Embed Size (px)
Citation preview
Cell Biology and Histology
SEVENTH EDITION
Leslie P. Gartner, PhD Professor of Anatomy (Retired) Department of Biomedical Sciences University of Maryland Dental School Baltimore, Maryland
James L. Hiatt, PhD Professor Emeritus Department of Biomedical Sciences University of Maryland Dental School Baltimore, Maryland
®Wolters Kluwer Health Philadelphia • Baltimore • New York • London Buenos Aires· Hong Kong· Sydney· Tokyo
tahir99 - V
RG
&
vip.persi
anss.ir
tahir99-VRG & vip.persianss.ir
Acquisitions Editor: Crystal Taylor Product Development Editor: Amy Weintraub
Production Project Manager: Priscilla Crater
Design Coordinator: Holly Reid McLaughlin
Manufacturing Coordinator: Margie Orzech Compositor: S4Carlisle Publishing Services
Copyright© 2015 Wolters Kluwer Health.
351 West Camden Street
Baltimore, MD 21201
Two Commerce Square, 200 1 Market Street Philadelphia, PA 19103
Copyright© 201 1 , 2007, 2003, 1998, 1993, 1988 Lippincott Williams & Wilkins, a Wolters Kluwer business.
Korean Translation, 2005, published by ShinHeung Medscience, Inc.
Spanish Translation, 2008, published by Lippincott Williams & Wilkins
Japanese translation, 2007, published by Medical Sciences International, LTD
Greek translation, 2006, published by Parissianos Publishing Company
All rights reserved. This book is protected by copyright. No part of this book may be reproduced in any form or by
any means, including photocopying, or utilized by any information storage and retrieval system without written
permission from the copyright owner. The publisher is not responsible (as a matter of product liability, negligence, or otherwise) for any injury
resulting from any material contained herein. This publication contains information relating to general
principles of medical care that should not be construed as specific instructions for individual patients. Manufacturers' product information and package inserts should be reviewed for current information, including
contraindications, dosages, and precautions.
Printed in China
Library of Congress Cataloging-in-Publication Data Gartner, Leslie P., 1943- author.
Cell biology and histology I Leslie P. Gartner, James L. Hiatt. - Seventh edition.
p. ; em. - (Board review series) Includes bibliographical references and index.
ISBN 978- 1-45 1 1 -895 1-3 (paperback : alk. paper)
I. Hiatt, James L., 1934- author. II. Title. III. Series: Board review series.
[DNLM: l. Histological Techniques-Outlines. 2. Cytological Techniques-Outlines. QS 18.2]
QM553
61 1'.018-dc23
2014018636
DISCLAIMER Care has been taken to confirm the accuracy of the information present and to describe generally accepted
practices. However, the authors, editors, and publisher are not responsible for errors or omissions or for any
consequences from application of the information in this book and make no warranty, expressed or implied,
with respect to the currency, completeness, or accuracy of the contents of the publication. Application of this
information in a particular situation remains the professional responsibility of the practitioner; the clinical treatments described and recommended may not be considered absolute and universal recommendations.
The authors, editors, and publisher have exerted every effort to ensure that drug selection and dosage set
forth in this text are in accordance with the current recommendations and practice at the time of publication. However, in view of ongoing research, changes in government regulations, and the constant flow of information
relating to drug therapy and drug reactions, the reader is urged to check the package insert for each drug for any
change in indications and dosage and for added warnings and precautions. This is particularly important when
the recommended agent is a new or infrequently employed drug.
Some drugs and medical devices presented in this publication have Food and Drug Administration (FDA)
clearance for limited use in restricted research settings. It is the responsibility of the health care provider to
ascertain the FDA status of each drug or device planned for use in their clinical practice.
To purchase additional copies of this book, call our customer service department at (800) 638-3030 or fax
orders to {301) 223-2320. International customers should call {301) 223-2300. Visit Lippincott Williams & Wilkins on the Internet: http:/ /www.lww.com. Lippincott Williams & Wilkins
customer service representatives are available from 8:30 am to 6:00 pm, EST.
tahir99 - V
RG
&
vip.persi
anss.ir
tahir99-VRG & vip.persianss.ir

Preface
We were very pleased with the reception of the sixth edition of this book, as well as with the many favorable comments we received from students who used it in preparation for the USMLE Step l or as an outline and study guide for their histology and/or cell biology courses in professional schools or undergraduate colleges.
Many of the chapters have been extensively revised and updated to incorporate current information, and we have attempted to refine the content of the text to present material emphasized on National Board Examinations as succinctly as possible while still retaining the emphasis on the relationship between cell structure and function through the vehicle of cell and molecular biology. A tremendous amount of material has been compressed into a concise but highly comprehensive presentation, using some new and revised illustrations. The relevancy of cell biology and histology to clinical practice is illustrated by the presence of clinical considerations within each chapter as appropriate.
The greatest changes that occurred in the evolution of this book from its previous edition are that we have added many more clinical considerations and compressed information into tabular form. We believe that these changes make this board review book more interesting and pertinent and the presentation of material in tables conserves time in the review process for medical students in their preparation for the USMLE Step l.
We are sad to announce that Judy Strum, our coauthor throughout the first six editions of this review book, decided to complete her retirement from the faculty of the University of Maryland School of Medicine thereby withdrawing her participation in the preparation of the current edition of this textbook.
As always, we welcome comments, suggestions, and constructive criticism of this book. Please address all comments to [email protected]
Leslie P. Gartner, PhD
James L. Hiatt, PhD
iii
tahir99 - V
RG
&
vip.persi
anss.ir
tahir99-VRG & vip.persianss.ir

Acknowledgments
We thank the following individuals for their help and support during the preparation of this book: Crystal Taylor, our Acquisitions Editor; and Dana Battaglia and Amy Weintraub, our product Development Editor( s ), who helped us weave all of the loose ends into a seamless whole.
iv
tahir99-VRG & vip.persianss.ir
Contents
Preface iii
Acknowledgments iv
1.
2.
3.
PLASMA MEMBRANE
I. Overview-The Plasma Membrane (Plasmalemma; Cell Membrane) 1 I I . Fluid Mosaic Model of the Plasma Membrane 1
I l l . Plasma Membrane Transport Processes 5 IV. Cell-to-Cell Communication 7 V. Plasmalemma-Cytoskeleton Association 9
Review Test 12
NUCLEUS
I. Overview-The Nucleus 15 I I . Nuclear Envelope 15
I l l . Nucleolus 18 IV. Nucleoplasm 18 v. Chromatin 19
VI. Chromosomes 20 VII . DNA 21
VI I I . RNA 22 IX. Cell Cycle 25 X. Apoptosis (Programmed Cell Death)
XI. Meiosis 29
Review Test 31
CYTOPLASM AND ORGANELLES
I. Overview-The Cytoplasm 33 I I . Structural Components 33
I l l . Interactions among Organelles 49
Review Test 58
28
1
15
33
v
tahir99-VRG & vip.persianss.ir
vi Contents
4. EXTRACELLULAR MATRIX 61
I . Overview-The Extracellular Matrix 61 I I . Ground Substance 61
I l l . Fibers 64
Review Test 72
5. EPITHELIA AND GLANDS 75
I . Overview-Epithelia 75 I I . Lateral Epithelial Surfaces 77
I l l . Basal Epithelial Surfaces 80 IV. Apical Epithelial Surfaces 83 v. Glands 87
Review Test 89
6. CONNECTIVE TISSUE 92
I . Overview-Connective Tissue 92 I I . Extracellular Matrix 92
I l l . Connective Tissue Cells 93 IV. Classification of Connective Tissue 99
Review Test 1 03
7. CARTILAGE AND BONE 106
I . Overview-Cartilage 106 I I . Overview-Bone llO
I l l . Joints 120
Review Test 1 21
8. MUSCLE 124
I . Overview-Muscle 124 I I . Structure o f Skeletal Muscle 124
I l l . Contraction o f Skeletal Muscle 130 IV. Innervation of Skeletal Muscle 132 v. Cardiac Muscle 133
VI. Smooth Muscle 135 VI I . Contractile Nonmuscle Cells 139
Review Test 1 40
tahir99-VRG & vip.persianss.ir
Contents
9. NERVOUS SYSTEM
I. Overview-Nervous System 143 I I . Histogenesis o f the Nervous System 143
I l l . Cells o f Nervous System 145 IV. Synapses 151 v. Nerve Fibers 152
VI. Nerves 153 VII . Ganglia 155
VI I I . Histophysiology of Nervous System 155 IX. Somatic Nervous System and Autonomic Nervous System X. Central Nervous System 158
XI. Degeneration and Regeneration of Nerve Tissue 160
Review Test 162
10. BLOOD AND HEMOPOIESIS
I. Overview-Blood 166 I I . Blood Constituents 166
I l l . Blood Coagulation 172 IV. Bone Marrow 17 4 V. Prenatal Hemopoiesis 175
VI. Postnatal Hemopoiesis 175 VI I . Hemopoietic Growth Factors (CSFS) 179
Review Test 181
11. CIRCULATORY SYSTEM
I. Overview-Blood Vascular System 184 I I . Overview-Lymphatic Vascular System 195
Review Test 196
12. LYMPHOID TISSUE
I. Overview-The Lymphoid (Immune) System 199 I I . Cells of the Immune System 201
I l l . Antigen Presentation and the Role of MHC Molecules 209 IV. Immunoglobulins 210 V. Diffuse Lymphoid Tissue 211
VI. Lymphoid Organs 212
Review Test 218
157
vii
143
166
184
199
tahir99-VRG & vip.persianss.ir
viii Contents
13. ENDOCRINE SYSTEM
I. Overview-The Endocrine System 221 I I . Hormones 221
I l l . Overview-Pituitary Gland (Hypophysis) and Hypothalamus 222 IV. Overview-Thyroid Gland 228 V. Parathyroid Glands 232
VI. Overview-Adrenal (Suprarenal) Glands 234 VI I . Pineal Gland (Pineal Body, Epiphysis) 237
Review Test 239
14. SKIN
15.
I . Overview-The Skin 242 I I . Epidermis 242
I l l . Dermis 248 IV. Glands in the Skin 249 v. Hair, Hair Follicle, and Arrector Pili Muscle 251
VI. Nails 252
Review Test 254
RESPIRATORY SYSTEM
I. Overview-The Respiratory System 257 I I . Conducting Portion of the Respiratory System 257
I l l . Overview-Respiratory Portion of the Respiratory System 262
IV. Lung Lobules 269 V. Pulmonary Vascular Supply 269
VI. Pulmonary Nerve Supply 269
Review Test 270
16. DIGESTIVE SYSTEM: ORAL CAVITY AND ALIMENTARY TRACT
I. Overview-The Digestive System 273 I I . Oral Region 273
I l l . Divisions of the Alimentary Canal 278 IV. Digestion and Absorption 289
Review Test 291
221
242
257
273
tahir99-VRG & vip.persianss.ir
17. DIGESTIVE SYSTEM: GLANDS
I. Overview-Extrinsic Glands of the Digestive System 294 I I . Major Salivary Glands 294
I l l . Overview-Pancreas 296 IV. Liver 299 V. Gallbladder 304
Review Test 306
18. THE URINARY SYSTEM
I. Overview-The Urinary System 309 I I . Kidneys 309
I l l . Uriniferous Tubules 310 IV. Renal Blood Circulation 320 V. Regulation of Urine Concentration 321
VI. Excretory Passages 324
Review Test 327
19. FEMALE REPRODUCTIVE SYSTEM
I. Overview-Female Reproductive System 330 I I . Ovaries 330
I l l . Oviducts (Fallopian Tubes) 338 IV. Uterus 339 V. Cervix 341
VI. Fertilization and Implantation 342 VII . Placenta 343
VI I I . Vagina 345 IX. External Genitalia (Vulva) 345 X. Mammary Glands 346
Review Test 348
20. MALE REPRODUCTIVE SYSTEM
I. Overview-Male Reproductive System 350 I I . Testes 350
I l l . Genital Ducts 357 IV. Accessory Genital Glands 359 V. Urethra 361
VI. Penis 362
Review Test 363
Contents ix
294
309
330
350
tahir99-VRG & vip.persianss.ir
x Contents
21. SPECIAL SENSES
I. Overview-Special Sense Receptors 366 I I . Specialized Diffuse Receptors 366
I l l . Sense of Sight-Eye 368 IV. Sense of Hearing-Ear (Vestibulocochlear Apparatus) 378
Review Test 384
Comprehensive Examination 387 Index 405
366
tahir99-VRG & vip.persianss.ir
Plasma Membrane
A. Structure. The plasma membrane is approximately 7.5 nm thick and consists of two leaflets, known as the l i p i d b i layer that houses associated integra l and peripheral p rote ins. 1. The inner leaflet of the plasma membrane faces the cytoplasm, and the outer leaflet faces the
extracellular environment. 2. When examined by transmission electron microscopy, the plasma membrane displays a
trilaminar (un it membrane) structure.
B. Function 1. The plasma membrane envelops the cell and maintains its structural and functional integrity. 2. It acts as a semipermeable membrane between the cytoplasm and the external environment. 3. It permits the cell to recognize macromolecules and other cells as well as to be recognized by
other cells. 4. It participates in the transduction of extracellular signals into intracellular events. 5. It assists in controlling interaction between cells. 6. It maintains an electrical potential difference between the cytoplasmic and extracellular sides.
A. The l i p id b i layer (Figures 1 . 1 , 1 .2, and 1 .3) is freely permeable to small, lipid-soluble, nonpolar molecules but is impermeable to charged ions. 1. Molecular structure. The lipid bilayer is composed of phospholipids, glycolipids, and
cholesterol, of which, in most cells, phospholipids constitute the highest percentage. a. Phospho l ip ids are amphipath ic molecules, consisting of one polar (hydroph i l ic) head and
two nonpolar (hydrophobic) fatty acyl tails, one of which is usually unsaturated. b. The two leaflets are not identical; instead the distribution of the various types of
phospholipids is asymmetrical. (1) The polar head of each molecule faces the membrane surface, whereas the ta i ls project
into the interior of the membrane, facing each other. (2) The ta i ls of the two leaflets are mostly 16 to 18 carbon chain fatty acids, and they form
weak noncova lent bonds that attach the two leaflets to each other.
tahir99-VRG & vip.persianss.ir
2 BRS Ce l l B io logy and H isto logy
Carbohyd rate bound to l ip id and p rotei n 0
��m gggggggg ggggggggggggg�� �- Peripheral '--.____j protein
-I ntegral protei n
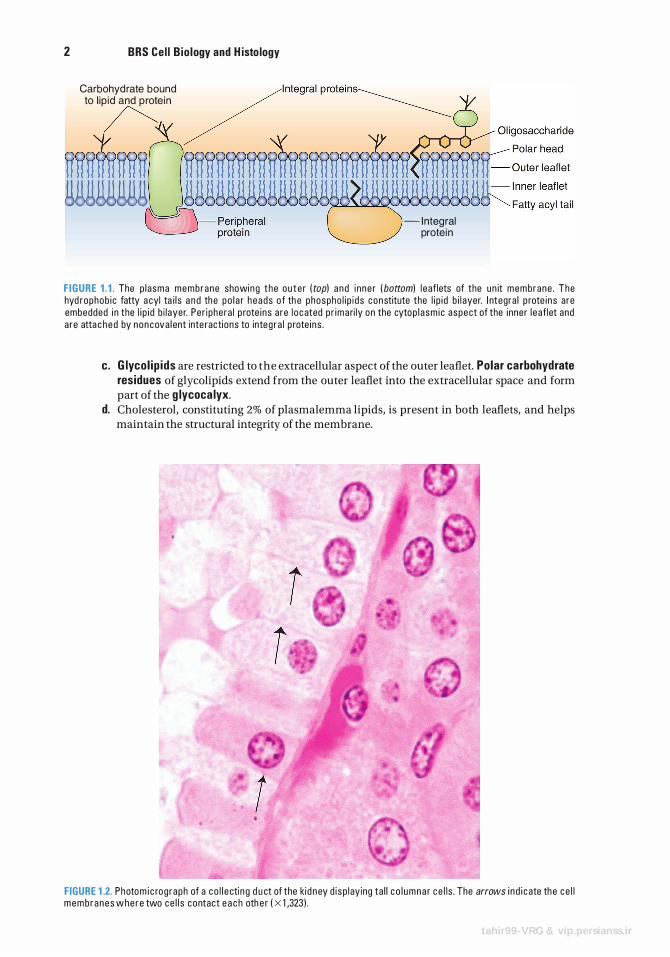
F IGURE 1 . 1 . The p l asma membrane showing t he ou te r ( top) and i nne r ( bottom) l e af lets of the un it membrane . The hyd rophob i c fatty a cyl ta i l s a n d the po l a r heads o f th e phospho l i p i ds constitute the l i p i d b i l ayer. I ntegra l p rote i ns are embedded i n the l i p i d b i l ayer. Per i phera l p rote i ns are l o cated p r ima ri ly on the cytop l a sm i c aspect of the i nner l e af let and are atta c h e d by noncova l ent inte racti ons to integ ra l p rote i ns .
c. G lyco l ip ids are restricted to the extracellular aspect of the outer leaflet. Polar carbohydrate residues of glycolipids extend from the outer leaflet into the extracellular space and form part of the g lycoca lyx.
d. Cholesterol, constituting 2% of plasmalemma lipids, is present in both leaflets, and helps maintain the structural integrity of the membrane.
t
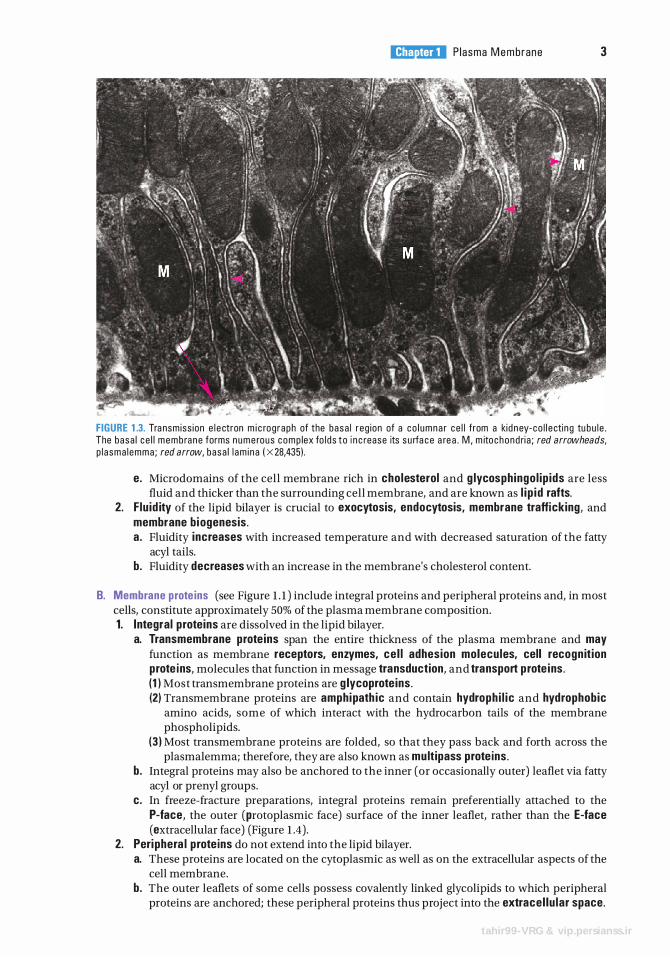
FIGURE 1 .2. Photo m i c rog raph of a co l l e cti n g d u ct of the kid n ey d i sp l ay ing ta l l c o l umna r c e l l s . The arrows i n d i c ate the ce l l memb ranes whe re two ce l l s contact e a c h oth e r ( X 1 ,323 ) .
tahir99-VRG & vip.persianss.ir
l!iitJtttDI Plasma Membrane 3
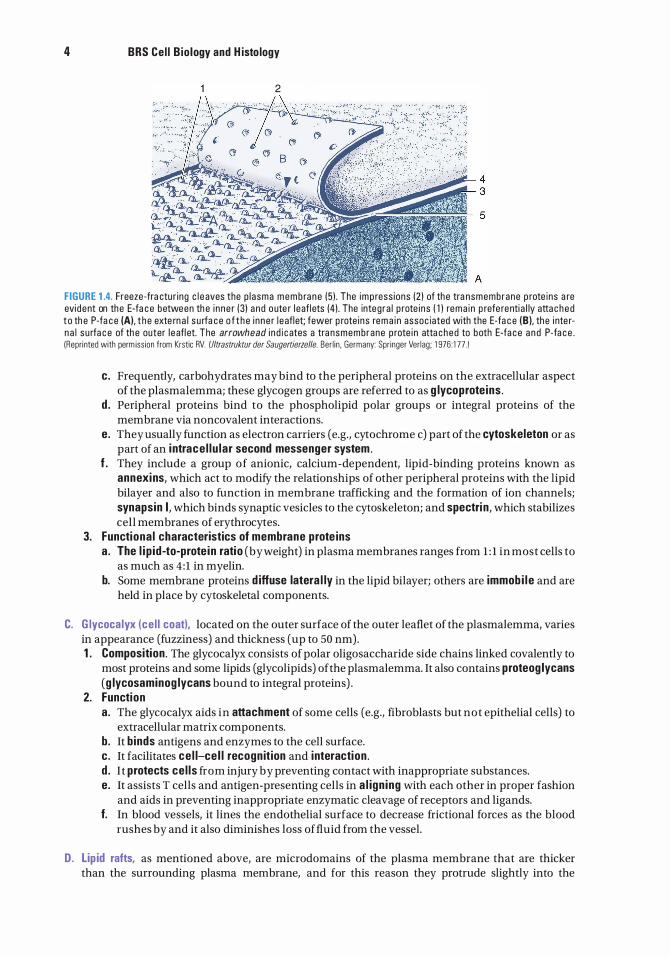
FIGURE 1 .3. Tra nsmiss ion e l e ctron m i c rog raph of the basa l reg ion of a co l umna r ce l l from a kid n ey-co l l e ctin g tu bu l e . The basa l c e l l memb ra n e forms n u m e rous comp lex fo l ds t o i n c rease its s u rfa c e a re a . M , m ito chond ri a ; red arrowheads, p l asma l emma ; red arrow, basa l l am i na ( X 28.435) .
e. Microdomains of the cell membrane rich in cholesterol and g lycosph ingo l ip ids are less fluid and thicker than the surrounding cell membrane, and are known as l i p i d rafts.
2. F lu id ity of the lipid bilayer is crucial to exocytosis, endocytosis, membrane trafficking, and membrane b iogenesis. a . Fluidity increases with increased temperature and with decreased saturation of the fatty
acyl tails. b. Fluidity decreases with an increase in the membrane's cholesterol content.
B. Membrane prote ins (see Figure 1 . 1 ) include integral proteins and peripheral proteins and, in most cells, constitute approximately 50% of the plasma membrane composition. 1. Integral proteins are dissolved in the lipid bilayer.
a. Transmembrane prote ins span the entire thickness of the plasma membrane and may function as membrane receptors, enzymes, ce l l adhesion molecules, cell recogn it ion prote ins, molecules that function in message transduction, and transport prote ins. (1) Most transmembrane proteins are g lycoprote ins . (2) Transmembrane proteins are amphipath ic and contain hydroph i l ic and hydrophobic
amino acids, some of which interact with the hydrocarbon tails of the membrane phospholipids.
(3) Most transmembrane proteins are folded, so that they pass back and forth across the plasmalemma; therefore, they are also known as multipass prote ins .
b . Integral proteins may also be anchored to the inner (or occasionally outer) leaflet via fatty acyl or prenyl groups.
c. In freeze-fracture preparations, integral proteins remain preferentially attached to the P-face, the outer (protoplasmic face) surface of the inner leaflet, rather than the E-face (extracellular face) (Figure 1 .4).
2. Periphera l prote ins do not extend into the lipid bilayer. a. These proteins are located on the cytoplasmic as well as on the extracellular aspects of the
cell membrane. b. The outer leaflets of some cells possess covalently linked glycolipids to which peripheral
proteins are anchored; these peripheral proteins thus project into the extracel lu lar space.
tahir99-VRG & vip.persianss.ir
4 BRS Ce l l B io logy and H isto logy
2
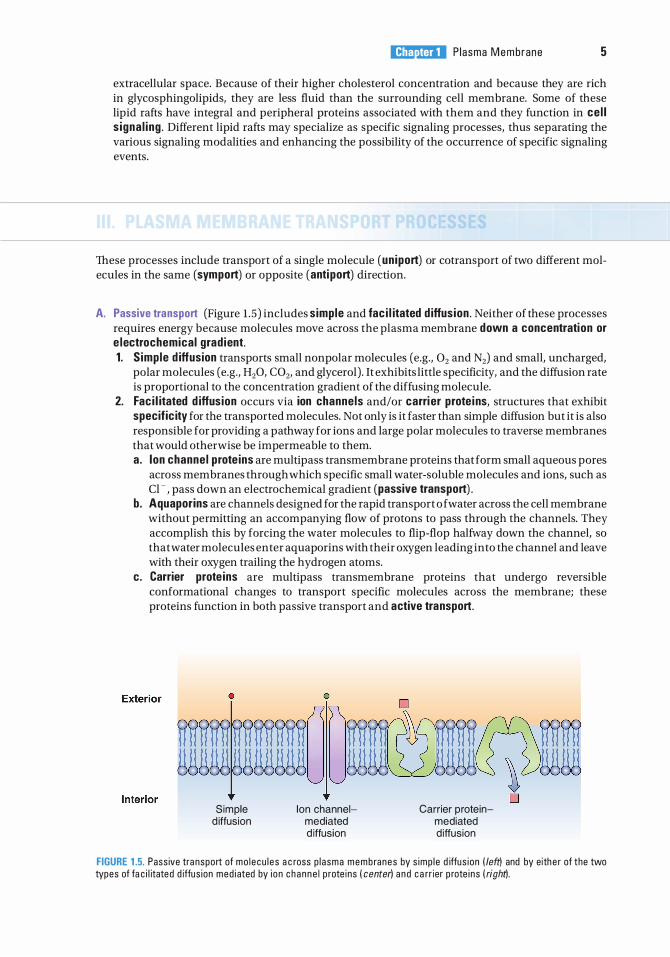
FIGURE 1 .4. Freeze-fra ctu r ing c l e aves the p l asma memb ra n e (5 ) . The imp ress ions (2 ) of the tra nsmembrane p rote ins a re evi dent on the E-fa c e between th e i n ne r (3) a nd o ute r l eafl ets (4) . The integ ra l p rote i ns ( 1 ) rema i n p refe renti a l ly atta c h e d t o th e P-fa c e (A), t h e exte rn a l s u rfa c e o f t h e i n ne r l e aflet; fewer p rote i ns rem a i n assoc iated with the E-fa c e (B), the i nte r· n a l su rfa c e of th e outer l e afl et. The arrowhead i n d i c ates a tra nsmembrane p rote i n atta ched to both E·fa c e a n d P·fa c e . (Repri nted with perm iss ion from Krstic RV. Ultrastruktur der Saugertierzelle. Ber l i n . Germany: Spr inger Ver lag; 1 976 : 1 77 . 1
c. Frequently, carbohydrates may bind to the peripheral proteins on the extracellular aspect of the plasmalemma; these glycogen groups are referred to as g lycoprote ins .
d . Peripheral proteins bind to the phospholipid polar groups or integral proteins of the membrane via noncovalent interactions.
e. They usually function as electron carriers (e.g., cytochrome c) part of the cytoskeleton or as part of an i ntrace l lu lar second messenger system .
f . They include a group of anionic, calcium-dependent, lipid-binding proteins known as annexins, which act to modify the relationships of other peripheral proteins with the lipid bilayer and also to function in membrane trafficking and the formation of ion channels; synapsin I , which binds synaptic vesicles to the cytoskeleton; and spectri n, which stabilizes cell membranes of erythrocytes.
3. Functiona l characteristics of membrane prote ins a . The l i p id-to-prote in ratio (by weight) in plasma membranes ranges from 1 : 1 in most cells to
as much as 4 : 1 in myelin. b. Some membrane proteins d iffuse latera l ly in the lipid bilayer; others are immob i l e and are
held in place by cytoskeletal components.
C. G lycoca lyx (ce l l coat). located on the outer surface of the outer leaflet of the plasmalemma, varies in appearance (fuzziness) and thickness (up to 50 nm) . 1 . Composition . The glycocalyx consists of polar oligosaccharide side chains linked covalently to
most proteins and some lipids (glycolipids) of the plasmalemma. It also contains proteog lycans (g lycosaminog lycans bound to integral proteins) .
2. Function a . The glycocalyx aids in attachment of some cells (e.g., fibroblasts but not epithelial cells) to
extracellular matrix components. b. It binds antigens and enzymes to the cell surface. c. It facilitates ce l l-ce l l recogn ition and i nteraction . d . I t protects ce l ls from injury by preventing contact with inappropriate substances. e. It assists T cells and antigen-presenting cells in a l ign ing with each other in proper fashion
and aids in preventing inappropriate enzymatic cleavage of receptors and ligands. f. In blood vessels, it lines the endothelial surface to decrease frictional forces as the blood
rushes by and it also diminishes loss of fluid from the vessel.
