Embed Size (px)
Citation preview

STUDIES ON THE THYROID FUNCTION IN NEPHROTIC SYNDROME
lcHIRO AKIYAMA, YASUYUKI SASAKI, EMIKO YANAGIDA
AND YURIKO SAIKI
8rd Department of Internal Medicine, Nagoya University School of Medicine (Director: Prof. Kenichi Usami)
INTRODUCTION
305
So far many workers have discussed the cause of nephrotic syndrome, particularly of lipoid nephrosis, but there still remain many obscure points. From clinical symptoms such as anasarca, the drop in basal metabolism and hypercholesterolemia seen in myxedema, and from the fact that thyroid substance is sometimes effective in nephrosis, Epstein 11 emphasized that nephrosis is mainly due to hypofunction of the thyroid gland. There are some reports of iodine determinations of whole blood made in order to determine the thyroid function in nephrosis, but very few where the thyroid function was examined, in order to determine the serum 2131 protein-bound iodine which is now considered to represent more accurately the function of the thyroid gland. Needless to say, the thyroid gland is an endocrine gland closely related to metabolism, oxygen consumption and protein metabolism.
We studied on the protein-bound iodine (PBI), basal metabolic rate (BMR), serum cholesterol, and electrophoretic analyses of plasma protein, in order to measure the thyroid function of patients with nephrotic syndromes, and by consideration of their relationships, we obtained several new findings that are reported below.
MATERIALS
This study was carried out on 9 cases with nephrotic syndrome from inpatients and outpatients at the Usami Clinic of Nagoya University Hospital, and as contrast cases, 12 healthy adults and 27 with thyroid diseases 4151617 l (8 with simple goitre, 10 with hyperthyroidism in a narrow sense and 9 with Basedow's disease) were selected. All patients were examined or venipunctured early in the morning in the fasting state. Administrations of various drugs and injections were withhold, and foods with large content of iodine were prohibited for at least several days before the day of examination. In female patients we avoided measurments during, and immediately before or after menstruation.
EXPERIMENTAL METHODS
The methods of measurment were as follows; (1) Protein-bound iodine (PBI) The determination of PBI was made by Barker's 3 " 1 alkaline incineration
Received for publication October 8, 1954.

306 I. AKIYAMA ET AL.
method. Ashing was carried out by placing the quartz test-tube in a muffle furnace for two hours at 600 ± 25° C. Photoelectric colorimeter was used for Colorimetric determination of iodine. We calculated by an ordinary graph of standard solution of potassium iodide.
(2) Basal metabolic rate (BMR) BMR was examined by Knipping's 101111121 apparatus, and calculated by the
graphs of Du Bois, Boothby and Sandiford. (3) Serum cholesterol Serum cholesterol was measured by the method of Schoenheimer-Sperry,l31
and colorimetric determination made by Beckmans' Spectrophotometer. (4) Plasma protein fraction Electrophoretic analyses of blood plasma were carried out with Tiselius'
apparatus 141151 (Type HT-A made by Hitachi) according to Schlieren-diagonal method. Plasma was dialyzed for 16-20 hours, before electrophoresis against 1/20 M phosphate buffer.
Experimental conditions were as follows ; electric voltage 100 v., electric current 15 milliamp., time of electrophoresis 30-60 min., temperature 3-16o C. Percentages of plasma protein fractions were determined by the weight measurments of an electrophoretic ascending pattern.
(1) Protein-bound iodine (PB!) (a) Normal adults (Table 1)
RESULTS
The PBI of normal adults varies from 4.6 to 8.4 r /dl, with an average of 6.13 r/dl, as shown in table 1, and indicates slightly higher values of both maximum and minimum. There are many reports on this, which are as follows: 4.0-8.0 r/dl (Basset 161 ); 3.5-7.0 r/dl (Riggs 171 ); 3.7-6.7 r/dl (Rapport 131 and Connor191201); 4.0-8.0 r/dl (Danowski 21 1 and Heineman 221); 4.5-8.2 r/dl (Barker 23 ');
TABLE 1. Serum Protein-Bound Iodine and Basal Metabolic Rate in Normal Adults
------------- --
Case I Name Age Sex ' SPBI BMR Oz COz I RQ X y
No. (Y jdll ( OC) (!) (!) (cal.) (cal.)
M. 0. 26 0 8.4 +10.0. ].73 1.45 I 0.83 I 1221 1110 T. G. 32 9 5.9 + 0.9 1.50 1.29 0.86 1065 1055 Y. 0. 28 0 6.3 - 1.3 2.10 2.00 0.95 1516 1536 H. s. 23 Q 5.2 + 11.1 • 2.01 1.61 0.80 1411 1270 H. M. 23 9 5.5 +14.6 1.94 1.18 0.61 1313 1146 S. N. 26 9 4.6 ' - 2.s I 1.53 1.23 0.80 1074 1101 K. A. 22 9 6.2 + 3.3 I 2.01 1.02 0.51 1321 1279 s. w. 26 9 7.0 + 6.6 I 1.72 0.99 0.78 1202 1128 M. N. 46 9 5.0 - 9.8 I 1.75 1.17 0.67 1197
i 1313
T. s. 57 Q 5.5 + 0.4 I 1.82 1.07 0.59 1227 1123 K. A. 36 0 7.5 K. N. 24 Q 6.4
Variation --~46 _ 8 4~9~8-- -T.so 0.99 0.51 1065 1055
• • i -+14.6 -2.10 -2.00 -0.95 -1516 -1536 - ----------~
Mean I 6.13 +3.3 1.81 1.30 0.74 '
1255 1206 --------- ------------- ----------

