Embed Size (px)
Citation preview
5/24/2016
1
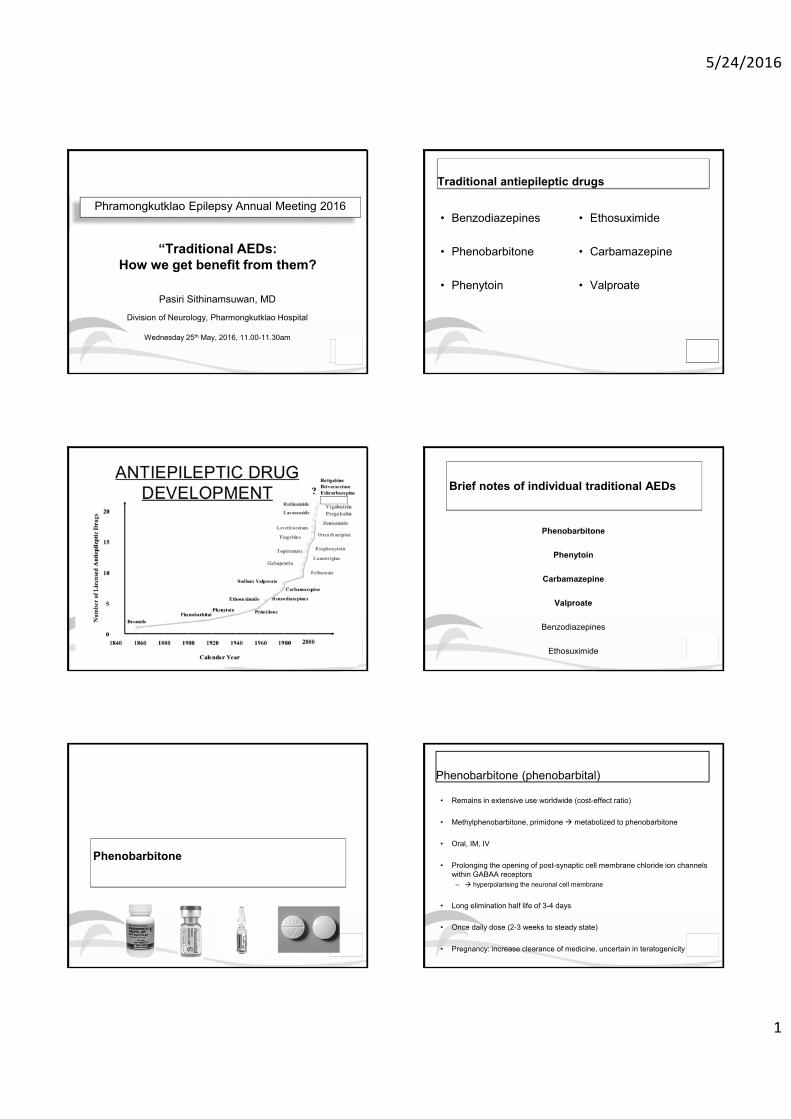
“Traditional AEDs: How we get benefit from them?
Pasiri Sithinamsuwan, MD
Division of Neurology, Pharmongkutklao Hospital
Wednesday 25th May, 2016, 11.00-11.30am
Phramongkutklao Epilepsy Annual Meeting 2016
Traditional antiepileptic drugs
• Benzodiazepines
• Phenobarbitone
• Phenytoin
• Ethosuximide
• Carbamazepine
• Valproate
Brief notes of individual traditional AEDs
Phenobarbitone
Phenytoin
Carbamazepine
Valproate
Benzodiazepines
Ethosuximide
Phenobarbitone
Phenobarbitone (phenobarbital)
• Remains in extensive use worldwide (cost-effect ratio)
• Methylphenobarbitone, primidoneÆ metabolized to phenobarbitone
• Oral, IM, IV
• Prolonging the opening of post-synaptic cell membrane chloride ion channels within GABAA receptors
– Æ hyperpolarising the neuronal cell membrane
• Long elimination half life of 3-4 days
• Once daily dose (2-3 weeks to steady state)
• Pregnancy: increase clearance of medicine, uncertain in teratogenicity
5/24/2016
2
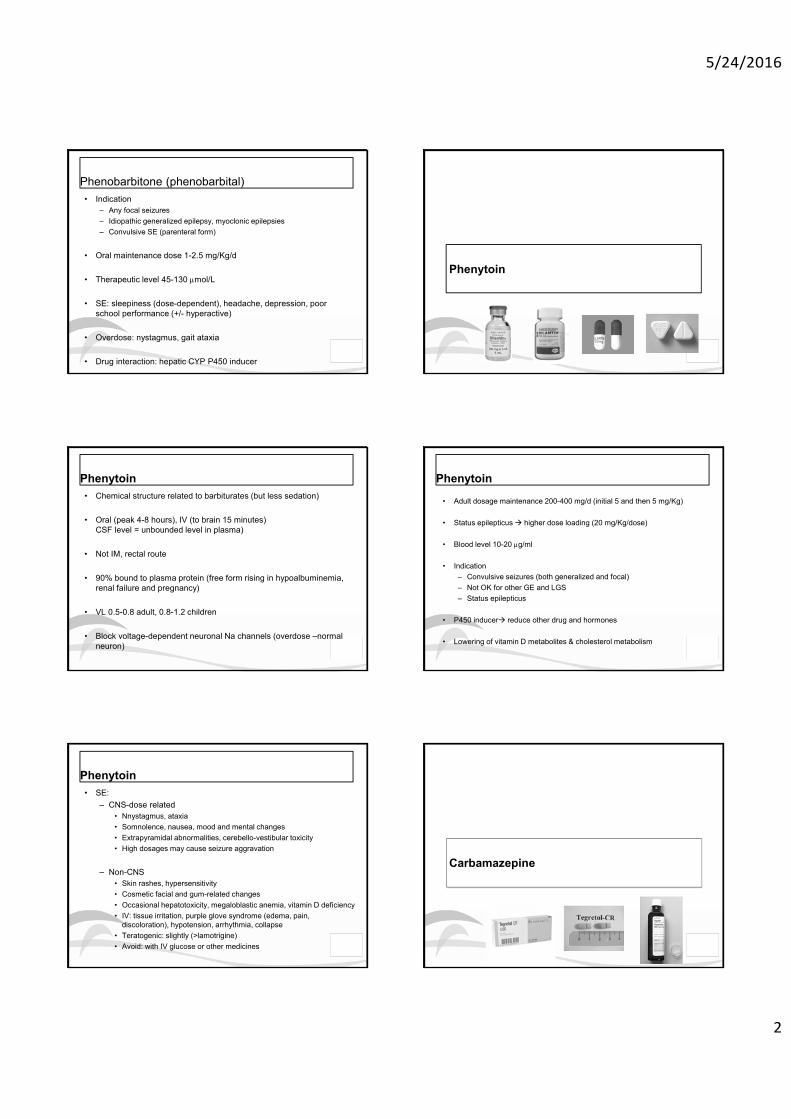
Phenobarbitone (phenobarbital)• Indication
– Any focal seizures– Idiopathic generalized epilepsy, myoclonic epilepsies– Convulsive SE (parenteral form)
• Oral maintenance dose 1-2.5 mg/Kg/d
• Therapeutic level 45-130 Pmol/L
• SE: sleepiness (dose-dependent), headache, depression, poor school performance (+/- hyperactive)
• Overdose: nystagmus, gait ataxia
• Drug interaction: hepatic CYP P450 inducer
Phenytoin
Phenytoin• Chemical structure related to barbiturates (but less sedation)
• Oral (peak 4-8 hours), IV (to brain 15 minutes)CSF level = unbounded level in plasma)
• Not IM, rectal route
• 90% bound to plasma protein (free form rising in hypoalbuminemia, renal failure and pregnancy)
• VL 0.5-0.8 adult, 0.8-1.2 children
• Block voltage-dependent neuronal Na channels (overdose –normal neuron)
