Embed Size (px)
Citation preview

THEALABAMAWISEWOMAN
POLICYANDPROCEDUREMANUAL
December2014

2
TableofContents
INTRODUCTION…………………………………………………………………………………………………………………………………........5
Purpose………………………………………………………………………………………………………………………………………..5
Mission…………………………………………………………………………………………………………………………………………5
FundingResponsibilites…………………………………………………………………………………………………………………5
ADPHRESPONSIBILITIES…………………………………………………………………………………………………………………………6
PROVIDERRESPONSIBILITIES…………………………………………………………………………………………………………………7
HIPAA……………………………………………………………………………………………………………………………………………7
PatientRights………………………………………………………………………………………………………………………………...7
InformedConsent……………………………………………………………………………………………………………………………7
PatientEnrollment………………………………………………………………………………………………………………………….8
RecordKeeping………………………………………………………………………………………………………………………………8
ReportingRequirements…………………………………………………………………………………………………………………8
Contracts/Reimbursement……………………………………………………………………………………………………………..8
ALWISEWOMANPATIENTFLOW……………………………………………………………………………………………………………..9
IntegratedOfficeVisit…………………………………………………………………………………………………………………….9
CVDScreening………………………………………………………………………………………………………………….9
RiskReductionCounseling……………………………………………………………………………………………….10
HealthyBehaviorOptionsSession……………………………………………………………………………………10
FollowUpAFTERIntegratedOfficeVisit……………………………………………………………………………………….10
NutritionalCounseling…………………………………………………………………………………………………….10
OneMonthMedicalFollowupOfficeVisit………………………………………………………………………..10
FollowupAssessment……………………………………………………………………………………………………..10
FollowUpServicesthroughtheALWISEWOMANSocialWorker…………………………………………………..10
ALWISEWOMANFLOWCHART………………………………………………………………………………………………………………12
ALWISEWOMANSCREENINGTESTS……………………………………………………………………………………………………….13
Height/Weight/BMI……………………………………………………………………………………………………………………..13

3
FastingLipidProfile…………………………………………………………………………………………………………………….13
FastingGlucose……………………………………………………………………………………………………………………………13
A1C……………………………………………………………………………………………………………………………………………..13
BloodPressure…………………………………………………………………………………………………………………………….13
HYPERTENSIONPOLICY…………………………………………………………………………………………………………………………14
ALERTVALUEPROTOCOL………………………………………………………………………………………………………………………15
ALERTANDDISEASE‐LEVELVALUES…………………………………………………………………………………………………….16
Glucose………………………………………………………………………………………………………………………………………..16
Cholesterol/Lipids……………………………………………………………………………………………………………………….16
BloodPressure…………………………………………………………………………………………………………………………….16
UNCONTROLLEDHYPERTENSIVEPARTICIPANTS………………………………………………………………………………….17
DATACOLLECTIONFORMS…………………………………………………………………………………………………………………....18
Purpose………………………………………………………………………………………………………………………………………18
DataCollectionRequirements………………………………………………………………………………………………………18
ALWWDataCollectionForm:BASELINE/RISKREDUCTION…………………………………………………………18
HICF1500BillingForm……………………………………………………………………………………………………………….18
ALWWHealthCoachingContactForm…………………………………………………………………………………………19
HowtoChangePatientInformation………………………………………………………………………………………………19
BILLINGANDREIMBURSEMENT…………………………………………………………………………………………………………….19
Requirements……………………………………………………………………………………………………………………………...19
IntegratedOfficeVisitReimbursement…………………………………………………………………………………………19
ClinicalLabTests…………………………………………………………………………………………………………………………20
RiskReductionCounselingCodes…………………………………………………………………………………………………20
NutritionalCounselingSessionCodes…………………………………………………………………………………………...20
MedicalFollowUpOfficeVisitCodes…………………………………………………………………………………………….20
APPENDICES……………………………………………………………………………………………………………………………………………21
A:NationalClinicalGuidelines,p.22‐25
B:AuthorizationforServices,p.26‐27
C:ABCCEDP/ALWWInformedConsent/ReleaseofInformation,p.28‐29

4
D:HypertensionFlowchart,p.30
E:ProgramDataForms,p.31
Baseline/RiskReductionForm,p.31‐32
ALWWContactForm,p.33‐34
HomeMonitoringBPAgreementContract,p.35
HICF1500Form,p.36
F:CPT/ReimbursementTable,p.37
G:ClearanceLetterforParticipationinPhysicalActivity,p.38
H:BloodPressureMeasurementProcedure,p.39
I:NEWLEAFHealthCoaching,AlabamaExpandedFoodandNutritionEducationProgram(EFNEP),Health
CoachingandLSPFlowChart,Community‐BasedResources,p.40‐44

5
INTRODUCTION
PURPOSE
In1993,theCentersforDiseaseControlandPrevention(CDC),withintheDivisionforHeartDiseaseandStrokePrevention(DHDSP),wasgivenauthoritybyCongresstofacilitatetheWISEWOMAN(Well‐IntegratedScreeningandEvaluationforWomanAcrosstheNation)program,withtheclearaimsofhelpingwomenages40to64yearstounderstand:1)theirriskfactorsfordevelopingCVDand/orotherchronicdiseasessuchasdiabetes,hyperlipidemia,andhypertension,and2)howtomakelifestylechangestopreventdiseaseandtoproduceoverallhealth.
Inthesummerof2013,CDCofferedtheopportunityforfederalfundingtostateswithcurrentbreastandcervicalcancerscreeningprogramstoapplyforadditionalfundingforWISEWOMANProgramservices.TheAlabamaBreastandCervicalCancerEarlyDetectionProgram(ABCCEDP)oftheAlabamaDepartmentofPublicHealth(ADPH)appliedforandwasgrantedfundingtoconducttheAlabamaWISEWOMANProgram(ALWISEWOMAN),operatingfromJuly01,2013throughJune29,2017.TheAlabamaDepartmentofPublicHealthisaccountabletotheCDCfortheappropriateuseofthesefunds.
MISSION
ThemissionofALWISEWOMANistomanageandreducecardiovasculardiseaseriskfactorsamongunderservedwomen,ages40to64inMobileCounty,Alabama.ALWISEWOMANwillprovidecomprehensivecardiovasculardiseaseriskfactorscreeningsforwomen40‐64receivingbreastandcervicalcancerscreeningsthroughABCCEDPatFranklinPrimaryHealthCareCenter(FPHC)andMobileCountyHealthDepartment(MCHD).Allprogramcomponentsarerelatedtothedeliveryofscreeninganddiagnosticservices,anddeliveryofsupporttothoseinneed.
AmongMobileCountywomen,ourtargetpopulation,deathratesarehighercomparedtoUSwomenforallmajorcauses;CVD‐relateddeathratesare19%higher,diabetes‐relatedratesare37%higher;canceris5%higher,cardiovasculardiseaseis14%higherandstroke‐relateddeathratesare36%higher.Alabama’s2010age‐adjustedmortalityratesreportedlargehealthdisparitiesexistingbetweenBlackwomenandWhitewomenlivinginMobileCounty.ComparedtoMobileCountyWhitewomen,MobileCountyBlackwomenhad:1)a31%highermortalityratefromCVD,2)a117%highermortalityratefromdiabetes,and3)a60%higherratefromstroke.Thesedatademonstrateasignificantneedtomonitorthecardiovascularhealthofat‐riskMobilewomenandtoprovidethemnecessaryskills,likethosefoundinevidence‐basedlifestyleprograms,forimprovingandmaintaininghealthybehaviors.
FUNDINGREQUIREMENTS
CDCrequires60%ofADPHgrantfundsbeusedforexpensesdirectlyforALWISEWOMANclinicalservices,suchas:
Screeningclinicalandbloodtestswithdiagnostictestingasneeded RiskAssessmentandRiskReductionCounseling NutritionalCounseling Reviewandinterpretationofclinicalandbloodtests,bothinwritingandorally SocialWorkServices Referralforcommunitysupportservicesusedtomaximizeparticipationinscreeningandrisk
reductionservicesClinicalservicesmustbeprovidedinaccordancewithNationalClinicalGuidelineslistedinAppendixA.

