L E B E R ' S I D I O P A T H I C S T E L L A T E R E T I N O P A T H Y
DENIS M. CARROLL, M . D . , AND RUDOLPH M. FRANKLIN, M . D .
New Orleans, Louisiana
Three patients with Leber's idiopathic stellate retinopathy—a 16-year-old girl, a 26-year-old man, and a 7-year-old girl—also had acute multifocal chorioretinitis. The second patient also had an associated idiopathic peripheral seventh nerve palsy. Extensive neurologic testing and viral cultures gave no explanation of the origin of the retinopathy. However, each of the patients had had an upper respiratory or gastrointestinal illness shortly before the onset of the condition, sug-gesting an infectious origin. In all three patients the optic disk swelling resolved spontaneously and the stellate exudate gradually faded.
Leber's stellate retinopathy has the fol-lowing features: (1) macular exudates in a star formation; (2) optic disk swelling; (3) unilaterality; (4) spontaneous resolution; and (5) an unknown cause.1 The clinical2 , 3
and fluorescein angiographic features4,5
have been described but, although Gass4 , 6
has suggested a viral cause, the exact nature of this condition remains specula-tive.
We studied three patients who had the usual clinical features of Leber's stellate retinopathy but who also had multiple foci of chorioretinitis during the active stage of the condition. To the best of our knowledge, this pattern has not been reported previously. One patient also had concurrent unilateral peripheral facial nerve paralysis (Bell's palsy).
CASE REPORTS
Case 1—This 16-year-old girl was first examined in January 1980 because of a 12-day history of decreased
visual acuity in her left eye. Several days before the onset of reduced vision, she had had a severe system-ic illness resembling influenza and consisting of fever, malaise, and headache. The symptoms had resolved spontaneously, and the patient was well until the visual loss in the left eye began. Medical, ocular, and family histories were noncontributory.
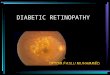
Our initial examination disclosed an uncorrected visual acuity of R.E.: 6/6 (20/20) and L.E. 6/120 (20/400). There was a relative afferent pupillary de-fect in the left eye. A slit-lamp examination disclosed a clear anterior segment with an occasional cell in the vitreous cavity of the left eye. Ophthalmoscopy of the right eye showed clear media with a normal optic disk and retinal vessels. There were three small focal white lesions in the midperipheral retina. All three lesions were less than 0.25 disk diameter in size and slightly elevated (Fig. 1). They appeared to involve the deeper layers of the retina and the choroid.
Ophthalmoscopy of the left eye showed 1 + vitre-ous cells. The left optic disk was markedly swollen
Accepted for publication Oct. 7, 1981. From the Lions Eye Research Laboratories, De-
partment of Ophthalmology, LSU Eye Center, LSU Medical Center School of Medicine, New Orleans, Louisiana. This study was supported in part by grant EY02377 from the National Eye Institute.
Reprint requests to Denis M. Carroll, M.D., LSU Eye Center, 136 S. Roman, New Orleans, LA 70112.
Fig. 1 (Carroll and Franklin). Case 1, right eye. One of three similar chorioretinal lesions (X 2).
96 AMERICAN JOURNAL OF OPHTHALMOLOGY 93:96-101, 1982
VOL. 93, NO. 1 LEBER'S STELLATE RETINOPATHY 97
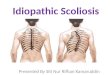
and elevated approximately 2 to 3 mm. The capillar-ies of the optic disk were dilated but no hemorrhages were present. A fine stellate pattern of exudate appeared in the macula with subretinal fluid extend-ing from the optic disk into the macular area. A small, focal, yellow-white, deep retinal lesion, simi-lar to those noted in the right eye, was located midway between the optic disk and the macula (Fig. 2). Visual field examination of the right eye gave normal results, but the left eye demonstrated a dense centrocecal scotoma. A- and B-scan ultrasono-graphic examinations disclosed a solid elevation of the optic nerve head of approximately 2 mm, with a shallow detachment of the retina extending from the optic disk to the macula. The orbits appeared to be normal.
