Embed Size (px)
Citation preview

Addressing Maternal Mortality in Malawi through Maternal
Death Audits
Jennifer Weiss, MPH Health and Nutrition Coordinator,
Concern Worldwide Malawi
CORE Global Health Practitioner Conference,
Spring 2015
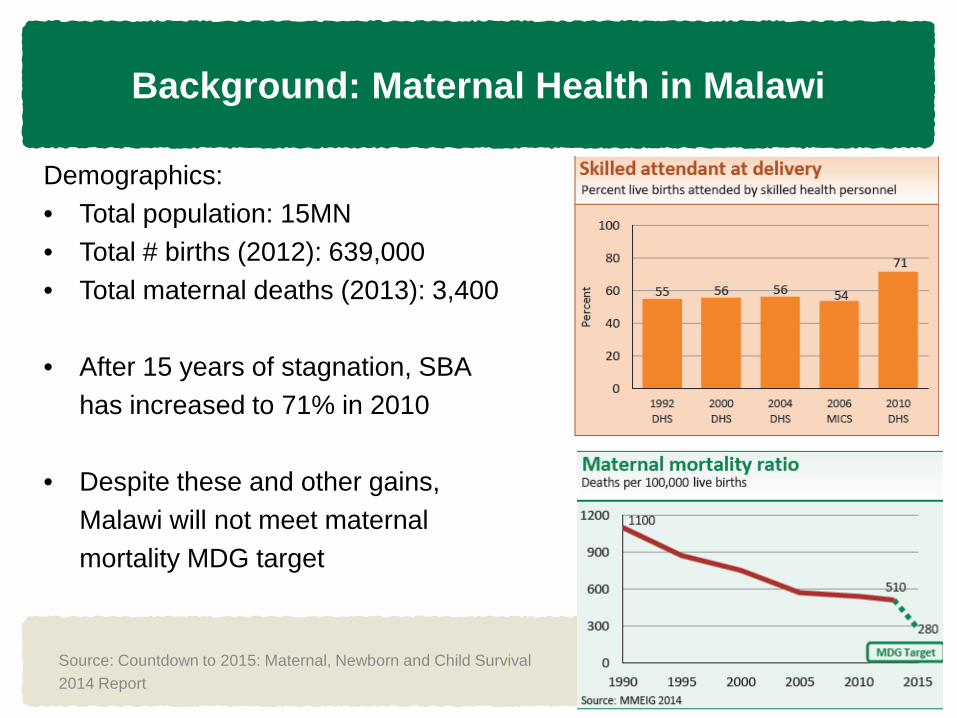
Background: Maternal Health in Malawi
Demographics: • Total population: 15MN • Total # births (2012): 639,000 • Total maternal deaths (2013): 3,400 • After 15 years of stagnation, SBA
has increased to 71% in 2010 • Despite these and other gains,
Malawi will not meet maternal mortality MDG target
Source: Countdown to 2015: Maternal, Newborn and Child Survival 2014 Report
Background: Maternal Health in Malawi
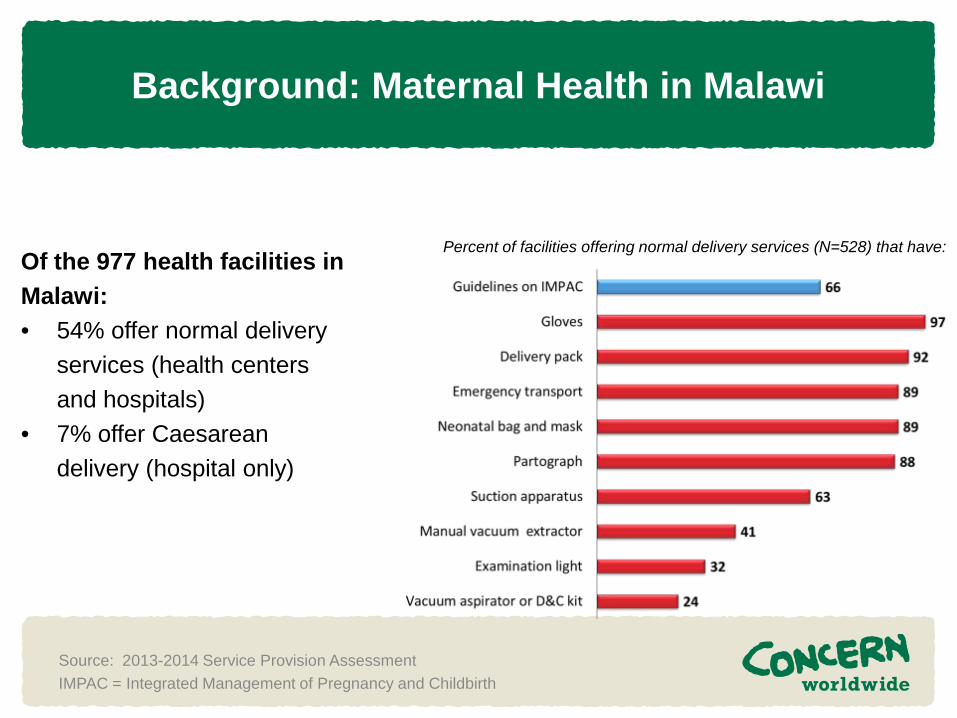
Of the 977 health facilities in Malawi: • 54% offer normal delivery
services (health centers and hospitals)
• 7% offer Caesarean delivery (hospital only)
Source: 2013-2014 Service Provision Assessment IMPAC = Integrated Management of Pregnancy and Childbirth
