Embed Size (px)
Citation preview
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 1/38
PROTEINURIA &
NEPHROTIC SYNDROME
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 2/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 3/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 4/38
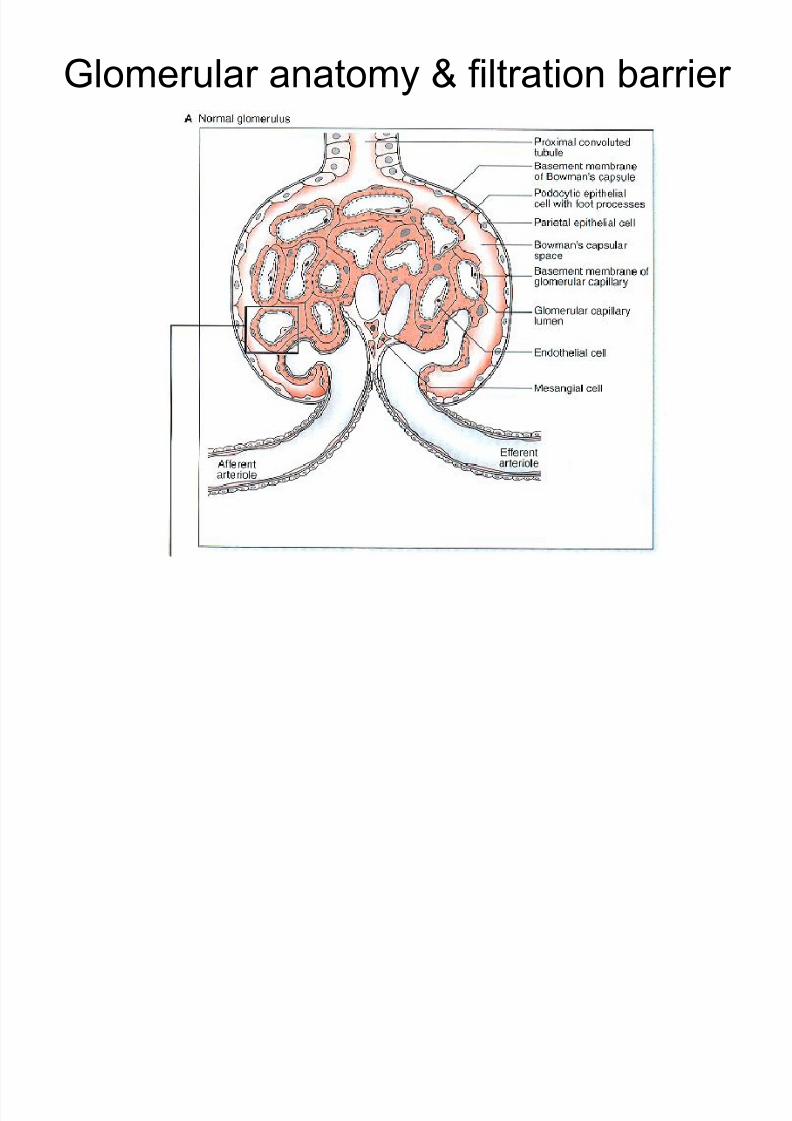
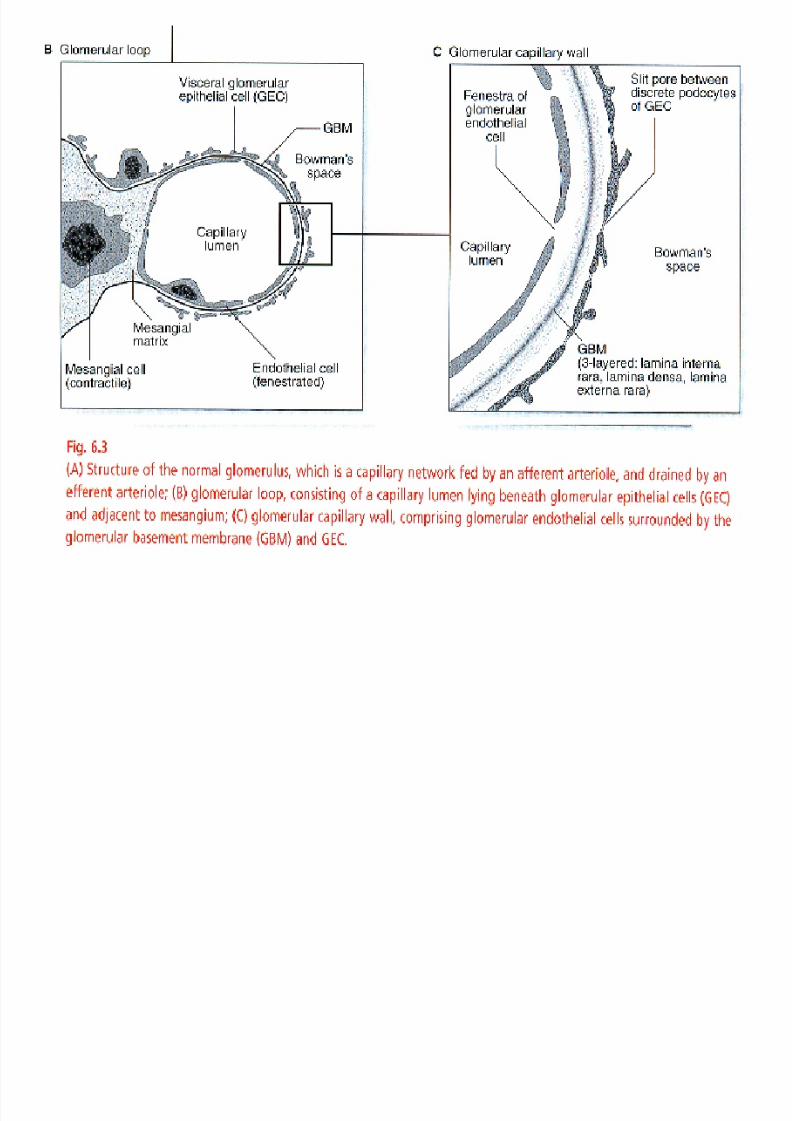
Glomerular anatomy & filtration barrier
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 5/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 6/38

7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 7/38
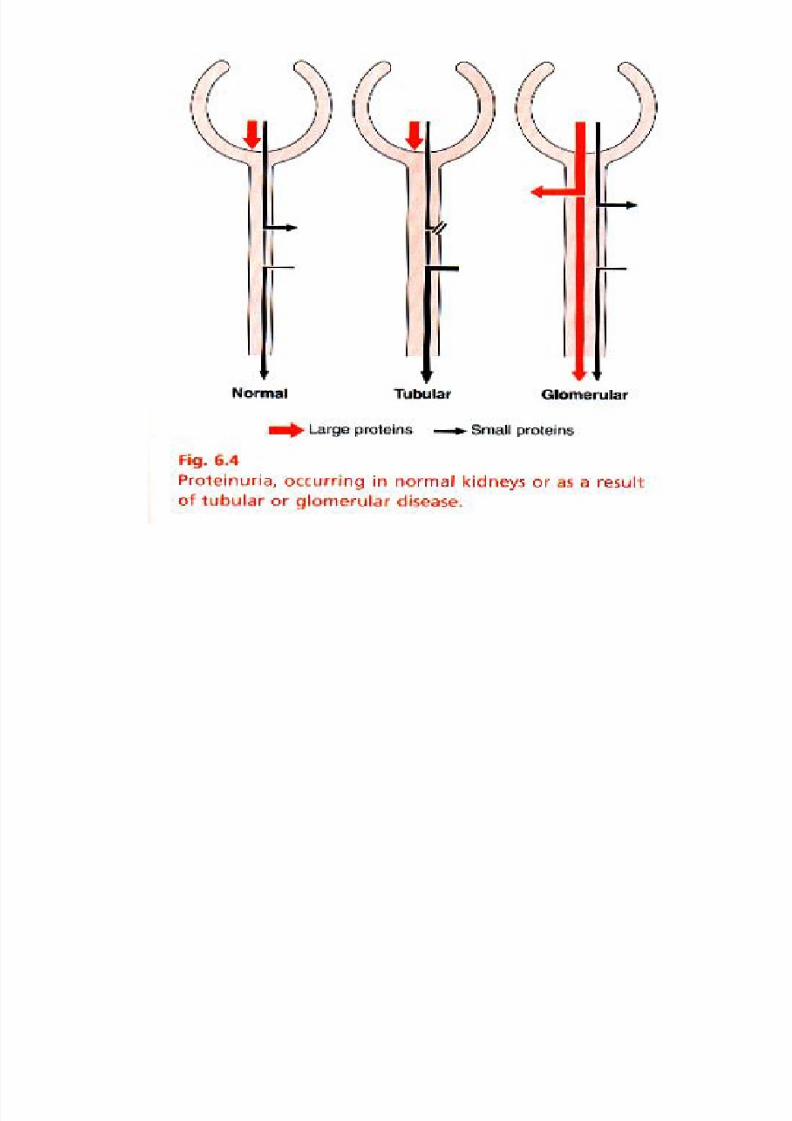
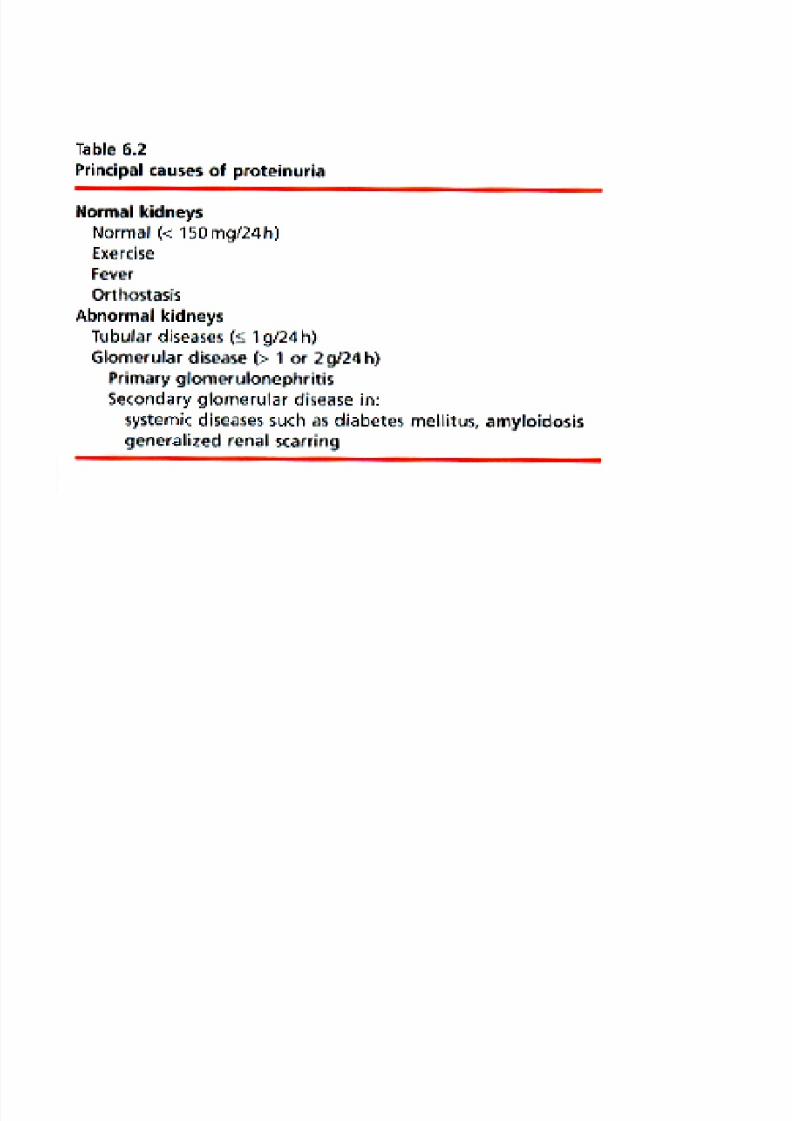
Proteinuria
