-
7/13/2019 MRI MSK Protocol
1/193
Protokol MRI Muskuloskeletal
Dr. Paulus Rahardjo
@2014
-
7/13/2019 MRI MSK Protocol
2/193
SHOULDER
-
7/13/2019 MRI MSK Protocol
3/193
ANATOMY
-
7/13/2019 MRI MSK Protocol
4/193
-
7/13/2019 MRI MSK Protocol
5/193
-
7/13/2019 MRI MSK Protocol
6/193
-
7/13/2019 MRI MSK Protocol
7/193
-
7/13/2019 MRI MSK Protocol
8/193
-
7/13/2019 MRI MSK Protocol
9/193
-
7/13/2019 MRI MSK Protocol
10/193
-
7/13/2019 MRI MSK Protocol
11/193
-
7/13/2019 MRI MSK Protocol
12/193
-
7/13/2019 MRI MSK Protocol
13/193
-
7/13/2019 MRI MSK Protocol
14/193
-
7/13/2019 MRI MSK Protocol
15/193
-
7/13/2019 MRI MSK Protocol
16/193
-
7/13/2019 MRI MSK Protocol
17/193
-
7/13/2019 MRI MSK Protocol
18/193
-
7/13/2019 MRI MSK Protocol
19/193
-
7/13/2019 MRI MSK Protocol
20/193
-
7/13/2019 MRI MSK Protocol
21/193
-
7/13/2019 MRI MSK Protocol
22/193
-
7/13/2019 MRI MSK Protocol
23/193
-
7/13/2019 MRI MSK Protocol
24/193
-
7/13/2019 MRI MSK Protocol
25/193
-
7/13/2019 MRI MSK Protocol
26/193
-
7/13/2019 MRI MSK Protocol
27/193
-
7/13/2019 MRI MSK Protocol
28/193
-
7/13/2019 MRI MSK Protocol
29/193
-
7/13/2019 MRI MSK Protocol
30/193
-
7/13/2019 MRI MSK Protocol
31/193
-
7/13/2019 MRI MSK Protocol
32/193
-
7/13/2019 MRI MSK Protocol
33/193
-
7/13/2019 MRI MSK Protocol
34/193
-
7/13/2019 MRI MSK Protocol
35/193
-
7/13/2019 MRI MSK Protocol
36/193
-
7/13/2019 MRI MSK Protocol
37/193
-
7/13/2019 MRI MSK Protocol
38/193
-
7/13/2019 MRI MSK Protocol
39/193
-
7/13/2019 MRI MSK Protocol
40/193
-
7/13/2019 MRI MSK Protocol
41/193
-
7/13/2019 MRI MSK Protocol
42/193
-
7/13/2019 MRI MSK Protocol
43/193
-
7/13/2019 MRI MSK Protocol
44/193
-
7/13/2019 MRI MSK Protocol
45/193
-
7/13/2019 MRI MSK Protocol
46/193
-
7/13/2019 MRI MSK Protocol
47/193
Shoulder MR Routine Protocol
Coronal obliqueFS PD FSE (tendinosis)
T2 FSE (cuff tear)
Axial
T2* (theta > TE) intrasubstance signal &
subscapularis tendon
FS PD FSE (paralabral cyst & articular cartilage)
Sagittal obliqueT2 FSE (cuff tear)
FS PD FSE (tendinosis)
P i P i
-
7/13/2019 MRI MSK Protocol
48/193
Patient Preparation
Have the patient to go to the toilet
Explain the procedure to the patient
Offer the patient ear protectors or ear plugs
Ask the patient to undress except forunderwear
Ask the patient to remove anything
containing metal (hearing aids, hair-
pins, body jewelry, necklace, etc.)