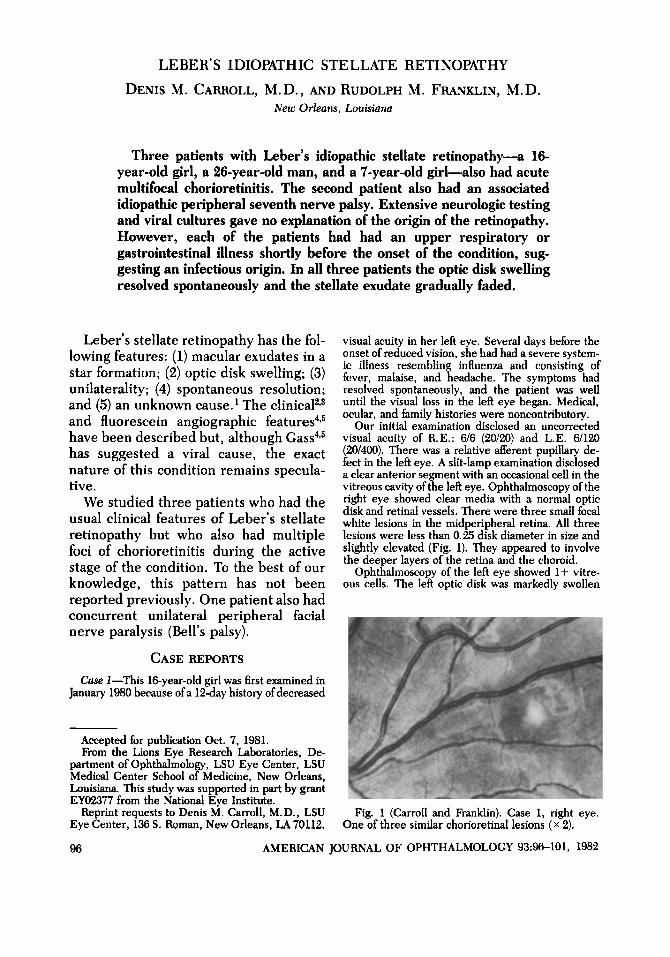
Fluorescein angiography demonstrated extensive leakage from the left optic disk and late hyperfluores-cence of the focal chorioretinal lesions in both eyes (Fig. 3).
Tests done when the patient entered the hospital (complete blood cell count, urinalysis, SMA-12, blood cultures, purified protein derivative tuberculin test, histoplasmin skin tests, VDRL test, and chest and skull X-rays with views of the optic foramina) all gave normal results. The patient was discharged after four days and observed but not treated.
A follow-up examination two weeks later disclosed a visual acuity of R.E.: 676 (20/20) and L.E.: 6/120 (20/400). The focal chorioretinal lesions in the right eye remained unchanged. The optic nerve swelling had lessened, and there was a marked reduction in the amount of subretinal fluid in the left eye. The macular star figure was still present.
Examination four weeks after onset disclosed that the visual acuity in the left eye had improved to 6/60 (20/200). The focal chorioretinal lesions in the right eye had faded slightly but were still visible. Further reduction in the optic nerve swelling in the left eye had occurred, along with resolution of all subretinal fluid. The macular star figure and focal chorioretinal lesion remained. Visual field examination showed that the centrocecal scotoma was reduced in size.
The patient was examined two months later in April 1980; at that time she reported that her vision had improved steadily. Her visual acuity had im-proved to R.E.: 674.5 (20/15) and L.E.: 6/60 +1 (20/200 +1). The afferent pupillary defect was still present in the left eye. Ophthalmoscopy of the right eye showed only faint white spots that corresponded to the previous focal chorioretinal lesions. Examina-tion of the left eye disclosed a flat optic disk nasally, with pale swelling of the temporal edge and slight swelling of the adjacent nerve fiber layer. The sub-retinal fluid was entirely absent, and only small punctate areas of intraretinal exudate remained in the macula.
