Embed Size (px)
Citation preview
1349
□ CASE REPORT □
Solid Pseudopapillary Neoplasm of the PancreasAssociated with Familial Adenomatous Polyposis
Tadahisa Inoue 1, Yuji Nishi 1, Fumihiro Okumura 1, Takashi Mizushima 1, Hirotada Nishie 1,
Hiroyasu Iwasaki 1, Kaiki Anbe 1, Takanori Ozeki 1, Kenta Kachi 1, Shigeki Fukusada 1,
Yuta Suzuki 1, Akira Mizuno 2, Masaki Kajikawa 2, Kazuko Watanabe 3 and Hitoshi Sano 1
Abstract
A man in his thirties visited our hospital for an evaluation of a 12×10-mm pancreatic solid tumor that was
accidentally detected on computed tomography performed for follow-up of familial adenomatous polyposis
(FAP). We diagnosed the patient with a solid pseudopapillary neoplasm (SPN) based on endoscopic
ultrasound-guided fine-needle aspiration, and he underwent pancreaticoduodenectomy. Small SPN tumors ap-
pear as solid tumors, without typical features of SPN, making the definitive diagnosis more difficult. The ge-
netic background of FAP patients can predispose them to SPN, and imaging of the pancreas should be per-
formed at prescribed intervals in FAP patients.
Key words: solid pseudopapillary neoplasm, familial adenomatous polyposis, β-catenin, endoscopic
ultrasound-guided fine-needle aspiration
(Intern Med 54: 1349-1355, 2015)(DOI: 10.2169/internalmedicine.54.4061)
Introduction
Solid pseudopapillary neoplasms (SPNs) of the pancreas
are rare, accounting for approximately 0.17-2.7% of all exo-
crine pancreatic tumors (1). Most SPN patients are women;
less than 10% of reported SPN patients in the literature are
men (2). SPN is usually detected as a heterogeneous mass
with a combination of solid and cystic areas, with larger tu-
mors containing areas of calcification in the tumor wall. In
contrast, small SPN tumors appear as solid tumors and lack
these typical features, making the definitive diagnosis more
difficult.
We herein present a case of SPN with a very small lesion
in an adult man. SPN was accidentally detected during
follow-up for familial adenomatous polyposis (FAP). The
clinicopathological features of SPN remain uncertain. How-
ever, it is possible that the genetic background of patients
with FAP predisposes them to developing SPN (3, 4). In
fact, patients with SPN associated with FAP have been re-
ported, although the number of cases is very few (5). We
believe that the present case is informative with respect to
the relationship between SPN and FAP. We thus present this
case along with a review of the literature.
Case Report
A Japanese man in his thirties visited our hospital for an
evaluation of a pancreatic tumor accidentally detected on
computed tomography (CT) performed for the follow-up of