THE THYROID FUNCTION IN NEPHROTIC SYNDROME 307
3-10 r/dl (Harsha 24l); 3-6 r/dl (Hardy 25l); 6.0-7.5 r/dl (Sogen 26l); 5.42 r/dl (Kumaoka271); and 4.2-8.9 r/dl (Shichijo).
(b) Patients with thyroid disease (Tables 2, 3, 4) The PBI in simple goitre varied from 6.0 to 8.1 r/dl and was 7.22 r/dl on
an average, indicating a little higher value. In cases of hyperthyroidism it was from 7.3 to 13.5 r/dl and was 9.84 r/dl on an average, indicating a far higher value than in simple goitre. In Basedow's disease it was from 10.5 to 19.5 r /dl and was 15.3 r/dl on an average, and in all cases was extremely high while
TABLE 2. BMR, Serum Cholesterol and SPBI in Patients with Simple Goitre
0 z I I I
. lsPBI I BMR ~ Name 1Age Sex
1 1
8 . ' l(y/dl)l (9(.)
1 . Y. H. ! 271
1
2 I T. 0.' 38 3 T. K. 24 4 s.u.:46 5 K. T. i 23 6 S.S.i32 7 ! H. S.: 47 8 T. K .. 22
Variation
Mean
--·-----~---
!? I 8.1 +10.11 !;2 6.7 I!+ 7.6, !;2 7.8 + 3.3: <;! 6.0 -11.7! <;! 6.5 '+ 3.9 !j1 7.2 + 9.4. !j1 7.8 +21.3 \) 7.5 1+8.9,
6.0 __: i1~7, 1 1 '
8.1 +21.3.
1.22 I +6.6]
1.44 1
2.20
Serufn-CholesterOl , (mg/dl) I
1····-=---'""-----co ' X i y ' 0 I 0 I 0 2 'I· RQ I -1i:J I v1il ,_.1i:J
I I I ro-+-1 ..+-J , V-+-1 I~ I
I 0 rn ~en I 4-1 (/) I-.........
(!)_ __ l_ica!.)l (caLli ~~ _ _:-tt:~ ~ 1.39 ~1. 0.72 1320
11199 1 I
1.57 0.90 1244 1156 170 I 85.00 I 85.00 50 1.50 1 0.88 1211 i 1172 170 : 52.501117.50 i 30 1.12 ! 0.78 100711140 232.5 11143.75 88.75' 62 1.24 'I o.72 1181 1136 195 . 85.00 ,11o.oo 144 1.41 0.97 1102 ' 1007 130 ! 40.00. 90.00 31 158 I 0.72 1520 11253 170 56.25 il13.75 33 1:33 o.72 1286 1181 187.5 . 87.50
1
1oo.oo I 47
1.12 , 0.12 10o7 1061 -l3o- ,-4o:oo : ss.-ocri 30 1 1 ' 1 ' 1 11
. 1253 232.5 '143.75 117.50 62
1~5~-~~~9.29[78.~11oo.nl4~4
TABLE 3. Serum Protein-Bound Iodine, Basal Metabolic Rate and Serum Cholesterol in Hyperthyroidism
0 z v Name rn ro
(.)
i Age Sex' SPBI I BMR
I
(y/dl) ( 0 ,;)
1 M. A.: 21 2F.S.,29 3 S. H. 24 4 S. I. 24 5 Y. S. 29 6 T. K. 22 7 N. N. 24 8 K. K. 25 9 M. N. 40
10 Y. H. ! 23
7.3 +17.0 11.7 +28.0 8.6 +38.8
13.5 +55.7 11.2 +25.7 10.7 1+43.7
9.4 +15.8 8.1 +23.4 9.4 +26.2 8.5 +31.4
(!)
1.86 2.10 2.16 2.55 ' 2.08 ' 2.30 2.15 2.10 1.90 2.21
Mean 9.84 : -'-30.6 2.14 .
COz
(!)
1.35 1.47 : 1.74. 1.48 1.50 1.32 1.44 1.48 i 1.41 1.50
1.32 !
1 1.74 '
Serum cholesterol (mg/dl)
X y 0- ---~·· ----~--
RQ H '-' 1-< -Q) a;V ~V
2~ ~~ E00 "§i ~~ ""~ ~.:g
. (cal.): (cal.] ___ -5 __ -5 __ _'B_ 0.73 1288 1101 0.70 1446 . 1128 215 0.81 1518 ' 1093 ' 140 0.57 171411101 110 0.72 1438 1146 122.5 0.57 1543 1074 0.67 1471 1270 0.70 1446 i 1172 240 0.74 . 1319 ! 1045 150 0.68 : 1516 I 1154 I 215
0.57 1288 I 1045 1 1 1
0.81 ! 1714 1270
56.25 1158.75 I 26 4s.oo I 9s.oo 132 35.00 75.00 32 20.00 1102.50 ' 16
61.25 178.75 I 26 60.00 1 90.00 i 40 63.751151.251 30
1.471 ·():69--;-147o ]1123 170.36 48.7511:1.6-~' zs.s6

308 I. AKIYAMA ET AL.
TABLE 4. Serum Protein-Bound Iodine, Basal Metabolic Rate and Serum Cholesterol in Basedow's Disease
Serum cholesterol (mgjdl)
C02 . RQ I X y I 2 I 2--1 --'-c~=2c-c-i -I, -;;;B I "'2 I i:JB! f-<
ci I I
: Name !Age Sexi SPBI · BMR ~ i I I I
u
1 K. H. 50 2 I T. I. 35 3 i M. N. 32 4 M. A. 18 5 ] T. I. 40 6 ' T. Y. 43 7 J. H. 37 8 F. K. 43 !J Y. H.· 25
Variation
Mean
...._;~ rn ~ rn +--~ rn , ----..
I
~ 0~ ~~ I (/)~ I~ IE-< o o ~ ~ o
(y/dl)_£2il'l (I) (l) (cal.) (cal.) "l'J __ _____.,=:<L___-51 16.4 I+ 78.31 2.45 1.64 0.6711678 i 941 172.S 73.75 1 98.75 42 12.3 1'+97.7 i 2.70 1.s2 o.s6 1809 1 913 112.s 23.75: 87.75 21 14.1 +81.21 3.68 1.96 0.53 ' 2455 . 1355 52.5 20.00 i 32.50 38 19.5 1+50.9 2.45 1.46 0.59 ' 1651 . 1094 75.0 23.75: 51.25 32 11.5 !+58.3, 2.55 1.58 0.6211724 1087 277.5 66.25 ,211.25 24 13.3 +79.6. 2.84 1.99 i 0.66 1940 1080 127.5 71.25 i 56.25 56 14.o '!+92.3 •
1
3 24 1.58 I' o.49 2262 1176 17s.o 6s.oo 11o.oo 37 10.7 +65.6 2.92 I 1.78 ' 0.61 1974 1192 105.0 50.00 I 55.00 48 10.5 +43.0 2.53 1.66 • 0.66 i 1728 . 1208 200.0 92.50 107.50 46
1 10.5 :.+43.0~-:Z::f5_!_1.46 . (f49-l 1651 -§l3-- 'ts.-6 ', 20.00 I 32.50! 21 l l l l l I l : l l ! l l I l
I 19.5 +97.3 3.6R . 1.99 . 0.67 ! 2455 ! 1355 I 277.5 0 92.50 211.25 56
I 13.59]+71.9 i 2.82 I 1.69 i 0.50 II 1913 I 1116 ! 144.171 54.03' 90.03 3~.22 I I I
the range of fluctuation was widest, but in individual cases the PBI in Basedow's diseases did not always indicate a higher value than in hyperthyroidism.
About the PBI in thyroid disease, Riggs and Man 28 1 stated that in hyperthyroidism it increased to 20 to 30 r /dl, but in most cases varied from 10 to 16 r %. Bernard 291 and Barker 231 reported values ranging from 8 to 35 r/dl. Hardy stated that in general thyroid toxicosis it is mostly within values ranging from 8 to 13 r/dl, and in certain marked thyrotoxic subjects it reached 16 r/dl. According to Sogen 30 > it ranges from 19 to 30 r/dl in five cases of Basedow's disease, and from 9.0 to 10.5 r I dl in five cases of incomplete Based ow's disease. Kumaoka 27 > reported that it varied from 8.4 to 20 r /dl in Basedow's disease, but in simple goitre was not so different from that in healthy persons.
(c) Patients with nePhrotic syndrome (Tables 5, 6) As shown in table 6, the PBI at first measurments after hospitalization were
2.7 r/dl (minimum), 6.4 r/dl (maximum), and 4.29 r/dl (average). In 6 cases, cases 1, 2, 3, 4, 5, 6. they were 2.7 r/dl (minimum), 4.2 r/dl (maximum) and 3.42 r I dl (average), and distinctly showed a decrease. In 3 cases, cases 7, 8, 9, they were 5.7 r/dl (minimum), 6.4 r/dl (maximum) and 6.03 r/dl (average) and were within the range seen in healthy persons. In cases No. 7 and 8, edema decreased gradually by treatment and the clinical picture of chronic nephritis with nephrosis appeared gradually, and the level of PBI showed an upper limit within normal range or a slightly increased value with the decrease in urine amount and protein. In cases No. 3 and 6, the initial low PBI level tended to return to normal with recovery of the general syndrome by treatment.
Peters et aP> stated that in two cases of nephrotic syndrome the PBI before treatment showed remarkably low values, namely 1.5 and 2.8 r /dl respectively. In 19 cases nephrosis of in Recant's 31 reports, the PBI ranged from 0.9 to 5.2 r/dl and with an average of 2.2 r/dl, figures markedly lower than our results.

