Embed Size (px)
Citation preview

1096
Original Articles Korean Circulation J 1998;;;;28((((7))))::::1096-1104
급성 하벽 심근경색증에서 경색관련혈관의 예측을 위한
초기 심전도의 유용성
동아대학교병원 순환기내과,1 광혜병원 내과2
차광수1·김영대1·김무현1·김형권2·김종성1
Usefulness of the Initial Electrocardiogram for Predicting the Infarct-Related Artery in Acute Inferior Myocardial Infarction
Kwang Soo Cha, MD1, Young-Dae Kim, MD1, Moo Hyun Kim, MD1, Hyeong Kweon Kim, MD2 and Jong Seong Kim, MD1 1Department of Cardiology, Dong-A University Hospital, Pusan, 2Department of Internal Medicine, Kwanghye General Hospital, Pusan, Korea ABSTRACT
Background and Objectives:Eectrocardiogram (ECG) may provide valuable informations regarding the infarct-related artery (IRA), which may be of guidance in selecting the therapeutic modality. ST segment elevation in inferior leads usually indicates occlusion of right coronary artery, less often left circumflex coronary artery or rarely occlusion of left anterior descending coronary artery may be the cause. We are to determine whether the initial ECG can differentiate the right coronary artery (RCA) or left circumflex artery (LCx) occlusion in acute inferior myocardial infarction (IMI). Materials and Method:We compared retrospectively the ECG recorded within 12 hours from the onset of chest pain with coronary angiograaphic findings in 85 patients(34% of all 250 patients) having electrocardiographic criteria for IMI. Results:1) Angiographic characteristics. Of the 85 patients, IRA was RCA in 65 (76%) (38[58%] proximal, 27[42%] distal to first right ventricular branch), and LCx in 20 (24%) (nine[45%] proximal to first obtuse marginal branch or involving a high first marginal branch, eleven[55%] distal obstruction). RCA dominance was more common in RCA occlusion group (100% vs 80%, p=0.001), and LCx dominance in LCx occlusion group (15% vs 0%, p=0.001). No significant difference was noted between two groups regarding vessels diseased, involvement of left anterior descending coronary artery and contralateral artery (RCA or LCx), location of the lesion. 2) Electrocardiographic characteritics. Lateral limb leads (I, aVL):ST segment depression (≥1 mm) was more common in RCA occlusion group (82% vs 45%, p=0.001). Isoelectric ST segment in I was more common in LCx occlusion group(100% vs 15%, p=0.001). Left precordial leads (V5,6):ST segment elevation (≥1 mm) was more common in LCx occlusion group (60% vs 15%, p=0.001). Isoelectric ST segment was more common in RCA occlusion group (57% vs 20%, p=0.004). ST segment depression (≥1 mm) was not different between two groups. Right precordial leads (V1-4):ST segment changes were not different between two groups. Lead I and left precordial leads (V5,6):Isoelectric ST segment in lead I and ST segment elevation (≥1 mm) in V5 or V6 was more common in LCx occlusion group (60% vs 5%, p<0.05, sensitivity 60% specificity 95% positive/negative predictive value
논문접수일:1998년 4월 2일
심사완료일:1998년 7월 21일
교신저자:김영대, 602-715 부산광역시 서구 동대신동 3가 1 동아대학교병원 순환기내과
전화:(051) 240-5620, 21·전송:(051) 242-1449
E-mail:[email protected]

1097
80%/89%, test accuracy 87%). Amplitude of R wave in V1:Amplitude of R wave in V was greater in LCx occlusion group (3.60±1.42 mm vs 2.20±1.42 mm, p<0.05). Conclusion:The initial electrocardiogram was useful in differentiating LCx occlusion from RCA occlusion in patients with IMI. Absence of ST segment depression in I and aVL, and ST segment elevation in V5,6, isoelectric ST segment in I, tall R wave in V1 were significantly more common in LCx occlusion. ((((Korean Circulation J 1998;28((((7)))):1096-1104)))) KEY WORDS:Acute inferior myocardial infarction·Infarct-related artery·Electrocardiogram.
서 론
급성 심근경색증 환자에서 성공적인 재관류를 이루고
경색의 크기를 감소시키기 위하여 최선의 치료 전략을
선택해야 하는 문제는 현대의 임상의사에게 매우 중요하
다. 심전도는 급성 심근경색증에서 가장 빠르고 쉽게 이
용할 수 있는 진단 방법일 뿐 아니라 치료 방침을 선택
하는데 도움을 줄 수 있는 경색관련혈관과 경색혈관내에
서 폐쇄 위치에 관한 정보를 제공해 줄 수 있다. 전흉부
유도에서 ST절이 상승되면 좌전하행 관상동맥의 폐쇄를
정확하게 예측할 수 있다. 하부 유도에서 ST절 상승은
보통 우관상동맥의 폐쇄에 의해 초래되나 좌회선 관상동
맥의 폐쇄에 의해서도 가능하며 드물게는 좌전하행 관상
동맥의 폐쇄가 원인이 된다.1-3) 심전도의 제한점과 좌회
선 관상동맥이 심장의 후부에 위치하는 이유로 좌회선
관상동맥의 폐쇄때 체표면 심전도에서 ST절 상승이 드
물게 초래되고 특히 하부 유도에서 ST절 상승은 50%
이하에서 관찰된다고 알려져 있다.4-6)
저자들은 급성 하벽 심근경색증에서 초기 심전도로
써 경색관련혈관(우관상동맥 또는 좌회선 관상동맥)을
구별할 수 있는지를 알아보기 위하여 급성 하벽 심근경
색증 환자에서 흉통 발생 12시간 이내에 기록된 초기
심전도와 관상동맥 조영소견을 비교하였다.
