Immunità e
Infiammazione VINCENT CASTRONOVO

MANGIARE
SENZA VENIR MANGIATI
Difesa
LIVELLO I Le barriere
LIVELLO II Immunità
innata
LIVELLO III Immunità specifica

PRIMA LINEA DI DIFESA
BARRIERE
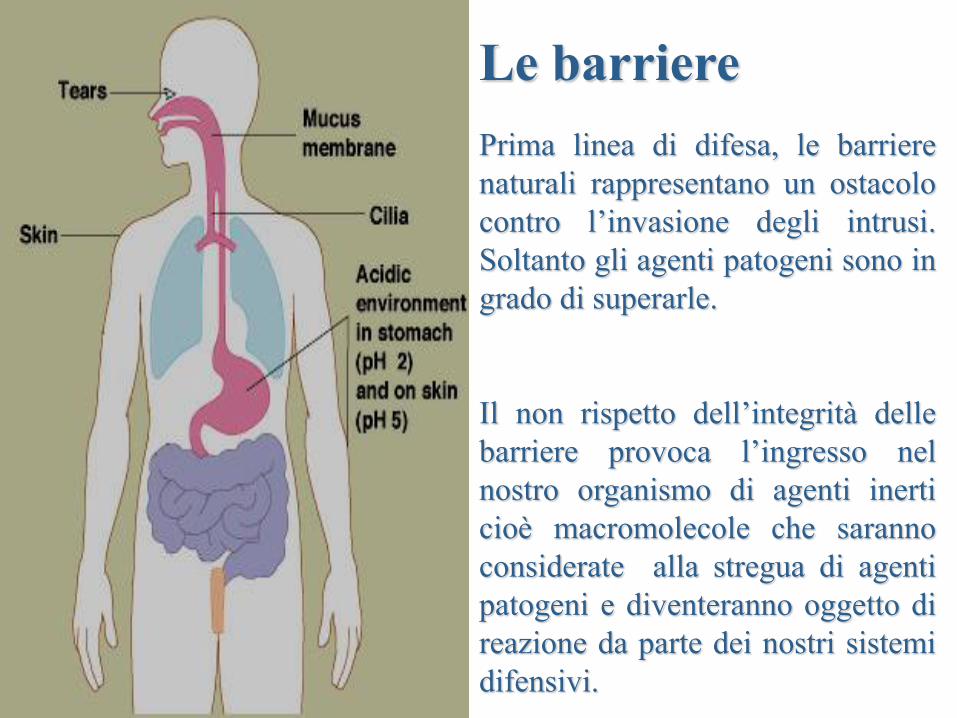
Le barriere
Prima linea di difesa, le barriere
naturali rappresentano un ostacolo
contro l’invasione degli intrusi.
Soltanto gli agenti patogeni sono in
grado di superarle.
Il non rispetto dell’integrità delle
barriere provoca l’ingresso nel
nostro organismo di agenti inerti
cioè macromolecole che saranno
considerate alla stregua di agenti
patogeni e diventeranno oggetto di
reazione da parte dei nostri sistemi
difensivi.

Le barriere
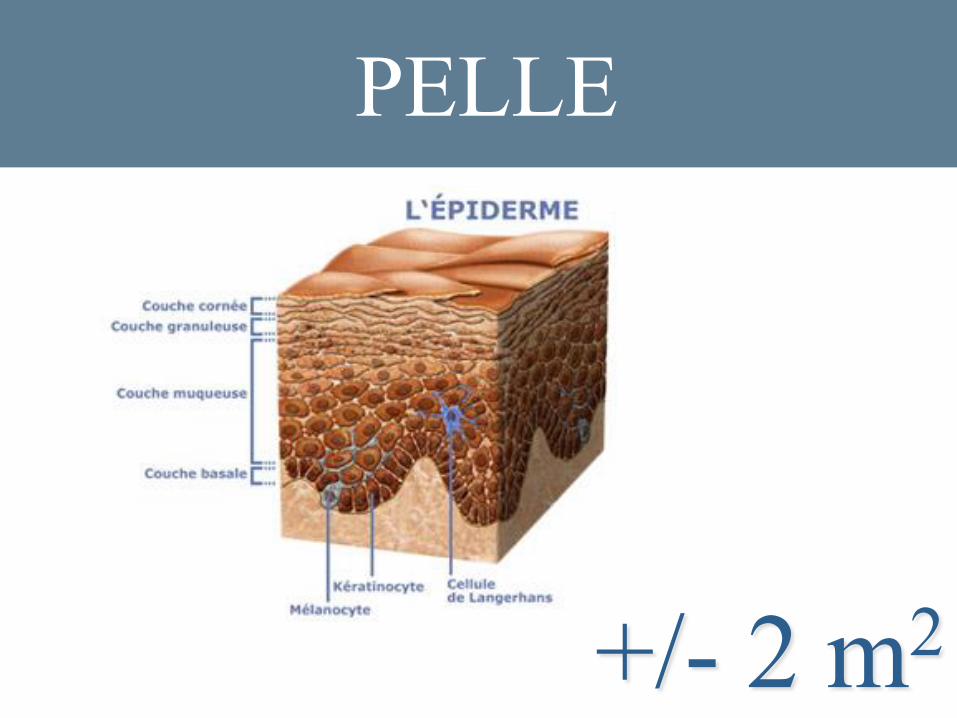
PELLE
+/- 2 m2
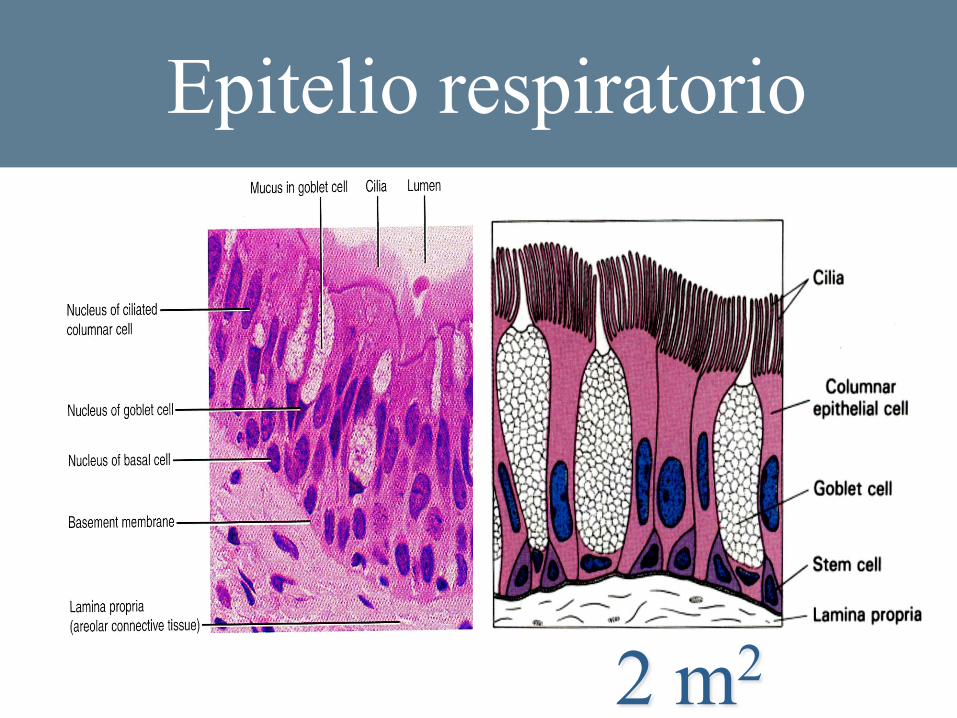
Epitelio respiratorio
2 m2
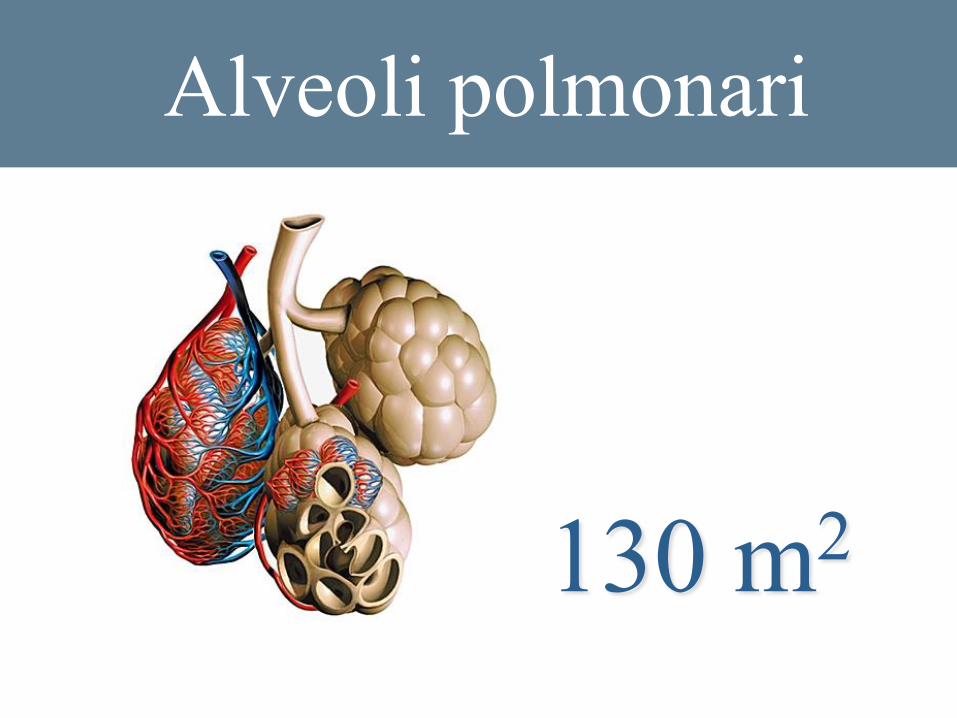
Alveoli polmonari
130 m2
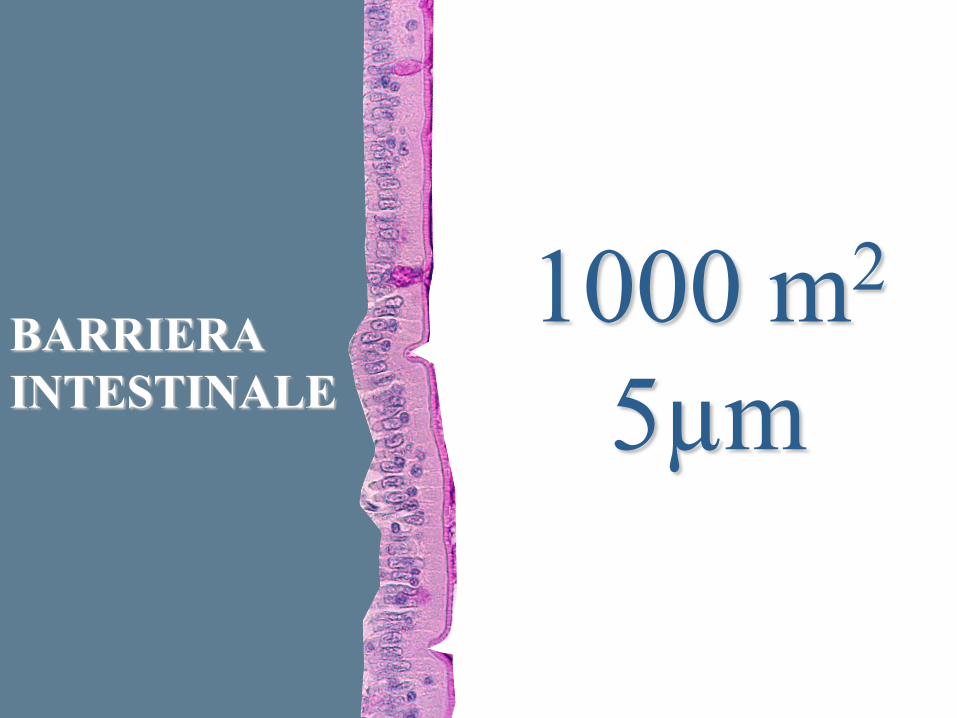
BARRIERA
INTESTINALE
1000 m2
5µm
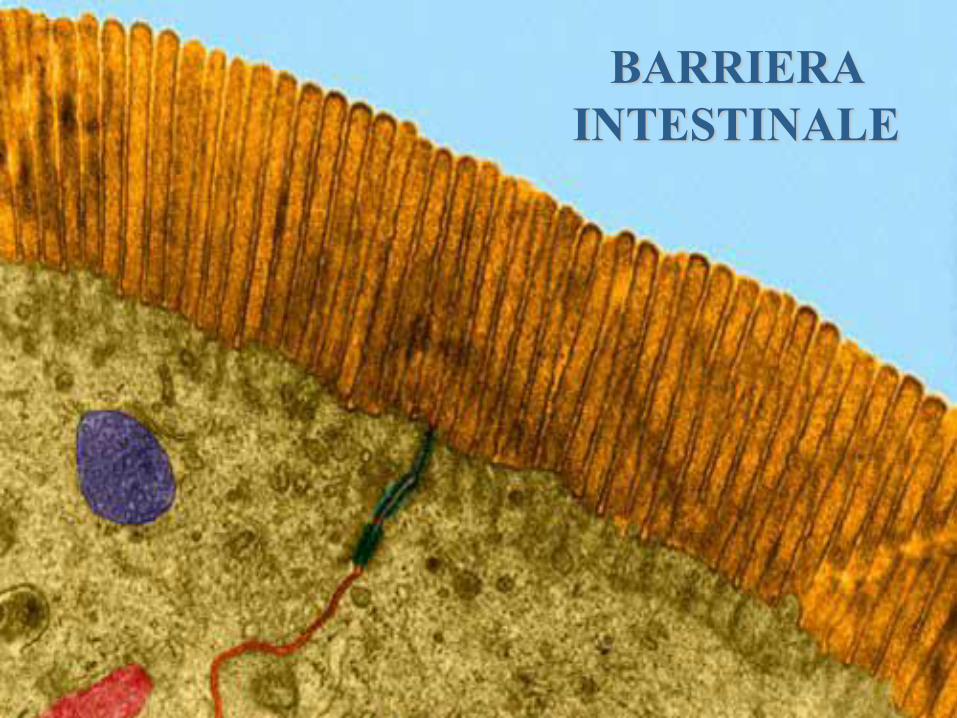
BARRIERA
INTESTINALE
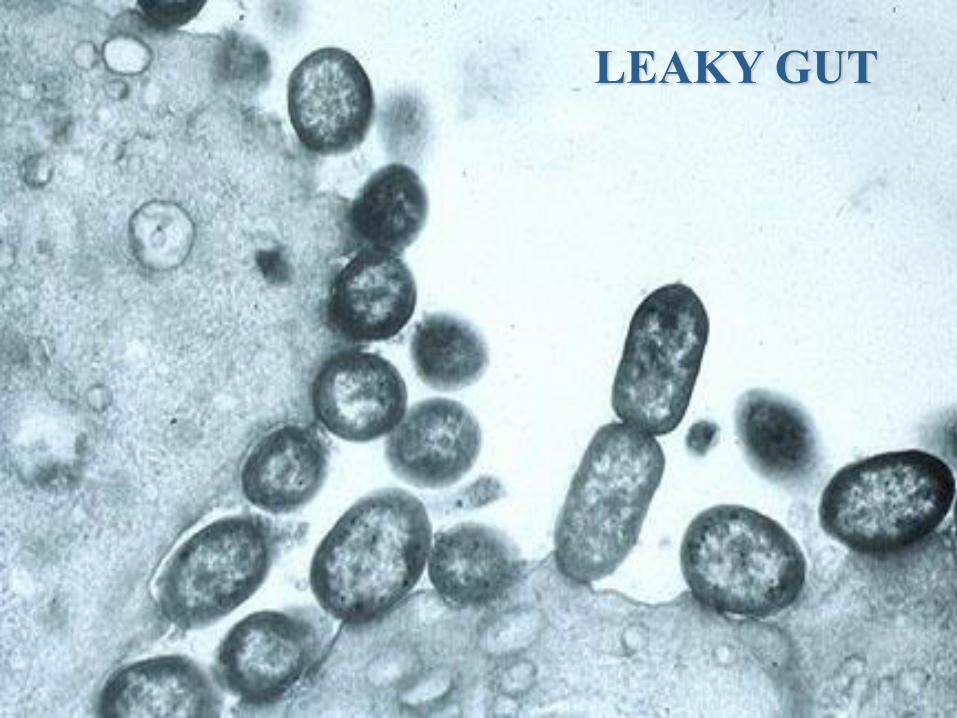
LEAKY GUT
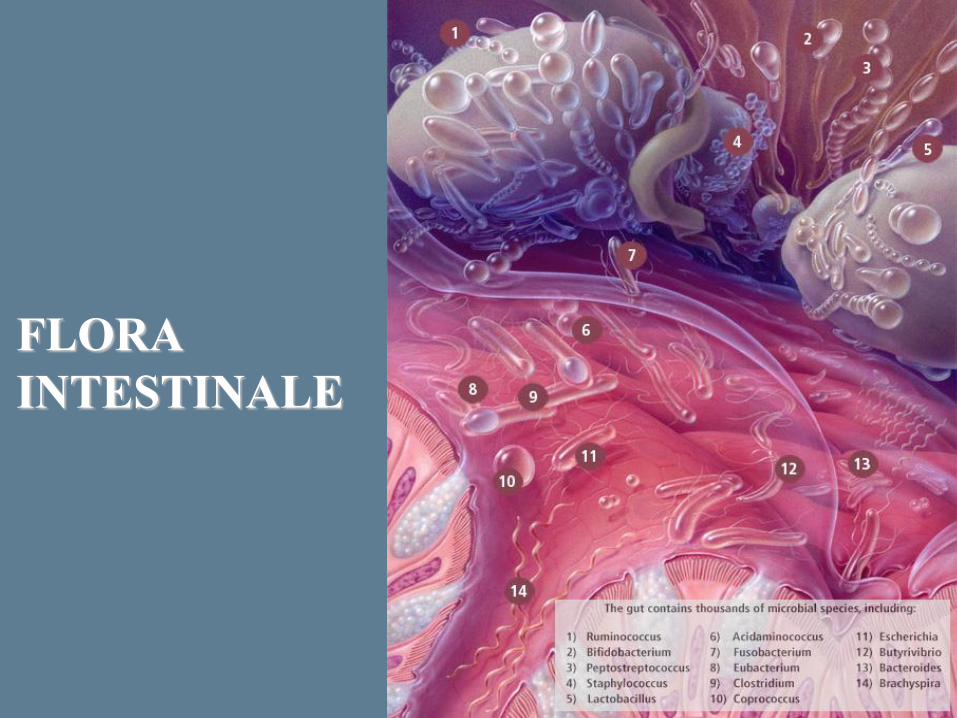
FLORA
INTESTINALE
SECONDA LINEA DI DIFESA
Il nemico è penetrato nel
nostro territorio!
SECONDA LINEA DI DIFESA
Cellule
Citochine/Chemochine
Fattori solubili
La Guerra
NOZIONE DI IMPORTANZA
FONDAMENTALE
I sistemi di difesa innati e
adattativi si sono sviluppati in
base al principio per cui solo i
veri nemici predatori sono in
grado di attraversare le barriere.
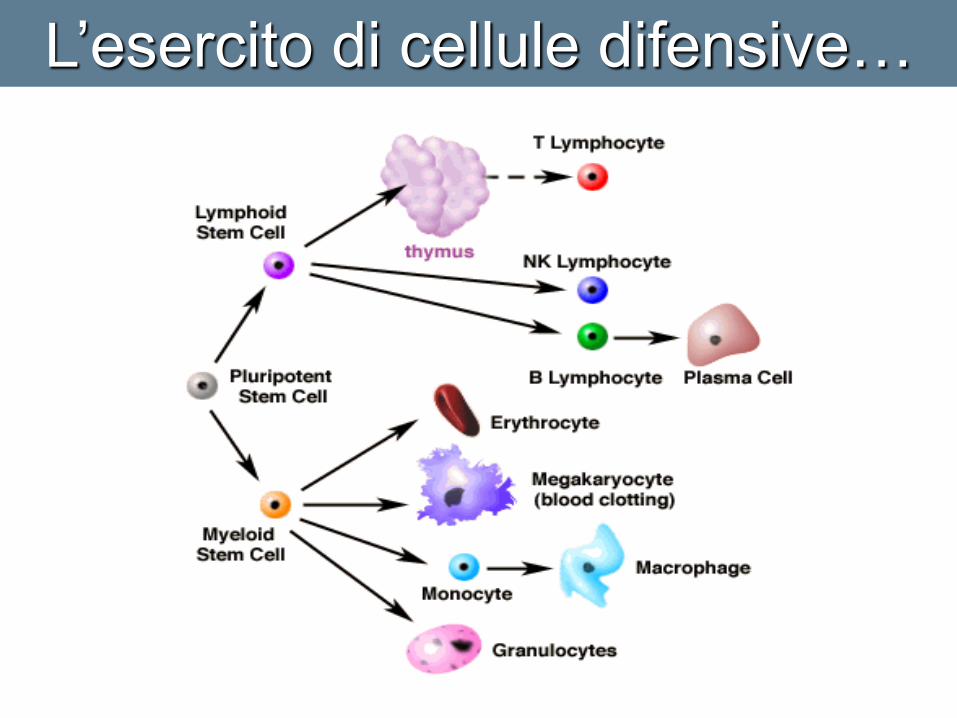
L’esercito di cellule difensive…
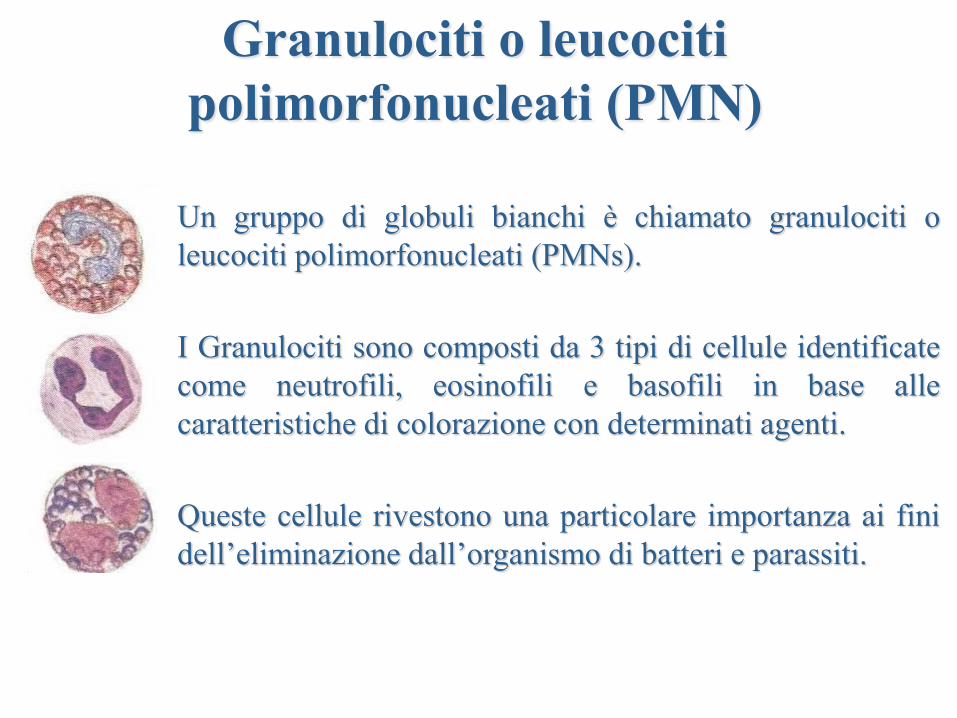
Un gruppo di globuli bianchi è chiamato granulociti o
leucociti polimorfonucleati (PMNs).
I Granulociti sono composti da 3 tipi di cellule identificate
come neutrofili, eosinofili e basofili in base alle
caratteristiche di colorazione con determinati agenti.
Queste cellule rivestono una particolare importanza ai fini
dell’eliminazione dall’organismo di batteri e parassiti.
Granulociti o leucociti
polimorfonucleati (PMN)
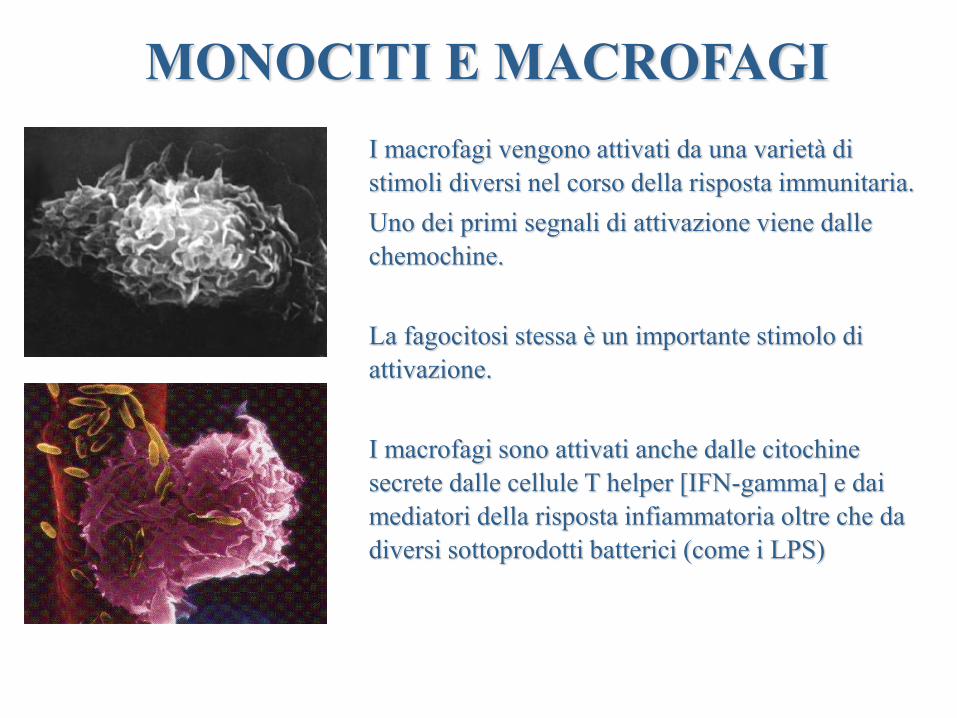
MONOCITI E MACROFAGI
I macrofagi vengono attivati da una varietà di
stimoli diversi nel corso della risposta immunitaria.
Uno dei primi segnali di attivazione viene dalle
chemochine.
La fagocitosi stessa è un importante stimolo di
attivazione.
I macrofagi sono attivati anche dalle citochine
secrete dalle cellule T helper [IFN-gamma] e dai
mediatori della risposta infiammatoria oltre che da
diversi sottoprodotti batterici (come i LPS)
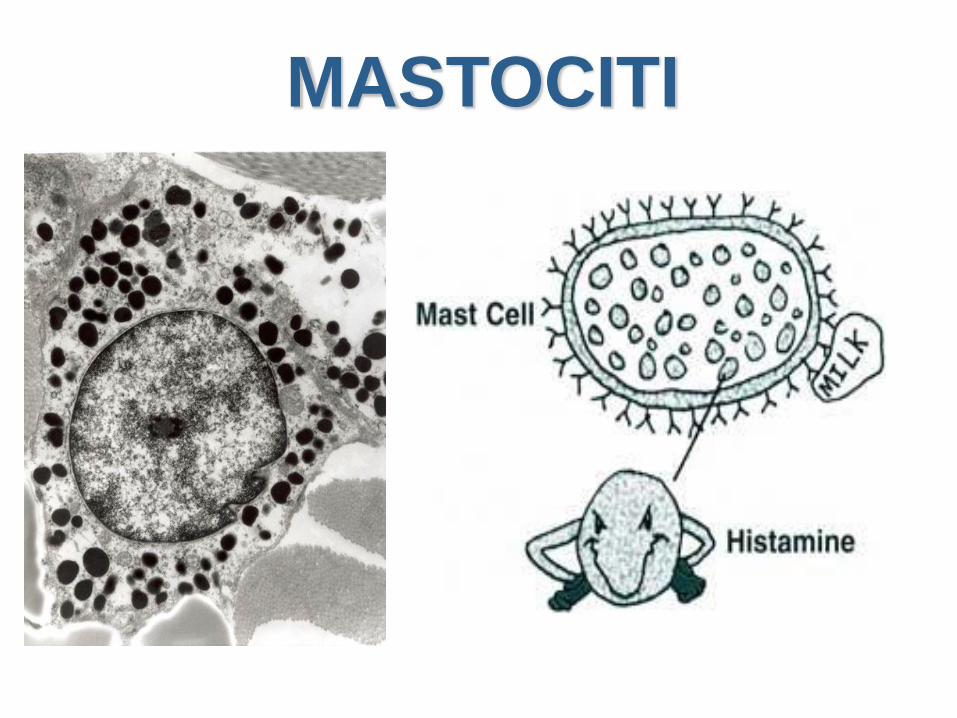
MASTOCITI
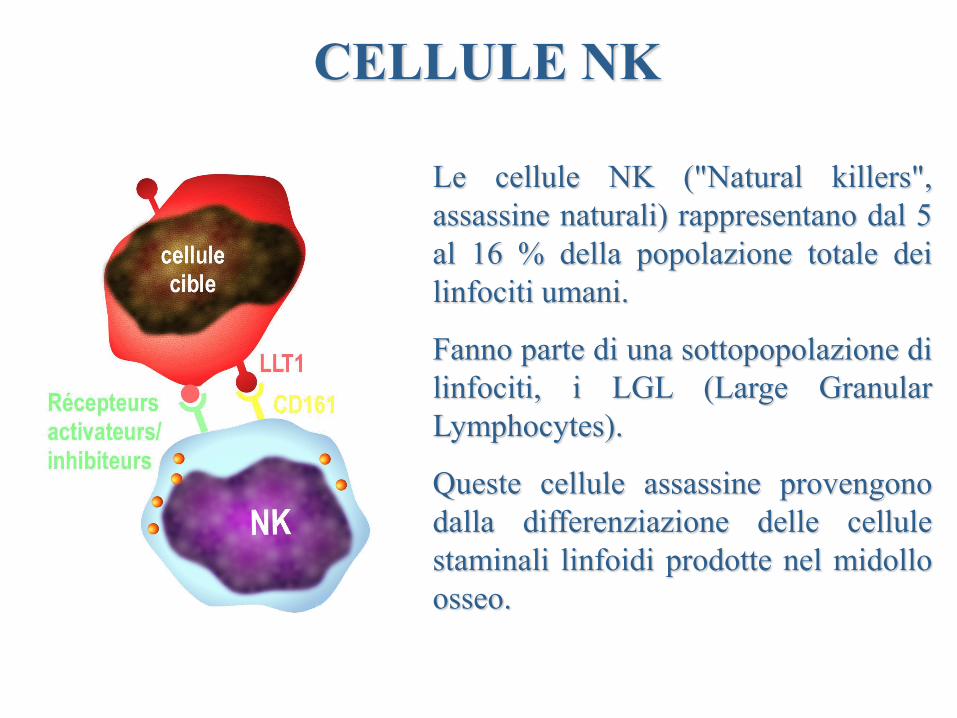
CELLULE NK
Le cellule NK ("Natural killers",
assassine naturali) rappresentano dal 5
al 16 % della popolazione totale dei
linfociti umani.
Fanno parte di una sottopopolazione di
linfociti, i LGL (Large Granular
Lymphocytes).
Queste cellule assassine provengono
dalla differenziazione delle cellule
staminali linfoidi prodotte nel midollo
osseo.

