Embed Size (px)
Citation preview

13.10.11.
1
SKOK, 2011
Kardiorespiratorna izdržljivost, trening snage i ishrana u redukciji telesne mase: naučni dokazi i
preporuke
www.chess.edu.rs
Doc. dr Marko Stojanović Prof. Dr Sergej Ostojić
GOJAZNOST
• Gojaznost-‐pretilost (lat. obesitas) je hronična bolest (bolesno stanje), koja se ispoljava prekomernim nakupljanjem masti u organizmu i povećanjem telesne težine.
• Svako povećanje telesne težine za 10% i više od idealne označava se kao gojaznost.
www.chess.edu.rs
Zašto bolesno stanje?
• Povezana sa nastankom niza oboljenja!!
• Hipertenzija • Diabetes mellitus • Oboljenja KVS • Srčani udar • Oboljenja unutrašnjih
organa posebno žučne kese • Osteoartritis • Neki tipovi kancera
www.chess.edu.rs
Zanimljivosti
• Jedan poseban fenomen koji nastaje kao posledica gojaznosti...
• Apnea u snu!! • Zbog prekomerne težine nastaju
prekidi u disanju koji traju sve dok se osoba ne probudi
• Lošiji san, smanjena radna sposobnost
• Ali i značajno povećana opasnost od srčanog udara
www.chess.edu.rs
• Epidemija ovog oboljenja je širom sveta u stalnom porastu, pa se gojaznost svrstava među vodeće bolesti savremene civilizacije.
• 1,7 milijardi ljudi na svetu je gojazno ili predgojazno (International Obesity Task Force)
• 220.000 hiljada smrti godišnje samo u Evropi!
• Oko 2,5 miliona u svetu
www.chess.edu.rs
• Danas se smatra da gojaznost nastaje kao posledica dejstva više različitih faktora (naslednih osobina, psiholoških, kulturoloških, socijalnih, metaboličkih, fizioloških i patofizioloških)
• multikauzalno oboljenje koje najčešće nastaje kao posledica interakcije genotipa (genetskih odlika individue) i faktora spoljne sredine.
www.chess.edu.rs

13.10.11.
2
Genetika? • Rezultati Finsko-‐Britanskog
istraživanja, objavljeni u američkom časopisu „Science“, pokazali su da na 16-‐tom ljudskom hromozomu postoji gen (nazvan FTO) koji utiče na gojaznost.
• Istraživanje sprovedeno na više od 40.000 ljudi pokazalo je da su osobe nosioci dva gena FTO izložene za 70% većoj opasnosti od pojave gojaznosti od osoba bez tog gena.
www.chess.edu.rs
Uticaj okruženja? • Druga polovina, koja deluje kao
okidač su spoljni faktori – nepravilno i neadekvatno
konzumiranje hrane, – smanjen nivo fizičke aktivnosti.
• Kada se u organizam duže vreme unosi veća količina energetski hranljivih materija nego što može da se potroši, ili....
• Kada se značajno smanji nivo energetske potrošnje u odnosu na unetu količinu energije...
• dolazi do posledičnog taloženja masti i povećanja telesne težine.
• Do gojaznosti neće doći ako postoji ravnoteža između unosa hrane i energetske potrošnje!
www.chess.edu.rs
Adipociti
• Najveće skladište energije u organizmu -‐ 1 g oslobađa 9 ccal
• Služi kao zaštita od naglih potresa unutrašnjih organa
• Štiti organizam od preteranog gubljenja toplote
• Značajan kao nosilac vitamina-‐ liposolubilnih
www.chess.edu.rs
Razvoj adipocita:
• Broj ćelija se povećava tokom predpuberteta i puberteta.
• Povećavaju volumen kako se pune mašću. • Kada dostignu maksimalni volumen, dele se! • Gojaznost nastaje kao posledica povećanja volumena i broja adipocita.
www.chess.edu.rs
Razvoj adipocita
• Sa mršavljanjem, volumen ćelija se smanjuje ali ne i njihov broj!
• Drugim rečima, možemo da ih “izduvamo” ali ne možemo da ih uklonimo!
• Što je najgore, one imaju tendenciju da se ponovo napune!
• Tj., sa povećanim brojem ćelija porast težine je brži.
www.chess.edu.rs

13.10.11.
3
Zašto se gojazni brže goje?
• Lipoprotein lipaza (LPL) podstiče skladištenje masti.
