Embed Size (px)
Citation preview

Prevention of CV Disease with Statins
葉宏一 MD, PhD
馬偕醫學院 醫學系 教授兼主任台北醫學大學 醫學科學研究所 兼任教授
馬偕紀念醫院 內科部 副主任

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

Framingham: HDL-C vs LDL-C as a predictor of CHD risk
0
0.5
1
1.5
2
2.5
3
Ris
k o
f C
AD
ove
r 4
year
s o
f fo
llo
w-u
p*
100 mg/dL160 mg/dL220 mg/dL
LDL-C
*Men aged 50–70
85 mg/dL65 mg/dL
45 mg/dL25 mg/dL
CHD RR
HDL-C
Gordon, Castelli et al. Am J Med 1977;62:707–714

0
2
4
6
8
10
12
14
16
18
Serum Total-C, mmol/L (mg/dL)
Dea
th r
ate
per
1000
men
Data from MRFIT study.Martin MJ et al. Lancet 1986;ii:933–936.
Elevated Cholesterol Levels are Associated with an Increased Risk of CHD Death
3.62(140)
4.14(160)
4.65(180)
5.17(200)
5.69(220)
6.21(240)
6.72(260)
7.24(280)
7.75(300)
n=12866, follow-up mean 7 years

0
5
10
15
20
25
30
35
Serum Total-C, mmol/L (mg/dL)
CH
D m
orta
lity
rate
s (%
)
Northern Europe
Southern Europe,Mediterranean
United States
Serbia
Southern Europe,Inland
Japan
Correlation Between Total-C and CHD Mortality in Men from Seven Countries
Data are from the Seven Countries Study of 12,467 men from Southern European Countries, the USA and Japan.Verschuren WM et al. JAMA 1995;274:131–136.
2.60(100)
3.25(125)
3.90(150)
4.50(175)
5.15(200)
5.80(225)
6.45(250)
7.10(275)
7.75(300)
8.40(325)
9.05(350)

S.E. AsiaChina
90.4
90.4
98.7
89.489.5
93.789.989.497.495.072.594.0
All 9 RF
49.232.520.19.917.9Overall 2
53.828.833.712.423.4Overall 1
50.551.459.67.918.9N. America
47.635.645.412.832.8S. America43.428.961.67.222.8Australia/NZ
67.726.758.021.038.443.835.65.510.022.158.715.937.012.119.4S. Asia74.140.058.317.129.9Africa70.541.626.715.59.7Middle East35.04.928.09.124.5E/C Europe44.638.963.614.922.0W. Europe
Lipids %All PS%Abd Obes %Diab %HTN %Region
NON-LIFESTYLE RISK FACTORS
Yusuf et al. Lancet, 2004
INTERHEARTPopulation Attributable Risk for 1st MI by Region and Overall

Definition: total cholesterol > 240 mg/dl or taking lipid-lpwering drugs
Data from Taiwan 3H survey
Prevalence of Hypercholesterolemia in Taiwan
高總膽固醇比例
Age

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

Disease progression
PHASE I: Initiation PHASE II: Progression PHASE III: Complication
Atherosclerosis and Thrombosis

Adapted from Fan J, Watanabe T. J Atheroscler Thromb. 2003;10:63–71.
Monocyte
Induction of adhesionmolecules and chemotaxis
AdhesionVCAM-1ICAM-1P-selectinE-selectin
MigrationMCP-1CCR-2oxLDL
oxidation
CytokinesMMPsEndothelin-1
Endothelialcells
Smooth muscle cells
Inti
ma
Internal elastic lamina
Lu
men
CD36SR-A
Differentiation(GM-CSF)
MacrophageFoam cell
T lymphocyte
CD40
IFN-gamma
LDL, β-VLDL, Lp(a)
Development of an Atheromalipid + inflammation