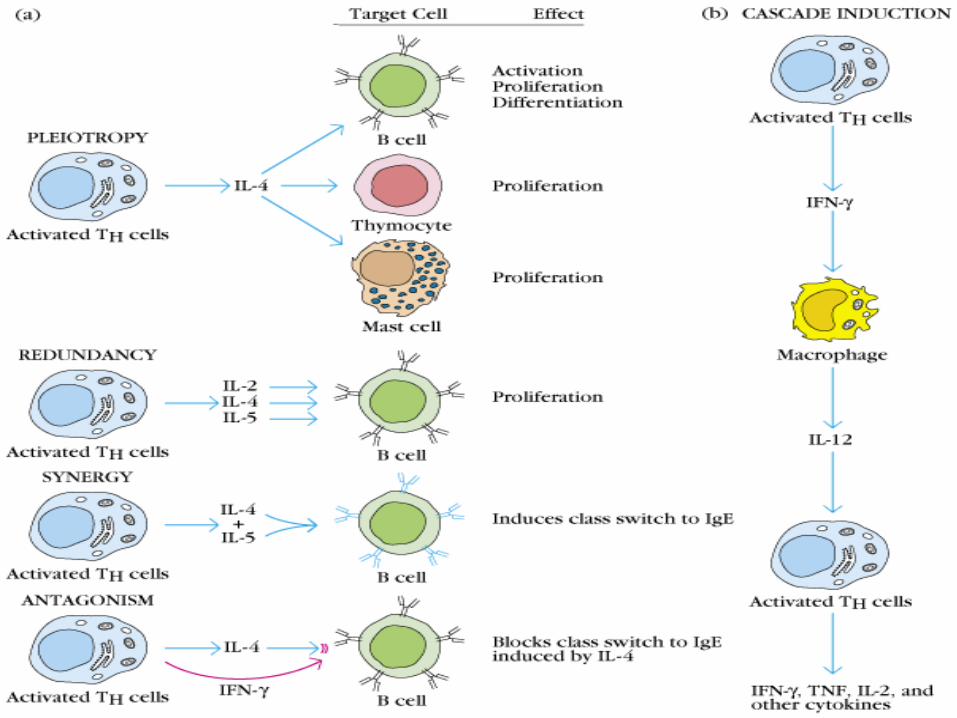
Citochine
Agenti di comunicazione
intercellulare
Immunità innata
Immunità innata (naturale, aspecifica)
La risposta all’invasione ha bisogno di 3
elementi:
Riconoscimento
Eliminazione
Comunicazione
Riconoscimento dei
microrganismi da parte del
sistema immunitario innato
Immunità innata
Cellule dendritiche
Macrofagi
Polinucleati
Enterociti
Immunità innata
DC
MF
PN
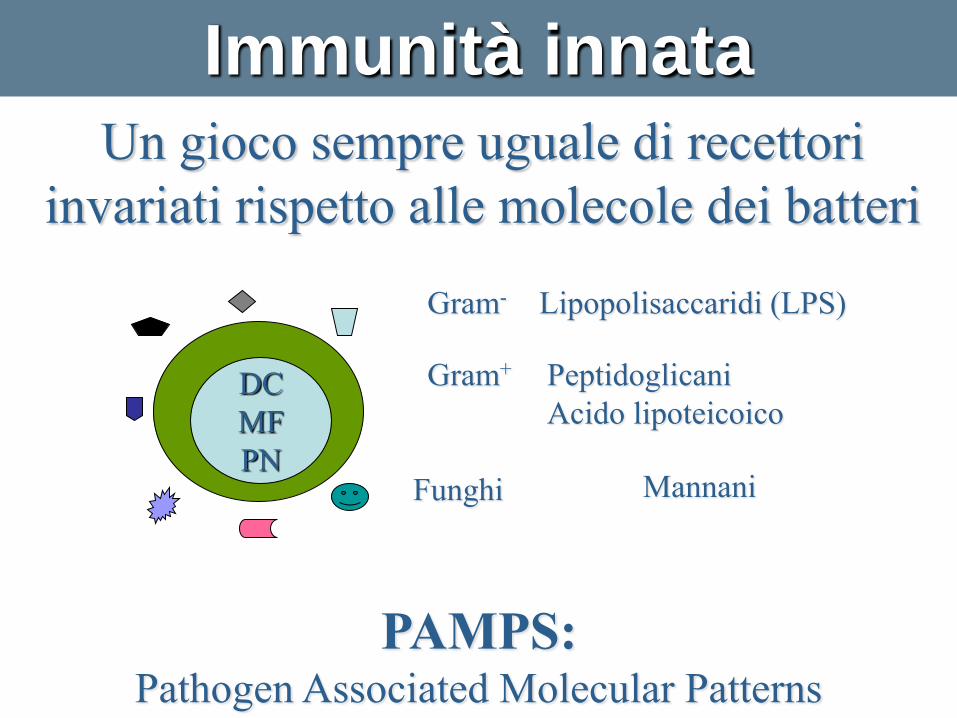
Un gioco sempre uguale di recettori
invariati rispetto alle molecole dei batteri
Gram-
Lipopolisaccaridi (LPS)
Gram+
Peptidoglicani
Acido lipoteicoico
Funghi
Mannani
Immunità innata
PAMPS: Pathogen Associated Molecular Patterns
Percezione intrinseca di ciò che è
batterico, vale a dire ciò che è
ostile…
Immunità innata
La tolleranza intrinseca al self
dell’immunità naturale è stata acquisita
dopo centinaia di milioni di anni di
evoluzione in seguito ai quali si sono
selezionati dei recettori capaci di
distinguere i sottoprodotti batterici e non
dai sottoprodotti del self…
Immunità innata

Limiti
Repertorio antibatterico limitato
Nessun adattamento alle mutazioni batteriche
Nessuna percezione dei batteri intracellulari
Immunità innata
Immunità innata
I PAMPS sono riconosciuti da recettori sulla superficie delle
cellule del sistema immunitario innato, i PRMs e PRRs(
Pattern-Recognition molecole/recettori)
Recettori di endocitosi
Recettori del mannosio dei macrofagi
Proteine di secrezione
CRP
Recettore di segnalizzazione
La famiglia dei recettori TOLL (TLR)
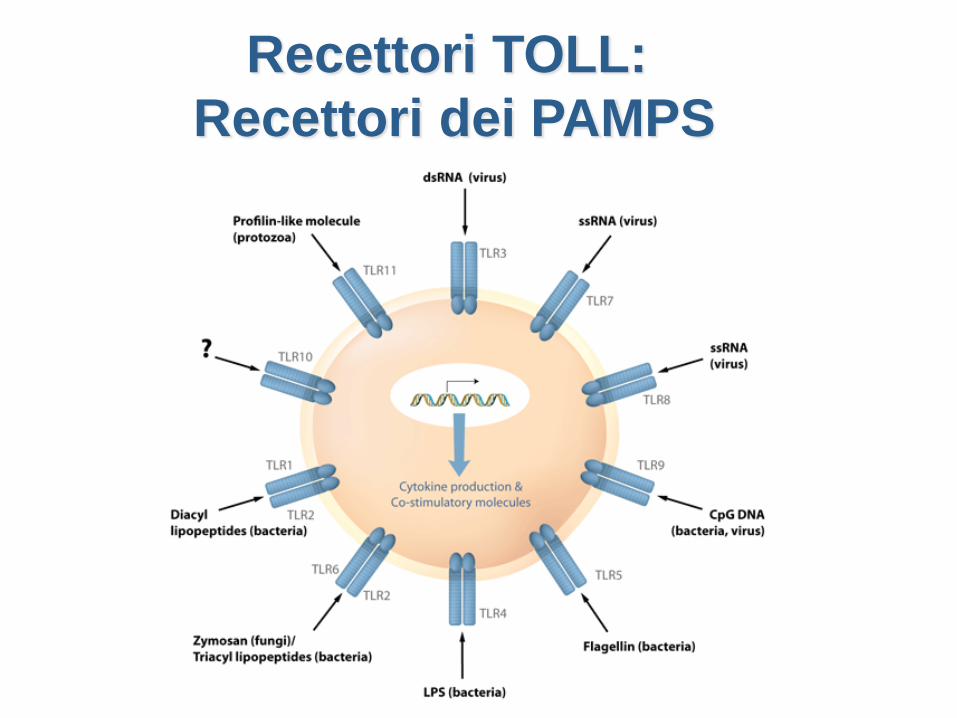
Recettori TOLL:
Recettori dei PAMPS
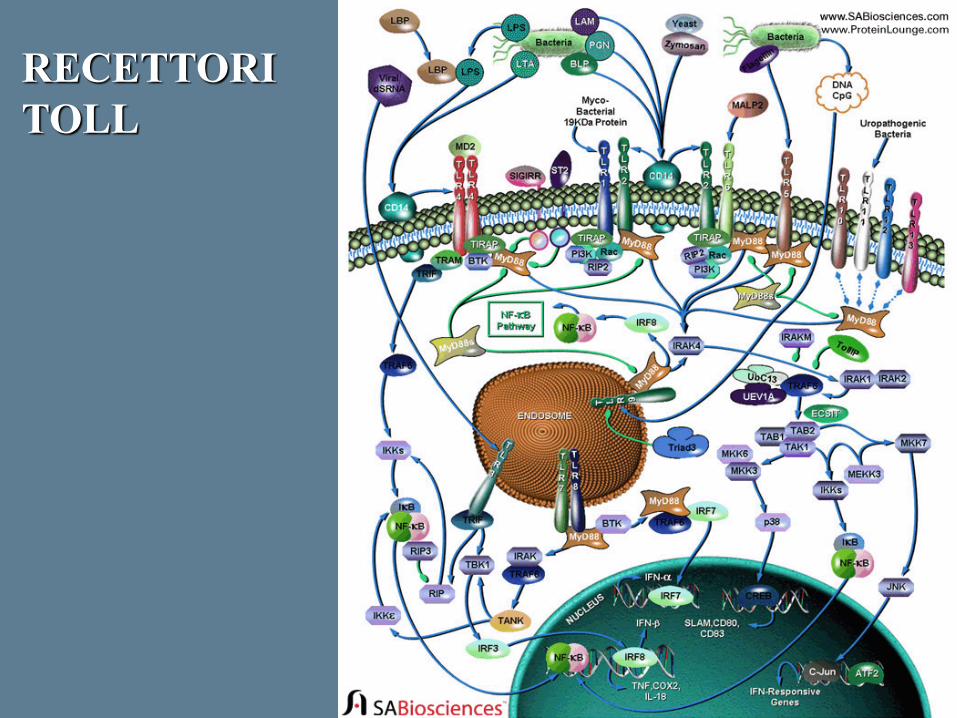
RECETTORI
TOLL

Ricezione del segnale

Chinasi Agenti di comunicazione intracellulare
Enzimi che traducono l’informazione
proveniente dall’esterno per coordinare una
risposta cellulare appropriata.
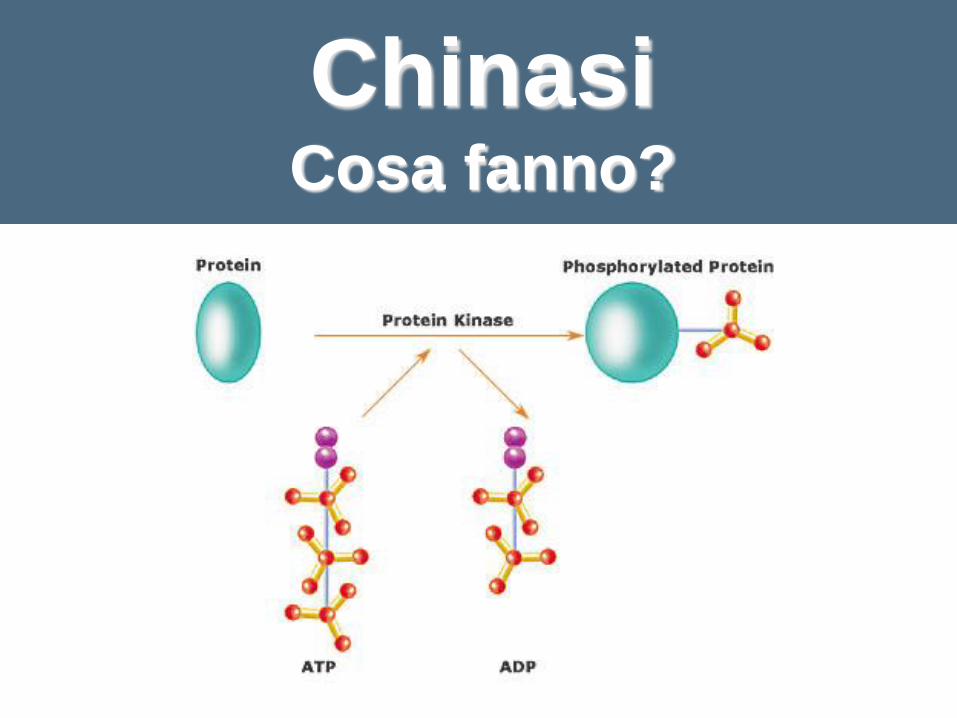
Chinasi Cosa fanno?

Fattore trascrizionale
Capo controllo
dell’immunità e
dell’infiammazione
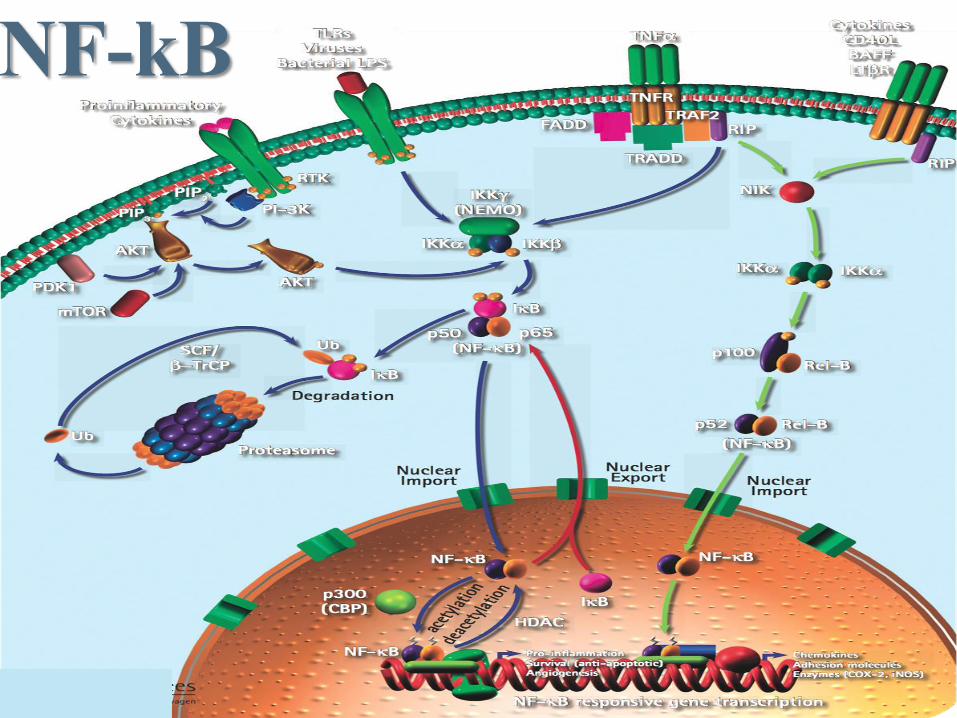
NF-kB
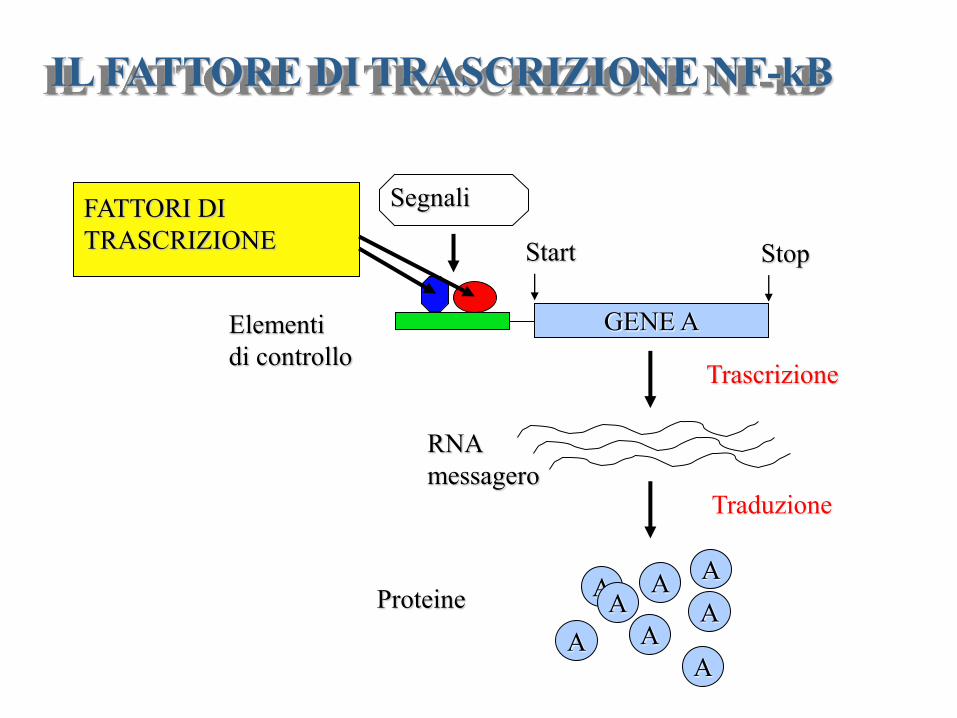
GENE A
Start Stop
Elementi
di controllo
Segnali
A A
A A
A A
A
A
RNA
messagero
Proteine
IL FATTORE DI TRASCRIZIONE NF-kB
Trascrizione
Traduzione
FATTORI DI
TRASCRIZIONE

