Embed Size (px)
DESCRIPTION
Good things to know
Citation preview
DOCTOR-PATIENT RELATIONSHIP
Interaction that is established between a doctor and patient with the goal of restoring health, alleviate suffering, and preventing disease The doctor needs to establish a dialogue with the patient that plays a
significant role in the success of therapy, as well as to apply theoretical and technical knowledge for DX & TX
There is a dialogue of the relevant medical procedures Also need to remember the family members, because the suffering can either
bring a family together or tear them apart Respect for the patient consists of reciprocity, communication, and concern
It is not shown in the “informed consent” but in the sensitive and attentive response to the nuances of patient behavior, both verbal and non-verbal
The doctor-patient relationship It is not only professional, but humane It displays the dignity of each party
Dignity is an emotional need of having public recognition by authority, personal, friends, family, social circles of having done things well It is an intrinsic quality of being human It is based on the recognition that the person is worthy of respect
It is developed in the hope of curing and being cured It needs empathy, trust, compassion, and sensitivity It is unequal in professional terms, but not in human terms The characteristics of the doctor needed to maintain a doctor-patient
relationship: Knowledge Wisdom Humanity Empathy Willingness to help when facing difficulties
Types of relationships Active-passive
Is provided for patients w/ a coma or if the patient is in a state where active participation is not possible
Guided cooperation Is established w/ patients that are in a condition where they can
cooperate with the doctor in their DX & TX, such as in some acute & chronic diseases such as pneumonia or arterial HTN
Mutual participation Not only compliance w/ TX, but the patient is actively participating in
the discussion of situations and attitudes related with the cause & evolution of the disease
In reality, seeing the patient as a client and the use of modern technology in medical practice has increased errors in the practice of medicine, violating the principles of medical ethics & facilitating the participation of lawyers in malpractice claims The dilemma of the specialist: they know more about the disease, but
understand less of being humane
Rights of the patient To receive adequate medical attention for their state of health and the
specific circumstances of their case, and to be informed when there is a need for references of any other doctor
To be treated w/ trust and that their health information is not divulged to those not expressively authorized
To be treated in a dignified & respectful manner. The doctor, nurses, and all personnel must identify themselves and respect at all times the patients personal and moral convictions
Have the option to obtain a second opinion on DX, TX, or PX To receive information that is sufficient, clear, timely, and accurate of DX,
PX, and TX To receive medical care in case of emergency at any health establishment,
whether public or private To be able to decide on the type of care without any form of pressure, as
well as to accept or reject each diagnostic procedure offered and the person performing the procedure
To have a clinical record w/ information that is truthful, clear, accurate, legible, and complete
Stress and surgery The response to all stressful stimuli, real or symbolic, is a complete
response of the individual, integrated at all levels, from the molecular level and the psychologic level, to the biochemical modifications and changes in behavior
The surgical procedure has many symbolic meanings, different for each operation and for each patient
The surgical procedure is a brutal assault, adding to the aggression of the disease itself, as it consists of pain, danger of death, violation of the body itself by a stranger, mutilation, and of transitory state of death with no guarantee of the brevity
Why is a good doctor-patient relationship important? b/c with it, you can arrive at a more precise DX for the disease b/c we will be able to motivate the patient to the extent possible b/c the patient and the family will be better able to appreciate our work b/c it is important to develop a good clinical history, a document that is
essential in the scientific and legal aspect How to have empathy for a patient? SMILING IS FREE
By first greeting the patient and encouraging them to introduce us to their problem
By being quiet during the interrogation By smiling and exhibiting the ability to listen with sincerity By talking when you need, and giving explanations about their condition By maintaining orderly records SMILING DOESN’T CURE, BUT ALLEVIATES. PRESENCE IS NOT
ENOUGH, BUT IS GRATIFYING
PREOPERATIVE EVALUATION
Integral determination of state of health of a patient that will be submitted for surgery, with the goal of identifying diseases that can affect the prognosis, the surgery itself, or the recuperation from surgery Objective
To evaluate surgical patients to determine if it is necessary to implement therapeutic measures (prophylaxis) so that the patient can tolerate the surgery without any major problems
To reduce Perioperative morbidity and mortality Requirements
Definition of actual physiological state of the patient To determine all pathological processes and their grade of activity Evaluation of nutritional status To delineate physical, cognitive, and emotional state To identify the surgical risk factors (pre/trans/post-operative) Plan of action to minimize risks
Advantages Evaluation of anesthetic risk
ASA 1 = healthy patient, w/o physical/metabolic abnormalities 2 = patient w/ mild-moderate deterioration of physical state
that does not interfere w/ their daily activities 3 = patient w/ severe metabolic/physical disorders that