THE THYROID FUNCTION IN NEPHROTIC SYNDROME 309
TABLE 5. Serum Protein-Bound Iodine, Basal Metabolic Rate and Serum Cholesterol in Patients with Nephrotic Syndrome
ci z a; Name (f) rn. (.)'
----SerUm cholesterol ___ _
I ~_ (~g/dl)_"-_ rn
y 8 8 8! s I ]B ~B I tB IE-< ~ 0~ Hf{SI~~-- li4 E-<- ~- w- ~
(y/dl)i (5'~) (I) (I) 1 (cal.) 1 (cal.), .e ~ 1 ~
COz. RQ X
~ i: ~:! i~ il u ~-~1~:~ i:~~ i i:~~ ~:~~-: i~~fl ii~g T ~~f~::~iil-i~t~l~t I: 3 s. N. 27 0 I 2 7 I' -190.6 1.52 I 1.35 0.8911078 I 1289 590 11440 150 75 * 4 z. s. 27 0 I 3.5 1.73 1.38 0.80 1214 1213 I 202.5 90 : 112.5 '140 -H-5 M. K. 21 0 4.0 ! + 9.7i 2.04 1.57 . 0.77 142511299 505 I 280 '!· 220 55 * 6 J . M. 24 0 I 4.2 I -12.3 1.66 1.08 I 0.65 11131 1289 647.5! 388 259.5 59 * 7 y. s. I' 311' " 'I 6.0 I +19.7 1.8! 1.11 I 0.61 1238 10341 240 I 50 190 I 21 + 8 T. N. 35 \i! 5.7 · -17.1 1.40 11.05 0.75 973 ' 1174 855 1338.75: 516.25 30 1tt 9 F. s. , 27 ·, " . 6.4 1 +20.o 1.98 1.06 1 o.54 1321 !no1 • 1o8o j 322.5 1757.5 13o
1 +
-- ---·-- 1---z:r- =--19.6 1.46TT.o6-fo.s4' - 973~-f634 1 -2o2.sf56--~112.s I 21 Variation I · I ! I I i I 1 I I 1 I I I : I
__ __§.!_l +20.01 2.04 1.57 I 0.99 . 1425 1299 1 1080 440 . 757.5 I 75 !
M_:_<1!1 ___ i_ 4.291-:~~81_1.!6 ~-1~~ 1_o.71 l185[l199 -544.4.264.6 1279.8 j 47.~[ __
TABLE 6. Serum Protein-Bound Iodine, Basal Metabolic Rate in Patients with Nephrotic Syndrome
Case i SPBI I Name Age Sex No. I I IY/~1)
1 T. K. 52 0 3.2 -------·· ~----
2 T. 0. 13 0 2.9
3 s. N. 27 0 2.7 3.2
4 z. s. 27 0 3.5 ·----------------------
5 M. K. 21 0 I
-----
6 J. M. 24 0
7 i
Y. s. 31 " -------------------------
8 I T. N. 35
. -------- ------ ----
9 F. s. 27
(2) Basal metabolic rate (BMR) (a) Healthy person (Table 1)
" \'
4.0
4.2 5.7 5.5
6.0 ·I-
5.7
I 8.4 8.6
6.4 7.5
BMR
(Jo') --------
-13.0
+ 5.4
-19.6 -20.2
0
+ 9.7
-12.3 - 6.3
+19.7
-17.1 +15.2 +22.7
+20.0 +21.9
Several investigators have reported on the range of BMR of healthy persons, as follows: ±15°.:;' (Du Bois 121 and Barker 231 ); ±10"0.:;' (Selye 31 1); -10-+16%,

310 I. AKIYAMA ET AL.
and +4% (average) by Bartel,32 l with -26- +9%, -9.% on an average after the injection of 1 g pentothal. In many other reports almost similar values have been obtained and our results of -9.8 to +14.6%, and +3.3.?;;' (average), agree with values reported by many investigators.
(b) Patients with thyroid diseases (Tables 2, 3, 4) Matsuura 5 l considered thyroid diseases with BMR of more than +205'£ as
hyperfunction of the thyroid gland. Du Bois 12l considered a patient with BMR of from +15 to +30% as a light case, from +30 to +50% as a moderate case, from +50 to +75% as a serious case and over +75% as a dangerous case. But in simple goitre the mean was +6.6%, ranging from -11.7 to +21.35'£, and the BMR Oz consumption (Oz), C02 production (COz), respiratory quotient (RQ), daily basal metabolic calorie (X) and standard metabolic calorie (Y) were almost no different from the normal. In hyperthyroidism BMR, varied from +17 to +55.7%, with +30.6% (average) and was almost +30 to +40% in many cases. In contrast with the normal RQ did not differ much, but X increased.
In Basedow's disease the BMR varied from + 43 to + 97.7%, with + 71.9% as average, and varied nearly from +50 to +80% in many cases, but there were no cases with a value of over +1005'.;;'. Both Oz and COz in this disease increased clearly in contrast with hyperthyroidism, and because of the striking increase of Oz, RQ became low, X indicated a high value and Y rather lower than normal.
(c) Patients with nephrotic syndrome (Table 5) In patients with nephrotic syndrome, the mean BMR, showed slightly low
values, and was -0.85';;' (Range, -19.6 to +20.05'C) and -15.5.% (Range, -19.6 to -12.3%) in four cases (cases 1, 3, 6, 8) with particularly marked edema, representing an obviously low value. Gradwohl 33 > reported that BMR was always below -20% in most cases of myxedema, whereas nephritis did not show such low values. In Duncan's 34 l report, the drop of BMR which has no relation with thyroid function was about -20% at a minimum, and Epstein 35 > noted the BMR to vary from -8 to -185'£ below normal.
(3) Serum cholesterol (a) Healthy person (Table 7) Serum total cholesterol of healthy persons is extremely variable, depending
upon the method of its determination or individual case. Peters 36 > and Van Slyke stated the serum total cholesterol to vary from 320 to 107 mg/dl, averaging 194 mg/dl. We found it to be 161.4 mg/dl on an average and to vary from 125 to 240 mg/dl, which was almost equal to that ranging from 130 to 200 mg/dl reported by Ball and Evans.37 l
(b) Patients with thyroid disease (Tables 2, 3, 4) In thyroid disease, especially in simple goitre and hyperthyroidism, serum
total cholesterol was slightly elevated as compared with normal adults in most ·Cases, but in Basedow's disease it decreased extremely in some cases. The ratio of free to total cholesterol was over 30 in most thyroid diseases.