NF-kB Il maestro della guerra
I-kB Il maestro della pace
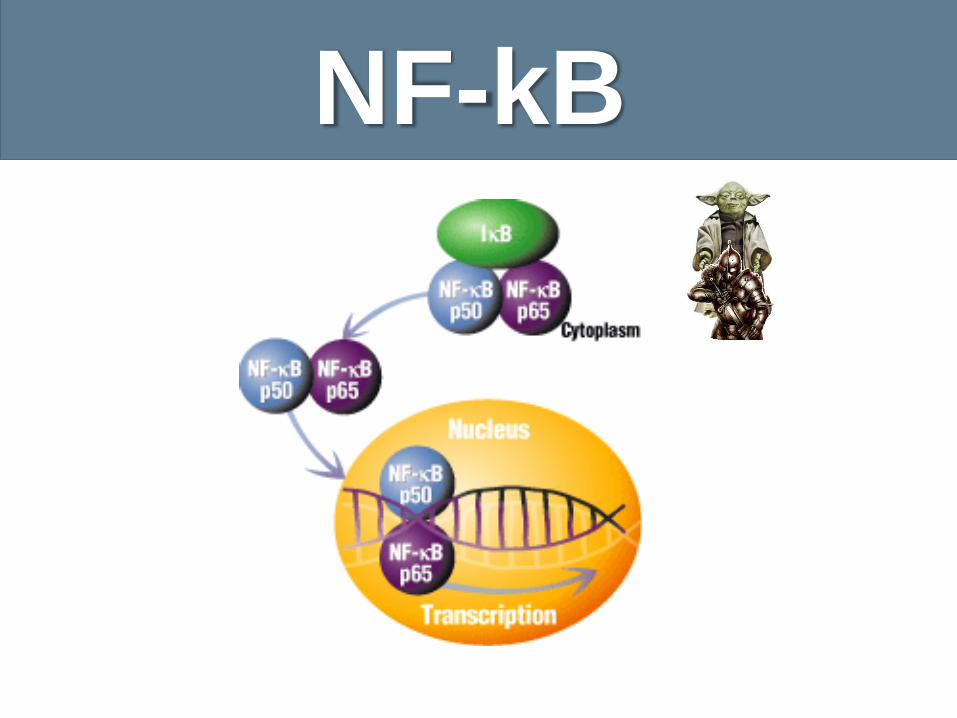
NF-kB
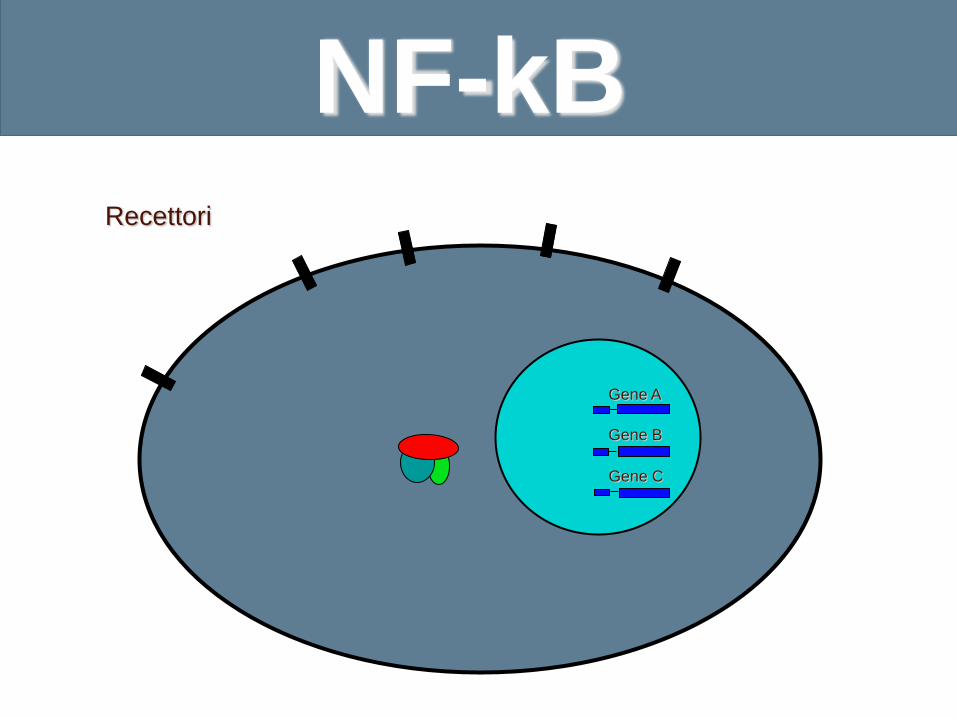
Recettori
Gene A
Gene B
Gene C
NF-kB
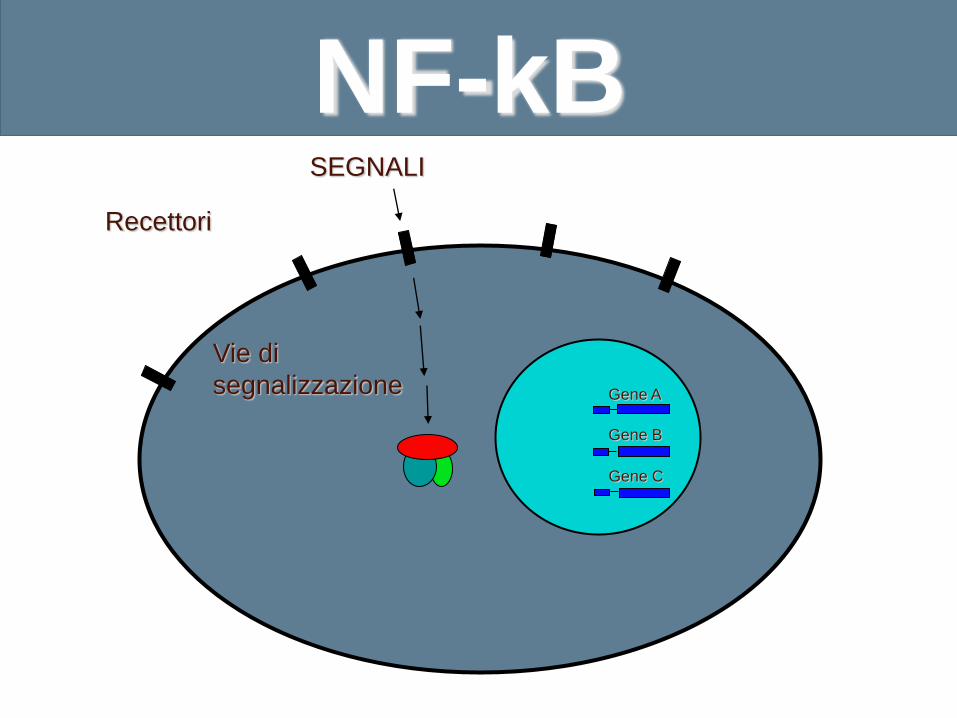
SEGNALI
Recettori
Vie di
segnalizzazione Gene A
Gene B
Gene C
NF-kB NF-kB
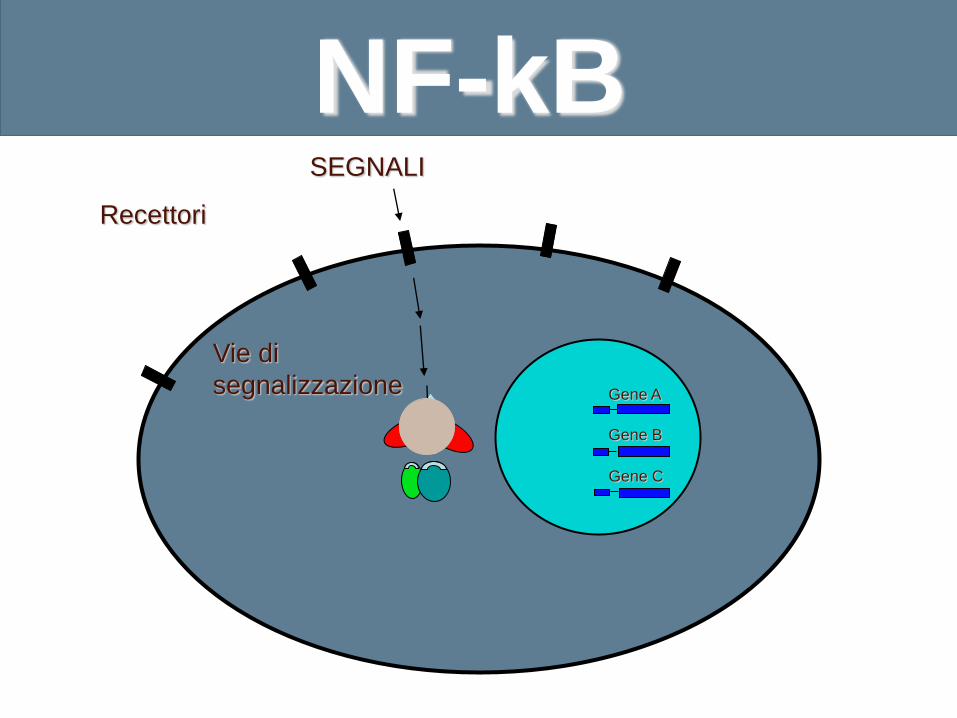
SEGNALI
Recettori
Gene A
Gene B
Gene C
Vie di
segnalizzazione
NF-kB
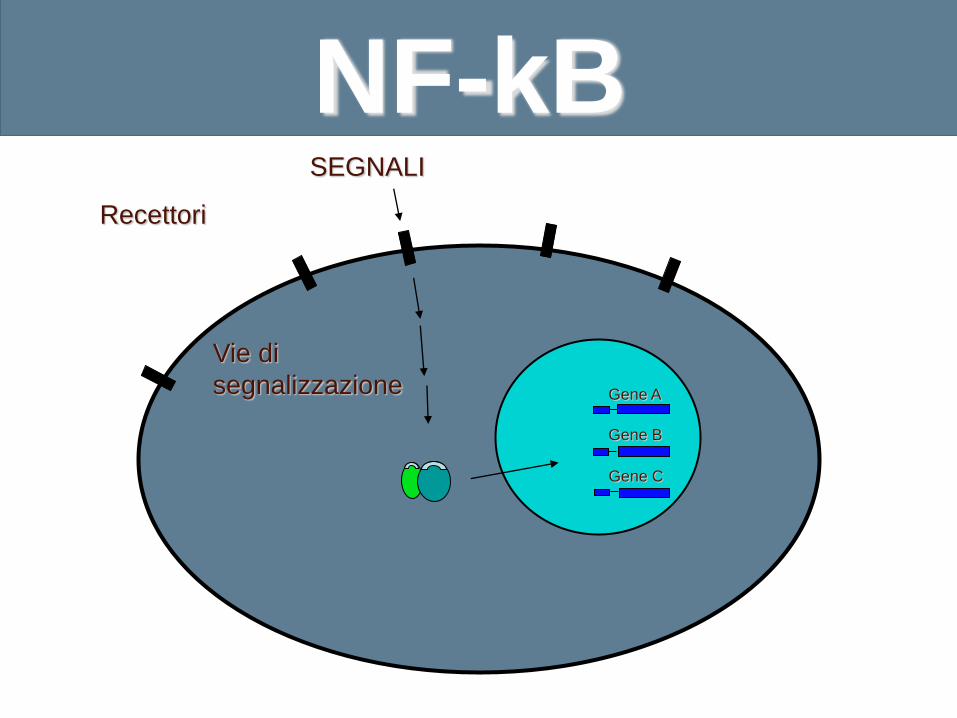
SEGNALI
Recettori
Gene A
Gene B
Gene C
Vie di
segnalizzazione
NF-kB
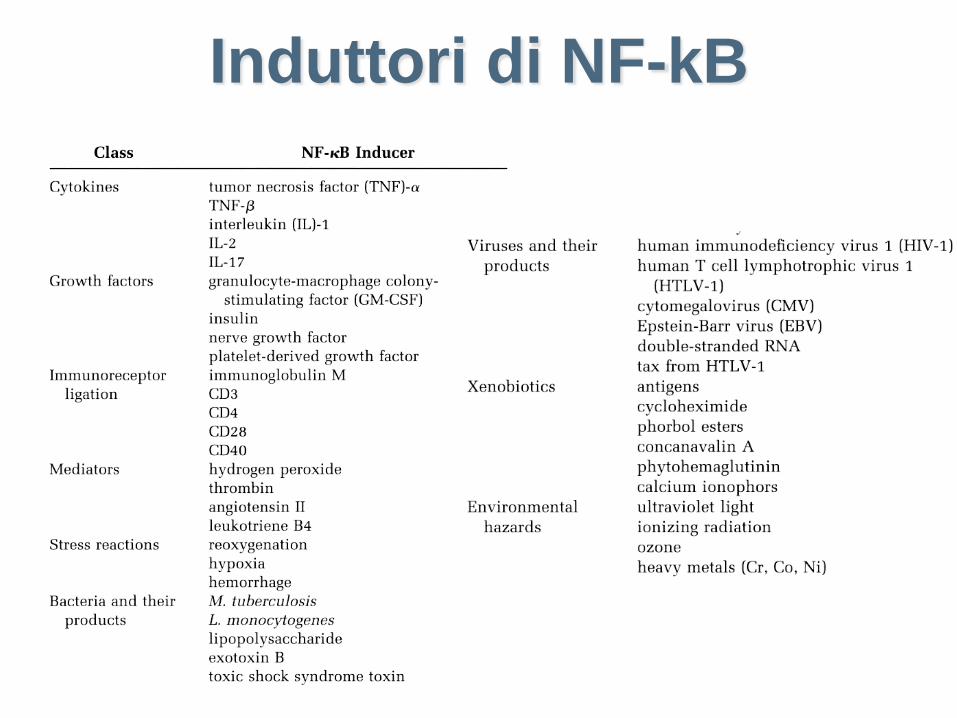
Induttori di NF-kB
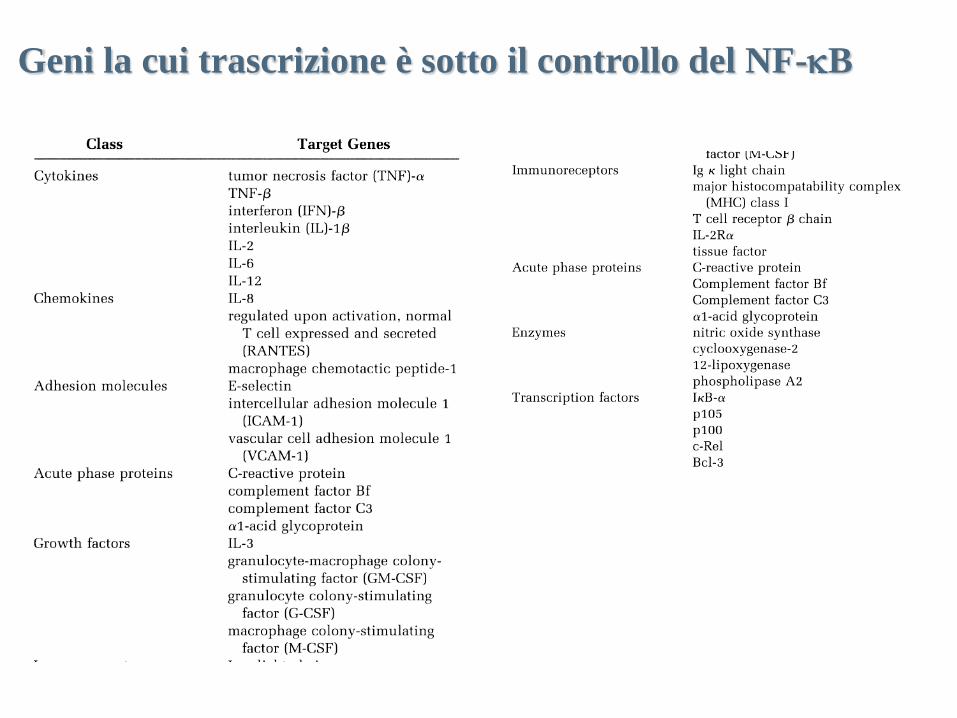
Geni la cui trascrizione è sotto il controllo del NF-kB
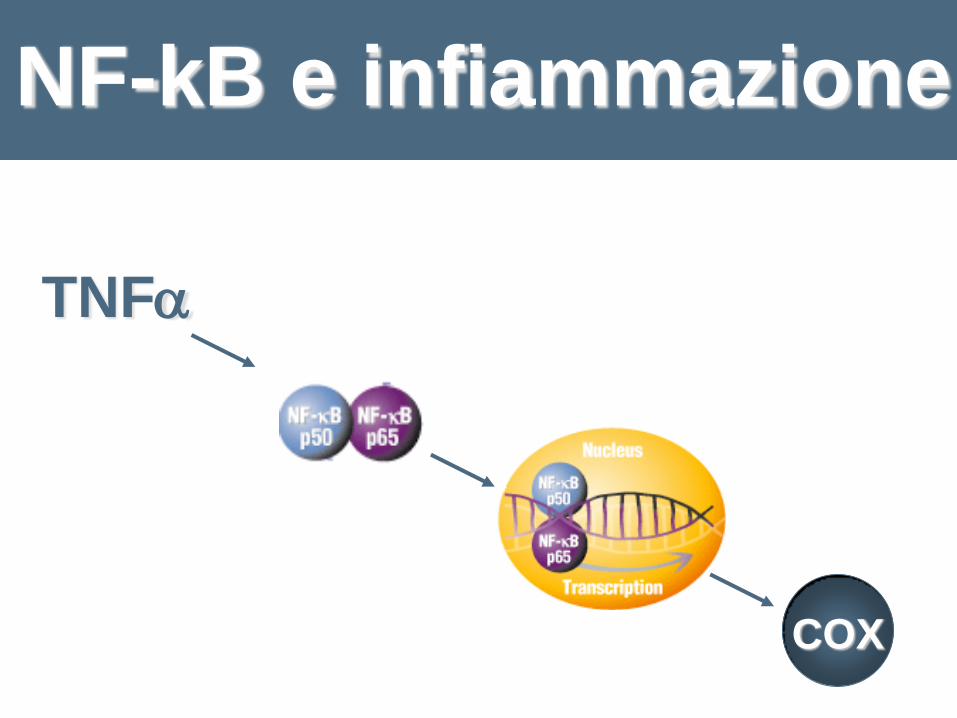
NF-kB e infiammazione
COX
TNF

IKK Chinasi che controlla l’infiammazione
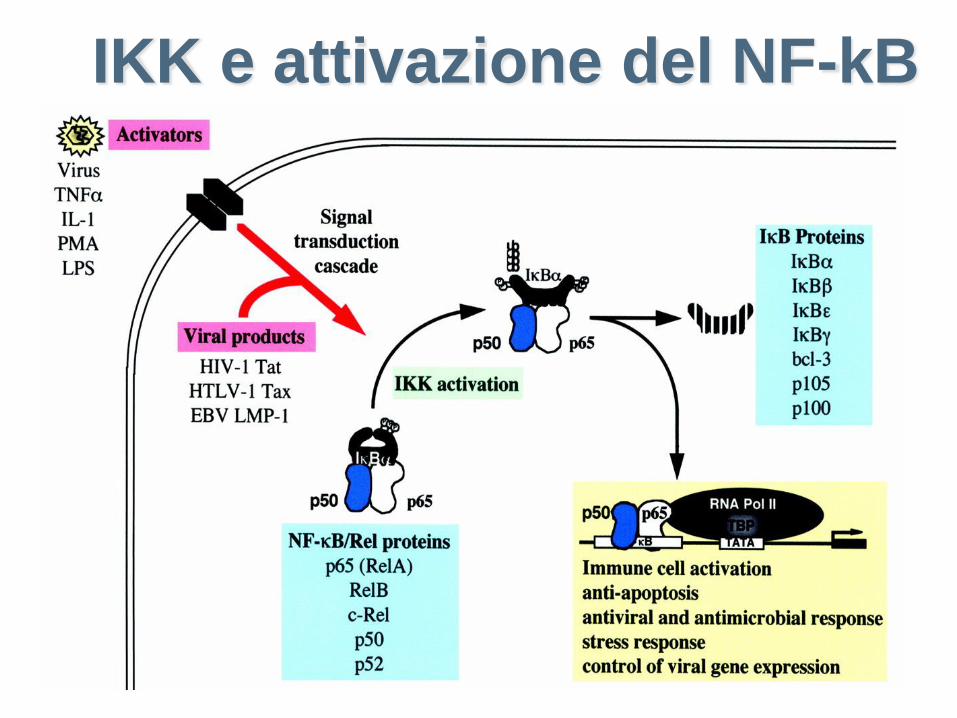
IKK e attivazione del NF-kB
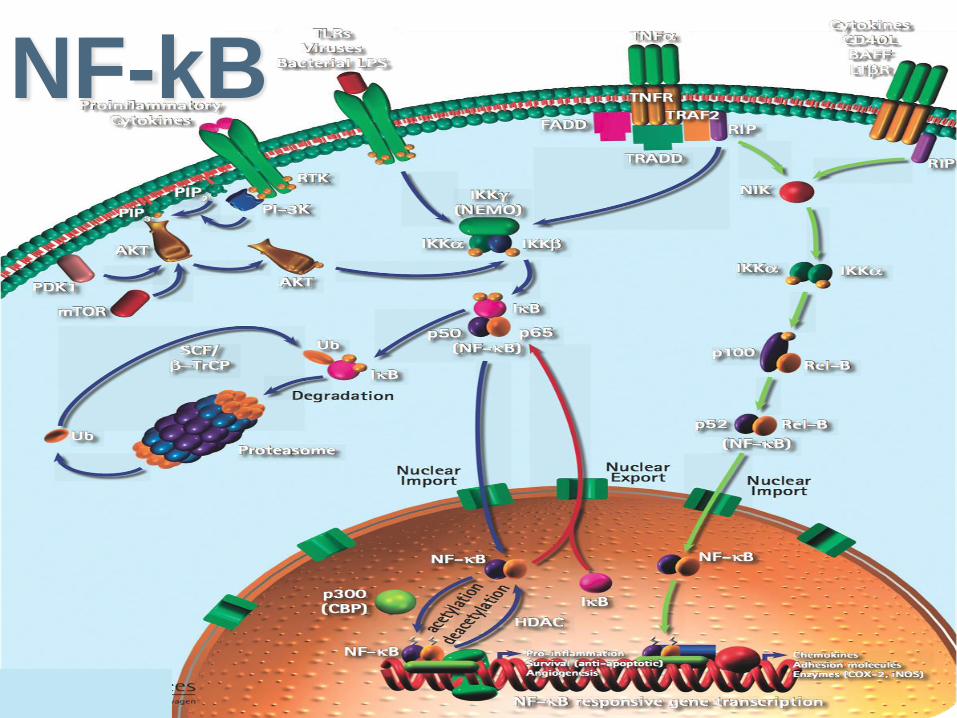
NF-kB
- Risposta immunitaria
- Infiammazioni
- Sopravvivenza allo stress (ossidoriduzioni, ionizzazioni,…)
- Traumi neurologici, morbo di Alzheimer,
morbo di Parkinson, tumori, artrite reumatoide.
NF-kB: Ruoli biologici
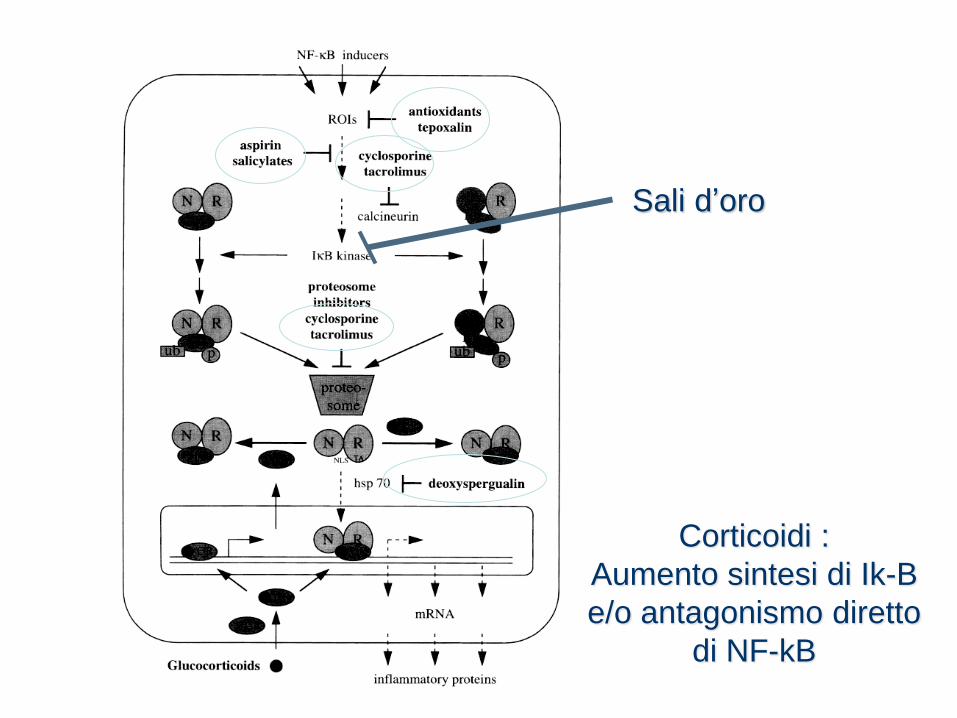
Sali d’oro
Corticoidi :
Aumento sintesi di Ik-B
e/o antagonismo diretto
di NF-kB
Le armi del nostro
sistema di difesa

Difese aspecifiche
I fattori solubili
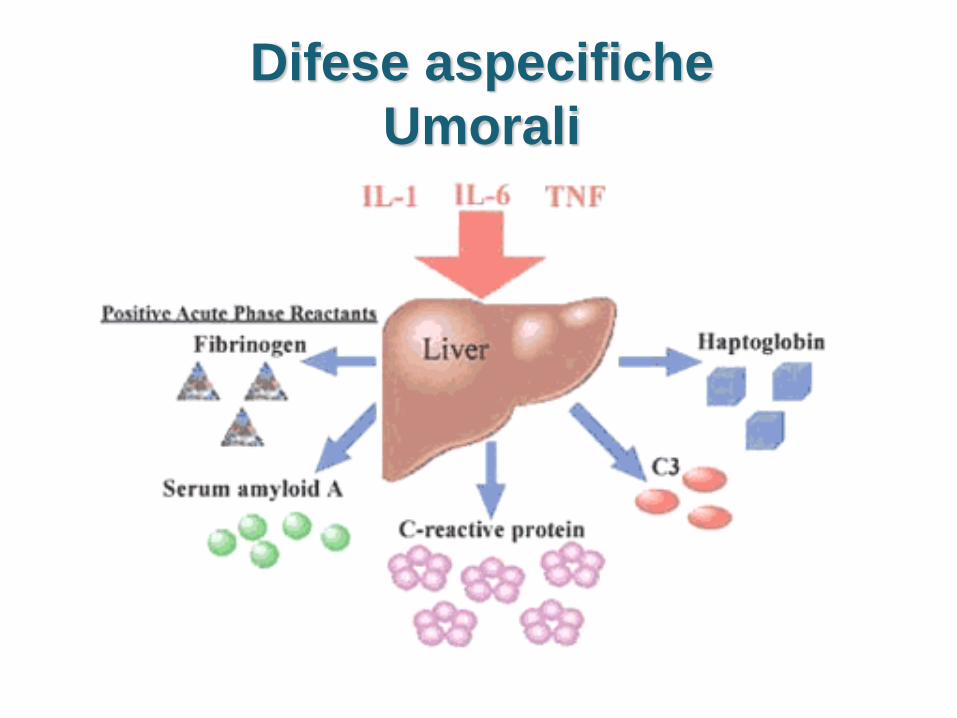
Difese aspecifiche
Umorali
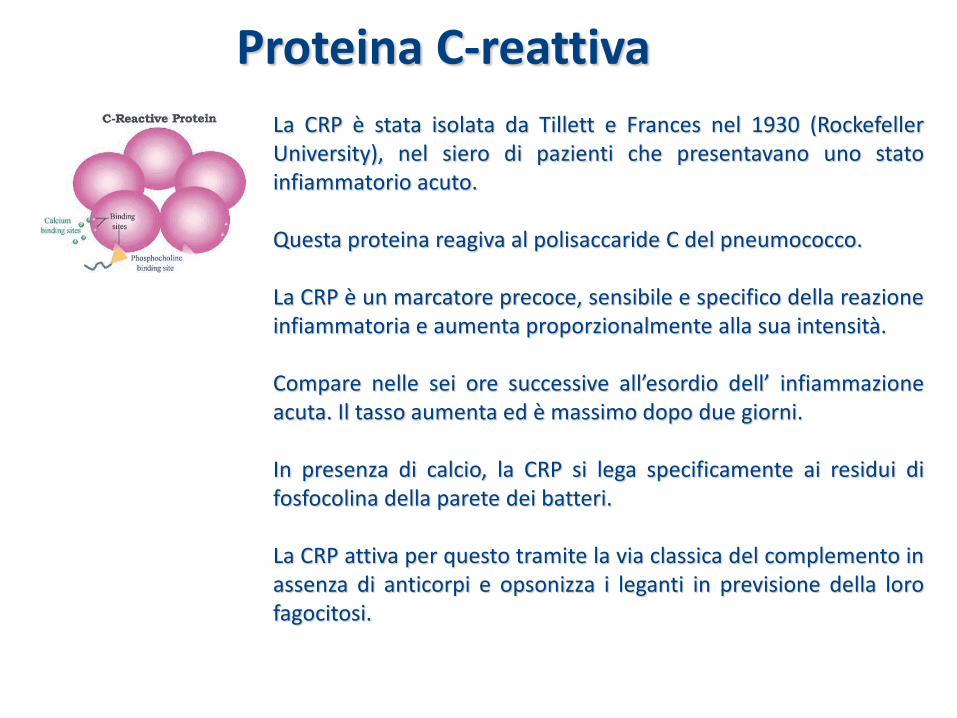
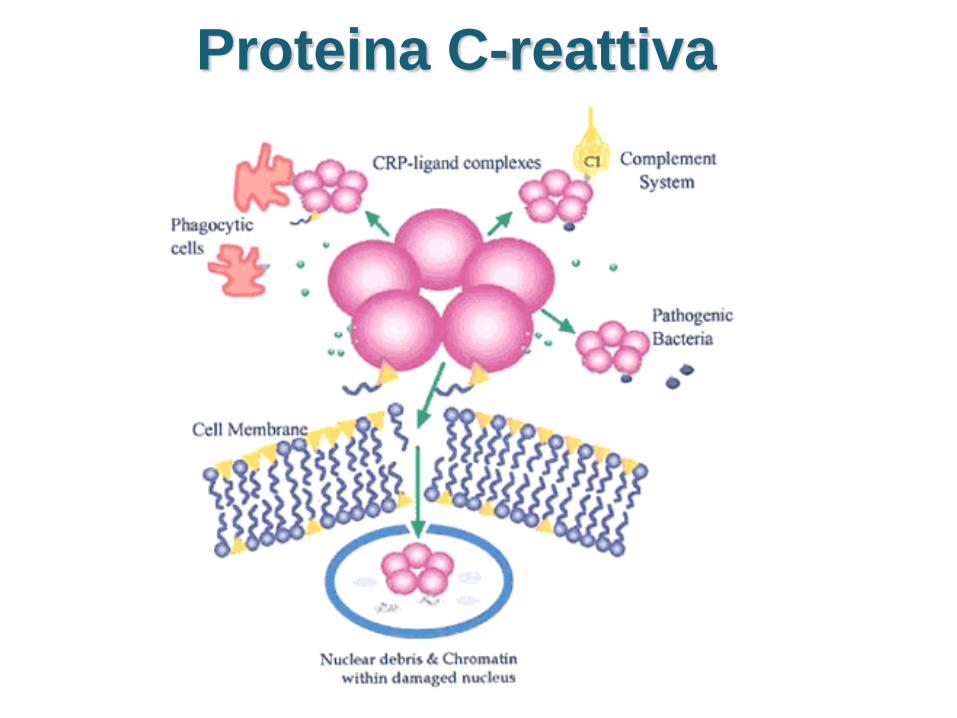
La CRP è stata isolata da Tillett e Frances nel 1930 (Rockefeller University), nel siero di pazienti che presentavano uno stato infiammatorio acuto. Questa proteina reagiva al polisaccaride C del pneumococco. La CRP è un marcatore precoce, sensibile e specifico della reazione infiammatoria e aumenta proporzionalmente alla sua intensità. Compare nelle sei ore successive all’esordio dell’ infiammazione acuta. Il tasso aumenta ed è massimo dopo due giorni. In presenza di calcio, la CRP si lega specificamente ai residui di fosfocolina della parete dei batteri. La CRP attiva per questo tramite la via classica del complemento in assenza di anticorpi e opsonizza i leganti in previsione della loro fagocitosi.
Proteina C-reattiva
Proteina C-reattiva

