Embed Size (px)
DESCRIPTION
October 2012
Citation preview

October 2012 | Volume I /No. 8October 2012 | Volume I /No. 8
A Publication of the San Mateo County Medical Association
October Is
Breast Cancer
Awareness Month
October 2012 | Volume I / No. 8

56595 (10/12) ©Seabury & Smith, Inc. 2012
d/b/a in CA Seabury & Smith Insurance Program Management
Sponsored by:
Scan tolearn more!
Please call Marsh at 800-842-3761.
We serve members who want assistance in evaluating the medical insurance choices before them. We can assist you with the information you need to make the critical choices on the road ahead.
So what can you do?
You still need to make important decisions now about rising health insurance premiums.
The Supreme Court’s Decision Doesn’t Change One Thing
Enroll in a qualified High-Deductible Health Plan and open a Health Savings Account. This provides
significant premium savings that can help fund your HSA account. With individual-only
coverage, you are eligible to contribute up to $3,100 to your account or $6,250 with
family coverage, on a tax-deductible* basis (members age 55–64 are eligible to
contribute another $1,000).
Investigate RAF Sales Health plans offer incentives through discounts off their risk adjustment factors (RAFs) for you to change health plans. Instead of your
medical rates increasing this year, we might be able to help you offset some of that increase.
Mercer Select HRKnowHow If you play a role in your medical group’s health care and benefit plan decisions, stay current on challenging issues. Access is included at no charge for all members who purchase group health insurance through Marsh (Seabury & Smith Insurance Program Management).
Includes:
group benefit plan administration.

October is Breast Cancer Awareness Month. Governor Jerry Brown recently
signed Senate Bill 1538, authored by State Senator Joe Simitian (D-Palo Alto),
which will require mammography services to inform patients if dense breast
tissue is found during an exam. Opponents of the legislation argue that mandated
notifi cation could raise health care costs and unnecessarily concern women.
The American College of Radiology says that there is insuffi cient evidence to
recommend routine ultrasound screening for women with dense breast tissue,
while the American College of Obstetricians and Gynecologists says it is up to
radiologists to decide whether mammograms are suffi cient. We are reprinting
an informative article from Radiology Today that explores arguments in favor and
against this kind of legislation. California is the fi fth state to sign on, and the law
goes into effect April 1, 2013.
Also happening in October is National Psoriasis Day, on October 29th. Psoriasis
is an auto-immune disease that affects 125 million people worldwide, but its
causes are not fully understood. Researchers believe that for a person to develop
psoriasis, the individual must have a combination of the genes that cause
psoriasis and be exposed to specifi c external factors known as “triggers.” The
National Psoriasis Foundation is opening a Northern California Chapter, and we
are including an article from its Community Development with information about
the disease and how interested members can get involved in the new division.
How would you rate your communication skills? Regardless of your profession,
you’ve probably heard of the Social Styles matrix. Behavioral styles are infl uenced
by two dimensions; assertiveness, or the degree of forcefulness in behavior,
and responsiveness, or the degree to which behavior is emotionally expressive.
Because approximately 25% of people fall into each category, you likely share a
social style with only 25% of the people you meet. What are the consequences if
you can’t adapt to the other 75%? We are including an article by Wilson Learning,
which gave a presentation at Kaiser this past summer. By understanding your
own style and by the styles of others you work with, you can achieve what the
authors call Versatility, and develop more effective working relationships.
President’s Message ................. 5
Reminding Ourselves of the Benefi ts of MICRA
Gregory Lukaszewicz, MD
Executive Report ....................... 7
The Value of Working with Your Colleagues to Effect Outcomes—SMCMA Committees
Sue U. Malone
Breast Density Notifi cation ..... 9
Kathy Hardy
Versatility: Avoiding the Hidden Costs of Interpersonal Communication Stress .......... 13
Michael Leimbach, PhD and Gene Daley, MBA
World Psoriasis Day—October 29, 2012 ..................... 15
Sonia Kalil
Hep B Free San Mateo ............ 17
Whitney Wood
Membership Update andClassifi ed Ads .......................... 18
Editor’s Introduction
BY RUSS GRANICH, MD
A Publication of the San Mateo County Medical Association
October 2012Volume I / No. 8
On the cover
Pink Ribbon Spring Flower by ForestWander Nature Photography. Copyright © 2004-2012 ForestWander.com. Reprinted with permission.
Editor’s Introduction
BY RUSS GRANICH, MD

DISABILITYL
IFE
IN
SU
RA
NC
E
LONG-TERM CARE
Protecting the rights of all policy- holders to be treated fairly and in good faith.Unfortunately, the same insurer
that readily accepts your premium
dollars may not be so eager to
pay benefits. Pillsbury & Levinson
lawyers pursue insurance bad
faith litigation on behalf of doctors
and their patients in coverage
disputes. We seek compensation
for our clients’ financial losses,
as well as punitive damages and
attorney’s fees. We have collected
hundreds of millions of dollars
in policy benefits for clients
throughout California in all types
of insurance matters.
415.433.8000 | 888.433.8335 pil lsburylevinson.com

