Amylin:The Other β Cell Hormone
John Buse, MD, PhDProfessor of Medicine
Chief, Division of EndocrinologyUNC School of Medicine
Chapel Hill, NC USA
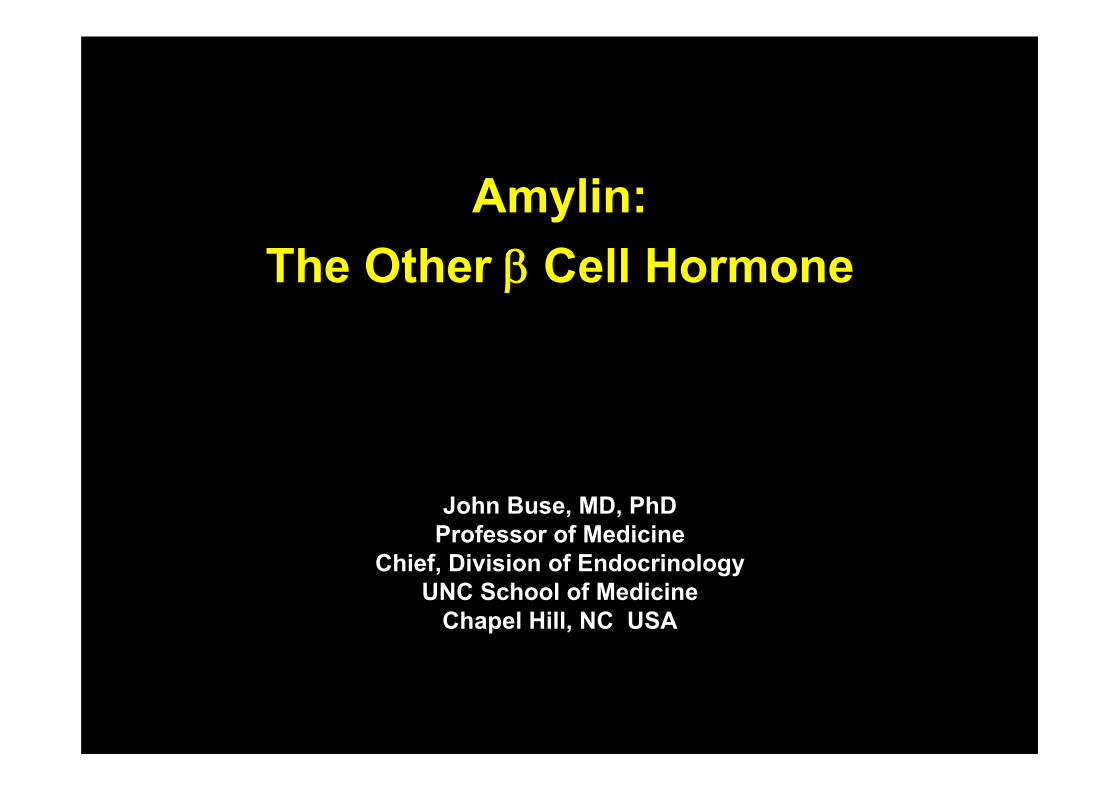
Beaumont K, et al. Mol Pharm. 1993; 44:493-497Muff R, et al. Endocrinology. 1999; 140:2924-2927
AmylinAmylin
Receptor image Adapted from Christopoulos G, et al. Mol Pharmacol. 1999; 56: 235-242
• Peptide hormone – co-localized and co-secreted with insulin– 37 amino acid peptide related to calcitonin, CGRP, adrenomedullin– Amylin gene - chromosome 12
• Neuroendocrine peptide– Receptor identified– Binding sites in CNS
Area postremaDorsal raphaeNucleus accumbens
C C
N N
Amylin Receptor
RAMP1 CTR
Amylin Binding Sites in the Brain
Dorsal Raphe
Nucleus Accumbens Area Postrema
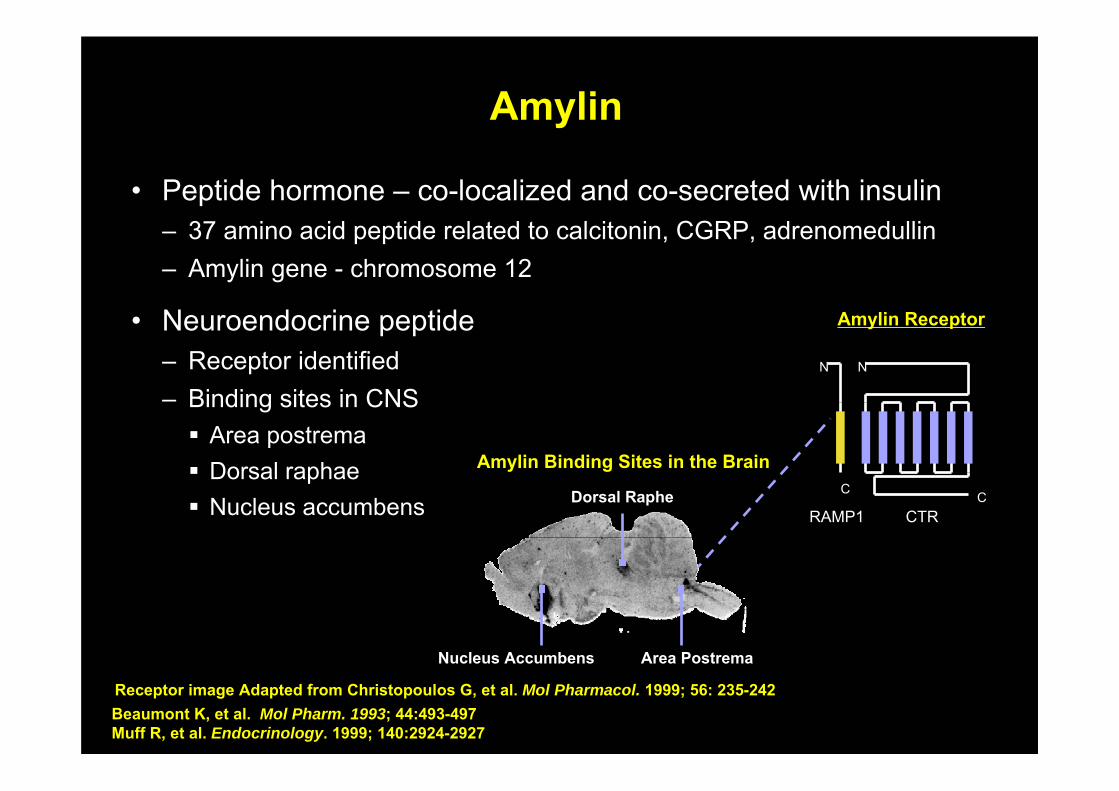
Amylin Is Co-Secreted With InsulinAmylin Is Co-Secreted With Insulin
Plas
ma
Insu
lin (p
M)
25
20
15
10
57 am Midnight5 pm12 noon
Time (24 h)
600
400
200
0
Meal Meal Meal
Plas
ma
Am
ylin
(pM
)
30
InsulinAmylin
Healthy adults; n = 6Data from Kruger D, et al. Diabetes Educ 1999; 25:389-398
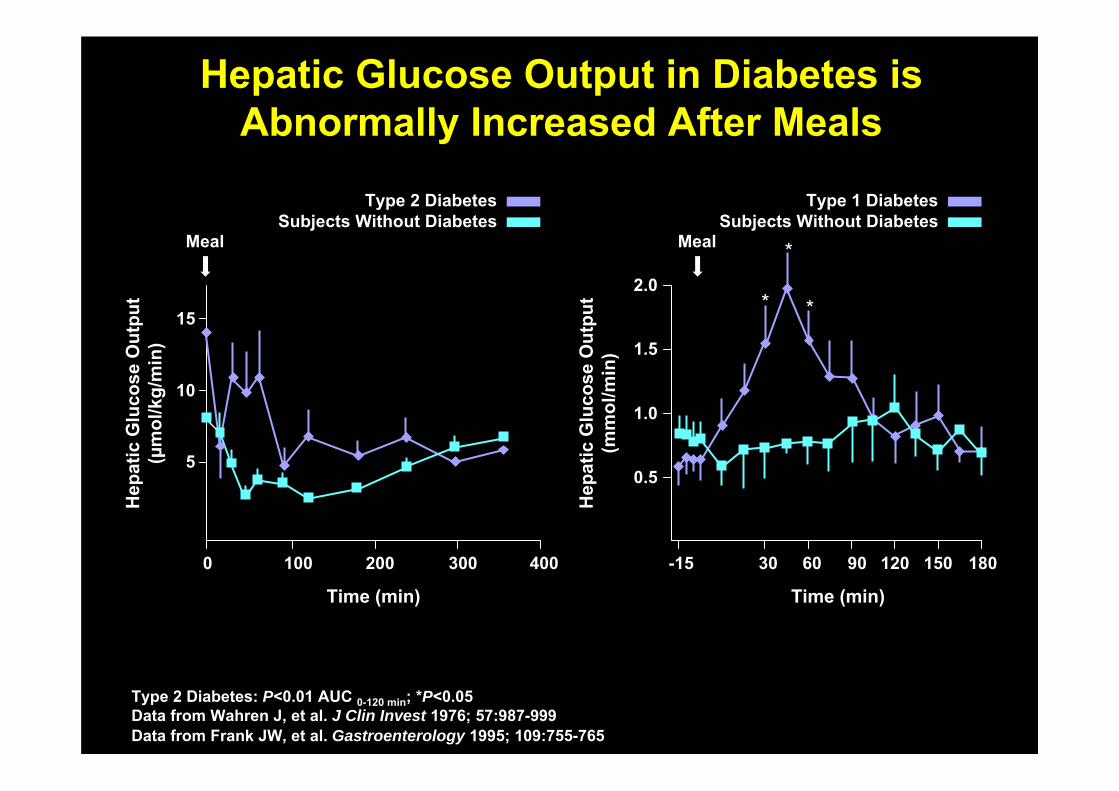
Hepatic Glucose Output in Diabetes is Abnormally Increased After Meals
Hepatic Glucose Output in Diabetes is Abnormally Increased After Meals
Time (min)H
epat
ic G
luco
se O
utpu
t (m
mol
/min
)
-15 30 60 90 120 150 180
2.0
1.5
1.0
0.5
Meal *
* *
Type 1 DiabetesSubjects Without Diabetes
Time (min)
Hep
atic
Glu
cose
Out
put
(µm
ol/k
g/m
in)
5