D. Lipid rafts, as mentioned above, are microdomains of the plasma membrane that are thicker than the surrounding plasma membrane, and for this reason they protrude slightly into the
l!iitJtttDI P l asma Membrane 5
extracellular space. Because of their higher cholesterol concentration and because they are rich in glycosphingolipids, they are less fluid than the surrounding cell membrane. Some of these lipid rafts have integral and peripheral proteins associated with them and they function in ce l l s igna l ing . Different lipid rafts may specialize as specific signaling processes, thus separating the various signaling modalities and enhancing the possibility of the occurrence of specific signaling events.
These processes include transport of a single molecule (un iport) or cotransport of two different molecules in the same (symport) or opposite (anti port) direction.
A. Passive transport (Figure 1 .5) includes simple and fac i l itated d iffusion . Neither of these processes requires energy because molecules move across the plasma membrane down a concentration or e lectrochemical grad ient. 1. S imple d iffusion transports small nonpolar molecules (e.g., 02 and N2) and small, uncharged,
polar molecules (e.g., H20, C02, and glycerol) . It exhibits little specificity, and the diffusion rate is proportional to the concentration gradient of the diffusing molecule.
2. Fac i l itated d iffusion occurs via ion channels and/or carri er prote ins, structures that exhibit specific ity for the transported molecules. Not only is it faster than simple diffusion but it is also responsible for providing a pathway for ions and large polar molecules to traverse membranes that would otherwise be impermeable to them. a. I on channel prote ins are multipass transmembrane proteins that form small aqueous pores
across membranes through which specific small water-soluble molecules and ions, such as Cl-, pass down an electrochemical gradient (passive transport) .
b . Aquaporins are channels designed for the rapid transport o f water across the cell membrane without permitting an accompanying flow of protons to pass through the channels. They accomplish this by forcing the water molecules to flip-flop halfway down the channel, so that water molecules enter aquaporins with their oxygen leading into the channel and leave with their oxygen trailing the hydrogen atoms.
c. Carrier prote ins are multipass transmembrane proteins that undergo reversible conformational changes to transport specific molecules across the membrane; these proteins function in both passive transport and active transport.
Simple d iffusion
lon channelmediated d iffusion
Carrier proteinmediated d iffusion
FIGURE 1 .5. Pass ive tra nsport of mo l e cu l e s a c ross p l asma memb ranes by s imp l e d iffus ion ( left) and by eithe r of the two types of fa c i l itated d iffus ion med i ated by i o n c h a n n e l p rote ins ( center) a n d c a rr ier p rote i ns ( righd.
6 BRS Ce l l B io logy and H isto logy
CLIN ICAL CONSIDERATIONS
Cystinur ia i s a he red ita ry cond itio n c a used by a bno rma l c a rri e r p rote i n s that a re u n a b l e to remove cysti n e from the u r i ne , resu lti ng i n the fo rmati on of k id ney stones .
Cystic f ibrosis i s a h e re d ita ry d i sease invo lvi n g a m utati o n i n the cystic librosis transmembrane conductance regu lator (CFTR) gene that p rod u ce s m a lfo rmed ch lor ide channel prote ins that a re u n a b l e to tra nspo rt c h l o r i de i ons, c a us i ng a n i n c rease in the entry of N a + i ons i nto the ce l l . The h igher i ntra c e l l u l a r c o n centrati o n of NaC I i n c reases th e f l ow of wate r i nto the c e l l , and the m u c i n that i s re l eased i nto t h e extra c e l l u l a r env i ro nme nt c a n not become no rma l ly hyd rated , th us m a ki ng the m u c us th i c ke r th an no rma l , wh i c h obstru cts the very sma l l b ro n ch i o l a r passageways of the l u ngs . As th e d isease prog resses, infecti ons resu lt, th e l u n gs b e come unab l e to fu n ctio n p rope rly, a n d the i n d iv id u a l s u c c u m bs to the d i sease a n d d i es .
B. Active transport i s an energy-requir ing process that transports a molecule aga inst an electrochemical gradient via carrier proteins. 1 . Na+ -K+ pump
a . Mechan ism. The Na + -K+ pump involves the anti port transport ofNa + and K+ ions mediated by the carrier protein, Na+ -K+ adenosine tri phosphatase (ATPase). (1) Three Na+ ions are pumped out of the cell and two K+ ions are pumped i nto the cell. (2) The hydrolysis of a single adenosine triphosphate (ATP) molecule by the Na+ -K+ ATPase
is required to transport five ions. b. Function
(1) The primary function is to mainta in constant ce l l vo lume by decreasing the intracellular ion concentration (and thus the osmotic pressure) and increasing the extracellular ion concentration, thus decreasing the flow of water into the cell.
(2) The Na+ -K+ pump also plays a minor role in the maintenance of a potentia l d ifference across the plasma membrane.
2. G lucose transport involves the symport movement of glucose across an epithelium (transepithe l ia l transport). Transport is frequently powered by an electrochemical Na+ gradient, which drives carrier proteins located at specific regions of the cell surface.
3. AlP-b ind ing cassette transporters (ABC transporters) are transmembrane proteins that have two domains, the intracellularly facing nucleotide-b ind ing domain (AlP-b ind ing domain ) and the membrane-spann ing domain (transmembrane domain) . In eukaryotes, ABC transporters function in exporting materials, such as toxins and drugs, from the cytoplasm into the extracellular space, using ATP as an energy source. ABC transporters may have additional functions, such as those of the placenta, which presumably protect the developing fetus from xenobiotics, macromolecules such as antibiotics, not manufactured by cells of the mother.
CLINICAL CONSIDERATIONS
Multidrug-resistant (MDR) prote ins a re ABC transporters that a re present in c e rta i n c a n c e r ce l l s that a re a b l e to transpo rt the cytotoxic d rugs a dm in
iste red to treat the ma l i g n ancy. I t has been shown that i n mo re th an one -th i rd o f the cancer pat ients, th e ma l i g n ant ce l l s deve l op MDR prote i ns that i nterfere with the treatm ent moda l ity be i ng used .
C. Fac i l itated d iffusion of ions can occur via ion channel proteins or ionophores. 1. Selective ion channel proteins permit only certain ions to traverse them.
a. K+ leak channels are the most common ion channels. These channels are ungated and leak K+ , the ions most responsible for establishing a potential difference across the plasmalemma.
b. Gated ion channels open only transiently in response to various stimuli. They include the following types: (1) Voltage-gated channels open when the potential difference across the membrane
changes (e.g., voltage-gated Na+ channels, which function in the generation of action potentials ; see Chapter 9 VIII B 1 e) .
(2) Mechanica l ly gated channels open in response to a mechanical stimulus (e.g., the tactile response of the hair cells in the inner ear) .
l!iitJtttDI Plasma Membrane 7
(3) Ligand-gated channels open in response to the binding of a s igna l ing molecule or i on . These channels include neurotransmitter-gated channels, nucleotide-gated channels, and G protein-gated K+ channels of cardiac muscle cells.
CLIN ICAL CONSIDERATIONS
Ligand-gated ion channels a re p roba b ly the l o c ation whe re a nesth eti c a g e nts a ct to b l o c k the sp re a d of a ctio n potenti a ls .
2. lonophores are lipid-miscible molecules that form a complex with ions and insert into the lipid bilayer to transport those ions across the membrane. There are two ways in which they perform this function: a. They enfold the ion and pass through the lipid bilayer. b. They insert into the cell membrane to form an ion channel whose lumen is hydrophilic. lonophores are frequently fed to cattle and poultry as antibiotic agents and growth-enhancing substances.
A. S igna l ing molecu les, secreted by signaling cells, bind to receptor molecules of target cells, and in this fashion, these molecules function in cell-to-cell communication in order to coordinate cellular activities. Examples of such signaling molecules that effect communications include neurotransmitters, which are released into the synaptic cleft (see Chapter 8 IV A l b; Chapter 9 IV B 5); endocrine hormones, which are carried in the bloodstream and act on distant target cells; and hormones released into the intercellular space, which act on nearby cells (paracrine hormones) or on the releasing cell itself ( autocrine hormones) . 1 . Li p id-so lub le s igna l ing molecules penetrate the plasma membrane and bind to receptors
within the cytoplasm or inside the nucleus, activating intracellular messengers. Examples include hormones that influence gene transcription.
2. Hydroph i l i c s igna l ing molecules bind to and activate cel l -surface receptors (as do some lipidsoluble signaling molecules) and have diverse physiologic effects (see Chapter 13). Examples include neurotransmitters and numerous hormones (e.g., serotonin, thyroid-stimulating hormone, insulin).
B . Membrane receptors are primarily integral membrane glycoproteins. They are embedded in the lipid bilayer and have three domains : an extracel lu lar domain that protrudes into the extracellular space and has binding sites for the signaling molecule, a transmembrane domain that passes through the lipid bilayer, and an i ntrace l l u la r domain that is located on the cytoplasmic aspect of the lipid bilayer and contacts either peripheral proteins or cellular organelles, thereby transducing the extracellular contact into an intracellular event.
CLIN ICAL CONSIDERATIONS
Venoms, such a s t hose o f some po i sonous sna kes, i n a ctivate a c etyl c ho l i n e re c e ptors o f s ke l eta l musc l e s a r co l emma at n e u romuscu l a r j u n ctions .
Auto immune d iseases m ay l e a d to th e p ro d u ctio n of a nti bod i es that s p e c ifi c a l ly b ind to and activate certa in p lasma membrane receptors. An exa m p l e i s Graves d isease ( hyperthyro i d i sm ) ( see C h a pter 1 3 1V B ) .
1 . Function a . Membrane receptors contro l plasmalemma permeab i l ity by regulating the conformation of
ion channel proteins. b . They regu l ate the entry of molecu les into the cell (e.g. , the delivery of cholesterol via
low-density lipoprotein receptors) . c. They b ind extrace l lu lar matrix molecules to the cytoskeleton via i ntegrins, which are
essential for cell-matrix interactions.
8 BRS Ce l l B io logy and H isto logy
d . They act as transducers to translate extracellular events into an intracellular response via the second messenger systems.
e. They permit pathogens that mimic normal ligands to enter cells. 2. Types of membrane receptors (See Table 1 .2) .
a . Channel- l i nked receptors bind a signaling molecule that temporarily opens or closes the gate, permitting or inhibiting the movement of ions across the cell membrane. Examples include n icoti n ic acetylcho l ine receptors on the muscle-cell sarcolemma at the myoneural junction (see Chapter 8 IV A) .
b. Catalytic receptors are single-pass transmembrane proteins. (1) Their extracellular moiety is a receptor and their cytop lasmic component is a protein
kinase. (2) Some catalytic receptors lack an extracytoplasmic moiety and, as a result, are
continuously activated; such defective receptors are coded for by some oncogenes. (3) Examples of catalytic receptors include the following:
(a ) Insu l i n binds to its receptor, which autophosphorylates. The cell then takes up the insulin-receptor complex by endocytosis, enabling the complex to function within the cell.
(b) G rowth factors (e.g., epidermal growth factor, platelet-derived growth factor) bind to specific catalytic receptors and induce mitosis.
c. G prote in-l inked receptors are transmembrane proteins associated with an ion channel or with an enzyme that is bound to the cytoplasmic surface of the cell membrane. (1) These receptors interact with heterotrimeric G prote in (guanosine triphosphate [GTP]
binding regulatory protein) after binding of a signaling molecule. The heterotrimeric G protein is composed of three subunits :� /3. and ycomplex. The binding ofthe signaling molecule causes either (a ) the dissociation of the a subunit from the � and y complex where the a subunit
interacts with its target or (b ) the three subunits do not dissociate, but either the a subunit and/or the � and y
complex become activated and can interact with their targets. This interaction results in the activation of i ntrace l l u la r second messengers, the most common of which are cyclic adenosine monophosphate (cAMP), Ca2+ , and the i nositol phospho l ip id-s igna l ing pathway.
(2) Examples include the following: (a ) Heterotrimeric G prote ins (Table l . l ) , which are folded in such a fashion that they
make seven passes as they penetrate the cell membrane. These are stimulatory G protein (G5) (Figure 1 .6); inhibitory G protein (G;)i phospholipase C activator G protein (Gq)i olfactory-specific G protein (G.11); transducin (G1) ; G., which acts to open K+ channels and close Ca2+ channels; and G12113, which controls the formation of the actin component of the cytoskeleton and facilitates migration of the cell.
(b) Monomeric G prote ins ( l ow-mo lecular-weight G prote ins) are small single-chain proteins that also function in signal transduction. 1. Various subtypes resemble Ras, Rho, Rab, and ARF proteins. 2. These proteins are involved in pathways that regulate cell proliferation and
differentiation, protein synthesis, attachment of cells to the extracellular matrix, exocytosis, and vesicular traffic.
CLINICAL CONSIDERATIONS
Cholera toxin i s a n exotoxi n p ro d u ced by the b a cteri u m Vibrio cholerae that a lters G. p rote i n , so that it is u n a b l e to hydro lyze its GTP mo l e c u l e .
As a resu lt, cAM P leve ls i n c rease i n th e s u rfa c e -a bso rptive ce l l s o f t h e i ntesti ne , l e a d i n g to excess ive loss of e l e ctrolytes a n d wate r a n d severe d i a rrh e a .
Pertussis toxin, t h e p ro d u ct o f t h e b a cter i um that c a uses whoop i n g c o ugh , i n se rts AD P-r i bose i nto the a subun its of tr ime ri c G p rote i ns, caus ing the a c c u m u lati o n of the i n a ctive form of G p rote i n s resu lti n g i n i rritati o n o f the m u c osa of the bron ch i a l p assages .
Defective G5 prote ins may l e ad to menta l reta rd ation , d im i n i shed g rowth a n d sexu a l d eve l opment, a n d d e c reased responses to c e rta i n ho rmones .
l!iitJtttDI P l asma Membrane 9
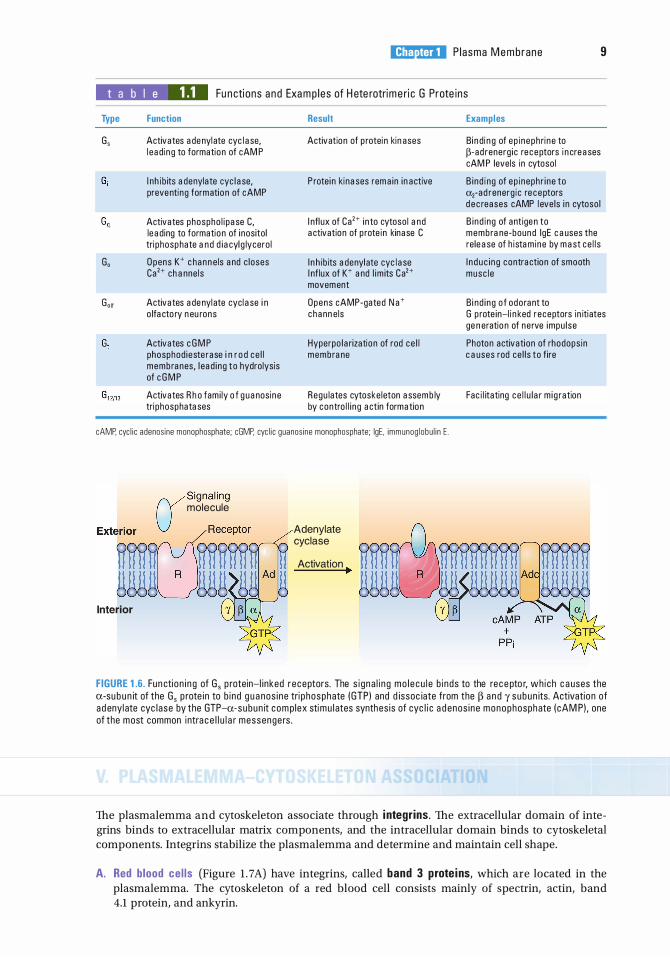
t a b I e 1.1 Fu ncti ons and Examp les of H ete rotrime ri c G Prote ins
Type
G,
G,
G,"
Function
Activates adenylate cyc lase, l eading to formation of cAM P
I nh ib its adenylate cyc lase, preventing formation of cAMP
Activates phospho l i pase C, leading to formation of i nositol tri phosphate and d iacyl g lycero l
O pens K+ c hannels and c loses Ca2+ channe ls
Activates adenylate cyclase in o lfacto ry neu rons
Activates c G M P phosphod ieste rase i n r o d ce l l membranes, l ead i ng t o hydrolysis of c G M P
Activates R h o fam i ly o f g uanosine tri phosphatases
Result
Activation of p rotein kinases
P rote i n kinases remain inactive
Infl ux of Ca2+ into cytoso l and activation of p rote in kinase C
I nhib its adenylate cyc lase I nf lux of K+ and l im its Ca2+ movement
Opens cAMP-gated Na+ c hannels
Hyperpo larization of rod ce l l membrane
Regu lates cytoske leton assemb ly by contro l l ing actin formation
cAMP, cyc l i c adenos ine monophosphate; cGMP. cyc l i c guanos ine monophosphate; lgE, immunog lobu l i n E .
USignal ing molecule
-���; ggggl:)ggg g "-r-1�'----__,/ Interior
Adenylate cyclase
Activation �
Examples
Binding of ep ineph rine to 13-ad renerg ic re ceptors increases cAM P levels in cytoso l
B i nd ing of ep inephr i ne to �-ad renerg ic re ceptors d e c reases cAMP l eve ls in cytoso l
B i nd ing of antigen to membrane-bound lgE causes the release of h i stamine by mast ce l l s
I n d u c ing contraction of smooth musc l e
B ind i ng o f odorant to G p rote in-l inked receptors in itiates generation of nerve impu l se
Photon activation of rhodops in causes rod ce l l s to fire
Fac i l itating ce l l u lar m i g ration
FIGURE 1.6. Fun cti on i ng of G, p rotein-l i nked receptors. The s i gna l i ng mo l e cu l e b i nds to the rec e pto r, wh ich c a uses the a-su b u n it of the G, p rote in to b i nd g u a nos i ne tri phosphate (GTPI and d issoc iate from the 13 a n d y subun its. Activation of a d enyl ate cyc l ase by the GTP-u-subun it com p lex stimu l ates synthes is of cyc l i c a d enos i ne monophosphate (cAM PI , one of the most common intra c e l l u l a r messengers .
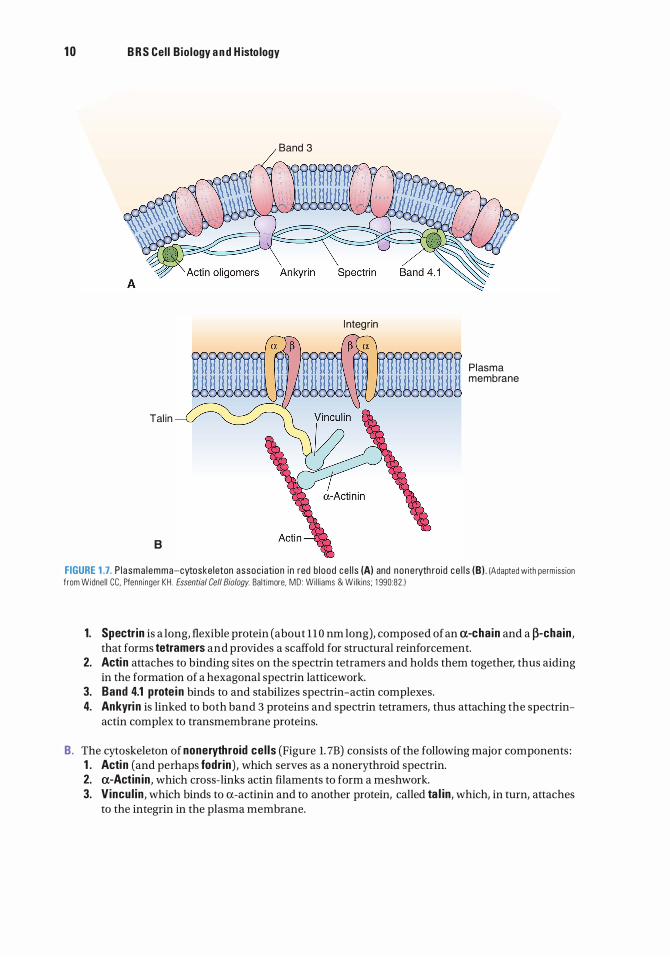
The plasmalemma and cytoskeleton associate through i ntegrins. The extracellular domain of integrins binds to extracellular matrix components, and the intracellular domain binds to cytoskeletal components. Integrins stabilize the plasmalemma and determine and maintain cell shape.
A. Red blood ce l ls (Figure 1 . 7A) have integrins, called band 3 prote ins, which are located in the plasmalemma. The cytoskeleton of a red blood cell consists mainly of spectrin, actin, band 4.1 protein, and ankyrin.
1 0 B R S Cel l B io logy a n d H isto logy
Band 3
Tal in
B
l nteg rin
P lasma membrane
FIGURE 1.7. P l asma l emma-cytoske leton assoc i ation in red b l ood ce l l s (A) and none ryth ro id ce l l s (B).IAdapted with permiss ion from Widne l l CC. Pfenn inger KH . Essential Gel/Biology. Balt imore, MD : Wi l l iams & Wi lkins ; 1 990:82. 1
1. Spectr in is a long, flexible protein (about 1 1 0 nm long), composed of an a-chain and a �-chain , that forms tetramers and provides a scaffold for structural reinforcement.
2. Actin attaches to binding sites on the spectrin tetramers and holds them together, thus aiding in the formation of a hexagonal spectrin latticework.
3. Band 4.1 prote in binds to and stabilizes spectrin-actin complexes. 4. Ankyri n is linked to both band 3 proteins and spectrin tetramers, thus attaching the spectrin
actin complex to transmembrane proteins.
B. The cytoskeleton of nonerythroid cel ls (Figure 1. 7B) consists of the following major components : 1 . Actin (and perhaps fodr in) , which serves as a nonerythroid spectrin. 2. a-Actin in , which cross-links actin filaments to form a meshwork. 3. Vincul in , which binds to a-actinin and to another protein, called ta l in , which, in turn, attaches
to the integrin in the plasma membrane.
l!iitJtttDI Plasma Membrane
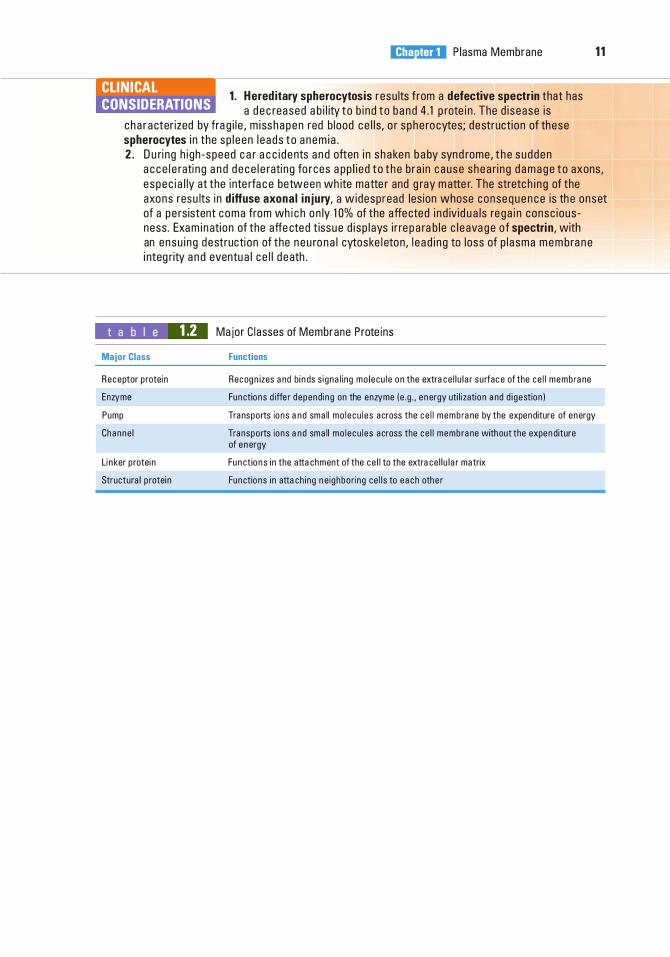
1 . Hered itary spherocytosis resu lts from a defective spectrin that has CLIN ICAL CONSIDERATIONS a d e c reased a b i l ity to b i nd to b a n d 4 . 1 p rote i n . The d i sease i s
c h a r a cter ized by fra g i l e , m i ss hapen red b lood c e l l s, o r s phe ro cytes; destructi on of these spherocytes i n the s p l e en l e a ds to a n em i a .
1 1
2 . D u ri ng h i gh - speed c a r a c c i d ents a n d often i n s h a ken b a by synd rome , t h e s udden a c c e l e rati n g a n d d e c e l e rati ng fo rces a pp l i e d t o t h e b ra i n c a u se s hea ri n g d a m a g e t o axons, e spec i a l ly at the i nte rfa c e between wh ite matte r and g ray m atte r. The stretc h i n g of the axons resu lts i n diffuse axona l in jury, a w idespread les ion whose conse q u e n c e is th e onset of a pe rsistent coma from wh i c h o n ly 1 0% of the affe cted i n d iv id u a ls re ga i n consc i ous ness . Exa m i n ati on of the affe cted t issu e d i s p l ays i r re p a ra b l e c l e ava g e o f spectri n , with an ensu i ng destructi on of the n e u ro n a l cytoske l eton, l e a d i n g to loss of p l a sma m e m bra n e i nteg rity a n d eventu a l c e l l d e ath .
t a b I e 1.2 Major Class
Receptor p rotein
Enzyme
Pump
Channe l
linker p rotein
Structural p rotein
Major C l asses of Membrane Prote ins
Functions
Recognizes and binds s i gnal ing mo l ecu l e on the extrace l l u lar su rfac e of the ce l l memb rane
Functions d iffe r depending on the enzyme (e . g . , energy uti l ization and d i gestion)
Transports ions and small mo l ecu l e s across the ce l l memb rane by the expenditure of energy
Transports ions and small mo l ecu l e s across the ce l l membrane without the expenditure of energy
Functions in the attachment of the ce l l to the extrace l l u lar matrix
Functions in attach ing neig hboring ce l l s to each othe r
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . A herpetologist is bitten by a poisonous snake and is taken to the emergency department with progressive muscle paralysis. The venom is probably incapacitating his
(A) Na + channels. (B ) Ca2+ channels. (C) phospholipids. (D ) acetylcholine receptors. (E) spectrin.
2. Cholesterol functions in the plasmalemma to
(A) increase fluidity of the lipid bilayer. (B ) decrease fluidity of the lipid bilayer. (C) facilitate the diffusion of ions through the
lipid bilayer. (D ) assist in the transport of hormones across
the lipid bilayer. (E ) bind extracellular matrix molecules.
3. The cell membrane consists of various components, including integral proteins. These integral proteins
(A) are not attached to the outer leaflet. (B ) are not attached to the inner leaflet. (C) include transmembrane proteins. (D ) are preferentially attached to the E-face. (E) function in the transport of cholesterol-
based hormones.
4. Which one of the following transport processes requires energy?
(A) Facilitated diffusion (B ) Passive transport (C) Active transport (D ) Simple diffusion
1 2
5 . Which one o f the following substances is unable to traverse the plasma membrane by simple diffusion?
(A) 02 (B ) N2 (C ) Na+ (D ) Glycerol (E ) C02
6. Symport refers to the process of transporting
(A) a molecule into the cell. (B ) a molecule out of the cell. (C) two different molecules in opposite
directions. (D ) two different molecules in the same
direction. (E) a molecule between the cytoplasm and the
nucleus.
7. One of the ways that cells communicate with each other is by secretion of various molecules. The secreted molecule is known as
(A) a receptor molecule. (B ) a signaling molecule. (C) a spectrin tetramer. (D ) an integrin. (E ) an anticodon.
8. Adrenocorticotropic hormone (ACTH) travels through the bloodstream, enters connective tissue spaces, and attaches to specific sites on target-cell membranes. These sites are
(A) peripheral proteins. (B ) signaling molecules. (C) G proteins. (D ) G protein-linked receptors. (E) ribophorins.
9. Examination of the blood smear of a young patient reveals misshapen red blood cells, and the pathology report indicates hereditary spherocytosis. Defects in which one of the following proteins cause this condition?
(A) Signaling molecules (B ) G proteins (C) Spectrin (D ) Hemoglobin (E) Ankyrin
l!iitJtttDI Plasma Membrane 13
1 0. Which of the following statements concerning plasma membrane components is TRUE?
(A) All G proteins are composed of three subunits.
(B ) The glycocalyx is usually composed of phospholipids.
(C) Ion channel proteins are energy dependent (require adenosine triphosphate) .
(D ) Gated channels are always open. (E) Ankyrin binds to band 3 of the red blood
cell plasma membrane.
Answers and Explanations
1 . D . Snake venom usually blocks acetylcholine receptors, preventing depolarization of the muscle cell. The Na+ and Ca2+ channels are not incapacitated by snake venoms (see Chapter 1 IV B) .
2. B . The fluidity of the lipid bilayer is decreased in three ways: ( 1 ) by lowering the temperature, (2) by increasing the saturation of the fatty acyl tails of the phospholipid molecules, and (3) by increasing the membrane's cholesterol content (see Chapter 1 II A 2).
