Embed Size (px)
Citation preview

1
Pelvic exsanguination
แพทยหญงปรญญา ปรญญาณฏฐ
อาจารยบรภทร สงขทอง ภาควชาศลยศาสตร คณะแพทยศาสตร
มหาวทยาลยสงขลานครนทร
Exsanguinating pelvic fracture เปนการหกของกระดกเชงกรานทผปวยมกมสญญาณชพไมคงท และ
อาจพบกระดกเชงกรานหกชนดไมมนคง (unstable pelvic fractures) ซงสมพนธกบกลไกลการบาดเจบแบบพลงงานสง (high energy mechanism) และเกดการบาดเจบของอวยวะอนรวมดวย (1)
กายวภาคกระดกเชงกราน (Anatomy)
กระดกเชงกราน (Pelvis) ประกอบดวยกระดก 3 สวน ประกอบกนเปนวง คอ
- Sacrum - Coccyx
- Hip bones ประกอบดวยกระดก 3 ชน o Ilium o Ischium o Pubis
กระดกเชงกรานแตละชนยดกนดวยเอน (Ligament)
- cartilage ทยดกระดก symphysis pubis ทางดานหนา - Superior and inferior pubic ligaments
- Ventral, interosseous และ dorsal sacroiliac ligaments เพมความแขงแรงของ pelvic ring - Sacrospinous ligament - Sacrotuberous ligament - Sacrospinous ligament

2
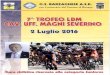
หลอดเลอดแดงทน าเลอดเขาสเชงกราน หลอดเลอดหลกคอ Internal iliac (hypogastric) artery ทแยกมาจาก common iliac artery โดยแบงออกเปน Parietal branches และ Visceral branches
- Parietal branches ไดแก
o Iliolumbar artery supplies bone and muscle in the iliac fossa
o Lateral sacral arteries supply the sacrum and coccyx
o Obturator artery divides into anterior and posterior branches which encircle the margin of the obturator foramen
o Superior and inferior gluteal arteries
o Internal pudendal artery
- Visceral branches ไดแก
o Umbilical arteries
o Superior and inferior vesical arteries supply the bladder, and the middle rectal artery supplies the rectum
o Uterine artery (Artery of the ductus deferens)
o Vaginal artery and middle rectal arteries

3
รปท1 กระดกเชงกรานและหลอดเลอด
อบตการณ (Incident)
อบตการณกระดกเชงกรานหกจากอบตเหตแบบ blunt mechanism รอยละ 9.3 ซงกระดกเชงกรานทหกท าใหอวยวะในชองทองมการบาดเจบไดรอยละ 16.5 โดยพบการบาดเจบของตบรอยละ 6.1 กระเพาะปสสาวะและ ทอปสสาวะรอยละ 5.8 มามรอยละ 5.2 กระบงลมรอยละ 2.1 ล าไสเลกรอยละ 2.0 ล าไสใหญรอยละ 1.2 ไสตรงรอยละ 0.9 ตบออนรอยละ 0.4 กระเพาะอาหารรอยละ 0.3 ล าไสเลกสวนตน (duodenum) รอยละ 0.1 (2)
ilium sacrum
pubis
ischium
coccyx

4
และในผปวยทมกระดกเชงกรานหกอยางรนแรงมอตราเสยชวต รอยละ 25-41.7 (ตารางท1) ตารางท1 อตราเสยชวตในผปวยทมกระดกเชงกรานหก
Author Publication n Mortality (%)
Wolfgang Ertel(3) 2000 174 29.9
Ertel W(4) 2001 20 25
Biffl WL(5) 2001 732 31
Hornez E(1) 2011 200 30
Lustenberger T(6) 2011 50 32
Zhiyong Hou(7) 2012 724 41.7
Classification
การแบงชนดของกระดกเชงกรานหกสามารถแบงไดหลายรปแบบ เชน Tile’s classification, Young-Burgess classification และ Orthopaedic Trauma Association (OTA) Classification ซงแผนกศลยกรรม มกนยมแบงชนดของกระดกเชงกรานหกแบบ Young-Burgess classification
Young-Burgess classification(9)
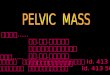
Young JW และคณะ แบงชนดการหกของกระดกเชงกรานจากภาพเอกซเรยในผปวยกระดกเชงกรานหก 142 คน และเผยแพรในป 1986 โดยแบงชนดตามกลไกการบาดเจบ คอ lateral compression (LC), anteroposterior compresion (APC), vertical shear (VS)และ combined mechanical injury(CMI)(9) (รปท 2)
LC: สมพนธกบการหกในแนวขวางของกระดก pubic rami (horizontally oriented pubic rami fractures anteriorly and variable injuries posteriorly)
LC I: The internal rotation of the pelvis causes a compression fracture of the sacrum on the side of impact
LC II: Crescent fracture present on the side of impact

