Embed Size (px)
Citation preview

LARYNGOSCOPE

INDICATIONS
In Infants Prior to endotracheal intubation in:• Neonatal asphyxia• Meconium aspiration• Respiratory distress syndrome• Tracheo oesophageal fistula• Mechanical ventilation
.
In Older Children Prior to endotracheal intubation:• Resuscitation• During admoinistration of general anaesthesia• Epiglottitis• Kerosene poisoning Direct Laryngoscopy• In cord palsy• Anatomical lesions• Foreign body
Contraindications
• Diseases or injuries of cervical spine.• Moderate or marked respiratory obstruction.

PROCEDURE
1. Gauze piece placed on upper teeth to protect against trauma.
2. After lubrication, the laryngoscope is held by the handle in the left hand. Right hand is used to retract the lips and guide the scope.
3. It is introduced by one side of the tongue which is pushed to the opposite side till posterior third of tongue is reached.
4. It is advanced behind the epiglottis and lifted forward without levering it on the upper teeth or jaw
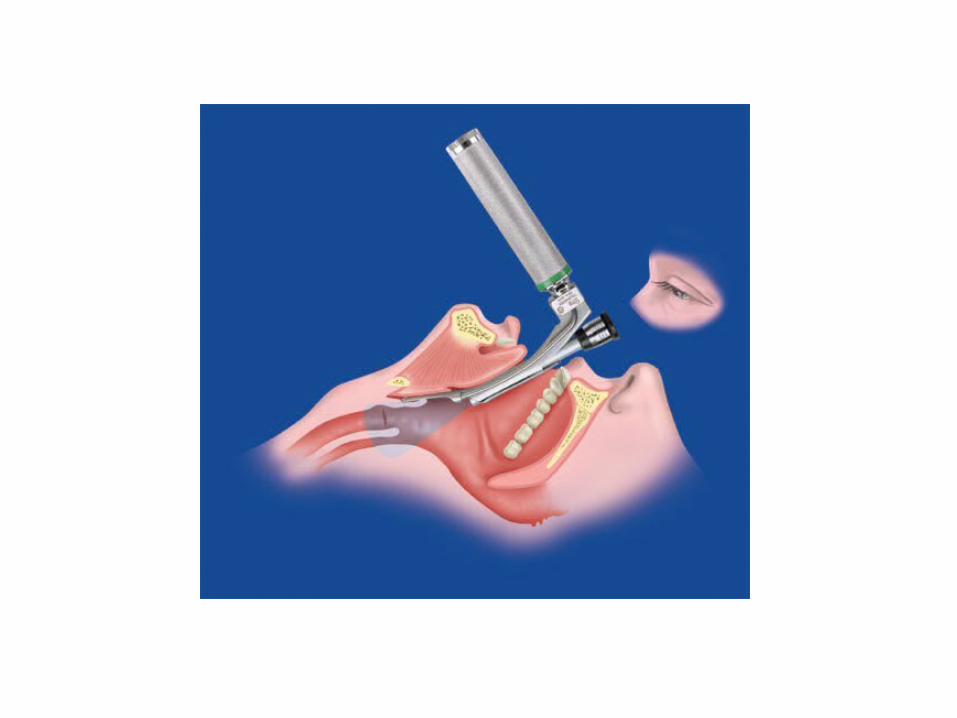
Following structures are examined serially:1. Base of tongue2. Right and left valleculae3. Epiglottis4. Right and left pyriform sinuses5. Arypeiglottic folds6. Arytenoids7. Post cricoid region8. False cords9. Anterior and posterior commissure10. Ventricles and vocal cords11. Subglottic area

Complications
• Mechanical injury injury to local tissues like teeth,tongue,palate• Stimulation of posterior pharyngeal wall may
cause vago-vagal episode leading to hypoxia, bradycardia.
• Hyperextension of neck may cause damage to cervical spine.
OXYGEN RESERVIOR
Small corrugated ,tube like structure usually made of plastic.
Has 2 open ends
One end is connected to air inlet of ambu bag, other end should be
left open.
USES:
Increase the FiO2 of the oxygen delivered to the patient by ambu
bag from 40% to more than 90%.

