Embed Size (px)
Citation preview

Cardiologia PediatricaSeconda Università degli Studi di Napoli
A.O. R.N. dei Colli-MonaldiNapoli
Cardiologia PediatricaSeconda Università degli Studi di Napoli
A.O. R.N. dei Colli-MonaldiNapoli
Valutazione del neonato con sospetta ipertensione polmonare
Hypoxiemic infant
•Full or near-term neonate
•O2 test:•PaO2 >100mmHg: lungdisease• PaO2 50-100mmHg: lungdisease or congenital heartdisease (CHD)• PaO2 < 50mmHg: persitent pulmonaryhypertension of the newborn (PPHN) or (CHD)
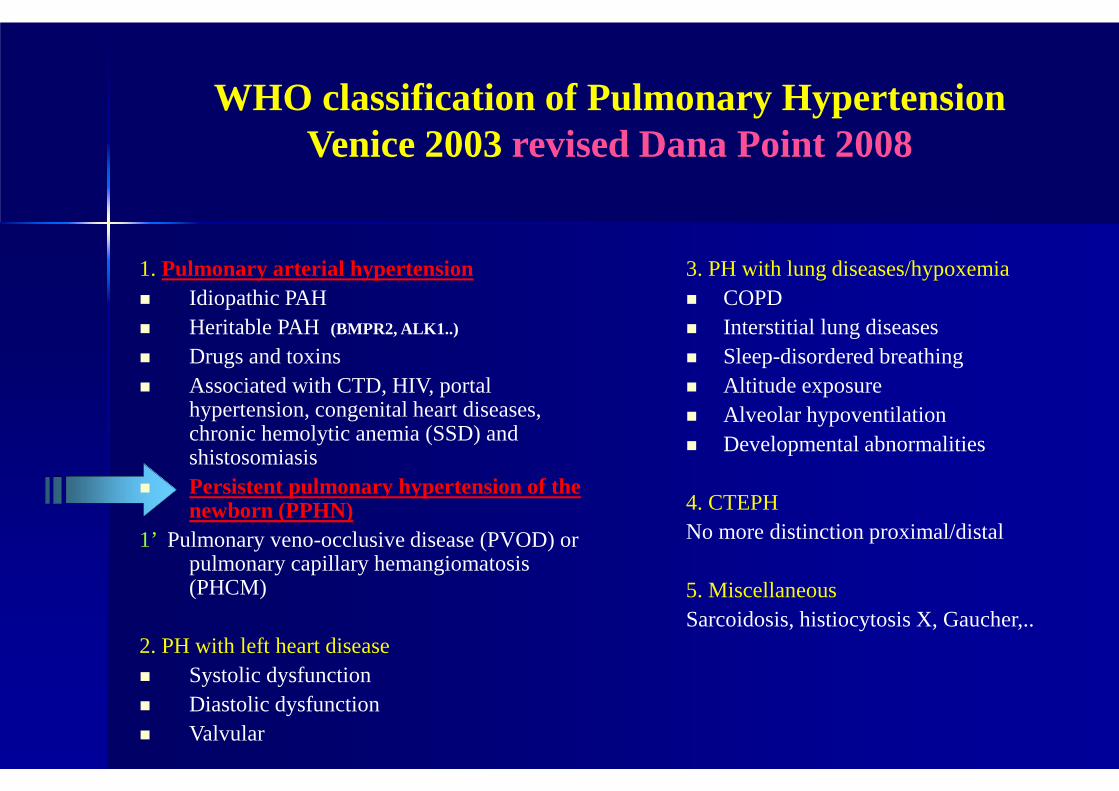
WHO classification of Pulmonary HypertensionVenice 2003revised Dana Point 2008
1. Pulmonary arterial hypertension � Idiopathic PAH� Heritable PAH (BMPR2, ALK1..)
� Drugs and toxins� Associated with CTD, HIV, portal
hypertension, congenital heart diseases, chronic hemolytic anemia (SSD) and shistosomiasis
� Persistent pulmonary hypertension of the newborn (PPHN)
1’ Pulmonary veno-occlusive disease (PVOD) or pulmonary capillary hemangiomatosis(PHCM)
2. PH with left heart disease� Systolic dysfunction� Diastolic dysfunction� Valvular
3. PH with lung diseases/hypoxemia� COPD� Interstitial lung diseases� Sleep-disordered breathing� Altitude exposure� Alveolar hypoventilation� Developmental abnormalities
4. CTEPHNo more distinction proximal/distal
5. MiscellaneousSarcoidosis, histiocytosis X, Gaucher,..
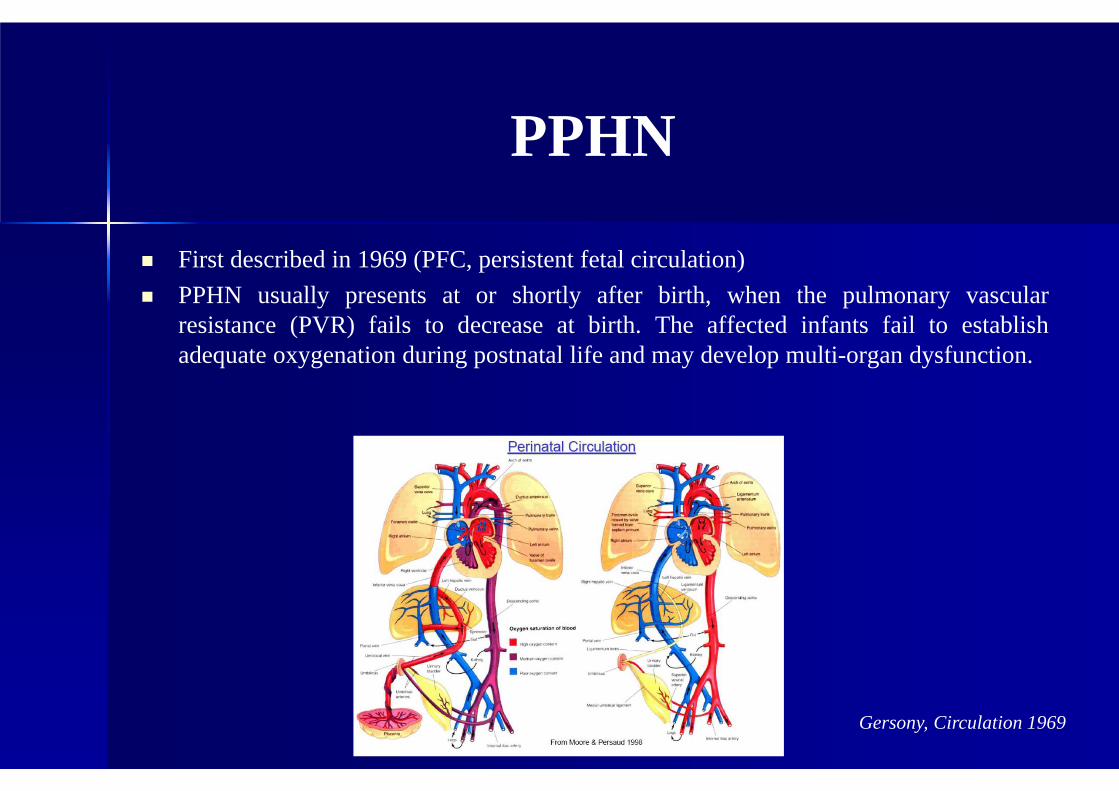
PPHN
� First described in 1969 (PFC, persistent fetal circulation)
� PPHN usually presents at or shortly after birth, when the pulmonary vascularresistance (PVR) fails to decrease at birth. The affected infants fail to establishadequate oxygenation during postnatal life and may develop multi-organ dysfunction.