Difesa aspecifica
La febbre
IL COMPLEMENTO
Il complemento

La fagocitosi
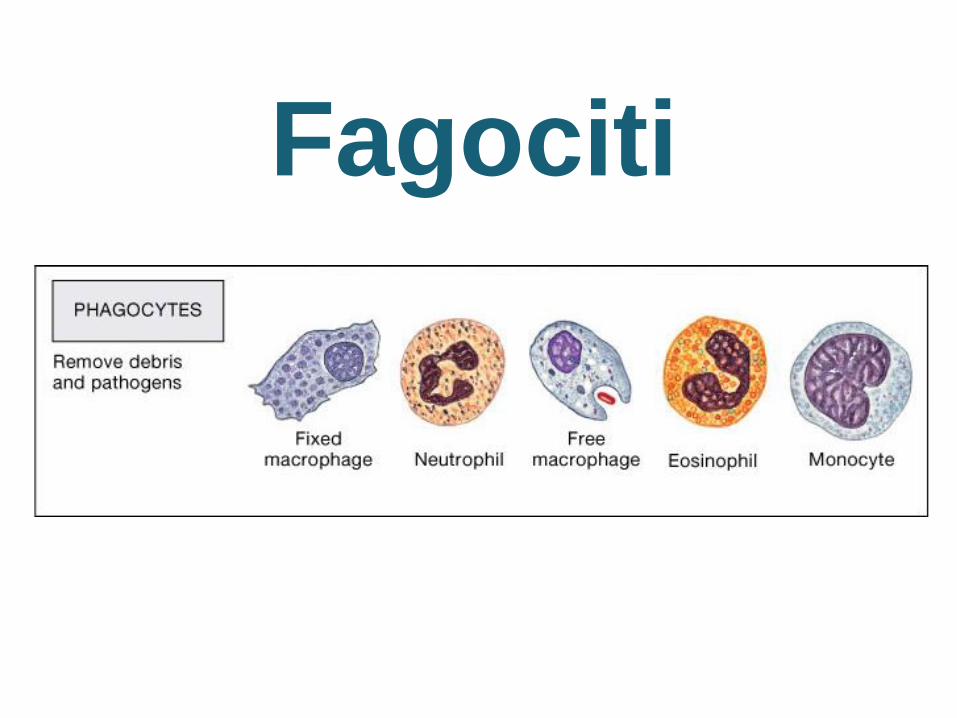
Fagociti
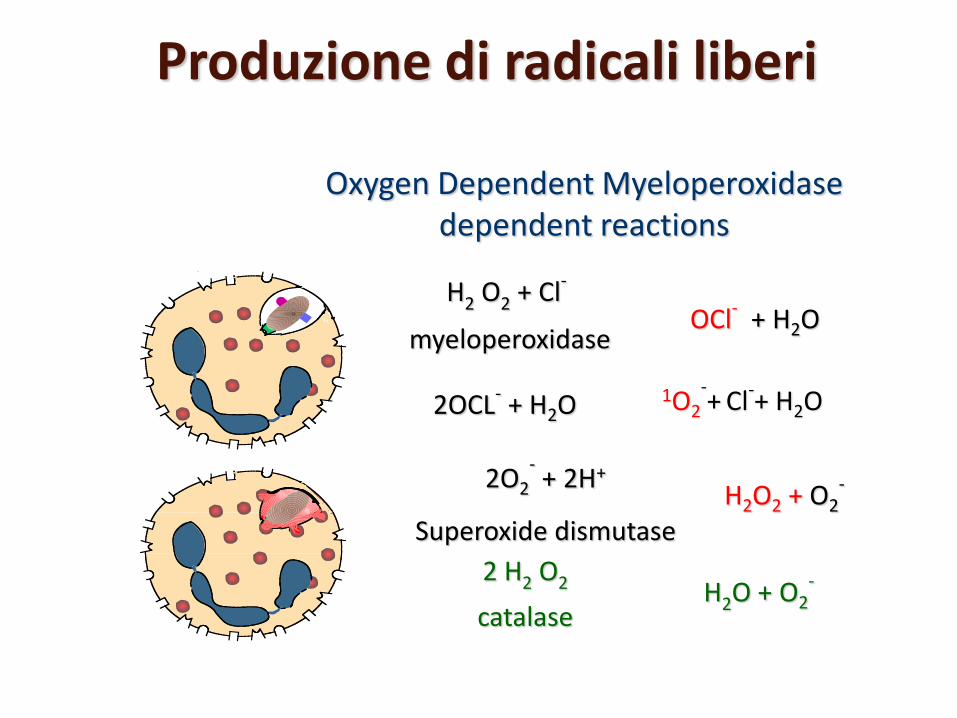
Oxygen Dependent Myeloperoxidase dependent reactions
H2O2 + O2- 2O2
- + 2H+
Superoxide dismutase
H2 O2 + Cl-
myeloperoxidase OCl
- + H2O
H2O + O2- 2 H2 O2
catalase
2OCL- + H2O 1O2
-+ Cl
-+ H2O
Produzione di radicali liberi
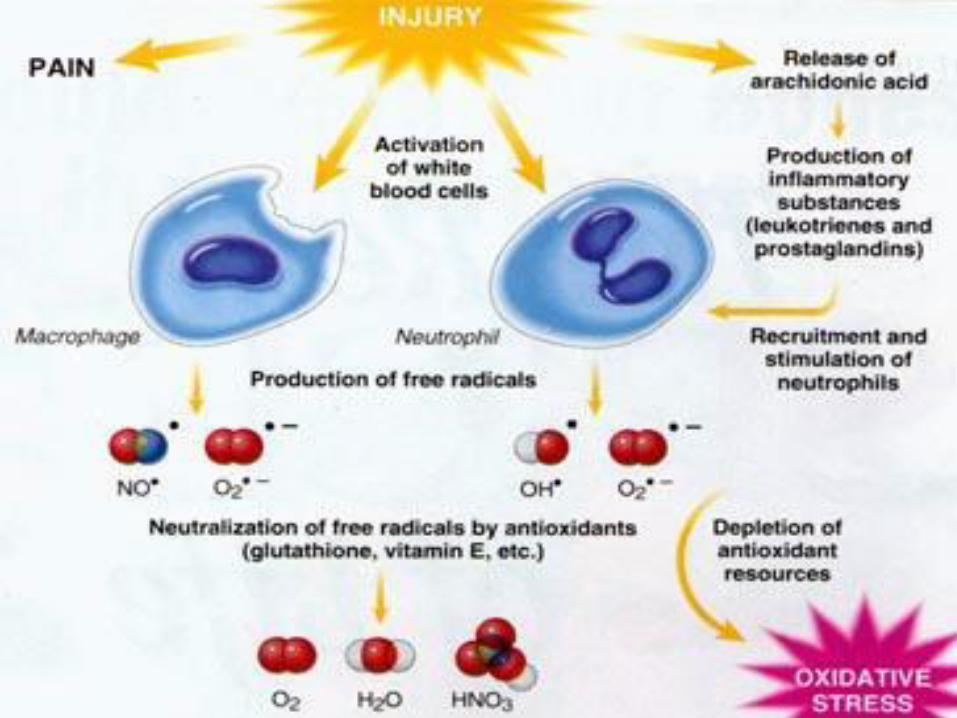
La reazione infiammatoria è un processo
fisiologico indispensabile alla sopravvivenza
del nostro organismo continuamente
esposto all’aggressione di organismi
batterici, agenti fisici e chimici …
L’infiammazione è il campo di
battaglia in cui le nostre difese
specifiche e aspecifiche
combattono il nemico.
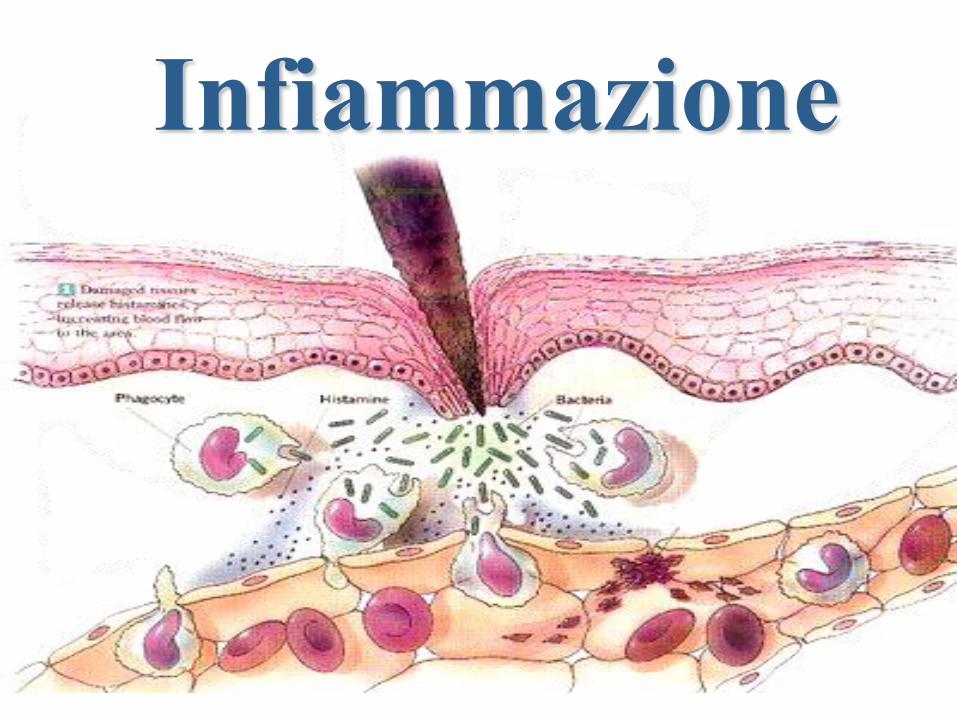
Infiammazione

DIFESA
INFIAMMAZIONE
LIVELLO I Le Barriere
LIVELLO II Immunità
innata
LIVELLO III Immunità specifica
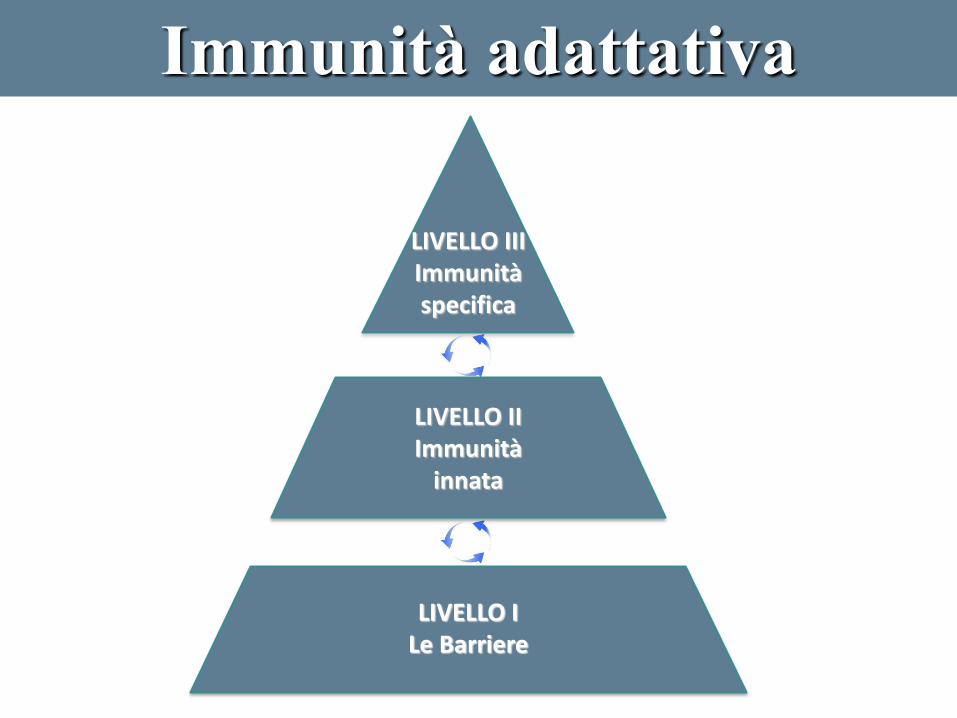
Immunità adattativa
Immunità
adattativa
• Là dove ha luogo la maggior parte
dell’azione evolutiva
• Dipende dal contatto tra le cellule ospiti e
gli antigeni (anticorps generation)
• Due categorie principali di risposte :
immunità umorale e immunità cellulare
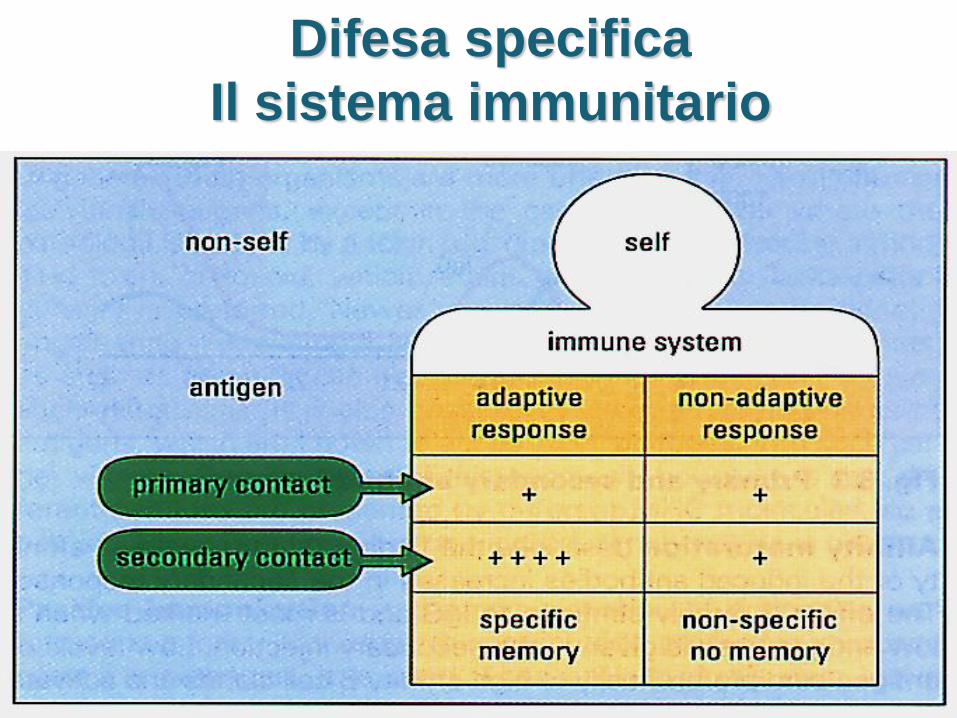
Difesa specifica
Il sistema immunitario
Il sistema immunitario
INNATO
ADATTATIVO
Immunità adattativa
L’immunità adattativa
ricorre alle stesse armi
dell’immunità innata
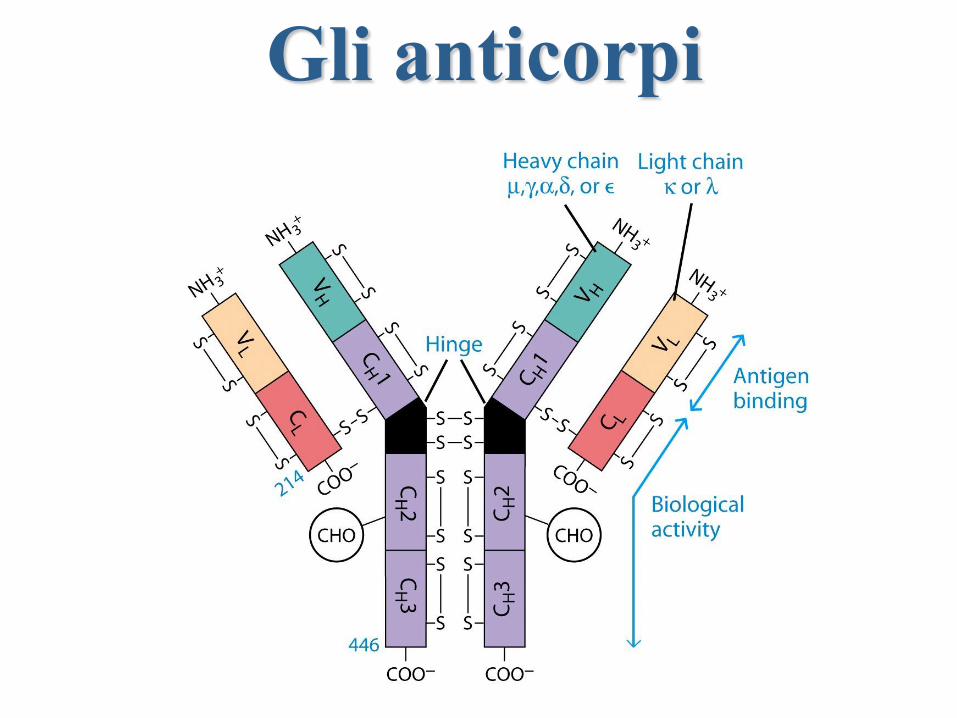
Gli anticorpi

