Embed Size (px)
Citation preview
Bone Tumor
&
Tumor-like lesions
By : dr. Manal Nageeb

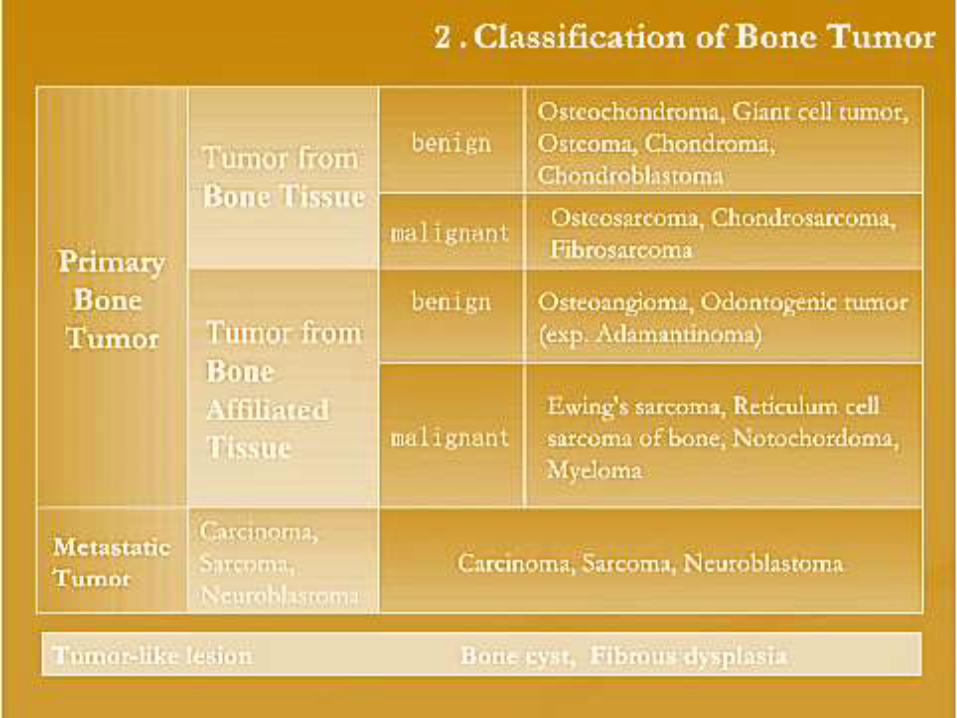
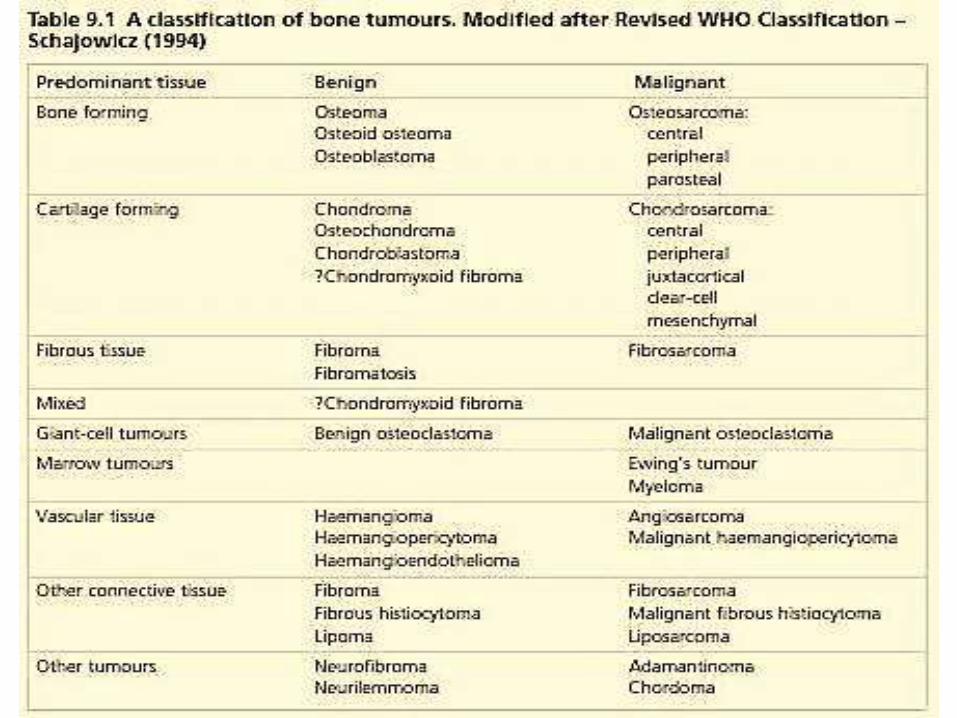
tumor OR tumor-like lesion .“classification”>Types
> Dx in general .
>DDx .
>staging .
>principle ttt in general .
>specific .
Aim :


Diagnosis :
> Clinical presentation 1- History
2- examination
> Imaging >> X-Ray
>BIOPSY
> Laboratory investigation
- Asymptomatic >> more likely with benign Lesions
>>Malignant tumors, too, may remain silent if they are
slow-growing and situated where there is room for
inconspicuous expansion (e.g. the cavity of the pelvis).
- Age
- Pain
- Swelling
- Neurological symptoms
- Pathological fracture
HISTORY:

* If there is a lump,
Where does it arise?
Is it discrete or ill-defined?
Is it soft or hard, or pulsatile?
And is it tender?
EXAMINATION :
X-RAYSQUESTIONS TO ASK WHEN STUDYING AN
X-RAY
Is the lesion solitary or are there multiple lesions?
What type of bone is involved?
Where is the lesion in the bone?
