Embed Size (px)
DESCRIPTION
Â
Citation preview

PhysicianS A N M A T E O C O U N T Y
October 2013 | Volume 2, Issue 9
A publication of the San Mateo County Medical Association
Avoiding the Medicare Quality Reporting Penalty in 2015
Stop Using SOAP!My Patient, MySelf...Who’s First in
Your Life Leadership?
MICRA Under Attack

Health care reform is in full-swing with the heftiest legislation set for 2014 — when health insurance will become available to millions of Americans who were previously uninsured.
HEALTHCARE REFORM THE BASICS FOR INDIVIDUALS
Individual Mandate
Penalty—
Guaranteed issue
Health Insurance Exchange
Subsidies
Premiums
Annual or lifetime limits
Out of Pocket expenses
Beginning January 1, 2014, new regulations provide most Americans access to affordable health insurance that covers essential care. The regulations that facilitate this include:
DID YOU KNOW?
MINIMUM ESSENTIAL BENEFITS INCLUDE:
FOR MORE INFORMATION, CALL A MARSH CLIENT ADVISOR AT 800-842-3761.
Marsh and the Association do not provide tax or legal advice. Please consult with your own advisors to determine how the law’s changes and your decisions impact your personal situation.
LEARN MORE
Sponsored by:
Physicians who do not meet reporting requirements under the Physician Quality Reporting System (PQRS) in 2013 will be subject to a 1.5% Medicare reimbursement penalty in 2015. This issue of San Mateo County Physician features an informative article about how physicians can meet the requirements and avoid the penalty. We’re also including an update on the latest efforts to overturn MICRA. I have also written an article for this issue, “Stop Using SOAP!” which includes my observations about how physician note-taking has changed, and how it could be
improved. Our final feature describes how physicians can develop proactive leadership styles--in the reactive field of medicine--in order to avoid stress, depression and burnout in their own lives and provide better care to patients.
Editorial CommitteeRuss Granich, MD, Chair; Sharon Clark, MD; Edward Morhauser, MD; Gurpreet Padam, MD; Sue U. Malone, SMCMA Executive Director; Shannon Goecke, Managing Editor
Editorial and Advertising Inquiries
San Mateo County Physician is published ten times per year by the San Mateo County Medical Association. Members are encouraged to submit articles, commentary and letters to the editor. Opinions expressed by authors are their own and not necessarily those of the SMCMA. San Mateo County Physician reserves the right to edit contributions for clarity and length, as well as to reject any material submitted.
Advertising in San Mateo County Physician is a great way to reach out to the San Mateo County medical community. Classifi ed ads begin at $40 (for up to fi ve lines) for members. Acceptance and publication of advertising does not constitute approval or endorsement by the San Mateo County Medical Association of products or services advertised.
For more information, contact managing editor Shannon Goecke at (650) 312-1663 or [email protected].
Visit our website at smcma.org, like us at-facebook.com/smcma, and follow us at twitter.com/SMCMedAssoc.
SMCMA LeadershipAmita Saxena,, MD.....................................................................PresidentVincent Mason, MD........................................................ President-ElectMichael Norris, MD............................................. Secretary- TreasurerGregory C. Lukaszewicz, MD........................... Immediate Past President
Manjul Dixit, MD; Russ Granich, MD; Edward Koo, MD; C.J. Kunnappilly, MD; Susan Nguyen, MD; Michael O’Holleran, MD; Chris Threatt, MD; Kristen Willison, MD; David Goldschmid, MD, CMA Trustee; Scott A. Morrow, MD, Health Officer, County of San Mateo; Dirk Baumann, MD, AMA Alternate Delegate
Introduction | Russ Granich, MD
Physician
President’s Message House of Delegates: Democracy in Action ....................................................................... 5
Amita Saxena, MD
Executive Report | Covered California—Bumps ............................ 7
Sue U. Malone
Avoiding the Medicare Quality Reporting Penalty in 2015 .......... 8
ACCMA Staff
MICRA Under Attack ...................................................................... 10
SMCMA-CMA Staff
Stop Using SOAP! .......................................................................... 12
Russ Granich, MD
My Patient, MySelf, MySelf, My Patient...Who’s First in Your Life Leadership? ............................................. 14
Paula-Jo Husack, MFT
Member Updates, Classified Ads, Index of Advertisers .............. 18
On the cover: “3 foot tall Inflatable Jack O Lanterns adorn front yard in Saugus,
Massachusetts,” from Wikimedia Commons user Anthony92931. Used with permission.
S A N M A T E O C O U N T Y
O C T O B E R 2 0 1 3
© 2013 San Mateo County Medical Association

Stage 2 Meaningful Use, Preparations, New Criteria
Meaningful Use Stage 2: Core Measures, Menu Measures, Quality Measures
2014 Edition Standards and Certification Criteria
Presented by Lori Hack, principal and CEO of Object Health LLC, a management consulting group that helps health care organizations and communities improve operational efficiencies and clinical health outcomes. Learn more at www.objecthealth.com.
DATE & TIMETuesday, December 3, 2013
Check-in/buffet: 6:15 P.M.; Program: 6:30 - 7:45 P.M.
LOCATIONSan Mateo County Medical Association
777 Mariners Island Boulevard, Suite 100, San Mateo
COSTSMCMA Members & Staff: 1 Course: $99 / Non-Members: 1 Course: $199
REGISTRATIONPlease return your completed registration form (available at smcma.org) and payment
to fax (650) 312-1664, email [email protected], or mail to SMCMA, 777 Mariners Island Boulevard, Suite 100, San Mateo, CA 94404.

OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 5
President’s Message | Amita Saxena, MD
It’s like driving a car at night. You never see further than your headlights, but you can make the whole trip that way.
—E. L. Doctorow
I recently attended the annual House of Delegates meeting of the California Medical Association (CMA), which was held from October 11 through October 13 at the Disneyland Convention Center in Anaheim. I was part of a seven-member delegation from the San Mateo County Medical Association; Dr. Dirk Baumann, Dr. JD Hoff, Dr. Vince Mason, Dr. Alex Ding, Dr. Bill Tatomer, and Dr. Steve Kmucha were also there to represent San Mateo County physicians. The House of Delegates, or HOD, is the legislative body of the CMA and is charged with establishing the policies that govern the Association as well as electing the CMA’s president. It convenes every year to debate and act on resolutions that deal with multiple issues relating to the practice of medicine, public health and CMA governance. There is an excellent chart on the CMA website (go to cmanet.org and click “About CMA”) that illustrates the organizational structure of the CMA. But I don’t think that a chart can convey all the atmospheric details of what goes on at the HOD. And those details can be helpful in understanding why physician participation in organized medicine is so important.
There were 466 voting delegates to the HOD, and they came from a mixture of individual component medical societies (such as your delegation from SMCMA), as well as mode of practice forums (e.g., solo & small group, medium group), and sections (e.g., young physicians, residents, medical students) The goal is to create a legislative body that is representative of the diversity of physicians in our state. The SMCMA is part of the District 7 caucus to the HOD, which includes San Mateo, Santa Clara, Monterey and Santa Cruz Counties) and the chairman is our own Dr. Dirk Baumann.
There are six reference committees that are responsible for reading all the submitted resolutions, working with CMA to analyze their potential impact, and making recommendations to the HOD as to whether resolutions should be approved. Our own Dr. JD Hoff was chairman of
the committee on insurance and physician reimbursement. I would encourage you to look at the CMA website for the full scope and breadth of submitted resolutions—it’s pretty impressive.
The HOD is governed by the rules of parliamentary procedure, and any delegate could speak on any resolution they felt merited discussion. The debate could be lively, but it was always respectful. We listened to opposing viewpoints in a way that enriched my knowledge of the issues and broadened my perspective. Was it a smooth process? Not always…the rules of parliamentary procedure are complex and can seem arcane at times. Some folks got so caught up in the details of the process that they seemed to ignore the substance of what was being said. Others simply wanted their time at the microphone, their opportunity to share their opinions with a body of their peers. One speaker noted quite accurately that the most vocal folks did not always reflect the opinions of the silent majority, who often waited until a vote was called to surprise everyone.
The topic of change was a big one at the HOD, as there were several proposals that would substantially alter the governance structure of the CMA. Those who were in favor of these changes insisted they were needed to bring the CMA into the 21st century and affirm its relevance to modern medicine and a new generation of physicians. Those who were against the changes argued that they were being implemented too quickly without adequate time for study and analysis of unintended consequences. The debate sounded strikingly similar to that over health care reform, and the direction of medicine in general. It seemed we were divided into two camps: one that was passionately fighting to hang on to traditions and structures that had worked well in the past, and one that felt change was both necessary and inevitable to keep the institution strong and relevant.
So what impressions did I bring home with me? Here they are, in no particular order:
Change is hard, but inevitable. Resistance to change has roots in fear: how do we know we’ve made the “right”
House of Delegates: Democracy in Action

6 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
change? How do we know when we’ve crafted the “perfect” solution? How do we know there won’t be unintended consequences that might be worse? The answer is, we don’t know, but we have the capacity to adapt and solve new problems as they arise. We don’t need to be perfect; we just need to be faith in our ability to evolve with change.
Physicians need to learn the rules of engagement in order to work effectively. Those rules can change depending on the situation: Parliamentary procedure is very different from contract negotiation, which is very different from talking with patients or your peers. Trying to ignore those rules only makes someone look less competent then they really are, and that is never a good thing.
Try not to lose sight of the forest when you are focusing on the trees. The process of discussion should not supersede the purpose, and that is to move an organization forward.
We have to learn to trust each other if we are to move forward. The “us vs. them” mentality only divides our strength and weakens our influence. We also have to be trustworthy to our peers: we need to stay open to opinions
that differ from ours, and we need to communicate openly and honestly with our peers.
Participating in the HOD is watching democracy in action. It is the grassroots backbone of the CMA: it provides a forum where members can submit resolutions that address issues that are important to them. The approved resolutions become official policy of the CMA, and since lawmakers in Sacramento look to the CMA for “what medicine thinks about issues,” these have the potential to direct public policy and create change through legislation. Like most democracies, this process is not always straightforward; it can be messy, loud, chaotic, and at times confrontational. But listening to the debate allowed me to broaden my perspective, giving me a larger context for issues outside my specialty and mode of practice. It also gave me a renewed sense of pride in my profession. We can shape the direction of our profession, we can speak up for our patients and our colleagues, and we can make our voices heard by those who will ultimately shape public policy. ■
President’s Message | Amita Saxena, MD
Make sure you’re prepared.10,500 alleged HIPAA violations.*
In 2012, physicians faced over
For decades, The Doctors Company has provided the highest-quality medical malpractice insurance. Now, the professionals of The Doctors Company Insurance Services offer the expertise to protect your practice from risks beyond malpractice. From slips and falls to emerging threats in cyber security—and everything in between. We seek out all the best coverage at the most competitive prices. So talk to us today and see how helpful our experts can be in preparing your practice for the risks it faces right now—and those that may be right around the corner.
Call (800) 852-8872 today for a quote or a complimentary insurance assessment.
www.thedoctors.com/TDCISCA License #0677182
*Source: Health Information Privacy/Security Alert
Medical Malpractice Employment Practices Liability
Workers’ Compensation Directors and Officers/Management Liability
Health and Disability Errors and Omissions Liability
Property and General Liability Billing Errors and Omissions Liability

OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 7
Executive Report | Sue U. Malone
As I write this message, I cannot access the Covered California website beyond the home page and there are only a few days left in October. Everyone--patients and physicians--are finding the situation troubling. You can imagine the frustration of the individually covered patients who have received termination letters from their carriers effective December 31st because their existing coverage does not cover all of the “essential health benefits” required under the ACA, so they must go out and find new coverage that will be inclusive (but will also be more expensive).
As it is now operating, the Covered California website is misleading because, if one clicks on general coverage questions, the webpages load as expected and can be printed out. However, the interactive screens are sluggish and often don’t work at all. All the informational pages guide you back to the first “Welcome” page, where you are instructed to “Start Here” to obtain coverage. The only problem is that after clicking the “Start Here” button, you are informed that the page cannot be displayed.
On the physician side, it has been very stressful as most physicians do not know whether they are in any of the networks serving San Mateo County (Anthem, Blue Shield, Health Net PPOs, and Chinese Community Health Plan HMO). Most physicians have no recollection of signing up for the Covered California Plan and many physicians may be included in these networks because they signed an “all products” clause with a plan years earlier and are finding out that they are a plan participant in a Covered California network.
The website was designed to include a provider and hospital directory, but there were so many inconsistencies in the data that the directory was disabled and to date is not yet back online. Since this tool is designed for the consumer (not the physician), it allows the consumer to see whether a physician
and a hospital are in one or more networks in a particular zip code. The best approach for physicians is to verify whether you are in a Covered California plan by calling the participating health plans directly to determine your status. The provider relations contact numbers are:
Blue Shield of California800-258-3092
Anthem Blue Cross800-677-6669
Health Net800-641-7761
Chinese Community Health Plan415-523-5615
It is interesting to note that while the federal government created a website for the 34 states that do not have their own exchanges (and, of course, you have read about all that website’s difficulties), the 15 other states, including California and the District of Columbia, each built their own healthcare marketplaces. In California, Covered California signed a five-year, $595 million contract with Accenture, including $199 million for design, implementation and maintenance of costs through June 2017. It makes me wonder why the Feds didn’t undertake design of the entire network for all states, as the IT costs have now mounted to more than $1.1 billion for the 15 states that built their own websites. Yes, I know the Feds have done a poor job of developing their website, but somehow, if given sufficient time, it may have provided a uniform site for all to use, at less cost. Oh, by the way, some of the IT companies were retained by as many as five other states, as well as the federal government, so it sounds like they are double-dipping. ■
Covered California—Bumps

8 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
As part of the Physician Quality Reporting System (PQRS), Medicare will impose a 1.5% penalty in 2015 on physicians and other providers who do not successfully report at least one individual quality measure for at least one patient in 2013. The purpose of this article is to help physicians avoid the penalty in 2015 by providing guidance on how to report at least one measure for at least one patient using Medicare claims.
Since most physicians already submit Medicare claims for reimbursement, adding the additional PQRS reporting information to the claim will be the least burdensome way for most physicians to avoid the penalty. This article also touches upon how physicians can qualify for a quality reporting bonus and discusses some additional PQRS reporting options. However, this article is not intended to be an exhaustive discussion of PQRS, and resources are listed at the end of the article for those desiring additional information.
Avoiding the Penalty in 2015 through Claims-Based ReportingFor many physician practices not yet participating in PQRS, the simplest way to avoid the penalty in 2015 will be to report on one quality measure for at least one patient (preferably a few patients) on your Medicare claims. The process can be broken down into three steps: 1) selecting an appropriate measure; 2) identifying your Medicare patients to whom the measure applies; and, 3) reporting the quality measure on your Medicare claims after an applicable patient encounter.
Step One: Select an Appropriate Measure
Quality measures form the basis of the PQRS program, and are intended to provide information to Medicare about an aspect of care, such as prevention, chronic- and acute-care management, procedure-related care, resource utilization, and care coordination. For purposes of avoiding the penalty in 2015, physicians should select
a quality measure relating to an aspect of care that you will encounter in your Medicare patient population. Review the list of individual measures that are reportable by claims on pages 16-17, and select the most frequent measure that applies to your Medicare patients. Although there are many individual measures that can be reported via claims, some physicians may not find specialty-specific measures. Nevertheless, there may be a measure that reflects a general aspect of care that is not specialty-specific that may be applicable and can be reported for purposes of avoiding the penalty.
Step Two: Learn the Details for Each Measure
After you have selected which measure to report, it is important to review the specifications for the measure with your billing staff. This will help ensure that eligible Medicare patients are appropriately identified and quality measures are accurately reported on claims. Measure specifications are developed by the Centers for Medicare and Medicaid Services (CMS), and can be accessed at www.cms.hhs.gov/PQRS..
Although the details vary across measures, each measure specification developed by CMS shares a common format and provides important information about: which Medicare patients are eligible for reporting the measure based on patient demographics (age and gender), diagnosis (ICD 9 codes), and primary service(s) provided (CPT codes); the various “quality codes” that are used for reporting on Medicare claims; and, the clinical rationale and information about the measure. It is important to review this information carefully since compliance with these specifications is required for measures you report to be counted. For example, you will not get credit for reporting if the Medicare patient is outside of the age range indicated or whose diagnosis code is not listed on the measure specification.
Step Three: Start Reporting on Your Medicare Claims
Once you understand which Medicare patients are eligible and the “quality codes” and modifiers that may be used to report the measure, you are ready to start reporting.
AVOIDING THE MEDICARE QUALITY REPORTING PENALTY IN 2015
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z

OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 9
The final step is to establish a process in your office to ensure that you consistently identify eligible patients, correctly document the correlating clinical information in the patient’s chart, and accurately report the information on your Medicare claims. To ensure you successfully report for at least one patient, it is recommended that you overshoot the target and report the quality measure you select for at least several patients.
With claims-based reporting, a quality code is billed like any other procedure or E/M code (on Line 24 of the CMS 1500 form or electronic equivalent). However, quality codes are billed at a $0.00 charge (or $0.01 if your billing system will not accept zero), and are denied by Medicare with remark code N365 indicating the code is not payable but is counted for tracking purposes. Quality codes are only counted when submitted in combination with an eligible diagnosis and service. Quality codes submitted by themselves or along with services that have already been paid will not be counted (i.e. no retroactive claims-based reporting).
As with any other “billed” Medicare service, quality measures should be supported by documentation in the medical record, which will provide some protection in the event of an audit. Documentation should indicate in clinical terms the basis for the quality code that is reported; it is not sufficient to simply write the code in the medical record.
Earning PQRS IncentivesPhysicians and other eligible providers may earn an incentive equal to 0.5% of allowed charges for 2013 and for 2014. To qualify, physicians must report at a higher frequency on at least three different individual measures (instead of just the one measure required to avoid the penalty) or one measures group (consisting of three or more related individual measures). Individual measures must be reported for at least 50% of eligible Medicare patient encounters, and all individual measures within a measures group must be reported for at least 20 unique Medicare patients.
For claims-based reporting, the process for earning the incentive is similar to the process outlined above for
avoiding the penalty—select measures, learn the reporting requirements, and start reporting on Medicare claims. To qualify for the incentive bonus, you should identify the three most frequently occurring measures (or the most applicable measures group) and you should report the measures as frequently as you can for eligible Medicare patients. Because the threshold to receive the incentive is so high, it is advisable for physician practices to implement processes that enable 100% reporting, which will maximize your chances of receiving the incentive bonus. This might include training your front-office staff or medical assistants to screen patients for reporting eligibility prior to each visit based on demographic and diagnosis information, and placing some sort of flag in the patient’s record to indicate eligibility. Some practices may even find it helpful to use tracking forms that can be placed in the eligible patient’s chart prior to the visit, completed by the physician and clinical staff during the encounter, and then used by billing staff to complete the reporting process. Also, physicians should be advised that the reporting period in January 1st to December 31st, and it may be challenging or even impossible to meet the 50% reporting threshold for the 2013 incentive.
Regardless of whether you report individual measures or measure-groups, it is important to choose measures that occur frequently in your practice. By choosing relatively common measures or measure-groups, you will improve the likelihood of meeting the reporting thresholds. CMS encourages physicians to also consider your own quality improvement goals when selecting measures. While a physician’s goals for their patients should always be the primary driver behind any quality improvement initiative, they are unfortunately not even considered by CMS when determining penalties or incentives. Rather, avoiding the penalty in 2015 and obtaining incentives in 2013 and 2014 is entirely contingent on selecting measures that occur with enough frequency to ensure accurate reporting at or above PQRS minimum thresholds.
More Info about PQRS Reporting
EHR and Registry Reporting
In addition to claims-based reporting, physicians and other eligible providers can report PQRS measures
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
CONTINUED ON PAGE 17