6
CDCalsorequiresnomorethan40%ofgrantfundsbeusedforactivities/servicesnotdirectlybenefitingALWISEWOMANparticipants,suchas:
Managementactivities* Recruitmentandoutreach Professionaldevelopment Datamanagement,qualityassurance,andqualityimprovement Developmentandmaintenanceofpartnerships Communityengagement Surveillanceandevaluationactivities Travel Evaluation
*Nomorethat10%ofADPHfundscanbeusedforadministrativecosts.The10%administrativecostsareconsideredtobepartofthe40%distribution
Note:NofundsmaybeusedtopayforinpatienthospitalservicesforALWISEWOMANparticipants
ADPHRESPONSIBILITIES
CDCprovidesaframeworkandguidelinesthatADPHischargedwithfollowingasarecipientofCDCWISEWOMANfunds.TheseguidelinesareimplementedthroughADPHincombinationwithADPHfiscalandprogrammaticguidelinesandestablishthebasisforcontractedproviderstoplan,implement,andevaluatetheprovisionofservices.ADPHisresponsibletoensureALWISEWOMANprovidersprovidequalitypatientcareinallfacetsoftheprogram,including:1)allcomponentsoftheIntegratedOfficeVisit,2)allALWISEWOMANSocialWorkerfollowupservices,and3)therescreeningservicesat12‐18months.
ADPHhascontractedwithtwohealthcareagencies,FranklinPrimaryHealthCareCenterandtheMobileCountyHealthDepartment,toprovidefortheALWISEWOMANProgram,thefocusofwhichiscardiovasculardiseaseprevention.
ADPHensurescontractedprovidersuseestablishedCDC‐approvedprotocolsforALWISEWOMANservicedelivery.
ContractedprovidersareaccountabletotheADPHfortheappropriateuseoffunds. SupervisionofALWISEWOMANstaffwillbeperintuitionalguidelinesandincompliancewithstate
licensurerequirements.
Inadditiontoprovidingfinancialsupport,ADPHwillassistcontractedprovidersthrough:
GuidanceinhiringoftwolicensedsocialworkerswhowillserveasALWISEWOMANSocialWorkers,oneperfacility
Professionaleducation,programdevelopmenttrainings,datamanagementtrainings,andmeetingsforcontractedproviderstaff
Technicalassistancewithprogramplanning,development,implementation,operations,andevaluationinaccordancewithfederalandstategovernmentdirectives
Programguidanceinimplementingandmaintaininganelectronictracking/follow‐upandreferralsystemforthedeliveryofprogramservices
Technicalassistancewithqualityassuranceandimprovementactivities Assistancewithenhancingand/ordevelopingpublic/participanteducationactivities Assistancewithprogrampromotionandrecruitmentofeligibleparticipants Standardizedformsandtemplatesforallmandatoryfiscalandprogrammaticreportingrequirements List(s)ofallowableCPTcodesandreimbursementratesforprogramservices
7
Annualupdatesofeligibilityguidelinesincludingincomeeligibility Regularprograminformation/updatesviae‐mail,conferencecalls,trainings,webinars,meetings,and
sitevisits
PROVIDERRESPONSIBILITIES
TheAlabamaWISEWOMANPolicyandProcedureManualprovidesprogramguidanceforALWISEWOMANproviders,FranklinPrimaryHealthCareCenterandtheMobileCountyHealthDepartment,indeliveringappropriatescreeningservicesforALWISEWOMANparticipants.
A. HIPAA
ALWISEWOMANprovidersarerequiredtofollowtheU.S.DepartmentofHealthandHumanServicesPrivacyRuleandimplementtherequirementsoftheHealthInsurancePortabilityandAccountabilityActof1996(“HIPAA”).TheStandardsforPrivacyofIndividuallyIdentifiableHealthInformation(“PrivacyRule”)establishesasetofnationalstandardsfortheprotectionofcertainhealthinformation.TheU.S.DepartmentofHealthandHumanServices(“HHS”)issuedthePrivacyRuletoimplementtherequirementoftheHealthInsurancePortabilityandAccountabilityActof1996(“HIPAA”).ThePrivacyRulestandardsaddresstheuseanddisclosureofindividuals’healthinformation—called“protectedhealthinformation”byorganizationssubjecttothePrivacyRule—called“coveredentities,”aswellasstandardsforindividuals'privacyrightstounderstandandcontrolhowtheirhealthinformationisused.WithinHHS,theOfficeforCivilRights(“OCR”)hasresponsibilityforimplementingandenforcingthePrivacyRulewithrespecttovoluntarycomplianceactivitiesandcivilmoneypenalties.
B. PatientRights
ALWISEWOMANcontractedprovidersarerequiredto:
Protecttheuse/disclosureofanywoman’smedicalorsocialinformationofaconfidentialnature Considermedicalservicesandinformationcontainedinmedicalrecordsasconfidential Disclosethewoman’smedicalrecordstocontractedABCCEDPphysiciansormedicalfacilitiesaccepting
thewoman Disclosethewoman’smedicalrecordstotheABCCEDPStateOffice Disclose—insummaryorotherform—informationwhichdoesnotidentifyindividualsorproviders,if
suchinformationisincompliancewithapplicablefederalandstateregulations,andtheexchangeofmedicalrecordinformationisinkeepingwithestablishedmedicalstandardsandethics
C. InformedConsentParticipantsoftheALWISEWOMANagreetohavepersonalandfamilyhistoryinformationcollectedandsharedwiththeADPH. BysigningtheALWISEWOMANconsentform,theparticipantgrantspermissiontohealthcare
providerstoreportallinformationconcerningscreeningstestsandprocedures,treatment,patientnavigationservices,andanyrelatedcareoractivitytoADPH.
ThisformmustbecompletedatthetimewhentheparticipantenrollsintheALWISEWOMANProgram. Anewconsentformmustbesignedateachannualrescreening.Verbalconsentatthetimeofannual
rescreeningisnotacceptable.SeeAppendixB,AuthorizationforServicesForm
D. PatientEnrollment
ForenrollmentintoALWISEWOMAN,thescreeningprovidermustcompletethefollowing:

8
Determineeligibilitybasedonincome,age,andinsurancestatus ObtainatrackingnumberforallWISEWOMANparticipantsthroughtheweb‐basedEnrollmentsite
Med‐IT@http://Med‐ITweb.comduringthepatient’sinitialorannualvisit InordertocreateaWISEWOMANtrackingnumberinMed‐IT,firstselectthecorrectpatientor
createanewpatientandthenclick“SetAppointment”ontheMed‐ITEnrollmentPage ThencheckWISEWOMANboxonthe“ScreeningGuidelines”pagealongwithBCC,thencreatean
appointmentdate TheWISEWOMANtrackingnumberwillhavea“W“beforethenumber
E. Record‐Keeping
Copiesofthesignedpatientconsentforms,theWISEWOMANbaselinedata/riskreductionform,andallALWWContactformsaretobeenteredintothepatient’spermanentmedicalrecord/E.H.R.maintainedbytheprimaryprovider.
Theprovidermustdocumentalleducationprovidedtoparticipants. Theprovidermustestablishasystemfortrackingwomenwhichnotifiesherwhenitistimeforroutine
screening,followups,rechecks,andrescreeningvisits. EnsureallwomenfoundtohaveALERTvaluesarereferredformedicalevaluationandtreatment
immediatelyorwithin7days,theintegratedofficevisitcountingasDAY1andthatALERTworkupsarecompletedanddocumentedintheEHR
EnsureallwomenfoundtohaveABNORMAL/DISEASE‐LEVELvaluesarereferredformedicalevaluationandtreatmentimmediatelyorwithin30days,theintegratedofficevisitcountingasDAY1,andthatthisfollowupiscompleteanddocumentedintheHER
F. ReportingRequirement
ToreceivereimbursementbyADPH,thescreeningproviderwillsubmit,bythe15thofthemonth,thefollowing:
ALWISEWOMANDataCollectionForm:Baseline/RiskReduction AnyALWISEWOMANContactForms TheHealthInsuranceClaimForm(HIFA1500)completewithallservicescodesanddateofservice
G. Contract/Reimbursement
ALWISEWOMANprovidersmustmaintaincurrentandapplicablefederaland/orstatelicenses. Allscreeningprovidersmustagreetoaccepttheprogram‐approvedreimbursementfeeaspaymentin
fullforservicesrendered.Thatreimbursement,bylaw,cannotbeoverthecurrentMedicarereimbursementrate.SeeAppendixFforReimbursementTable
H. QualityAssurance/QualityImprovement
ProvidersarerequiredtoparticipateinqualityassuranceandqualityimprovementactivitiesasdeemedappropriatebytheADPH.Thisincludescompliancewithcontractualperformancemeasuresandparticipationinscheduledsitevisitsandprofessionaldevelopmenttrainings.

