-
7/29/2019 Anemia - Blok HIS-K9
1/34
NUTRITIONAL CARE IN
ANEMIA
Nutrition DepartementFaculty of MedicineUniversity of North
Sumatera
-
7/29/2019 Anemia - Blok HIS-K9
2/34
Definition Deficit of circulating RBC associated with
diminished oxygen-carrying capacity of the
blood
Most common hematologic disorder by far
Hb < 12 g/dL Hb < 13 or 13.5 g/dL
-
7/29/2019 Anemia - Blok HIS-K9
3/34
Classification
Microcytic (small cell)
- Major nutritional cause is iron deficiency
- Minor pirydoxin & copper deficiency
Normocytic anemia
- PEM & various chronic disease
Macrocytic
- Vitamin B12 & folic acid deficiency
-
7/29/2019 Anemia - Blok HIS-K9
4/34
Iron-deficiency anemiaisthemostcommon nutritional anemiaand
perhaps
the most common nutritional deficiencydisorder in the world
-
7/29/2019 Anemia - Blok HIS-K9
5/34
Characterized by the production of smallerythrocytes and
diminished level of
circulating hemoglobin
Last stage of iron deficiency
Represent the end point of a long period of
iron deprivation
-
7/29/2019 Anemia - Blok HIS-K9
6/34
The greatest risk :
- Between 6 month 4 year
- Early adolescent- During the menstruating years
- During pregnancy
-
7/29/2019 Anemia - Blok HIS-K9
7/34
Causes of Iron Deficiency
Dietary inadequacy the most common cause- poor diet
(vegetarian)
Inadequate absorption Diarrhea ; intestinal disease ; atrophic
gastritis ; Achlorhydria ; partial or total gastrectomy ; drug
interference
Increased Iron requirement Pregnancy Infancy Adolescence
lactation Increased excretion
- excessive menstrual blood- hemorrhage from injury- chronic
blood loss
-
7/29/2019 Anemia - Blok HIS-K9
8/34
Dietary Iron
Heme Fe (meat, fish and poultry) best
absorbed
Non-heme Fe (cereal, vegetables) taken up lessavidly
Heme Fe 20% bioavailable, nonheme only 3%
Ionic Fe (Fe++) also well absorbed
>1/3 of Fe from fortification of flour
Tea inhibits Fe absorption
-
7/29/2019 Anemia - Blok HIS-K9
9/34
Iron Absorption
Proximal small bowel, esp duodenum
Enhanced by gastric acid (Fe+2 is valance
absorbed) Heme Fe > non-heme Fe
Reciprocal relationship to iron stores
Direct relationship to erythropoiesis; with
ineffective erythropoiesis Inhibited by inflammation,
phytates
-
7/29/2019 Anemia - Blok HIS-K9
10/34
Plasma
Fe
16%
65%
4%
15%
-
7/29/2019 Anemia - Blok HIS-K9
11/34
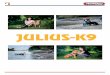
IRONBody Compartments - 75 kg man
Stores1000 mg
Tissue500 mg
Red Cells2300 mg
30 mgAbsorption < 1 mg/day
Excretion < 1 mg/day
-
7/29/2019 Anemia - Blok HIS-K9
12/34
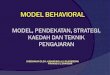
IRON STORESIron Deficiency Anemia
Stores0 mg
Tissue500 mg
Red Cells1500 mg
3 mg
Absorption 2-10 mg/day
Excretion Dependent on Cause
-
7/29/2019 Anemia - Blok HIS-K9
13/34
Mechanisms for maintaining iron balance :
- continuous reutilization of iron
- regulation of the absorption of iron
- access to specific storage protein (ferritin)
-
7/29/2019 Anemia - Blok HIS-K9
14/34
Typical diet : formerly ~10-15 mg/d,
now ~24 mg/d
10-15% comes from heme sources (meats &
seafood)
85-90% comes from non heme sources (dried
beans, peas, leafy green vegetable)
> 1/3 of Fe from fortification of flour.
-
7/29/2019 Anemia - Blok HIS-K9
15/34
Medical Management
Treatment should focus on the underlying
disease, although this is often difficult
Repletion of iron stores, not merely
alleviation of the anemia should be the
goal
-
7/29/2019 Anemia - Blok HIS-K9
16/34
Therapy
Oral ferrous form
- ferrous sulfate most widely used
- 50 - 200 mg elemental Fe/d (60 mg,
1-3 x / day)
- 6.0 mg elemental Fe/kg per day in children
- Duration- 6 months
Parenteral-Fe dextran 50 mg/ml, 100 mg/d im/iv
- more expensive & not as safe
-
7/29/2019 Anemia - Blok HIS-K9
17/34
IRON THERAPY
Response
Initial response takes 7-14 days
Modest reticulocytosis (7-10%)
Correction of anemia requires 2-3 months
6 months of therapy beyond correction of
anemia needed to replete stores, assuming nofurther loss of
blood/iron
Parenteral iron possible, but problematic
-
7/29/2019 Anemia - Blok HIS-K9
18/34
If supplementation fails, maybe that :
1. The patients may not be taking themedication, most likely
because ofunpleasant side effect
2. Bleeding may be continuing3. The supplemental iron is not
being absorbed
Parenteral route
-
7/29/2019 Anemia - Blok HIS-K9
19/34
Medical Nutrition Therapy
In addition to supplementation, attention
should be given to the amount of absorbable
dietary iron
Liver, kidney, beef, egg yolk, dried fruit, dried
peas and beans, nuts, green leafy vegetables,
whole grain breads and cereals, and fortifiedfood.
