Embed Size (px)
Citation preview

Primary OsteoarthritisPrimary Osteoarthritis
Primary Osteoarthritis (OA): Outline Epidemiology Classification Pathogenesis Genetics Clinical Features Imaging Management
What is OA? “ . . . a heterogeneous group of conditions that lead to
joint symptoms and signs which are associated with defective integrity of articular cartilage, in addition to related changes in the underlying bone and at the joint margins.”
Associated with aging but not due to aging OA ≠ degenerative joint disease
Involves dynamic biochemical/-mechanical & cellular processes Can be defined pathologically, radiographically or clinically
Altman RD, et al. Arthritis Rheum 1986; 29:1039-1049.
Epidemiology OA is a condition found worldwide
Most common type of arthritis Affected 21 million Americans in 1990 Projected to affect 25% of the population (67 million) by 2030
Accounts for more functional limitation, work loss and physical disability than any other chronic disease
Due to its effect on ambulation/mobility, OA of the knee and hip is associated with considerable medical costs Costs range from 1-3% of GNP in developed countries 478,000 total knee replacements and 234,000 total hip replacements in 2004 Aggregate expenditures increased by $185.5 billion per year in 2007
Due to our aging population and the epidemic of obesity, the burden is only expected to increase
Kotlarz H et al. Arthritis Rheum 2009; 60(12):3546-3553.
Epidemiology Incidence and prevalence higher in women than men,
especially after age 50
Racial/ethic differences have been recognized Absence of hip OA in Asians Differences between African- and Caucasian-Americans
Many persons in the population have joint symptoms without x-ray changes and vice versa
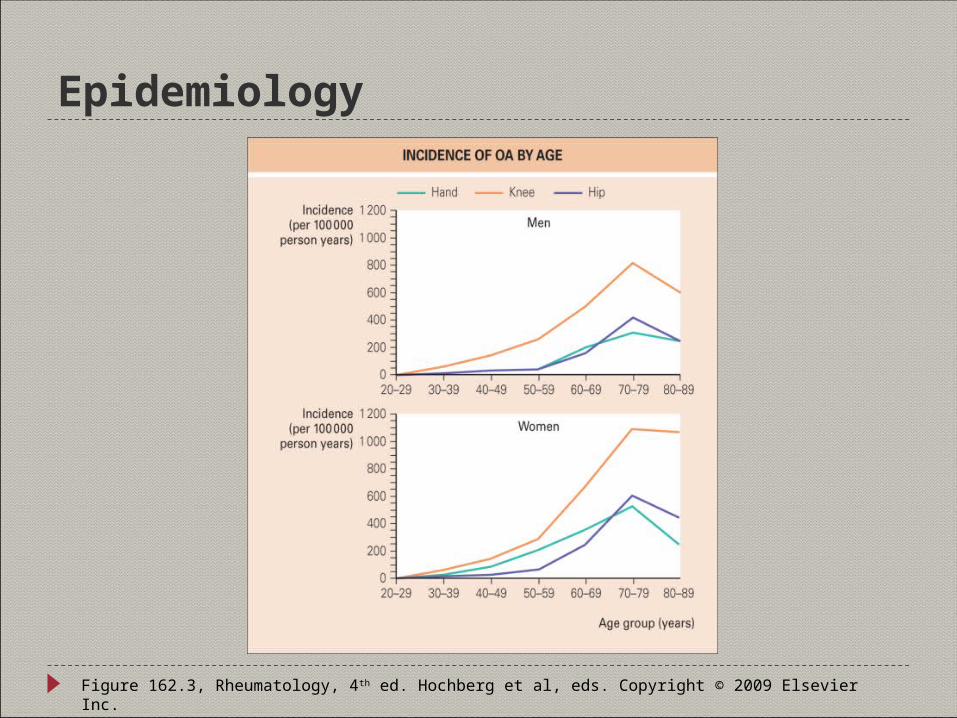
Epidemiology
Figure 162.3, Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
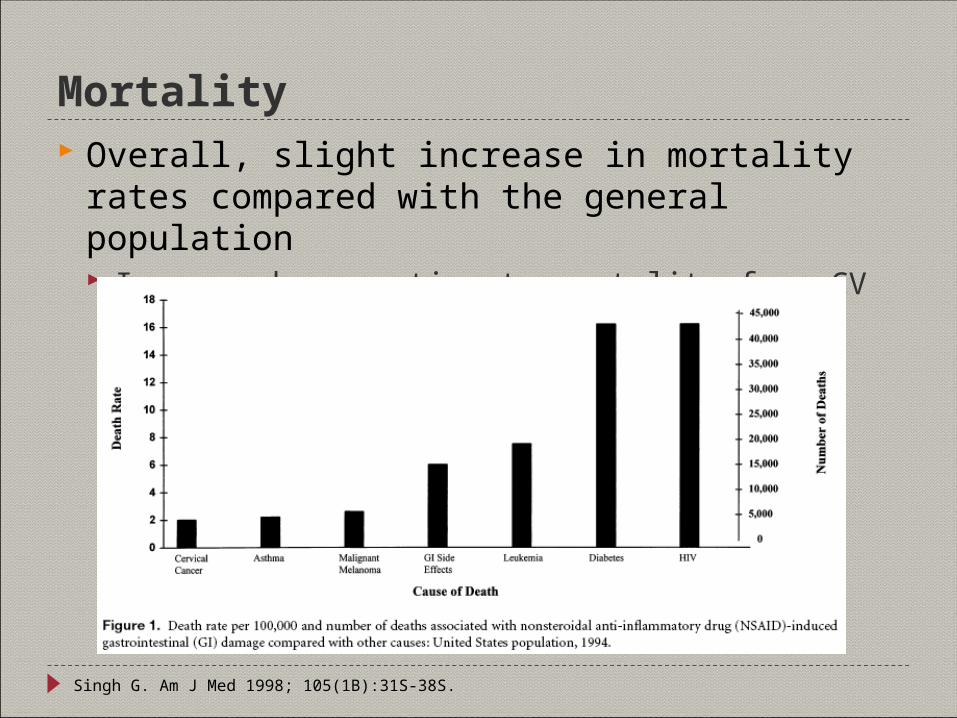
Mortality Overall, slight increase in mortality rates compared with
the general population Increased proportionate mortality from CV and GI conditions
Singh G. Am J Med 1998; 105(1B):31S-38S.
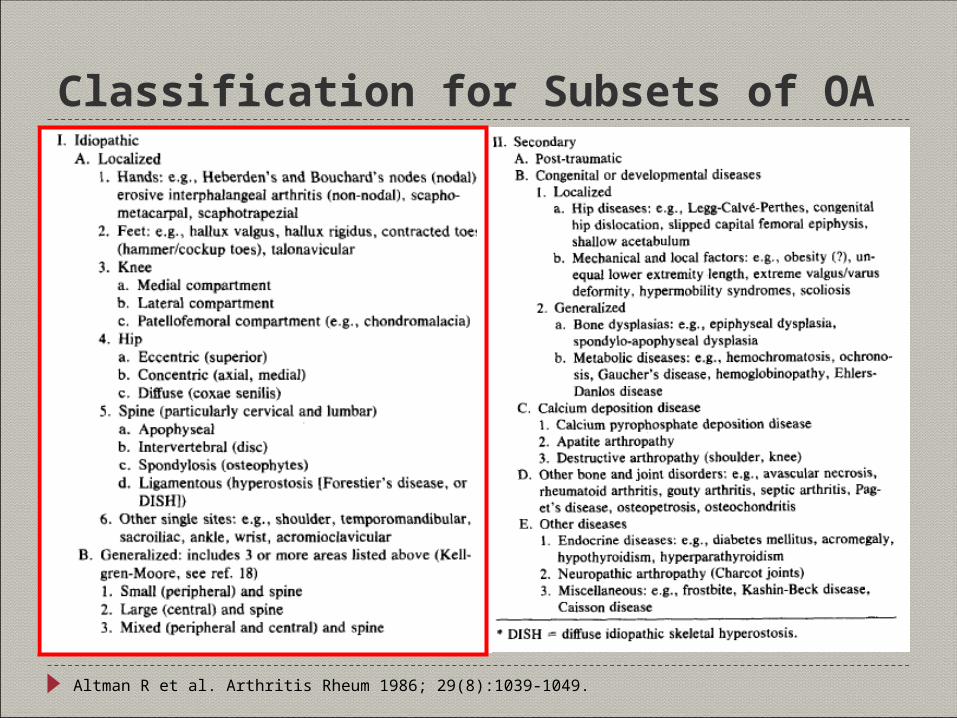
Classification for Subsets of OA
Altman R et al. Arthritis Rheum 1986; 29(8):1039-1049.
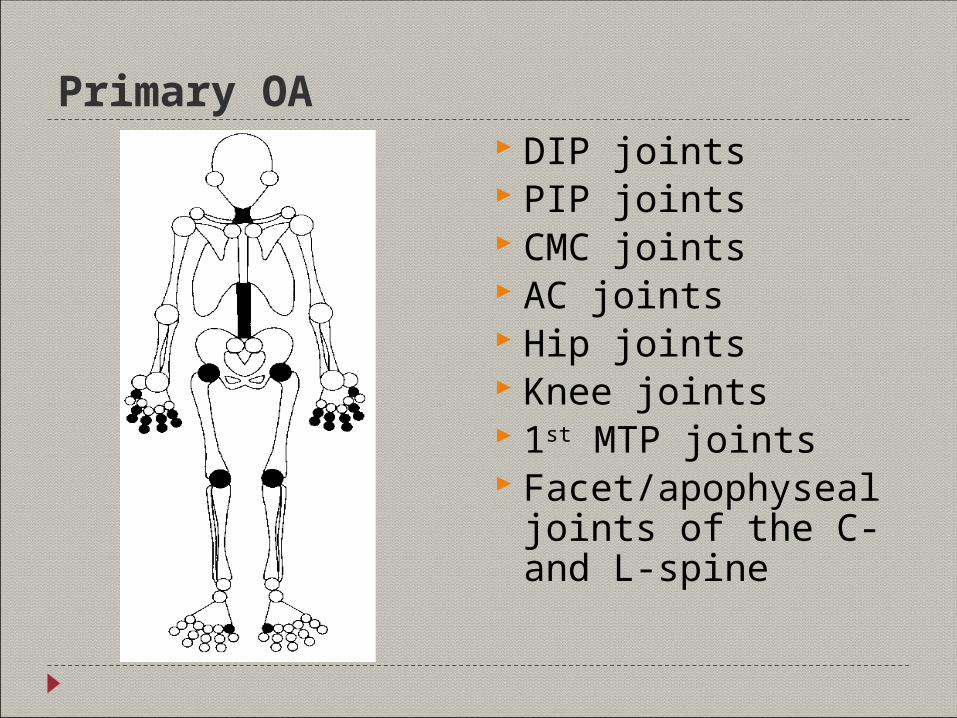
Primary OA DIP joints PIP joints CMC joints AC joints Hip joints Knee joints 1st MTP joints Facet/apophyseal joints
of the C- and L-spine
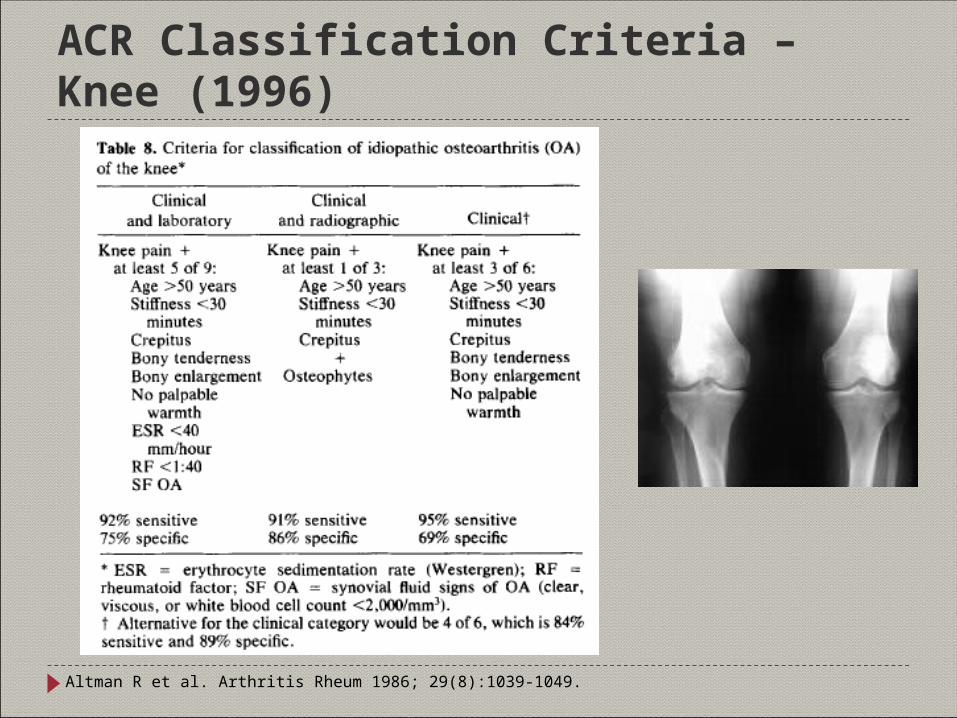
ACR Classification Criteria – Knee (1996)
Altman R et al. Arthritis Rheum 1986; 29(8):1039-1049.
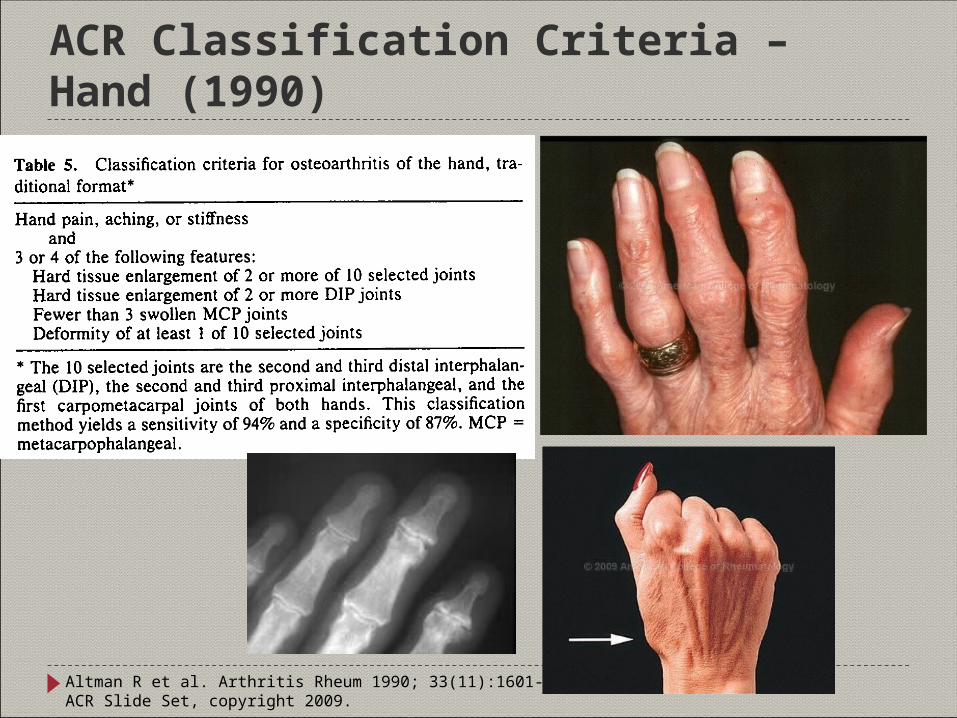
ACR Classification Criteria – Hand (1990)
Altman R et al. Arthritis Rheum 1990; 33(11):1601-1610.ACR Slide Set, copyright 2009.