10
15
0 100 200 400300
Meal
Type 2 DiabetesSubjects Without Diabetes
Type 2 Diabetes: P<0.01 AUC 0-120 min; *P<0.05Data from Wahren J, et al. J Clin Invest 1976; 57:987-999Data from Frank JW, et al. Gastroenterology 1995; 109:755-765
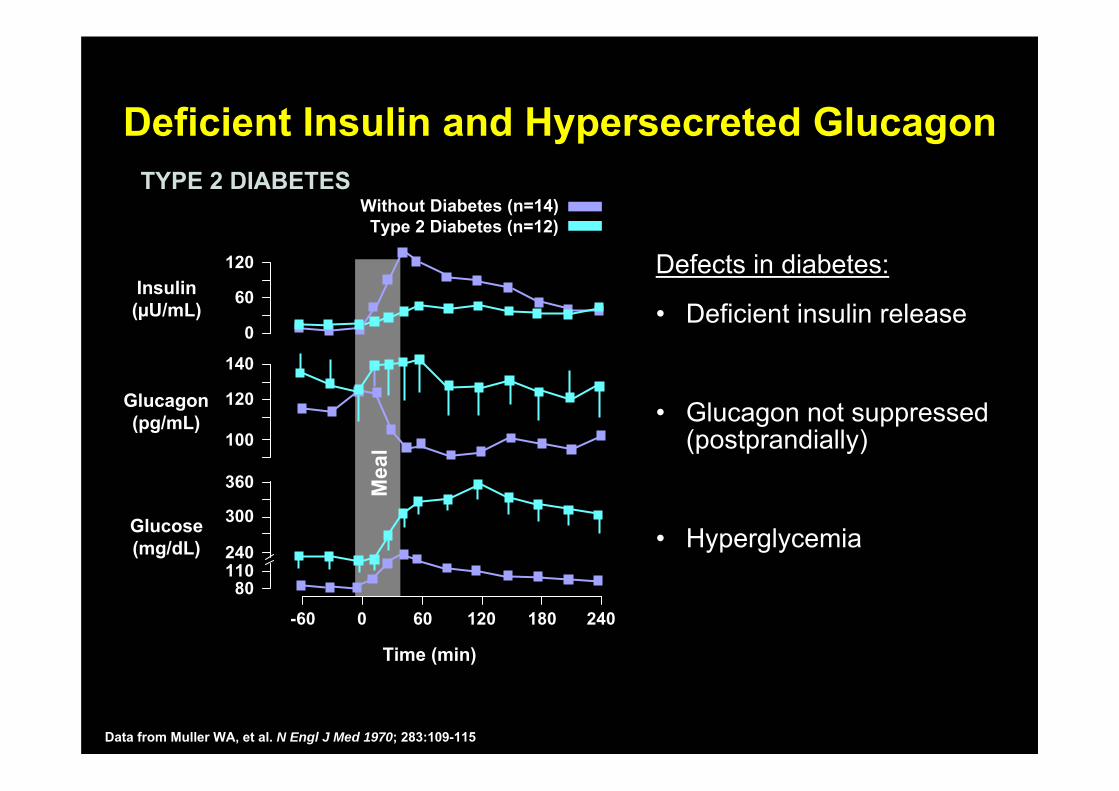
Deficient Insulin and Hypersecreted GlucagonDeficient Insulin and Hypersecreted Glucagon
Defects in diabetes:
• Deficient insulin release
• Glucagon not suppressed(postprandially)
• Hyperglycemia
Mea
l
120
60
0
Insulin(µU/mL)
100
120
140
-60 0 60 120 180 240
Time (min)
Glucagon(pg/mL)
360
300
240110
80
Glucose(mg/dL)
Without Diabetes (n=14)Type 2 Diabetes (n=12)
TYPE 2 DIABETESTYPE 2 DIABETES
Data from Muller WA, et al. N Engl J Med 1970; 283:109-115
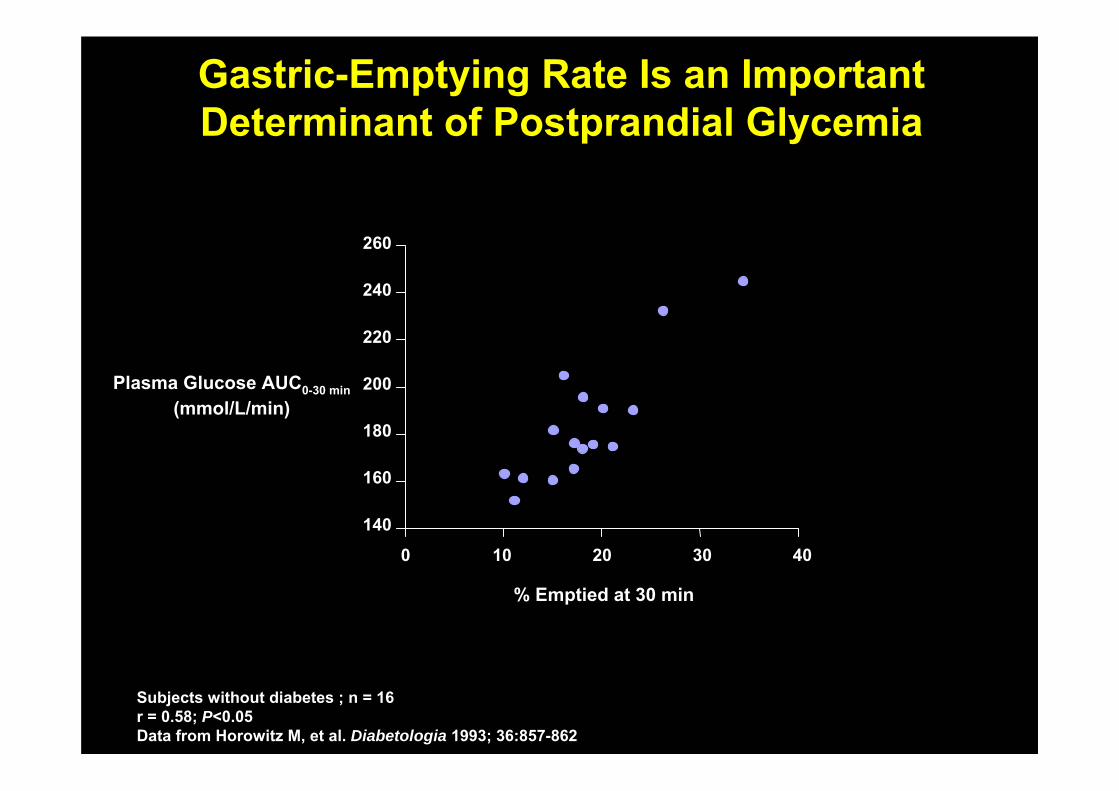
Plasma Glucose AUC0-30 min(mmol/L/min)
Gastric-Emptying Rate Is an Important Determinant of Postprandial GlycemiaGastric-Emptying Rate Is an Important Determinant of Postprandial Glycemia
% Emptied at 30 min
260
10 20 30 400
240
220
200
180
160
140
Subjects without diabetes ; n = 16r = 0.58; P<0.05Data from Horowitz M, et al. Diabetologia 1993; 36:857-862
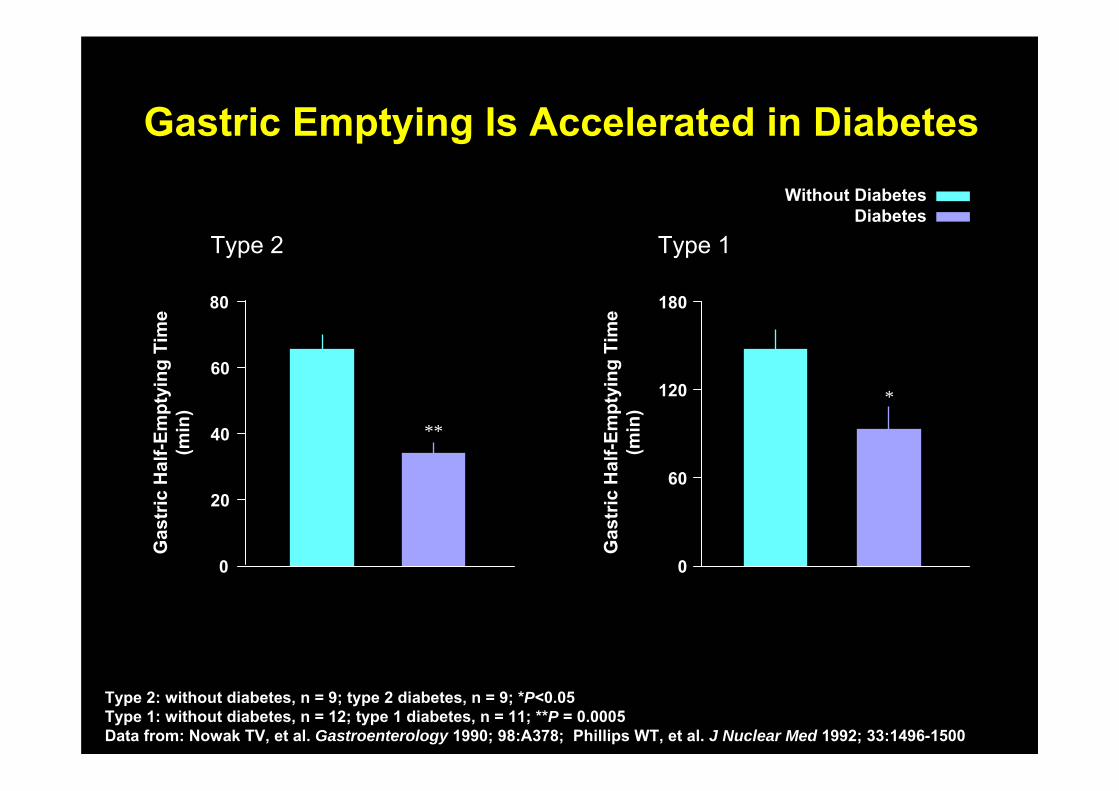
Gastric Emptying Is Accelerated in DiabetesGastric Emptying Is Accelerated in Diabetes
Type 1
*
Without DiabetesDiabetes
0
120
180
60
0
20
40
60
80
Type 2
**
Gas
tric
Hal
f-Em
ptyi
ng T
ime
(min
)
Gas
tric
Hal
f-Em
ptyi
ng T
ime
(min
)
