Embed Size (px)
Citation preview

mokslinës klinikinës studijos
464 teorija ir praktika 2010 - T. 16 (Nr. 4), 464–466 p.
RUPTURED ILIAC ARTERY ANEURYSM AFTER ABDOMINAL AORTIC ANEURYSM RESECTION: A CASE REPORT
PLYŠUSI KLUBO ARTERIJOS ANEURIZMA PO BUVUSIOS PILVO AORTOS ANEURIZMOS REZEKCIJOS (KLINIKINIO ATVEJO PRISTATYMAS)
Tomas Janušauskas1,2, Eugenijus Janušauskas2, Vygantas Kazlauskas2, Dalia Triponienė1, Vytautas Triponis1
¹Vilniaus universiteto Medicinos fakulteto Širdies ir kraujagyslių ligų klinika ²Vilniaus miesto universitetinės ligoninės Kraujagyslių chirurgijos centras
¹Clinic of Heart and Vascular Diseases, Vilnius University Faculty of Medicine²Department of Vascular Surgery, Vilnius City University Hospital
SANTRAUKAReikšminiai žodžiai: pilvo aortos aneurizma, plyšusi klubo arterijos aneurizma.Tikslas. Pristatyti plyšusios klubinės arterijos aneurizmos klinikinį atvejį po buvusios pilvo aortos aneurizmos rezekcijos.Metodas. Straipsnyje pristatomas 62 metų paciento, hospitalizuoto dėl ūmaus pilvo skausmo ir šoko, plyšusios klubo arte-rijos aneurizmos klinikinis atvejis. Šiam pacientui prieš septynis mėnesius buvo atlikta pilvo aortos aneurizmos rezekcija ir aortos rekonstrukcija bifurkaciniu protezu. Abipus bendrosios klubo arterijos buvo persiūtos, tačiau vidinės klubo arterijos liko funkcionuojančios. Pilvo aortos ir bendrųjų klubo arterijų aneurizmos diagnozuotos planinio pilvo ultragarsinio tyrimo metu penkeri metai iki operacijos. Plyšusios kairės bendrosios klubo arterijos aneurizmos dydis ir hematomos vieta patikslinta kompiuterine tomogra� ja. Rezultatai. Ligonis skubiai operuotas atliekant abipus klubo arterijų aneurizmų rezekciją ir persiuvant klubo arterijas. Paci-entas mirė praėjus dviem valandoms po operacijos dėl šoko sukeltų komplikacijų.
ABSTRACTKey words: Abdominal aortic aneurysm, ruptured iliac artery aneurysm.Objective. To present a case of ruptured iliac artery aneurysm after abdominal aortic aneurysm resection.Methods. We report a case of ruptured iliac artery aneurysm in 62 year old man with acute pain of abdomen and shock. Ab-dominal aortic aneurysm resection and aortic reconstruction with bifurcated vascular graft was performed seven months pre-viously. Both common iliac arteries were ligatured, but internal iliac arteries were left functional. Abdominal aortic aneurysm and aneurysms of both common iliac arteries were detected on a routine ultrasound scan � ve years before the reconstruction. � e size of the aneurysm and the location of a haematoma after rupture were speci� ed on CT.Results. � e treatment involved the urgent open resection of ruptured left common iliac artery aneurysm and right common iliac artery aneurysm and ligature of iliac arteries. � e patient died two hours after the operation due to shock complications.
Tomas JanušauskasVilniaus miesto universitetinė ligoninėAntakalnio g. 57, [email protected]
INTRODUCTION We report a case of iliac artery aneurysm rupture seven
months after aortobifemoral graft implantation for aortic and both common iliac arteries aneurysms. � e rupture oc-curred because of persisted circulation in the left iliac artery aneurysm. � e tactics of open surgery used in the case is critically evaluated.
CASE REPORT An abrupt onset of severe abdominal pain and weakness
developed in a 62 years old man. � e pain and progressive faintness have been persisting for 48 hours. On admission
to the Vascular Surgery Department of Vilnius Universi-ty City Hospital the patient was somnolent and his blood pressure reading was of 100/60 mm Hg and a heart rate of 100 beats/min. Physical examination revealed that the abdomen was soft with some tenderness. A painful pulsatile abdominal mass was felt by palpation. Blood test included a white blood cell count of 6.8x109/l, haemoglobin level of 72 g/l, hematocrit level of 22 % and serum creatinine level of 680 µmol/l. � e patient had a low urine output. A ten year history of arterial hypertension was noted. No ot-her signi� cant comorbidities were found. Five years ago the patient has passed routine examination and the abdominal
Copyright © 2010 MEDICINOS TEORIJA IR PRAKTIKA. ISSN 1392-1312. All rights reserved.