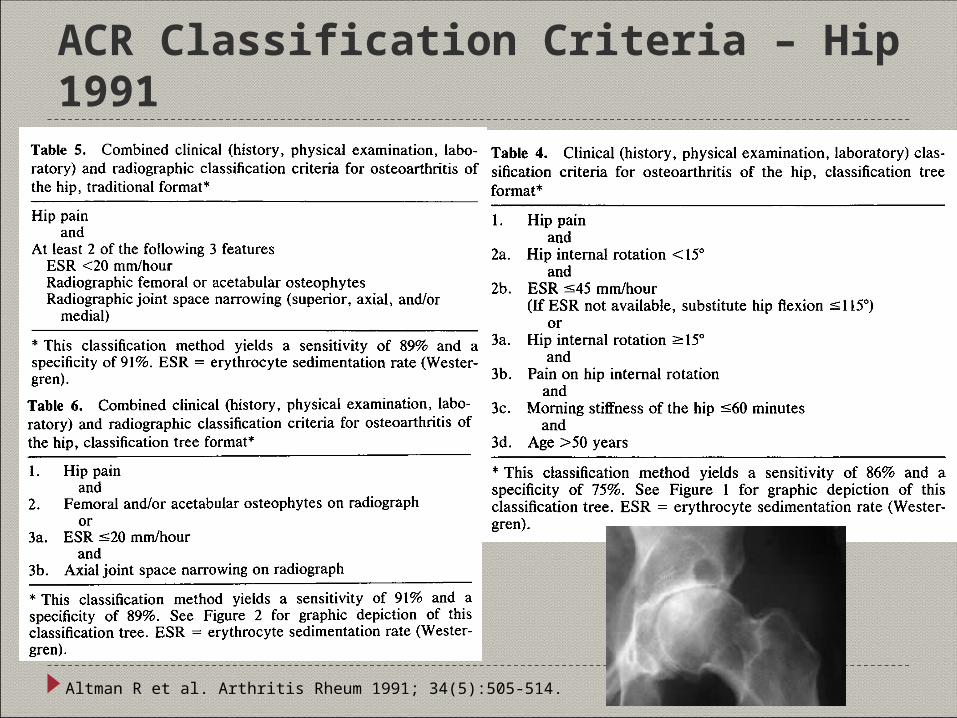
ACR Classification Criteria – Hip 1991
Altman R et al. Arthritis Rheum 1991; 34(5):505-514.
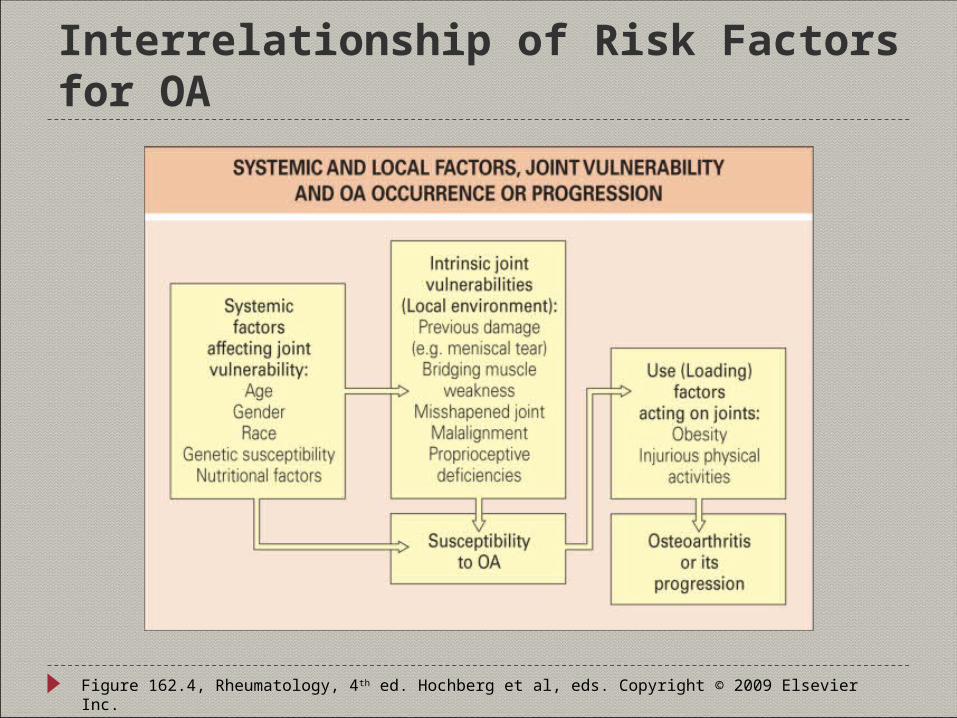
Interrelationship of Risk Factors for OA
Figure 162.4, Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
Genetic Predisposition to OA Familial aggregation
Generalized OA (BLSA, GARP) 2-8 fold increase in risk for siblings for TJR for OA
High heritability in twin studies Candidate genes
AGC1, ASPN, COL9A2, COL9A3, COL11A2, ESR1, FZRB, IL1A, IL1PN, PTGS2 and VDR genes
Genome wide linkage analyses Areas on chromosomes 2, 6 and 11
Valdes AM and Spector TD. Med Clin N Am 2009; 93(1):45-46.
Etiopathogenesis of OA Complex
Changes in bone and cartilage integral components of process Inflammation plays an important role in the production of
symptoms and signs as well as the progression of disease
Affects all of the tissues of the joint
“OA can be thought of as a mechanically driven but chemically mediated active disease process of joints in which attempted (or aberrant) repair is one of the dominant aspects of the process”
Dieppe P. Stepping away from OA. 1999 NIH conference.
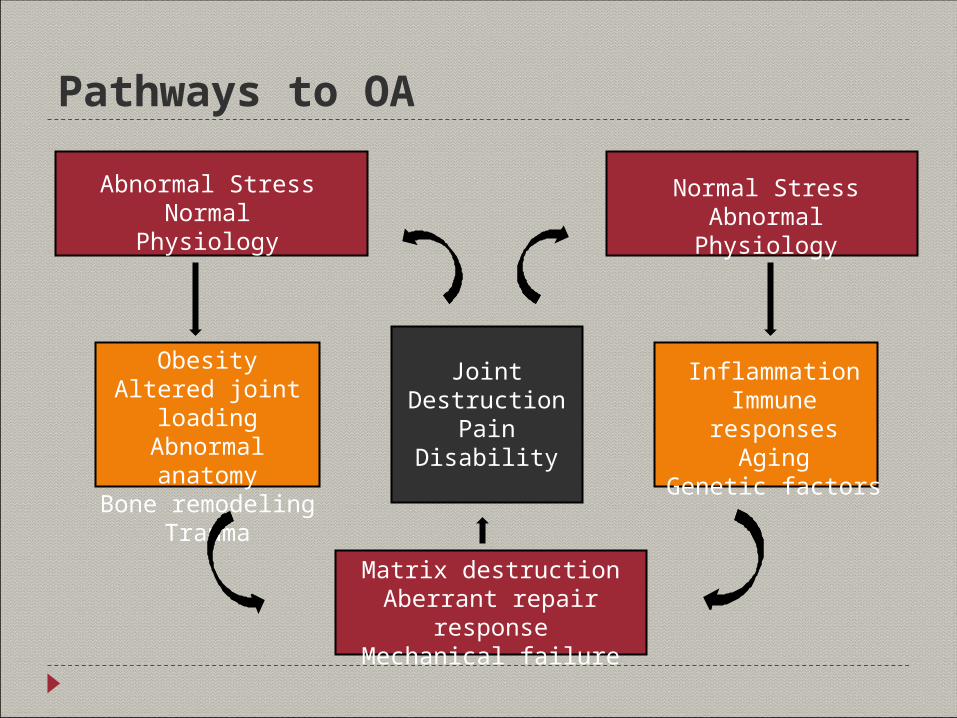
Pathways to OA
Abnormal StressNormal Physiology
Normal StressAbnormal Physiology
ObesityAltered joint loadingAbnormal anatomyBone remodeling
Trauma
JointDestruction
PainDisability
Matrix destructionAberrant repair response
Mechanical failure
InflammationImmune responses
AgingGenetic factors
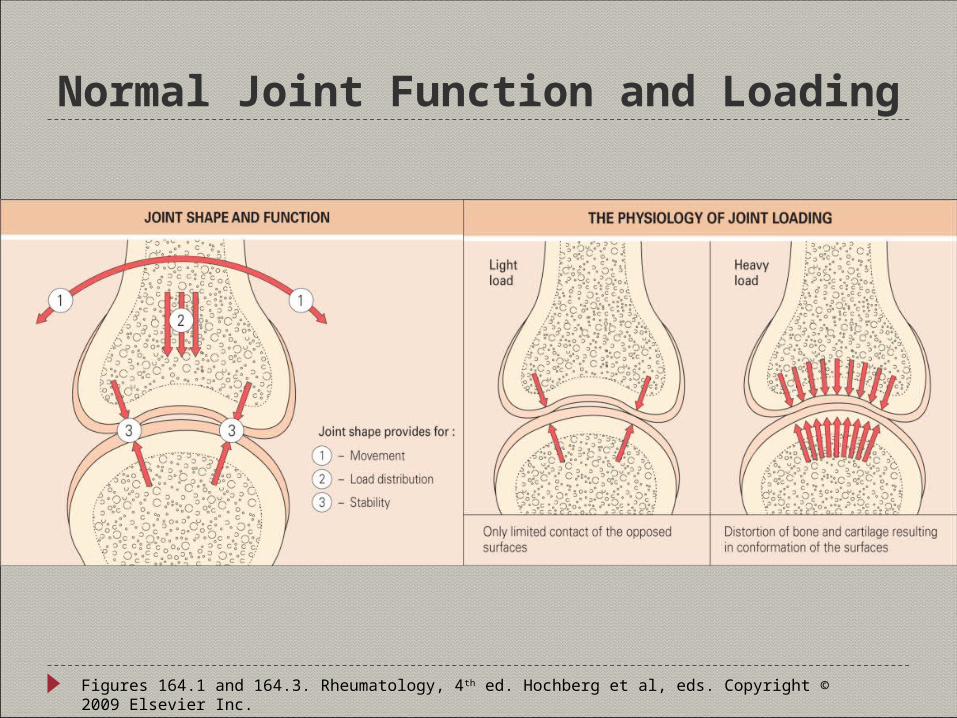
Normal Joint Function and Loading
Figures 164.1 and 164.3. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
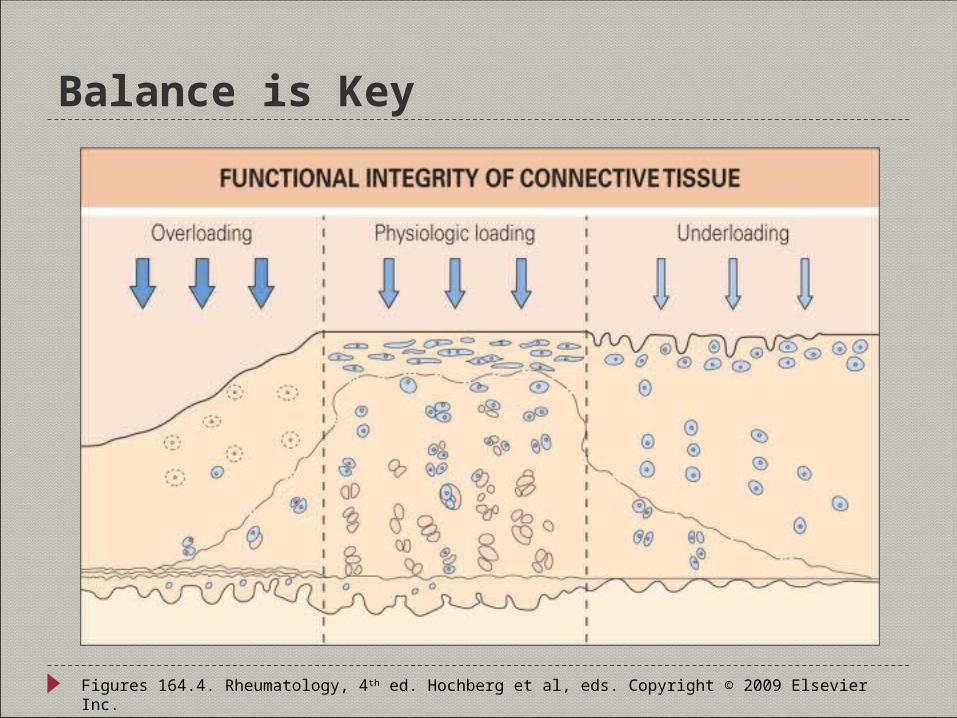
Balance is Key