9
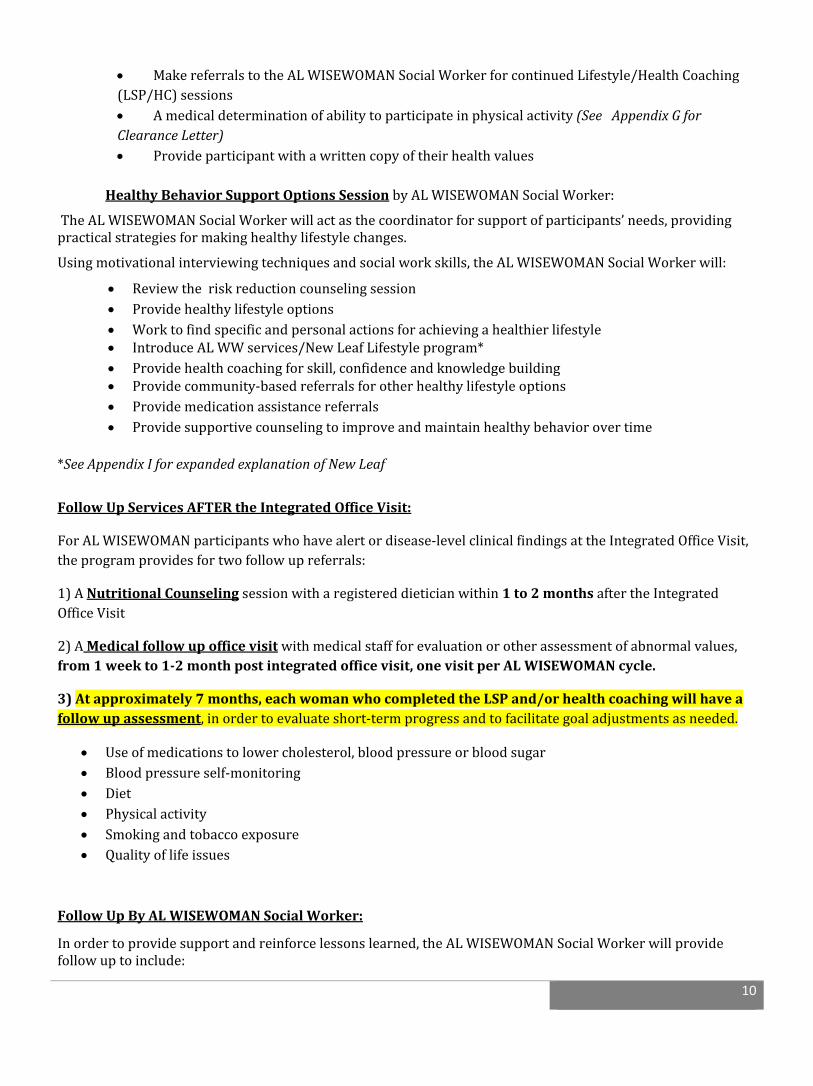
ALABAMAWISEWOMANPATIENTFLOW‐seeflowchartonpage12
ALWISEWOMANofferscurrently‐enrolledABCCEDPwomen,ages40to64,thefollowing:
Cardiovasculardiseaseriskfactorscreeningstodetermineriskfactors Riskreductioncounselingtohelpwomenundertheirrisksanddiscusstheparticipant’sreadinessto
embracemorehealthfulbehaviors Healthcoachingandsupporttohelpwomendiscoverhealthylifestylebehaviorstoprevent,minimize,
ordelaytheonsetofchronicdisease
Theprogramincludesabaselinescreeningvisitfollowedbyarescreeningvisitin12‐18months.
BaselineScreening/TheIntegratedOfficeVisit
ALWISEWOMANparticipantswillreceiveanIntegratedOfficeVisitwhichprovides:1)theirannualbreastandcervicalcancerscreeningsand2)cardiovasculardisease(CVD)work‐uptodeterminetheirriskfordevelopingchronicdiseasessuchasheartdisease,stroke,anddiabetes.
ALWISEWOMANparticipantswillbecalledforappointmentschedulingandwillbeaskedtobefastingfortheirscreeninglabtests.
TheIntegratedOfficeVisit
TheIntegratedOfficeVisitconsistsoffourmajorsections:
1. Annualbreastandcervicalcancerscreenings2. CVDriskfactorscreeningtests3. Risk‐reductioncounselingbymedicalstaff4. AHealthyBehaviorSupportOptionsSessionbytheALWISEWOMANSocialWorker
CVDriskfactorscreeningtestsinclude: Highbloodpressure(2bloodpressurereadingswithacalculatedaverage) Highcholesterol(Fastinglipidpanel) Diabetes(Fastingglucosefornon‐diabeticparticipants*;A1CbyPOCfordiabeticparticipants) Height,WeightandBMI,waistandhipmeasurements Smokingstatus Medicalhistoryandriskfactorassessment Healthylifestyleassessment Physicalandemotionalwell‐beingassessment
*Ifnon‐diabeticpatientisnotfastingattimeofappointment,anA1CbyvenipuncturewillbedrawnandtestedatareferencelabapprovedforNGSPcertifiedandstandardizedDCCTassay.
TheRiskReductionCounselingSessionbymedicalstaffwillinclude: Reviewmedicalhistory,healthylifestyleassessment,labandclinicalresults ConductaCVD10‐yearriskcalculationanddiscussCVDrisks Determinehypertensivepatientswiththeirtargetbloodpressurereading Determineparticipant’spriorityareasandreadinesstochange Discussdietandphysicalactivity
10
MakereferralstotheALWISEWOMANSocialWorkerforcontinuedLifestyle/HealthCoaching(LSP/HC)sessions Amedicaldeterminationofabilitytoparticipateinphysicalactivity(SeeAppendixGforClearanceLetter) Provideparticipantwithawrittencopyoftheirhealthvalues
HealthyBehaviorSupportOptionsSessionbyALWISEWOMANSocialWorker:
TheALWISEWOMANSocialWorkerwillactasthecoordinatorforsupportofparticipants’needs,providingpracticalstrategiesformakinghealthylifestylechanges.
Usingmotivationalinterviewingtechniquesandsocialworkskills,theALWISEWOMANSocialWorkerwill:
Reviewtheriskreductioncounselingsession Providehealthylifestyleoptions Worktofindspecificandpersonalactionsforachievingahealthierlifestyle IntroduceALWWservices/NewLeafLifestyleprogram* Providehealthcoachingforskill,confidenceandknowledgebuilding Providecommunity‐basedreferralsforotherhealthylifestyleoptions Providemedicationassistancereferrals Providesupportivecounselingtoimproveandmaintainhealthybehaviorovertime
*SeeAppendixIforexpandedexplanationofNewLeaf
FollowUpServicesAFTERtheIntegratedOfficeVisit:
ForALWISEWOMANparticipantswhohavealertordisease‐levelclinicalfindingsattheIntegratedOfficeVisit,theprogramprovidesfortwofollowupreferrals:
1)ANutritionalCounselingsessionwitharegistereddieticianwithin1to2monthsaftertheIntegratedOfficeVisit
2)AMedicalfollowupofficevisitwithmedicalstaffforevaluationorotherassessmentofabnormalvalues,from1weekto1‐2monthpostintegratedofficevisit,onevisitperALWISEWOMANcycle.
3)Atapproximately7months,eachwomanwhocompletedtheLSPand/orhealthcoachingwillhaveafollowupassessment,inordertoevaluateshort‐termprogressandtofacilitategoaladjustmentsasneeded.
Useofmedicationstolowercholesterol,bloodpressureorbloodsugar Bloodpressureself‐monitoring Diet Physicalactivity Smokingandtobaccoexposure Qualityoflifeissues
FollowUpByALWISEWOMANSocialWorker:
Inordertoprovidesupportandreinforcelessonslearned,theALWISEWOMANSocialWorkerwillprovidefollowuptoinclude:

11
Supportivecounselingandfollowuponprogresstowardgoals Aninvitationtomonthlysupportmeetingsheldthroughoutthecommunity Followupcallstobemadetoparticipantsbeginningorchanginghypertensionmedicationregimewithin10
days Followupforallcommunityreferralswithin10workingdaysofappointment Schedulingofrescreeningappointmentat12to18months Remindercallsforrescreeningappointment Quarterlycontact,ataminimum Followupasneeded
12
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.