• Normal urine < 150 mg/day in adults
– Small MW proteins filtered across GCW
– Tamm-Horsfall proteins secreted by tubular
cells• Abnormal proteinuria
– Failure of the GCW filtration barrier – glomerular proteinuria
– Decreased reabsorption into, or increasedrelease from, tubular cells – tubular proteinuria
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 8/38
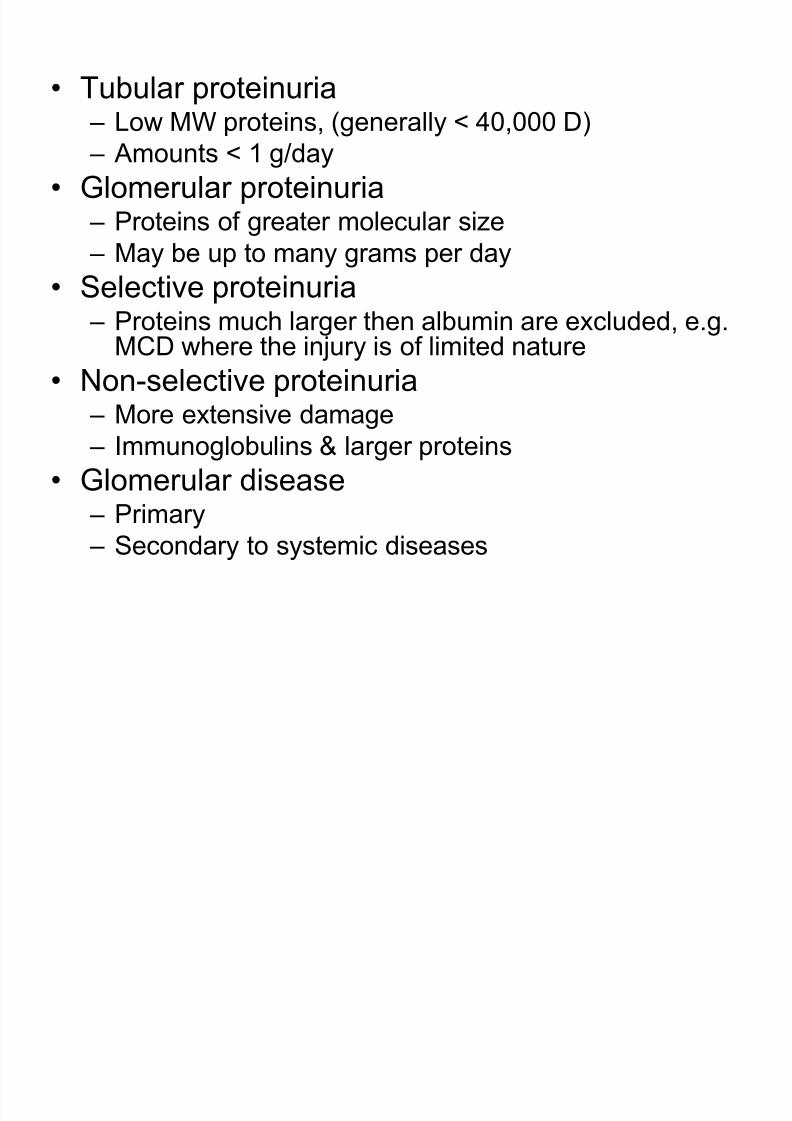
• Tubular proteinuria – Low MW proteins, (generally < 40,000 D)
– Amounts < 1 g/day
• Glomerular proteinuria – Proteins of greater molecular size
– May be up to many grams per day
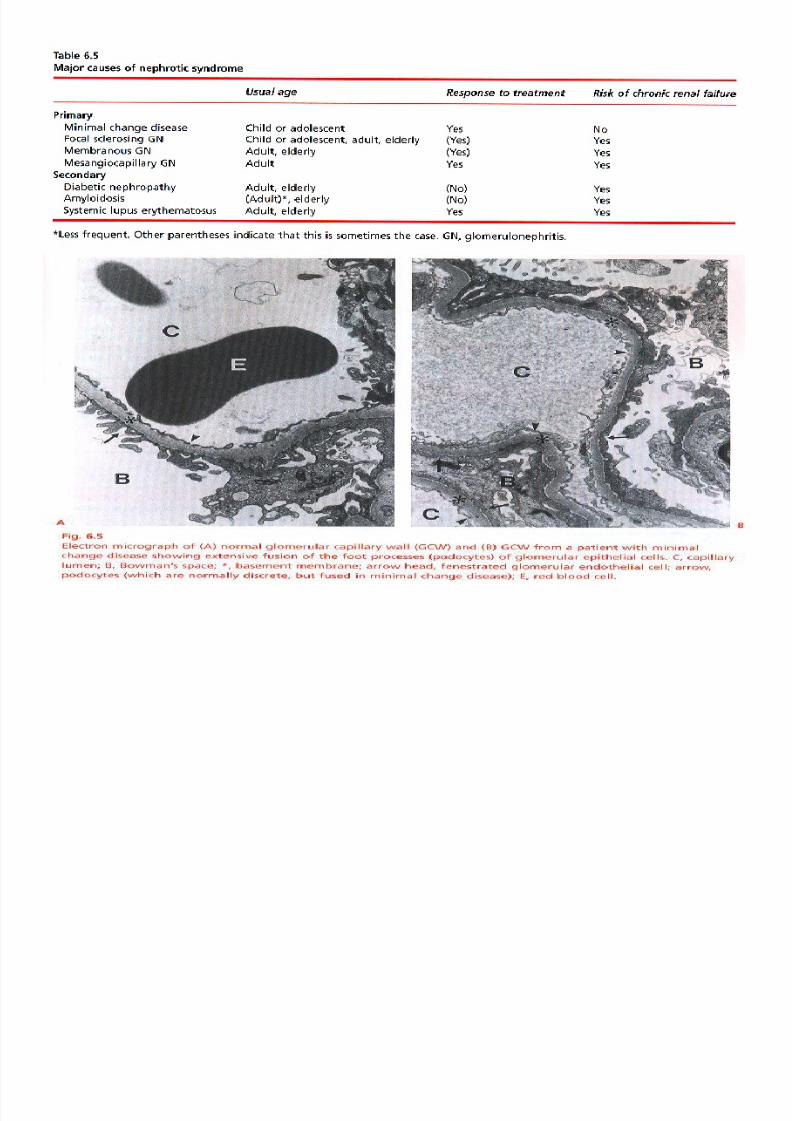
• Selective proteinuria – Proteins much larger then albumin are excluded, e.g.