Gersony, Circulation 1969
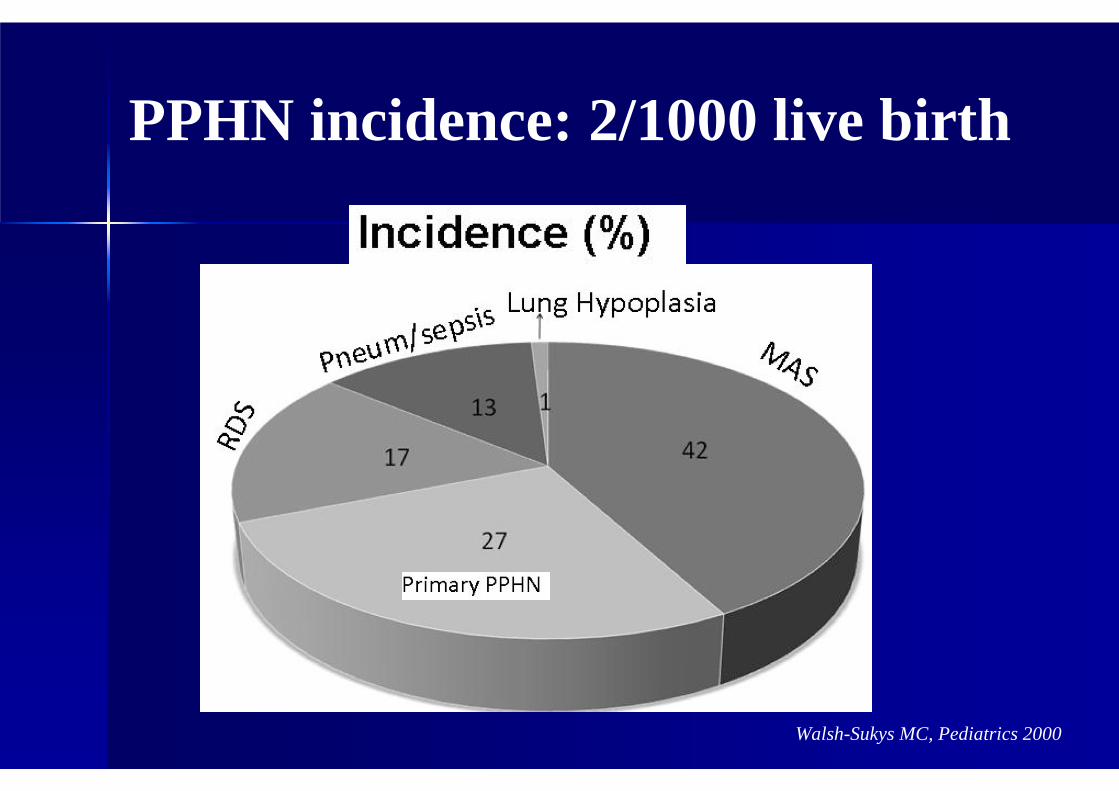
Walsh-Sukys MC, Pediatrics 2000
PPHN incidence: 2/1000 live birth
PPHN
� The severity of PPHN can run the full spectrum from mild and transientrespiratory distress to severe hypoxemia and cardio-pulmonary instability thatrequire intensive care support.
� Prompt diagnosis and management, including a timely referral to a tertiarycare center, can dramatically improve the chances of survival.
� Although mortality rates for PPHN were reported as 11–34% during 1980s,current mortality rates are <10% at most tertiary care centers.
Hageman JR , Am J Dis Child. 1984Davis JM, Pediatr Pulmonol. 1988Konduri GG, Pediatrics 2004
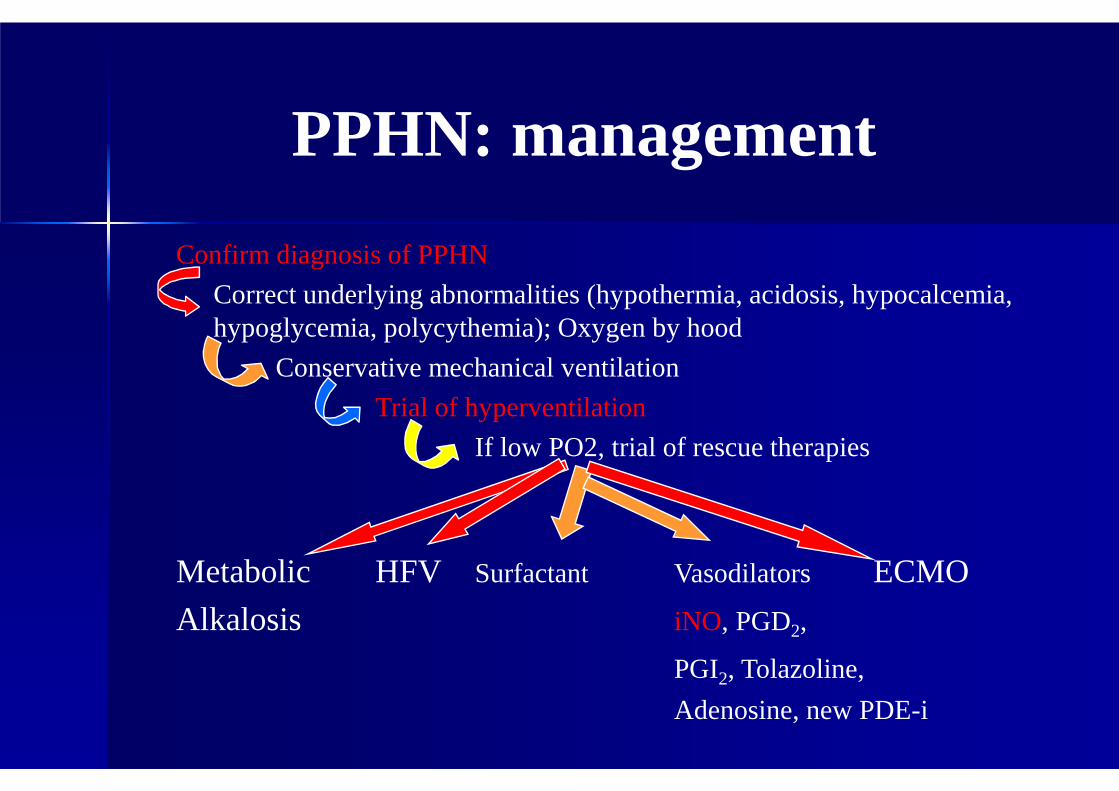
PPHN: management
Confirm diagnosis of PPHN
Correct underlying abnormalities (hypothermia, acidosis, hypocalcemia, hypoglycemia, polycythemia); Oxygen by hood
Conservative mechanical ventilation
Trial of hyperventilation
If low PO2, trial of rescue therapies
Metabolic HFV Surfactant Vasodilators ECMO
Alkalosis iNO, PGD2,
PGI2, Tolazoline,
Adenosine, new PDE-i
PPHN or CHD ?
Roleof echocardiography
� It is important to perform echocardiography to exclude cardiac disease and to assess cardiac function.
� Infants with severe persistent hypoxaemiashould be assessed by an experienced paediatric echocardiographer.
Echo findings in PPHN
• RV dilation
• Anomalous value of pulmonary ejection wave (AcT/ET <0.3)
• PAPs > 35 mmHg
• Right-to-left (or bidirectional) ductal or interatrialshunt
Estimation of Pulmonary Artery Pressure (PAP)
Echocardiographic parameters (direct or indirect)� Tricuspid Regurgitation
� Pulmonary regurgitation� Ductal Flow
� Atrial Shunting� Other Shunts
� Cardiac Function and Output
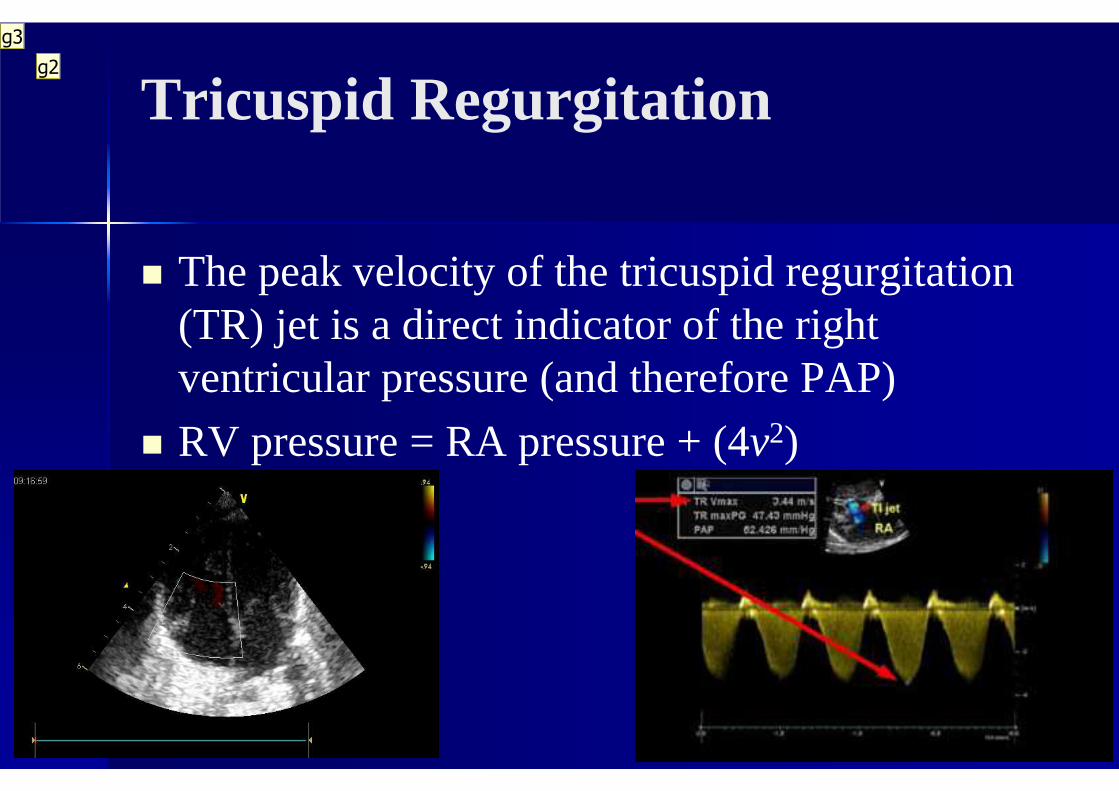
Tricuspid Regurgitation
� The peak velocity of the tricuspid regurgitation (TR) jet is a direct indicator of the right ventricular pressure (and therefore PAP)
� RV pressure = RA pressure + (4v2)
g2
g3

Diapositiva 12
g2 n This is the most accurate way of determining PAP.