3. C. Integral proteins are not only closely associated with the lipid bilayer but also tightly bound to the cell membrane. These proteins frequently span the entire thickness of the plasmalemma and are thus termed transmembrane proteins (see Chapter 1 II B 1 ) .
4 . C. Active transport requires energy. Facilitated diffusion, which i s mediated by membrane proteins, and simple diffusion, which involves passage of material directly across the lipid bilayer, are types of passive transport (see Chapter 1 III B) .
5. C. Na+ and other ions require channel (carrier) proteins for their transport across the plasma membrane. The other substances are small nonpolar molecules and small uncharged polar molecules. The molecules can traverse the plasma membrane by simple diffusion (see Chapter 1 III A 2) .
6. D . The coupled transport of two different molecules in the same direction is termed "symport" (see Chapter 1 III B) .
7. B . Cells can communicate with each other by releasing signaling molecules, which attach to receptor molecules on target cells (see Chapter 1 IV A).
8. D. G protein-linked receptors are sites where ACTH and some other signaling molecules attach. Binding of ACTH to its receptor causes G5 protein to activate adenylate cyclase, setting in motion the specific response elicited by the hormone (see Chapter 1 IV B 2 c) .
9. C. Hereditary spherocytosis is caused by a defect in spectrin that renders the protein incapable of binding to band 4. 1 protein, thus destabilizing the spectrin-actin complex of the cytoskeleton. Although defects in hemoglobin (the respiratory protein of erythrocytes) also cause red blood cell anomalies, hereditary spherocytosis is not one of them (see Chapter 1 V A) .
1 0. E . Ankyrin is linked both to band 3 proteins and to spectrin tetramer, thus attaching the spectrin-actin complex to transmembrane proteins of the erythrocyte. There are two types of
1 4
G proteins : trimeric and monomeric; glycocalyx (the sugar coat o n the membrane surface) is composed mostly of polar carbohydrate residues; only carrier proteins can be energy requiring; gated channels are open only transiently (see Chapter 1 V A) .
Nucleus
I. OVERVIEW-THE NUCLEUS ( Fi gu re 2.1)
A. Structure. The nucleus, the largest organelle of the cell, includes the nuclear enve lope, nucleo lus, nuc leop lasm, and chromatin and contains the genetic material encoded in the deoxyribonucle ic acid (DNA) of chromosomes.
B. Function. The nucleus directs protein synthesis in the cytoplasm via r ibosomal r ibonucle ic acid (rRNA), messenger RNA (mRNA), and transfer RNA (tRNA). All types ofRNAs, including regu latory RNAs (noncoding RNAs), are synthesized in the nucleus.
The nuclear envelope surrounds the nuclear material and consists of two parallel membranes separated from each other by a narrow perinuclear cisterna. These membranes fuse at intervals, forming openings called nuclear pores in the nuclear envelope.
A. Outer nuclear membrane 1. This membrane is about 6 nanometers (nm) thick. 2. It faces the cytoplasm and is continuous at certain sites with the rough endoplasmic reticulum
(RER) . 3. A loosely arranged mesh of intermediate filaments (vimentin) surrounds the outer nuclear
membrane on its cytoplasmic aspect. 4. R ibosomes stud the cytoplasmic surface of the outer nuclear membrane. These ribosomes
synthesize proteins that enter the perinuclear cisterna.
B. Inner nuclear membrane 1. The inner nuclear membrane is also about 6 nm thick. 2. It faces the nuclear material but is separated from it and is supported on its inner surface
by the nuclear lamina, fibrous lamina that is 80 to 300 nm thick and composed primarily of lamins A, 81 , 82, and C. These intermediate filament proteins form an orthogonal trellis that binds to transmembrane receptor molecules, such as emerin and various l amina-associated po lypeptides traversing the inner nuclear membrane. The various lamins assist in organizing the nuclear envelope, directing the formation of nuclear pore complexes (NPCs), and the
1 5
1 6 B R S Cel l B io logy a n d H isto logy
p
p
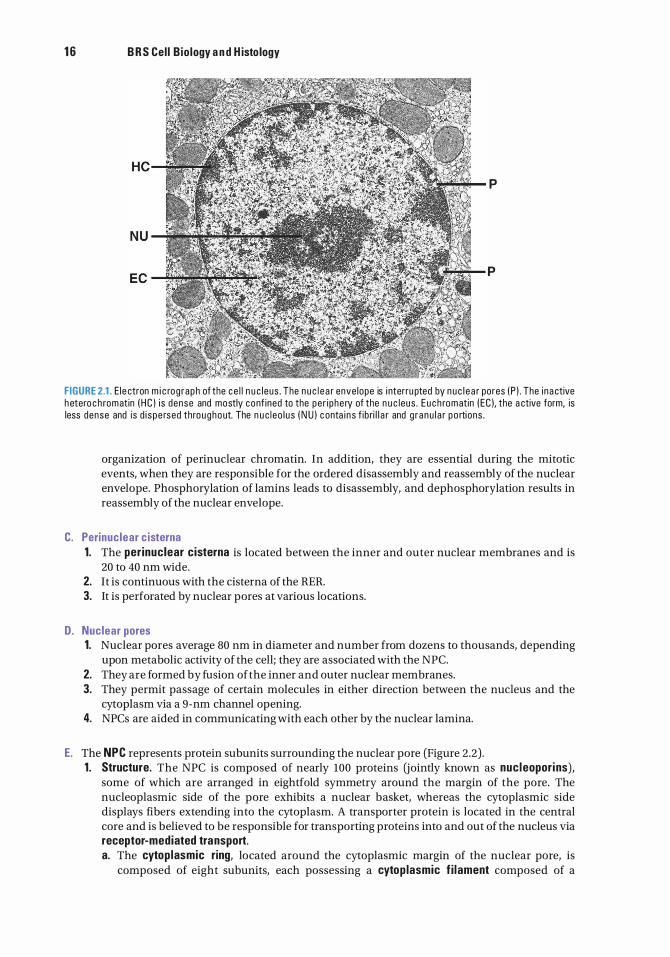
FIGURE 2.1. E le ctron m i c rog raph of the c e l l n u c l eus . The n u c l e a r enve lope is i nterru pted by n u c l e a r pores ( P ) . The i na ctive h etero c h romatin ( H C ) i s dense and mostly conf ined to the pe r i phe ry of the n u c leus . E u c h romatin ( EC ), the a ctive form, is less dense and i s d i s pe rsed throughout. The n u c l eo l u s ( N U ) c onta i n s f ib ri l l a r and g r anu l a r p o rti ons .
organization of perinuclear chromatin. In addition, they are essential during the mitotic events, when they are responsible for the ordered disassembly and reassembly of the nuclear envelope. Phosphorylation of lamins leads to disassembly, and dephosphorylation results in reassembly of the nuclear envelope.
C. Perinuclear cisterna 1. The per inuclear cisterna is located between the inner and outer nuclear membranes and is
20 to 40 nm wide. 2. It is continuous with the cisterna of the RER. 3. It is perforated by nuclear pores at various locations.
D. Nuclear pores 1. Nuclear pores average 80 nm in diameter and number from dozens to thousands, depending
upon metabolic activity of the cell; they are associated with the NPC. 2. They are formed by fusion of the inner and outer nuclear membranes. 3. They permit passage of certain molecules in either direction between the nucleus and the
cytoplasm via a 9-nm channel opening. 4. NPCs are aided in communicating with each other by the nuclear lamina.
E. The NPC represents protein subunits surrounding the nuclear pore (Figure 2.2) . 1 . Structure. The NPC is composed of nearly 100 proteins (jointly known as nucleopori ns),
some of which are arranged in eightfold symmetry around the margin of the pore. The nucleoplasmic side of the pore exhibits a nuclear basket, whereas the cytoplasmic side displays fibers extending into the cytoplasm. A transporter protein is located in the central core and is believed to be responsible for transporting proteins into and out of the nucleus via receptor-mediated transport. a. The cytop lasmic ring, located around the cytoplasmic margin of the nuclear pore, is
composed of eight subunits, each possessing a cytop lasmic f i lament composed of a
Cytoplasmic f i laments
Luminal spoke r ing
Cytoplasmic r ing
l!1Jli!llltl N uc l e u s
N uclear r ing
Distal r ing
1 7
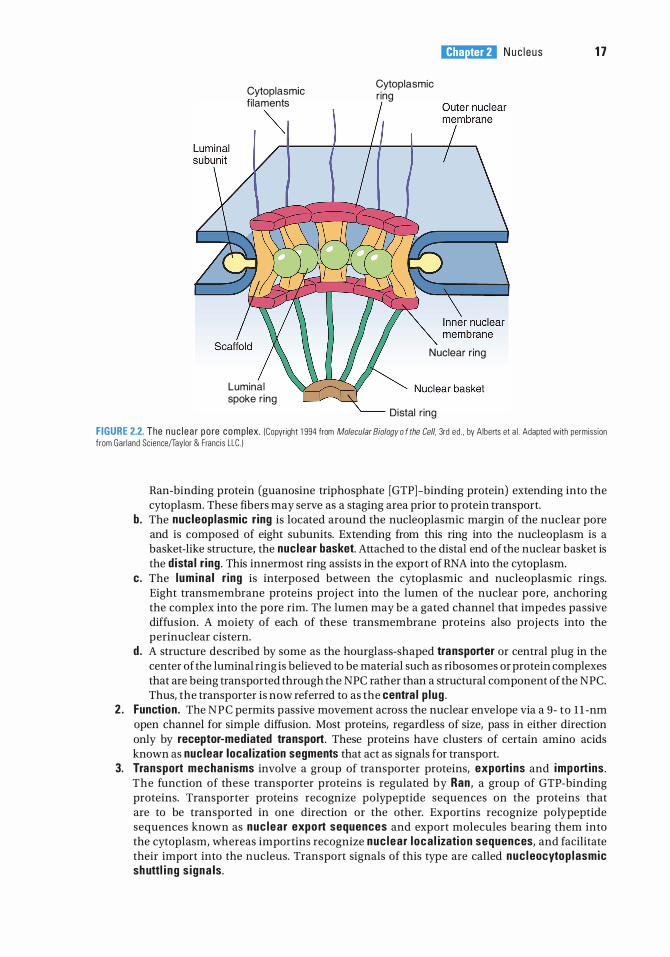
FIGURE 2.2. The n u c l e a r po re comp lex. (Copyright 1 994 from Molecular Biology o f the Cell. 3rd ed . , by Alberts et a l . Adapted with permiss ion from Gar land Sc ience/Taylor & Franc is LLC. )
Ran-binding protein (guanosine triphosphate [GTP] -binding protein) extending into the cytoplasm. These fibers may serve as a staging area prior to protein transport.
b. The nucleoplasmic r ing is located around the nucleoplasmic margin of the nuclear pore and is composed of eight subunits. Extending from this ring into the nucleoplasm is a basket-like structure, the nuclear basket. Attached to the distal end of the nuclear basket is the d ista l r ing . This innermost ring assists in the export of RNA into the cytoplasm.
c. The l um ina l r ing is interposed between the cytoplasmic and nucleoplasmic rings. Eight transmembrane proteins project into the lumen of the nuclear pore, anchoring the complex into the pore rim. The lumen may be a gated channel that impedes passive diffusion. A moiety of each of these transmembrane proteins also projects into the perinuclear cistern.
d . A structure described by some as the hourglass-shaped transporter or central plug in the center of the luminal ring is believed to be material such as ribosomes or protein complexes that are being transported through the NPC rather than a structural component of the NPC. Thus, the transporter is now referred to as the centra l p lug .
2 . Function . The NPC permits passive movement across the nuclear envelope via a 9- to 1 1 -nm open channel for simple diffusion. Most proteins, regardless of size, pass in either direction only by receptor-mediated transport. These proteins have clusters of certain amino acids known as nuclear local ization segments that act as signals for transport.
3. Transport mechan isms involve a group of transporter proteins, exporti ns and import ins . The function of these transporter proteins is regulated by Ran, a group of GTP-binding proteins. Transporter proteins recognize polypeptide sequences on the proteins that are to be transported in one direction or the other. Exportins recognize polypeptide sequences known as nuc lear expo rt sequences and export molecules bearing them into the cytoplasm, whereas importins recognize nuc lear l oca l izati on sequences, and facilitate their import into the nucleus. Transport signals of this type are called nuc l eocytop lasmic shuttl i ng s igna ls .
1 8 B R S Cel l B io logy a n d H isto logy
A. Structure . The nucleolus is a nuclear inclusion that is not surrounded by a membrane. It is observed in interphase cells that are actively synthesizing proteins; more than one nucleolus can be present in the nucleus. It contains mostly rRNA and proteins, such as nucleostemin , nuc leo l in , and f ibri l l a rin , along with a modest amount of DNA. I t possesses nucleo lar organizer reg ions (NORs), portions of the chromosomes (in humans, chromosomes 13, 14, 15, 21 , and 22) where rRNA genes are located; these regions are involved in reconstituting the nucleolus during the G, phase of the cell cycle. The nucleolus contains four distinct regions. 1. Fibri l l a r centers are composed of the NORs of the five chromosomes listed above, the
ribonucleoprotein (RNP) signal recogn it ion particle, and RNA po lymerase I , the enzyme required for the transcription of rRNA.
2. The pars f ibrosa is composed of 5-nm fibrils surrounding the fibrillar centers and contains transcriptiona l ly active DNA, r ibosomal genes, and a substantial quantity of rRNA. Additionally, the RNP fi bri l lar in and the phosphoproteins nuc leo l in are located in the pars fibrosa; these proteins participate in the processing of rRNA precursors to form mature rRNA.
3. The pars g ranu losa is composed of 1 5-nm matur ing r ibosomal precursor particles where 185 rRNA and 285 rRNA subunits are assembled. Ribosomal proteins, manufactured in and imported from the cytoplasm, are combined with rRNA to form the small and large ribosomal subunits that are then individually exported into the cytoplasm, where ribosomal assembly is completed (see Chapter 3, Cytoplasm and Organelles IIIB 1 a) . Additionally, a protein that resembles guanine nucleotide-binding protein, known as nuc leostemin , is located in the pars granulosa. Large quantities of this protein are present in cancer cells and stem cells because it functions in regulating the cell cycle and it also has a direct influence on cell differentiation.
4. Nucleo lar matrix is a fiber network participating in the organization of the nucleolus.
B. Function . The nucleolus is involved in the synthesis of rRNA and its preliminary assembly into ribosome subunit precursors as well as in the primary processing of micro RNAs. The nucleolus also sequesters certain nucleolar proteins, such as nucleostemin, that function as cell cycle checkpoint signaling proteins. These cell cycle regulator proteins remain sequestered in the nucleolus until their release is required for targets in the nucleus and/ or the cytoplasm. Following prophase of the cell cycle, the nucleolus disintegrates because the NORs of chromosomes 13, 14, 15, 21, and 22 are unavailable for transcription. Subsequent to telophase, the NORs unwind and facilitate the reconstitution of the nucleolus.
Nucleoplasm is the protoplasm within the nuclear envelope, in which the chromosomes and nucleoli are embedded. It is a viscous matrix composed mostly of water, whose viscosity is increased by the various types of macromolecules (some from the NPCs) and ions along with transcriptional processing apparatus that are suspended or dissolved in it. It is believed by most authors that the nucleoplasm is ordered by the presence of a cytoskeletal-like framework known as the nuclear matrix. Other authors dispute the presence of this structure.
A. Nuclear matrix acts as a scaffold that aids in organizing the nucleoplasm. 1. Structural components include fibrillar elements, nuclear pore-nuclear lamina complex,
residual nucleoli, and a residual RNP network. 2. Functiona l components are involved in the transcription and processing of mRNA and rRNA,
steroid receptor-binding sites, carcinogen-binding sites, heat shock proteins, DNA viruses, viral proteins (T antigen), and perhaps many other functions that are as yet not known.
l!1Jli!llltl N uc l e us 19
3 . A nucleoplasmic reticu lum i s continuous with the endoplasmic reticulum of the cytoplasm and the nuclear envelope. It contains nuclear calcium functioning within the nucleus and possesses receptors for inositol 1 ,4,5 -triphosphate, regulating calcium signals within compartments of the nucleus related to gene transcription, protein transport, and perhaps other functions.
B. Nuclear particles. 1. lnterchromatin g ranu les are clusters of irregularly distributed particles (20-25 nm in diameter)
that contain RNP and various enzymes. 2. Perichromatin granules (Figure 2 . 1 ) are single dense granules (30-50 nm in diameter)
surrounded by a less dense halo . They are located at the periphery of heterochromatin and exhibit a substructure of 3-nm packed fibrils. a. Perichromatin granules contain 4.7S RNA and two peptides similar to those found in
heterogeneous nuclear RNPs (hnRNPs) . b. They may represent messenger RNPs (mRNPs). c . The number of granules increases in liver cells exposed to carcinogens or temperatures
above 37°C. 3. The hnRNP particles are complexes of precursor mRNA (pre-mRNA) and proteins and are
involved in processing of pre-mRNA. 4. Sma l l nuclear RNPs (snRNPs) are complexes of proteins and smal l RNAs and are involved in
hnRNP splicing or in cleavage reactions.
A. Structure. Chromatin consists of DNA double helix complexed with histones and nonh istone proteins . It resides within the nucleus as heterochromatin and euchromatin. The euchromatin/ heterochromatin ratio is higher in malignant cells than in normal cells. 1 . Heterochromatin is chromatin that is condensed because it is not being transcribed and
comprises approximately 90% of the total chromatin in the cell. It is formed from euchromatin that is folded into 30-nm-thick filaments. a. When examined under the light microscope (LM), it appears as basophilic clumps of
nucleoprotein. b. Although transcriptiona l ly inactive, recent evidence indicates that heterochromatin
functions in maintaining the integrity of chromosomal centromeres and telomeres and, during meiosis, it also has a role in interchromosomal interactions and chromosomal segregation.
c. Heterochromatin corresponds to one of two X chromosomes and is therefore present in nearly all somatic cells of female mammals. During interphase, the inactive X chromosome, referred to as the Barr body (or sex chromatin), is visible as a dark-staining body within the nucleus.
2. Euchromatin, constituting approximately 10% of the total chromatin, is transcriptiona l ly active and appears in light micrographs as a lightly stained region of the nucleus. Viewed with the transmission electron microscope (TEM), euchromatin appears as electron-lucent regions among heterochromatins and is composed of 10-nm strings of nucleosomes (see Sections VI and VII in this chapter) .
B. Function. Chromatin has several functions that include 1 . folding of the DNA strand into small enough volume to be able to contain it within the nucleus
of the cell; 2. protecting the DNA from physical damage during and between cell divisions; 3. controlling the activity of DNA, that is, permitting or preventing its transcription; 4. controlling the precise duplication of the DNA in preparation for cell division; 5. facilitating the repair of DNA in case of replication error or due to physical or chemical insult.
20 BRS Cel l B io logy and H isto logy
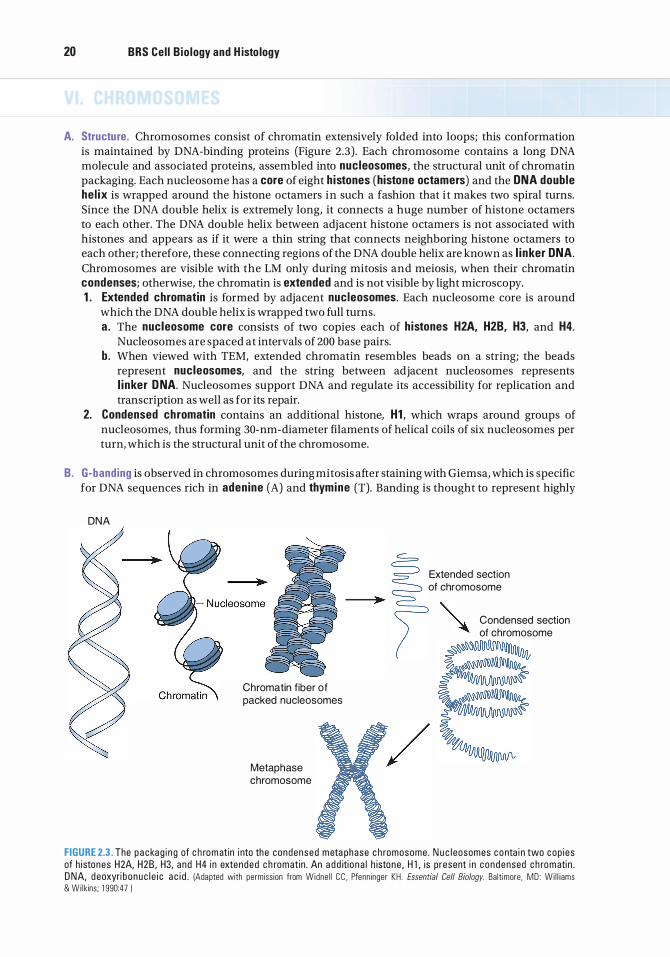
A. Structure . Chromosomes consist of chromatin extensively folded into loops; this conformation is maintained by DNA-binding proteins (Figure 2.3) . Each chromosome contains a long DNA molecule and associated proteins, assembled into nucleosomes, the structural unit of chromatin packaging. Each nucleosome has a core of eight h istones (histone octamers) and the DNA double he l ix is wrapped around the histone octamers in such a fashion that i t makes two spiral turns. Since the DNA double helix is extremely long, it connects a huge number of histone octamers to each other. The DNA double helix between adjacent histone octamers is not associated with histones and appears as if it were a thin string that connects neighboring histone octamers to each other; therefore, these connecting regions of the DNA double helix are known as l i nker DNA. Chromosomes are visible with the LM only during mitosis and meiosis, when their chromatin condenses; otherwise, the chromatin is extended and is not visible by light microscopy. 1 . Extended chromatin is formed by adjacent nucleosomes. Each nucleosome core is around
which the DNA double helix is wrapped two full turns. a . The nucleosome core consists of two copies each of histones H2A, H2B, H3, and H4.
Nucleosomes are spaced at intervals of 200 base pairs. b . When viewed with TEM, extended chromatin resembles beads on a string; the beads
represent nucleosomes, and the string between adjacent nucleosomes represents l i nker DNA. Nucleosomes support DNA and regulate its accessibility for replication and transcription as well as for its repair.
2. Condensed chromatin contains an additional histone, H1 , which wraps around groups of nucleosomes, thus forming 30-nm -diameter filaments of helical coils of six nucleosomes per turn, which is the structural unit of the chromosome.
B. G-banding is observed in chromosomes during mitosis after staining with Giemsa, which is specific for DNA sequences rich in adenine (A) and thymine (T). Banding is thought to represent highly
DNA
Chromatin f iber of packed nucleosomes
Metaphase chromosome
Extended section of chromosome
" Condensed section � of chromosome
FIGURE 2.3. The p a c kag i ng of c h romatin i nto the condensed m eta phase c h romosome . N u c l eosomes c o nta i n two cop i es of h istones H2A, H2B , H3, a nd H4 in extended c h romat in . An a d d iti o n a l h istone , H l , is present i n c ondensed c h romati n . D NA, d eoxyri bonuc l e i c a c i d . )Adapted with permiss ion from Widne l l C C . Pfenn inger KH . Essential Cell Biology. Balt imore. MD : Wi l l iams & Wi l kins ; 1 990:47 )
l!1Jli!llltl Nuc l eus 21
folded DNA loops. G-banding is characteristic for each species and is used to identify particular chromosomes and chromosomal anomalies.
C. Karyotype refers to the number and morphology of chromosomes and is characteristic for each species. 1 . Hap lo id number (n) is the number of chromosomes in germ cells (23 in humans) . 2. D ip lo id number (2n) is the number of chromosomes in somatic cells (46 in humans).
D. The total genetic complement of an individual is stored in its chromosomes. In humans, the genome consists of22 pairs of autosomes and 1 pair of sex chromosomes (either XX or XV), totaling 23 homologous pairs, or 46 chromosomes.
E. Each chromosome is composed of two chromatids joined together at a small point called the centromere.
DNA is a long double-stranded helical linear molecule composed of multiple nucleotide sequences. It stores the individual's genetic information and acts as a template for the synthesis of RNA. The complete nucleotide sequences of a human are located in the 46 chromosomes of each cell and if stretched out and placed end to end it would measure almost 6 ft in length.
A. Nucleotides are composed of a base (purine or pyrimidine), a deoxyribose sugar, and a phosphate group. 1 . The purines are aden ine (A) and guan ine (G). 2. The pyrimid ines are cytosine (C) and thymine (T).
B. The DNA double hel ix consists of two complementary DNA strands held together by hydrogen bonds between the base pairs A-T and G-C.
C. Exons are regions of the DNA molecule that code for specific RNAs.
D. l ntrons are regions of the DNA molecule, between exons, that do not code for RNAs.
E. A codon is a sequence of three bases in the DNA molecule that codes for a s ing le amino ac id .
F. A gene is a segment of the DNA molecule, located in a specific region of a chromosome. I t i s responsible not only for the formation of a single RNA molecule but also for the regulatory sequences that control the expression of a particular trait. In certain viruses, a gene may be composed of RNA rather than DNA.
G. A genome is the complete set of hereditary information that an individual possesses. These are classified into two categories, genes and non coding segments of the DNA (or RNA in some viruses) . In fact, only about 2% of the genome is composed of genes (which code for proteins/ polypeptides), whereas most of the remainder is no nco ding, in that they do not code for proteins/ polypeptides but possess regulatory or other functions.
CLIN ICAL CONSIDERATIONS
Oncogenes a re th e resu lt of mutations of certa in regulatory genes, c a l l e d proto-oncogenes, which no rm a l ly stim u l ate or i n h i b it c e l l
p ro l iferati on a n d deve l o pment.
1 . G e n eti c a c c i dents or v i ruses may l e a d to the fo rmat ion of o n cogenes . 2 . Whateve r be th e i r o r i g i n , oncogenes dom i n ate th e no rma l a l l e l e s ( p roto - oncogenes) , c a us i ng
deregulation of c e l l d iv is ion , wh i ch l eads to a c a n ce rous state. 3. B l a d d e r c a n c e r and a c ute mye l ogenous l e u kem i a a re c a used by oncogenes .
22 BRS Cel l B io logy and H isto logy
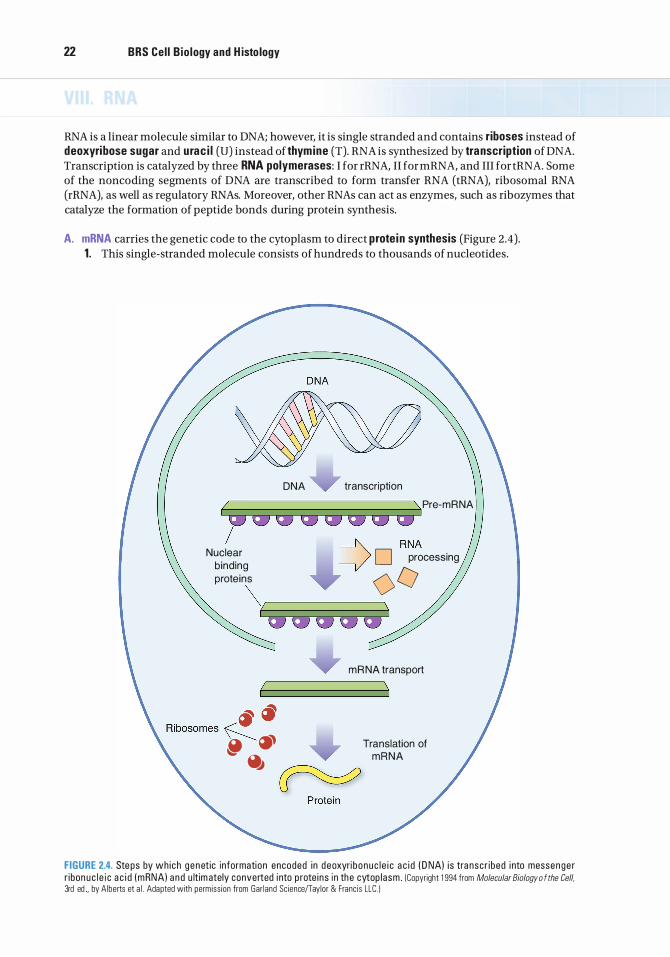
RNA is a linear molecule similar to DNA; however, it is single stranded and contains riboses instead of deoxyribose sugar and urac i l (U) instead of thymine (T). RNA is synthesized by transcription of DNA. Transcription is catalyzed by three RNA polymerases: I for rRNA, II for mRNA, and III for tRNA. Some of the noncoding segments of DNA are transcribed to form transfer RNA (tRNA), ribosomal RNA (rRNA), as well as regulatory RNAs. Moreover, other RNAs can act as enzymes, such as ribozymes that catalyze the formation of peptide bonds during protein synthesis.
A. mRNA carries the genetic code to the cytoplasm to direct prote in synthesis (Figure 2.4). 1. This single-stranded molecule consists of hundreds to thousands of nucleotides.