Percent of facilities offering normal delivery services (N=528) that have:
Background: Maternal Health in Malawi
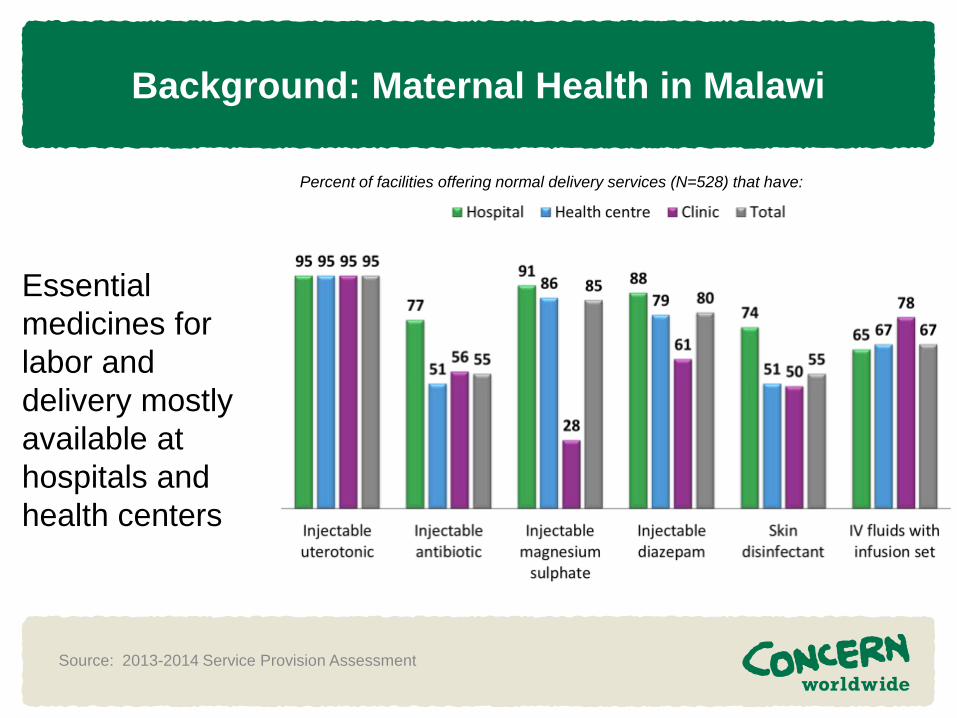
Percent of facilities offering normal delivery services (N=528) that have:
Source: 2013-2014 Service Provision Assessment
Essential medicines for labor and delivery mostly available at hospitals and health centers
Project Overview
• Project Name: Improving Opportunities
and Use of Reproductive Health Among Women and Youth (OUR WAY)
• Dates: 2013-2016 • Location: Nkhotakota District, Central
Region, Malawi • Donors: Scottish Government, Merck for
Mothers, Elizabeth Taylor AIDS Foundation
Project Overview
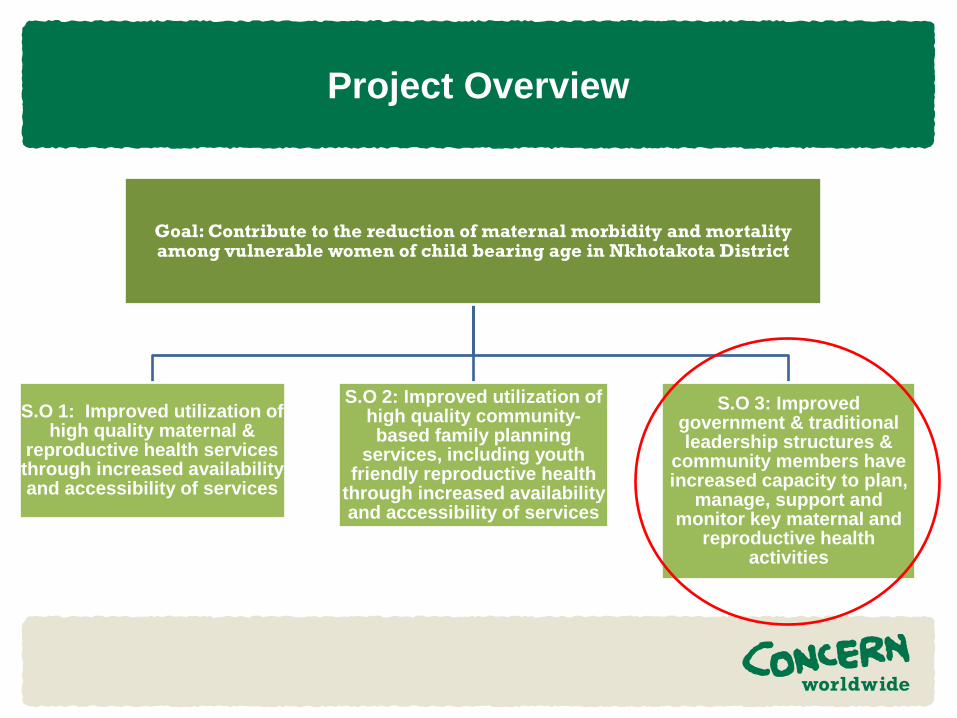
Goal: Contribute to the reduction of maternal morbidity and mortality among vulnerable women of child bearing age in Nkhotakota District
S.O 1: Improved utilization of high quality maternal &
reproductive health services through increased availability and accessibility of services
S.O 2: Improved utilization of high quality community-based family planning
services, including youth friendly reproductive health
through increased availability and accessibility of services
S.O 3: Improved government & traditional leadership structures &
community members have increased capacity to plan,
manage, support and monitor key maternal and
reproductive health activities
Maternal Death Surveillance and Response (MDSR) in Malawi
• 2003: Maternal death reviews commenced at
district hospitals • Maternal deaths made notifiable event in 2009 • In 2013, MOH Reproductive Health Department
moved to more robust system of MDSR: • Form of continuous surveillance linking health
information system and quality improvement processes
• Promotes routine identification and timely notification of maternal deaths
• Helps in quantification and determination of causes and avoidability of maternal deaths.