Case 2—This 26-year-old man was first examined in August 1980 because of a 12-day history of blurred vision in the left eye and a three-day history of left-sided facial weakness. He had noted stomach cramps, diarrhea, and malaise just before the onset of visual loss. Medical, ocular, and family histories were noncontributory. Our initial examination disclosed an uncorrected visual acuity of R.E.: 6/4.5 — 1 (20/15 - 1 ) and L.E.: 6/24 - 1 (20/80 - 1 ) . Refraction in the left eye improved the visual acuity to 6/15 —12 (20/50) with a —1.00 sphere. Ocular motility was
Fig. 2 (Carroll and Franklin). Case 1, left eye. Note the markedly swollen optic disk, the macular star figure, and the focal white chorioretinal lesion be-tween the optic disk and the macula.
Fig. 3 (Carroll and Franklin). Case 1, right eye. Late-phase fluorescein angiogram shows hyperfluo-rescence of two focal chorioretinal lesions. The upper lesion is the one shown in Figure 1.
98 AMERICAN JOURNAL OF OPHTHALMOLOGY JANUARY, 1982
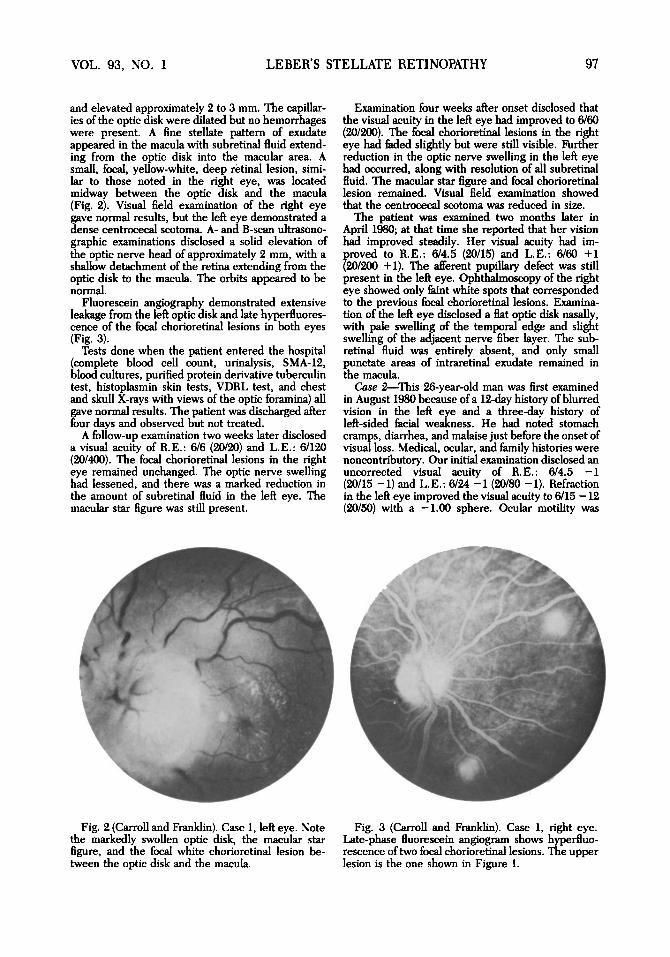
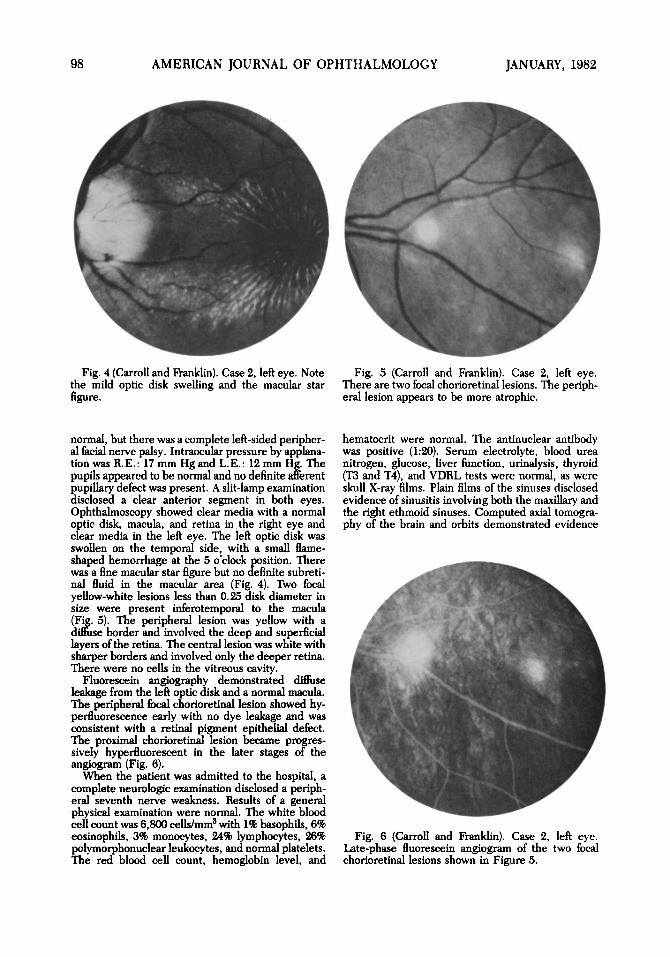
Fig. 4 (Carroll and Franklin). Case 2, left eye. Note the mild optic disk swelling and the macular star figure.
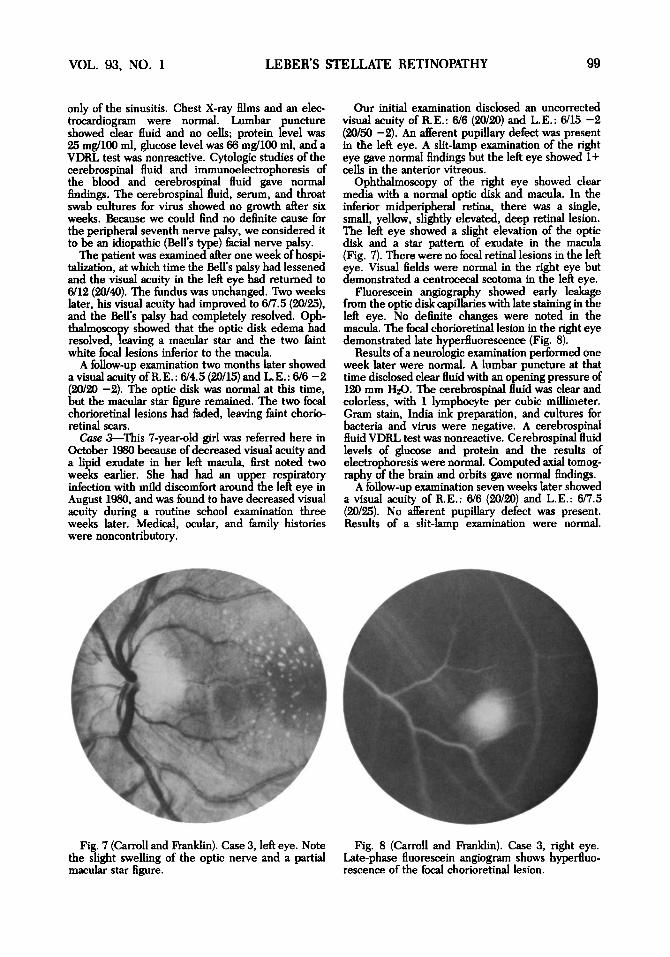
Fig. 5 (Carroll and Franklin). Case 2, left eye. There are two focal chorioretinal lesions. The periph-eral lesion appears to be more atrophic.
