Embed Size (px)
Citation preview

Surg Today (2011) 41:837–840DOI 10.1007/s00595-010-4366-1
Case Report
Sentinel Lymph Node Biopsy in Patients with Male Breast Carcinoma: Report of Two Cases
MASAHIRO KITADA, KEISUKE OZAWA, KAZUHIRO SATO, SATOSHI HAYASHI, and TADAHIRO SASAJIMA
Department of Surgery, Asahikawa Medical University, 2-1-1-1 Midorigaoka-Higashi, Asahikawa, Hokkaido 078-8510, Japan
AbstractThe incidence of male breast cancer is low, and treat-ment strategies similar to those used for female breast cancer patients are frequently used for male patients. However, the safety and utility of sentinel lymph node biopsies (SLNBs) for male breast cancer have not been proven. Among the fi ve cases of male breast cancer who received surgery at our hospital, mastectomy with SLNB was performed in two of the cases. The fi rst patient was 77 years old and the second was 74 years old, and both presented as outpatients with chief complaints of a mammary mass. Clinical diagnoses were T1N0 in both cases, and mastectomies with SLNB were performed. The sentinel lymph node was identifi ed using the dye method. Postoperatively, the patients were hormone receptor-positive, and they are now being followed while continuing to take oral tamoxifen.
Key words Male breast cancer · Sentinel lymph node biopsy
Introduction
Recently the number of cases of breast cancer has increased, but clinical advances in the treatment of breast cancer have also been made, including improved breast conservation rates and increased use of sentinel lymph node biopsy (SLNB), molecular targeted therapy, and preoperative chemotherapy (primary systemic therapy). Conversely, male breast cancer is a rare disor-der, accounting for <1% of all breast cancers, making it diffi cult to conduct large-scale clinical trials or establish an optimal standard of care. However, treatment strate-
gies similar to those used for female breast cancer typi-cally provide successful effects and similar toxicity to that observed in women. In addition, lymph node dis-section and SLNB have been reported in some preop-erative N0 patients. In our hospital, among the 1230 surgeries performed for breast cancer between January 2000 and December 2009, fi ve (0.41%) were male breast cancer patients. This paper reviews the surgical proce-dure selected for these fi ve patients, as well as their breast tumor tissue type and their histopathological diagnosis. We also report the details for two patients who received SLNB, both of whom were found to be lymph node negative during the preoperative diagnosis.
Case Reports
Male Breast Cancer Surgical Cases
The mean age of male breast cancer patients was higher (74.1 years) than for females (51.4 years) with breast cancer. One patient showed intracystic papillary carci-noma. In all cases, masses were palpable and identifi ed on ultrasonography. The cytology was class 3 in the patient with intracystic papillary carcinoma and class 5 in the other four patients. In the patient with class 3 disease, an excisional biopsy of the mass was performed for defi nitive diagnosis. All fi ve patients underwent a mastectomy, and SLNB was performed in two cases (cases 3 and 4).
The tissue type was found to be intracystic papillary carcinoma in one patient, papillotubular carcinoma in one patient, and solid-tubular carcinoma in three patients. Patient 1 (who had intracystic papillary carci-noma) had stage TisN0 disease, Patient 2 was classifi ed as having T4bN1, patient 5 as having T2N1, and patients 3 and 4 were classifi ed as having T1N0 disease. Patients 3 and 4 underwent SLNB. All fi ve patients were hormone
Reprint requests to: M. KitadaReceived: April 5, 2010 / Accepted: June 30, 2010

838 M. Kitada et al.: SLNB in Patients with Male Breast Carcinoma
receptor-positive, and all received oral tamoxifen as postoperative chemotherapy. One patient died 4 years 3 months after surgery due to another disease. The remaining patients have survived without recurrence (Table 1).
