Embed Size (px)
Citation preview

Use of Preintervention IntravascularUltrasound in Patients With Acute
Myocardial InfarctionAtsushi Tanaka, MD, Takahiko Kawarabayashi, MD, Haruyuki Taguchi, MD,Yoshiharu Nishibori, MD, Tsunemori Sakamoto, MD, Yukio Nishida, MD, and
Junichi Yoshikawa, MD
This study was designed to determine whether preinter-vention intravascular ultrasound (IVUS) imaging can as-sist in predicting the likelihood of acute coronary occlu-sion after primary angioplasty. Primary angioplasty is inwidespread use for the treatment of acute myocardialinfarction (AMI), although its usefulness is sometimescompromised by postprocedural acute coronary occlu-sion. If preintervention IVUS could be used to predictacute coronary occlusion, the task of determining treat-ment strategies for AMI would be significantly eased.Preintervention IVUS was performed without complica-tions in 46 patients with AMI using manually preparedcontrast medium. Coronary angiography was per-formed 1 hour after successful percutaneous translumi-nal coronary angioplasty. Acute coronary occlusion was
seen in 13 of 46 patients (28%). There were no differ-ences in the clinical characteristics and angiographicresults between the patients with and without occlusion.In patients with acute occlusion, the incidence of eccen-tric plaque (85% vs 36%, p <0.01) and echolucent area(92% vs 15%, p <0.01) was significantly higher than inthe occlusion-free patients. Most of the echolucent areaswere associated with eccentric plaques (88%). Eccentricplaques characterized by echolucent areas are prone toacute occlusion after primary balloon angioplasty forAMI. Preintervention IVUS is both a safe and a usefuladjunct to primary angioplasty. �2002 by ExcerptaMedica, Inc.
(Am J Cardiol 2002;89:257–261)
Intravascular ultrasound (IVUS) has been used topredict acute coronary occlusions after angioplasty
and to determine the cause of suboptimal results ofprimary angioplasty.1 If IVUS before interventionwere capable of predicting acute occlusion, the task ofdetermining treatment strategies for acute myocardialinfarction (AMI) would be greatly eased. This studysought to record the morphologic features of coronaryartery lesions using IVUS imaging before primaryangioplasty for AMI, and to determine whether find-ings from preintervention IVUS are of use in acutecoronary occlusion after primary balloon angioplasty.
METHODSSubjects: Of 72 consecutive patients with AMI ad-
mitted to Baba Memorial Hospital between September1997 and August 1999, a total of 46, all of whomunderwent IVUS imaging before acute-stage percuta-neous transluminal coronary angioplasty (PTCA),were enrolled in the present study.
No patient received thrombolytic therapy. A diag-nosis of AMI was based on chest pains lasting �30minutes, ST-segment elevation on the electrocardio-gram, and elevated serum creatine kinase levels.
Instances in which AMI occurred suddenly on ef-fort or at rest, without the patient complaining ofeffort angina before the onset of AMI, were classifiedas “sudden-onset AMI.” Patients in whom AMI oc-curred gradually, with pre-AMI effort angina, wereclassified as “changing-onset AMI.”
Criteria for exclusion: Of the original 72 patients, 26were excluded from the study because of the follow-ing criteria: cardiogenic shock (n � 2); heart failurerequiring mechanical ventilation (n � 4); inability toundergo coronary angiography (n � 6); ultimate re-ferral for coronary bypass (n � 3); culprit arterydifficult to identify on emergency coronary angio-grams (n � 1); restenosis of the culprit lesion afterPTCA (n � 4); distal lesions into which it was diffi-cult to insert an IVUS catheter (n � 5) or lesion on abend (n � 1).
Informed consent: The protocol of this study wasapproved by the ethics committee of Baba MemorialHospital. We obtained written informed consent fromall participants before coronary angiography.
Primary angioplasty and coronary angiography:Coronary angiography in all patients was per-
formed using a Judkins-type catheter via the femoralartery. PTCA was performed using a 7Fr guidingcatheter, 0.014-inch guidewire, and a monorail bal-loon catheter according to conventional methods. Theballoon type was semicompliant in all patients. Theballoon was inflated at the recommended nominalpressure.
Thrombolysis In Myocardial Infarction (TIMI)grade 3 flow and residual stenosis �50% were taken
From the Baba Memorial Hospital, Sakai; and First Department ofInternal Medicine, Osaka City University Medical School, Osaka,Japan. Manuscript received May 29, 2001; revised manuscript re-ceived and accepted October 10, 2001.