Type 2: without diabetes, n = 9; type 2 diabetes, n = 9; *P<0.05Type 1: without diabetes, n = 12; type 1 diabetes, n = 11; **P = 0.0005Data from: Nowak TV, et al. Gastroenterology 1990; 98:A378; Phillips WT, et al. J Nuclear Med 1992; 33:1496-1500
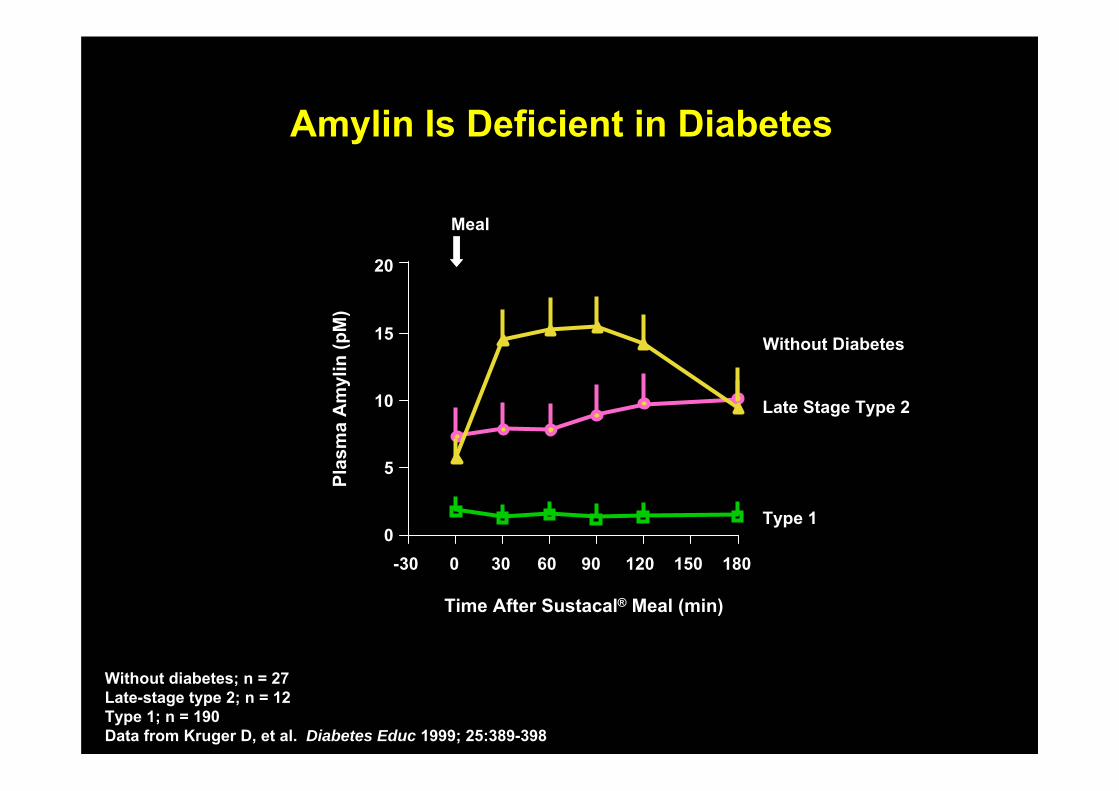
Amylin Is Deficient in DiabetesAmylin Is Deficient in Diabetes
Time After Sustacal® Meal (min)
0
5
10
15
20
-30 0 30 60 90 120 150 180
Meal
Late Stage Type 2
Type 1
Without DiabetesPl
asm
a A
myl
in (p
M)
Without diabetes; n = 27Late-stage type 2; n = 12Type 1; n = 190Data from Kruger D, et al. Diabetes Educ 1999; 25:389-398
Plasma Glucose
Tissues
GlucoseDisposal
Rate ofglucose
appearance
Rate ofglucose
disappearance
Stomach
BrainFoodIntake
—
GastricEmptying
—Liver
GLP-1
Gut
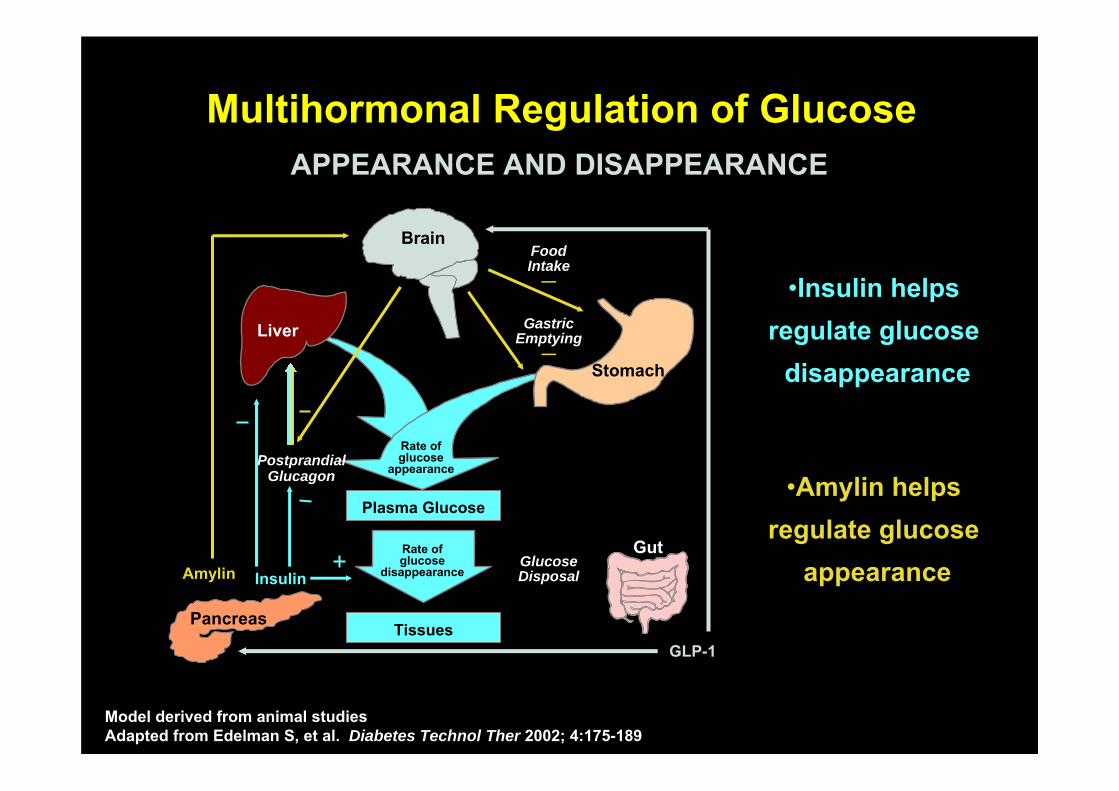
Multihormonal Regulation of GlucoseMultihormonal Regulation of Glucose
PostprandialGlucagon
Pancreas
Insulin
•Insulin helps regulate glucose
disappearance
Amylin
•Amylin helps regulate glucose
appearance
APPEARANCE AND DISAPPEARANCEAPPEARANCE AND DISAPPEARANCE
Model derived from animal studiesAdapted from Edelman S, et al. Diabetes Technol Ther 2002; 4:175-189
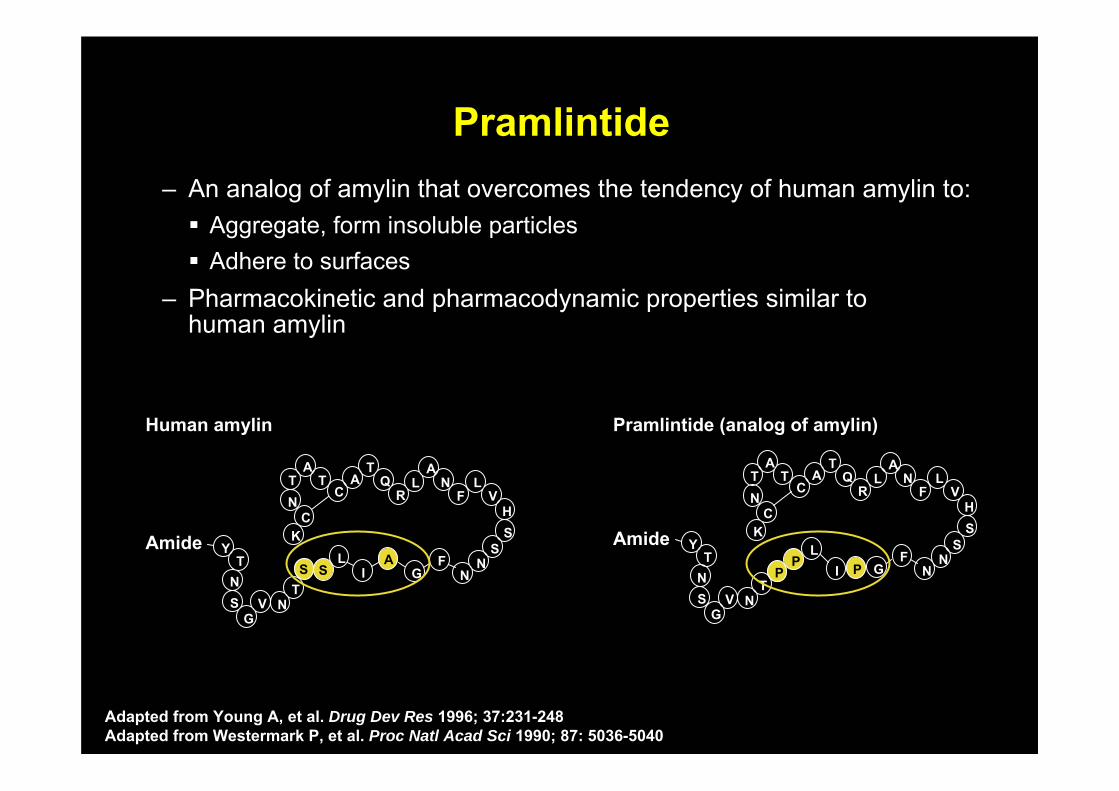
PramlintidePramlintide– An analog of amylin that overcomes the tendency of human amylin to:
Aggregate, form insoluble particles Adhere to surfaces
– Pharmacokinetic and pharmacodynamic properties similar to human amylin
Human amylin Pramlintide (analog of amylin)
AmideS S
AY
TNS
GV N
T
T TT
N
AA
A
LI
KS
SC
CQ
RL N
NNF
G
FL
VH
Amide
PP P