OXYGEN MASK
Usually made up of plastic or rubber.
TYPES:
Uncushioned
Cushioned
ADVANTAGES(of cushioned mask)
The mask conforms to the face
Requires less pressure to obtain air tight seal
Less chances of damage to eyes or other structures of the face
SHAPES:
Round
Anatomically shaped-somewhat triangular in shape
Tip over the nose.
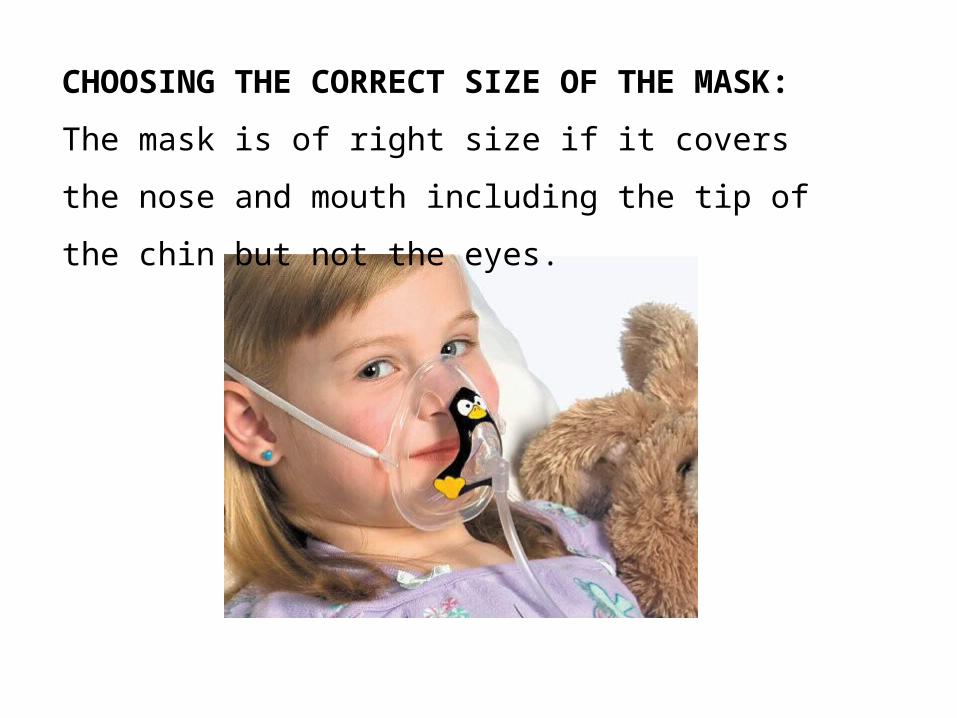
CHOOSING THE CORRECT SIZE OF THE MASK:
The mask is of right size if it covers the nose and mouth
including the tip of the chin but not the eyes.

OXYGEN HOOD
Plastic hood that can be placed over an infant’s head
It has an inlet which can be connected to the oxygen source
Front portion is chiselled such that it lies over infant’s neck while
allowing easy access.
Used to administer humified oxygen to infant in all conditions
associated with hypoxia

ADVANTAGES:
non invasive
Allows humidification of oxygen
DISADVANTAGES:
Oxygen flow may be insufficient in cases where respiratory drive is
poor
Any change in the position of the hood may result in oxygen leaking
outside the hood thus decreasing oxygen concentration
Oral feeding is difficult
Poorly tolerated leading to excessive crying or struggling by the
child
spacer

• Spacers are bottle-shaped plastic devices which have a mouth piece at one end and other end has an opening which the MDI can be attached.

• The disadvantage of MDI is that it requires perfect co-ordination between inspiration and activation of device.
• This may not possible in small children,to eliminate this problem spacer is adviced.
How to use MDI with spacer device
• Remove the cap of MDI shake it and insert in to spacer device.
• Place mouth piece of spacer in mouth or attach to face mask in case of infants and younger children
• Start breathing in and out gently and observe movements of valve.
• Once breathing pattern is established press canister and continue to breath 5-10 times
• Remove the device from mouth and wait for 30 seconds before repeating
Advantage
• MDI when used alone (withot spacer )rarely deliver the full amount of inhailed medicines to the lung (majority get deposited in oropharynx)
thus, spacers should always be used along with MDI’s to increase efficiency and decrease side effects