DNA transcription
� \. Pre-mRNA
, QIJ QIJ QIJ QIJ=>QIJ QIJ :: Nuclear D processing binding 0 proteins V �/ \ [ I QIJ QIJ QIJ QIJ QIJ
� � Ribosomes �
� � � �
m R NA transport
Translation of mANA
FIGURE 2.4. Ste ps by wh ich genet ic informati on encoded in d eoxyri b onuc l e i c a c i d ( D NA) i s tra nscr i bed i nto messenge r r i bon uc l e i c a c i d ( mRNA) a n d u lt im ately converted i nto p rote i ns i n the cytop lasm . (Copyright 1 994 from Molecular Biology o f the Cell. 3rd ed . by Alberts et a l . Adapted with permiss ion from Gar land Sc ience/Taylor & Franc is LLC. )
l!1Jli!llltl N uc l e us 23
2. mRNA contains codons that are complementary to the DNA codons from which it was transcribed, including one start codon (AUG ) for i n itiating protein synthesis and one of three stop codons (UAA, UAG, or UGA) for terminati ng protein synthesis.
3. mRNA is synthesized in the following series of steps. a. RNA po lymerase I I recognizes a promoter on a single strand of the DNA molecule and binds
tightly to it. b. The DNA helix unwinds about two turns, separating the DNA strands and exposing the
codons that act as the template for synthesis of the complementary RNA molecule. c. RNA polymerase II moves along the DNA strand and promotes base pairing between DNA
and complementary RNA nucleotides. d . When RNA polymerase II recognizes a cha in terminator (stop codons-UAA, UAG, or UGA)
on the DNA molecule, it terminates its association with the DNA and is released to repeat transcription.
e. The primary transcript, pre-mRNA after the introns are removed, associates with proteins to form hnRNP .
f . Exons are spliced through several steps, involving spl iceosomes producing an mRNP. g . Proteins are removed as the mRNP enters the cytoplasm, resulting in functional mRNA. h . RNA segments remaining from the transcription process as introns were once thought to
be degraded and recycled because they were believed to have no function. However, recent evidence shows that these RNA segments may become modified to perform regulatory functions that parallel regulatory proteins related to development, gene expression, and evolution.
B. tRNA is folded into a cloverleaf shape and contains approximately 80 nucleotides, terminating in adenylic acid (where amino acids attach) . 1 . Each tRNA combines with a specific amino acid that has been activated by an enzyme. 2. One end of the tRNA molecule possesses an anticodon, a triplet of nucleotides that recognizes
the complementary codon in mRNA. If recognition occurs, the anticodon ensures that the tRNA transfers its activated amino acid molecule in the proper sequence to the growing polypeptide chain.
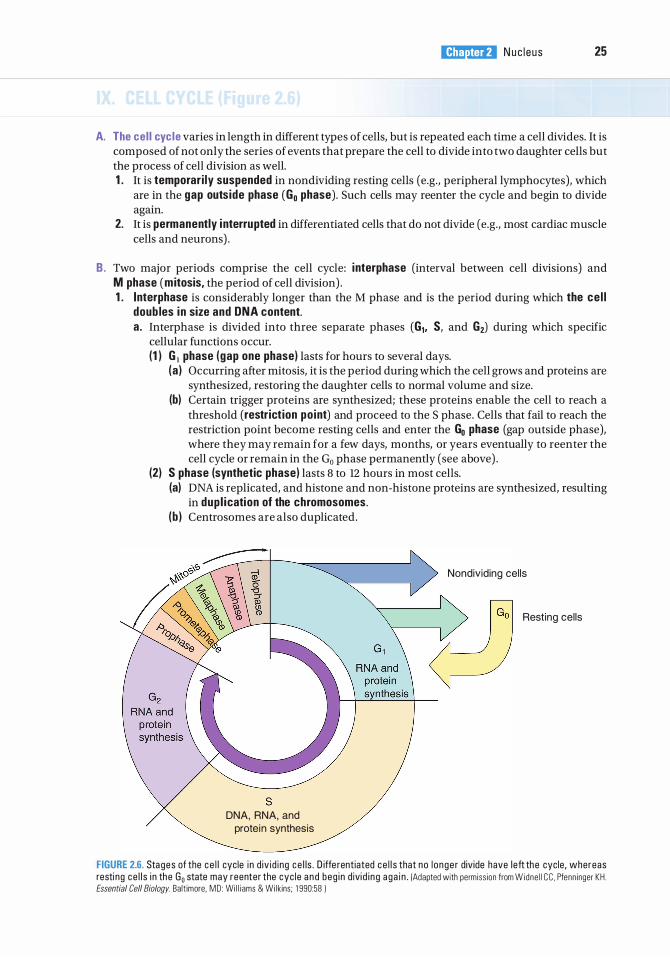
C. R ibosoma l RNA associates with many different proteins (including enzymes) to form ribosomes. 1. rRNA associates with mRNA and tRNA during protein synthesis. 2. rRNA synthesis takes place in the nucleolus and is catalyzed by RNA polymerase I. A single 45S
precursor rRNA (pre-rRNA) is formed and processed to form ribosomes as follows (Figure 2.5) : a. Pre-rRNA associates with ribosomal proteins and is cleaved into the three sizes (28S, 18S,
and 5.8S) of rRNAs present in ribosomes. b. The RNP containing 28S and 5.8S rRNA then combines with 5S rRNA, which is synthesized
outside of the nucleolus, to form the large subunit of the ribosome. c. The RNP containing 18S rRNA forms the sma l l subunit of the ribosome.
D. Regulatory RNAs include micro RNA (miRNA), large intergenic noncoding RNA (lincRNA), and small interfering RNAs (siRNAs). 1 . MicroRNAs (miRNAs), first discovered in the roundworm in the 1990s, are very small segments
of single-stranded RNA molecules of only 19 to 25 nucleotides in length that function to regulate gene expression. Although miRNAs are transcribed from DNA, they are noncoding and are not translated into proteins. Recent research demonstrated the presence of a diverse population of more than 1 ,000 human miRNAs that regulate developmental and physiological processes. Some miRNAs methylate specific regions of the DNA, thus preventing transcription from taking place, whereas other miRNAs insert into a matching portion of the mRNA strand, which prevents the translation of the mRNA; thus, the miRNA acts to regulate gene expression. It has been estimated that miRNAs may regulate a third or more of human genes. Because each miRNA can control hundreds of gene targets, they may influence most genetic pathways. In addition to functioning in gene expression, miRNAs also act as "central switchboards" of signaling networks that control stem cell homeostasis as well as various disease processes such as fibrosis, metastasis, and the biology of malignant cells.

24 BRS Cel l B io logy and H isto logy
5'
-f. ,,!"' -3'
Nuclear envelope
458 rRNA precursor
0 Modification
(methylation)
trimming
N ucleolus
N uclear pore
Cytoplasm
408 ribosomal subunit
�
8 80S ribosome
FIGURE 2.5. Format ion of ri bosoma l r i bonuc l e i c a c i d ( rRNA) and its p rocess ing i nto r i bosoma l s ubun its, wh i c h o c c u rs i n th e n u c l eo l us . (Repr i nted with permiss ion from Swanson et a l . BRS Biochemistry, Molecular Biology, and Genetics. 5th ed . Ba lt imore , MD : Wolters K luwer Hea lth/L ipp i ncott W i l l iams & Wi lkins ; 2009:265.)
2. Large i ntergenic noncoding RNAs ( l incRNAs), more than 200 nucleotides in length, also function in gene regulation. Since each cell of a female possesses two X chromosomes, one of the X chromosomes is transcribed to form lincRNAs that specifically coat that particular X chromosome and prevents the transcription of its genes. Other lincRNAs prevent the transcription of various genes on different chromosomes. Still other lincRNAs compete with certain mRNAs for miRNAs, thereby acting as decoys that protect the mRNAs from the inhibitory actions of miRNAs and facilitating the translation of the mRNA to synthesize a particular protein.
3. Sma l l i nterferi ng RNAs (siRNAs) are similar to miRNAs; they are 19 to 25 nucleotides in length, but they frequently arise from the genome of RNA viruses that infect a cell (although some siRNAs are transcribed from the cell's own genome) . They resemble miRNAs in their mode of action in that they also methylate specific regions of the DNA and thus interfere with the process of transcription.
CLINICAL CONSIDERATIONS
miRNAs have been shown to repress c e rta i n c a n c e r- re l ated g e n es . Add iti o n a l ly, m i RNAs a re known to d e p ress a n g i o genes is , wh i c h may
become usefu l i n c l i n i c a l ly restr icti n g c a n c e r g rowth . Thus , i t i s expe cted that m i RNAs may p rove usefu l i n the d i a g nos i s a n d treatment of c a n c e r. Ce rta i n oth e r m i RNAs a p p e a r h ave been shown to reg u l ate d iffe renti ation ( i . e . , rep ress ing a d i p o cyte formati on , an u n de rsta n d i n g that may l e a d to a c l i n i c a l tre atme nt m o d a l ity fo r obes ity) . Sti l l oth e r m i RNAs rep ress c e rta i n c a n c e r- re l ated g e n es, s u c h as l u n g c a n c e r whe re h u m a n l u n g c a n c e r ce l l s treated with m i R NA had red u c e d the rate of th e i r p ro l iferati on , s l owed g re atly th e i r c a p a b i l ity to m i g rate, and red u ced the i r invas ive a b i l iti es . Add iti o n a l ly, th e treated ce l l s h a d a g reater rate of a p o ptos is ; th us , i t i s expe cted that m i R NAs may p rove usefu l i n the d i a g nos i s a n d treatment o f c a n c e r.
l!1Jli!llltl N uc l e u s 25
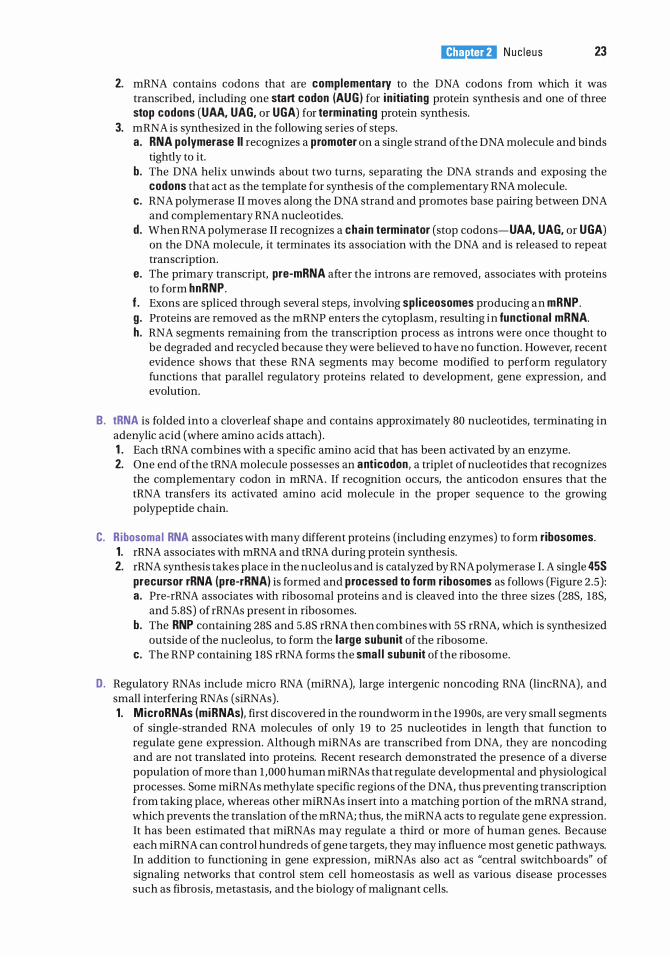
A. The cel l cyc le varies in length in different types of cells, but is repeated each time a cell divides. It is composed of not only the series of events that prepare the cell to divide into two daughter cells but the process of cell division as well. 1 . It is temporar i ly suspended in nondividing resting cells (e.g., peripheral lymphocytes), which
are in the gap outs ide phase (G0 phase) . Such cells may reenter the cycle and begin to divide again.
2. It is permanently interrupted in differentiated cells that do not divide (e.g., most cardiac muscle cells and neurons) .
B . Two major periods comprise the cell cycle: i nterphase (interval between cell divisions) and M phase (mitosis, the period of cell division) . 1 . Interphase is considerably longer than the M phase and is the period during which the ce l l
doub les in size and DNA content. a . Interphase is divided into three separate phases (G1, S, and G2) during which specific
cellular functions occur. (1 ) G 1 phase (gap one phase) lasts for hours to several days.
(a ) Occurring after mitosis, it is the period during which the cell grows and proteins are synthesized, restoring the daughter cells to normal volume and size.
(b) Certain trigger proteins are synthesized; these proteins enable the cell to reach a threshold (restrict ion po int) and proceed to the S phase. Cells that fail to reach the restriction point become resting cells and enter the G0 phase (gap outside phase), where they may remain for a few days, months, or years eventually to reenter the cell cycle or remain in the G0 phase permanently (see above) .
(2) S phase (synthetic phase) lasts 8 to 12 hours in most cells. (a) DNA is replicated, and histone and non-histone proteins are synthesized, resulting
in dup l ication of the chromosomes. (b ) Centrosomes are also duplicated.
s DNA, RNA, and
protei n synthesis
Nondividing cel ls
Rest ing cel ls
FIGURE 2.6. Stages of the ce l l cycle i n d iv id ing ce l ls . D iffe rentiated ce l l s that no l o nge r div ide have le ft the cycle, whereas resti ng ce l l s i n the G0 state may reenter the cyc le a n d beg i n d ivi d i n g a ga i n . IAdapted with permiss ion from Widne l l cc . Pfenn inger KH . Essential Cell Biology. Balt imore. MD : Wi l l i ams & Wi lk ins; 1 990:58 )
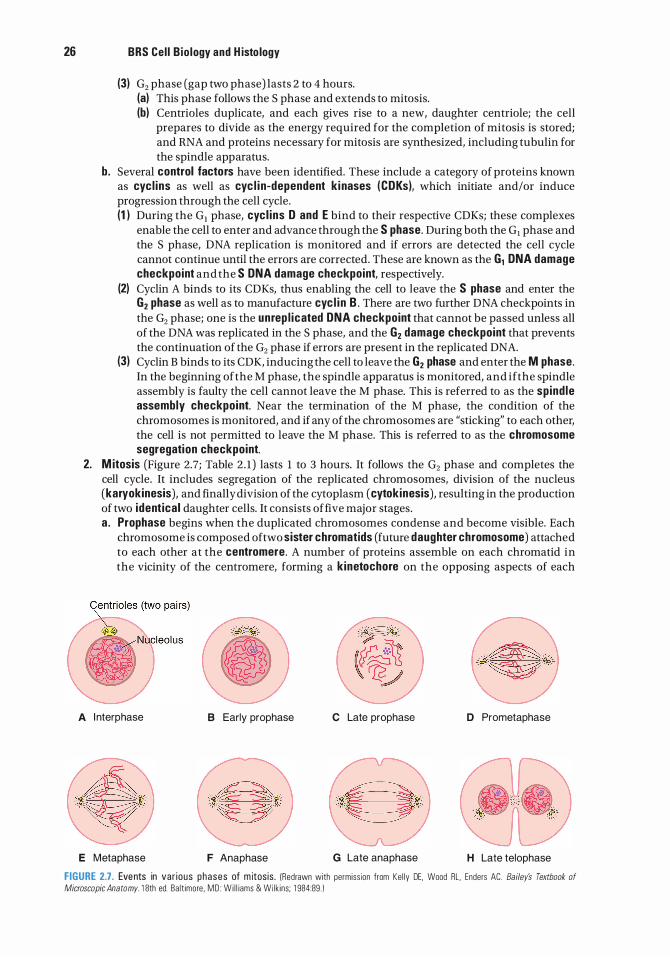
26 BRS Cel l B io logy and H isto logy
(3) G2 phase (gap two phase) lasts 2 to 4 hours. (a) This phase follows the S phase and extends to mitosis. (b) Centrioles duplicate, and each gives rise to a new, daughter centriole; the cell
prepares to divide as the energy required for the completion of mitosis is stored; and RNA and proteins necessary for mitosis are synthesized, including tubulin for the spindle apparatus.
b. Several control factors have been identified. These include a category of proteins known as cycl ins as well as cyc l i n-dependent k i nases (CDKs), which initiate and/or induce progression through the cell cycle. (1 ) During the G1 phase, cycl ins D and E bind to their respective CDKs; these complexes
enable the cell to enter and advance through the S phase. During both the G1 phase and the S phase, DNA replication is monitored and if errors are detected the cell cycle cannot continue until the errors are corrected. These are known as the G1 DNA damage checkpoint and the S DNA damage checkpoint, respectively.
(2) Cyclin A binds to its CDKs, thus enabling the cell to leave the S phase and enter the G2 phase as well as to manufacture cyc l i n B . There are two further DNA checkpoints in the G2 phase; one is the unrep l icated DNA checkpoint that cannot be passed unless all of the DNA was replicated in the S phase, and the G2 damage checkpoint that prevents the continuation of the G2 phase if errors are present in the replicated DNA.
(3) Cyclin B binds to its CDK, inducing the cell to leave the G2 phase and enter the M phase. In the beginning of the M phase, the spindle apparatus is monitored, and if the spindle assembly is faulty the cell cannot leave the M phase. This is referred to as the spind le assembly checkpoint. Near the termination of the M phase, the condition of the chromosomes is monitored, and if any of the chromosomes are "sticking" to each other, the cell is not permitted to leave the M phase. This is referred to as the chromosome segregation checkpoint.
2. M itosis (Figure 2.7; Table 2 . 1 ) lasts l to 3 hours. It follows the G2 phase and completes the cell cycle. It includes segregation of the replicated chromosomes, division of the nucleus (karyokinesis), and finally division of the cytoplasm (cytokinesis), resulting in the production of two ident ical daughter cells. It consists of five major stages. a . Prophase begins when the duplicated chromosomes condense and become visible. Each
chromosome is composed of two sister chromatids (future daughter chromosome) attached to each other at the centromere. A number of proteins assemble on each chromatid in the vicinity of the centromere, forming a kinetochore on the opposing aspects of each
A I nterphase 8 Early prophase C Late prophase D Prometaphase
E Metaphase F Anaphase G Late anaphase H Late telophase
FIGURE 2.7. Events in var ious phases of m itos is . (Redrawn with permiss ion from Ke l ly DE. Wood RL. Enders AC. Bailey's Textbook of
Microscopic Anatomy. 1 8th ed. Ba lt imore . MD : Wi l l iams & Wilk ins; 1 984:89 . 1
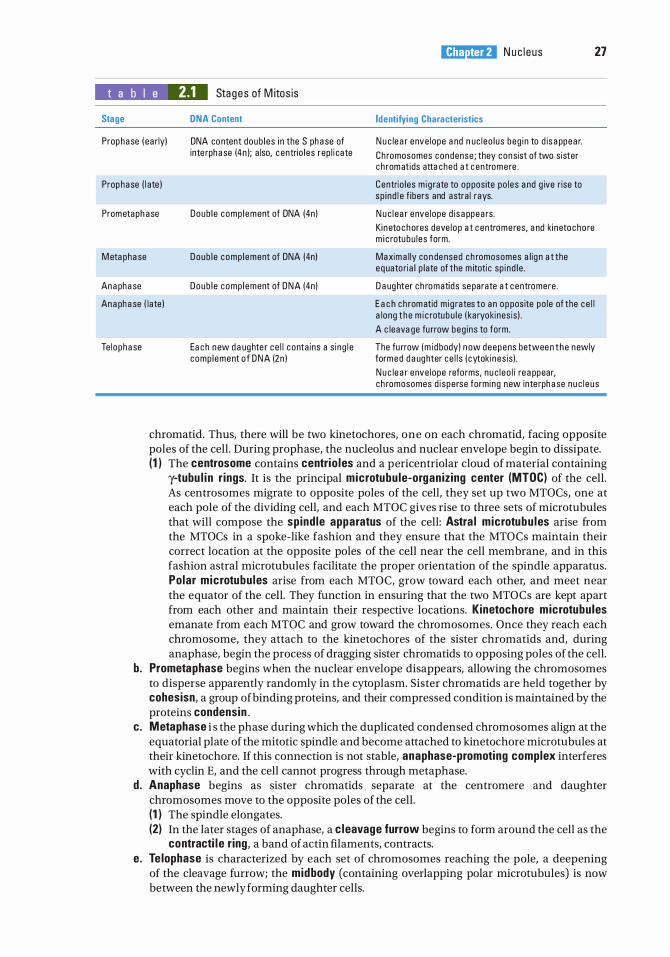
l!1Jli!llltl N uc l e u s 27
t a b I e 2.1 Stages of M itos is
Stage DNA Content Identifying Characteristics
Prophase ( early) DNA content doub les in the S phase of inte rphase (4n); also, c entrio les rep l i cate
N u c lear enve lope and nuc leo l us beg in to d isappear.
Ch romosomes condense ; they consist of two s ister c h romatids attached at c entrome re .
Prophase ( late ) Centrio les m ig rate to opposite po les and g ive r ise to sp ind l e f ibers and astral rays.
Prometaphase Doub le comp lement of DNA (4n) N u c l ear enve lope d isappears.
M etaphase Doub l e comp lement of DNA (4n)
Kinetochores deve l op at c entrome res, and kinetocho re m i c rotubu l es form.
Maximal ly condensed c h romosomes al ign at the equatorial p late of the m itoti c sp ind le .
Anaphase
Anaphase ( late )
Doub l e comp lement of DNA (4n) Daughter c h romatids separate at c entromere .
Each ch romatid m ig rates to an opposite po le of the c e l l a long t h e m i c rotubu l e ( karyokines is ) .
Te lophase Each new daughte r ce l l contains a s ing l e comp lement o f DNA (2n)
A c leavage fu rrow beg ins to form.
The fu rrow (m i dbody) now deepens between the newly formed daughter ce l l s ( cytokines is ) .
N u c lear enve lope refo rms, nu c l eo l i reappear, c h romosomes d i sperse forming new inte rphase nu c l e us
chromatid. Thus, there will be two kinetochores, one on each chromatid, facing opposite poles of the cell. During prophase, the nucleolus and nuclear envelope begin to dissipate. (1 ) The centrosome contains centrio les and a pericentriolar cloud of material containing
y-tubu l i n r ings. It is the principal microtubu le-organ izing center (MTOC) of the cell. As centrosomes migrate to opposite poles of the cell, they set up two MTOCs, one at each pole of the dividing cell, and each MTOC gives rise to three sets of microtubules that will compose the spind le apparatus of the cell: Astra l microtubu les arise from the MTOCs in a spoke-like fashion and they ensure that the MTOCs maintain their correct location at the opposite poles of the cell near the cell membrane, and in this fashion astral microtubules facilitate the proper orientation of the spindle apparatus. Polar microtubu les arise from each MTOC, grow toward each other, and meet near the equator of the cell. They function in ensuring that the two MTOCs are kept apart from each other and maintain their respective locations. Kinetochore microtubules emanate from each MTOC and grow toward the chromosomes. Once they reach each chromosome, they attach to the kinetochores of the sister chromatids and, during anaphase, begin the process of dragging sister chromatids to opposing poles of the cell.
b. Prometaphase begins when the nuclear envelope disappears, allowing the chromosomes to disperse apparently randomly in the cytoplasm. Sister chromatids are held together by cohesisn, a group of binding proteins, and their compressed condition is maintained by the proteins condensin .
c . Metaphase i s the phase during which the duplicated condensed chromosomes align at the equatorial plate of the mitotic spindle and become attached to kinetochore microtubules at their kinetochore. If this connection is not stable, anaphase-promoting complex interferes with cyclin E, and the cell cannot progress through metaphase.
d . Anaphase begins as sister chromatids separate at the centromere and daughter chromosomes move to the opposite poles of the cell. (1 ) The spindle elongates. (2) In the later stages of anaphase, a c leavage furrow begins to form around the cell as the
contracti l e r ing, a band of actin filaments, contracts. e. Te lophase is characterized by each set of chromosomes reaching the pole, a deepening
of the cleavage furrow; the midbody (containing overlapping polar microtubules) is now between the newly forming daughter cells.
28 BRS Cel l B io logy and H isto logy
(1) Micro tubules in the midbody are depolymerized, facilitating cytokinesis and formation of two identical daughter cells.
(2) The nuclear envelope is reestablished around the condensed chromosomes in the daughter cells, and nucleo l i reappear. Nucleoli arise from the specific nucleolar organ iz ing reg ions (called secondary constriction sites), which are carried on five separate chromosomes in humans (see Section III Nucleolus in this chapter) .
(3) The daughter nuclei gradually enlarge, and the condensed chromosomes disperse to form the typical interphase nucleus with heterochromatin and euchromatin.
(4) It appears that at the end of cytokinesis the mother centriole of the duplicated pair moves from the newly forming nuclear pole to the intercellular bridge. This event is necessary to initiate disassembly of the midbody microtubules and complete the separation of the daughter cells. If this event fails, DNA replication is arrested at one of the G1 checkpoints during the next interphase.
lifiW��\- Transformed ce l ls
1 . Tra nsformed ce l l s h ave l ost th e i r a b i l ity to respond to reg u l ato ry s i g na l s contro l l i n g the ce l l cyc l e , a n d by th i s , t hey may u n d e rgo c e l l d iv is ion i n d efi n ite ly, th us becom i ng c a n c e rous .
2 . V inca a lkalo ids may a rrest th ese ce l l s i n m itosis, whereas d r ugs that b l o c k pu r i ne and pyrim i d i n e synth es is may a rrest th ese ce l l s i n the S phase of the c e l l cyc l e .
Apoptosis i s programmed cell death whereby cells are removed from tissues in an orderly fashion as a part o f normal maintenance or during development.
A. Cells that undergo programmed cell death have several morpholog ica l features. 1. They include chromatin condensation, breaking up of the nucleus, and bleb bing of the plasma
membrane. 2. The cell shrinks and is fragmented into membrane-enclosed fragments called apoptotic
bodies.
B. Apoptotic cells do not pose a threat to surrounding cells, because changes in their plasma membranes make them subject to rapid phagocytosis by macrophages and by neighboring cells. Macrophages that phagocytose apoptotic cells do not release cytokines that initiate the inflammatory response.
Further, apoptotic cells may be inhibited by several survival factors produced by certain cells, growth factors, hormones, proteins, etc.
C. The signals that induce apoptosis may occur through several mechanisms. 1. Genes that code for enzymes, called caspases, play an important role in the process. 2. Certain cytokines, such as tumor necrosis factor, may also activate caspases that degrade
regulatory and structural proteins in the nucleus and cytoplasm, leading to the morphological changes characteristic of apoptosis.
D. Defects in the process of programmed cell death contribute to many major diseases. 1. Excessive apoptosis causes extensive nerve cell loss in Alzheimer disease and stroke. 2. Insufficient apoptosis has been linked to cancer and other autoimmune diseases.
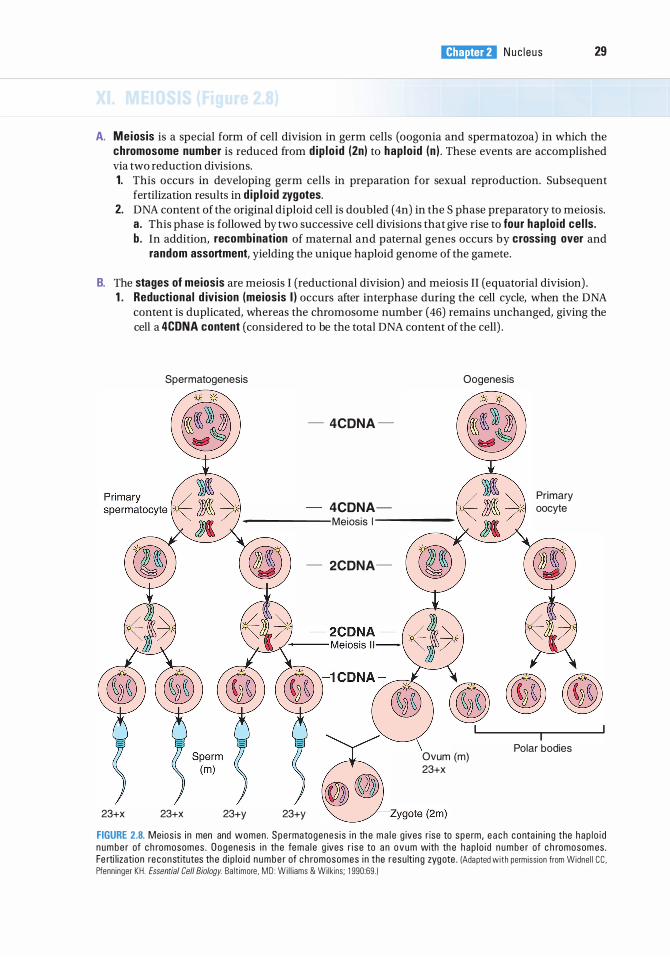
l!1Jli!llltl N uc l e u s 29
A. Meiosis is a special form of cell division in germ cells (oogonia and spermatozoa) in which the chromosome number is reduced from d ip lo id (2n) to hap lo id (n ) . These events are accomplished via two reduction divisions. 1. This occurs in developing germ cells in preparation for sexual reproduction. Subsequent
fertilization results in d ip lo id zygotes. 2. DNA content of the original diploid cell is doubled ( 4n) in the S phase preparatory to meiosis.
a. This phase is followed by two successive cell divisions that give rise to four hap lo id cel ls. b . In addition, recombination of maternal and paternal genes occurs by crossing over and
random assortment, yielding the unique haploid genome of the gamete.