Figures 164.4. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
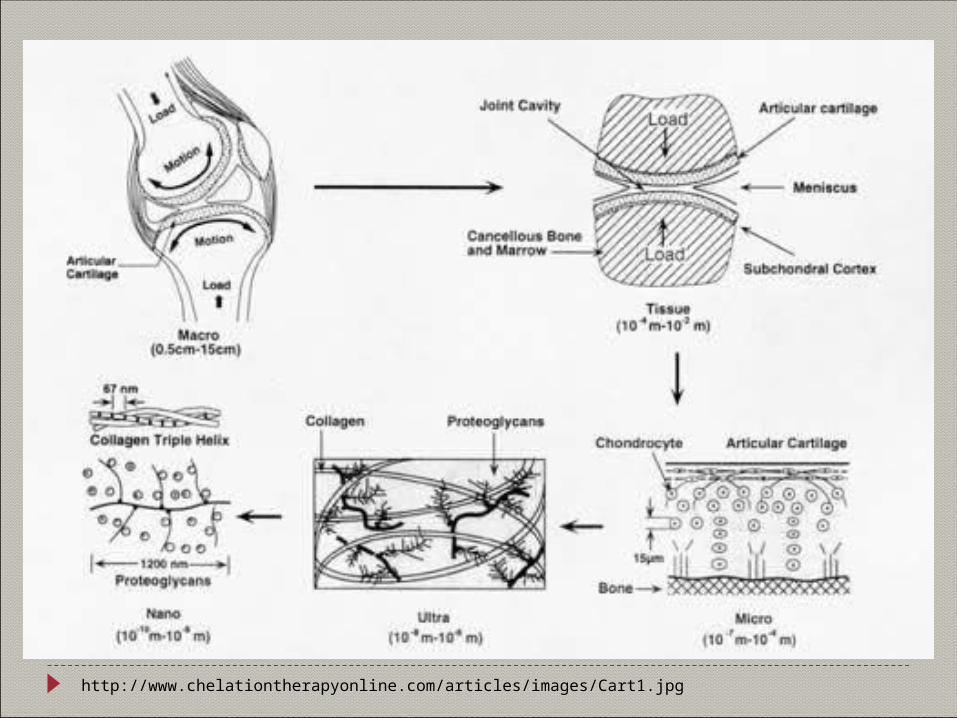
http://www.chelationtherapyonline.com/articles/images/Cart1.jpg
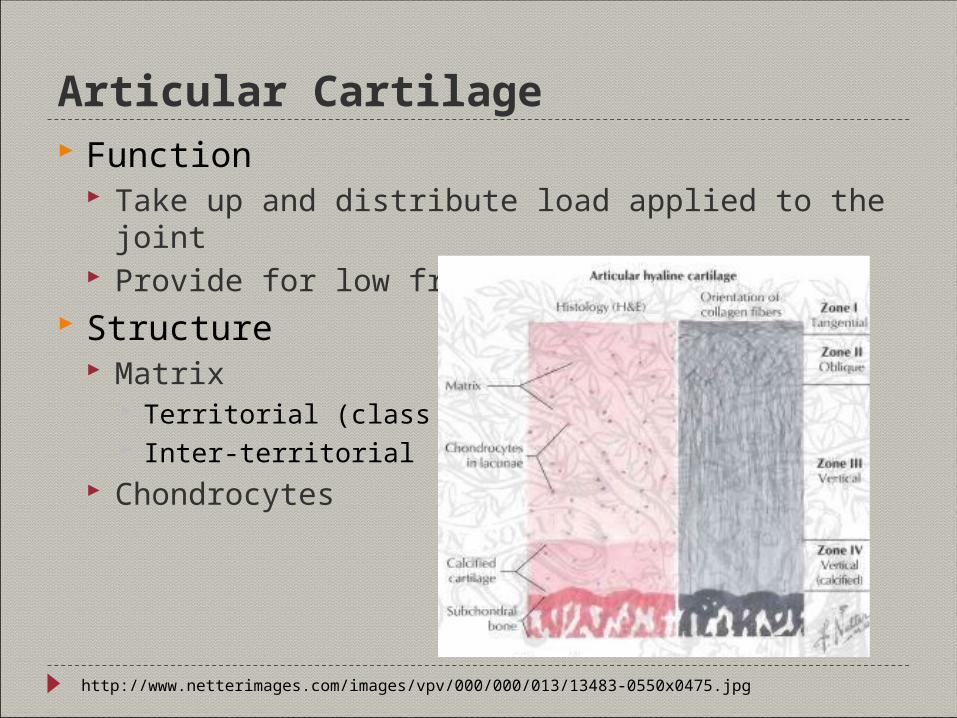
Articular Cartilage Function
Take up and distribute load applied to the joint Provide for low friction movement
Structure Matrix
Territorial (class to cells) Inter-territorial
Chondrocytes
http://www.netterimages.com/images/vpv/000/000/013/13483-0550x0475.jpg
Chondrocytes Synthesize and secrete matrix components
Collagens (Types II, IX, XI, also Types X and VI) Aggrecan (link and core proteins, KS, CS) Leucine rich repeat (LRR) proteins (e.g. decorin) Other macromolecules (e.g. COMP, CMP [matrilin-1])
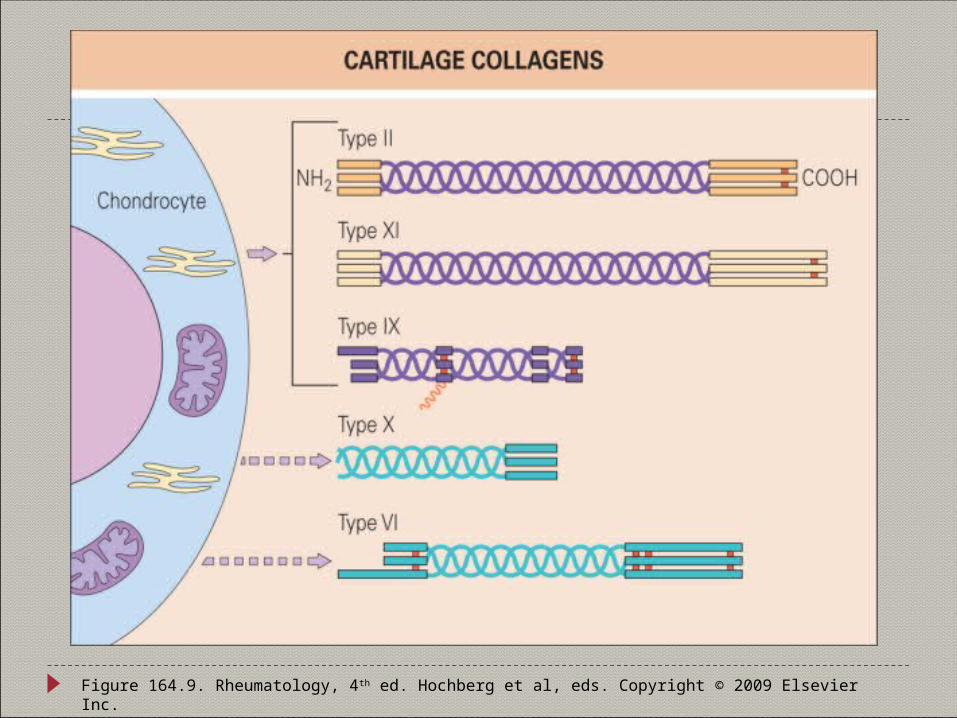
Figure 164.9. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
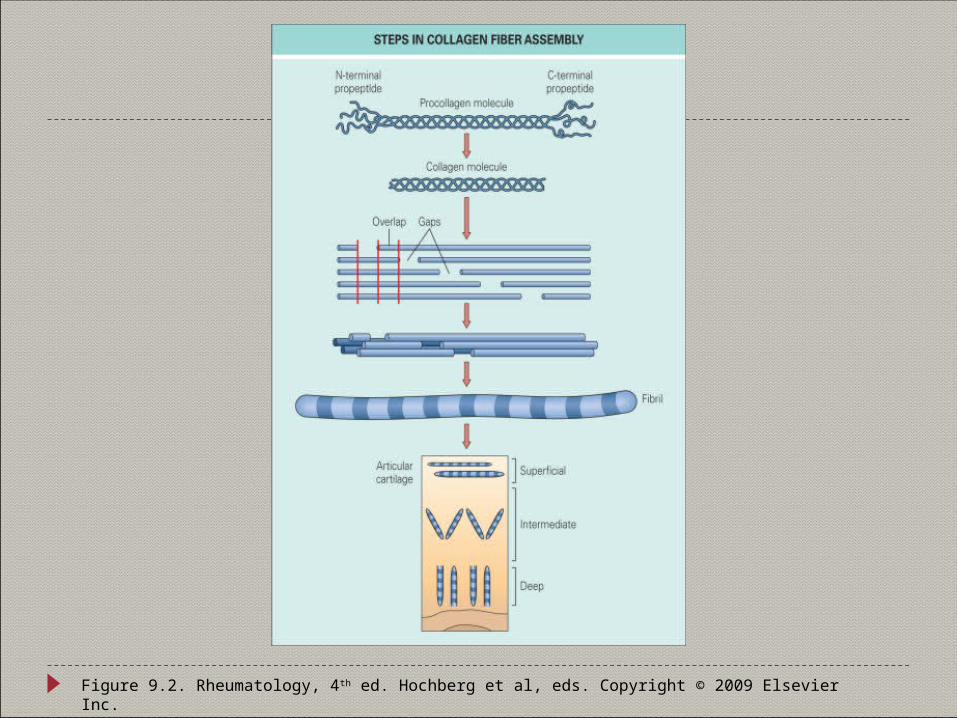
Figure 9.2. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
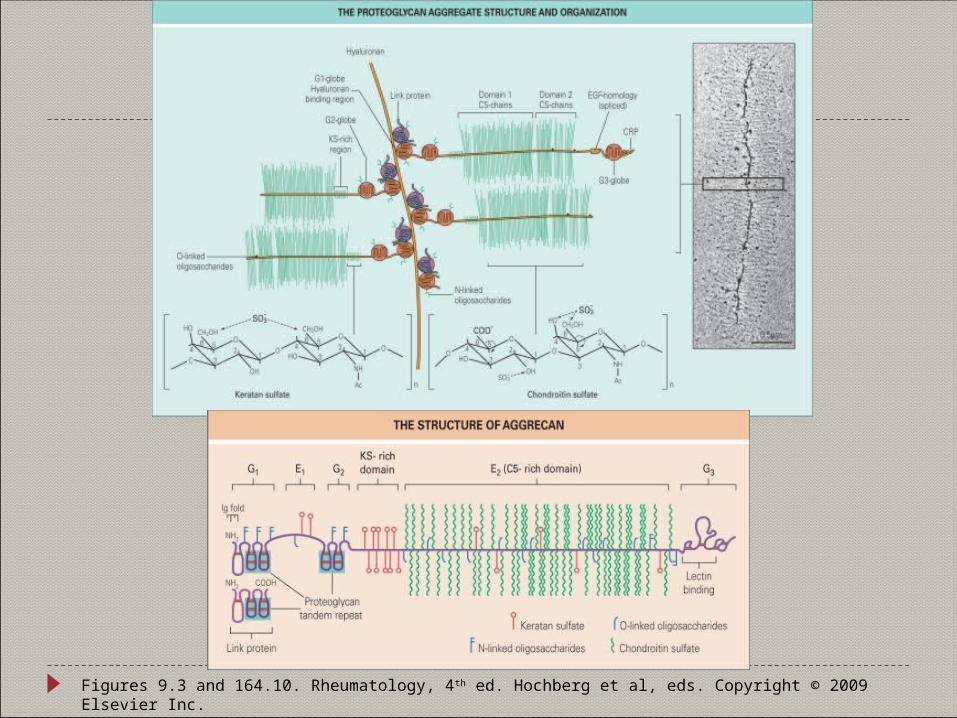
Figures 9.3 and 164.10. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
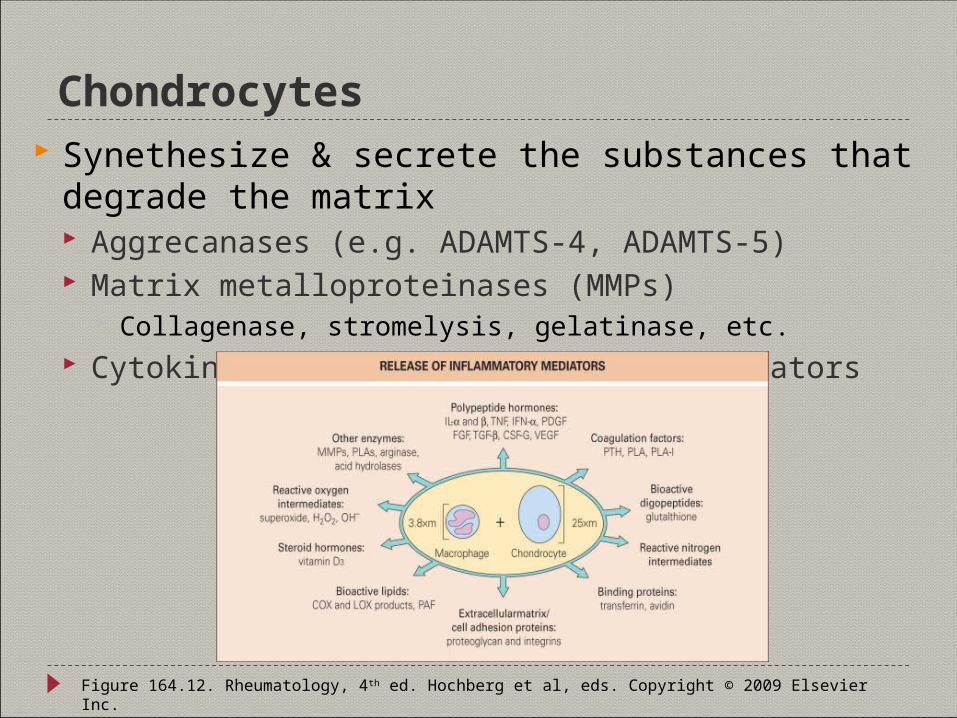
Chondrocytes Synethesize & secrete the substances that degrade the
matrix Aggrecanases (e.g. ADAMTS-4, ADAMTS-5) Matrix metalloproteinases (MMPs)
Collagenase, stromelysis, gelatinase, etc. Cytokines and other inflammatory mediators
Figure 164.12. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
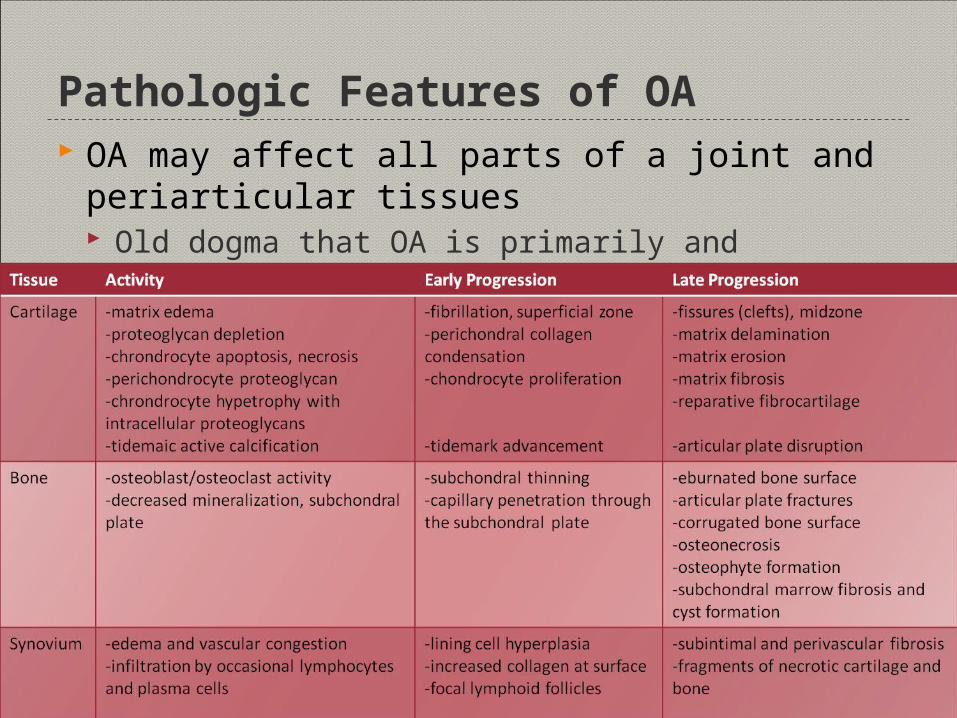
Pathologic Features of OA OA may affect all parts of a joint and periarticular tissues
Old dogma that OA is primarily and predominately a cartilage abnormality is no longer true
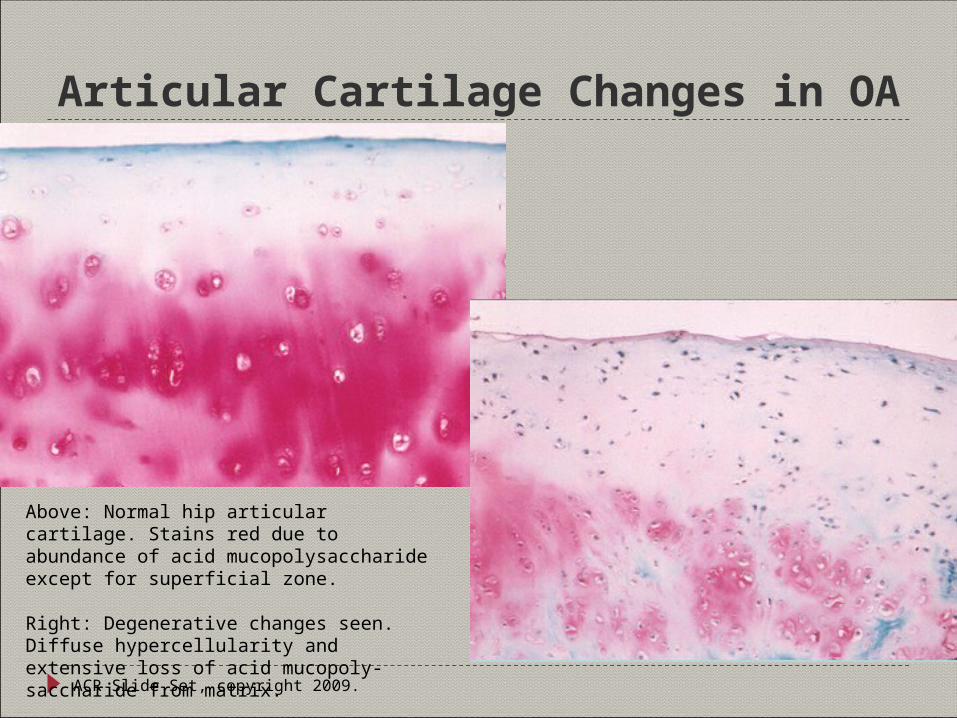
Articular Cartilage Changes in OA
ACR Slide Set, copyright 2009.