FAP. The patient had a history of FAP and colon cancer,
while his father, paternal grandmother and all six paternal
uncles and aunts also had colon cancer and his sister had
colon polyposis. He currently had no symptoms, and the
laboratory findings were normal, including the levels of tu-
mor markers (Table). CT of the abdomen revealed a 12×10-
mm round solid mass in the pancreatic head (Fig. 1). The
tumor was increasingly enhanced, although the extent of en-
hancement was less than that observed in the non-tumor pa-
renchyma of the pancreas (Fig. 2). No cystic areas or sites
1Department of Gastroenterology, Gifu Prefectural Tajimi Hospital, Japan, 2Department of Surgery, Gifu Prefectural Tajimi Hospital, Japan and3Department of Pathology, Gifu Prefectural Tajimi Hospital, Japan
Received for publication September 7, 2014; Accepted for publication October 13, 2014
Correspondence to Dr. Tadahisa Inoue, [email protected]
Intern Med 54: 1349-1355, 2015 DOI: 10.2169/internalmedicine.54.4061
1350
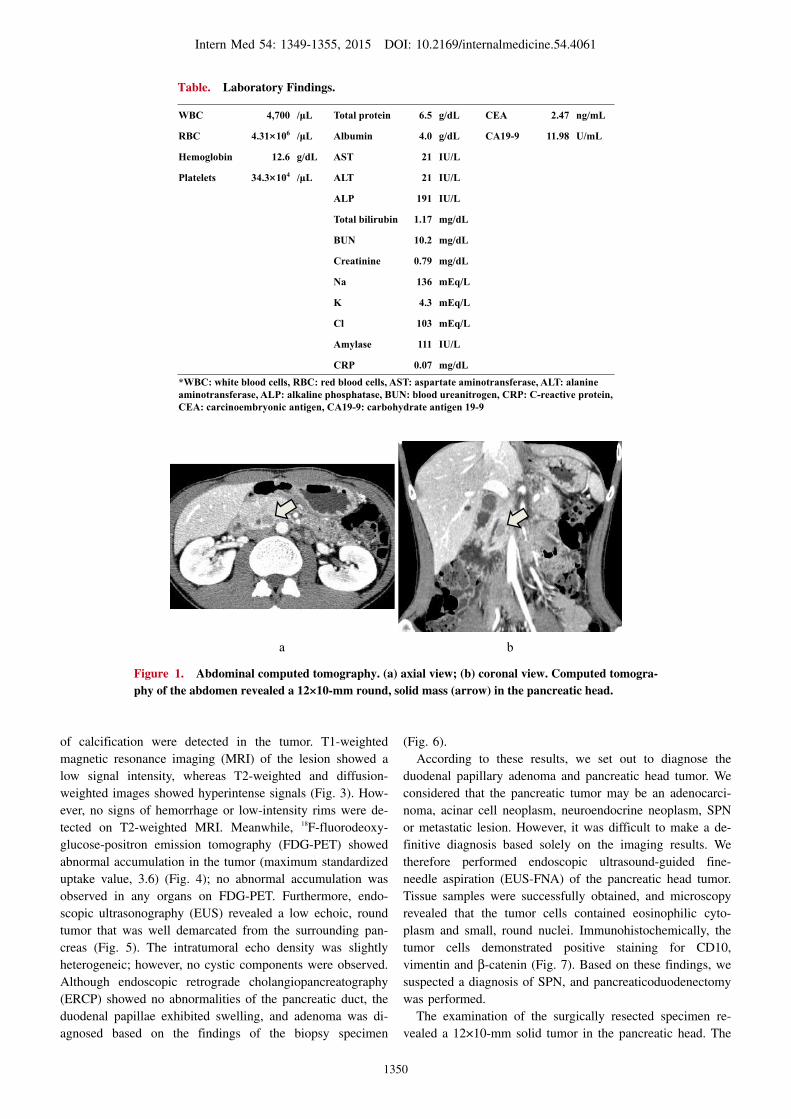
Figure 1. Abdominal computed tomography. (a) axial view; (b) coronal view. Computed tomogra-phy of the abdomen revealed a 12×10-mm round, solid mass (arrow) in the pancreatic head.
a b
Table. Laboratory Findings.
WBC 4,700 / L Total protein 6.5 g/dL CEA 2.47 ng/mL
RBC 4.31×106 / L Albumin 4.0 g/dL CA19-9 11.98 U/mL
Hemoglobin 12.6 g/dL AST 21 IU/L
Platelets 34.3×104 / L ALT 21 IU/L
ALP 191 IU/L
Total bilirubin 1.17 mg/dL
BUN 10.2 mg/dL
Creatinine 0.79 mg/dL
Na 136 mEq/L
K 4.3 mEq/L
Cl 103 mEq/L
Amylase 111 IU/L
CRP 0.07 mg/dL*WBC: white blood cells, RBC: red blood cells, AST: aspartate aminotransferase, ALT: alanineaminotransferase, ALP: alkaline phosphatase, BUN: blood ureanitrogen, CRP: C-reactive protein,CEA: carcinoembryonic antigen, CA19-9: carbohydrate antigen 19-9
of calcification were detected in the tumor. T1-weighted
magnetic resonance imaging (MRI) of the lesion showed a
low signal intensity, whereas T2-weighted and diffusion-
weighted images showed hyperintense signals (Fig. 3). How-
ever, no signs of hemorrhage or low-intensity rims were de-
tected on T2-weighted MRI. Meanwhile, 18F-fluorodeoxy-
glucose-positron emission tomography (FDG-PET) showed
abnormal accumulation in the tumor (maximum standardized
uptake value, 3.6) (Fig. 4); no abnormal accumulation was
observed in any organs on FDG-PET. Furthermore, endo-
scopic ultrasonography (EUS) revealed a low echoic, round
tumor that was well demarcated from the surrounding pan-
creas (Fig. 5). The intratumoral echo density was slightly
heterogeneic; however, no cystic components were observed.