SAN MATEO COUNTY PHYSICIAN | PAGE 5
Reminding Ourselves of the Benefi ts of MICRA
PRESIDENT’S MESSAGE
BY GREGORY LUKASZEWICZ, MD
While in college at Dartmouth, I spent a semester studying international relations and European Monetary Policy at the London School of Economics (given all the events in Europe over the past several years, I should have paid more attention, but monetary policy is tough enough). Because the leading civilian United States representative to NATO was a Dartmouth grad, our program was invited to Brussels to see the headquarters of NATO and the European Economic Community. During a dinner party with various civilian and military members of NATO, a U.S. colonel informed us college students that the American public must be re-educated as to the cost of freedom every twenty years. Though at the time it seemed a bit over-the-top to a 21- year-old college student, I can now certainly understand how these sentiments could come from a man who, as he put it, was signing up for Vietnam while his classmates were all protesting.
I was reminded of this anecdote just recently while discussing the recent bill in the State Legislature designed to undermine the Medical
Injury Compensation Reform Act of 1975 (MICRA). As a physician who has only practiced under MICRA’s protections, I know it is important to remember, and fight to uphold, the benefits that this legislation has provided not only to California physicians but our health care delivery system in general.
MICRA was introduced in response to the crisis facing physicians and our health care system due to the escalating cost of medical malpractice lawsuits. At the time, these exorbitant costs were threatening to drive many providers, particularly in very-high risk specialties, out of business and out of the state. Beyond the threat to physicians, these costs threatened the entire health care system by potentially limiting the number of adequate providers and thus patient access. MICRA was passed in 1975 with bi-partisan support in the state legislature and signed into law by then Governor Jerry Brown.
MICRA included the following provisions:
• limits on awards for pain and suffering or non-economic damages to $250,000
• limits to attorney fees
• protections for patients for the recovery of economic damage such as loss of future income or future medical expenses
• the opportunity to settle disputes through binding arbitration
• allowances for a payment schedule over a period of time rather than in one lump sum
• need for notification of a pending claim
• statute of limitations on claims
Over the years MICRA has stood up to challenges in both the State Supreme Court and the California Court of Appeals, as well as in the state legislature. Most recently, during the last legislative session, President pro Tem of the State Senate Darrell Steinberg (D-Sacramento) authored Senate Bill 1528, which would allow plaintiffs covered by Medi-Cal to recover more for medical expenses from a lawsuit than was originally paid in the first place. Since Medi-

6 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012
Cal paid these original costs for the medical services provided, the state could then seek to recover these expenses and thus recover more money than it actually paid in the first place. The purpose of SB 1528 was to help cover the cost of the Medi-Cal program. Fortunately, this bill did not pass in the State Assembly (43 noes to 13 yeses).
For those of us who may take MICRA for granted, it is good to re-educate ourselves about the benefits it has provided to physicians, patients, and the health care system as a whole. Though some may argue that patients who have been injured through malpractice or negligence are the ones left bearing the true costs of MICRA, the only financial limits placed upon a lawsuit are in fact related to non-economic damages (pain and suffering, which by no means am I trying to downplay or dismiss).
In addition, the health care system is already facing a crisis in terms of ever-escalating costs. Without MICRA we could only expect those costs to rise at an even greater rate, putting an even greater burden on a health care system facing a financial crisis. If the health care system were to fail because of these uncontrolled costs, all of society would suffer.
We can expect further challenges to MICRA in the future. How do we meet these challenges? By staying organized as physicians, communicating with our representatives to the state legislature, and making our voice heard through our professional organizations (in particular the California Medical Association, which has the staff and lobbyists with the knowledge and ability to influence policy at the state level). Unless we act, we risk facing the same crisis in medical malpractice that is being seen in other states and that once threatened our own health care system./
President’s Message: RemindingOurselves of the Benefi ts of MICRAcontinued
SMCMA2013 Membership Directory& Desk Reference
Production for the 2013 edition of the SMCMA Membership Directory is already underway. Please send any updates to your member profile (including new photos) to Gina Cromosini at (650) 312-1663, fax (650) 312-1664, or [email protected].