재료 및 방법
재 료
1992년 1월부터 1997년 9월사이 급성 흉통으로 동
아대학교병원을 내원하여 급성 심근경색증으로 처음
진단되어 치료받았던 521명중 심전도에서 전벽 또는
비Q파 심근경색증 환자 271명(52%)를 제외시키고 급
성 하벽 심근경색증 환자 250(48%)명중에서 아래의
포함기준을 만족하는 91명(36%, 남자 75명 여자 16명,
평균 나이 58±9세)을 얻었다. 포함기준은 (1) 30분 이
상 지속되는 흉통 시작후 12시간 이내에 내원하여 심전
도검사를 하였거나 12시간 이내에 기록된 심전도를 가
지고 내원한 경우에서, (2) 사지 유도 Ⅱ, Ⅲ, aVF중 두
개 이상의 유도에서 1 mm 이상의 ST절 상승을 보이며,
(3) 입원 동안 관상동맥 및 좌심실 조영술을 받은 경우
로 하였고, 심방세동 또는 각차단이 있었던 경우는 제외
하였고 WPW 증후군은 한 예도 없었다(Fig. 1). 91명중
좌전하행 관상동맥의 폐쇄에 의하여 하부 및 전흉부 유
도에서 ST절 상승이 동시에 초래되었던 6명을 제외한
85명(전체 급성 하벽 심근경색증 환자 250명의 34%)
의 대상군에서 흉통 발생 12시간 이내에 기록된 초기 심
전도와 관상동맥 조영소견을 비교하였다.
심전도 분석
흉통 시작 12시간 이내에 기록된 심전도의 유무와
관상동맥 및 좌심실 조영술의 시행 유무를 확인하여 대
상군 85명을 선정한 후 관상동맥 및 좌심실 조영소견
에 대한 지식 없이 심전도를 분석하였다. ST절 편위
(deviation)는 J점에서 0.08초 후에 측정하였고, 측벽
유도(Ⅰ, aVL, Ⅴ5, Ⅴ6)를 포함한 모든 유도에서 1
mm(0.1 mV) 이상의 ST절 상승 또는 하강이 있는 경
우 유의한 편위로 인정하였다.
Fig. 1. Summary of the selection of study population. MI:myocardial infarction.

Korean Circulation J 1998;28(7):1096-1104 1098
관상동맥 및 좌심실 조영소견 분석
관상동맥 및 좌심실 조영소견의 분석은 심전도 분석
과 다른 시기에 환자의 심전도에 대하여 알지 못하는
다른 조사자에 의하여 일괄적으로 행하여졌다. 경색관
련혈관의 정의는 관상동맥 조영술에서 완전 또는 아완
전 폐쇄가 있거나 관상동맥내 혈전 또는 죽상반 파열의
증거가 잔여 협착과 동반되어 있는 관상동맥의 분포 영
역이 이면성(biplane) 좌심실 조영술에서 무운동(as-
ynergy)을 보이는 좌심실 분절과 일치될 때로 하였다.
유의한 관상동맥 협착은 주요 심외막 관상동맥 분절에
제일 심하게 보이는 사면에서 내경 협착이 75% 이상
인 경우로 정의하였다. 우관상동맥과 좌회선 관상동맥
에 동시에 유의한 협착이 있었던 10명에서는 병변의
형태적 특징과 무운동성 좌심실 분절과의 연관을 고려
하여 경색관련혈관을 정하였다. 병변의 위치는 우관상
동맥 협착의 경우 제일우심실분지(first right vent-
ricular branch)의 근위부에 위치할 때 근위부 병변으로,
좌회선 관상동맥 협착의 경우 제일둔각변연분지(first
obtuse marginal branch)의 근위부에 위치하거나 좌회
선 관상동맥의 상부에서 분지하는 제일둔각변연분지의
근위부에 위치할 때 근위부 병변으로 정의하였다.
통계 및 분석
자료 분석은 PC-SAS version 6.12 프로그램을 이용
하여 하였다. 연속 변수는 평균±표준편차로 표시하였으며
양 군사이의 비교는 Student’s t test를 이용하여 검정하
였고, 범주형 변수는 절대 수치(%)로 표시하였으며 양 군
사이의 비교는 검사의 적절성을 고려하여 Chi-squareχ2
test 또는 Fisher’s exact test를 이용하여 검정하였다. p
값이 0.05 미만인 경우에 통계적 유의성을 두었다.