Antigeni
Antigene : Molecola estranea che provoca una reazione
immunitaria
Virus dell’influenza
Proteina di superficie
RICONOSCIUTA dai
linfociti
ANTIGENE > reazione immunitaria
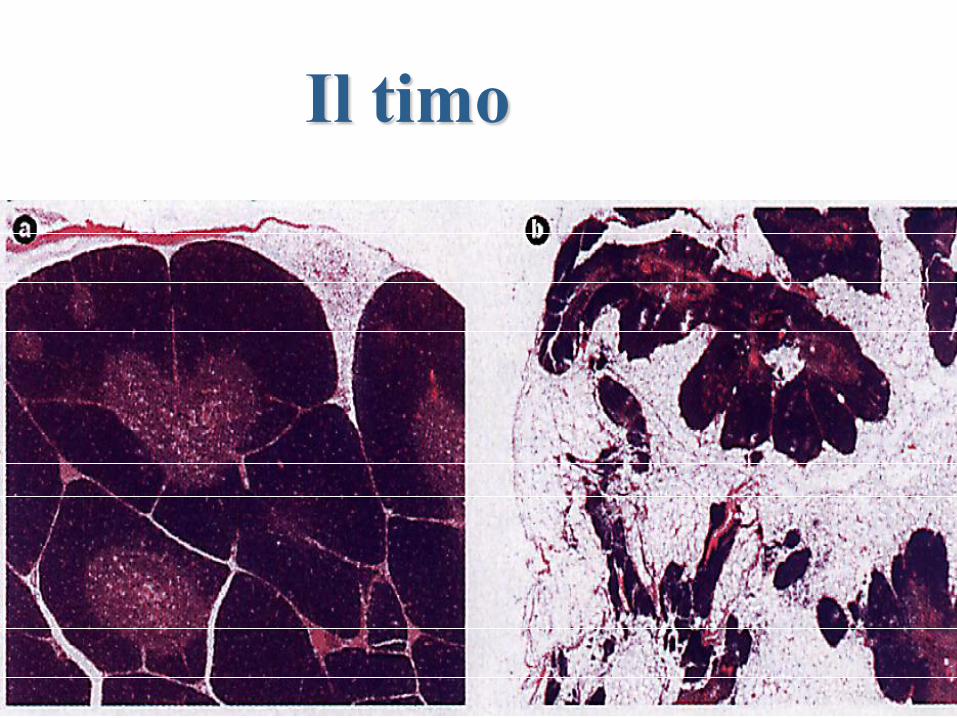
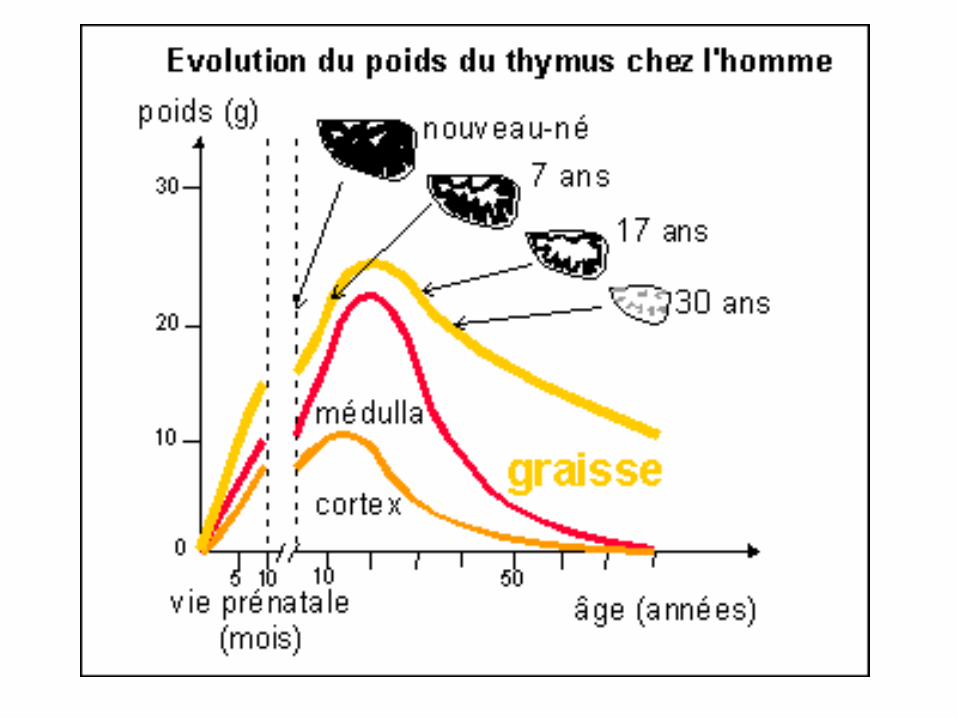
Il timo
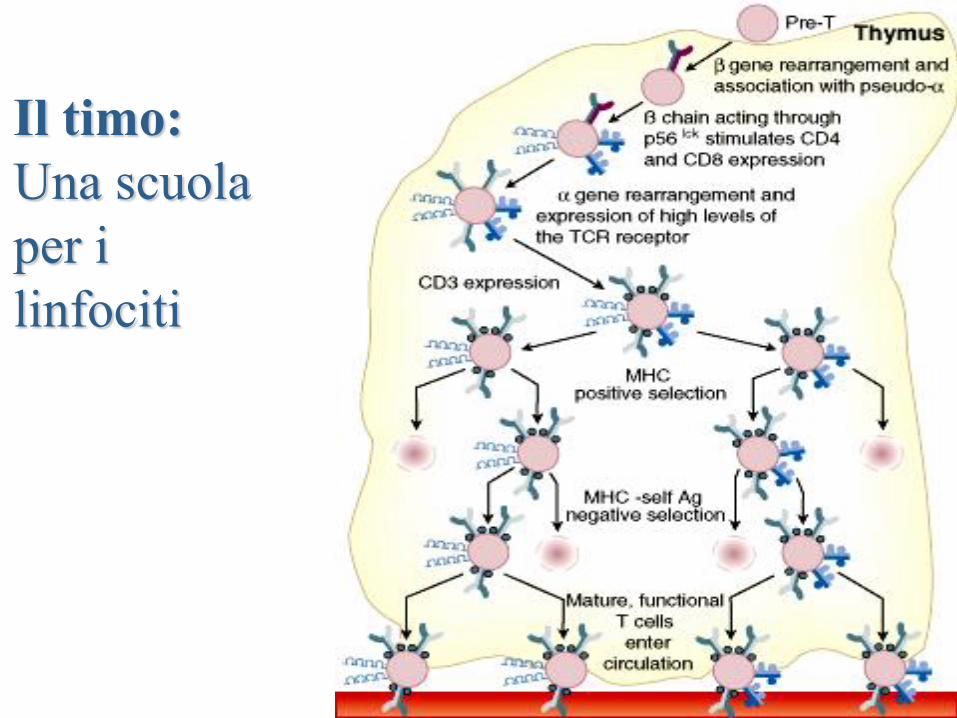
Il timo:
Una scuola
per i
linfociti
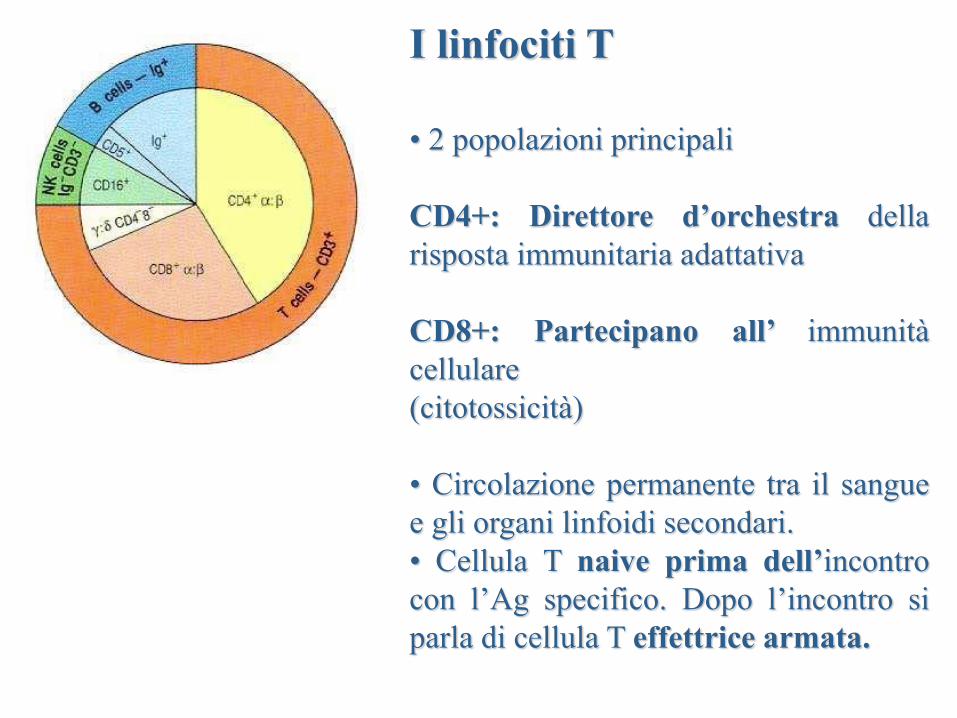
I linfociti T
• 2 popolazioni principali
CD4+: Direttore d’orchestra della
risposta immunitaria adattativa
CD8+: Partecipano all’ immunità
cellulare
(citotossicità)
• Circolazione permanente tra il sangue
e gli organi linfoidi secondari.
• Cellula T naive prima dell’incontro
con l’Ag specifico. Dopo l’incontro si
parla di cellula T effettrice armata.
• I LT naive circolano in permanenza tra gli organi linfatici
secondari all’incontro con l’Ag specifico
• LT CD4+ sono programmati per diventare cellule secretrici di
citochine e cellule memoria
• LT CD8+ sono programmati per diventare delle cellule
effettrici citotossiche (CTL CD8+) e delle cellule memoria
I linfociti T
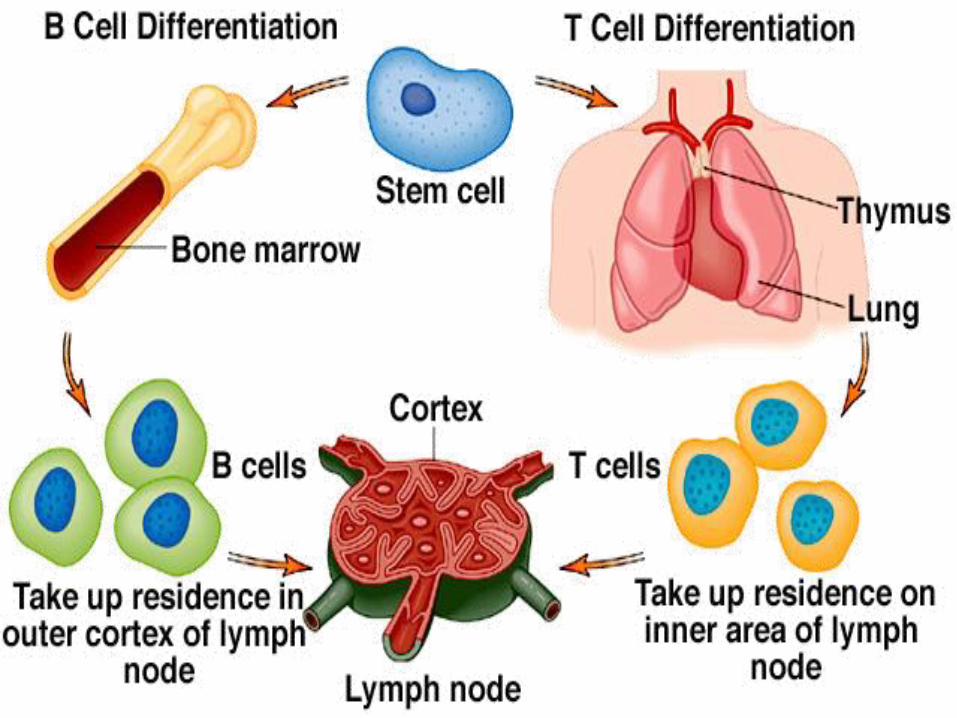
I linfociti B completano la maturazione
diventando competenti nel midollo osseo
Linfociti B
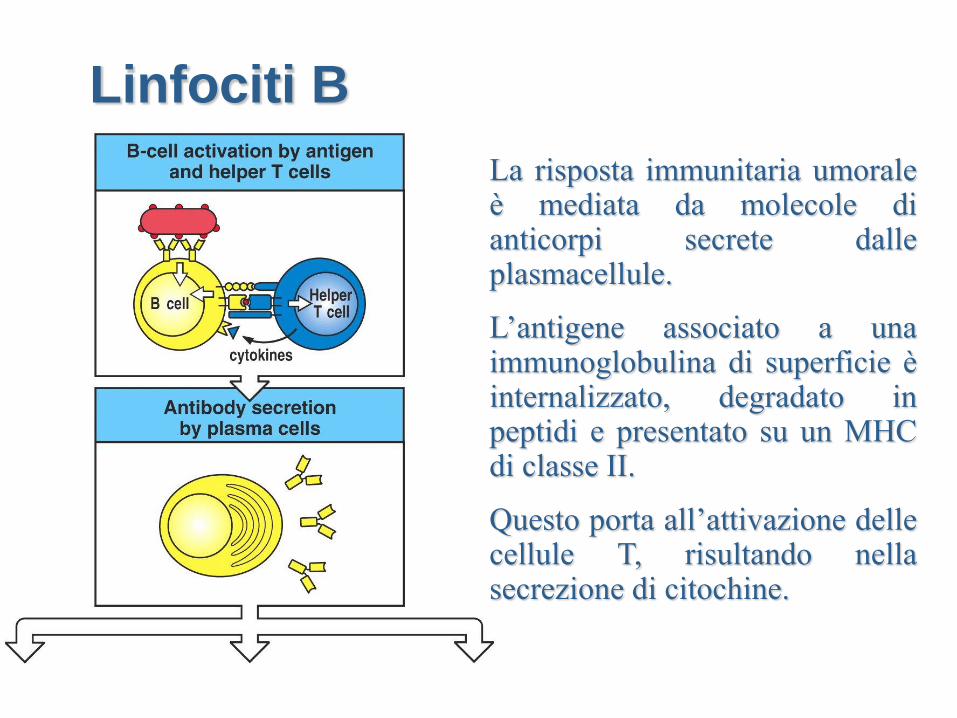
Figure 9-1 part 1 of 2 La risposta immunitaria umorale è mediata da molecole di anticorpi secrete dalle plasmacellule.
L’antigene associato a una immunoglobulina di superficie è internalizzato, degradato in peptidi e presentato su un MHC di classe II.
Questo porta all’attivazione delle cellule T, risultando nella secrezione di citochine.
Linfociti B
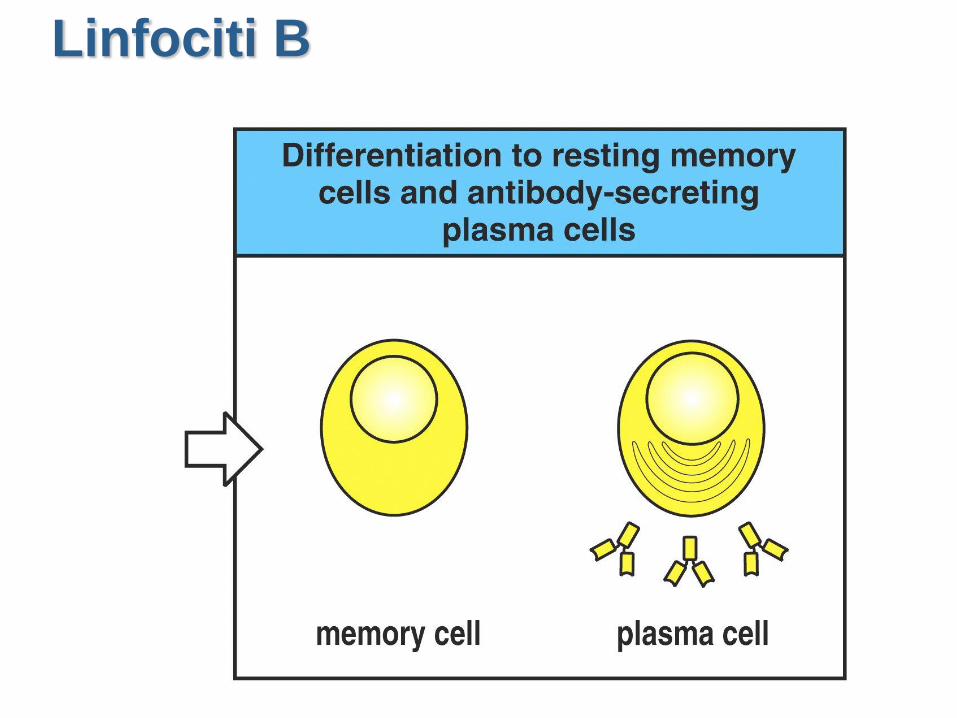
Figure 9-5 part 2 of 2 Linfociti B
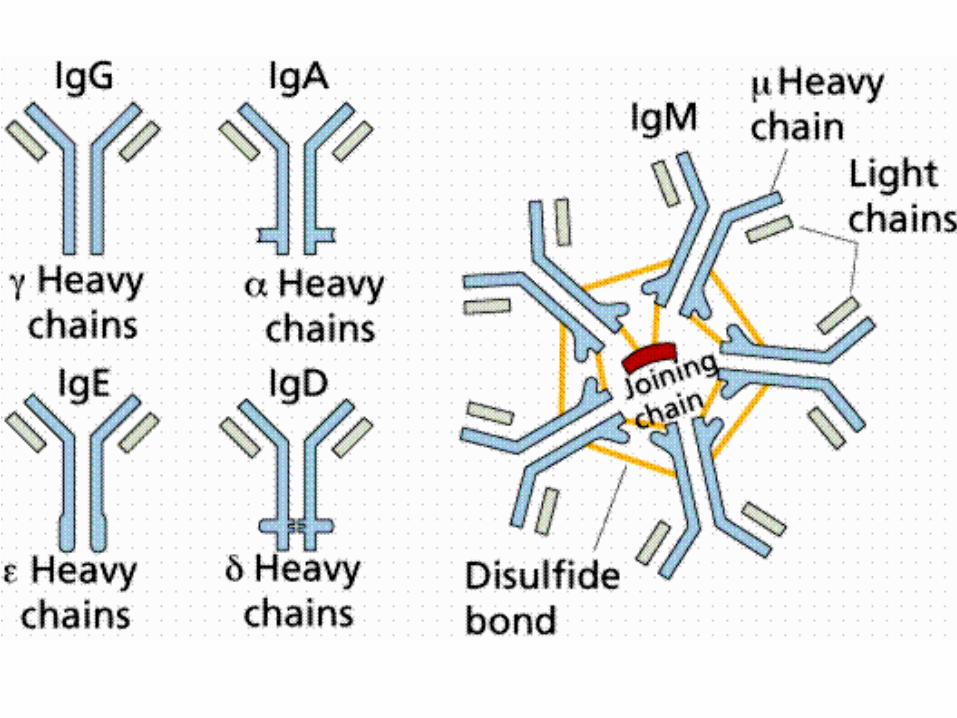
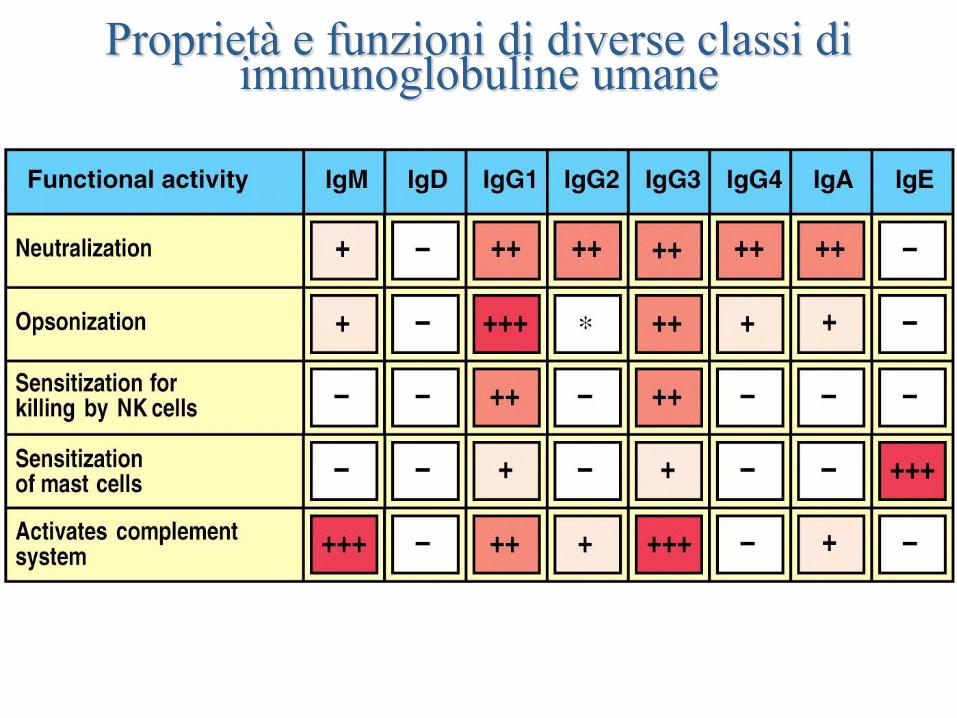
Figure 9-19 part 1 of 2
Proprietà e funzioni di diverse classi di immunoglobuline umane
Immunità specifica
Le risposte alle cellule B si
concentrano sui patogeni al di fuori
delle cellula; le risposte alle cellule
T si concentrano sui patogeni
intracellulari
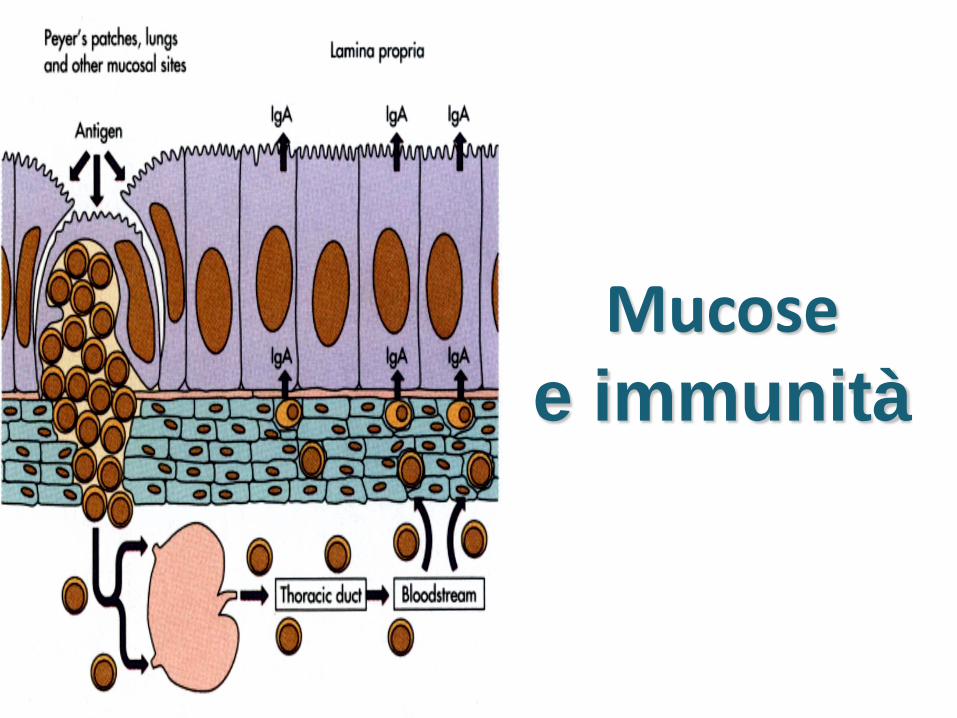
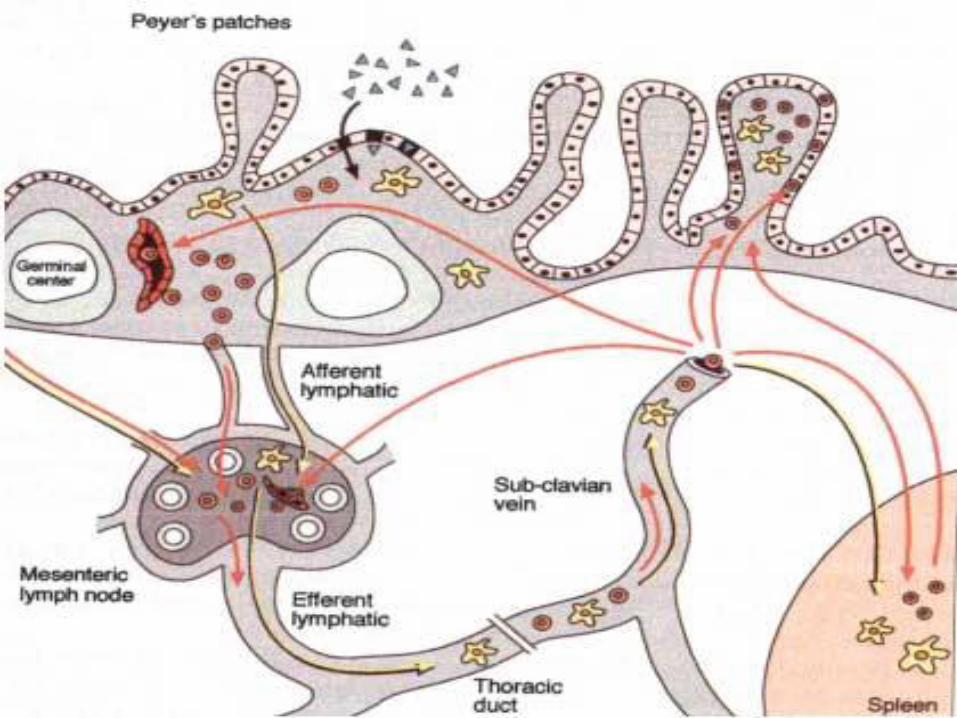
Mucose e immunità
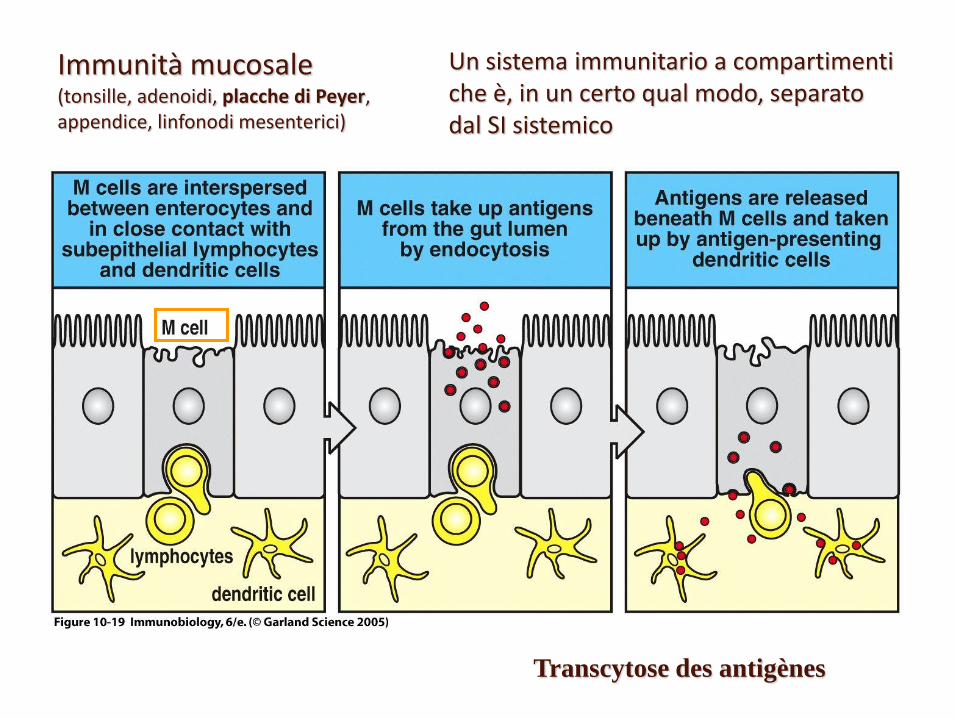
Immunità mucosale (tonsille, adenoidi, placche di Peyer, appendice, linfonodi mesenterici)
mucus no mucus here mucus
Un sistema immunitario a compartimenti che è, in un certo qual modo, separato dal SI sistemico
Transcytose des antigènes