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

*Selective inhibitor of intestinal cholesterol absorption
Adapted from 1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486–2497. 2. Ezetrol (ezetimibe) product information. WPC 072005. Merck Sharp and Dohme. NSW, Australia. 2006. 3. Nippon Rinsho. 1994 Dec;52(12):3279-84.
↓ 18%
↓ 15–30%
↓ 8%Ezetimibe*2
No change or increase
Bile acid sequestrants1
↑ 1%
↑ 3–5%
↓ 18–55% ↓ 7–30%Statins1 ↑ 5–15%
↓ 5–20% ↓ 20–50%Fibric acids1 ↑ 10–20%
↓ 5–25% ↓ 20–50%Nicotinic acid1 ↑ 15–35%
LDL-C effect
Triglyceride effectDrug class/agents
HDL-C effect
↓ 10–17% No changeProbucol3 ↓ up to 40%
Impact of Existing Drug Therapies on Lipid Parameters

HMG-CoAHMG-CoAreductasereductase
AcetylCoA
HMG-CoA
Mevalonate Farnesylpyrophosphate
Squalene Cholesterol
Farnesylatedproteins
Dolichol
E,E,E-Geranylgeranylpyrophosphate
Geranylgeranylatedproteins
Ubiquinones
Rasprotein
Farnesyl-transferase
Cholesterol Biosynthesis Pathway

HMG-CoA Reductase inhibitirors
TXA2 t-PAPAI-1
+
RhoA
N0
SMChypertrophy
Vascularinflammation
Endothelialdysfunction
hs-CRPMMPsTF Adhesion molecule
ROS
ET-1
RhoARac1 AT1 receptor
Atherosclerosis Hypertension
Cardiovascular Diseases
Plaquestability
Thrombotic effect
Platelet activatin
SMCproliferation Vasoconstriction
Macrophage growth
Takemoto and Liao, 2001

Double dose of statins results in ~6% reduction of LDL
Change in LDL-C From Baseline (%)0 -10 -20 -30 -40 -50 -60
10mg*
-5 -15 -25 -35 -45 -55
20mg**
40mg†
10mg
20mg
80 mg
10mg
20mg
40mg
80mg
10mg
20mg
40mg
RosuvastatinAtorvastatinSimvastatinPravastatin
40mg
*P<.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg.**P<.002 vs atorvastatin 20, 40 mg; simvastatin 20, 40, 80 mg; pravastatin 20, 40 mg.†P<.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg.Adapted from Jones et al. Am J Cardiol 2003;92:152–160.
The STELLAR Trial
STELLAR = Statin Therapies for Elevated Lipid Levels Compared Across Doses to Rosuvastatin.

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

Risk factors: FHx, HTN, smoking, male ≥45, female ≥55, HDL-C <40 mg/dL
ATP III: Lipid-Lowering Treatment Guidelines

Reimbursement guidelines from BNHI, Taiwan
血脂異常之
起步治療準則血脂濃度
≧2 個危險因子
( 如附註二 )
TC/HDL-C>5 或
HDL-C<40mg/dl 治療目標
有
心
血
管
疾
病
患
者
同時予以非藥物治療
TC 200mg/dl≧ × × <160mg/dl(87/7/1)
LDL-C 130mg/dl≧ × × ≦100mg/dl(87/7/1)
TG 200mg/dl ≧( 需同時合併有 TC/HDL-C>5 或是 HDL-C <40mg/dl)
× ˇ < 150mg/dl(87/7/1)
冠狀動脈粥狀硬化 , 腦血管病變 , 周邊血管粥狀硬化
*
*
或
糖
尿
病
(ˇ)需符合此項條件 (×)不需符合此項條件 周邊血管粥狀硬化有缺血性症狀且經血管都卜勒超音波或血管攝影證實者

全民健保降血脂藥物給付規定(畫線部分為91/9/1 後適用)
血脂異常之
起步治療準則血脂濃度
≧2 個危險因子
( 如附註二 )
TC/HDL-C>5 或
HDL-C<40mg/dl 治療目標
無
心
血
管
疾
病
患
者
有下列情況之一時
,應給予
TC
LDL-C
≧200mg/dl
≧240mg/dl
≧130mg/dl
≧160mg/dl
TG 200mg/dl≧
( 需同時合併有 TC/HDL-C>5 或是HDL-C<40mg/dl)
ˇ
×
ˇ
×
×
×
×
×
<200mg/dl
<240 mg/dl
<130mg/dl
<160mg/dl
× ˇ <200mg/dl(87/4/1)
︵
如
附
註
一
︶
三至六個月非藥物治療
*
*高血壓 , 糖尿病 , 男≧ 45歲 , 有早發性冠心病家族史 , 女≧ 55歲或停經沒有雌激素療法, 吸菸