MCD where the injury is of limited nature
• Non-selective proteinuria
– More extensive damage – Immunoglobulins & larger proteins
• Glomerular disease – Primary
– Secondary to systemic diseases
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 9/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 10/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 11/38
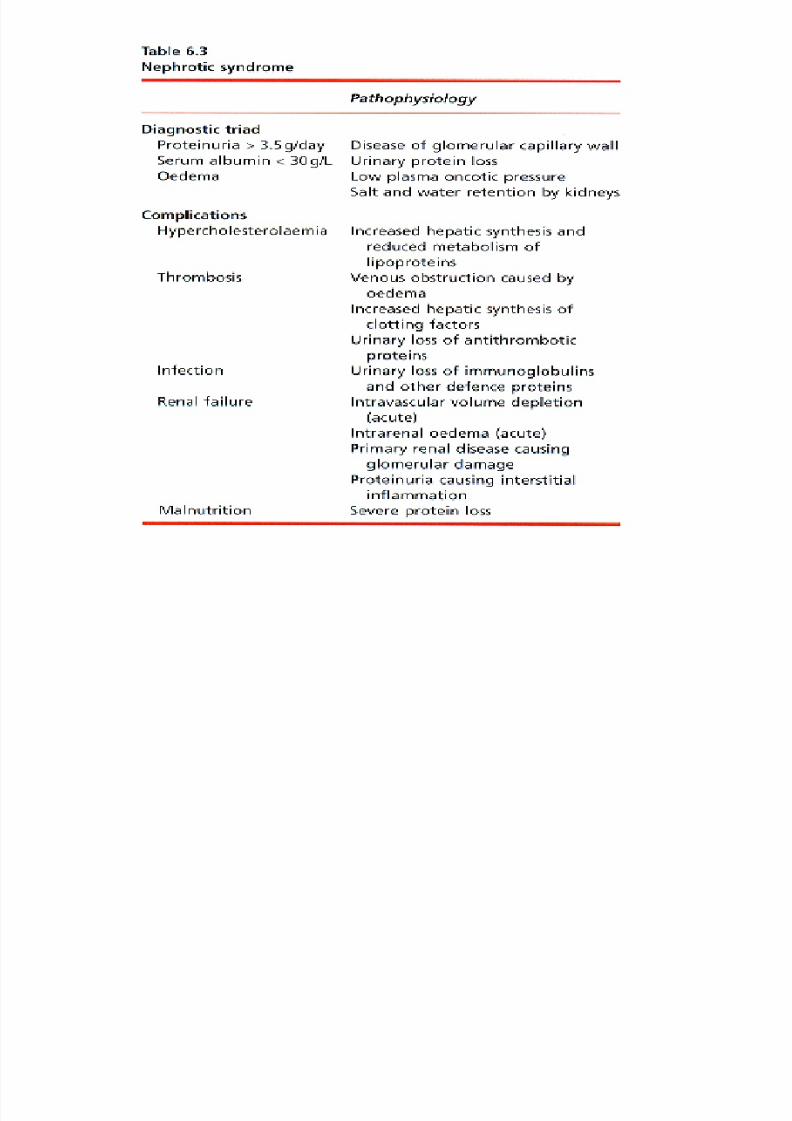
Case
• 6 y/o girl with progressive swelling on her
face, ankles, BP 95/60, otherwise normal.
PMHx (-). UA: protein++++
• Cr=0.5 mg/dl, Alb 1.3 g/dl,
urine microscopy: many hyaline casts,
24h U protein =6g, cholesterol elevated
• Patient was referred to a nephrologist for a
possible renal biopsy
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 12/38
• Percutaneous renal biopsy can be performed toestablish the correct diagnosis & prognosis in patients
with suspected parenchymal renal disease.• It is usually a safe procedure, but bleeding complications
can occur.
• It may not be used
– when the diagnosis is In little doubt, – when it is unlikely to lead to a change in therapy,
– when the chance for complication is greater than usual
• Abnormalities may be – Segmental, involving part of a glomerulus only
– Global, the whole glomerulus
– Focal, involving a few glomeruli only
– Diffuse, involving most glomeruli
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 13/38
.
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 14/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 15/38
Treatment
• In general, the primary forms of GN causing NSare treated with corticosteroids; which have anti-inflammatory action
• In some cases immunosuppressive drugs are
used – Cyclophosphamide
– Azathioprine / Imuran
– Mycophenolic acid / MMF
– Cyclosporin• With secondary GN, treatment is directed
towards the primary disease
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 16/38
GLOMERULONEPHRITIS
&
ACUTE NEPHRITICSYNDROME

7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 17/38
Acute glomerulonephritis
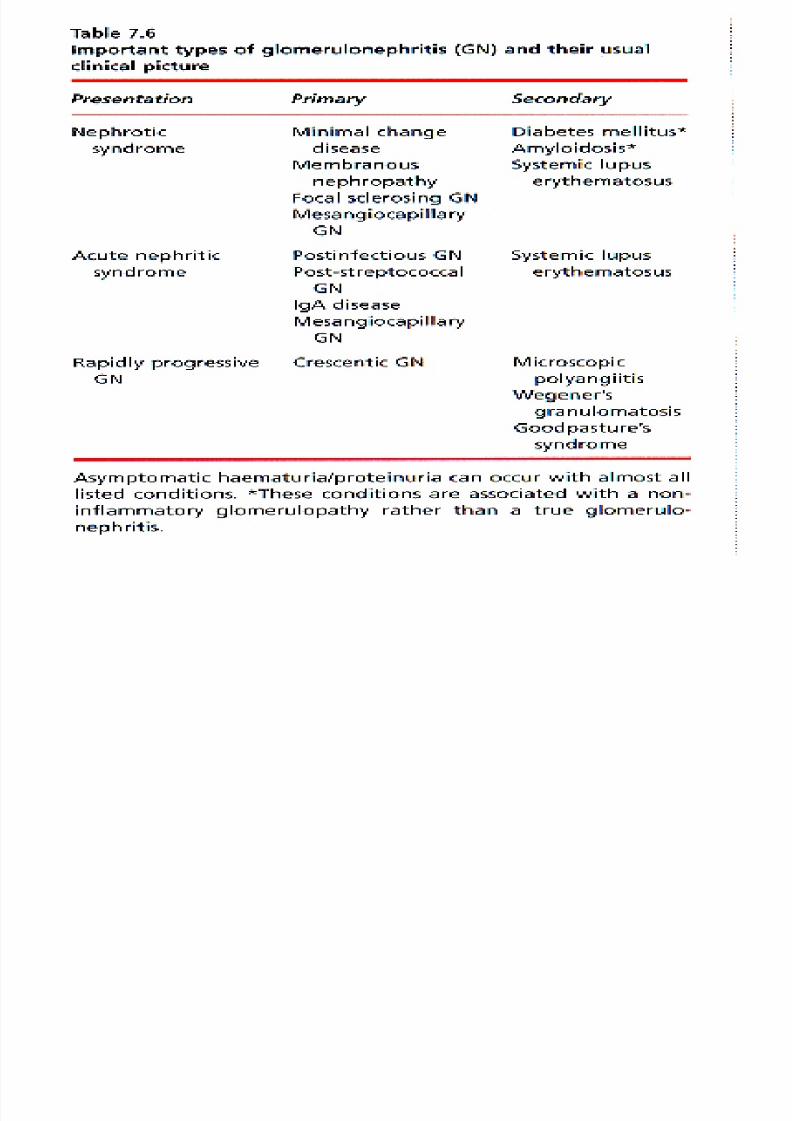
• Inflammatory renal disease involving theglomeruli of all or some of the millionnephrons of each kidney
• Classification based on pathologicalappearance of glomeruli, and other components of the nephron; blood
vessels, interstitium• Primary or idiopathic
• Secondary to a another (systemic) disease
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 18/38
• To confirm the presence of renal inflammation, urine
sediment examination should be performed on acentrifuged sample of fresh urine (casts may breakdownwithin 1-2h)
• When cells or cellular debris aggregate in the tubular lumen, they may form casts of the tuble
• Granular or cellular casts (epithelial, red, or white cells)indicate the presence of renal parenchymal disease
• Hyaline – proteinaceous – casts are found withproteinuria
• An active sediment contains elements consistent withrenal inflammation and/or cell necrosis
• A benign sediment may contain a few cells and onlyhyaline casts.