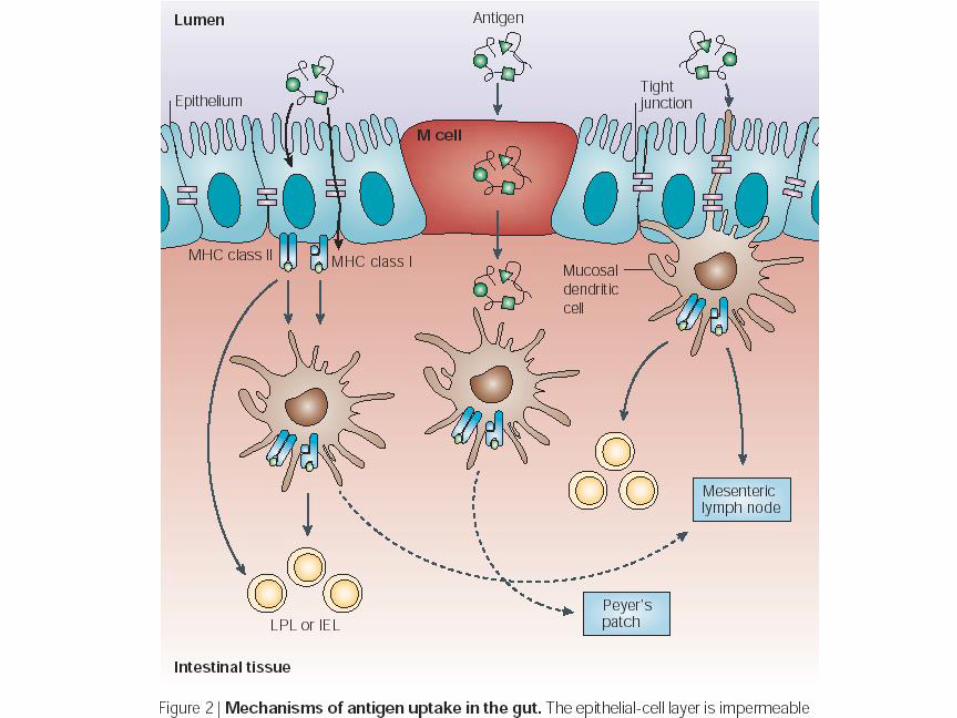
Le cellule M facilitano l’assimilazione degli Ag
IgA Mucosale
• 2 sottoclassi nell’uomo
• IgA1- monomerica, IgA predominante nel siero
• IgA2- polimerica, si riscontra soprattutto nelle
secrezioni esterne.
• J-chain- richiesta per la formazione dell’IgA polimerica,
J-chain gko di topo- IgA monomerica ma è secreta.
• La perdita di 13 aa in una zona cerniera diminuisce la
suscettibilità dell’IgA2 alla divisione proteolitica.
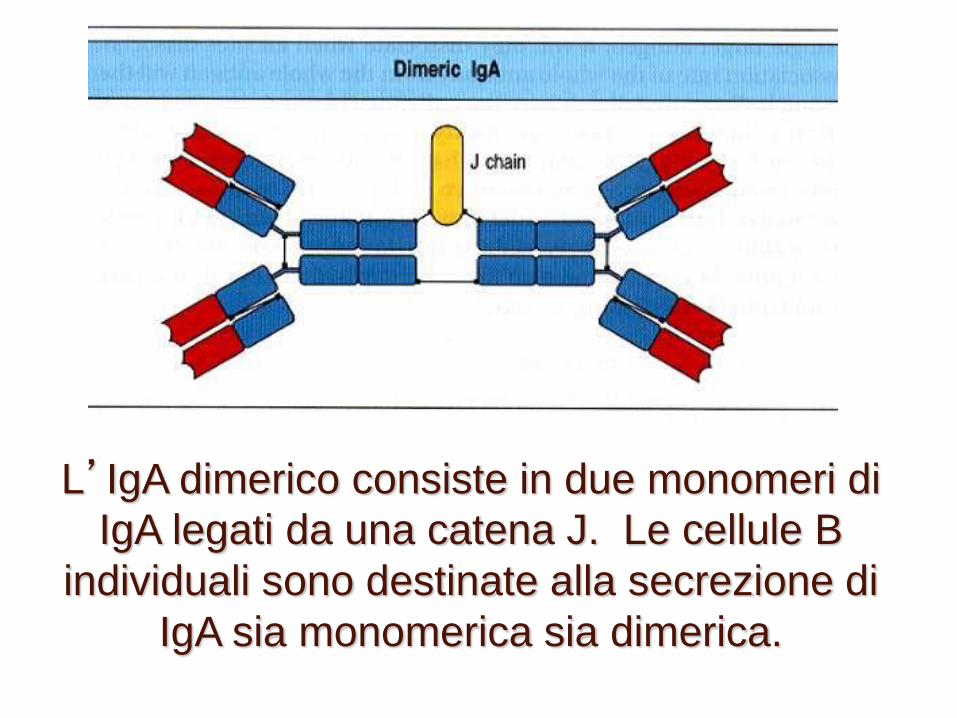
L’IgA dimerico consiste in due monomeri di
IgA legati da una catena J. Le cellule B
individuali sono destinate alla secrezione di
IgA sia monomerica sia dimerica.
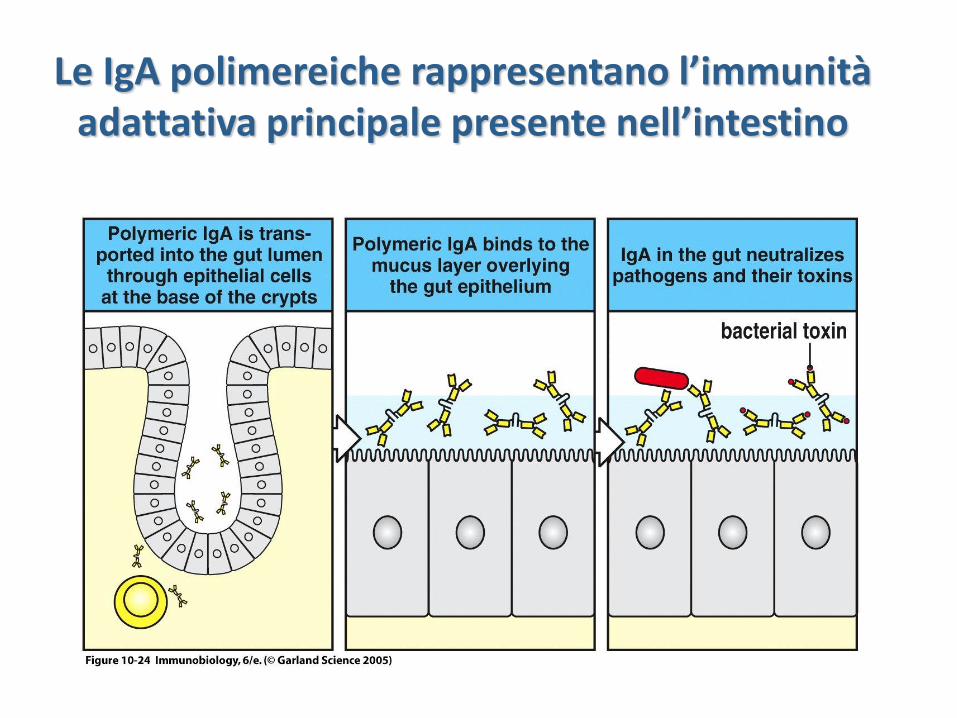
Le IgA polimereiche rappresentano l’immunità adattativa principale presente nell’intestino
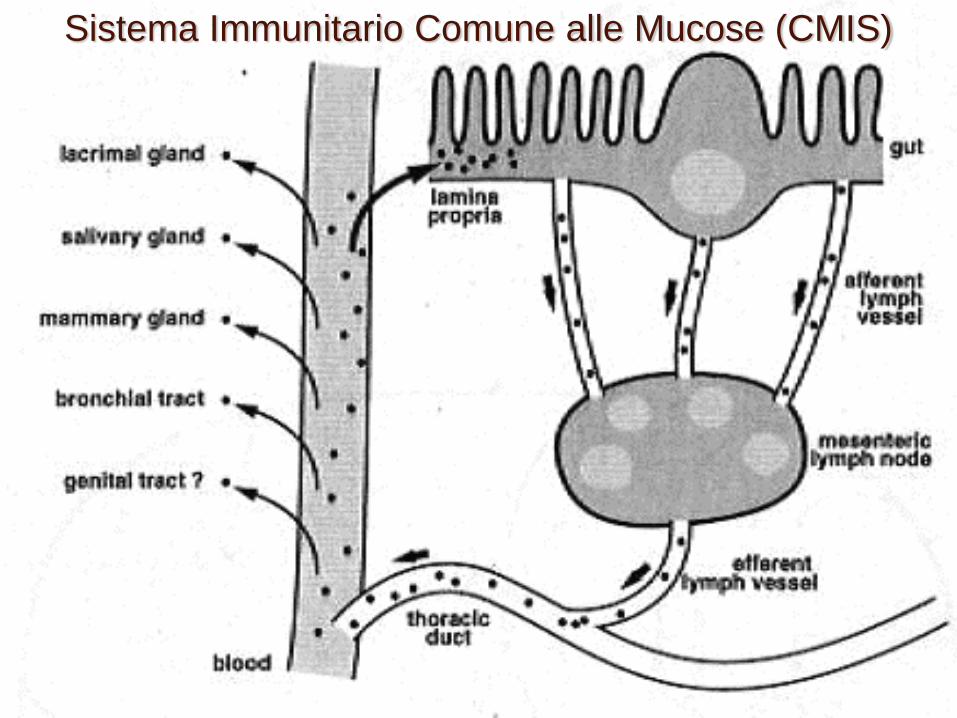
Sistema Immunitario Comune alle Mucose (CMIS)
Tolleranza mucosale
• Induzione di un’assenza di risposta sistemica mediante
somministrazione di antigene i.n. o orale.
• L’idea: evitare lo sviluppo di allergie alimentari.
• Alto dosaggio unico, basse dosi multiple.
• Assenza di risposta sistemica– in presenza di risposta
mucosale alle IgA
• Un solo recettore di struttura data su
ciascuna cellula (e sulle sue cellule figlie).
• Una multitudine di recettori diversi a
livello della popolazione
Immunità adattativa
TCR : T cell receptor
BCR : B cell receptor
« Il » recettore specializzato delle
cellule dell’immunità adattativa
Immunità adattativa
Il suo legante : l’antigene
Fa fronte alla diversità dei batteri e
alle loro mutazioni mediante una
generazione aleatoria e continua di
nuovi recettori
Vantaggi
Immunità adattativa
Immunità adattativa
Percezione analitica di sequenze
peptidiche ma nessuna percezione
intrinseca di ciò che è batterico
o meno, ostile o meno
Immunità adattativa
Percepisce i batteri intracellulari
grazie al sistema di campionamento e
di presentazione da parte delle
molecole del Complesso Maggiore di
Istocompatibilità (CMH)
Vantaggi
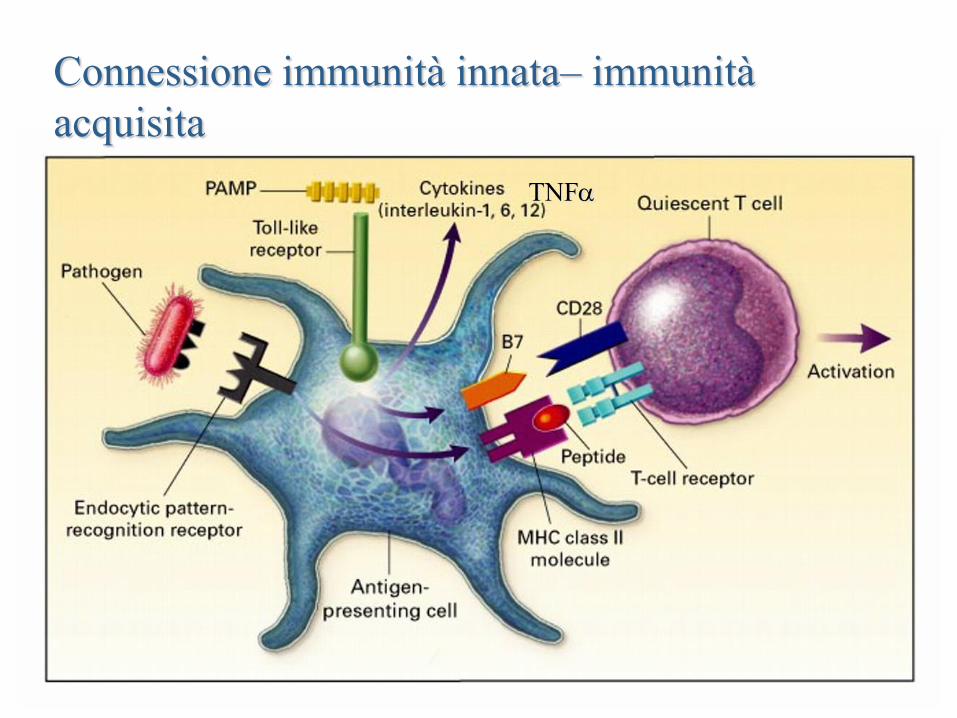
Connessione immunità innata– immunità
acquisita
TNF
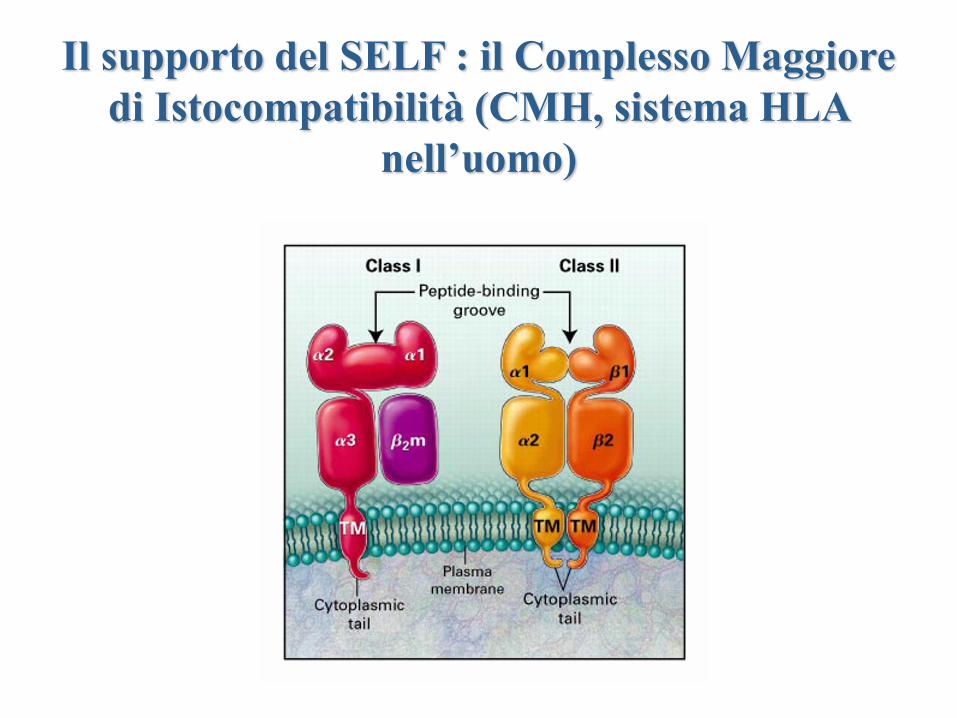
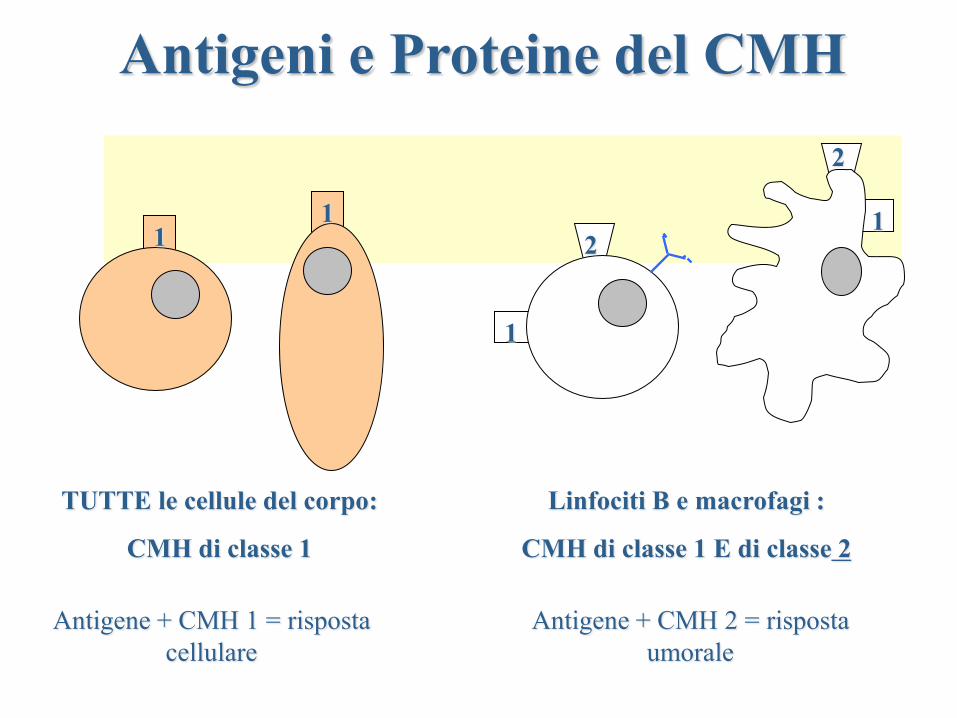
Il supporto del SELF : il Complesso Maggiore
di Istocompatibilità (CMH, sistema HLA
nell’uomo)
CMH : Complexe Majeur d’Histocompatibilité = empreintes
digitales des cellules
Protéines servant de “présentoir” aux antigènes
TUTTE le cellule del corpo:
CMH di classe 1
1 1
Linfociti B e macrofagi :
CMH di classe 1 E di classe 2
1
2
1
2
Antigene + CMH 1 = risposta
cellulare
Antigene + CMH 2 = risposta
umorale
Antigeni e Proteine del CMH
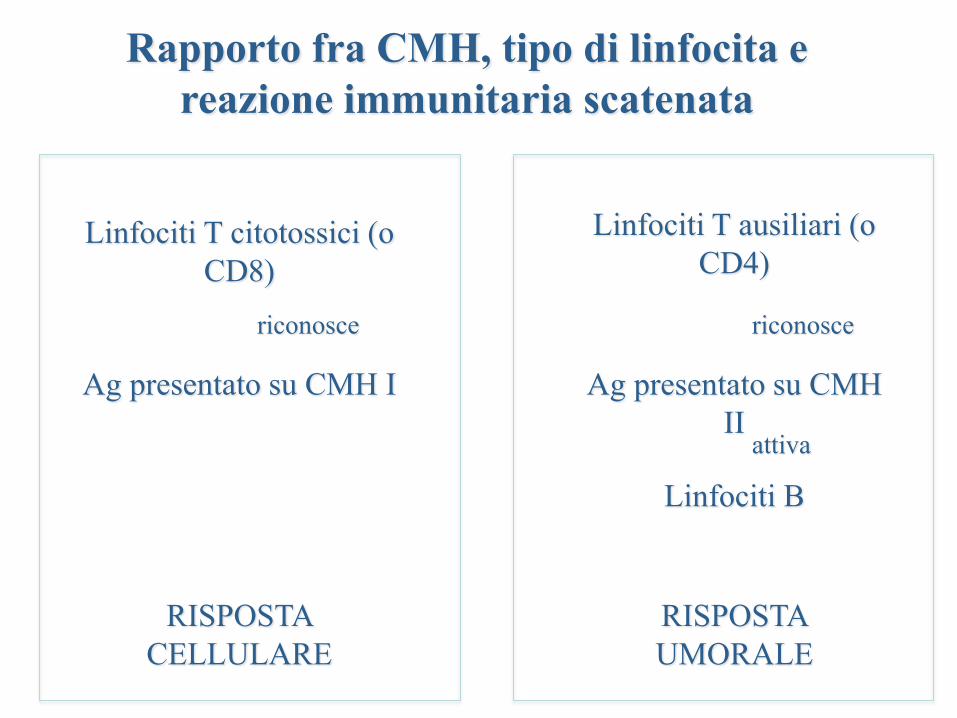
Rapporto fra CMH, tipo di linfocita e
reazione immunitaria scatenata
Ag presentato su CMH I
Linfociti T citotossici (o
CD8)
RISPOSTA
CELLULARE
riconosce
Ag presentato su CMH
II
Linfociti T ausiliari (o
CD4)
Linfociti B
RISPOSTA
UMORALE
riconosce
attiva
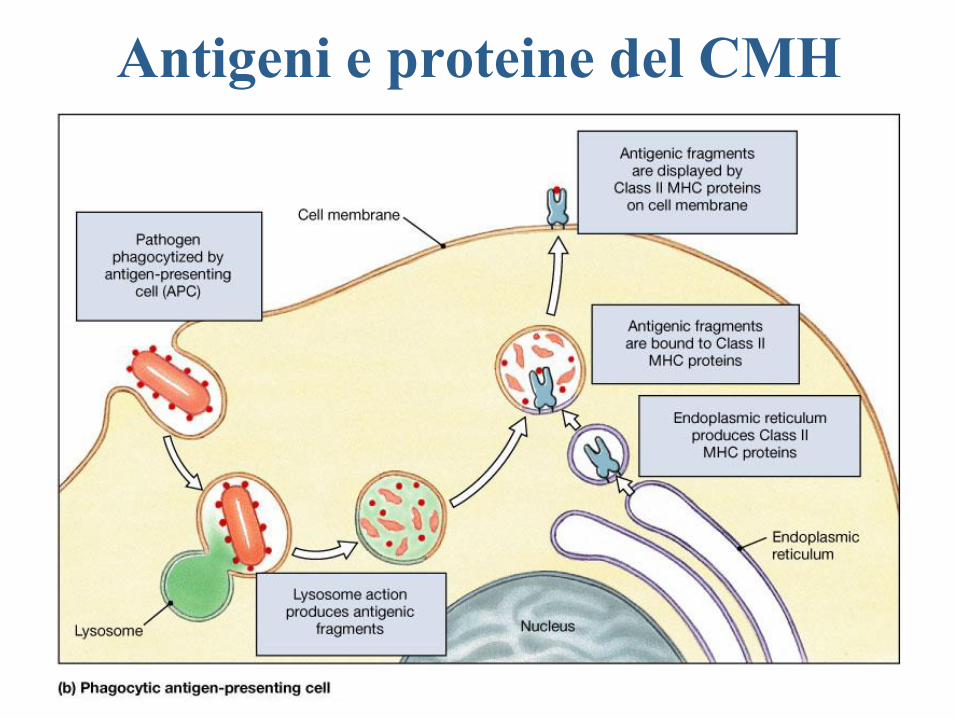
Antigeni e proteine del CMH
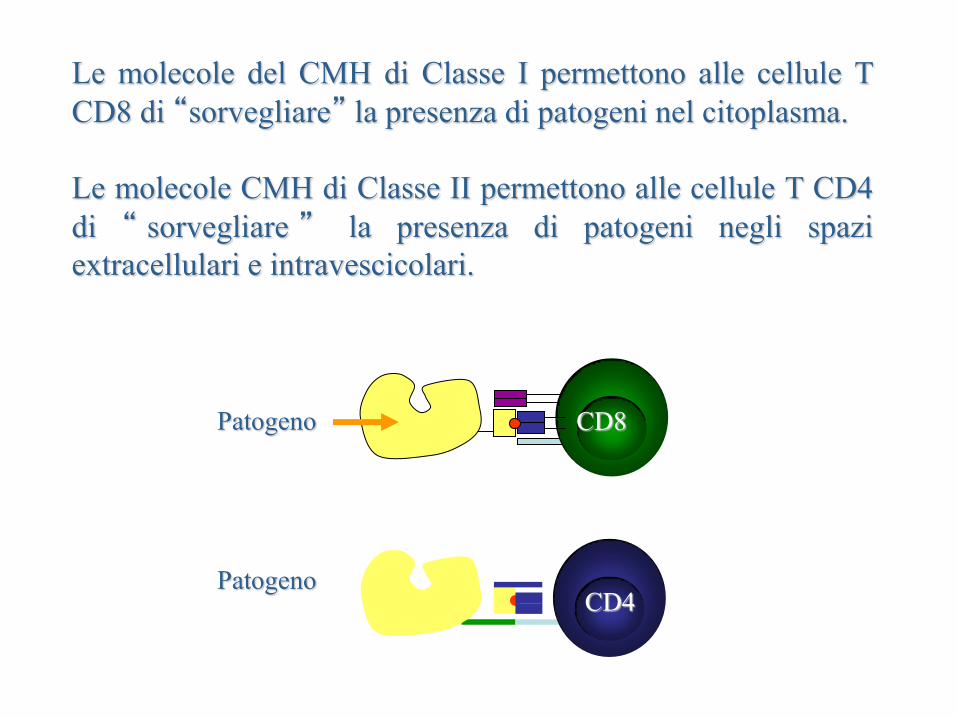
Le molecole del CMH di Classe I permettono alle cellule T
CD8 di “sorvegliare” la presenza di patogeni nel citoplasma.
Le molecole CMH di Classe II permettono alle cellule T CD4
di “ sorvegliare ” la presenza di patogeni negli spazi
extracellulari e intravescicolari.
Patogeno CD4
Patogeno CD8
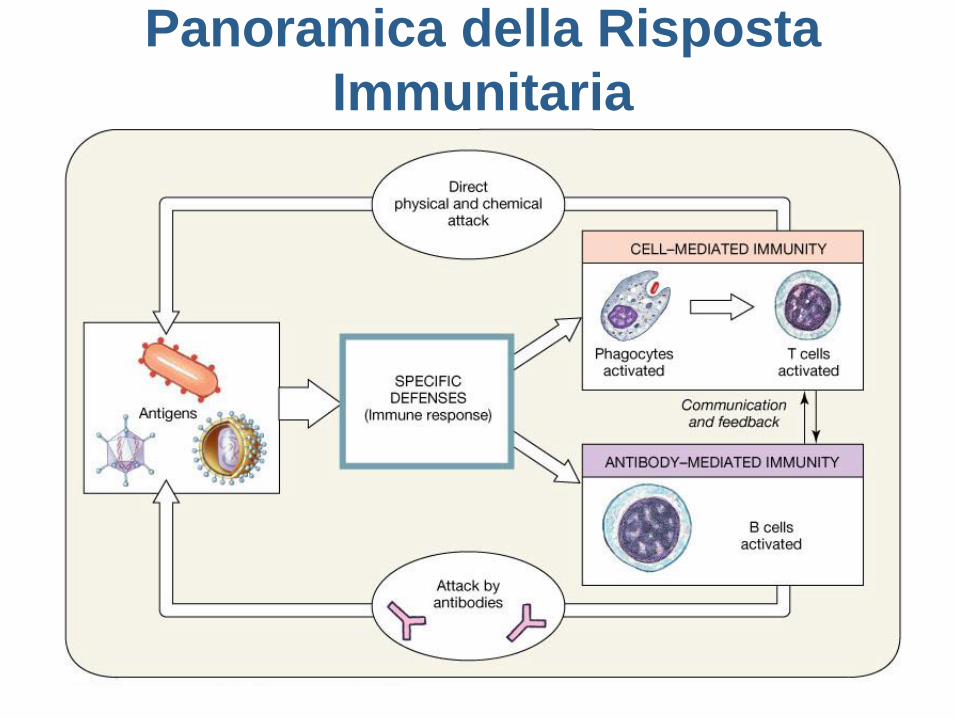
Panoramica della Risposta
Immunitaria

REGOLAZIONE DELLE
RISPOSTE IMMUNITARIE
SPECIFICHE
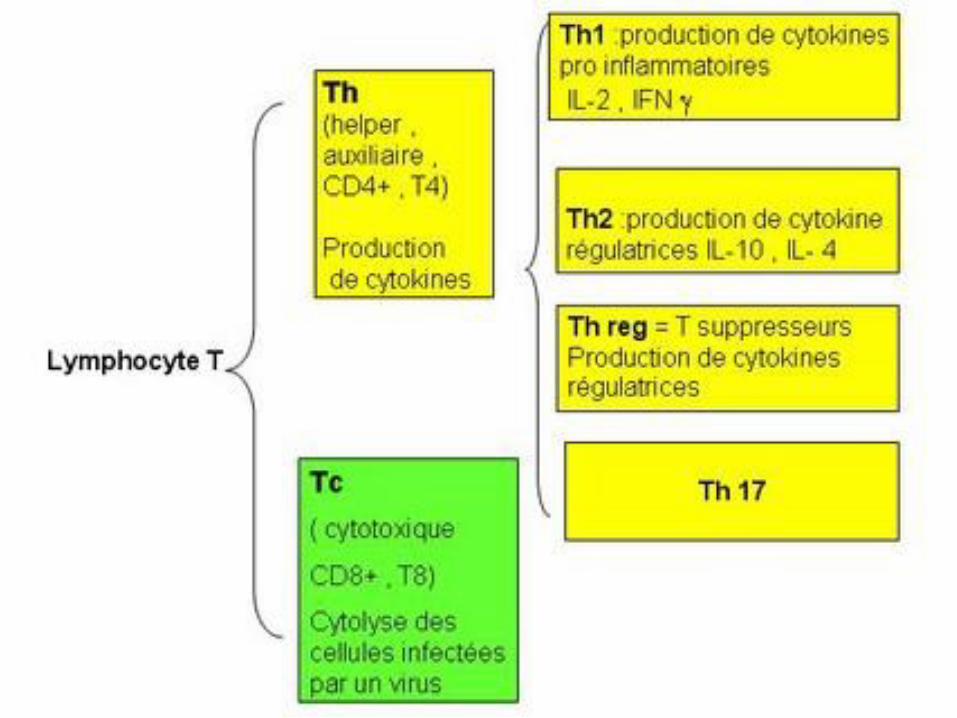
I LINFOCITI T CD4
Th1, Th2, TH17 e
Treg

OFFESA
INFIAMMAZIONE
Allergie
Malattie Autoimmuni
MALATTIE AUTOIMMUNI
Poliartrite reumatoide
Psoriasi
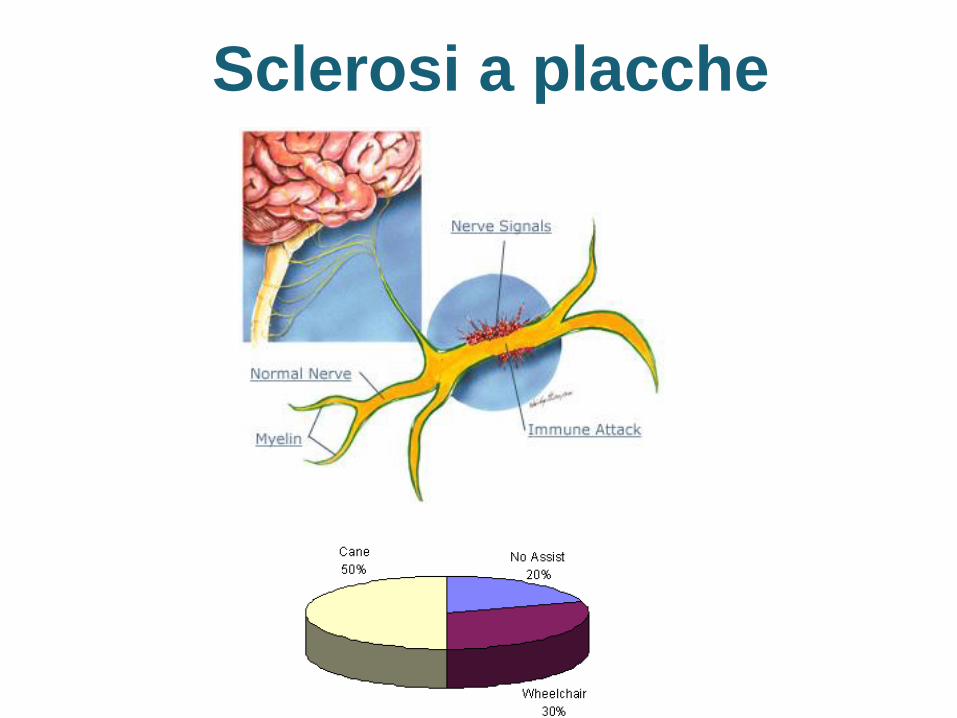
Sclerosi a placche
Morbo di Crohn
Lupus eritematoso
Guillain-Barré
Tiroiditi
...
Insieme di disordini immunitari che vanno da malattie molto
comuni come l’artrite reumatoide, la tiroidite di Hashimoto, il
morbo di Graves, l’aterosclerosi a patologie meno frequenti
come la sclerosi a placche, il diabete di tipo I, il lupus
eritematoso sistemico….
L’autoimmunità è la causa a monte di oltre 80 patologie
croniche che colpiscono il 20% circa della popolazione dei
paesi industrializzati.
MALATTIE AUTOIMMUNI

Mimetismo antigenico
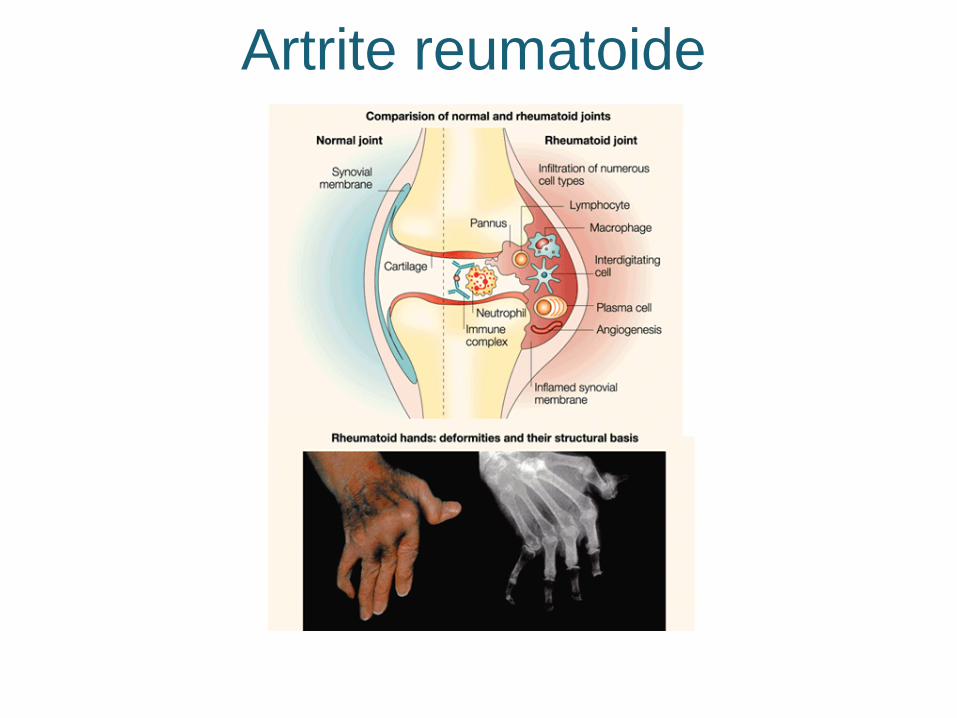
Artrite reumatoide
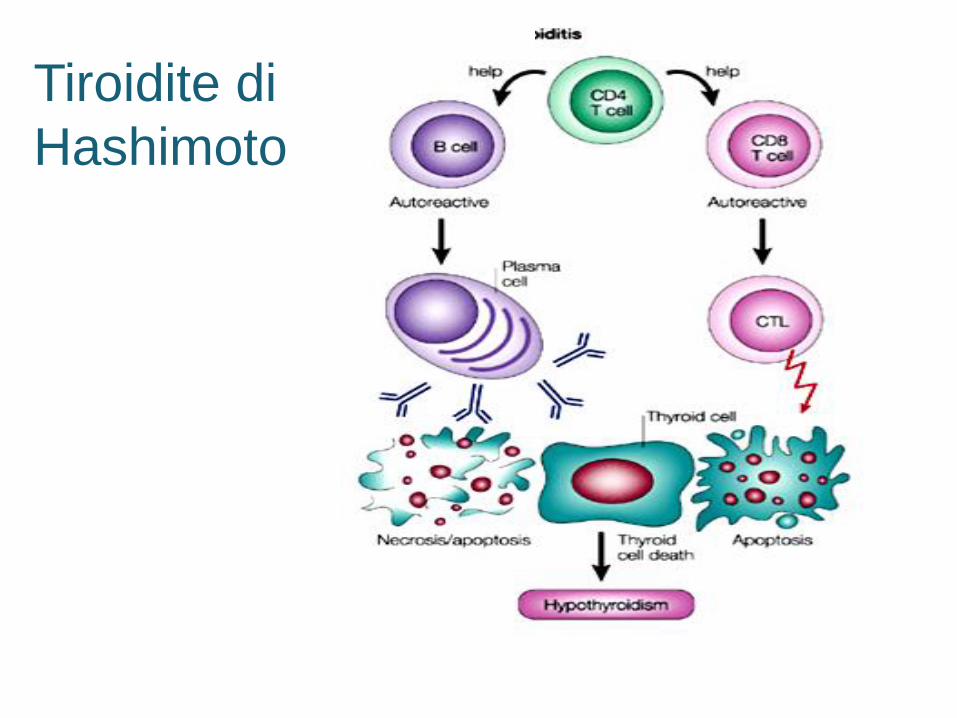
Tiroidite di
Hashimoto
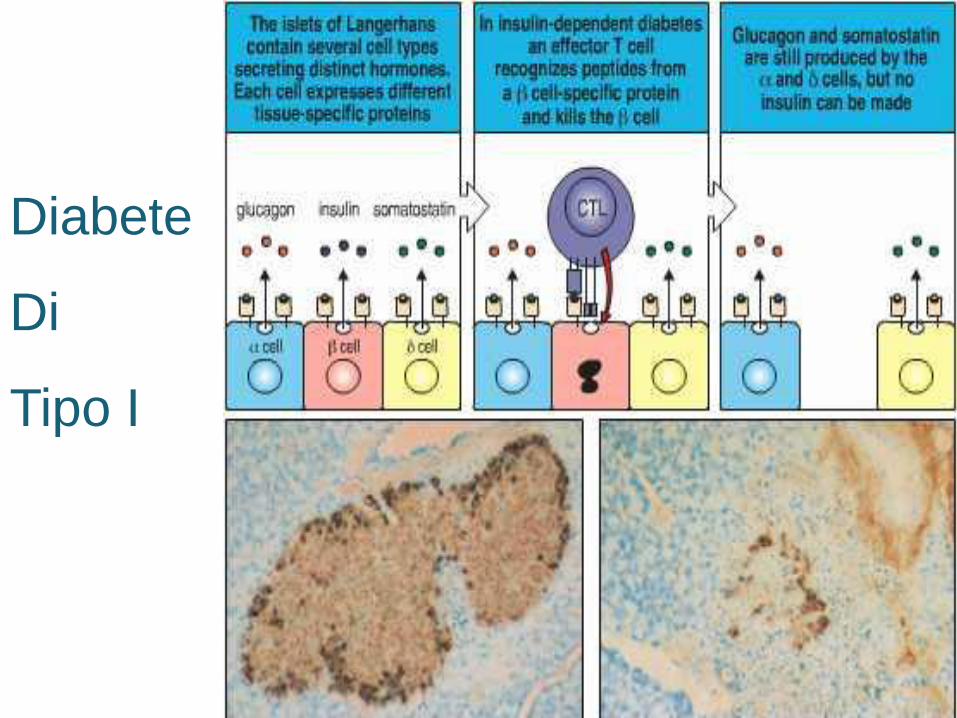
Diabete
Di
Tipo I
Aterosclerosi
Sclerosi a placche