interfere w/ daily activities 4 = patient w/ severe life-threatening disorders 5 = moribund patient w/ limited life-expectancy w/in the next
24 hours Preparation of surgery includes recommendation for fasting & any
indication for pre-medication Prevention of possible complications Treatment of existing pathologies Formulation of anesthetic plan Obtainment of informed consent
Document which establishes communication from the doctor to the patient informing them of the surgical process that is to come, the alternative options, potential complications, risks and benefits, that the patient accepts with their signature
Separate authorization for: Blood transfusions Anesthesia & its risks
Risks Respiratory
Pulmonary dysfunction It is important to evaluate respiratory function in patients w/
pulmonary problems in case they deteriorate, which represents a major risk of presenting w/ complications such as atelectasis, hypoxia, and pneumonia postoperatively
Risk factors Intense smoker
Cough Obesity Advanced age Intra-thoracic operations Pre-existing lung disease
Risk I = normal Risk II = chronic smoker, controlled chronic pulmonary
disease, acceptable VC & respiratory volume Risk III = chronic smoker, controlled chronic pulmonary
disease, acceptable VC & respiratory volume, limited pulmonary function tests
Risk IV = Acute or active chronic pulmonary disease, w/ poor pulmonary function, hypoxia, hypercapnia
Pulmonary thromboembolism Low risk = TX w/ compressive measures Moderate risk = TX w/ compressive measures, low-dose
heparin (5000 U tid or bid) High risk = TX w/ compressive measures, heparin, or LMWH,
or warfarin Cardiovascular
Based on: Risk I = normal patient Risk II = patient older than 40 or less than 40 & arrhythmic, or w/
previous heart surgery, or hypertensive, or MI more than 6 months ago
Risk III = patient older than 40 or less than 40 & arrhythmic, or w/ previous heart surgery, or hypertensive, MI more than 6 months ago, or with history of infarct less than 6 months ago
Risk IV = decompensated cardiac function, need to evaluate for risk in arterial & venous system studies
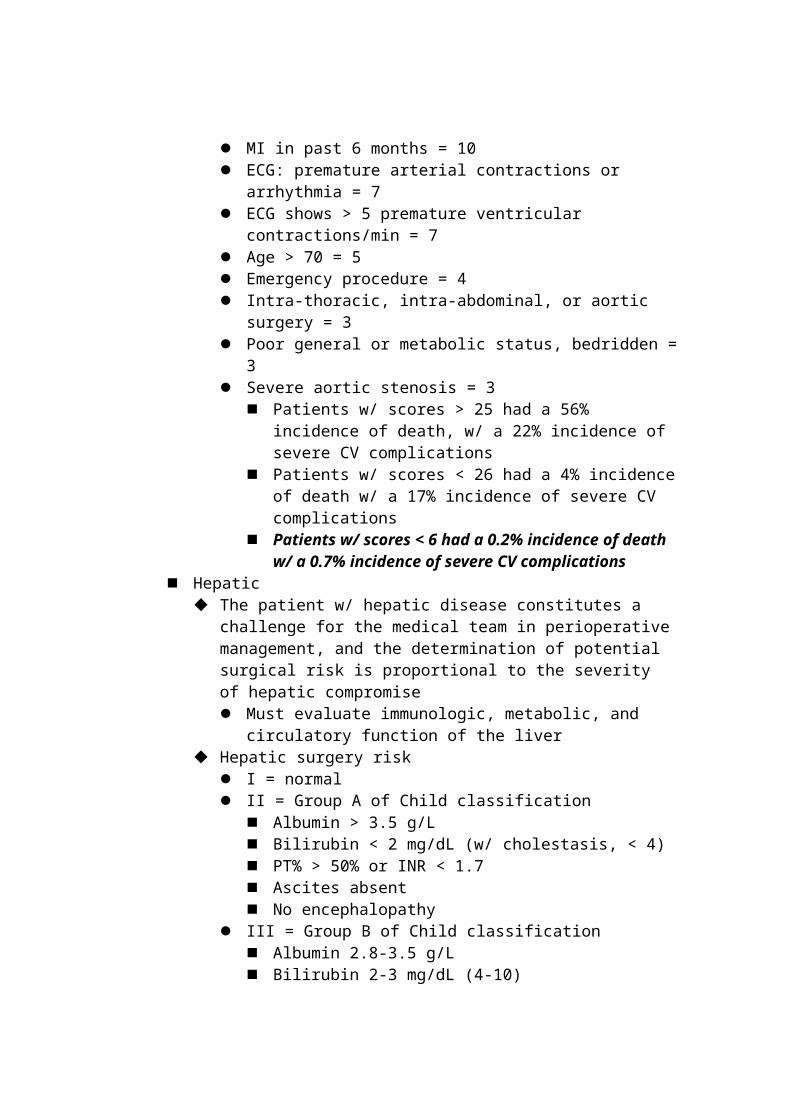
Goldman Cardiac Risk Index S3 = 11 Elevated JVP = 11 MI in past 6 months = 10 ECG: premature arterial contractions or arrhythmia = 7 ECG shows > 5 premature ventricular contractions/min = 7 Age > 70 = 5 Emergency procedure = 4 Intra-thoracic, intra-abdominal, or aortic surgery = 3 Poor general or metabolic status, bedridden = 3 Severe aortic stenosis = 3
Patients w/ scores > 25 had a 56% incidence of death, w/ a 22% incidence of severe CV complications
Patients w/ scores < 26 had a 4% incidence of death w/ a 17% incidence of severe CV complications
Patients w/ scores < 6 had a 0.2% incidence of death w/ a 0.7% incidence of severe CV complications
Hepatic
The patient w/ hepatic disease constitutes a challenge for the medical team in perioperative management, and the determination of potential surgical risk is proportional to the severity of hepatic compromise Must evaluate immunologic, metabolic, and circulatory function of
the liver Hepatic surgery risk
I = normal II = Group A of Child classification
Albumin > 3.5 g/L Bilirubin < 2 mg/dL (w/ cholestasis, < 4) PT% > 50% or INR < 1.7 Ascites absent No encephalopathy
III = Group B of Child classification Albumin 2.8-3.5 g/L Bilirubin 2-3 mg/dL (4-10) PT% 30-50% or INR 1.8-2.3 Mild ascites Grade 1 or 2 encephalopathy
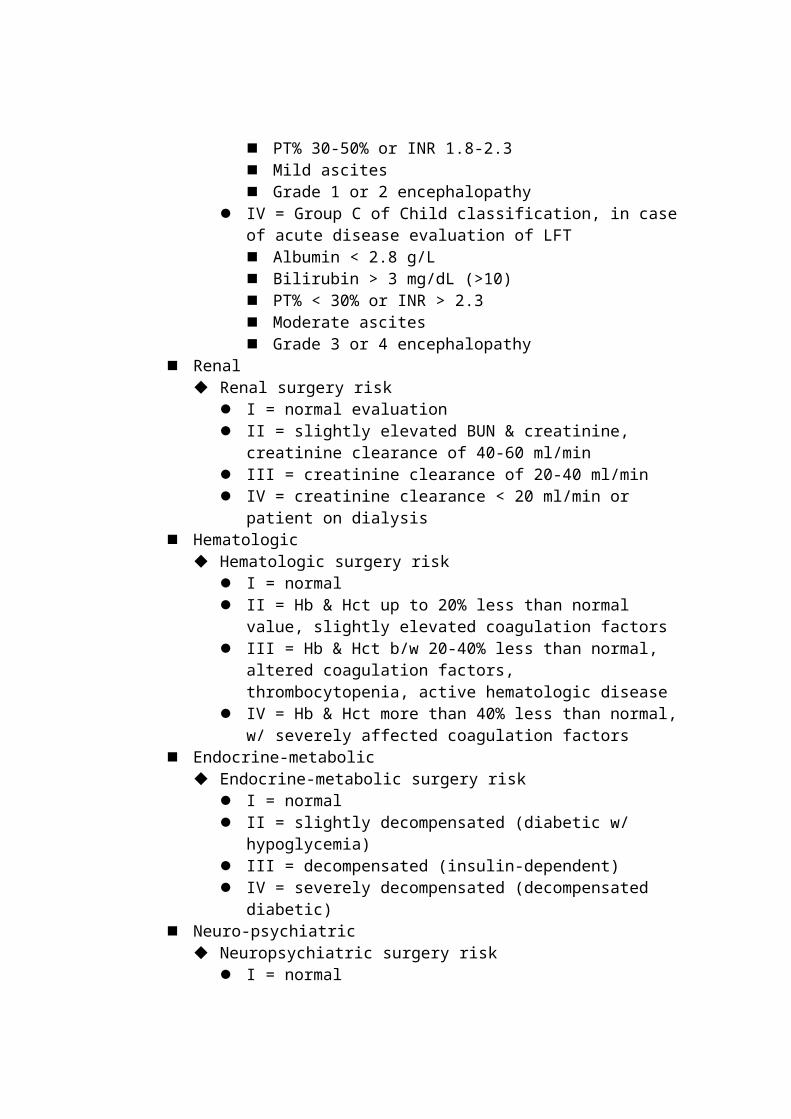
IV = Group C of Child classification, in case of acute disease evaluation of LFT Albumin < 2.8 g/L Bilirubin > 3 mg/dL (>10) PT% < 30% or INR > 2.3 Moderate ascites Grade 3 or 4 encephalopathy
Renal Renal surgery risk
I = normal evaluation II = slightly elevated BUN & creatinine, creatinine clearance of 40-
60 ml/min III = creatinine clearance of 20-40 ml/min IV = creatinine clearance < 20 ml/min or patient on dialysis
Hematologic Hematologic surgery risk
I = normal II = Hb & Hct up to 20% less than normal value, slightly elevated
coagulation factors III = Hb & Hct b/w 20-40% less than normal, altered coagulation
factors, thrombocytopenia, active hematologic disease IV = Hb & Hct more than 40% less than normal, w/ severely
affected coagulation factors Endocrine-metabolic
Endocrine-metabolic surgery risk I = normal II = slightly decompensated (diabetic w/ hypoglycemia) III = decompensated (insulin-dependent) IV = severely decompensated (decompensated diabetic)
Neuro-psychiatric Neuropsychiatric surgery risk
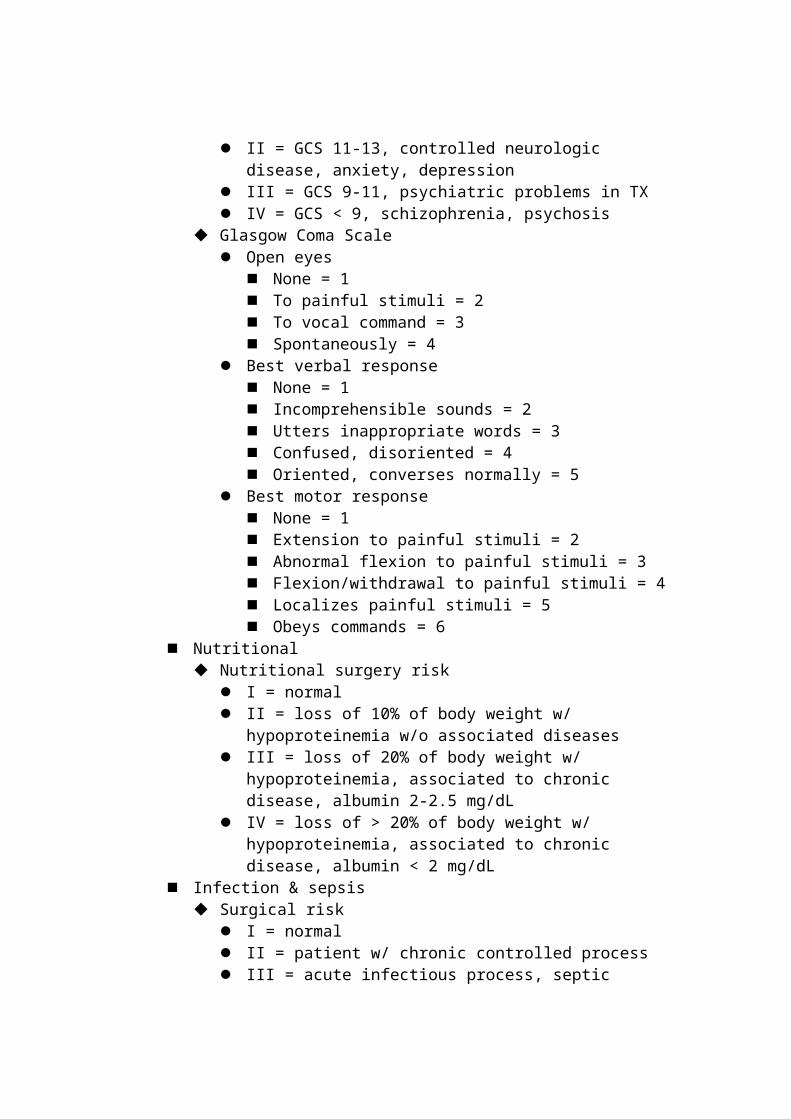
I = normal II = GCS 11-13, controlled neurologic disease, anxiety, depression III = GCS 9-11, psychiatric problems in TX IV = GCS < 9, schizophrenia, psychosis
Glasgow Coma Scale Open eyes
None = 1 To painful stimuli = 2 To vocal command = 3 Spontaneously = 4
Best verbal response None = 1 Incomprehensible sounds = 2 Utters inappropriate words = 3 Confused, disoriented = 4 Oriented, converses normally = 5
Best motor response None = 1 Extension to painful stimuli = 2 Abnormal flexion to painful stimuli = 3 Flexion/withdrawal to painful stimuli = 4 Localizes painful stimuli = 5 Obeys commands = 6
Nutritional Nutritional surgery risk
I = normal II = loss of 10% of body weight w/ hypoproteinemia w/o
associated diseases III = loss of 20% of body weight w/ hypoproteinemia, associated to
chronic disease, albumin 2-2.5 mg/dL IV = loss of > 20% of body weight w/ hypoproteinemia, associated
to chronic disease, albumin < 2 mg/dL Infection & sepsis
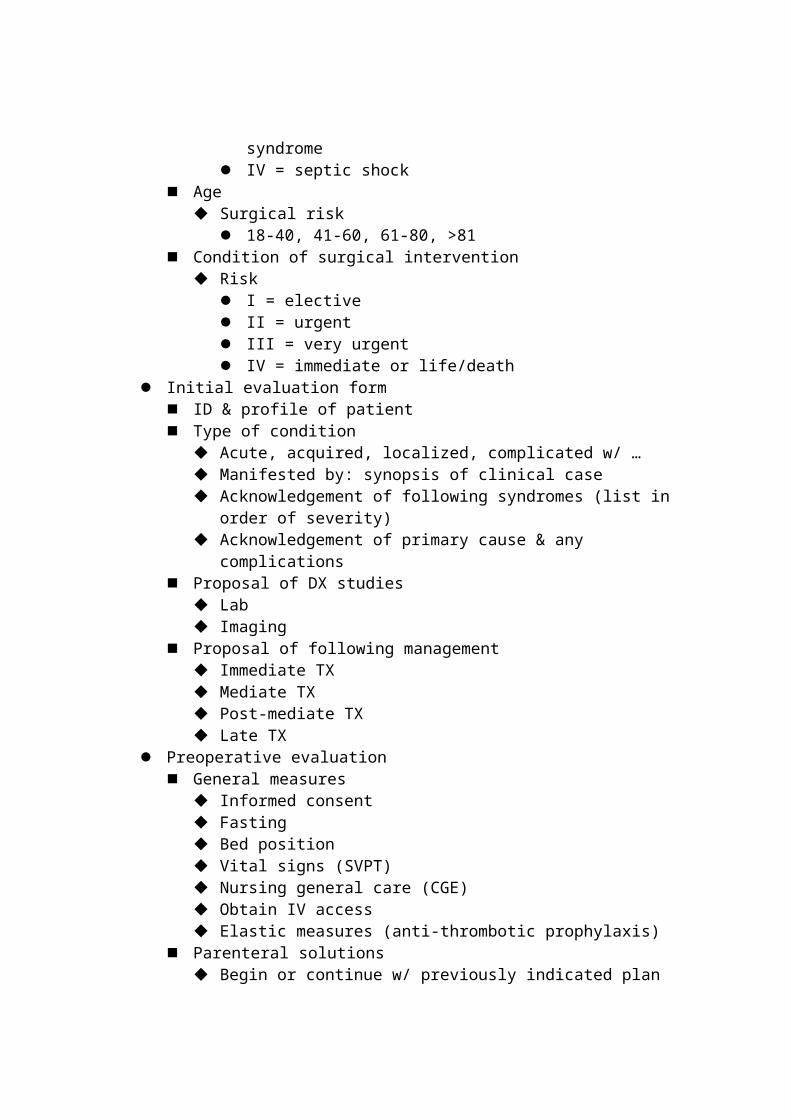
Surgical risk I = normal II = patient w/ chronic controlled process III = acute infectious process, septic syndrome IV = septic shock
Age Surgical risk
18-40, 41-60, 61-80, >81 Condition of surgical intervention
Risk I = elective II = urgent III = very urgent
IV = immediate or life/death Initial evaluation form
ID & profile of patient Type of condition
Acute, acquired, localized, complicated w/ … Manifested by: synopsis of clinical case Acknowledgement of following syndromes (list in order of severity) Acknowledgement of primary cause & any complications