Above: Normal hip articular cartilage. Stains red due to abundance of acid mucopolysaccharide except for superficial zone.
Right: Degenerative changes seen. Diffuse hypercellularity and extensive loss of acid mucopoly-saccharide from matrix.
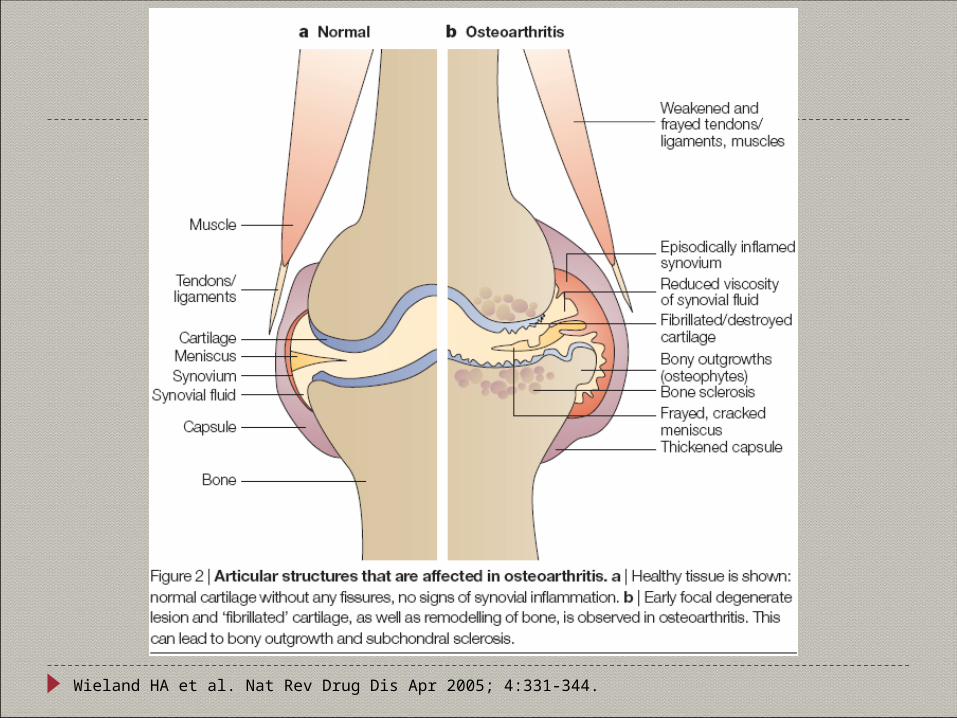
Wieland HA et al. Nat Rev Drug Dis Apr 2005; 4:331-344.
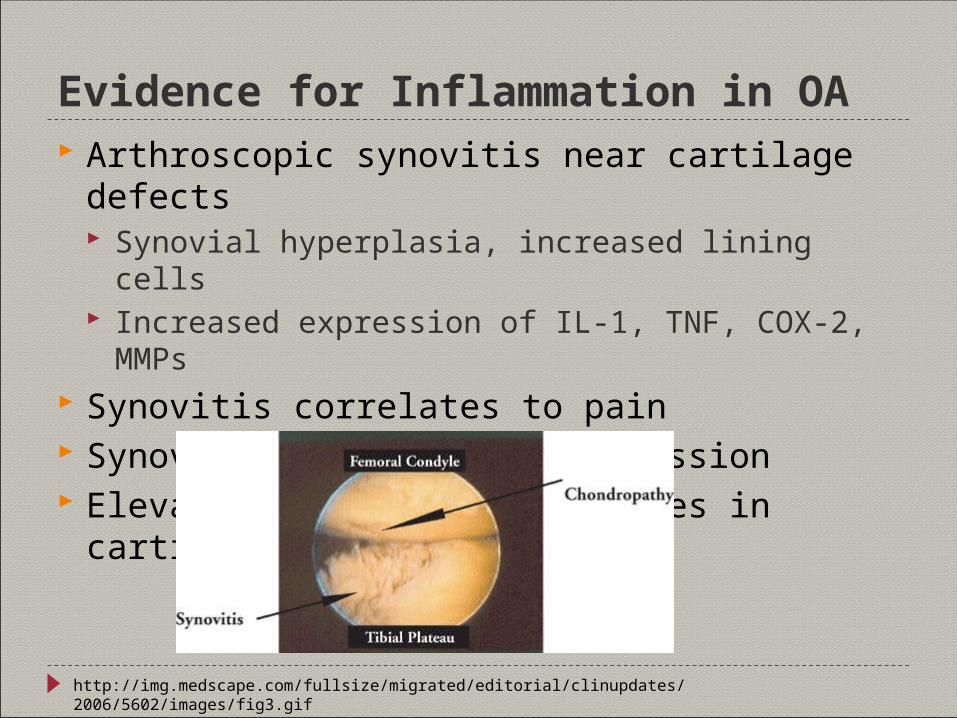
Evidence for Inflammation in OA Arthroscopic synovitis near cartilage defects
Synovial hyperplasia, increased lining cells Increased expression of IL-1, TNF, COX-2, MMPs
Synovitis correlates to pain Synovitis predicts OA progression Elevated proinflammatory genes in cartilage from OA pts
http://img.medscape.com/fullsize/migrated/editorial/clinupdates/2006/5602/images/fig3.gif
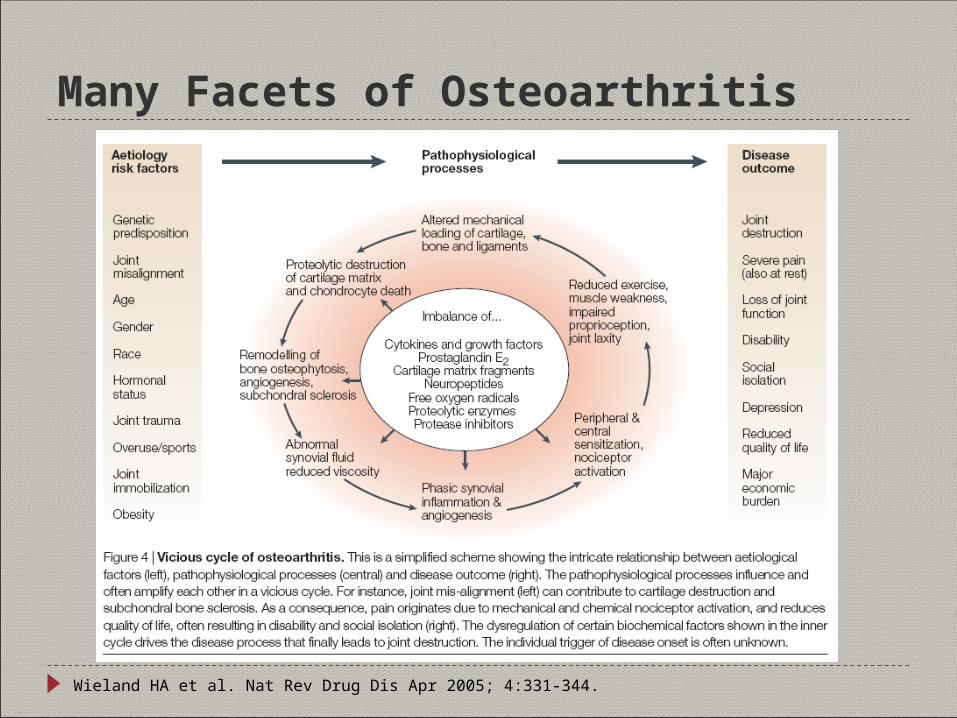
Many Facets of Osteoarthritis
Wieland HA et al. Nat Rev Drug Dis Apr 2005; 4:331-344.
Potential Mechanisms of Pain in OA Bone
Periostitis associated with osteophyte formation
Subchondral microfractures Bone angina due to decreased
blood flow and elevated intraosseous pressure
Synovium Irritation of sensory nerve endings
within synovium and/or joint capsule from osteophytes
Synovial inflammation due to release of PGs, LTs & cytokines
Joint effusion causing stretching of joint capsule
Periarticular Muscle spasm and weakness Joint instability and/or subluxation Bursitis
Anserine and/or prepatellar Trochanteric and/or ischial
Tendonitis IT band syndrome
Neuropathic
http://www.painstudy.com/images/KneePain.jpg
Imaging in OA Anatomical Imaging
Conventional radiography (plain radiographs) Most important imaging method in OA Widely available, inexpensive and readily understood
Establish the diagnosis and/or severity of OA Monitor disease progression and possible therapeutic responses Look for complications of the disorder or of treatment
Physiologic Imaging MRI Radionucleotide scans
Plain Radiographs Quality influenced by sensitivity of imaging system & radiographic view(s)
Standardized views to better compare serial exams WB views sometimes needed to evaluate joint space
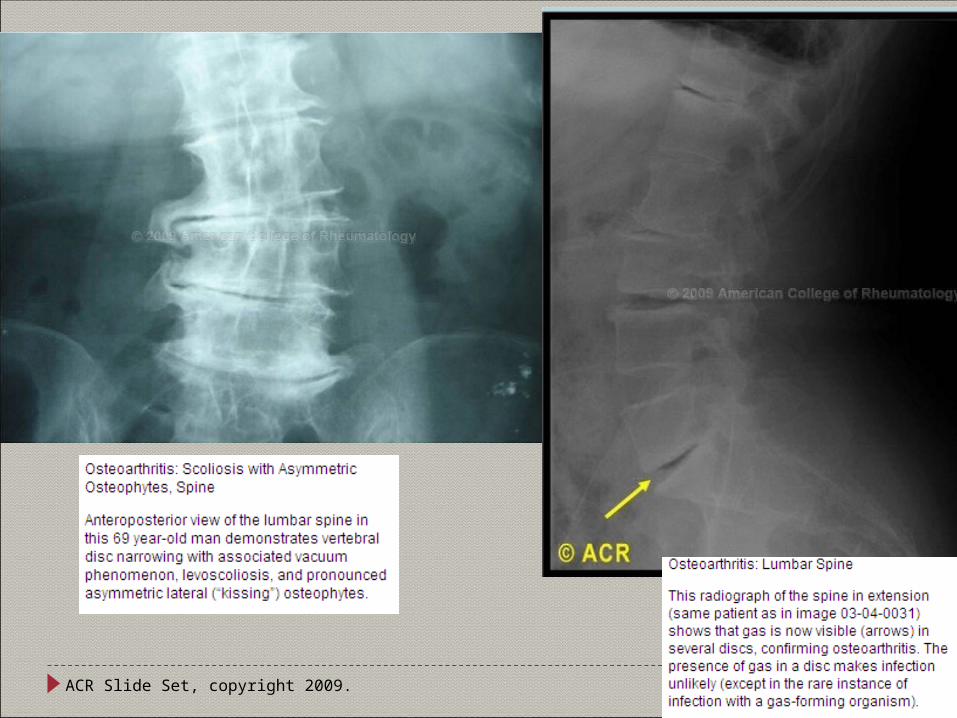
Radiologic features associated with OA Osteophytosis Subchondral bone sclerosis Joint space narrowing (JSN) Subchondral lucencies Remodeling and attrition of bone
Not perfect Observational studies have demonstrated that although odds of knee pain
increase with increasing radiographic severity (osteophytes >> JSN), the relation between radiographic changes and pain and function in OA is not strong
Further confounding this relation, recent data suggest that knee pain itself can modify the measurement of joint space width (JSW) in weight-bearing extended-view radiographs
Hunter DJ and Conaghan PG. Curr Opin Rheum Mar 2006;18:157-162.