• LPL je smešten u adipocitima. • Gojazni imaju više ćelija, dakle više LPL. • Blagi porast energetskog unosa teže posledice ostavlja na gojazne osobe!
www.chess.edu.rs
Kontrola telesne težine strategija
Kontrolisana ishrana
& Fizička aktivnost
www.chess.edu.rs
Kada se u organizam duže vreme unosi veća količina energetski hranljivih materija nego što može da se potroši, ili....
Se smanji nivo energetske potrošnje u odnosu na unetu količinu energije...
Kalorijski deficit
• Kalorijski deficit od oko 500 kcal/dan dovodi do gubitka oko 0,7 kg/ nedeljno. • Ovo se može ostvariti samo smanjenim unosom. • Ipak , lakše je ostvariti kalorijski deficit sa kombinovanim režimom smanjenog
unosa i povećane potrošnje putem vežbanja. • Primer: 500 kcal kalorijskog deficita može se ostvariti smanjenim unosom od
250 kcal i povećanom potrošnjom od 250 kcal.
www.chess.edu.rs
Energetska vrednost unete hrane manja od energije utrošene u toku dana
OK, ali KAKO?
FIZIČKA AKTIVNOST!
1. Kardiorespiratorna izdržljivost • Pre svega služi za poboljšanje aerobne sposobnosti • Tako posmatrana, FITT principi su:

13.10.11.
4
Kardiorespiratorna izdržljivost
• Koristi se i u programima za redukciju telesne težine. • Zašto? • Sagori najviše energije u jedinici vremena!
www.chess.edu.rs
Interesantno…
• Porast fizičke aktivnosti uz smanjeni energetski unos dovodi do gubljena telesne mase - A kategorija dokaza – Ipak, važi samo u slučaju
nedrastičnog smanjenja kalorijskog unosa!
– Ukoliko je drastično smanjen unos kalorija - fizička aktivnost ne doprinosi smanjenju telesne mase
• Uz zadržavanje energetskog unosa: – 150 m/n - nema efekata – 150-225 m/n - relativno
skromni efekti – 225-400 m/n - relativno
veliki efekti (5-7 kg za 6-12 nedelja)
• B kategorija dokaza
Appropriate Physical Activity Intervention Strategies for Weight Loss and Prevention of Weight Regain for Adults-‐ ACSM 2009)
FITT principi... • Do tri puta nedeljno • 65-‐90% Hr max • Preko 30 min (poželjno 60) -‐minimum 8 nedelja • Bilo koji tip aktivnosti koji angažuje velike grupe mišića
www.chess.edu.rs
2. Trening snage
• “Da bi izgubili težinu, potrebno je da radite sa težinom”.
• Dobro programiranim treningom snage takođe je moguće potrošiti određeni broj kalorija na treningu.
• Uz neke dodatne efekte koji se ostvaruju ovim tipom vežbanja.
www.chess.edu.rs
• Povećava se FFM-‐nemasna masa tela!
• Drugim rečima-‐ povećava se količina skeletnih mišića
• Skeletni mišići-‐ motor u vašim kolima.
• Veći moto r-‐ veća potrošnja goriva...
• Čak i dok stojite na semaforu!
www.chess.edu.rs
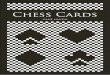
• Konceptualni model uticaja treninga sa opterećenjem na bazalni metabolizam i gubitak masnih naslaga u organizmu! (WEIGHT LOSS AND PREVENTION OF WEIGHT REGAIN-‐ ACSM 2009)
• RADI LI ZAISTA?
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.9
Less research has been conducted using resistance train-ing as part of an exercise intervention compared to aerobicexercise. This may be caused by the diminished energy andfat use compared to aerobic exercise during a typical sessionof the same duration. However, differences in hormonalresponse to resistance exercise (potential for acute stimulationof metabolic rate and fat oxidation after the activity) andenhancement of muscle protein balance (potential to chroni-cally increase total energy expenditure) provide some justifi-cation for the examination of benefits on body weight andcomposition. Studies evaluating the effect of resistance train-ing on body weight and composition are summarized below.There is less evidence for the effect of resistance exercise onbody composition than body weight because some studiesdid not assess body composition.