THE THYROID FUNCTION IN NEPHROTIC SYNDROME
TABLE 7. Serum Cholesterol in Normal Adult
Case No.
'
Name
~----
1 M. 0. 2 A. G. 3 Y. 0. 4 K. S. 5 S. N. 6 E. Y. 7 I. A. 8 K. T. 9 S. A.
Variation
Mean
Total cholesterol
(ll_l~/d!)
15o I
172.5 152.5 125 240 135 155 167.5 155
125-240
161.4
Free cholesterol
( !llgJdl)
50 58.75 35 35 82.5 40 36.25 52.5 60
35-82.5
50
(c) Patients with nephrotic syndrome (Table 5)
Cholesterin I
ester .1
F/T (mgjd!)
f~~~:-1 ~ 117.5 II 23
90 28 157.5 34
95 I 30 118.25 I 23 115 31 95 38
90-157.5
111.4
23-38
30.3
311
In patients with nephrotic syndrome, serum total and free cholesterols were both elevated and their averages were respectively 544.4 mgm% and 264.6 mgm%. In 5 cases out of 9, serum total cholesterol was more than 500 mg/dl, and in one case it indicated a value more than 1000 mg/dl. Stepp 33 > observed a high total cholesterol level of over 1 000 mgm% in lipoid nephrosis and below 1 500 mgm ?& in glomerulonephritis with nephrosis.
(4) Plasma protein fraction (a) Healthy adults (Table 8)
TABLE 8. Plasma Protein Fraction in Healthy Persons
Case I i TP I A il G I A+,. I Globulin (gjdl) F
No. Name (g/dlil(gjdl) (g/dli[(g/d!)! ~; !~ ,-;- (g/dl): ~~~-~/A_ r/G
1 1. I. T. ' 85.4 : 4.761 2.981 5.471 0.71 . 0.99 : 1.28 0.80 1.60 I 0.27 0.43 2 K. T. 8.27 I 4.44 ' 3.16 5.21 0.77 1.03 . 1.36 : 0.67 1.41 0.31 0.43 3 , Y. Y. 8.94 4.70 I 3.58 i 5.49 0.79 1.23 1.56 0.66 1.31 0.33 0.44 4 K. y. 8.27 4.28 : 3.49 ~ 4.88 0.60 1.10 : 1.79 I 0.50 1.23 i 0.42 0.51 5 s. M. 8.40 4.76 3.13 I' 5.42 0.66 0.92 i 1.55 • 0.51 1.52 : 0.33 0.50 6 G. F. 9.20 5.31 3.39 6.01 0.70 1.20 1.49 i 0.50 1.56 I 0.28 0.44 7 A. s. 8.34 4.86 ' 2.96 I' 5.45 0.59 0.79 1.58 ' 0.52 1.64 I 0.34 0.53 8 Z. S. 7.95 4.67 2.64 5.20 0.53 0.84 ' 1.27 I 0.64 1.76 0.27 0.48 9 M. A. 8.74 4.75 3.37 . 5.46 0.71 1.09 1.57 I 0.62 1.41 0.33 0.47
10 s. y. 9.01 4.59 3.78 5.42 0.83 1.38 1.57 i 0.64 . 1.21 0.34 0.42 11 H. M. 8.27 4.08 3.58 4.87 0.79 1.22 1.57 : 0.61 I 1.15 0.38 0.44 12 K. S. 8.87 4.78 3.31 5.61 0.83 1.22 1.26 0.78 I 1 44 0.26 0.38 13 E. Y. 8.20 4.10 3.46 4.83 I 0.73 1.00 i 1.73 0.6411.18 0.42 0.50 14 y. M. 7.61 4.25 2.75 4.92 0.67 .I 0.89 : 1.19 0.61 1.54 0.28 0.43 15 T. y. 8.21 4.61 2.99 5.12 0.51 0.86 i 1.62 0.61 I 1.54 0.35 0.54
Variation 4.08- ~2~414:s:r .o:57-p.79 11.19 -6:50--1.15 10.26 6:38---9.20 -5.31 1 -3.78• -6.01' -0.83 -1.38: -1.79 -0.80 -1.761-0.42 -0.54
·- ------ --~-----1 ----··· . --- --,------
Mean 8.45 : 4.60 3.24 5.29 0.69 1.05 1.50 0.61 1.42 0.33 0.49

312 I. AKIYAMA ET AL.
(b) Patients with thyroid disease (Tables 9, 10, 11)
In thyroid disease total protein increased in most cases, but there were no distinct differences for each thyroid disease. In hyperthyroidism and Basedow's
disease total protein showed a tendency to increase slightly in comparison with simple goitre.
In each type of thyroid disease, albumin was reduced in almost all cases and decreased fairly much in a very few cases, but we could not find a special difference between the three thyroid disease.
Plasma globulin was increased in almost all cases of the three thyroid dis· eases, and especially a-globulin and r-globulin were increased considerably in many cases, while p-globulin and fibrinogen were increased slightly in many
cases. But in simple goitre, compared with the other thyroid diseases, there were many cases in which a-globulin indicated a slightly tendency to decrease
and r-globulin a tendency to increase. Therefore in all thyroid diseases, the
ratio of albumin to globulin was low, the ratio r/ A high and the ratio r/G low in a few cases, while albumin+ a-globulin decreased in almost all cases. Saito et al.391 found decrease of albumin, increase of globulin, especially of p-globulin and r-globulin, and fall in the ratio of albumin to globulin, while in many cases a-globulin and fibrinogen were relatively increased. Shirer determined the total protein, albumin and globulin (Euglobulin, Pseudoglobulin I, II) in hyper
thyroidism and found marked decrease of albumin and increase of globulin, especially of euglobulin and pseudoglobulin I. Lewis 401 reported that in hyperthyroidism there is decrease of albumin, but did not find a constant change in globulin.
TABLE 9. Plasma Protein Fraction in Patients with Simple Goitre
Nome I Agel Sexi ( ;~:! 1
,;dll 1 ,;dli :::J. ~~~:J/:1~, ; ( g~dli; A/G I d A YjG
-l--T-.-K-. -:-3s-- \l 7.72 i. 3.93 -3.o3 4.69-~~o~~~·'i'6_ T511 0.76 T 1.31- o:38 I
24 "'_1-7:82_1 3_.o_9_• _4.1_8_1~.()() 1 o!1_1_._o9 __ 2_.18_·_o_.s_s _! 0.74 0.70 I o.s2
0.50
2 T. K.
3
4 I
Y. u. I 46 I '? ! 8.32 I 3.25 I 4.:-5 4.16 I 0.9111.08: 2.36 I 0.72 0.75 - 0.721 0.54
F. T. 23--1 -'?- 9.97 - 4.23 4.75 5.23 ' 1.00 1.50! 2.24: 1.00 I 0.89 0.53 0.47
5 I H. s. 47
~ l-;~ 32
Variation
Mean
\l 1 -8.831
17.67 I
12 9.9o I
I -7-:67 l
9.97
8.60
1.83 5.64 2.58 0.75 1.83 i 3.061 1.36
3.19 . 3.84 'I -3~7- -Q4811.-6o-l 1.76 i o.64 I
4.78 1
3.92 , 5.46 o.68. o.681 2.56 i 1.20 1
1.83 ~-3.03----:z.58- 0,48110,68 I 1.5tT. o
1· .. ,35651
l l l ! l l l : ' 4.78 5.64 5.46 I 1.00. 1.83 3.06 I
3.47 4.24 1 4.25 o.78: 1.22 2.24 o.89
0.33 1.67
o.83 I o.55 1.22 ! 0.54
0.54
0.46 0.65
0.33 0.38 1 0.46 1 1 1 1
1.31 i 1.67 0.65
0.87 0.72 I 0.53