YT
NS
GV N
T
T TT
N
AA
A
LI
KS
SC
CQ
RL N
NNF
G
FL
VH
Adapted from Young A, et al. Drug Dev Res 1996; 37:231-248Adapted from Westermark P, et al. Proc Natl Acad Sci 1990; 87: 5036-5040
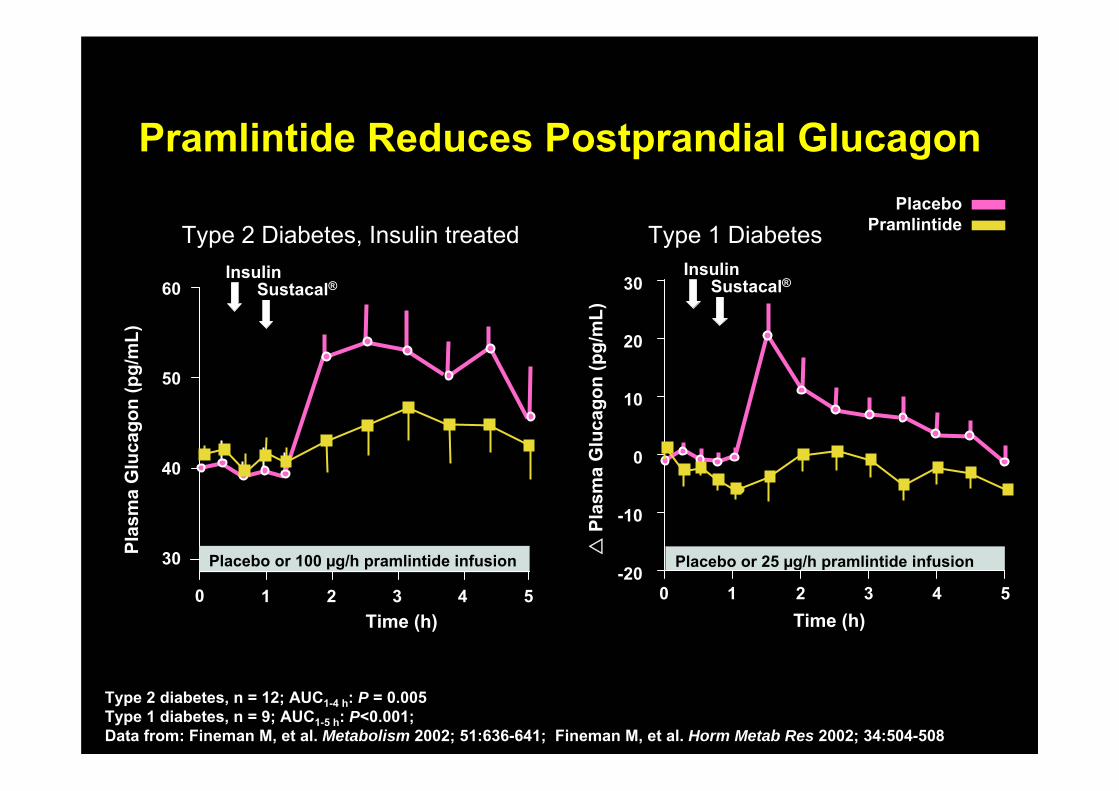
Pramlintide Reduces Postprandial GlucagonPramlintide Reduces Postprandial Glucagon
Type 1 Diabetes
Time (h)
PlaceboPramlintide
Placebo or 25 µg/h pramlintide infusion-20
0
10
20
30
-10
InsulinSustacal®
0 2 3 4 51
Type 2 Diabetes, Insulin treated
Time (h)
Plas
ma
Glu
cago
n (p
g/m
L)
InsulinSustacal®60
40
30
50
Placebo or 100 µg/h pramlintide infusion
0 1 2 3 4 5Pl
asm
a G
luca
gon
(pg/
mL)
Type 2 diabetes, n = 12; AUC1-4 h: P = 0.005Type 1 diabetes, n = 9; AUC1-5 h: P<0.001; Data from: Fineman M, et al. Metabolism 2002; 51:636-641; Fineman M, et al. Horm Metab Res 2002; 34:504-508
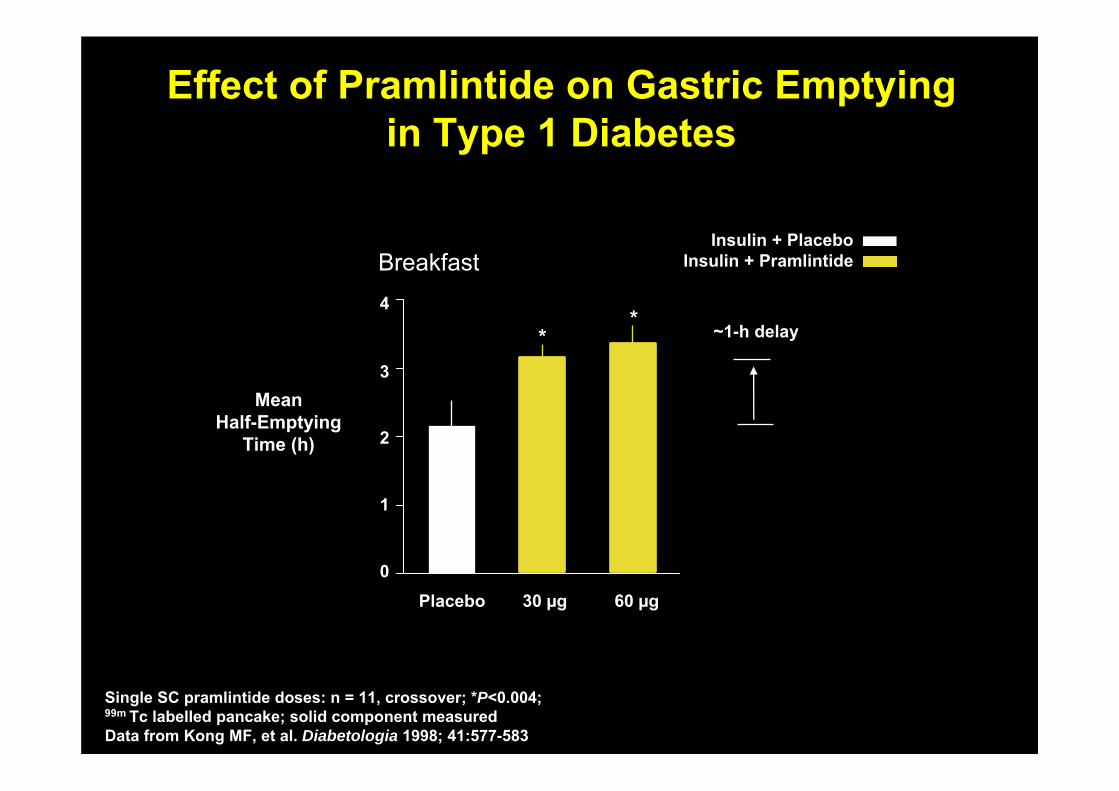
Effect of Pramlintide on Gastric Emptyingin Type 1 Diabetes
Effect of Pramlintide on Gastric Emptyingin Type 1 Diabetes
MeanHalf-Emptying
Time (h)
0
1
2
3
4~1-h delay*
60 µg
*
30 µgPlacebo
Insulin + PlaceboInsulin + PramlintideBreakfast
Single SC pramlintide doses: n = 11, crossover; *P<0.004; 99m Tc labelled pancake; solid component measuredData from Kong MF, et al. Diabetologia 1998; 41:577-583
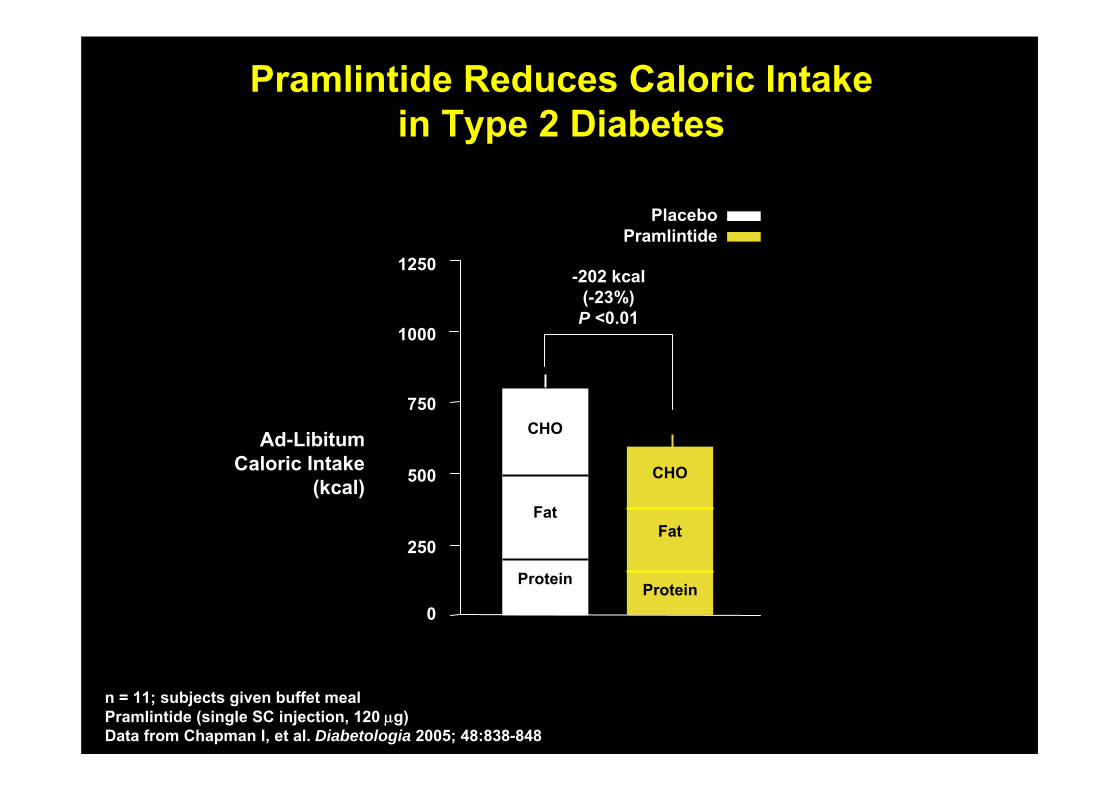
Pramlintide Reduces Caloric Intakein Type 2 Diabetes
Pramlintide Reduces Caloric Intakein Type 2 Diabetes
0
250
500
750
1000
1250
Protein
CHO
Fat
CHO
Fat
Protein
-202 kcal(-23%)P <0.01