normal, but there was a complete left-sided peripher-al facial nerve palsy. Intraocular pressure by applana-tion was R.E.: 17 mm Hg and L.E.: 12 mm Hg. The pupils appeared to be normal and no definite afferent pupillary defect was present. A slit-lamp examination disclosed a clear anterior segment in both eyes. Ophthalmoscopy showed clear media with a normal optic disk, macula, and retina in the right eye and clear media in the left eye. The left optic disk was swollen on the temporal side, with a small flame-shaped hemorrhage at the 5 o'clock position. There was a fine macular star figure but no definite subreti-nal fluid in the macular area (Fig. 4). Two focal yellow-white lesions less than 0.25 disk diameter in size were present inferotemporal to the macula (Fig. 5). The peripheral lesion was yellow with a diffuse border and involved the deep and superficial layers of the retina. The central lesion was white with sharper borders and involved only the deeper retina. There were no cells in the vitreous cavity.
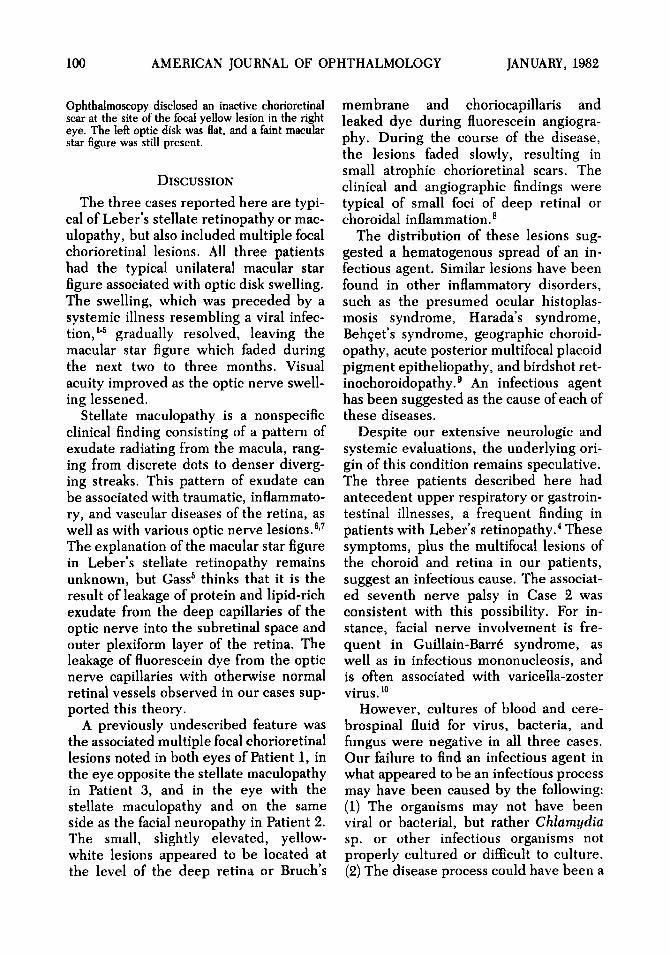
Fluorescein angiography demonstrated diffuse leakage from the left optic disk and a normal macula. The peripheral focal chorioretinal lesion showed hy-perfluorescence early with no dye leakage and was consistent with a retinal pigment epithelial defect. The proximal chorioretinal lesion became progres-sively hyperfluorescent in the later stages of the angiogram (Fig. 6).
When the patient was admitted to the hospital, a complete neurologic examination disclosed a periph-eral seventh nerve weakness. Results of a general physical examination were normal. The white blood cell count was 6,800 cells/mm3 with 1% basophils, 6% eosinophils, 3% monocytes, 24% lymphocytes, 26% polymorphonuclear leukocytes, and normal platelets. The red blood cell count, hemoglobin level, and
hematocrit were normal. The antinuclear antibody was positive (1:20). Serum electrolyte, blood urea nitrogen, glucose, liver function, urinalysis, thyroid (T3 and T4), and VDRL tests were normal, as were skull X-ray films. Plain films of the sinuses disclosed evidence of sinusitis involving both the maxillary and the right ethmoid sinuses. Computed axial tomogra-phy of the brain and orbits demonstrated evidence
Fig. 6 (Carroll and Franklin). Case 2, left eye. Late-phase fluorescein angiogram of the two focal chorioretinal lesions shown in Figure 5.
