Embed Size (px)
Citation preview

PRACTICAL APPROACH TO PATIENTS WITH NEPHROTIC SYNDROME
Vasant Sumethkul M.D.Professor of MedicineRamathibodi HospitalRamathibodi HospitalMahidol University

ตัวอยางผปวยตวอยางผูปวย
หญิงไทยโสดอายุ 40 ป มาโรงพยาบาลดวยอาการบวม
ป 1 ื และยุบ เปนและหาย มา 1 เดอน
มีประวัติปสสาวะเปนฟอง แตไมมีเลือด
และปริมาณปสสาวะออกดี
ไ โี ป ํ ั ป ิ ป ป ํไมมโีรคประจําตัว และปฏิเสธการทานยาเปนประจํา

T 36 BP 140/90 HR 80
Not pale, no jaundice, pitting edema 4+Not pale, no jaundice, pitting edema 4+
Heart no gallop rhythmHeart no gallop rhythm
L i iLung no crepitation
Abdomen no palpable mass, fluid thrill
Positive, no superficial vein dilatation



CBC Hb 13.0 WBC 8500 PMN 70 L30platelet 240,000
UA sp gr 1020, protein 4+, RBC 3-5WBC 0-1, oval fat body 1-2, no castWBC 0 1, oval fat body 1 2, no cast spot UPCR = 4
TP 70 G/L, Albumin 20 G/L, Ch l 350 /dl T i l id 300 /dlChol 350 mg/dl, Triglyceride 300 mg/dl
BUN 10 mg/dl, Serum Cr 1.2 mg/dl


What should you do next ?
1. Screen for ANA, anti DNA,C3, C4, CH 50, , , ,
2. Bed rest and furosemide 40 mg/dayg y
3 Start prednisolone 1 mg/kg/day3. Start prednisolone 1 mg/kg/day
4 C ll t 24 h i t i4. Collect 24 hour urine protein




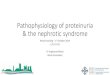
3% 4%3% 3%
other
IgA4%
19%
3% IgA
IgM
Membranous
29%
Membranous
ain
10%
cgn
dn
18%1%4%6%
fsgs
lupus18%1%4%
mes gn
minimal change
Figure 3: Renal Histopathology of patients with nephrotic range proteinuria (N=217)

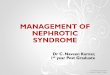
Percent of Secondary Glomerulonephritis
100%post inf
lupus
60%
80%henoch-sc
MM
20%
40% light_c
DN
0%
20%
Cryo
Anti GBM<20 20-40 40-60 >60
AmyloidosAge group (yrs)
Figure 2: Secondary glomerulonephritis by age (n=391)

ผล ANA negative, anti DNA negativeC3, C4 and CH 50 within normal limitHBsAg negative, anti HCV negative,g g , g ,Anti HIV (with consent) negative
CXR no pulmonary infiltrationStool examination ; no parasite found; p
ผูปวยยังมีอาการบวม และน้าํหนักขึ้น 2 กโิลกรัม ใน 1 weekู

What should you do next ?
1. Bed rest and furosemide 40 mg/dayg y
2. Start prednisolone 1 mg/kg/day2. Start prednisolone 1 mg/kg/day
3 Advise renal biopsy3. Advise renal biopsy
4 R t ti i4. Repeat serum creatinine

Percent of Primary GN
80%
100%mini
60%
80% Membranous
fsgs
mes gn
20%
40%mes gn
IgM
IgA
0%
<20 20-40 40-60 >60
mpgn
crescentic gn<20 20 40 40 60 >60
Age group (yrs)
Figure 1: Primary glomerulonephritis by age (n=568)


The patient deny renal biopsy and received prednisolone 50 mg/daily for 4 weeks. How can you characterize the response to corticosteroid ?to corticosteroid ?
1 Diuresis1. Diuresis2. Decrease body weight3 D t i i3. Decrease proteinuria4. Increase serum albumin5. Decrease serum cholesterol

Clinical findings that strongly against the diagnosis of MCNS
1. RBC cast2. Hypocomplementemia2. Hypocomplementemia3. Gross hematuria4 Severe uncontrolled hypertension4. Severe uncontrolled hypertension5. Rapidly progressive renal failure6 O l6. Organomegaly






The patient received prednisolone 50 mg/daily for 8 weeks. Spot UPCR decrease to 1.5pSerum albumin = 25 G/L.
What should you do next ?1 Continue prednisolone 50 mg/daily to1. Continue prednisolone 50 mg/daily to
16 weeks2 Add l h h id 100 /d2. Add cyclophosphamide 100 mg/day3. Add cyclosporin 150 mg/day4. Advise renal biopsy




The patient agree for renal biopsy at
8 weeks, the results are shown here.
What is your diagnosis ?




After renal biopsy, the patient receive prednisolone 30-40 mg/daily and cyclophosphamide 100 mg/day for y p p g yanother 8 weeks.
At 16 weeks, proteinuria is 2+spot UPCR = 0 5spot UPCR = 0.5Serum albumin increase to 38 G/L
What should you do next ?

1. Increase prednisolone to 40 mg/day and continue cyclophosphamide 100 mg/day for another 4 weeks
2. Add cyclosporin ; keep trough level 75-120 ng/dl
3. Continue low dose of Prednisolone and cyclophosphamide and add ACEI keep BP < 130/80
4. Repeat renal biopsy


Response to therapy of MCNS
1. Complete remission:
Proteinuria trace or negative X 2
i i /24 hour Proteinuria < 300 mg/day
2 Partial remission:2. Partial remission:
Proteinuria < 1-2 gram/dayg y
Proteinuria < 50 % of baseline with normal
serum albumin

Steroid non responsive (resistance) MCNS
1 P t i i > 3 5 /d ft 16 k1. Proteinuria > 3.5 gram /day after 16 weeks
2 Patients who do not have criteria for partial2. Patients who do not have criteria for partial
remission after adequate therapy q py

If renal biopsy shows FSGS :If renal biopsy shows FSGS :
What is the different approach ?










If renal biopsy showsIf renal biopsy shows Membranous glomerulonephritis :
What is the different approach ?What is the different approach ?









SUMMARY
1. The prediction of renal pathology from clinical setting is not accurate
2. The long term prognosis of patient with g p g pnephrotic syndrome is generally good
3. Over immunosuppression should be avoided

Thank you for your attention