n The jet of blood leaking through the tricuspid valve is interrogated with Dopplergiovannella.russo; 12/10/2013
g3 n It is important to know the systemic blood pressure to determine whether PAP is above systemic BP. giovannella.russo; 12/10/2013
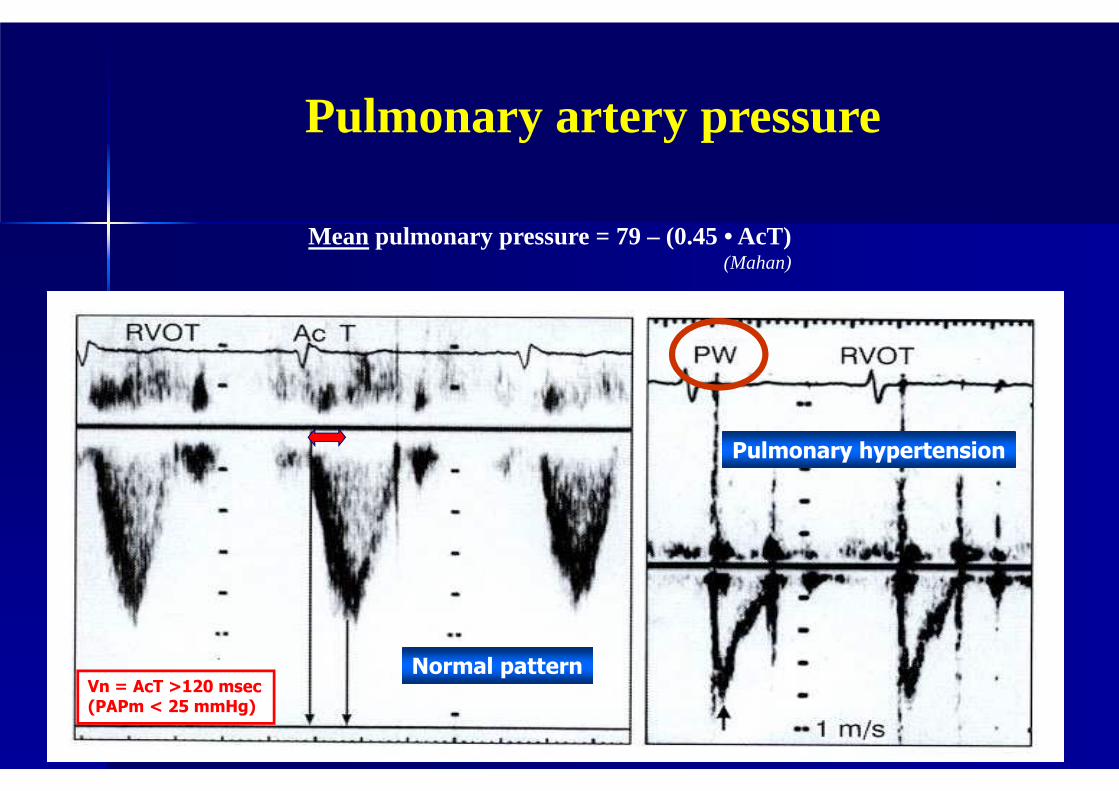
Mean pulmonary pressure = 79 – (0.45 • AcT)(Mahan)
Normal pattern
Pulmonary hypertension
Vn = AcT >120 msec(PAPm < 25 mmHg)
Pulmonary artery pressure
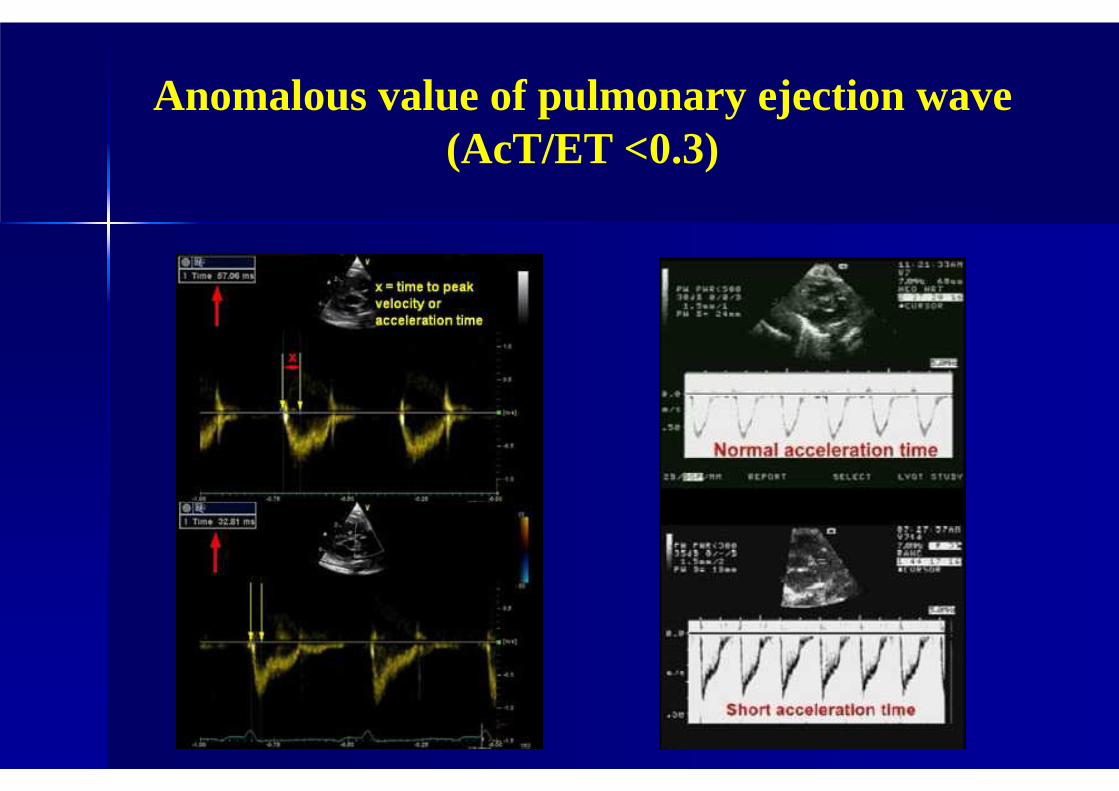
Anomalous value of pulmonary ejection wave (AcT/ET <0.3)
Ductal Flow
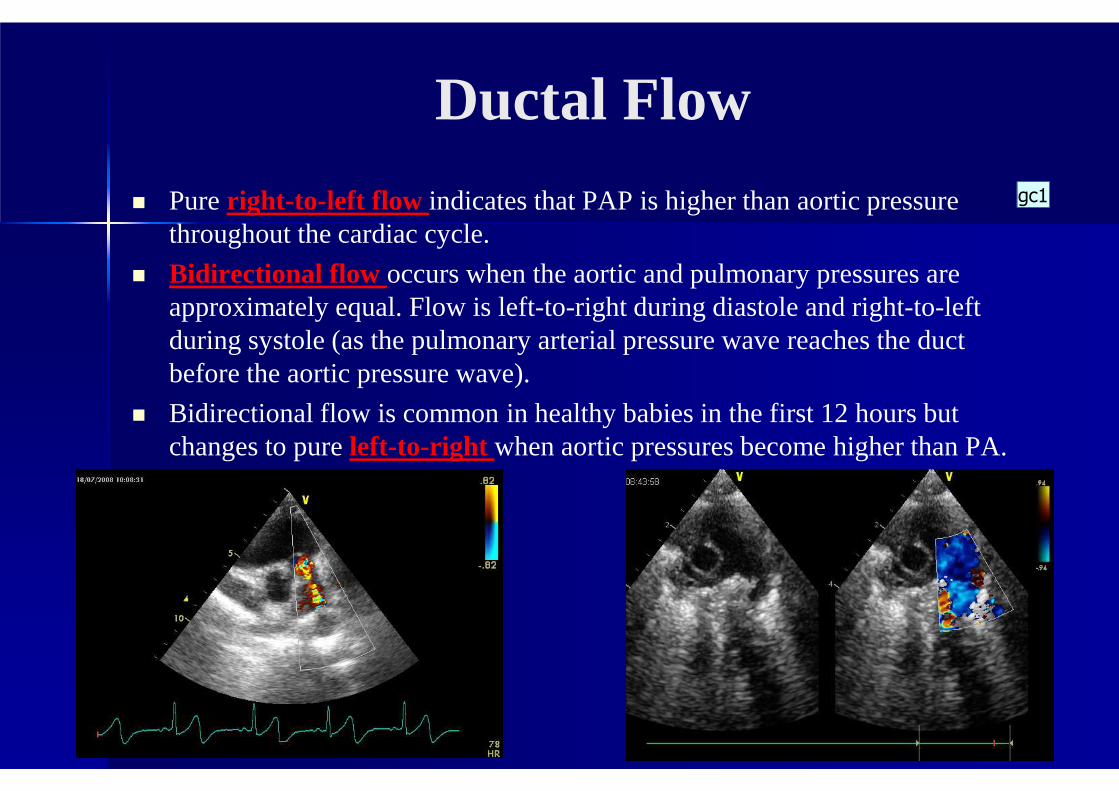
� Pure right-to-left flow indicates that PAP is higher than aortic pressure throughout the cardiac cycle.