13
ALWISEWOMANSCREENINGTESTS:
ProvidersmustensureallwomenenrolledinALWISEWOMANwithALERTordisease‐level(abnormal)screeningresultshaveaccesstoappropriatemedicalevaluationinthetimeframespecified,thatitiscomplete,andthatisdocumentedintheparticipant’sEHR
ProvidersmustcomplywithCDCNationalClinicalGuidelinesandallADPHprotocols.(SeeAppendixA) Providersmustensureparticipantsarefasting,totheextentisitpossible,fortheirlabtests.Tobe
consideredfasting,awomanmustnothaveneatenortakeninfluidsfor9hours Providersareencouragedtoestablishatrackingsystemthatincludesreminderstoparticipantstokeep
theirappointmentsfortheofficevisit,mammography,laboratorybloodtests,andotherrelatedscreeningtestsorprocedures.
Height/Weight/BMI/Waist/Hipmeasurements:
EachparticipantmusthaveaheightandweighttakenwithBMIcalculated,alongwithhipandwaistmeasurementswhendesired.
FastingLipidProfile:
ThisfastingprofilewillbeorderedinlieuoftotalcholesterolandHDL‐CsinceALWISEWOMANparticipantsaretobefasting*.Thisprofileincludesatotalcholesterol,LDL‐cholesterol,HDL‐cholesterol,andtriglycerides.
*Forthosewomenwhoarenotfasting,checkonlytheTotalcholesterolandHDL‐cholesterol.
FastingGlucose:
Allparticipantswhoarenotdiabeticwillbescreenedbyfastingglucose.Intheeventthatafastingglucosecannotbedrawnforanon‐diabeticparticipant,anA1CpercentagecanbetestedbutONLYifthebloodiscollectedbyvenipunctureandtestedinalabbyNGSPcertifiedandstandardizedDCCTassay.
NOTE:Afastingglucoseisnotdoneonanyparticipantdiagnosedwithdiabetes;instead,anA1Cisdrawn
A1C:
ParticipantspreviouslydiagnosedwithdiabeteswillreceiveanHbA1Cbyministick.
BloodPressure:Eachparticipantmusthavetwobloodpressuremeasurementstakenandtheaveragecalculated.Theaveragedbloodpressurenumberisthefinalbloodpressurereading.NOTE:Whenthesystolicanddiastolicbloodpressurereadingsfallintotwodifferentcategories,thehighercategoryshouldbeusedtoclassifythebloodpressurelevel.Forexample,160/80mmHgwouldbeStage2hypertension(highbloodpressure).Thehigherreadingofthesystolicbloodpressureof160mmHgdeterminestheclassificationofStage2hypertension.
14
HYPERTENSIONDetectionandControl
Long‐termobjectivesfortheWISEWOMANProgramincludedeveloping“systemsthat
monitor,improve,andsustainthecardiovascularhealthofthepopulationserved.”(Version2,WISEWOMANTechnicalAssistanceandGuidanceDocument,page7)Preventing,wheneverpossible,andcontrollinghypertensionarecriticalstepsinaccomplishingthatbroadgoal.
TheAlabamaWWProgramhasmadethedetection,treatment,andmanagementofhypertensionamongparticipantsamajorfocus.ByfollowingscreeningguidelinesrequiredbyCDC,weanticipateidentifying:1)un‐diagnosedhypertensiveparticipants,2)hypertensivewomenwhohavebeendiagnosedinthepastbuttheirdiseaseisuncontrolled,and3)diagnosedhypertensivewomenwhoneedregularmonitoringandmaintenanceinordertoreducefurtherriskforseriouscardiovascularcomplications.
ManagementofStage1andStage2hypertensionisacomplexprocessinvolvingmanyhealthcareproviders:physicians,physicianassistants,nurses,socialworkers,dietaryandpharmacystaff,andmentalhealthpersonnel.Theseprofessionalsareneededtoensurethebestpossibleoutcomesforhypertensivepatients,andAlabamaWISEWOMANisdesignedtoinvolvethisteamintheinstructionandmanagementofitshypertensivewomen.
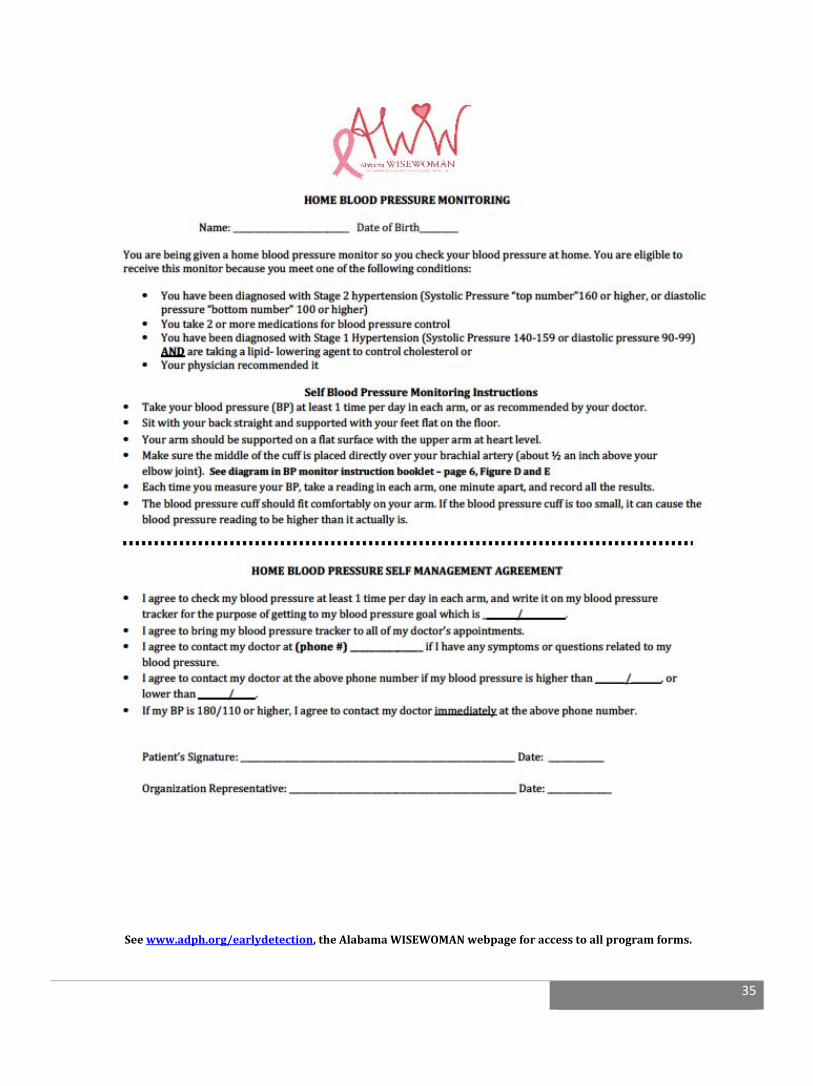
Inadditiontoteam‐basedefforts,self‐monitoringbloodpressure(SMBP)deviceswillbeavailabletoeligibleWWparticipantsasanotherpracticalandconvenienttoolfortrackingandmonitoringhypertension,outsideofamedicalsetting.Thesemonitorswillbeprovidedtoparticipantsfree‐of‐chargewho:1)havebeendiagnosedwithStage2hypertension,or2)havebeendiagnosedwithStage1hypertensionandwhotakeacholesterolorlipid‐reducingmedication,or3)whotaketwoormorebloodpressuremedications,or4)arerecommendedbytheirphysician.
Inordertoreceiveamonitor,AlabamaWWparticipantsmustagreetothefollowingstipulations:
Tochecktheirbloodpressureatleastonetimeperday,ineacharm,andrecordthe
results Tobringintheirbloodpressuretrackertoalldoctorappointmentssothattheir
readingsmaybesharedwiththeirhealthcareprovider Tocontacttheirhealthcareprovideriftheyhaveanysymptomsorquestionsrelatedto
theirbloodpressurereadings Tocontacttheirhealthcareprovideriftheirbloodpressurereadshigherthana
specifiedlevelasdefinedbytheirphysician Toimmediatelycontacttheirhealthcareprovideriftheirbloodpressurereadingis
180/110orhigher
ProtocolsformanagingallaspectsofhypertensionarefoundintheAlabamaWWPolicyand
ProcedureManual,inthefollowingdocuments: TheAlertValueProtocol,page15 ProceduresformanagingDisease‐levelhypertensionlevels,pages16‐17 TheAlabamaWWHypertensionFlowChart,page30 TheHomeBloodPressureMonitoringSelf‐ManagementPolicyandAgreement,page35

15
ALERTVALUEPROTOCOL:
Alertvalues(veryhighvalues)forbloodpressureandglucose,singlyorincombination,cancausedamagetothebloodvessels(arteriosclerosis),brain(stroke),heart(heartattack),kidneys(renalfailure),andeyes(compromisedvision/blindness).
Policy:
TheProviderisresponsibleforensuringWWparticipantswithalertvaluesareevaluatedimmediately,i.e.,thesamedaythereadingsweretaken,orwithin7days—theintegratedofficevisitcountingasDAY1.
Theseriousimplicationsofalertvaluesrepresentforthehealthstatusofprogramparticipants,therearenoexceptionstothispolicy.
Participantswhowereseenrecentlybytheirclinicianorwillbeseenbytheircliniciansoonarenotexceptionstothisguideline.
Providersneedtotrackparticipantsbytelephonetoensurethattheykeeptheirmedicalappointment.
Providersneedtoensurethatallproviderstaffiseducated/re‐educatedconcerningthemanagementofalertvalues.
Ifwomenwithalertscreeningvaluesarenotseenintheexpectedtimeframe,providersshouldconsiderdoinganassessmentofthereferralprocedurestoidentifyareaswhereareasofimprovementareneeded.
AllwomenwithalertvaluesshouldbereferredtotheWISEWOMANSocialWorkertoprovideaccesstoWISEWOMANservices,followuponmedicalmanagement,andassistancewithprescriptionmedications.
DocumentationforAlertValueFollow‐up:
Providersmustdocumentintheparticipant’sEHR,thefollowinginformationforanypatientwithanalertvalue:
Thedatethemedicalevaluationwasstartedandcompleted Alltreatmentinformation Providersmustdocumentanyreasonswhyaparticipantdidnotreceivemedicalevaluationand
treatmentwithinthesevenbusinessdays,inpatient’sEHR
Pleaseseepage30fortheAlabamaWISEWOMANHypertensionFlowChart

16
ALERTandDISEASE‐LEVELVALUES:
Womenwithalertlevelglucosereadingsaretobeevaluatedimmediately.Thosewithdisease‐levelreadingswhoarenotalreadytakingmedicationmustbeevaluatedimmediatelyorwithina30‐dayperiod.Theseevaluationsmustbedocumentedonthescreeningformandinthepatient’smedicalrecord.
Glucose:
ALERTfastingglucose:≤50mg/dlor≥250mg/dl
ALERTAction:WomenwhohaveAlertfastingglucosevaluesmustreceivemedicalattentionimmediatelyorwithin7days—theintegratedofficevisitcountingasDAY1—attheclinic,officeoremergencyroom.SeeAlertValueProtocol,pg14
Diseaselevelfastingglucose:≥126mg/dl
Disease‐LevelAction:Womenfoundtohavedisease‐levelglucoseresultswhoareNOTalreadybeingtreatedmustreceiveamedicalevaluationimmediatelyorwithin30days—theintegratedofficevisitcountingasDAY1.Cholesterol/lipids:
Diseaselevels:
Disease‐levelAction:Allwomenfoundtohavedisease‐levelfastingcholesterol/lipidresultswhoareNOTalreadybeingtreatedmustreceiveamedicalevaluationimmediatelyorwithin30days—theintegratedofficevisitcountingasDAY1.BloodPressure:(SeeAppendixDandHforHypertensionFlowchartandproperbloodpressuremeasurementprocedures)Eachparticipantmusthavetwobloodpressuremeasurementstakenandtheaveragecalculated.Theaveragedbloodpressurenumberisthefinalbloodpressurereading.NOTE:Whenthesystolicanddiastolicbloodpressurereadingsfallintotwodifferentcategories,thehighercategoryshouldbeusedtoclassifythebloodpressurelevel.Forexample,160/80mmHgwouldbeStage2hypertension(highbloodpressure).Thehigherreadingofthesystolicbloodpressureof160mmHgdeterminestheclassificationofStage2hypertension.
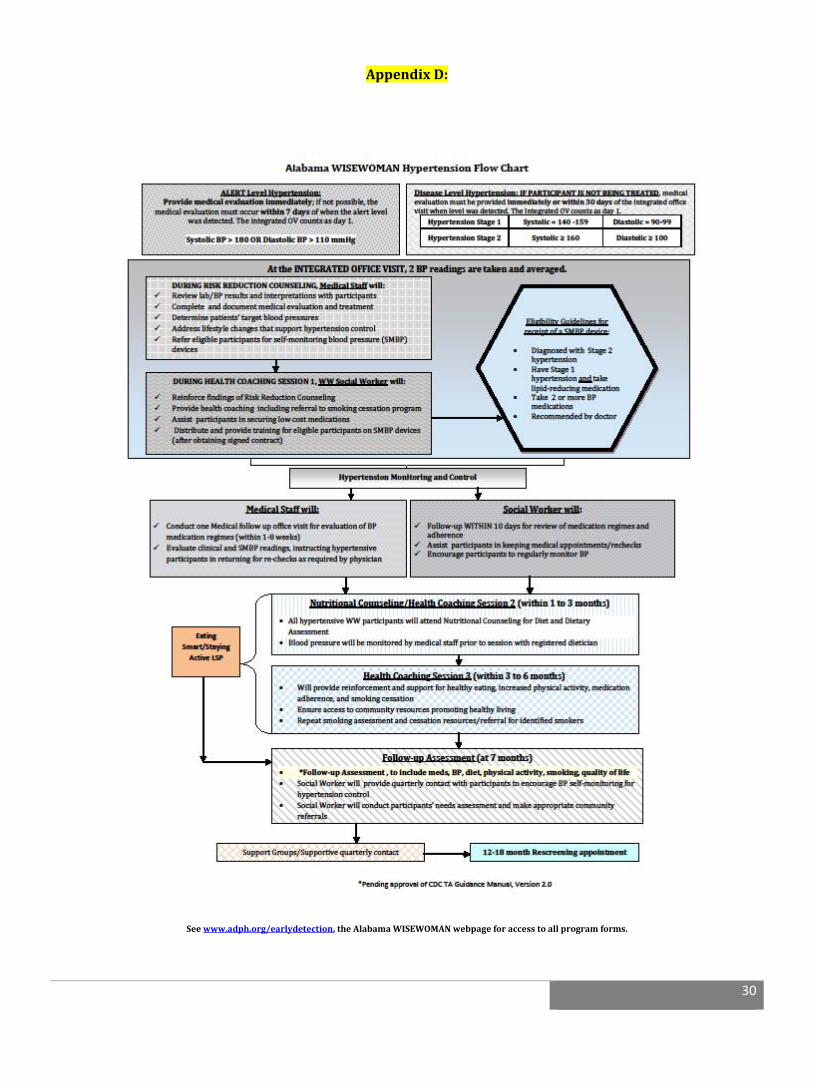
ALERTBloodPressure:SystolicBPof>180mmHgorDiastolicof>110mmHg
AlertAction:AnywomanwhohasanalertBPvaluemustreceiveimmediatemedicalattentionorwithin7days—theintegratedofficevisitcountingasDAY1—attheclinic,officeoremergencyroom.SeeAlertValueProtocol,p.15
Fastingtotalcholesterol ≥240mg/dl
FastingLDL‐cholesterol 160‐189mg/dl
Fastingtriglycerides 200‐499mg/dl

