Embed Size (px)
Citation preview

1
Muscle Soreness and Damage
Dr Alison Jenkinson
SR2002

2
Outline
• Muscle damage
• Delayed onset muscle soreness (DOMS)
• Measurement of muscle damage
• Repeated bout effect

3
Exercise Induced Muscle Damage
A single bout of unaccustomed eccentric exercise can cause symptoms of muscle damage loss of contractile force pain/soreness (delayed onset) muscle tenderness swelling reduced range of movement

4
Muscle Damage• Suggested causes of muscle damage
– mechanical• disruption of sarcomeres
– temperature• structural and/or metabolic alterations influenced by
higher local muscle temperature
– metabolic/chemical• impaired mitochondrial respiration
• increased free radical production

5
Suggested Causes• Mechanism of muscle damage are unclear
• Eccentric contractions use fewer motor units than concentric contractions to produce a given force– therefore there is a greater force per unit area in
the active muscle fibres ie greater stress
• May disrupt the sarcolemma, sarcoplasmic reticulum and myofibrillar structures

6swollen mitochondria
Structural damage
sarcolemmal disruptiondilated transverse
(T) tubules
distortion of myofibrillar components
fragmented sarcoplasmic reticulum
lesions of the plasma membrane
cytoskeletal
damage
changes in the extracellular
myofibre matrix

7
Muscle Damage• However, the differences in the time course
of markers of muscle damage suggest that mechanical damage is not the only cause of muscle damage
• Therefore other processes – mechanical– temperature– metabolic/chemical
may also be involved

8
Muscle Damage• Damage to muscle can produce a range of
symptoms– increased plasma enzymes eg creatine kinase– increased myoglobin– increased protein metabolites– structural damage to muscle fibres
• can be assessed by light and electron microscopy
– temporary impairment of muscle function

9
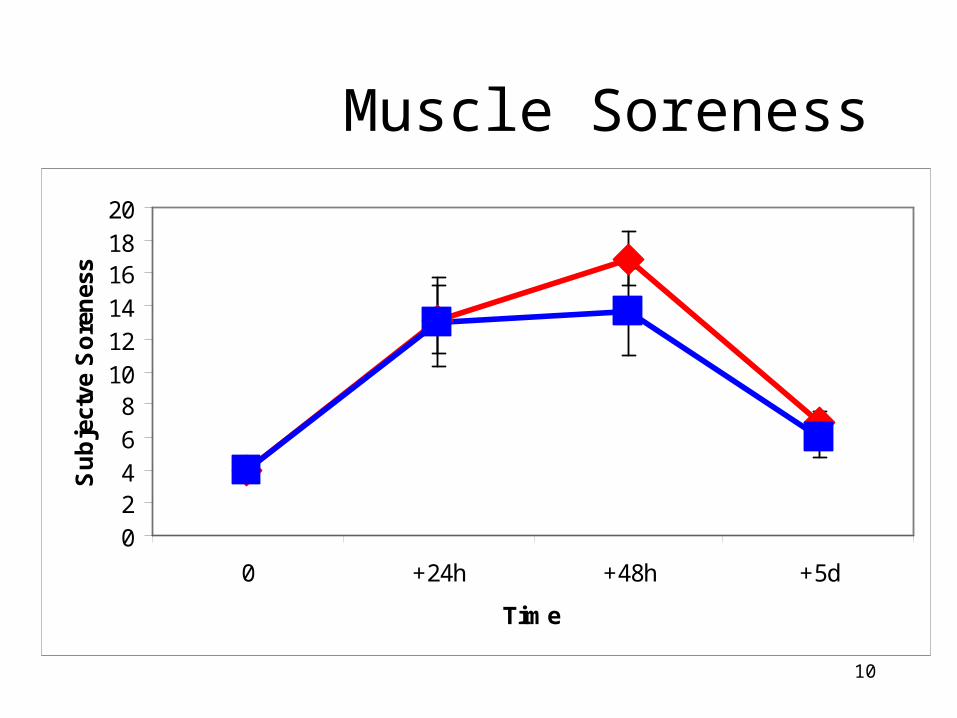
DOMS• The perception of muscle soreness often does not
become evident until 24h to 48h after exercise.• Peak soreness appears to occur at 2-3d after
exercise• Delayed-Onset Muscle Soreness (DOMS)• Discomfort usually subsides by 5-7d after
exercise• Generally measured subjectively
10
Muscle Soreness• ?
02468101214161820
0 +24h +48h +5d
Time
Su
bje
ctve
So
ren
ess

11
Creatine Kinase
• When muscle fibres become damaged creatine kinase can diffuse through holes in the plasma membrane of the muscle cell and appear in the circulation
• The presence of increased concentrations of this enzyme in the serum or plasma demonstrates the presence of muscle damage

