Embed Size (px)
Citation preview

E-Mail [email protected]
Original Research
Cardiology 2014;129:216–223 DOI: 10.1159/000366096
Role of the MAPKs/TGF-β1/TRAF6 Signaling Pathway in Atrial Fibrosis of Patients with Chronic Atrial Fibrillation and Rheumatic Mitral Valve Disease
Daoliang Zhang a Xu Liu a Xiaoqing Chen a Jun Gu a Feng Li b Wei Zhang b Yue Zheng b
Departments of a Cardiology and b Cardiac Surgery, Shanghai Chest Hospital, Shanghai Jiaotong University, Shanghai , PR China
significantly increased in CAF compared to SR patients. Con-
clusion: The MAPKs/TGF-β1/TRAF6 signaling pathway is in-volved in atrial fibrosis of CAF patients, and TRAF6 may be-come a new target for the treatment of atrial fibrosis.
© 2014 S. Karger AG, Basel
Introduction
Atrial fibrillation (AF) is the most common arrhyth-mia seen in clinical practice, and AF-related abnormali-ties in hemodynamics and thrombotic events may sig-nificantly increase disability and mortality [1–3] . CAF is very common in rheumatic heart disease patients, and AF in these patients is closely related to atrial fibrosis second-ary to atrial structural remodeling. The pathogenesis of atrial fibrosis and the underlying signaling pathways are still poorly understood [4] .
Tumor necrosis factor receptor-associated factors (TRAFs) are important adapter molecules in the cyto-plasm. They have a specific TRAF domain of about 230 amino acids at the C terminus. To date, a total of 6 TRAFs have been identified in mammals. TRAF6, one member of the TRAF family, exerts biological effects via signal transduction. Our previous study showed that the mito-gen-activated protein kinases (MAPKs)/transforming
Key Words
Chronic atrial fibrillation · Atrial fibrosis · Rheumatic mitral valve disease · MAPKs/TGF-β1/TRAF6 signaling pathway
Abstract
Objective: Atrial remodeling is involved in atrial fibrillation (AF), and atrial fibrosis is an important marker of atrial re-modeling. On the basis of our previous animal studies of the mitogen-activated protein kinases (MAPKs)/transforming growth factor β1 (TGF-β1)/tumor necrosis factor pathway in atrial fibrosis, we undertook investigation of this signaling pathway in atrial fibrosis of patients with chronic AF (CAF) and rheumatic mitral valve disease. Methods: Fifty-six rheu-matic mitral valve disease patients were divided into CAF (course of AF >12 months) and sinus rhythm (SR) groups. Left atrial appendage tissue was collected during heart surgery, and pathological examination was done to evaluate atrial fibrosis. Protein and mRNA expression of TGF-β1, TRAF6 and connective tissue growth factor (CTGF) and protein expres-sion of phosphorylated MAPKs and TGF-β-activated kinase 1 (TAK1) were measured. Results: Histological examination re-vealed that the severity of atrial fibrosis in CAF patients was significantly higher, mRNA and protein expression of TGF-β1, TRAF6 and CTGF in CAF were significantly increased, and the protein expression of phosphorylated MAPKs and TAK1 was
Received: June 3, 2014 Accepted after revision: July 24, 2014 Published online: November 4, 2014
Xu Liu Department of Cardiology, Shanghai Chest Hospital Shanghai Jiaotong University, 241 West Huaihai Road Shanghai 200030 (PR China) E-Mail xkliuxu @ 126.com
© 2014 S. Karger AG, Basel0008–6312/14/1294–0216$39.50/0
www.karger.com/crd
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Role of the MAPKs/TGF-β1/TRAF6 Signaling Pathway in AF
Cardiology 2014;129:216–223DOI: 10.1159/000366096
217
growth factor β1 (TGF-β1)/TRAF6 signaling pathway is involved in Ang II-induced proliferation of fibroblasts collected from mouse atrium and the resultant atrial structural remodeling [5] .