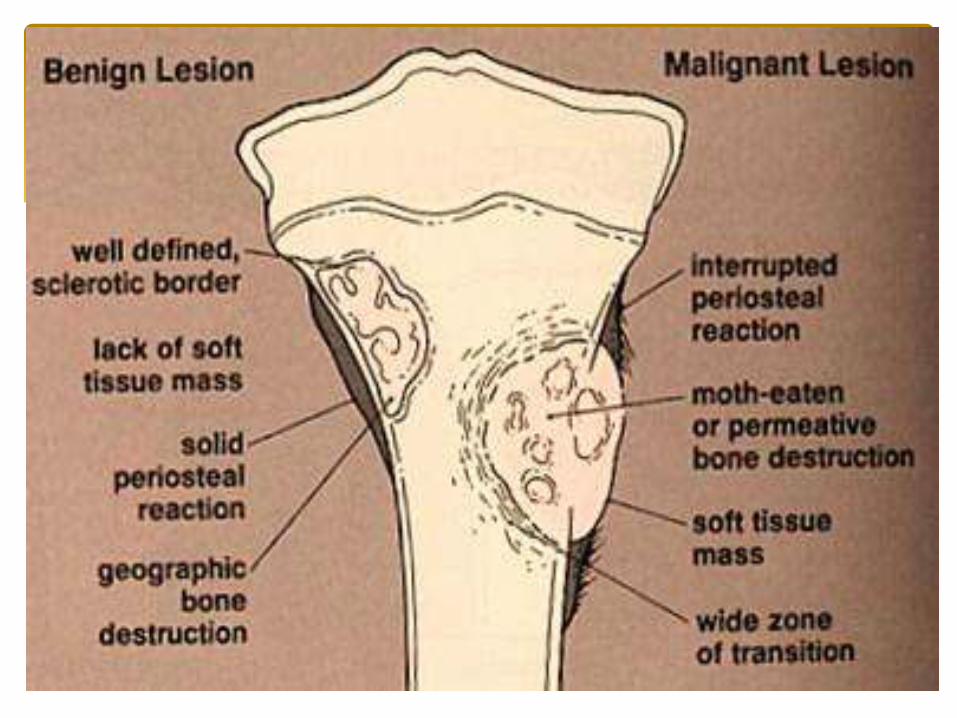
Are the margins of the lesion well- or ill-defined?
Are there flecks of calcification in the lesion?
Is the cortex eroded or destroyed?
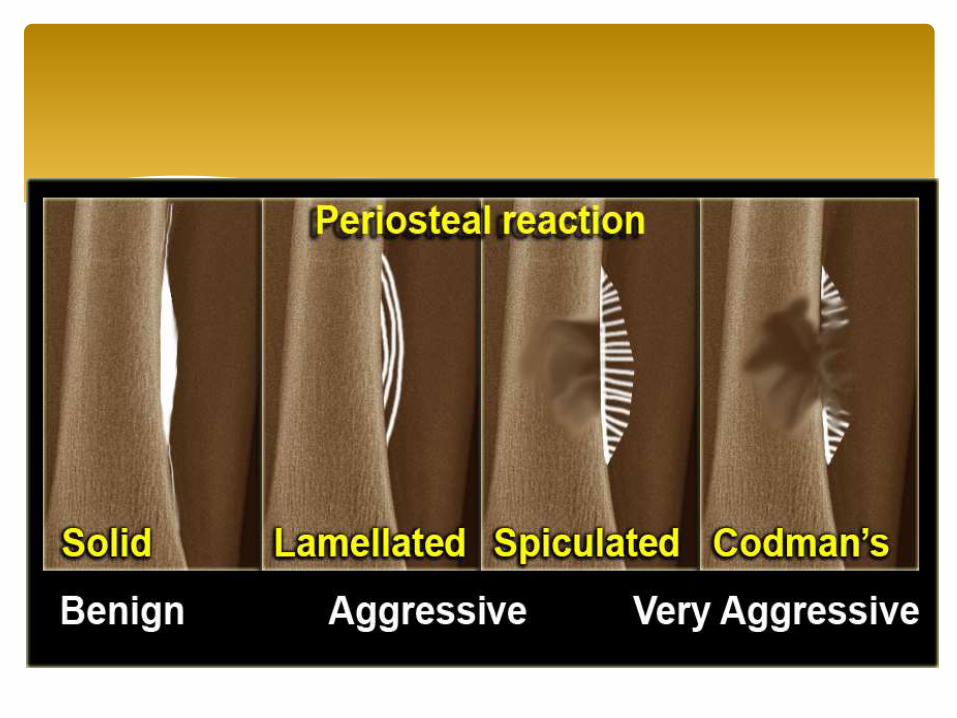
Is there any periosteal new-bone formation?
Does the tumors extend into the soft tissues?
IMAGING :


>> RADIONUCLIDE SCANNING
Scanning with 99mTc-methyl diphosphonate (99mTc-
MDP) >> this can be helpful in revealing the site of a small tumors .
>> COMPUTED TOMOGRAPHY (CT)
>> it shows more accurately both intraosseous and extraosseous
extension of the tumor and the relationship to surrounding
structures.
Others :
MAGNETIC RESONANCE IMAGING (MRI)
Its greatest value is in the assessment of tumor spread:
(a) within the bone.
(b) into a nearby joint.
(c) into the soft tissues.
BIOPSY- Needle biopsy
- Open biopsy
Blood tests >> are often necessary to exclude other
conditions.
E g :- infection or metabolic bone disorders, or
a ‘brown tumor ’ in hyperparathyroidism.