Phenytoin
• Adult dosage maintenance 200-400 mg/d (initial 5 and then 5 mg/Kg)
• Status epilepticusÆ higher dose loading (20 mg/Kg/dose)
• Blood level 10-20 Pg/ml
• Indication– Convulsive seizures (both generalized and focal)– Not OK for other GE and LGS– Status epilepticus
• P450 inducerÆ reduce other drug and hormones
• Lowering of vitamin D metabolites & cholesterol metabolism
Phenytoin• SE:
– CNS-dose related • Nnystagmus, ataxia• Somnolence, nausea, mood and mental changes• Extrapyramidal abnormalities, cerebello-vestibular toxicity• High dosages may cause seizure aggravation
– Non-CNS• Skin rashes, hypersensitivity• Cosmetic facial and gum-related changes• Occasional hepatotoxicity, megaloblastic anemia, vitamin D deficiency • IV: tissue irritation, purple glove syndrome (edema, pain,
discoloration), hypotension, arrhythmia, collapse• Teratogenic: slightly (>lamotrigine)• Avoid: with IV glucose or other medicines
Carbamazepine
5/24/2016
3
Carbamazepine• Oral: tablet, liquid, sustained release available
• Mechanism: blocking voltage dependent sodium ion channels in cell membranes
• Enzyme inducer, auto-inducer (CYP P450 3A4 inducer)
• Maintenance dose 10-20 mg/Kg/d
• Level 25-50 mol/L (? Reliable with clinical)
Carbamazepine
• Indication– First choice of focal epilepsies (not Generalized)– Mood stabilizers, neuropathic pain
• SE: – Rashes (>5%), hepatitis– SJS, TEM (check HLA-B*1502 before prescribing)– Over dose: nystagmus, blurred vision, ataxia, drowsiness– Uncommon: hypoNa, bradycardia and heart block,
asymptomatic neutropenia, vitamin D deficiency
• Pregnancy: little evidence for teratogen ? Dose related (700 mg/d)
Valproate
Sodium valproate (valproic acid, VPA)
• Previously, a solvent for barbiturate hypnotics, accidentally discovered to be more effective than barbiturate