Neither randomized controlled (42,108,123,125) nor in-tervention studies without a sedentary comparison group(63,66,79,88,115) provide evidence for a reduction in bodyweight when resistance training is performed without anymodification of diet. However, the studies since 1999 areequally split concerning whether resistance training willcause a loss of body fat. Some studies report a modestreduction in body fat (63,66,88,125) when resistancetraining was continued for 16–26 wk, whereas othersreported no effect on body fat for interventions of 12–52 wk in duration (44,88,108,115). It is noteworthy that onestudy (88) reported a differential response on body fatdepending on age and gender; reduction in body fat wasobserved only for older men with no effect for young menor young or old women. Slightly more studies reported anincrease in lean mass after resistance training withoutmodification of diet (63,64,108,125) than those reportingno effect (44,115,123). Some of the differences amongstudies could be secondary to differences in body compo-sition technique used, duration of intervention, or specificexercise prescription. Combining resistance training withaerobic training has been shown to be superior for bodyweight and fat loss (3,110) and to result in greater lean bodymass (110) when compared to aerobic exercise alone inseveral randomized controlled trials but not others (26).
When resistance training is added to a reduced energyintake intervention, the energy restriction seems to over-shadow the resistance training. None of the recentlyperformed randomized controlled trials (73,75,82,117) ob-served a greater body weight loss for interventions lastingfrom 4 to 16 wk. Most studies did not detect greater bodyfat loss with resistance training over energy restriction alone(75,82,117), although one study (73) examined body fat atvarious sites using magnetic resonance imaging and re-ported a superior loss of subcutaneous body fat with thecombination of resistance training with diet compared todiet modification alone. On the other hand, most studiescombining resistance training with energy restriction reportimproved lean body mass compared to dieting alone(73,75,82,117).
Only two recent randomized controlled studies haveexamined the effect of resistance exercise on prevention ofweight gain or regain after weight loss (84,123). One studydemonstrated no difference in weight regain during a 6-month period after a very low energy diet for 90 subjectsassigned to walking, resistance training, or no exercise (84).A larger group of subjects (n = 164) was recruited forevaluation of regular resistance training to prevent gain infat mass for 2 yr (123). No differences were noted in bodyweight change during this period; however, total body fatdecreased more and intra-abdominal fat increased less forthe treatment group compared to the control.
There is a potentially interesting interaction betweenresistance training and dietary protein in interventions withoverweight individuals. Two randomized controlled trialscompared the effects of resistance training when combinedwith diets that varied in protein content (31,86). The higherprotein intervention was superior for either body weight andtotal fat lost (86) or prevention of lean tissue loss (31). Inone study, this was accomplished through a doubling of theoverall protein content of the diet to 1.6 gIkgj1 (86),whereas the other (31) used a high-protein supplement (10 gprotein) immediately after each resistance workout.
There is little literature and no clear pattern for outcomesof weight and body composition when the dose for
FIGURE 1—Conceptual model of resistance training and the potential effect on energy expenditure. A conceptual model that includes both theenergy expenditure from increased muscle mass and the potential energy expenditure from increased activities of daily living. RMR, restingmetabolic rate.
WEIGHT LOSS AND PREVENTION OF WEIGHT REGAIN Medicine & Science in Sports & Exercised 465
SPEC
IALCOMMUNICATIO
NS

13.10.11.
5
RMR (Resting Metabolic Rate)
• Jedna serija u treningu snage dovodi do porasta energetske potrošnje u miru za oko 5% u sledećih 72 sata …
• Ili oko 400 kilokalorija… (Heden et all, 2011) • Što je skoro isto kao i kada se rade tri serije!!! • Zaključak: čak i minimalno uključivanje treninga snage značajno doprinosi porastu kalorijske potrošnje!
www.chess.edu.rs
FITT
• 2 do 3 puta nedeljno • Dinamički režim rada • 70-‐85% od 1-‐RM • 6-‐12 ponavljanja u seriji • Do 3 serije-‐ ali i jedna je OK! • 4-‐10 vežbi, od čega pola za
velike mišićne grupe • Minimum 8 nedelja • Posebna napomena: težiti
što kraćim pauzama između serija.
www.chess.edu.rs
IDEALNI PROGRAM... Kombinovani trening
www.chess.edu.rs
Osnovni program
• Početi sa treningom za razvoj kardiorespiratorne izdržljivosti
• Podizati obim treninga do 45 minuta rada • Nakon toga na kraju treninga ubaciti vežbe sa sopstvenim telom (čučnjevi, sklekovi , trbuh, leđa)
• Jedna serija
www.chess.edu.rs
Osnovni program 2 • Umesto vežbi sa sopstvenim telom, ubaciti vežbe snage po preporuci za redukciju telesnih masti (početi sa najmanjim brojem vežbi i serija)
• Temeljne vežbe snage!
www.chess.edu.rs

13.10.11.