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 7
EXECUTIVE REPORT
The Value of Working with Your Colleagues to Effect Outcomes—SMCMA Committees
BY SUE U. MALONE
A few weeks ago members received a sign-up form to volunteer to work on one of SMCMA’s committees. I urge you to look over the opportunities and get involved.
Among the standing committees are three peer review committees, all of which serve doctors and their patients. Two committees focus on patient complaints; one reviews patient complaints about physician fees and mediates differences of opinion. The second committee focuses on complaints (Professional Relations) regarding standards of medical care and medical ethics. When such complaints are made, a physician case manager is asked to review the complaint(s) and present fi ndings to the whole committee. The committee drafts a letter of response, which the physician-respondent has an opportunity to review for accuracy (not for editing), is drafted and before it is released back to the complainant. We fi nd that most often a complaint is generated due to a lack of understanding about the care provided or communication problems between the physician had with the patient. Once the patient understands, often we can diffuse his or her negative feelings toward the physician.
Another of our committees, Medical Review & Advisory committee, meets in the evening, on call, to hear case presentations by a specialist in the same medical specialty when a medical malpractice suit has been fi led by a
patient against one of our doctors. The attorneys defending the physician are present to learn from our physicians about standard of care in our community. Often the issues are complex and provide for some very stimulating discussion. There is no question that physicians learn from the discussions that take place in these peer review activities/
By the way, physicians receive CME credit for participating on our peer review committees. I also want to mention that we make every effort to maintain confi dentiality of the cases presented. The name of any physician whose care is being questioned is not named, nor is any facility that also may be named in a complaint.
As an aside, at the most recent Medical Review & Advisory Committee meeting, the physicians received a report back on the fi nal outcome of the cases reviewed in the last two years. Even in situations where the majority of our committee felt the standard was not met, the typical case resulted in a settlement, dismissal by the court, or a verdict in favor of the defense.
Our Bioethics Committee is another enthusiastic group that discusses bioethical issues and develops guidelines on health care policy. Two recent examples of their work is a survey on gift giving by pharmaceutical companies. Another example is the development of a model policy on
Health Care Decisions for Patients Without Surrogates. Although California law provides legal guidance for the medical management of patients who lack medical decision-making ability, it contains no provisions concerning medical decisions for patients who also lack a surrogate decision-maker.
If you enjoy meeting with local legislators who impact policy at the local, state, and national levels, join the Legislative Committee. The committee meets with all local and state candidates running for offi ce for the county Board of Supervisors and the state Assembly and Senate, as well as periodically throughout the year. It is quite common to our committee to fi rst meet candidates running for local offi ce who end up in the State Legislature and even Congress.
SMCMA is also seeking your help in studying public health and environmental issues, promoting our Hepatitis B campaign, and developing ideas for content in our very own San Mateo County Physician.
The more that our members participate on committees, the more that each member takes away from the experience and the more impact that our committees can have. I urge you to consider volunteering. If you can’t fi nd the committee sign-up form, don’t worry—it is on our website at www.smcma.org/about/committees-and-commissions. /

8 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012
Trust and Estate Planning:
Representing healthcare
providers and their families for
over 40 years.
Hinshaw, Marsh, Still & Hinshaw
www.hinshawestateplanning.com | www.hinshaw-law.com
Healthcare Labor Law

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 9
BY KATHY HARDY
Breast Density Notifi cation
Editor’s Note: In September 2012, Governor Jerry Brown signed legislation designed to help improve breast cancer detection and prevention. Senate Bill 1538, authored by State Senator Joe Simitian (D-Palo Alto), will require mammography services to inform patients if dense breast tissue is found during an exam. California is the fi fth state to enact such legislation. The law will go into effect on April 1, 2012.
To highlight some of the issues affecting physicians, we are reprinting this article from the August 2012 issue of Radiology Today.
Is breast density notifi cation too much information for women?
The pervasive thought among breast imagers is that it may not be the amount of information but what follows that could further complicate women’s breast cancer screening decisions. Most breast imagers believe knowledge about breast density will prove benefi cial, but it may complicate women’s screening decisions, lead to confusion about screening follow-up, increase the potential for false-positives, and create additional healthcare costs.
In four states—Connecticut, New York, Texas, and Virginia—the plain-language report that women receive following their regular screening mammograms must now include information regarding whether they have dense breast tissue. With legislation pending in at least 11 more states and a bill introduced in the US House of Representatives, women across the country may be learning more about their breasts—regardless of whether they want to or know what to do with that information.
“Providing information like this enables women and their physicians to be proactive about their own healthcare,” says Jean Weigert, MD, FACR, director of women’s imaging with the Hospital of Central Connecticut. “But you need data to determine if providing this information is helpful.”
It is common knowledge within the breast imaging community that dense breast tissue is one factor
determining whether a woman is at high risk of having undetected breast cancer. Dense breast tissue contains less fat and more connective tissue, which appears white on a mammogram. Cancer also appears white on a mammogram, and thus tumors are often hidden behind the dense tissue. However, dense tissue is not the only factor when labeling a woman at high risk of breast cancer.
“Breast density is just one of the things women need to know,” says Barbara Monsees, MD, FACR, chief of breast imaging at Washington University School of Medicine in St Louis and chair of the ACR’s Breast Imaging Commission. “They need to talk to their physicians about the other risk factors, such as family history. They need to put dense breast tissue into context with the other risk factors before coming to any conclusions.”
In its position statement, the ACR supports an FDA mandate that dense breast tissue notifi cation be included in the mammography report. The organization also supports patient education and encourages patients to “take charge of their own care” but remains cautious when it comes to how this information will be interpreted.
Similarly, in a letter to the FDA’s National Mammography Quality Assurance Advisory Committee on recording breast density in mammography reports and patient lay summaries, the Society of Breast Imaging supports the dialogue between patient and physician regarding breast density. However, the society remains cautious regarding whether the specifi cs of breast density are benefi cial or will lead to confusion or other unintended consequences for women.
The ACR believes consistency is a key part of integrating dense breast notifi cation into the mammography process, beginning with the language used in the report summary.
“ACR wrote a sample lay letter to help radiologists deal with the notifi cation process,” Monsees says. “The letter states that if a patient has dense breast tissue, she is to consult with her physician regarding a next course of action. It does not mention supplemental screening.”
What constitutes dense breast tissue is another consideration within the issue. The ACR’s Breast Imaging
Reprinted with the permission of Radiology Today © 2012. Great Valley Publishing, Co.