� Bidirectional flow occurs when the aortic and pulmonary pressures are approximately equal. Flow is left-to-right during diastole and right-to-left during systole (as the pulmonary arterial pressure wave reaches the duct before the aortic pressure wave).
� Bidirectional flow is common in healthy babies in the first 12 hours but changes to pure left-to-right when aortic pressures become higher than PA.
gc1
Diapositiva 15
gc1 The direction and velocity of ductal blood flow can give useful information on PAP. gabriella carrozza; 13/10/2013
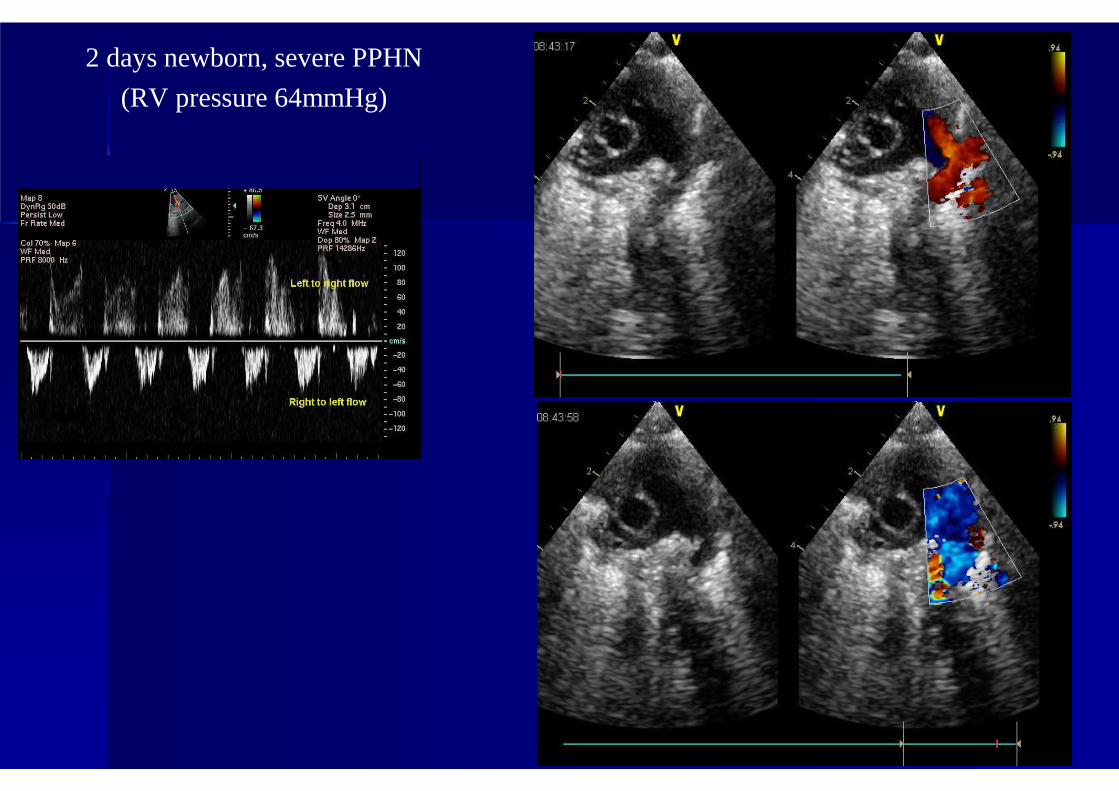
2 days newborn, severe PPHN
(RV pressure 64mmHg)
Atrial Shunting
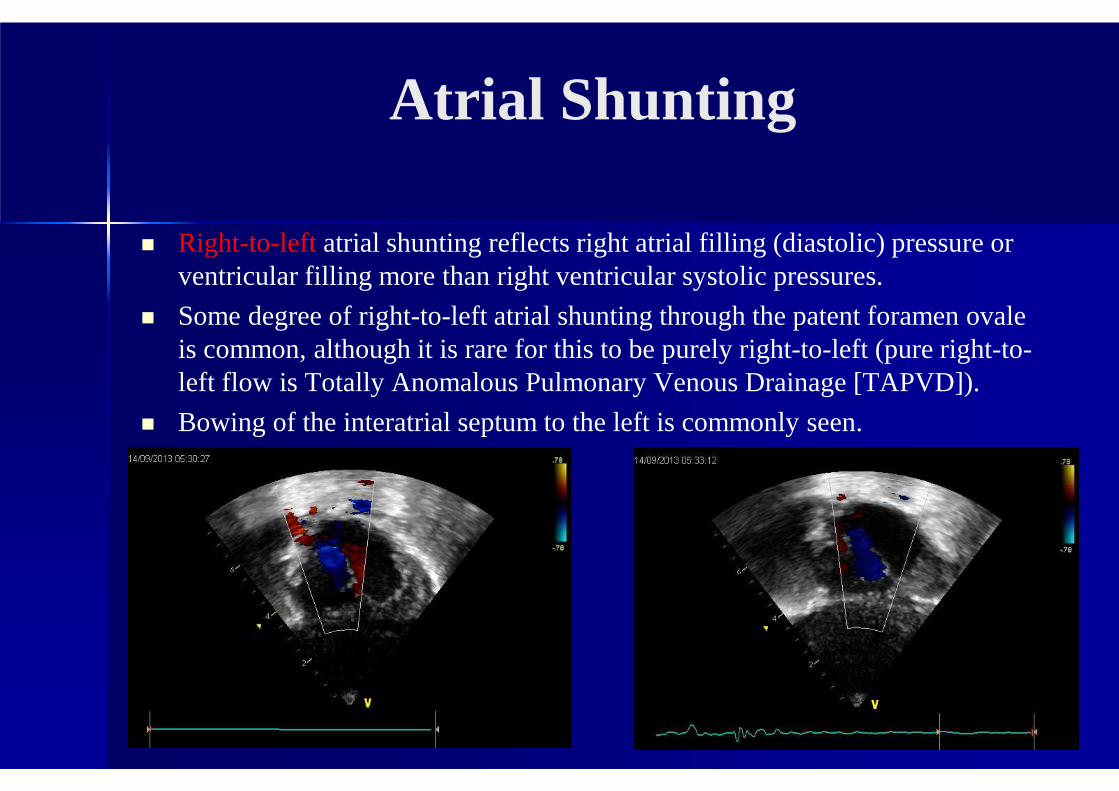
� Right-to-leftatrial shunting reflects right atrial filling (diastolic) pressure or ventricular filling more than right ventricular systolic pressures.
� Some degree of right-to-left atrial shunting through the patent foramen ovaleis common, although it is rare for this to be purely right-to-left (pure right-to-left flow is Totally Anomalous Pulmonary Venous Drainage [TAPVD]).
� Bowing of the interatrial septum to the left is commonly seen.
Other Shunts
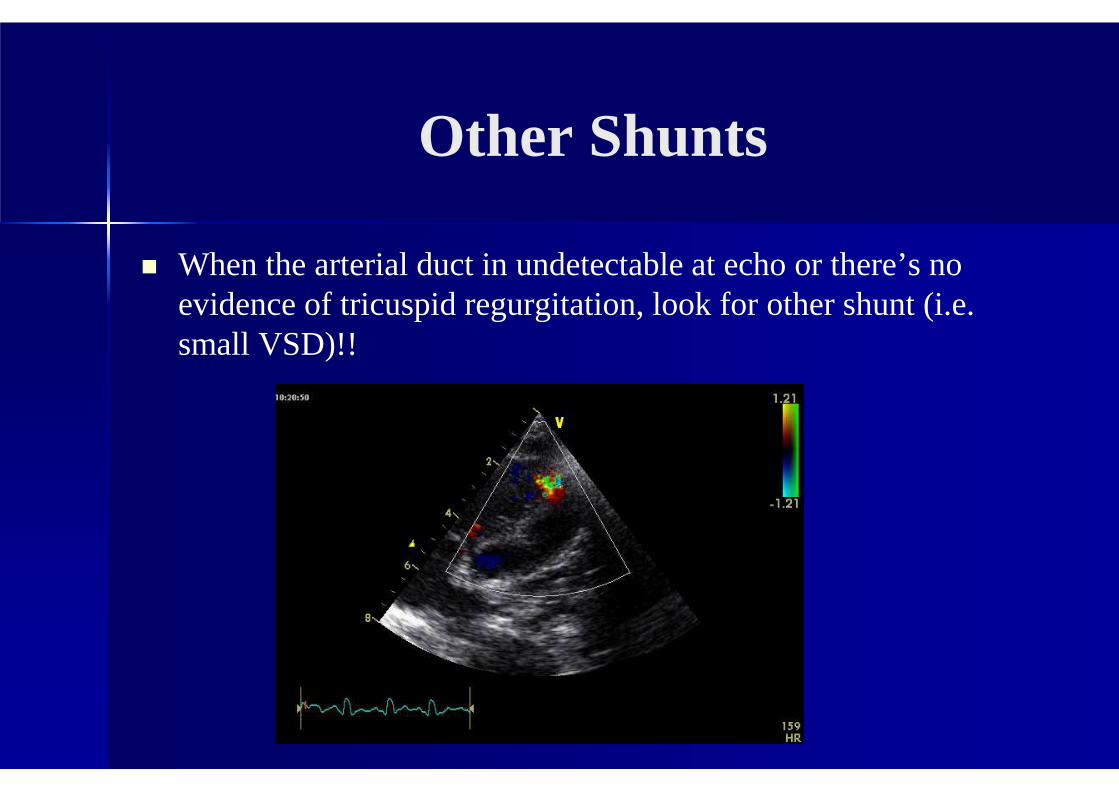
� When the arterial duct in undetectable at echo or there’s no evidence of tricuspid regurgitation, look for other shunt (i.e. small VSD)!!