Although endoscopic retrograde cholangiopancreatography
(ERCP) showed no abnormalities of the pancreatic duct, the
duodenal papillae exhibited swelling, and adenoma was di-
agnosed based on the findings of the biopsy specimen
(Fig. 6).
According to these results, we set out to diagnose the
duodenal papillary adenoma and pancreatic head tumor. We
considered that the pancreatic tumor may be an adenocarci-
noma, acinar cell neoplasm, neuroendocrine neoplasm, SPN
or metastatic lesion. However, it was difficult to make a de-
finitive diagnosis based solely on the imaging results. We
therefore performed endoscopic ultrasound-guided fine-
needle aspiration (EUS-FNA) of the pancreatic head tumor.
Tissue samples were successfully obtained, and microscopy
revealed that the tumor cells contained eosinophilic cyto-
plasm and small, round nuclei. Immunohistochemically, the
tumor cells demonstrated positive staining for CD10,
vimentin and β-catenin (Fig. 7). Based on these findings, we
suspected a diagnosis of SPN, and pancreaticoduodenectomy
was performed.
The examination of the surgically resected specimen re-
vealed a 12×10-mm solid tumor in the pancreatic head. The

Intern Med 54: 1349-1355, 2015 DOI: 10.2169/internalmedicine.54.4061
1351
Figure 2. Dynamic contrast-enhanced computed tomography. (a) non-enhanced; (b) arterial phase; (c) portal venous phase; (d) equilibrium phase. The pancreatic head tumor was increasingly en-hanced, although the extent of enhancement was less than that observed in the non-tumor parenchy-ma of the pancreas.
a b c d
Figure 3. Magnetic resonance imaging. (a) T1-weighted images (in phase); (b) T1-weighted images (out of phase); (c) T2-weighted images; (d) diffusion-weighted images. T1-weighted magnetic reso-nance imaging of the pancreatic head tumor (arrow) showed a low-intensity signal; T2- and diffusion-weighted images showed a hyperintense signal.
cut section contained a yellow, solid tumor that was well de-
marcated from the surrounding pancreas. The tumor did not
contain cystic components, and the histological findings
were similar to those of the EUS-FNA specimen. In particu-
lar, tumor cells with eosinophilic cytoplasm and small,
round nuclei were arranged around fibrovascular stalks and
displayed a pseudopapillary structure (Fig. 8). The final
pathological diagnosis of the pancreatic head tumor was
SPN. In contrast, the duodenal papillae was diagnosed as