결 과
대상 환자의 임상적 특징 및 혈관조영 소견의 특징
경색관련혈관은 대상 환자 85명중 65명(76%)에서 우
관상동맥(근위부 38명[58%], 원위부 27명[42%]), 20
명(24%)에서 좌회선 관상동맥(근위부 9명[45%], 원위
부 11명[55%])이었다. 우관상동맥 우위(dominance)는
Table 1. Clinical and angiographic characteristics of the 85 patients
Left circumflex artery (n=20) Right coronary artery (n=65) P value
Age (yr) 56.05±7.74 58.85±10.06 NS Male sex 19 (95%) 50 ( 77%) NS Angiographic diagnosis
1 VD 15 (75%) 50 ( 77%) NS 2 VD 3 (15%) 11 ( 17%) NS 3 VD 2 (10%) 4 ( 6%) NS
Dominance RCA 16 (80%) 65 (100%) 0.001 LCx 3 (15%) 0 ( 0%) 0.001 Balanced 1 ( 5%) 0 ( 0%) NS
LAD disease 4 (20%) 9 ( 14%) NS Contralateral artery disease 4 (20%;RCA) 6 (9%;LCx) NS Lesion location
Proximal 9 (45%) 38 ( 58%) NS Distal 11 (55%) 27 ( 42%) NS
Collaterals to IRA 2 (10%) 14 ( 22%) NS Total CK (U/L) 2718.17±1485.89 3241.17±1618.64 NS CK-MB (U/L) 241.83±140.11 325.00±191.73 NS Segments of RWMA 3.45±0.86 3.29±0.69 NS
VD:vessel diseased;RCA:right coronary artery;LCx:left circumflex coronary artery;LAD:left anterior des-cending coronary artery;IRA:infarct-related artery;CK:creatine kinase;CK-MB:creatine kinase-MB fraction;RWMA:regio-nal wall motion abnormalities

1099
우관상동맥 폐쇄군에서 유의하게 많았다(100% vs 80%,
p=0.001). 좌회선 관상동맥 우위는 좌회선 관상동맥 폐
쇄군에서 유의하게 많았다(15% vs 0%, p=0.001). 병
변 혈관의 수, 좌전하행 관상동맥 질환, 반대측 혈관(우관
상동맥 또는 좌회선 관상동맥)의 병변, 병변 부위의 위치
등은 양 군에서 유의한 차이가 없었다(Table 1).
심전도 특징
측부 사지유도(Ⅰ, aVL)
Ⅰ 또는 aVL 유도에서 ST절 상승(1 mm 이상)은
좌회선 관상동맥 폐쇄군과 우관상동맥 폐쇄군사이에
유의한 차이가 없었다(5% vs 3%). Ⅰ 또는 aVL 유도
에서 ST절 하강(1 mm 이상)은 우관상동맥 폐쇄군에
서 유의하게 많았다(82% vs 45%, p=0.001, 예민도
82% 특이도 55% 양성예측율 85% 음성예측율 48%
검사정확도 75%)(Table 2, 3). Ⅰ 유도에서 등전위
(isoelectric) ST절은 좌회선 관상동맥 폐쇄군에서 유
의하게 많았다(100% vs 15%, p=0.001)(Table 2).
좌흉부유도(V5,6)
V5 또는 V6 유도에서 ST절 상승(1 mm 이상)은 좌
회선 관상동맥 폐쇄군에서 유의하게 많았다(60% vs
15%, p=0.001, 예민도 60% 특이도 85% 양성예측율
55% 음성예측율 87% 검사정확도 79%)(Table 2 and
3). V5 또는 V6 유도에서 ST절 하강(1 mm 이상)은 양
군사이에 유의한 차이가 없었다(20% vs 28%). V5 또는
V6 유도에서 등전위 ST절은 우관상동맥 폐쇄군에서 유
의하게 많았다(57% vs 20%, p=0.004)(Table 2).
우흉부유도(V1-4)
좌회선 관상동맥 폐쇄군과 우관상동맥 폐쇄군사이에
V1-4 유도에서 ST절 상승 및 하강, 등전위 ST절은 유
의한 차이가 없었다(5% vs 5%, 30% vs 43%, 65%
vs 52%)(Table 2).
Ⅰ 유도 및 좌흉부유도(V5,6)
Ⅰ 유도에서 등전위 ST절과 V 5,6 유도에서 ST절 상
승은 좌회선 관상동맥 폐쇄군에서 유의하게 많았다(60 %vs
5%, p<0.05, 예민도 60% 특이도 95% 양성예측율 80%
음성예측율 89% 검사정확도 87%)(Table 2, 3).
V1 유도에서 R파의 크기
V1 유도에서 R파의 크기는 좌회선 관상동맥 폐쇄군
에서 유의하게 높았다(3.60±1.42mm vs 2.20±1.42
mm, p<0.05)(Table 2).