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

Statin Clinical Trials
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statins
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

Statin Clinical Trials
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statin
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

On-treatment LDL-C & CHD Events in Statin Trials
Adapted from Rosensen, Exp Opin Emerg Drugs 2004;9:269; LaRosa J et al, N Engl J Med, 2005;352:1425
NCEP2004
ASCOT - PBO
ASCOT - Rx
PROVE-IT - PRAPROVE-IT - ATV80
TNT - ATV10TNT - ATV80
AFCAPS - Rx
HPS - Rx WOSCOPS - PBO
AFCAPS - PBO
AFCAPS - Rx
WOSCOPS - Rx
4S - Rx
LIPID - Rx
4S - PBO
CARE - Rx
LIPID - PBO
CARE - PBO
0
10
20
30
40(1.0)
60(1.6)
80(2.1)
100(2.6)
120(3.1)
140(3.6)
160(4.1)
180(4.7)
Secondary Prevention
Primary Prevention
200(5.2)
Eve
nt
rate
(%
)
LDL-C achieved mg/dL (mmol/L)
HPS - PBO
HPS - Rx
NCEP 2001Eur Joint 2003

Cholesterol Treatment Trialists’ CollaborationCholesterol Treatment Trialists’ Collaboration
Lancet Vol 376 November 13, 2010Lancet Vol 376 November 13, 2010Lancet Vol 376 November 13, 2010Lancet Vol 376 November 13, 2010
• randomised trials involving at least 1000 participants and at least 2 years’ treatment duration
• more versus less intensive statin regimens (5 trials; 39612 individuals; median follow-up 5.1 years)
• statin versus control (21 trials; 129526 individuals; median follow-up 4.8 years).

Cholesterol Treatment Trialists’ CollaborationCholesterol Treatment Trialists’ Collaboration

MVE per 1.0 mmol/L reduction in LDL-C, by baseline prognostic factor
MVE per 1.0 mmol/L reduction in LDL-C, by baseline prognostic factor

Cause-specific mortality per 1.0 mmol/L reduction in LDL-C
Cause-specific mortality per 1.0 mmol/L reduction in LDL-C

Site-specific cancer incidence per 1.0 mmol/L reduction in LDL-C
Site-specific cancer incidence per 1.0 mmol/L reduction in LDL-C

On-treatment LDL-C & CHD Events in Statin Trials
Adapted from Rosensen, Exp Opin Emerg Drugs 2004;9:269; LaRosa J et al, N Engl J Med, 2005;352:1425
NCEP2004
ASCOT - PBO
ASCOT - Rx
PROVE-IT - PRAPROVE-IT - ATV80
TNT - ATV10TNT - ATV80
AFCAPS - Rx
HPS - Rx WOSCOPS - PBO
AFCAPS - PBO
AFCAPS - Rx
WOSCOPS - Rx
4S - Rx
LIPID - Rx
4S - PBO
CARE - Rx
LIPID - PBO
CARE - PBO
0
10
20
30
40(1.0)
60(1.6)
80(2.1)
100(2.6)
120(3.1)
140(3.6)
160(4.1)
180(4.7)
Secondary Prevention
Primary Prevention
200(5.2)
Eve
nt
rate
(%
)
LDL-C achieved mg/dL (mmol/L)
HPS - PBO
HPS - Rx
NCEP 2001Eur Joint 2003

Tx based on hsCRP levelTx based on hsCRP level

JUPITER
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statin
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