B. The stages of meiosis are meiosis I (reductional division) and meiosis II (equatorial division) . 1 . Reductional d ivision (meiosis I ) occurs after interphase during the cell cycle, when the DNA
content is duplicated, whereas the chromosome number (46) remains unchanged, giving the cell a 4CDNA content (considered to be the total DNA content of the cell) .
23+X
Spermatogenesis
- 4CDNA -
4CDNA-------Me ios is 1 ------
- 2CDNA-
\
Oogenesis
Ovum (m) 23+X
23+X 23+y 23+y
Primary oocyte
Polar bodies
FIGURE 2.8. Meios is i n men and women . Spe rmatogenes i s i n th e ma l e g ives r ise to spe rm, e a c h c o nta i n i n g the hap l o i d n umbe r of c h romosomes . O o genes is i n the fema l e g ives r i s e to a n ovum with th e hap l o i d n u m b e r of c h romosom es. Fe rti l izati on reconstitutes the d i p l o i d n umbe r of c h romosomes i n the resu lti n g zygote . (Adapted wi th permiss ion from Widne l l CC , Pfenn inger KH . Essential Cell Biology. Ba lt imore . MD : W i l l iams & Wi lkins ; 1 990:69. )
30 BRS Cel l B io logy and H isto logy
a . Prophase I is divided into five stages (leptotene, zygotene, pachytene, diplotene, and diakinesis), which accomplish the following events : (1 ) Chromatin condenses into the visible chromosomes, each containing two chromatids
joined at the centromere. (2) Homologous maternal and paternal chromosomes pair via the synaptonemal complex,
forming a tetrad . Crossing over (random exchanging of genes between segments of homologous chromosomes) occurs at the chiasmata, thus i ncreasing genetic d iversity.
(3) The nucleolus and nuclear envelope disappear. b. Metaphase I
(1 ) Homologous pairs of chromosomes align on the equatorial plate of the spindle in a random arrangement, facilitating genetic mixing.
(2) Spindle fibers from either pole attach to the kinetochore of any one of the chromosome pairs, thus ensuring genetic mixing.
c. Anaphase I (1 ) This phase is similar to anaphase in mitosis except in mitosis the two chromatids
are pulled apart and each is delivered to each pole of the cell, whereas in anaphase I of meiosis the four chromatids are separated in such a fashion that two chromatids remain held together as they are being pulled to each pole of the cell.
(2) Chromosomes migrate to the poles. d . Te lophase I is similar to telophase in mitosis in that the nuclear envelope is reestablished
and two daughter cells are formed via cytokinesis. (1 ) Each daughter cell now contains 23 chromosomes (n) number but has a 2CDNA content
(the diploid amount) . (2) Each chromosome is composed of two similar sister chromatids (but not genetically
identical following recombination). 2. Equator ia l d ivision (meiosis II) begins soon after the completion of meiosis I, following a brief
interphase without DNA rep l ication (no S phase) . a . The sister chromatids are portioned out between the two daughter cells formed in meiosis
I . The two daughter cells then divide, resulting in the distribution of chromosomes into four daughter cells, each containing its own unique recombined genetic mater ia l ( 1CDNA;n ) . Thus, every gamete contains its own unique set of genetic materials.
b. The stages of meiosis II are similar to those of mitosis; thus, the stages are named similarly (prophase II, metaphase II, anaphase II, and telophase II) .
c. Meiosis II occurs more rapidly than mitosis.
Nondisjunction of Chromosomes D u ri n g p rophase I of me i os is I , c h romosome pa i rs a l i g n th emse lves at
th e e q u ato ri a l p l ate and exc h a n g e g e n et ic mate ri a l s . D u ri n g a n a phase I , the c h romosome pa i rs wi l l s epa rate a n d beg i n th e i r m i g rati ons to oppos ite po les . Sometimes , th e membe rs of a p a i r fa i l to sepa rate, resu lti n g in o ne d a u g hter c e l l c onta i n i n g a n extra c h romosome (n + 1 = 24), whereas the d a u g hte r ce l l at th e oppos ite po le i s m inus a c h romosome ( n - 1 = 22) . Th is deve l o pment is kn own as nond isjunction . U pon ferti l izati on with a no rma l g a m ete c o nta i n i n g 23 c h romosom es, the resu lti n g zygote w i l l c onta i n e ith e r 47 c h romosomes (tri somy fo r that extra c h romosome ) o r 45 c h romosomes (monosomy fo r tha t m iss i ng c h romosome ) . C h romosomes 8, 9 , 1 3, 1 8, a n d 2 1 a re most fre q uently affe cted by nond isj u n ct ion .
Aneuplo idy, d efi n ed as a n a bno rma l n u m b e r of c h romosomes, can be d etected by ka ryotyp i n g .
1 . Down syndrome (trisomy 21 ) i s c h a ra cte r ized by m e nta l reta rdati on , s ho rt statu re, stu b by a p p e n d a g es, c ongen ita l h e a rt ma lfo rmati ons, a n d oth e r d efe cts.
2. K l inefelter syndrome (XXV) i s a n e u p l o idy of th e sex c h romosomes, c h a ra cte r ized by inferti l ity, va ri a b l e d e g rees of mascu l i n izati on , a n d sma l l testes .
3. Turner syndrome (XO) i s monosomy of the sex c h romosomes, c h a ra cte r ized by sho rt statu re , ste r i l ity, and var ious oth e r a bno rma l iti es .
Review Test
Directions: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . The nuclear pore complex
(A) permits free communication between the nucleus and the cytoplasm.
(B ) is bridged by a unit membrane. (C) is located only at specific nuclear pore sites. (D ) permits passage of proteins via receptor-
mediated transport. (E) has a luminal ring that faces the cytoplasm.
2. Which one of the following nucleotides is present only in RNA?
(A) Thymine (B ) Adenine (C ) Uracil (D ) Cytosine (E ) Guanine
3. Anticodons are located in
(A) mRNA. (B ) rRNA. (C ) tRNA. (D ) snRNP. (E ) hnRNP.
4. DNA is duplicated in the cell cycle during the
(A) G2 phase. (B) S phase. (C) M phase. (D) G, phase. (E) G0 phase.
5. A male child at puberty is determined to have Klinefelter syndrome. Although the parents have been informed of the clinical significance, they have asked for an explanation of what happened. Identify the item that should be discussed with the parents.
(A) Trisomy of chromosome 21 (B ) Loss of an autosome during mitosis (C) Loss of the Y chromosome during meiosis (D ) Nondisjunction of the X chromosome (E ) Loss of the X chromosome
6. Which one of the following is an inclusion not bounded by a membrane that is observable only during interphase?
(A) Nuclear pore complex (B ) Nucleolus (C) Heterochromatin (D ) Outer nuclear membrane (E) Euchromatin
7. A structure that is continuous with RER is the
(A) nuclear pore complex. (B ) nucleolus. (C) heterochromatin. (D ) outer nuclear membrane. (E) euchromatin.
8. Identify the structure that controls movement of proteins in and out of the nucleus.
(A) Nuclear pore complex (B ) Nucleolus (C) Heterochromatin (D ) Outer nuclear membrane (E) Euchromatin
9. The site of transcriptional activity is the
(A) nuclear pore complex. (B ) nucleolus. (C) heterochromatin. (D ) outer nuclear membrane. (E) euchromatin.
1 0. Clumps of nucleoprotein concentrated near the periphery of the nucleus are called
(A) nuclear pore complex. (B ) nucleolus. (C) heterochromatin. (D ) outer nuclear membrane. (E) euchromatin.
31
Answers and Explanations
1 . D . The NPC contains a central aqueous channel that permits passage of small water-soluble molecules. However, movement of proteins in and out of the nucleus is selectively controlled by the NPC via receptor-mediated transport (see Chapter 2 II E) .
2. C. DNA contains the purines, adenine and guanine, and the pyrimidines, cytosine and thymine. In RNA, uracil, a pyrimidine, replaces thymine (see Chapter 2 VII A, VIII) .
3. C. Each tRNA possesses a triplet of nucleotides, called an anticodon, which recognizes the complementary codon in mRNA (see Chapter 2 VIII B) .
4. B . The S (synthesis) phase of the cell cycle is the period during which DNA replication and histone synthesis occur, resulting in duplication of the chromosomes. At the end of the S phase, each chromosome consists of two identical chromatids attached to one another at the centromere (see Chapter 2 IX B) .
5. D . Klinefelter syndrome occurs only in men. This condition results from nondisjunction of the X chromosome during meiosis, resulting in an extra X chromosome in somatic cells. These cells therefore have a normal complement of autosomal chromosomes (22 pairs), and instead of one pair of sex chromosomes (XY), there is an extra X chromosome. These individuals have an XXY genotype, resulting in 47 total chromosomes rather than the normal complement of 46. This syndrome is an example of trisomy of the sex chromosomes. Down syndrome is an example of an autosomal trisomy, specifically trisomy of chromosome number 2 1 . Both syndromes have profound complications (see Chapter 2 XI B Clinical Considerations).
6. B . The nucleolus is an inclusion, not bounded by a membrane, within the nucleus. It is observable during interphase but disappears during mitosis (see Chapter 2 III A) .
7. D. The outer nuclear membrane is continuous with the RER (see Chapter 2 II A) .
8. A. The NPC selectively controls movements of water-soluble molecules and proteins in and out of the nucleus (see Chapter 2 II E) .
9. E. The pale-staining euchromatin is the transcriptionally active chromatin in the nucleus (see Chapter 2 V A) .
1 0. C. Heterochromatin is the dark-staining nucleoprotein near the periphery of the nucleus. I t i s transcriptionally inactive, but may be responsible for proper chromosome segregation during meiosis (see Chapter 2 V A).
32
Cytoplasm and Organelles
I. OVERVIEW-THE CYTOPLASM
The cytoplasm contains three main structural components : organe l les, inc lusions, and the cytoskeleton . The fluid component is called the cytosol. The functional interactions among certain organelles result in the uptake and release of material by the cell, protein synthesis, and intracellular digestion.
A. Organel les (Figure 3 . 1 ) are metabolically active units of cellular matter.
1 . The p lasma membrane, which envelops the cell and forms a boundary between it and adjacent structures, is discussed in Chapter 1 .
2 . R ibosomes a . Structure. Ribosomes are nonmembranous organelles that are 12 nanometers (nm) wide
and 25 nm long and consist of a sma l l and a l a rge subunit. The two subunits are composed of several types of ribosomal ribonucleic acids (rRNAs) and numerous proteins (Table 3 . 1 ; Figure 2.5) .
b. Ribosomes may be free in the cytosol or bound to membranes of the rough endoplasmic reticulum (RER) or the cytoplasmic surface of the outer nuclear membrane. Whether free or bound, the ribosomes constitute a single interchangeable population.
c. A po lyribosome (po lysome) is a cluster of ribosomes along a single strand of messenger ribonucleic acid (mRNA) where every ribosome is concurrently engaged in protein synthesis.
d . Function. Ribosomes are the sites where mRNA is translated i nto prote in . Proteins destined for transport (secretory, membrane, and lysosomal) are synthesized on polyribosomes bound to the RER, whereas proteins not destined for transport are synthesized on polyribosomes in the cytosol. Protein synthesis that forms proteins not destined for transport occurs in the following manner (synthesis of proteins destined to be transported is discussed below in Section III b) : (1 ) The sma l l r ibosomal subunit binds both mRNA and activated transfer ribonucleic acids
(tRNAs); the codons of the mRNA then base-pa i r with the corresponding anticodons of the tRNAs.
(2) Next, an initiator tRNA recognizes the start codon (AUG) on the mRNA.
33
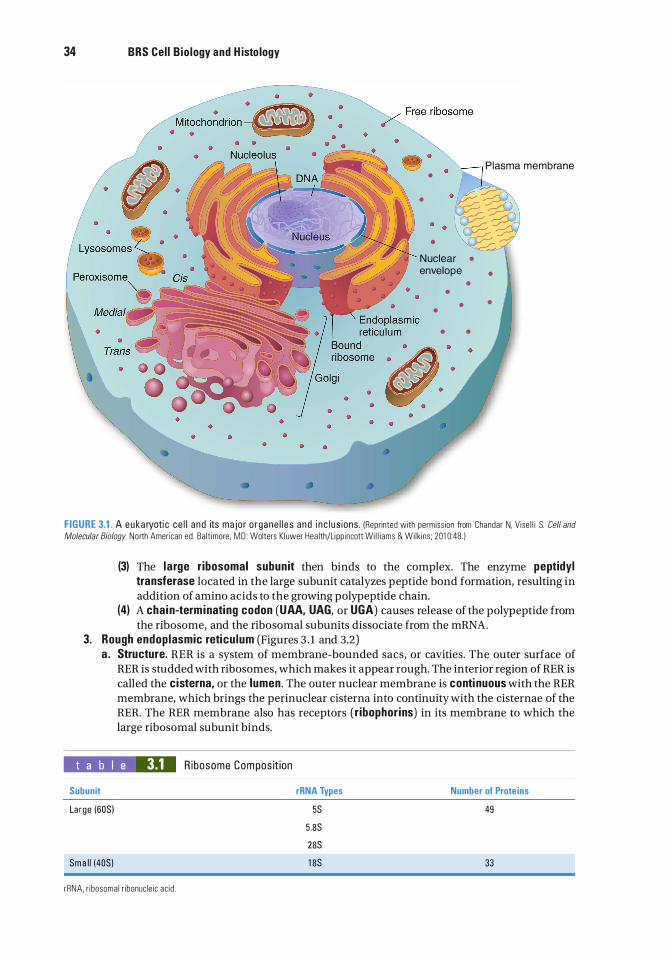
34 BRS Cel l Bio logy and H isto logy
Plasma membrane •
•
•
N uclear • envelope •
• •
• • •
• •
FIGURE 3.1 . A euka ryoti c c e l l a nd its ma jor o rgane l l e s a nd i n c l u s ions . (Reprinted with permiss ion from Chandar N. Vise l l i S. Cell and
Molecular Biology. North American ed . Ba lt imore . MD : Wolters Kl uwer Hea lth/Li pp incott Wi l l i ams & Wi lk ins ; 201 0:48 )
(3) The l a rge ribosomal subunit then binds to the complex. The enzyme peptidyl transferase located in the large subunit catalyzes peptide bond formation, resulting in addition of amino acids to the growing polypeptide chain.
(4) A chain-term inating codon (UAA, UAG, or UGA) causes release of the polypeptide from the ribosome, and the ribosomal subunits dissociate from the mRNA.
3. Rough endoplasmic reticu lum (Figures 3 . 1 and 3.2) a . Structure. RER is a system of membrane-bounded sacs, or cavities. The outer surface of
RER is studded with ribosomes, which makes it appear rough. The interior region of RER is called the cisterna, or the lumen. The outer nuclear membrane is continuous with the RER membrane, which brings the perinuclear cisterna into continuity with the cisternae of the RER. The RER membrane also has receptors (r ibophorins) in its membrane to which the large ribosomal subunit binds.
t a b I e 3.1 R ibosome Compos it ion
Subunit
Large (60S)
Smal l (40S)
rRNA. r ibosoma l r ibonuc le ic ac id .
rRNA Types
5S
5 .8S
28S
1 8S
Number of Prote ins
49
33
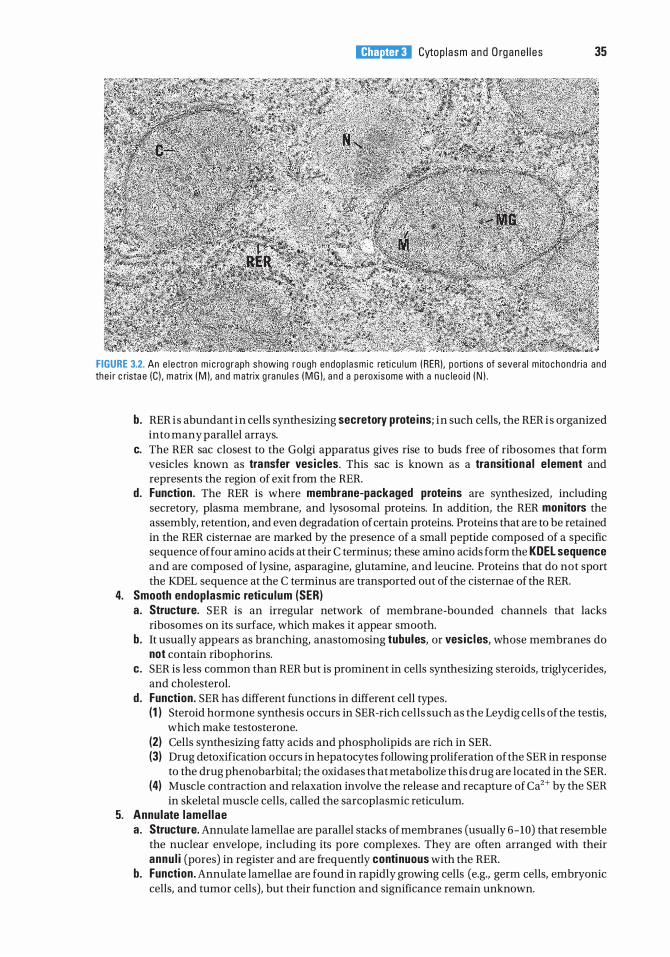
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s 35
FIGURE 3.2. An e l e ctron m i c rog raph s howing rough endop l asm i c reti c u l u m ( RERI . po rti ons of severa l m ito chond ri a a nd the i r c rista e (C ) , m atrix ( M I. a nd m atrix g ranu l e s ( M G I. a n d a pe roxisome with a n u c leo i d ( N ) .
b. RER is abundant in cells synthesizing secretory prote ins; in such cells, the RER i s organized into many parallel arrays.
c. The RER sac closest to the Golgi apparatus gives rise to buds free of ribosomes that form vesicles known as transfer vesic les. This sac is known as a transitiona l e lement and represents the region of exit from the RER.
d. Function. The RER is where membrane-packaged prote ins are synthesized, including secretory, plasma membrane, and lysosomal proteins. In addition, the RER mon itors the assembly, retention, and even degradation of certain proteins. Proteins that are to be retained in the RER cisternae are marked by the presence of a small peptide composed of a specific sequence of four amino acids at their C terminus; these amino acids form the KDEL sequence and are composed of lysine, asparagine, glutamine, and leucine. Proteins that do not sport the KDEL sequence at the C terminus are transported out of the cisternae of the RER.
4. Smooth endoplasmic reticu lum (SER) a . Structure. SER is an irregular network of membrane-bounded channels that lacks
ribosomes on its surface, which makes it appear smooth. b. It usually appears as branching, anastomosing tubules, or vesic les, whose membranes do
not contain ribophorins. c. SER is less common than RER but is prominent in cells synthesizing steroids, triglycerides,
and cholesterol. d . Function. SER has different functions in different cell types.
(1 ) Steroid hormone synthesis occurs in SER-rich cells such as the Leydig cells of the testis, which make testosterone.
(2) Cells synthesizing fatty acids and phospholipids are rich in SER. (3) Drug detoxification occurs in hepatocytes following proliferation of the SER in response
to the drug phenobarbital; the oxidases that metabolize this drug are located in the SER. (4) Muscle contraction and relaxation involve the release and recapture of Ca2+ by the SER
in skeletal muscle cells, called the sarcoplasmic reticulum. 5. Annulate lamel lae
a . Structure. Annulate lamellae are parallel stacks of membranes (usually 6-10) that resemble the nuclear envelope, including its pore complexes. They are often arranged with their annu l i (pores) in register and are frequently conti nuous with the RER.
b. Function. Annulate lamellae are found in rapidly growing cells (e.g., germ cells, embryonic cells, and tumor cells), but their function and significance remain unknown.
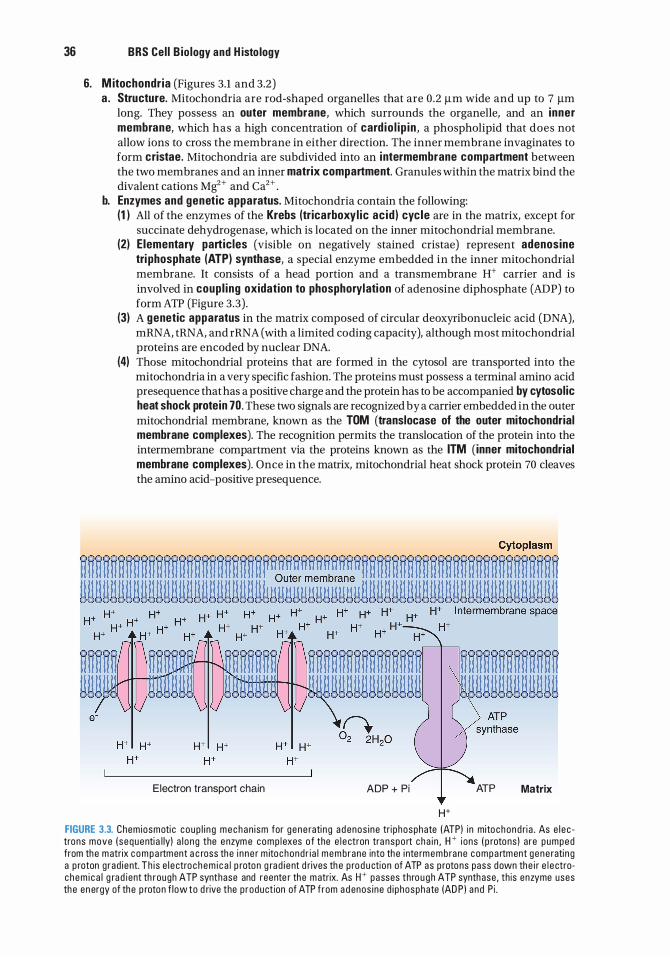
36 BRS Cel l B io logy and H isto logy
6. M itochondr ia (Figures 3.1 and 3.2) a . Structure. Mitochondria are rod-shaped organelles that are 0 .2 J.Lm wide and up to 7 J.Lm
long. They possess an outer membrane, which surrounds the organelle, and an inner membrane, which has a high concentration of card io l ip in , a phospholipid that does not allow ions to cross the membrane in either direction. The inner membrane invaginates to form cristae. Mitochondria are subdivided into an i ntermembrane compartment between the two membranes and an inner matrix compartment. Granules within the matrix bind the divalent cations Mg2+ and Ca2+ .
b. Enzymes and genetic apparatus. Mitochondria contain the following: (1 ) All of the enzymes of the Krebs (tricarboxyl ic ac id ) cyc le are in the matrix, except for
succinate dehydrogenase, which is located on the inner mitochondrial membrane. (2) Elementary particles (visible on negatively stained cristae) represent adenosine
tri phosphate (ATP) synthase, a special enzyme embedded in the inner mitochondrial membrane. It consists of a head portion and a transmembrane H+ carrier and is involved in coupl ing oxidation to phosphorylation of adenosine diphosphate (ADP) to form ATP (Figure 3.3) .
(3) A genetic apparatus in the matrix composed of circular deoxyribonucleic acid (DNA), mRNA, tRNA, and rRNA (with a limited coding capacity), although most mitochondrial proteins are encoded by nuclear DNA.
(4) Those mitochondrial proteins that are formed in the cytosol are transported into the mitochondria in a very specific fashion. The proteins must possess a terminal amino acid presequence that has a positive charge and the protein has to be accompanied by cytosolic heat shock protein 70. These two signals are recognized by a carrier embedded in the outer mitochondrial membrane, known as the TOM (translocase of the outer mitochondrial membrane complexes). The recognition permits the translocation of the protein into the intermembrane compartment via the proteins known as the ITM (inner mitochondrial membrane complexes). Once in the matrix, mitochondrial heat shock protein 70 cleaves the amino acid-positive presequence.
Electron transport chain ADP + Pi ATP Matrix
H+
FIGURE 3.3. Chem iosmoti c coup l i n g m e c h an i sm for gene rati n g a d enos i ne tri phosphate (ATP) i n mito chond ri a . As e l e c trons move ( sequenti a l ly) a l o ng the e nzym e comp l exes o f the e l e ctron tra nspo rt cha i n , W i ons ( p rotons ) a re pumped from the m atrix c o m p a rtment a c ross the i n ne r m itochond r i a l mem brane into the i nte rmemb rane compa rtment gene rati n g a p roton g rad i ent. Th i s e l e ctro c h e m i c a l p roton g rad i e nt d rives th e p ro d u ction of ATP as p rotons pass down the i r e l e ctroc hem i c a l g ra d ient th rough ATP synthase and reente r the m atrix. As W passes thro u g h ATP synthase , th is enzyme uses the en ergy of the p roton f low to d rive the p roduct ion of ATP f rom a d enos i ne d i phosphate (AD P ) a nd P i .
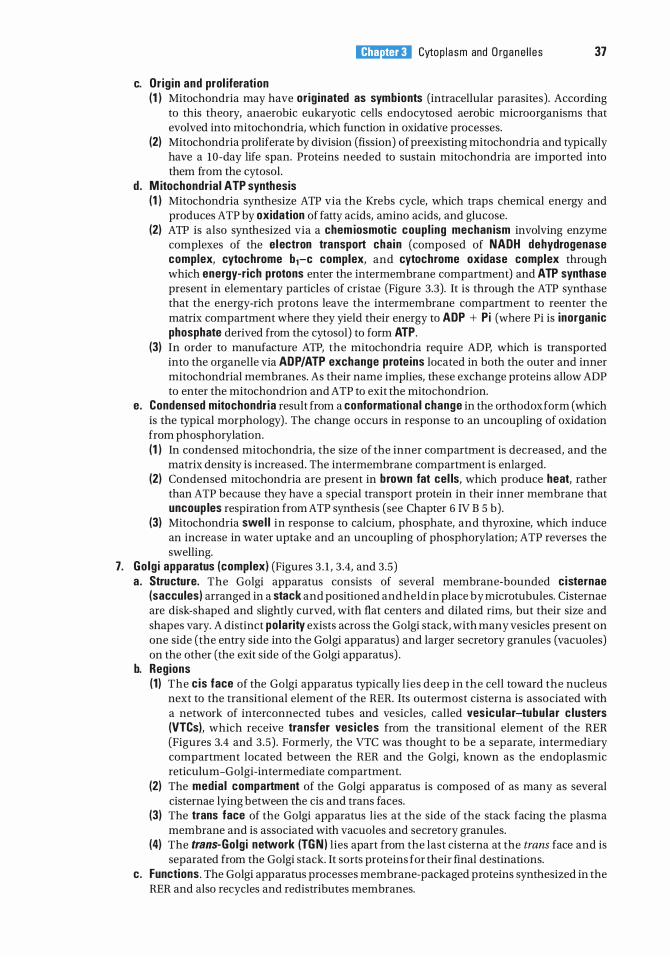
c. Or ig in and prol iferation
l!1i!tttttiil Cytop l a sm and O rgane l l e s 37
(1 ) Mitochondria may have or ig inated as symbionts (intracellular parasites) . According to this theory, anaerobic eukaryotic cells endocytosed aerobic microorganisms that evolved into mitochondria, which function in oxidative processes.
(2) Mitochondria proliferate by division (fission) of preexisting mitochondria and typically have a 10-day life span. Proteins needed to sustain mitochondria are imported into them from the cytosol.
d . M itochondr ia l ATP synthesis (1 ) Mitochondria synthesize ATP via the Krebs cycle, which traps chemical energy and
produces ATP by oxidation of fatty acids, amino acids, and glucose. (2) ATP is also synthesized via a chem iosmotic coupl ing mechan ism involving enzyme
complexes of the electron transport cha in (composed of NADH dehydrogenase complex, cytochrome b1-c complex, and cytochrome oxidase complex through which energy-r ich protons enter the intermembrane compartment) and ATP synthase present in elementary particles of cristae (Figure 3.3). It is through the ATP synthase that the energy-rich protons leave the intermembrane compartment to reenter the matrix compartment where they yield their energy to ADP + Pi (where Pi is inorganic phosphate derived from the cytosol) to form ATP.
(3) In order to manufacture ATP, the mitochondria require ADP, which is transported into the organelle via ADP/ATP exchange prote ins located in both the outer and inner mitochondrial membranes. As their name implies, these exchange proteins allow ADP to enter the mitochondrion and ATP to exit the mitochondrion.
e. Condensed mitochondr ia result from a conformational change in the orthodox form (which is the typical morphology) . The change occurs in response to an uncoupling of oxidation from phosphorylation. (1 ) In condensed mitochondria, the size of the inner compartment is decreased, and the
matrix density is increased. The intermembrane compartment is enlarged. (2) Condensed mitochondria are present in brown fat cel ls, which produce heat, rather
than ATP because they have a special transport protein in their inner membrane that uncoup les respiration from ATP synthesis (see Chapter 6 IV B 5 b) .
(3) Mitochondria swel l in response to calcium, phosphate, and thyroxine, which induce an increase in water uptake and an uncoupling of phosphorylation; ATP reverses the swelling.