-
7/29/2019 Anemia - Blok HIS-K9
20/34
Factorsaffecting absorption
Enhancing factors :
- Ascorbic acid
- MFP
Inhibiting factors :
- Carbonates
- Oxalates
- Phytates
- Tanin
-
7/29/2019 Anemia - Blok HIS-K9
21/34
Prevention
Iron supplementation, i.e. giving iron tablets
to certain target groups Iron fortification of certain foods
Education about food in order to improve the
absorption
-
7/29/2019 Anemia - Blok HIS-K9
22/34
Recommendations :
Improve food choices to increase amount of
total dietary iron
Include a source of vitamin C at every meal Include MFP at every
meal if possible
Avoid drinking a large amounts of tea or
coffee with meals
-
7/29/2019 Anemia - Blok HIS-K9
23/34
MACROCYTIC ANEMIAS
Characterized by an MCV greater than 100 3
Also called megaloblastic anemias large,immature red cell
precursors (megaloblasts)
accumulate in the bone marrow
-
7/29/2019 Anemia - Blok HIS-K9
24/34
Vitamin B12 Deficiency
Most often caused by impaired absorption
Strict vegetarian (vegans) who consumeno dairy products, eggs or
meat
increased risk for deficiencies
The main cause of vitamin B12 deficiency
is PERNICIOUS ANEMIA
-
7/29/2019 Anemia - Blok HIS-K9
25/34
Vitamin B12 deficiency should be
considered when the plasma concentration
< 150 200 pg/ml
If there is a deficiency, the plasma folate
level may be elevated to 15 or 20 ng/ml ~
impaired tissue folate uptake and turnover
(methyl-folate trap)
-
7/29/2019 Anemia - Blok HIS-K9
26/34
The development of vitamin B12 deficiency
First stage, characterized by a negative vitamin B12
balance,
During which the plasma vitamin B12 level is marginal and
onlyvitamin B carries in plasma (transcobalamins) may beabnormally
low
Subsequently, the plasma vitamin B12 level fallsWhen the level
reaches 100 150 pg/ml, neutrophils begins toappear
hypersegmented
Finally, macroovalocytes appear, the MCV is elevated and the
Hblevel drops
Anemia develops IN THE LATER STAGES of vitamin B12 deficiency
like iron deficiency
-
7/29/2019 Anemia - Blok HIS-K9
27/34
Dietary Sources
Found ONLY in food of animal origin Most meat and dairy products
contain B12
Beef liver : an especially rich sources
RDA
and 2 g / day
During pregnancy 2,2 g / dayDuring lactation 2,6 g / day
-
7/29/2019 Anemia - Blok HIS-K9
28/34
Remission of the sign & symptoms a singleintramuscular
injection of 100 to 1000 g of
cyanocobalamins or hydroxocobalamins
Daily administration of 100 g for several days
For PA patients & other who need continued
parenteral therapy injections of 100 g everymonth
-
7/29/2019 Anemia - Blok HIS-K9
29/34
Folic Acid Deficiency
Large, immature red blood cells
DNA synthesis slows & cells lose their
ability to divide
The nucleus of the cells is not released as normally
immature blood cells are enlarged & oval shaped
-
7/29/2019 Anemia - Blok HIS-K9
30/34
Causes of Folic Acid Deficiency
Insufficient intake
RDA : 180 g / day
200 g / day
During pregnancy 400 g / day
During lactation 260 - 280 g / day
Suboptimal folate intake during early pregnancy (even
withoutother manifestations of folate deficiency major risk factor
forneural tube birth effects
Person who rarely consume green leafy vegetables or othersources
of folate
-
7/29/2019 Anemia - Blok HIS-K9
31/34
Associated with a variety of intestinal disorderssuch as Crohns
disease, celiac disease andtropical sprue
Alcoholics
Cigarette smokers
Drug-nutrient interactions (e.g. anticonvulsants,diuretics,
antibiotics and antimalarials)
-
7/29/2019 Anemia - Blok HIS-K9
32/34
Dietary Sources
Widely distributed in : Yeast
Liver and other organ meat
Leafy vegetables
Fresh fruit
Enriched bread and cereal products
Oranges juice the highest contributor of folic acid to
theAmerican diet
Between 50% and 90% of folate in the food destroyedby prolonged
cooking and processing
-
7/29/2019 Anemia - Blok HIS-K9
33/34
Treatment
Plasma level should be usedto guide therapy
Readily resolved with a 1 mg daily oral supplement
In the patients with malabsorption,
Initial treatment parental folate
Maintenance oral therapy
-
7/29/2019 Anemia - Blok HIS-K9
34/34