JUPITERJustification for the Use of Statins in Primary Prevention: a
n Intervention Trial Evaluating Rosuvastatin
• a randomized, double-blind, placebo-controlled primary prevention trial (26 countries)
• studied over 17,802 patients (men>= 50 yrs; women>= 60 yrs; 6,801 women; 5,577 with metabolic syndrome) without evidence of cardiovascular disease and low to normal LDL-C (<130 mg/dl, median 108 mg/dl), but elevated C-reactive protein (hs-CRP 2 mg/L)≧ .
• rosuvastatin (20 mg) vs placebo
ACCACC 2008 2008


JUPITERPrimary Trial Endpoint : MI, Stroke, UA/Revascularization, CV Death
Placebo 251 / 8901
Rosuvastatin 142 / 8901
HR 0.56, 95% CI 0.46-0.69P < 0.00001
Number Needed to Treat (NNT5) = 25
- 44 %
0 1 2 3 4
0.0
00
.02
0.0
40
.06
0.0
8
Cu
mu
lati
ve In
cid
ence
Number at Risk Follow-up (years)
Rosuvastatin
Placebo
8,901 8,631 8,412 6,540 3,893 1,958 1,353 983 544 157
8,901 8,621 8,353 6,508 3,872 1,963 1,333 955 534 174
Ridker et al NEJM 2008

JUPITERDual Target Analysis: LDLC<70 mg/dL, hsCRP<2 mg/L
LDL > 70 mg/dLand / or
hsCRP > 2 mg/LHR 0.64 (0.49-0.84)
LDL < 70 mg/dL and
hsCRP < 2 mg/L HR 0.35 (0.23-0.54)
Placebo HR 1.0
(referent)
P < 0.0001
0 1 2 3 4
0.00
0.02
0.04
0.06
0.08
Cu
mu
lati
ve
In
cid
en
ce
Number at Risk Follow-up (years)
RosuvastatinPlacebo
7,716 7,699 7,678 6,040 3,608 1,812 1,254 913 508 1457,832 7,806 7,777 6,114 3,656 1,863 1,263 905 507 168

Anti-inflammatory effects of LDL-C reducion on hsCRP
• >90% of the reduction in CRP was directly associated with the magnitude of LDL cholesterol reduction, with no difference between high-dose statins or statin-ezetimibe combinations
Kinlay S. JACC 2007

ANDROMEDA=A raNdomised, Double-blind, double-dummy, multicentre, phase IIIb, parallel-group study to compare the ANDROMEDA=A raNdomised, Double-blind, double-dummy, multicentre, phase IIIb, parallel-group study to compare the efficacy and safety of Rosuvastatin (10 mg and 20 mg) and atOrvastatin (10 Mg and 20 mg) in patiEnts with type II DiAbetes efficacy and safety of Rosuvastatin (10 mg and 20 mg) and atOrvastatin (10 Mg and 20 mg) in patiEnts with type II DiAbetes mellitus; hsCRP=high-sensitivity C-reactive protein; RSV=rosuvastatin; ATV=atorvastatinmellitus; hsCRP=high-sensitivity C-reactive protein; RSV=rosuvastatin; ATV=atorvastatin*p<0.05 vs ATV at same time point; *p<0.05 vs ATV at same time point; ‡‡p<0.001 vs baselinep<0.001 vs baseline
Betteridge DJ et al. Betteridge DJ et al. Am J CardiolAm J Cardiol 2007 in press ;Betteridge DJ et al. 2007 in press ;Betteridge DJ et al. Atheroscler Suppl Atheroscler Suppl 2005; 6: 102 Abs W16-P-0072005; 6: 102 Abs W16-P-007Betteridge DJ et al. EAS April 2005. Poster presentationBetteridge DJ et al. EAS April 2005. Poster presentation
ANDROMEDA – reduction in hsCRP in patients with baseline CRP ≥2 mg/L
Median Median
changechangefrom from
baselinebaseline(%)(%)
00
––2020
––4040
––6060
––3232
––5252
––4343
n=120n=120 n=121n=121 n=115n=115 n=112n=112
––4444
**‡‡
‡‡
‡‡
‡‡
8 weeks 8 weeks
RSV 10 mg RSV 10 mg ATV 10 mg ATV 10 mg
16 weeks 16 weeks
RSV 20 mg RSV 20 mg ATV 20 mg ATV 20 mg