mokslinës klinikinës studijos
465 teorija ir praktika 2010 - T. 16 (Nr. 4)
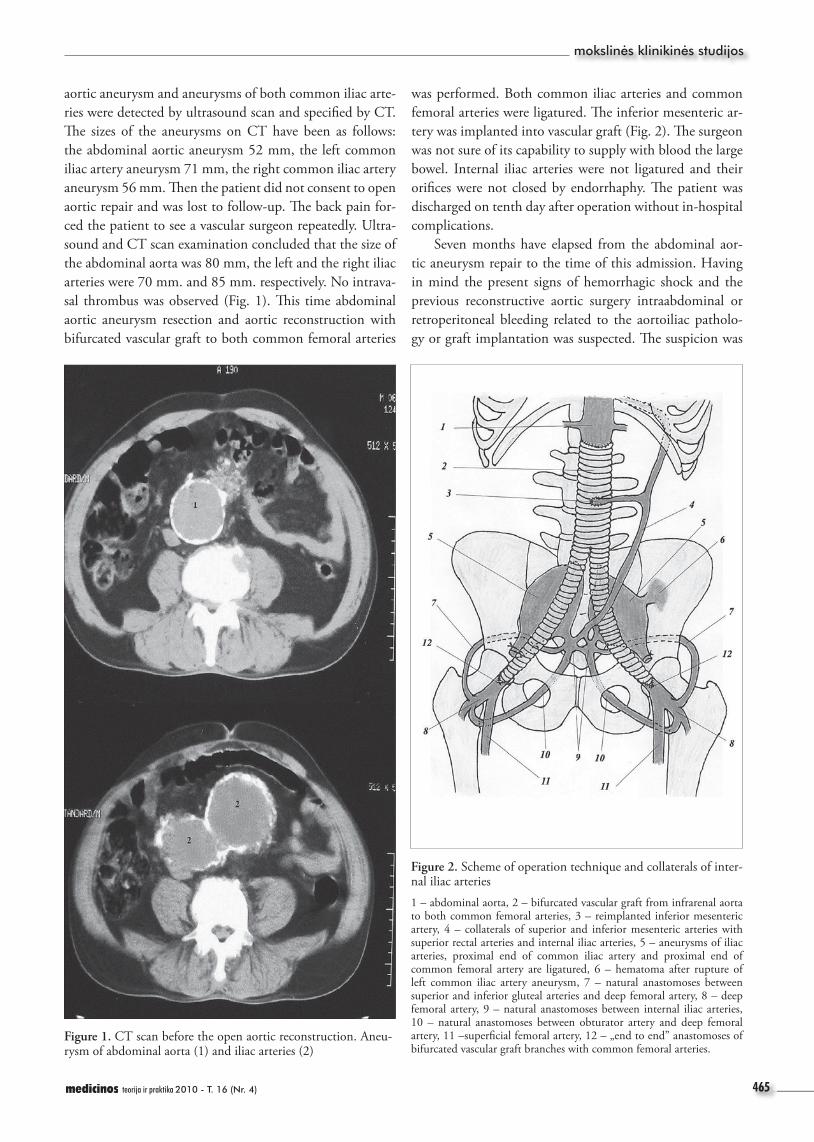
aortic aneurysm and aneurysms of both common iliac arte-ries were detected by ultrasound scan and speci� ed by CT. � e sizes of the aneurysms on CT have been as follows: the abdominal aortic aneurysm 52 mm, the left common iliac artery aneurysm 71 mm, the right common iliac artery aneurysm 56 mm. � en the patient did not consent to open aortic repair and was lost to follow-up. � e back pain for-ced the patient to see a vascular surgeon repeatedly. Ultra-sound and CT scan examination concluded that the size of the abdominal aorta was 80 mm, the left and the right iliac arteries were 70 mm. and 85 mm. respectively. No intrava-sal thrombus was observed (Fig. 1). � is time abdominal aortic aneurysm resection and aortic reconstruction with bifurcated vascular graft to both common femoral arteries
Figure 2. Scheme of operation technique and collaterals of inter-nal iliac arteries1 – abdominal aorta, 2 – bifurcated vascular graft from infrarenal aorta to both common femoral arteries, 3 – reimplanted inferior mesenteric artery, 4 – collaterals of superior and inferior mesenteric arteries with superior rectal arteries and internal iliac arteries, 5 – aneurysms of iliac arteries, proximal end of common iliac artery and proximal end of common femoral artery are ligatured, 6 – hematoma after rupture of left common iliac artery aneurysm, 7 – natural anastomoses between superior and inferior gluteal arteries and deep femoral artery, 8 – deep femoral artery, 9 – natural anastomoses between internal iliac arteries, 10 – natural anastomoses between obturator artery and deep femoral artery, 11 –super� cial femoral artery, 12 – „end to end” anastomoses of bifurcated vascular graft branches with common femoral arteries.