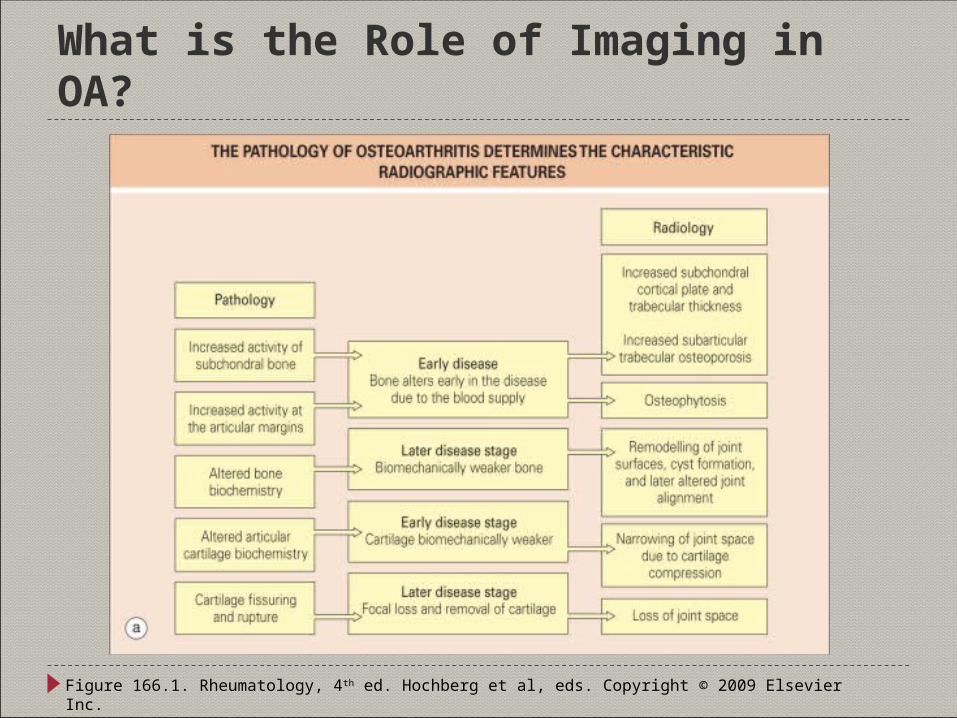
What is the Role of Imaging in OA?
Figure 166.1. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
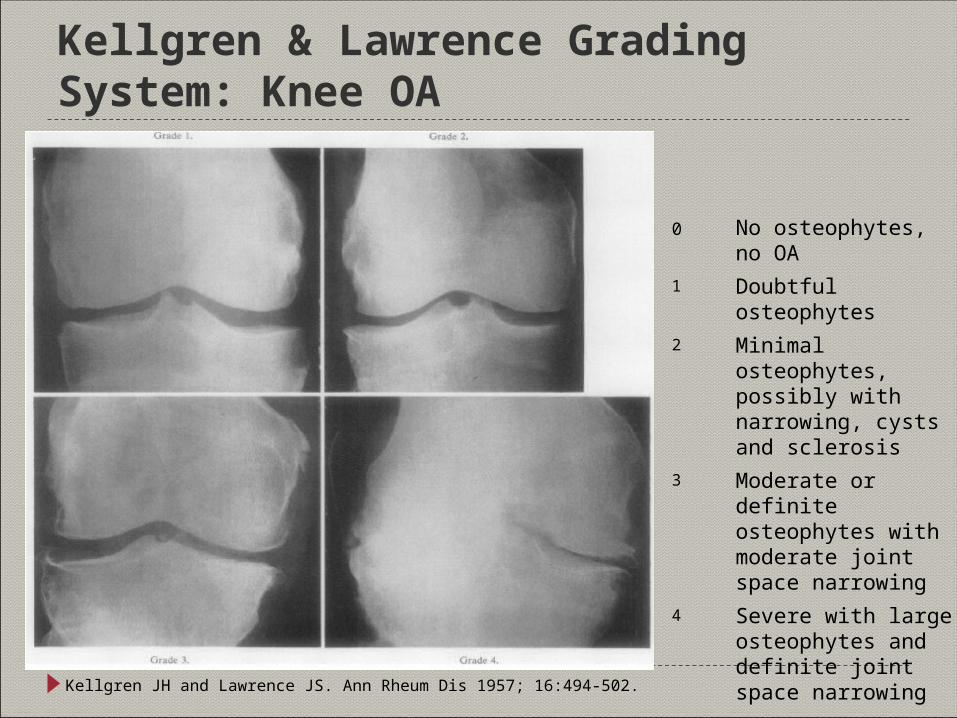
Kellgren & Lawrence Grading System: Knee OA
Kellgren JH and Lawrence JS. Ann Rheum Dis 1957; 16:494-502.
0 No osteophytes, no OA1 Doubtful osteophytes2 Minimal osteophytes,
possibly with narrowing, cysts and sclerosis
3 Moderate or definite osteophytes with moderate joint space narrowing
4 Severe with large osteophytes and definite joint space narrowing
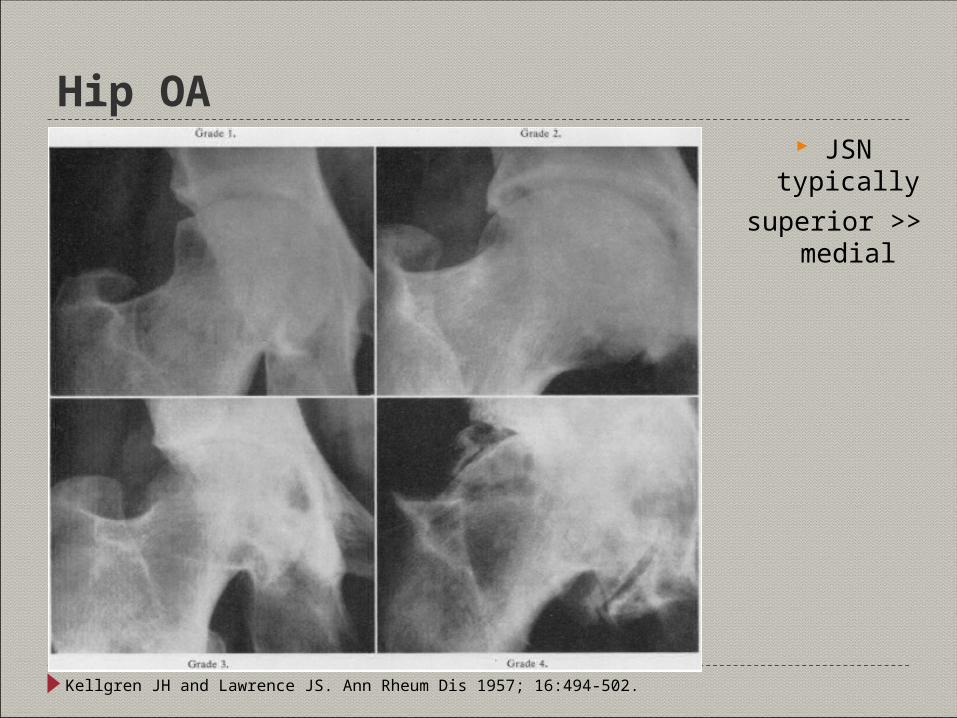
Hip OA JSN typically
superior >> medial
Kellgren JH and Lawrence JS. Ann Rheum Dis 1957; 16:494-502.
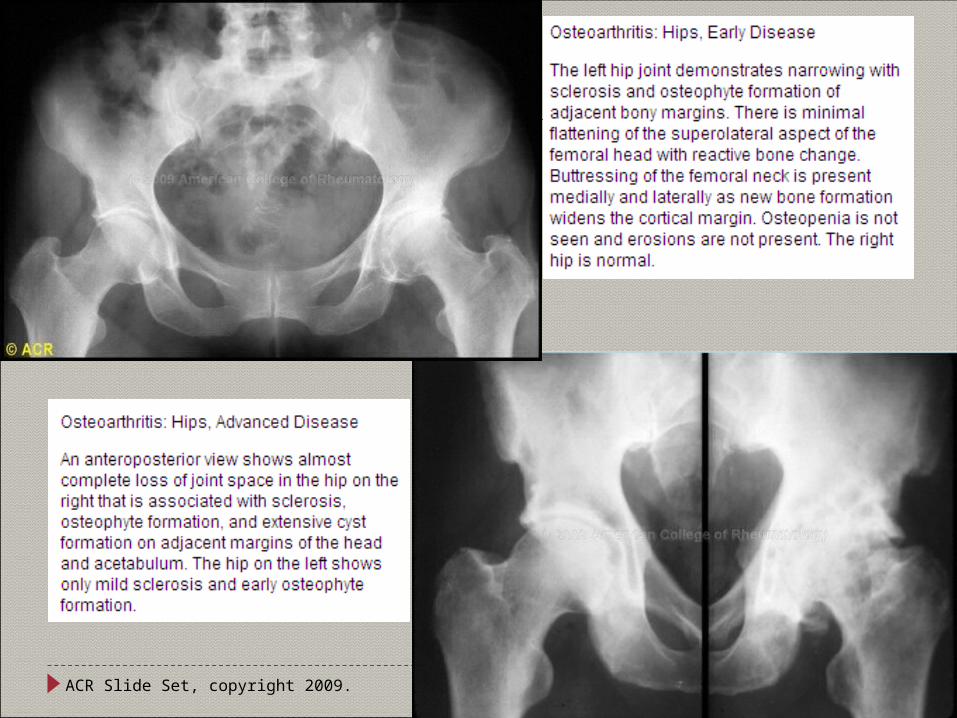
ACR Slide Set, copyright 2009.
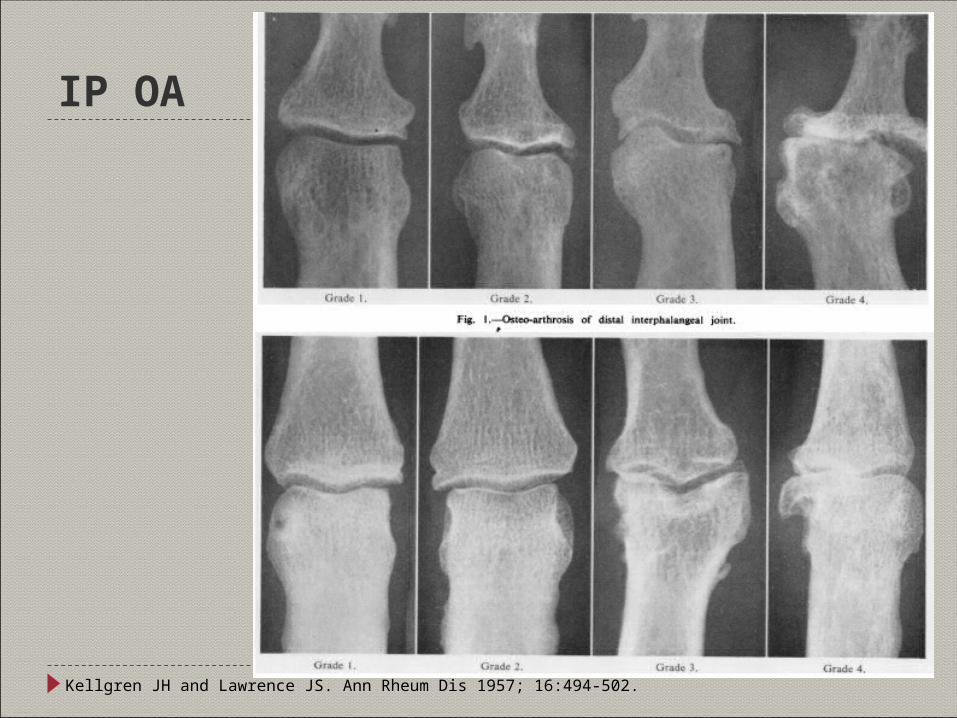
IP OA
Kellgren JH and Lawrence JS. Ann Rheum Dis 1957; 16:494-502.
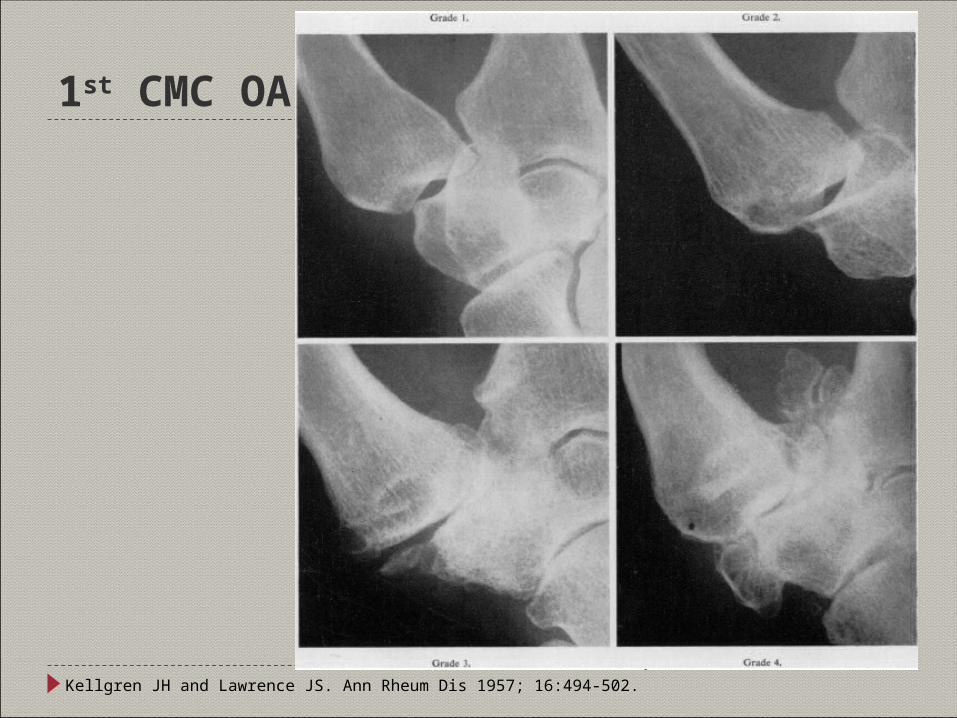
1st CMC OA
Kellgren JH and Lawrence JS. Ann Rheum Dis 1957; 16:494-502.