7. Go lg i apparatus (complex) (Figures 3 . 1 , 3 .4, and 3.5) a. Structure. The Golgi apparatus consists of several membrane-bounded cisternae
(saccules) arranged in a stack and positioned and held in place by microtubules. Cisternae are disk-shaped and slightly curved, with flat centers and dilated rims, but their size and shapes vary. A distinct polarity exists across the Golgi stack, with many vesicles present on one side (the entry side into the Golgi apparatus) and larger secretory granules (vacuoles) on the other (the exit side of the Golgi apparatus) .
b. Regions (1 ) The cis face of the Golgi apparatus typically l ies deep in the cell toward the nucleus
next to the transitional element of the RER. Its outermost cisterna is associated with a network of interconnected tubes and vesicles, called ves icu lar-tubu lar c lusters (VTCs), which receive transfer vesic les from the transitional element of the RER (Figures 3.4 and 3 .5) . Formerly, the VTC was thought to be a separate, intermediary compartment located between the RER and the Golgi, known as the endoplasmic reticulum-Golgi-intermediate compartment.
(2) The media l compartment of the Golgi apparatus is composed of as many as several cisternae lying between the cis and trans faces.
(3) The trans face of the Golgi apparatus lies at the side of the stack facing the plasma membrane and is associated with vacuoles and secretory granules.
(4) The trans-Golg i network (TGN ) lies apart from the last cisterna at the trans face and is separated from the Golgi stack. It sorts proteins for their final destinations.
c. Functions. The Golgi apparatus processes membrane-packaged proteins synthesized in the RER and also recycles and redistributes membranes.
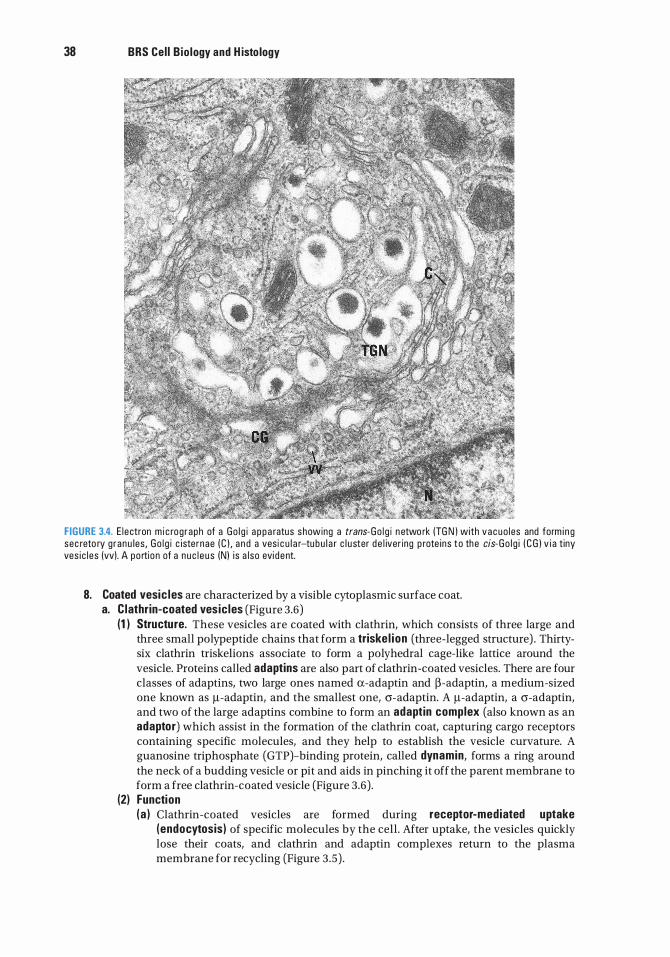
38 BRS Cel l Bio logy and H isto logy
FIGURE 3.4. E l ectron m i c rog raph of a Go l g i a p p a ratus showing a trans-Go l g i n etwo rk (TG N ) with vacuo les and form i n g sec reto ry g ranu les , Go l g i c isternae ( C ) , a n d a vesi c u l a r-tu b u l a r c l u ster d e l iver ing p rote ins t o the cis-Go l g i ( C G ) v i a t iny ves i c l es (vv). A po rtion of a n u c l e u s (N) i s a l so evi dent.
8. Coated vesic les are characterized by a visible cytoplasmic surface coat. a. C lathrin-coated vesic les (Figure 3.6)
(1 ) Structure. These vesicles are coated with clathrin, which consists of three large and three small polypeptide chains that form a triske l ion (three-legged structure) . Thirtysix clathrin triskelions associate to form a polyhedral cage-like lattice around the vesicle. Proteins called adaptins are also part of clathrin-coated vesicles. There are four classes of adaptins, two large ones named a-adaptin and �-adaptin, a medium-sized one known as f.L-adaptin, and the smallest one, cr-adaptin. A f.L-adaptin, a cr-adaptin, and two of the large adaptins combine to form an adaptin complex (also known as an adaptor) which assist in the formation of the clathrin coat, capturing cargo receptors containing specific molecules, and they help to establish the vesicle curvature. A guanosine triphosphate (GTP)-binding protein, called dynamin, forms a ring around the neck of a budding vesicle or pit and aids in pinching it off the parent membrane to form a free clathrin-coated vesicle (Figure 3.6) .
(2) Function (a ) Clathrin-coated vesicles are formed during receptor-mediated uptake
(endocytosis) of specific molecules by the cell . After uptake, the vesicles quickly lose their coats, and clathrin and adaptin complexes return to the plasma membrane for recycling (Figure 3 .5) .
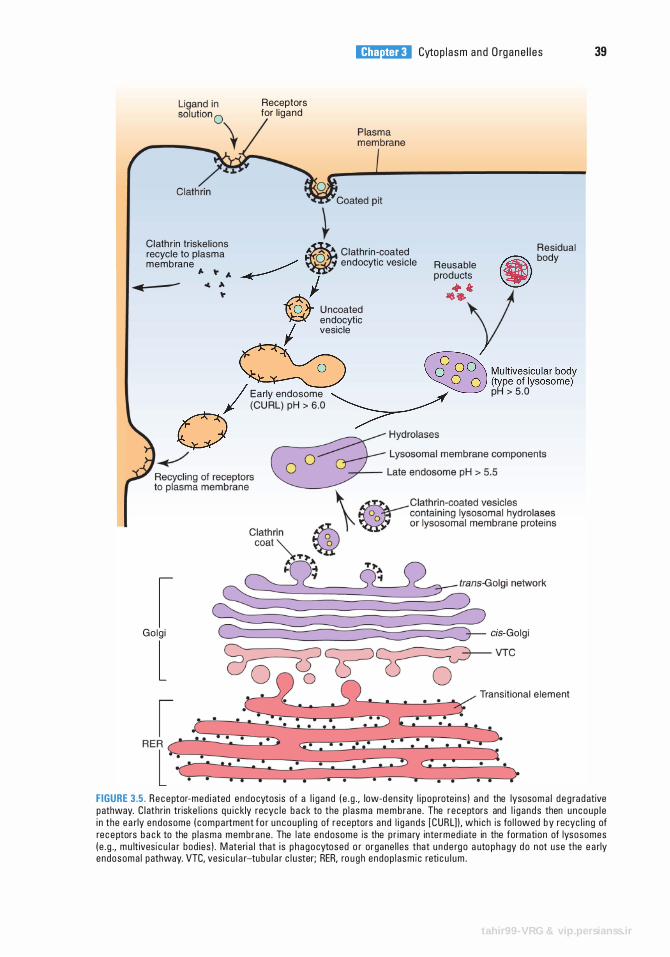
Receptors for l igand
t
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s
Clath r in tr iske l ions il Residual recycle to plasma Clathr in -coated membrane � endocytic vesic le Reusable • body
,. " A � ./ prod ucts � � � � � + t " -t:(j{ U ncoated ��y W endocyt1c I ves1cle
� � M ultivesicu lar body � � (type of lysosome)
I Early endosome � � pH > 5 . 0 (CU RL) pH > 6 .0 � 0
�
I Golg i cis-Golg i
l Transit ional e lement
39
FIGURE 3.5. Receptor-med i ated endocytosis of a l i g and ( e . g . , low-d ens ity l i p op rote i ns ) a nd the lysosoma l d e g ra d ative pathway. C l athr in triske l i ons q u i c kly recyc le b a c k to the p l asma mem brane . The receptors and l i g ands then u ncoup l e i n the ea rly endosome ( c ompa rtment f o r u ncoup l i n g of receptors a nd l i g ands [CURL] ) , wh i ch is fo l l owed by recyc l i n g of rec e ptors b a c k to the p l asma membrane . The l ate endosome is the p r ima ry inte rmed i ate in the formati on of lysosomes ( e . g . , m u lt ivesi c u l a r bod ies ) . M ateri a l that i s p h agocytosed o r organe l l es that u nde rg o a uto p h a gy d o not use the e a rly endosoma l pathway. VTC, ves i c u l a r-tu b u l a r c l u ster; RER, ro u g h endop l asm i c reti c u l u m .
tahir99-VRG & vip.persianss.ir
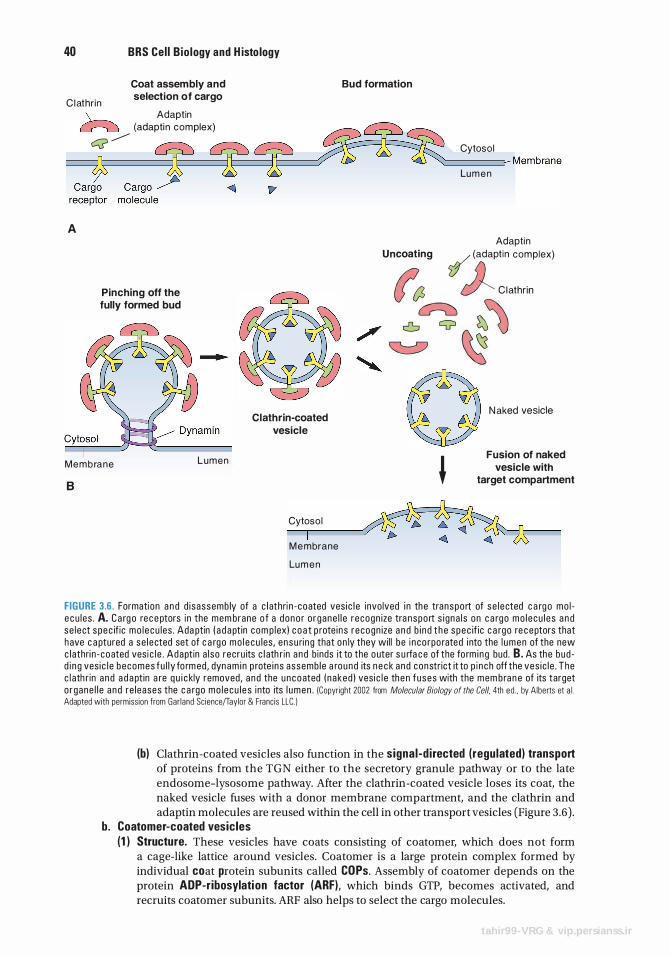
40 BRS Cel l Bio logy and H isto logy
Bud formation
C l athr in
Coat assembly and selection of cargo
A
\__ Adaptin cr---2J (adapti n complex)
Q �
Pinching off the fully formed bud
Clathrin-coated vesicle
Cytoso l
Lu m e n
Adaptin Uncoating � (adaptin complex)
� ))__ C l ath, lo
���� 0 N ak'd "''"'
Fusion of naked M e m b ra n e L u m e n � vesicle with
B
Cytoso l
M e mbrane
Lu m e n
target compartment
FIGURE 3.6. Formation a n d d i sassemb ly of a c l athri n - coated ves i c l e invo lved i n the transpo rt of se l ected c a rg o mo l e c u les . A. C a rg o rec e ptors in the mem brane o f a dono r o rgane l l e r ecogn ize tra nspo rt s i gna l s on c a rgo mo l ecu l e s a n d se l ect spec if ic mo l e cu les . Ada ptin ( a d a pt in com p lex) c o a t p rote i ns r ecogn ize a n d b i nd t h e spec if ic c a rgo re ceptors that have c a ptured a se l ected set of c a rg o mo l e c u les , ensu ri ng that on ly they wi l l be i n co rpo rated i nto the l umen of the new c lathri n - coated vesi c l e . Adaptin a l so recru its c l ath r in a nd b inds it to the o uter s u rfa c e of the fo rm i ng bud . B. As the bud d i ng ves i c l e becomes fu l l y fo rm ed , dynam i n p rote i ns assemb le a round its n e c k and constrict it to p i n ch off the ves i c l e . The c l ath r in a nd a d a pt in a re q u i c kly removed, a nd the uncoated ( naked ) ves i c l e the n f uses with the mem bra n e of its target o rgane l l e a nd re leases the c a rgo mo l e cu l e s into its l umen . (Copyright 2002 from Molecular Biology of the Cell, 4th ed . , by Alberts et a l . Adapted with permiss ion from Gar land Sc ience/Taylor & Franc is LLC. )
(b) Clathrin-coated vesicles also function in the signal -d i rected (regulated) transport of proteins from the TGN either to the secretory granule pathway or to the late endosome-lysosome pathway. After the clathrin-coated vesicle loses its coat, the naked vesicle fuses with a donor membrane compartment, and the clathrin and adaptin molecules are reused within the cell in other transport vesicles (Figure 3.6) .
b. Coatomer-coated vesicles (1 ) Structure. These vesicles have coats consisting of coatomer, which does not form
a cage-like lattice around vesicles. Coatomer is a large protein complex formed by individual coat protein subunits called COPs. Assembly of coatomer depends on the protein ADP-ribosylati on factor (ARF), which binds GTP, becomes activated, and recruits coatomer subunits. ARF also helps to select the cargo molecules.
tahir99-VRG & vip.persianss.ir
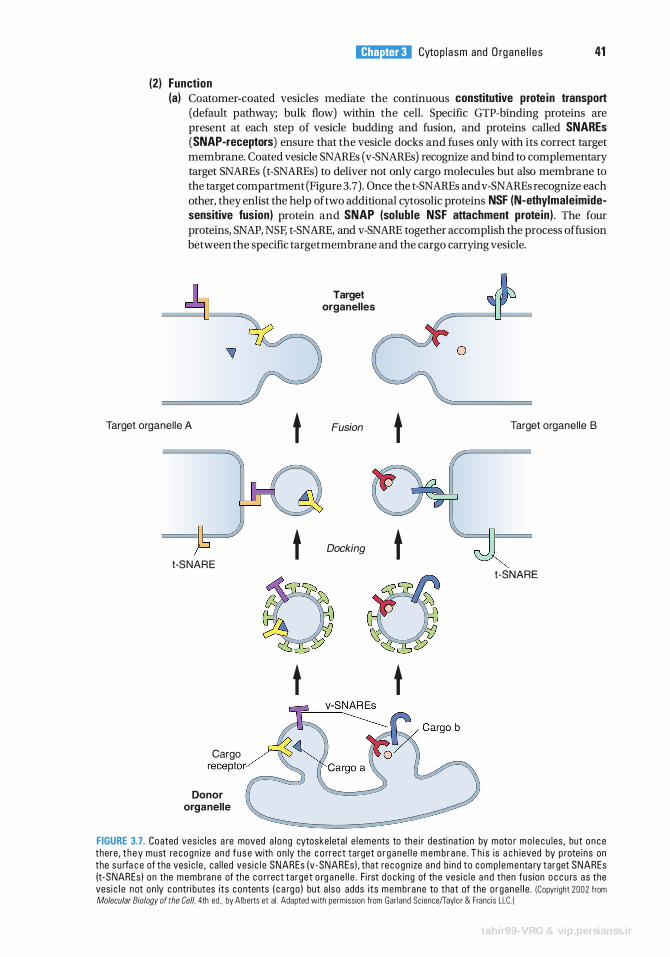
(2) Function
l!1i!tttttiil Cytop l a sm and O rgane l l e s 41
(a) Coatomer-coated vesicles mediate the continuous constitutive protein transport (default pathway; bulk flow) within the cell. Specific GTP-binding proteins are present at each step of vesicle budding and fusion, and proteins called SNAREs (SNAP-receptors) ensure that the vesicle docks and fuses only with its correct target membrane. Coated vesicle SNAREs (v-SNAREs) recognize and bind to complementary target SNAREs (t-SNAREs) to deliver not only cargo molecules but also membrane to the target compartment (Figure 3.7). Once the t-SNAREs and v-SNAREs recognize each other, they enlist the help of two additional cytosolic proteins NSF (N-ethylmaleimidesensitive fusion) protein and SNAP (soluble NSF attachment protein) . The four proteins, SNAP, NSF, t-SNARE, and v-SNARE together accomplish the process affusion between the specific target membrane and the cargo carrying vesicle.
Target organel le A
t-SNARE
Cargo receptor
Donor organelle
t
t
Target organelles
Fusion
Docking
t
t
0 0 t t
0
Target organel le B
t-SNARE
FIGURE 3.7. Coated ves ic les a re moved a l o ng cytoske leta l e l ements to the i r desti nat ion by moto r m o l e c u les , but o n c e there , t h e y must recogn ize a nd f u s e with on ly the c o rrect target o r g a n e l l e m e m b r a n e . T h i s is a c h ieved by p rote i ns on the s u rfa c e of the vesi c l e , ca l l ed ves i c l e SNAREs (v -SNAREs ) , that recogn ize a nd b i nd to comp l ementa ry target SNAREs (t-SNAREs) on the memb ra n e of the c o rrect target o rg a ne l l e . Fi rst d o c ki ng of th e vesi c l e a n d then fus ion o c c u rs as the vesi c l e not on ly contri butes i ts contents ( c a rgo ) but a l so adds i ts membrane to that of the o rgane l l e . )Copyright 2002 from Molecular Biology of the Cell, 4th ed., by Alberts et al. Adapted with permiss ion from Gar land Sc ience/Taylo r & Franc is LLC. )
tahir99-VRG & vip.persianss.ir
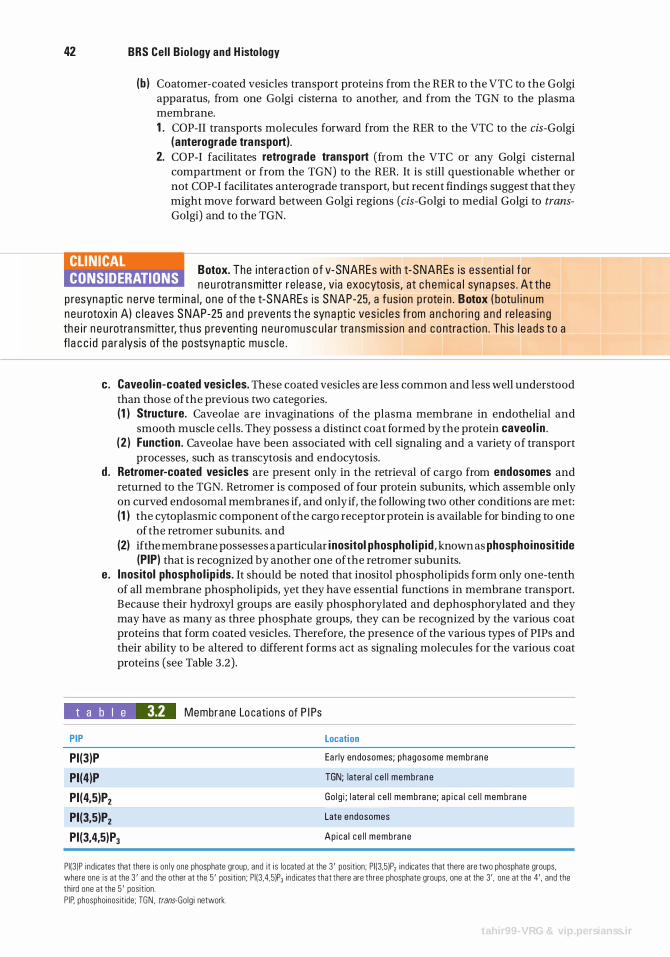
42 BRS Cel l B io logy and H isto logy
(b ) Coatomer-coated vesicles transport proteins from the RER to the VTC to the Golgi apparatus, from one Golgi cisterna to another, and from the TGN to the plasma membrane. 1 . COP-II transports molecules forward from the RER to the VTC to the cis-Golgi
(anterograde transport). 2. COP-I facilitates retrograde transport (from the VTC or any Golgi cisternal
compartment or from the TGN) to the RER. It is still questionable whether or not COP-I facilitates anterograde transport, but recent findings suggest that they might move forward between Golgi regions (cis-Golgi to medial Golgi to transGolgi) and to the TGN.
CLINICAL CONSIDERATIONS
Botox. The i ntera cti on o f v-SNAREs with t-SNAREs is essenti a l for n e u rotra nsm itte r re l ease , v ia exocytos is , at c h e m i c a l syn a pses . At the
p resyna pti c n e rve te rm i n a l , one of the t-S NAREs is S NAP-25, a fus ion p rote i n . Botox ( botu l i n um neu rotoxin A) c l eaves S NAP-25 a n d p reve nts t h e syna pt ic ves i c l e s from a n c h o ri n g a n d re l e as i ng th e i r n e u rotra nsm itte r, t hus p reventi n g n e u romusc u l a r tra nsm iss ion a n d contra cti on . Th is l e ads to a fl a c c i d pa ra lysis of the postsyna pt ic musc l e .
c. Caveol in-coated vesic les. These coated vesicles are less common and less well understood than those of the previous two categories. (1 ) Structure. Caveolae are invaginations of the plasma membrane in endothelial and
smooth muscle cells. They possess a distinct coat formed by the protein caveol i n . ( 2 ) Function . Caveolae have been associated with cell signaling and a variety of transport
processes, such as transcytosis and endocytosis. d . Retromer-coated vesicles are present only in the retrieval of cargo from endosomes and
returned to the TGN. Retromer is composed of four protein subunits, which assemble only on curved endosomal membranes if, and only if, the following two other conditions are met: (1 ) the cytoplasmic component of the cargo receptor protein is available for binding to one
of the retromer subunits. and (2) ifthe membrane possesses a particular i nositol phosphol i p id , known as phosphoinositide
(PIP) that is recognized by another one of the retromer subunits. e. Inositol phospho l ip ids. It should be noted that inositol phospholipids form only one-tenth
of all membrane phospholipids, yet they have essential functions in membrane transport. Because their hydroxyl groups are easily phosphorylated and dephosphorylated and they may have as many as three phosphate groups, they can be recognized by the various coat proteins that form coated vesicles. Therefore, the presence of the various types of PIPs and their ability to be altered to different forms act as signaling molecules for the various coat proteins (see Table 3.2) .
t a b I e 3.2 Membrane Lo cations of P I Ps
PIP
PI(3)P
PI(4)P
PI(4,5)P2
PI(3,5)P2
PI(3,4,5)P3
Location
Ea rly endosomes; phagosome membrane
TGN; late ra l c e l l membrane
Go l g i ; l ate ra l c e l l membrane; a p i c a l c e l l membrane
Late endosomes
Ap ica l c e l l membrane
PII3)P i nd i cates that there is on ly one phosphate group. and it i s located at the 3 ' posit ion; PI I3.5)P2 i nd icates that there are two phosphate groups. where one is at the 3 ' and the other at the 5 ' pos it ion; P I I3 .4,5)P3 ind icates that there are three phosphate groups. one at the 3' , one at the 4' . and the th i rd one at the 5 ' pos it ion . P IP. phosphoinos it ide ; TGN . trans-Go lg i network.
tahir99-VRG & vip.persianss.ir
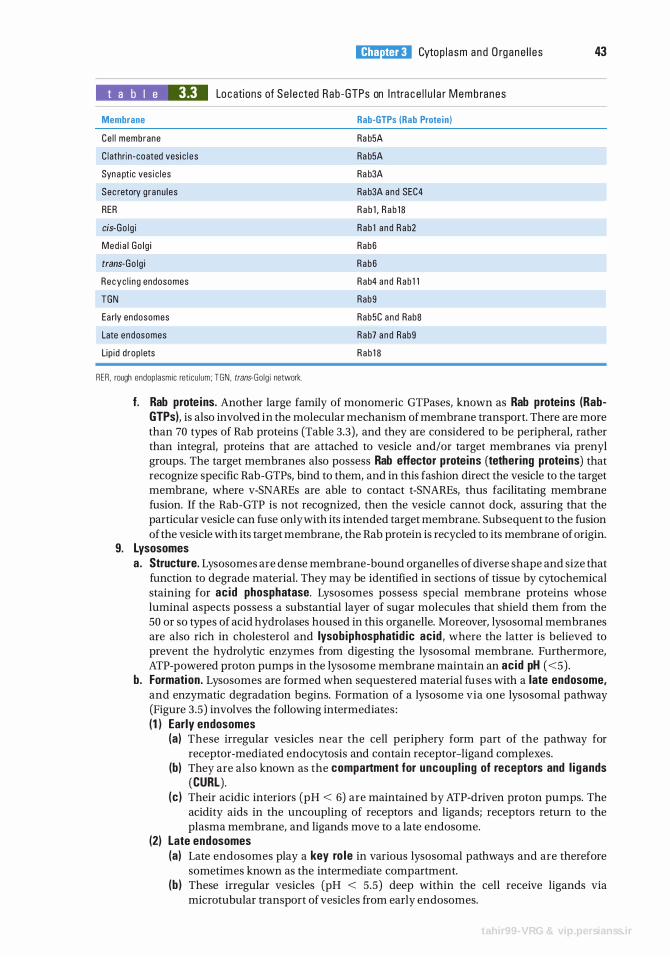
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s 43
t a b I e 3.3 Locations of Se l e cted Rab -GTPs on I ntra c e l l u l a r Memb ranes
Membrane Rab-GTPs (Rab Protein )
Ce l l membrane
C l athri n -coated vesi c l e s
Syna ptic ves i c l es
Sec retory g ranu l es
Ra b5A
Ra b5A
Ra b3A
Ra b3A and SEC4
R a b 1 , R a b 1 8
Rab 1 a nd Rab2
Rab6
RER
cis-Go l g i
Med i a l Go l g i
trans-Go l g i Rab6
Recyc l i n g endosomes
TGN
Rab4 and Rab 1 1
Rab9
Ea rly endosomes
Late endosomes
Rab5C and Rab8
Rab7 a nd Rab9
Rab 1 8 Li p id d rop lets
REA . rough endop lasmic ret i cu l um; TGN . trans-Go lg i network.
f. Rab prote ins. Another large family of monomeric GTPases, known as Rab proteins (RabGTPs), is also involved in the molecular mechanism of membrane transport. There are more than 70 types of Rab proteins (Table 3.3), and they are considered to be peripheral, rather than integral, proteins that are attached to vesicle and/or target membranes via prenyl groups. The target membranes also possess Rab effector proteins (tethering proteins) that recognize specific Rab-GTPs, bind to them, and in this fashion direct the vesicle to the target membrane, where v-SNAREs are able to contact t-SNAREs, thus facilitating membrane fusion. If the Rab-GTP is not recognized, then the vesicle cannot dock, assuring that the particular vesicle can fuse only with its intended target membrane. Subsequent to the fusion of the vesicle with its target membrane, the Rab protein is recycled to its membrane of origin.
9. Lysosomes a . Structure. Lysosomes are dense membrane-bound organelles of diverse shape and size that
function to degrade material. They may be identified in sections of tissue by cytochemical staining for acid phosphatase. Lysosomes possess special membrane proteins whose luminal aspects possess a substantial layer of sugar molecules that shield them from the 50 or so types of acid hydro lases housed in this organelle. Moreover, lysosomal membranes are also rich in cholesterol and lysob iphosphatid ic acid , where the latter is believed to prevent the hydrolytic enzymes from digesting the lysosomal membrane. Furthermore, ATP-powered proton pumps in the lysosome membrane maintain an acid pH ( <5) .
b. Formation. Lysosomes are formed when sequestered material fuses with a late endosome, and enzymatic degradation begins. Formation of a lysosome via one lysosomal pathway (Figure 3.5) involves the following intermediates : (1 ) Early endosomes
(a) These irregular vesicles near the cell periphery form part of the pathway for receptor-mediated endocytosis and contain receptor-ligand complexes.
(b) They are also known as the compartment for uncoupl ing of receptors and l igands (CURL).
(c ) Their acidic interiors (pH < 6) are maintained by ATP-driven proton pumps. The acidity aids in the uncoupling of receptors and ligands; receptors return to the plasma membrane, and ligands move to a late endosome.