Nebulizer

• Nebulizers are devices which are useful in delivering aerosolized drugs to lungs in patients suffering from acute severe episodes of asthma, bronchiolitis or status asthmaticus.
• They are especially helpful when when inspiratory effort is weak as in case of infants,prolonged episodes of asthma.
How to use nebulizer?
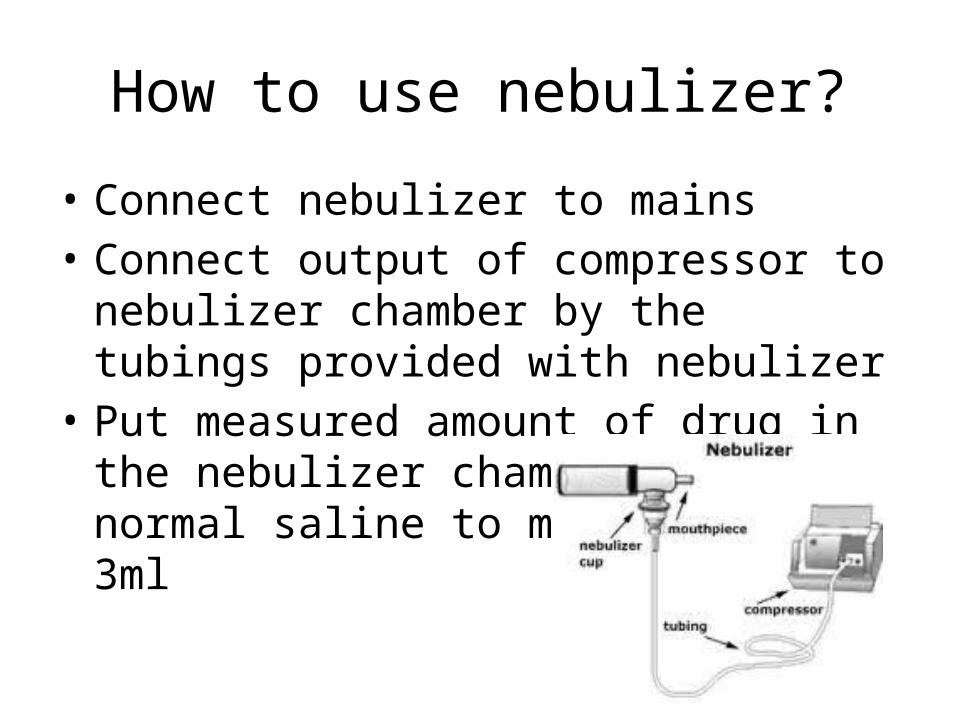
• Connect nebulizer to mains• Connect output of compressor to nebulizer
chamber by the tubings provided with nebulizer
• Put measured amount of drug in the nebulizer chamber and normal saline to make it 2.5-3ml
• Switch on the compressor and look for aerosol coming out from other end of nebulizer
• Attach facemask to this end of nebulizer chamber and fit it to cover nose and mouth of child
• Encourage child to take tidal breathing with open mouth
Drugs which can be delivered to lungs by nebulizer
• Bete -2 agonist – salbutamol• Inhaled anticholinergics- Ipratropium Bromide• Inhaled steroids- Budesonide• Inhaled racemic epinephrine – in case of
bronchiolytis• Inhaled chromolyn sodium- for maintanance
therapy of asthma.