ACR Slide Set, copyright 2009.
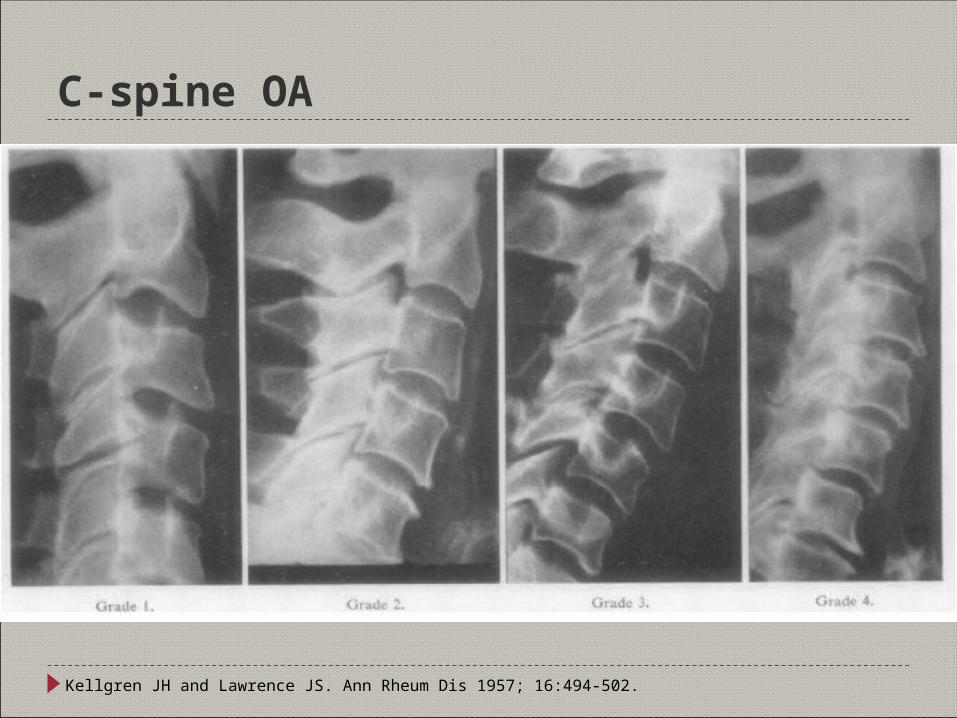
C-spine OA
Kellgren JH and Lawrence JS. Ann Rheum Dis 1957; 16:494-502.
ACR Slide Set, copyright 2009.
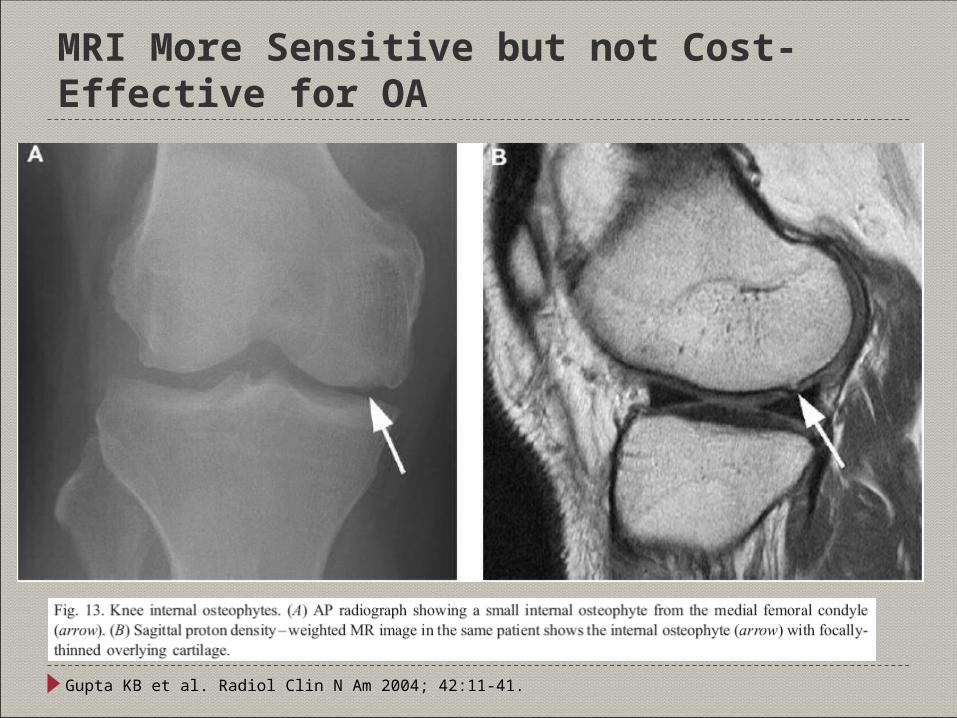
MRI More Sensitive but not Cost-Effective for OA
Gupta KB et al. Radiol Clin N Am 2004; 42:11-41.
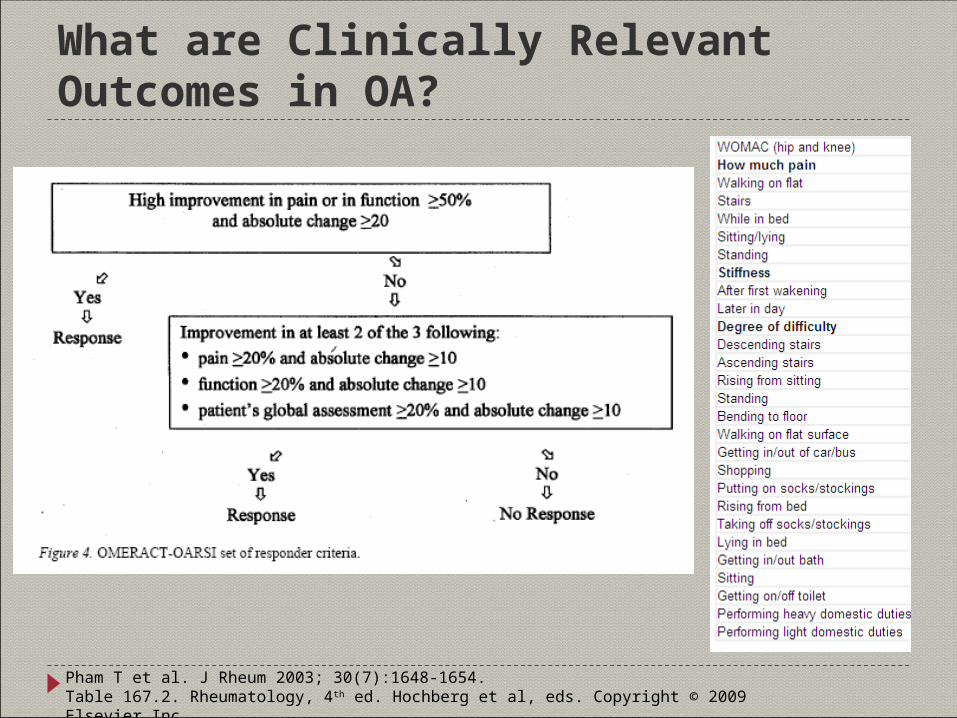
What are Clinically Relevant Outcomes in OA?
Pham T et al. J Rheum 2003; 30(7):1648-1654.Table 167.2. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
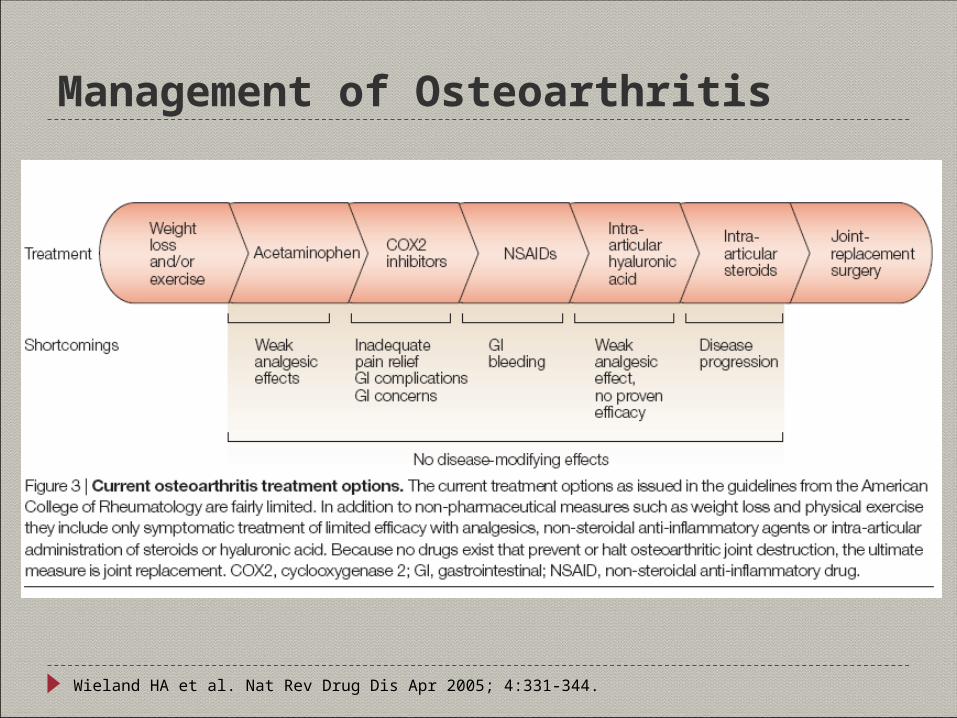
Management of Osteoarthritis
Wieland HA et al. Nat Rev Drug Dis Apr 2005; 4:331-344.
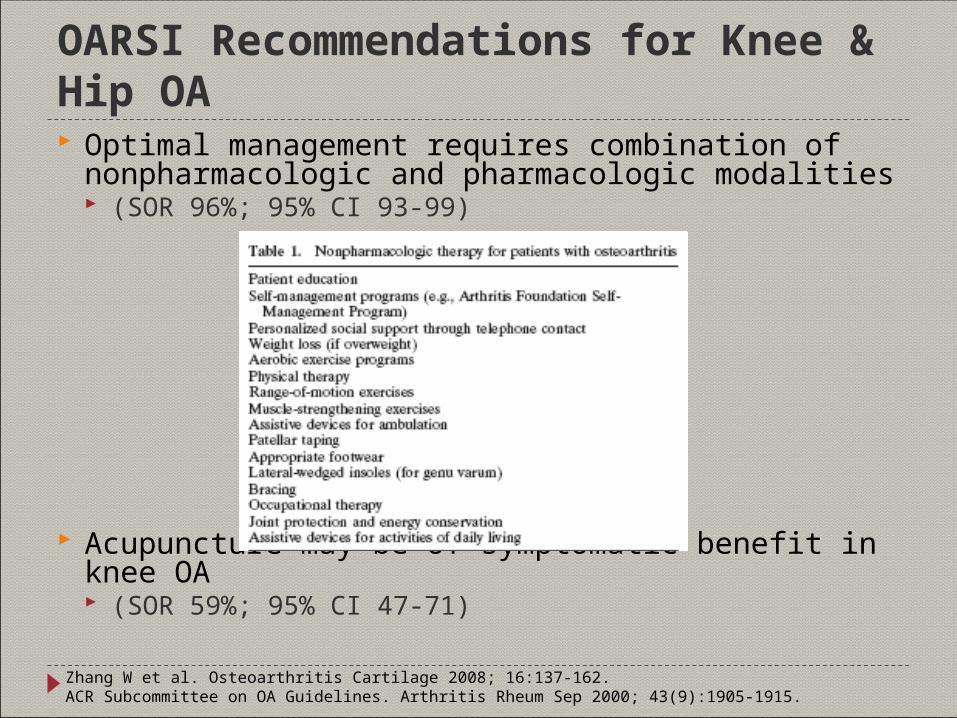
OARSI Recommendations for Knee & Hip OA Optimal management requires combination of
nonpharmacologic and pharmacologic modalities (SOR 96%; 95% CI 93-99)
Acupuncture may be of symptomatic benefit in knee OA (SOR 59%; 95% CI 47-71)
Zhang W et al. Osteoarthritis Cartilage 2008; 16:137-162.ACR Subcommittee on OA Guidelines. Arthritis Rheum Sep 2000; 43(9):1905-1915.
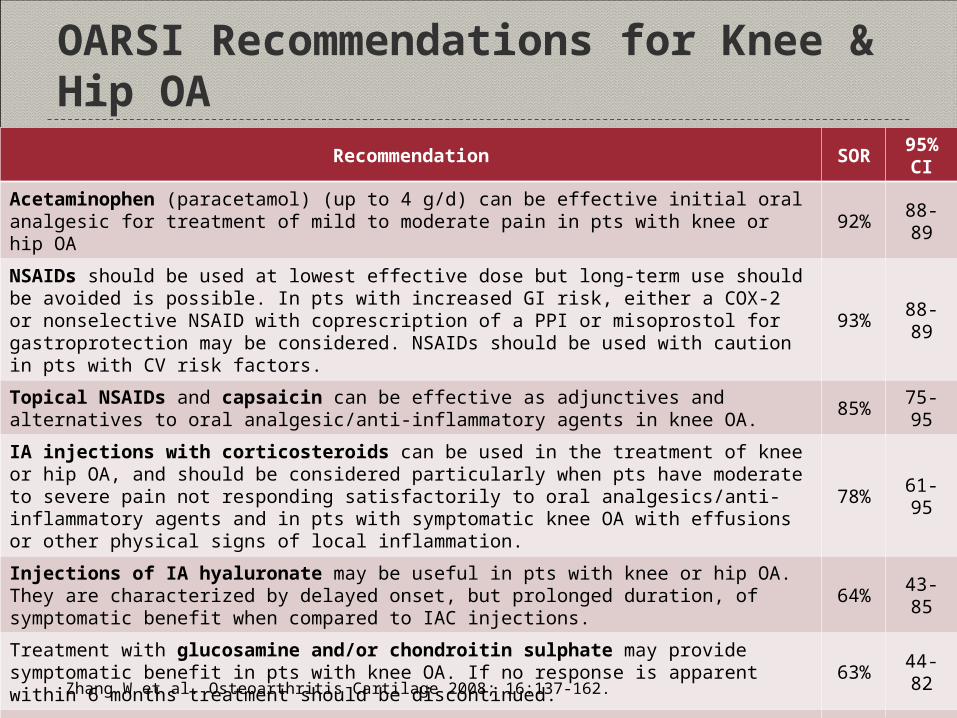
OARSI Recommendations for Knee & Hip OARecommendation SOR 95% CI
Acetaminophen (paracetamol) (up to 4 g/d) can be effective initial oral analgesic for treatment of mild to moderate pain in pts with knee or hip OA 92% 88-89
NSAIDs should be used at lowest effective dose but long-term use should be avoided is possible. In pts with increased GI risk, either a COX-2 or nonselective NSAID with coprescription of a PPI or misoprostol for gastroprotection may be considered. NSAIDs should be used with caution in pts with CV risk factors.