17
Disease‐LevelBloodPressure:
*JNC8guidelinefor≥60yearoldswithoutdiabetesorchronickidneydisease(CKD)=<150/90mmHgAction:Allwomenfoundtohavedisease‐levelBPresultswhoareNOTalreadybeingtreatedmustreceiveamedicalevaluationimmediatelyorwithin30days—theintegratedofficevisitcountingasDAY1.
ForUncontrolledHypertensiveParticipants:SeeAppendixDforHypertensionFlowChartAllwomenwithuncontrolledhypertensionmustreceivepatientnavigationservicesandfollowuptoinclude:
Medicationcounselingthroughateamapproachofphysicians,medicalstaff,pharmacists,nutritionistsandSocialWorkers
HealthCoaching/supportivecounseling Counselingontheimportanceofbloodpressuremonitoringandeducatedonbloodpressuremonitoring
opportunitiesinthecommunity
NOTE:Ataminimum,allhypertensiveWISEWOMANparticipantsmusthavetheirbloodpressurecheckedanddocumentedinthepatient’srecordat1,3,and6monthsfromtheenrollmentdate.
HypertensionStage1* Systolic≥140‐159 Diastolic≥90‐99
HypertensionStage2 Systolic≥160 Diastolic≥100

18
DATACOLLECTIONFORMS
Purpose
ALWISEWOMANhasmandatoryreportingrequirementsanddataelementsthatarerequiredbytheCDC.ThedatacollectedfromtheWISEWOMANformsprovidesevidencetothefundingagenciesthatmoniesusedbyWISEWOMANprogramsareusedto:
EnsureALWISEWOMANwomenreceivecardiovasculardiseasescreeningtestsinconjunctionwithABCCEDPscreenings
Ensurewomenwithalertvaluesanddisease‐levelvaluesarefollowedaccordingtoCDCguidelines
Ensuretheprogramisreachingthein‐needsegmentofthepopulation
EvaluatetheeffectivenessoftheWISEWOMANProgram
Ensuretheavailabilityofhighqualitydataforprogramplanningaswellasqualityassuranceoftheprogram.
DataCollectionRequirements
ALWISEWOMANprogramusesseveraldatacollectionformsfordatareporting.SeeAppendixE,p.29.
A. AlabamaWISEWOMANDataCollectionForm:Baseline/RiskReductionB. TheAlabamaWISEWOMANContactformC. HICF1500formorUBform
GeneralInformationconcerningallForms
Allformsshouldbefilledcorrectly. TheoriginalformswillbesenttotheProgramManagerwithaninvoicebythe15thofeachmonth. AllformscanbeprintedfromtheMed‐ITEnrollmentwebsite. Copiesofallformsmustbekeptinthewoman’sfile. Theresultsofthelabtestsshouldbecarefullyrecordedsothatwomenreceiveadequatefollowupand
providersreceiveproperpayment. TheALWISEWOMANConsentformappearsonthebackoftheABCCEDPScreeningform.Theconsent
mustbesignedbeforeanyservicesarerendered,andthesigneddocumentmustbemaintainedinthepatient’smedicalrecord.
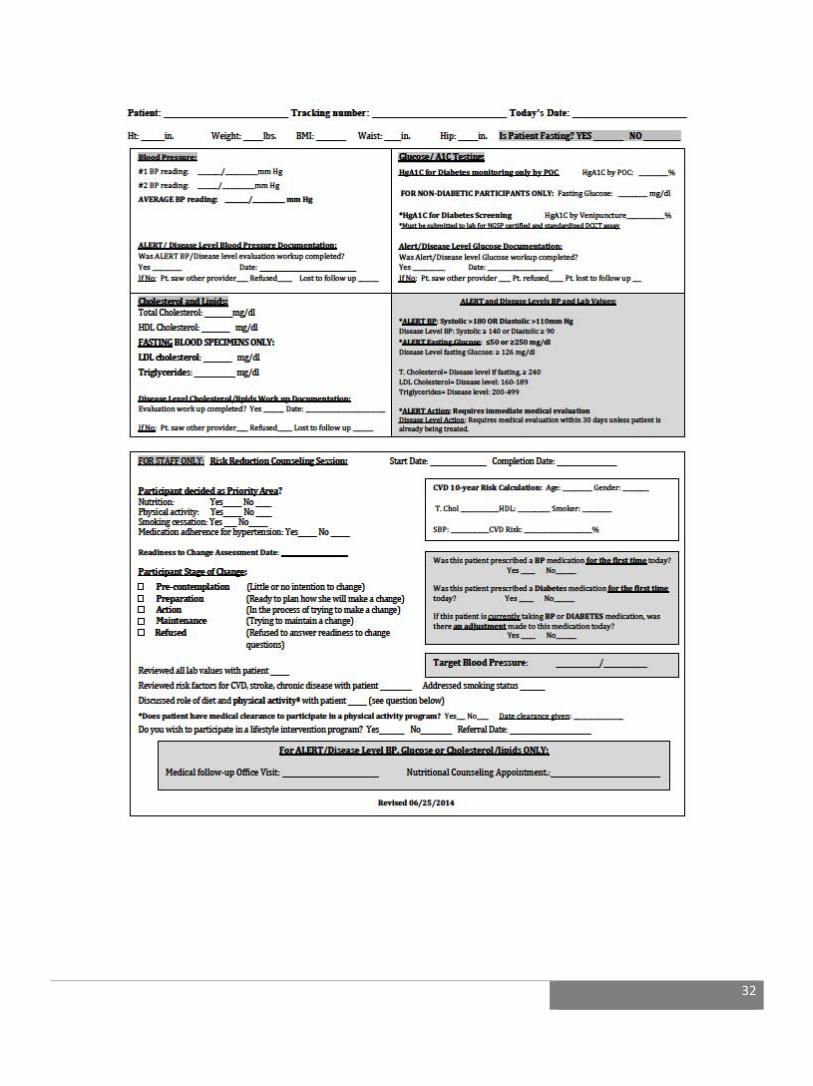
ALWISEWOMANDataCollectionForm:Baseline/RiskReductionThisformshouldbefilledonallWISEWOMANpatientsattheinitialofficevisitorintegratedofficevisit.ThepurposeoftheBaseline/RiskReductionForm:
Toprovidedocumentationofthepatienthistory,healthassessmentinformation,baselinelabandclinicalvaluesandriskreductioncounselinginformation.
Toserveasthemonthlydatareportonprovideractivityandthedocumentationforbilling. Totrackpatientsregardingmedicationcomplianceandlifestyleprograms,etc. GeneratedbytheprimaryprovideratthetimeoftheWISEWOMANscreening.
TheHICF1500formisthestandardbillingformusedtosubmitchargesaccruedforALWISEWOMANservicestoaccuratelyreimburseproviders.