• The commonly used nebulizer solution of salbutamol contains 5mg of salbutamol per ml of solution.
• The dosage of salbutamol is 0.15mg/kg/dose• Amount should be diluted with about 2-3ml of
normal saline before nebulization.
Tongue depressor
• A tongue depressor is a device used in medical practice to depress the tongue to allow for examination of the mouth and throat
• They are usually made of stainless steel & can be sterilized by autoclave,but nowerdays disposable tongue depressors are available which can be disposed off after use
• They are available in two shapes
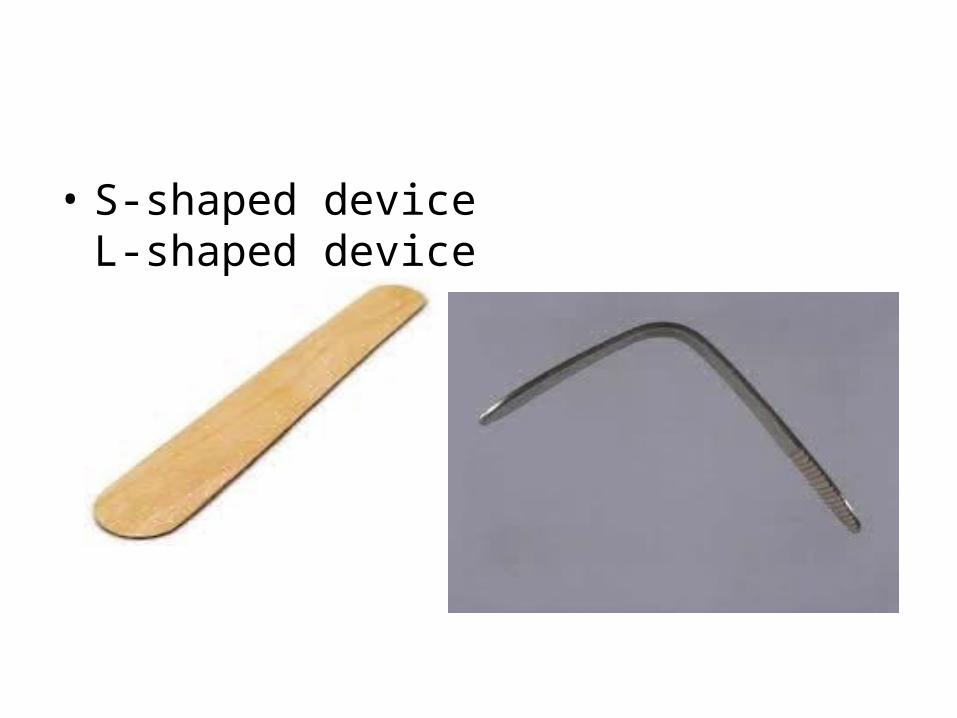
• S-shaped device L-shaped device
uses
• To examine the gag reflex• To examine the pharynx,oral cavity,tonsils• To examine the movements of the palate &
the uvula• Spatula test-to test for the spasm of the
masseter muscles in a suspected Tetanus case by trying to insert the tongue depressor in between teeth.
• CLINICAL THERMOMETER• INFANT FEEDING TUBE• SIMPLE RUBBER CATHETER
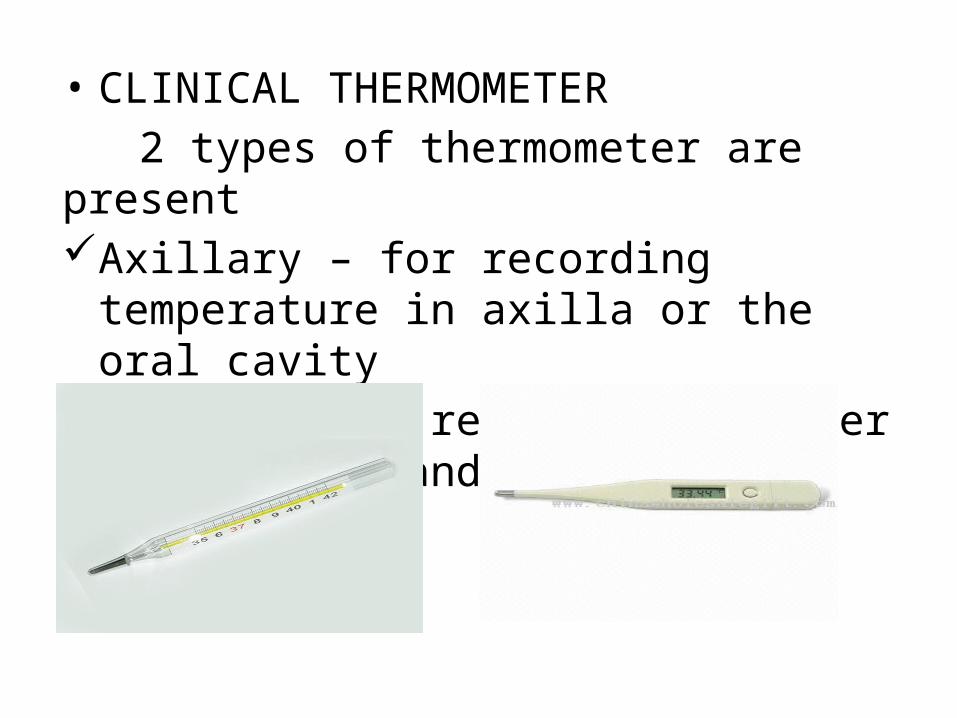
• CLINICAL THERMOMETER 2 types of thermometer are presentAxillary – for recording temperature in axilla
or the oral cavityRectal – the rectal thermometer has a stout
and a blunt bulb
• The clinical thermometer is calibrated over the range from 95-110 F
• Nowadays, digital thermometers of various types are available. They provide quick results(45 seconds – 1 minute as compared to traditional which take 3-5 mins)
• An even better device is available which when inserted into the external auditory canal gives the temperature of tympanic membrane (core body temperature) within a few seconds.
• Disadvantage of this device is that it is difficult to use in case of presence of wax and may accidently damage the ear .
• Uses – • Used to record the body temperature Hypothermia: In premature infants Infants with septicemia In children with PEM
Hyperpyrexia: In children with acute infections In tetanus Sunstroke Pontine hemorrhage• After use it should be washed with water and stored in a jar
partly filled with a chemical disinfectant like alcohol (70%)
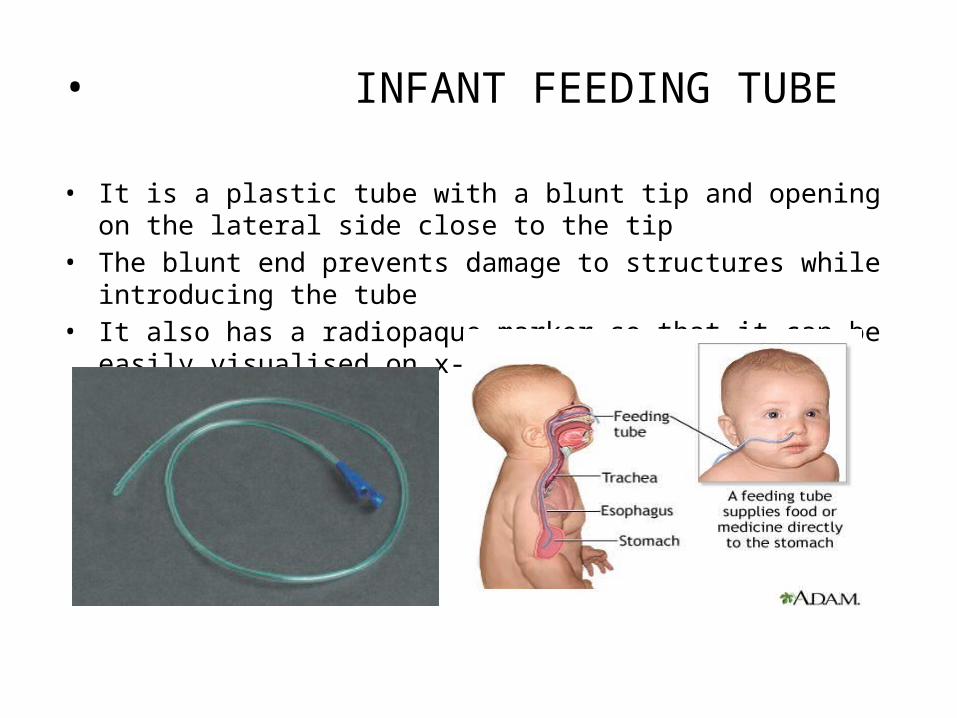
• INFANT FEEDING TUBE
• It is a plastic tube with a blunt tip and opening on the lateral side close to the tip
• The blunt end prevents damage to structures while introducing the tube• It also has a radiopaque marker so that it can be easily visualised on x-ray
sizes• Number 5 to number 12 are usually used in pediatric practice
Indications• Diagnostic purposes Diagnosis of internal bleeding in stomach and upper GIT Diagnosis of TB Diagnosis of tracheo-oesophageal fistula Diagnosis of poisoning Localisation of oesophageal strictures Gastric analysis
• Therapeutic purposes Nasogastric feeds Management of haematemesis Management of poisoning Administration of drugs Pre-operatively to decompress the stomach if an emergency surgery is to
be carried out and sufficient time for fasting is not available
• Other causes As an oxygen catheter For nasal , endotracheal and tracheostomy suction As a tourniquet
PROCEDURE• The approximate length that the tube should be inserted can be measured
by adding distance from the nose to the tragus to the distance from the tragus to xiphoid. After inserting the tube and removing the stomach contents via a syringe , the tube is fixed with the help of an adhesive tape.