• Plain tablet, sustained release form, IV, syrup
• Suppresses the spread of seizure activity via multiple mechanisms – Elevation of brain GABAergic, inhibitory activity– Decreases cortical excitability– Limits high-frequency repetitive firing of Na+- dependent action
potentials (blockade of Na+ channels)
Sodium valproate (valproic acid, VPA)
• A board spectrum antiepileptic drug
• Indications
– Drug of choices in generalized epilepsies (including absence)
– In JME: very good response (long life Rx)
– Also well effective in focal epilepsies
– Psychiatric (bipolar)
– Migraine prevention
Sodium valproate (valproic acid, VPA)• Enzyme inhibitor (with clinical benefit if on with lamotrigine)
• A small volume of distribution (high affinity for plasma albumin
– Lower protein binding: late pregnancy, elderly, liver, renal
• Adverse events
– Hair loss, weight gain, tremor, PCOS
– Hepatic failure, pancreatic necrosis• 1:15,000 usually in severely ill babies and young children
– Pregnancy: teratogenic dose dependent (1st trimester)
5/24/2016
4
• “Traditional AEDs: How we get benefit from them?
Clinical practice guideline
Evidence based support
National policy e.g. NLEM
FDA approval
Expert opinion
Clinical practice guideline
Clinical Practice Guidelines
NICE 2015 ILAE 2013 AAN 2015 THAI 2015
How to start & select AED?• The AED treatment strategy should be individualized
• When possible choose which AED to offer based on the epilepsy syndrome
• If this is not clear, base the decision on the presenting seizure
• AED therapy should only start on the recommendation of a specialist & once the diagnosis of epilepsy is confirmed
• The decision to start therapy should be taken between the person and specialist after a full discussion of the risks and benefits to treatment
NICE guideline 2015, ILAE guideline 2013, AAN guideline 2015, THAI guideline 2011