Table 2. Electrocardiographic characteristics of the 85 patients
Left circumflex artery (n=20)
Right coronary artery (n=65) P value
Lateral limb leads (I, aVL) ST elevation (≥1 mm) 1 ( 5%) 2 ( 3%) NS ST depression (≥1 mm) 9 ( 45%) 53 (82%) 0.001
Isoelectric ST in I 20 (100%) 10 (15%) 0.001 Lateral precordial leads (V5,6)
ST elevation (≥1 mm) 12 ( 60%) 10 (15%) 0.001 ST depression (≥1 mm) 4 ( 20%) 18 (28%) NS Isoelectric ST 4 ( 20%) 37 (57%) 0.004
Precordial leads (V1-4) ST elevation (≥1 mm) 1 ( 5%) 3 ( 5%) NS ST depression (≥1 mm) 6 ( 30%) 28 (43%) NS Isoelectric ST 13 ( 65%) 34 (52%) NS
Combined isoelectric ST in I and ST elevation in V5,6 12 ( 60%) 3 ( 5%) <0.05 R wave amplitude in V1 (mm) 3.60±1.42 2.20±1.42 <0.05 R/S ratio in V1>1 2 ( 10%) 1 ( 2%) NS Peak R wave amplitude in I, aVL (mm) 4.79±1.25 5.83±2.43 NS Peak R wave amplitude in V5,6 (mm) 10.74±4.43 12.91±4.09 NS

Korean Circulation J 1998;28(7):1096-1104 1100
고 찰
Table 3. Summary of diagnostic accuracy for the significant electrocardiographic variables
ECG variable IRA Sensitivity Specificity PPV NPV Test accuracy
ST depression (≥1 mm) in I, aVL RCA 82% 55% 85% 48% 75% Isoelectric ST in I LCx 100% 85% 67% 100% 88% ST elevation (≥1 mm) in V5,6 LCx 60% 85% 55% 87% 79% Isoelectric ST in V5,6 RCA 57% 80% 90% 36% 62% Isoelectric ST in I and ST LCx 60% 95% 80% 89% 87% elevation (≥1 mm) in V5,6 IRA: infarct-related artery;PPV:positive predictive value;NPV:negative predictive value;RCA: rightcoronary artery;LCx:left circumflex coronary artery
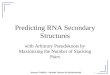
Fig. 2. Typical electrocardiograms of right coronary artery (RCA) (A) and left circumflex coronary artery (LCx)(B) occlusion in acute inferior myocardial infarction. A:ST segment depression in Ⅰ, aVL and no ST-segment el-evation in V5,6 suggest RCA occlusion. No ST segment depression in V1-4 may suggest involvement of right ventricle.Occlusion of proximal RCA prior to right ventricular branch was demonstrated in coronary angiography. B:No STsegment depression in Ⅰ, ST segment elevation in V 5,6, tall R wave in V 1 suggest LCx occlusion and large infarction.Occlusion of proximal LCx prior to first obtuse marginal branch was demonstrated in coronary angiography.
AAAA BBBB

1101
본 연구는 급성 하벽 심근경색증 환자에서 흉통 발생
12시간 이내에 기록된 초기 심전도가 경색관련혈관(우
관상동맥 또는 좌회선 관상동맥)을 예견하는데 유용함을
보여주었다. 즉, Ⅰ와 aVL 유도에서 ST절 하강이 없는
경우, V5,6 유도에서 ST절 상승, Ⅰ 유도에서 등전위 ST
절, V1 유도에서 큰 R파 등은 좌회선 관상동맥 폐쇄와
연관된 하벽 경색증때 유의하게 많았고 예민도, 특이도,
예측도, 진단정확도가 높은 인자들이었다(Table 3).
Ⅰ, aVL 유도
Ⅰ과 aVL 유도는 좌심실의 상측면을 향하고 있으며
특히 aVL 유도는 하벽에 대하여 진정으로 상대적인
(reciprocal) 유일한 유도로 여겨지고 있다. Dunn 등
7)의 협착 부위와 심전도 변화 부위의 상관성에 관한
연구에서 좌심실 측벽의 침범은 근위부 좌회선동맥이
나 둔각변연분지(obtuse marginal branch)의 병변을
예측할 수 있고, 하부 유도의 변화는 원위부 좌회선동
맥이나 원위부 변연분지(distal marginal branch)의 협
착때 흔하고 측부 유도의 변화는 중간부 좌회선동맥 협
착때 흔히 나타났다. Hasegawa 등8)은 근위부 좌회선
동맥 폐쇄때 aVL 유도에서 ST절 상승이 생기고 원위
부 좌회선동맥 폐쇄때 하부 유도에서 ST절 상승이 생
긴다고 하였다. 하벽 심근경색증때 측부 사지유도에서
ST절 하강은 단순한 상호 현상으로 경색이 후부, 첨부
또는 우심실 영역으로 확장되는 것에 의해 영향을 받지
않는 것으로 여겨지고 있다.9)
Ⅰ, aVL 유도에서 ST절 상승은 Huey 등,6) Bairey
등,10) Kanemoto 등11)의 연구에서 좌회선동맥 폐쇄때
유의하게 많았으며(각각 32% vs 3%, 17% vs 0%,
43% vs 8%), Hasdai 등12)의 연구에서 Ⅰ과 aVL 유도
에서 유의한 ST절 하강이 없는 경우 근위부 좌회선동맥
폐쇄를 시사하였다(각각 예민도 71%와 86%, 특이도
65%와 100%). Kontos 등13)의 연구에서는 Ⅰ 유도에
서 ST절 상승 또는 등전위는 좌회선동맥 폐쇄때 유의하
게 많았으나(67% vs 38%), aVL 유도에서 ST절 상승
은 경색관련혈관의 구별에 도움이 되지 못하였다(0% vs
3%). 본 연구에서도 Ⅰ 유도에서 ST절 등전위는 좌회
선동맥의 폐쇄때 유의하게 많았다(100% vs 15%).
반면 Ⅰ, aVL 유도에서 ST절 하강은 Huey 등,6)
Bairey 등,10) Kanemoto 등11)의 연구에서 우관상동맥
폐쇄때 유의하게 많았으며(각각 78% vs 44%, 81%
vs 33%, 69% vs 29%), Hasdai 등12)의 연구에서 Ⅰ
과 aVL 유도에서 유의한 ST절 하강이 있는 경우 우관
상동맥 폐쇄를 시사하였다(각각 예민도 70%와 100%,
특이도 63%와 38%). Kontos 등13)의 연구에서 Ⅰ 유
도에서 ST절 하강은 우관상동맥 폐쇄때 유의하게 많
았으나(58% vs 23%), aVL 유도에서 ST절 하강은 경
색관련혈관의 구별에 도움이 되지 못하였다(90% vs
77 %). 본 연구에서도 Ⅰ, aVL 유도에서 ST절 하강은
우관상동맥 폐쇄때 유의하게 많았다(82% vs 45%).