The history of JUPITER
• 2008 Nov, AHA: JUPITER (paper in NEJM)
• 2009 Feb, ISC : Stroke (09 Dec. paper in circulation)
• 2009 Mar, ACC: VTE / Dual treatment target
• 2009 Sep, ESC: Elderly
• 2009 Sep: NNT (Circulation Cardiovascular Quality and Outcomes. 2009)
• 2009 Nov, AHA: Women / IFG / Very low LDL-C
• 2009 Dec, news: FDA voted

Venous thromboembolismVenous thromboembolism

JUPITERTotal Venous Thromboembolism
0 1 2 3 4
0.0
00
0.0
05
0.0
10
0.0
15
0.0
20
0.0
25
Cu
mu
lati
ve In
cid
ence
Number at Risk Follow-up (years)
Rosuvastatin
Placebo
8,901 8,648 8,447 6,575 3,927 1,986 1,376 1,003 548 161
8,901 8,652 8,417 6,574 3,943 2,012 1,381 993 556 182
HR 0.57, 95%CI 0.37-0.86P= 0.007
Placebo 60 / 8901
Rosuvastatin 34 / 8901
- 43 %
Glynn et al NEJM 2009
Ridker PM et al on behalf of the JUPITER Trial Study Group N Engl J Med 2009;360

Systolic Heart FailureSystolic Heart Failure

CORONA and GISSI-HF
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statin
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

CORONA
NEJM 2007
Rosuvastatin in older patients with systolic heart failure
• Patients (≥ 60 yr; n=5011) with systolic heart failure of ischemic cause (EF < 0.4, NYHA II-IV)
• 10 mg rosuvastatin daily• LDL-C 45%; hsCRP 37% • Median follow-up of 32.8 m
onths• Primary outcome: death fr
om CV causes, non-fatal MI, and nonfatal stroke

GISSI-HF / Statin
LANCET 2008
Rosuvastatin in patients with chronic heart failure
• Patients (68±11 yr; n=4631) with heart failure (NYHA II-IV)
• 10 mg rosuvastatin daily• LDL-C 32% (1st yr), 27
% (2nd yr); hsCRP 16% • Median follow-up of 3.9 y
rs, average EF < 0.4, • Primary outcome: death • Secondary outcome: de
ath + CV hospitalization
Death
Death + CV Hospitalization

Stroke / TIAStroke / TIA

SPARCL
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statin
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

SPARCLSPARCLThe Stroke Prevention by The Stroke Prevention by Aggressive Reduction in Aggressive Reduction in
Cholesterol LevelsCholesterol Levels
4731 patients who with a stroke or TIA within 1-6 months before study entry
LDL-C 100 to 190 mg/dl
No known coronary heart disease
80 mg of atorvastatin per day or placebo
NEJM. 2006

High-Dose Atorvastatin after Strokeor Transient Ischemic Attack (SPARCL)
NJEM. 2006
73 mg/dl73 mg/dl
129 mg/dl129 mg/dl

Chronic Kidney DiseaseChronic Kidney Disease

4D, AURORA, SHARP
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statin
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

4D: primary endpoint(cardiac death, nonfatal MI, and stroke)
NEJM 2005
20 mg
RR = 0.92 (95% CI 0.77-1.10)P=0.37

Placebo
AURORA: primary endpointTime to first major CV event
(cardiac death, nonfatal MI, stroke)
No. at risk:
Rosuvastatin 1390 1152 962 826 551 148
Placebo 1384 1163 952 809 534 153
Cumulative incidence of primary endpoint (%)
Years from randomization
Rosuvastatin
HR=0.96 (95% CI 0.84–1.11)P=0.59
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5
NEJM 2009
10 mg

Statin in Diabetic Hemodialysis Patients- post hoc analysis of the AURORA
J Am Soc Nephrol. 2011 May 12. [Epub ahead of print]
32% P=0.008

0 1 2 3 4 5
Years of follow-up
0
5
10
15
20
25
Prop
ortio
n su
fferin
g ev
ent (
%) Risk ratio 0.83 (0.74 – 0.94)
Logrank 2P=0.0022 Placebo
Eze/simv
SHARP: major atherosclerotic eventsCKD grade 3-5