Goal of AED treatment
• Complete seizure free without side effects
National Institute for Health and Clinical Excellence (NICE) guideline 2015
5/24/2016
5
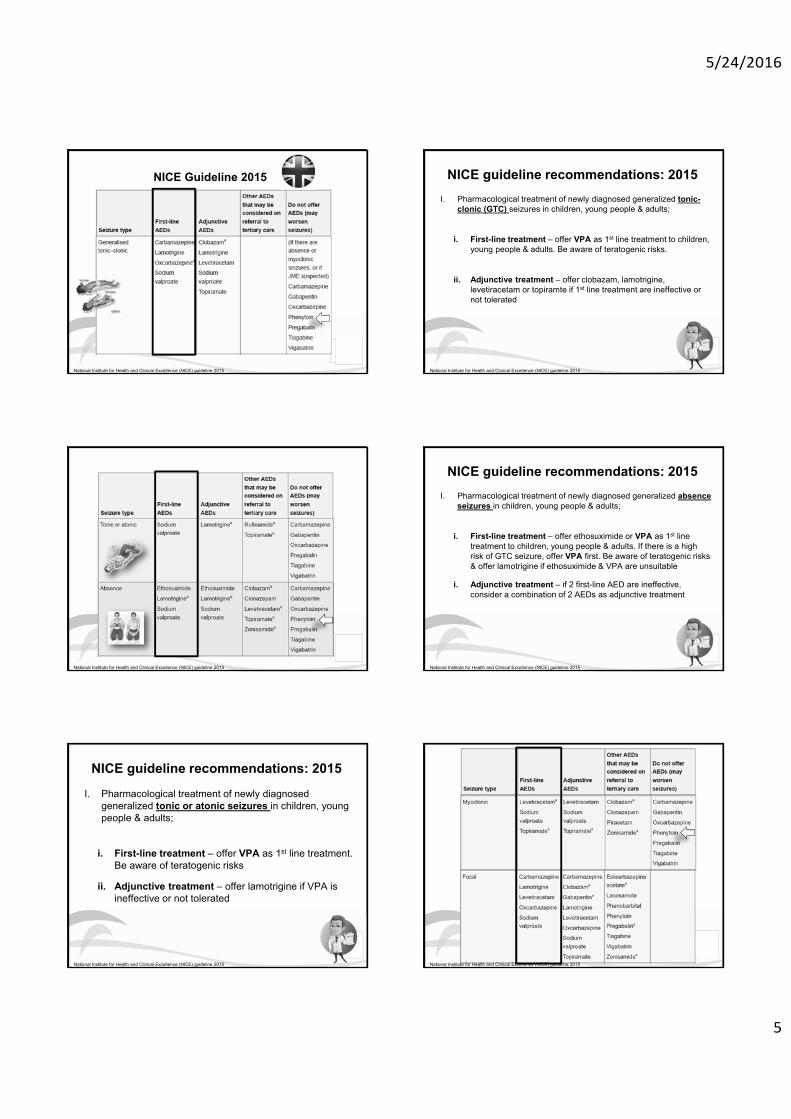
NICE Guideline 2015
National Institute for Health and Clinical Excellence (NICE) guideline 2015
NICE guideline recommendations: 2015I. Pharmacological treatment of newly diagnosed generalized tonic-
clonic (GTC) seizures in children, young people & adults;
i. First-line treatment – offer VPA as 1st line treatment to children, young people & adults. Be aware of teratogenic risks.
ii. Adjunctive treatment – offer clobazam, lamotrigine, levetiracetam or topiramte if 1st line treatment are ineffective or not tolerated
National Institute for Health and Clinical Excellence (NICE) guideline 2015
National Institute for Health and Clinical Excellence (NICE) guideline 2015
NICE guideline recommendations: 2015I. Pharmacological treatment of newly diagnosed generalized absence
seizures in children, young people & adults;
i. First-line treatment – offer ethosuximide or VPA as 1st line treatment to children, young people & adults. If there is a high risk of GTC seizure, offer VPA first. Be aware of teratogenic risks & offer lamotrigine if ethosuximide & VPA are unsuitable
i. Adjunctive treatment – if 2 first-line AED are ineffective, consider a combination of 2 AEDs as adjunctive treatment
National Institute for Health and Clinical Excellence (NICE) guideline 2015
NICE guideline recommendations: 2015
I. Pharmacological treatment of newly diagnosed generalized tonic or atonic seizures in children, young people & adults;
i. First-line treatment – offer VPA as 1st line treatment. Be aware of teratogenic risks
ii. Adjunctive treatment – offer lamotrigine if VPA is ineffective or not tolerated