Address for reprints: Atsushi Tanaka, MD, Department of Cardiol-ogy, Baba Memorial Hospital, 4-244, Hamadera-funao-cho Higashi,Sakai, 592-8555 Japan. E-mail: [email protected].
257©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 89 February 1, 2002 PII S0002-9149(01)02224-X

as the criteria for “successful PTCA.” Because mostacute occlusions occur within 1 hour of intervention inJapan,2 coronary angiography was performed both 15minutes and 1 hour after successful conclusion of thePTCA procedure.
Acute coronary occlusion was defined as postpro-cedural TIMI grade 3 flow decreasing to TIMI grade 1or 0 flow within 1 hour of primary balloon angio-plasty. On this basis, patients were divided into 2groups—an acute occlusion group and an acute occlu-sion-free group. In the event of TIMI grade 2 flow anda large dissection being observed during coronaryangiography 1 hour after the procedure, stenting wasperformed.
All patients received 10,000 IU of heparin beforeangioplasty. Three thousands units of heparin wereadministered every hour during the procedure to main-tain an activated clotting time of �300 seconds. Afterangioplasty, intravenous infusion of heparin was con-tinued for at least 24 hours to maintain an activatedclotting time of 180 to 200 seconds. We administratedthe following antiplatelet therapy: aspirin 80 mg/day
after PTCA, and aspirin 80 mg/day and ticlopidine200 mg/day after stent implantation following PTCA.
Angiographic analysis: Coronary angiograms werereviewed separately by 2 independent observers (YoN and TS) unaware of the IVUS findings and clinicaldata. Quantitative angiography was performed off-lineusing the CMS-QCA system (CMS-MEDIS [MedicalImaging Systems, Leiden, the Netherlands]). The de-gree of perfusion was evaluated according to TIMIcriteria.3 Dissection was defined as the presence ofcontrast material in both the perfusing and nonperfus-ing lumina. Thrombus was defined as a filling defectseen in multiple projections surrounded by contrastand in the absence of calcification.
IVUS imaging protocol: All IVUS studies were per-formed before any catheter-based intervention onlyafter intracoronary administration of 200 �g of nitro-glycerin. The IVUS catheter (3.2Fr, Ultra cross, Bos-ton Scientific Scimed Inc., Maple Grove, Minnesota)was carefully advanced distal to the lesion under flu-oroscopic guidance. It was then pulled back automat-ically from the distal portion at 0.5 mm/s, facilitatingobservation of the lesion. IVUS images were recordedon S-VHS videotape for off-line analysis. While pull-ing back the catheter, we manually infused a contrastmedium for IVUS imaging, carefully observing thelesion.
Preparation of the contrast medium and the methodof infusion: A 17-ml contrast medium (Ioxaglic acid,Eiken Co. Ltd., Tokyo, Japan) was placed into a 25-mlplastic disposable syringe. Sonication was performedfor 3 minutes using a sonicator (Branson Japan Co.Ltd., Kanagawa, Japan) to separate the contrast me-dium into 2 layers. The lower part of the layer wasused as a positive contrast medium for IVUS imagingof the lumen. The other contrast medium was dilutedtwofold with saline solution and was used as a nega-tive contrast medium for identifying the lumen duringIVUS imaging. These contrast media for IVUS imag-ing were manually infused in doses of 3 to 5 ml underfluoroscopic guidance in a manner similar to that forconventional coronary angiography. The dose atwhich the coronary artery was filled on fluoroscopicimages without the myocardium being stained was
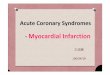
FIGURE 1. A, coronary angiograms obtained after crossing thewire. The midportion of the right coronary artery shows totalocclusion. B, C, and D, IVUS images obtained before primaryangioplasty. B, the lumen is filled with bright speckled echo ma-terials. C, the dissection is clearly visible. D, “echolucent area.”The low echoic material is pooled in eccentric plaque coveredwith a thin high echogenic layer. Acute coronary occlusion oc-curred after primary angioplasty in this patient, and bailoutstenting was required.
TABLE 1 Clinical Characteristics
Acute OcclusionGroup (n � 13)
Acute Occlusion-FreeGroup (n � 33)
Age (yrs) 62 � 9.0 63 � 10.9Men 11 (85%) 24 (73%)Coronary risk factors
Systemic hypertension 9 (69%) 20 (61%)Diabetes mellitus 6 (46%) 12 (36%)Smoking 10 (77%) 24 (73%)Hypercholesterolemia 6 (46%) 12 (36%)Family history 0 2 (6%)
Previous myocardial infarction 0 0Previous angioplasty 0 0Previous coronary bypass 0 0
Data are expressed as mean � SD or number (%).