low-grade adenoma without malignancy. No other lesions
were observed in the resected area, including the duodenum.
Discussion
SPN of the pancreas was first reported by Frantz in
1959 (6). According to the WHO classification, SPN is “a
low-grade malignant neoplasm composed of poorly cohe-
sive, monomorphic epithelial cells forming solid and pseu-
dopapillary structures. These neoplasms frequently undergo
hemorrhagic-cystic degeneration and occur predominantly in
young women (7).” The reported incidence of SPN is ex-
tremely low, accounting for only 0.17-2.7% of all exocrine
pancreatic tumors (1). In addition, only 10% of reported
Intern Med 54: 1349-1355, 2015 DOI: 10.2169/internalmedicine.54.4061
1352
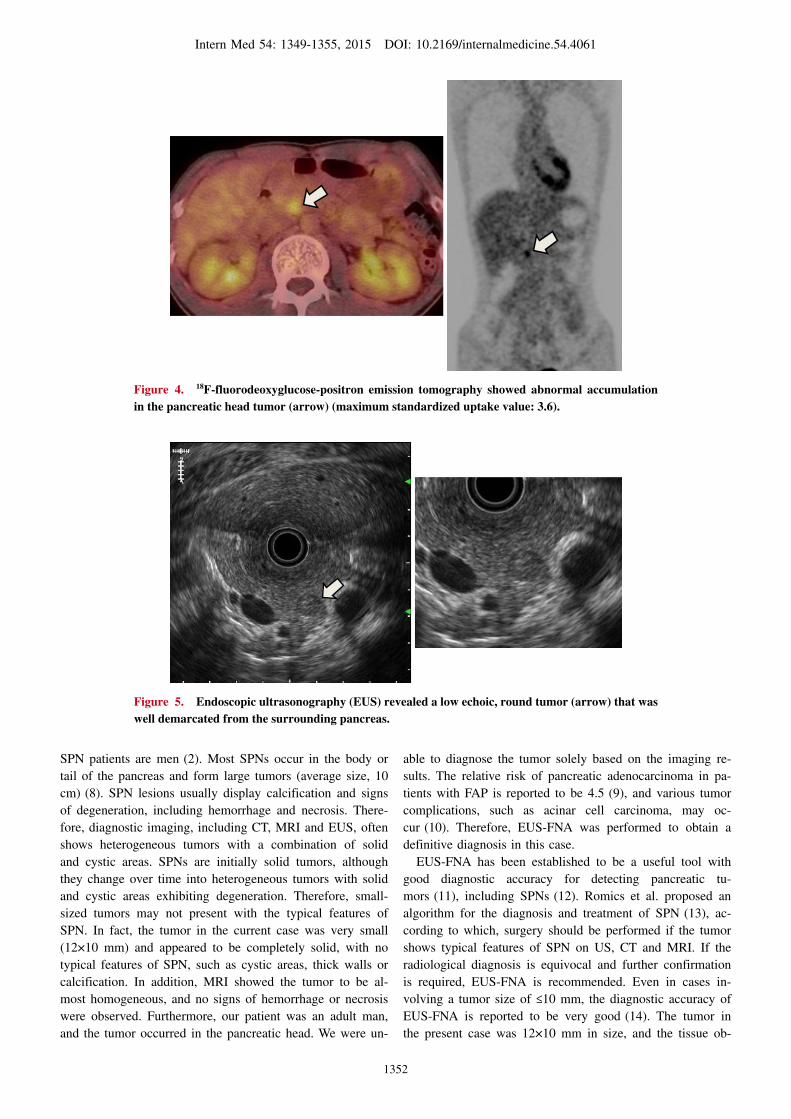
Figure 4. 18F-fluorodeoxyglucose-positron emission tomography showed abnormal accumulation in the pancreatic head tumor (arrow) (maximum standardized uptake value: 3.6).
Figure 5. Endoscopic ultrasonography (EUS) revealed a low echoic, round tumor (arrow) that was well demarcated from the surrounding pancreas.
SPN patients are men (2). Most SPNs occur in the body or
tail of the pancreas and form large tumors (average size, 10
cm) (8). SPN lesions usually display calcification and signs
of degeneration, including hemorrhage and necrosis. There-
fore, diagnostic imaging, including CT, MRI and EUS, often
shows heterogeneous tumors with a combination of solid
and cystic areas. SPNs are initially solid tumors, although
they change over time into heterogeneous tumors with solid
and cystic areas exhibiting degeneration. Therefore, small-
sized tumors may not present with the typical features of
SPN. In fact, the tumor in the current case was very small
(12×10 mm) and appeared to be completely solid, with no
typical features of SPN, such as cystic areas, thick walls or
calcification. In addition, MRI showed the tumor to be al-
most homogeneous, and no signs of hemorrhage or necrosis
were observed. Furthermore, our patient was an adult man,
and the tumor occurred in the pancreatic head. We were un-
able to diagnose the tumor solely based on the imaging re-
sults. The relative risk of pancreatic adenocarcinoma in pa-
tients with FAP is reported to be 4.5 (9), and various tumor
complications, such as acinar cell carcinoma, may oc-
cur (10). Therefore, EUS-FNA was performed to obtain a
definitive diagnosis in this case.