10 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
When trial attorneys announced earlier this year that they were working to scrap California’s Medical Injury Compensation Reform Act (MICRA), CMA warned that their campaign would be riddled with misinformation designed to muddle the issue for voters. Unfortunately, we didn’t know how right we would be.
The initiative, The Troy and Alana Pack Patient Safety Act of 2014, is being put forth by Consumer Watchdog, a political advocacy group backed heavily by California’s trial attorneys. Troy and Alana Pack, ages 10 and 7, were killed in 2003 by a driver under the influence of alcohol and prescription drugs. The initiative’s provisions include mandatory random drug and alcohol testing for physicians and mandatory physician drug and alcohol testing after reports of adverse events, as well as mandatory use by physicians of the electronic CURES database to track patient prescriptions dispensed in California.
The initiative would also retroactively adjust MICRA’s current $250,000 cap on non-economic damages to roughly $1.2 million and allow for further increases based on the Consumer Price Index (CPI) going forward. Lifting the cap would inflate jury awards, substantially increasing the legal fees attorneys can collect from their clients.
However, a recent mailer distributed by Consumer Watchdog made no mention of the proposed initiative’s attempt to more than quadruple MICRA’s cap on non-economic damages. Instead, it focused exclusively on the drug overdose and physician accountability issues, and included the names of hundreds of California physicians who had made political contributions to candidates who have opposed the initiative, suggesting those doctors are afraid to submit to mandatory drug testing (“Who’s afraid to pee in a cup?” the mailer asked.)
This brazen approach illustrates that Consumer Watchdog and its trial lawyers will stop at nothing in their effort to overturn MICRA. Knowing that California voters oppose more lawsuits, higher health care costs and reduced access to care, the lawyers have deceptively cloaked their plans for MICRA in provisions relating to drug testing and prescription drugs. But make no mistake, the real money-maker for lawyers is lifting MICRA’s cap on economic damages.
In the months since trial lawyers launched their latest attack, California physicians and other allies have rallied to MICRA’s defense at a near-historic rate.
We cannot afford to allow these tactics to prove successful. MICRA protects patients involved in medical liability lawsuits by authorizing unlimited economic compensation for any and all economic or out-of-pocket costs, including past and future lost income and medical care along with unlimited punitive damages. Under MICRA, patients can also receive up to $250,000 for non-economic damages. This cap allows medical liability cases to move forward while discouraging lawyers from filing frivolous suits. MICRA also limits how much lawyers can take as payment, ensuring more money goes to patients, not lawyers.
More lawsuits mean higher health costs for patients and providers—which get passed on to the consumer. An analysis by California’s former independent legislative analyst found that this measure would increase health care costs for consumers and taxpayers by nearly $10 billion annually. And the current Legislative Analyst found that this ballot measure could increase state and local government health care costs by “hundreds of millions of dollars annually.”
MICRAUNDER ATTACK!
Trial lawyers have begun an all-out assault on California’s landmark tort reform law.
OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 11
By increasing lawsuits and costs for medical providers, this measure will lead to reduced access to doctors and hospitals and fewer options for affordable, quality health care. The result will be even longer lines in emergency rooms, extended waits for appointments with specialists, and reduced access to women’s services like OB/GYNs, especially in rural and underserved communities.
A broad coalition of doctors, nurses, emergency room physicians, OB/GYN’s, hospitals, Planned Parenthood,
community health centers and hundreds of other organizations strongly oppose the trial lawyers’ measure and will mount a vigorous campaign to defeat it.
As a SMCMA-CMA member, you will be kept in the loop with the latest developments on the MICRA fight. Visit www.cmanet.org/micra to learn more. ■
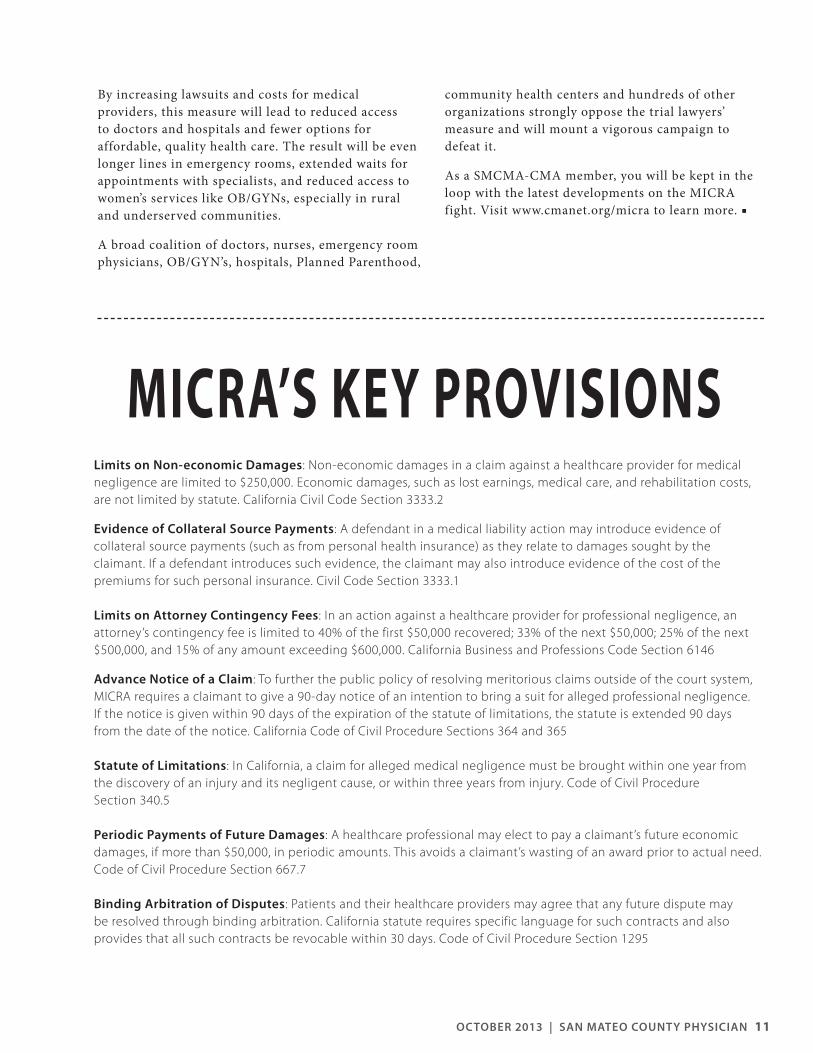
Limits on Non-economic Damages: Non-economic damages in a claim against a healthcare provider for medical negligence are limited to $250,000. Economic damages, such as lost earnings, medical care, and rehabilitation costs, are not limited by statute. California Civil Code Section 3333.2
Evidence of Collateral Source Payments: A defendant in a medical liability action may introduce evidence of collateral source payments (such as from personal health insurance) as they relate to damages sought by the claimant. If a defendant introduces such evidence, the claimant may also introduce evidence of the cost of the premiums for such personal insurance. Civil Code Section 3333.1
Limits on Attorney Contingency Fees: In an action against a healthcare provider for professional negligence, an attorney’s contingency fee is limited to 40% of the first $50,000 recovered; 33% of the next $50,000; 25% of the next $500,000, and 15% of any amount exceeding $600,000. California Business and Professions Code Section 6146
Advance Notice of a Claim: To further the public policy of resolving meritorious claims outside of the court system, MICRA requires a claimant to give a 90-day notice of an intention to bring a suit for alleged professional negligence. If the notice is given within 90 days of the expiration of the statute of limitations, the statute is extended 90 days from the date of the notice. California Code of Civil Procedure Sections 364 and 365
Statute of Limitations: In California, a claim for alleged medical negligence must be brought within one year from the discovery of an injury and its negligent cause, or within three years from injury. Code of Civil Procedure Section 340.5
Periodic Payments of Future Damages: A healthcare professional may elect to pay a claimant’s future economic damages, if more than $50,000, in periodic amounts. This avoids a claimant’s wasting of an award prior to actual need. Code of Civil Procedure Section 667.7
Binding Arbitration of Disputes: Patients and their healthcare providers may agree that any future dispute may be resolved through binding arbitration. California statute requires specific language for such contracts and also provides that all such contracts be revocable within 30 days. Code of Civil Procedure Section 1295
MICRA’S KEY PROVISIONS