P i i i
-
7/13/2019 MRI MSK Protocol
49/193
Positioning
Supine
Shoulder coil (oval surface coil, flexible coil)
Arm in neutral rotation or supination
Cushion the legs
-
7/13/2019 MRI MSK Protocol
50/193
Ti & T i k
-
7/13/2019 MRI MSK Protocol
51/193
Tips & Tricks
Positioning: Secure coil at the side with sandbags
Place sandbags or a strap across the lower arm in
supination (if this should prove difficult it is easier
to have the lower arm in neutral rotation)
Get the shoulder to be imaged as far into the
isocenter of the magnet as possible
It may be necessary to position the patient in themagnet at an
oblique angle of 45 (place cushions
at the shoulder, buttocks, and knees)
Sh ld i l
-
7/13/2019 MRI MSK Protocol
52/193
Shoulder, axial
-
7/13/2019 MRI MSK Protocol
53/193
Sagittal oblique(orthogonal to sequence 2
or parallel to the glenoid cavity)
-
7/13/2019 MRI MSK Protocol
54/193
C l Obli ( ll l t th
-
7/13/2019 MRI MSK Protocol
55/193
Coronal Oblique (parallel to the
supraspinatus muscle on the axial)
slice) Sequence 2
-
7/13/2019 MRI MSK Protocol
56/193
ELBOW
Positioning
-
7/13/2019 MRI MSK Protocol
57/193
Positioning
Prone: arms straight above the head, palms
against the table, secureOr supine: arms straight alongside the
body
Or slight lateral decubitus: arm immobilized bythe body
Surface or wraparound coil
Tips & Tricks
If necessary, immobilize the forearm with a
sandbagTry to position the elbow to be imaged in the
isocenter of the magnet
Elbow Protocol
-
7/13/2019 MRI MSK Protocol
58/193
Elbow Protocol
Coronal T1/PD FSE (sclerosis, tendinosis) Coronal FS PD FSE
(ligament and tendon tear)
Axial T1/PD FSE
Axial FS PD FSE (biceps, ulnar nerve, collateral lig. and
tendons) Sagittal T1/PD FSE (triceps, olecranon bursa)
Sagittal FS PD FSE (triceps, capitellar chondral surface)
Hints
TR = 3000 msec and FS PD FSE - TE 40-50 msec
10 cm FOV
Axial plane extend to radial tuberosity
T2* GRE used if poor fat suppression
-
7/13/2019 MRI MSK Protocol
59/193
Coronal
-
7/13/2019 MRI MSK Protocol
60/193
Axial
-
7/13/2019 MRI MSK Protocol
61/193
Sagittal
-
7/13/2019 MRI MSK Protocol
62/193
WRIST
Positioning
-
7/13/2019 MRI MSK Protocol
63/193
Positioning
Prone: arm extended above the head, palm
flat on the table, secure,
surface coil
Or supine: arm extended alongside the body
Tips & Tricks
If necessary immobilize forearm with sandbag
Wrist MR Routine Protocol
-
7/13/2019 MRI MSK Protocol
64/193
Wrist - MR Routine Protocol
CoronalT1 or PD FSE
FS PD FSE
AxialT1 or PD FSE
FS PD FSE
STIR or T2* for heterogenoufat suppresion
SagittalFS PD FSE
-
7/13/2019 MRI MSK Protocol
65/193
Coronal
-
7/13/2019 MRI MSK Protocol
66/193
Axial
-
7/13/2019 MRI MSK Protocol
67/193
Sagittal
-
7/13/2019 MRI MSK Protocol
68/193
HIP
Hip Protocol
-
7/13/2019 MRI MSK Protocol
69/193
Hip Protocol
Coronal T1/PD FSE (acetabular sclerosis)
Coronal FS PD FSE (subchondral edema, labral tears and
cysts)
Coronal FS PD FSE with cardiac coil
(femoroacetabularimpingement)
Axial FS PD FSE (labrum, iliopsoas bursa, muscle)
Sagittal FS PD FSE (anterior labral tears and femoral head
morphology) HintsHints
TR = 3000 msec and FS PD FSE - TE 40-50 msec
Coronal use cardiac coil with FOV = 16 cm