Cases of Patients Who Underwent SLNB
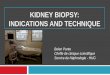
Case 1: 77-Year-Old ManIn early June of 2009, the patient noticed a mammary mass and was evaluated in the outpatient breast clinic. Fine-needle aspiration cytology revealed class V disease. The patient was being followed for Hunt’s syndrome. His height was 174 cm and his weight 64 kg. Breast examina-tion of the right E area showed a 1.5 × 1.8-cm elastic-hard, well-defi ned, somewhat poorly mobile mass. No axillary lymph nodes were palpable. Ultrasonography showed a lobulated solid mass in the right breast. The interior was hypoechoic, the margins were partially irregular and indistinct, posterior echoes were enhanced, halo(+), and the patient was given a diagnosis of category 4 disease (Fig. 1a). Computed tomography revealed a mass in the right breast, but no enlargement of axillary or cervical lymph nodes (Fig. 1b). In addition, no evidence of distant metastasis was seen. The patient was diagnosed as having stage T1N0M0 disease, and a mastectomy with SLNB (using the dye method with measurement of indocyanine green [ICG] fl uorescence) was performed. On intraop-erative rapid pathologic diagnosis, the sentinel node (SN) showed no metastases (2/0), and therefore we carried out a sampling resection around the SN while an axillary lymph node dissection was omitted. The patient’s histopathological diagnosis was p-stage (T1cN0(sentinel node(0/2), level I (0/1)M0), papillotubular carcinoma, Grade I, ly(−) v(−), 1.4 cm, n(−), ER(2+), PgR(3+), HER2(−). Postoperatively, the patient has been treated with oral tamoxifen. As of the time of writing, no signs of recurrence have been identifi ed.
Case 2: 74-Year-Old ManStarting in February of 2009, the patient noticed a lump below the left nipple that gradually increased in size. He was evaluated at our hospital in June of 2009.
Fine-needle aspiration cytology revealed class V disease. During this same period, in February 2009, the patient underwent a total gastrectomy for gastric cancer (p-stage I). The patient’s height was 165 cm and weight 72 kg. Breast examination of the BD area below the nipple showed a 2.5 × 3.0-cm elastic-hard, well-defi ned, poorly mobile mass. No enlarged axillary lymph nodes were
Table 1. Cases of male breast cancer
Case Age (years) Pathology Surgery Stage T N Grade ER PgR HER2
1 65 Papi-tub Bt+Ax 1 1 — 1 1+ 2+ 3+2 81 Solid-tub Bt+Ax 3b 4b 1 3 2+ 1+ —3 77 Papi-tub Bt+SN 1 1 — 1 2+ 3+ —4 74 Solid-tub Bt+SN 1 1 — 2 3+ 2+ 2+5 78 Solid-tub Bt+Ax 3b 4b 1 3 3+ — 2+
Papi-tub, papillotubular carcinoma; solid-tub, solid tubular carcinoma; Bt, breast resection; Ax, dissection of axillary lymph node; SN, sentinel node sampling resection; ER, estrogen receptor; PgR, progesterone receptor; HER2, human epidermal growth factor receptor 2
a
b
Fig. 1. a Ultrasonography showed a solid mass in the right breast. b Chest computed tomography revealed a mass in the right breast

M. Kitada et al.: SLNB in Patients with Male Breast Carcinoma 839
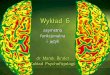
evident. Ultrasonography showed an isoechoic mass with a solid interior. The margins were generally well defi ned, with some partial irregularity (Fig. 2a). Com-puted tomography revealed a mass in the left breast, but no enlargement of axillary or cervical lymph nodes (Fig. 2b). No metastases to other organs were identifi ed. Stage T2N0M0 disease was diagnosed, and a mastec-tomy with SLNB was performed. Intraoperative patho-logical diagnosis showed no lymph node metastases, and therefore we performed a sampling resection around the SN, and an axillary lymph node dissection was omitted. The patient’s histopathological diagnosis was stage I (T1cN0(sentinel node(0/2), level I (0/3))M0), solid-tubular carcinoma, grade II, 1.7 cm, ly(+), v(−), ER(3+), PgR(2+), HER2(2+), n0(0/2). His postopera-tive course was satisfactory, and tamoxifen was admin-istered orally. No signs of recurrence have been seen to date.