19
TheAlabamaWISEWOMANContactformwillbecompletedwheneverthereisanycontactbetweentheparticipantandtheWISEWOMANSocialWorkerandtheNutritionalCounselor.ThepurposeofthisFormisto:
Collectpatientparticipationinlifestyleprogramandtrackcompletedsessions Providedocumentationofpatientreferralstocommunityresources,includingsmokingcessation
programs ToserveasthemonthlydatareportforSocialWorkeractivity ToprovidetrackinganddocumentationfortheNutritionalCounselingsessions
HowtoChangeClientInformation
Iftherearechangesinclientinformationafteryouhavesubmittedthescreeningformsorfollow‐upformsfortheclient,notifytheWISEWOMANSocialWorkerinwritingofthechangetobemade.Includeinyournotethefollowing,sothatthecorrectrecordischanged:
NamethatiscurrentlyinWISEWOMANprogramrecords SocialSecurityNumber DateofBirth MED‐ITTrackingNumber InitialofficevisitDate Namethatthecurrentnamewillbechangedto
BILLINGANDREIMBURSEMENTCurrentProceduralTerminology(CPTCodes)/Reimbursement
Requirement:ProvidersarerequiredtouseappropriateCPTCodesasdefinedbyCDC.Guidance:CurrentProceduralTerminology(CPT)isalistingofdescriptivetermsandidentifyingcodesforreportingmedicalservicesandproceduresperformedbyphysicians.Thepurposefortheterminologyistoprovideauniformlanguagethatwillaccuratelydescribemedical,surgical,anddiagnosticservices,andwilltherebyprovideaneffectmeansforreliablenationwidecommunicationamongphysicians,patientsandthirdparties.
AL WISEWOMAN funds can only be used to reimburse for services outlined by CDC as approvedproceduresandatthecurrentMedicarereimbursementamounts.
ALWISEWOMANfundscannotbeusedfortreatmentservicesofanykindNOTE:Treatmentservicesincludemedicationandotherhighlyspecializedcounselingsuchasdiabeteseducationprograms.Giventhatno‐costtobaccocessationresourcesanddiabeteseducationprogramsarereadilyavailableandaccessibleinthecommunity,ALWISEWOMANfundscannotbeusedtoreimbursefortheseservices.
ALWISEWOMANfundscannotbeusedtoreimbursecostsrelatedtoALERTvaluemedicalevaluationssuchasambulancetransportationorsubsequenthospitalizations.
AlabamaWISEWOMANPaidServices:
Clinicallaboratorytestsatinitialscreening

20
RiskReductioncounselingsessionwithmedicalprofessional
NutritionalCounselingsessionwitharegistereddietician
OneFollowupOfficeVisitwithmedicalprofessional
IntheIntegratedOfficeVisit,theclinicalscreeningportionisfundedthroughABCCEDP.ALWISEWOMANfundspayforlabtestingandtheriskreductioncounselingsegmentoftheIntegratedOfficeVisit.
ClinicalLaboratoryTests:
TheALWISEWOMENprogramwillpayforthefollowingscreeninglabtestsforALWISEWOMANparticipants:83718,82947,80061,82948,or83036
NOTE:NofastingglucoseistobeperformedonanyALWISEWOMANparticipantwhohadbeendiagnosedwithDiabetes.
RiskReductionCounseling:
Med‐ITReimbursementCodes99401,99402,99403willbeusedforWISEWOMANprogramriskreductioncounseling.CDCprotocolsrequiretheprovisionofriskreductioncounselingtoeachWISEWOMANProgramparticipant,includingwomenwithandwithoutrisksforcardiovasculardisease.Providerswillbereimbursedforthetimespentconductingriskreductioncounselingservices.Reimbursementshouldbefortheriskreductioncounselingthatisprovidedandisbilledseparatelyfromthetimespentconductingtheclinicalscreeningservicesthatarepartoftheofficevisit.Theriskreductioncounselingservicescantakeplaceonthesamedayasthescreeningofficevisitoronadifferentdaybutmustbebilledseparately.CDCrequiresriskreductioncounselingtobeprovidedattheofficevisitbaseduponwhateverassessmentsandtestresultsareavailable.Ifalltestresultsareavailable,includingbloodwork,riskreductioncounselingisrequiredtotakeplaceattheofficevisit.Thisisreferredtoascompletedriskreductioncounselingattheofficevisit.Ifpartoftheassessments,measurements,andtestresultsareavailablebutnotallofthem,riskreductioncounselingistobeprovidedontheinformationthatisavailableattheofficevisit,aCDCrequirement.Thisisreferredtoaspartialriskreductioncounselingattheofficevisit.Tocompletetheriskreductioncounselingprovidersarerequiredtofollow‐upwithparticipantsbytelephoneorface‐to‐face.Providersarereimbursedonlyforcompletedriskreductioncounseling.Theuseoftheministickduringtheofficevisitallowsforriskreductioncounselingtobecompletedduringtheofficevisit,eliminatingtheneedtocarryoutfollowupatalatertime.
NutritionalCounselingSessions
OutsideoftheIntegratedOfficeVisit,ALWISEWOMANwillpayforonenutritionalcounselingsessionwitharegistereddietician.AppropriateCPTcodeis:97802or99804
MedicalFollowupOfficeVisit
MedicalstaffwillmeetwithALWISEWOMANparticipantswithALERTorabnormalscreeningtestswhowereputonmedicationorhadachangeindosageforonefollowupvisitperWISEWOMANcycle.ALWISEWOMANfundswillpayforthefollowingcodes:99202,99203,99211,99212,and99213.
FollowupAssessment(Version2,CDCTAmanual,pendingIRBapproval)
Followupassessment,inordertoevaluateshort‐termpatientprogress,isrequiredbyCDCforallwhocompletehealthcoachingand/orLSP.Evaluationmustcover,ataminimum:medications,bloodpressure,diet,physicalactivity,smoking,andqualityoflifeissues.PerCDCTechnicalAssistancemanual,version2.0,thisassessmentmayormaynotincludeanofficevisit.Untilfirmerguidelinesareset,AlabamaWWwillconducttheseassessments,andanyadditionallabtesting,onacase‐to‐casebasis.

21
APPENDICES

22
AppendixA:
NationalClinicalGuidelines
Overview National clinical, diet, and lifestyle guidelines translate the best available science
to practice. Guidelines assist clinicians and patients in making health care
decisions. Guidelines do not take the place of the health care provider’s
judgment.
Clinical practice guidelines on Hypertension, Cholesterol, Overweight and Obesity
are developed through collaborative efforts of national organizations. Additional
guidelines on diseases and lifestyle are developed by national organizations such
as the American Heart Association, American Diabetes Association and the
American College of Cardiology. All the national guidelines are based on a
rigorous review process.
Requirements
Grantees must ensure that WISEWOMAN service providers follow standard care
practices, generally the current national guidelines. Each WISEWOMAN health
care facility should have a Medical Director or Board that establishes which
specific set of guidelines that facility will follow and also provides guidance for
situations not addressed by guidelines.
Guidance Grantees should assure the quality of all WISEWOMAN services provided.
Examples of methods to assure standards of care are met for clinical and
preventive services are:
Specify expectations regarding adherence to current guidelines in contractual agreements, training, and program manuals.
Provide professional development and technical assistance on guidelines and quality assurance regarding their use.
Conduct chart audits and/or data audits.
References/
Resources
Cardiovascular Risk and Blood Pressure
Million Hearts® Evidence‐based Treatment Protocols for Improving Blood
Pressure Control
http://millionhearts.hhs.gov/resources/protocols.html
Go AS, Bauman MA, Coleman King SM, Fonarow GC, Lawrence W,
Williams KA, Sanchez E. An effective approach to high blood pressure control: A
Science Advisory From the American Heart Association, the American College of
Cardiology, and the Centers for Disease Control and Prevention. Hypertension.

23
2014;63:878–885.
http://hyper.ahajournals.org/content/63/4/878
Centers for Disease Control and Prevention. Hypertension Control: Action Steps
for Clinicians. Atlanta, GA: Centers for Disease Control and Prevention, US Dept. of
Health and Human Services; 2013.
http://millionhearts.hhs.gov/resources/action_guides.html
2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report from
the American College of Cardiology/American Heart Association Task Force on
Practice Guideline
http://circ.ahajournals.org/content/early/2013/11/11/01.cir.0000437741.48606.
98.citation
Guideline on the Assessment of Cardiovascular Risk Slide Set
The Seventh Report of the Joint National Committee on Prevention, Detection,
Evaluation, and Treatment of High Blood Pressure (JNC 7).
http://www.nhlbi.nih.gov/guidelines/hypertension/
Cholesterol
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce
Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines.
http://circ.ahajournals.org/content/early/2013/11/11/01.cir.0000437739.71477.
ee.citation
Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic
Cardiovascular Risk in Adults Slide Set
Diabetes
American Diabetes Association Standards of Medical Care in Diabetes—2014.
http://care.diabetesjournals.org/content/37/Supplement_1/S14.full
Overweight and Obesity
2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in
Adults: A Report of the American College of Cardiology/ American Heart
Association Task Force on Practice Guidelines and The Obesity Society.

24
http://circ.ahajournals.org/content/early/2013/11/11/01.cir.0000437739.71477.
ee
Guideline for the Management of Overweight and Obesity in Adults Slide Set
Tobacco Control
Best Practices for Comprehensive Tobacco Control Programs—2014; Centers for
Disease Control and Prevention
http://www.cdc.gov/tobacco/stateandcommunity/best_practices/
Diet &Lifestyle Guidelines
The 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular
Risk: A report of the American College of Cardiology/American Heart Association
Task Force on Practice Guidelines.
http://circ.ahajournals.org/content/early/2013/11/11/01.cir.0000437740.48606.
d1.citation
Million Hearts. Healthy Eating & Lifestyle Resource Center.
http://recipes.millionhearts.hhs.gov/
Dietary Guidelines for Americans, 2010.
http://www.cnpp.usda.gov/DGAs2010‐PolicyDocument.htm
Your Guide to Lowering Your Blood Pressure With DASH: DASH Eating Plan
http://www.nhlbi.nih.gov/health/public/heart/hbp/dash/new_dash.pdf
2008 Physical Activity Guidelines for Americans.
http://www.health.gov/paguidelines/guidelines/default.aspx
Position Stand: American College of Sports Medicine (ACSM) Quantity and
Quality of Exercise for Developing and Maintaining Cardiorespiratory,
Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance
for Prescribing Exercise. http://journals.lww.com/acsm‐
msse/Fulltext/2011/07000/Quantity_and_Quality_of_Exercise_for_Developing.26
.aspx
GET THE FACTS: Sodium and the Dietary Guidelines.