5
LC III: Fractures have an LC I or LC II fracture on the side of impact, with an associated open-book type injury present contralaterally
APC: Injury to the anterior structures in the form of pubic symphysis separation or vertically oriented pubic rami fractures, along with varying degrees of posterior injury
APC I: No posterior instability with diastasis of the pubic symphysis
limited to less than 2.5 cm
APC II: Associated with some degree of posterior instability due to injury to the anterior sacroiliac complex allowing greater than 2.5 cm of symphyseal diastasis and anterior SI widening, the posterior SI ligaments are intact
APC III: Complete disruption of the SI joint leading to widening and instability
VS: Unstable injury patterns with vertical displacement of the hemipelvis due to symphyseal diastasis or rami fractures, anteriorly, and iliac wing fractures, sacral fractures, or sacroiliac joint dislocations present posteriorly
CMI: Combination of the injury patterns

6
รปท2 การแบงชนดของกระดกหกแบบ Young-Burgess classification
Diagnostic tool
Clinical Exam (การตรวจรางกาย)
The American College of Surgeons Advanced Trauma Life Support (ATLS) 9th edition แนะน าใหตรวจกระดกเชงกราน (pelvic examination) ในผปวยอบตเหตทกราย
การตรวจกระดกเชงกราน (pelvis) เพอคนหากระดกเชงกรานหกแบบ unstable pelvic fractures มหลายวธ เชน การตรวจพบวากระดกเชงกรานสามารถขยบได (Unstable pelvic ring) อาการปวดหรอ กดเจบบรเวณ
Young-Burgess Shock Trauma Pelvic Fracture Classification (J Trauma 30(7): 848-856

7
กระดกเชงกราน และกระดกเชงกรานผดรป เปนการตรวจดความมนคงของกระดกเชงกราน โดยใชมอกดบรเวณกระดกเชงกรานอยางนมนวลใหกระดกเชงกรานเคลอนเพยงเลกนอยในแนวตรงและ แนวหมน(11)
Grant PT ศกษาแบบprospective ในป 1990 ในผปวย 36 คน พบวา การตรวจพบกระดกเชงกรานแยกออก (springing of pelvis) มความไว (sensitivity) ในการตรวจพบกระดกเชงกรานหก รอยละ59 และมความจ าเพาะ (specificity) รอยละ59 ซงแตกตางกบการศกษาของ Gonzalez RP และคณะ ในป 2002 ทศกษาผปวย blunt trauma 2,176 คน โดยมผปวยทกระดกเชงกรานหก 97 คน (รอยละ4.5) มความไวในการตรวจพบกระดกเชงกรานหก รอยละ93(12) และการศกษาแบบ Meta-analysis review ในป 2004 โดย Sauerland S และคณะ ศกษาผปวย 5,454 คน พบวาความไวในการตรวจกระดกเชงกรานแลวพบกระดกเชงกรานหก รอยละ90 และความจ าเพาะ รอยละ90(13)
Shlamovitz GZ และคณะ ไดศกษาความไวและความจ าเพาะในการตรวจกระดเชงกรานวธตางๆ จากการดจากแฟมประวตผ ปวยblunt trauma 1,502 คน ในป 2009 โดยมผ ปวยทกระดกเชงกรานหกแบบ unstable pelvic fractures 34 คน พบว าหากตรวจพบ Unstable pelvic ring ความไวในการตรวจพบ unstable pelvic fractures รอยละ26 และความจ าเพาะ รอยละ 99.9 และถาหากตรวจพบวามอาการปวดหรอกดเจบบรเวณกระดกเชงกราน ความไวในการพบ unstable pelvic fractures รอยละ 100 และความจ าเพาะ รอยละ 93 นอกจากนหากพบกระดกเชงกรานผดรป ความไวในการพบ unstable pelvic fractures รอยละ 55 และความจ าเพาะ รอยละ 97(11)
จากหลกฐานเชงประจกษดงกลาวขางตน ความไวและความจ าเพาะของการตรวจรางกายเพอวนจฉยกระดกเชงกรานหกแตกตางกน ดงนนอาจใชการตรวจรางกายหลายๆวธรวมกนเพอประเมนกระดกเชงกรานหก