THE THYROID FUNCTION IN NEPHROTIC SYNDROME 313~
TABLE 10. Plasma Protein Fraction in Hyperthyroidism
i r· ----~-- Globulin - I
~~ Name AgeiSex TP A G 'j A+IX _ _IMcll_l____ F A/G, y/A
() ' I (g/dl) (gjdl)(gjdl)(gjdl) IX I (3 I y l(g/d!) I
YjG
1 M.A. 1J2G~-~-,I-S.94!-3~9]_- 4.29 i 5.03IL12 1.12 1 2~05 0.74 I 0.91 ___ _ ' ! I I 0.52 I
0.48 - ---~--~--------I
2- ~~~~- Q- '_~:~~ ~:~~ I
4.27 i 3.93 1.03 I 3.29 : 5.02 0.69
I
0.68 I 0.71 I' 0.48 1.32 I 0.48 I 0.63
4 H. S. 29
4.15 I 4.94 0.97 1
3.69 4.81 1.12 . ---
3.581 5.131 0.78 3.69 4.81 1.12
] .00 i 0.40 ' 0.40 1.00 ! 0.39 ; 0.39
o.89 1.22 1, o.44
1.12 i 1.00 0.39 0.53 0.39
5 N.N.j241 Q ! 9.70
! 10.20
3.31 5.32 4.38 i 1.07.
---;-K. K.j251 Q 8.28
I
7 M. N. 140 Q 7.98 3.48 1
8.23 3.14 1
9
Variation
Mean
I
7.94 3.441 8.81 4.01
I 7.1941
2.116
10.20. 5.22
8.66 . 3.66 '
3.751' 3.66
3.29 1
I I
5.32 :
4.03
4.38 '1
o.94[ o.75. 2.o6, o.75 4.79 I 0.7811.05 1.831 1.14 :
2.83 .. 0.65 0.52 I 1.451' 0.40 I
I ' I I , 1.591 3.07' _1}_5 i
0.93 1 0.59 I o.55 1.10 ' 0.46 0.50
6.49 0.39 0.39 I I I
1.33 0.93 1.001
2.00 0.97 ' 0.93 0.54 0.53
TABLE 11. Plasma Protein Fraction in Basedow's Disease
- i i 1 1 Globulin I , j~ Name Age Sex TP I A j G I A+" :--~g/dl)___ F A/G I Y/A [ yjG
I (g;'dl)l(g/dl)l(gjdl) (g/dl) IX ! {3 I y lig/dl I I
1 , F. K. 1 27 · ; 9.44 : 4.30 4.03r;~22 1
-0.921
1.Z8 iBii 1.11 1
1~o;,-1 -o.~31 0.45-
2 Y. }LI~_' Q I ~:~~ I t~~~-g~ I ~:~~ I ~:~~I t~~ i ~:ig_: -- --~ I g:~~ 3 I T y ! 43 i Q i 7.94 ! 3.09 3.88 4.06 I 0.97 1.161. 1.751 0.56 ; 0.45
• • i I 8.53 . 3.79 3.48 4.75 . 0.96 1.26 . 1.26 I 0.33 0.36
--<--J. ~- , ;;T ~T ~:~~ ,- ~:~~ g~ -g:~~ , i:~~ 6:~~ g:~~ -5~-K.-.l:~ Q 8.38 3.03 , 4.39 1 -4.09 0.96 -1.142:29 o.96-o.70 J 0.75 0.52
6 r. Y. 1 -1sl Q 9.27 3.3o --5.47-,--4.30 [1.oo: 1.33j3.14 o.5o I 0.61-, o.95 o.58
7_; T. r_._l4o :i_i 10.07 I_ 3.041 5:26_j_4:16[l.l2J2.o7[-2.o71 1.771 o.58-,o.68j 0.39
8! H. M. I 571 Q I 8.42 i 3.97 . -3:71, 4.22 i 0.25 r 1.7SI1~73 :o~i4 1~o7-!0.44! 0.47
9 F. K. 431 Q 1 7:z9 ,-3.6113.08 -, 3.99 -,0.38 'I o.6oT2.J.o·-o:60:-u7-10:58 o.68 i ' I I I !
lo[ Y. H.~~-Q- 8.63 iml 4.36 I 4.35 . 1.20--I-:05 2.11 ~- 0.72J 0.67 0.48
7.29 3.03 2.73 3.99 0.25 0.60 I 0.97 . 0.43 0.58 I 0.121 I 0.35 Variation I I I I ! I I I i I I I
10.07 4.51 5.47 ! . ' I 1.65 0.95 0.68 ~~1.?_~-2.07 _ 3.14 ! __ l._Z?_
----
Mean 8.70 3.63 i 4.13 ' 4.49 0.86! 1.30 !
1.97 I 0.951 0.93 0.56 i 0.47 ----------

314 I. AKIYAMA ET AL.
(c) Patients with nephrotic syndrome (Table 12)
In nephrosis and chronic nephritis with nephrosis, total protein and albumin decreased distinctly. Globulin, especially a-globulin increased in all cases, and 11-globulin and fibrinogen both increased in almost all cases, but r-globulin decreased distinctly. So the ratio of albumin to globulin was low, the ratio of rglobulin to albumin high, the ratio of r-globulin to globulin low, and albumin + a-globulin decreased considerably in all cases too.
Regarding the plasma protein fraction in nephrosis, Longsworth 411 reported marked decrease of albumin and distinct increase of a-globulin and $-globulin. Luether 421 found an obvious increase in a-globulin, $-globulin and fibrinogen and decrease in r-globulin. Malmros and Blix 431 reported increase of fibrinogen and a-globulin, normal or relative increase of )9-globulin, while r-globulin value lay at the lower limit of normal or below it. Further, Yamada,411 Miyoshi, 151 Hirai/61
Shimao and Narukawa in Japan reported on the marked decrease of total proteins and albumin, remarkable increase of a-globulin, j3-globulin and fibri
nogen, and decrease of r-globulin.
TABLE 12. Plasma Protein Fraction in Patients with Nephrotic Syndrome ----- ----- ---------------------
~ -
; I j I 1 Globulin [ 1 : I ~ 0 Name Agel Sex TP I A G i A+" - (g/dl) . I F 1
1' A/G I y/A yjG
uZ ; lrg/dl) (g/dll 1(g/d!)l(g/dll " 13 Y <g/dll .J -~----1 I c. K. i 52 ! 0 I 5.24 1.59 2:72~---2.45 !-0.86 -0.93 0.93[ 0.93 . 0.59 i 0.58 0.34
2 I M. 0. 131 o -6.63~1.30~-3:71.- 2~41 J.67 0.54 0.71 0.29 i 0.41 0.12
6.78 o.82 11 4.47 : 2.31 1.49 1.99 o0._9699 1 01_.6493--~-o0 .. 2196 1
1
1.20 0.22 3 S. N. 27 0 6.14 1.13 4.38 1 2.44 1.31 2.38 0.61 0.16
6.28 o.95 1 3.87 i 2.56 1.61 o. 73 1.53 ! 1.46 1 o.zs i 1.61 0.40
4
5
I
z. s. 27 I 0 I
M. K. 21 o
5.23 : 5.63 6.08 I
6.14
7.24
1.41 : 1.45 1.57 1.50
1.73
2.85 I 2.49 1.08 1.24 0.53 I 0.97 0.38 2.98 . 2.90 1.45 0.68 0.83 i 1.20 0.59 3.44 2.85 1.28 1.28 0.88 i 1.07 0.56 3.48 2.89 1.39 1.16 0.93 . 1.16 0.62 '
0.19 0.28 0.26 0.27
3.88 ! 3.46 11.731 1.32 0.83 1.63 0.45 0.47 0.21 ~------- I , ~~~~~~
6 1 24 0 6.44 1.43 4.66 4.17 2.74 • 1.081 0.84 o.35 ! 0.31 o.s8 o.18 I J. M. 6.16 1.62 3.35 3.13 . 1.51 i 1.19 0.65 1.19 0.48 : 0.40 0.19
-7-~-~~-~-135 1
1 9 , ~:~~ tg~ . u~ . i:~~~[1l~-is~ 1 ~:~~ i u~ 8:~~ g:~fi g:~~
I 8.78 2.50 4.33 3.60 I 1.10 I 2.01 1.221 1.95 0.58 0.49 : 0.28 ---+--------7-------sj_:"_-__S. • 27 9 I 8.16 ; 1.40 5.29 2.80 11.40 i 2.6211.27 1.47 o.27 o.91 o.24
9 Y. s. 31 1 9 , 8~18 3.40 3.77 1 4.41 . l.o1~0.Ssl1.88 1.01 o.88 o.7o o.18
5.23 -0~82 2.72 2.3i 0~86'-0)3 6.65-(f35 ()jg 0.38 6:12-Variation I I I I I ! I I I I I I
8.78 3.40 4.66 4.41 2.74: 2.62 1.88 1.95 0.88 1.61 0.40 ---------------------- ---
Mean 6.61 1.54 3.91 3.07 1.53 1.41 0.97 1.16 . 0.41 0.69 . 0.23

