Embed Size (px)
Citation preview

Revitalize Our Children:

Revitalize Our Children:
How health care providers can understand and help our overweight children
Revitalize Our Children:
Objectives: Review prevalence of pediatric obesity Identify co morbidities of overweight
conditions in children Identify risk factors for pediatric obesity Suggest prevention and treatment strategies
David B. Jack, M.D.

Corpulence
Obesity now affects 17% of all children and adolescents in the United States - triple the rate from just one generation ago
Since 1980, obesity prevalence among children and adolescents has almost tripled

Background Differences
There are significant racial and ethnic disparities in obesity prevalence among U.S. children and adolescents. In 2007—2008, Hispanic boys, aged 2 to 19 years, were significantly more likely to be obese than non-Hispanic white boys, and non-Hispanic black girls were significantly more likely to be obese than non-Hispanic white girls.
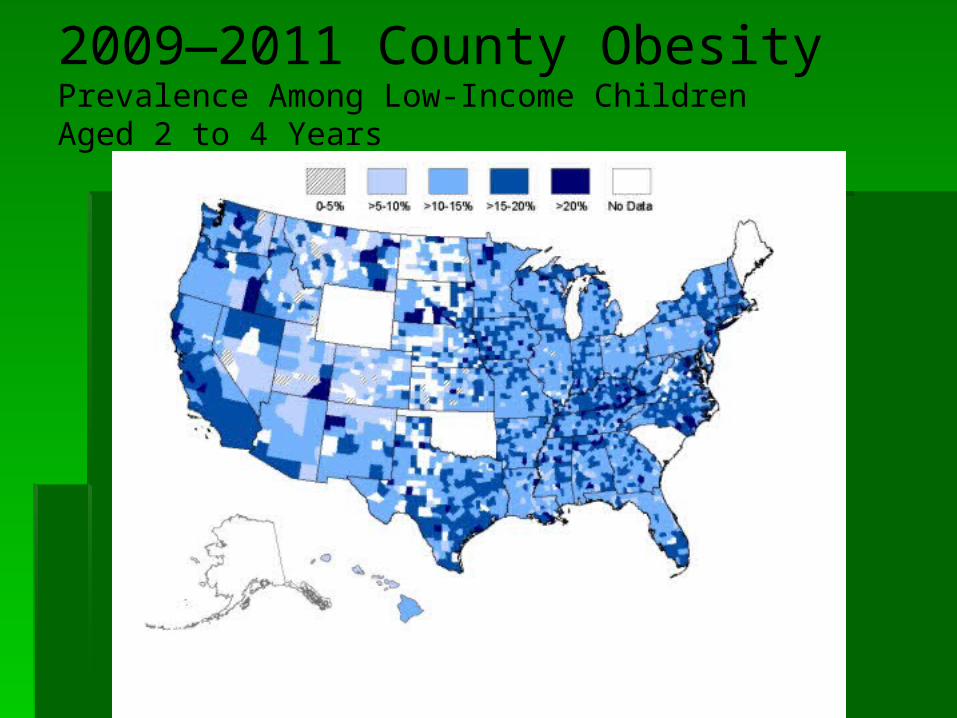
2009—2011 County Obesity Prevalence Among Low-Income ChildrenAged 2 to 4 Years

Washington ranks 18 in overall prevalence with 29.5% of children considered either overweight or obese.