8
Routine X-rays
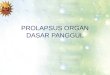
ตาม ATLS guideline แนะน าใหท าเอกซเรยกระดกเชงกราน (film pelvis AP view) (รปท 3) ในขนตอนของ adjunct to the primary survey เพอตรวจหาการหกของกระดกเชงกรานโดยเฉพาะในผปวยทมการบาดเจบหลายระบบ ซงความไวในการตรวจพบความผดปกตของกระดเชงกรานจาก A-P pelvic x-ray รอยละ 87(12)
รปท 3 Film pelvis AP view
Gillott A และคณะ ศกษาประโยชนของการใช routine pelvic X-ray ในผปวย blunt trauma 699 คน แบบ prospective ในป 1988 พบวาหากตรวจพบความผดปกตจากเอกซเรย ผปวยจะม Injury Severity Score การใหเลอด และอบตการเกดการบาดเจบตอหนาอก และทองสงกวาผปวยทไมพบความผดปกตของเอกซเลย จงแนะน าใหท า routine pelvic X-ray ในผปวย blunt trauma(14)
C K Salvino และคณะ ศกษาประโยชนของการท าเอกซเรยกระดกเชงกรานในผปวย blunt trauma ทกรายจ านวน 1,395 คน ในป 1992 พบวาผปวยทไมเจบบรเวณกระดกเชงกราน และตรวจรางกายไมเจบตรวจพบกระดกเชงกรานหกจากเอกซเรยกระดกเชงกรานเพยง รอยละ 0.4 ซงผปวยเหลานมกระดกหกเพยงเลกนอยไมมผลตอการเปลยนแปลงการรกษา เมอเทยบคาใชจายในการท าเอกซเรยกบประโยชนแลวแนะน าวาไมตองเอกซเรยในผปวย blunt trauma ทกราย(15)
ตอมาในป 2006 Obaid AK และคณะ ศกษา retrospective review ในผปวยอบตเหตทพบกระดกเชงกรานหกจากภาพเอกซเรย 174 คน จากผปวยทตรวจพบกระดกเชงกรานหกจากเอกซเรยคอมพวเตอร 521 คน พบวาความไวในการตรวจพบกระดกเชงกรานหกจากเอกซเรยกระดกเชงกรานในผปวยอบตเหต รอยละ78 จงแนะน าวาใชเอกซเรยกระดกเชงกรานเปนเครองมอในการคดกรองในผปวย hemodynamic unstable patients(16)