10 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012
Breast Density Notifi cationcontinued
Reporting and Data System classifi cation, designed to standardize mammography reporting and reduce the confusion in breast imaging interpretation, describes four categories of breast tissue density and instructs radiologists to include this density information in the medical report. In its statement on dense breast notifi cation, the ACR says it would support an FDA mandate that this same information be included in the mammography report. Weigert adds that a density-measuring algorithm does exist, but the software can be cost-prohibitive to some facilities.
“Determining tissue density is very subjective,” Monsees says. “The interpretation can differ from doctor to doctor or practice to practice. It worries us that the interpretation of dense breast tissue is too variable. We don’t want to confuse people or undermine their confi dence in mammography as a screening tool.”
Consistency is a pillar of breast imagers’ attempts to maintain a high level of confi dence in mammography, which remains the gold standard when it comes to detecting breast cancer. Studies have reported varying statistics regarding what age to begin screening mammography and how often to perform it. The US Preventive Services Task Force recommendations issued in 2009 reignited and complicated the debate about when and how to screen; some worry that dense breast notifi cation may further complicate the discussion. There is some concern that for women with fatty breasts, such information could convey a false sense of security.
Multiple Factors
“What if a woman is told she does not have dense breast tissue but she has a strong family history of breast cancer?” Monsees says. “We wouldn’t want her to think that she’s not at high risk for breast cancer.”
One unintended consequence of dense breast notifi cation is the potential for increased ultrasound orders and the accompanying risk of more false-positives and benign breast biopsies. Mammography plus ultrasound performed by trained expert radiologists detected more cancers than mammography alone in the ACRIN 6666 study, Monsees says. However, the study, which involved women who were already at high risk of breast cancer, also revealed that the combined screening strategy of mammography and ultrasound resulted in far more recalls, biopsies, and recommendations for short interval follow-up than mammography alone.
“The downside is that you have the potential for more false-positives when you have mammography followed by
ultrasound,” she says. “In the ACRIN study, the women were already at a high risk. What happens when we apply this screening process to the general population and the ultrasounds are performed by technologists, not specially trained experts? We need data from the general population before deciding whether or not this is benefi cial.”
The breast imaging community continually grapples with quantity vs. quality when it comes to breast imaging. Carol H. Lee, MD, FACR, attending radiologist at Memorial Sloan-Kettering Cancer Center in New York and chair of the ACR’s Breast Imaging Commission Communications Committee, notes that just as breast density is a big issue, so too is the topic of overdiagnosis. “On the one hand we’re saying there are too many false-positives and too much screening,” Lee says. “On the other hand, there is the breast density notifi cation issue that will likely lead to more screening. As breast imagers, we’re caught between two imperatives: screen less vs. screen more.”
Weigert notes that as women in Connecticut started to receive notifi cation that they had dense breast tissue, they weren’t necessarily convinced that ultrasound was their next logical step. “Even if they knew about their dense breasts, they were afraid of the false-positives associated with ultrasound,” she says. “It’s a matter of building confi dence over time. Breast imagers are more likely to order ultrasound, but general practice radiologists are more likely to call for biopsies. No one gets upset when they have a negative biopsy.”
As states begin to implement this legislation, education plays an important role in the fi rst stages. Weigert says in the fi rst several months after Connecticut enacted its law in 2009, she found that many referring physicians were not aware that the legislation had gone into effect. Letters sent to physicians explaining the law includes suggestions for how to prepare staff and patients to handle this new aspect of breast screening.
Automated Ultrasound
The next steps for radiology practices could come in the form of new technology, particularly in the ultrasound realm. With the standard handheld ultrasound performed in most cases, Weigert says the process is full of variables. Technicians may use slightly different techniques as they scan patients. The process is labor intensive, with the technician looking closely at the monitor to make sure they capture everything necessary to provide the radiologist with a proper view of the patient.

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 11
“There is a level of anxiety for the technicians,” she says. “They need to fi nd everything and then bring the images to me. The patient is anxious as well.”
Weigert believes that implementing automated whole-breast ultrasound would make the process a “true screen,” with the technician taking all the images and then providing an entire data set for the radiologist to read. However, while FDA-approved automated ultrasound technology exists, the equipment is expensive and not often covered by insurance.
Weigert suggests that establishing a code for screening breast ultrasound could help pave the way for more insurers to cover this modality as a follow-up to screening mammography. Right now, ultrasound is considered a diagnostic code.
“The paradox here is that screening modalities are perceived as being low cost,” she says. “Actually, screening is more costly, time consuming, and labor intensive than diagnostic.”
One ancillary benefi t of breast density notifi cation is that this recorded information is then available for use in studies and clinical trials. In Weigert’s case, she now has a pool of women from which she can gather data for study purposes. In 2011, she presented a clinical study of more than 1,000 patients that looked at how breast-specifi c gamma imaging (BSGI) plays a role in early breast cancer detection by adding specifi city as well as sensitivity to breast cancer detection. Comparing BSGI with mammography and ultrasound, the study concluded that BSGI has greater sensitivity and comparable specifi city compared with ultrasound and mammography. Three of the cases used in this study were discovered through dense breast notifi cation.
While the issue isn’t specifi cally on the merits of ultrasound, the data surrounding the use of this modality as a follow-up to mammography does play a role in the dense breast notifi cation debate, particularly when insurance companies are deciding whether to cover screening ultrasound or MRI. A concern among breast imagers is that unless supplemental screening is reimbursed by insurers, there may be a disparity in follow-up between women who can afford to pay for the additional screening exam and those who cannot.
Waiting for Data
As dense breast notifi cation legislation begins to spread across the country, more breast imagers are assessing the pros and cons of providing women with this level of
information. Weigert admits that she was not a believer at fi rst, noting her concern for an increase in false-positives. Her acceptance is increasing, but she is still looking for more good evidence that this is the right decision for women.
“Making dense breast notifi cation mandatory without scientifi c research to back it up is not a smart thing to do,” she says. “It’s a very emotional decision. But as we build a body of data, it’s more likely to be a good thing.” /
Kathy Hardy is a freelance writer based in Phoenixville, Pennsylvania. She is a frequent contributor to Radiology Today.
ABOUT THE AUTHOR