Washington State:
% Children Ages 6- 17 with TV in Bedroom:
32.0%
% Children Ages 12-17 Not Eating Family Meals Most Days of Week:
25.8%
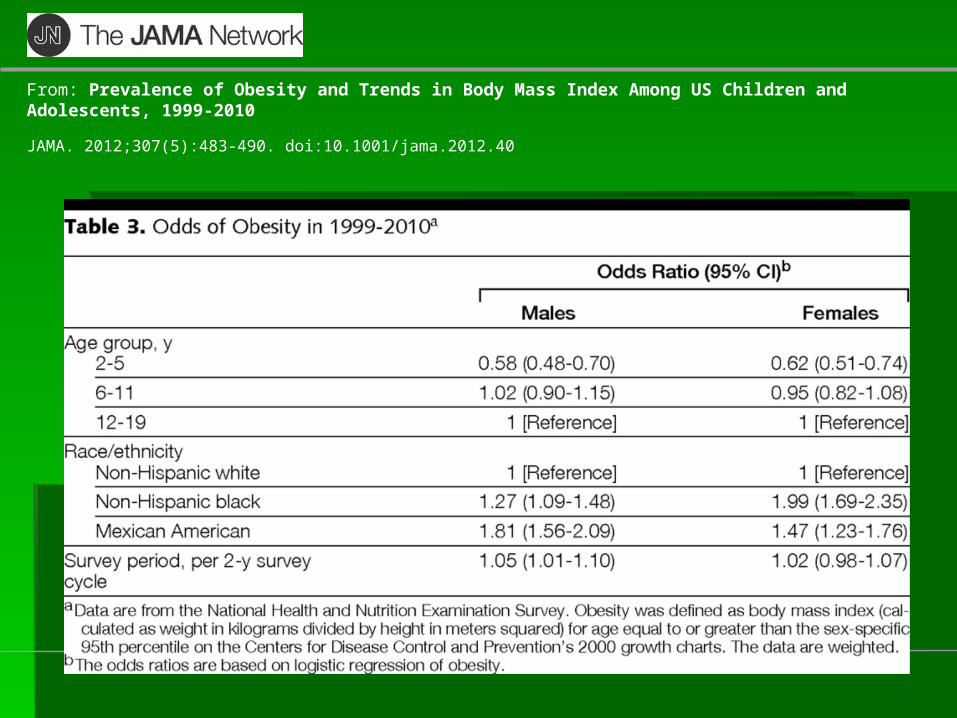
Copyright © 2012 American Medical Association. All rights reserved.
From: Prevalence of Obesity and Trends in Body Mass Index Among US Children and Adolescents, 1999-2010
JAMA. 2012;307(5):483-490. doi:10.1001/jama.2012.40

What Causes Childhood Obesity?

Sugar drinks and less healthy
foods on school campuses. About 55 million school-aged children are enrolled in
schools across the United States, and many eat and drink meals and snacks there
More than half of U.S. middle and high schools still offer sugar drinks and less healthy foods for purchase
Students have access to sugar drinks and less healthy foods at school throughout the day from vending machines and school canteens and at fundraising events, school parties, and sporting events

Advertising of less healthy foods.
Nearly half of U.S. middle and high schools allow advertising of less healthy foods, which impacts students' ability to make healthy food choices
Foods high in total calories, sugars, salt, and fat, and low in nutrients are highly advertised and marketed through media targeted to children and adolescents, while advertising for healthier foods is almost nonexistent in comparison

Lack of daily, quality physical activity
Most adolescents fall short of the 2008 Physical Activity Guidelines for Americans recommendation of at least 60 minutes of aerobic physical activity each day, as only 18% of students in grades 9—12 met this recommendation in 2007
Daily, quality physical education in school can help students meet the Guidelines. However, in 2009 only 33% attended daily physical education classes

No safe and appealing place, in many
communities, to play or be active. Many communities are built in ways that make
it difficult or unsafe to be physically active. For some families, getting to parks and recreation centers may be difficult, and public transportation may not be available. For many children, safe routes for walking or biking to school or play may not exist. Half of the children in the United States do not have a park, community center, and sidewalk in their neighborhood. Only 27 states have policies directing community-scale design.

Limited access to healthy affordable foods
Some people have less access to stores and supermarkets that sell healthy, affordable food such as fruits and vegetables, especially in rural, minority, and lower-income neighborhoods
Supermarket access is associated with a reduced risk for obesity
Choosing healthy foods is difficult for parents who live in areas with an overabundance of food retailers that tend to sell less healthy food, such as convenience stores and fast food restaurants

Greater availability of high-energy-dense foods
and sugar drinks. High-energy-dense foods are ones that have a lot of
calories in each bite A high-energy-dense diet is associated with a higher
risk for excess body fat during childhood Sugar drinks are the largest source of added sugar and
an important contributor of calories in the diets of children in the United States
High consumption of sugar drinks, which have few, if any, nutrients, has been associated with obesity
On a typical day, 80% of youth drink sugar drinks

Increasing portion sizes
Portion sizes of less healthy foods and beverages have increased over time in restaurants, grocery stores, and vending machines
Children eat more without realizing it if they are served larger portions

Lack of breastfeeding support.
Breastfeeding protects against childhood overweight and obesity
However, in the United States, while 75% of mothers start out breastfeeding, only 13% of babies are exclusively breastfed at the end of 6 months
The success rate among mothers who want to breastfeed can be improved through active support from their families, friends, communities, clinicians, health care leaders, employers, and policymakers.
Children who are breastfed for six months are less likely to become obese