12 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
Now that I have your attention, I am talking about the mnemonic “SOAP,” not the cleaning product. Most of us come from the age when we were taught to document progress notes in the SOAP format. If you look at numerous guides for students and residents, such as Mosby’s Practical Guide for the Care of the Medical Patient, 1998 edition, it describes the SOAP note as:
S (Subjective): observations and patient concerns
O (Objective): description of physical findings and recording of lab, x-ray and EKG data. However, when one looks at the example, it includes pertinent data in a concise manner, such as “CXR: RUL infiltrate”
A (Assessment): analysis and tentative diagnosis
P (Plan): planned diagnostic studies and therapeutic regimens
When using this format, a physician can write a brief note that has all the essential elements and is easy to read (legibility aside!), and you, the reader, know what is going on with the patient and what’s happening next. Most notes were less than a page. All was well in the realm of charting, or so it seemed. Of course we relied on the doctor’s putting the relevant information in their note, but this was the golden age of charting, so let’s assume they did. Then, along came regulators who want to make sure we have certain elements documented. Along came payors who want us to substantiate our fees. And then, the most fabulous yet vexing change: the electronic medical record! Now, if you actually print out a note, it can vary from three to 15 pages in length and not really say anything more, just be filled with data, and to put it simply: indecipherable. Often, the actual thinking part of the note, where the doctor puts his or her thoughts, differential and plans, is smaller than before. I always tell my students, that’s what will differentiate you from the rest: the thinking part of the note.
Before you start thinking I am a dinosaur and was charting with a stone and chisel early in my career, I’ll let you know that I am very compulsive and leave no
stone unturned (yes, pun intended). As a palliative care consultant, I need to make sure I understand what is going on with a patient before I can help clarify his or her goals of care, so I am a strong believer in comprehensive notes. The issue is that using the formula suitable for a handwritten note is not working in the EMR. Let’s take a few examples: I’ll start with “copy and paste.” I wish all EMRs deactivated this function. I saw a patient with end-stage cancer, on dialysis, who elected to stop dialysis after the next session. I talked to the hospitalist and had a comprehensive plan for medication titration, etc. Several days later I reviewed the chart and saw under “subjective”: “Patient wants to have one more dialysis.” Turns out the patient had their last dialysis a few days earlier but the doctor kept copying his previous note without correcting it. How often do you see the same exact exam, the same assessment, etc. every day? How do you know the patient was actually seen and examined? How did we know the doctor actually was thinking about what he or she was doing? I also do utilization and quality reviews for Medicare and the VA, looking at more than one thousand charts per year, and this type of copying and pasting is way too common.
Copying and pasting also allows providers to fill their notes with data that is easily accessible with a simple
STOP USING SOAP!
RUSS GRANICH, MD

OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 13
click. In the pre-EMR days, reports often were in transit, verbal or buried in a chart, so it was important to record the result, but no one ever wrote the whole report. Now the entire report ends up with totally extraneous information such as the amount of isotope used in a nuclear study. The person who might be interested in this is not reading that note. I can’t tell you how often I think I am reading the doctor’s impression only to find out it is the impression from a report copied into the note.
The EMR is a wonderful thing, so much information is available, the ability to communicate is phenomenal and all sorts of protections can be built in from drug interactions to alerting you of a completed POLST. However, when we document, we need to be more thoughtful and careful. What is the real purpose of a note? It is a way of documenting what you did and that you addressed issues. It shows your thought process, what you think and what you plan to do. It is a communication tool to covering doctors, consultants, nursing and to your future self, so you know what you’ve done already. It is a way to store information that you personally feel you need in a note. It is a way to assure regulatory compliance. It is a chronicle of what has passed.
I propose that we think about structuring our note differently. The first part should contain the information for your colleagues and staff. Basically a free text, not copied, version of what we used to write. It should contain what has happened since the last note; a brief summary of pertinent findings (exam and studies); and finally your assessment and plan. It could be just a few lines but at most, a half page. Then put a nice space or something to indicate that part of the note is done. The next section should have a more detailed examination
and current data. It can include the necessary regulatory and compliance issues, such as why we are continuing restraints. Follow that with the information you really need or want to have at your fingertips. One example that sticks in my mind is an ICU patient who after several weeks in the ICU still had his home medications listed in his daily progress note. I found this confusing and a distraction but the intensivist told me that when the patient may be able to resume some of these medications, they want to try to get them back on the same medications rather than using alternatives. That made
sense to me, but I didn’t need to read it. I’ve been trying to come up with a clever mnemonic, but can’t seem to find something clever to immortalize me. Perhaps a SOAPY note: a brief SOAP note followed by all the stuff you need, but few others need to read in the daily care of the patient.
AISI, aside from 2MI in UR note, YKW drives me CRZ @TEOTD? Why are there abbreviations in an electronic note!? TCOY TNT.*
About the Author
Russ Granich, MD, is Chief of the Home Care Department at Kaiser Permanente Medical Group in South San Francisco. He is also medical director of Hospice and Home Health. Board-certified in internal medicine and hospice & palliative care, he completed his education at Boston University School of Medicine and his residency at California Pacific Medical Center. He is currently chair of the SMCMA’s Editorial Committee.
The EMR is a wonderful thing, so
much information is available,
the ability to communicate is
phenomenal and all sorts of
protections can be built in from
drug interactions to alerting you
of a completed POLST. However,
when we document, we need to
be more thoughtful and careful.
What is the real purpose of a
note?
*As I see it, aside from too much information in your note, you know what drives me crazy at the end if the day? Why are there abbreviations in an elctronic note!? Take care of yourself til next time.

14 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
Remember Bill Cosby as Heathcliff Huxtable, MD; Obstetrics & Gynecology, of The Cosby Show? And Dr. Nick Riviera (aka Dr. Nick) of The Simpsons? Both of these characters took care of themselves, alongside their patient responsibilities. Dr. Huxtable put his family first and foremost, eventually moved his practice into the home. Dr. Nick, on the other hand, balanced his personal/professional responsibilities, “keeping the coroner away” from patients and cutting costs. Both physicians showed proactive leadership styles, in a profession built on reactive behaviors. re•ac•tive adjective \rē-•ak-tiv\:
(1) done in response to a problem or situation: reacting to problems when they occur instead of doing something to prevent them. (2) the practice of Western medicine. (3) leadership style connoting action after the need or situation.
Proactive leadership in the practice of medicine is part of preventive primary care, especially in an integrative health model. It addresses patients’ wholeness. The tasks involved in your management of patients’ health, even in specialties, is seen by the brain as “reactive.” These examples of proactive leadership through prevention are talked and walked in big strides today. Still, the brain receives the most “brain-training” “reactive” tasks. Add this to your education and training history and it’s a well established brain “groove.” Finally, factor in your own personal lifepath history of reactive behaviors, whether they were by your design or your family’s. This will show what your style is: proactive vs. reactive life leadership.
This article focuses on “reactive,” as it is the most prevalent. It is also the most challenging to pause, when trying to balance life. It’s a major player in physicians’ depression, anxiety, addictions, and burnout. So, let’s be preventive,
“proactive,” right now. Come with me on your life leadership adventure. Take inventory: How many years have you lived life in reactive mode? What years have had a balance of both? Brain studies show that flexing from one to the other in daily life over a month has significant positive impact. It’s a big challenge; though we teach proactive tactics that are small, manageable, and accessible daily. That way, the sequence of the crazy-busy Bay Area life can have mental and physiological “breaks” in
momentum. Physicians brains across specialties train for 40,000 hours; this is a conservative calculation. This includes undergrad, medical school, internship, and second/third-year residencies. By the time that “M.D.” is stitched on your clinic coat, your brain’s “muscle memory” for fact-finding and problem-solving is set in cement, not Jell-o. That M.D. title is a gold-medal equivalent. Your brain has become automatic in this event-response cycle. Add
the average 59.6-hour work week today for “full-time” doctors. This does not measure the thought time when away from patient and administrative duties. It can seem impossible to cross from My Patient to MySelf on a regular basis, especially when you can’t see a space large enough to accommodate your need. Whole-person, whole-life leadership teaches us to scale-down the size of our proactive time and to add repetitions. The resulting new brain-training will bring an easy fluidity in time. Both newer and senior physicians, coming to me for assessment and treatment, have noted the bottom-line: For centuries, the practice of medicine has been reactive. That’s just its design. Patients come in with problems. We’re the healers, with the solutions; to make them well once more. “Or, I enlist the appropriate specialist to expand the players
MY PATIENT, MYSELF; MYSELF, MY PATIENT:Who’s First in Your Life Leadership?
For centuries, the practice of
medicine has been reactive.
That’s just its design. Prevention
education, which is a proactive
brain process, is done less by the
physicians and more by other
health team members.

OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 15
in this Game of Clue.” One reactive process segues to another: Meniscus torn? Limp to the Orthopod for the fix. Acne weeping? Grab a tissue—quick—and get to the Dermdoc. As a physician, you react to the presenting condition. Prevention education, which is a proactive brain process, is done less by the physicians and more by other health team members, as studies report. The movement toward whole-person, whole-life wellness, supported by body-mind-spirit resources, has accelerated in this century. We can say West has now met East. Prevention actions cause our brains, which are “grooved” easily into reactive mode, to slam on the brakes and readjust to accommodate. It’s as though we have emerged in a foreign land for our brains. At first, it’s an uncomfortable change for brain-patterning, going from reactive to proactive, reactive to proactive, and back again. Then uncomfortable becomes comfortable, as the new behaviors and thought patterns settle in to the new “familiar.” What a dynamic switch from that classic Western medicine practice pattern.
“I’m not sure which came first: Caretaking in my family…even emotionally…or at the clinic 20 years ago. I just know it’s hard to get to MySelf and my needs.” Their concerns today are similar to those of the clients I saw at the beginning of my practice. This common comment has been repeated throughout my years in practice.
Even with healthcare systems changing to prevention modality, we’re still reactive-dominant. We’re card-carrying members of the animal kingdom, who are primally wired for fight-or-flight. Now, add living in the Bay Area. A silo of necessary lifestyle tasks awaits us. Achievement-oriented brains live here and want to stay here, particularly in the San Francisco/Peninsula corridor. The check-list of daily life is never completed. Plus, the absence of distinct seasons means that nature is not driving us to stay inside, relax and relate. Yet these are core to our brains’ successful, sustainable transitions from reactive to proactive, reactive to proactive. Our career cultures promote work without limits; not rest and
rejuvenation. We work after work, even though we say we’re at home. We “work” at getting to the gym or doing our yoga classes. We “work” at our kids’ schools, sports, camps. We work on the house and around the house. We work at getting an overnight away with just the two of us. Our San Francisco/Peninsula sociological history points to lots of adrenalin-based work here.
Our environment is hyper-stimulated; we are; our kids are. We say we do less than our neighbors, yet it’s still too, too much. There’s a gross imbalance of work, play, rest, relaxation. A physicians’ lifestyle study of 2012 showed 48% percent of all physicians in America take only a total of two to four weeks off a year, whether in private or organizational practice; whether working two years or twenty. Yet, 25% of internists and primary-care
physicians are still only taking one to two weeks off a year. Could work-related thoughts be more prevalent within primary care, because of its intimate patient relationships and variety of problem-solving?, There’s more “brain time” after the jacket is hung up for the day? In San Mateo County, the hours spent in administrative work adds 10-20% to the physicians’ work week; much more than this when they’re in a learning curve. There’s less time on all fronts. How can a life leadership commitment model be learned, practiced, and
sustained? It can be, with focus, practice, and guidance. You already have that excellent skill set. The timing is right for a proactive choice. There’s ease in your choosing, instead of a health threat making it for you.
To Darwin, two-legged creatures with medical degrees today, have ancestors that emerged from water way back. To spiritual deities, human beings came through birth or miracles. Human beings are primal, reactive members of the animal kingdom, wired to fight or flight. Succeeding through the long road to become a physician develops left-brain, logic even more. The reactive dominance can be balanced by learning the science and art of interruption. Stop the familiar “groove.” “Install” a pause
Twenty-five percent of internists
and PCPs are still only taking
one to two weeks off a year.
Could work-related thoughts be
more prevalent within primary
care, because of its intimate
patient relationships and variety
of problem-solving? There’s
more “brain time” after the
jacket is hung up for the day?