6
Napredni program I
• Promeniti redosled fitnes programa • Prebaciti trening snage pre kardio treninga. • Logika: ispražnjeni glikogenski depoi uticaće da se u
kardio treningu dodatno troše masne rezerve! • Moguće je uraditi trening snage većeg intenziteta
što će dodatno pozitivno uticati na energetsku potrošnju u samom treningu
• Ali i u povećanom bazalnom metabolizmu...
www.chess.edu.rs
Napredni program II
• Programi se rade odvojenim danima • Svaki po tri puta • Omogućava veliki intenzitet i obim treninga svim danima
• Veoma zahtevan! • Preporučuje se dobro treniranim rekreativcima!
www.chess.edu.rs
Kontrolisana ishrana
Trenutna znanja Osnovne smernice
Position of the American Dietetic Association: Weight Management (2009)
Koliko kalorija uneti ? • Prema energetskim potrebama! • Koje je poželjno utvrditi
merenjem (indirektna kalorimetrija)
• Ako nije dostupna, koristiti Mifflin - St.Jeor jednačinu (ADA,2009) za RMR
• Muškarci: • 10*težina (kg) + (6,25* TV (cm))
– (5 *god)+5 • Žene: • 10*težina (kg) + (6,25* TV (cm))
– (5 *god)- 161
• U cilju gubitka masnih naslaga, redukcija energetskog unosa od 500-100 kcal/d dovodi do gubitka od oko 0,5-1 kg nedeljno!
• Gornja preporučena vrednost!
• Minimalni energetski unos – M: 1200-1400 kcal/d – F : 1000-1200kcal/d
• (Strychar , 2006)
Kakva kompozicija makronutrijenata je optimalna?
Praksa • Veliki broj različitih dijeta
– Niskokalorijske (low-calorie)
– Niskomasne (low-fat) – Niskougljenohidratne (Low-
carbohydrate) – Ekstremno nisko
ugljenohidratne • Problem sa yo-yo efektom
– Ekstremno niskomasne • Isto kao prethodno
Trenutno znanje • Najveći broj sistematskih
preglednih članaka nagoveštava da niskokalorijske dijete (bez uticaja na kompoziciju makronutrijenata) imaju najbolje dugoročne efekte!
acid concentrations due to severe negative energy balance.71
Sudden death can occur, rarely, in vulnerable patients withcomorbidities, especially if the energy intake is less than2520 kJ per day.75 Sudden deaths resulting from very-low-calorie diets in the 1970s were attributed to the poor quality ofdietary protein; an inadequate supply of electrolytes, vitaminsand minerals; and extended use without adequate medical su-pervision.73,75
Physicians can refer patients to a registered dietitian toreceive a diet plan, or patients may consume commercialdiet products (e.g., sachets), which are available on pre-scription. These formulations should not be confused withmeal replacement products, which can be part of low-calo-rie diets. Low-calorie diets that use a meal replacementstrategy (1 or 2 meals substituted with a commercial forti-fied product containing about 840 kJ) induced greaterweight loss at 1 year (about 7%–8% of body weight) com-
pared with the traditional low-calorie diets without meal re-placements (3%–7% of body weight).76 Meal replacementsand very-low-calorie diets can assist patients control energyintake by reducing the need to make decisions about foodportion size.70
Overall, very-low-calorie diets present a number of med-ical risks but offer rapid weight loss. Intensive monitoring isrequired on the part of the physician, and patients must learnto maintain their weight loss when returning to normal eat-ing patterns.