Proposal of DX studies Lab Imaging
Proposal of following management Immediate TX Mediate TX Post-mediate TX Late TX
Preoperative evaluation General measures
Informed consent Fasting Bed position Vital signs (SVPT) Nursing general care (CGE) Obtain IV access Elastic measures (anti-thrombotic prophylaxis)
Parenteral solutions Begin or continue w/ previously indicated plan
Reset solutions Maintenance solutions
Medications Continue w/ medications already initiated
Abx Anaglesics, KCL
Add Omeprazole 40 mg c/24 hours Enoxaparin 20 mg c/ 12 hours SC
Special measures Supplemental O2 (nasal points 4-5 L) Vigilance of tubes (NG, urinary, catheters) Note entry and exit of balance of liquids every 12 hours Solicit CXR, interconsult w/ cardio, w/ anesthesiologist Justification of indications Pass to operating room at 7 AM
Transoperative evaluation Anesthesia Anti-sepsis of operating region Technique of preparation of operating field Technique of laparotomy
Description of surgical technique Technique of closure of laparotomy
Postoperative evaluation Recuperation: ICU, hospital bed
General measures Position Mobilization of bed O2 Vital signs every 15 min General nursing care
Parenteral solutions Mixed solution 1 L for 4 hours NaCl 1 L for 4 hours Dextrose 5% 1 L for 8 hours + 2 ampules of KCL
Medications Ketorolac or Meperidine every 4-6 hours Continue Abx, enoxaparin, omeprazole
Special measures O2 nasal Monitor functioning of tubes & catheters Change of position & exercise every 4-6 hours Form of balance of liquids Removal of NG tube when hear intestinal sounds Initiate PO De-ambulation in 12-36 hours Discharge the following day w/ appointment to remove sutures in 8
days
PERIOPERATIVE ANALGESIA Pain
Characteristics of postoperative pain Nociceptive Involve inflammatory mediators such as:
Prostaglandins Histamine Serotonin Bradykinin
Involves A delta fibers Is acute, w/ variable intensity
30% of recently operated patients suffer from intense pain 40% of recently operated patients suffer from moderate pain 20% of recently operated patients suffer from mild pain
Objective of perioperative analgesia Decrease the stress response, which fundamentally consists of a
neurovegetative response manifested by: Elevation of BP, HR, CO Greater oxygen consumption (organic respiration to surgical stress)
Avoid hyper-excitability of neurons of dorsal horn, by a single dose of
preoperative analgesia Permit “normal” activity of patient, with supplemental analgesics Decrease hospital stay and costs Decrease postoperative complications
Thrombosis d/t delayed de-ambulation Pulmonary alterations d/t retention of secretions or hypoventilation Atelectasis Eschar Thromboembolism Muscular contraction d/t pain
International Association for the Study of Pain (IASP) Recommendations NSAIDs for parenteral use in acute pain
Antipyretic analgesics Propacetamol ampoule of 1-2g IV qid Metamizol ampoule of 2g IV/IM tid/qid Ketorolaco ampoule of 30mg IV/SC/IM qid
Potent analgesic, but w/ moderate anti-inflammatory activity w/ similar analgesic & anti-inflammatory actions to other
NSAIDs, but 350 times more potent than aspirin Inhibits platelet aggregation & can damage gastric mucosa Administration (PO, IV, IM, SC, rectal): the max plasma
concentration can be achieved in 30-60 min, w/ max effects in 2 hours, and lasts 6 hours
It is partially metabolized in the liver & excreted in the urine Renal elimination is prolonged in renal insufficiency & elderly Efficacy
30mg of ketorolac IM = 100mg of meperidine IM (12 mg of morphine IM)
Dosage Ketorolac 30mg qid (no more than 120mg/d for 5 days IV)
In elderly above 65, 15mg qid (no more than 60mg/d for 5 days IV)
Anti-inflammatory analgesics Ketoprofeno ampoule of 100mg IV tid Diclofenaco ampoule of 75mg IM bid Dipirona 1g IV slow infusion (max 4g/d) repeated tid/qid
Opioid analgesics Tramadol 100mg diluted in 100ml physiologic fluid passed in 10
minutes, repeated qid (max 400mg/d) Dextropropoxifeno 38mg/dipirona 1g in 100ml physiologic fluid,
repeated tid (max 152mg/4g/day) Morfina
Full agonist of receptors mu, delta, and kappa Fundamental activity on mu receptors Absorbed via all routes except transdermal Excreted via urine (half-life of 2-4 hours)
Epidural analgesia Most used epidural analgesics are local anesthetics (bupivacaine,
ropivacaine, and lidocaine) and opioids Opioid (fentanyl)
Duration of action is relatively short w/ lipophilic character (prevents the incidence of late respiratory depression associated with epidural morphine)
Most probable side effect of fentanyl is pruritis, which responds normally to a decrease in dose or antihistamines
Can resemble sedation, especially in the elderly, that only respond to a decrease in velocity of perfusion or to removal of medication
Other possible secondary effects are nausea, delay of intestinal motility, and occurrence of distended bladder
Protocol of epidural analgesia w/ PCA pump 200ml saline + 200mg bupivacaine + 600microg fentanyl at 5-
10 ml/hour w/ bolus of 1 ml 200ml of 0.2% ropivacaine + 600microg fentanyl at 5-10
ml/hour w/ bolus of 1 ml Examples of perioperative analgesia
Infiltration of wound: at the end of surgery, a local anesthetic of long duration (0.25% bupivacaine)
Peribulbar or retrobulbar block for ocular surgery or topical analgesics In children, regional anesthesia before surgery reduces the
requirements of general anesthesia w/ subsequent lower incidence of N/V and early & high tolerance
Patterns of treatment Once the surgery is completed, the patient is moved to recuperation
Pain is controlled = initiate IV analgesic protocol Pain is not controlled
Mild pain = NSAID Metamizol 2g Ketorolaco 30mg Propacetamol 2g
Moderate pain = NSAID + Tramadol 50mg + Metoclopramida 10mg in 100cc saline
Severe pain = potent opiate Meperidine 25mg every 4-6 hours until pain is controlled Morphine 2-5mg & later 1mg until pain is controlled