Ad-LibitumCaloric Intake
(kcal)
PlaceboPramlintide
n = 11; subjects given buffet meal Pramlintide (single SC injection, 120 μg)Data from Chapman I, et al. Diabetologia 2005; 48:838-848
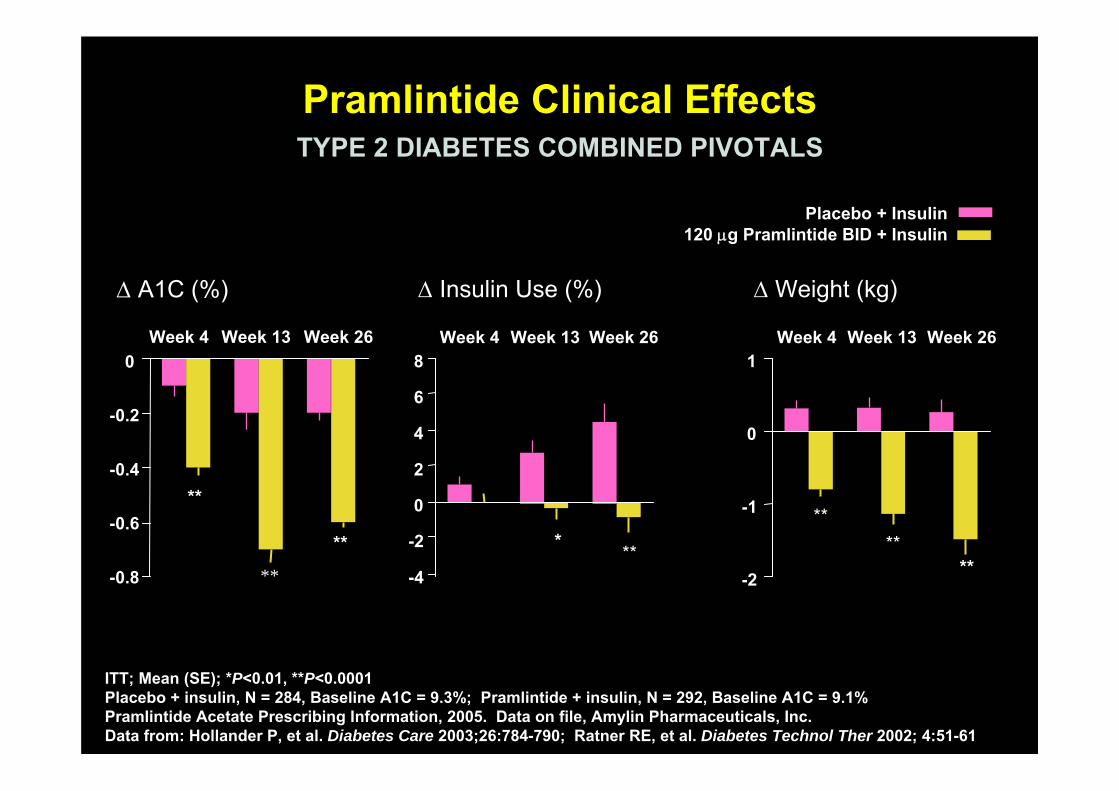
Pramlintide Clinical EffectsPramlintide Clinical Effects
-2
-1
0
1
* **
**
**
****
****-4
-2
0
2
4
6
8
-0.8
-0.6
-0.4
-0.2
0
Δ Insulin Use (%)Δ A1C (%) Δ Weight (kg)
Week 4 Week 13 Week 26Week 4 Week 13 Week 26Week 4 Week 13 Week 26
Placebo + Insulin120 μg Pramlintide BID + Insulin
TYPE 2 DIABETES COMBINED PIVOTALSTYPE 2 DIABETES COMBINED PIVOTALS
ITT; Mean (SE); *P<0.01, **P<0.0001 Placebo + insulin, N = 284, Baseline A1C = 9.3%; Pramlintide + insulin, N = 292, Baseline A1C = 9.1%Pramlintide Acetate Prescribing Information, 2005. Data on file, Amylin Pharmaceuticals, Inc.Data from: Hollander P, et al. Diabetes Care 2003;26:784-790; Ratner RE, et al. Diabetes Technol Ther 2002; 4:51-61
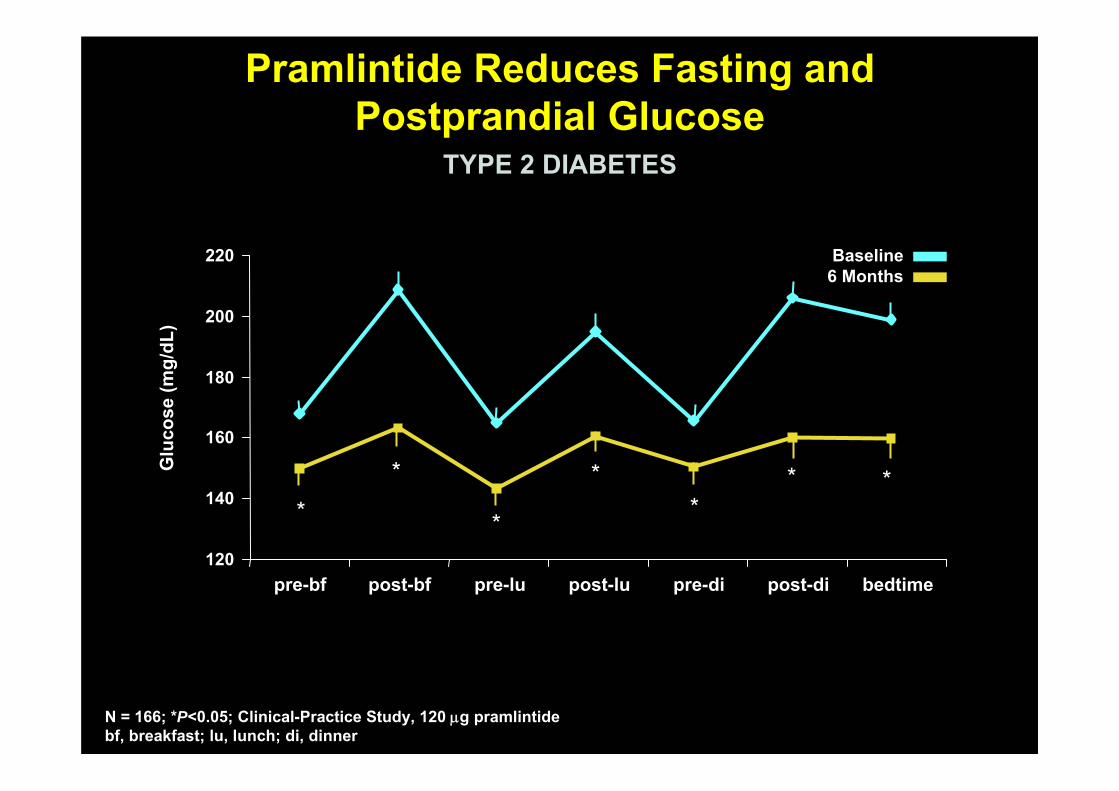
Pramlintide Reduces Fasting andPostprandial Glucose
Pramlintide Reduces Fasting andPostprandial Glucose
Baseline6 Months
120
140
160
180
200
220
Glu
cose
(mg/
dL)
pre-bf post-bf pre-lu post-lu pre-di post-di bedtime
**
*
**
* *
TYPE 2 DIABETESTYPE 2 DIABETES
N = 166; *P<0.05; Clinical-Practice Study, 120 μg pramlintidebf, breakfast; lu, lunch; di, dinner
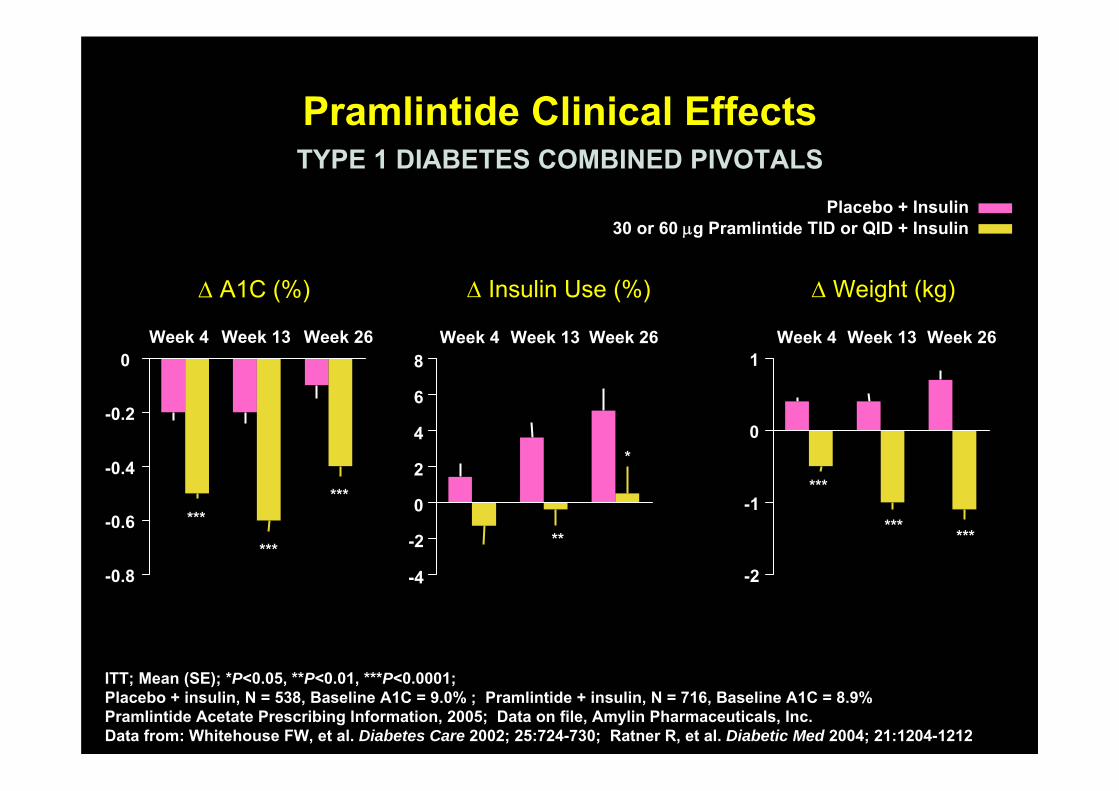
Pramlintide Clinical EffectsPramlintide Clinical Effects
-0.8
-0.6
-0.4
-0.2
0
-4
-2
0
2
4
6
8
-2
-1
0
1
***
***
***
**
*