EUS-FNA has been established to be a useful tool with
good diagnostic accuracy for detecting pancreatic tu-
mors (11), including SPNs (12). Romics et al. proposed an
algorithm for the diagnosis and treatment of SPN (13), ac-
cording to which, surgery should be performed if the tumor
shows typical features of SPN on US, CT and MRI. If the
radiological diagnosis is equivocal and further confirmation
is required, EUS-FNA is recommended. Even in cases in-
volving a tumor size of �10 mm, the diagnostic accuracy of
EUS-FNA is reported to be very good (14). The tumor in
the present case was 12×10 mm in size, and the tissue ob-
Intern Med 54: 1349-1355, 2015 DOI: 10.2169/internalmedicine.54.4061
1353
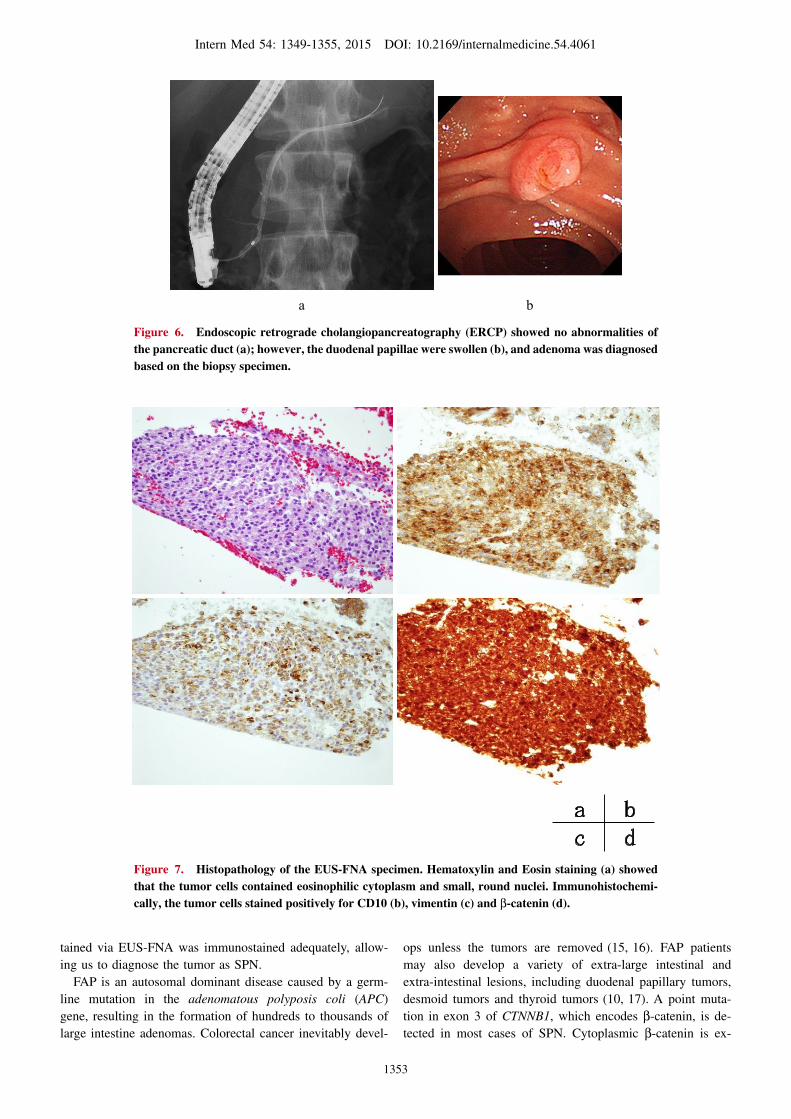
Figure 6. Endoscopic retrograde cholangiopancreatography (ERCP) showed no abnormalities of the pancreatic duct (a); however, the duodenal papillae were swollen (b), and adenoma was diagnosed based on the biopsy specimen.
a b
Figure 7. Histopathology of the EUS-FNA specimen. Hematoxylin and Eosin staining (a) showed that the tumor cells contained eosinophilic cytoplasm and small, round nuclei. Immunohistochemi-cally, the tumor cells stained positively for CD10 (b), vimentin (c) and β-catenin (d).
tained via EUS-FNA was immunostained adequately, allow-
ing us to diagnose the tumor as SPN.