Currently, the effects of TRAF6 on atrial structure re-modeling and the potential mechanisms involved are poorly understood, and, in particular, no study of TRAF6 involvement in atrial remodeling has been conducted in the human atrium. On the basis of our previous studies on atrial structural remodeling using in vitro culture of mouse fibroblasts, we hypothesize that TRAF6 plays a crucial role in the pathogenesis of AF. The current study was undertaken to detect the expression of TRAF6 and molecules in the TRAF6 signaling pathway in the atria of patients with chronic AF (CAF).
Materials and Methods
Patients and Sample Collection A total of 56 patients who received surgery due to rheumatic
mitral valve disease were recruited from Shanghai Chest Hospital. According to the presence or absence of chronic AF, patients were classified as those with nonfamilial CAF that was confirmed by elec-trocardiographic examination (the CAF group; course of CAF >12 months; n = 30) and mitral valve disease patients with sinus rhythm (SR) and without AF (the SR group; n = 26). Before surgery, all pa-tients received cardiac Doppler echocardiography and coronary an-giography. Patients with hyperthyroidism, chronic heart failure, sick sinus syndrome, familial isolated AF, chronic pulmonary heart disease, cardiomyopathy or kidney disease, and those receiving a second heart surgery were excluded from the present study. Phar-macotherapy was discontinued in all patients 12 h before surgery.
Left atrial appendage tissue was collected before extracorpo-real circulation was instituted and was then divided into several blocks. One block was fixed in 10% formalin solution for further pathological examination, and the other blocks were stored in tubes in liquid nitrogen at –80 ° C. Informed consent was obtained from each patient and the study was approved by the Ethics com-mittee of Shanghai Chest Hospital. Laboratory personnel were blind as to the cardiac rhythms. All the procedures were done in accordance with the Declaration of Helsinki of the World Medical Association.
Histological Examination and Quantification of the Fibrotic Area Left atrial appendage tissue in 10% formalin solution was di-
vided into several parts, and subjected to pathological examination following HE staining and Masson staining. After Masson stain-ing, 4 sections were randomly selected from each patient for quan-tification of atrial fibrosis. These sections were observed under a Nikon eclipse 50i microscope, and 5 fields were randomly selected from each section. Myocytes were red, and collagen fibers were blue. Collagen fibers in the endocardium were determined, and observation was done at 400× magnification. Representative pho-tographs were captured with the NIS-Elements F camera system,
and the proportion of collagen fibers was quantified with Image-Pro Plus 6.0 analysis. The proportion of fibrotic area was calcu-lated as: fibrotic area/total area ×100%.
Quantitative Real Time PCR Total RNA was extracted from tissue specimens with TRIzol
(Invitrogen, Carlsbad, Calif., USA) and used to synthesize single-stranded complementary DNA with a high-capacity complemen-tary DNA reverse transcription kit (Toyobo, Osaka, Japan). Quan-titative real time RT-PCR involved the use of gene-specific primers (see table 1 for details) and SYBR kit (Takara, Otsu, Japan). Glyc-eraldehyde-3-phosphate dehydrogenase (GAPDH) was used as an internal control. Results were expressed as the fold difference for each gene against GAPDH by the use of the 2 –ΔΔCt method.
Western Blot Assay Total protein was extracted and protein concentration was mea-
sured with Protein Extraction Kit (Thermo Scientific, Waltham, Mass., USA) and BCA Protein Assay Kit (Thermo Scientific), re-spectively. Protein samples were separated on 12% SDS-PAGE gels and transferred onto nitrocellulose membranes. After blocking with 5% BSA in tris-buffered saline Tween, the membranes were incu-bated overnight at 4 ° C with primary antibodies against TGF-β1, connective tissue growth factor (CTGF), TRAF6 (Santa Cruz Bio-technology, Santa Cruz, Calif., USA), extracellular signal-regulated kinase1/2 (ERK1/2), phospho-ERK1/2, p38 MAPK, phospho-p38MAPK, phospho-c-Jun NH(2)-terminal kinase (JNK), TGF-β-activated kinase 1 (TAK1), phospho-TAK1, GAPDH (Cell Signaling Technology, Danvers, Mass., USA) and JNK (Bioworld, St. Louis Park, Minn., USA). After washing, the membranes were incubated with horseradish peroxidase-conjugated secondary antibody for 2 h at room temperature. Western blots were developed using Super-Signal West Femto Chemiluminescent Substrate (Thermo Scientif-ic) and quantified by scanning densitometry. The ratio of the protein interested was subjected to GAPDH and was densitometrically ana-lyzed by Quantity One (Bio-Rad, Hercules, Calif., USA).