93% 88-89
Topical NSAIDs and capsaicin can be effective as adjunctives and alternatives to oral analgesic/anti-inflammatory agents in knee OA. 85% 75-95
IA injections with corticosteroids can be used in the treatment of knee or hip OA, and should be considered particularly when pts have moderate to severe pain not responding satisfactorily to oral analgesics/anti-inflammatory agents and in pts with symptomatic knee OA with effusions or other physical signs of local inflammation.
78% 61-95
Injections of IA hyaluronate may be useful in pts with knee or hip OA. They are characterized by delayed onset, but prolonged duration, of symptomatic benefit when compared to IAC injections. 64% 43-85
Treatment with glucosamine and/or chondroitin sulphate may provide symptomatic benefit in pts with knee OA. If no response is apparent within 6 months treatment should be discontinued. 63% 44-82
The use of weak opioids and narcotic analgesics can be considered for the treatment of refractory pain in pts with hip or knee OA, where other pharmacologic agents have been ineffective or are contradicted. Stronger opioids should only be used for the management of severe pain in exceptional circumstances. Nonpharmacologic therapies should be continued in such pts and surgical tmts should be considered.
82% 74-90
Zhang W et al. Osteoarthritis Cartilage 2008; 16:137-162.
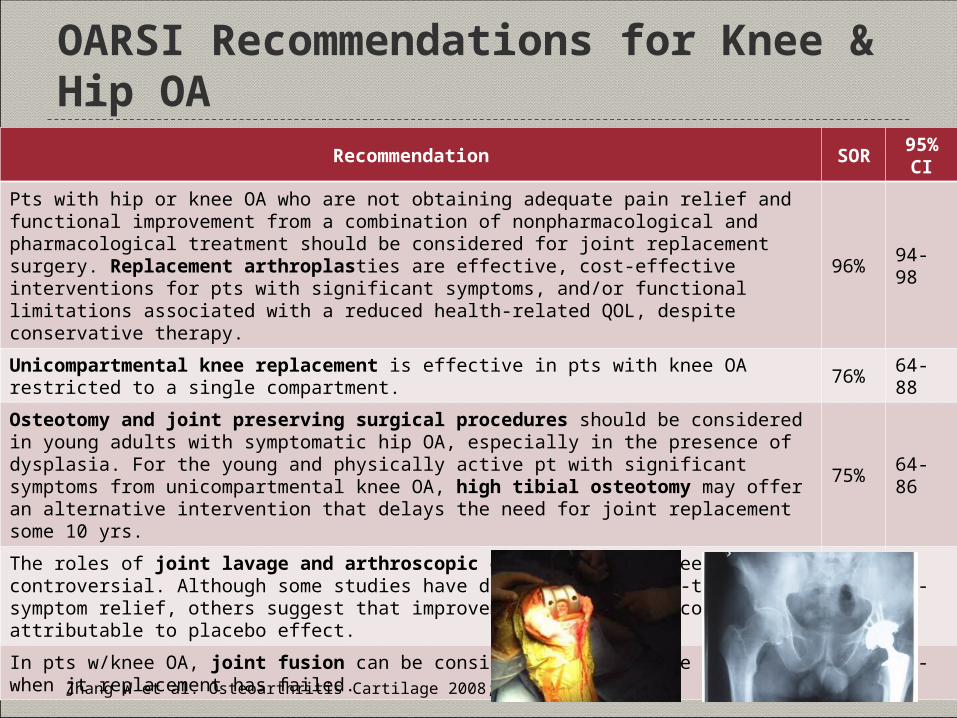
OARSI Recommendations for Knee & Hip OARecommendation SOR 95% CI
Pts with hip or knee OA who are not obtaining adequate pain relief and functional improvement from a combination of nonpharmacological and pharmacological treatment should be considered for joint replacement surgery. Replacement arthroplasties are effective, cost-effective interventions for pts with significant symptoms, and/or functional limitations associated with a reduced health-related QOL, despite conservative therapy.
96% 94-98
Unicompartmental knee replacement is effective in pts with knee OA restricted to a single compartment. 76% 64-88
Osteotomy and joint preserving surgical procedures should be considered in young adults with symptomatic hip OA, especially in the presence of dysplasia. For the young and physically active pt with significant symptoms from unicompartmental knee OA, high tibial osteotomy may offer an alternative intervention that delays the need for joint replacement some 10 yrs.
75% 64-86
The roles of joint lavage and arthroscopic debridement in knee OA are controversial. Although some studies have demonstrated short-term symptom relief, others suggest that improvement in symptoms could be attributable to placebo effect.
60% 47-82
In pts w/knee OA, joint fusion can be considered as a salvage procedure when jt replacement has failed. 69% 57-82
Zhang W et al. Osteoarthritis Cartilage 2008; 16:137-162.
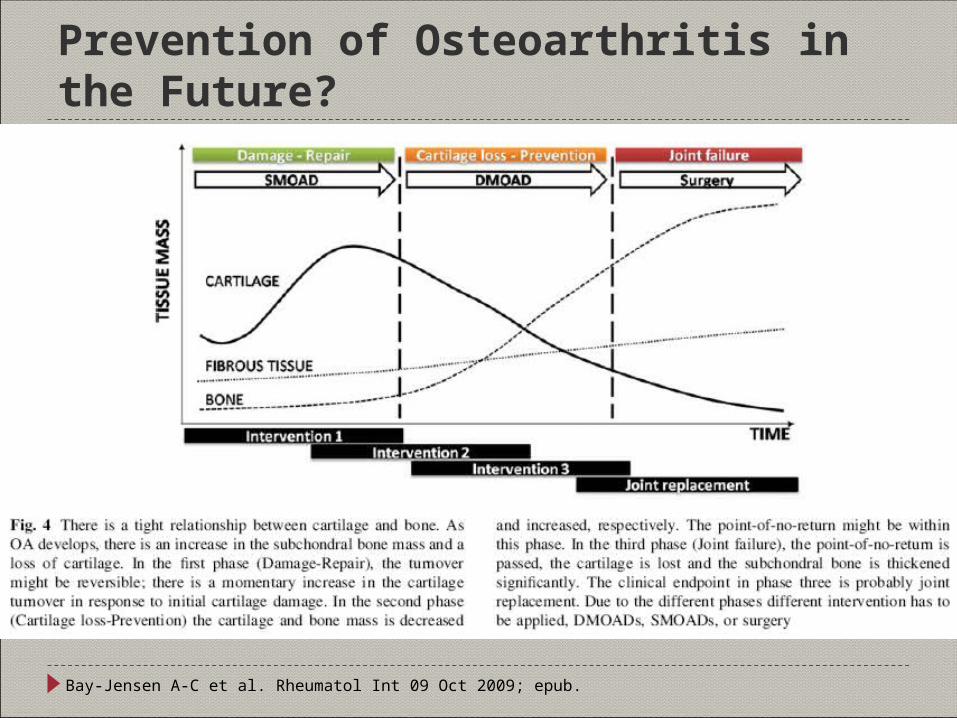
Prevention of Osteoarthritis in the Future?
Bay-Jensen A-C et al. Rheumatol Int 09 Oct 2009; epub.
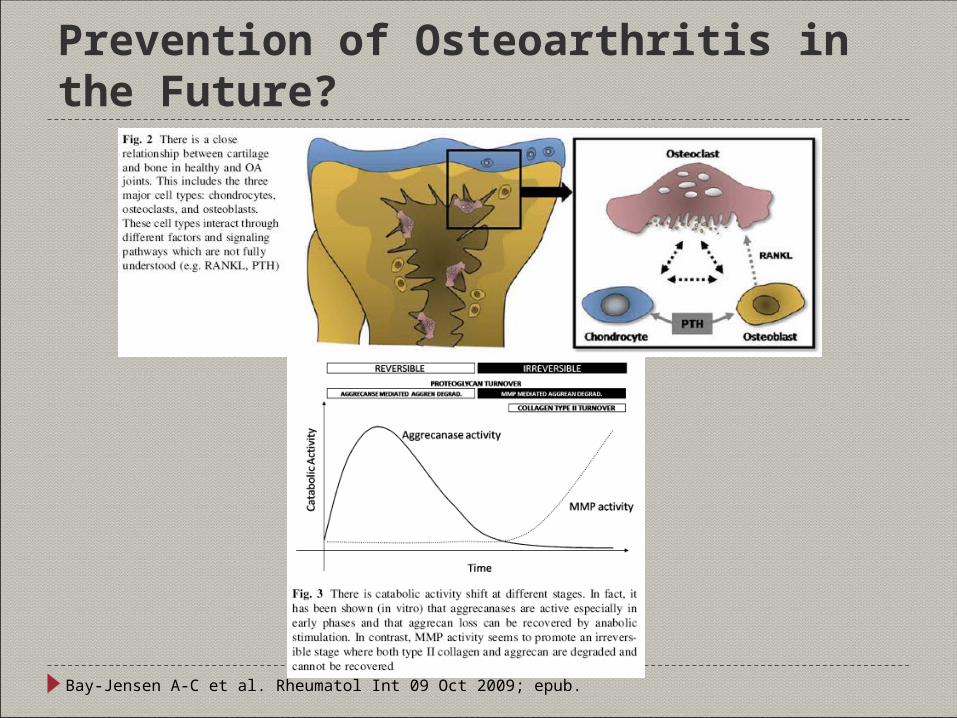
Prevention of Osteoarthritis in the Future?
Bay-Jensen A-C et al. Rheumatol Int 09 Oct 2009; epub.
DMOADs? Potential disease-modifying drugs for OA
Anti-resorptive agents N-containing bisphosphonates Calcitonin Strontium ranelate
Cytokine inhibitors Diacerein, IL1-R antagonist, ICE inhibitors
Matrix metalloprotease inhibitors Doxycycline
Nutritional supplements Glucosamine sulfate and chrondroitin sulfate
Growth factors
Hunter DJ. Med Clin N Am Jan 2009; 93(1):223-234.Qvist P et al. Pharmacol Res Jul 2008; 58:1-7.
Other Forms of Idiopathic Other Forms of Idiopathic Osteoarthritis Osteoarthritis
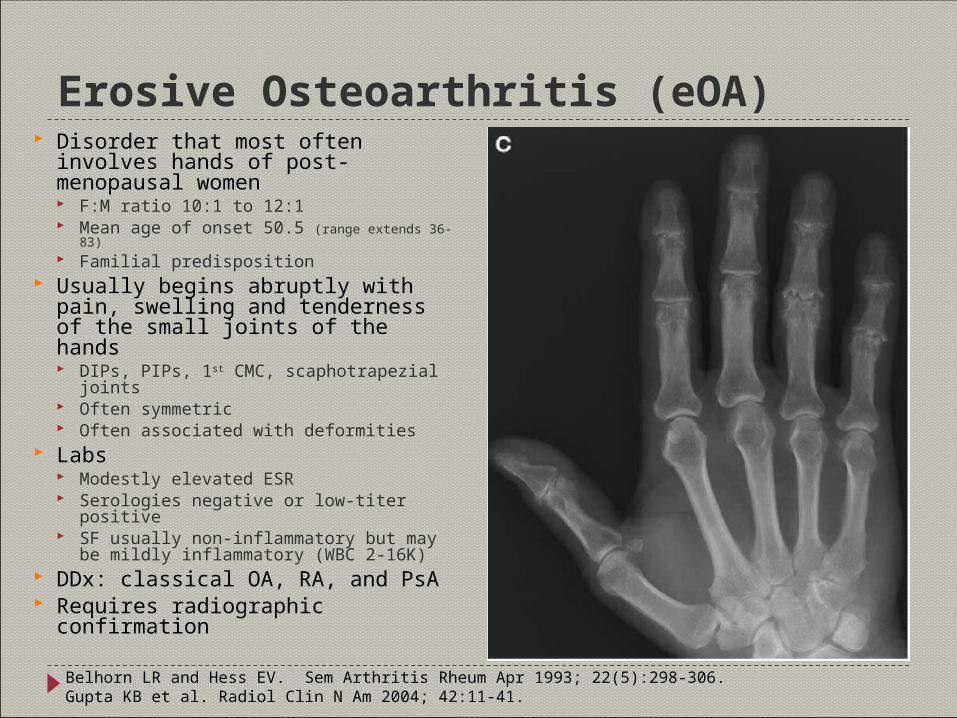
Erosive Osteoarthritis (eOA) Disorder that most often involves
hands of post-menopausal women F:M ratio 10:1 to 12:1 Mean age of onset 50.5 (range extends 36-83) Familial predisposition
Usually begins abruptly with pain, swelling and tenderness of the small joints of the hands DIPs, PIPs, 1st CMC, scaphotrapezial joints Often symmetric Often associated with deformities
Labs Modestly elevated ESR Serologies negative or low-titer positive SF usually non-inflammatory but may be
mildly inflammatory (WBC 2-16K) DDx: classical OA, RA, and PsA Requires radiographic confirmation
Belhorn LR and Hess EV. Sem Arthritis Rheum Apr 1993; 22(5):298-306.Gupta KB et al. Radiol Clin N Am 2004; 42:11-41.
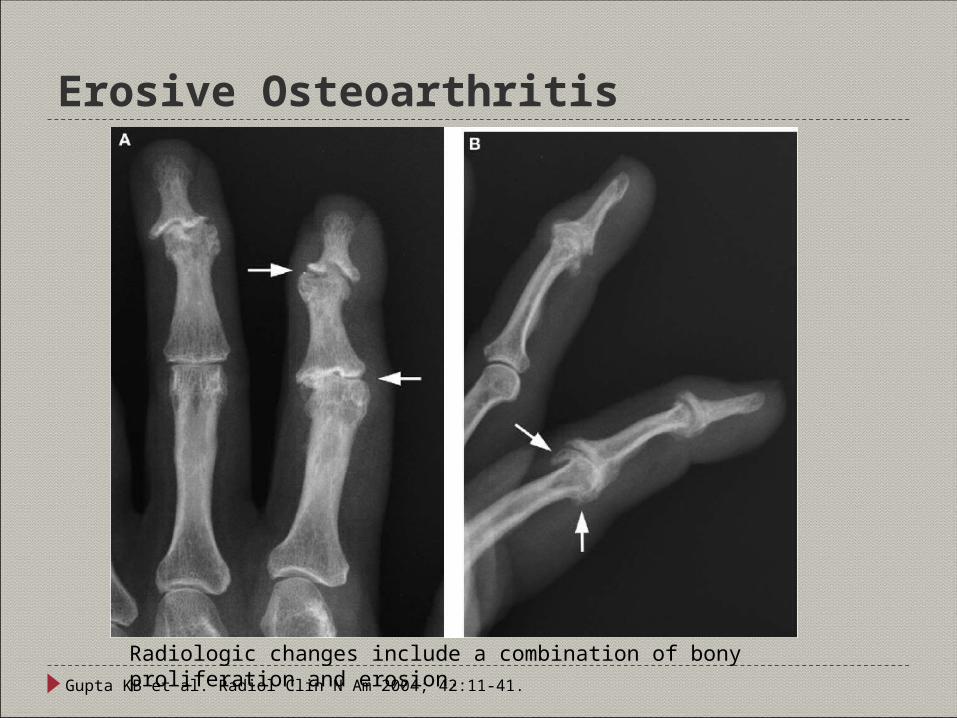
Erosive Osteoarthritis
Gupta KB et al. Radiol Clin N Am 2004; 42:11-41.