FAP is an autosomal dominant disease caused by a germ-
line mutation in the adenomatous polyposis coli (APC)
gene, resulting in the formation of hundreds to thousands of
large intestine adenomas. Colorectal cancer inevitably devel-
ops unless the tumors are removed (15, 16). FAP patients
may also develop a variety of extra-large intestinal and
extra-intestinal lesions, including duodenal papillary tumors,
desmoid tumors and thyroid tumors (10, 17). A point muta-
tion in exon 3 of CTNNB1, which encodes β-catenin, is de-
tected in most cases of SPN. Cytoplasmic β-catenin is ex-

Intern Med 54: 1349-1355, 2015 DOI: 10.2169/internalmedicine.54.4061
1354
Figure 8. Histopathology of the surgical specimen. A 12×10-mm solid tumor was detected in the pancreatic head (a). The cut section revealed a yellow, solid tumor (arrow) that was well demarcated from the surrounding pancreas (b). Tumor cells with eosinophilic cytoplasm and small, round nuclei were arranged around fibrovascular stalks and displayed a pseudopapillary structure (c, d).
pressed at low levels under normal conditions and increased
in most patients with SPN (18, 19). The FAP-related muta-
tion in APC activates the Wnt/β-catenin signaling pathway.
As a result, the cytoplasmic β-catenin expression increases,
as it does in cases involving the SPN-related CTNNB1 muta-
tion (20). Therefore, patients with FAP may develop tumors
commonly seen in those with CTNNB1. However, based on
our literature search, we were able to find only one case of
concurrent FAP and SPN (5). The fact that both FAP and
SPN are rare diseases and FAP can easily complicate cases
of pancreatic and duodenum papilla cancer may explain the
reduced rate of concurrent SPN cases. The current patient
was confirmed to have an APC mutation on a genetic ex-
amination, and the tumor specimen was shown to express
cytoplasmic β-catenin. These factors suggest that this case
of SPN occurred as a result of the FAP-related mechanism
described above. Furthermore, the present patient was male
with primary onset in the pancreatic head, which is atypical
for SPN. A case of FAP with primary onset in the pancre-
atic head has also been reported in a woman (5). Therefore,
a causal relationship with the site of onset is suspected, al-
though the details remain unclear due to the lack of avail-
able cases.
SPN is classified as a low-grade malignant neoplasm.
SPN patients treated with complete surgical resection have a
good prognosis (21). However, approximately 15-20% of
cases of SPN manifest with malignant behavior, including
perineural or vascular infiltration and metastasis (22, 23).
Fatal cases of recurrence have been reported (24). Therefore,
the diagnosis of SPN and subsequent surgical resection
should be performed without delay. In the present case, we
detected the tumor at a very early stage by chance because
CT was performed for the follow-up of FAP. As patients
with FAP may develop a variety of tumors, routine imaging
of the pancreas should be conducted at designated intervals
and practitioners should keep in mind the fact that FAP can
predispose patients to SPN.
The authors state that they have no Conflict of Interest (COI).
References
1. Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of
the pancreas: review of 718 patients reported in English literature.
J Am Coll Surg 200: 965-972, 2005.
2. Sperti C, Berselli M, Pasquali C, Pastorelli D, Pedrazzoli S. Ag-
gressive behavior of solid-pseudopapillary tumor of the pancreas
in adults: a case report and review of the literature. World J Gas-
troenterol 14: 960-965, 2008.
3. Adamthwaite JA, Verbeke CS, Stringer MD, Guillou PJ, Menon
KV. Solid pseudopapillary tumour of the pancreas: diverse presen-

Intern Med 54: 1349-1355, 2015 DOI: 10.2169/internalmedicine.54.4061
1355
tation, outocome and histology. JOP 7: 635-642, 2006.
4. Gou S, Yu J, Wang C, Liu T, Cui P, Li X. Three female familial
cases of solid pseudopapillary tumors with a protease serine 1
gene mutation. Pancreas 42: 168-173, 2013.
5. Ruo L, Coit DG, Brennan MF, Guillem JG. Long-term follow-up
of patients with familial adenomatous polyposis undergoing pan-
creaticoduodenal surgery. J Gastrointest Surg 6: 671-675, 2002.
6. Frantz VK. Tumors of the pancreas. In: Atlas of tumor pathology,
1st series. Armed Forces Institute of Pathology, Washington, DC,
USA, 1959: 32-33.