Statistics Data for continuous variables were expressed as the mean ±
SEM. A χ 2 test was used to compare categorical variables between two groups. All statistical analyses were performed using SPSS 16.0. Statistical significance was assumed with p < 0.05.
Table 1. Primer sets for PCR amplification
Gene Oligonucleotide primer sequences (5′–3′)TGF-β1 forward: TGGCGATACCTCAGCAACC
reverse: CTCGTGGATCCACTTCCAG
TRAF6 forward: TTGTGCTAGTGCCCTCGAGAAreverse: CTGGAGGAAAAACTGGGGTGA
CTGF forward: GTTTGGCCCAGACCCAACTreverse: GGAACAGGCGCTCCACTCT
GAPDH forward: ATGCCAGTGAGCTTCCCGTCAGCreverse: GGTATCGTGGAAGAACTCATGAC
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Zhang/Liu/Chen/Gu/Li/Zhang/Zheng Cardiology 2014;129:216–223DOI: 10.1159/000366096
218
Results
Clinical Information of Patients The clinical characteristics of the patients are summa-
rized in table 2 . No significant differences were observed between groups in ejection fraction, sex or age. CAF was accompanied by a significant enlargement of the left atri-al diameter (p < 0.01) and a marked increase in pulmo-nary artery pressure (p < 0.05). As expected, a significant difference between the two groups was noted in the use of digitalis and β-blockers (p < 0.01), 2 drugs used to treat AF.
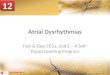
Pathological Examination and Quantification of Fibrotic Area HE staining and Masson staining of the atrial append-
age were done to evaluate atrial fibrosis ( fig. 1 ). When compared to SR patients ( fig. 1 b), HE staining showed muscle fibers in the atrial appendage of the CAF group to exhibit disordered arrangement and cellular enlarge-ment ( fig. 1 a). Patients in both groups had been diag-nosed with rheumatic mitral valve disease, and thus Mas-son staining showed evident atrial fibrosis in both groups. However, atrial fibrosis in the CAF group was more se-
vere than that in the SR group ( fig. 1 c, d). The proportion of fibrotic area in the CAF group was also significantly higher than that in the SR group ( fig. 1 e). These results therefore suggest a potential relationship between AF and atrial fibrosis.
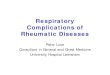
Quantitative Real Time PCR Real time PCR showed that the mRNA expression of
TGF-β1, TRAF6 and CTGF in the CAF group was mark-edly higher than that in the SR group (p < 0.01; fig. 2 ), results suggesting a potential role for TRAF6 in the patho-genesis of AF.
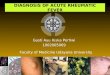
Western Blot Assay Western blot assay showed that the protein expression
of phosphorylated p38 MAPKs, ERK1/2 and JNK in the CAF group was significantly higher than that in the SR group (p < 0.05; fig. 3 ). In addition, when compared with the SR group, the protein expression of TGF-β1, TRAF6, CTGF and phosphorylated TAK1 increased significantly in the CAF group (p < 0.01; fig. 4 ). These data also sug-gest that the MAPKs/TGF-β1/TRAF6 signaling pathway is involved in the pathogenesis of CAF-related atrial fi-brosis.