16 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
and proactive thought or behavior. Yes, there will be a return to the reactivity. Over time, though, you’ll notice a powerful change. The need for increased awareness and oversight of our emotions, body sensations, and senses is imperative for our whole life leadership. Right-brain development balances intellectual, logical left-brain dominance. We can be more confident at the controls of our whole-person, whole-life management. The game plan seems simple: My Patient, MySelf becomes MySelf, My Patient; My Patient, MySelf; MySelf, My Patient…Give it movement. Place it on a circular model; not the classic, all-or-nothing linear model. The circle never ends until we do. That’s the idea. The 400+ physicians I’ve known through coaching, counseling, and workshop trainings knew the urgency for change and wanted it. One woman physician, who was recovering from life-threatening illness, said, “We’re trained in answers, solutions from baselines we know. Life leadership is just plain on another planet from medicine and my multi-tasking mommy role…but it’s a necessity to both, now.” A physician new to California and to the University medicine scene, and the first in his extended family to take the education leap, came in when his blood pressure hit the top of Coit Tower, and stayed. His extended family had overseen his life leadership, as they worked to put him through medical school and he worked to add scholarship monies. Life leadership? He interpreted that getting the title would bring life leadership; with his future wife and extended family adding to it for him. He has learned his own life oversight is core. It’s key.
With time, attention and training, My Patient, MySelf circles to MySelf, My Patient. Your proactive approach brings ownership to life quality: yours. Let’s take your thoughts a few more steps forward to action. Check out these primary life elements, which comprise your professional and personal, whole-life experience:
1. Environment: personal spaces, such as home, car, office, yard, etc.
2. Family of origin: the one into which you were born3. Extended family: through marriage or partnership4. Family of choice: the one you have created5. Finance/money6. Individuality/autonomy7. Job/career8. Love/intimacy9. Parenting
10. Physical: health, diet, exercise11. Purpose: life meaning12. Sexuality13. Social14. Spirituality
When have you last updated the status of your primary life elements? With which elements are you currently reactive? Proactive? Both? With which elements are you detached or passive, hoping a issue within will go away? Or, inattentive, knowing the issue is there but not allocating time to it? Some of these decisions can impinge on your long-term wellness plans. This is where the discipline of whole-life leadership enters center stage. Its construct interrupts our brain’s well-trained, reactive repetitions. It trains us to take action, at least through conscious awareness; to go “toward” ourselves, instead of “out there in the world,” away from ourselves. This change alone launches new brain repetitions, slow and unnatural at first. Finally, effective self attachment and awareness is formed. It becomes the “new familiar.” It’s easier to recognize our innermost wants and needs. It lays track for the life balance that’s missing. When we’re balanced, our productivity increases and sustains. It pays off both personally and professionally.
pro.ak.tiv adjective \pro-•ak-tiv\:
(1) of a person, policy, or action creating or controlling a situation by causing something to happen rather than responding to it after it has happened. (2) leadership style connoting planned, purposeful action before the need or situation dictates. (3) farsightedness.
MySelf, My Patient, MySelf, My Patient, MySelf…Are you ready? ■
About the Author
Paula-Jo (PJ) Husack, MA, LFMT, GCP is a licensed Marriage & Family Therapist. She is also a certified EMDR Therapist; and one of an international network of providers, trained to use EMDR for performance enhancement. She sees individuals, couples, families, organizational working (and performing) groups. Her practice is a resource library for the range of life’s situations.
OCTOBER 2013 | SAN MATEO COUNTY PHYSICIAN 17
{CONTINUED FROM PAGE 9}
through EHR systems (either directly or through a data-submission vendor) or through approved registries. Practices utilizing EHR systems should consult your vendors about implementing PQRS reporting in your practice, either for purposes of avoiding the penalty or earning the incentive bonus.
One advantage of utilizing registry reporting is the ability to “retroactively” report quality measures for patient encounters for which the Medicare claim has already been submitted. Registry reporting provides a mechanism for physicians to report quality measures separate from the claims process. However, registry reporting may be an additional process or system in your medical practice, and you may prefer to utilize claims-based reporting.
Group Practice Reporting Option
The PQRS Group Practice Reporting Option (GPRO) is open to medical groups of any size, and provides different options depending on the size of the medical group. For example, in 2013, Group practices ranging in size from 25-99 eligible professionals will report 29
quality measures for 218 consecutive Medicare patients, or 411 consecutive patients for group practices with 100 or more professionals. Practices wishing to use GPRO must submit a self-nomination letter indicating interest in participation. The next opportunity for GPRO participation will be for the 2014 reporting period.
Validation Process if Fewer than Three Measures Can Be Reported
If fewer than three quality measures can be reported, physicians may still earn the incentive. CMS uses a “measure-applicability validation process” to verify whether a physician could have reported on additional measures before determining whether reporting requirements for the bonus have been met. CMS analyzes claims to determine if other measures could have been reported (based on ICD-9 and CPT codes). If CMS finds that 30 or more patients/encounters during the reporting period were eligible for reporting another measure, the physician practice will not have met the reporting requirements. Financial Incentive Paid to TIN
PQRS tracks compliance with the reporting requirements at the individual provider level (using the NPI number), but the PQRS payment will be made to the Taxpayer Identification Number (TIN) used by the reporting physician. Participating physicians within the same practice (using a common TIN) should expect to receive the physicians’ incentives in a lump sum. Likewise, physicians who see patients on behalf of more than one practice (and, therefore, use more than one TIN when submitting Medicare claims) should expect their PQRS payment to be made to the respective TIN under which the services were reported.
Additional PQRS Resources For more information about PQRS, the California Medical Association has published a guide that is available online at www.cmanet.org. For official PQRS information, please visit the CMS website at www.cms.gov/pqrs. ■
Reprinted from the Alameda-Contra Costa County Medical Association (ACCMA) BULLETIN.
For a full list of PQRS measures that can be reported through Medicare claims, please visit www.smcma.org/pqrs.
Tracy Zweig AssociatesA R E G I S T R Y & P L A C E M E N T F I R M
INC.
www.tracyzweig.com
Voice: 800-919-9141 or 805-641-9141
FAX : 805-641-9143
Locum Tenens
Permanent Placement
Physicians Nurse Practitioners
Physician Assistants
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z

18 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2013
INDEX OF ADVERTISERS The Doctors’ Management Company ...................................... 6The Magnolia of Millbrae. ............................ Inside Back CoverMarsh.......................................................................Inside Front CoverNORCAL ..............................................................Outside Back CoverOffi ce Space for Rent: Burlingame ......................................................... 18Tracy Zweig Associates. .................................................................. 15
For advertising information, please call (650) 312-1663 or email [email protected].
NEW SMCMA MEMBERS
Richard Aulwurm, MDSeptember 29, 2013
George Benson, MDAugust 11, 2013
Harry Roth, MDAugust 11, 2013
IN MEMORIAM
Christina Rincon, MDFM/San Mateo
Connor Lundy, MDEM/South San Francisco
Robert Osteroff, MDGE, IM/Burlingame
Timothy Litwin, MDIM/Daly City
Christine Jacobson, MD*D/San Bruno
Irene Lee-Klass, MDFM/San Mateo
Erinn Hama, MDEM/South San Francisco
Kevin Chao, MDNS/Redwood City
Natalya Denissov, MD*FM/Redwood City
Tarini Anand, MDwIM/Burlingame
Edouard Aboian, MD*VS/Burlingame
Amy Alers, MD*N, *CLP/Burlingame
OFFICE SPACE FOR RENT IN BURLINGAME
Nice office available for rent, approximately 1,500 square feet, at 1828 El Camino Real, Suite 707, in Burlingame. Available November 2013. Direct inquiries to Carol Hiroshima at [email protected] or (650) 697-7079.
THE PENINSULA’S PREMIER RETIREMENT COMMUNITYRCFE# 415600154
201 Chadbourne Avenue | Millbrae, CA 94030
(888) 862-6915(650) 697-7700
www.themagnolia.com
GET A NEW TAKE
ON YOUR
BUCKET LIST.

777 Mariners Island Boulevard, Suite 100San Mateo, California 94404
ADDRESS SERVICE REQUESTED
NORCAL Mutual is owned and directed by its physician-policyholders, therefore we
promise to treat your individual needs as our own. You can expect caring and personal
service, as you are our first priority. Contact your broker or call 877-453-4486 today.
Visit norcalmutual.com/start for a premium estimate.
NORCAL Mutual is owned and directed by its physician-policyholders, therefore we
promise to treat your individual needs as our own. You can expect caring and personal
service, as you are our first priority. Contact your broker or call 877-453-4486 today.
Visit norcalmutual.com/start for a premium estimate.
A N O R C A L G R O U P C O M PA N Y
N O R C A L M U T U A L .C O M
N O R C A L M U T U A L I S P R O U D T O B E E N D O R S E D B Y T H E S A N M A T E O C O U N T Y M E D I C A L A S S O C I A T I O N





