25
http://www.cdc.gov/salt/pdfs/sodium_dietary_guidelines.pdf
The U.S. National Physical Activity Plan, 2010.
http://www.physicalactivityplan.org/theplan.php

26
AppendixB:
AuthorizationforServices
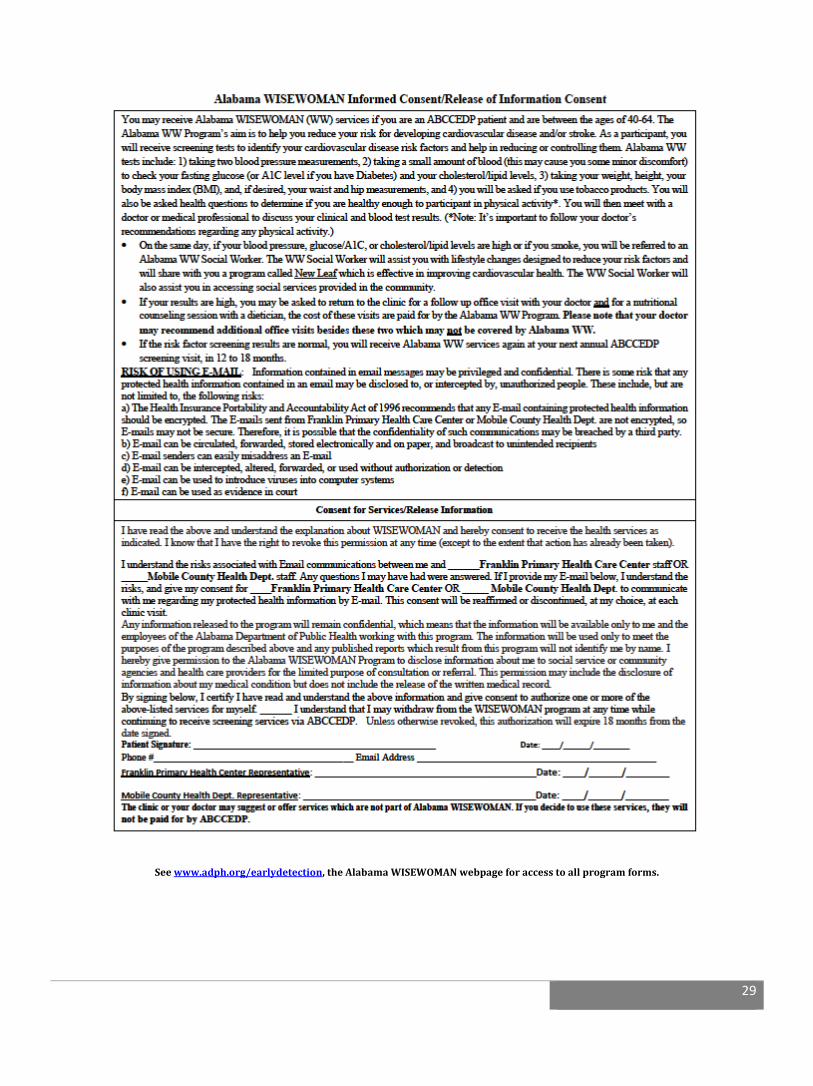
TheAlabamaWISEWOMANProgram’saimistohelpyoureduceyourriskofcardiovasculardiseaseandstroke.EligibilitycriteriaforWISEWOMANarecurrentenrollmentintheABCCEDP.Theservicesprovidedthroughthisprogramincludemedicalscreeningstoevaluateyourbloodpressure,glucoseandcholesterollevel.Thesetestsrequirethatyouprovideasmallsampleofblood.Thisroutinefingerprickmaycauseyousomeminordiscomfort.Youwillhaveyourweight,heighttaken,yourBMIcalculated,andwillbeaskedifyouusetobaccoproducts.
Iunderstandifmybloodpressure,glucoseandcholesterollevelsareinthenormalrange,Iwillberescreenedfortheseriskfactorsatmyannualbreastandcervicalcancerscreeningvisitin12to18months.
Iunderstandifmybloodpressure,glucoseorcholesterollevelsareslightlyelevatedIwillbereferredtoaSocialWorker.IunderstandthatIwillbeaskedhealthquestionstodetermineifIamhealthyenoughtoparticipantinphysicalactivity.Iagreetofollowmyprovider’srecommendationregardingparticipatinginanyphysicalactivity.
IunderstandthatasaWISEWOMANparticipant,IwillmeetwithaSocialWorkerwhowillutilizealifestyleprogramshowntobeeffectiveinimprovingcardiovascularhealth.IunderstandImightqualifyforsocialservicesprovidedinthecommunity.IherebygivepermissiontotheAlabamaWISEWOMANProgramtodiscloseinformationaboutmetosocialserviceagencies,communityagencies,andhealthcareprovidersforthelimitedpurposeofconsultationorreferral.Thispermissionmayincludethedisclosureofinformationaboutmymedicalconditionbutdoesnotincludethereleaseofthewrittenmedicalrecord.Ihavebeengivenanopportunitytodiscusshowthisformwillbeused.IknowthatIhavetherighttorevokethispermissionatanytime(excepttotheextentthatactionhasalreadybeentaken).
RISKOFUSINGE‐MAIL
Informationcontainedinemailmessagesmaybeprivilegedandconfidential.Thereissomeriskthatanyprotectedhealthinformationcontainedinanemailmaybedisclosedto,orinterceptedby,unauthorizedpeople.Theseinclude,butarenotlimitedto,thefollowingrisks:
a.TheHealthInsurancePortabilityandAccountabilityActof1996recommendsthatanyE‐mailcontainingprotectedhealthinformationshouldbeencrypted.TheE‐mailssentfromtheAlabamaDepartmentofPublicHealtharenotencrypted,soE‐mailsmaynotbesecure.Therefore,itispossiblethattheconfidentialityofsuchcommunicationsmaybebreachedbyathirdparty.
b.E‐mailcanbecirculated,forwarded,storedelectronicallyandonpaper,andbroadcasttounintendedrecipients.
c.E‐mailsenderscaneasilymisaddressanE‐mail.
d.E‐mailcanbeintercepted,altered,forwarded,orusedwithoutauthorizationordetection.
e.E‐mailcanbeusedtointroducevirusesintocomputersystems.
f.E‐mailcanbeusedasevidenceincourt.
IacknowledgethatIhavereadandfullyunderstandthisconsentform.IunderstandtherisksassociatedwithcommunicationofE‐mailbetweenmeandtheAlabamaDepartmentofPublicHealth/FranklinPrimaryHealthCenterstaff.AnyquestionsImayhavehadwereanswered.IfIprovidemyE‐mailbelow,Iunderstandtherisks,andgivemyconsentfortheAlabamaDepartmentofPublicHealth/FranklinPrimaryHealthCaretocommunicatewithmeregardingmyprotectedhealthinformationbyE‐mail.Thisconsentwillbereaffirmedordiscontinued,atmychoice,ateachclinicvisit.

27
Bysigningbelow,IcertifyIhavereadandunderstandtheaboveinformationandgiveconsenttoauthorizeoneormoreoftheabove‐listedservicesformyself.
______IunderstandthatImaywithdrawfromtheWISEWOMANprogramatanytimewhilecontinuingtoreceivescreeningservicesviaABCCEDP.
Unlessotherwiserevoked,thisauthorizationwillexpire18monthsfromthedatesigned.
WISEWOMANSignature:______________________________________Date:_____________________________
Phone#:_______________________________________________________________________
EmailAddress:__________________________________________________________________________
FranklinPrimary/DepartmentofPublicHealthRepresentative Date
Note:TheclinicoryourdoctormaysuggestorofferserviceswhicharenotpartofAlabamaWISEWOMAN.Ifyoudecidetousetheseservices,theywillnotbepaidforbyABCCEDP.

28
AppendixC:
29
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.
30
AppendixD:
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.

31
AppendixE:ProgramDataForms
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.
32

33

34
35
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.

36
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.

37
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.
AppendixF:CPT/ReimbursementTable

38
Seewww.adph.org/earlydetection,theAlabamaWISEWOMANwebpageforaccesstoallprogramforms.

39
AppendixH:
BloodPressureMeasurementTechnique
Accuratebloodpressuremeasurementsarecriticalfordetectingandmanaginghighbloodpressure.Bloodpressuremeasurementsshouldbedoneusingthefollowingpropertechnique(adaptedfromJNC6andJNC71): Patientsshouldnotsmoke,exercise,orhavecaffeineforatleast30minutesbeforetheirbloodpressure
ismeasured.
Patientsshouldbeseatedquietlyforatleast5minutesinachair(ratherthanonanexamtable),withfeetonthefloorandarmssupportedatheartlevel.
Anappropriatesizedcuffshouldbeused(cuffbladderencirclingatleast80%ofthearm).
Amercurysphygmomanometer,arecentlycalibratedaneroidmanometer,oravalidatedelectronicdeviceshouldbeused.
Atleasttwomeasurementsshouldbetakenandrecorded,separatedbyaminimumof2minutes.Ifthefirsttworeadingsdifferbymorethan5mmHg,additionalmeasurementsshouldbetaken.