THE THYROID FUNCTION IN NEPHROTIC SYNDROME 315
DISCUSSION
The range of fluctuation and average values of PBI, BMR serum cholesterol and plasma protein fractions in healthy adults and in various types of thyroid disease have already been reported.
In nephrotic syndrome, PBI decreased notably in many cases and remained within normal range in a few cases. In cases in which the clinical syndrome took a turn for the better by treatment, the PBI level attained the upper limit of normal or tended to be higher than the normal concentration. The mean BMR was -0.8.%' (from -19.6 to +20.6%) and almost the same as in a healthy adult, but in cases with distinguished ascites it was -15.5~'.; (from -19.6 to -12.3 ?0 ), indicating an extreme drop.
In serum cholesterol, the mean total and free cholesterols were 544.4 mg/dl and 264.6 mg/dl respectively, showing a marked increase.
Further, in the plasma protein fraction, total protein and albumin were decreased in all cases, and globulin, especially a-globulin increased in all cases, and jj-globulin and fibrinogen in almost all cases.
On the relation between PBI and BMR, Salter,'1' 1 Curtis and Swenson,43 '
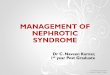
Riggs 1' 1 etc. stated that the PBI was a better index of thyroid function than the BMR alone. Silver and Tyson,191 Perkin and Hurxthal 501 found no correlation between the PSI and BMR. Dodds and his associates stated that in the main a high BMR was associated with a high PSI, but there was no quantitative relation seen between the two. Regarding the relation between the two, Bulman 511 found empirically the best equation describing the relationship to be : 0~ BMR- 29 =log (r ?0 iodine), and Salter 521 demonstrated a significant correlation to exist by using a logarithmic relationship: BMR =log (blood iodine -3). According to my results, as shown in fig. 1, PBI changed generally together with BMR, but in certain cases did not indicate a parallel relation.
Considering the serum cholesterol and PBI in Basedow's 531 disease, serum cholesterol indicated mostly a descending tendency, being in reciprocal relationship to the increase of PBI, but in other thyroid diseases it did not always decrease. In nephrotic syndrome a high cholesterol and a low PBI were found in many cases. The fact that changes in each serum cholesterol fraction were not proportional to those of PBI was considered to show that serum cholesterol had no direct relation to PBI. Therefore, as Hurxthal 541 551 has already pointed out, it seems difficult to estimate thyroid deficiency from the serum cholesterol level.
Next, we found that hypercholesterolemia in nephrotic syndrome 56 1 was induced by various conditions such as: 1) The phenomenon to compensate for the fall in osmotic pressure induced by hypoproteinemia. 2) The disturbances from removal of cholesterol from the blood stream. 3) The excessive mobilization of deposit fat. 4) The hypofunction of the reticuloendotherial system.
There are many reports on the iodine metabolism in renal dysfunction. Schlayer and Takayasu 5' 1 performed an experiment to see from which of the glomerule and tubule iodine was excreted, by impairing separately the blood vessel and the tubule in rabbit kidney with various toxins, and arrived at the conclusion that iodine was excreted from the tubule, because iodine excretion

316
100
ci 80
'i 70
::D 60
50
4-0
20
10
0
-10
-20
0
0
Oo
oo . .. 0 ...
.. ... 0
0 . 0
I. AKIYAMA ET AL.
• Ncnmal Adults . Thyc oid d ioeases • • Bw:.edows' disease
• o Nephrotic syndrome
• • • •
• . • .. .
. . . 0 •• 0
-. .
I I I I I I I I I I I I I I I I I I I I I
- 30o 2 o 4 5 G '7 s s 10 11 12 10 t4 t5 16 1'7 13 19 eo 21 P.B.I. %t.
FIG. 1. Relation between PBI and BMR.
was distinctly disturbed by an injury to the tubule but not by impairment of the glomerule. From clinical investigation Monakow 581 supported this hypothesis and Leschke 591 stated that glomerule had no relation with iodine excretion. But Frey reported that iodine was excreted not only from the tubule but also from the glomerule, and Potter and Bell, Ito 601 etc. confirmed this. Kobayashi 611
stated that in acute nephritis, blood iodine increased only in serious cases, and in mild and improved cases remarkable changes were not noticed, but was increased often in chronic nephritis and nephrosclerosis and decreased or tended to decrease in nephrosis. In addition he reported the high blood iodine value in experimental rabbit nephritis caused by various toxins. Baldauf et al.621
reported the extremely high value of blood iodine in two juvenile nephritis. On the other hand Turner et al.631 and Curtis et al.641 stated that whole blood iodine in non-insufficient renal diseases was generally low or normal as is seen in hypothyroidism. As above·mentioned, it is not yet clear whether the iodine excretion is related to the glomerule or the tubule in renal disturbance, but it is likely that whole blood iodine in nephrosis decreases or indicates a value near normal. However, reports on PBI in renal dysfunction are extremely few, Peters et aZ.Z1 and Recant 31 determined the PBI in nephrosis, and found a low value in hypoproteinemia, especially by hypoalbuminemia. Moreover they thought that its low value could not be explained only by the urinary PEL Peters et al.631 stated that in hypoprotein diseases such as cirrhosis of the liver, the PBI showed always a low value, having no parallel relation to the degree of protein deficiency, and except for the low BMR and hypercholesterolemia none indicated the symptom of hypothyroidism.