7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 19/38

7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 20/38
Nephritic Syndrome
• Hematuria, Hypertension, reduced GFR
• Active urinary sediment and Hematuria areindicative of renal inflammation
• Oliguria & renal impairment are aconsequence of glomerular infiltration withinflammatory cells & release of vasoactive
hormones & cytokines• Hypertension is the result of salt & water
retention & vasoactive hormone release
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 21/38
Consequences of glomerular disease
• Proteinuria; due to impaired filtration barrier of GCW
• Hematuria; due to leak into Bouwman’s space acrossGCW or into tubular lumen
• Renal impairment; multifactorial – Acute inflammatory process
• Proliferation intrinsic glomerular cells
• Glomerular infiltration with leukocytes• Haemodynamic changes induced by vasoactive hormones &
cytokines
– Chronic renal scarring• Caused by continuing inflammation,hypertension, proteinuria &
other factors
– Structural and/or functional damage of glomeruli andtubulointerstitium
• Hypertension – Salt and water retention
– Glomerular capillary & arteriolar scarring
– Neurohumoral changes, in particular activation of Renin- Angiotensin system
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 22/38
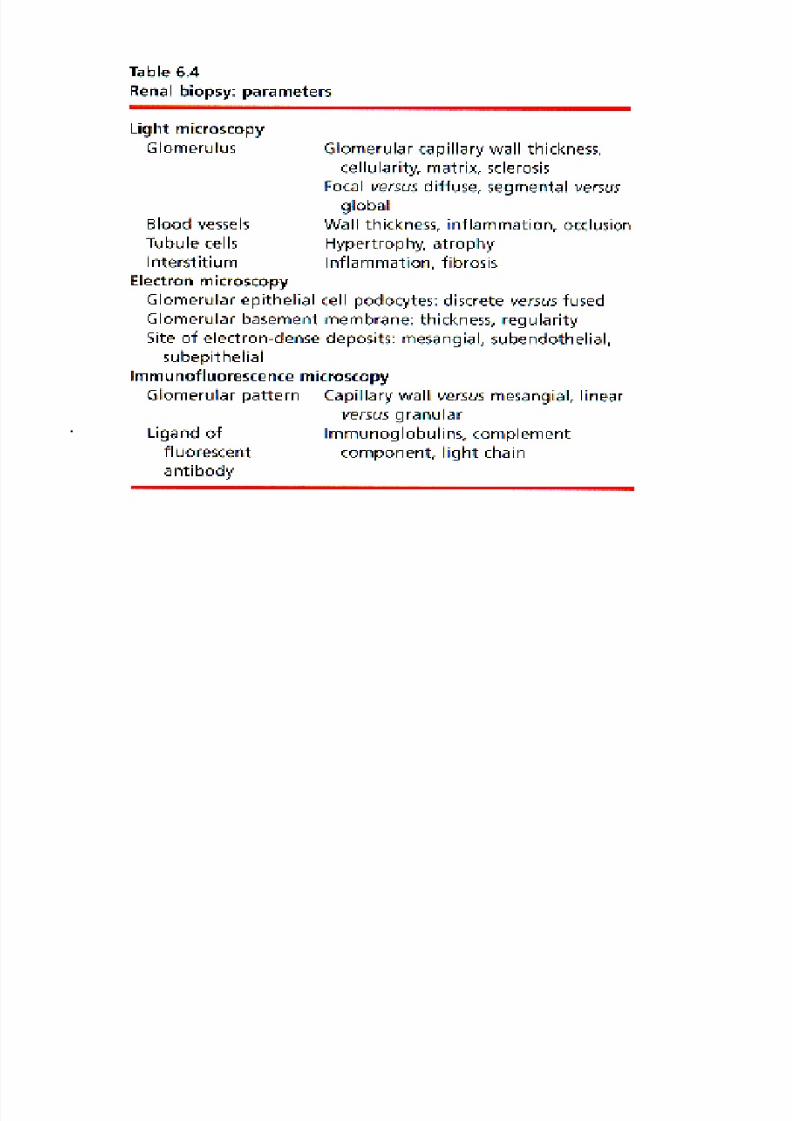
Diagnosis of glomerular disease /
nephritic syndrome• Combination of clinical features, serologic tests, and
renal biopsy
• A positive test result suggest the primary diagnosis, butdoes not prove that it is the cause of the renal disease
• Renal biopsy usually establishes the diagnosisdefinitively
• GN may occur in isolation or as part of a multisystemdisease
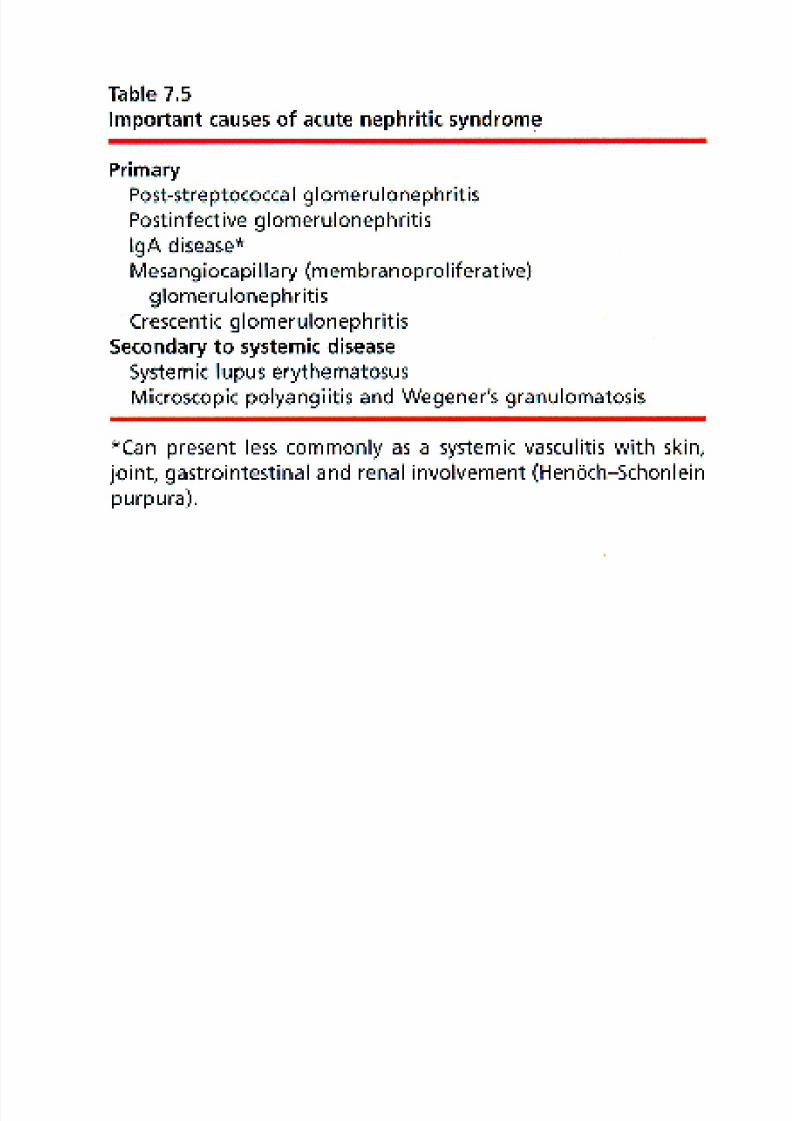
• Acute nephritic syndrome can occur either restricted tothe kidney or involve multiple organ (systemic disease)
• Without rapid treatment, irreversible renal failure maydevelop over a short period
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 23/38
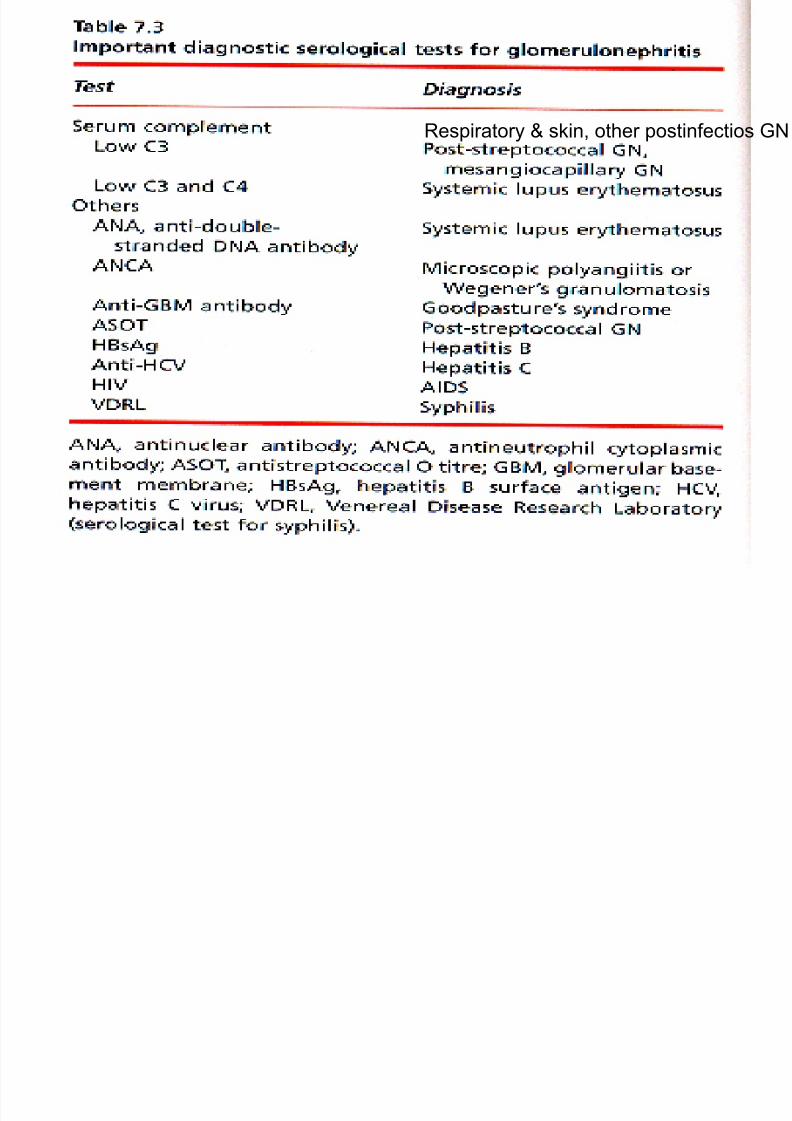
Respiratory & skin, other postinfectios GN
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 24/38
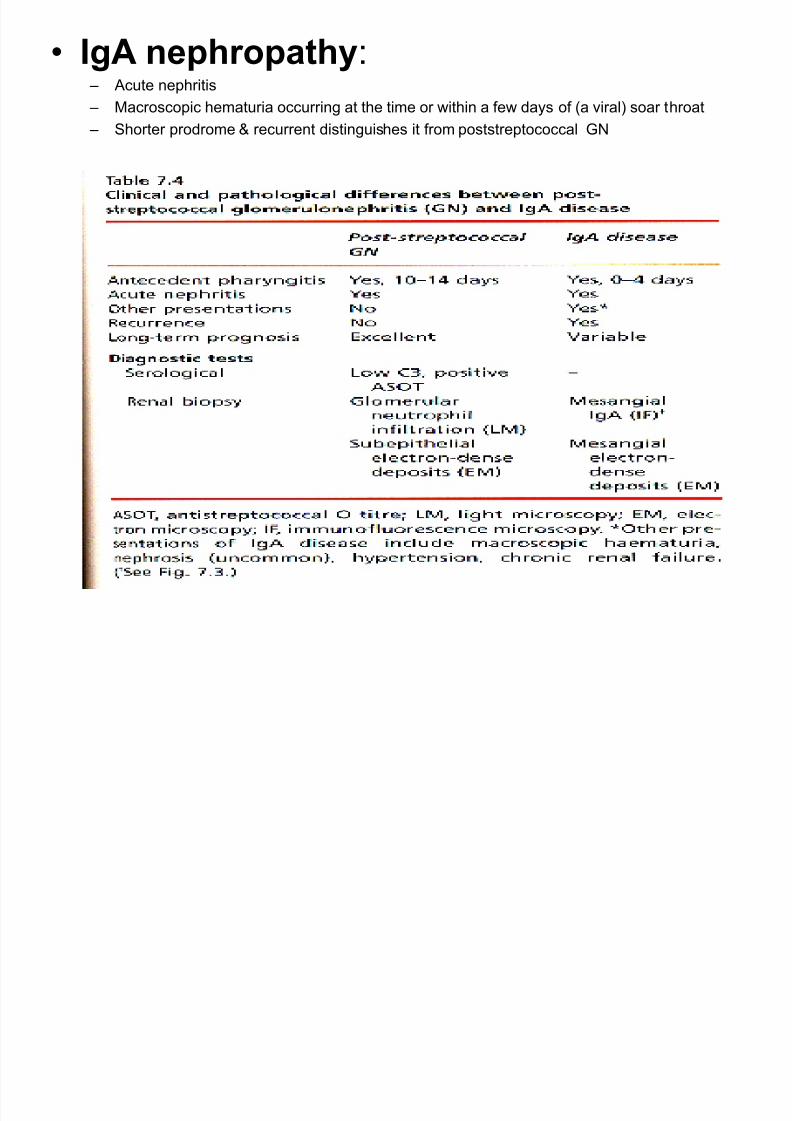
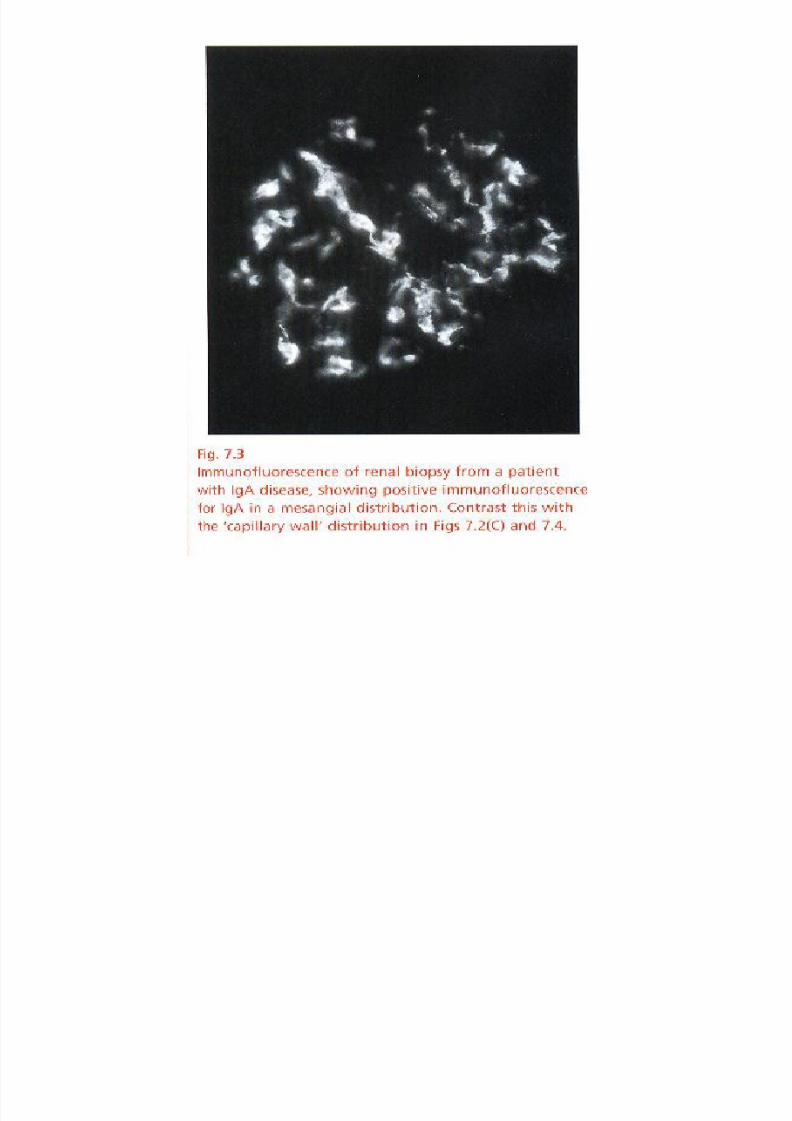
• IgA nephropathy: – Acute nephritis
– Macroscopic hematuria occurring at the time or within a few days of (a viral) soar throat
– Shorter prodrome & recurrent distinguishes it from poststreptococcal GN
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 25/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 26/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 27/38