12 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 13
How has your medical center or practice responded to the economic climate of the past several years? How are you preparing for the years ahead? If yours is like most, you’ve probably experienced a variety of cost-cutting measures and other productivity enhancement initiatives. While these kinds of changes are necessary, they can impact overall performance in unexpected ways, specifically the day-to-day stress from an uncertain and changing work environment. This stress shows up in relationship tension with colleagues and, unless addressed, will breed conflicts, misunderstandings, and overall failures to communicate that weaken performance just when your organization needs the high performance. Yet, there is a powerful tool available that can reduce these barriers to productivity—and therefore impact clinical care, efficiency, patient satisfaction and profitability—it’s called Versatility.
Versatility—The Answer to Performance Sapping Relationship Tension and Stress
Versatility is defined as the ability to understand differences in communication preferences and to adapt to make others more open and receptive—creating more effective and productive relationships. Versatility is a skill that can be learned, and people who have it find it far easier to work together with others toward shared organizational goals.
To understand Versatility and how it can affect relationships, consider people with whom you have regular contact. Do you know a pediatrician who is “too reserved” for your taste? Is there a medical assistant who seems to you to be “too opinionated,” “too emotional,” “too willing (or unwilling) to compromise”? Chances are your reactions to these people are an indicator of differences in Social Style—how we habitually communicate and interact with others. When you find it easy to communicate and work with someone, there’s a high probability you share the same social style.
When your communication is difficult, it is often because of unrecognized social style differences. For example, when visiting an Analytical pediatrician, a nurse or another physician may adopt a similar behavioral posture, which can increase comfort and trust in his or her counterpart.
BY MICHAEL LEIMBACH, PHD, AND GENE DALEY, MBA
Versatility: Avoiding the Hidden Costs of Interpersonal Communication Stress
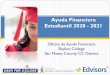
TASK
Directed
PEOPLE
Directed
ASK
Directed
TELL
Directed
Analytical Driver
Amiable Expressive
THE SOCIAL STYLES MODEL
© Wilson Learning Worldwide
Social Styles and the 75% Problem
Wilson Learning’s social style model defines four primary communication styles—Driver, Expressive, Amiable, and Analytical.
As the model shows, the four styles vary in terms of behaviors reflecting the dimensions of Assertiveness (Tell versus Ask) directedness and Responsiveness (People versus Task) orientation. Drivers and Expressives tend to be more Tell oriented, while Amiables and Analyticals are more Ask oriented. Analyticals and Drivers are more Task-first oriented, while Amiables and Expressives are more People-first oriented. Because about 25 percent of people fall into each of these four categories, you likely share a social style with only about 25 percent of the people you meet. What are the consequences when we can’t adapt to the other 75 percent?

14 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012
Versatility: Avoiding the Hidden Costs of Interpersonal Communication Stresscontinued
Consider the communication challenges faced by a non-versatile physician who has a different social style than three-fourths of her staff members. In this case an Amiable medical assistant will not be comfortable with a Driver physician who seems too focused on tasks and less concerned with personal relationships. An Analytical nurse won’t like to be told things she already knows—but at the same time she doesn’t want gaps in information that the physician could have provided. These kinds of misalignments create the potential for friction, misunderstanding, and lowered productivity.
Increasing Versatility
For most of us, interpersonal behaviors and preferences are habitual and largely outside of our awareness. Versatility comes with the recognition that people do have different styles and that each style has unique strengths. Once people know their own style and understand style differences, they can learn how to modify behaviors to make it easier to work together and make decisions in a way that is more effective for the whole team.
Suppose, for example, a physician leader or office manager has several Amiable employees. The physician leader can make an effort to show a personal interest in them and offer more guidance, support and recognition than they might provide to experienced Driver employees, who want the freedom to solve problems themselves.
When those same Amiable employees interact with an RN who has a reserved, serious attitude, their ability to identify the RN’s Social Style (Analytical) allows them to adapt their style in terms of speech (more logical and formal), as well as body posture and facial expressions (erect, attentive posture with fewer gestures and expressions) for more comfortable, successful interactions.
Another example can be seen in the pharmaceutical rep calling on an Expressive pharmacist who has a negative perception of a drug. Using versatility skills to engage the pharmacist and get her to talk about her feelings could help overcome the animosity and lead to a successful sale.
When making decisions, managers can adapt to different expectations and needs based on their recognition of employees’ styles. For example, expressives want managers to involve them in a decision making when it affects the whole group, and Amiables like to have the group involved in brainstorming and problem solving. On the other hand, Analyticals are not as interested in group
decision making and typically prefer to be involved only when decisions or actions affect them directly.
Versatility: Key to Improved Business Results
Healthcare organizations can experience dramatic, measurable improvements in performance when their staff learn how to adapt to others’ social styles, including the social styles of patients. In one study, building versatility skills yielded a 52 percent improvement in ability to identify styles and recognize tension when the individual is stressed. In the same organization, 46 percent of employees reported a moderate to large improvement in work productivity. As one clinic manager reported, “I’ve been more sensitive to my Driver style and the style of others during [coaching] sessions and as a result, I believe the sessions have been more productive and conversation/feedback has been freer flowing.”
While there are multiple ways to improve communication in a given situation, the single most important factor for enhancing communication effectiveness across the board is Versatility. As more leaders are required to take on greater responsibilities for improved efficiencies in today’s healthcare environment, building this kind of capability provides a real competitive advantage for the individual and the organization as a whole. /
Michael Leimbach, Ph.D., is Vice President of Global Research and Design for Wilson Learning Worldwide. With more than 25 years in the fi eld, Michael provides leadership for researching and designing Wilson Learning’s diagnostic, learning, and performance improvement capabilities.
Gene Daley, M.B.A., is an Independent Consultant for Wilson Learning Worldwide. With more than 20 years in the fi eld, Gene has facilitated leadership development programs for thousands of healthcare professionals—helping to balance one’s clinical responsibilities with a marked improvement in leadership and
performance management skills.
To learn more about the concepts shared within this article and how Wilson Learning can assist you in addressing these issues, contact Wilson Learning at 1-800-328.-937 or visit wilsonlearning-americas.com.
ABOUT THE AUTHORS