V5,6 유도
V5,6 유도는 좌심실의 상측면을 향하는 Ⅰ, aVL 유도
와는 달리 심첨부 근처의 하측면을 향하고 있어 우관상
동맥 또는 좌회선동맥의 폐쇄에 의한 하부-심첨부 허
혈에 의하여 영향을 받게 된다. 즉 V5,6 유도에서 ST절
하강은 경색관련혈관의 예견에 도움이 되지 못할 것이
다. Huey 등,6) Bairey 등,10) Kanemoto 등,11) Hasdai
등,12) Kontos 등13)의 연구에서 V5,6 유도에서 ST절
하강은 경색관련혈관의 구별에 도움이 되지 못하였고
본 연구에서도 양 군에서 빈도가 유사하였다(20% vs
28%). 하벽 심근경색증에서 V5,6 유도에서 ST절 하강
이 있으면 좌전하행동맥을 포함하는 다혈관질환을 예
견할 수 있다고 보고되고 있다.14-16)
Huey 등,6) Bairey 등,10) Kanemoto 등11)의 연구에
서 V5,6 유도에서 ST절 상승은 좌회선동맥 폐쇄때 유
의하게 많았으나(각각 47% vs 9%, 83% vs 24%,
36% vs 8%), Kontos 등13)의 연구에서는 경색관련혈
관의 구별에 도움이 되지 못하였다(46% vs 22%). 본
연구에서 V5,6 유도에서 ST절 상승은 좌회선동맥 폐쇄
때 유의하게 많았다(60% vs 15%).
V1-4 유도
하벽 심근경색증때 동반되는 전흉부 ST절 하강의 원인
으로 하벽 ST절 벡터에 대하여 단순히 대칭적인 상호 변
화,14)17-21) 좌심실의 후측벽을 포함한 광범위한 하벽 경
색,22-26) 동시에 발생한 전벽 심근의 허혈27-29)이 제시되
고 있다. Lew 등30)은 전흉부 ST절 하강과 하벽 ST절
상승의 연관성이 우심실 침범과 측벽 ST절 상승이 배제
될 경우 증가된다고 하며 전흉부와 하벽의 ST절 변화의
상호 관계가 우심실과 좌심실 측부의 침범 여부에 따라
변화한다고 하였다. 심근 관류스캔을 이용한 다른 연구에

Korean Circulation J 1998;28(7):1096-1104 1102
서 하벽 경색때 전흉부 ST절 하강은 후부 또는 측부 허
혈과 허혈의 위험에 있는 심근이 증가될 때 나타나며 좌
전하행동맥 질환과는 연관되지 않는다고 하였다.23)31)32)
Huey 등,6) Bairey 등,10) Kanemoto 등11)의 연구에
서 V1-4 유도에서 ST절 하강은 경색관련혈관의 구별
에 도움이 되지 못하였고 본 연구에서도 양 군에서 빈
도가 유사하였다(30% vs 43%). Kontos 등13)의 연구
에서는 V1 또는 V2 유도에서 ST절 하강이 좌회선동맥
폐쇄때 유의하게 많았고(92% vs 41%), 좌회선동맥 폐
쇄에 대하여 특이성은 없으나 예민한 지표라 하였으며
(예민도 약 90%, 특이도 약 55%), V1 또는 V2 유도에
서 ST절 하강이 없는 경우 좌회선동맥 폐쇄를 배제할
수 있는 음성예측율이 높다(약 95%)고 하였다. 하벽 심
근경색증때 경색관련혈관에 따른 전흉부 유도에서 ST절
하강 빈도의 차이에 대한 설명으로 우관상동맥 폐쇄때는
약 50%에서 우심실이 침범되어 전흉부 유도의 ST절 상
호 변화가 상쇄되어 ST절 하강이 감소하는데 비하여 측
벽 또는 후측벽을 침범하는 좌회선동맥 폐쇄때는 전흉부
유도에서 ST절 하강이 증가한다고 하였다.30-33)
우관상동맥 페쇄는 우심실의 허혈 또는 경색을 동반
하므로 우심실 침범의 지표인 V1-4 유도에서 ST절 상
승이 존재하면 경색관련혈관의 구별에 도움이 되리라
여겨지지만,34) Huey 등,6) Bairey 등,10) Kontos 등13)
의 연구에서 V1-4 유도에서 ST절 상승은 경색관련혈
관의 구별에 도움이 되지 못하였고 본 연구에서도 양
군에서 각각 5%로 빈도가 동일하였다.
V4R 유도에서 ST-T절의 변화
V4R 유도는 하벽 경색증때 우심실경색의 진단뿐만
아니라 폐쇄 혈관을 예측하는데도 이용될 수 있다.35)
V4R 유도에서 ST절 상승이 있는 경우 근위부 우관상
동맥 폐쇄를 시사하고 ST절 상승이 없는 경우 원위부
우관상동맥이나 좌회선동맥의 폐쇄를 의미하는데 T파
가 양성이면 원위부 우관상동맥 폐쇄를, T파가 음성이
면 좌회선동맥 폐쇄를 시사한다. 그러나 V4R 유도에서
ST절 상승은 10시간이 경과하면 대부분 소실되므로
급성 하벽 경색증 환자에서는 내원 즉시 표준 심전도와
함께 V4R 유도를 기록하여야 한다.