National Institute for Health and Clinical Excellence (NICE) guideline 2015 National Institute for Health and Clinical Excellence (NICE) guideline 2015
5/24/2016
6
NICE guideline recommendations: 2015
I. Pharmacological treatment of newly diagnosed generalized myoclonic seizures in children, young people & adults;
i. First-line treatment – offer VPA as 1st line treatment. Be aware of teratogenic risks
ii. Adjunctive treatment – consider levetiracetam or topiramate if VPA is unsuitable or not tolerated. Be aware that topiramate has a less favourable side effect profiles than levetiracetam & VPA
National Institute for Health and Clinical Excellence (NICE) guideline 2015
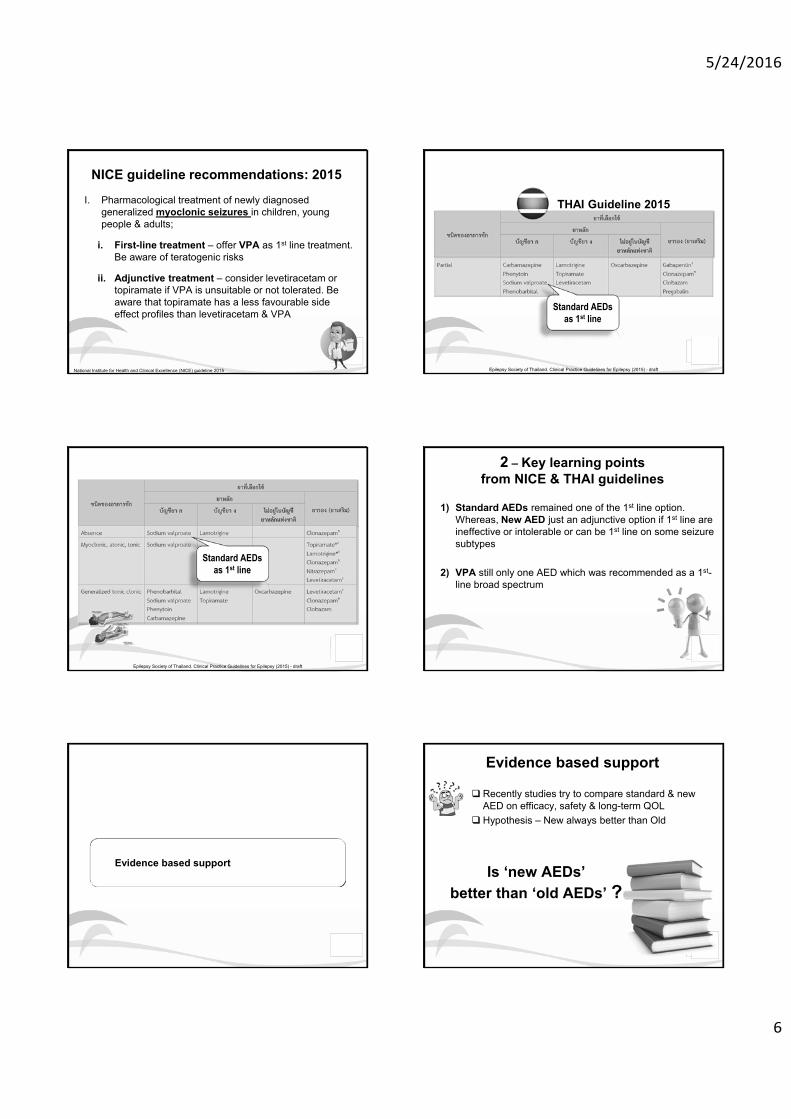
THAI Guideline 2015
Standard AEDsas 1st line
Epilepsy Society of Thailand. Clinical Practice Guidelines for Epilepsy (2015) - draft
Standard AEDsas 1st line
Epilepsy Society of Thailand. Clinical Practice Guidelines for Epilepsy (2015) - draft
1) Standard AEDs remained one of the 1st line option. Whereas, New AED just an adjunctive option if 1st line are ineffective or intolerable or can be 1st line on some seizure subtypes
2) VPA still only one AED which was recommended as a 1st-line broad spectrum
2 – Key learning pointsfrom NICE & THAI guidelines
Evidence based support
Evidence based support
Is ‘new AEDs’ better than ‘old AEDs’ ?
� Recently studies try to compare standard & new AED on efficacy, safety & long-term QOL
� Hypothesis – New always better than Old
5/24/2016
7
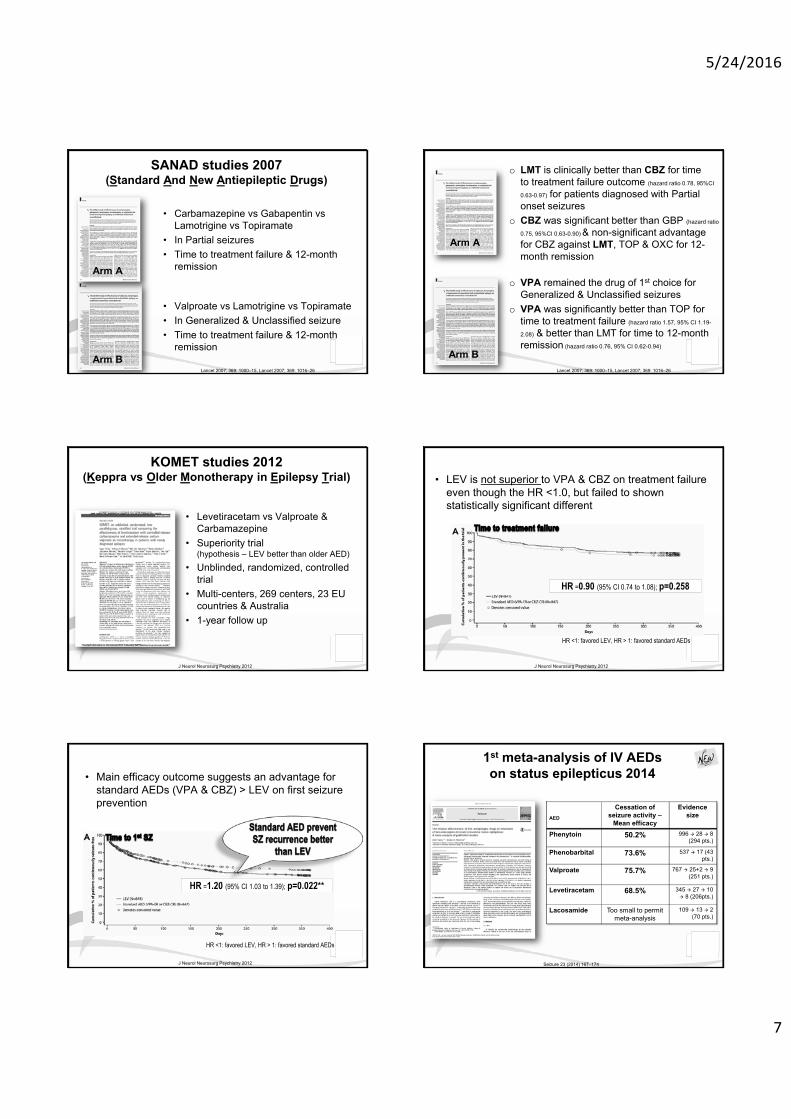
SANAD studies 2007(Standard And New Antiepileptic Drugs)
Arm A
Arm B
• Carbamazepine vs Gabapentin vs Lamotrigine vs Topiramate
• In Partial seizures• Time to treatment failure & 12-month
remission
• Valproate vs Lamotrigine vs Topiramate• In Generalized & Unclassified seizure• Time to treatment failure & 12-month
remission
Lancet 2007; 369: 1000–15, Lancet 2007; 369: 1016–26