CKD vs. non-CKDHR=1.35 (95% CI 1.18 –1.54)P<0.0001
CKD in TNTCKD grade 2-4
CKD in TNTCKD grade 2-4

Hypolipidemic therapy in prevention of non-fatal MI and coronary revascularization in CKD patients
Hypolipidemic therapy in prevention of non-fatal MI and coronary revascularization in CKD patients
Lancet 2011

Non-fatal non-hemorragic and non-fatal hemorrhagic stroke
Non-fatal non-hemorragic and non-fatal hemorrhagic stroke
Lancet 2011

Cumulative Incidence of CV End Points in CKD patients from JUPITER Study
*Primary end point: non-fatal MI, nonfatal stroke, hospital stay for unstable angina, arterial revascularization, or CV death*Primary end point: non-fatal MI, nonfatal stroke, hospital stay for unstable angina, arterial revascularization, or CV death
1638 1638 1574 1538 1281 1574 1538 1281 871 550 871 550 352 247 129 39 352 247 129 391629 1629 1557 1510 1234 1557 1510 1234 838 838 516 345 243 131 40 516 345 243 131 407259 7054 7259 7054 6871 6871 5256 3020 1407 1000 736 409 118 5256 3020 1407 1000 736 409 118
7269 7061 6840 5272 3033 1447 988 712 400 1347269 7061 6840 5272 3033 1447 988 712 400 134
Follow-up (years)Follow-up (years)
Cu
mu
lati
ve I
ncid
en
ce
Cu
mu
lati
ve I
ncid
en
ce
Primary End Point*
No. at RiskNo. at Risk
00
CKDCKD RosuvastatinRosuvastatinPlaceboPlacebo
No CKDNo CKD RosuvastatinRosuvastatinPlaceboPlacebo
110.000.00
22 33 44
CKD, placeboCKD, placebo
0.050.05
0.100.10
0.150.15
No CKD, placeboNo CKD, placebo
No CKD, rosuvastatinNo CKD, rosuvastatin
CKD, rosuvastatinCKD, rosuvastatin
Ridker PM et al. Ridker PM et al. J Am Coll Cardiol.J Am Coll Cardiol. 2010; 2010;5555(12):1266-1273.(12):1266-1273.

Studies using surrogate marker
ComparatorsStatin vs placebo
- statin alone
- combined with non-statinStatin vs statin
- different statin
- same statin, different dose
- combined with non-statin
End pointsDisease outcomeSurrogate marker

2.7*
Pravastatin
Significant atheroscleroticprogression from baseline
-0.4†
Atorvastatin
No significant change frombaseline; atheroscleroticprogression was stopped
REVERSAL:REVERSAL: Primary end point: % Primary end point: %change in total atheroma volumechange in total atheroma volume
Cha
nge
in T
AV
(%
)
-1
0
1
2
3
*Progression vs baseline (P=0.001); †No change vs baseline (P=0.98)
P=0.02
JAMA. 2004

Example of regression of atherosclerosis with Example of regression of atherosclerosis with rosuvastatin in ASTEROID, measured by IVUSrosuvastatin in ASTEROID, measured by IVUS
BaselineIVUS
Follow-upIVUS
24 monthsrosuvastatin
Atheroma Area10.16 mm2
Lumen Area6.19 mm2
Atheroma Area5.81 mm2
Lumen Area5.96 mm2
Ref: Nissen S et al. JAMA 2006; 295: e-publication ahead of print

Time (years)
Ch
an
ge in
IM
T o
f 12 c
aro
tid
sit
es (
mm
)
-0.01
+0.01
0.00
+0.02
21
+0.03
Pro
gre
ssio
n
Reg
ressio
n
P=NS(CRESTOR vs. zero slope)
Placebo+0.0131 mm/yr
(n=252)
Rosuvastatin 40 mg-0.0014 mm/yr
(n=624)
P<0.0001 (CRESTOR vs. placebo)
Placebo; Change in CIMT (95% CI)
Rosuvastatin 40 mg; Change in CIMT (95% CI)
METEOR primary endpoint:Rate of change of maximum IMT at 12 carotid sites
Rosuvastatin vs placebo
Crouse JR, et al. JAMA 2007;297:(doi:10.1001/jama.297.12.joc70024)