Table 2. Clinical data of patients
AF (n = 30) SR (n = 26) p value
Sex (male/female) 9/21 8/18 0.95Age, years 58±1.5 53±1.9 0.07LVEF, % 58.7±1.3 58.3±1.4 0.83LA, mm 57.0±1.5 47.0±1.5 <0.001*LVEDd, mm 49.3±1.3 53.5±2.1 0.08LVESd, mm 31.0±1.3 34.2±2.1 0.19IVSd, mm 9.4±0.3 9.2±0.3 0.56LVPWd, mm 9.3±0.3 8.8±0.2 0.21PAP, mm Hg 48.7±2.6 40.6±2.4 0.03*Medication, n
Diuretics 7 4 0.46β-Blockers 11 1 0.003*Digitalis 12 2 0.005*ACEI or AT antagonist 9 6 0.56Calcium antagonist 5 3 0.58Aldosterone antagonist 2 1 0.64Statin 1 1 0.92Nitrate 1 0 0.35
Values are means ± SEM. * p < 0.05. ACEI = Angiotensin-converting enzyme inhibitor; AT antagonist = an-giotensin receptor I antagonist; IVSd = interventricular septum; LA = left atrium; LVEDd = left ventricular end-diastolic diameter; LVEF = left ventricular ejection fraction; LVESd = left ventricular end-systolic diameter; LVPWd = left ventricular posterior wall depth; PAP = pulmonary artery pressure.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Role of the MAPKs/TGF-β1/TRAF6 Signaling Pathway in AF
Cardiology 2014;129:216–223DOI: 10.1159/000366096
219
Discussion
Our results show that TRAF6 expression in CAF pa-tients is markedly increased, and that the expression of mol-ecules in the MAPKs/TGF-β1/TRAF6 signaling pathway is
also increased significantly in these patients. The results of our previous study on mouse fibroblasts have indicated that this signaling pathway is an important one in the pathogen-esis of atrial fibrosis [5] . The above findings show that MAPKs/TGF-β1/TRAF6 is an important pathway involved
Fig. 1. HE ( a , b ) and Masson’s trichrome ( c , d ) staining of the atrial appendage in AF ( a , c ) and SR ( b , d ) pa-tients. Original magnification ×200. Compared with SR patients, atrial muscle distribution showed disarray and myocytolysis in AF patients. There was a significant dif-ference in the fibrosis score between the two groups ( e ). Bars indicate the mean ± SEM. * * p < 0.01.
0
2
4
6
8
10
Fibr
osis
scor
e (%
)
SR AF
**
e
Colo
r ver
sion
avail
able
onlin
e
a b
c d
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Zhang/Liu/Chen/Gu/Li/Zhang/Zheng Cardiology 2014;129:216–223DOI: 10.1159/000366096
220
in Ang II-induced CTGF expression and plays a crucial role in atrial structural remodeling in humans.
AF is the most common arrhythmia, and previous studies have shown that atrial remodeling is the basis for the occurrence and maintenance of AF [6, 7] , and that atrial remodeling is also irreversible. Radiofrequency catheter ablation has been a focus in clinical cardiac elec-trophysiology since the 1990s, and clinical studies have shown that catheter ablation is effective for paroxysmal AF. However, chronic AF patients who have received catheter ablation have a high incidence of recurrence, and a second or even greater number of catheter ablations is
necessary to eliminate AF [8] . Failure of catheter ablation in chronic AF may be attributed to atrial remodeling due to the repeated attacks of AF.
Atrial fibrosis will cause changes in the structure and function of the atrium, and is caused by collagen fiber de-position due to abnormal metabolism in the extracellular matrix. The pathogenesis of atrial fibrosis and the under-lying signaling pathways are still poorly understood, and several pathways are potentially associated with myocar-dial fibrosis [4] . Of these pathways, the role of the renin-angiotensin-aldosterone system (RAAS) in atrial struc-tural remodeling has been extensively studied, and clini-
0
50
100
150
SR AF
TGF-
**
a0
50
100
150
200
SR AF
TRAF6
**
b0
50
100
150
SR AF
CTGF
**
c
Fig. 2. The mRNA expression of TGF-β1 ( a ), TRAF6 ( b ) and CTGF ( c ) in the CAF group was markedly higher than that in the SR group. Bars correspond to the mean ± SEM. All experiments were performed 3 times. * * p < 0.01.