40
AppendixI:HealthCoaching/NEWLEAFLifestyleProgramHealthCoachingID#:AL13HCG001
KeyElements LifestyleProgram
Setting Athealthfacilityorcommunity‐basedfacility
Timing/OccurrenceAfterriskreductioncounselingoratanypointthatthewomanindicatesreadiness,
Intendedparticipants
Participantswhohaveindicatedaninterestandreadiness
Numberofsessions
3sessions
Deliverymethods
Utilizingmotivationalinterviewing:
1. Session1:Face‐to‐facevisitimmediatelyfollowingriskreductioncounseling(typicallylasting60minutes)
2. Sessions2and3:eitherface‐to‐face,inagroupsettingorbyphone.(typicallylasting15‐60minutesbasedontypeofsessionandparticipantneed)
3. Follow‐upwithinfourweeksaftercompletiontoassessprogressandreinforcegoals.Followupcontact,eitherbyphone,emailorletterasneeded.(Followupviaphoneoremail,5‐10minutes).AftertheNewLeafsessionsarecomplete,contactwithparticipantswillbemaintainedtoprovidecontinuedsupportandensurereturnforannualrescreening.
Content
ThefocusofANewLeaf…ChoicesforHealthyLivingistoprovidepracticalstrategiesforincorporatingchangesindietandphysicalactivitytoprevent/treatcardiovasculardisease,diabetes,obesityandotherchronicdisease.Itisacomprehensiveprogramdesignedtohelpimprovehealthyeatingbehaviors,increasephysicalactivity,controlhypertension,improvelipidprofile,achieveahealthyweightandceasetobaccouse.ThecoreelementsofNewLeafisanassessmentofdiet,physicalactivityandsmoking,goalsetting,selfefficacy,guidelinesandstrategies,feedback,followupandsocialsupport.
Follow‐uprequired
Follow‐upwithinfourweeksaftercompletionofeachsessiontoassessprogressandreinforcegoals.Toencourageparticipationandoffersupport,eachfacilitywillconductmonthlycommunitymeetingsfeaturingdifferenttopics/speakers(12meetingsperyear).Eachmeetingwillincludeademonstrationandrelevantdoorprize.
41
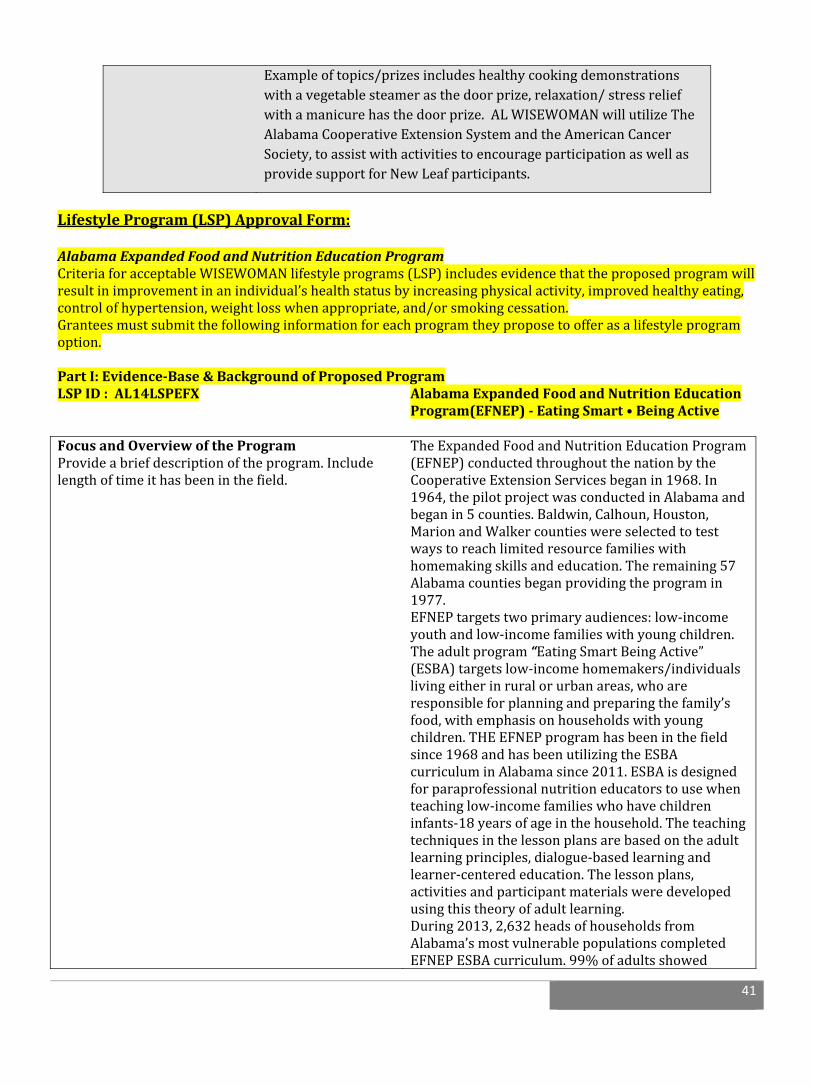
LifestyleProgram(LSP)ApprovalForm:AlabamaExpandedFoodandNutritionEducationProgramCriteriaforacceptableWISEWOMANlifestyleprograms(LSP)includesevidencethattheproposedprogramwillresultinimprovementinanindividual’shealthstatusbyincreasingphysicalactivity,improvedhealthyeating,controlofhypertension,weightlosswhenappropriate,and/orsmokingcessation.Granteesmustsubmitthefollowinginformationforeachprogramtheyproposetoofferasalifestyleprogramoption.PartI:Evidence‐Base&BackgroundofProposedProgramLSPID:AL14LSPEFX AlabamaExpandedFoodandNutritionEducation
Program(EFNEP)‐EatingSmart•BeingActive
FocusandOverviewoftheProgramProvideabriefdescriptionoftheprogram.Includelengthoftimeithasbeeninthefield.
TheExpandedFoodandNutritionEducationProgram(EFNEP)conductedthroughoutthenationbytheCooperativeExtensionServicesbeganin1968.In1964,thepilotprojectwasconductedinAlabamaandbeganin5counties.Baldwin,Calhoun,Houston,MarionandWalkercountieswereselectedtotestwaystoreachlimitedresourcefamilieswithhomemakingskillsandeducation.Theremaining57Alabamacountiesbeganprovidingtheprogramin1977.EFNEPtargetstwoprimaryaudiences:low‐incomeyouthandlow‐incomefamilieswithyoungchildren.Theadultprogram“EatingSmartBeingActive”(ESBA)targetslow‐incomehomemakers/individualslivingeitherinruralorurbanareas,whoareresponsibleforplanningandpreparingthefamily’sfood,withemphasisonhouseholdswithyoungchildren.THEEFNEPprogramhasbeeninthefieldsince1968andhasbeenutilizingtheESBAcurriculuminAlabamasince2011.ESBAisdesignedforparaprofessionalnutritioneducatorstousewhenteachinglow‐incomefamilieswhohavechildreninfants‐18yearsofageinthehousehold.Theteachingtechniquesinthelessonplansarebasedontheadultlearningprinciples,dialogue‐basedlearningandlearner‐centerededucation.Thelessonplans,activitiesandparticipantmaterialsweredevelopedusingthistheoryofadultlearning.During2013,2,632headsofhouseholdsfromAlabama’smostvulnerablepopulationscompletedEFNEPESBAcurriculum.99%ofadultsshowed
Exampleoftopics/prizesincludeshealthycookingdemonstrationswithavegetablesteamerasthedoorprize,relaxation/stressreliefwithamanicurehasthedoorprize.ALWISEWOMANwillutilizeTheAlabamaCooperativeExtensionSystemandtheAmericanCancerSociety,toassistwithactivitiestoencourageparticipationaswellasprovidesupportforNewLeafparticipants.

42
improvementinoneormorenutritionbehaviorssuchasmakinghealthyfoodchoices,readingnutritionlabels,planningmealsandfeedingchildrenbreakfast.Positivechangesinthesebehaviorswillimproveparticipants’healthandqualityoflife.AlabamaWISEWOMANisusingESBAasanLSPoptionduetotheimpactitwillhaveonourparticipantsandtheirfamilies.
Dosage/intensityoftheprogram(i.e.frequencyofcontactandduration)
TheESBAcurriculumconsistsofeightcorelessonstaughtover5‐7weeks.Each90minutelessonisdesignedtobetaughtinorder.Eachlessonincludesafoodpreparationactivity,handsonlearnercenteredactivitiesandaphysicalactivitysegment.
Keyactivitiesandthemodeofdelivery(e.g.,inperson,byphone)
GroupsessionsareprovidedinEnglish.Thenutritioneducatoractsasa

43
44
Community‐BasedReferrals:
ThegoalsofALWISEWOMANwillbeaccomplishedthroughpartnerships/referralsmadewithcommunityprogramsandwithADPHChronicDiseasepartners,suchas:
TheCardiovascularHealthProgram,theAlabamaTobaccoControlProgram,OfficeofWomen’sHealth,OfficeofMinorityHealth,TheNutritionandPhysicalActivityDivision,LivingWellAlabamaProgramandtheDiabetesPreventionandControlProgram,providingALWISEWOMANwitheducationmaterialsorasareferralsourceforparticipantsseekinganalternativeLSP
TheAlabamaQuitNowTobaccoquitlineandtheAmericanLungAssociation’sFreedomfromSmoking,availableasagroupclinic,anonlineprogramoraself‐helpbook
YMCAprogramspromotinghealthydiets,physicalactivityandprogresstracking,suchastheHealthyFamilyHomeInitiative
TheAlabamaExtensionService,toprovidenutritionalinformationandhealthylivingdemonstrations
TheAlabamaFarmer’sMarketAuthorityandlocalgrowers,tomakehealthyfoodsavailabletoparticipantsintheirownneighborhoods
TheAmericanCancerSocietyandtheircommunityhealthworkers(CHWs)whowillassistinthedevelopmentandcirculationofthequarterlyALWISEWOMANnewsletter,featuringarticlesonhowtoincorporateexerciseintodailylife,successstories,andhealthycookingtechniques/recipes.CHWswillassistin:1)securinglocationsintargetedcommunitiestoholdmonthlysupportmeetings,2)schedulingspeakersandfacilitatingdemonstrations,and3)indatacollection,developmentandmaintenanceofacommunityresourceguide.
Prescriptionmedicationassistanceprograms Communityorganizationsandbusinesses,toprovideaccesstolow‐costresourcesthatpromote
healthybehaviorsandappropriatechronicdiseasemanagementinthecommunity