VOL. 93, NO. 1 LEBER'S STELLATE RETINOPATHY 99
only of the sinusitis. Chest X-ray films and an elec-trocardiogram were normal. Lumbar puncture showed clear fluid and no cells; protein level was 25 mg/100 ml, glucose level was 66 mg/100 ml, and a VDRL test was nonreactive. Cytologic studies of the cerebrospinal fluid and immunoelectrophoresis of the blood and cerebrospinal fluid gave normal findings. The cerebrospinal fluid, serum, and throat swab cultures for virus showed no growth after six weeks. Because we could find no definite cause for the peripheral seventh nerve palsy, we considered it to be an idiopathic (Bell's type) facial nerve palsy.
The patient was examined after one week of hospi-talization, at which time the Bell's palsy had lessened and the visual acuity in the left eye had returned to 6/12 (20/40). The fundus was unchanged. Two weeks later, his visual acuity had improved to 677.5 (20/25), and the Bell's palsy had completely resolved. Oph-thalmoscopy showed that the optic disk edema had resolved, leaving a macular star and the two faint white focal lesions inferior to the macula.
A follow-up examination two months later showed a visual acuity of R.E.: 674.5 (20/15) and L.E. : 6/6 - 2 (20/20 —2). The optic disk was normal at this time, but the macular star figure remained. The two focal chorioretinal lesions had faded, leaving faint chorio-retinal scars.
Case 3—This 7-year-old girl was referred here in October 1980 because of decreased visual acuity and a lipid exudate in her left macula, first noted two weeks earlier. She had had an upper respiratory infection with mild discomfort around the left eye in August 1980, and was found to have decreased visual acuity during a routine school examination three weeks later. Medical, ocular, and family histories were noncontributory.
Our initial examination disclosed an uncorrected visual acuity of R.E.: 676 (20/20) and L.E.: 6/15 - 2 (20/50 —2). An afferent pupillary defect was present in the left eye. A slit-lamp examination of the right eye gave normal findings but the left eye showed 1+ cells in the anterior vitreous.
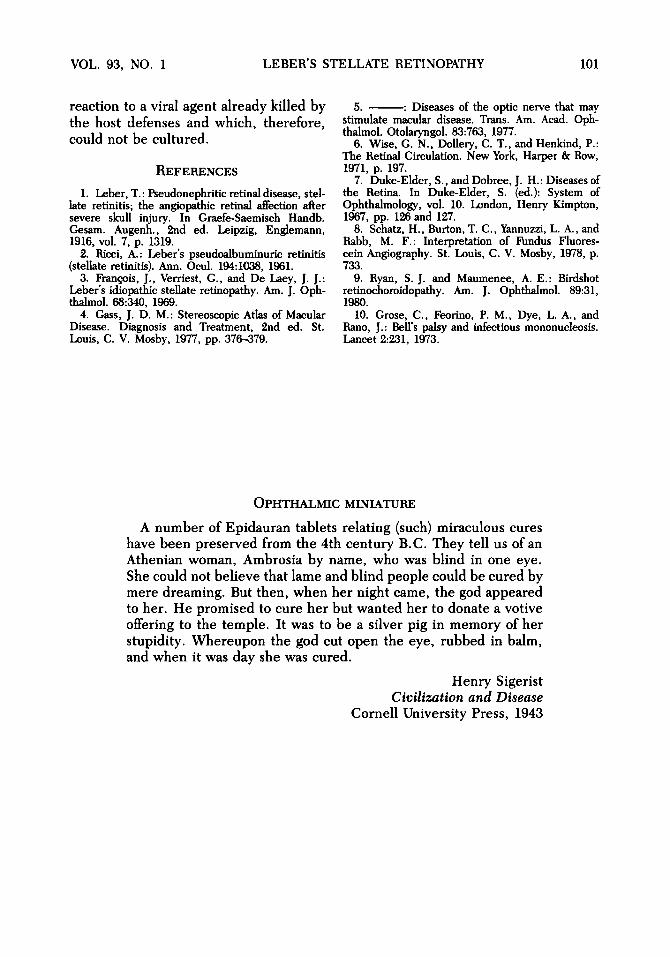
Ophthalmoscopy of the right eye showed clear media with a normal optic disk and macula. In the inferior midperipheral retina, there was a single, small, yellow, slightly elevated, deep retinal lesion. The left eye showed a slight elevation of the optic disk and a star pattern of exudate in the macula (Fig. 7). There were no focal retinal lesions in the left eye. Visual fields were normal in the right eye but demonstrated a centrocecal scotoma in the left eye.