IV vs. intraarticular contrast for femoroacetabular impingement
-
optional Radial imaging for labrumoptional
Use anterior-most coronal images to diagnose acetabular
dysplasia
Positioning
-
7/13/2019 MRI MSK Protocol
70/193
PositioningSupine
Body array coil (body coil, wraparound coil)
Cushion the legs with a small roll under the knees (do
notelevate the
thighs too much)
Have the patient cross the arms over the upper abdomen
Tips & Tricks
Positioning aid:
Center on anterior inferior iliac spine
If the coronal images show vascular artifacts due to the
iliacvessels, switching the phase encoding gradient to HF mayhelp
(with oversampling in order to avoid foldover)
Coronal across the femoral heads
-
7/13/2019 MRI MSK Protocol
71/193
(allow for an oblique presentation of
the pelvis)
Axial across the femoral heads and
-
7/13/2019 MRI MSK Protocol
72/193
Axial across the femoral heads and
acetabula (caudad to the lower aspect of
the greater trochanter)
Sagittal across both femoral heads
-
7/13/2019 MRI MSK Protocol
73/193
Sagittal across both femoral heads
-
7/13/2019 MRI MSK Protocol
74/193
KNEE
-
7/13/2019 MRI MSK Protocol
75/193
Knee Protocol Axial T1/PD FSE (sclerosis)
Axial FS PD FSE (patellofemoral cartilage)
Sagittal FS PD FSE (meniscal morph., cruciates, articular
cartilage)
Sagittal T2* GRE (meniscal deg., patellar
tendon,chondrocalcinosis)
Coronal T1/PD FSE (sclerosis, condylar erosions)
Coronal FS PD FSE (collateral ligaments, meniscal root (g
attachments)
Hints
TR = 3000 msec and FS PD FSE - TE 40-50 msec
FOV 12-14 cm Do not externally rotate knee
Use sagittal plane to diagnose trochlear groove lesions
Evaluate meniscal root attachments on posterior-most
coronalslices
Positioning
-
7/13/2019 MRI MSK Protocol
76/193
Positioning
Supine, feet first
Knee coil (wrap around)Place knee into the coil (check that it
really is
the one due for investigation)
1015 external rotation gives better imagingof the anterior
cruciate ligament
Center the joint in the coil and secure the
knee in the coilCushion other leg
-
7/13/2019 MRI MSK Protocol
77/193
-
7/13/2019 MRI MSK Protocol
78/193
Patellar
cartilage
-
7/13/2019 MRI MSK Protocol
79/193
Patellar
cartilage
-
7/13/2019 MRI MSK Protocol
80/193
Trochlear
cartilage
Patellar
cartilage
-
7/13/2019 MRI MSK Protocol
81/193
-
7/13/2019 MRI MSK Protocol
82/193
S i l d A i l Sli
-
7/13/2019 MRI MSK Protocol
83/193
Sagittal and Axial Slices
-
7/13/2019 MRI MSK Protocol
84/193
-
7/13/2019 MRI MSK Protocol
85/193
LAT
Meniscus
-
7/13/2019 MRI MSK Protocol
86/193
LAT
Meniscus
-
7/13/2019 MRI MSK Protocol
87/193
LAT
Meniscus
-
7/13/2019 MRI MSK Protocol
88/193
LAT
Meniscus
-
7/13/2019 MRI MSK Protocol
89/193
ACL PCL
-
7/13/2019 MRI MSK Protocol
90/193
ACL PCL
-
7/13/2019 MRI MSK Protocol
91/193
ACL PCL
-
7/13/2019 MRI MSK Protocol
92/193
PCL
-
7/13/2019 MRI MSK Protocol
93/193
MED
Meniscus
-
7/13/2019 MRI MSK Protocol
94/193
MED
Meniscus
-
7/13/2019 MRI MSK Protocol
95/193
MED
Meniscus
-
7/13/2019 MRI MSK Protocol
96/193
MED
Meniscus
-
7/13/2019 MRI MSK Protocol
97/193
-
7/13/2019 MRI MSK Protocol
98/193
-
7/13/2019 MRI MSK Protocol
99/193
-
7/13/2019 MRI MSK Protocol
100/193
CORONAL SLICES
-
7/13/2019 MRI MSK Protocol