임상적 응용
본 연구와 다른 연구6-8)10-13)34)의 결과를 종합하면
첫째, 하부 유도에서 ST절 상승이 있으면서,
1) Ⅰ, aVL 유도에서 ST절 하강은 우관상동맥의 폐
쇄때 많고, ST절 하강이 없으면(ST절 상승 또는 등전
위) 근위부 좌회선동맥 폐쇄가 많다.
2) V5,6 유도에서 ST절 상승은 좌회선동맥때 많고, ST
절 하강은 경색관련혈관의 구별에 도움이 되지 못하며 좌
전하행동맥을 포함하는 다혈관질환일 가능성이 있다.14-16)
3) V1-4 유도에서 ST절 하강은 대부분의 연구에서
는 경색관련혈관의 구별에 도움이 되지 못하였으나 한
연구13)에서 좌회선동맥 폐쇄때 많았고, ST절 상승은
경색관련혈관의 구별에 도움이 되지 못했다.
4) V1 유도에서 비정상 R파는 좌회선동맥 폐쇄때 많
고 광범위한 경색과 다혈관질환을 시사하였다.
5) V4R 유도에서 ST절 상승이 있는 경우 근위부 우
관상동맥 폐쇄를 시사하고, ST절 상승이 없는 경우 T
파가 양성이면 원위부 우관상동맥 폐쇄를, T파가 음성
이면 좌회선동맥 폐쇄를 시사한다.34)
둘째, 임상적으로 급성 심근경색증이 의심되나 하부
유도와 측부 유도 모두에서 ST절 상승이 보이지 않는
경우도 좌회선동맥 폐쇄가 많다.6)
급성 하벽 심근경색증에서 경색관련혈관과 폐쇄 위치
를 빠르고 정확하게 진단할 수 있으면 치료 방침을 결정
하고 동반될 합병증과 그 심한 정도를 예견하고 대처하
는데 도움이 될 것이다. 예컨대 우관상동맥에 대한 일차
적 풍선확장술이 다른 중한 합병증을 초래할 수 있다는
점에서 우관상동맥의 폐쇄에 의한 하벽 심근경색증때 지
연 풍선확장술을 상황에 따라 고려할 수도 있으며, V1 유
도에서 비정상 R파가 보이는 하벽 심근경색증때 좌회선
동맥에 의한 경색이 광범위하며 다혈관질환임을 예견하
고 적극적인 치료 방법을 강구해야 할 것이다.6)36)37)
요 약
연구배경:
심전도는 급성 심근경색증에서 치료 방침을 선택하
는데 도움을 줄 수 있는 경색관련혈관의 확인과 경색혈
관내에서 폐쇄 병변의 위치에 관한 정보를 제공해 줄
수 있다. 하부 유도에서 ST절 상승은 보통 우관상동맥
의 폐쇄에 의해 초래되나 좌회선 관상동맥의 폐쇄에 의
해서도 가능하며 드물게는 좌전하행 관상동맥의 폐쇄
가 원인이 된다. 저자들은 급성 하벽 심근경색증 환자

1103
에서 흉통 발생 12시간 이내에 기록된 초기 심전도로
써 경색관련혈관(우관상동맥 또는 좌회선 관상동맥)을
구별할 수 있는지를 알아보았다.
재료 및 방법:
1992년 1월부터 1997년 9월사이 급성 하벽 심근경
색증으로 진단된 250명중 85명(34%)의 환자에서 흉
통 발생 12시간 이내에 기록된 심전도와 관상동맥 조
영소견을 후향적으로 비교하였다.
결 과:
1) 혈관조영 소견의 특징
경색관련혈관은 대상 환자 85명중 65명(76%)에서 우
관상동맥(근위부 38명[58%], 원위부 27명[42%]), 20
명(24%)에서 좌회선 관상동맥(근위부 9명[45%], 원위
부 11명[55%])이었다. 우관상동맥 우위(domin-ance)
는 우관상동맥 폐쇄군에서 유의하게 많았다(100% vs
80%, p=0.001). 좌회선 관상동맥 우위는 좌회선 관상동
맥 폐쇄군에서 유의하게 많았다(15% vs 0%, p=0.001).
병변 혈관의 수, 좌전하행 관상동맥 질환, 반대측 혈관(우
관상동맥 또는 좌회선 관상동맥)의 병변, 병변 부위의 위
치 등은 양 군에서 유의한 차이가 없었다.
2) 심전도 특징:
측부 사지유도(Ⅰ, aVL):Ⅰ 또는 aVL 유도에서
ST절 하강(1 mm 이상)은 우관상동맥 폐쇄군에서 유
의하게 많았다(82% vs 45%, p=0.001). Ⅰ 유도에서
등전위(isoelectric) ST절은 좌회선 관상동맥 폐쇄군에
서 유의하게 많았다(100% vs 15%, p=0.001).
좌흉부유도(V5,6):V5 또는 V6 유도에서 ST절 상승
(1 mm 이상)은 좌회선 관상동맥 폐쇄군에서 유의하게
많았다(60% vs 15%, p=0.001). 등전위 ST절은 우
관상동맥 폐쇄군에서 유의하게 많았다(57% vs 20%,
p=0.004). ST절 하강(1 mm 이상)은 양 군사이에 유
의한 차이가 없었다(20% vs 28%).
흉부유도(V1-4):좌회선 관상동맥 폐쇄군과 우관상
동맥 폐쇄군사이에 V1-4 유도에서 ST절 상승 및 하강,
등전위 ST절은 유의한 차이가 없었다(5% vs 5%,
30 % vs 43%, 65% vs 52%).