Fluorescein angiography showed early leakage from the optic disk capillaries with late staining in the left eye. No definite changes were noted in the macula. The focal chorioretinal lesion in the right eye demonstrated late hyperfluorescence (Fig. 8).
Results of a neurologic examination performed one week later were normal. A lumbar puncture at that time disclosed clear fluid with an opening pressure of 120 mm H2O. The cerebrospinal fluid was clear and colorless, with 1 lymphocyte per cubic millimeter. Gram stain, India ink preparation, and cultures for bacteria and virus were negative. A cerebrospinal fluid VDRL test was nonreactive. Cerebrospinal fluid levels of glucose and protein and the results of electrophoresis were normal. Computed axial tomog-raphy of the brain and orbits gave normal findings.
A follow-up examination seven weeks later showed a visual acuity of R.E.: 6/6 (20/20) and L.E.: 6/7.5 (20/25). No afferent pupillary defect was present. Results of a slit-lamp examination were normal.
Fig. 7 (Carroll and Franklin). Case 3, left eye. Note the slight swelling of the optic nerve and a partial macular star figure.
Fig. 8 (Carroll and Franklin). Case 3, right eye. Late-phase fluorescein angiogram shows hyperfluo-rescence of the focal chorioretinal lesion.
100 AMERICAN JOURNAL OF OPHTHALMOLOGY JANUARY, 1982
Ophthalmoscopy disclosed an inactive chorioretinal scar at the site of the focal yellow lesion in the right eye. The left optic disk was flat, and a faint macular star figure was still present.
DISCUSSION
The three cases reported here are typi-cal of Leber's stellate retinopathy or mac-ulopathy, but also included multiple focal chorioretinal lesions. All three patients had the typical unilateral macular star figure associated with optic disk swelling. The swelling, which was preceded by a systemic illness resembling a viral infec-tion,1"6 gradually resolved, leaving the macular star figure which faded during the next two to three months. Visual acuity improved as the optic nerve swell-ing lessened.
Stellate maculopathy is a nonspecific clinical finding consisting of a pattern of exudate radiating from the macula, rang-ing from discrete dots to denser diverg-ing streaks. This pattern of exudate can be associated with traumatic, inflammato-ry, and vascular diseases of the retina, as well as with various optic nerve lesions.6'7
The explanation of the macular star figure in Leber's stellate retinopathy remains unknown, but Gass5 thinks that it is the result of leakage of protein and lipid-rich exudate from the deep capillaries of the optic nerve into the subretinal space and outer plexiform layer of the retina. The leakage of fluorescein dye from the optic nerve capillaries with otherwise normal retinal vessels observed in our cases sup-ported this theory.
A previously undescribed feature was the associated multiple focal chorioretinal lesions noted in both eyes of Patient 1, in the eye opposite the stellate maculopathy in Patient 3, and in the eye with the stellate maculopathy and on the same side as the facial neuropathy in Patient 2. The small, slightly elevated, yellow-white lesions appeared to be located at the level of the deep retina or Bruch's
membrane and choriocapillaris and leaked dye during fluorescein angiogra-phy. During the course of the disease, the lesions faded slowly, resulting in small atrophic chorioretinal scars. The clinical and angiographic findings were typical of small foci of deep retinal or choroidal inflammation.8
The distribution of these lesions sug-gested a hematogenous spread of an in-fectious agent. Similar lesions have been found in other inflammatory disorders, such as the presumed ocular histoplas-mosis syndrome, Harada's syndrome, Behcet's syndrome, geographic choroid-opathy, acute posterior multifocal placoid pigment epitheliopathy, and birdshot ret-inochoroidopathy.9 An infectious agent has been suggested as the cause of each of these diseases.