7. Bosman FT, Carneiro F, Hruban RH, et al. WHO Classification of
tumours of the Digestive System. 4 th Ed. JARC Press, Lyon,
2010: 327-330.
8. Mao C, Guvendi M, Domenico DR, Kim K, Thomford NR,
Howard JM. Papillary cystic and solid tumors of the pancreas; a
pancreatic embryonic tumor? Studies of three cases and cumula-
tive review of the world’s literature. Surgery 118: 821-828, 1995.
9. Giardiello FM, Offerhaus GJ, Lee DH, et al. Increased risk of thy-
roid and pancreatic carcinoma in familial adenomatous polyposis.
Gut 34: 1394-1396, 1993.
10. Groen EJ, Roos A, Muntinghe FL, et al. Extra-intestinal manifes-
tations of familial adenomatous polyposis. Ann Surg Oncol 15:
2439-2450, 2008.
11. Hewitt MJ, McPhail MJ, Possamai L, Dhar A, Vlavianos P,
Monahan KJ. EUS-guided FNA for diagnosis of solid pancreatic
neoplasms: a meta-analysis. Gastrointest Endosc 75: 319-331,
2012.
12. Jani N, Dewitt J, Eloubeidi M, et al. Endoscopic ultrasound-
guided fine-needle aspiration for diagnosis of solid pseudopapil-
lary tumors of the pancreas: a multicenter experience. Endoscopy
40: 200-203, 2008.
13. Romics L Jr, Olah A, Belagyi T, Hajdu N, Gyurus P, Ruszinko V.
Solid pseudopapillary neoplasm of the pancreas-proposed algo-
rithms for diagnosis and surgical treatment. Langenbecks Arch
Surg 395: 747-755, 2010.
14. Uehara H, Ikezawa K, Kawada N, et al. Diagnostic accuracy of
endoscopic ultrasound-guided fine needle aspiration for suspected
pancreatic malignancy in relation to the size of lesions. J Gastro-
enterol Hepatol 26: 1256-1261, 2011.
15. Tudyka VN, Clark SK. Surgical treatment in familial adenomatous
polyposis. Ann Gastroenterol 25: 201-206, 2012.
16. Cruz-Correa M, Giardiello FM. Familial adenomatous polyposis.
Gastrointest Endosc 58: 885-894, 2003.
17. Iwama T, Tamura K, Morita T, et al. A clinical overview of famil-
ial adenomatous polyposis derived from the database of the Poly-
posis Registry of Japan. Int J Clin Oncol 9: 308-316, 2004.
18. Tanaka Y, Kato K, Notohara K, et al. Frequent β-catenin mutation
and cytoplasmic/nuclear accumulation in pancreatic solid-
pseudopapillary neoplasm. Cancer Res 61: 8401-8404, 2001.
19. Huang SC, Ng KF, Yeh TS, Chang HC, Su CY, Chen TC. Clini-
copathological analysis of beta-catenin and axin-1 in solid pseu-
dopapillary neoplasms of the pancreas. Ann Surg Oncol 130: 554-
559, 2013.
20. Abraham SC, Wu TT, Klimstra DS, et al. Distinctive molecular
genetic alterations in sporadic and familial adenomatous
polyposis-associated pancreatoblastomas: frequent alterations in
the APC/beta-batenin pathway and chromosome 11p. Am J Pathol
159: 1619-1627, 2001.
21. Yu PF, Hu ZH, Wang XB, et al. Solid pseudopapillary tumor of
the pancreas: A revies of 553 cases in Chinese literature. World J
Gastroenterol 16: 1209-1214, 2010.
22. Chung YE, Kim MJ, Choi JY, et al. Differentiation of benign and
malignant solid pseudopapillary neoplasms of the pancreas. J
Comput Assist Tomogr 33: 689-694, 2009.
23. Huang HL, Shih SC, Chang WH, Wang TE, Chen MJ, Chan YJ.
Solid-pseudopapillary tumor of the pancreas: clinical experience
and literature review. World J Gastroenterol 11: 1403-1409, 2005.
24. Yang F, Jin C, Long J, et al. Solid pseudopapillary tumor of the
pancreas: a case series of 26 consecutive patients. Am J Surg 198:
210-215, 2009.
Ⓒ 2015 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imonline/index.html