>> Anemia, increased ESR and elevated serum alkaline
phosphatase levels are non-specific findings they may
help in differentiating between benign and malignant
bone lesion
LABORATORY INVESTIGATIONS:
1. Soft-tissue haematoma
2. Bone infection Osteomyelitis
3. Myositis ossificans
4. Stress fracture
5. Tendon avulsion injuries
6. gouty tophus
DIFFERENTIAL DIAGNOSIS
Benign >> Latent , Active , Aggressive
Malignant :
i. SURGICAL STAGE >> low grad OR high grad
ii. STAGING OF SOFT-TISSUE TUMOURS >> TNM
STAGING OF BONE TUMOURS
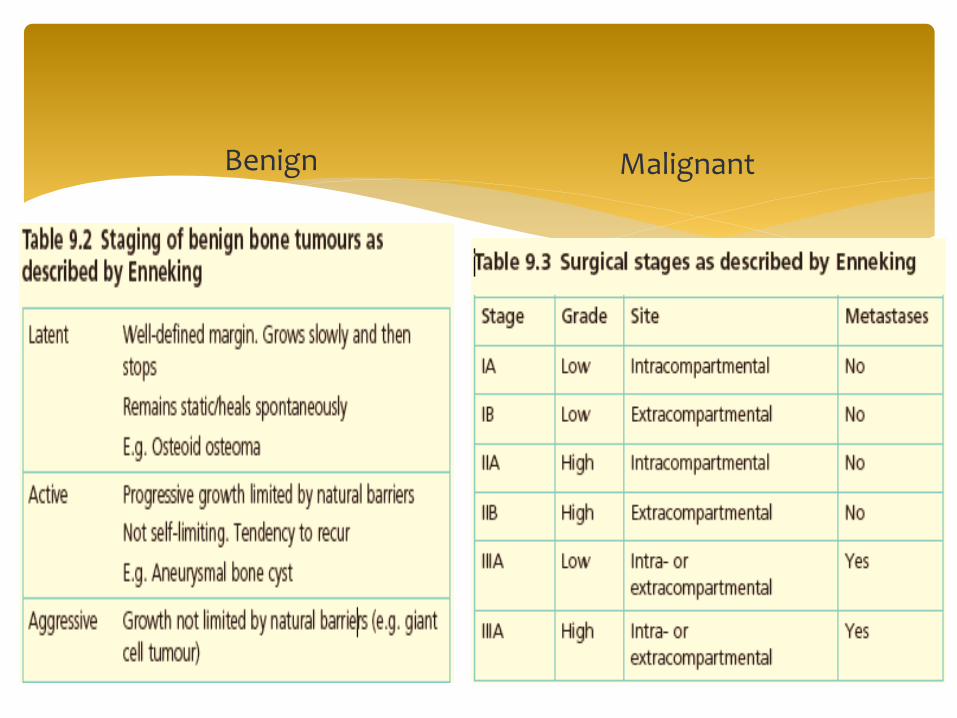
Benign Malignant
According to type :
Benign >> asymptomatic OR symptomatic
Malignant
Methods of management:
TUMOUR EXCISION
1- Intracapsular excision and curettage .
2- Marginal excision.
3- Wide excision.
4- Radical resection.
Principle of ttt in general

LIMB SALVAGE
>Short diaphyseal segments can be
replaced by vascularized or non-vascularized bone
grafts.
>Longer gaps may require custom-made
implants.
>Osteo-articular segments can be replaced by
large allografts, endoprostheses or allograft–prosthetic
composites.
AMPUTATION.
MULTI-AGENT CHEMOTHERAPY.
RADIOTHERAPY



1 - NON-OSSIFYING FIBROMA (NOF)
Age : childern ‘ < 30 yrs ,
Clinical : asymptomatic Or may pathologic # (rare)
On x-ray : well defined ,radiolucent area surrounded by a thin margin of dense bone , may be cystic .
Location : metaphysis of long bones .
ttt : if asymptomatic >> not need ttt ,,, if patho - # present >>curettage and bone grafting.
1- benign bone tumors :
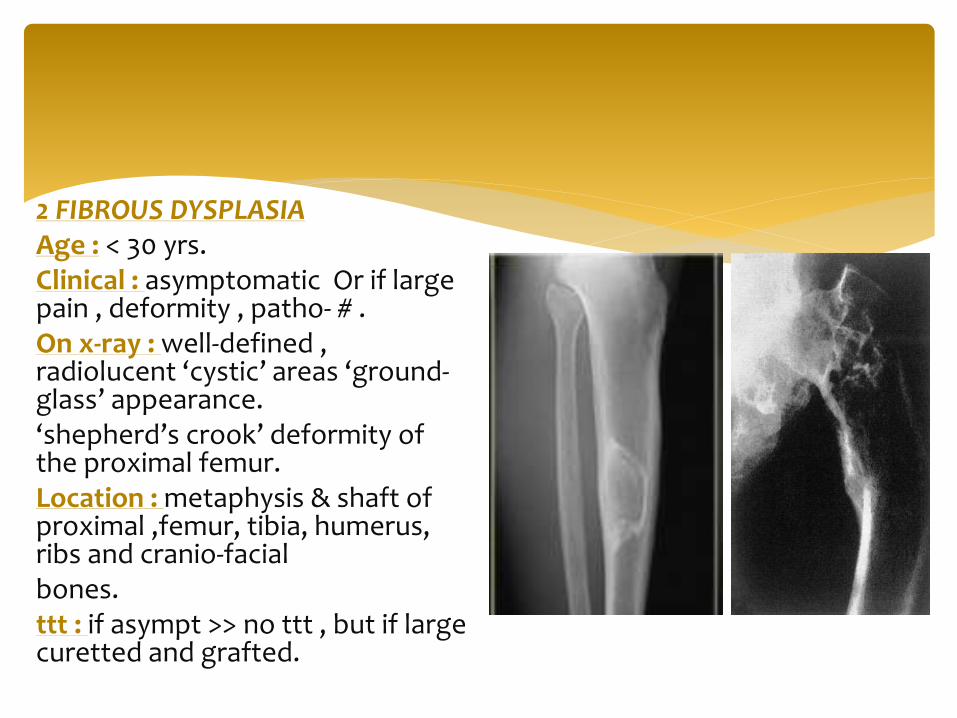
2 FIBROUS DYSPLASIAAge : < 30 yrs. Clinical : asymptomatic Or if large pain , deformity , patho- # .On x-ray : well-defined , radiolucent ‘cystic’ areas ‘ground-glass’ appearance. ‘shepherd’s crook’ deformity of the proximal femur.Location : metaphysis & shaft of proximal ,femur, tibia, humerus, ribs and cranio-facialbones.ttt : if asympt >> no ttt , but if large curetted and grafted.