9
Matthias P Hilty และคณะศกษายอนหลงในผปวยจ านวน 452 คน ทเปนผปวย blunt trauma มการบาดเจบหลายต าแหนง แตhemodynamic stable และ clinically stable pevis พบวามกระดกเชงกรานหกทตรวจพบจากเอกซเรย รอยละ 9 และมความไว รอยละ 67 จากการวจยนจงแนะน าวาใหท าเอกซเรยคอมพวเตอรกระดกเชงกรานโดยไมตองเอกซเรย หากสามารถท าได(17)
Chih-Yuan Fu และคณะ retrospectively reviewed ในป 2013 ในผปวย major torso injuries 726 คน พบวาไมมความแตกตางระหวางการใชเอกซเรยกระดกเชงกรานเทยบกบเอกซเรยคอมพวเตอรในการตรวจพบความผดปกต รอยละ 51.7 และตรวจไมพบความผดปกต รอยละ 61.0 (P=0.7) จงมความเหนวาการตรวจดวยเอกซเรยกระดกเชงกรานชวยลดการท าเอกซเรยคอมพวเตอรไดในผปวยทสงสยมเลอดออกทหลงเยอบชองทอง (retroperitoneal hemorrhage)
Diagnosticc peritoneal lavage (DPL) Steve G. Hubbard ศกษาผปวยทมกระดกเชงกรานหก 222 คน ในป 1979 false-positive lavage results
รอยละ 29 ไมพบวาม false-negative results(18)
Mendez C ศกษาในป 1994 ผปวยจ านวน 497 คนท าDPL พบวา ความไวในการตรวจพบกระดกเชงกรานหก รอยละ94 ความจ าเพาะ รอยละ99 positive predictive value รอยละ 98 และ negative predictive value รอยละ97(19)
Focused Assessment with Sonography for Trauma (FAST)
Ballard RB และคณะ ศกษาผลการท า FAST ปกต ในผปวยอบตเหตแบบ blunt mechanism 1490 คน ทมกระดกสนหลงหก หรอ กระดกเชงกรานหก ในป 1999 พบวา ผล FAST ปกตแตมกระดกเชงกรานหก รอยละ 68.6 และ false negative 13 คนจากผปวยทมกระดกเชงกรานหก 70 คน คดเปนรอยละ 18.6 จงแนะน าวาผปวยทมกระดกเชงกรานหกแบบ pelvic ring-type ใหเอกซเรยคอมพวเตอรชองทองเนองจากมโอกาสพบการบาดเจบไดสง(13)
Friese RS และคณะ ศกษาแบบ retrospective ในป 2007 โดยใช FAST ในการตรวจหาเลอดทออกหลงเยอบชองทอง (hemoperitoneum) ในผปวยกระดกเชงกรานหก พบวา FAST ไมเหมาะในการตรวจยนยนการม

10
เลอดออกหลงเยอบชองทอง เนองจาก มความไว รอยละ 26 ความจ าเพาะ รอยละ96 Positive predictive values รอยละ85 และ negative predictive values รอยละ63 (23)
Daniel C. Cullinane และคณะ ท าsystematic literature ศกษางานวจย 1,432 งานวจยทตพมพชวงป 1999-2010 พบวา หากมกระดกเชงกรานหกแบบเปดสมด ความไวของ FAST ในการตรวจพบความผดปกต รอยละ 75 จงแนะน าใหท าเอกซเรยคอมพวเตอรเพอเพมความแมนย าในการรวจพบการบาดเจบ(20)
CT scan
จากการศกษาของ James W. Davis และคณะในป 2008 พบวาความไวในการท าเอกซเรยคอมพวเตอร รอยละ 98(24) นอกจากนการพบcontrast blush จากเอกซเรยคอมพวเตอรยงชวยวนจฉยเลอดทออกจากหลอดเลอดแดง(20)
Management
Algorithm
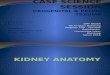
Karim Brohi ไดเสนอแนวทางการดแลผปวย Exsanguinating Pelvis Injuries ป 2008 ใน trauma.org ดงรปท 4 โดยกลาวถงผปวยทมกระดกเชงกรานหกแบบ unstable pelvic fracture และผปวยม hemodynamic instability โดย hemodynamic instability หมายถงผปวยทอยในกลมทไมตอบสนองตอการใหสารน า (non-responders) หรอ ตอบสนองตอการไดรบสารน าเพยงชวคราว (transient responders) กลาวคอ การตอบสนองของระบบหวใจและหลอดเลอดเมอใหสารน า 250-500 mL bolus ซงถาหากพบวาผปวยยงมเลอดออกอยางตอเนอง หรอ ผปวยไมตอบสนองตอการใหสารน า แนะน าใหดแลผปวยแบบ permissive hypotension strategy จนกวาสามารถควบคมเลอดออกได นอกจากนสารน าทใหแนะน าใหเลอด รวมถง clotting factors และหลกเลยงการให crystalloid fluid