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 15
World Psoriasis Day is a global event that sets out to raise awareness and give voice to the 125 million people worldwide living with psoriasis and psoriatic arthritis.
Psoriasis is the most common autoimmune disease in the country, affecting as many as 7.5 million Americans, or about two percent of the population. Up to 30 percent of people with psoriasis will develop psoriatic arthritis, which causes swelling of the joints. Psoriasis can occur on any part of the body and is associated with other serious health conditions, such as diabetes, heart disease, obesity, hypertension and depression.
In an effort to raise awareness for psoriasis on the local stage, the National Psoriasis Foundation (NPF) has just opened its first office in San Francisco to support the estimated 400,000 Northern California residents who live with psoriasis and psoriatic arthritis as well as the family members who support them and the medical professionals who treat them. This October, the NPF will be developing a Northern California Division, which will focus on providing disease education and assistance to community members, galvanizing volunteers to engage in state and federal advocacy, and spearhead local fundraising activities to support critical psoriasis research.
Those interested in taking a leadership role in the development of the Northern California Division of the National Psoriasis Foundation are welcome to attend the First Organizational Meeting on Thursday, November 15th, 2012 from 6:30-8:00 p.m. at the Silicon Valley Community Foundation Conference Center, 1300 S. El Camino Real, San Mateo.
What is psoriasis? Psoriasis is a chronic, non-contagious genetic disease that occurs when faulty signals in the immune system prompt skin cells to regenerate too quickly. There are five types of psoriasis: plaque, guttate, inverse, pustular and erythrodermic. The most common form is plaque psoriasis, which appears on as patches of raised, red skin covered by flaky white buildup of dead skin cells. These plaques are often itchy and painful, and they can crack and bleed.
Who gets psoriasis? Psoriasis affects men and women equally. It can strike at any age, but it is most commonly diagnosed between the ages of 15 and 35.
Approximately 10 to 15 percent of people with psoriasis get it before age ten. It rarely appears in infants. Psoriasis occurs in all ethnicities, but is most prevalent in Caucasians.
What causes psoriasis? The cause of psoriasis is unknown, but it is understood that the immune system and genetics play major roles in its development. Most researchers agree that the immune system is somehow mistakenly triggered, which causes a series of events, including acceleration of skin cell growth. A normal skin cell matures and falls off the body in 28 to 30 days. A skin cell in a patient with psoriasis takes only 3 to 4 days to mature and instead of falling off (shedding), the cells pile up on the surface of the skin, forming psoriasis lesions. Triggers can include emotional stress, injury to the skin, smoking, some types of infection or a reaction to treatment with certain drugs.
How is psoriasis diagnosed? No special blood tests or diagnostic tools exist to diagnose psoriasis. Physicians usually examine the affected skin to make a diagnosis. Less often, they may examine a piece of skin (biopsy) under a microscope.
How is psoriasis treated? Treatment is individualized for each person and depends on the severity of the disease, the type of psoriasis and how the patient reacts to certain treatments. What works for one person will not necessarily work for another person.
Topical treatments: Topical treatments—medications applied to the skin—are usually the first line of defense in treating psoriasis. Topicals slow down or normalize excessive cell reproduction and reduce the inflammation associated with psoriasis.
There are many effective topical treatments for psoriasis. While many can be purchased over the counter (OTC), others are available by prescription only.
Phototherapy: Phototherapy or light therapy, involves exposing the skin to ultraviolet light on a regular basis and under medical supervision. Treatments are done in a doctor’s office or psoriasis clinic or at home with a phototherapy unit. The key to success with light therapy is consistency.
BY SONIA KALIL
World Psoriasis Day – October 29, 2012