THE THYROID FUNCTION IN NEPHROTIC SYNDROME 317
Recant et al.31 reported that in certain patients with nephrosis, the thyroid gland may be elevated slightly in function in order to compensate for the continuous excretion of thyroid hormone into the urine. Though the exact nature of the protein-bound 661 671681691 iodine has not been determined at present, it is generally believed that PBI may be thyroxine or a thyroxine-like substance.
By filter paper partition chromatography with the use of radioactive iodine (!131) in rats, Laidlaw et al.70 1 obtained results where a large portion of plasma iodine existed in the form of thyroxine and the circulating thyroid hormone was truely thyroxine, and not thyroglobulin or a thyroxine-containing peptide. By the same method Taurog et al.711 supported the view that plasma iodine is thyroxine and diiodotyrosine, and that organic iodine in plasma appeared to be identical with thyroxine. Gross'21 found that in the plasma, practically all the butanol-extractable radioactivity was present as thyroxine, with a very small amount of diiodotyrosine and iodide. In hyperthyroidism Rosenberg'31 did not detect, monoiodotyrosine, diiodotyrosine and acetylthyroxine as constituents of the plasma PBI, and stated that the circulating thyroid hormone in Graves' disease was thyroxine. Separating the PBI into thyroxine and nonthyroxine, DanowskF11751761 stated that thyroxine was about eighty or ninety per cent plasma PBL Taurog and Chaikoff"1 carried out iodine analyses on the plasma protein fractions and stated that albumin, a-globulin, and j3-globulin were capable of binding thyroxine to a high degree, and r-globulin much less potent as a thyroxine binder, and consequently iodine was considered to bind with the smaller protein molecules in plasma.
Further they reported that the a-globulin fraction had the highest concentration of iodine, r-globulin the lowest, and albumin the largest carrier of plasma iodine, as g/dl of albumin in plasma was greater than in the others, but they could not plasma iodine only by a single plasma protein fraction.
By filter paper electrophoresis and standard electrophoresis Larson et al. 751 reported that a small abnormal peak of protein-bound radioactive iodine was seen just beyond the a-2 area, especially in the ascending limb. Deis et al.79 1
studied the nature of the circulating thyroid hormone in euthyroid and hyperthyroid subjects using paper electrophoresis, and P 31 as a trace isotope. According to their reports, radioactivity is localized in two major zones, one in the most slowly moving albumin and the other in a zone of low protein concentration just ahead of a-2 globulin, after twenty-four hours. Soon after the administration of 1131, most of the radioactivity was associated with the albumin fraction, but in the hyperthyroid individual there was a rapid shift to the alpha region. A similar though considerably slower shift occurred in the euthyroid ·subject.
Present evidence indicates that the hormonal iodine is carried by the a-globulin fraction. The tracer iodine became concentrated faster, attained higher levels, and declined more rapidly at this site in the hyperthyroid than in the euthyroid subjects.
Considering the reports of investigators above-mentioned, PBI is subnormal in nephrotic syndrome and this low value is perhaps due to hypoproteinemia, namely, to the remarkable decrease of albumin (hypoalbuminemia) carrying

318 I. AKIYAMA ET AL.
the circulating thyroid hormone, but as the a-globulin having the highest concentration of iodine seems to play an important role in this respect, the low PBI in nephrotic syndrome appears to have a relation with the decrease of albumin + a-globulin rather than with albumin.
Experimentally a low PBI in nephrotic syndrome is found in cases in which the decrease of plasma albumin or albumin+ a-globulin is marked, but the low PBI value is not always in proportion to the low plasma albumin or albumin + a-globulin.
In hyperthyroidism increase of plasma albumin or albumin+ a-globulin is not found, in spite of the markedly high PBI value. In hypothyroidism Lewis 80 )
reported low plasma albumin, low a-globulin, and high 8-globulin, while Gildea 811
found hyperproteinemia to be an aid in diagnosis when whole plasma protein was over 7.7 g/dl.
From the above-mentioned facts, it is believed that the plasma PBI value does not change according to the variations in plasma protein fraction, namely albumin or albumin+ a-globulin. Therefore, we cannot deny the view that the low PBI value in nephrotic syndrome will have relations not only with the decrease of albumin or albumin+ a-globulin, but also with the thyroid function, especially with its lowering.
CONCLUSIONS
1) In nephrotic syndrome, serum protein-bound iodine decreased in almost all cases, and BMR dropped clearly in cases with marked edema, but the rate of drop did not always run parallel with the decrease of protein-bound iodine.
2) Hyperthyroid conditions tended to diminish the level of the blood cholesterol, and nephrotic syndrome was accompanied by a markedly elevated blood cholesterol. However, the degree of rise and fall did not always bear a reciprocal relationship with that of PBI.
3) The low protein-bound iodine in nephrotic syndrome showed a relationship with albumin or albumin+ a-globulin regarded as the normal vehicle for thyroid hormone, but we could not always find a correlation between the two.
4) From the facts that in hyperthyroidism with high protein-bound iodine, albumin or albumin+ a-globulin decreased in many cases, and the low proteinbound iodine seen in nephrotic syndrome was not always proportionate to the decrease in albumin or albumin+ a-globulin, it is considered that the proteinbound iodine does not hold a parallel relationship to plasma albumin or albumin+ a-globulin fraction. Hence, it is believed that the low protein-bound iodine in nephrotic syndrome is not only due to the hypoproteinemia induced by marked decrease in albumin or albumin+ a-globulin fraction, but also may have some relationship with hypothyroidism.
(A part of this report was published in No. 3, Vol. 43 of Journal of Japanese Society of Internal Medicine.)

THE THYROID FUNCTION IN NEPHROTIC SYNDROME
REFERENCES
1. EPSTEIN, A. A. Am.]. med. Sci. 154: 638, 1917; 163: 167, 1922. ·2. PETERS, ]. P. AND E. B. MAN. ]. clin. Invest. 27: 397, 1948. 3. RECANT, L. AND S. R. RIGGS. ]. clin. Invest. 31: 789, 1952.
319
4. TSUNOI, K. Thyroid Diseases and its Treatment. Tokyo: lgakushoin, 1950 (Japanese). 5. MATSUURA, S. Archive of Endocrinology. Kyoto: Nagaishoten, 1950 (Japanese). 6. MAR UTA, S. The Japanese journal of Endocrinology. 29 : 91, 1953 (Japanese). 7. KUMAOKA, S. The journal of japanese Society of Internal Med. 42: 244, 1953 (Japa
nese). 8. BARKER, S. B., M. ]. HUMPHREY AND M. H. SOLEY. ]. clin. Invest. 30: 55, 1951. 9. BARKER, S. B. AND M. ]. HUMPHREY. ]. Clin. Endocrinol. 10: 1136, 1950.
10. HARDY, ]. D. AND C. RIEGEL. Am.]. med. Sci. 221: 359, 1951. 11. ONO, M. Examination of respiratory function, p. 21. Tokyo: Igakushoin, 1953 (Japa
nese). 12. KANA!, I. AND T. SUGITA. The Method of clinical examination, 8th Ed., p. 325. Tokyo:
Kaneharashoten, 1949 (Japanese). 13. SPERRY, W. M. AND M. WELFF. ]. biol. Chern. 187: 1, 97, 1950. 14. HIRAI, H. AND K. SHIMAO. Seikagaku 21: 54, 1949 (Japanese). 15. HIRAI, H. AND K. SH!MAO. Yakurigaku 3: 141, 1949 (Japanese). 16. BASSETT, A. M., A. H. COONS AND W. T. SALTER. Am.]. med. Sci. 202: 516, 1941. 17. RIGGS, D. S. cf. 18. 18. RAPPORT, R. L. AND G. M. CURTIS. ]. Clin. Endocdnol. 10: 753, 1950. 19. CONNOR, A. C., R. E. SWENSON, C. W. PARK, E. C. GANGLOFF, R. LIEBERMAN AND
G. M. CuRTIS. Surgery 25: 510, 1949. 20. CONNOR, A. C., G. M. CURTIS AND R. E. SWENSON. ]. Clin. Endocrinol. 9: 1185, 1949 . . 21. DANOWSKI, T. S., S. HEDENBURG AND G. H. GREENMAN. ]. Clin. Endocrinol. 9: 768,
1949. 22. HEINEMAN, M. ET AL. ]. clin. Invest. 27: 91, 1948. '23. BARKER. S. B. Progress in clinical Endocn'nology, p. 61. New York: Grune and Stra-
tion, 1950. '24. HARSHA, W. N. Am. ]. med. Sci. 221: 626, 1951. 25. HARDY, ]. D. AND C. RIEGEL. Am.]. med. Sci. 221: 359, 1951. '26. SOGEN, A. ]. ]ap. Soc. Int. Med. 41: 187, 1952 (Japanese). 27. KUMAOKA, S. ]. ]ap. Soc. Int. Med. 41: 654, 1952 (Japanese). '28. RIGGS, D. S .. E. B. MAN AND ]. H. MEANS. Thyroid and its Diseases, 2nd Ed., p. 165.
Philadelphia: Lippincott Co., 1948. '29. HALLMAN, B. L., P. K. BONDY AND M. A. HAGEWOOD. Arch. int. Med. 87: 817, 1951. 30. SOGEN, A. ]. ]ap. Soc. Int. Med. 41: 482, 1952 (Japanese). 31. SEL YE, H. Text book of clinal Endocrinology, 2nd Ed., p. 700. Canada: Acta Inc., 1947. 32. BARTELS, E. C. ]. Clin. Endocrinol. 10 : 1126, 1950 . .33. GRADWOHL, R. B. H. Clinical LaboraiOJy Methods and Diagnosis, Vol. 2, p. 2198. St.
Lovis : Mosby Co., 1948. 34. DUNCAN, G. G. Diseases of metabolism, 2nd Ed., p. 2198. Philadelphia and London:
W. B. Saunders Co., 1947. 35. EPSTEIN, A. A. ]. Am. med. Ass. 87 : 913, 1926 . .36. YOSHIKAWA, H. Rinshoikagaku (Rinshohen). Tokyo: Kyodoishoshupansha, 1949 • .37. BALL, W. G. AND G. EVANS. Diseases of the kidney, p. 203. London: J. and A. Churghill,
1932. :38. VOLHARD, F. AND E. BECHER. Die klinischen Methoden der Nierenfunktions priifung,
p. 128. Berlin und Wien: Urban and Schwarzenberg, 1929.