Cardiac Function and Output
•Quantitative assessment of cardiac function may assist with decisions and assessments of the roles of inotropes, inhaled nitric oxide, and other interventions affecting cardiac output.
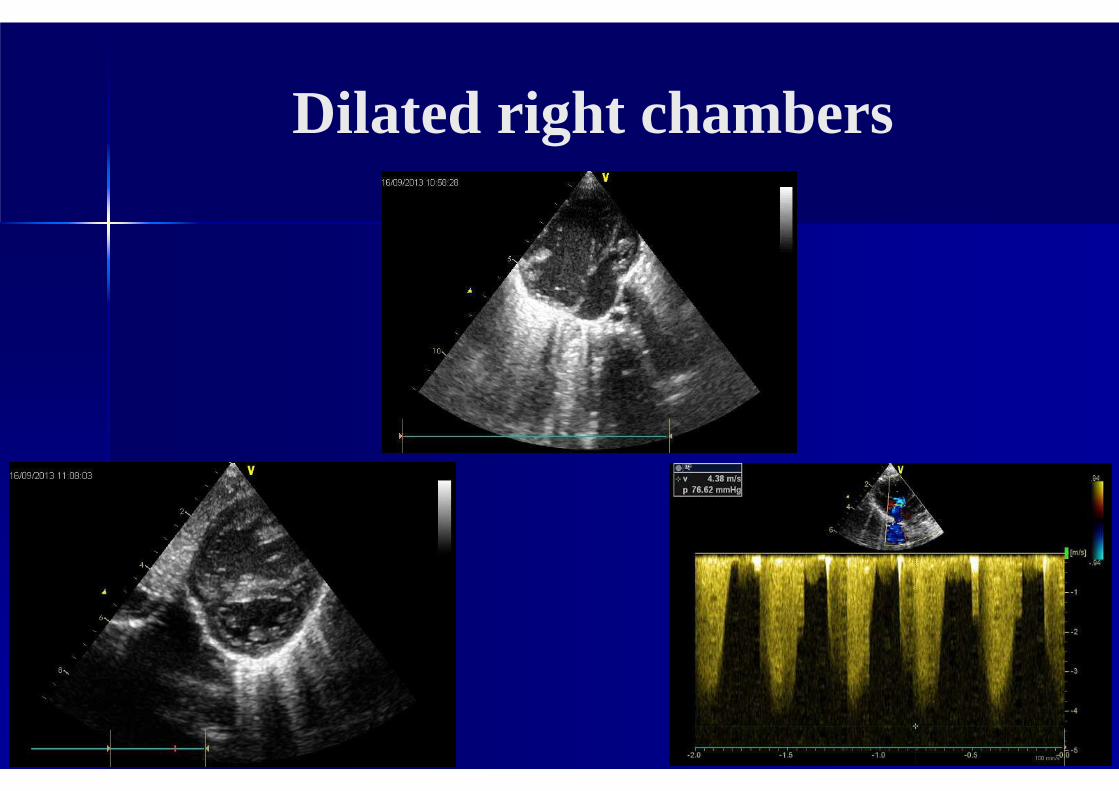
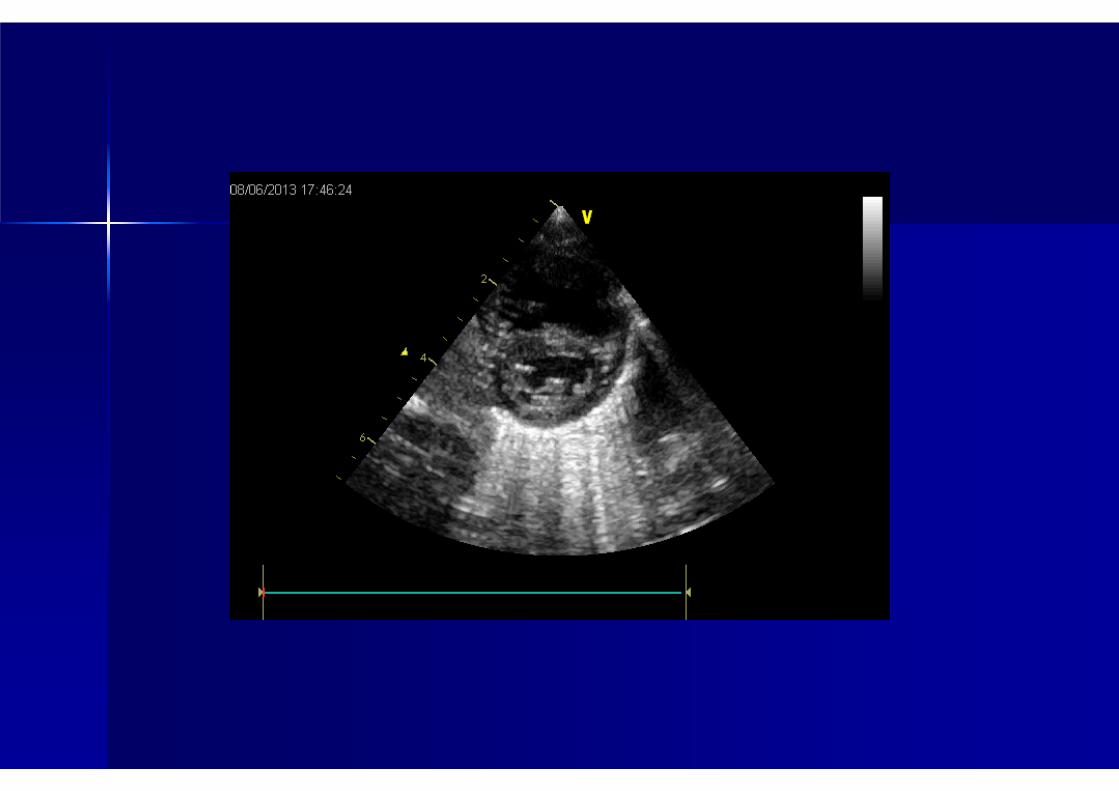
Dilated right chambers
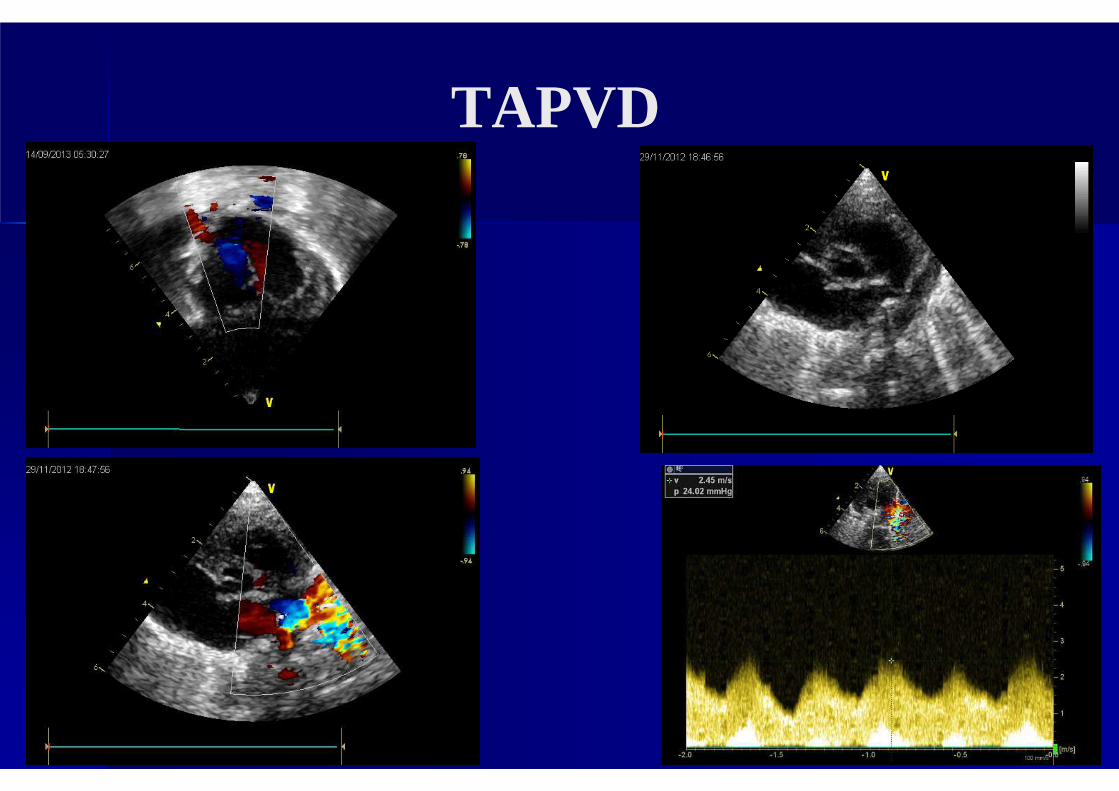
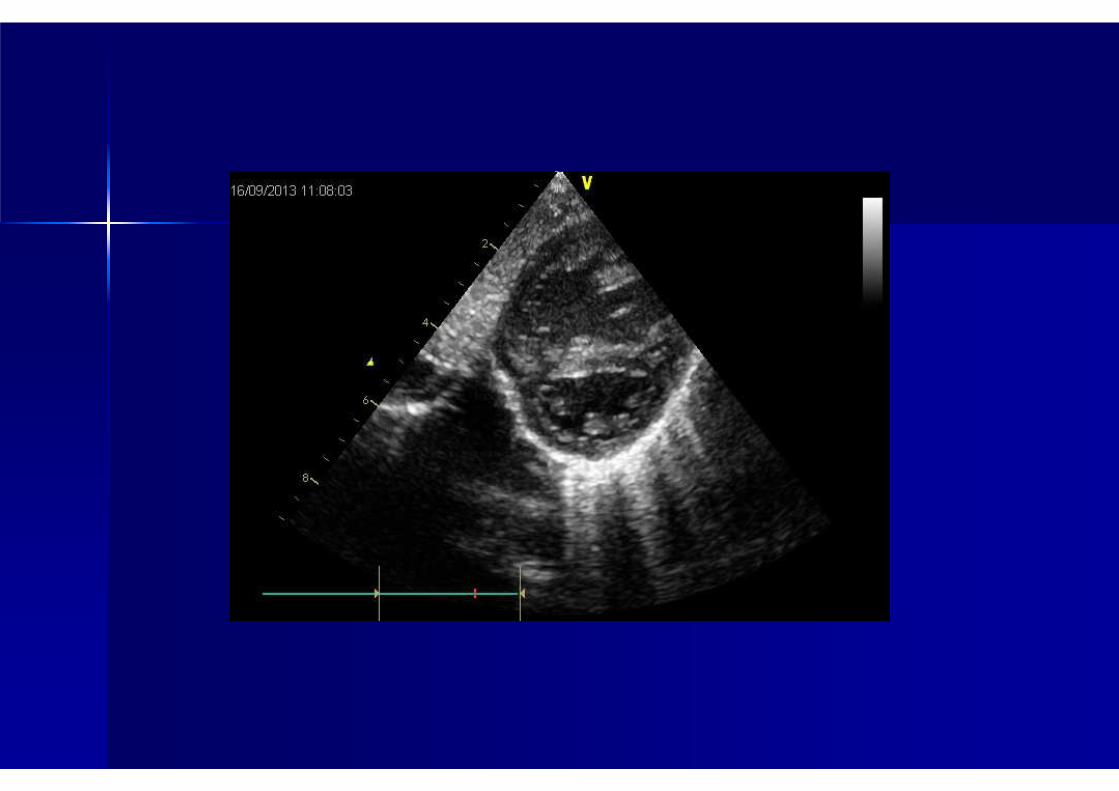