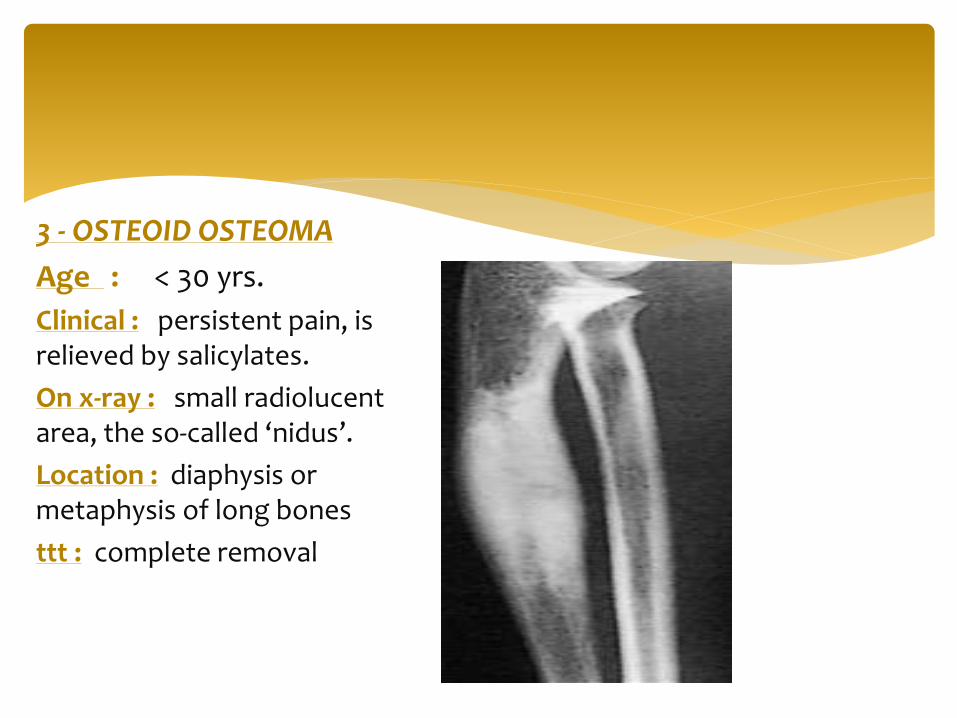
3 - OSTEOID OSTEOMA
Age : < 30 yrs.
Clinical : persistent pain, is relieved by salicylates.
On x-ray : small radiolucent area, the so-called ‘nidus’.
Location : diaphysis or metaphysis of long bones
ttt : complete removal
5- OSTEOBLASTOMA
Age : usually adult
Clinical : pain and local muscle spasm.
On x-ray : well-demarcated osteolytic lesion
which may contain small flecks of ossification.
Location : spine and the flat bones
ttt : excision and bone grafting.
4- CHONDROBLASTOMAAge : young adult or children
Clinical :constant ache in the joint; the tenderspot is actually in the adjacent bone.On x-ray : well-demarcated radiolucent area with no hint of central calcification.Location : epiphysis, of the proximal humerus, femur or tibia.ttt : marginal excision or by curettage and alcohol or phenol cauterization –and replaced with bone grafts
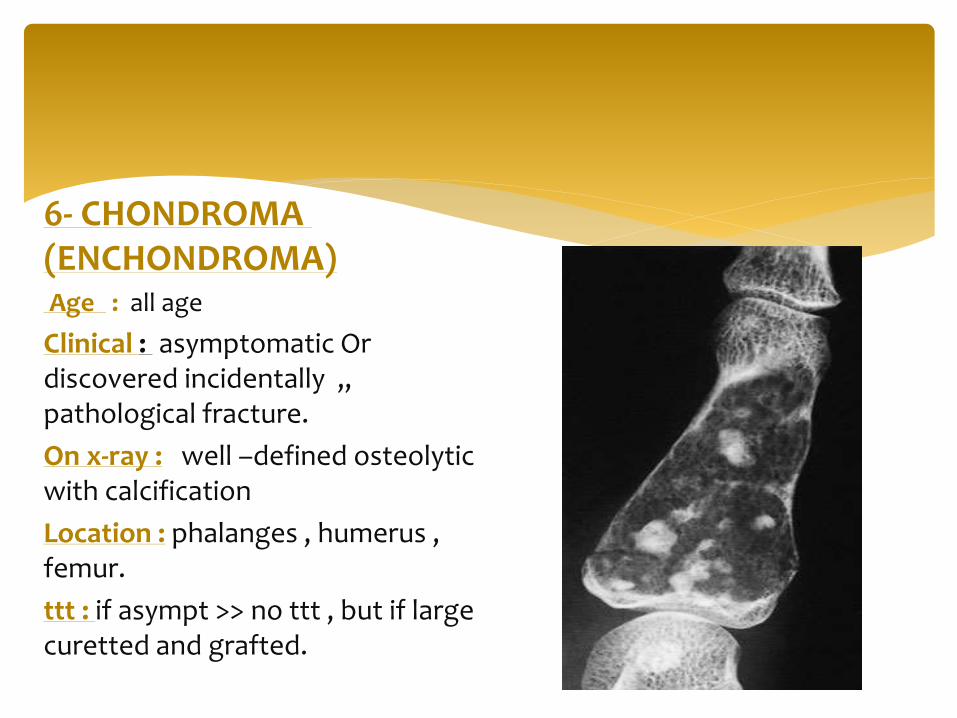
6- CHONDROMA (ENCHONDROMA)Age : all age
Clinical : asymptomatic Or discovered incidentally ,, pathological fracture.
On x-ray : well –defined osteolytic with calcification
Location : phalanges , humerus , femur.
ttt : if asympt >> no ttt , but if large curetted and grafted.
Signs of malignant transformation in patients over
30 years are:
(1) the onset of pain;
(2) enlargement of the lesion; and
(3) cortical erosion.