101/193
(parallel to the condyles)
-
7/13/2019 MRI MSK Protocol
102/193
-
7/13/2019 MRI MSK Protocol
103/193
MED
Meniscus
-
7/13/2019 MRI MSK Protocol
104/193
MED
Meniscus
-
7/13/2019 MRI MSK Protocol
105/193
ACL PCL
-
7/13/2019 MRI MSK Protocol
106/193
MCL
PCL
-
7/13/2019 MRI MSK Protocol
107/193
MCL
PCL
-
7/13/2019 MRI MSK Protocol
108/193
LCL
PCL
-
7/13/2019 MRI MSK Protocol
109/193
PCL
-
7/13/2019 MRI MSK Protocol
110/193
Sagittal and Axial Slices
-
7/13/2019 MRI MSK Protocol
111/193
Sagittal and Axial Slices
Coronal (parallel to the condyles)
-
7/13/2019 MRI MSK Protocol
112/193
Coronal (parallel to the condyles)
Sagittal
-
7/13/2019 MRI MSK Protocol
113/193
Sagittal
Axial
-
7/13/2019 MRI MSK Protocol
114/193
Axial
Tips & Tricks
-
7/13/2019 MRI MSK Protocol
115/193
Cushion the knee well (sandbags, wedges)
To avoid repeatedly having to set up two scout sequences (in the
off-
center position), have a right and left sagittal scout set up
for the knee
in the standard scout program; one scout always displays the
joint
while the other does not
In children, comparative images of the two knees may be
performed
with the knees in the head coil. Secure the knees with cushions,
and
for the sequences either adjust TR according to the number of
slices orrun the sequences separately for each side
The anterior cruciate ligament is delineated best at 1520 of
external
rotation, the posterior cruciate ligament at 0 or 5 internal
rotation
-
7/13/2019 MRI MSK Protocol
116/193
ANKLE
-
7/13/2019 MRI MSK Protocol
117/193
ANATOMY
-
7/13/2019 MRI MSK Protocol
118/193
-
7/13/2019 MRI MSK Protocol
119/193
N *
-
7/13/2019 MRI MSK Protocol
120/193
N *
-
7/13/2019 MRI MSK Protocol
121/193
N *
-
7/13/2019 MRI MSK Protocol
122/193
N *
-
7/13/2019 MRI MSK Protocol
123/193
N *
-
7/13/2019 MRI MSK Protocol
124/193
N *
-
7/13/2019 MRI MSK Protocol
125/193
N *
-
7/13/2019 MRI MSK Protocol
126/193
N *
-
7/13/2019 MRI MSK Protocol
127/193
N *
-
7/13/2019 MRI MSK Protocol
128/193
N *
-
7/13/2019 MRI MSK Protocol
129/193
N *
-
7/13/2019 MRI MSK Protocol
130/193
*N
-
7/13/2019 MRI MSK Protocol
131/193
N *
-
7/13/2019 MRI MSK Protocol
132/193
N *
-
7/13/2019 MRI MSK Protocol
133/193
N *
-
7/13/2019 MRI MSK Protocol
134/193
N *
-
7/13/2019 MRI MSK Protocol
135/193
-
7/13/2019 MRI MSK Protocol
136/193
-
7/13/2019 MRI MSK Protocol
137/193
PERONEAL
-
7/13/2019 MRI MSK Protocol
138/193
BREVIS
LONGUS
-
7/13/2019 MRI MSK Protocol
139/193
-
7/13/2019 MRI MSK Protocol
140/193
-
7/13/2019 MRI MSK Protocol
141/193
-
7/13/2019 MRI MSK Protocol
142/193
-
7/13/2019 MRI MSK Protocol
143/193
-
7/13/2019 MRI MSK Protocol
144/193
-
7/13/2019 MRI MSK Protocol
145/193
-
7/13/2019 MRI MSK Protocol
146/193
-
7/13/2019 MRI MSK Protocol
147/193
-
7/13/2019 MRI MSK Protocol
148/193
-
7/13/2019 MRI MSK Protocol
149/193
-
7/13/2019 MRI MSK Protocol
150/193
MRI Normal tibiofibular ligaments
-
7/13/2019 MRI MSK Protocol
151/193
g
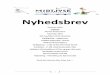
MRI Normal tibiofibular ligaments
-
7/13/2019 MRI MSK Protocol
152/193
Axial T1-weighted MRimage obtained at the
joint level
demonstrates the
anterior (straight
arrows) and posterior
(curved arrow)
tibiofibular ligaments.