COMPLICATIONS IN SURGERY Any divergence from the predicted course in the systemic recuperation of
operated patient Are the result of the primary disease, the surgical intervention, and other
non-related factors For early detection, it is necessary to repeatedly evaluate the patient Prevention of complications begins before surgery
Important factors in postoperative stage Early mobilization
Adequate respiratory care Liquid and electrolyte balance
Classification Anatomical area
Neurologic Respiratory Cardiovascular Digestive Renal
Extension of anatomical area Local Systemic
Time of presentation Immediate (first phase): w/in OR & up to recuperation area
Anesthetic induction-beginning of surgery Dysrhythmias HR alterations Cardiac arrest Bleeding Defective hemostasis
During the time of surgery Prolongation of estimated operative time Change in route of access Shock state Transfusions
w/ conclusion of surgery-anesthetic reversion Sutures Installation of drainage systems Equipment for immobilization Late recuperation of alert state
Odontologic (loss of dental pieces) Ocular (conjunctivitis, corneal lesions) Musculoskeletal (lumbalgia, pharyngitis, laryngitis, phlebitis) Dehiscence of wounds, rupture of sutures, N/V, headache
Recent (second phase): in bed or intensive therapy Respiratory
Dyspnea Respiratory insufficiency Pulmonary infection Pulmonary thromboembolism Pneumonia Pneumothorax Atelectasis
Cardiovascular Tachycardia Arrhythmias Shock HF
Phlebitis DVT
Neurologic Disorientation Loss of consciousness Headache
Renal Renal insufficiency Oliguria Hydroelectrolytic disequilibrium
Late (third phase): w/ discharge and until full recovery Headache Pulmonary infections Respiratory insufficiency Phlebitis DVT Depression GI dysfunction Hepatic insufficiency Renal insufficiency Eschar Anemia Muscular weakness Myalgia Anorexia
Probability of presentation Avoidable vs inevitable Predictable vs unpredictable
Complications of surgical wounds Evaluate health status of patient Anti-sepsis of operative area, as well as adequate hemostasis Prophylactic antibiotic therapy
Seroma Accumulation of ECF
Separates layers of skin Cuts numerous lymphatic vessels
TX Drain by puncture Tetracycline 1g in 150ml saline Re-intervention to ligate lymphatics
Hematoma Accumulation of blood & clots Frequent, imperfect hemostasis
Pain Increase in local temperature Swelling Ecchymoses
If small, drain w/ open puncture & give prophylactic Abx
Keloids Excessive accumulation of collagen tissue in response to trauma TX
Extirpation w/ or w/o graft Partial resection Radiotherapy Local steroids (triamcinolone)
Dehiscence of wounds Partial or total rupture of any of the layers of a wound
5% in older than 60 M > F On postoperative day 5-8
Etiology Infection Poor surgical technique Poor selection of suture material Anemia, DM, uremia, malnutrition, cirrhosis Deficient tissue perfusion
3 important risk factors Inadequate closure: use of insufficient amount of sutures or placement
too close to the border Increase in intra-abdominal pressure: obesity, cirrhosis, cough Deficient curing of wound d/t seroma, hematoma
Evisceration Exposure of abdominal contents outside the limits of the parietal
peritoneum Increase in intra-abdominal pressure Dehiscence of surgical wound
Syndrome of abdominal compartmentalization Cellulitis
Inflammatory process d/t bacterial infection which extends via skin or subcutaneous tissue Edema Redness Heat/hyperthermia Headache
Local measures Cold compression Local cleaning Topical Abx
Systemic measures Abx therapy Synthetic & selective
Necrotizing fascitis Local
Erythema Distant tumefaction Distant cellulitis
Absence of crepitus Systemic
Toxemia Mental apathy Dehydration Negative cultures
Associated w/ DM, Immunosuppression TX
Ample debridement Systemic Abx therapy
Gaseous gangrene Rare, is produced by anaerobic bacteria Is related to the type of surgery Clinical presentation
Intense pain at wound 12-72 hours postoperatively Hyperthemia (39.5-41) Tachycardia (120-140) Grayish pallor Severe shock Subcutaneous crepitus Alterations in consciousness Diaphoresis
TX Debridement of wound Abx Hyperbaric oxygen therapy Amputation
MC systemic complications in surgery S/S
Fever = atelectasis/infections/post-transfusion/drugs/thrombophlebitis Tachycardia & anxiety = hypovolemia Dyspnea = hypoxemia, arrhythmias, sepsis, pain Hypotension = hypovolemia, sepsis, HF, anaphylaxis, bleeding Oliguria = hypovolemia, ARF
MANAGEMENT OF BURN PATIENTS Burns
Lesions in skin d/t physical (temperature), chemical, electrical, and radiational over-exposure Differ in severity, extension, and depth of affected tissue
Superficial (epidermal) Dress w/ tulle gras and gauze if extensive until healed (usually
w/in 1 week) Superficial partial thickness
Dress w/ tulle gras and gauze & re-assess at 48 hours Heal w/in 2-3 weeks
Low exudate May be suitable for Hypafix, wash dressing daily
and take off with oil in 1 week High exudate
If contaminated or signs of infection, apply antimicrobials & need to refer
If not contaminated, continue w/ tulle gras or Bactigras and review every 2 days until healed
If not healed w/in 2-3 weeks Requires surgery (refer to burn unit)
Deep partial thickness Obvious deep dermal injury
Requires surgery, preferably w/in 5 days, unless < 1cm2 in area
If no obvious deep dermal injury Dress w/ tulle gras and gauze, reassess at 48 hours
Signs of improvement in healing Re-dress and review every 2 days
If unhealed at 2 weeks, requires surgery & refer to burn unit
If no signs of improvement in healing If unhealed at 2 weeks, requires surgery & refer to
burn unit Management
Airway: compromised or at risk of compromise? Yes = intubate No = BREATHING
Breathing: compromised? Yes = cause
Mechanical: escharotomies CarboxyHb: intubate & ventilate Smoke inhalation: nebulizers, ventilation Blunt injury: invasive ventilation, chest drain
CIRCULATION Circulation: compromised perfusion to an extremity?