11
การเอกซเรยคอมพวเตอรนน หากน าผปวย hemodynamic instability ไปเอกซเรยคอมพวเตอรนนจะท าใหชอคนานขน ผปวยมโอกาสเสยชวตมากขน แตหากผปวย hemodynamic stable จะน าผปวยไปเอกซเรย คอมพวเตอรหรอไมนน ตองพจารณาจากระยะทางทใชในการเดนทางไปเอกซเรยคอมพวเตอร ระยะเวลาในการ
ท าเอกซเรยคอมพวเตอร และความเชยวชาญของทมแพทยทดแลผปวย สวนผปวยทตอบสนองตอการใหสารน า (volume responder) สามารถพจารณาเอกซเรยคอมพวเตอรได และไมใชแนวทางนในการดแลผปวย
กระดกเชงกรานหกมกมประวต high mechanism injury มกมการบาดเจบของอวยวะหลายระบบ การเสยเลอดในผปวยกระดกเชงกรานหกอาจมาจากผวกระดกทหก การบาดเจบของหลอดเลอดด า หรอ หลอดเลอดแดง ดงนนหากผปวยมภาวะชอคแนะน าใหดแลผปวยแบบมการบาดเจบของหลอดเลอดรวมดวย ดวยการใหเลอดและสวนประกอบของเลอดอยางเพยงพอ (massive blood transfusion) ปองกนภาวะ coagulopathy และ hypothermia
รปท4 แนวการดแลผปวยทมกระดกเชงกรานหกและ hemodynamic instability (Karim Brohi)

12
การใส Pelvic binder ชวยลดเลอดออกได โดยทวไปแลว Karim Brohi แนะน าใหใสจนกวาจะสามารถยดตงกระดกได (Permanent pelvic fixation)
กอนจะน าผปวยไปท า angiogram หรอ embolization ควรประเมนสาเหตเลอดออกทอวยวะอนนอกเหนอจากกระดกเชงกรานหก เชนการท า FAST หรอ DPL โดยหากพบเลอดออกจากสาเหตอนหรอ ตองรอท า angiogram นานกวา 30 นาทหรอ กระดกเชงกรานหกแบบเปด แนะน าใหน าผปวยเขาหองผาตด เพอหามเลอดในต าแหนงทเลอดออก ท า Preperitoneal pelvic packing และ distal aortic compression (at the bifurcation) +/- ligation of the internal iliac arteries
กระดกเชงกรานหกมกมการบาดเจบตอหลอดเลอด internal iliac artery ดงนนการท า angiogram จงมกจะ embolization internal iliac artery
ใหการรกษาผปวยใน intensive care unit (ICU) และท าเอกซเรยคอมพวเตอรเพอประเมนชนดของกระดกเชงกรานหก และอาจเอกซเรยสมองในกรณทมการบาดเจบตอศรษะ
หลงจากท า pelvic packing หรอ angiogram แลวหากผปวยม hemodynamic stable และการะดกเชงกรานหกแบบ open book ใหท า external fixation
นอกจากนจากการประชม the First Italian Consensus Conference ในป2013 เสนอแนวทางดแลผปวยกระดกเชงกรานหกทม hemodynamic unstable ดงรปท5

13
รปท5 การดแลผปวยกระดกเชงกรานหกและ hemodynamic unstable (Stefano Magnone และคณะ)
Pelvic binder
การท าควรท าใหคม greater trochanters แตไมสงกวา iliac crests ดงรปท 6 เพอให pelvic ring คงตวไมขยบไปมาชวยลดเลอดทออกจากผวกระดกทหก แตไมสามารถหามเลอดทออกจากหลอดเลอดแดงได
รปท 6 ต าแหนงทเหมาะสมของ pelvic binder

14
Bonner TJ ศกษา Accurate placement of a pelvic binder improves reduction of unstable fractures of the pelvic ring ในป 2011 จากการทบทวนภาพเอกซเรย 172 ภาพ พบวา ต าแหนงของอปกรณอยท greater trochanters รอยละ 50 และอยในต าแหนงทสงเกนไป รอยละ 39 ท าใหความแตกตางของรอยหกระหวางใสในต าแหนงทสงเกนไปทยบกบต าแหนงทเหมาะสม 2.8 เทา (p < 0.01)(25)
Preperitoneal pelvic packing (PPP)
เลอดทออกจากกระดกเชงกรานหก มาจากการบาดเจบของหลอดเลอดด า รอยละ 80-90 หลอดเลอดแดง รอยละ 10-20
ป 1995 Pohlemann และคณะ น าเสนอวธการท า retroperitoneal pelvic packing ดงรปท 7 ในผปวยทมกระดกเชงกรานหกแบบ type C จ านวน 19 คน โดยยดกระดกทหกแบบ pelvic C-clamp และท า retroperitoneal pelvic packing ควบคมเลอดทออกจากหลอดเลอดด าได รอยละ 73.7 ซงผปวยกลมนม mortality rate รอยละ 58 (26)
ขนตอนการท า Retroperitoneal packing ดงรปท 8 (27)
- Open abdominal wall
o A midline incision from the umbilicus to the symphysis is made.
o The abdominal musculature is divided until the peritoneum is reached without opening the peritoneum
o Manually dissect the retroperitoneal space down into the pelvic space along the pelvic bones
- Access to the retroperitoneal space in the left pelvic area is made.
o The left hand pushes the peritoneum and intestines medial and cranial.
o Swabs are placed into the newly created space with the right hand. (A haematoma would have dissected this space)