Ⅰ 유도 및 좌흉부유도(V5,6):Ⅰ 유도에서 등전위
ST절과 V5,6 유도에서 ST절 상승은 좌회선 관상동맥
폐쇄군에서 유의하게 많았다(60% vs 5%, p<0.05, 예
민도 60% 특이도 95% 양성예측율 80% 음성예측율
89% 검사정확도 87%).
V1 유도에서 R파의 크기:V1 유도에서 R파의 크기
는 좌회선 관상동맥 폐쇄군에서 유의하게 높았다(3.60
±1.42 mm vs 2.20±1.42 mm, p<0.05).
결 론:
초기 심전도는 급성 하벽 심근경색증 환자에서 우관상
동맥 폐쇄와 좌회선 관상동맥 폐쇄를 구별하는데 유용하
였다. Ⅰ와 aVL 유도에서 ST절 하강이 없는 경우, V5,6
유도에서 ST절 상승, Ⅰ 유도에서 등전위 ST절, V1 유도
에서 큰 R파는 좌회선 관상동맥 폐쇄때 유의하게 많았다.
중심 단어:급성 하벽 심근경색증·경색관련혈관·심전도.
REFERENCES
1) Hamby RI, Hoffman I, Hilsenrath J, Aintablian A, Sha-nies S, Padmanabhan VS. Clinical, hemodynamic and angiographic aspect of inferior and anterior myocardial infarctions in patients with angina pectoris. Am J Cardiol 1974;34:513-9.
2) Roeske WR, Savage RM, O’Rourke RA, Bloor CM. Clinicopathologic correlations in patients after myoca-rdial infarction. Circulation 1981;63:36-45.
3) Fuchs RM, Achuff SC, Grunwald L, Yin F, Griffith L. Elec-trocardiographic localization of coronary artery narrowings: studies during myocardial ischemia and infarction in pati-ents with one-vessel disease. Circulation 1982;66: 1168-76.
4) Stadius ML, Maynard C, Fritz JK, Davis K, Ritchie JL, Sheehan F, et al. Coronary anatomy and left ventricular function in the first 12 hours of acute myocardial infar-ction: the Western Washington Randomized Intracoronary Streptokinase Trial. Circulation 1985;72:292-301.
5) O’Keefe JH Jr, Rutherford BD, McConahay DR, Ligon RW, Johnson WL Jr, Giorgi LV, et al. Early and late re-sults of coronary angioplasty without antecedent throm-bolytic therapy for acute myocardial infarction. Am J Cardiol 1989;64:1221-30.
6) Huey BL, Beller GA, Kaiser DL, Gibson RS. A compre-hensive analysis of myocardial infarction due to left circ-umflex artery occlusion: comparison with infarction due to right coronary artery and left anterior descending art-ery occlusion. J Am Coll Cardiol 1988;12:1156-66.
7) Dunn RF, Newman HN, Bernstein L, Harris PJ, Roubin GS, Morris J, et al. The clinical features of isolated left circumflex coronary artery disease. Circulation 1984;69: 477-84.
8) Hasegawa K. A study of electrocardiographic ST-seg-ment deviations of acute stage in myocardial infarction caused by right coronary or left circumflex artery obstr-uction. J Jap Coll Cardiol 1986;26:1308.
9) Birnbaum Y, Sclarovsky S, Mager A, Strasberg B, Rec-havia E. ST segment depression in aVL: a sensitive ma-rker for acute inferior myocardial infarction. Eur Heart J 1993;14:4-7.
10) Bairey CN, Shah PH, Lew AS, Hulse S. Electrocardiog-raphic differentiation of occlusion of the left circumflex versus the right coronary artery as a cause of inferior

Korean Circulation J 1998;28(7):1096-1104 1104
acute myocardial infarction. Am J Cardiol 1987;60:456-9. 11) Kanemoto N, Hosokawa J. Early diagnosis of the site of
infarction and the infarct-related coronary artery in pat-ients with acute inferior myocardial infarction. Jpn Heart J 1992;33:423-35.
12) Hasdai D, Birnbaum Y, Herz I, Sclarovsky S, Mazur A, Solodky A. ST segment depression in lateral limb leads in inferior wall acute myocardial infarction. Eur Heart J 1995;16:1549-53.
13) Kontos MC, Desai PV, Jesse RL, Ornato JP. Usefulness of the admission electrocardiogram for identifying the in-farct-related artery in inferior wall acute myocardial inf-arction. Am J Cardiol 1997;79:182-4.
14) Lew HY, Yun YS, Kang HS, Choue CW, Kim KS, Kim MS, et al. The prognostic significance of maximal prec-ordial ST-segment depression in patients with acute inf-erior myocardial infarction. Kor Circ J 1996;26:781-6.
15) Strasberg B, Pinshas A, Barbash GI, Hod H, Rat S, Har ZY, et al. Importance of reciprocal ST segment depres-sion in leads V5 and V6 as an indicator of disease of the left anterior descending coronary artery in acute inferior wall myocardial infarction. Br Heart J 1990;63:339-41.
16) Hasdai D, Sclarovsky S, Solodky A, Sulkes J, Strasberg B, Birnbaum Y. Prognostic significance of maximal pre-cordial ST-segment depression in right (V1 to V3) versus left(V4 to V6) leads in patients with inferior wall acute myocardial infarction. Am J Cardiol 1994;74:1081-4.