258 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 89 FEBRUARY 1, 2002

regarded as the optimum dose of the IVUS contrastmedium.
Analysis of IVUS images: As previously described,the morphologic features of IVUS findings were in-terpreted by 2 independent observers (Yo N and HT)unfamiliar with angiographic and clinical data. A cul-prit lesion was considered eccentric if the ratio oflesion thickness on opposite sides of the lumen was�0.5 or if there was an arc of disease-free vessel wall.Fissure was defined as an abrupt, focal, superficialbreak in the linear continuity of the plaque that ex-tended in a radial direction. Dissection was defined asrupture of the vessel wall creating �1 neolumina. Anecholucent area was defined as a pooling of lowechoic material covered with a thin high echoic layer.A typical image is shown in Figure 1. Bright echoes atthe surface of the lumen with an arc of �90° ofacoustic shadowing were defined as superficial cal-cium. Bright echoes deep in the vessel wall �90° withacoustic shadowing were defined as deep wall cal-cium.
Validation of plaque composition and measure-ment of external elastic membrane cross-sectionalarea by IVUS have been reported previously.4–6
Computer planimetry (TapeMeasure, Indec Systems,Mountain View, California) was used to measure le-sion site and reference segment external elastic mem-brane cross-sectional area. We measured externalelastic membrane cross-sectional area, the area en-compassed by the ultrasonic media-adventitia border,by tracing the leading edge of the adventitia.
Statistical analysis: Results are expressed as mean� SD for continuous variables. Qualitative data arepresented as number (%). Continuous variableswere compared by Student’s t test, and categoricaldata by Fisher’s exact test. A multivariate logisticregression model was used to determine predictorsof acute occlusion. Independent variables includedin the model were classic coronary risk factors,IVUS morphology (echolucent area, dissection, cal-cium deposit), IVUS measurements (lesion lumen
cross-sectional area, lesion externalelastic membrane cross-sectionalarea), angiographic findings (throm-bus, dissection, TIMI grade, lesionsite), and procedure of angioplasty(balloon-to-artery ratio, inflationpressure, residual stenosis after pri-mary angioplasty). A p value �0.05was considered statistically signifi-cant.
RESULTSBaseline clinical characteristics and
angiographic results: Acute occlusionwas seen in 13 patients (28%). Theuse of glycoprotein IIb/IIIa inhibitorsis yet to be approved in Japan. Ac-cordingly, none was used in thepresent study.
All of these cases were detectedwithin 15 minutes of “successful” balloon angio-plasty. All 13 occlusions were “rescued” using stentimplantation. One month later, there was no incidenceof recurrent occlusion in any patient. Patient charac-teristics are summarized in Table 1.
Preintervention angiographic results and angioplastyprocedures are summarized in Table 2.
Preintervention IVUS findings: Coronary artery le-sions were observed with IVUS in all patients withoutany serious complications. Adequate images were ob-tained from all patients. Coronary artery lesions wereobserved with IVUS within mean 5.24 � 6.32 hoursof the onset of AMI.
Blood flow distal to the lesion was detected in allcases, and the lumen identified. Bright speckled echomaterial was observed in all cases during the infusionof negative contrast medium at the stenotic lesion ormore distal occluded site.
Compared with coronary angiograms, IVUS was amore sensitive modality for detecting fissure or dis-section (IVUS 42% vs coronary angiography 7%, p�0.01).
Acute coronary occlusion and IVUS findings: Thepreintervention IVUS findings are summarized in Ta-ble 3. Eccentric plaque was more frequently observedin the acute occlusion group than in the acute occlu-sion-free group (85% vs 36%, p �0.01). The inci-dence of echolucent areas was significantly higher inthe acute occlusion group than in the acute occlusion-free group (echolucent area, acute occlusion group92% vs acute occlusion-free 15%, p �0.01). Multi-variate regression analysis showed that only echolu-cent area was predictive of acute occlusion (p �0.05).
Clinical manifestations of patients with echolucentarea: Table 4 lists the clinical manifestations of pa-tients presenting with an echolucent area. Sudden on-set-type AMI was more frequently observed in pa-tients with than without an echolucent area (82% vs48%, p � 0.03). Bailout stent implantation was re-quired more often in those with than without anecholucent area (94% vs 52%, p �0.01).