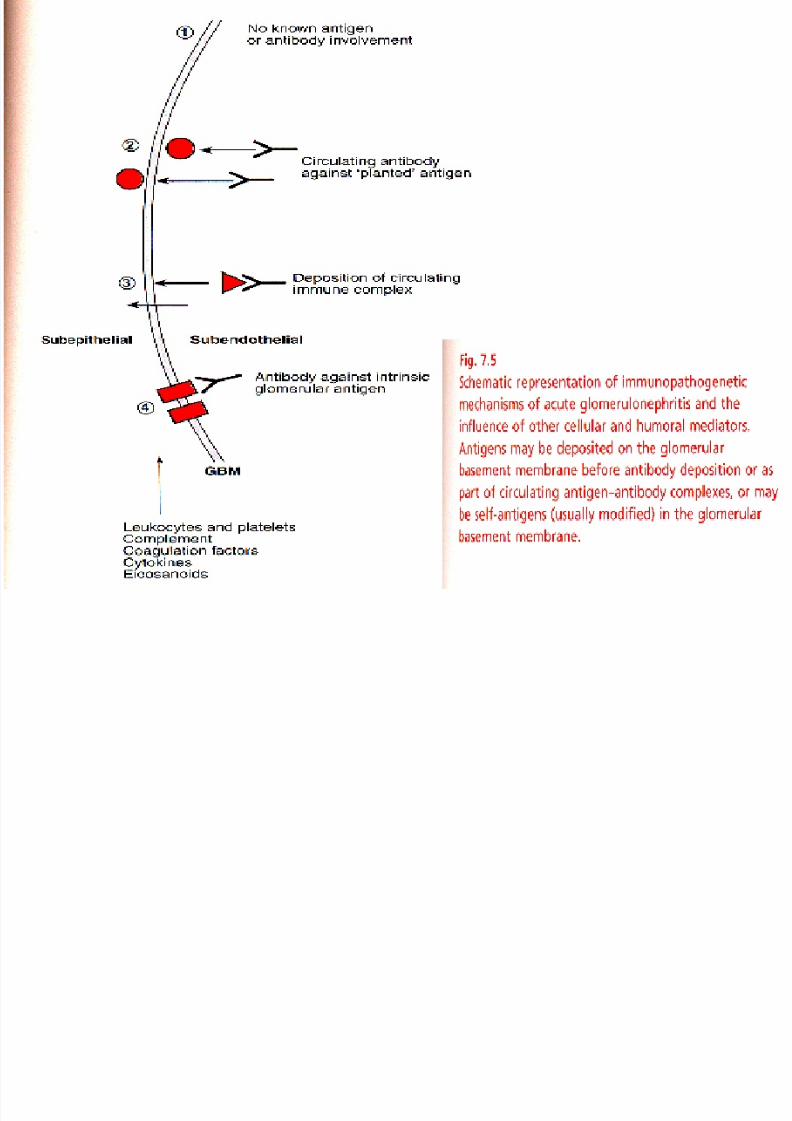
Pathologenesis of acute glomerulonephritis
• GN may be initiated by an immune response to – An exogenous antigen, e.g. streptococcal
– An endogenous antigen, e.g. DNA in SLE
– Autoimmune response to a renal antigen, e.g. GBM in Goodpasteur’ssyndrome
• The antibodies involved in these responses form the basis for diagnostic serological tests
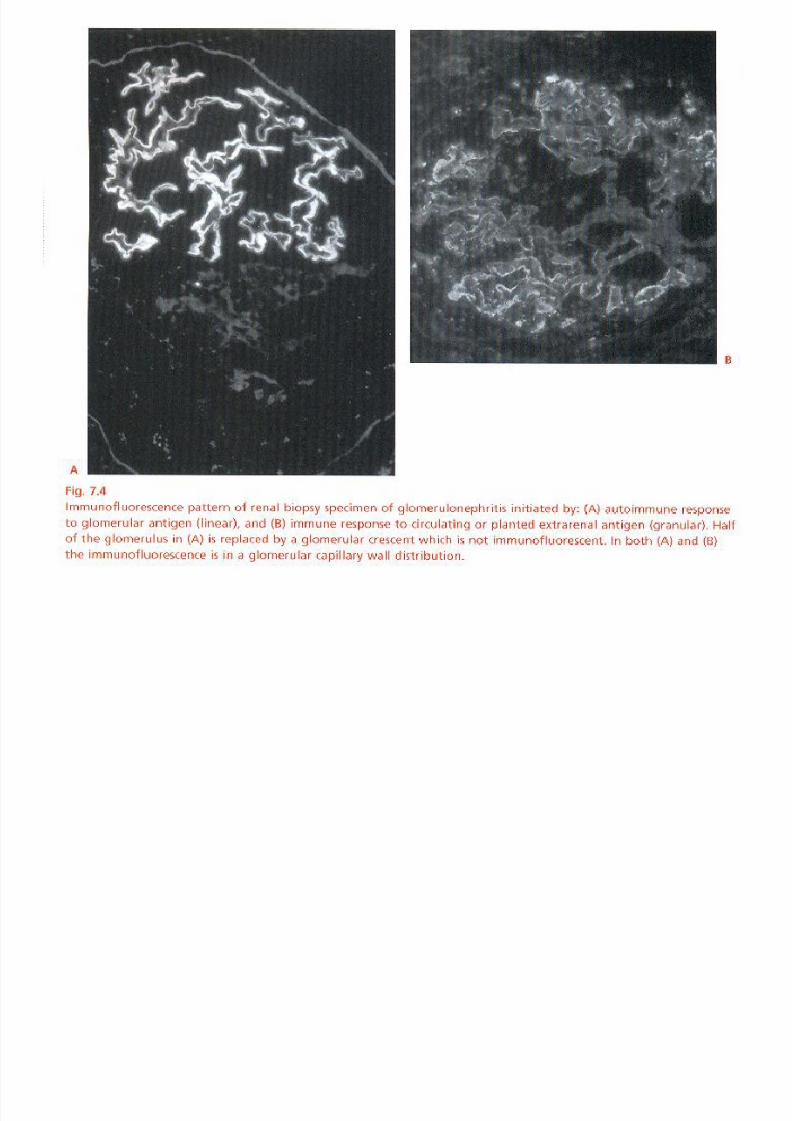
• Ag is part of a circulating IC , or is deposited in the kidney to form anIC in situ – the IF pattern is discontinues or granular
– Corresponding electron-dense deposits are seen wit EM
– E.g. membranous GN, post-streptococcal GN, and SLE
• If the AB is directed against an intrinsic renal Ag – IF pattern is continuous / linear
– No electron-dense deposits on EM
– E.g. Goodpasteur’s syndrome
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 28/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 29/38
Pathology of acute GN
• The glomerulus may be altered in a # of ways in GN – Intrinsic cells – endothelial, mesangial, epithelial – may
proliferate
– Circulating leukocytes may infiltrate
– Platelets may accumulate mesangial matrix may expand
– The GBM may change
– Scarring may develop
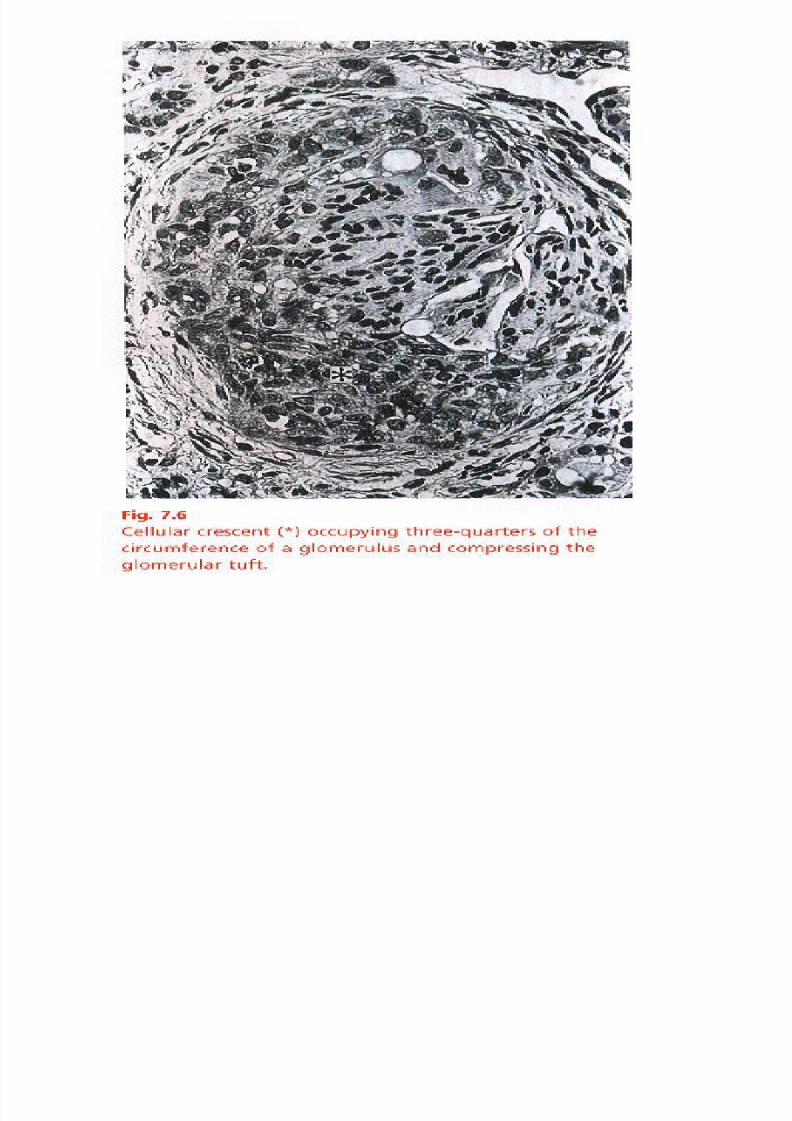