17) Lee SK, Baek HJ, Suh SM, Chun BD, Lee CK, Kim SW, et al. Clinical significance of precordial ST segment depre-ssion in patients with acute inferior myocardial infarction. Kor J Int Med 1992;43:447-51.
18) Lew HY, Yun YS, Kang HS, Choue CW, Kim KS, Kim MS, et al. The significance of the precordial ST-segment depression (V1-3) in acute inferior myocardial infarction. Kor J Int Med 1997;53:398-403.
19) Wasserman AG, Ross AM, Bogaty D, Richardson DW, Hutchinson RG, Rois JC. Anterior ST segment depression during acute inferior myocardial infarction: evidence for the reciprocal change theory. Am Heart J 1983;106: 516-20.
20) Ferguson DW, Pandian N, Kioschos M, Marcus ML, White CW. Angiographic evidence that reciprocal ST-segment depression during acute myocardial infarction does not indicate remote ischemia: Analysis of 23 pati-ents. Am J Cardiol 1984;53:55-62.
21) Tzivoni D, Chenzbraun A, Keren A, Benhorin J, Gottlieb S, Lonn E, et al. Reciprocal electrocardiographic chan-ges in acute myocardial infarction. Am J Cardiol 1985; 56:23-6.
22) Goldberg HL, Borer JS, Jacobstein JG, Kluger J, Sch-eidt SS, Alonso DR. Anterior S-T segment depression in acute inferior myocardial infarction: indicator of post-erolateral infarction. Am J Cardiol 1981;48:1009-15.
23) Gibson RS, Crampton RS, Watson DD, Taylor GJ, Car-abello BA, Holt ND, et al. Precordial ST-segment depre-ssion during acute inferior myocardial infarction: clinical, scintigraphic and angiographic correlations. Circulation 1982;66:732-41.
24) Ong L, Valdellon B, Coromilas J, Brody R, Reiser P, Morrison P. Precordial S-T segment depression in inferior myocardial infarction Evaluation by quantitative thall-ium-201 scintigraphy and technetium-99m ventriculogr-
aphy. Am J Cardiol 1983;51:734-9. 25) Ruddy TD, Tasuda T, Gold HK, Leinbach RC, Newell
JB, McKusick KA, et al. Anterior ST segment depre-ssion in acute myocardial infarction as a marker of greater inferior, apical and posterolateral damage. Am Heart J 1986;112:1210-6.
26) Wong CK, Freedman SB, Bautovich G, Bailey BP, Bernstein L, Kelly DT. Mechanism and significance of precordial ST-segment depression during inferior wall acute myocardial infarction associated with severe narr-owing of the dominant right coronary artery. Am J Ca-rdiol 1993;71:1025-30.
27) Cha DH, Tahk SJ, Jang YS, Kim HS, Yoon JH, Chung NS, et al. The significance of reciprocal ST-segment dep-ression in acute inferior myocardial infarction. Kor Circ J 1991;21:1-6.
28) Cho JG, Ahn YK, Park JH, Jeong MH, Park JC, Kang JC. Reciprocal ST-segment depression in acute inferior myocardial infarction: possible indicator of concomitant left anterior descending coronary artery stenosis. Kor Circ J 1993;23:350-5.
29) Salcedo JR, Baird MG, Chambers RJ, Beanlands DS. Significance of reciprocal ST segment depression in an-terior precordial leads in acute inferior myocardial infar-ction: concomitant left anterior descending artery disease? Am J Cardiol 1981;46:915-21.
30) Lew AS, Maddahi J, Shah PK, Weiss AT, Peter T, Ber-man DS, et al. Factors that determine the direction and magnitude of precordial ST-segment deviations during inferior wall acute myocardial infarction. Am J Cardiol 1985;55:883-8.
31) Lew AS, Weiss AT, Shah PK, Maddahi J, Peter T, Ganz W, et al. Precordial ST segment depression during acute inferior myocardial infarction: early thallium-201 scinti-graphic evidence of adjacent posterolateral or infer-oseptal involvement. J Am Coll Cardiol 1985;5:203-9.
32) Edmunds JJ, Gibbons RJ, Bresnahan JF, Clements IP. Significance of anterior ST-depression in inferior wall ac-ute myocardial infarction. Am J Cardiol 1994;73:143-8.
33) Zehender M, Kasper W, Kauder E, Schonthaler M, Geibel A, Olschewski M, et al. Right ventricular infar-ction as an independent predictor of prognosis after acute inferior myocardial infarction. N Engl J Med 1993;328: 981-8.
34) Geft IL, Shah PK, Rodriguez L, Hulse S, Maddahi J, Berman DS, et al. ST elevations in leads V1-V5 due to right ventricular infarction and their mechanism. Am J Cardiol 1984;53:991-6.
35) Braat SH, Gorgels APM, Bar FW, Wellens HJ. Value of the ST-T segment in lead V4R in inferior wall myocardial infarction to predict the site of coronary arterial occl-usion. Am J Cardiol 1988;62:140-2.
36) Gacioch GM, Topol EJ. Sudden paradoxic clinical dete-rioration during angioplasty of the occluded right cor-onary artery in acute myocardial infarction. J Am Coll Cardiol 1989;14:1202-9.
37) Abbotsmith CW, Topol EJ, George BS, Stack RS, Kere-iakes DJ, Candela RJ, et al. Fate of patients with acute myocardial infarction with patency of the infarctrelated vessel achieved with successful thrombolysis versus res-cue angioplasty. J Am Coll Cardiol 1990;16:770-8.