Television and Media
Children 8—18 years of age spend an average of 7.5 hours a day using entertainment media, including TV, computers, video games, cell phones, and movies. Of those 7.5 hours, about 4.5 hours is dedicated to viewing TV

Television and Media
Eighty-three percent of children from 6 months to less than 6 years of age view TV or videos about 1 hour and 57 minutes a day
Television and Media
TV viewing is a contributing factor to childhood obesity because it may take away from the time children spend in physical activities; lead to increased energy intake through snacking and eating meals in front of the TV; and, influence children to make unhealthy food choices through exposure to food advertisements

Health Risks Now
Childhood obesity can have a harmful effect on the body in a variety of ways. Obese children are more likely to have– High blood pressure and high cholesterol, which are
risk factors for cardiovascular disease (CVD). In one study, 70% of obese children had at least one CVD risk factor, and 39% had two or more
Increased risk of impaired glucose tolerance, insulin resistance and type 2 diabetes

Health Risks Now
Childhood obesity can have a harmful effect on the body in a variety of ways. Obese children are more likely to have–
Breathing problems, such as sleep apnea, and asthma
Joint problems and musculoskeletal discomfort

Health Risks Now
Childhood obesity can have a harmful effect on the body in a variety of ways. Obese children are more likely to have– Fatty liver disease, gallstones, and gastro-
esophageal reflux (i.e., heartburn) Obese children and adolescents have a greater risk
of social and psychological problems, such as discrimination and poor self-esteem, which can continue into adulthood


Health Risks Later In Life
Obese children are more likely to become obese adults Adult obesity is associated with a number of serious
health conditions including heart disease, diabetes, and some cancers
If children are overweight, obesity in adulthood is likely to be more severe

Young children ages 2 to 5 have a lower prevalence of
overweight and obesity than older youth.

Among young people ages 2 to 19:
About 31.8 percent are considered to be either overweight or obese, and 16.9 percent are considered to be obese
About 1 in 3 boys (33 percent) are considered to be overweight or obese, compared with 30.4 percent of girls
About 18.6 percent of boys and 15 percent of girls are considered to be obese

Children and Adolescents Ages 6 to 19:
Almost 1 in 3 (33.2 percent) are considered to be overweight or obese, and 18.2 percent are considered to be obese
More than 2 in 5 black and Hispanic youth (more than 41 percent) are considered to be overweight or obese*
About 25.7 percent of black, 22.9 percent of Hispanic, and 15.2 percent of white youth are considered to be obese*
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. Journal of the American Medical Association. 2012; 307(5):483–90.

Childhood Obesity
Obesity now affects 17% of all children and adolescents in the United States - triple the rate from just one generation ago
Since 1980, obesity prevalence among children and adolescents has almost tripled

How Do We Diminish the Problem?





• Build a Healthy Plate With Fruits• Build a Healthy Plate With Vegetables• Build a Healthy Plate With Dry Beans and Peas• Meat and Meat Alternates• Build a Healthy Plate With Whole Grains• Build a Healthy Plate With Less Salt and Sodium• Fats and Oils: Build a Healthy Plate With Options Low in Solid Fats
• Build a Healthy Plate With Less Added Sugars• Make Water Available Throughout the Day• Provide Opportunities for Active Play Every Day• Encourage Active Play and Participate With Children• Promote Active Play Through Written Policies and Practices• Limit Screen Time• Appendix B: Care for Children With Food Allergies (updated 1/17/13)

Fat Prevention Begins At Home

Fat Prevention Begins At Home

Make Meal Times a Family Affair

Be a Good Role Model -----

Not a Poor Example

Beans and Peas
Help children feel full longer and maintain a healthy weight
Promote proper digestion and make children’s “potty time” easier by providing dietary fiber
Add shape, texture, and flavor to children’s plates

Fruits, Vegetables
Add color, texture, and flavor to children’s plates Give children the vitamins and minerals they need
to grow and play Add color, crunch, and flavor to children’s plates Promote proper digestion, help children feel full,
and provide fiber for fullness

Decreasing Solid Fats
Make food fun “Kangaroo Pockets” (stuff half a whole-grain pita pocket with
sliced chicken, romaine lettuce, shredded carrots, and a little salad dressing)
Try “Crunchy Baked Chicken” (oven-baked chicken tenders coated in crushed whole-grain cereal or breadcrumbs)

Have children help with cooking and let them choose healthy foods

Decreasing Solid Fats
Have children help cook Make a “fruit and yogurt parfait” by topping nonfat plain yogurt
with whole-grain cereal and fresh or frozen berries, banana
slices, fruit canned in 100% juice, a favorite fruit

Encourage Active Play
Display posters and pictures of children and adults being physically active.