Figure 1. CT scan before the open aortic reconstruction. Aneu-rysm of abdominal aorta (1) and iliac arteries (2)
was performed. Both common iliac arteries and common femoral arteries were ligatured. � e inferior mesenteric ar-tery was implanted into vascular graft (Fig. 2). � e surgeon was not sure of its capability to supply with blood the large bowel. Internal iliac arteries were not ligatured and their ori� ces were not closed by endorrhaphy. � e patient was discharged on tenth day after operation without in-hospital complications.
Seven months have elapsed from the abdominal aor-tic aneurysm repair to the time of this admission. Having in mind the present signs of hemorrhagic shock and the previous reconstructive aortic surgery intraabdominal or retroperitoneal bleeding related to the aortoiliac patholo-gy or graft implantation was suspected. � e suspicion was
mokslinës klinikinës studijos
466 teorija ir praktika 2010 - T. 16 (Nr. 4)
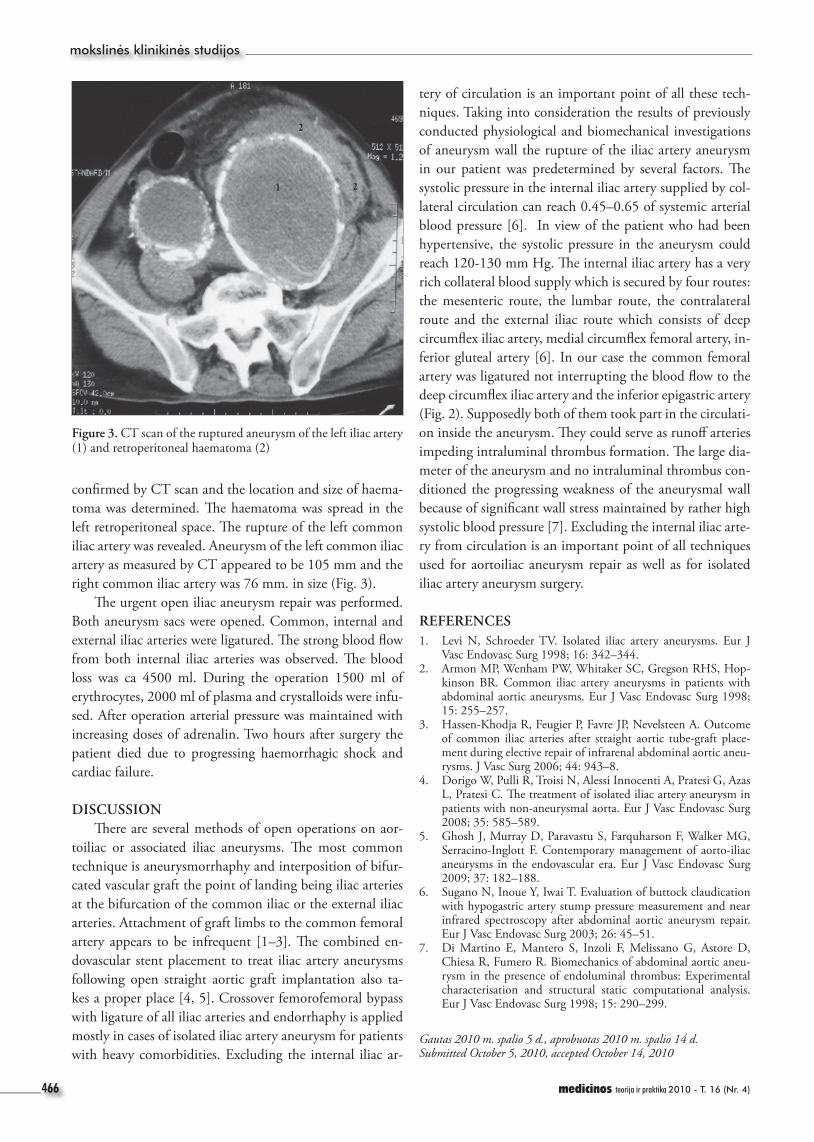
con� rmed by CT scan and the location and size of haema-toma was determined. � e haematoma was spread in the left retroperitoneal space. � e rupture of the left common iliac artery was revealed. Aneurysm of the left common iliac artery as measured by CT appeared to be 105 mm and the right common iliac artery was 76 mm. in size (Fig. 3).