16 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012
Systemic Treatment: Systemic medications are prescription drugs that work throughout the body. They are usually used for individuals with moderate to severe psoriasis and psoriatic arthritis. Systemic medications are also used in those who are not responsive or are unable to take topical treatments or use phototherapy. Systemic psoriasis drugs are taken by mouth in liquid or pill form or given by injection.
Biologics: Biologics, protein-based drugs derived from living cells cultured in a laboratory, are relatively new treatments. Biologics are given by injection or IV. Different from the traditional systemic drugs that impact the entire immune system, biologics target specific parts of the immune system.
“It is important that psoriasis patients know there are many different treatment options out there, including phototherapy and internal medications,” states Dr. John Koo of the UCSF Psoriasis Center. “By getting involved with the National Psoriasis Foundation’s local division, patients can learn about these treatment options, meet others living with psoriasis, and be a part of community effort to increase awareness for psoriatic disease. Patients who are involved with groups like this often benefit by learning more about their condition and getting better at managing their symptoms.”
This information is from the National Psoriasis Foundation (NPF), the world’s largest nonprofit organization serving people with psoriasis and psoriatic arthritis. The mission of the NPF is to find a cure for psoriasis and psoriatic arthritis and to eliminate their devastating effects through research, advocacy and education. For more information, visit www.psoriasis.org. /
Sonia Kalil is Community Development Manager for the Northern California Division of the National Psoriasis Foundation.
To learn more about the National Psoriasis Foundation, visit www.psoriasis.org. For more information about the local division of NPF, visit www.psoriasis.org/in-your-area/northern-california.
World Psoriasis Daycontinued
Tracy Zweig AssociatesA R E G I S T R Y & P L A C E M E N T F I R M
INC.
www.tracyzweig.com
Voice: 800-919-9141 or 805-641-9141
FAX : 805-641-9143
Locum Tenens
Permanent Placement
Physicians Nurse Practitioners
Physician Assistants
Websitesmcma.org
Facebookfacebook.com/smcma
Twittertwitter.com/SMCMedAssoc
LinkedInlinkedin.com/company/san-mateo-county-medical-association
Connect with SMCMA
ABOUT THE AUTHOR

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 17
UPCOMING CLINICS
October 14, 2012 San Agustin Church 3700 Callan Boulevard, SSF
October 21, 2012United Methodist Church 1474 Southgate Avenue, Daly City
October 28, 2012 Cross Road Christian Center 444 E. Market Street, Daly City
November 4, 2012 American Filipino Church of Christ 461 Linden Avenue, San Bruno
November 18, 2012 St. Francis of Assisi 1425 Bay Road, East Palo Alto
SAN MATEO MEDICAL CENTER RECURRING MOBILE CLINICS
Monday – 11:00 A.M. - 5:00 P.M. S. San Francisco, Linden & Pine
Tuesday – 10:00 A.M. - 2:00 P.M.Redwood City, Fair Oaks Community Center
Wednesday – 10:00 A.M. - 2:00 P.M.Redwood City, 5th & Spring Street
Thursday 9:30 A.M. – 1:30 P.M.San Mateo, 5th & Railroad
Friday, 10:00 A.M. - 2:00 P.M.San Bruno, San Bruno & Green
WHAT IS HEP B FREE SAN MATEO?
San Mateo Hep B Free is a community-based program with the goal of eradicating hepatitis B throughout San Mateo County by increasing awareness of the disease, promoting testing for and immunization against hepatitis B, and providing physicians to care for patients with chronic hepatitis B.
This health issue is of special importance to Asian and Pacific Islander community groups because liver cancer from hepatitis B represents the leading cause of cancer death in certain Asian populations. Without proper care, one in four Asian and Pacific Islanders living with chronic hepatitis B will die from liver cancer or liver failure.
The original Hep B Free campaign was launched in San Francisco in 2007 and has now been replicated around the country as a model in hepatitis B prevention.
HOW CAN I HELP?
Hep B Free relies heavily on the many volunteers that contribute their time and energy to forward our objectives. SMCMA strongly encourages its members to pledge to vaccinate all their patients who are at high-risk for contracting Hepatitis B. Additionally, volunteers are always needed at Hep B Free’s regular vaccination clinics. For more information, please contact Whitney Wood at (650) 312-1663 or [email protected].
COMMUNITY PARTNERS
San Mateo County Medical Association
San Mateo County Health System
Asian Liver Center at Stanford University
AsianWeek Foundation
Gilead Sciences, Inc.
Self Help for the Elderly
Hospital Consortium of San Mateo
Hospital Council of Northern and Central California
Chinese Hospital – Daly City Clinic
Mills-Peninsula Health Services
NORCAL Mutual Insurance Company
San Mateo Medical Center
Sequoia Hospital
Seton Medical Center
Subaru
SUPPORTING OFFICIALS
Senator Leland Yee
Assemblymember Jerry Hill
Congresswoman Jackie Speier
Assemblymember Richard Gordon
Assembly Speaker Pro Tempore Fiona Ma
SMC Board of Supervisors Dave Pine
SMC Board of Supervisors Carole Groom
SMC Board of Supervisors Rose Jacobs Gibson
SMC Board of Supervisors Adrienne J. Tissier
Councilmember Wayne Lee
San Mateo Councilman David Lim
Mayor of Palo Alto Laura Martinez
Assessor Recorder of San Francisco Phil Ting