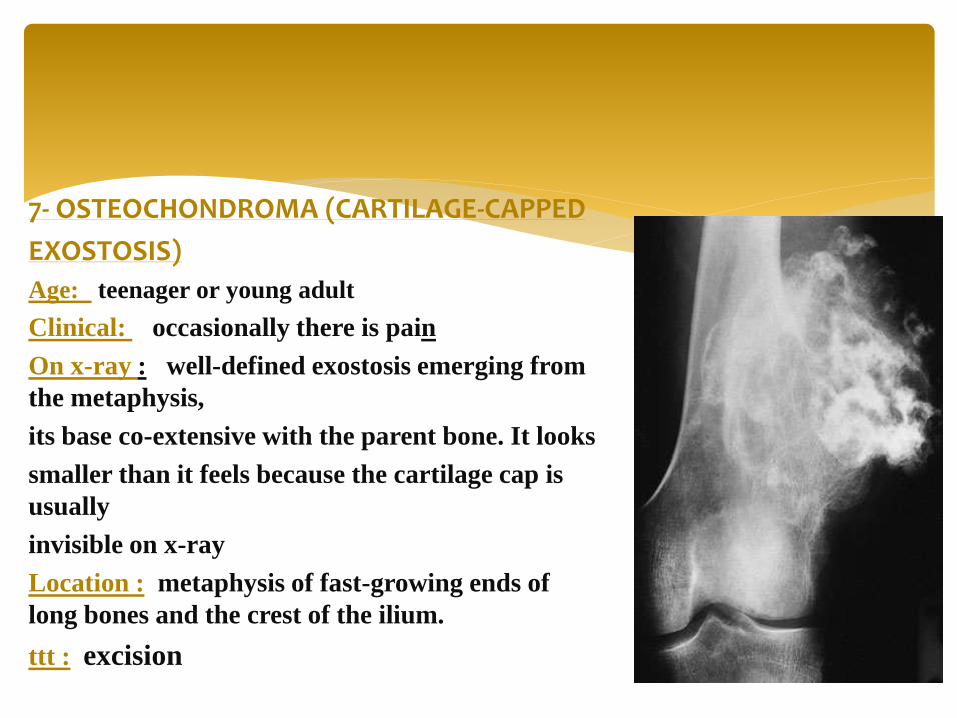
7- OSTEOCHONDROMA (CARTILAGE-CAPPED
EXOSTOSIS)
Age: teenager or young adult
Clinical: occasionally there is pain
On x-ray : well-defined exostosis emerging from
the metaphysis,
its base co-extensive with the parent bone. It looks
smaller than it feels because the cartilage cap is
usually
invisible on x-ray
Location : metaphysis of fast-growing ends of
long bones and the crest of the ilium.
ttt : excision
8- cystic Lesions of bone
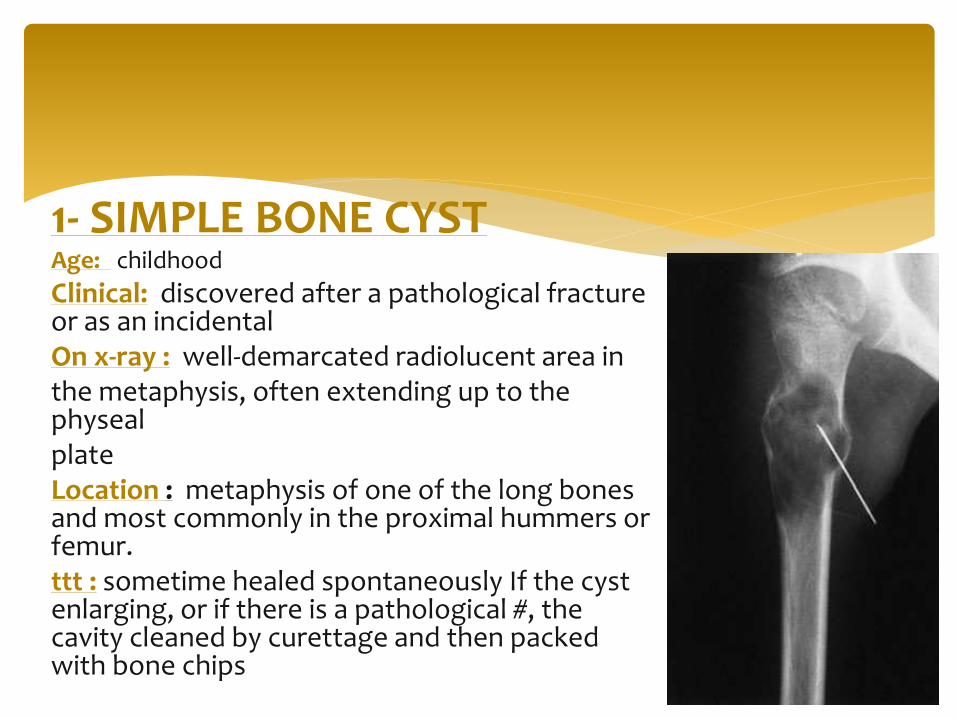
1- SIMPLE BONE CYSTAge: childhood
Clinical: discovered after a pathological fracture or as an incidentalOn x-ray : well-demarcated radiolucent area inthe metaphysis, often extending up to the physealplateLocation : metaphysis of one of the long bones and most commonly in the proximal hummers or femur.ttt : sometime healed spontaneously If the cyst enlarging, or if there is a pathological #, the cavity cleaned by curettage and then packed with bone chips

Others
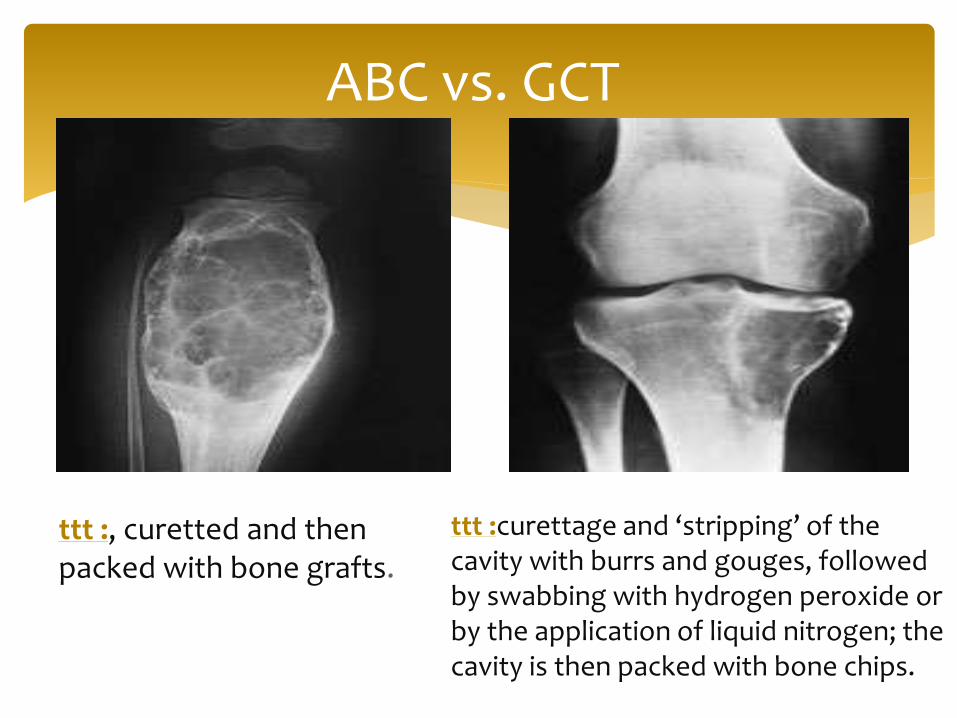
ABC vs. GCT
ttt :, curetted and then packed with bone grafts.