• Hallmark of severe disease is development of aglomerular crescent
– A cellular, fibrinous, and later, fibrous lesion in Bouwman’sspace
– The greater the size, and the number of crescents, the moresevere the disease
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 30/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 31/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 32/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 33/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 34/38
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 35/38
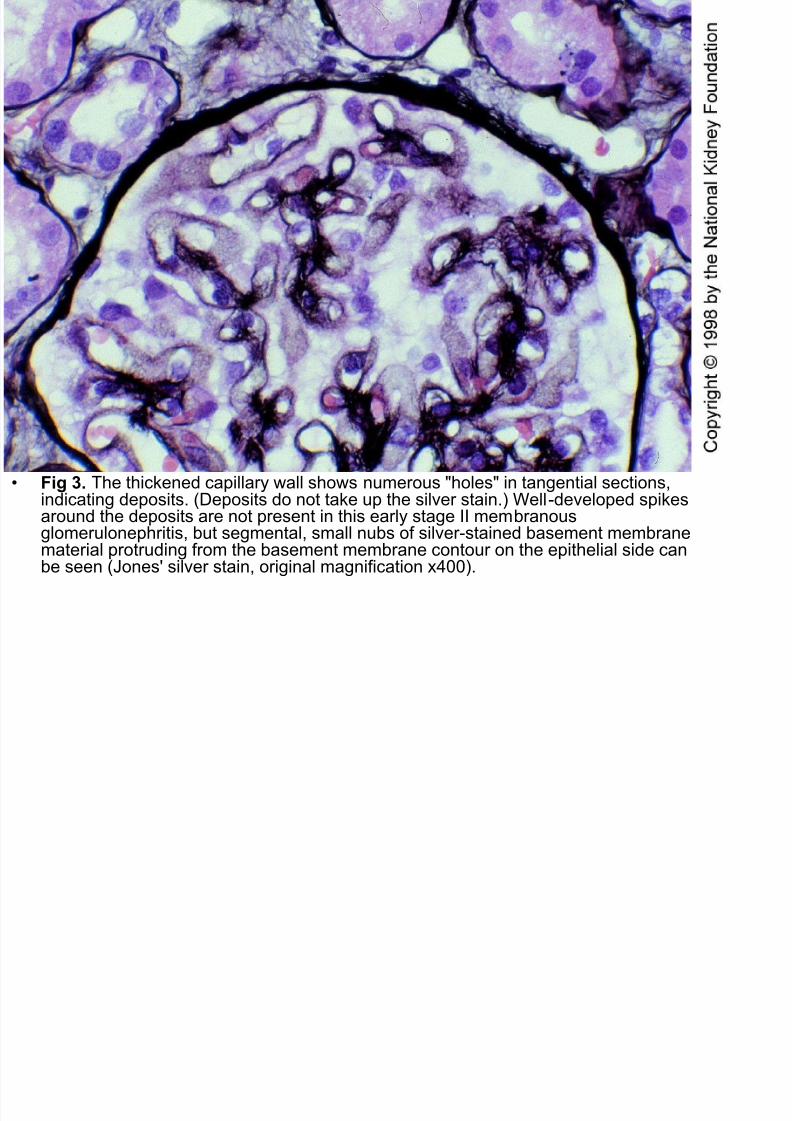
• Fig 3. The thickened capillary wall shows numerous "holes" in tangential sections,indicating deposits. (Deposits do not take up the silver stain.) Well-developed spikesaround the deposits are not present in this early stage II membranousglomerulonephritis, but segmental, small nubs of silver-stained basement membrane
material protruding from the basement membrane contour on the epithelial side canbe seen (Jones' silver stain, original magnification x400).
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 36/38
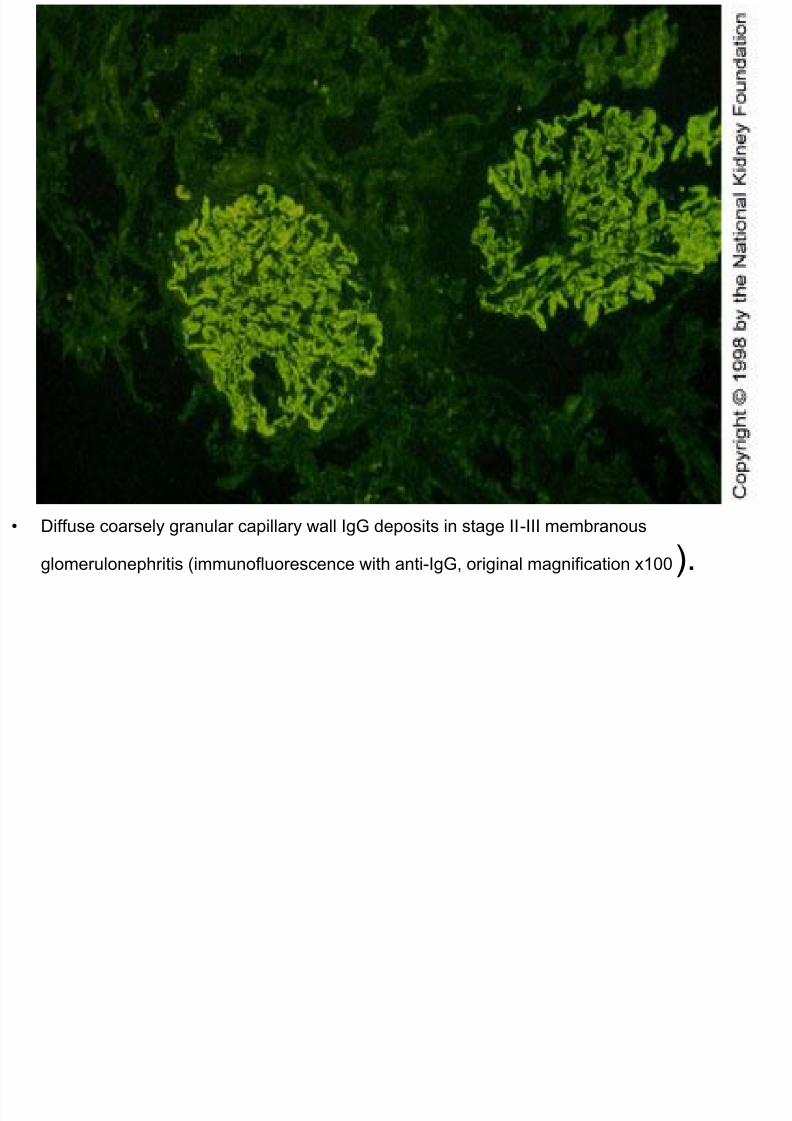
• Diffuse coarsely granular capillary wall IgG deposits in stage II-III membranous
glomerulonephritis (immunofluorescence with anti-IgG, original magnification x100).