***
*** ***
Week 4 Week 13 Week 26Week 4 Week 13 Week 26Week 4 Week 13 Week 26
Δ Insulin Use (%)Δ A1C (%) Δ Weight (kg)
Placebo + Insulin30 or 60 μg Pramlintide TID or QID + Insulin
TYPE 1 DIABETES COMBINED PIVOTALSTYPE 1 DIABETES COMBINED PIVOTALS
ITT; Mean (SE); *P<0.05, **P<0.01, ***P<0.0001; Placebo + insulin, N = 538, Baseline A1C = 9.0% ; Pramlintide + insulin, N = 716, Baseline A1C = 8.9%Pramlintide Acetate Prescribing Information, 2005; Data on file, Amylin Pharmaceuticals, Inc.Data from: Whitehouse FW, et al. Diabetes Care 2002; 25:724-730; Ratner R, et al. Diabetic Med 2004; 21:1204-1212
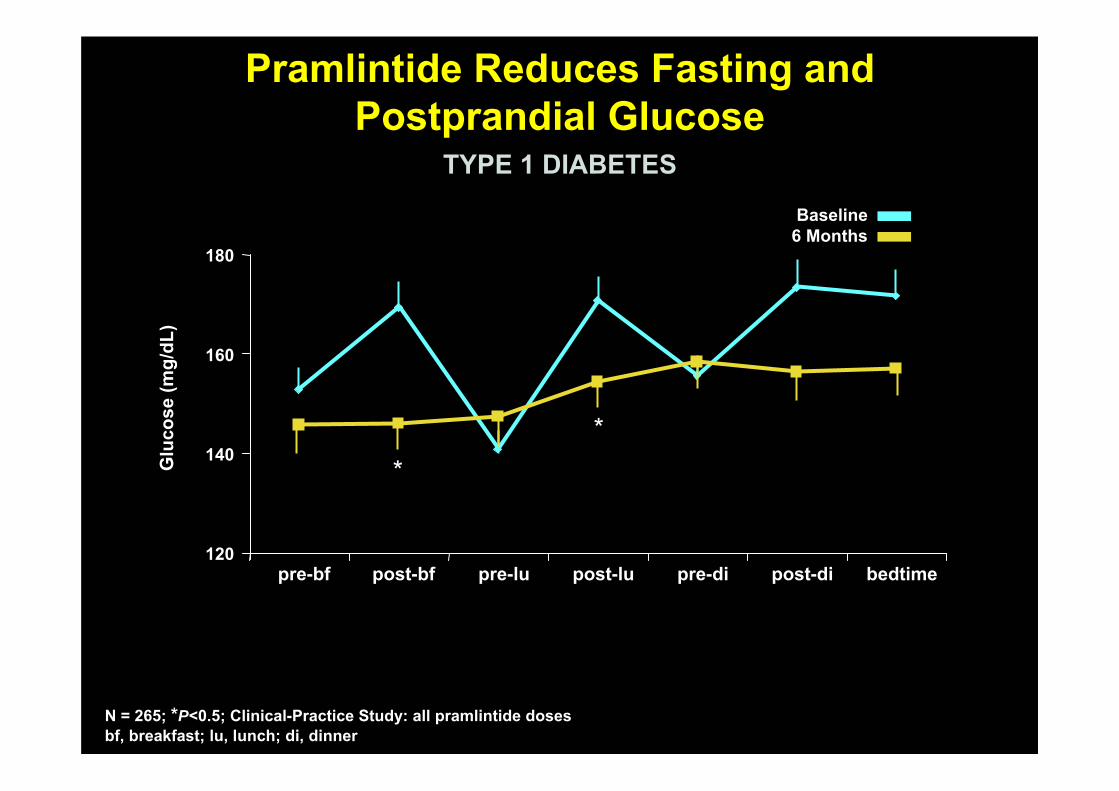
Pramlintide Reduces Fasting andPostprandial Glucose
Pramlintide Reduces Fasting andPostprandial Glucose
120
140
160
180
pre-bf post-bf pre-lu post-lu pre-di post-di bedtime
Glu
cose
(mg/
dL)
Baseline6 Months
**
TYPE 1 DIABETESTYPE 1 DIABETES
N = 265; *P<0.5; Clinical-Practice Study: all pramlintide doses bf, breakfast; lu, lunch; di, dinner
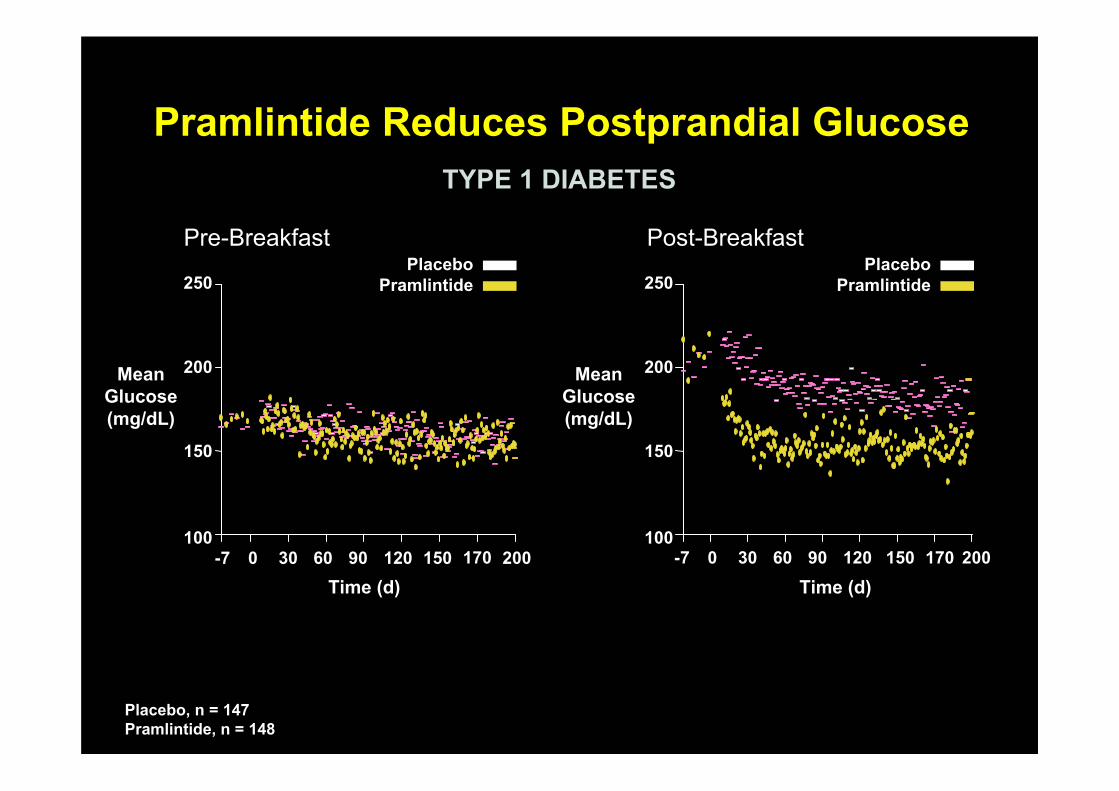
Pramlintide Reduces Postprandial GlucosePramlintide Reduces Postprandial Glucose
Pre-Breakfast Post-Breakfast
100
150
200
250
Mean Glucose (mg/dL)
Time (d)-7 30 60 90 1200 150 200170
Time (d)-7 30 60 90 1200 150 200170
100
150
200
250
Mean Glucose (mg/dL)
PlaceboPramlintide
PlaceboPramlintide
TYPE 1 DIABETESTYPE 1 DIABETES
Placebo, n = 147Pramlintide, n = 148
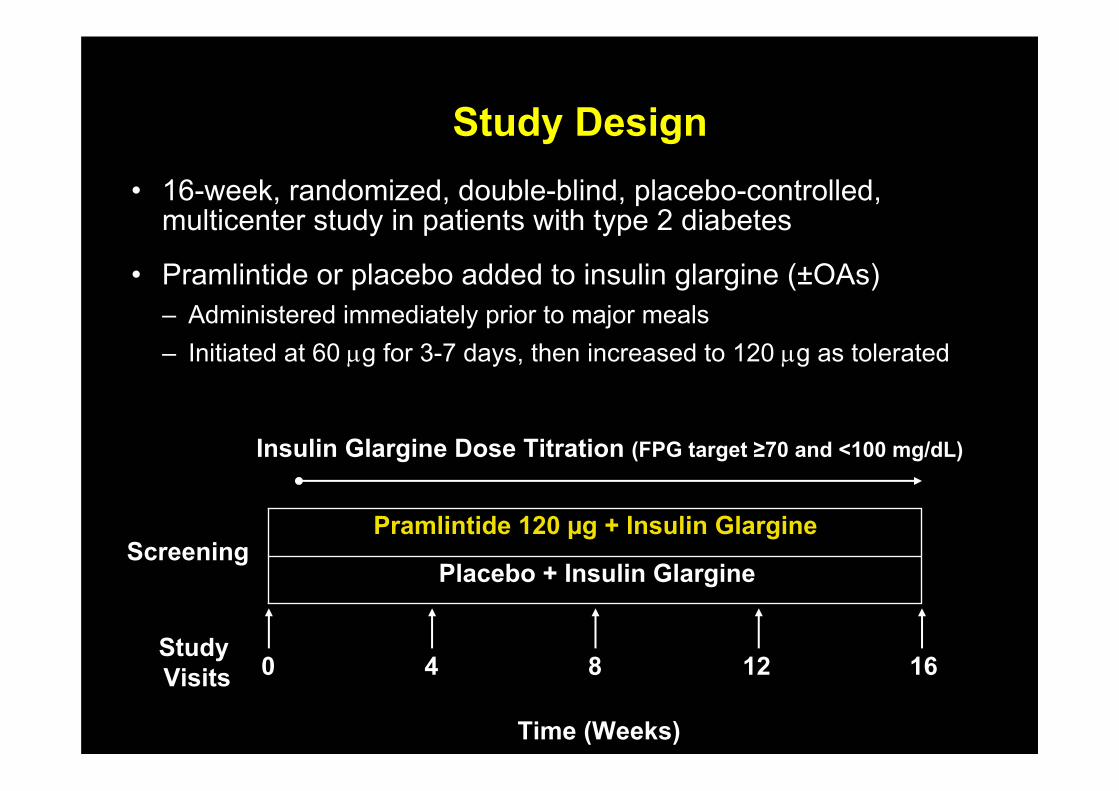
Study DesignStudy Design