ttt :curettage and ‘stripping’ of the cavity with burrs and gouges, followed by swabbing with hydrogen peroxide or by the application of liquid nitrogen; the cavity is then packed with bone chips.
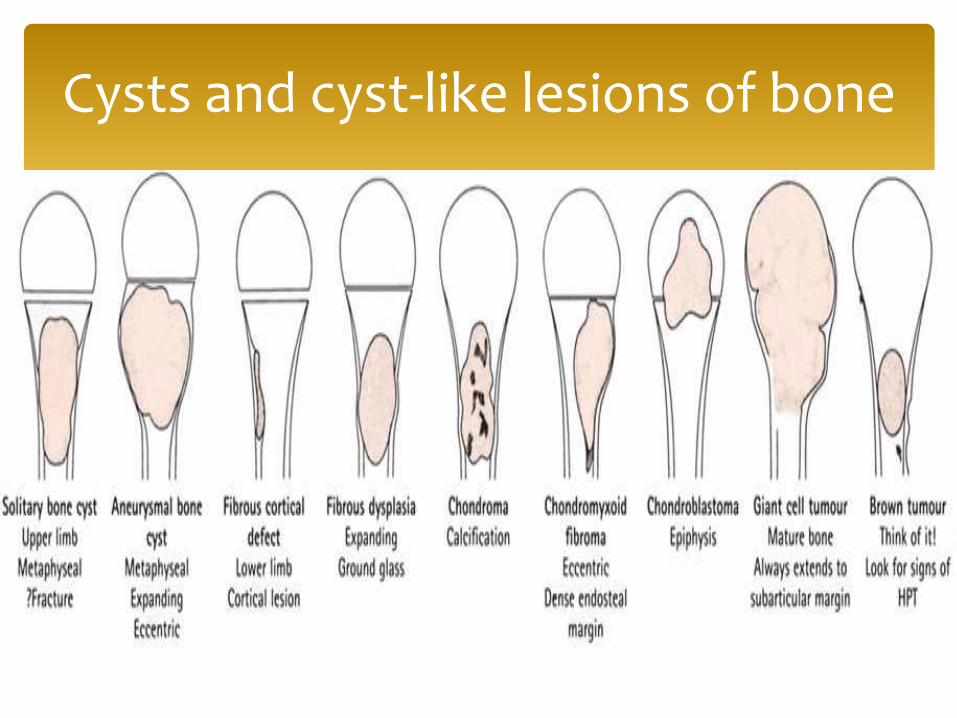
Cysts and cyst-like lesions of bone
1- PRIMARY MALIGNANT BONE TUMOURS .
CHONDROSARCOMA
OSTEOSARCOMA
EWING’S SARCOMA
MULTIPLE MYELOMA
2- METASTATIC BONE TUMOURS .
MALIGNANT BONE
TUMOURS

CHONDROSARCOMA
Incidence : The highest incidence is in the fourth and fifth
decades and men are affected more often than women.
Clinical : Patients may complain of a dull ache or a
gradually
enlarging lump. Medullary lesions may present as a
pathological fracture.
1- PRIMARY MALIGNANT BONE
TUMOURS .
Location : may develop in any of the bones that normally develop in
cartilage,
Almost 50 % , appear in the metaphysis of one of the
long tubular bones, mostly in the lower limbs. The
next most common sites are the pelvis and the ribs.
Despite the relatively frequent occurrence of benign
cartilage tumors in the small bones of the hands and
feet, malignant lesions are rare at these sites.
Chondrosarcomas take various forms:
Depending on :
A- their location in the bone (central or peripheral);
B- whether they develop without precedent (primary
chondrosarcoma) or by malignant change in a pre-existing
benign lesion (secondary chondrosarcoma);
C- the predominant cell type in the tumour.