AF
p-p38MAPK
p38MAPK
p-ERK1/2
ERK1/2
JNK
p-JNK
46 kDaa
54 kDa
46 kDa54 kDa
42 kDa44 kDa
42 kDa44 kDa
43 kDa
43 kDa
SR
0
50
100
150
SR AFp-
JNK/
JNK
dens
itorn
etry
(% o
f SR)
*
d0
50
100
150
SR AF
p-ER
K/ER
K de
nsito
rnet
ry (%
of S
R) *
c0
50
100
150
SR AF
p-p3
8/p3
8 de
nsito
rnet
ry (%
of S
R)
*
b
Fig. 3. a Representative Western blot of MAPKs. Each band rep-resents 1 patient with either AF or SR. The protein expression of phosphorylated p38 MAPKs ( b ), ERK1/2 ( c ) and JNK ( d ) in the
CAF group was significantly higher than that in the SR group. Bars correspond to the mean ± SEM. All experiments were performed 3 times. * p < 0.05.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Role of the MAPKs/TGF-β1/TRAF6 Signaling Pathway in AF
Cardiology 2014;129:216–223DOI: 10.1159/000366096
221
cal studies reveal that RAAS inhibitors may benefit patients with AF after pulmonary vein isolation [9] . In addition, basic and clinical studies have shown that RAAS inhibitors can suppress atrial fibrosis and atrial structural remodeling and delay AF [10, 11] .
Ang II is a central factor in the RAAS and may cause vascular contraction, increase cardiac afterload, promote left ventricular hypertrophy, indirectly elevate atrial pres-sure and increase the extensibility of myocytes. In addi-tion, Ang II can increase oxidative stress and, in this way, induce inflammatory collagen fiber deposition, causing atrial fibrosis. In animals with angiotensin-converting enzyme overexpression, Ang II levels increased markedly
and evident atrial enlargement, atrial fibrosis and finally AF were seen [12] . Basic studies have demonstrated that Ang II can promote atrial structural remodeling via the TGF-β1/Smad2/3 signaling pathway [13] . Also, Ang II may bind to its receptor to exert effects via the PKCα-TRAF6-TAK1 signaling pathway [14] . Animal experi-ments indicate that Ang II receptor antagonists may re-verse atrial structural remodeling secondary to rapid atri-al pacing and prevent AF [10] . In the left atrial tissues of AF patients, expression of the type I angiotensin receptor, AT1R, is upregulated, and the synthesis of the extracel-lular matrix increased significantly, suggesting that the AT1R is associated with atrial fibrosis and AF [15] . CTGF
AF
TGF-
TRAF6
CTGF
GAPDH
a82 kDa
82 kDa
37 kDa
38 kDa
60 kDa
SR
0
200
SR AF
dens
itorn
etry
(% o
f SR)
**
e
0
200
SR AFTG
F-de
nsito
rnet
ry (%
of S
R)
**
b
0
200
SR AF
GAPD
Hde
nsito
rnet
ry (%
of S
R)
**
d0
200
SR AF
TRAF
6 GA
PDH
dens
itorn
etry
(% o
f SR)
**
c
Fig. 4. a Representative Western blot of TGF-β1, TRAF6, CTGF and TAK1. Each band represents 1 patient with either AF or SR. The protein expression of TGF-β1 ( b ), TRAF6 ( c ), CTGF ( d ) and
phosphorylated TAK1 ( e ) increased significantly in the CAF group. Bars correspond to the mean ± SEM. All experiments were performed 3 times. * * p < 0.01.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Zhang/Liu/Chen/Gu/Li/Zhang/Zheng Cardiology 2014;129:216–223DOI: 10.1159/000366096
222
is an important cytokine involved in Ang II-induced atri-al fibrosis and atrial structural remodeling [16, 17] .
In recent years, studies have shown that MAPKs acti-vation plays an important role in the pathogenesis of atri-al structural remodeling. MAPKs are a group of crucial downstream molecules of Ang II and are involved in Ang II-induced increase in TGF-β1 expression [17–19] . Ang II-induced increase in TGF-β1 expression has been re-garded as a major mechanism underlying Ang II-induced atrial fibrosis. In our previous study, the results showed that Ang II could increase MAPKs activation in mouse fibroblasts, upregulate the expression of TGF-β1 and CTGF, and promote the proliferation of fibroblasts [5] . In the present study, our findings indicate that atrial ac-tivity of MAPKs in the CAF group is significantly higher than that in the SR group.
