-
Dept. of PathologyMedical CollegeHunan Normal
University()*Chapter 3Acid-Base Balance and Imbalance
*Disorders are big problems in clinic.
http://v.qihuang99.com/player/1777.html?1777-0-2
-
*Acid-Base Balance and Imbalance Acid-base homeostasis
Parameters of acid-base balance Simple acid-base disturbance
Metabolic acidosis Respiratory acidosis Metabolic alkalosis
Respiratory alkalosis
-
The process which is regulated automatically by the body to keep
relatively stable between acidity and basicity.Q: Why balanced
pH?Normal pH range: 7.35 ~ 7.45 Section 1 Acid-base Homeostasis
Outside the acceptable range of pH,proteinsare denatured and
digested,enzymeslose their ability to function, anddeathmay
occur.*
-
Concepts of Acid and Base 2. Base: an acceptor of H+. 1. Acid: a
donor of hydrogen ions ( H+).
Normally, acid substances are much more than alkaline ones, when
people take regular diet. *
-
Acids Volatile acid () Fixed acid ()
-
An acid excreted through the lungs as a gas.Volatile AcidSources
of CO2: Metabolism of biomoleculesCO2H2O
H2CO3
(300-400 L/d)
H+
HCO3-
H2CO3 is the only volatile acid in our body (13-15 mol/d). *
-
Fixed (non-volatile) AcidAcid produced in the body from sources
other than CO2.Excreted by the kidneys.Sources:From proteins:
sulfate, phosphate, urateFrom carbohydrates:
Lactate, pyruvate, glycerateFrom lipids:
Adenylate, pyrophosphate
All acids (except H2CO3) are fixed acids.*
- Bases (Alkali)SourcesAmino acid metabolism (NH3) Fruits and
vegetables Citric acid, maleic acid, oxalic acidWhy bases produced
from acids?Fruits CO2, H2O and ions (e.g., Na+) Bases
-
2. Regulation of Acid-Base Balance Buffer SystemsBloodCellsBone
Lungs Kidneys
Three Levels
-
Buffer systems in the bloodAbility53
5
7
35
All fixed acids can be buffered by these buffer systems. *
-
Bicarbonate/Carbonic Acid Buffer System HCO3-/H2CO3The ratio of
HCO3- vs H2CO3 determines the blood pH.HCl + HCO3- Cl- + H2CO3 CO2
+ H2O NaOH + H2CO3 NaHCO3 + H2O
H2CO3/HCO3- is an open buffer system, because CO2 can be
eliminated from the lungs and HCO3- can be regulated by the
kidneys.*
-
Phosphate Buffer SystemNa2HPO4/NaH2PO4Primarily functions in the
kidneys and the cells.
-
Mainly functions in the cells Protein Buffer System Pr/HPr
-
Hb-/HHbHbO2-/HHbO2Hemoglobin Buffer SystemOnly in RBCRegulates
volatile acid
Hb/HHb functions to regulate volatile (not fixed) acids. *
-
Mechanism of Buffering in the Plasma HCl + NaHCO3 NaCl + H2CO3
CO2 + H2O NaOH + H2CO3 NaHCO3 + H2O
-
Cl-Cl-HCO3-HCO3-Mechanism of Buffering in the Cells
-
Regulation of Acid-Base Balance by the LungsRegulation of
Volatile Acid
-
Regulation Through Chemoreceptors
1) Regulation through central chemoreceptors. PaCO2 (main way)
2) Regulation through peripheral chemoreceptors in the carotid body
and aortic body. PaO2*
-
3. Respiratory Regulation of Acid-Base Balance Pulmonary
regulation Volatile acid
1) Regulation through central chemoreceptors. PaCO2 (main way)
2) Regulation through peripheral chemoreceptors in the carotid body
and aortic body. PaO2
3) Other: nerve reflex regulation, central nervous
regulation.