TAPVD
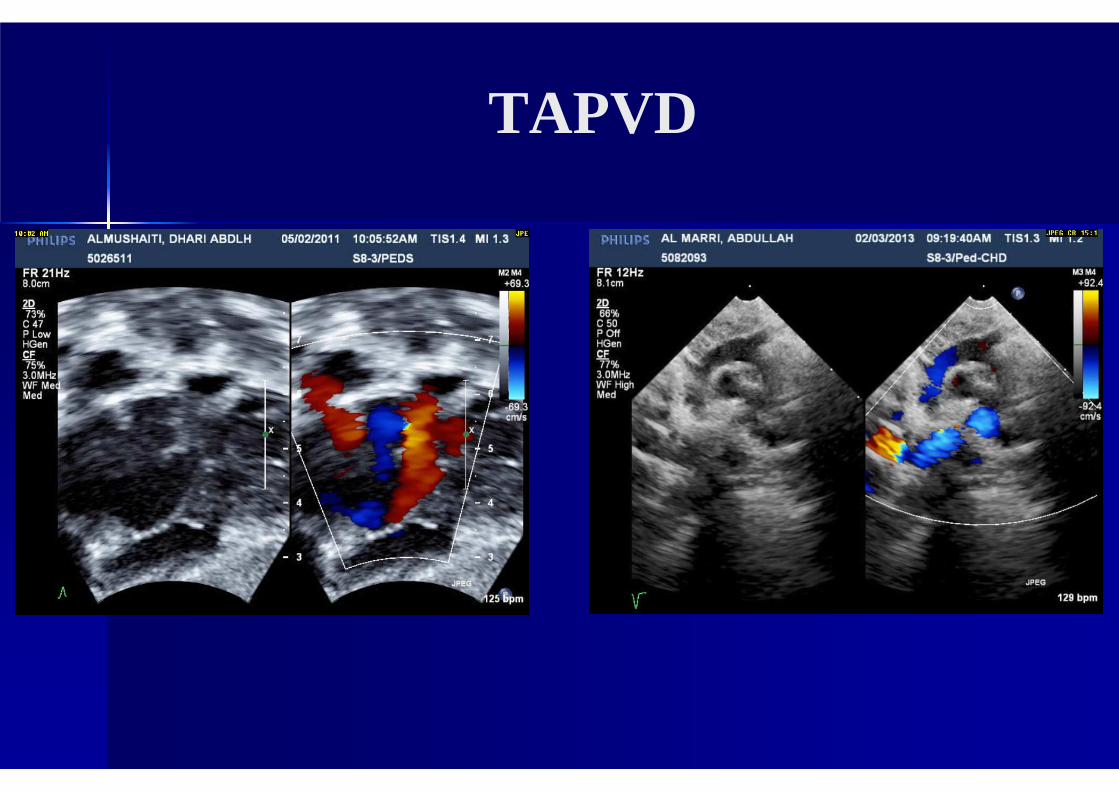
TAPVD
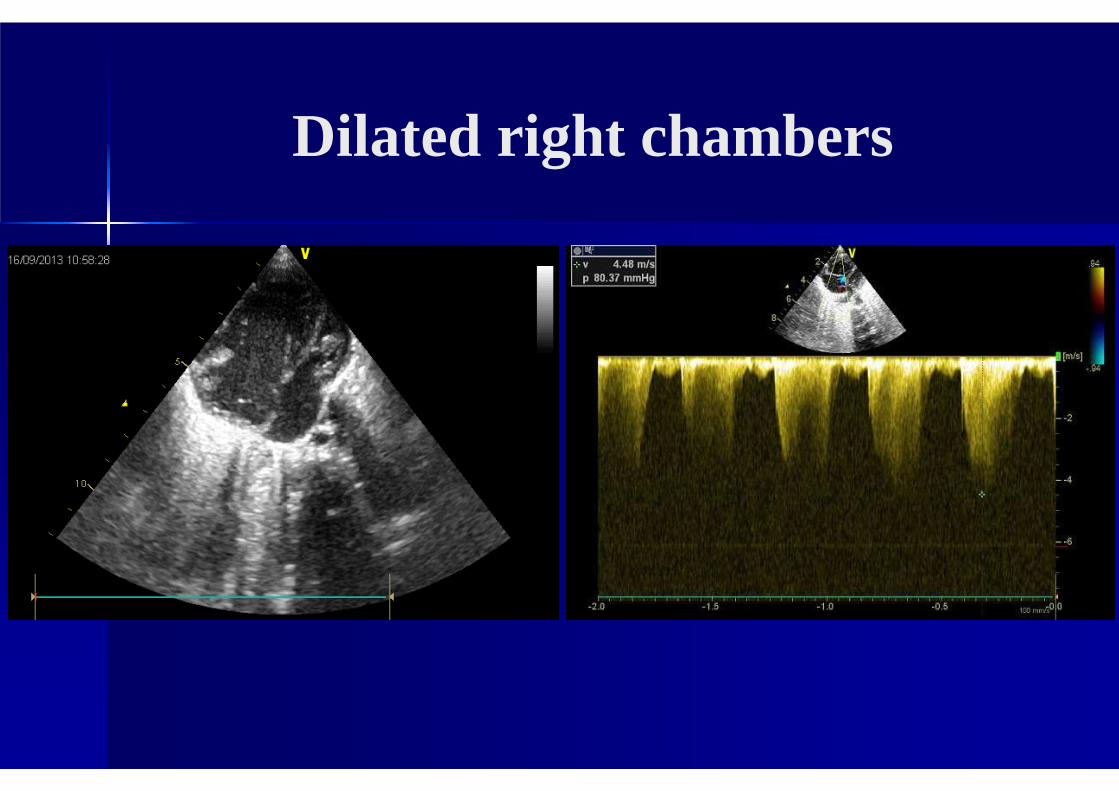
Dilated right chambers
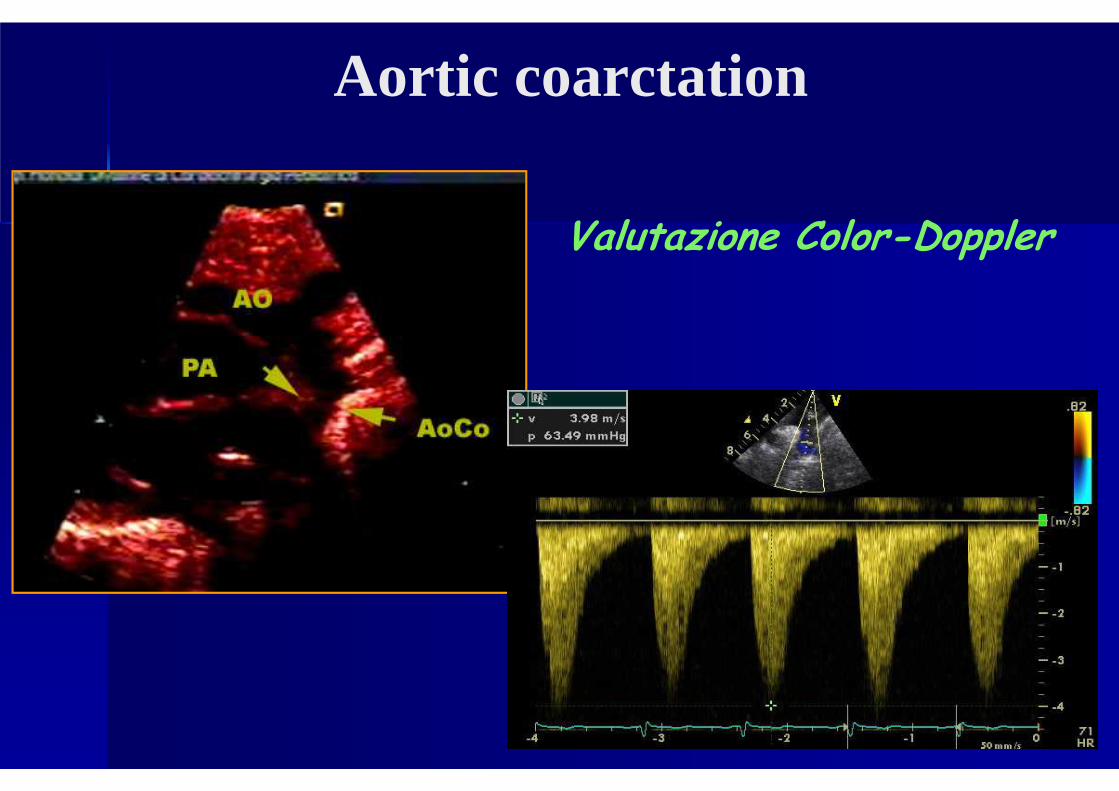
Valutazione Color-Doppler
Aortic coarctation
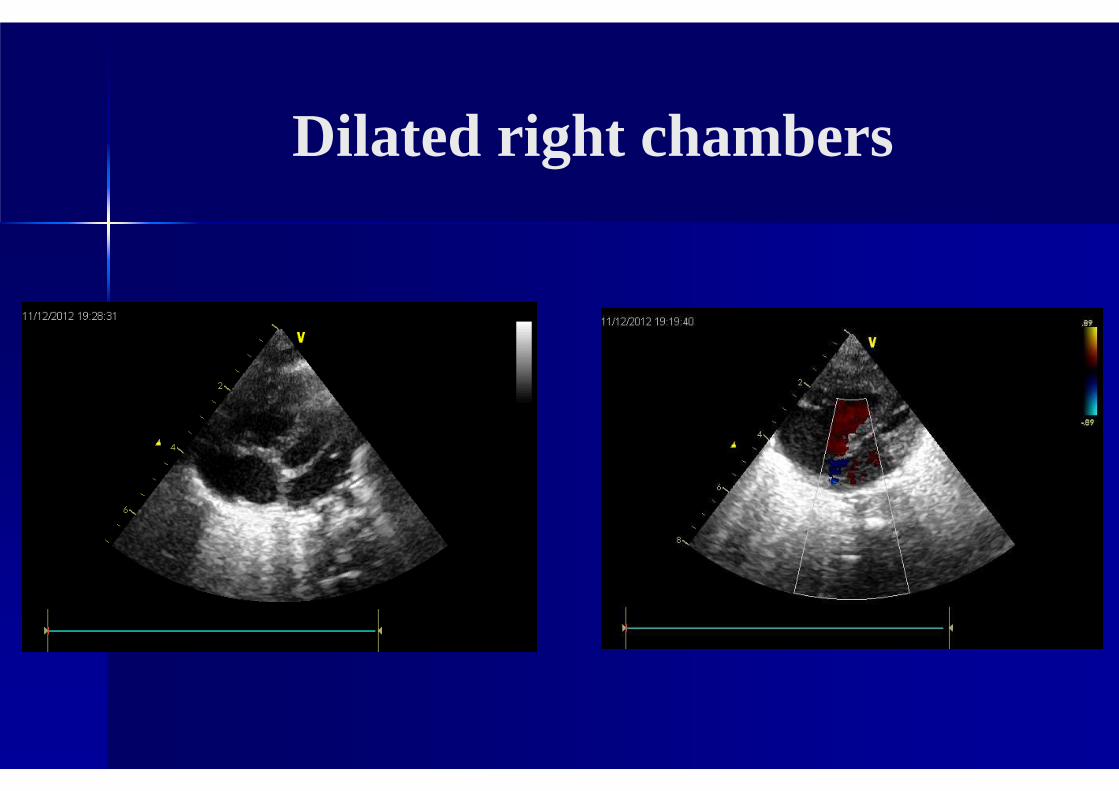
Dilated right chambers
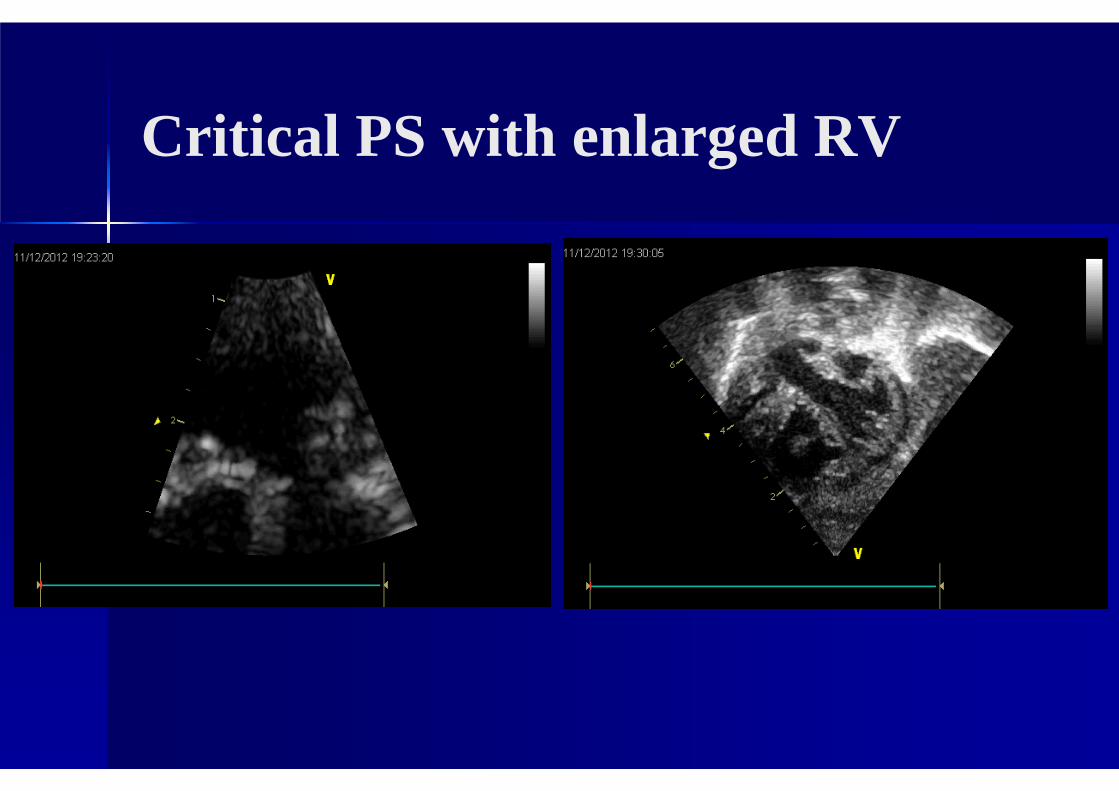
Critical PS with enlarged RV
� PPHN is uncommon.
� Clinical evaluation, O2 challenge, echo are mandatory for diagnostic work-up.
� Diagnosis is polyparametric.
� Echo is necessary to exclude CHD.
� Therapy: iNO
� No randomized clinical trials but expert opinion…
Take - home message (PPHN)
Elevated PAP is generally associated with decreased pulmonary blood flow and increased pulmonary vascular resistance. Not uncommonly, there is enlargement of the RV and RA, as well as the main pulmonary artery.