(2) Late endosomes (a) Late endosomes play a key ro le in various lysosomal pathways and are therefore
sometimes known as the intermediate compartment. (b ) These irregular vesicles (pH < 5.5) deep within the cell receive ligands via
microtubular transport of vesicles from early endosomes.
tahir99-VRG & vip.persianss.ir
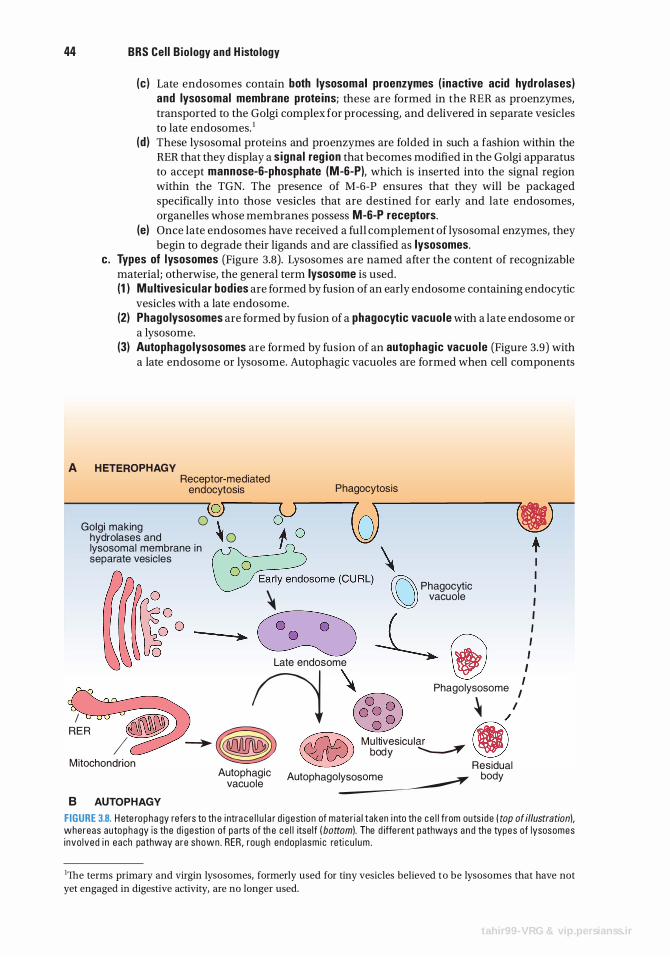
44 BRS Cel l Bio logy and H isto logy
(c) Late endosomes contain both lysosomal proenzymes ( inactive acid hydrolases) and lysosomal membrane prote ins; these are formed in the RER as proenzymes, transported to the Golgi complex for processing, and delivered in separate vesicles to late endosomes. 1
(d ) These lysosomal proteins and proenzymes are folded in such a fashion within the RER that they display a signal reg ion that becomes modified in the Golgi apparatus to accept mannose-6-phosphate (M-6-P), which is inserted into the signal region within the TGN. The presence of M-6-P ensures that they will be packaged specifically into those vesicles that are destined for early and late endosomes, organelles whose membranes possess M-6-P receptors.
(e) Once late endosomes have received a full complement of lysosomal enzymes, they begin to degrade their ligands and are classified as lysosomes.
c . Types of lysosomes (Figure 3.8). Lysosomes are named after the content of recognizable material; otherwise, the general term lysosome is used. (1 ) Mu ltives icu lar bodies are formed by fusion of an early endosome containing endocytic
vesicles with a late endosome. (2) Phago lysosomes are formed by fusion of a phagocytic vacuole with a late endosome or
a lysosome. (3) Autophagolysosomes are formed by fusion of an autophagic vacuole (Figure 3.9) with
a late endosome or lysosome. Autophagic vacuoles are formed when cell components
A H ETEROPHAGY Receptor-mediated
endocytosis Phagocytosis
(Q) Golgi making 0 \.
hydrolases and � 0 lysosomal membrane i n separate vesicles
(o) \ n Phagocytic � 'U) vacuole
� -L La" '"d"'ome iJ
I I I I I I I I
I I
,:E R � fj � Phagolysosome � / � . / �� � M���:sicu l� M 1tochondnon � Residual
8 AUTOPHAGY
Autophagic Autophagolysosome body vacuole �
FIGURE 3.8. H ete rophagy refers to th e i ntra c e l l u l a r d i g estion of mater i a l taken i nto the c e l l from outs i de ( top of illustrationl, whereas auto p h a gy is the d i gestion of pa rts of th e c e l l itse lf ( bottoml. The d iffe rent pathways and the types of lysosomes i nvo lved i n each pathway a re shown . RER , roug h endop lasm ic reti c u l um .
1The terms primary and virgin lysosomes, formerly used for tiny vesicles believed to be lysosomes that have not
yet engaged in digestive activity, are no longer used.
tahir99-VRG & vip.persianss.ir
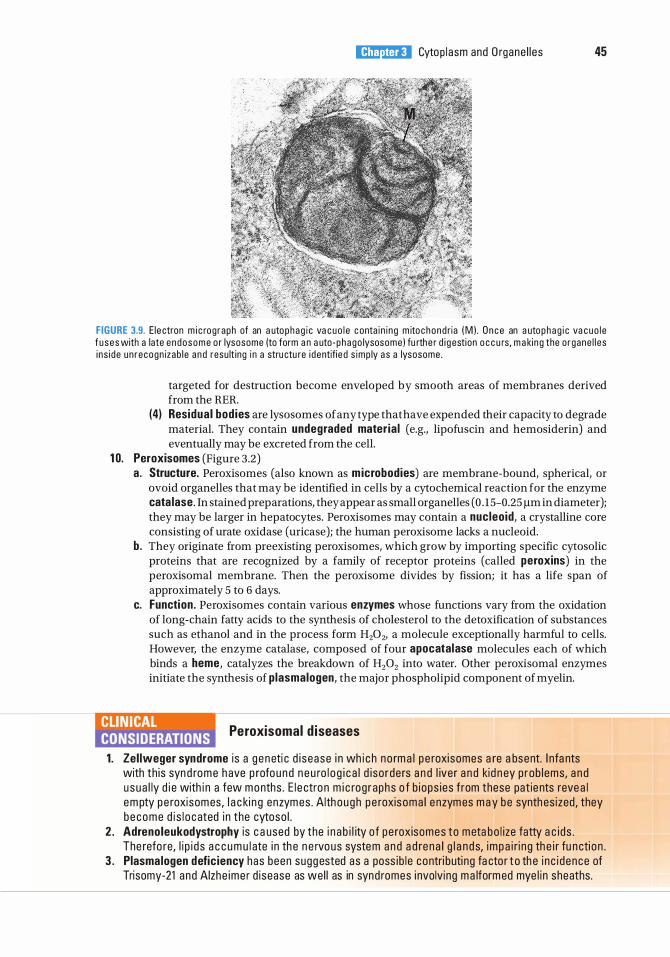
l!1i!tttttiil Cytop l asm and O rgane l l es 45
FIGURE 3.9. E le ctron m i c rog raph of an a utophag i c va cuo l e c onta i n i ng m ito chond ria ( M ) . O n c e an a utophag i c va cuo l e f u ses with a late e ndosome o r lysosome (to form a n a uto- phago lysosome ) fu rthe r d i g estion o c c u rs, m a ki ng the o rgane l l es i ns i de un recogn izab l e a nd resu lt ing i n a stru ctu re i dentifi e d s imp ly a s a lysosome .
targeted for destruction become enveloped by smooth areas of membranes derived from the RER.
(4) Residual bodies are lysosomes of any type that have expended their capacity to degrade material. They contain undegraded mater ia l (e.g., lipofuscin and hemosiderin) and eventually may be excreted from the cell.
1 0. Peroxisomes (Figure 3.2) a. Structure. Peroxisomes (also known as microbodies) are membrane-bound, spherical, or
ovoid organelles that may be identified in cells by a cytochemical reaction for the enzyme cata lase. In stained preparations, they appear as small organelles ( 0 . 15-0.25 flm in diameter); they may be larger in hepatocytes. Peroxisomes may contain a nucleoid, a crystalline core consisting of urate oxidase (uricase); the human peroxisome lacks a nucleoid.
b. They originate from preexisting peroxisomes, which grow by importing specific cytosolic proteins that are recognized by a family of receptor proteins (called peroxins) in the peroxisomal membrane. Then the peroxisome divides by fission; it has a life span of approximately 5 to 6 days.
c. Function. Peroxisomes contain various enzymes whose functions vary from the oxidation of long-chain fatty acids to the synthesis of cholesterol to the detoxification of substances such as ethanol and in the process form H202, a molecule exceptionally harmful to cells. However, the enzyme catalase, composed of four apocatalase molecules each of which binds a heme, catalyzes the breakdown of H202 into water. Other peroxisomal enzymes initiate the synthesis of plasmalogen, the major phospholipid component of myelin.
I!YHIJ!II Peroxisomal d iseases
1 . Zel lweger syndrome i s a g e neti c d i sease i n wh i c h no rm a l p e roxi somes a re a bsent. I nfa nts with th is syn d rome h ave p rofo u nd n e u ro l o g i c a l d i so rders a n d l iver a n d kid n ey p rob l ems, a n d u s u a l ly d i e with i n a few months . E l e ctro n m i c rog raphs o f b iops ies from these pat ie nts reve a l em pty pe roxisomes, l a c ki n g enzymes . Alth o ugh pe roxisoma l e nzymes m a y be synth es ized , they become d i s l o c ated i n the cytoso l .
2 . Adrenoleukodystrophy is c a used by the i n a b i l ity of pe roxisomes to meta bo l ize fatty a c i ds . The refo re, l i p i d s a c c u m u l ate i n th e n e rvous system a n d a d re n a l g l a n d s, impa i r i n g th e i r fu n cti o n .
3 . Plasmalogen deficiency has been sugg ested as a poss i b l e contri buti ng fa cto r t o th e i n c i dence of Trisomy-21 and Alzhe ime r d isease as we l l as in synd romes i nvolving m a lformed mye l i n sheaths.
46 BRS Cel l B io logy and H isto logy
B . Inc lusions. Inclusions are accumulations of material that is not metabo l ica l ly active. They are usually present in the cytosol only temporari ly . 1 . G lycogen appears as small clusters (or in hepatocytes as larger aggregates, known as rosettes)
of electron-dense 20- to 30-nm �-particles, which are similar in appearance to but larger than ribosomes. Glycogen is not bound by a membrane but frequently lies close to the SER. Glycogen serves as a stored energy source that can be degraded to glucose, which enters the bloodstream to elevate blood sugar levels.
2. Li p id droplets vary markedly in size and appearance depending on the method of fixation, and they are not bound by a membrane. Lipid droplets are storage forms of tri g lycerides (an energy source) and cholestero l (used in the synthesis of steroids and membranes) .
3. Lipofuscin appears as membrane-bound, electron-dense granular material varying greatly in size and often containing lipid droplets. Lipofuscin represents a residue of undigested material present in residual bodies. Because the amount of this material increases with age, it is called age p igment. It is most common in nondividing cells (e.g., cardiac muscle cells, neurons), but is also found in hepatocytes.
C. Cytoske leton. The cytoskeleton is the structural framework within the cytosol. It functions in maintaining cell shape, stabilizing cell attachments, facilitating endocytosis and exocytosis, and promoting cell movement. It includes the following major components : 1 . Microtubu les
a. Structure. Microtubules are straight, hollow tubules 25 nm in diameter and made of tubu l i n . They have a rigid wall composed of 13 protofilaments, each of which consists of a linear arrangement of tubulin dimers; each dimer consists of nonidentical a- and �-tubu l in subun its that are linked end to end, so that an a-tubulin subunit of one dimer i s linked to the �-tubulin subunit of the next dimer.
b. Microtubules are polar, in that they have a plus end W-tubulin end) and a minus end (a-tubulin) . Polymerization (assembly) and depolymerization (disassembly) occur preferentially at the plus end, but only when GTP, in the presence of magnesium ions, is bound to tubulin dimers. The minus end of a microtubule is usually not free, but is affixed to the microtubule-organizing center (discussed below C.2 . ) .
c. Microtubu les have microtubu le-associated prote ins (MAPs, such as MAP1 , MAP2, MAP3, MAP4, and MAP tau), which stabilize them, control their lengthening, and bind them to other cytoskeletal components and organelles. Other MAPs, such as Lis 1, facilitate neuronal migration, which permits the development of gyri and sulci in the brain.
CLIN ICAL CONSIDERATIONS
I n d ivi d u a l s who d o not possess th e L i s 1 MAPs a re bo rn with smooth c e re b r a l h em i sphe res, a c ond itio n kn own a s l issencephaly. Ch i l d ren with th is
c ond it ion ra re ly s u rvive past 15 yea rs of age and d i s p l ay var ious g r ades of m e nta l reta rdati on . Those most seve re ly affe cted d i e d u ri ng the fi rst few months of l ife .
d . Microtubules are also associated with kines in and cytop lasmic dyne in, two forcegenerating proteins (motor prote i ns), which serve as motors for vesicle or organelle movement. Kinesin moves cargo toward the plus end of the microtubule (outward, toward the cell periphery), whereas cytoplasmic dynein moves it toward the minus end (inward, toward the center of the cell) .
e. Function. Microtubules maintain cell shape; aid in the transport of macromolecules, vesicles, and organelles within the cytosol; assemble into the mitotic spindle during mitosis and ensure the correct distribution of chromosomes to daughter cells; and assist in the formation of cell appendages called cilia and flagella, which beat rhythmically and precisely.
2. Centrosome (Microtubule Organizing Center, MTOC) and Centrioles (see Figures 2.7 and 3 . 10) a. Structure. The centrosome is located near the nucleus. It contains two centrio les and a
cloud of pericentrio lar materia l . The centrioles exist as a pair of cylindrical rods (each 0.2 J-lm wide and 0.5 J-lm long) at right angles to one another. Each member of the pair is
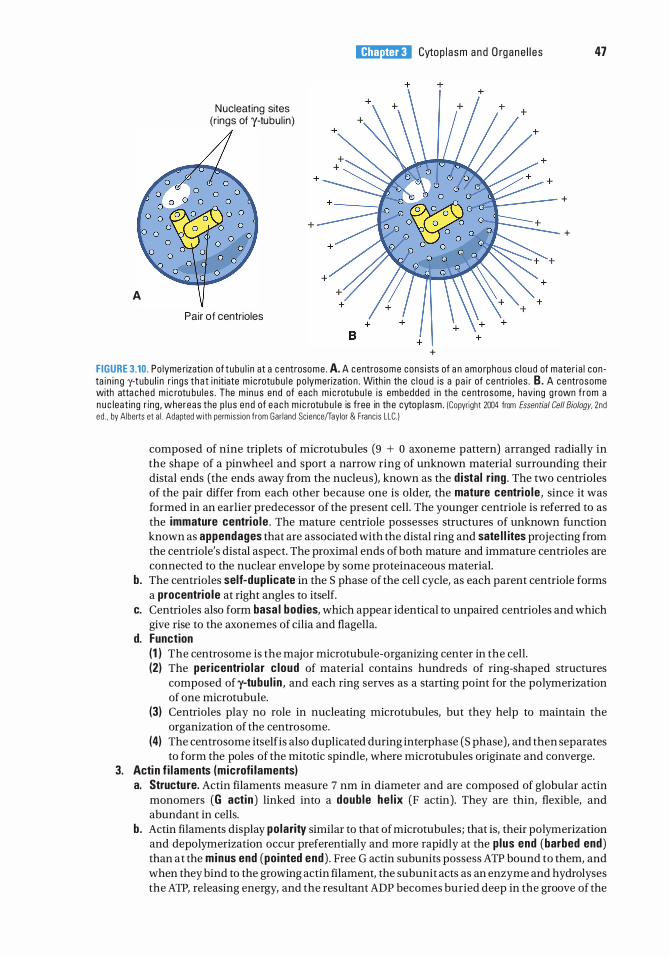
A
Nucleating sites (r ings of y-tubu l in)
Pair of centrioles
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s
+
47
+
+
FIGURE 3.10. Po lyme rization of tubu l i n at a c e ntrosome . A. A centrosome cons i sts of a n amo rphous c l o ud of mater i a l con ta i n i ng y-tubu l i n r ings that i n itiate m i c rotubu l e po lymerizati on . With in the c l o ud i s a pa i r of c entri o l es . B. A centrosome with atta ched m ic rotu bu l es . The m i nus end of each m i c rotubu l e is embedded i n the centrosome, hav ing g rown f rom a n u c leat ing r ing , whereas the p l u s end of e a c h m i c rotu b u l e is free in the cytop l asm . ICopyr ight 2004 from Essential Gel/Biology, 2nd ed . , by Alberts et a l . Adapted with permiss ion from Gar land Sc ience/Taylor & Franc is LLC. )
composed of nine triplets of microtubules (9 + 0 axoneme pattern) arranged radially in the shape of a pinwheel and sport a narrow ring of unknown material surrounding their distal ends (the ends away from the nucleus), known as the d istal r ing . The two centrioles of the pair differ from each other because one is older, the mature centrio le , since it was formed in an earlier predecessor of the present cell. The younger centriole is referred to as the immature centrio le . The mature centriole possesses structures of unknown function known as appendages that are associated with the distal ring and sate l l ites projecting from the centriole's distal aspect. The proximal ends of both mature and immature centrioles are connected to the nuclear envelope by some proteinaceous material.
b. The centrioles self-dupl icate in the S phase of the cell cycle, as each parent centriole forms a procentrio le at right angles to itself.
c. Centrioles also form basa l bodies, which appear identical to unpaired centrioles and which give rise to the axonemes of cilia and flagella.
d. Function (1 ) The centrosome is the major microtubule-organizing center in the cell. (2) The pericentrio lar c loud of material contains hundreds of ring-shaped structures
composed of y-tubu l in , and each ring serves as a starting point for the polymerization of one microtubule.
(3) Centrioles play no role in nucleating microtubules, but they help to maintain the organization of the centrosome.
(4) The centrosome itselfis also duplicated during interphase (S phase), and then separates to form the poles of the mitotic spindle, where microtubules originate and converge.
3. Actin f i laments (microfi laments) a. Structure. Actin filaments measure 7 nm in diameter and are composed of globular actin
monomers (G actin ) linked into a double he l ix (F actin). They are thin, flexible, and abundant in cells.
b. Actin filaments display polarity similar to that ofmicrotubules; that is, their polymerization and depolymerization occur preferentially and more rapidly at the plus end (barbed end) than at the minus end (pointed end) . Free G actin subunits possess ATP bound to them, and when they bind to the growing actin filament, the subunit acts as an enzyme and hydrolyses the ATP, releasing energy, and the resultant ADP becomes buried deep in the groove of the
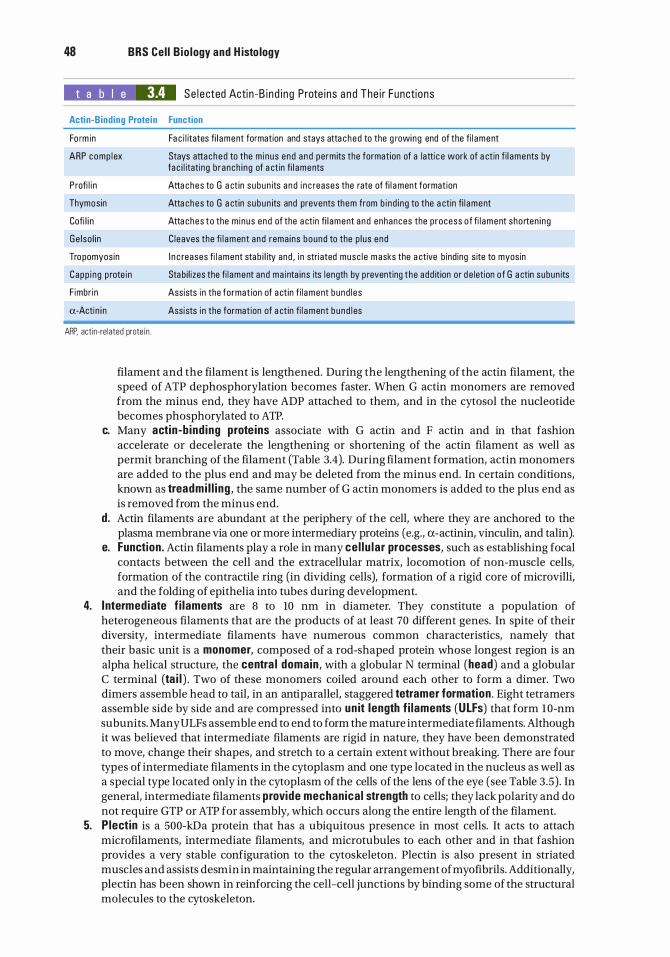
48 BRS Cel l B io logy and H isto logy
t a b I e 3.4 Se l e cted Acti n -B i n d i n g P rote i ns a n d The i r Functions
Actin-Binding Protein Function
Fo rm in Fa c i l itates fi l ament formation and stays atta ched to the g rowing end of the fi l ament
ARP comp l ex Stays attached to the m inus end a nd perm its the formation of a latti c e work of a ctin f i l aments by fa c i l itating b ranch i ng of a ctin fi l aments
Profi l i n Atta ches to G a ct in subun its a nd i n c reases the rate of fi l ament formation
Thyme sin Atta ches to G a ct in subun its and prevents them from b i nd i ng to the a ctin fi l ament
Cofi l i n Atta ches to the m inus end of the a ctin fi l ament a nd enhances the p rocess of fi l ament shorten i ng
Ge lso l i n C l eaves the fi l ament and rema ins bound to the p l us end
Tropomyosin I n c reases fi l ament stab i l ity and , i n stri ated musc l e m asks the a ctive b ind ing s ite to myosin
Capp i ng p rote in Stabi l izes the fi l ament and ma inta ins its l ength by p reventing the add ition or d e letion of G a ctin subun its
F imbr in Assists i n the format ion of a ct in f i l ament bund l es
a-Actin i n Assists i n the formation of a ct in fi l ament bund l es
ARP. actin-related prote in .
filament and the filament is lengthened. During the lengthening of the actin filament, the speed of ATP dephosphorylation becomes faster. When G actin monomers are removed from the minus end, they have ADP attached to them, and in the cytosol the nucleotide becomes phosphorylated to ATP.
c. Many actin-b ind ing prote ins associate with G actin and F actin and in that fashion accelerate or decelerate the lengthening or shortening of the actin filament as well as permit branching of the filament (Table 3.4). During filament formation, actin monomers are added to the plus end and may be deleted from the minus end. In certain conditions, known as treadmi l l i ng , the same number of G actin monomers is added to the plus end as is removed from the minus end.
d. Actin filaments are abundant at the periphery of the cell, where they are anchored to the plasma membrane via one or more intermediary proteins (e.g., a-actinin, vinculin, and talin).
e. Function . Actin filaments play a role in many ce l lu lar processes, such as establishing focal contacts between the cell and the extracellular matrix, locomotion of non-muscle cells, formation of the contractile ring (in dividing cells), formation of a rigid core of microvilli, and the folding of epithelia into tubes during development.
4. Intermediate f i laments are 8 to 10 nm in diameter. They constitute a population of heterogeneous filaments that are the products of at least 70 different genes. In spite of their diversity, intermediate filaments have numerous common characteristics, namely that their basic unit is a monomer, composed of a rod-shaped protein whose longest region is an alpha helical structure, the centra l domain , with a globular N terminal (head) and a globular C terminal (ta i l ) . Two of these monomers coiled around each other to form a dimer. Two dimers assemble head to tail, in an anti parallel, staggered tetra mer formation . Eight tetramers assemble side by side and are compressed into un it length f i laments (ULFs) that form 10-nm subunits. Many ULFs assemble end to end to form the mature intermediate filaments. Although it was believed that intermediate filaments are rigid in nature, they have been demonstrated to move, change their shapes, and stretch to a certain extent without breaking. There are four types of intermediate filaments in the cytoplasm and one type located in the nucleus as well as a special type located only in the cytoplasm of the cells of the lens of the eye (see Table 3 .5) . In general, intermediate filaments provide mechanica l strength to cells; they lack polarity and do not require GTP or ATP for assembly, which occurs along the entire length of the filament.
5. P lectin is a 500-kDa protein that has a ubiquitous presence in most cells. It acts to attach microfilaments, intermediate filaments, and microtubules to each other and in that fashion provides a very stable configuration to the cytoskeleton. Plectin is also present in striated muscles and assists des min in maintaining the regular arrangement of myofibrils. Additionally, plectin has been shown in reinforcing the cell-cell junctions by binding some of the structural molecules to the cytoskeleton.
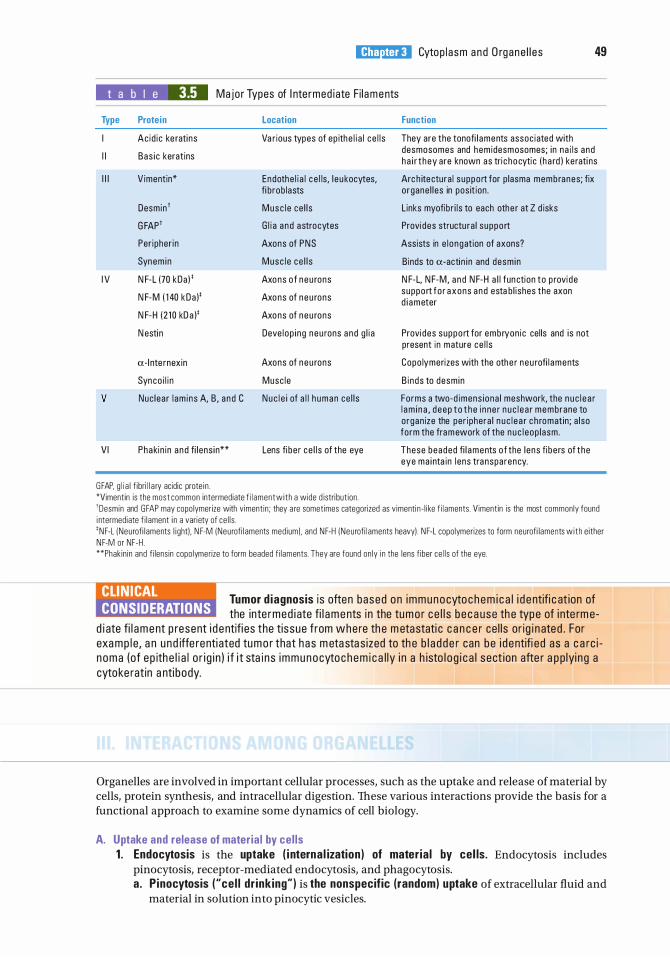
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s 49
t a b I e 3.5 Majo r Types of I nte rmed i ate F i l aments
Type
I
I I
I l l
I V
v
VI
Protein
Acid ic ke rati ns
Bas i c keratins
V imentin*
Desmin1
G FAP1
Per ipher in
Synem in
N F-L (70 kDa ) '
N F-M ( 1 40 kDa )'
N F-H ( 2 1 0 kD a )'
N esti n
a-l nte rnexin
Synco i l i n
Location
Va r ious types of ep ithe l i a l ce l l s
Endothe l i a l c e l ls, l e u kocytes, fi b rob lasts
Musc l e ce l l s
G l i a a nd astrocytes
Axons of PNS
Musc l e ce l l s
Axons o f n eu rons
Axons of n eu rons
Axons of n eu rons
Deve l op i ng neu rons a nd g l i a
Axons of n eu rons
Musc le
Nuc lea r l am ins A, B , a nd C Nuc l e i of a l l h uman ce l l s
Phakin in a nd fi l ens i n** Lens fi be r ce l l s of the eye
GFAP, g l i a l f ibri l l a ry acidic prote in . *Vimentin is the most common intermediate f i l ament wi th a wide d istri but ion .
Function
They are the tonofi l aments assoc iated with desmosomes and hem idesmosomes; in na i ls and h a i r t hey are known as tri c hocyti c ( h a rd ) ke rati ns
Arc h ite ctura l s uppo rt for p lasma membranes; fix o rgane l l es in pos it ion .
L inks myofib r i l s to each othe r at Z d isks
Provides structu ra l suppo rt
Assists in e l ongation of axons?
Binds to a-acti n i n and desm in
N F-L, N F-M, a nd N F-H a l l fun ction to p rovi de suppo rt fo r axons a nd esta b l ishes the axon d i ameter
Provides suppo rt for embryon ic cel ls and is not present in mature ce l l s
Copo lymerizes with the othe r neu rofi l aments
B i nds to desm in
Fo rms a two-d imens iona l meshwork, the n u c l e a r l am i n a , d eep t o t h e i n ne r n u c l e a r membrane to o rgan ize the per iphera l n u c l e a r c h romatin ; a lso form the fram ework of the n u c l eop l asm .
These beaded fi l aments of the l ens fi be rs of the eye ma i nta in l ens tra nsparency.
'Desmin and GFAP may copo lymerize with vimentin; they a re sometimes categorized as vimenti n - l i ke f i laments. Vimentin is the most commonly found i ntermediate f i lament i n a variety of ce l l s . 'NF-L INeurofi laments l i ght). N F-M INeurofi laments med ium) . and NF-H INeu rofi laments heavy). NF-L copolymerizes to form neurofi laments wi th either NF-M or NF-H. **Phak in in and f i lens in copo lymerize to form beaded f i laments. They are found on ly i n the lens f iber ce l l s of the eye.
CLIN ICAL CONSIDERATIONS
Tumor d iagnosis i s often based on immunocyto c h e m i c a l i d e ntifi c at ion of the inte rmed i ate fi l aments i n the tu mo r ce l l s b e c a use th e type of i nte rm e
d i ate fi l ament p resent i d e ntifi es the tissue from whe re th e m etastati c c a n c e r ce l l s o r ig i n ated . For exa mp l e , a n und iffe renti ated tum o r that has m eta sta s ized to th e b l a d d e r can be i d entifi ed as a c a rc i n oma (of ep ith e l i a l o r i g i n ) i f i t sta i ns immunocyto chem i c a l ly i n a h isto l o g i c a l sect ion afte r a p p lyi n g a cytoke ratin a nti body.