o LMT is clinically better than CBZ for time to treatment failure outcome (hazard ratio 0.78, 95%CI
0.63-0.97) for patients diagnosed with Partial onset seizures
o CBZ was significant better than GBP (hazard ratio
0.75, 95%CI 0.63-0.90) & non-significant advantage for CBZ against LMT, TOP & OXC for 12-month remission
Arm A
Arm B
o VPA remained the drug of 1st choice for Generalized & Unclassified seizures
o VPA was significantly better than TOP for time to treatment failure (hazard ratio 1.57, 95% CI 1.19-
2.08) & better than LMT for time to 12-month remission (hazard ratio 0.76, 95% CI 0.62-0.94)
Lancet 2007; 369: 1000–15, Lancet 2007; 369: 1016–26
KOMET studies 2012(Keppra vs Older Monotherapy in Epilepsy Trial)
• Levetiracetam vs Valproate & Carbamazepine
• Superiority trial (hypothesis – LEV better than older AED)
• Unblinded, randomized, controlled trial
• Multi-centers, 269 centers, 23 EU countries & Australia
• 1-year follow up
J Neurol Neurosurg Psychiatry 2012
• LEV is not superior to VPA & CBZ on treatment failure even though the HR <1.0, but failed to shown statistically significant different
HR =0.90 (95% CI 0.74 to 1.08); p=0.258
J Neurol Neurosurg Psychiatry 2012
HR <1: favored LEV, HR > 1: favored standard AEDs
HR =1.20 (95% CI 1.03 to 1.39); p=0.022**
HR <1: favored LEV, HR > 1: favored standard AEDs
• Main efficacy outcome suggests an advantage for standard AEDs (VPA & CBZ) > LEV on first seizure prevention
J Neurol Neurosurg Psychiatry 2012
1st meta-analysis of IV AEDs on status epilepticus 2014
Seizure 23 (2014) 167–174
AED
Cessation of seizure activity –
Mean efficacy
Evidencesize
Phenytoin 50.2% 996 Æ 28 Æ 8 (294 pts.)
Phenobarbital 73.6% 537 Æ 17 (43 pts.)
Valproate 75.7% 767 Æ 25+2 Æ 9 (251 pts.)
Levetiracetam 68.5% 345 Æ 27 Æ 10 Æ 8 (206pts.)
Lacosamide Too small to permit meta-analysis
109 Æ 13 Æ 2 (70 pts.)