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

Statins – Therapeutic RatioStatins – Therapeutic Ratio
Therapeutic Effects
Adverse Effects
Cardiovascular protection
Muscle
Liver
Drug interactions
Benefit
Risk

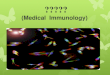
Rhabdomyolysis and % LDL-C ReductionRhabdomyolysis and % LDL-C Reduction
JACCJACC 2007 2007

Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K
Muscle effects - Benefit:Risk CK >10 x ULN: Frequency by LDL-C Reduction
0.0
0.5
1.0
1.5
2.0
2.5
3.0
20 30 40 50 60 70
LDL-C reduction (%)
Occu
rren
ce o
f C
K >
10 ×
ULN
(%
)
Cerivastatin (0.2, 0.3, 0.4, 0.8 mg)
Rosuvastatin (10, 20, 40 mg)
Pravastatin (20, 40 mg)
Atorvastatin (10, 20, 40, 80 mg)
Simvastatin (40, 80 mg)

↑↑Liver Enzymes and % LDL-C ReductionLiver Enzymes and % LDL-C Reduction
JACCJACC 2007 2007

Rate of Elevated Liver Enzymes by Statin Rate of Elevated Liver Enzymes by Statin Dose CategoryDose Category
JACCJACC 2007 2007

Shimada T et al. J Pharmacol Exp Ther 1994;270(1):414.
CYP3A4CYP2D6
CYP2C
CYP1A2CYP2E1
Relative Importance of P450s in Drug Metabolism
CYP450

Potential Drug Interactions3A4
• Simvastatin
• Atorvastatin
• Lovastatin
• Diltiazem
• Clopidogrel
• Amiodarone
• Cimetidine
• Ery/clarithromycin
• Ketoconazole
• Carbamazepine
• St John’s wort
• Grapefruit juice
2C9
• Fluvastatin
• Phenytoin
• Fluconazole
• Warfarin
• Rosuvastatin

No clear difference between statins in terms of diabetes risk
Lancet, Lancet, Published Published Online February 17, 2010Online February 17, 2010

• one additional case of diabetes per 255 patients taking statin therapy for 4 years (12·23 cases per1000 patient-years with statin treatment and 11·25 cases per 1000 patient-years with control therapy).
• Re reduction in major coronary events (coronary heart disease death and non-fat
al myocardial infarction) of 5·4 events per 255 patients treated for 4 years compared with control therapy for a 1 mmol/L reduction in LDLcholesterol concentration.
Lancet 2010; 375: 735–42
: Statins and risk of incident diabetes -a collaborative meta analysis

Content
• Epidemiology
• Pathophysiology
• Pharmacological Treatment
• Guidelines
• Statin clinical trials
• Adverse effects
• Real world practice

REALITY Asia Study: Objectives
• To evaluate lipid-lowering
therapy prescribing patterns
and cholesterol goal
achievement in patients
with and without CHD and
other risk factors in the “real
world” setting in 6 major
Asian countries
Adapted from REALITY Study Protocol.

Cholesterol Goal Attainment in the Real World:
Results: Comparison of Overall Goal Attainment in Europe and Asia
45%
58%
24%
54%
51%
42%
41%
30%
26%
55%
32%
29%
33%
14%
24%
27%
27%
54%
0% 10% 20% 30% 40% 50% 60% 70%
Overall AsiaSingapore
TaiwanMalaysiaThailand
KoreaOverall EU
SwedenFrance
UKNetherlandsSwitzerland
NorwayItaly
GermanySpain
HungaryFinland