Pramlintide 120 µg + Insulin Glargine
Placebo + Insulin Glargine
0 4 8 12 16
Insulin Glargine Dose Titration (FPG target ≥70 and <100 mg/dL)
Screening
Time (Weeks)
• 16-week, randomized, double-blind, placebo-controlled, multicenter study in patients with type 2 diabetes
• Pramlintide or placebo added to insulin glargine (±OAs)– Administered immediately prior to major meals– Initiated at 60 μg for 3-7 days, then increased to 120 μg as tolerated
Study Visits
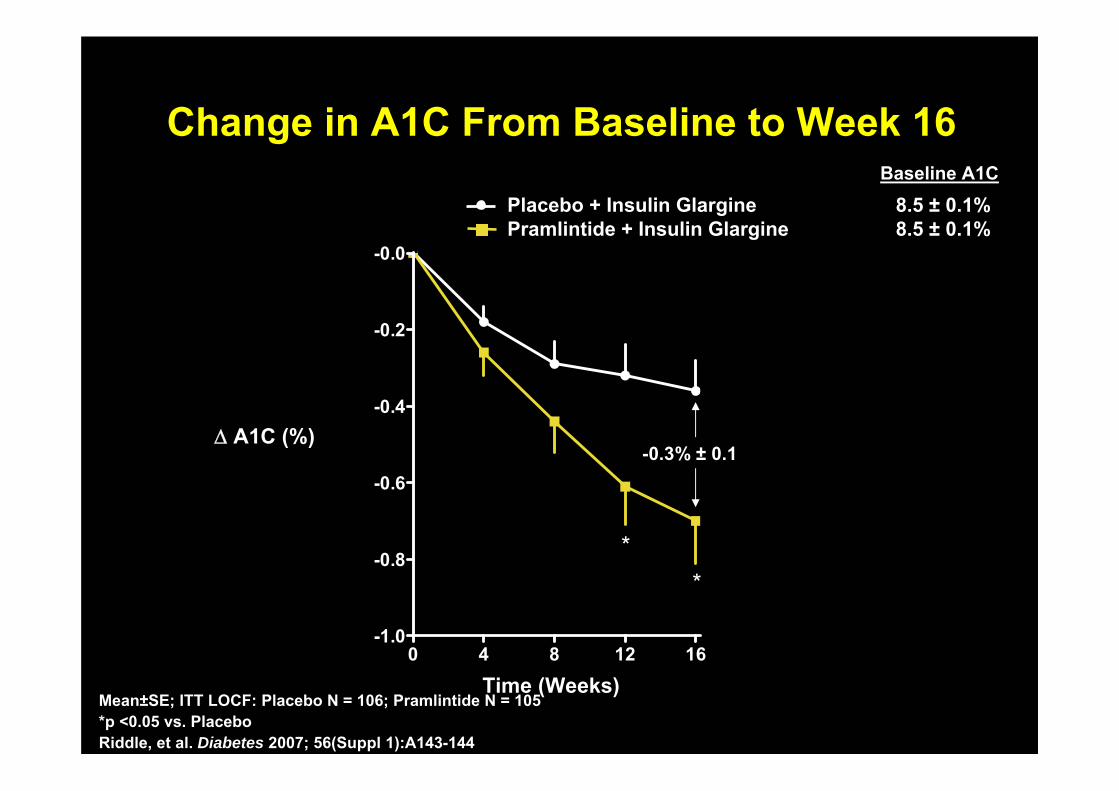
Change in A1C From Baseline to Week 16Change in A1C From Baseline to Week 16
Mean±SE; ITT LOCF: Placebo N = 106; Pramlintide N = 105*p <0.05 vs. PlaceboRiddle, et al. Diabetes 2007; 56(Suppl 1):A143-144
0 4 8 12 16-1.0
-0.8
-0.6
-0.4
-0.2
-0.0
**
-0.3% ± 0.1
Baseline A1C
Placebo + Insulin GlarginePramlintide + Insulin Glargine
8.5 ± 0.1%8.5 ± 0.1%
Δ A1C (%)
Time (Weeks)
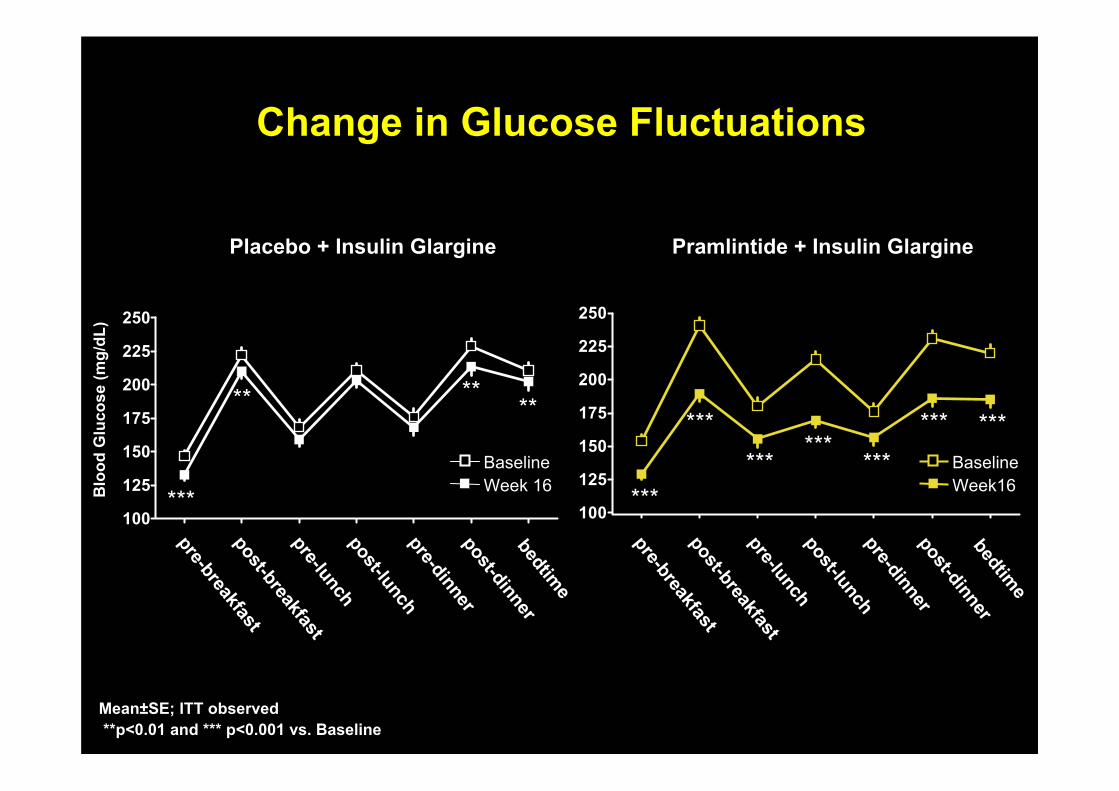
Change in Glucose FluctuationsChange in Glucose Fluctuations
100
125
150
175
200
225
250
BaselineWeek16
******
***
Mean±SE; ITT observed**p<0.01 and *** p<0.001 vs. Baseline
100
125
150
175
200
225
250
pre-breakfastpost-breakfastpre-lunchpost-lunchpre-dinnerpost-dinnerbedtime
pre-breakfastpost-breakfastpre-lunchpost-lunchpre-dinnerpost-dinnerbedtime
BaselineWeek 16
Pramlintide + Insulin GlarginePlacebo + Insulin Glargine
Blo
od G
luco
se (m
g/dL
)
****** ***
*****
****
***
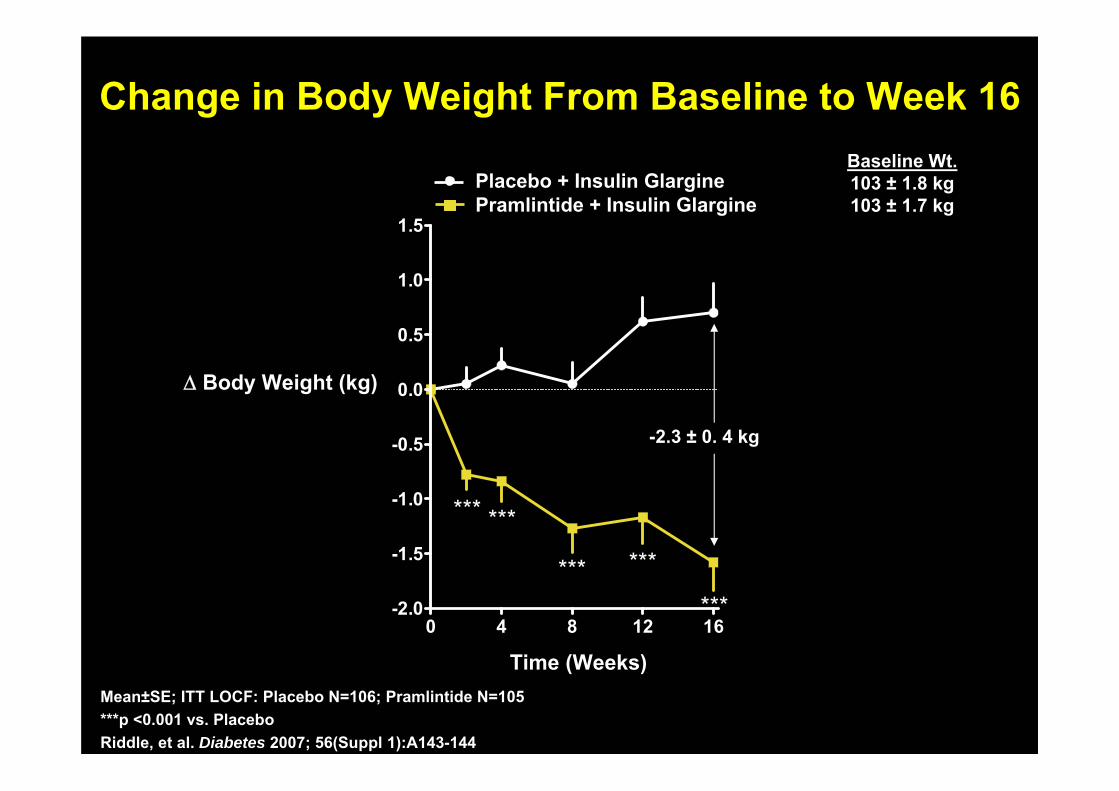
Change in Body Weight From Baseline to Week 16Change in Body Weight From Baseline to Week 16