5/24/2016
8
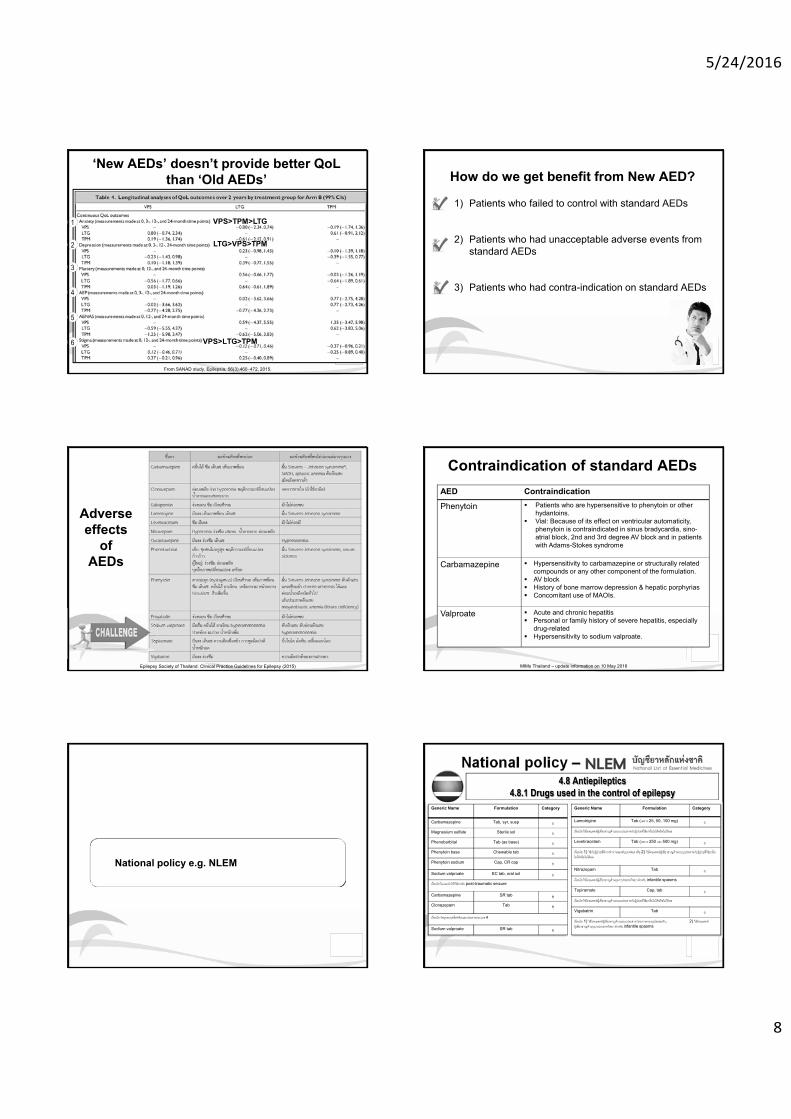
‘New AEDs’ doesn’t provide better QoLthan ‘Old AEDs’
From SANAD study, Epilepsia, 56(3):460–472, 2015.
1
2
3
4
5
6
VPS>TPM>LTG
VPS>LTG>TPM
LTG>VPS>TPM
1) Patients who failed to control with standard AEDs
2) Patients who had unacceptable adverse events from standard AEDs
3) Patients who had contra-indication on standard AEDs
How do we get benefit from New AED?
Epilepsy Society of Thailand. Clinical Practice Guidelines for Epilepsy (2015)
Adverse effects
of AEDs
MIMs Thailand – update information on 10 May 2016
Contraindication of standard AEDsAED ContraindicationPhenytoin � Patients who are hypersensitive to phenytoin or other
hydantoins.� Vial: Because of its effect on ventricular automaticity,
phenytoin is contraindicated in sinus bradycardia, sino-atrial block, 2nd and 3rd degree AV block and in patients with Adams-Stokes syndrome
Carbamazepine � Hypersensitivity to carbamazepine or structurally related compounds or any other component of the formulation.
� AV block� History of bone marrow depression & hepatic porphyrias� Concomitant use of MAOIs.
Valproate � Acute and chronic hepatitis� Personal or family history of severe hepatitis, especially
drug-related� Hypersensitivity to sodium valproate.
National policy e.g. NLEM
National policy –4.8 Antiepileptics
4.8.1 Drugs used in the control of epilepsyGeneric Name Formulation Category
Carbamazepine Tab, syr, susp กMagnesium sulfate Sterile sol กPhenobarbital Tab (as base) กPhenytoin base Chewable tab กPhenytoin sodium Cap, CR cap กSodium valproate EC tab, oral sol กเงื่อนไข ไมแ่นะนําให้ใช้สําหรับ post-traumatic seizure
Carbamazepine SR tab ขClonazepam Tab ข
เงื่อนไข วตัถอุอกฤทธ์ิต่อจิตและประสาทประเภท 4