Normal talofibular ligaments.
-
7/13/2019 MRI MSK Protocol
153/193
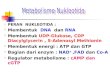
Normal talofibular ligaments.
-
7/13/2019 MRI MSK Protocol
154/193
Axial T1-weighted MRimage depicts the
anterior talofibular
ligament (arrow).
The posterior
talofibular ligament
normally
demonstrates a
striated pattern due to
interspersed fat (*).
NORMAL ATFL (arrow) and NON-VISUALIZED ATFL/ TEAR
-
7/13/2019 MRI MSK Protocol
155/193
Calcaneofibular
-
7/13/2019 MRI MSK Protocol
156/193
Normal calcaneofibular
ligament.
-
7/13/2019 MRI MSK Protocol
157/193
g
Axial T1-weighted MRimage shows the
calcaneofibular
ligament (straight
arrows) immediatelyadjacent to the
peroneal tendons
(curved arrow).
Chronic tear of the calcaneofibular ligament. Axial
T2-weighted
MR image demonstrates marked thickening and waviness of the
calcaneofibular ligament (arrows).
-
7/13/2019 MRI MSK Protocol
158/193
g ( )
Calcaneofibular
-
7/13/2019 MRI MSK Protocol
159/193
Sequential coronal T1-weighted
Injury of the calcaneofibular
ligament.
-
7/13/2019 MRI MSK Protocol
160/193
g
Sequential coronalT1-weighted MR
images
demonstrate
increased signal
intensity and
thickening of the
calcaneofibular
ligament (*)
Achilles tendinosis
-
7/13/2019 MRI MSK Protocol
161/193
Acute Achillesperitendinosis.
Sagittal T2-weightedMR image shows a
reticular pattern ofincreased signalintensity in the preAchilles
tendon fat (*),
a finding that indicatesthe presence ofedema.
-
7/13/2019 MRI MSK Protocol
162/193
Chronic tendinosis ofthe Achilles tendon.
Sagittal T1-weighted
MR image shows
fusiform thickening of
the Achilles tendon
without evidence of
Increased
intrasubstance signal
intensity (arrows).
Partial and Total tear
-
7/13/2019 MRI MSK Protocol
163/193
Ankle Protocol
-
7/13/2019 MRI MSK Protocol
164/193
Sagittal T1/PD FSE (sclerosis)
Sagittal FS PD FSE (soft tissue, subchondral edema, cartilage)
Coronal T1/PD FSE (sclerosis)
Coronal FS PD FSE (tibiotalar chondral surf., osteochondral
lesions)
Axial T1/PD (sensitivity for tendinopathy and ligament
sprains)
Axial FS PD FSE (sens. for tenosynovitis and ligament
disruption)
Hints
TR = 3000 msec
FS PD FSE - TE 40-50 msec
Include Achilles tendon and plantar fascia in sagittal plane
Image in neutral ankle position, plantar flexion foreshortens
ATFL Tibialis anterior requires axial or coronal oblique
Lisfranc ligament evaluation requires axial parallel to
tarsometatarsal
Positioning
Supine
-
7/13/2019 MRI MSK Protocol
165/193
p
Knee coil (head coil or wraparound coil forboth ankles)
Secure ankle in coil
Cushion the other leg well
Sagittal
-
7/13/2019 MRI MSK Protocol
166/193
Coronal
-
7/13/2019 MRI MSK Protocol
167/193
Axial
-
7/13/2019 MRI MSK Protocol
168/193
Tips & Tricks
Optimized imaging of the
-
7/13/2019 MRI MSK Protocol
169/193
p g g
Calcaneonavicular and deltoid ligaments(tibiocalcanean and
talotibial part): coronal slicein maximum dorsiflexion (1020)
Anterior and posterior talofibular ligaments: axial
slice in maximum dorsiflexion (1020)Calcaneofibular ligament:
axial slice in maximum
plantar flexion (4050)
Deltoid ligament (tibionavicular and anteriortalotibial part):
coronal slice in maximum plantarflexion (4050)
MRI of the Achilles Tendon
-
7/13/2019 MRI MSK Protocol
170/193