Encourage Active Play
Make a chart for tracking physical activity with children’s and child care providers’ names Have children place a sticker or a stamp by
their name every time they participate in active play



Intermountainlive.org

Limit Screen Time
Play music

Limit Screen Time
Organize puzzle time Have easy puzzles children can do alone or
in pairs

Limit Screen Time
Draw, color, create a sculpture, or use play dough

Limit Screen Time
Read with or to children; Provide books

Limit Screen Time

Limit Screen Time
Having the TV on can disturb children’s sleep and play, even if it is on in the background

Limit Screen Time
TV and some DVDs include advertisements for unhealthy foods

Limit Screen Time
The more time children spend playing video games, the more likely they are to have difficulty concentrating in school

Limit Screen Time
Many video games contain violence Computer games can impair children’s
sleep at night, possibly causing them to spend less time in deep sleep. Sleep is important for children’s health and development

Limit Screen Time We know from research that, at least for
boys, the more time they spend playing video games and watching TV, the less active they are

Mistreatment
Almost 100% of obese teenage girls have been at least verbally abused about their weight
Studies show discrimination in school and work settings and in dating and relationships

Body Image
“Skinny” is the only good body type One quarter of all girls age 6 and 7 have
dieted Dieting numbers nearly identical for average
and overweight girls

Body Image
“No one at school eats
lunch because they
don’t want to get fat.”

Food Discussions
Emphasize health, not weight Discuss food in terms of its capacity to provide
energy, and to improve thinking and strength
Do not allow “fat talk” Love children and ourselves Support children in hobbies and passions that have
nothing to do with weight Value their accomplishments
Change the Model
Do not make parties about cupcakes, ice cream, brownies and Cheetos
Try different kinds of foods as a treat Do not associate parties with sugar and
fat food indulgences---fun does not just come with lots of sugar!

Personal Experience
David Gourley Elementary School Disadvantaged neighborhood Half of students do not speak English Attended by speaker 50 years ago when it
first opened Little community support
Became a “Health Mentor”





Congratulations To
___ ___ for Outstanding Achievements and Participation in the
Gold Medal Schools Program for the 2007-2008 School Year
_______________________ _____________
GMS Mentor Date





References
1.) Barlow SE and the Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007;120 Supplement December 2007:S164—S192.
2.) Freedman DS, Mei Z, Srinivasan SR, Berenson GS, Dietz WH. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: the Bogalusa Heart Study. J Pediatr. 2007;150(1):12—17.e2.
3.) Whitlock EP, Williams SB, Gold R, Smith PR, Shipman SA. Screening and interventions for childhood overweight: a summary of evidence for the US Preventive Services Task Force. Pediatrics. 2005;116(1):e125—144.
4.) Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lancet. May 15 2010;375(9727):1737—1748.
5.) Sutherland ER. Obesity and asthma. Immunol Allergy Clin North Am. 2008;28(3):589—602, ix.
6.) Taylor ED, Theim KR, Mirch MC, et al. Orthopedic complications of overweight in children and adolescents. Pediatrics. Jun 2006;117(6):2167—2174.
7.) Dietz W. Health consequences of obesity in youth: Childhood predictors of adult disease. Pediatrics 1998;101:518—525.
8.) Swartz MB and Puhl R. Childhood obesity: a societal problem to solve. Obesity Reviews 2003; 4(1):57—71.

References, cont.
9.) Biro FM, Wien M. Childhood obesity and adult morbidities. Am J Clin Nutr. May 2010;91(5):1499S—1505S.
10.) Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med 1997;37(13):869—873.
11.) Serdula MK, Ivery D, Coates RJ, Freedman DS. Williamson DF. Byers T. Do obese children become obese adults? A review of the literature. Prev Med 1993;22:167—177.
12.) National Institutes of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: the Evidence Report. Bethesda, MD: National Institutes of Health, U.S. Department of Health and Human Services; 1998.
13.) Freedman DS, Khan LK, Dietz WH, Srinivasan SR, Berenson GS. Relationship of childhood overweight to coronary heart disease risk factors in adulthood: The Bogalusa Heart Study. Pediatrics 2001;108:712—718.





