320 I. AKIYAMA ET AL.
39. SAITO, Y., H. ICHIJI, AND M. SEKI. jap.]. of Endocrinol. 28: 138, 1952 (Japanese).
40. LEWIS, L. A. AND E. P. McCULLAGH. Am. ]. med. Sci. 208: 727, 1944.
41. LONGSWORTH, L. G., T. SHEDLOWSKY AND D. A. MACINNES. cf. A. Gutmau: Advances· in protein chemistry. Vol. 4 Plasma proteins in Disease, p. 180. New York: Academic press inc., 1950.
42. LUETSCHER, ]. A. cf. A. Gutman: Advances in protein chemistry. Vol. 4 Plasma protein in Disease, p. 180. New York: Academic press inc., 1950.
43. MALMROS, H. AND G. BLIX. cf. A. Gutman: Advances in protein chemistry. Vol. 4· Plasma protein in Disease, p. 180. New York: Academic press inc., 1950.
44. YAMADA, E. ]. fap. Soc. Int. Med. 42: 388, 1953 (Japanese).
45. MIYOSHI, K. Rinslzo 5: 729, 1952 (Japanese).
46. HIRAI, H. AND K. SHIMAO. Seikagaku 21: 109, 1949 (Japanese).
47. SALTER, W. T., A. M. BASSETT AND T. S. SAPPINGTON. cf. 66.
48. CURTIS, M. G. AND R. E. SWENSON. cf. 66.
49. SILVER, S. AND M. C. TYSON. cf. 66.
50. PERKIN, H. G. AND L. M. HURXTHAL. ]. clin. Invest. 18: 733, 1939.
51. BULMAN, G. cf. 66.
52. SALTER, W. T. cf. 66.
53. PETERS, P. AND E. B. MAN. ]. clin. Invest. 29: 1-11, 1950.
54. HURXTHAL, L. M. Arch. in!. Med. 52: 86, 1933.
55. HURXTHAL, L. M. Arch. int. Med. 53 : 762, 1934.
56. OSHIMA, K. Rinsho ]inzo Byogaku. Tokyo: Igakushoin, 1948 (Japanese).
57. SCHLAYER, D. AND R. TAKAY ASU. Dtsch. Arch. Klin. Med. 98: 17, 1912.
58. MoNAKOW, P. V. Dtsch. Arch. Klin. Med. 102: 248, 1911.
59. LESCHKE, E. Z. klin. Med. 81: 14, 1915.
60. ITO, S. fap. Soc. Pharma. 22: 1, 1936 (Japanese).
61. KOBAYASHI, S. Kyotofuritsu ]. med. Sci. 37: 609, 1943 (Japanese).
62. BALDAUF, L. K. AND L. PINCUSSEN. Klin. Wschr. 9: 1505, 1930.
63. TURNER, K. B., A. DE LAMATER AND W. D. PROVINCE. ]. clin. Invest. 19: 5151, 1940-
64. CURTIS, G. M. AND M. B. FERTMAN. cf. 66.
65. PETERS, ]. P. AND E. P. MAN. ]. clin. Invest. 29: 1, 1950.
66. RAPPORT, R. L. AND G. M. CURTIS. ]. Clin. Endocrinol. 10: 735, 1950.
67. ROBBINS, ]., ]. E. BALL, D. V. BECHER AND R. W. RAWSON. ]. Clin. Endocrinol. and' Metabolism 12: 856, 1952.
68. GORDON, A. H., ]. GROSS, D. O'CONNOR AND R. PITT-RIVERS. Nature 169: 19, 1952.
69. KLEIN, E. Dtsch. Med. Wschr. 77: 1353, 1952.
70. LAIDLOW, ]. C. Nature 164: 927, 1949.
71. T AUROG, A., I. L. CHAIKOFF AND W. TONG. ]. bioi. Chern. 184: 99, 1950.
72. GROSS,]., C. P. LEBLOUD, A. E. FRANKLIN AND ]. H. QUASTEL. Science 111: 605, 1950-
73. ROSENBERG, I. N. ]. clin. Invest. 30: 1, 1951.
74. DANOWSKI, T. S. ET AL. ]. Clin. Endocrinol. 10: 532, 1950. 75. DANOWSKI, T. S. Problems of American medicine, p. 65. Tokyo: Shindan to Tiryo sha.
1950 (Japanese).
76. DANOWSKI. T. S. ]. clin. Invest. 10: 996, 1950.
77. TAUROG, A. AND I. L. CHAIKOFF. ]. bioi. Chern. 176: 639, 1948.
78. LARSON, F. C., W. P. DEISS AND E. C. ALBRIGHT. Science 115: 626, 1952.

THE THYROID FUNCTION IN NEPHROTIC SYNDROME 321
79. DEISS, W. P., E. C. ALBRIGHT AND F. C. LARSON. ]. clin. Invest. 3! : 1000, 1952.
80. LEWIS, L. A. AKD D. R. McCULLAGH. cf. Clinical study of hypoproteinemia. Tokyo:
Kyodoishoshupan, 1950 (Japanese).
81. GILDEA, A. E., E. B. MAN AND ]. P. PETERS. cf. Clinical study of hypoproteinemia.
Tokyo: Kyodoishoshupan, 1950 (Japanese).