Yes = escharotomies No = NEUROLOGICAL DISABILITY
Neurologic disability: impaired GCS score? Yes = consider hypoxia or hypovolemia No = EXPOSURE
Exposure: fully assess burn areas & depth, full examination of concomitant injuries, keep warm
Fluids: calculate resuscitation formula based on surface area & time since burn
Heat burns Cutaneous cellular damage caused by increase in temperature at the cellular
level T < 45 = w/o evident damage T = 45-50 = diverse grades of lesion T > 50 = evident cellular damage w/ presence of denaturation of
cellular proteins Skin
0.25 sq m in children (up to 1.8 sq m in adults) Epidermis
Stratum corneum Stratum lucidum Stratum granulosum Stratum spinosum Stratum basale
Dermis Formed by fibroconnective tissue Amorphous in the region of blood vessels Nervous plexus 2 layers
Papillary dermis Reticular dermis
Hypodermis Subcutaneous tissue
Etiology Multiple causes
MCC Direct flame Hot liquids Direct contact w/ hot metals Electric current
Other causes Chemical (acidic/alkali) Spark Atomic radiation
Extension of burn Should be quantified while taking into account the extent of the burn Rule of 9 (in children)
Head = 9 (18) Anterior thorax = 9 Anterior abdomen = 9 Right superior extremity = 9 Left superior extremity = 9 Right inferior extremity = 18 (14) Left inferior extremity = 18 (14) Genitals = 1
Rule of palm Adults = palm of the hand including fingers = 1% of total surface
area Children = palm of hand including fingers = 2% of total surface
area Classification
Depth First degree = epidermis
Painful erythema Intact basal membrane Management
Healthy in 5-7 days spontaneously apart from basal layer Only require application of moisturizer In case of important discomfort (burning), prescribe an
analgesic Second degree
Superficial Erythema Presence of ampoules Underlying tissue is white w/ pressure Is painful Management
Debridement of ampoules Cleaning w/ water & soap everyday is there is no NaCl Apply sterile dressing Healthy in 3-4 weeks Generally do not require reconstructive procedures
Deep More pallor Can be gray or opaque Hypoesthetic
Third degree Extensive destruction of skin Painless lesions Coffee-colored or black lesions Dry, hard, w/ no elasticity No vesicles No sensitivity Management
In burn unit Always require reconstruction First, only apply sterile dressing
Immediate IV fluid therapy Burn of airways
Symptoms: can cause swelling that blocks airflow Charred mouth Burned lips Burns on head, face, or neck Wheezing Change in voice Difficulty breathing, coughing Singed nose hairs or eyebrows Dark, carbon-stained mucus
Incidence of burns Mortality & frequency of burns
Scalding = 22% (mortality of 10%)
Inflammatory liquids = 16% (6%) Explosions = 11% (13%) Burning homes = 5% (44%)
Causes of burns in children Scalding = 42% Inflammatory liquids = 10% Oils = 7%
Sites of burns Forearm Hand/wrist Arm Face
Special burns Chemical burns
Acids = cause denaturation of cellular proteins Alkali = cause caseation of cellular proteins Management
Immediate removal of whatever is causing damage Apply continuous irrigation (running water) for 1-2 hours (2-4
hours for alkali burns) Do not apply neutralizing agents
If burns for phosphorus, lithium, or sodium, no water Electric burns
Low-voltage < 1000 V High-voltage > 1000 V Non-evident lesions Can cause arrhythmias At least, maintain medical observation for 24 hours, w/ ECG every 8
hours & continual monitoring Management
Definitive management of burns Apply graft
Partial thickness Complete thickness
Fluid therapy Restoration of liquids when possible Begin application of formulas when the burnt surface is at least 20% or
if lesions are of second/third degree Remember that fist degree burns do not require restoration of liquids Formulas
Evans Brooke Parkland
First 24 hours: Hartman (Ringer’s lactate) 4ml/kg/%SA burnt of second/third degree Half in the first 8 hours Quarter in the next 8 hours Quarter in the next 8 hours
Diuresis of 30-70 ml/h Second 24 hours
Dextrose 5% in water to conserve Na at 140 mEq/L Colloid solution (plasma) to conserve blood volume in
patients w/ burns of second/third degree affecting more than 40% of total body surface area
Diuresis of 30-100 ml/h Hypertonic (Monafo) Half Carbajal
First 24 hours Ringer’s lactate: 5000ml/sq m burnt in adults
2000ml/sq m burnt in children Colloid: 12.5g/L of Ringer’s lactate
Second & third 24 hours Ringer’s lactate: 2500ml/sq m burnt in adults
2000ml/sq m burnt in children Colloid: 12.5g/L of Ringer’s lactate
Escharectomy Cut skin to free the tension of eschar When there is vascular compromise distally or w/ respiration Performed in ER
Factors for hospitalization Burns of > 10% of total body surface area in patients under 10 & over 50 Burns of > 20% of total body surface area in patients b/w 10-50 Burns of third degree greater than 5% in any age Pre-existing medical disorders Extremes of life Chemical burns Inhalation lesions Presence of other major trauma Burns of special areas
Control of pain Meperidine 25-50mg infusion every 2-4 hours Morphine sulfate 2.5-5.0mg IV Hydromorphine chlorhydrate 0.5-1.0mg IV repeated every 2-4 hours Antihistamine
TX A,B,C Initiate fluid therapy w/ strict control of liquids Realization of ambulatory surgical process in case it is needed Complete evaluation & transfer to burn unit Debridement & excision of necrotic tissue
Autografts Grafts: mallados Flaps Cultivated skin Heterografts & allografts
Synthetic substitute for skin (Integra) Split skin graft donor site management
Split-thickness skin grafting is recommended for third & fourth degree burns
Involves harvesting skin from an unaffected part of the patient (epidermis & superficial dermis) Donor sites heal in 10-14 days but can be very uncomfortable Potential for complications
Extreme discomfort Intense pain Leakage of blood Serous fluid & infection
Traditional dressing w/ open-weave tulle impregnated w/ petroleum jelly, covered by an absorbent layer of gauze & cotton wool
Goals Promote rapid wound healing Reduce pain Provide a barrier to infection Absorb copious amounts of exudate Be easy to handle & apply Be removable w/o traumatizing the new epidermis Not impede the morality of the patient No antigenic or allergenic Reduce the risk of hypertrophic scarring Inexpensive & accessible
Dressings Tulle gras: tulle adheres firmly to raw surface until healing is
complete Silver sulfadiazine: Abx cream that is effective in reducing risk of
infection Calcium alginates: promote blood clotting & wound healing by
creating a moist environment Film dressings Biological dressings
Topical antibiotics Silver sulfadiazine Sodium mafenide Platinum nitrate of 0.5% Iodopolivinilpirrolidona (isodyne)
Complications of burn patients Cardiovascular
Hypovolemic shock Acute MI HTN Myocarditis
Respiratory Inhalation wound
Pneumonia Acute respiratory insufficiency Pulmonary edema
Renal Renal insufficiency Myoglobinuria
GI Curling ulcers Hepatic dysfunction Alithiasic cholecystitis
Metabolic & nutritional Lack of nutrition Prolonged catabolism
Endocrine Suprarenal bleeding Insulin/glucagon disequilibrium
Neurologic Burn encephalopathy w/ carbon monoxide intoxication
ACID-BASE DYSEQUILIBRIUM The respiratory apparatus have sensitive chemoreceptors in the concentration of
H+ in the CNS, in the aorta, and in the bifurcation of the carotids The principal function of the cardio-respiratory function is supplying the
cells of the body with the blood flow to enable to be viable in ideal conditions
The kidney participates in the maintenance of acid-base equilibrium via: Regulates urinary excretion of circulating bicarbonate Excretes hydrogen ions
The most important buffer is sodium bicarbonate which reacts w/ carbonic acid Other substances that act as significant buffers are Hb, other proteins,
phosphates, and carbonates Arterial blood gases (ABG)
Evaluate the state of acid-base equilibrium (used preferentially in peripheral venous blood)
Evaluate hemodynamic state, using venous saturation of oxygen in central venous blood
Essential applications The evaluation of diffusion of gases at the pulmonary & systemic level The evaluation of the relation b/w acids & bases of ECF
pH Measures the global results of acid-base equilibrium It is not a parameter of evaluation of respiratory function Time of respiratory alteration If a respiratory process is acute or chronic, or when a chronic process
becomes acute PaCO2
Measures partial pressure of CO2 in arterial blood Is a parameter that is related to respiration
PaO2 Measures the partial pressure of oxygen in arterial blood Is a parameter which uses oxygenation in respiration
HCO3 Measures basic component of acid-base equilibrium Acute or chronic process
Anion gap To maintain electroneutrality
Positive load (cations) must equal negative load (anions) If not, normal anion gap is 8-16 mEq/L calculated by:
Na – Cl – HCO3 Metabolic acidosis
When HCO3 decreases, pH decreases = acidosis The body tends to increase the level of ventilation (hyperventilation) and
the CO2 decreases pH < 7.35 HCO3 < 22 mEq/L PaCO2 < 35 mmHg (if there is compensation)
Uncompensated metabolic acidosis (compensated) pH < 7.23 (7.32) PaCO2 = 35 mmHg (< 27 mmHg) HCO3 < 19.2 mEq/L (< 13 mEq/L)
Etiology Loss of bicarbonate d/t diarrhea Excessive production of organic acids d/t hepatic diseases a/o