TABLE 2 Coronary Angiographic Findings and Angioplasty Procedure
Acute OcclusionGroup (n � 13)
Acute Occlusion-FreeGroup (n � 33)
Coronary artery examinedLeft anterior descending 7 (54%) 21 (64%)Left circumflex 1 (8%) 2 (6%)Right coronary 5 (38%) 10 (30%)
TIMI grade 0 or 1 11 (85%) 22 (67%)With collateral vessels 9 (69%) 16 (48%)Thrombus 2 (15%) 8 (24%)Dissection 2 (15%) 1 (3%)Reference diameter (mm) 2.81 � 0.71 2.82 � 0.74Balloon-to-artery ratio 1.13 � 0.22 1.14 � 0.33Inflation pressure (atm) 8.6 � 2.2 7.7 � 2.3Dissection after primary angioplasty (%) 3 (23%) 10 (33%)Residual stenosis after primary angioplasty (%) 19.2 � 11.3 26.4 � 15.9
Data are expressed as mean � SD or number (%).
CORONARY ARTERY DISEASE/PREINTERVENTION IVUS IN AMI 259

DISCUSSIONAcute coronary occlusion and findings of preinter-
vention IVUS: The rate of the patients with acute cor-onary occlusion observed in this report (28%) washigh compared with that previously reported.7–10 Thiswas considered to be caused by including the patientsin the category of those with acute occlusion whenthey had TIMI flows of 0 to 1 on angiography per-formed 15 minutes after successful PTCA.
The presence of an echolucent area is stronglyassociated with acute occlusion after primary balloonangioplasty. Our results suggested that acute coronaryocclusion arose from lesion morphology rather thanthe aspect of the angioplasty procedure. Preinterven-tion IVUS can be performed safely and provides thede novo culprit lesion morphology during the acutephase. Therefore, we consider that preinterventionIVUS is useful in AMI.
The morphologic features of the echolucent areaare similar to those of the lipid pool observed inpathologically vulnerable plaques. Plaque rupture isthought to be a major cause of acute coronary syn-dromes including AMI. Thrombus is formed as a
result of plaque rupture and exposure of the lipid poolcontents to blood, leading to rapid coronary arteryocclusion.11 Balloon angioplasty causes vascular in-jury. This injury may expose the contents of theecholucent area to the lumen of the coronary artery,subsequently causing rapid thrombus formation.These thrombi obstruct the coronary artery lumen. Inother words, “artificial plaque rupture” caused by bal-loon angioplasty may take place in acute coronaryocclusion after primary balloon angioplasty.
Clinical manifestation of patients with echolucentarea: Most of the plaques in our study containing anecholucent area were associated with eccentric plaqueand fissure/dissection. This plaque morphology wasreminiscent of the features of pathologic plaque rup-ture. Of course, AMI occurred suddenly in most ofthese patients.
In contrast, approximately 50% of patients with-out an echolucent area presented with a changing-onset type of AMI. These patients had morpholo-gies that were different from those in patients withan echolucent area. Concentric plaque was fre-quently observed in these patients. Fissure or dis-section was exhibited in only 28% of cases. Theseresults suggest that the cause of AMI is not plaquerupture alone. According to 1 pathologic study,plaque erosion may be one cause of acute coronarysyndrome.12 Repeated thrombus formation and or-ganization in the site of erosion may graduallymake the coronary artery lumen narrow, which mayresult in the changeable pattern of onset. Furtherstudy of this type of AMI is needed.
Study limitations: The interpretation of plaques inthe present study was performed according to estab-lished IVUS criteria. However, ultrasound classifica-tion of echolucent plaque can be difficult due to manyfactors, including instrumental and operator settings(especially gain settings), visual effects (especiallyduring the use of ultrasound contrast media), anddifficulty in distinguishing between real echolucentplaque and plaque with signal attenuation due to tightlumen. Other scenarios for IVUS signal attenuationinclude microcalcification and angle dependencies ofultrasound waves reflected by fibrous cap.