There may be flattening or even bowing of the interventricular septum to the left if RV pressures exceed LV pressures.
As cardiac output is dependent on venous return to the RA and LA, cardiac output (both RVO and LVO) is frequently reduced with PPHN.
Severe PPHN may be associated with LVO below 100ml/kg/min (normal 150-300ml/kg/min)
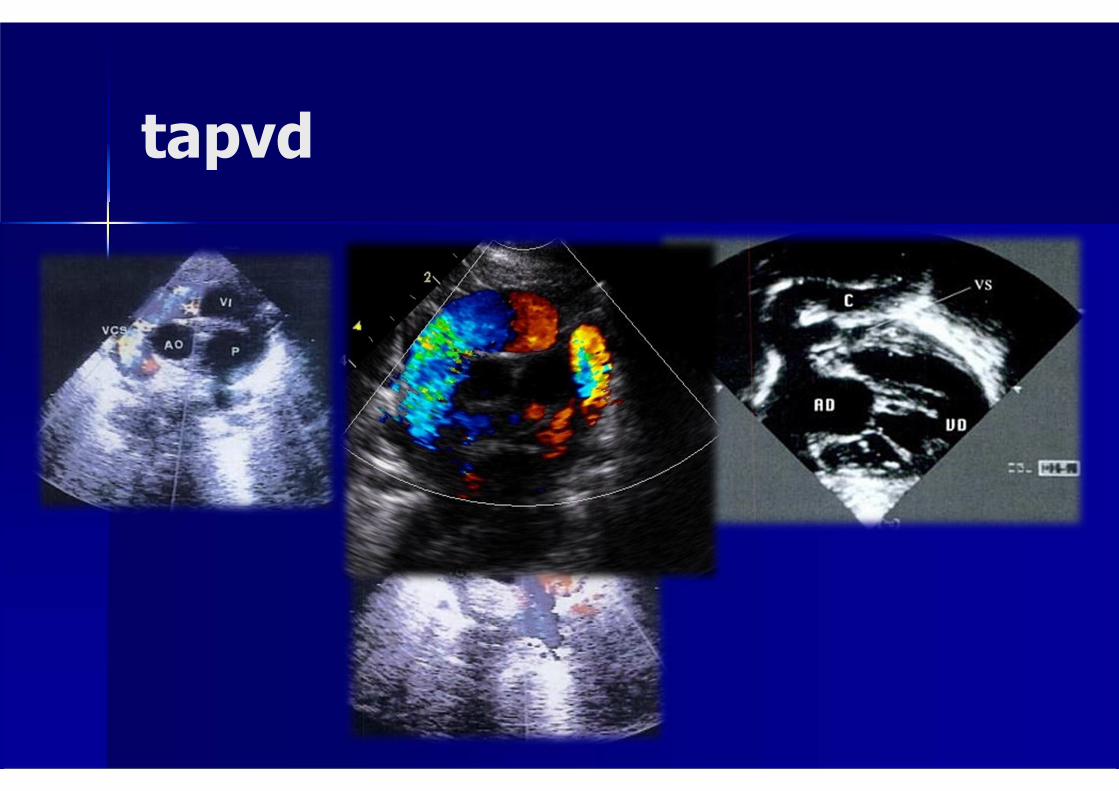
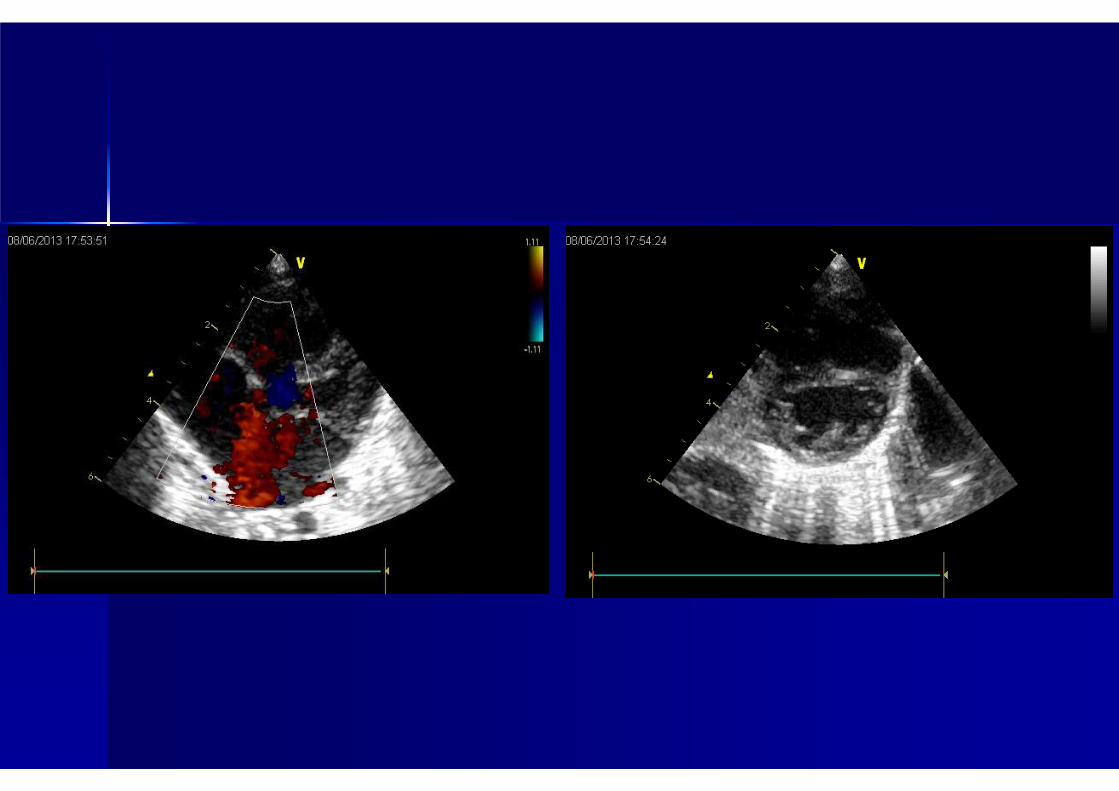
tapvd
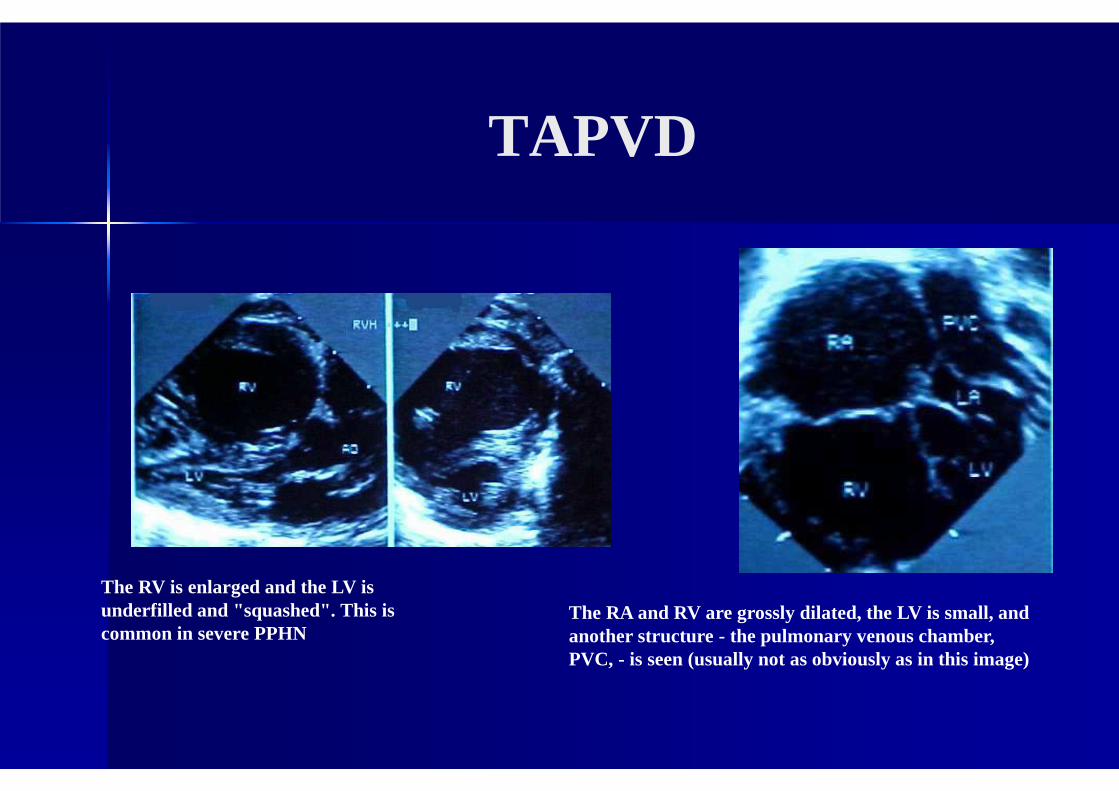
TAPVD
The RV is enlarged and the LV is underfilled and "squashed". This is common in severe PPHN
The RA and RV are grossly dilated, the LV is small, and another structure - the pulmonary venous chamber, PVC, - is seen (usually not as obviously as in this image)