-
Object: Regulating CO2 eliminated content to keep HCO3- / H2CO3
= 20/1Method: CO2 can freely diffuse across the blood-brain barrier
and result in H+ increased in CSF. The chemoreceptors in medullary
respiratory center are very sensitive to the changes of H+
concentration. Increased H+ can excite respiratory
center.Characteristics PaCO2 (+ breath) 80mmHg (- breath) CO2
anaesthesia (narcosis)Regulation through central chemoreceptors
-
Regulation by the Kidneys Excrete fixed acidsH+-Na+ (NH4+-Na+)
exchange to excrete H+ (or NH4+)Retaining Na+ Maintain plasma
[HCO3-]
Na+-HCO3- co-transported into capillaries
c. The effects of carbonic anhydrase CA on the apical side H+ +
HCO3- H2CO3 CO2 + H2O*
-
Na+
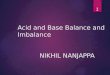
Excretion of H+ and Reabsorption of HCO3- at the proximal tubule
CapillaryEpithelial CellTubuleH2O + CO2H+
Na+H2CO3HCO3-H+CACA: Carbonic anhydrase
-
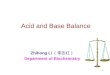
H2O + CO2H+
H2CO3HCO3-H+GlutamineNH3NH4++NH3NH3Na+NH4++Na+Excretion of
NH4+CACapillaryEpithelial CellTubule
-
CellsLungsKidneysPlasmaProduction and Regulation of Acids and
Bases
11.psd
12.bin
CO2 can also bind to HB in the plasma. *
-
Characteristics of Acid-Base RegulationsBuffer systems in the
bloodFast;Buffer effect can not be sustained.Buffer in the
cellsVery strong and fast (34 h);Electrolytes imbalance
(hyperkalemia) may occur.Respiratory RegulationStrong and very fast
(peak in 30 min);Eliminate volatile acid (CO2) [and fixed
acids].Renal RegulationStrong in eliminating fixed acids and
retaining HCO3-; Slow (3-5 days).
-
*Acid-Base Balance and Imbalance Acid-base homeostasis
Parameters of acid-base balance Simple acid-base disturbance
Metabolic acidosis Respiratory acidosis Metabolic alkalosis
Respiratory alkalosis
-
Section 2
Parameters of Acid-Base Balance(Blood Gas Analysis)1. pH2.
PaCO23. SB 4. AB5. BB6. BE7. AG
-
1. pHpH < 7.35: AcidosispH > 7.45: Alkalosis 2. Normal
value 7.35 7.45 (average7.40)
pH is the negative logarithm of H+ concentration. pH is measured
in the artery blood. *
-
Henderson-Hasselbalch Equation= 6.1 + 1.3 = 7.4
-
2. PaCO2Partial pressure of carbon dioxide (CO2) in plasma
(artery) Significance: respiratory parameterNormal Value: 33~46
mmHg (Average: 40PaCO2 : Respiratory Acidosis Metabolic Alkalosis
after compensation
PaCO2 : Respiratory Alkalosis Metabolic Acidosis after
compensation
PaCO2 is mainly regulated by respiration (elimination). PaCO2 is
the best respiratory parameter. The respiratory control of CO2 is
so efficient that CO2 retention does not develop even if CO2
production is largely increased (when respiratory function is
normal). *
-
Normal Value: 2227 mmol/L (Average: 24)3. Standard Bicarbonate,
SBSB : Metabolic Alkalosis SB : Metabolic AcidosisNot affected by
respiration.Only reflecting metabolic factor.
Hb fully oxygenated meaning 100% oxygen saturation. SB increases
also in respiratory acidosis after compensation of the kidneys.SB
decreases also in respiratory alkalosis after compensation of the
kidneys. *
-
Actual Bicarbonate, ABReflecting: Both metabolic and respiratory
factorsNormal Value: the same as SB (24 mmol/L)
AB = [HCO3-]*
-
AB > SB, PaCO2 Respiratory acidosis (metabolic alkalosis
after compensation)AB < SB, PaCO2 Respiratory alkalosis
(metabolic acidosis after compensation)In physiological
situation:AB = SBIn pathological situation: AB SBAB vs. SB
Not necessary to compare between AB and SB, since PaCO2 is the
best respiratory parameter.ABSBABSB*
-
4. Buffer Base, BB Meaning: BB Metabolic alkalosisBB Metabolic
acidosisNormal: 4552 mmol/L (Average: 48 )The sum of all alkaline
buffer substances in plasma (HCO3-, HPO42-, Pr-, Hb-, HbO2-)
Reflects metabolic situation. *
-
5. Base Excess, BEThe amount of a fixed acid or base that must
be added to a blood sample to achieve a pH of 7.4 under standard
condition. Normal value: -3.0 - +3.0
For pH higher than 7.4, an acid must be added the BE value is
positive. *
-
6. Anion GapAG The difference between undetermined anion (UA)
and undetermined cation (UC) in the plasma (AG = UA - UC).AG
(AG>16): Fixed acids(metabolic acidosis)AG: little clinic
meaningAG = Na+ - (Cl- + HCO-3) = 140 - (104 + 24) = 12 mmol/L (10
~ 14 mmol/L)
Na+, Cl-, HCO3- are determined ions. Undetermined anions
include: negatively charged proteins, phosphate, sulfate, lactate,
ketone bodies, etc. *
-
*Acid-Base Balance and Imbalance Acid-base homeostasis
Parameters of acid-base balance Simple acid-base disturbance
Metabolic acidosis Respiratory acidosis Metabolic alkalosis
Respiratory alkalosis
-
pHTypes of Acid-Base Disturbance
-
*Acid-Base Balance and Imbalance Acid-base homeostasis
Parameters of acid-base balance Simple acid-base disturbance
Metabolic acidosis Respiratory acidosis Metabolic alkalosis
Respiratory alkalosis
-
1) Concept 2) Causes* 3) Classification 4) Compensation* 5)
Blood gas parameters 6) Effects on organism* 7) Principles of
treatment1. Metabolic Acidosis (MAc) Metabolic acidosis
-
2. Causes Acids too much
Bases too little Metabolic acidosis is defined as a decrease of
pH induced by primary decrease in plasma HCO3- concentration. 1.