Despite our extensive neurologic and systemic evaluations, the underlying ori-gin of this condition remains speculative. The three patients described here had antecedent upper respiratory or gastroin-testinal illnesses, a frequent finding in patients with Leber's retinopathy.4 These symptoms, plus the multifocal lesions of the choroid and retina in our patients, suggest an infectious cause. The associat-ed seventh nerve palsy in Case 2 was consistent with this possibility. For in-stance, facial nerve involvement is fre-quent in Guillain-Barré syndrome, as well as in infectious mononucleosis, and is often associated with varicella-zoster virus.10
However, cultures of blood and cere-brospinal fluid for virus, bacteria, and fungus were negative in all three cases. Our failure to find an infectious agent in what appeared to be an infectious process may have been caused by the following: (1) The organisms may not have been viral or bacterial, but rather Chlamydia sp. or other infectious organisms not properly cultured or difficult to culture. (2) The disease process could have been a
VOL. 93, NO. 1 LEBER'S STELLATE RETINOPATHY 101
reaction to a viral agent already killed by the host defenses and which, therefore, could not be cultured.
REFERENCES
1. Leber, T. : Pseudonephritic retinal disease, stel-late retinitis; the angiopathic retinal affection after severe skull injury. In Graefe-Saemisch Handb. Gesam. Augenh., 2nd ed. Leipzig, Englemann, 1916, vol. 7, p. 1319.
2. Ricci, A.: Leber's pseudoalbuminuric retinitis (stellate retinitis). Ann. Ocul. 194:1038, 1961.
3. François, J . , Verriest, G., and De Laey, J. J . : Leber's idiopathic stellate retinopathy. Am. J. Oph-thalmol. 68:340, 1969.
4. Gass, J. D. M.: Stereoscopic Atlas of Macular Disease. Diagnosis and Treatment, 2nd ed. St. Louis, C. V. Mosby, 1977, pp. 376-379.
5. : Diseases of the optic nerve that may stimulate macular disease. Trans. Am. Acad. Oph-thalmol. Otolaryngol. 83:763, 1977.
6. Wise, G. N., Dollery, C. T., and Henkind, P.: The Retinal Circulation. New York, Harper & Row, 1971, p. 197.
7. Duke-Elder, S., and Dobree, J. H.: Diseases of the Retina. In Duke-Elder, S. (ed.): System of Ophthalmology, vol. 10. London, Henry Kimpton, 1967, pp. 126 and 127.
8. Schatz, H., Burton, T. C , Yannuzzi, L. A., and Rabb, M. F.: Interpretation of Fundus Fluores-cein Angiography. St. Louis, C. V. Mosby, 1978, p. 733.
9. Ryan, S. J. and Maumenee, A. E.: Birdshot retinochoroidopathy. Am. J. Ophthalmol. 89:31, 1980.
10. Grose, C , Feorino, P. M., Dye, L. A., and Rano, J . : Bell's palsy and infectious mononucleosis. Lancet 2:231, 1973.
OPHTHALMIC MINIATURE
A number of Epidauran tablets relating (such) miraculous cures have been preserved from the 4th century B.C. They tell us of an Athenian woman, Ambrosia by name, who was blind in one eye. She could not believe that lame and blind people could be cured by mere dreaming. But then, when her night came, the god appeared to her. He promised to cure her but wanted her to donate a votive offering to the temple. It was to be a silver pig in memory of her stupidity. Whereupon the god cut open the eye, rubbed in balm, and when it was day she was cured.
Henry Sigerist Civilization and Disease
Cornell University Press, 1943
Recommended