endocrine alterations Shock Intoxications d/t drugs (salicylates) Inadequate excretion of acids d/t renal insufficiency Parenteral nutrition
S/S Rapid & deep breathing Fruity breath Hypotension Ventricular arrhythmias N/V Deterioration of level of consciousness, headache, confusion, & coma
TX Correct the cause of acidosis Correct the input of deficit of bases (input of bicarbonate if pH < 7.2)
Complications Hypovolemic shock, septic shock Hyperchloremia Deficiency of insulin High-output diarrhea Terminal phase of renal failure Fistula (pancreatic, duodenal, ileal) Non-adaptive ileostomy
Metabolic alkalosis If bicarbonate increases & produces an increases of pH, and is produced by
an increases in bases or HCO3 The body produces hypoventilation by increasing the level of CO2
pH > 7.45 HCO3 > 26 mEq/L PaCO2 > 45 mmHg (if there is compensation)
Etiology Loss of acids d/t prolonged vomiting or gastric aspiration Loss of K+ by increase in renal excretion (w/ diuretics) Alkaline antacids
S/S Slow & shallow breathing Muscular hypertonia Restlessness Fasciculations Confusion Irritability Coma
TX Administration of NaCl or KCl depends on the severity of
hypokalemia, before cases of severe or persistent alkalosis can require NH4Cl
Complications Hyperchloremic
Loss of chloride Gastric aspiration Vomiting Cerebral edema
Respiratory acidosis When bicarbonate increases, pH decreases The organism increases bases, eliminates acidic urine by the kidney,
pH < 7.35 HCO3 > 26 mEq/L (if there is compensation) PaCO2 > 45 mmHg
Uncompensated respiratory acidosis (compensated) pH < 7.22 (7.36) PaCO2 > 70 mmHg HCO3 > 27.4 mEq/L
Etiology CNS depression d/t drugs, lesions, or illness Asphyxia Hypoventilation d/t pulmonary disease, cardiac disease,
musculoskeletal disease, or neuromuscular disease S/S
Diaphoresis Headache Tachycardia
Confusion Nervousness
TX Treat the disease Mechanical ventilation in severe forms a/o accompanied by hypoxemia Assisted ventilation before a chronic hypercapnia is indicated only if
there is an acute increase in PCO2 Respiratory alkalosis
If the bicarbonate decreases & CO2 also decreases d/t hyperventilation, there is an increase in pH
pH > 7.45 HCO3 < 22 mEq/L (if there is compensation) PaCO2 < 35 mmHg Etiology
Hyperventilation for pain, anxiety, or inadequate use of ventilator Respiratory stimulation for drugs, asthma, hypoxia, fever Hepatic insufficiency Exercise
Uncompensated respiratory alkalosis (compensated) pH > 7.53 (7.38) PaCO2 < 23 mmHg HCO3 < 18.7 mEq/L (< 14.2 mEq/L)
S/S Rapid and deep breathing Paresthesia Anxiety Fasciculations
TX First treat the cause Then treat the hyperventilation w/ sedatives or have the patient breathe
into a brown paper bag Complications
Sepsis Pneumonia Thoracic trauma Pain Hyperthermia Anxiety Tachycardia Hepatic failure Mechanical ventilation
ABG Renal compensatory conditions or primary respiratory situations, are slow
to be evident w/in 48 hours, however respiratory compensation to metabolic abnormalities subsequent to primary metabolic alterations are done in a matter of minutes, given the large volume of CO2 that is managed by the lungs in the short term
Acidosis
Alteration of electrical status of multiple proteins Enzymatic systems fail Hyperkalemia Hyperchloremia Alterations in state of consciousness Muscular weakness Failure of cardiac rhythm
Coronary & cerebral vasodilation Pulmonary vasoconstriction Decrease in RV pressure Myocardial depression
Alkalosis Tetany (reduction of Ca++ ions) Hypokalemia (entry of K+ into ICF) Coronary & cerebral vasoconstriction Pulmonary vasodilation Diaphragmatic depression Hypokalemia & Hypochloremia
Surgery Acid-base disorders most frequent in surgical patients is metabolic acidosis Non-lethal acid-base disorders in surgical patients are metabolic alkalosis
& respiratory alkalosis
ORGANIC RESPONSE TO SEVERE LESION Response to lesion
Set of organizational changes that occur during the process of convalescence following an organic lesion. In what is lost in the acute form, the local & systemic homeostasis, and
the favorable circumstances, permitting anatomical, functional, and psychic re-establishment: Physiologic field
Series of events aimed at restoring homeostasis & repairing the tissue damage as quickly as possible
Courses w/ a self-immune response, but do not develop SIRS Express clinically the presence of generalized systemic
endothelial inflammation, independent of the productive cause
3 or more of the following conditions Temperature > 38 or < 36 HR > 90/min Respiratory rate > 20/min or PaCO2 < 32 WBC > 12000 or < 4000 or 10% bands
w/ a duration of 5-10 days from surgery, ADH & aldosterone levels returned to normal & to recover and a tenth of cortisol recuperates its circadian rhythm of secretion
Pathophysiologic field Set of events, beyond the horizon of their physiological
development & lead to the extremes of the body:
Immunologic dissonance Hypercatabolic state Cardio-circulatory instability
Consisting of all previous events that decimate the functional reserve, to the extent that the response itself becomes a threat to life
Etiology of acute & deep loss of homeostasis Severe accidental lesion
Multiple trauma Severe burns
Extensive elective lesions Transplants Surgical TX of cancer Surgical control of abdominal sepsis Orthopedic surgery of extremities under ischemia Hip surgery Colon surgery Cardiac surgery w/ extra-corporeal pump
Severe disease Shock Sepsis Organic failure: renal, hepatic, intestinal Acute respiratory failure
Pneumonia Severe asthma Acute pulmonary edema Decompensated COPD
Severe disease Extensive tissue infarct Severe intoxications Systemic vasculitis Cancer in advanced stages DKA Severe pancreatitis AIDS
Triggers therapeutics Blood-derived transfusions Idiosyncratic & drug response
Anaphylaxis Malignant hyperthermia Epidermal necrolysis
Immunotherapy, chemotherapy, a/o radiotherapy Prolonged transoperative hypotension Alveolar recruitment Thrombolysis (follows w/ ischemia-reperfusion)
Metabolic response to trauma Ebb phase
Defend homeostasis (perfusion volumes, pH)
3-24 hours Decreased balance of N2 Diminished tissue perfusion Cold, clammy skin Slow capillary filling Diminished central temperature
Flux phase Lesion has priority: mobilization of protein stores
1-14 days Catabolic phase Increased metabolic load Decreased balance of N2
Lesion & body have priority: reconstitution of protein stores Weeks Anabolic phase Increased balance of N2
High cardiac output Hypermetabolism Increased energy output Accentuated protein catabolism
Pathophysiology of the problem (sepsis) The monocyte-macrophage system is being stimulated by bacteria or its
products, and secretes inflammatory mediators or pro-inflammatory cytokines including TNF, IL1, IL2, IL6, IL8 Simultaneous secretion of anti-inflammatory cytokines such as IL4,
IL10, w/ the goal of modulating of action of pro-inflammatory cytokines
Monocytes release an inflammatory response Pro-inflammatory = SIRS = death Balanced response = resolution Anti-inflammatory = CARS = death
Apoptosis & necrobiosis The type of cellular death determines immunologic function of
surviving cells (CD4 T cells) Apoptotic cells: induce anergy or presence of anti-inflammatory
cytokines & block the immune response: auxillary Th2 cells & IL4 & IL10
Necrotic cells: Induce an inflammatory state creating an immune response & incrementing antimicrobial defenses: Th1
Neuroendocrine response Physiologic
Retain Na & water for guaranteeing circulating volume Maintain catabolism of macromolecules that provide substrates for
synthesis of energy, conservation of acid-base state Modulate the immunologic response, maintenance of epithelial barriers
& reparation of sites of lesion Nutrition
Set of interconnected factors to achieve:
Homeostasis Energy Growth Restoration of organism
The nutrition of human organism, depends on cellular metabolism which consists of 2 fundamental phases Anabolism
Biosynthesis of macromolecules To grow & maintain structure (proteins) For caloric-energy reserve (glycogen, lipids)
Catabolism Oxidation of nutrients for the production of energy (AcCoA + O2 =
ATP) and the elimination of waste products (CO2, NH2) Nutrition in fasting & stress (trauma, surgery, sepsis)
The stimulus of the neural & endocrine systems block the adaptation & establish a hypercatabolism, which in these situations is proportional to the magnitude of stress Greater requirement for glucose, fat, and protein for muscle repair
of injured tissues The effects of catabolic hormones will be reflected in the
proteolysis Increments of Basal Energy Needs following type of stress:
Elective surgery: 10-25% Trauma: 10-30% Sepsis: 50-80% Burns: 100-200%
Complications of malnutrition Delay of scarring Depression of immunocompetence Decrease in resistance to infection Sepsis Death
CV response Physiologic
Adequate flow & perfusion pressure to organic demand Its ability to generate pressure produces interstitial fluid continually w/
continual flow, carrying oxygen & energetic substrates of cells Transporters & mediators leads to the elimination of substances
Intravascular volume depletion and hypotension Generalized or localized reduction in renal blood flow = ischemic ARF
GI, renal, and dermal losses: hemorrhage, shock Large vessel renal vascular disease
Renal artery thrombosis/embolism, operative arterial cross-clamping, renal artery stenosis
