Trigeminal Nerve Anatomy And Significance
ByMohamed Kharabish

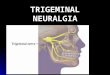
Is the fifth cranial nerve also it is the largest and most complex of the 12 cranial nerves (CNs). It supplies sensations to the face, mucous membranes, and other structures of the head. It is the motor nerve for the muscles of mastication and contains proprioceptive fibers.
Trigeminal Nerve

It exits the brain by a large sensory root and a smaller motor root coming out of the pons at its junction with the middle cerebral peduncle. It passes laterally to join the gasserian (semilunar) ganglion in the Meckel cave.


trigeminal nerve (one on each side of the pons) has three major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). The ophthalmic and maxillary nerves are purely sensory, and the mandibular nerve has sensory (or "cutaneous") and motor functions.

*Ophthalmic branch is sensory
*Maxillary branch is sensory
*Mandibular branch is mixed


Mnemonic for the exit of trigeminal nerve branches
standing: superior orbital fissure (frontal branch of trigeminal nerve)Room: foramen Rotundum (maxillary branch of trigeminal nerve)Only: foramen Ovale (mandibular branch of trigeminal nerve)


Clinical significance of trigeminal
nerve

Trigeminal neuralgia (TN)
Trigeminal neuralgia (TN), also known as tic douloureux, is a distinctive facial pain syndrome that may become recurrent and chronic. It is characterized by unilateral pain following the sensory distribution of cranial nerve V (typically radiating to the maxillary or mandibular area in 35% of affected patients) and is often accompanied by a brief facial spasm or tic..

Signs and symptomsTN presents as attacks of stabbing unilateral facial pain, most often on
the right side of the face. The number of attacks may vary from
less than 1 per day to 12 or more per hour and up to hundreds per day.
Triggers of pain attacks include the following: Chewing, talking, or smiling . Drinking cold or hot fluids . Touching, shaving, brushing
teeth, blowing the nose . Encountering cold air from an
open automobile window .

Pain localization is as follows:
Patients can localize their pain precisely The pain commonly runs along the line dividing either the mandibular and maxillary nerves or the maxillary and ophthalmic portions of the nerve In 60% of cases, the pain shoots from the corner of the mouth to the angle of the jaw In 30%, pain jolts from the upper lip or canine teeth to the eye and eyebrow, sparing the orbit itself In less than 5% of cases, pain involves the ophthalmic branch of the facial nerve

The pain has the following qualities:Characteristically severe, paroxysmal, and lancinating Commences with a sensation of electrical shocks in the affected area Crescendos in less than 20 seconds to an excruciating discomfort felt deep in the face, often contorting the patient's expression Begins to fade within seconds, only to give way to a burning ache lasting seconds to minutes Pain fully abates between attacks, even when they are severe and frequent Attacks may provoke patients to grimace, wince, or make an aversive head movement, as if trying to escape the pain, thus producing an obvious movement, or tic; hence the term "tic douloureux"


Other diagnostic clues are as follows:
Patients carefully avoid rubbing the face or shaving a trigger area, in contrast to other facial pain syndromes, in which they massage the face or apply heat or ice Many patients try to hold their face still while talking, to avoid precipitating an attack In contrast to migrainous pain, attacks of TN rarely occur during sleep

Not TN pain



Etiology

Trigeminal neuralgia (TN) is most likely multifactorial.Most cases of trigeminal neuralgia are idiopathic, but compression of the trigeminal roots by tumors or vascular anomalies may cause similar pain,



Trigeminal neuralgia is divided into 2 categories, classic and symptomatic. The classic form, considered idiopathic, actually includes the cases that are due to a normal artery present in contact with the nerve, such as the superior cerebellar artery or even a primitive trigeminal artery.

To summarize the causes

inflammatory
Vascular
Neoplastic
Idiopathic

Vascular
• AV malformation• Aneurysms• abnormal
vascular course of the superior cerebellar artery

Inflammatory • Meningeal irritation• Multiple sclerosis• Lyme Disease • Sarcoidosis

Neoplastic cerebellopontine angle
tumors

Management


Pharmacological :
Anticonvulsant Agents
Skeletal Muscle Relaxants ((Baclofen (Lioresal, Gablofen))
Tricyclic Antidepressants ((Amitriptyline))
Toxins ((BOTOX))

Carbamazepine (Tegretol)
Carbamazepine is the criterion standard in the medical management of trigeminal neuralgia. A 100-mg tablet may produce significant and complete relief within 2 hours, and, for this reason, a 100 mg twice a day (bid) prescription is suitable to start. If this initial dose fails, one may push the dose to 1200 mg daily (qd), as the patient will tolerate, for initial relief; maintenance doses generally are lower, 100-800 mg daily bid. If using the extended-release caplet, begin with 200 mg qd and increase as needed to a maximum dose of 1200 mg/d bid. Titrating slowly improves tolerance.


Oxcarbazepine (Trileptal)Oxcarbazepine is a close cousin of carbamazepine and presumably works on similar mechanisms. This agent offers a better tolerance and is easier to manage.


Other anti convulsant agents
Gabapentin (Neurontin)
Lamotrigine (Lamictal, Lamictal ODT, Lamictal XR)
Phenytoin (Dilantin, Phenytek)
Topiramate (Topamax)


Non pharmacological
ttt






Recommended