ALLERGIE
Riniti
Congiuntiviti
Eczemi
Asma
Diarree
...
Attivazione del
Sistema immunitario
contro molecole
o organismi
non patogeni
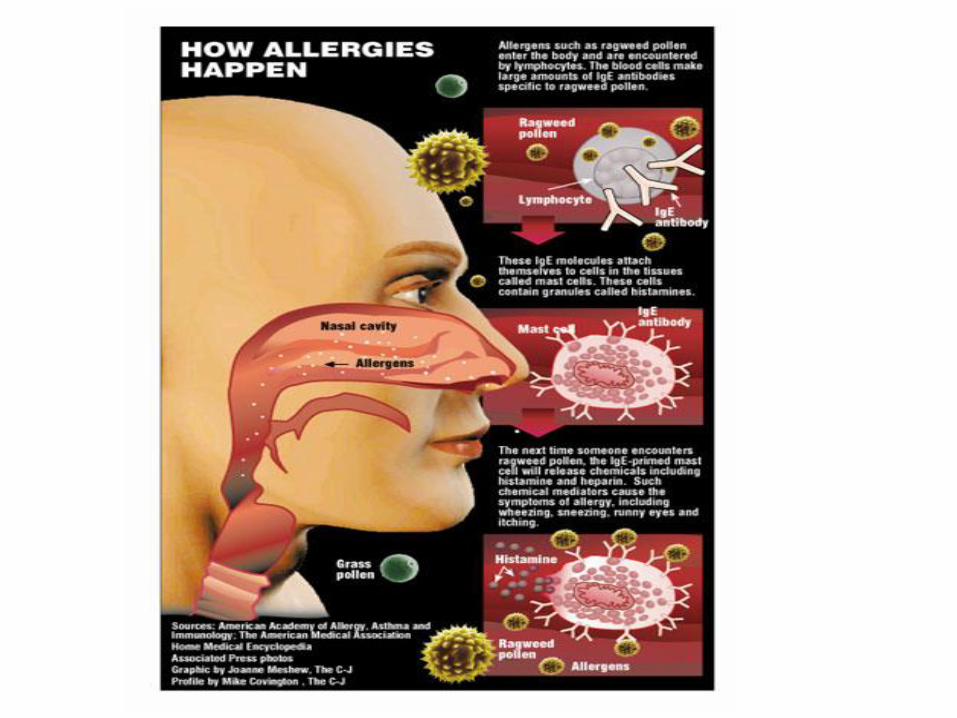
ALLERGIE

Allergeni
Allergie
Alimentari
E contro la flora
Batterica
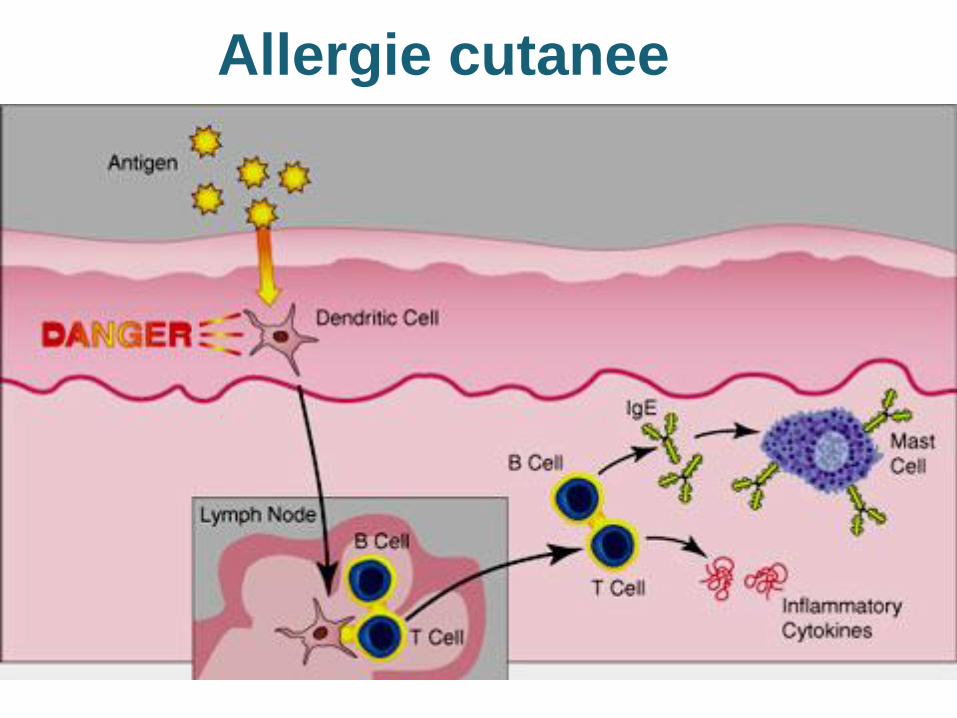
Allergie cutanee
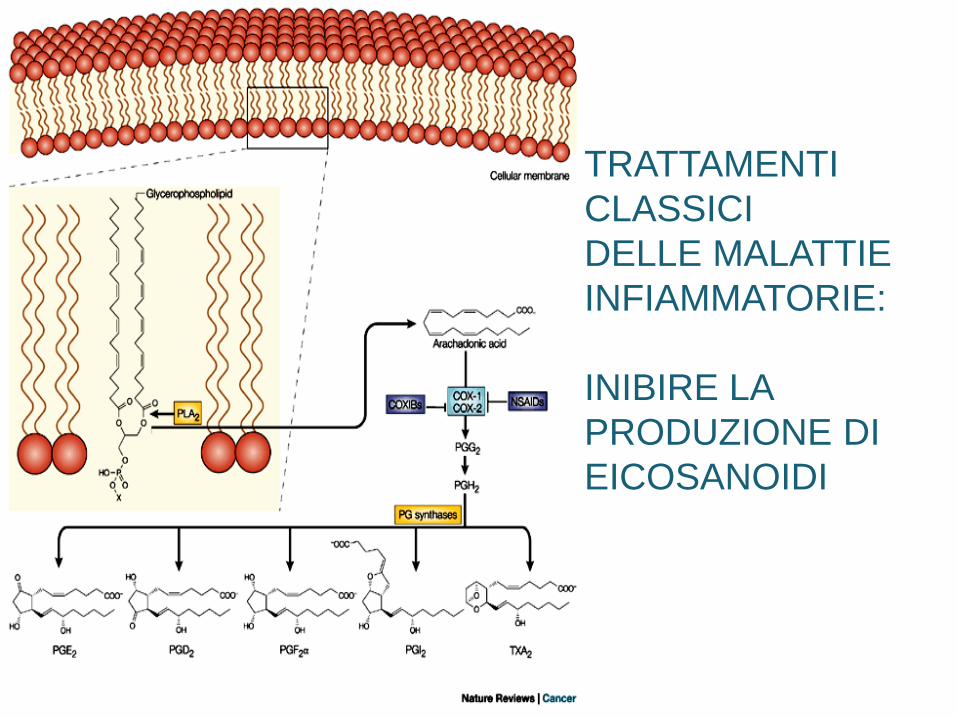
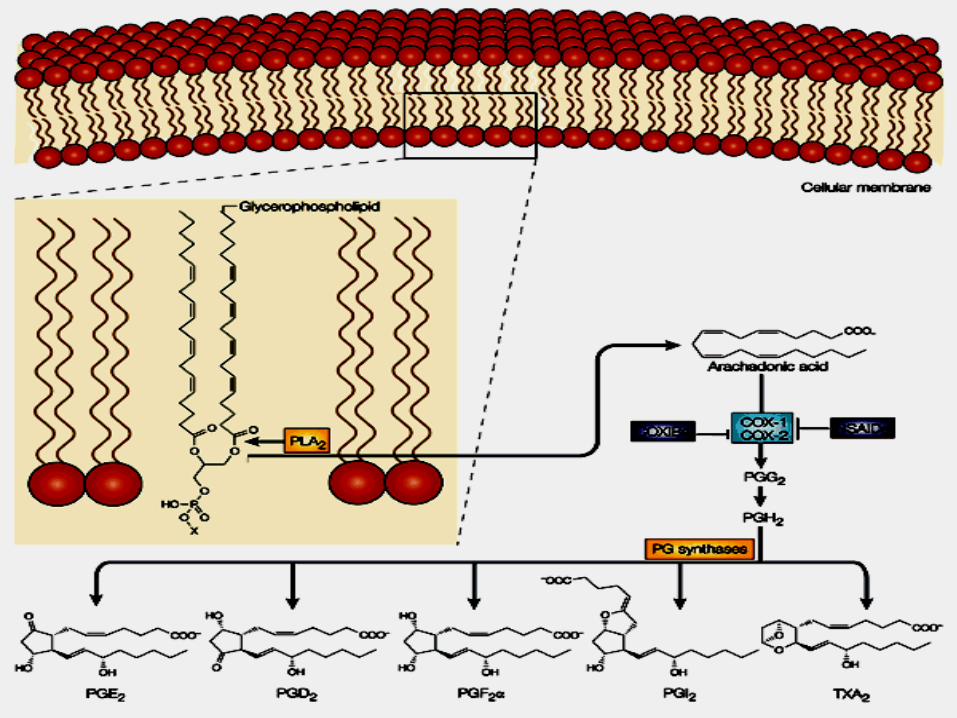
TRATTAMENTI
CLASSICI
DELLE MALATTIE
INFIAMMATORIE:
INIBIRE LA
PRODUZIONE DI
EICOSANOIDI
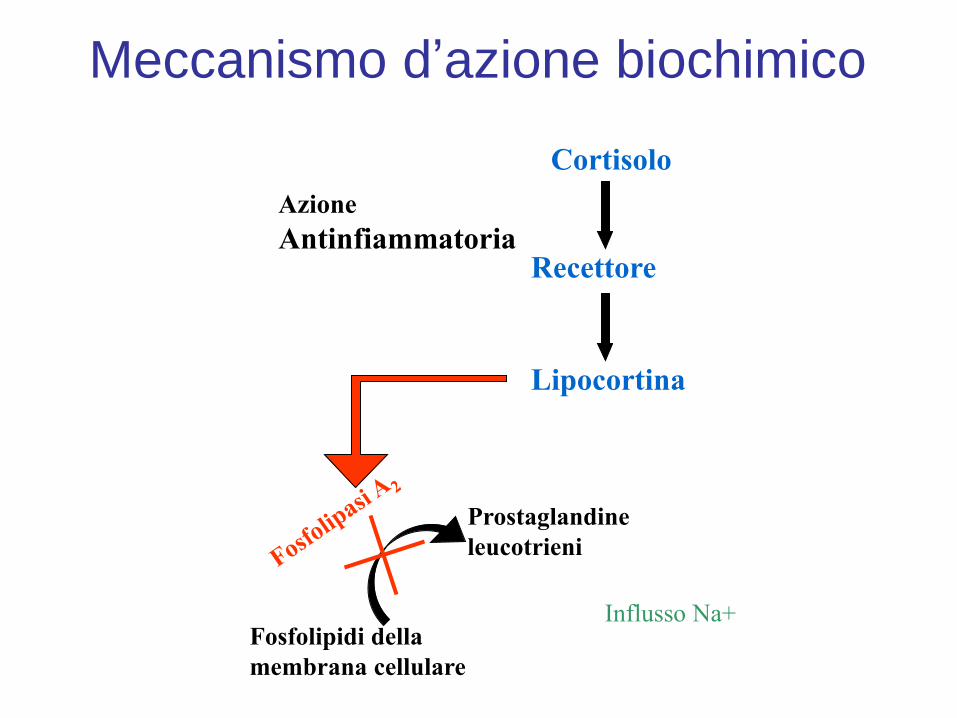
Meccanismo d’azione biochimico
Influsso Na+
Cortisolo
Recettore
Lipocortina
Fosfolipidi della
membrana cellulare
Prostaglandine
leucotrieni
Azione
Antinfiammatoria
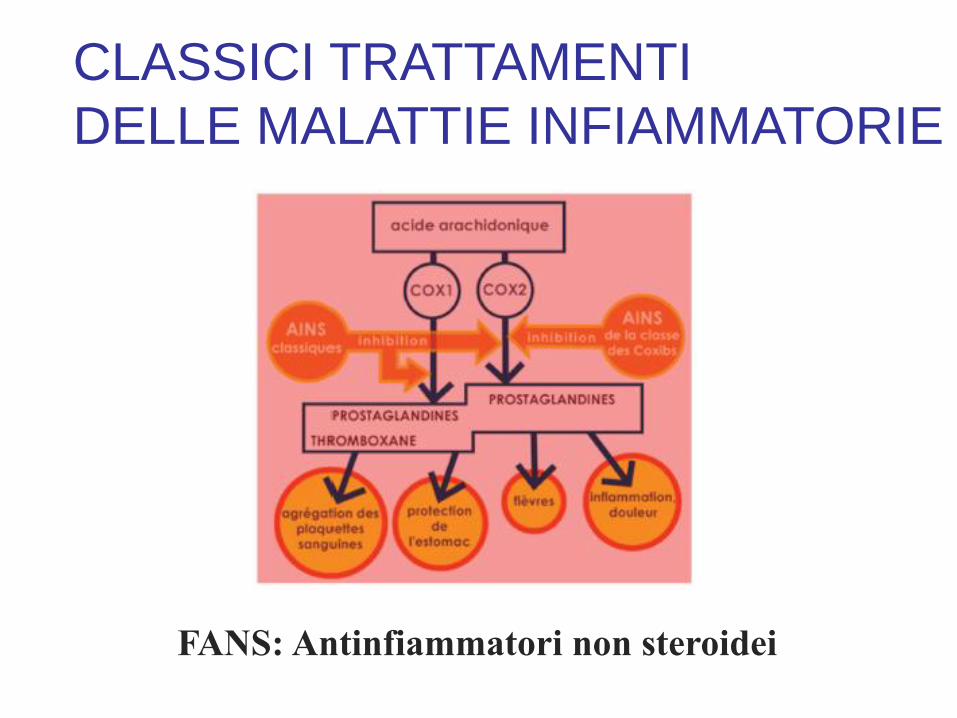
CLASSICI TRATTAMENTI
DELLE MALATTIE INFIAMMATORIE
FANS: Antinfiammatori non steroidei
Nutrition and immunology: from the clinic to cellular biology and back again.
Chandra RK.
Proc Nutr Soc. 1999 Aug;58(3):681-3.
Diet and immunity have been known to be linked to each other for centuries. In the
last 30 years systematic studies have confirmed that nutrient deficiencies impair
immune response and lead to frequent severe infections resulting in increased
mortality, especially in children. Protein-energy malnutrition results in reduced
number and functions of T-cells, phagocytic cells and secretory immunoglobulin A
antibody response. In addition, levels of many complement components are
reduced. Similar findings have been reported for moderate deficiencies of individual
nutrients such as trace minerals and vitamins, particularly Zn, Fe, Se, vitamins A,
B6, C and E. For example, Zn deficiency is associated with profound impairment of
cell-mediated immunity such as lymphocyte stimulation response, decreased
CD4+:CD8+ cells, and decreased chemotaxis of phagocytes. In addition, the level
of thymulin, which is a Zn-dependent hormone, is markedly decreased. The use of
nutrient supplements, singly or in combination, stimulates immune response and
may result in fewer infections, particularly in the elderly, low-birth-weight infants
and malnourished critically-ill patients in hospitals. The interactions between
nutrition and the immune system are of clinical, practical and public health
importance.
Palmitate activates the NF-kappaB transcription factor and induces IL-6 and
TNFalpha expression in 3T3-L1 adipocytes. Ajuwon KM, Spurlock ME.
J Nutr. 2005 Aug;135(8):1841-6.
Fatty acids and their metabolites regulate gene expression and immunological pathways.
Furthermore, obese individuals frequently have increased circulating fatty acid concentrations,
and localized inflammation in adipose tissue may facilitate the systemic inflammation associated
with the insulin resistance of obesity. Although palmitate induces inflammation (i.e., activates
proinflammatory pathways) in myotubes, the effects of fatty acids on inflammatory processes in
adipocytes have not been established. Therefore, we examined the potential for palmitate,
laurate, and docosahexaenoic acid (DHA) to modulate inflammation in 3T3-L1 adipocytes.
Palmitate, but not DHA or laurate, induced nuclear factor kappaB (NF-kappaB)-driven luciferase
activity and interleukin-6 (IL-6) expression (P < 0.05). Inhibition of fatty acyl Co-A synthase
(FACS) with triacsin C suppressed palmitate-induced NF-kappaB activation (P < 0.05), but
caused an additive increase in palmitate-induced IL-6 expression (P < 0.05). Disrupting
mitogen-activated protein kinase/Erk kinase (MEK) and protein kinase C (PKC) activity with
U0126 and Bisindolylmaleimide (Bis), respectively, suppressed palmitate-induced IL-6
expression (P < 0.05), but had no effect on NF-kappaB reporter gene activity (P > 0.05).
However, the phosphoinositide-3 kinase (PI3K) inhibitor, wortmannin, alone and additively with
palmitate, activated the NF-kappaB reporter gene and induced IL-6 expression (P < 0.05).
Palmitate also induced the mRNA expression of tumor necrosis factor alpha (TNFalpha) (P <
0.05), but the increase in mRNA abundance was not reflected in a greater protein concentration
in the media (P > 0.05). These data indicate that palmitate induces inflammation in adipocytes,
and that this is not a generalized effect of all SFA. Furthermore, PI3K may act constitutively to
suppress inflammation. Consequently, inhibition of this enzyme may promote and exacerbate
the inflammation in adipose tissue that is associated with obesity and insulin resistance.
PRESA IN CARICO NUTRIZIONALE E FUNZIONALE DELLE MALATTIE DISIMMUNITARIE
• Ridurre il rischio di ingresso di antigeni non ostili
Digestione, Barriera intestinale
• Ridurre l’intensità della risposta infiammatoria
Equilibrio AA/EPA, Regolatori del NFKB
•Impedire l’accumulo di lesioni ossidative e da carbonili
inflitte ai tessuti attaccati • Antiossidanti
• Aumentare l’immunotolleranza:
Probiotici, Vitamina D
LIVELLO I Le barriere
LIVELLO II Immunità
innata
LIVELLO III Immunità specifica
Medicina nutrizionale
Ripristinare le barriere
Tight junctions, leaky intestines, and pediatric diseases. Liu Z, Li N, Neu J.
Acta Paediatr. 2005 Apr;94(4):386-93.
BACKGROUND: Tight junctions (TJs) represent the major barrier
within the paracellular pathway between intestinal epithelial cells.
Disruption of TJs leads to intestinal hyperpermeability (the so-called
"leaky gut") and is implicated in the pathogenesis of several acute and
chronic pediatric disease entities that are likely to have their origin
during infancy. AIM: This review provides an overview of evidence
for the role of TJ breakdown in diseases such as systemic
inflammatory response syndrome (SIRS), inflammatory bowel
disease, type 1 diabetes, allergies, asthma, and autism.
CONCLUSION: A better basic understanding of this structure might
lead to prevention or treatment of these diseases using nutritional or
other means.
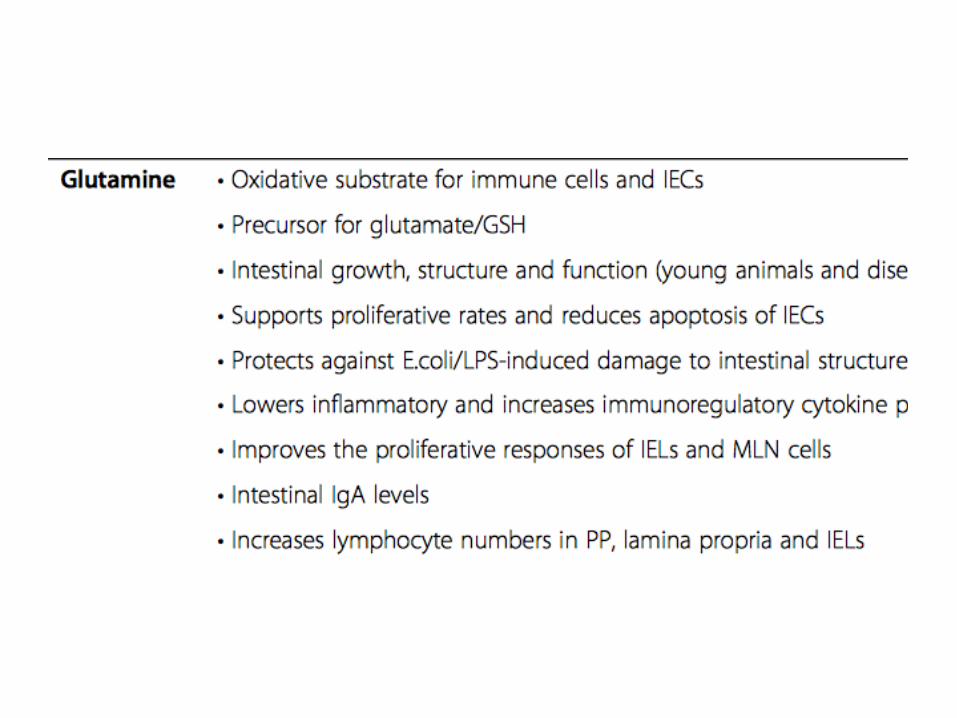
L-GLUTAMMINA
Effect of glutamine on the intestinal permeability
changes induced by indomethacin in humans.
Hond ED, Peeters M, Hiele M, Bulteel V, Ghoos Y, Rutgeerts P.
Department of Gastroenterology, University Hospital Leuven, Leuven, Belgium.
Aliment Pharmacol Ther. 1999 May;13(5):679-85
BACKGROUND: Long-term non-steroidal anti-inflammatory drug (NSAID) intake may
induce increased intestinal permeability, eventually resulting in enteropathy. Because
increased permeability might be related to cell damage resulting from energy depletion,
it was hypothesized that glutamine--the major energy source of the intestinal mucosal
cell--might prevent permeability changes. METHODS: The 6-h urinary excretion of 51Cr-
EDTA after an oral load of 51Cr-EDTA was used in this study as a measure for intestinal
permeability. Healthy volunteers underwent a series of permeability tests: (i) basal test;
(ii) test following NSAID (indomethacin); (iii) test following NSAID in combination with
glutamine and/or misoprostol. RESULTS: The NSAID induced increased permeability in
all volunteers. Pre-treatment with glutamine (3x7 g daily, 1 week before NSAID-dosing)
did not prevent the NSAID-induced increase in permeability. Multiple doses of glutamine
close in time to NSAID-dosing resulted in significantly lower permeability compared to
the NSAID without glutamine. Co-administration of misoprostol with the multiple-dose
scheme of glutamine resulted in a further reduction in the NSAID-induced increase in
permeability. CONCLUSIONS: Glutamine decreases the permeability changes caused
by NSAID-dosing when it is administered close in time, and misoprostol has a
synergistic effect.
Inflammation rather than nutritional depletion determines glutamine concentrations and
intestinal permeability.
Hulsewe KW, van der Hulst RW, van Acker BA, von Meyenfeldt MF, Soeters PB.
Clin Nutr. 2004 Oct;23(5):1209-16.
AIM: Nutritional depletion has been correlated with low plasma and mucosal glutamine
concentrations and with increased intestinal permeability. Since nutritional depletion often is
associated with (chronic) inflammatory stress, this study was designed to establish the influence of
depletion and inflammation on glutamine concentrations and gut barrier function. METHODS:
Anthropometric parameters were calculated from 26 patients who required artificial nutrition.
Glutamine concentrations in plasma and gut mucosa, gut permeability and mucosal morphology
were assessed. For determination of the degree of inflammation erythrocyte sedimentation rates
and (pre)albumin concentrations were measured. On the basis of these parameters patients were
divided into two groups having significant inflammatory stress or not. Similarly, a depleted and a
non-depleted group was formed based on percentage ideal body weight, fat-free mass index
(FFMI) and percentage weight loss. Glutamine concentrations, gut permeability and villus
morphology were compared between the groups. RESULTS: The presence of inflammatory activity
had significant negative effects on glutamine concentrations in contrast to the presence or absence
of nutritional depletion. Similarly, intestinal permeability increased during active inflammation but not
in depleted patients. FFMI but not inflammation was related to villus height. CONCLUSIONS: The
presence of inflammation significantly affects glutamine concentrations and gut permeability, in
contrast to the presence of depletion of body cell mass per se. On the other hand, villus
morphology is not influenced by changes in systemic inflammatory activity whereas nutritional
status possibly does affect villus height.
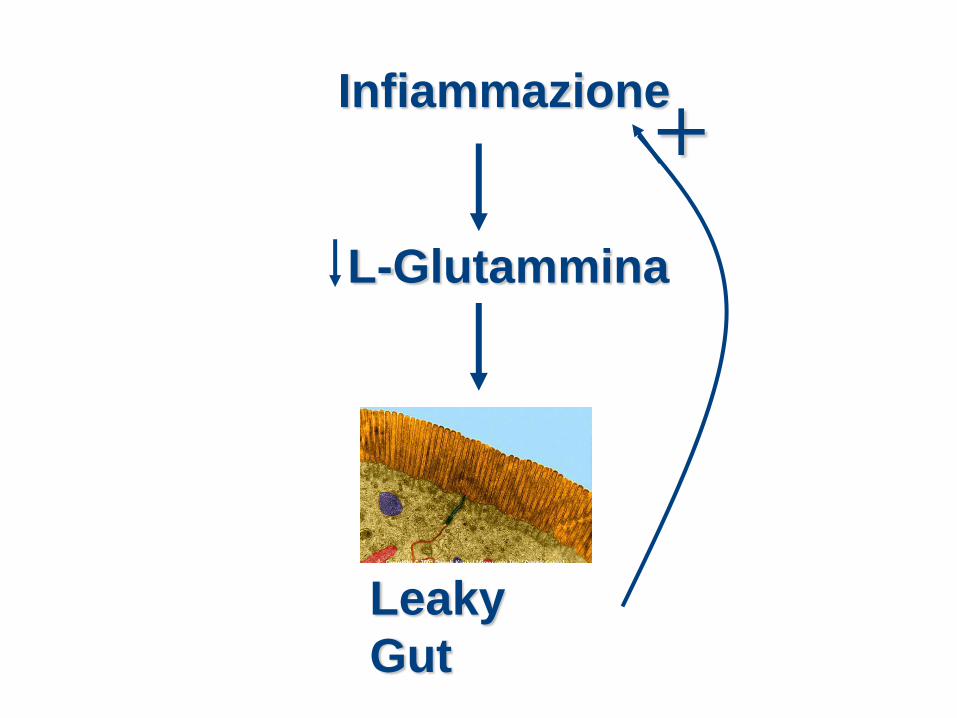
Infiammazione
L-Glutammina
Leaky
Gut
+
Probiotici
Prebiotici
Probiotics in primary prevention of atopic disease: a
randomised placebo-controlled trial. Kalliomaki M, Salminen S, Arvilommi H, Kero P, Koskinen P, Isolauri E.
Lancet 2001 Apr 7;357(9262):1076-9
BACKGROUND: Reversal of the progressive increase in frequency of atopic disease
would be an important breakthrough for health care and wellbeing in western
societies. In the hygiene hypothesis this increase is attributed to reduced microbial
exposure in early life. Probiotics are cultures of potentially beneficial bacteria of the
healthy gut microflora. We assessed the effect on atopic disease of Lactobacillus GG
(which is safe at an early age and effective in treatment of allergic inflammation and
food allergy). METHODS: In a double-blind, randomised placebo-controlled trial we
gave Lactobacillus GG prenatally to mothers who had at least one first-degree
relative (or partner) with atopic eczema, allergic rhinitis, or asthma, and postnatally
for 6 months to their infants. Chronic recurring atopic eczema, which is the main sign
of atopic disease in the first years of life, was the primary endpoint. FINDINGS:
Atopic eczema was diagnosed in 46 of 132 (35%) children aged 2 years. Asthma was
diagnosed in six of these children and allergic rhinitis in one. The frequency of atopic
eczema in the probiotic group was half that of the placebo group (15/64 [23%]
vs31/68 [46%]; relative risk 0.51 [95% CI 0.32-0.84]). The number needed to treat
was 4.5 (95% CI 2.6-15.6). INTERPRETATIONS: Lactobacillus GG was effective in
prevention of early atopic disease in children at high risk. Thus, gut microflora might
be a hitherto unexplored source of natural immunomodulators and probiotics, for
prevention of atopic disease.
Il Lactobacillus GG si è dimostrato efficace nella prevenzione
dell’atopia precoce in bambini ad alto rischio. Pertanto la
microflora intestinale potrebbe rappresentare una fonte finora
inesplorata di immunomodulatori naturali e probiotici per la
prevenzione dell’atopia.
Oral probiotic control skin inflammation by acting on both effector and regulatory T cells.
Hacini-Rachinel F, Gheit H, Le Luduec JB, Dif F, Nancey S, Kaiserlian D. PLoS One. 2009;4(3):e4903. Probiotics are believed to alleviate allergic and inflammatory skin disorders, but their impact on pathogenic effector T cells remains poorly documented. Here we show that oral treatment with the probiotic bacteria L. casei (DN-114 001) alone alleviates antigen-specific skin inflammation mediated by either protein-specific CD4(+) T cells or hapten-specific CD8(+) T cells. In the model of CD8(+) T cell-mediated skin inflammation, which reproduces allergic contact dermatitis in human, inhibition of skin inflammation by L. casei is not due to impaired priming of hapten-specific IFNgamma-producing cytolytic CD8(+) effector T cells. Alternatively, L. casei treatment reduces the recruitment of CD8(+) effector T cells into the skin during the elicitation (i.e. symptomatic) phase of CHS. Inhibition of skin inflammation by L. casei requires MHC class II-restricted CD4(+) T cells but not CD1d-restricted NK-T cells. L casei treatment enhanced the frequency of FoxP3(+) Treg in the skin and increased the production of IL-10 by CD4(+)CD25(+) regulatory T cells in skin draining lymph nodes of hapten-sensitized mice. These data demonstrate that orally administered L. casei (DN-114 001) efficiently alleviate T cell-mediated skin inflammation without causing immune suppression, via mechanisms that include control of CD8(+) effector T cells and involve regulatory CD4(+) T cells. L. casei (DN-114 001) may thus represent a probiotic of potential interest for immunomodulation of T cell-mediated allergic skin diseases in human.
Anti-inflammatory effects of bifidobacteria
by inhibition of LPS-induced NF-kappaB
activation. Riedel CU, Foata F, Philippe D, Adolfsson O, Eikmanns BJ, Blum S.
Microbiology Department and Alimentary Pharmabiotic Centre, University
College Cork, Cork, Ireland. [email protected].
World J Gastroenterol. 2006
AIM: Different strains of bifidobacteria were analysed for their effects on HT-29
intestinal epithelial cells (IECs) in in vitro models both of the non-inflamed and
inflamed intestinal epithelium. METHODS: A reporter gene system in HT-29
cells was used to measure levels of NF-kappaB activation after challenge with
bifidobacteria or after bacterial pre-treatment following LPS challenge. IL-8
protein and pro-inflammatory gene expression was investigated using normal
HT-29 cells. RESULTS: None of the bifidobacteria tested induced activation of
nuclear factor kappaB (NF-kappaB) indicating that bifidobacteria themselves
do not induce inflammatory events in IECs. However, six out of eight
bifidobacteria tested inhibited lipopolysaccharide- (LPS-) induced NF-kappaB
activation in a dose- and strain-dependent manner. In contrast, NF-kappaB
activation in response to challenge with tumor necrosis factor-alpha (TNF-
alpha) was affected by none of the tested bifidobacteria, indicating that the
inhibitory effect of bifidobacteria is specific for LPS-induced inflammation in
IECs. As shown with two of the six inhibition-positive bifidobacteria, LPS-
induced inhibition of NF-kappaB activation was accompanied by a dose-
dependent decrease of interleukin 8 (IL-8) secretion and by lower mRNA levels
for IL-8, TNF-alpha, cyclooxygenase 2 (Cox-2), and intercellular adhesion
molecule 1 (ICAM-1). CONCLUSION: Some strains of bifidobacteria are
effective in inhibiting LPS-induced inflammation and thus might be appropriate
candidates for probiotic intervention in chronic intestinal inflammation.
Ripristinare gli equilibri
Medicina nutrizionale
Il rapporto fra gli
acidi grassi
Determina l’intensità
della reazione
infiammatoria
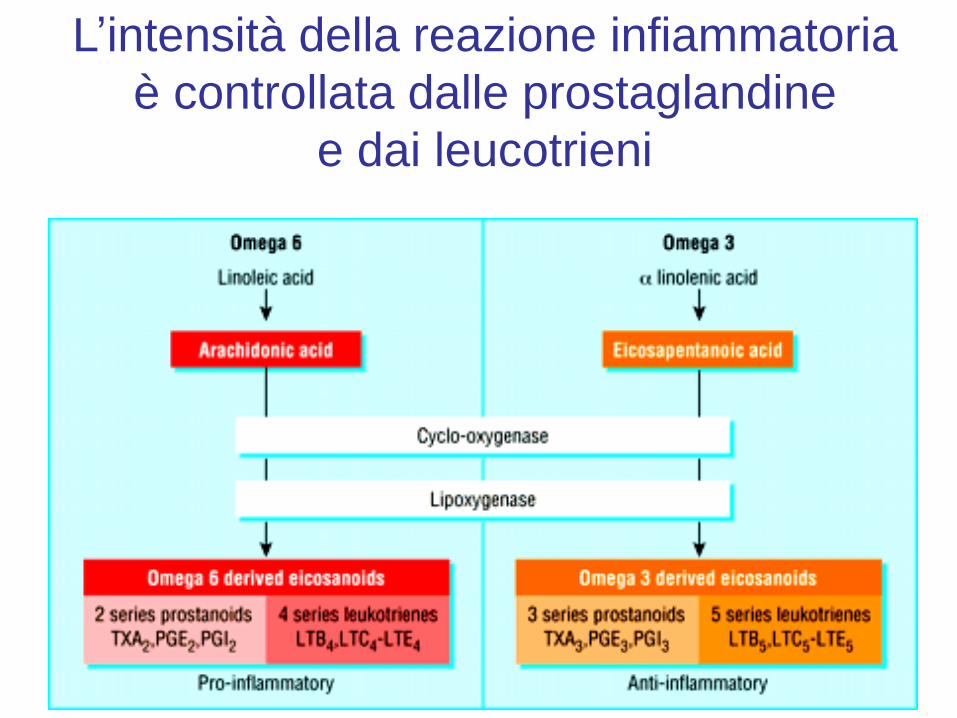
L’intensità della reazione infiammatoria
è controllata dalle prostaglandine
e dai leucotrieni
Acidei grassi OMEGA-3
I nutrienti
antinfiammatori
per eccellenza
The role of fish oils in the treatment of rheumatoid arthritis. Cleland LG, James MJ, Proudman SM.
Rheumatology Unit, Royal Adelaide Hospital, Adelaide, South Australia, Australia.
Drugs. 2003;63(9):845-53.
Fish oils are a rich source of omega-3 long chain polyunsaturated fatty acids (n-3 LC
PUFA). The specific fatty acids, eicosapentaenoic acid and docosahexaenoic acid, are
homologues of the n-6 fatty acid, arachidonic acid (AA). This chemistry provides for antagonism
by n-3 LC PUFA of AA metabolism to pro-inflammatory and pro-thrombotic n-6 eicosanoids, as
well as production of less active n-3 eicosanoids. In addition, n-3 LC PUFA can suppress
production of pro-inflammatory cytokines and cartilage degradative enzymes.In accordance with
the biochemical effects, beneficial anti-inflammatory effects of dietary fish oils have been
demonstrated in randomised, double-blind, placebo-controlled trials in rheumatoid arthritis (RA).
Also, fish oils have protective clinical effects in occlusive cardiovascular disease, for which
patients with RA are at increased risk.Implementation of the clinical use of anti-inflammatory
fish oil doses has been poor. Since fish oils do not provide industry with the opportunities for
substantial profit associated with patented prescription items, they have not received the
marketing inputs that underpin the adoption of usual pharmacotherapies. Accordingly, many
prescribers remain ignorant of their biochemistry, therapeutic effects, formulations, principles of
application and complementary dietary modifications. Evidence is presented that increased
uptake of this approach can be achieved using bulk fish oils. This approach has been used with
good compliance in RA patients. In addition, an index of n-3 nutrition can be used to provide
helpful feedback messages to patients and to monitor the attainment of target levels.Collectively,
these issues highlight the challenges in advancing the use of fish oil amid the complexities of
modern management of RA, with its emphasis on combination chemotherapy applied early.
Conformemente agli effetti biochimici si sono dimostrati effetti
antinfiammatori interessanti con gli oli di pesce alimentari in studi
randomizzati in doppio cieco verso placebo nell’artrite reumatoide
(RA). Gli oli di pesce dimostrano anche effetti clinici di protezione
nei confronti delle patologie cardiovascolari occlusive nel gruppo
di pazienti per i quali la RA rappresenta un maggior rischio.
L’applicazione dell’utilizzo clinico di dosi di oli di pesce
antinfiammatori è limitata. Nella misura in cui gli oli di pesce non
rappresentano per l’industria possibilità di profitti sostanziali del
tipo di quelli associati a prodotti brevettati e sottoposti a
prescrizione, non hanno ricevuto il contributo di marketing che
sostiene l’adozione delle consuete farmacoterapie. Di
conseguenza molti prescrittori restano all’oscuro della loro
biochimica, degli effetti terapeutici, di formulazioni, principi
d’applicazione e modifiche alimentari da associarvi.