TGF-β1 is a key fibrogenic growth factor. TGF-β1 can regulate cell proliferation, apoptosis and migration, and modulate the synthesis of the extracellular matrix (such as to upregulate fibronectin and collagen fiber expres-sion) [20] . Moreover, TGF-β1 overexpression may cause atrial fibrosis and AF [21] . Ang II- or TGF-β1-induced increase in CTGF expression is an important factor in-volved in atrial fibrosis and AF [16, 17] . In the present study, when compared with SR patients, the mRNA and protein expression of TGF-β1 and CTGF increased mark-edly in the atria of CAF patients.
There is evidence showing that TGF-β1 can promote atrial fibrosis via the Smad signaling pathway [13] . TGF-β1 binds to the TGF-β II receptor on the cell mem-brane and then recruits the type I receptor to form a het-erologous complex on the cell membrane. The type I re-ceptor may be phosphorylated by the type II receptor ki-nase and activated. Activated type I receptor further binds to Smad protein and then phosphorylates Smad2/3, two members of the Smad family. Phosphorylated Smad2/3 forms a complex with cytoplasmic Smad4. This complex then translocates into the nucleus and binds to the Smad binding element on the promoter of relevant genes to reg-ulate their expression [22] .
In addition to acting on the classic Smad pathway, TGF-β1 may exert effects via Smad-independent path-ways. There is evidence showing that TRAF6/TAK1 plays a key role in the activation of the TGF-β1/non-Smad sig-naling pathway. TGF-β1 activates the TGF-β receptor and then ubiquitinates TRAF6, an action that results in the binding of TRAF6 to TAK1. Lysine 63 and lysine 158 of TAK1 are ubiquitinated, which activates TAK1 and its downstream pathway [23, 24] . Available studies have shown that TGF-β1-induced activation of the TRAF6/
TAK1 signaling pathway is involved in cell apoptosis, in-flammation and epithelial-mesenchymal transition [25] . In in vitro studies on mouse fibroblasts, our results showed that Ang II could stimulate TGF-β1 on atrial fi-broblasts, an action that conferred effects in a Smad-in-dependent manner [5] . In the present study, the protein expression of TRAF6, CTGF and phosphorylated TAK1 increased markedly in the atrium of the CAF group when compared with the SR group, suggesting that the TGF-β1/TRAF6 signaling pathway is involved in atrial fibrosis.
When atrial structural remodeling is present following atrial fibrosis, this condition is difficult to reverse. Thus, the primary prevention of AF and timely therapy of mild-to-moderate atrial structural remodeling are very impor-tant. In animal models, drugs such as statins, n-3 unsatu-rated fatty acids and Ang II-converting enzyme inhibitors/Ang II receptor antagonists have been found to inhibit atri-al structural remodeling and reduce the incidence of AF [4, 26–30] . With the progression of studies on molecular mechanisms underlying atrial remodeling, some drugs tar-geting atrial remodeling may be helpful to control the oc-currence of AF and the maintenance of SR. Our results show that TRAF6 plays a crucial role in the pathogenesis of atrial remodeling and that the MAPKs/TGF-β1/TRAF6 signaling pathway is important for atrial fibrosis. These findings suggest that blocking this signaling pathway is a promising way to inhibit atrial fibrosis and prevent or delay atrial remodeling, and may be used to prevent and treat AF.
There are limitations in the present study. We directly compared the expression of related proteins in the atrium between two groups, and did not isolate atrial fibroblasts and investigate the influence of Ang II and TRAF6 on the proliferation of human atrial fibroblasts and the MAPKs/TGF-β1/TRAF6 signaling pathway. Thus, we only con-firmed previous findings in vivo that this signaling path-way is altered in CAF patients with atrial fibrosis.
Taken together, our findings suggest that TRAF6 ex-pression increases significantly in the atrium of CAF pa-tients, and that the MAPKs/TGF-β1/TRAF6 signaling pathway is altered in CAF patients with atrial fibrosis. Our findings demonstrate that this pathway is important for Ang II-induced CTGF expression. We speculate that TRAF6 may become a new target for therapy of Ang II-induced atrial fibrosis, which may benefit the prevention and therapy of AF in future.