Sagittal
Coronal & Axial
-
7/13/2019 MRI MSK Protocol
171/193
-
7/13/2019 MRI MSK Protocol
172/193
CERVICAL SPINE
Positioning
-
7/13/2019 MRI MSK Protocol
173/193
Supine on cervical spine coilCushion the legs
Arms straight alongside the body (cushion
them, if needed)
Sagittal
-
7/13/2019 MRI MSK Protocol
174/193
Axial
-
7/13/2019 MRI MSK Protocol
175/193
Cervical spine,
axial, parallel to
the relevant
end plates
Coronal
-
7/13/2019 MRI MSK Protocol
176/193
Tips & TricksIn patients with increased kyphosis cushion the
pelvis; in patients with
cervical spine problems it may be advisable to elevate the head
somewhat
-
7/13/2019 MRI MSK Protocol
177/193
and cushion it
Cushion the neckIf needed, have the patient put on a neck brace
(under the coil, secures
the neck and ensures stability)
Before running sequence 1, have the patient swallow and clear
his/her
throat
In patients with severe scoliosis ensure that enough slices
capture thelateral aspects
In patients with a short neck the upper part of the cervical
spine coil
may not fit: either use phased-array coil or acquire the images
without
the upper strap (image quality will be poorer); for phased-array
coil
select cervical and thoracic
Positioning aids:
Cervical spine: center on the middle of the throat (lower in
patients
with a short neckalmost all the way to the jugular fossa)
-
7/13/2019 MRI MSK Protocol
178/193
THORACIC SPINE
Positioning
Supine
-
7/13/2019 MRI MSK Protocol
179/193
Cushion the legs and secure them ifnecessary
The arms should be alongside the bodyexcept in obese patients,
where they should
be raised above the head
Positioning aid:
Center on a spot about 23 inches (58 cm)
below the jugular fossa(or on the center of the sternum)
Sagittal
-
7/13/2019 MRI MSK Protocol
180/193
Axial
-
7/13/2019 MRI MSK Protocol
181/193
Coronal
-
7/13/2019 MRI MSK Protocol
182/193
Tips & Tricks
-
7/13/2019 MRI MSK Protocol
183/193
In patients with increased kyphosis cushionthe back; in those
with additional neck
complaints it may be advisable to elevate and
cushion the head
In patients with severe scoliosis, ensure that
in the sagittal images enough slices capture
the lateral aspects
-
7/13/2019 MRI MSK Protocol
184/193
LUMBAR SPINE
Positioning
-
7/13/2019 MRI MSK Protocol
185/193
SupineSpine coil
Cushion the legs and secure them if needed
Arms alongside the body (over the head forobese patients)
Sagittal
-
7/13/2019 MRI MSK Protocol
186/193
Axial
-
7/13/2019 MRI MSK Protocol
187/193
-
7/13/2019 MRI MSK Protocol
188/193
Tips & Tricks
In patients with increased kyphosis; cushion the back;in those
with
-
7/13/2019 MRI MSK Protocol
189/193
in those with
additional neck complaints it may be advisable toelevate and
cushion the head
If the patient is in pain, secure cushions to the outsideof the
knees with straps (this relaxes the back muscles)
In patients with severe scoliosis, ensure that enoughslices will
capture the lateral aspects
Positioning aid:
Center on a spot about 23 inches (58 cm) above thesuperior
anterior iliac spine or iliac crest (in a tallpatient)
-
7/13/2019 MRI MSK Protocol
190/193
SACROILIAC JOINTS
Sagittal
-
7/13/2019 MRI MSK Protocol
191/193
Axial oblique
-
7/13/2019 MRI MSK Protocol
192/193
Coronal Oblique
-
7/13/2019 MRI MSK Protocol
193/193