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 37/38
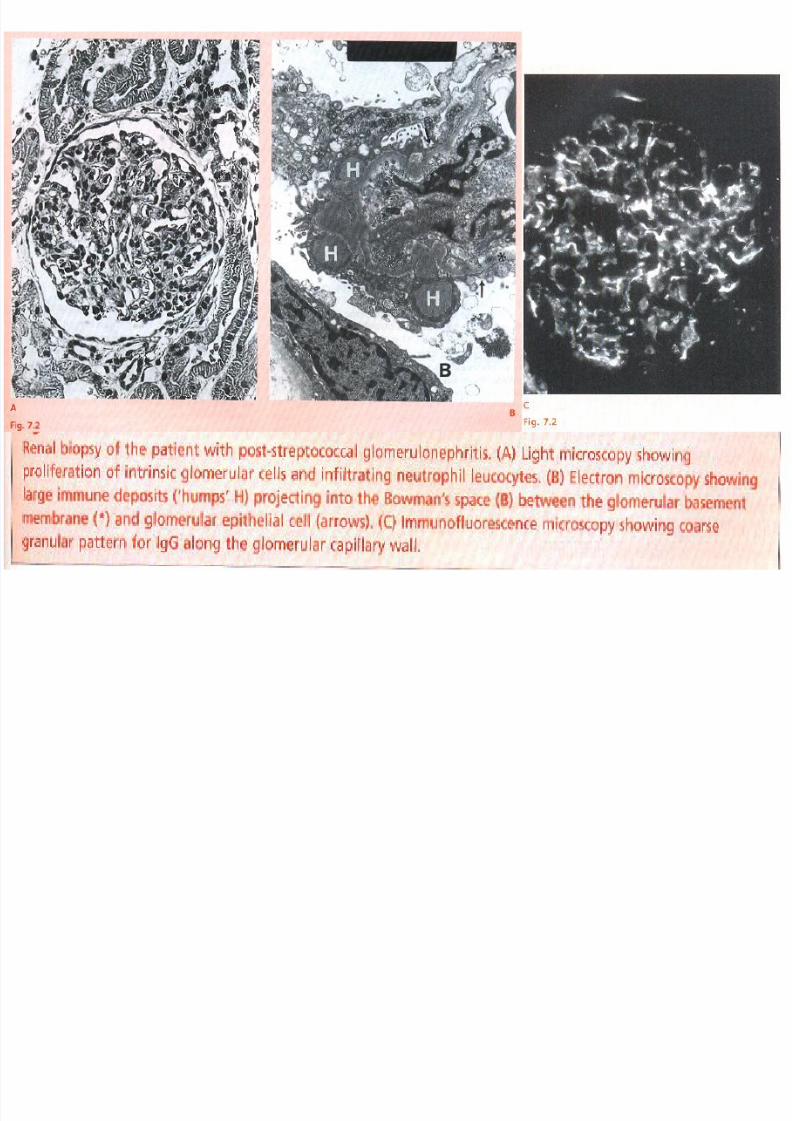
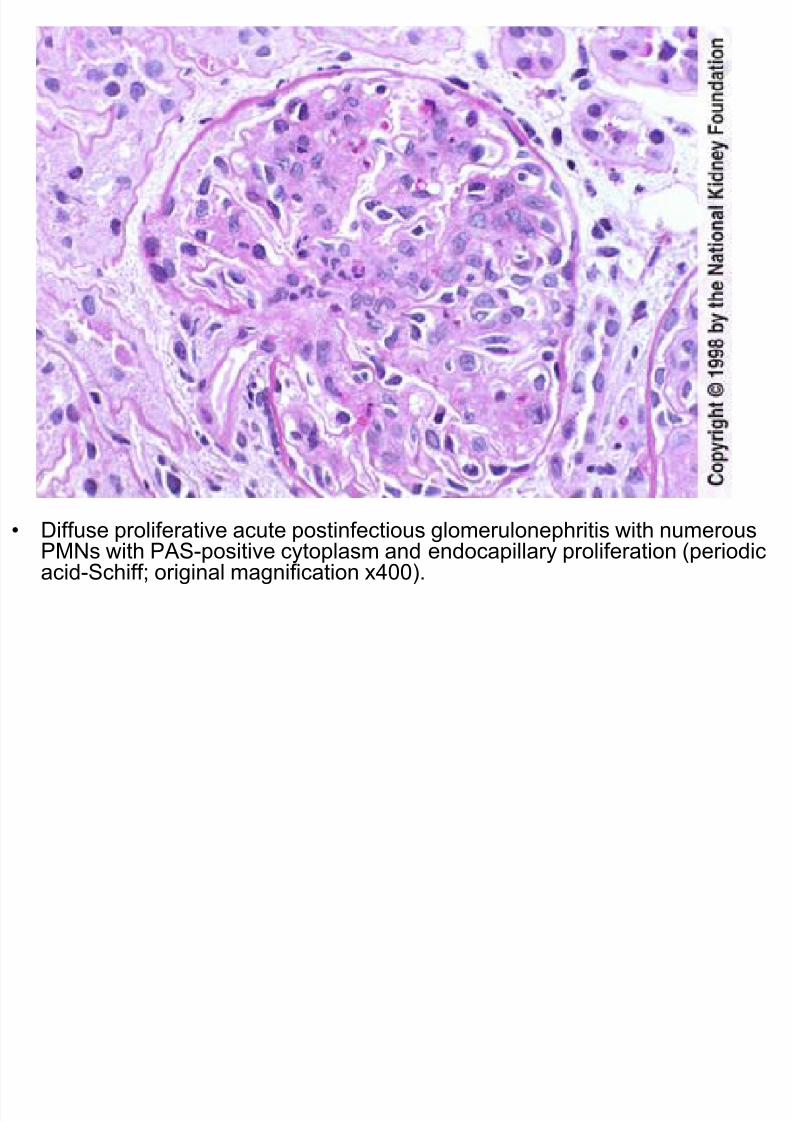
• Diffuse proliferative acute postinfectious glomerulonephritis with numerous
PMNs with PAS-positive cytoplasm and endocapillary proliferation (periodicacid-Schiff; original magnification x400).
7/29/2019 PROTEINURIA &
http://slidepdf.com/reader/full/proteinuria- 38/38
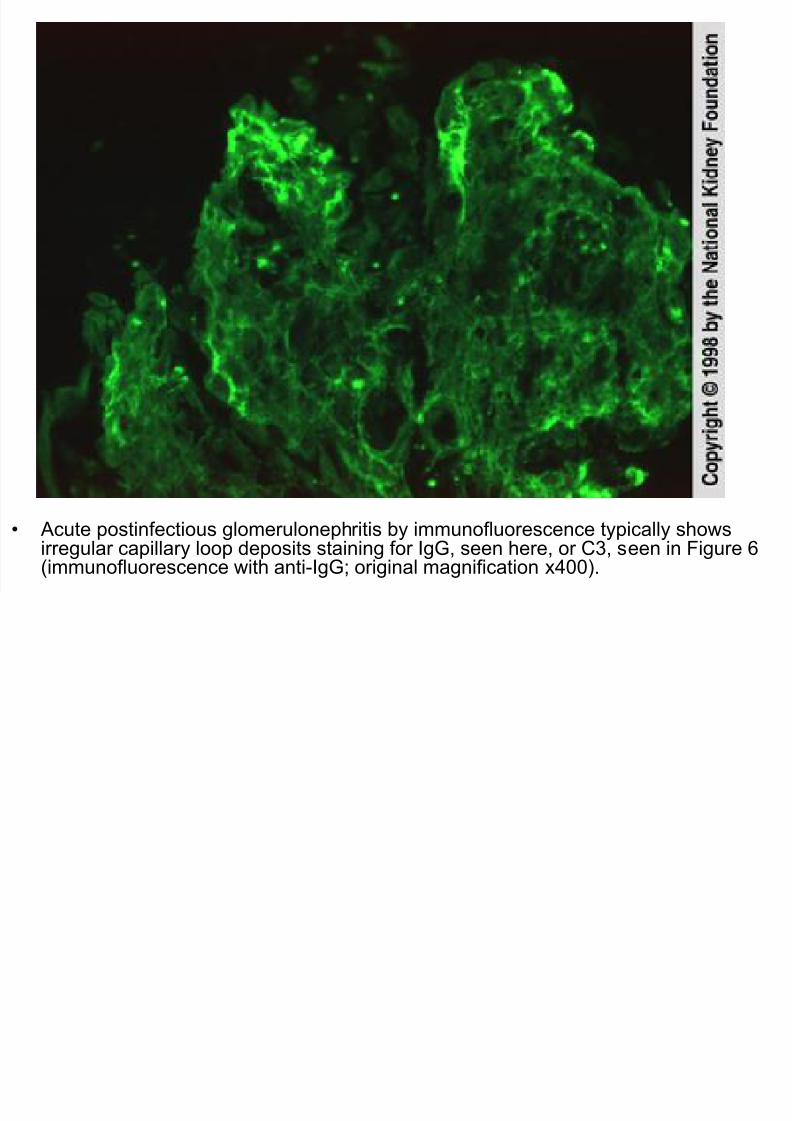
• Acute postinfectious glomerulonephritis by immunofluorescence typically shows
i l ill l d it t i i f I G h C3 i Fi 6(i fl ith ti I G i i l ifi ti 400)





