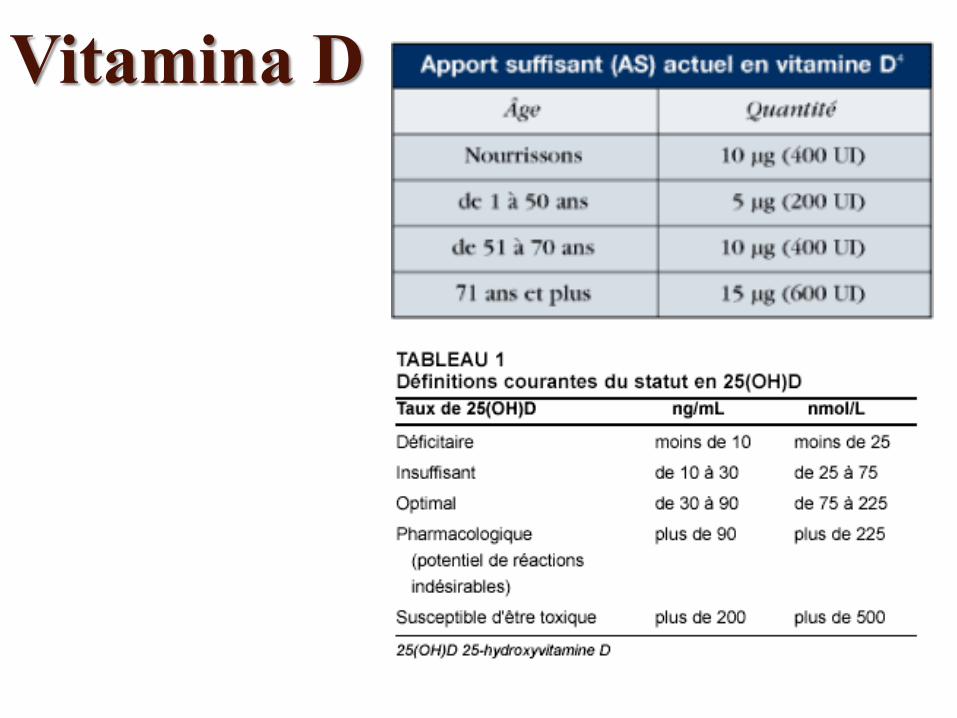
Vitamina D
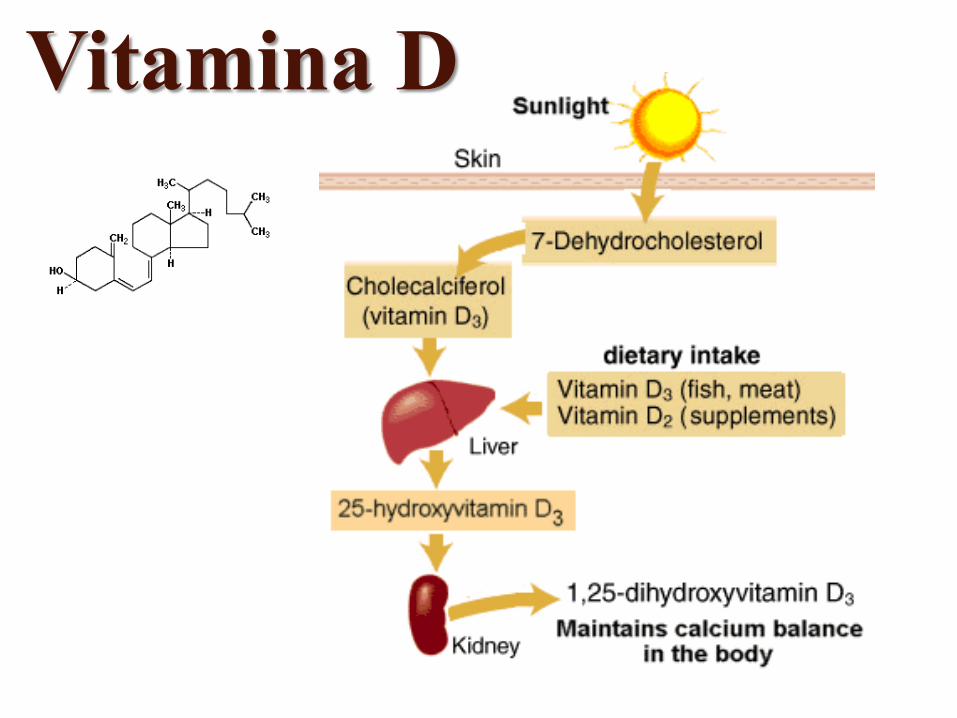
Vitamina D
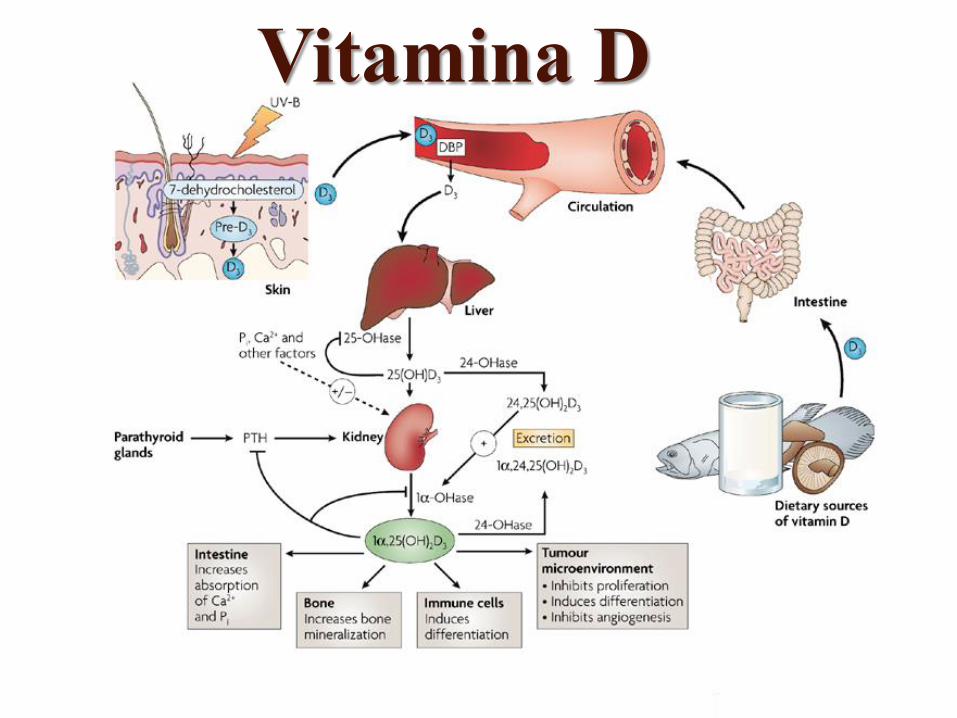
Vitamina D
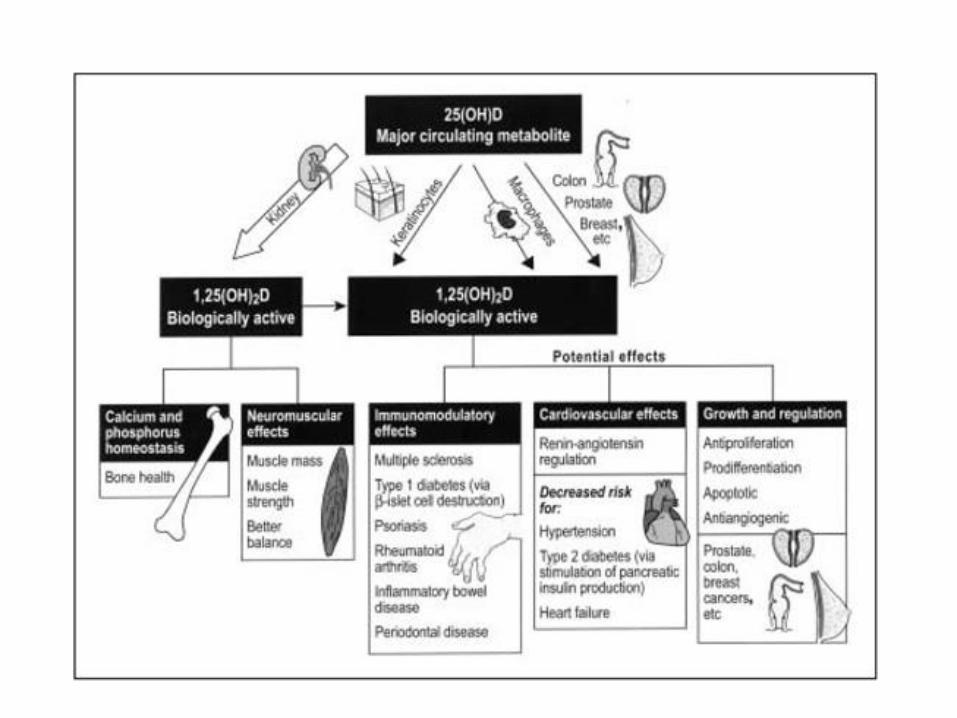
Vitamin D: its role and uses in immunology. Deluca HF, Cantorna MT.
FASEB J. 2001 Dec;15(14):2579-85.
In recent years there has been an effort to understand possible noncalcemic roles of
vitamin D, including its role in the immune system and, in particular, on T cell-
medicated immunity. Vitamin D receptor is found in significant concentrations in the
T lymphocyte and macrophage populations. However, its highest concentration is in
the immature immune cells of the thymus and the mature CD-8 T lymphocytes. The
significant role of vitamin D compounds as selective immunosuppressants is
illustrated by their ability to either prevent or markedly suppress animal models of
autoimmune disease. Results show that 1,25-dihydroxyvitamin D3 can either prevent
or markedly suppress experimental autoimmune encephalomyelitis, rheumatoid
arthritis, systemic lupus erythematosus, type I diabetes, and inflammatory bowel
disease. In almost every case, the action of the vitamin D hormone requires that the
animals be maintained on a normal or high calcium diet. Possible mechanisms of
suppression of these autoimmune disorders by the vitamin D hormone have been
presented. The vitamin D hormone stimulates transforming growth factor TGFbeta-1
and interleukin 4 (IL-4) production, which in turn may suppress inflammatory T cell
activity. In support of this, the vitamin D hormone is unable to suppress a murine
model of the human disease multiple sclerosis in IL-4-deficient mice. The results
suggest an important role for vitamin D in autoimmune disorders and provide a fertile
and interesting area of research that may yield important new therapies.
D-hormone and the immune system. Cantorna MT, Mahon BD.
J Rheumatol Suppl. 2005 Sep;76:11-20.
D-hormone [1,25(OH)2 D3] is an important immune system regulator that has been
shown to inhibit development of autoimmune diseases including experimental
inflammatory bowel disease (IBD), rheumatoid arthritis (RA), multiple sclerosis (MS),
and type 1 diabetes. Paradoxically, other immune mediated diseases (experimental
asthma) and immunity to infectious organisms were not found to be affected by D-
hormone treatment. The effectiveness of D-hormone treatment of autoimmune
diseases is due to inhibition of the development and function of Th1 cells and the
induction of other Th cells including Th2 cells. We report results of microarray
analysis of colons from D-hormone treated mice with experimental IBD. Two hundred
thirty-nine genes were inhibited and 298 genes were upregulated in the colon by D-
hormone treatment of mice with IBD. Of interest was the D-hormone mediated
inhibition of 3 tumor necrosis factor-alpha (TNF-alpha, lipopolysaccharide-induced
TNF-alpha factor, and TNF receptor) related genes in the colon. It is likely that the
effectiveness of D-hormone treatment of experimental autoimmunity is due in part to
the inhibition of the TNF family of genes. D-hormone is a selective regulator of the
immune system, and the outcome of D-hormone treatment depends on the nature
(infectious disease, asthma, autoimmune disease, etc.) of the immune response.
Vitamin D: a natural inhibitor of multiple sclerosis. Hayes CE.
Proc Nutr Soc. 2000 Nov;59(4):531-5.
Inheriting genetic risk factors for multiple sclerosis (MS) is not sufficient to cause this demyelinating
disease of the central nervous system; exposure to environmental risk factors is also required. MS
may be preventable if these unidentified environmental factors can be avoided. MS prevalence
increases with decreasing solar radiation, suggesting that sunlight may be protective in MS. Since
the vitamin D endocrine system is exquisitely responsive to sunlight, and MS prevalence is highest
where environmental supplies of vitamin D are lowest, we have proposed that the hormone, 1, 25-
dihydroxycholecalciferol (1,25-(OH)2D3), may protect genetically-susceptible individuals from
developing MS. Evidence consistent with this hypothesis comes not only from geographic studies,
but also genetic and biological studies. Over-representation of the vitamin D receptor gene b allele
was found in Japanese MS patients, suggesting it may confer MS susceptibility. Fish oil is an
excellent vitamin D source, and diets rich in fish may lower MS prevalence or severity. Vitamin D
deficiency afflicts most MS patients, as demonstrated by their low bone mass and high fracture
rates. However, the clearest evidence that vitamin D may be a natural inhibitor of MS comes from
experiments with experimental autoimmune encephalomyelitis (EAE), a model of MS. Treatment of
mice with 1,25-(OH)2D3 completely inhibited EAE induction and progression. The hormone
stimulated the synthesis of two anti-encephalitogenic cytokines, interleukin 4 and transforming
growth factor beta-1, and influenced inflammatory cell trafficking or apoptosis. If vitamin D is a
natural inhibitor of MS, providing supplemental vitamin D to individuals who are at risk for MS would
be advisable.
Vitamina D
Ripristinare l’ambiente
molecolare originale
Medicina nutrizionale
NF-kB

Le spezie possono bloccare
l’attivazione del NF-κB
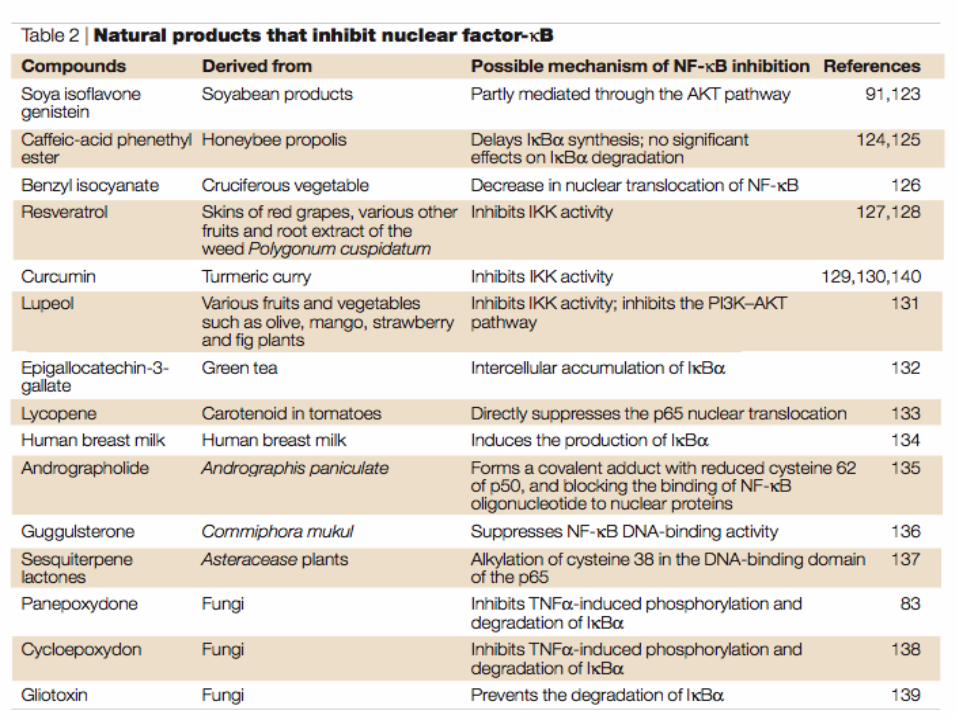
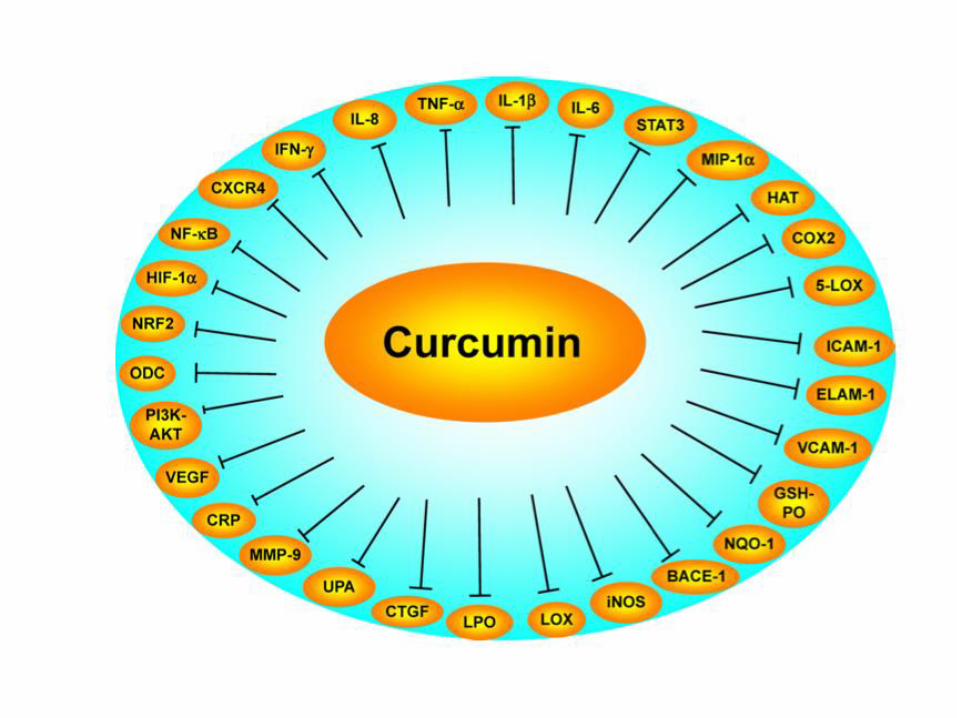
Medicina nutrizionale
Spegnere il fuoco

Valutazione
MALATTIE AUTOIMMUNI Valutazione nutrizionale e funzionale
• Vitamina D
• Microbiota intestinale (Mou)
• Permeabilità intestinale ( IgG
alimentare)
• CRP
• Profilo acidi grassi
• Indicatori stress ossidativo
• Difese antiossidanti
Recommended