15
- Packing the swab
o The first is placed posteriorly just below the sacro-iliac joint o The second sponge is placed anteriorly to the first (in the middle of the pelvic brim) o The third sponge is placed in the retropubic space, deep, and lateral to the bladder
o When one side is completed, the bladder is retracted laterally toward that side o The other side is packed
รปท 7 ขนตอนการท า retroperitoneal pelvic packing
Pohlemann, T. et al. The technique of packing for control of hemorrhage in complex pelvic fractures.
Tech. Orthop., 9: 267-270, 1995.

16
รปท 8 Retroperitoneal packing (27)
Stefano Magnone และคณะ ไดรายงานผลการประชม the First Italian Consensus Conference ในป2013 เกยวกบกระดกเชงกรานหกในผปวยอบตเหตสรปวา PPP สามารถควบคมเลอดทออกไดดเมอใชวธ salvage technique รวมกบการท า external fixation และ emergent angiography(28)
External fixation (EF)
External fixation ใชในการยดตงกระดกเชงกรานทหกแบบ unstable pelvic ring ในรปท 9 ม 2 วธ คอ external fixator ใชยดตงกระดกเชงกรานหกชนด B ตาม OTA classificationและ pelvic C-clamp ใชยดตงกระดกทหกชนด unstable C(29)
รปท 9 External fixation
Anterior or posterior EF เปนหตถการทสามารถท าไดทงในหองฉกเฉนและหองผาตด ในผปวยทม hemodynamic unstable และกระดกเชงกรานหกแบบ unstable pelvic fracture เพอชวยลดเลอดทออกจากผวกระดกทแตก และหลอดเลอดด า(28)
Bach et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2008 16:4

17
Indication
- Anterior pelvic instability - Open anterior pelvic fracture - Pelvic fracture with multiple trauma, especially intraabdominal injuries and requiring open
exploration, and initial stabilization tool of a staged method for definitive pelvic fixation
Contraindications
- Pelvic fracture though the iliac wing - Acetabulum fracture that need open reconstruction
Relative contraindication
- Pure vertical displacement of both SI joints - Posterior unstable fracture of pelvis, especially those with vertical translation (29)
Angiography
รปท 10 Angiography

18
Stefano Magnone แนะน าใหท า angiogram และ/หรอ embolization ดงแสดงในรปท 10 ในผปวยกระดกเชงกรานหกทม hemodynamic unstable และหากหลงท ายงมเลอดออกอก แนะน าใหท า angiogram และ/หรอ embolization อกครง นอกจากนในผปวยกระดกเชงกรานหกท hemodynamic stable แตเหนเลอดออกจากหลอด
เลอดแดงในเอกซเรยคอมพวเตอรกแนะน าใหท า angiogram และ/หรอ embolization เชนเดยวกน(28)
M. W. Barentsz ในป 2011 ท า angio-embolization ผปวยกระดกเชงกรานหก 19 คน hemodynamic unstableกอนท าembolization รอยละ 53 พบวาม success rate รอยละ 74 จงแนะน าใหท า embolization ในผปวยกระดกเชงกรานหกหลงทม hemodynamic unstable หลงจากผาตดและ ยงมเลอดออกอยทเหนไดจากเอกซเรย
คอมพวเตอร (30)
สรป
Exsanguinating pelvic fracture เปนการบาดเจบตอกระดกเชงกรานทมอตราการเสยชวตสง จากการเสยเลอดจากผวกระดกทหก หลอดเลอดแดง หลอดเลอดด า และสมพนธกบการบาดเจบตออวยวะอน ดงนนการดแลผปวยทรวดเรว และถกตอง จะชวยโอกาสรอดชวต แนวทางการควบคมเลอดทออกมหลายวธ ซงตอง
เลอกใชใหเหมาะสมกบผปวยในแตละสถานการณ