Very-low-fat diets
Many of the very-low-fat diets, which contain about 10%–15%total fat, were originally designed to prevent or reverse heartdisease.14 Two of the most well-known very-low-fat diets,which are now promoted for weight loss, are the Ornish and
CMAJ • January 3, 2006 • 174(1) | 60
Review
Table 1: Characteristics of weight-loss diets
Diet type Strategy Weight-loss efficacy Effects on lipids Adverse clinical effects
Low calorie Energy intake reduced by2000–4000 kJ (500–1000 kcal)Total daily energy intakecomposed of:• 50%–55% carbohydrates• 10%–15% proteins• 20%–35% fatsSaturated fat intake restricted
6 mo: about 8% of bodyweight (4–13 kg)8,58,60,61,72
≥ 1 yr: about 4% of bodyweight (2–11 kg)8,59,74
Using Step I NCEP diets,decreases in totalcholesterol and low-density lipoproteincholesterol levels andvariable effects ontriglyceride and high-density lipoproteincholesterol levels14–15
Headache, constipation60
Lowcarbohydrate(e.g., Atkinsdiet)
No restriction of energy intakeCarbohydrates restricted to 3%–10% of total daily energy intakeNo restrictions on protein orfat intakeNo restrictions on saturated fatintakeVitamin and mineralsupplementation
6 mo: about 13% of bodyweight (8–12 kg)58,6
≥ 1 yr: about 4% of bodyweight (5 kg)59,61
Decreases in triglyceridelevels; variable effectson total cholesterol andlow-density lipoproteinlevels58-61 and high-density lipoproteinlevels59
Constipation, headache,halitosis, muscle cramps,diarrhea, general weakness,rash60
Reports of a small number ofcardiac events59,60
Long-term effects on CV risksnot assessedNot suitable if kidney or liverfunction is impaired
Very lowcalorie
Daily energy intake restrictedto 1600–3500 kJ (400–800 kcal)using a government-regulatedcommercial product or dietprepared by a registereddietitianVitamin and mineralsupplementationWeekly monitoring by physicianUse restricted to 16 wk andfollowed by a LCD
4 mo: about 30%–40% ofbody weight (13–32 kg)8,72,73,74
≥ 1 yr: VLCD + LCDabout 30% of body weight(7–20 kg)8,72,73,74
Decreases in totalcholesterol, low-densitylipoprotein cholesteroland triglyceridelevels71,73
Dry mouth, constipation,headache, dizziness ororthostatic hypotension,fatigue, cold intolerance, dryskin, menstrual irregularities,hair loss73
Gout, cholelithiasis, excessiveloss of lean body mass, acutepsychosis, cardiac disturbancesand sudden death71-73
Not suitable for long-term use
Very low fat Energy intake reducedTotal daily energy intakecomposed of:• 60%–80% carbohydrates• 10%–15% proteins• 10%–15% fatsSaturated fat intake restrictedSmall amounts of meat andmeat alternatives; very highintake of fibre
4 mo: about 10% of bodyweight (9 kg)14
≥ 1 yr: about 6%–12% ofbody weight (6–11 kg)77
(diet plus exercise)
Decreases in totalcholesterol and low-density lipoproteincholesterol levels andvariable effects ontriglyceride and high-density lipoproteincholesterol levels14,77,78
Flatus, abdominal fullness14
Note: NCEP = National Cholesterol Education Program, CV = cardiovascular, LCD = low-calorie diet, VLCD = very-low-calorie diet.

13.10.11.
7
Pred kraj....
www.chess.edu.rs
Problemi vezani za pothranjenost
• Premalo masnih naslaga u organizmu može da prouzrokuje niz reproduktivnih, kardiovaskularnih i imunih problema! – Ispod 10–12% za žene – Ispod 5% za muškarce
www.chess.edu.rs
Ciljevi programa za redukciju telesne mase
• Inicijalni cilj treba da bude gubitak oko 10% težine u roku od 6 meseci (ACSM, ADA)
• Istraživanja su pokazala da postoje i mnogo efikasniji programi, ali se nakon završetka eksperimentalnog tretmana težina vraća na stare vrednosti ili čak i više od toga.
• Važno zbog motivacije i postavljanja ciljeva-‐ nerealni ciljevi dovode do napuštanja programa!
www.chess.edu.rs
Za sladokusce…
Novi recepti naučne kuhinje…
1. Više, a isto teško?
• Uključivanje većeg broja mišićnih grupa u toku aktivnosti dovodi do interesantnog fenomena: – Povećava se energetska potrošnja za isti subjektivni osećaj zamora!
– NPR, nordijsko hodanje (Figard-‐Fabre et al. 2011)
– Jedan od načina za postizanje povećane kalorijske potrošnje
www.chess.edu.rs
2. Ekscentrični trening snage
• Dovodi do značajnijeg porasta kalorijske potrošnje u miru od tradicionalnog treninga snage! – Oko 9% čak do 72 sata nakon treninga (Hackney et al, 2008)
• Za napredne programe-‐ i promociju sopstvenog znanja – ekcentrični trening snage!
www.chess.edu.rs

13.10.11.
8
3. Mleko za telesnu kompoziciju žena
• dve čaše mleka nakon treninga snage u toku 12 nedelja (Tarnopolsky et al,2010)
• Žene koje su unosile mleko ostvarile su značajno veći porast mišićnog tkiva od osoba koje su unosile istu količinu energetskog napitka
• Takođe, značajno veći gubitak masnih naslaga. • Značajno poboljšana telesna kompozicija
www.chess.edu.rs
Najvažniji znak na svetu je -‐ znak pitanja -‐ (Konije)
SKOK 2011
Doc dr Marko Stojanović Prof. Dr Sergej Ostojić
www.chess.edu.rs