1. Iwabuchi M, Haruta S, Taguchi A, Ichikawa Y, Genda T, Katai S, Imaoka T,Shimizu Y, Owa M. Intravascular ultrasound findings after successful primaryangioplasty for acute myocardial infarction: predictors of abrupt occlusion. J AmColl Cardiol 1997;30:1437–1444.2. Nobuyoshi M. Coronary Angiography and Intervention (in Japanese). Tokyo,Japan: Igakushoin, 1990:422–430.3. The TIMI IIIB Investigators. Effects of tissue plasminogen activator and acomparison of early invasive and conservative strategies in unstable angina andnon-Q-wave myocardial infarction. Results of the TIMI IIIB Trial. Thrombolysisin Myocardial Ischemia. Circulation 1994;89:1545–1556.4. Nishimura RA, Edwards WD, Warnes CA, Reeder GS, Holmes DR Jr, TajikAJ, Yock PG. Intravascular ultrasound imaging: in vitro validation and patho-logic correlation. J Am Coll Cardiol 1990;16:145–154.5. Tobis JM, Mallery J, Mahon D, Lehmann K, Zalesky P, Griffith J, Gessert J,Moriuchi M, McRae M, Dwyer ML. Intravascular ultrasound imaging of humancoronary arteries in vivo. Analysis of tissue characterizations with comparison toin vitro histological specimens. Circulation 1991;83:913–926.6. Potkin BN, Bartorelli AL, Gessert JM, Neville RF, Almagor Y, Roberts WC,Leon MB. Coronary artery imaging with intravascular high-frequency ultrasound.Circulation 1990;81:1575–1585.7. Grines CL, Browne KF, Marco J, Rothbaum D, Stone GW, O’Keefe J, Overlie
TABLE 3 IVUS Findings
Acute OcclusionGroup (n � 13)
Acute Occlusion-FreeGroup (n � 33)
IVUS imagesEccentric 11 (85%)* 12 (36%)Fissure/dissection 8 (62%) 11 (33%)Echolucent area 12 (92%)* 5 (15%)Superficial calcium 5 (38%) 12 (36%)Deep wall calcium 3 (23%) 13 (39%)
Distal EEM CSA (mm2) 13.1 � 4.6 12.6 � 4.9Lesion EEM CSA (mm2) 13.0 � 4.9 13.0 � 4.5Lesion lumen CSA (mm2) 1.9 � 0.5 2.2 � 0.9Proximal EEM CSA (mm2) 17.0 � 3.7 15.1 � 5.0
*p �0.01.Data are expressed as mean � SD or number (%).CSA � cross-sectional area; EEM � external elastic membrane.
TABLE 4 Clinical Manifestations of Patients With and WithoutEcholucent Area
With EcholucentArea (n � 17)
Without EcholucentArea (n � 29)
Systemic hypertension 12 (71%) 17 (59%)Diabetes mellitus 6 (35%) 12 (41%)Smoker 13 (76%) 21 (72%)Hypercholesterolemia
(�220 mg/dl)6 (35%) 12 (41%)
Obesity 3 (18%) 4 (14%)Family history 0 2 (6%)Sudden-onset AMI 14 (82%) 14 (48%)IVUS images
Eccentric plaque 15 (88%)* 8 (28%)Fissure/dissection 11 (65%)* 8 (28%)Superficial calcium 7 (41%) 10 (34%)Deep wall calcium 6 (35%) 10 (34%)
*p �0.03.Data are expressed as number (%).
260 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 89 FEBRUARY 1, 2002

P, Donohue B, Chelliah N, Timmis GC, et al. A comparison of immediateangioplasty with thrombolytic therapy for acute myocardial infarction. The Pri-mary Angioplasty in Myocardial Infarction Study Group. N Engl J Med 1993;328:673–679.8. Buccino KR, Brenner AS, Browne KF. Acute reocclusion during percutaneoustransluminal coronary angioplasty: immediate and long-term outcome. CathetCardiovasc Diagn 1989;17:75–79.9. Detre KM, Holmes DR Jr, Holubkov R, Cowley MJ, Bourassa MG, Faxon DP,Dorros GR, Bentivoglio LG, Kent KM, Myler RK. Incidence and consequencesof peri-procedural occlusion. The 1985–1986 National Heart; Lung: and BloodInstitute Percutaneous Transluminal Coronary Angioplasty Registry. Circulation1990;82:739–750.
10. Brodie BR, Grines CL, Ivanhoe R, Knopf W, Taylor G, O’Keefe J, WeintraubRA, Berdan LG, Tcheng JE, Woodlief LH, Califf RM, O’Neill WW. Six-monthclinical and angiographic follow-up after direct angioplasty for acute myocardialinfarction. Final results from the Primary Angioplasty Registry. Circulation1994;90:156–162.11. Richardson PD, Davies MJ, Born GV. Influence of plaque configuration andstress distribution on fissuring of coronary atherosclerotic plaques. Lancet 1989;2:941–944.12. van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of intimalrupture or erosion of thrombosed coronary atherosclerotic plaques is character-ized by an inflammatory process irrespective of the dominant plaque morphology.Circulation 1994;89:36–44.
CORONARY ARTERY DISEASE/PREINTERVENTION IVUS IN AMI 261