� e urgent open iliac aneurysm repair was performed. Both aneurysm sacs were opened. Common, internal and external iliac arteries were ligatured. � e strong blood � ow from both internal iliac arteries was observed. � e blood loss was ca 4500 ml. During the operation 1500 ml of erythrocytes, 2000 ml of plasma and crystalloids were infu-sed. After operation arterial pressure was maintained with increasing doses of adrenalin. Two hours after surgery the patient died due to progressing haemorrhagic shock and cardiac failure.
DISCUSSION � ere are several methods of open operations on aor-
toiliac or associated iliac aneurysms. � e most common technique is aneurysmorrhaphy and interposition of bifur-cated vascular graft the point of landing being iliac arteries at the bifurcation of the common iliac or the external iliac arteries. Attachment of graft limbs to the common femoral artery appears to be infrequent [1–3]. � e combined en-dovascular stent placement to treat iliac artery aneurysms following open straight aortic graft implantation also ta-kes a proper place [4, 5]. Crossover femorofemoral bypass with ligature of all iliac arteries and endorrhaphy is applied mostly in cases of isolated iliac artery aneurysm for patients with heavy comorbidities. Excluding the internal iliac ar-
Figure 3. CT scan of the ruptured aneurysm of the left iliac artery (1) and retroperitoneal haematoma (2)
tery of circulation is an important point of all these tech-niques. Taking into consideration the results of previously conducted physiological and biomechanical investigations of aneurysm wall the rupture of the iliac artery aneurysm in our patient was predetermined by several factors. � e systolic pressure in the internal iliac artery supplied by col-lateral circulation can reach 0.45–0.65 of systemic arterial blood pressure [6]. In view of the patient who had been hypertensive, the systolic pressure in the aneurysm could reach 120-130 mm Hg. � e internal iliac artery has a very rich collateral blood supply which is secured by four routes: the mesenteric route, the lumbar route, the contralateral route and the external iliac route which consists of deep circum� ex iliac artery, medial circum� ex femoral artery, in-ferior gluteal artery [6]. In our case the common femoral artery was ligatured not interrupting the blood � ow to the deep circum� ex iliac artery and the inferior epigastric artery (Fig. 2). Supposedly both of them took part in the circulati-on inside the aneurysm. � ey could serve as runo� arteries impeding intraluminal thrombus formation. � e large dia-meter of the aneurysm and no intraluminal thrombus con-ditioned the progressing weakness of the aneurysmal wall because of signi� cant wall stress maintained by rather high systolic blood pressure [7]. Excluding the internal iliac arte-ry from circulation is an important point of all techniques used for aortoiliac aneurysm repair as well as for isolated iliac artery aneurysm surgery.
REFERENCES 1. Levi N, Schroeder TV. Isolated iliac artery aneurysms. Eur J
Vasc Endovasc Surg 1998; 16: 342–344.2. Armon MP, Wenham PW, Whitaker SC, Gregson RHS, Hop-
kinson BR. Common iliac artery aneurysms in patients with abdominal aortic aneurysms. Eur J Vasc Endovasc Surg 1998; 15: 255–257.
3. Hassen-Khodja R, Feugier P, Favre JP, Nevelsteen A. Outcome of common iliac arteries after straight aortic tube-graft place-ment during elective repair of infrarenal abdominal aortic aneu-rysms. J Vasc Surg 2006; 44: 943–8.
4. Dorigo W, Pulli R, Troisi N, Alessi Innocenti A, Pratesi G, Azas L, Pratesi C. � e treatment of isolated iliac artery aneurysm in patients with non-aneurysmal aorta. Eur J Vasc Endovasc Surg 2008; 35: 585–589.
5. Ghosh J, Murray D, Paravastu S, Farquharson F, Walker MG, Serracino-Inglott F. Contemporary management of aorto-iliac aneurysms in the endovascular era. Eur J Vasc Endovasc Surg 2009; 37: 182–188.
6. Sugano N, Inoue Y, Iwai T. Evaluation of buttock claudication with hypogastric artery stump pressure measurement and near infrared spectroscopy after abdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg 2003; 26: 45–51.
7. Di Martino E, Mantero S, Inzoli F, Melissano G, Astore D, Chiesa R, Fumero R. Biomechanics of abdominal aortic aneu-rysm in the presence of endoluminal thrombus: Experimental characterisation and structural static computational analysis. Eur J Vasc Endovasc Surg 1998; 15: 290–299.
Gautas 2010 m. spalio 5 d., aprobuotas 2010 m. spalio 14 d.Submitted October 5, 2010, accepted October 14, 2010




