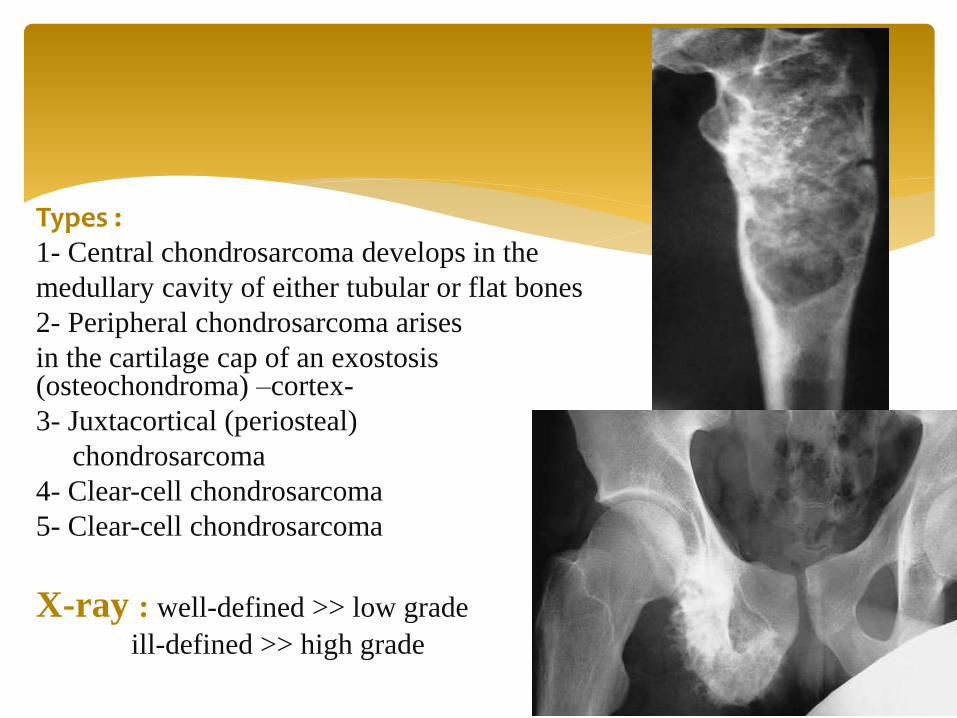
Types :1- Central chondrosarcoma develops in the
medullary cavity of either tubular or flat bones
2- Peripheral chondrosarcoma arises
in the cartilage cap of an exostosis (osteochondroma) –cortex-
3- Juxtacortical (periosteal)
chondrosarcoma
4- Clear-cell chondrosarcoma
5- Clear-cell chondrosarcoma
X-ray : well-defined >> low grade
ill-defined >> high grade

Wide excision and prosthetic replacement
The tumour does not respond to either radiotherapy or chemotherapy.
OSTEOSARCOMAIncidence : occur predominantly in children and adolescents and men are affected more often than women.
Treatment

Clinical : Pain is usually the first symptom; it is constant, worse
at night and gradually increases in severity. Sometimes
the patient presents with a lump. Pathological fracture
is rare.
Location: It may affect any bone but most commonly involves the
long-bone metaphyses, especially around the knee and
at the proximal end of the humerus.
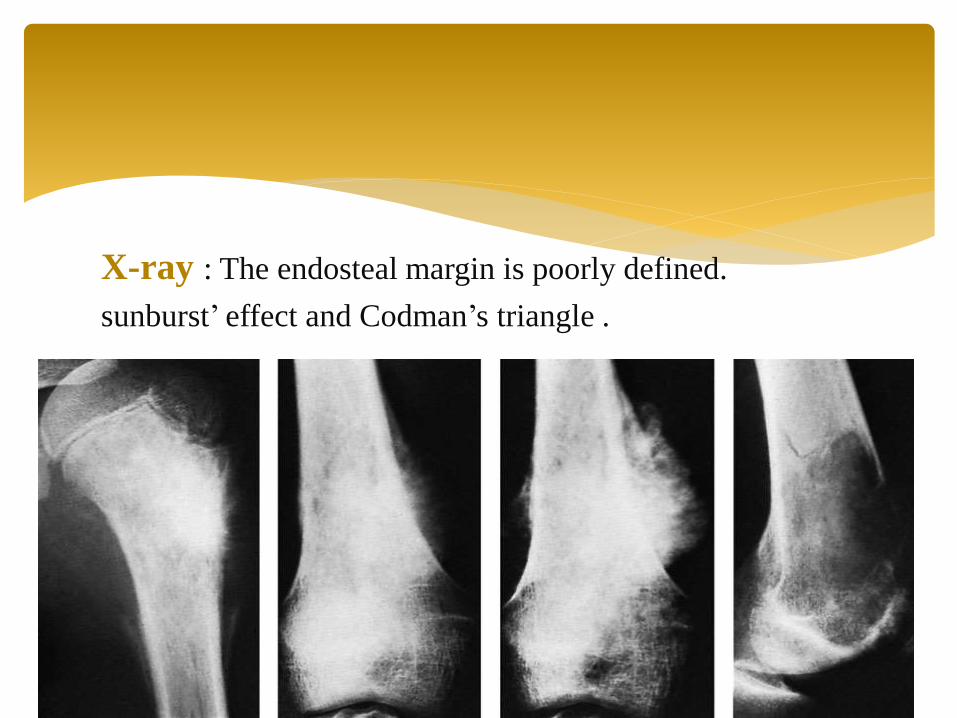
X-ray : The endosteal margin is poorly defined.
sunburst’ effect and Codman’s triangle .
eradicate the primary lesion completely
Depending on the site of the tumour, preparations
would have been made to replace that segment
of bone with either a large bone graft or a custommade
implant; in some cases an amputation may be
more appropriate.
respond to chemotherapy.
Treatment
EWING’S SARCOMA
Incidence : It occurs most commonly between the ages of
10 and 20 years , and males more than females .
Clinical : The patient presents with pain – often throbbing
in character – and swelling. Generalized illness and
pyrexia, together with a warm, tender swelling .
Location : usually in a tubular bone and especially in the
tibia, fibula or clavicle.

X-ray : area of bone
destruction
New bone formation ‘onion-
peel’ effect.
‘sunray’ appearance and
Codman’s triangles.
The best results are achieved by a combination of all three
methods: a course of preoperative neoadjuvant
chemotherapy; then wide excision if the tumour is in a
favorable site, or radiotherapy followed by local excision
if it is less accessible; and then a further course of
chemotherapy for 1 year.
Treatment
MULTIPLE MYELOMAIncidence : The patient, typically aged 45–65, presents.
Clinical : weakness, backache, bone pain or a pathological fracture.
Hypocalcaemia may cause symptoms such as
thirst, polyuria and abdominal pain.
Localized tenderness and restricted hip movements could be due to a plasmacytoma in the proximal femur.
In late cases there may be signs of cord or nerve root compression, chronic nephritis and recurrent infection.

Location : any bone .