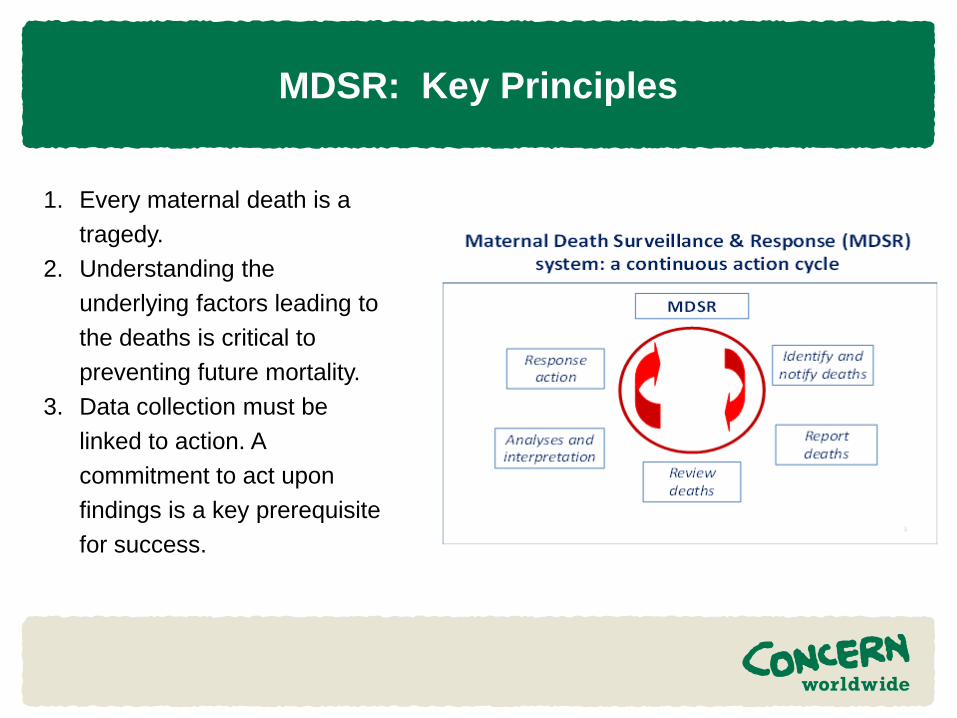
MDSR: Key Principles
1. Every maternal death is a tragedy.
2. Understanding the underlying factors leading to the deaths is critical to preventing future mortality.
3. Data collection must be linked to action. A commitment to act upon findings is a key prerequisite for success.
MDSR Processes: Facility Level
• Facilitated by District Safe Motherhood Coordinator
• Attending clinicians at delivery present results
• Participation by NGOs, health facility safe motherhood committee
• Ideally takes place within two weeks of death
• Tone is participatory and constructive
• After audit, there is report and recommendations made to DHO.
• Findings also shared with each health facility safe motherhood committee
Dr. Wanangwa Chisenga and his team at the Nkhotakota District Hospital
MDSR Processes: Facility Level Top Three Issues Identified: 1. Referrals from health centers to hospital
• Triage by hospital switchboard operator – how to prioritize where to send ambulance?
• Who accompanies woman to hospital (in ambulance or private vehicle)?
• Lack of documentation (clinician’s notes, partographs) during referrals
• Time from onset of complications to the decision to make referral
2. Lack of training for attending clinician 3. Laboratory capacity, specifically
around availability of blood (lack of storage for re-agents, power cuts)
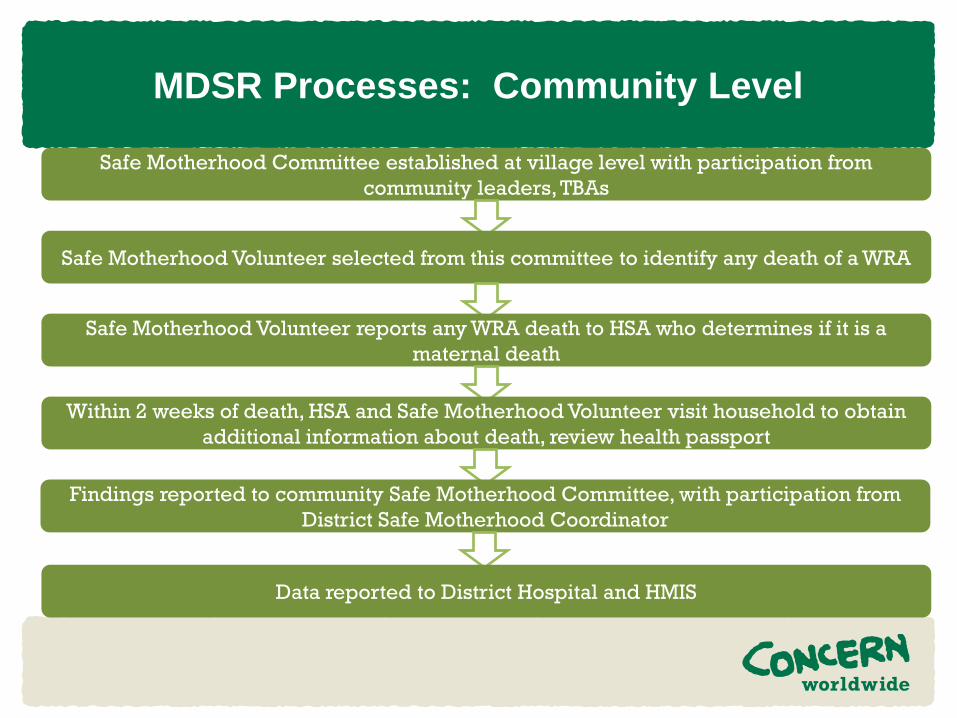
MDSR Processes: Community Level