Conflict of Interest
The authors declare no potential conflicts of interest.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM

Role of the MAPKs/TGF-β1/TRAF6 Signaling Pathway in AF
Cardiology 2014;129:216–223DOI: 10.1159/000366096
223
References
1 Tan AY, Zimetbaum P: Atrial fibrillation and atrial fibrosis. J Cardiovasc Pharmacol 2011; 57: 625–629.
2 Kostin S, Klein G, Szalay Z, Hein S, Bauer EP, Schaper J: Structural correlate of atrial fibril-lation in human patients. Cardiovasc Res 2002; 54: 361–379.
3 Beyerbach DM, Zipes DP: Mortality as an endpoint in atrial fibrillation. Heart Rhythm 2004; 1:B8–B19.
4 Burstein B, Nattel S: Atrial fibrosis: mecha-nisms and clinical relevance in atrial fibrilla-tion. J Am Coll Cardiol 2008; 51: 802–809.
5 Gu J, Liu X, Wang QX, Tan HW, Guo M, Ji-ang WF, Zhou L: Angiotensin II increases CTGF expression via MAPKs/TGF-β1/TRAF6 pathway in atrial fibroblasts. Exp Cell Res 2012; 318: 2105–2115.
6 Allessie M, Ausma J, Schotten U: Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovasc Res 2002; 54: 230–246.
7 Iwasaki YK, Nishida K, Kato T, Nattel S: Atri-al fibrillation pathophysiology: implications for management. Circulation 2011; 124: 2264–2274.
8 Weerasooriya R, Khairy P, Litalien J, Macle L, Hocini M, Sacher F, Lellouche N, Knecht S, Wright M, Nault I, Miyazaki S, Scavee C, Clementy J, Haissaguerre M, Jais P: Catheter ablation for atrial fibrillation: are results maintained at 5 years of follow-up? J Am Coll Cardiol 2011; 57: 160–166.
9 Klemm HU, Heitzer T, Ruprecht U, Meinertz T, Ventura R: Impact of angiotensin-convert-ing enzyme inhibitors and angiotensin II re-ceptor blockers on the long-term outcome af-ter pulmonary vein isolation for paroxysmal atrial fibrillation. Cardiology 2010; 117: 14–20.
10 Nakashima H, Kumagai K: Reverse-remodel-ing effects of angiotensin II type 1 receptor blocker in a canine atrial fibrillation model. Circ J 2007; 71: 1977–1982.
11 Huang G, Xu JB, Liu JX, He Y, Nie XL, Li Q, Hu YM, Zhao SQ, Wang M, Zhang WY, Liu XR, Wu T, Arkin A, Zhang TJ: Angiotensin-converting enzyme inhibitors and angioten-sin receptor blockers decrease the incidence of atrial fibrillation: a meta-analysis. Eur J Clin Invest 2011; 41: 719–733.
12 Xiao HD, Fuchs S, Campbell DJ, Lewis W, Dudley SC Jr, Kasi VS, Hoit BD, Keshelava G, Zhao H, Capecchi MR, Bernstein KE: Mice with cardiac-restricted angiotensin-convert-ing enzyme (ACE) have atrial enlargement, cardiac arrhythmia, and sudden death. Am J Pathol 2004; 165: 1019–1032.
13 He X, Gao X, Peng L, Wang S, Zhu Y, Ma H, Lin J, Duan DD: Atrial fibrillation induces myocardial fibrosis through angiotensin II type 1 receptor-specific Arkadia-mediated downregulation of Smad7. Circ Res 2011; 108: 164–175.
14 Loniewski KJ, Patial S, Parameswaran N: Sen-sitivity of TLR4- and -7-induced NFκB1 p105-TPL2-ERK pathway to TNF-receptor-associated-factor-6 revealed by RNAi in mouse macrophages. Mol Immunol 2007; 44: 3715–3723.
15 Boldt A, Wetzel U, Weigl J, Garbade J, Lauschke J, Hindricks G, Kottkamp H, Gum-mert JF, Dhein S: Expression of angiotensin II receptors in human left and right atrial tissue in atrial fibrillation with and without underly-ing mitral valve disease. J Am Coll Cardiol 2003; 42: 1785–1792.