19
References
1. Hornez E. Management of exsanguinating pelvic trauma: Do we still need the radiologist? J Visc Surg. 2011 Oct;148(5):e379–e384.
2. Demetriades D, Karaiskakis M, Toutouzas K, Alo K, Velmahos G, Chan L. Pelvic fractures: epidemiology and predictors of associated abdominal injuries and outcomes. J Am Coll Surg. 2002 Jul;195(1):1–10.
3. Ertel W, Eid K, Keel M, Trentz O. Therapeutical Strategies and Outcome of Polytraumatized Patients with Pelvic Injuries A Six-Year Experience: A Six-Year Experience. Eur J Trauma. 2000 Dec;26(6):278–86.
4. Ertel W, Keel M, Eid K, Platz A, Trentz O. Control of severe hemorrhage using C-clamp and pelvic packing in multiply injured patients with pelvic ring disruption. J Orthop Trauma. 2001 Oct;15(7):468–74.
5. Biffl WL, Smith WR, Moore EE, Gonzalez RJ, Morgan SJ, Hennessey T, et al. Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann Surg. 2001 Jun;233(6):843–50.
6. Lustenberger T, Meier C, Benninger E, Lenzlinger PM, Keel MJB. C-clamp and pelvic packing for control of hemorrhage in patients with pelvic ring disruption. J Emerg Trauma Shock. 2011 Oct;4(4):477–82.
7. Hou Z, Smith WR, Strohecker KA, Bowen TR, Irgit K, Baro SM, et al. Hemodynamically Unstable Pelvic Fracture Management by Advanced Trauma Life Support Guidelines Results in High Mortality. Orthopedics [Internet]. 2012 Mar 7 [cited 2014 Aug 11]; Available from: http://www.slackinc.com/doi/resolver.asp?doi=10.3928/01477447-20120222-29
8. Tile null. Acute Pelvic Fractures: I. Causation and Classification. J Am Acad Orthop Surg. 1996 May;4(3):143–51.

20
9. Young JW, Burgess AR, Brumback RJ, Poka A. Pelvic fractures: value of plain radiography in early assessment and management. Radiology. 1986 Aug;160(2):445–51.
10. Anandakumar V, Hussein FK, Varuun B, Zhu R. Predictive parameters for angiography and embolization in the bleeding pelvic fracture. J Clin Orthop Trauma. 2013 Jun;4(2):70–4.
11. Shlamovitz GZ, Mower WR, Bergman J, Chuang KR, Crisp J, Hardy D, et al. How (Un)Useful is the Pelvic Ring Stability Examination in Diagnosing Mechanically Unstable Pelvic Fractures in Blunt Trauma Patients?: J Trauma Inj Infect Crit Care. 2009 Mar;66(3):815–20.
12. Gonzalez RP, Fried PQ, Bukhalo M. The utility of clinical examination in screening for pelvic fractures in blunt trauma. J Am Coll Surg. 2002 Feb;194(2):121–5.
13. Sauerland S, Bouillon B, Rixen D, Raum MR, Koy T, Neugebauer EAM. The reliability of clinical examination in detecting pelvic fractures in blunt trauma patients: a meta-analysis. Arch Orthop Trauma Surg. 2004 Mar;124(2):123–8.
14. Gillott A, Rhodes M, Lucke J. Utility of routine pelvic X-ray during blunt trauma resuscitation. J Trauma. 1988 Nov;28(11):1570–4.
15. Salvino CK, Esposito TJ, Smith D, Dries D, Marshall W, Flisak M, et al. ROUTINE PELVIC X-RAY STUDIES IN AWAKE BLUNT TRAUMA PATIENTS: A SENSIBLE POLICY? J Trauma Inj Infect Crit Care. 1992 Sep;33(3):413–6.
16. Obaid AK, Barleben A, Porral D, Lush S, Cinat M. Utility of plain film pelvic radiographs in blunt trauma patients in the emergency department. Am Surg. 2006 Oct;72(10):951–4.
17. Hilty MP, Behrendt I, Benneker LM, Martinolli L, Stoupis C, Buggy DJ, et al. Pelvic radiography in ATLS algorithms: a diminishing role? World J Emerg Surg. 2008;3(1):11.
18. Hubbard SG. Diagnostic Errors With Peritoneal Lavage in Patients With Pelvic Fractures. Arch Surg. 1979 Jul 1;114(7):844.