12
• Plasma creatine kinase activity may not increase until 48h after exercise with peak levels occurring up to 7d after specific eccentric exercise
• Static isometric exercise may significantly increase plasma CK within 3-6h and peak around 18-24h
Schematic of CK Response to Exercise
0
200
400
600
800
1000
1200
1400
0 1 2 3 4 5 6 7 8
Days after Exercise
Pla
sm
a C
K U
/L
Eccentric Exercise
Isometric Exercise

13
Creatine Kinase• ?
0
100
200
300
400
500
600
700
800
0 +24h +48h +5d
Time
U/L

14
Creatine Kinase
• Downhill running (which also involves muscle shortening concentric contractions) also tends to have a peak CK response around 24h
• Concentric v Eccentric exercise?– Specific eccentric exercise results in more marked
increases in CK than isometric exercise, concentric exercise and downhill running
– Specific eccentric exercise appears to produce extensive muscle damage

15
Creatine Kinase• There is a large amount of variation between
individuals in their CK response to exercise– Peak concentration of CK can vary– Time to peak concentration can vary
• May be related to – gender– age– race– level of training

16
Muscle Damage• Some markers of muscle damage
(not requiring muscle biopsy samples)– creatine kinase– subjective muscle soreness– force production
• loss of force production
• recovery of force production
– range of movement
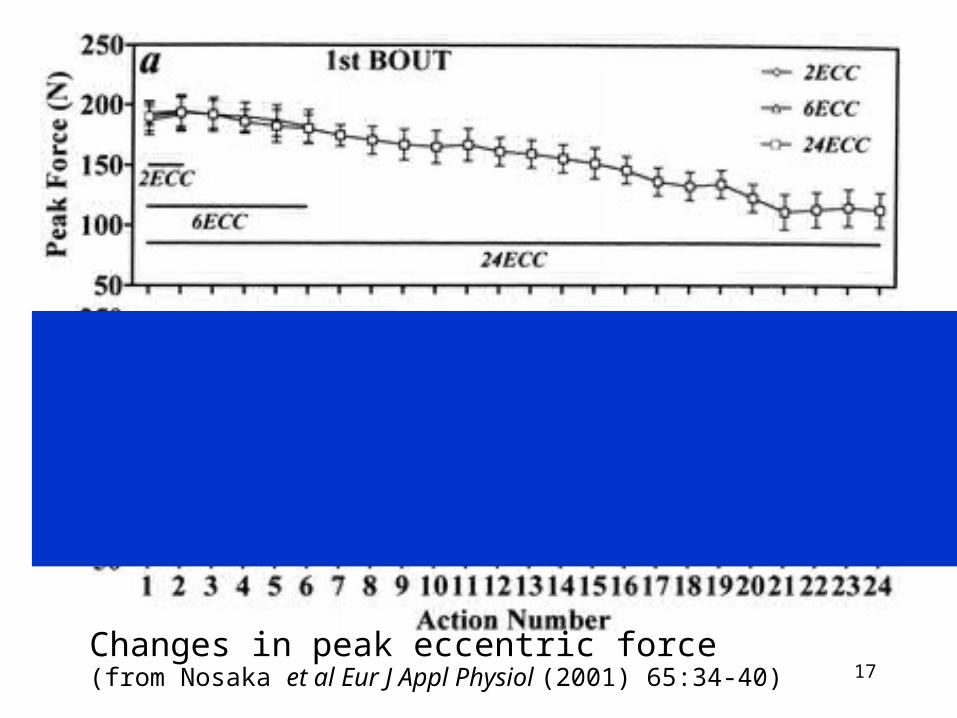
17Changes in peak eccentric force (from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

18Changes in maximal isometric force (from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

19Changes in muscle soreness (from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

20Changes in plasma creatine kinase activity(from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

21Changes in peak eccentric force (from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

22Changes in maximal isometric force (from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

23Changes in muscle soreness (from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)

24Changes in plasma creatine kinase activity(from Nosaka et al Eur J Appl Physiol (2001) 65:34-40)
25
Repeated Bout Effect Amount of muscle damage influenced by the
number of maximal eccentric contractions Repeated bouts of eccentric contractions
appear to offer some protection against muscle damage in subsequent bouts.
Adaptation and protection against damage after a second bout of exercise appears to be possible from as few as 2 contractions in the 1st bout

26
Summary
• Although the mechanisms of muscle damage are unclear it seems likely that there is some physical damage in response to eccentric exercise
• Followed by other metabolic processes leading to alterations in CK and DOMS
• Training (repeated bouts) appears to reduce the muscle damaging effects