Radiologic changes include a combination of bony proliferation and erosion.
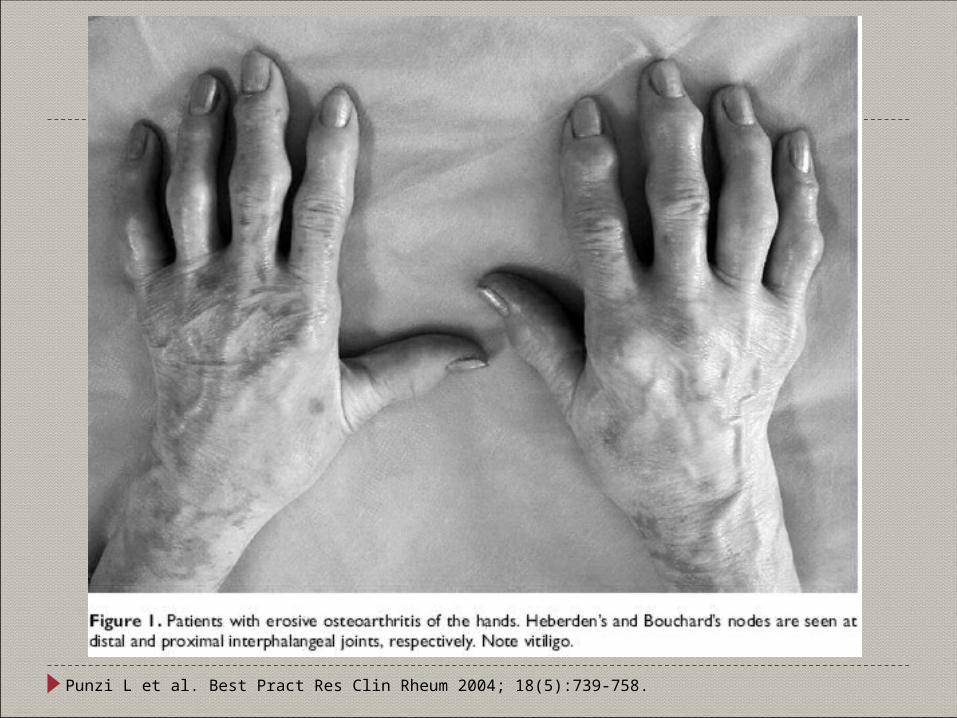
Punzi L et al. Best Pract Res Clin Rheum 2004; 18(5):739-758.
Erosive Osteoarthritis Treatment Nonpharmacologic therapies
Physical therapy, occupational therapy ROM exercises, moist heat (paraffin baths)
Pharmacologic therapies No definitive therapeutic approach
IA steroid injections can be efficacious in reducing symptoms NSAIDs (especially if there appears to be an inflammatory component) Analgesics (acetaminophen, capsaicin)
Possible use – inconclusive studies, investigational therapies Hydroxychloroquine Glucosamine and chondroitin sulfate Methotrexate Gold salts Others – anakinra, intraarticular infliximab, systemic adalimumab
Surgical intervention Synovectomy, arthrodesis of destroyed actively inflamed joints
Belhorn LR and Hess EV. Sem Arthritis Rheum Apr 1993; 22(5):298-306.
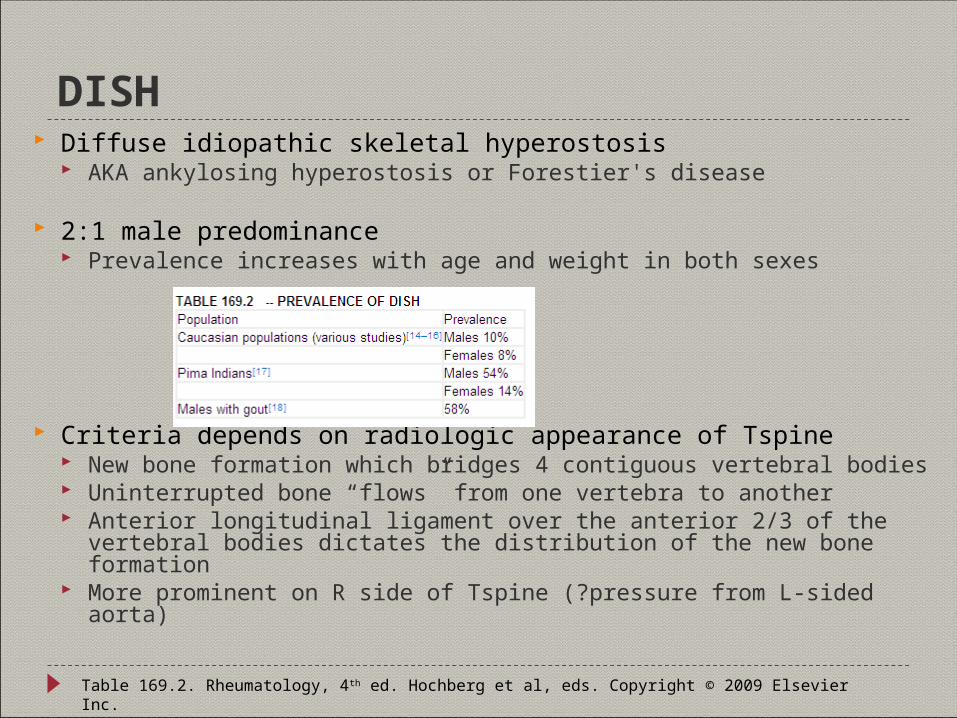
DISH Diffuse idiopathic skeletal hyperostosis
AKA ankylosing hyperostosis or Forestier's disease
2:1 male predominance Prevalence increases with age and weight in both sexes
Criteria depends on radiologic appearance of Tspine New bone formation which bridges 4 contiguous vertebral bodies Uninterrupted bone “flows” from one vertebra to another Anterior longitudinal ligament over the anterior 2/3 of the vertebral bodies dictates
the distribution of the new bone formation More prominent on R side of Tspine (?pressure from L-sided aorta)
Table 169.2. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.

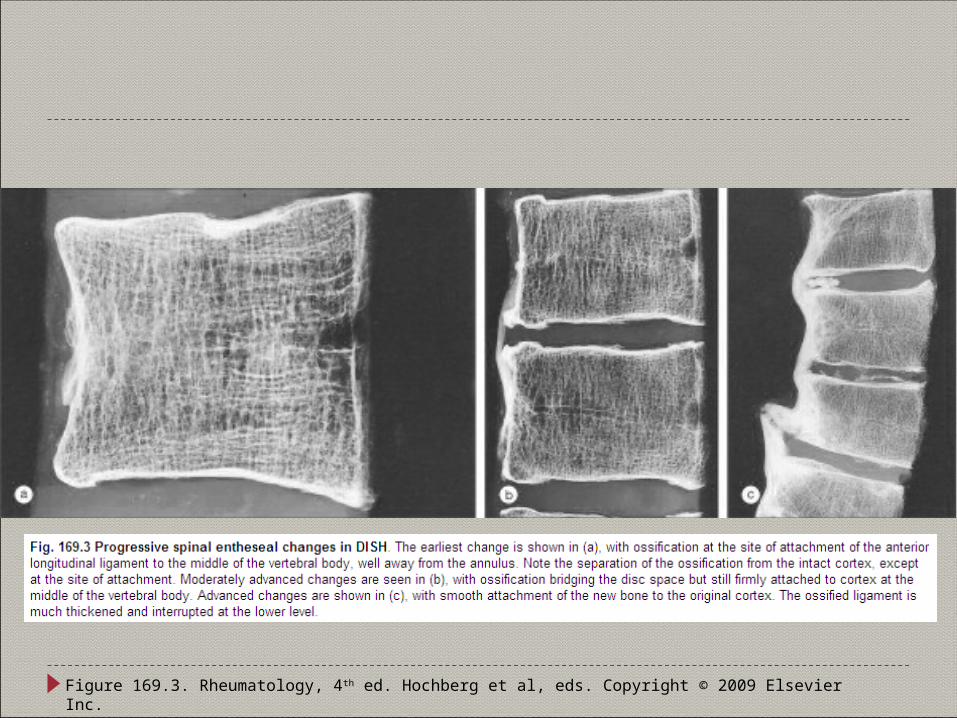
Figure 169.3. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
DISH Can occur at other joints as well Clinical features
Deposition of bone usually asymptomatic apart from stiffness of neck, back, or peripheral joints
Can have a peripheral enthesopathy which can cause pain Symptoms may arise from compression of important structures
Dysphagia with C-spine DISH Myelopathy/quadriplegia with ossification of posterior longitudinal ligament Spinal stenosis due to marked osteophytosis
Can co-exist with inflammatory arthritis Associated with diabetes, IGT, obesity DDx includes AS or other SpA, DDD, primary OA, acromegaly
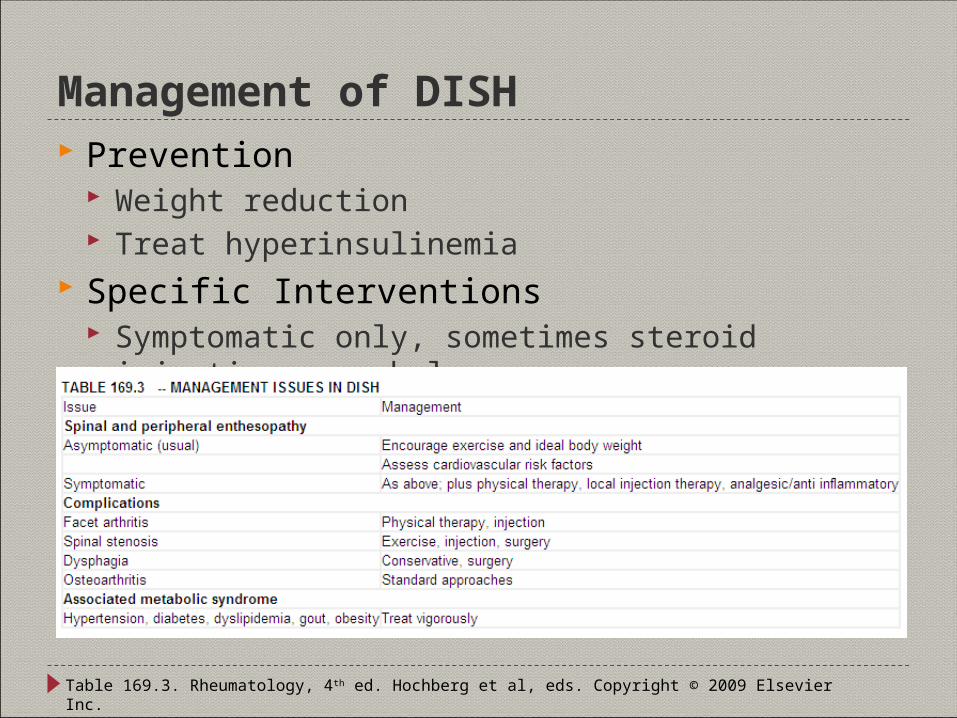
Management of DISH Prevention
Weight reduction Treat hyperinsulinemia
Specific Interventions Symptomatic only, sometimes steroid injections can help
Table 169.3. Rheumatology, 4th ed. Hochberg et al, eds. Copyright © 2009 Elsevier Inc.
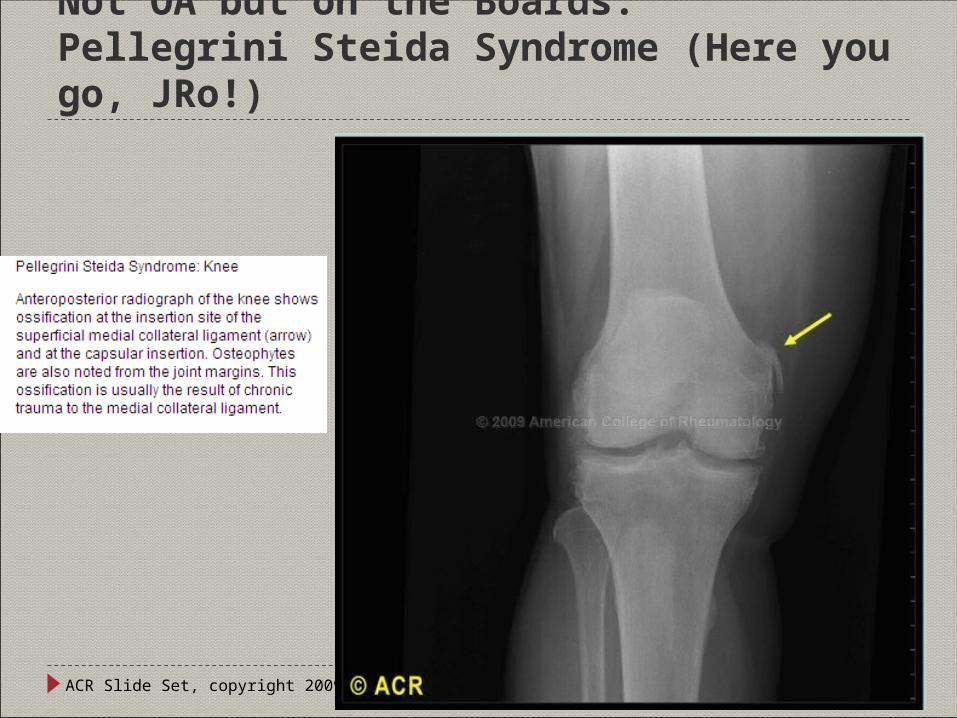
Not OA but on the Boards:Pellegrini Steida Syndrome (Here you go, JRo!)
ACR Slide Set, copyright 2009.
Questions?Questions?