21
19. Mendez C, Gubler KD, Maier RV. Diagnostic accuracy of peritoneal lavage in patients with pelvic fractures. Arch Surg Chic Ill 1960. 1994 May;129(5):477–481; discussion 481–482.
20. Cullinane DC, Schiller HJ, Zielinski MD, Bilaniuk JW, Collier BR, Como J, et al. Eastern Association for the Surgery of Trauma Practice Management Guidelines for Hemorrhage in Pelvic Fracture—Update and Systematic Review: J Trauma Inj Infect Crit Care. 2011 Dec;71(6):1850–68.
21. Cullinane DC, Schiller HJ, Zielinski MD, Bilaniuk JW, Collier BR, Como J, et al. Eastern Association for the Surgery of Trauma Practice Management Guidelines for Hemorrhage in Pelvic Fracture—Update and Systematic Review: J Trauma Inj Infect Crit Care. 2011 Dec;71(6):1850–68.
22. Ballard RB, Rozycki GS, Newman PG, Cubillos JE, Salomone JP, Ingram WL, et al. An algorithm to reduce the incidence of false-negative FAST examinations in patients at high risk for occult injury. Focused Assessment for the Sonographic Examination of the Trauma patient. J Am Coll Surg. 1999 Aug;189(2):145–150; discussion 150–151.
23. Friese RS, Malekzadeh S, Shafi S, Gentilello LM, Starr A. Abdominal ultrasound is an unreliable modality for the detection of hemoperitoneum in patients with pelvic fracture. J Trauma. 2007 Jul;63(1):97–102.
24. Davis JW, Moore FA, McIntyre RC, Cocanour CS, Moore EE, West MA. Western Trauma Association Critical Decisions in Trauma: Management of Pelvic Fracture With Hemodynamic Instability: J Trauma Inj Infect Crit Care. 2008 Nov;65(5):1012–5.
25. Bonner TJ, Eardley WGP, Newell N, Masouros S, Matthews JJ, Gibb I, et al. Accurate placement of a pelvic binder improves reduction of unstable fractures of the pelvic ring. J Bone Joint Surg Br. 2011 Nov;93(11):1524–8.
26. Pohlemann T, G??nsslen A, Bosch U, Tscherne H. The Technique of Packing for Control of Hemorrhage in Complex Pelvic Fractures: Tech Orthop. 1994;9(4):267–70.

22
27. Bach A, Bendix J, Hougaard K, Christensen E. Retroperitoneal packing as part of damage control surgery in a Danish trauma centre – fast, effective, and cost-effective. Scand J Trauma Resusc Emerg Med. 2008;16(1):4.
28. Magnone S, Coccolini F, Manfredi R, Piazzalunga D, Agazzi R, Arici C, et al. Management of hemodynamically unstable pelvic trauma: results of the first Italian consensus conference (cooperative guidelines of the Italian Society of Surgery, the Italian Association of Hospital Surgeons, the Multi-specialist Italian Society of Young Surgeons, the Italian Society of Emergency Surgery and Trauma, the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care, the Italian Society of Orthopaedics and Traumatology, the Italian Society of Emergency Medicine, the Italian Society of Medical Radiology -Section of Vascular and Interventional Radiology- and the World Society of Emergency Surgery). World J Emerg Surg WJES. 2014; 9(1):18.
29. Techniques in Orthopaedics: June 2002 - Volume 17 - Issue 2 - pp 221-227 External Fixation for Pelvic Ring Injuries Rubel, Iván F. M.D.; Kloen, Peter M.D.; Borens, Olivier M.D.; Helfet, David L. M.D.
30. Barentsz MW, Vonken EPA, van Herwaarden JA, Leenen LPH, Mali WPTM, van den Bosch MAAJ. Clinical Outcome of Intra-Arterial Embolization for Treatment of Patients with Pelvic Trauma. Radiol Res Pract. 2011;2011:1–7.

23