16 Ko WC, Hong CY, Hou SM, Lin CH, Ong ET, Lee CF, Tsai CT, Lai LP: Elevated expression of connective tissue growth factor in human atrial fibrillation and angiotensin II-treated cardiomyocytes. Circ J 2011; 75: 1592–1600.
17 Liu B, Yu J, Taylor L, Zhou X, Polgar P: Mi-croarray and phosphokinase screenings lead-ing to studies on ERK and JNK regulation of connective tissue growth factor expression by angiotensin II 1a and bradykinin B2 receptors in Rat1 fibroblasts. J Cell Biochem 2006; 97: 1104–1120.
18 Li L, Fan D, Wang C, Wang JY, Cui XB, Wu D, Zhou Y, Wu LL: Angiotensin II increases periostin expression via Ras/p38 MAPK/CREB and ERK1/2/TGF-β1 pathways in car-diac fibroblasts. Cardiovasc Res 2011; 91: 80–89.
19 Naito T, Masaki T, Nikolic-Paterson DJ, Tan-ji C, Yorioka N, Kohno N: Angiotensin II in-duces thrombospondin-1 production in hu-man mesangial cells via p38 MAPK and JNK: a mechanism for activation of latent TGF-β1. Am J Physiol Renal Physiol 2004; 286:F278–F287.
20 Khan R, Sheppard R: Fibrosis in heart disease: understanding the role of transforming growth factor-β in cardiomyopathy, valvular disease and arrhythmia. Immunology 2006; 118: 10–24.
21 Verheule S, Sato T, Everett T, Engle SK, Otten D, Rubart-von der Lohe M, Nakajima HO, Nakajima H, Field LJ, Olgin JE: Increased vul-nerability to atrial fibrillation in transgenic mice with selective atrial fibrosis caused by overexpression of TGF-β1. Circ Res 2004; 94: 1458–1465.
22 Evans RA, Tian YC, Steadman R, Phillips AO: TGF-β1-mediated fibroblast-myofibroblast terminal differentiation – the role of Smad proteins. Exp Cell Res 2003; 282: 90–100.
23 Yamashita M, Fatyol K, Jin C, Wang X, Liu Z, Zhang YE: TRAF6 mediates Smad-indepen-dent activation of JNK and p38 by TGF-β. Mol Cell 2008; 31: 918–924.
24 Yafei N, Belin J, Smith T, Crompton M: Cy-closporin and mitochondrial phospholipid degradation. Biochem Soc Trans 1990; 18: 884–885.
25 Landstrom M: The TAK1-TRAF6 signalling pathway. Int J Biochem Cell Biol 2010; 42: 585–589.
26 Kumagai K, Nakashima H, Urata H, Gondo N, Arakawa K, Saku K: Effects of angiotensin II type 1 receptor antagonist on electrical and structural remodeling in atrial fibrillation. J Am Coll Cardiol 2003; 41: 2197–2204.
27 Sakabe M, Shiroshita-Takeshita A, Maguy A, Dumesnil C, Nigam A, Leung TK, Nattel S: Omega-3 polyunsaturated fatty acids prevent atrial fibrillation associated with heart failure but not atrial tachycardia remodeling. Circu-lation 2007; 116: 2101–2109.
28 Shiroshita-Takeshita A, Brundel BJ, Burstein B, Leung TK, Mitamura H, Ogawa S, Nattel S: Effects of simvastatin on the development of the atrial fibrillation substrate in dogs with congestive heart failure. Cardiovasc Res 2007; 74: 75–84.
29 Li D, Shinagawa K, Pang L, Leung TK, Cardin S, Wang Z, Nattel S: Effects of angiotensin-converting enzyme inhibition on the develop-ment of the atrial fibrillation substrate in dogs with ventricular tachypacing-induced con-gestive heart failure. Circulation 2001; 104: 2608–2614.
30 Savelieva I, Kakouros N, Kourliouros A, Camm AJ: Upstream therapies for manage-ment of atrial fibrillation: review of clinical evidence and implications for European Soci-ety of Cardiology guidelines. Part I: primary prevention. Europace 2011; 13: 610–625.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 11
/12/
2014
2:3
1:42
AM