Sodium valproate SR tab ข
Generic Name Formulation Category
Lamotrigine Tab (เฉพาะ 25, 50, 100 mg) งเงื่อนไข ใช้โดยแพทย์ผู้ เชี่ยวชาญด้านระบบประสาทกับผู้ ป่วยท่ีใช้ยาอ่ืนไมไ่ด้หรือไมไ่ด้ผล
Levetiracetam Tab (เฉพาะ 250 และ 500 mg) งเงื่อนไข 1) ใช้กับผู้ ป่วยท่ีมกีารทํางานของตบับกพร่อง หรือ 2) ใช้โดยแพทย์ผู้เชี่ยวชาญด้านระบบประสาทกับผู้ ป่วยท่ีใช้ยาอ่ืนไมไ่ด้หรือไมไ่ด้ผล
Nitrazepam Tab งเงื่อนไข ใช้โดยแพทย์ผู้ เชี่ยวชาญด้านกมุารประสาทวิทยา สําหรับ infantile spasms
Topiramate Cap, tab งเงื่อนไข ใช้โดยแพทย์ผู้ เชี่ยวชาญด้านระบบประสาทกับผู้ ป่วยท่ีใช้ยาอ่ืนไมไ่ด้หรือไมไ่ด้ผล
Vigabatrin Tab งเงื่อนไข 1) ใช้โดยแพทย์ผู้ เชี่ยวชาญด้านระบบประสาท โดยการควบคมุโรคลมชกั, 2) ใช้โดยแพทย์ผู้ เชี่ยวชาญด้านกมุารประสาทวิทยา สําหรับ infantile spasms
5/24/2016
9
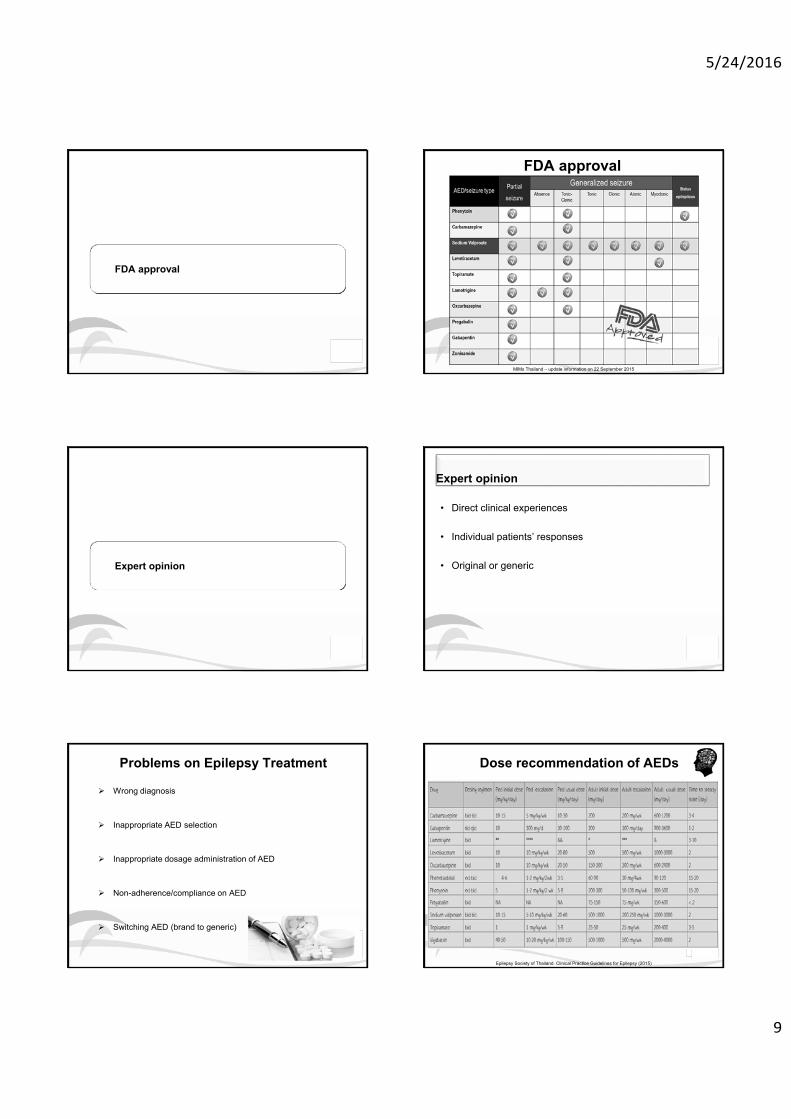
FDA approval
FDA approval
MIMs Thailand – update information on 22 September 2015
Expert opinion
Expert opinion
• Direct clinical experiences
• Individual patients’ responses
• Original or generic
Problems on Epilepsy Treatment
¾ Wrong diagnosis
¾ Inappropriate AED selection
¾ Inappropriate dosage administration of AED
¾ Non-adherence/compliance on AED
¾ Switching AED (brand to generic)
Epilepsy Society of Thailand. Clinical Practice Guidelines for Epilepsy (2015)
Dose recommendation of AEDs
5/24/2016
10
Summary
• Traditional antiepileptic medications show the benefit in treating epilepsies compared to newer medications with high cost-benefit ration
• All world-class and national guidelines recommend traditional antiepileptic medications as the first choice for both focal and generalized epilepsies
• The appropriate selection esp. board-spectrum antiepileptic medications provides the best outcome for patients with epilepsy
Module 4