Concept Metabolic acidosis
-
Production of fixed acids Lactic acidosis (
glycolysis)Ketoacidosis ( lipolysis) Excessive intake of acids
Aspirin (acetylsalicylic acid) poisoning Excessive intake of NH4Cl,
etc. 1) Acids too much (consuming HCO3-) Elimination of acidsRenal
failure (GFR)Renal Tubule Acidosis (RTA): excretion of H+ in the
collecting tubule. Hyperkalemia H+-K+ exchange Metabolic
acidosis
RTA type IHypoxia (shock) and some drugs like metformin can
cause lactic acidosis. (by increasing intracellular
glycolysis)NH4Cl is used as the acid to correct metabolic acidosis.
NH4Cl is used as a (expectorant eliminating sputum)*
-
HCO3- loss Loss from intestinal juice(diarrhea) HCO3-
dilutionmassive infusion of glucose or NS in a short time. HCO3-
reabsorption 2) Bases too littleRenal Tubular Acidosis (RTA)
Metabolic acidosis
RTA type II (Inhibition of Carbonic Anhydrase HCO3-
reabsorption)*
-
3. Classification 2) High AG metabolic acidosis primary HCO3- AG
due to any kind of fixed acids except Cl- (Normochloremic MAc)e.g.,
shock, renal failureNormal AG metabolic acidosis
primary HCO3- compensatory of Cl- (Hyperchloremic MAc)HCO3-
losing : diarrhea, intestinal fistulas;HCO3- reabsorption : RTA
Normal Normal AG MAc High AG MAc Metabolic acidosis
*
-
4. Compensation
Pulmonary regulation is a main way in metabolic acidosis.
Metabolic acidosis
Compensation limit by the lungs: PaCO2 = 10 mmHg*
-
Example 1. 1 diabetes patient pH 7.32, HCO3- 15 mmol/L, PaCO2 30
mmHg predict PaCO2 = 1.515 + 82 = 30.52 = 28.532.5 measured PaCO2 =
30, within 28.532.5; Therefore, simple MAcEquationpredict PaCO2 =
1.5[HCO3- ] 82 JudgementIf measured PaCO2 within predicted PaCO2 ,
simple MAcIf measured > predicted maximum, CO2 retention, MAc +
RAcIf measured < predicted minimum, CO2 too less, MAc + RAl
Metabolic acidosis
-
1.2 shock patient with pneumonia: pH 7.26HCO3- 16 mmol/LPaCO2 37
mmHg predicted PaCO2 = 1.516 + 82 = 322 = 3034 measured PaCO2 =37,
exceed predict maximum 34; Therefore, MAc + RAc Metabolic
acidosis
*
-
pH PaCO2
HCO3-
AB
SB BB
BE (negative value increased)(in the case of simple MAc) 5.
Changes of blood gas parameters : Metabolic acidosis
AB < SBTo distinguish the type of acid-base disturbance,
examine pH, PaCO2, HCO3- and AG. *
-
6. Effects on organism1) Cardiovascular system Cardiac
arrhythmias in connection with hyperkalemia Metabolic acidosis
Causes?*
-
Negative inotropic (contractive) action
inhibit the binding of Ca2+ with troponin inhibit the influx of
Ca2+ from extracellular space
inhibit the release of Ca2+ into cytoplasm from endoplasmic
reticulum.H+ directly impairs myocardial contraction
Response of vascular smooth muscle to catecholamine (CA).
