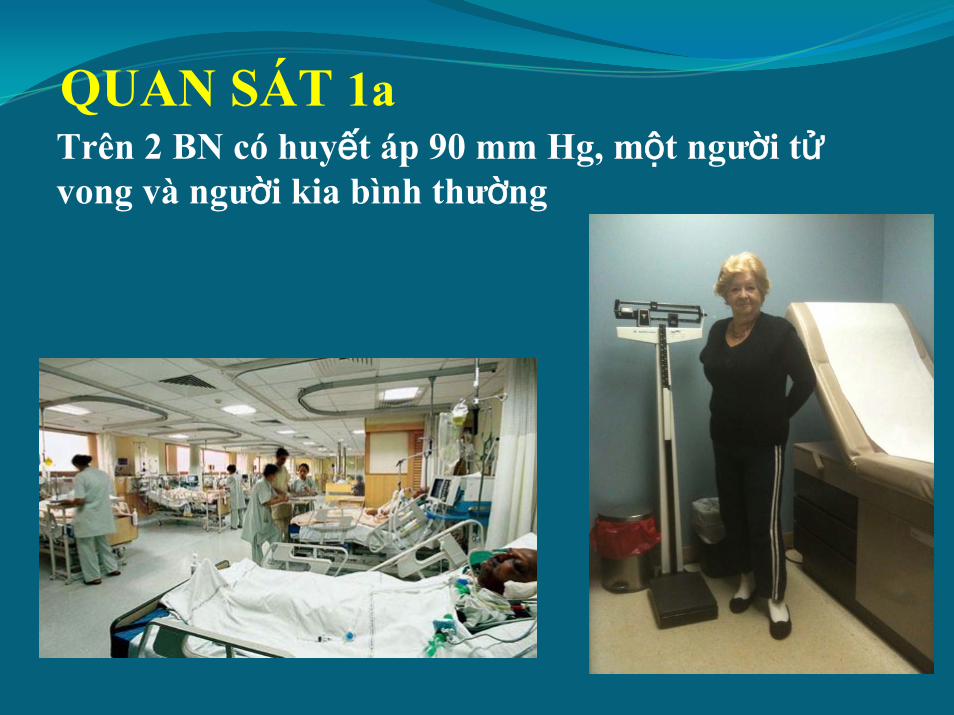
QUAN SÁT 1aTrên 2 BN có huyết áp 90 mm Hg, một người tửvong và người kia bình thường
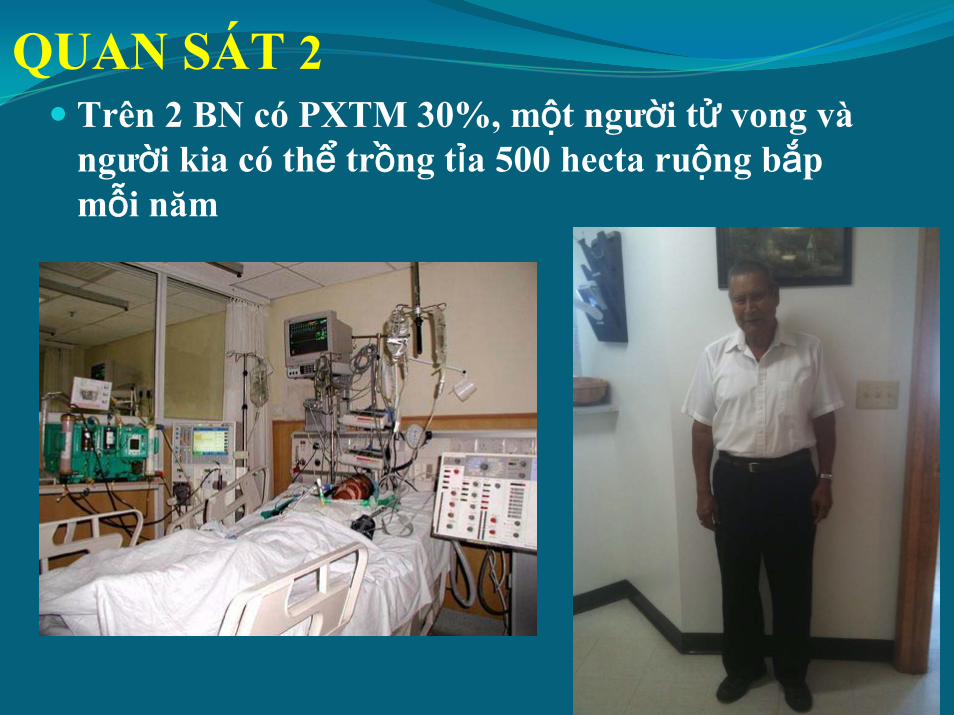
QUAN SÁT 2 Trên 2 BN có PXTM 30%, một người tử vong và người kia có thể trồng tỉa 500 hecta ruộng bắp mỗi năm
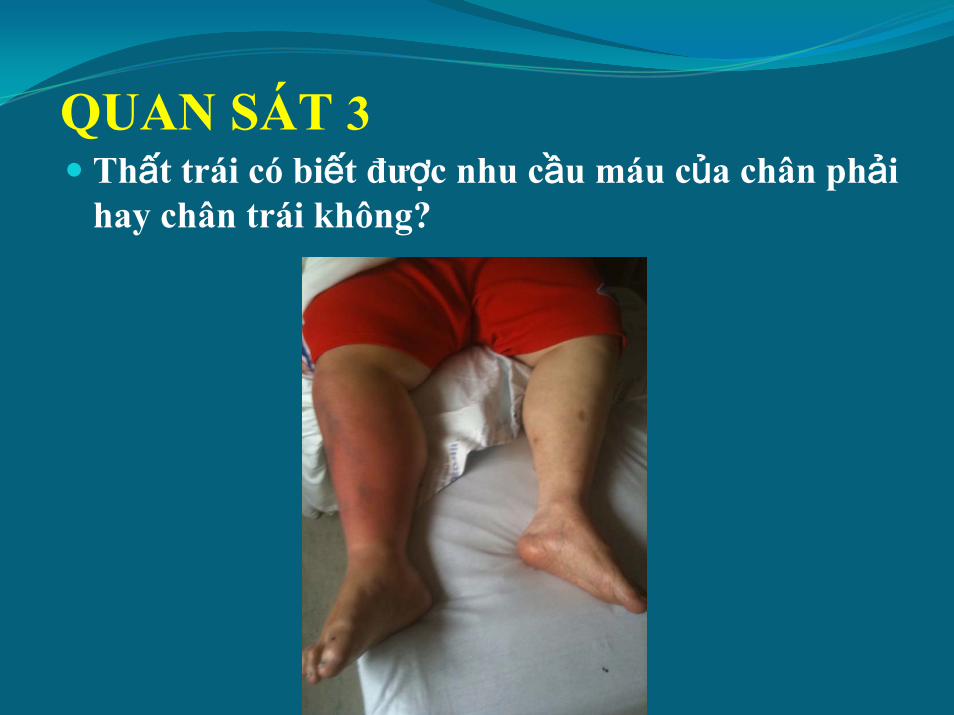
QUAN SÁT 3Thất trái có biết được nhu cầu máu của chân phải hay chân trái không?
The identity of the left ventricle:It is a pump which provide a stroke volume to the aortic root
Định dạng của thất trái là gì? Một cái bơm tạo nên thể tích tống máu vào gốc ĐM chủ
BN có PXTM 30%, một người tử vong và người kia có thể trồng tỉa 500 hecta ruộng bắp mỗi năm. It is not the EF. It is the stroke volume that keeps the patient alive and active
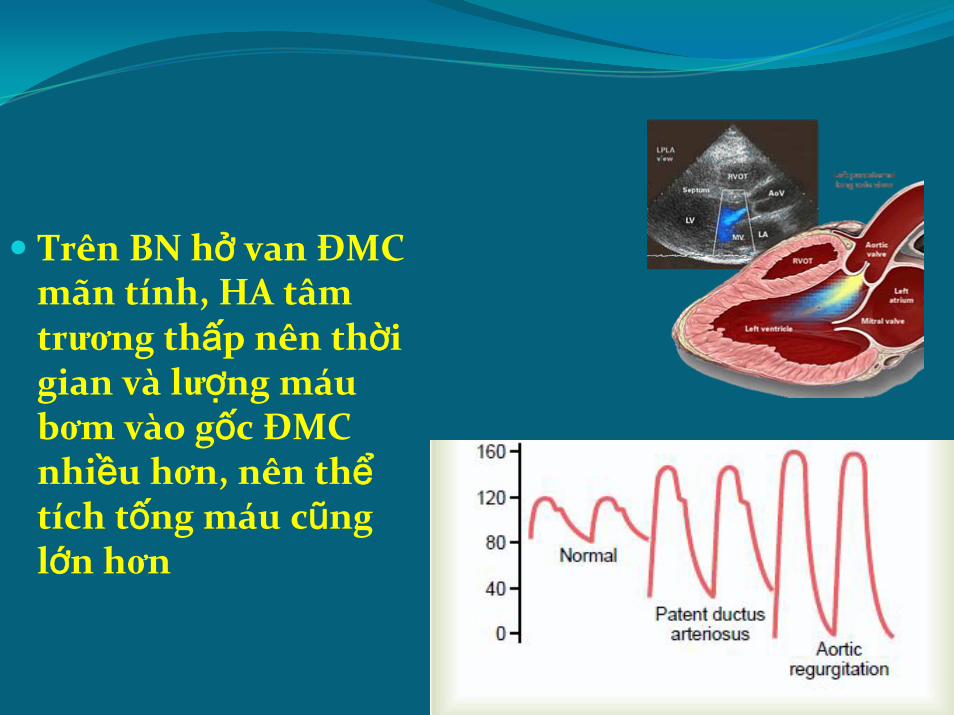
Trên BN hở van ĐMC mãn tính, HA tâm trương thấp nên thời gian và lượng máu bơm vào gốc ĐMC nhiều hơn, nên thểtích tống máu cũng lớn hơn
Why does patient with IWMI have lower mortality than AWMI?
The wall motion from the anterior LV wall is more important for the dynamic of the stroke volume than the wall motion of the inferior wall.
If there is anterior wall hypokinesis, then the stroke volume decreases sharply. In case of IWMI, with loss of contraction of the inferior wall area, the stroke volume does not decrease as much
Is Mitral Regurgitation Beneficial in Patients with Dilated Cardiomyopathy?
Because the LV volume is smaller so less energy is used to maintain a stroke volume
Compensation by Enlargement of the Heart
To reduce overexertion because of high excursion in Side B to maintain SVn, compensation by enlargement of the heart occurs.
Sn = 19625 mm3
Di = 50 mmEn = 7.32 mm
*To maintain Sn, rf is calculated by:
rf =