Small vessel renal vascular disease Vasculitis Atheroembolism HUS
Malignant hypertension Scleroderma Preeclampsia Sickle cell anemia Hypercalcemia Transplant rejection
Sepsis Hepatorenal syndrome Medications
Cyclosporine Tacrolimus ACE inhibitors NSAIDs Radioconstrast agents Amphotericin B
Decreased effective intravascular volume CHF HF Cirrhosis Nephrosis Peritonitis
Immunoendothelial response At the local level, limits the damage, destroys infecting agents, removes
dead tissue, and limits necrosis & apoptosis Promotes local hemostasis & tissue repair At the systemic level protects the body against invasive pathogens
Pathophysiology (in sepsis) Bacterial aggression, triggers a series of immunologic responses to
combat the aggression that also causes damage to the body Vascular endothelium
Rolling mediated by selectins PMN: L-selectin Endothelium: P/E-selectin
Firm adhesion mediated by integrins PMN: LFA-1, Mac-1 Endothelium: ICAM-1, VCAM-1
Transmigration PECAM, VLA-4
Identification of organic dysfunction like markers of severe sepsis Altered consciousness, confusion, psychosis Tachypnea
PaO2 < 70 mmHg SaO2 < 90% PaO2/FiO2 < 300
Icterus Positive enzymes
Decreased albumin Increased PT
Tachycardia Hypotension Decreased central venous pressure
Oliguria/anuria Increased creatinine
Decreased platelets Increased PT Decreased protein C Increased D-dimers
LIQUIDS & ELECTROLYTES Homeostasis is maintained by coordinated action of hormonal adaptations
TBW (50-75%) of body mass, and changes w/ sex, age, & fat content In newborns, 75-77% In children 1-12 months, 65.5% In children 1-10 years, 61.7% In adults, b/w 50-60% of body mass In relation to sex, in adolescence, there is a greater water content in
males d/t the higher fat content in women ICF represents 40% of mass ECF represents 20% of mass Plasma constitutes 5% of mass Interstitium constitutes 15% of mass Transcellular fluid (lymph, peritoneal, pericardial, pleural, CSF) 1-2%
Regulation of body water Regulation of entry & excretion Thirst, which is regulated by the medial hypothalamic center, is a major
defense against depletion of liquid & hypertonicity Kidneys: RAS & ADH Excretion of body water is regulated by a variation in the rhythm of
urinary flow ADH or vasopressin
Controls reabsorption of water in renal tubules Regulates hydroelectrolytic balance of body fluids Increases cellular permeability in distal tubules & in collecting
ducts Decrease formation of urine
Sufficient kidney is a major ally to a patient undergoing inadequate management of liquids & electrolytes The kidney is the effector organ in the response to loss of
hydroelectrolytic homeostasis The kidney makes fine adjustments on the volume of body water &
electrolyte concentration Effective circulating volume
The proportion of circulating volume that inhibits compensatory response of homeostatic receptors
Entry Liquids: 1200 ml
Food: 1000 ml Metabolic: 350 ml
Loss Urine: 1500 ml Passive loss: 900 ml Sweat 50 ml Feces 100 ml
Electrolytes Cations in body water include Na, K, Ca, Mg
Na+ Excreted via the kidneys & via skin by sweating Excreted in great quantities when body temperature is high, during
exercise, fever, or emotional tension Hyponatremia < 135 mEq/L
Causes Pseudo-hyponatremia induced by active osmotic molecules
(glucose, mannose, glycine) Provoke a displacement of water, w/o altering the
quantity of sodium, which decreases the concentration (dilutional hyponatremia)
An increase of 100 g/dL glucose provokes a decrease in 1.7 mEq/L of Na
Pseudo-hyponatremia induced by active non-osmotic molecules (TG, proteins) These molecules reduce the relative % of water in a
determined volume of plasma Elevation of 1 g/dL of TG decreases natremia by 1.7
mEq/L Elevation of 1 g/dL of plasma proteins cuases a
decrease in natremia of 1 mEq/L Loss of Na
Renal Diuretics Osmotic diuretics Hypoaldosteronism Nephropathy w/ salt loss Diuresis Postobstructive
Digestive Vomiting Drainage tube Fistulas Obstruction Diarrheas
Cutaneous Sweating Burns
Drugs
Physical exercise CNS alterations: hemorrhage, astrocytomas,
hypopituitarism S/S
GI: N/V Peripheral nervous system: muscle tremors, visual
alterations CNS: lethargy, convulsions, coma
TX Hyponatremia w/ diminished ECF
Administration of isotonic saline solutions Na = (140 mEq/L – Na actual) x (0.6 x weight)
Hyponatremia w/ minimally increased ECF Initial TX is based on restriction of fluids In the presence of neurologic symptoms, administer
hypertonic saline solution (20%) along w/ small doses of loop diuretics (furosemide)
For more severe cases, administer urea at 10-30% which provokes osmotic diuresis
Hyponatremia w/ increased ECF Characterized by the presence of edema, and is related
with HF, nephrotic syndrome, and cirrhosis TX is based on restriction of liquids & salt along w/
administration of loop diuretics Hypernatremia > 150 mEq/L
Pathophysiology Insufficient action of ADH
Deficit of central production Loss of renal response
Excessive loss of water Renal Extra-renal
Positive salt balance Iatrogenic Primary hyperaldosteronism
S/S Thirst Can be accompanied by polyuria Diarrhea Sweating Neurologic disorders
TX Objectives
Correct triggering cause Correct osmolarity Normalization of ECF
Hypernatremia w/ hypovolemia Isotonic solutions until no signs of dehydration
Continue to use hypotonic solutions until correction of hypernatremia 0.45% saline solution 5% dextrose solution
Hypernatremia w/o hypovolemia Water PO If not possible, parenteral 5% dextrose
K+ Renal excretion is accelerated w/ ACTH & cortisone Increased serum concentration of K+ produces a clinical effect on
cardiac muscle Decreased ECF concentration of K+ produces weakness w/ loss of
smooth & striated muscle tone, along w/ circulatory failure Hypokalemia < 3.5 mEq/L
Severity Mild: 3-3.5 mEq/L or a deficit of 150-300 mEq Moderate: 2.5-3 mEq/L or a deficit of 300-500 mEq Severe: < 2.5 mEq/L or a deficit of > 500 mEq
Causes GI loss: diarrhea, laxatives Renal loss: hyperaldosteronism, K+-wasting diuretics,
penicillin, Amphotericin B Intracellular changes (alkalosis) Malnutrition
S/S Weakness, fatigue Paralysis, respiratory difficulty Muscle disorder (rhabdomyolysis) Constipation Paralytic ileus Leg tremors
TX Minimize extensive loss of K+ & replace K+
Administration of IV K+ is recommended when arrhythmias are present or hypokalemia is severe When indicated, max replacement of K+ IV is 10-
20 mEq/h w/ continuous ECG monitoring Hyperkalemia > 5.0 mEq/L
Repeat test Confirm test w/ ECG
Peaked T wave Short QT interval Fat QRS complex Slow conduction velocity
TX Average elevation (5-6 mEq/L): remove K+ from body
Diuretic: Furosemide 1mg/kg IV slow infusion Kayexalate: 15-30 in 50-100 mL of 20% sorbitol
solution Dialysis: peritoneal or hemodialysis
Moderate elevation (6-7 mEq/L): change ICF K+ NaHCO3 50 mEq IV Glucose-insulin IV Albuterol nebulizers 10-20 mg
Severe elevation (> 7 mEq/L) 10% CaCl2 at 5-10 mL IV over 2-5 minutes 50 mEq IV NaHCO3 for over 5 minutes Glucose-insulin IV Albuterol 20 mg Diuresis (40-80 mg IV furosemide) Kayexalate enema Dialysis
Anions in body water include Cl-, HCO3-, HPO4- Organ monitor of hydro-electrolytic disorders
Of volume Substance: water Organ: kidney Manifestation: oliguria, anuria
Of concentration Substance: sodium Organ: brain Manifestation: coma
Of composition Substance: potassium Organ: muscle Manifestation: ileus, arrhythmias, weakness
Increase in requirements Increase HR Postural changes in pulse Hypotension Decrease in diuresis Decrease in capillary filling Lab data: Na, urea, osmolarity
Hydro-electrolytic management Delay recuperation of patients Is a frequent cause of morbidity Is a cause of death MC in surgical patients
Combined depletion w/ dehydration Depletion vs dehydration
Depletion (dehydration) Affects intravascular & interstitial space (ICF &
interstitial) Loss of isotonic fluid (hypotonic) Fast velocity of development of disorder (slow) Shock hemodynamic state (normal)
Fluid therapy w/ isotonic solution (w/ hypotonic solution) Velocity of TX in minutes (infusion in hours)
Hyponatremia Hypokalemia Loss in surgical patients
Internal loss Sequestration of liquids
Severe pancreatitis Sepsis Metabolic ileus Intestinal obstruction
Blood loss Transoperative hemorrhage GI hemorrhage Hemorrhagic phase of DIC Fractures of the pelvis & long bones
External loss Evaporation via integral barriers
Hyperthermia Hyperventilation
Evaporation via loss of barriers Extensive burns Transoperative exposure of serous cavities Open abdomen for management of abdominal sepsis
GI loss V/D Drainage or GI aspiration Spontaneous fistulas Crohn’s disease Posttraumatic fistulas Surgical fistulas: external derivation of biliary tree Ileostomy, colostomy, jejunostomy, duodenostomy
Loss d/t drains Peritoneal drains Pleural drains Drains in spaces created by surgical dissection
UTI loss Osmotic polyuria (mannitol, hyperglycemia) Use of diuretics
Fluid therapy: restoration of liquids Fluid therapy in shock is based on the rescue & maintenance of renal
function, considering diuresis as a monitor of perfusion Depending on the type & rate of loss, establish the type & speed of
replacement The correction of intravascular volume depletion must be made
in minutes, while a hydro-electrolytic correction (which is not life-threatening) must be made w/in 24-48 hours