SIMPLE RUBBER CATHETER• It is made up of indian rubber with a blunt tip and opening on the lateral
side . • The infant feeding tube can be used as a simple catheter in small infants• Sterilised by autoclaving.

• SIZE OF CATHETER• English scale- used in calibrating simple rubber catheter diameter of the catheter= (number of catheter) + 2 /2
• French scale – used in calibrating foley’s catheter 1 french = 1/3 mm (diameter of catheter)
INDICATIONS• URINARY CAUSES Diagnostic To differentiate between anuria and retention of urine To collect sterile sample for urine culture In procedures such as cystography and ascending pyelography Diagnosis of hematuria Diagnosis and localisations of strictures in the urethra
Therapeutic To relieve acute retention of urine To monitor the urine output in shock , renal failure In case of paraplegia To administer bladder wash
• NON- URINARY CAUSES
Bowel wash To administer enema To relieve flatus As an oxygen catheter For nasal/endotracheal suction/tracheostomy suction As a tourniquet
PROCEDURE After observing complete aseptic precautions (wash up – antiseptic cleaning
and draping of genital parts), the catheter tip is lubricated with lignocaine jelly and slowly the catheter is guided into the urethra till drops of urine appear from the distal end
COMPLICATIONS Trauma – leading to bleeding and in chronic cases – stricture formation Infection Allergy to India rubber Para – phimosis in cases of forcible retraction of prepuce while introducing
the catheter