Cholesterol Goal Attainment in the Real World: The REALITY ASIA Study
Results: Cholesterol Goal Attainment by Risk and Country
All Patients
32.4%
15.9%
42.4%36.5% 34.9%
66.7%
42.5%
64.2%
74.1%
52.9%
83.2%
63.3%
80.8%87.5% 84.4%
80.9%
31.5%
61.7%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Singapore Taiwan Thailand Malaysia Korea Overall
CHD/diabetic Patients nonCHD with 2 or more risk factors nonCHD with less than 2 risk factors
Approximately 84% of CHD/diabetic patients and 76% of patients overall failed to attain goal.
Curr Med Res Opin. 2008

Pan-Asian CEPHEUS (Pan Asian survey on undertreatment of hypercholesterolemia)
Eur J Cardiovasc Prev Rehabil. 2011

LDL goals of patients
49.1%
32.1%
18.5%
0.3%0%
10%
20%
30%
40%
50%
60%
<70 mg/dl (n=3,557) <100 mg/dl (n=2,325) <130mg/dl (n=1,343) <160 mg/dl (n=25)
% o
f P
atie
nts
79
• Half the patients (49.1%) in the study fulfilled the criteria for the very high risk category (< 70 mg/dl) when stratified as per the 2004 updated NCEP ATP III guidelines.
LDL Goals of Patients

Proportion of patients attaining their 2004 updated NCEP ATP III-recommended LDL-C goals
80
% of Patients attaining their 2004 updated NCEP ATP III* guidelines recommended LDL-C goals
• Overall 49.1% LDL-C goal attainment rate among all patients surveyed across Asia.• Proportion of patients attaining their respective LDL-C goal decreased with increasing cardiovascular
risk.

Percentage of Patients at LDL-C goals recommended by the 2004 updated NCEP ATP
III* guidelines
81
% of Patients at LDL-C goals recommended by 2004 updated NCEP ATP III* guidelines
• For patients in Hong Kong the treatment goal attainment rate was 82.9% while patients in other countries had very low LDL-C attainment rate (31.3 – 52.7%).

Changes in the lipid-lowering drug since first prescribed a drug
82
Changes in the lipid-lowering drug since first prescribed a drug
• For 64.1% of patients, initial treatment remained the same.

Achievement of LDL-C goals among patients
83
Achievement of LDL-C goals among patients
• Rate of LDL-C goal attainment was similar in primary and secondary prevention patients.
Prevention Metabolic Syndrome

Comparison of Pan-Asian CEPHEUS with Pan-European CEPHEUS
84
Point of ComparisonPan-European
CEPHEUSPan-Asian CEPHEUS
Proportion of patients achieving NCEP ATP III targets for LDL-C
57.4% 49.1%
Mean baseline LDL-C concentrations
105±36 mg/dl 144.5 ±45.6 mg/dl
Proportion of patients on statins
90.3% 85.1%

• Only about 50% of patients with high LDL-C achieve goal on current lipid lowering therapies
– Non-compliance– Lack of effective treatment– Fear of high dose titration
• More effective cholesterol-loweringagents are needed to attain LDL-C goals1,2
1Kotseva, K, Wood D, de Backer, G et al. 20012Pearson T et al. 2000
Why Only about 50% of patients with high LDL-C achieve goal ?

Unmet Need
• Even with current therapies, many patients, especially those considered at high and very high risk, are not achieving the goals
• Special populations, such as those FH and other forms of severe hypercholesterolemia, do not achieve even old goals
• Perhaps the largest need, however, is for the growing number of patients who are statin adverse

Statin AdversePrimo study (7924 hyperlipidemic patients)
a Percentage values relative to the total number of patients who had or did not have muscular symptoms.
b Odds ratios were calculated using pravastatin as the reference.c P values were determined by Pearson’s Chi-square test.
Cardiovasc Drugs Ther 2005

Conclusion• The beneficial effect of statin is mainly in preve
ntion of CHD caused by atherosclerosis• Statin is not effective in reducing CV events in
patients with systolic HF• Statin is effective in reducing atherosclerotic C
V events in patients with CKD• Hypercholesterolemia is prevalent in Taiwan; h
owever, cholesterol goal attainment is not satisfactory
• A substantial number of patients with hypercholesterolemia can not tolerate statins

Thanks for your attention
Mackay Medical College馬偕醫學院