Metabolic acidosis
Endoplasmic reticulum in myocardial cells is called sarcoplasmic
reticulum.*
-
2) Central nervous system The main manifestations are
inhibitory: lethargy, disorientation, unconsciousness, or
coma.Mechanism: 4) Respiratory system:deep and rapid respiration (
Kussmauls breathing).3) Osseous system: calcium phosphate in bone
buffers chronic metabolic acidosis rickets and osteodystrophy (in
chronic renal failure).GABA (Gamma-aminobutyric Acid) (inhibitory
neurotransmitter) Glutamate decarboxylasepHGluGABA Metabolic
acidosis
Effect on the nervous system: GABA (=Gamma-aminobutyric Acid)
(inhibitory neurotransmitter).Effect on respiration: H+ excites
respiratory center through peripheral chemoreceptors.*
-
Mechanism of Production of -GABA Metabolic acidosis
-
5) Urinary system Urine is usually acidic in MAc. But:
paradoxical alkaline urine (hyperkalemia) Metabolic acidosis
-
7. Principles of prevention and treatment ) Correction of
underlying disorders. ) Administration of NaHCO3 1.5% NaHCO3 or 1/6
M sodium lactate After the correction of acidosis, attention should
be paid to prevent hypokalemia and convulsion () (induced by
decreased free Ca2+ (hypocalcemia)). 3) Correction of
water-electrolyte disturbances : Metabolic acidosis
Aconvulsionis a medical condition where body muscles contract
and relax rapidly and repeatedly, resulting in an uncontrolled
shaking of the body.*
-
Hypocalcemia convulsion Metabolic acidosis
This happens in metabolic acidosis or alkalosis?*
-
H+: hydrogen ion H+: hydrogen ionsK+: potassium ionsNa+: sodium
ionsCl-: chloride ionsCa2+:Calcium ionsNH4+: ammonium
ionsHCO3-:bicarbonate ionsHPO2- :phosphatic ionsCO2: carbon
dioxideH2CO3:carbonic acidNH3: ammonia
mmol: millimolnmol: nanomolmmHg: millimetre of mercury
column
*Disorders are big problems in clinic.
http://v.qihuang99.com/player/1777.html?1777-0-2Outside the
acceptable range of pH,proteinsare denatured and
digested,enzymeslose their ability to function, anddeathmay
occur.*Normally, acid substances are much more than alkaline ones,
when people take regular diet. *H2CO3 is the only volatile acid in
our body (13-15 mol/d). *All acids (except H2CO3) are fixed
acids.*Fruits (even tasted acid) can be metabolized to CO2, H2O and
inorganic ions (such as Na). The latter becomes base when dissolved
in water. *All fixed acids can be buffered by these buffer systems.
*H2CO3/HCO3- is an open buffer system, because CO2 can be
eliminated from the lungs and HCO3- can be regulated by the
kidneys.*Hb/HHb functions to regulate volatile (not fixed) acids. *
1) Regulation through central chemoreceptors. PaCO2 (main way) 2)
Regulation through peripheral chemoreceptors in the carotid body
and aortic body. PaO2* c. The effects of carbonic anhydrase CA on
the apical side H+ + HCO3- H2CO3 CO2 + H2O*CO2 can also bind to HB
in the plasma. *pH is the negative logarithm of H+ concentration.
pH is measured in the artery blood. *PaCO2 is mainly regulated by
respiration (elimination). PaCO2 is the best respiratory parameter.
The respiratory control of CO2 is so efficient that CO2 retention
does not develop even if CO2 production is largely increased (when
respiratory function is normal). *Hb fully oxygenated meaning 100%
oxygen saturation. SB increases also in respiratory acidosis after
compensation of the kidneys.SB decreases also in respiratory
alkalosis after compensation of the kidneys. *AB = [HCO3-]*Not
necessary to compare between AB and SB, since PaCO2 is the best
respiratory parameter.ABSBABSB*Reflects metabolic situation. *For
pH higher than 7.4, an acid must be added the BE value is positive.
*Na+, Cl-, HCO3- are determined ions. Undetermined anions include:
negatively charged proteins, phosphate, sulfate, lactate, ketone
bodies, etc. *RTA type IHypoxia (shock) and some drugs like
metformin can cause lactic acidosis. (by increasing intracellular
glycolysis)NH4Cl is used as the acid to correct metabolic acidosis.
NH4Cl is used as a (expectorant eliminating sputum)*RTA type II
(Inhibition of Carbonic Anhydrase HCO3- reabsorption)*
*Compensation limit by the lungs: PaCO2 = 10 mmHg*
* AB < SBTo distinguish the type of acid-base disturbance,
examine pH, PaCO2, HCO3- and AG. *Causes?*Endoplasmic reticulum in
myocardial cells is called sarcoplasmic reticulum.*Effect on the
nervous system: GABA (=Gamma-aminobutyric Acid) (inhibitory
neurotransmitter).Effect on respiration: H+ excites respiratory
center through peripheral chemoreceptors.*Aconvulsionis a medical
condition where body muscles contract and relax rapidly and
repeatedly, resulting in an uncontrolled shaking of the body.*This
happens in metabolic acidosis or alkalosis?*