X-rays: generalized
osteoporosis .
Treatment :
treatment of
pathological fractures
Incidence : in patients over 50 -70 years bone metastases are seen
more frequently than all primary malignant bone tumors together.
Source : The commonest source is carcinoma of the breast; next in
frequency are carcinomas of the prostate, kidney, lung, thyroid,
bladder and gastrointestinal tract.
Location : The commonest sites for bone metastases are the
vertebrae, pelvis, the proximal half of the femur and the humerus.
Spread is usually via the blood stream;
occasionally, visceral tumors spread directly to adjacent
bones (e.g. the pelvis or ribs).
2- METASTATIC BONE TUMOURS
Clinical : Pain is the commonest – and often the only – clinical feature. The sudden appearance of backache or
thigh pain in an elderly person.
Sudden collapse of a vertebral body or a fracture of the mid-shaft of a long bone .
In children under 6 years of age, metastatic lesions
are most commonly from adrenal neuroblastoma. The
child presents with bone pain and fever; examination
reveals the abdominal mass.
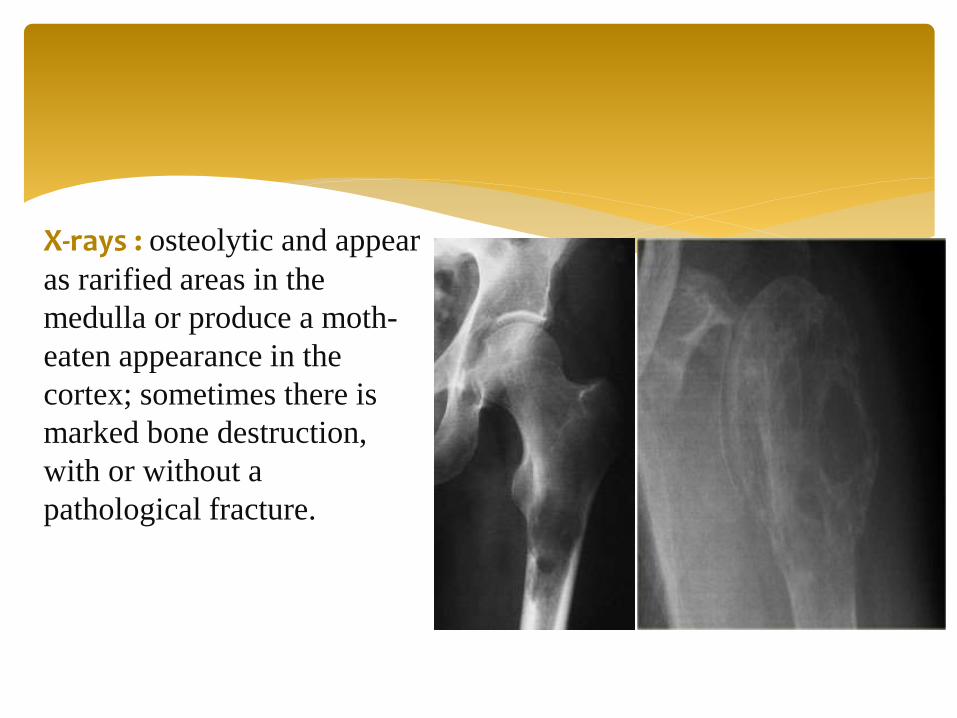
X-rays : osteolytic and appear
as rarified areas in the
medulla or produce a moth-
eaten appearance in the
cortex; sometimes there is
marked bone destruction,
with or without a
pathological fracture.
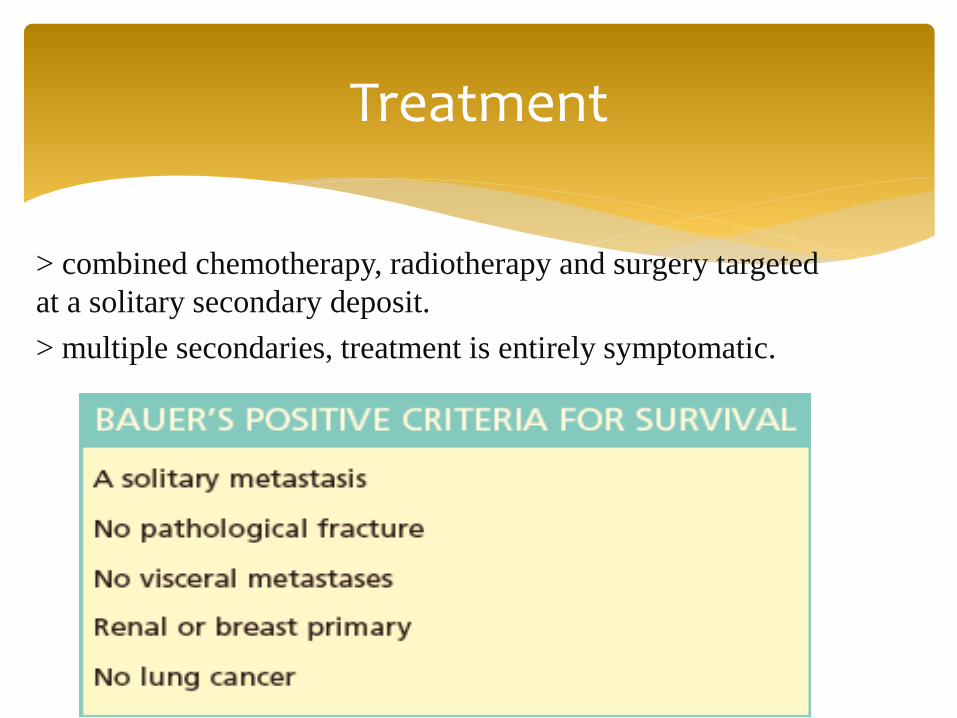
> combined chemotherapy, radiotherapy and surgery targeted
at a solitary secondary deposit.
> multiple secondaries, treatment is entirely symptomatic.
Treatment
FIBROUS TUMOURS
SYNOVIAL TUMOURS
MUSCLE TUMOURS
Other tumors

GOOD LUCK