Discussion
The overall number of breast cancer cases is increasing, but male breast cancer remains rare, accounting for <1% of all breast cancers.1 In our case experience over the last 10 years, the incidence has only been 0.41%. Causes of male breast cancer include Klinefelter’s syn-drome, gynecomastia, trauma, and effects of irradiation, but no specifi c etiology was apparent in any of our patients. In terms of past medical history, one patient had multiple cancers of the stomach. All patients had noticed the masses themselves and were diagnosed within 6 months. With regard to diagnosis, the masses were readily detectable on ultrasonography. Four patients had solid masses with class 5 cytology. One patient with intracystic papillary carcinoma had class 3 cytology, so an excisional biopsy was performed.
In male breast cancer surgery, because males have little breast tissue, breast-conservation surgery is of little signifi cance. A mastectomy is performed in most cases, but few established reports have described minimal axillary dissection. In early-stage N0 breast cancer in women, SLNB is already used as standard care in many medical centers. The safety and usefulness of SLNB has also been reported for male patients.2–4 In addition, although few data are available, the American Society of Clinical Oncology guidelines recommend that SLNB be performed the same as in female breast cancer.5 We currently use dye injection of ICG with subsequent measurement of fl uorescence to differenti-ate malignant from normal lymph nodes. For intraop-erative rapid pathological diagnosis, the SNs are sliced at 2-mm intervals and stained with hematoxylin and eosin. We performed the same procedure in our two male breast cancer patients. The SNs were identifi ed, and no false negatives were observed.
The postoperative course of treatment for male patients is also the same as in female breast cancer.6 Hormone receptor positivity tends to be higher than in women, and tamoxifen is the mainstay of treatment.7 However, hormone-sensitivity patterns in male breast cancer are thought to be similar to postmenopausal breast cancer, and because aromatase activity in male breast cancer tissue is higher than in females, it is not surprising that aromatase inhibitors have been shown to be effective against male breast cancer.8,9 Although the number of cases seen at our institution was small, and no results have yet been achieved that will lead to standard-ized treatment, the use of SLNB should continue to be investigated in the future, including for recurrent cases.
References
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics. CA Cancer J Clin 2007;57:43–66.
a
b
Fig. 2. a Ultrasonography showed a solid mass in the left breast. b Chest computed tomography revealed a mass in the left breast

840 M. Kitada et al.: SLNB in Patients with Male Breast Carcinoma
2. Cimmino VM, Degnim AC, Sabel MS, Diehl KM, Newman LA, Chang AE. Effi cacy of sentinel lymph node biopsy in male breast cancer. J Surg Oncol 2004;86:74–7.
3. Boughie JC, Bedrosian I, Meric-Bernstam F, Ross MI, Kuerer HM, Akins JS, et al. Comparative analysis of sentinel lymph node opera-tion in male and female breast cancer patients. J Am Coll Surg 2006;203:474–80.
4. Flynn LW, Park J, Patil SM, Cody HS III, Port ER. Sentinel lymph node biopsy is successful and accurate in male breast carcinoma. J Am Coll Surg 2008;206:616–21.
5. Lyman GH, Builiano AE, Somerfi eld MR, Clarke-Pearson D, Flowers C, Jahanzeb M, et al. American Society of Clinical Oncol-ogy guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol 2005;23:7703–20.
6. Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is male breast cancer similar or different than female breast cancer? Breast Cancer Res Treat 2004;83:77–86.
7. Friedman MA, Hoffman PG, Dandolos EM, Lagios MD, Johnston WH, Siiteri PK. Estrogen receptors in male breast cancer: clinical and pathologic correlations. Cancer 1981;47:134–7.
8. Zabolotny BP, Zalai CV, Meterissian SH. Successful use of letrozale in male breast cancer; a case report and review of hormonal therapy for male breast cancer. J Surg Oncol 2005;90:26–30.
9. Giordano SH, Valero V, Buzdar AU, Hortobagyi GN. Effi cacy of anastrozole in male breast cancer. Am J Clin Oncol 2002;25:235–7.