0 4 8 12 16-2.0
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
Time (Weeks)
*** ***
*** ***
***
-2.3 ± 0. 4 kg
Mean±SE; ITT LOCF: Placebo N=106; Pramlintide N=105***p <0.001 vs. PlaceboRiddle, et al. Diabetes 2007; 56(Suppl 1):A143-144
Placebo + Insulin GlarginePramlintide + Insulin Glargine
Baseline Wt.103 ± 1.8 kg103 ± 1.7 kg
Δ Body Weight (kg)
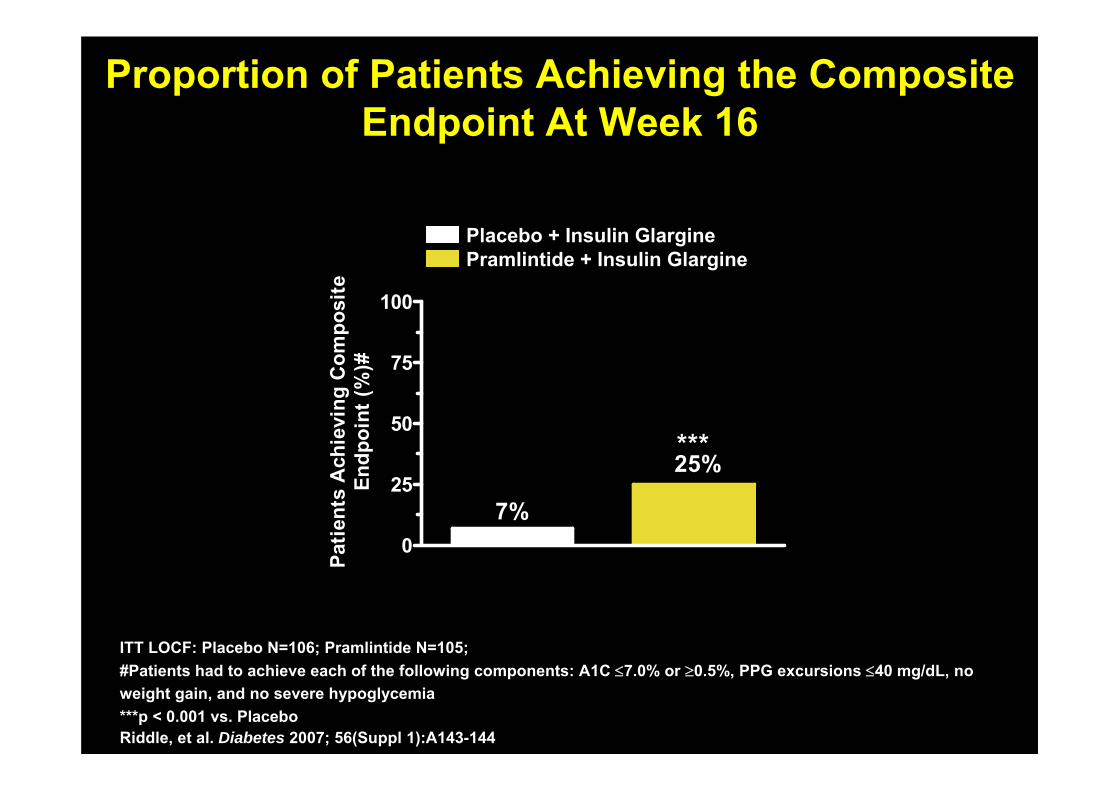
Proportion of Patients Achieving the Composite Endpoint At Week 16
Proportion of Patients Achieving the Composite Endpoint At Week 16
ITT LOCF: Placebo N=106; Pramlintide N=105; #Patients had to achieve each of the following components: A1C ≤7.0% or ≥0.5%, PPG excursions ≤40 mg/dL, no weight gain, and no severe hypoglycemia ***p < 0.001 vs. PlaceboRiddle, et al. Diabetes 2007; 56(Suppl 1):A143-144
0
25
50
75
100
25%***
7%
Patie
nts
Ach
ievi
ng C
ompo
site
Endp
oint
(%)#
Placebo + Insulin Glargine Pramlintide + Insulin Glargine
ConclusionsConclusions♦ Amylin, a newly discovered islet-hormone, has an
important role in glucose regulation, particularly postprandial hyperglycemia
♦ Synthetic amylin (pramlintide), provides an opportunity to replace this peptide to both improve glycemia and reduce weight.
♦ Careful patient selection, in addition to physicians comfortable with insulin use, are both important for success
Recommended














![激 素 [ Hormone ]](https://img.pdfslide.tips/doc/110x75/568137ed550346895d9fa81b/-hormone-.jpg)