In patients w/ hypovolemia, 50% of the volume is given in the
first administration, and then given in thirds or quarters Crystalloids
Establish circulating volume (Na concentration) Short half-life (30-40 sec) Spread to interstitium (edema) Dilution of plasma proteins Contains water, electrolytes, a/o sugars Prepared
NaCl 0.9% Dextrose 5% Ringer’s lactate
Colloids Increase plasma osmotic pressure & retain water in intravascular
space Prolonged half-life Establish circulating volume Natural colloids
Plasma Albumin
Hyper-oncotic Half-life of 24 hours High cost Risk of anaphylaxis
Synthetic colloids Gelatin: half-life of 4-5 hours
Haemaccel: 330-390 mmHg Gelofusin: 465 mmHg
Dextran Dextran 40 Dextran 70
Heta-almidon Penta-almidon
Combination of crystalloids & colloids Parameters of suspending liquids
Decrease in HR below 120 BP Normal urinary flow High pressure of filling
Acute loss Pathologic: replenish volume-by-volume w/ Hartmann solution Insensitive: 0.5 ml/kg/hr + 10% for each C of temperature above 38C
Care in management w/ liquids H2O: During input of load, can auscultate frequently wheezing in the
pulmonary fields that can indicate volume overload Na: The correction of sodium is not done rapidly, but the max changes per
day in serum sodium concentration is 8 mEq/L/d for women (10 for men) K: Via peripheral vein, the max concentration of K per L of solution is 40
mEq/L, and the max velocity of input is 10 mEq/hour. No input of K+ in
the immediate postop period Dextrose: in patients w/ metabolic response in the lesion, 100 g/d of
dextrose limits 50% of catabolism of proteins (Gamble principle), which is approximately 1.5 g/kg/day. In cases of hyperglycemia, dextrose solutions can initiate when the glucose level reaches 250 mg/dL, and an insulin scheme is established
NUTRITION IN THE SURGICAL PATIENT 40-70% of hospitalized patients in any moment, have malnutrition
MC is marasmus-type malnutrition (protein-caloric malnutrition) Input of preop nutrition during 7-10 days diminishes morbidity & mortality
associated w/ surgery Surgical patients present 3 problems in basic nutrition
Secondary malnutrition to prolonged postop fast related to postop complications
Chronic malnutrition in surgical candidates that have lost weight as a consequence of their disease
High energy demands in polytraumatic & burn patients, due to the severity of their disease
Transcendence of salvation of proteins Intestinal mucosa, immune system, and renal metabolism requires high
quantities of glutamine Proteins meet a un-substitutable biologic function Its consumption to obtain energy corresponds to loss of specific
functions Malnutrition
Any state in which nutritional deficit affects health Disorder of body composition characterizes by excess of ECF & deficit of
muscle mass Causes of malnutrition in surgery
Previous & prolonged situation of fast & semi-fasting Uncompensated increase in nutritional requirements taxing the disease Malattention on the part of professionals in attending to the patient Complication of medical/surgical TX of disease Nutrients administered via an inadequate route
Consequences of malnutrition Affect musculature Affect function of respiratory muscles Facilitate the presence of cardiac abnormalities (loss of muscle mass &
decrease in CO) Harmful effects over mass & function of enterocytes & colonocytes Delay of scarring of wounds Alter immune response
Evaluation of nutritional status Capacity of protein synthesis
Visceral: pre-albumin, transferring Muscular: nitrogen balance
Immunity
Lymphocyte count Response to Ag Markers of inflammation
Organic reserve Fat: impedance Muscle: force
Visceral proteins The mass of visceral proteins can be evaluated from serum concentrations
of transport proteins synthesized in the liver Albumin is easy to determine
2.8-3.5 g/dL = mild malnutrition 2.1-2.7 g/dL = moderate malnutrition < 2.1 g/dL = severe malnutrition
Preoperative nutritional support Conserve or improve nutritional status before surgery Diminish perioperative morbidity & mortality Prevent postoperative malnutrition Prevent depletion in hypercatabolic states Contraindications
Hemodynamic instability Not recuperable patient
Parenteral nutrition Administration of nutrients via venous route w/ specific catheters to cover
the energy needs & maintain an adequate nutritional status in those patients where enteral route is inadequate, insufficient or contraindicated
TPN = when it is the only input of nutrients PPN (partial parenteral nutrition) = when other inputs of nutrients as well The complications in perfusion of parenteral nutrition are related to the
catheter, the manipulation of system, and the solution of parenteral nutrition Peripheral parenteral nutrition
In smaller veins In relatively low requirements For short time (max 2 weeks) Indications
Intestinal inflammatory diseases Malabsorption syndrome Pancreatic insufficiency Gastrectomy Radiotherapy & chemotherapy
Central parenteral nutrition Used in patients w/ greater requirements Resectable gastric cancer, in which you can recuperate nutritional
status as fast as possible In ICU
Digestive indications Neonatal, congenital, or acquired pathologies Surgical interventions Intestinal malabsorption
Severe acute pancreatitis Post-chemotherapy, post-radiation Intestinal pseudo-obstruction Irreversible vomiting Cheilous ascites Chylothorax
Extra-digestive indications Hypercatabolic state: sepsis, polytruauma, burns, neoplasias,
transplants, cachexia Pre-term newborns of low weight Visceral failure: hepatic insufficiency or acute renal insufficiency Oncology: severe mucositis
Proteins In fasting, catabolized 75g of muscle protein
Need to ingest 1-1.5g of protein per kg to maintain reserve 6.25 g of protein contains 1 g of nitrogen
CHO Constitutes 50% of caloric input in diet Each g of monohydrate dextrose inputs 3.4 calories W/ administration of 100-150 g of glucose in fasting, which is 50% of
protein Lipids
Require 25g to favor absorption of lipid soluble vitamins In fast, break down 160g of fat in 24 hours Oxidation of 1g of lipids yields 9 Kcal
Oligoelements: Zn, Cu, Cr, Se Deficit of zinc doesn’t help wound scarring Cr potentiates action of insulin Se is an antioxidant Mn is a procoagulant
Iron Men: 1000mg (women: 300-500mg) Parenteral dosage is 0.5-1.0 mg/day
Vitamin C Cofactor in collagen synthesis Participates in tissue reparation
Standard formulas Dextrose = 10-25% of central parenteral nutrition (5% of peripheral) AA = 4.25% of central parenteral nutrition (same) Na+ = 36.5 mEq/L or a K+ = 36.5 mEq/L
Advantages of parenteral nutrition 100% absorption Continuous infusion Very complete Does not use digestive use, which is still useful in a specific group of
patients Disadvantages of parenteral nutrition
Alter the quality of mucosa & intestinal transit, producing bacterial
translocation & problems of eating later More expensive: require major manipulation, monitorization & special
physical place Complications are grave, w/ infection of the central venous catheter, w/
sepsis for nosocomial microorganisms Require change in all of central venous system
Increment of caloric dose Elective surgey = 10% of stress factor Trauma = 10-30% of stress factor Sepsis = 50-80% of stress factor
Enteral nutrition Technique to support nutrition which consists of administration of nutrients
Directly into GI tract, find tube in liquid environment Indications
GI tract is functional but… Not able to use optimally nutrients PO
d/t severe D, short intestinal syndrome If the needs are extremely increased and the patient cannot cover
them w/ ingestion burn patients, malnutrition
When the patient cannot swallow Advantages
Most physiologically normal means of input More trophic stimulation of GI tract Cheaper Easier to care for Require less invasive procedures for the patient
Contraindications Intestinal obstruction Intolerance to formula Diarrhea Gluten enteropathy Hypoperfusion
Routes of choice NG tube Trans-pyloric tube: nasoduodenal or nasojejunal Gastrostomy
Percutaneous endoscopy Radiology Surgery
Jejunostomy Types of solution
Polymeric Ensure/ Ensure fiber Osmolite 1 cal/cc (low osmolarity) Pulmocare (low in CHO high in proteins) Glucal Bott (low in CHO) Nephro, Suplena (nephropathy)
Advera (1 cal/cc) Alitreg (metabolic distress) Sevite 1 cal/cc (low osmolarity, to correct D or constipation)
Peptidic: when proteins are hydrolyzed Elemental: when proteins are in the form of AA
Complications Bronchoaspiration Infectious Metabolic (inadequate nutrients) Mechanic (obstruction of NG tube)
For specific pathologies Hepatic: decrease dosage of lipids or suppress input Pneumo: decrease CHO & increase lipids Renal: decrease input of proteins, Na, K, P, Mg Sepsis: increase immuno-nutrients, input AA for catabolism
Immuno-nutrition Arginine
High demand in catabolic states and in growth Improves the response of T cells to mitogens Improves the response to late sensitivity
Glutamine Energetic substrate of enterocyte Its precursor, glutamate, represents 61% of AA in plasma Favors support of enteral mass & mucosal integrity
Nucleotides Forms part of nucleic acids Are necessary for production of T cells, epithelial cells, &
interleukins Omega-3 FA
Does not produce Immunosuppression of Burns: increase proteins and non-protein calories