18 SAN MATEO COUNTY PHYSICIAN | OCTOBER 2012
Gregory C. Lukaszewicz, M.D. ...................................PresidentAmita Saxena, M.D. ...........................................President-ElectVincent Mason, M.D ...................................Secretary-TreasurerJohn D. Hoff, M.D ............................ .Immediate Past President
Beata Chauhan/ *GER, *IMRedwood City
Helen Hong/ *CD, *IMS. San Francisco
Sherwin Hua/ *NSRedwood City
Rex Huang/ *PSYRedwood City
Fawzi Khyat/ *GSS. San Francisco
Shu May Lee/ IMDaly City
Susan Longar/ *OPHDaly City
Peter Lunny/ EMS. San Francisco
Ming Teng/ *ROS. San Francisco
Samir Thadani/ *CD, *IMS. San Francisco
Editorial Committee
The July/August 2012 issue included an article by SMCMA member Jerry Saliman, MD, that was inadvertently printed with the incorrect title. The correct title is “For Better or For Worse.” San Mateo County Physician regrets the error.
Classifi ed Ads
Medical Offi ce Space Available for SubletFour exam rooms with running water and one MD offi ce available for up to four days weekly. May be able to provide offi ce staff if needed. Excellent location, opposite Peninsula Hospital. For details please contact Bonnie McGuire: [email protected] or 650-259-1480.
Place a classifi ed ad for $40 for up to fi ve lines for members and $75 for up to fi ve lines for non-members. Contact SMCMA at (650) 312-1663 or [email protected]
PhysicianSan Mateo
County
Sue U. Malone ......................................... Executive Director Shannon Goecke ......................................... Managing Editor
Article Submission
Members are always encouraged to submit articles, commentary and Letters to the Editor. Email your submission to the SMCMA Editorial Committee at [email protected] for consideration for publication in San Mateo County Physician.
Editorial and Advertising Offi ces
777 Mariners Island Boulevard, Suite 100San Mateo, CA 94404Tel (650) 312-1663Fax (650) [email protected]
Acceptance and publication of advertising in San Mateo County Physician does not constitute approval or endorsement by the San Mateo County Medical Association of products or services advertised. SMCMA reserves the right to reject any advertising.
Opinions expressed by authors are their own and not necessarily those of the SMCMA. San Mateo County Physician reserves the right to edit all contributions for clarity and length, as well as to reject any material submitted.
© Copyright 2012 San Mateo County Medical Association
Raymond Gaeta, M.D.Russ Granich, M.D.Edward Koo, M.D.C.J. Kunnappilly, M.D.Michael Norris, M.D.
Michael O’Holleran, M.D.Irwin Shelub, M.D.Chris Threatt, M.D. Kristen Willison, M.D.
David Goldschmid, M.D. ......................................CMA TrusteeScott A. Morrow..............Health Offi cer, County of San MateoDirk Baumann, M.D. .............................AMA Alternate Delegate
2011-2012 Offi cers & Board of Directors
New SMCMA Members
Russ Granich, M.D., ChairSharon Clark, M.D.Edward G. Morhauser, M.D
Gurpreet K. Padam, M.D.Michael Stevens, M.D
Corrections

OCTOBER 2012 | SAN MATEO COUNTY PHYSICIAN 19
We created the Tribute Plan to provide doctors with more than just a little gratitude for a career spent practicing good medicine. Now, the Tribute Plan has reached its five-year anniversary, and over 22,700 member physicians have qualified for a monetary award when they retire from the practice of medicine. More than 1,300 Tribute awards have already been distributed. So if you want an insurer that’s just as committed to honoring your career as it is to relentlessly defending your reputation, request more information today. Call The Doctors Insurance Agency at (415) 506-3030 or (800) 553-9293. You can also visit us at www.doctorsagency.com.
We do what no other medical liability insurer does. We reward loyalty at a level that is entirely unmatched. We honor years spent practicing good medicine with the Tribute® Plan. We salute a great career with an unrivaled monetary award. We give a standing ovation. We are your biggest fans. We are The Doctors Company.
Tribute Plan projections are not a forecast of future events or a guarantee of future balance amounts. For additional details, see www.thedoctors.com/tribute.

777 Mariners Island BoulevardSuite 100San Mateo, California 94404
ADDRESS SERVICE REQUESTED
Our passion protectsyour practice
CALL 1-800-652-1051 OR VISIT NORCALMUTUAL.COM
Proud to be endorsed by the San Mateo County Medical Association
At NORCAL Mutual, our numbers testify to great claims support for you. Of the claims we closed in 2011, 88% were closed without settlements or jury awards, compared to an industry average of 71%.* We won 86% of our trials, compared to 80% industry-wide.** You’re prepared for each stage of litigation and kept fully informed — and we don’t settle without your consent. We help you manage events so they don’t become claims, and, to back up our promise to stand by you, we remain financially stable, as evidenced by 29 consecutive years of “A” ratings by A.M. Best.
Our numbers add up to great claims support for your practice.
* Physicians Insurers Association of America Risk Management Review: 2011 Edition. **Jena et al. Research Letter, Online First: Outcomes of Medical Malpractice Litigation Against U.S. Physicians. Archives of Internal Medicine. May 14, 2012.
88 NO INDEMNITY
REGIONAL CLAIMSOFFICES
YEARS “A” RATED BY A.M. BEST29TR
IALS
86