Safe Motherhood Committee established at village level with participation from community leaders, TBAs
Safe Motherhood Volunteer selected from this committee to identify any death of a WRA
Safe Motherhood Volunteer reports any WRA death to HSA who determines if it is a maternal death
Within 2 weeks of death, HSA and Safe Motherhood Volunteer visit household to obtain additional information about death, review health passport
Findings reported to community Safe Motherhood Committee, with participation from District Safe Motherhood Coordinator
Data reported to District Hospital and HMIS
MDSR Processes: Community Level
• Community MDSR process not yet fully implemented. Key learning to date: • Sensitization of communities is
critical. Traditionally, maternal deaths are not discussed, especially during the grieving period. Sensitization must focus on how the MDSR process will help reduce maternal deaths.
• Focus away from diagnosing clinical cause of death but rather on ‘actionable intelligence’, identifying who influenced decisions during delivery
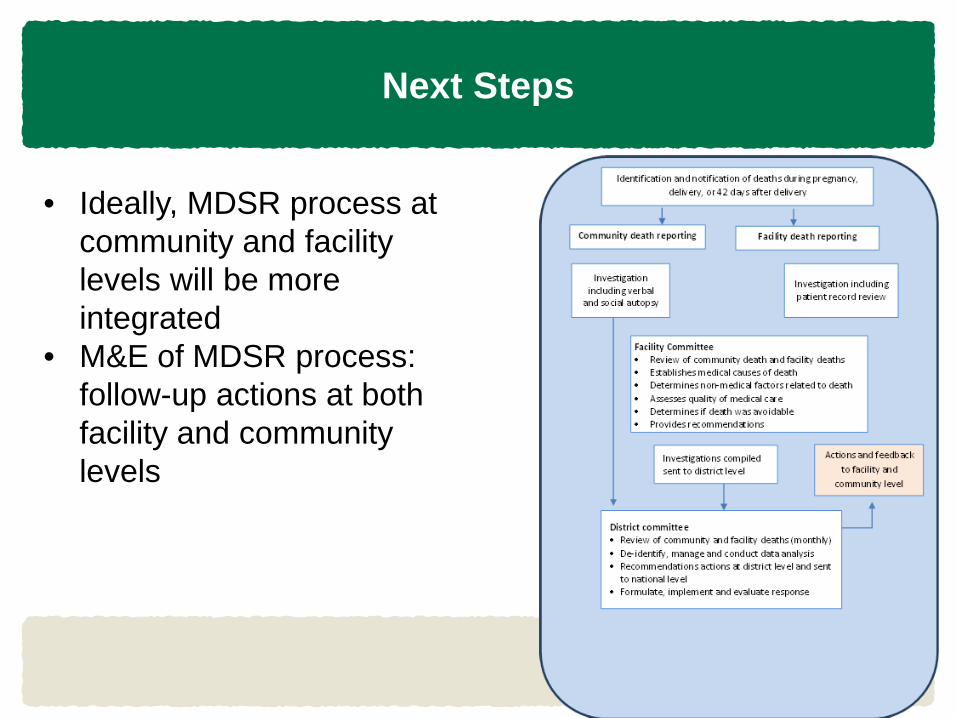
Next Steps
• Ideally, MDSR process at community and facility levels will be more integrated
• M&E of MDSR process: follow-up actions at both facility and community levels
Thank you
Mida Mateketa with her husband Kenneth at their home in Mandindi village, Malawi. Mida spent six weeks in the district hospital following complications during the delivery of her child.