Organelles are involved in important cellular processes, such as the uptake and release of material by cells, protein synthesis, and intracellular digestion. These various interactions provide the basis for a functional approach to examine some dynamics of cell biology.
A. Uptake and release of materia l by cel ls 1 . Endocytosis is the uptake ( i nterna l ization ) of mater ia l by cel ls. Endocytosis includes
pinocytosis, receptor-mediated endocytosis, and phagocytosis. a. P inocytosis ("ce l l dr inking") is the nonspecific (random) uptake of extracellular fluid and
material in solution into pinocytic vesicles.
50 BRS Cel l B io logy and H isto logy
b. Receptor-mediated endocytosis is the specific uptake of a substance ( l igand) , such as lowdensity lipoproteins (LDLs) and protein hormones, by a cell that has a plasma membrane receptor for that ligand. It involves the following sequence of events (Figure 3 .5) : (1 ) A ligand binds specifica l ly to its receptors on the cell surface. (2) Ligand-receptor complexes cluster into a c lathrin-coated pit, which invaginates and
gives rise to a clathrin-coated vesicle containing the ligand. (3) The cytoplasmic clathrin coat is rapidly lost, leaving an uncoated endocytic ves ic le
containing the ligand.
CLINICAL CONSIDERATIONS
Fami l i a l hypercholestero lemia i s assoc i ated with a d e c reased a b i l ity of c e l l s to ta ke i n c h o l este ro l , wh i c h no rma l ly is i n g ested by re c e ptor-med i
ated endo cytos is o f LD Ls .
1 . Th is d i sease is c a used by a n i n h e rited g e net ic d efect that resu lts i n a n i n a b i l ity to synth es ize LD L re c eptors o r i n the synthes is of d efe ctive re c e ptors u n a b l e to b ind e ith e r to LDLs o r to c l ath ri n - c oated p its .
2. It is c h a r a cter ized by a n e l evated l eve l of cho l e ste ro l in the b l oodstre a m . Th is fa c i l itates ea r ly deve l o pment of atherosc lerosis, wh i c h may be fata l .
c. Phagocytosis ("ce l l eati ng") i s the uptake o f microorganisms, other cells, and particulate matter (frequently of foreign origin) by a cell. Phagocytosis usually involves cell surface receptors. It is characteristic of cells-particularly macrophages and neutroph i ls-that degrade proteins and cellular debris, and involves the following sequence of events : (1 ) A macrophage binds via its Fe receptors to a bacterium coated with the antibody
immunoglobulin G (IgG) or via its C3b receptors to a complement-coated bacterium. (2) Binding progresses until the plasma membrane completely envelops the bacterium,
forming a phagocytic vacuole. 2. Exocytosis is the release of mater ia l from the cell via fusion of a secretory granule membrane
and the plasma membrane. It requ i res interaction of receptors in both the secretory granu le membrane and the p lasma membrane as well as the coalescence (adherence and joining) of the two phospholipid membrane bilayers. Exocytosis takes place in both regulated and constitutive secretion. a. Regulated (signal-directed) secretion is the release, in response to an extracel lu lar s ignal .
of enzymes, neurosecretions, and other materials stored in the cell. b. Constitutive secretion (default pathway) is the more or less conti nuous release of material
(e.g., collagen and plasma proteins) without any intermediate storage step. An extracellular signal is not required for constitutive secretion.
3. Membrane recycl ing maintains a relatively constant plasma membrane surface area following exocytosis. In this process, the secretory granule membrane added to the plasma membrane surface during exocytosis is retr ieved through endocytosis via clathrin-coated vesicles. This membrane is returned to the TGN via early endosomes for further recycling. Figure 3 . 1 1 illustrates endocytic pathways used by cells. More specific information concerning the mechanisms of membrane recycling and transference was presented in earlier sections of this chapter (see Section 8, Coated vesicles) .
B. Prote in synthesis 1. Synthesis of membrane-packaged protei ns involves translation of mRNAs encoding the
protein on polyribosomes at the surface of the RER, transport of the growing polypeptide chain across the RER membrane and i nto the c isterna ( lumen), and the processing of the polypeptide/protein within the RER. These water-soluble proteins will bud from the RER and be transported in vesicles either for transfer into the lumen (or interior) of another organe l le or for secretion from the cell.
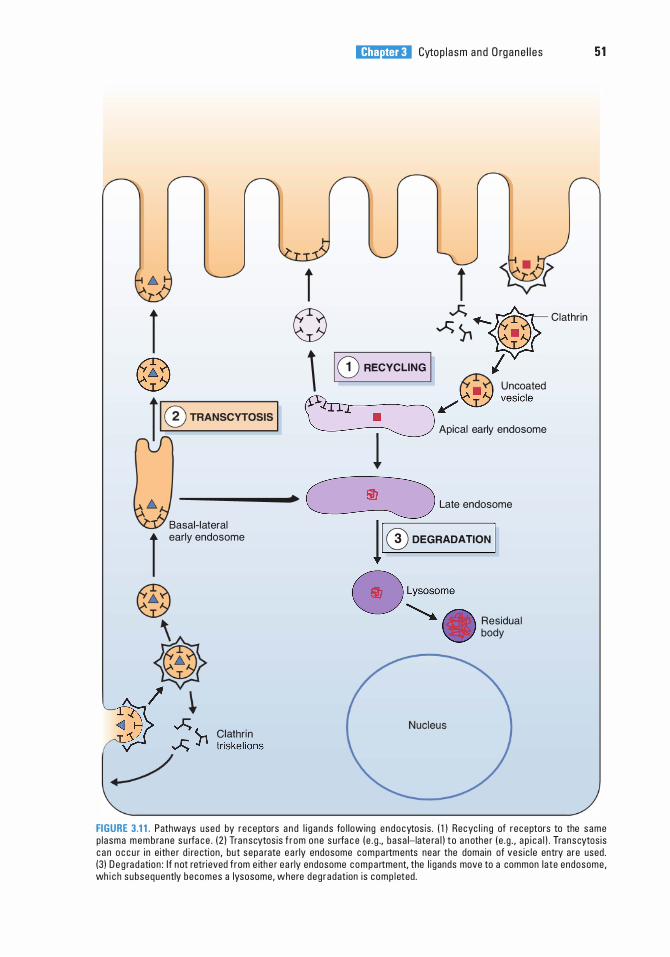
l ®
l ©
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s 51
l _;:;. ._ ft- Clathrin ..;:;" wr i I CD RECYCLING I I � U n�oated �/� ve'" ' ' l Apic.l eMiy ernlooome
--------+ � L•te eodooome
Basal- lateral l eocly eodooome
® ?$
-4� --;\ ... c'""''" � � J1 triskel ions
.-/
11 ® DEGRADATION I 8 Lyoooome
.......... . Residual body
FIGURE 3.1 1 . Pathways used by receptors a n d l i g ands fo l lowing endocytos is . ( 1 ) Recyc l i n g of receptors to the same p l asma memb ra n e s u rfa ce . ( 2 1 Transcytos is f r om one s u rfa c e ( e . g . , basa l-late ra l ) t o a n othe r ( e . g . , a p i c a l ) . Transcytos is c a n o c c u r i n e ithe r d i re ction , but sepa rate e a rly endosome c o m p a rtments near the doma in of ves i c l e entry are used . (3) D e g ra d ation : I f not retrieved from e ith e r ea rly endosome c o m p a rtment, the l i gands move to a common late endosome , wh i c h subsequently becomes a lysosome, where deg radat ion i s comp l eted .
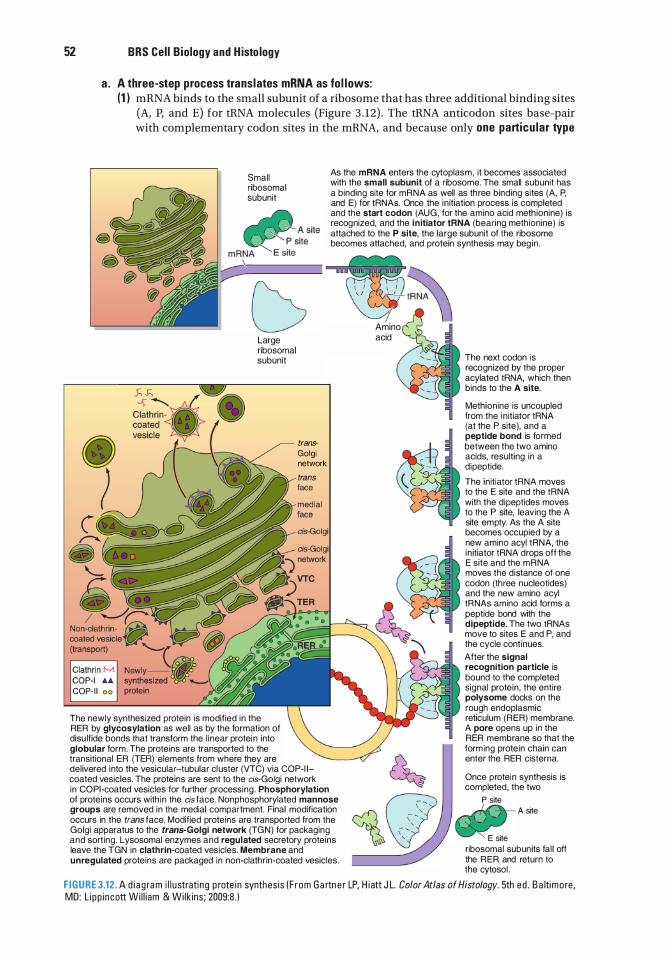
52 BRS Cel l B iology and H isto logy
a . A three-step process translates mRNA as fo l lows: (1 ) mRNA binds to the small subunit of a ribosome that has three additional binding sites
(A, P, and E) for tRNA molecules (Figure 3 . 12) . The tRNA anticodon sites base-pair with complementary codon sites in the mRNA, and because only one particu lar type
Small ribosomal subunit
As the mRNA enters the cytoplasm, it becomes associated with the small subunit of a ribosome. The small subunit has a binding site for mRNA as well as th ree binding sites (A, P, and E) for tRNAs. Once the in itiation process is completed and the start codon (AUG, for the amino acid meth ionine) is recognized, and the i n itiator !RNA (bearing meth ionine) is attached to the P site, the large subunit of the ribosome becomes attached, and protein synthesis may begin .
�
• I (
COP- I I o o
Large ribosomal subunit
The newly synthesized protein is modified in the RER by glycosylation as well as by the formation of disu lfide bonds that transform the l inear protei n into globular form. The proteins are transported to the transitional ER (TER) elements from where they are
trans· Golgi network
del ivered into the vesicular-tubular cl uster (VTC) via COP-1 1-coated vesicles. The proteins are sent to the cis-Golgi network in CO PI -coated vesicles for further processing. Phosphorylation of proteins occurs with in the cis face. Nonphosphorylated mannose groups are removed in the medial compartment. Final modification occurs in the trans face. Modified proteins are transported from the Golgi apparatus to the trans-Golgi network (TG N) for packaging and sort ing. Lysosomal enzymes and regulated secretory proteins leave the TGN in clathrin-coated vesicles. Membrane and unregulated proteins are packaged in non-clathrin-coated vesicles.
� !RNA
Amino acid
The next codon is recognized by the proper acylated !RNA, which then binds to the A site.
Methionine is uncoupled from the in itiator !RNA (at the P site), and a peptide bond is formed between the two amino acids, resulting in a d ipeptide.
The in itiator !RNA moves to the E site and the !RNA with the dipeptides moves to the P site, leaving the A site empty. As the A site becomes occupied by a new amino acyl !RNA, the in itiator !RNA drops off the E site and the m RNA moves the distance of one codon (three nucleotides) and the new amino acyl tRNAs amino acid forms a peptide bond with the dipeptide. The two tRNAs move to sites E and P, and the cycle cont inues. After the signal recognition particle is bound to the completed signal prote in , the entire polysome docks on the rough endoplasmic reticulum (RER) membrane. A pore opens up in the RER membrane so that the form ing prote in chain can enter the RER cisterna.
Once protein synthesis is completed, the two
P site A site
E site ribosomal subunits fal l off the RER and return to the cytosol .
F I G U R E 3.12. A d i a g ra m i l l u stratin g p rote in synthes is ( F r om G a rtn e r LP, H i att J L. Color Atlas of Histology. 5th ed . B a ltimo re , MD: L i pp i ncott Wi l l i am & Wilk ins ; 2009:8 . )
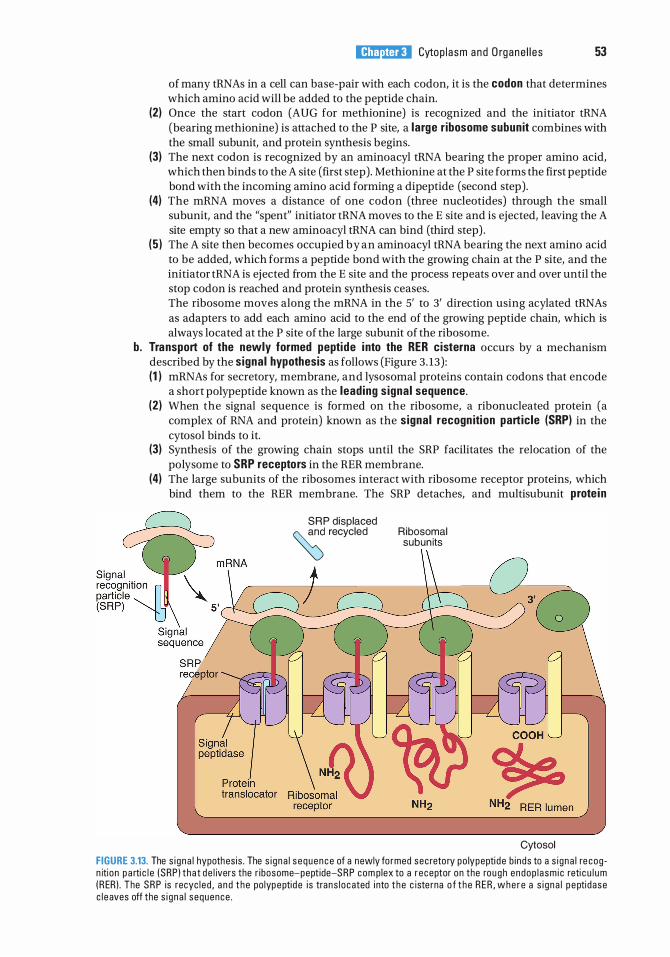
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s 53
of many tRNAs in a cell can base-pair with each codon, it is the codon that determines which amino acid will be added to the peptide chain.
(2) Once the start codon (AUG for methionine) is recognized and the initiator tRNA (bearing methionine) is attached to the P site, a large r ibosome subunit combines with the small subunit, and protein synthesis begins.
(3) The next codon is recognized by an aminoacyl tRNA bearing the proper amino acid, which then binds to the A site (first step). Methionine at the P site forms the first peptide bond with the incoming amino acid forming a dipeptide (second step).
(4) The mRNA moves a distance of one codon (three nucleotides) through the small subunit, and the "spent" initiator tRNA moves to the E site and is ejected, leaving the A site empty so that a new aminoacyl tRNA can bind (third step) .
( 5 ) The A site then becomes occupied by an aminoacyl tRNA bearing the next amino acid to be added, which forms a peptide bond with the growing chain at the P site, and the initiator tRNA is ejected from the E site and the process repeats over and over until the stop codon is reached and protein synthesis ceases. The ribosome moves along the mRNA in the 5' to 3' direction using acylated tRNAs as adapters to add each amino acid to the end of the growing peptide chain, which is always located at the P site of the large subunit of the ribosome.
b. Transport of the newly formed peptide into the RER cisterna occurs by a mechanism described by the signal hypothesis as follows (Figure 3 . 13) : (1 ) mRNAs for secretory, membrane, and lysosomal proteins contain codons that encode
a short polypeptide known as the leading s ignal sequence. (2) When the signal sequence is formed on the ribosome, a ribonucleated protein (a
complex of RNA and protein) known as the signal recogn ition particle (SRP) in the cytosol binds to it.
(3) Synthesis of the growing chain stops until the SRP facilitates the relocation of the polysome to SRP receptors in the RER membrane.
(4) The large subunits of the ribosomes interact with ribosome receptor proteins, which bind them to the RER membrane. The SRP detaches, and multisubunit prote in
S R P displaced � recycled Ribosomal
subun its
Cytosol FIGURE 3.13. The s i g na l hypothes is . The s i g na l s equence of a newly fo rmed sec reto ry po lypepti d e b i nds to a s i g na l re cog n itio n p a rti c l e (SRP ) that d e l ivers the r i bosome-pept ide-S R P com plex to a r eceptor on the rou g h endop l a sm i c reti c u l u m ( R ER) . The S R P is recyc l ed , a n d t h e po lypeptid e i s trans l ocated i nto t h e c iste rna o f t h e R E R , w h e r e a s i g n a l p e ptidase c l e aves off the s i g na l sequence .
54 BRS Cel l B io logy and H isto logy
translocators form a pore across the RER membrane. Synthesis resumes, and the newly formed polypeptide is threaded through the pore and into the RER cisterna (lumen).
c. Posttranslationa l mod ification i n the RER (1 ) After the newly formed polypeptide enters the cisterna, a signa l peptidase cleaves the
signal sequence from it. (2) The polypeptide is glycosylated. (3) Disulfide bonds form, converting the linear polypeptide into a globular form.
d. Prote in transport from the RER to the cis-Go lg i (Figure 3 . 14) (1 ) Transitional elements of the RER give rise to COP-I I coatomer-coated vesicles
containing newly synthesized protein. (2) These vesicles move to the VTCs, where they fuse with the membranes to deliver the
protein. (3) The VTC appears to be the first way station for the segregation of anterograde versus
retrograde transport in the secretory pathway. Either proteins move forward toward the c is-Go lg i , or if they are RER-resident proteins that escaped from the RER, they are captured by a specific membrane receptor protein and returned in COP-I coatomercoated ves ic les to the RER along a microtubule-guided pathway.
e. Anterograde transport from the VTC to the cis-Golgi is via COP-II coatomer-coated vesicles. f. Movement of mater ia l anterograde among the Go lg i subcompartments may occur by
cisternal maturation and/ or by vesicular transport, as follows : (1 ) Cisternae-containing proteins may change in biochemical composition as they move
intact across the stack. (2) Vesicles (COP-II-coated, according to some investigators) may bud off one cisterna and
fuse with the dilated rim of another cisterna. (3) Although both mechanisms have been observed, the precise way that anterograde
transport occurs across the Golgi stack of cisternae is unresolved. (4) Retrograde vesicular transport occurs between Golgi cisternae and between the Golgi
and the VTC or RER via CO P-I-coated vesicles. g . Prote in processing in the Go lg i complex (Figure 3 . 14) occurs as proteins move from the cis
to the trans face of the Golgi complex through d isti nct c isterna l subcompartments. Protein processing may include the following events, each of which occurs in a different cisternal subcompartment : (1 ) Proteins targeted for lysosomes are tagged with mannose 6-phosphate in the cis
cisterna. (2) Mannose residues are removed in cis and medial cisternae. (3) Some proteins undergo terminal glycosylation with sialic acid residues and galactose. (4) Sulfation and phosphorylation of amino acid residues take place. (5) A membrane similar in composition and thickness to the plasma membrane is
acquired. h. Sorting of prote ins in TGN (Figure 3.1 4)
(1 ) Regulated secretory prote ins are sorted from membrane and lysosomal proteins and delivered via clathrin-coated vesicles to condensing vacuoles, in which removal of water via ionic exchanges yields secretory g ranu les.
(2) Lysosomal prote ins are sorted into clathrin-coated regions of the TGN that have receptors for mannose 6-phosphate and are delivered to late endosomes via clathrincoated vesicles.
(3) P lasma membrane prote ins are sorted into coatomer-coated regions of the TGN and delivered to the plasma membrane in COP-II coatomer-coated vesicles.
2. Synthesis of transmembrane proteins also takes place on polyribosomes at the surface of the RER, but rather than entering the lumen, the transfer process is ha lted (by a stop-transfer sequence), and the transmembrane protein becomes anchored in the RER membrane. The ultimate destination of this protein will be the RER membrane, the membrane of another organelle, or the plasma membrane.
3. Synthesis of cytosol ic prote ins takes place on polyribosomes lying free in the cytosol and is directed by mRNAs that lack signal codons. Such proteins (e.g., protein kinase and hemoglobin) are released directly into the cytosol.
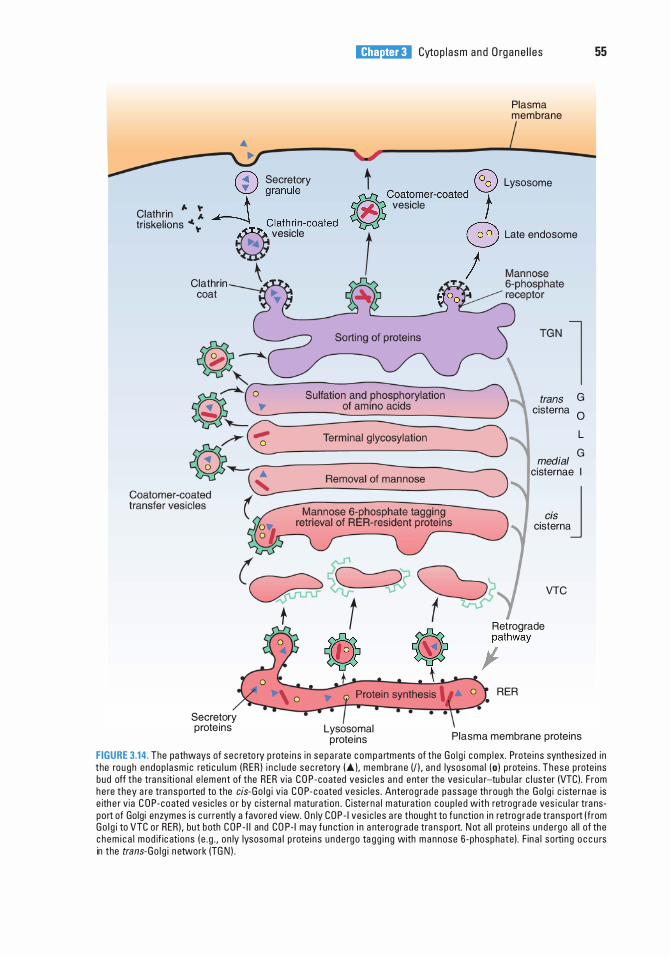
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s
Plasma membrane
55
• I �-----�-------���----------�-------� Secretory t � Lysosome
+ vesicle Clath rin " : triskel ions • "
W granule �Coatomer-coated \_.::.Jt � Clath rin-coated r::;:;-., � v"lole r r Lote eodoeome
Clathrin coat
Secretory prote ins
I. T,. "' 00 -4
trans G cisterna 0
L G medial
cisternae I
cis J cisterna
(Gd�� VTC
f t � Retmgcade � � ;athway
t \
Lysosomal prote ins
RER
Plasma membrane proteins FIGURE 3.14. The pathways of sec reto ry p rote i ns i n sepa rate c o m p a rtme nts of the Go l g i c omp l ex. Prote i ns synthes ized i n the rou g h endop l asm i c reti c u l u m (RER I i n c l u de sec reto ry I"' I , membra n e U l , a n d lysosoma l (o l p rote ins . These p rote ins bud off the tra ns iti ona l e l em ent of the RER via C O P-coated ves i c l e s a n d e nter the vesi c u l a r-tu b u l a r c l uster (VTCI . F rom he re they a re tra nspo rted to the cis-Go l g i v ia C O P-coated ves ic les . Anterog rade passage th rough the Go l g i c iste rnae is e ith e r v ia C O P-coated ves ic l es o r by c i sterna l m aturati on . C iste rna l m aturati on coup l ed with retrog rade ves i c u l a r tra nspo rt of Golg i enzymes is c u rrently a favo red view. O n ly COP - I ves i c l es a re thought to function i n retrog rade transport (from Go l g i to VTC o r RERI , but both C O P - I I and CO P- I may functi on i n a nte rog rade tra nspo rt. N ot a l l p rote i ns u nde rgo a l l of the c h e m i c a l mod if ic ati ons ( e . g . , o n ly lysoso m a l p rote i n s u n d e rgo ta gg i n g with m a n nose 6-phosphatel . F in a l so rti n g o c c u rs in the trans-Go l g i n etwork (TG N I .
56 BRS Cel l Bio logy and H isto logy
C. I ntrace l lu lar d igestion 1 . Non lysosomal d igestion is the degradation of cytosolic constituents by mechanisms outside
of the vacuolar lysosomal pathway. The major site for the degradation of unwanted proteins is the proteasome, a cylindrical complex of nonlysosomal proteases. Proteins marked for destruction are enzymatically tagged with ub iqu itin, a relatively small protein 76 amino acids long that is commonly occurring in the cytoplasm and the nucleus. It is the ubiquitination that delivers them to the proteasome, where they are broken down to small peptides, seven to eight amino acids long. a. Each proteasome is a 26S nonmembranous, cylindrical organelle with a hollow center;
it is composed of three subunits, a 20S core parti c le and two regu latory part ic les, 19S each, capping each end (entry face [top] and exit face [bottom] ) of the proteasome. The core particle is 15 nm tall with a diameter of 1 1 to 12 nm whose central lumen may be as small as 1 .3 nm in diameter or as large as 5.3 nm. Viewed from the side, the core particle is seen to be composed of four ring-shaped units, named a, �. �. and a, counting from entry face to exit face. The two a subunits bind the regulatory particles, whereas the luminal aspects of the two � subunits function as proteolytic enzymes. The regulatory subunit at the entry face acts as a lid that controls access to the lumen of the proteasome, whereas the regulatory subunit on the exit face permits the release of the products of proteolysis.
b. In order for a protein to be permitted entry into the lumen ofthe proteasome, the protein has to be ubiquitinated, a process that requires a set of three enzymes that attach a ubiquitin molecule to the targeted protein . The first enzyme, ub iqu it in-activat ing enzyme (E1 ), activates ubiquitin so that the second enzyme, ub iqu it in-conj ugati ng enzyme ( E2), can bind to the targeted protein . The third enzyme, ub iqu it i n - l i gase ( E3) can now transfer the ubiquitin molecule to the targeted protein. This process is repeated several times, so that a number of ubiquitin molecules may be attached to each other, forming a polyub iqu it in cha in bound to the targeted protein. E 1 , E2, and especially E3, come in many forms, indicating that recognition of a specific targeted protein is probably enzyme specific.
c. Once the targeted protein is polyubiquitinated (at least four ubiquitin molecules must be bound to the protein) it may bind, in the presence of ATP, to the regulatory particle at the entry face. The regulatory particle unhinges and, similar to a lid that is attached to a pot, lifts to allow the protein access to the lumen of the core particle. However, in order for the protein to be able to enter the narrow lumen of the core particle, two things must take place: ( 1 ) the target protein must be deubiquitinated and (2) the targeted protein must be unfolded, where the unfolding is an energy-requiring process. The unfolded protein is introduced into the lumen of the core particle, a procedure known as translocation . The targeted protein is then degraded by the enzymatic activity of the � subunits of the proteasome.
Although most proteins must be ubiquitinated before they may enter a proteasome, there are certain exceptions, especially if the cell is under stressful conditions such as exposure to high temperature, infectious agents, or higher than normal oxygen levels.
2. Lysosomal d igestion (Figure 3.8) is the degradation of material within various types of lysosomes by lysosomal enzymes. Different lysosomal compartments are involved, depending on the origin of the material to be degraded. a . Heterophagy is the ingestion and degradation of fore ign material taken into the cell by
receptor-mediated endocytosis or phagocytosis. (1 ) Digestion of endocytosed ligands occurs in multivesicular bodies (Figure 3.8) . (2) Digestion of phagocytosed microorganisms and foreign particles begins and may be
completed in phagolysosomes. b . Autophagy is the segregation of an organelle or other cell constituents within membranes
from the RER to form an autophagic vacuole (Figure 3.9), which is subsequently digested in an autophagolysosome.
c. Crinophagy is the fusion of hormone secretory granules and lysosomes and their subsequent digestion. Crinophagy is used to remove excess numbers of secretory granules from the cell.
l!1i!tttttiil Cytop l asm and O rgane l l es 57
CLIN ICAL CONSIDERATIONS
Lysosomal storage d iseases a re he red ita ry d i so rd e rs c a used by a d efic i e n cy i n s pec if ic lysosoma l a c i d hyd ro l a ses . The refo re, lysosomes a re
u n a b l e to d e g ra d e c e rta i n compounds, wh ich a c c u m u l ate a n d i nte rfe re with c e l l f uncti on . 1 . Tay-Sachs d isease is c h a ra cte r ized by g lyco l i p i d s ( n a m e ly, G M2 g a n g l i os i des ) a c c u m u l ati n g
i n t h e lysosomes o f n e u rons a s a resu lt o f a d efi c i e n cy o f t h e enzym e hexosa m i n i d ase A. The d i s e a se is most common i n c h i l d ren o f c e ntra l E u ro p e a n J ewish descent. The l a rg e bu i l d u p of g a n g l i os i des i n n e u rons of the b ra i n resu lts i n m a rked d egene rative c h a nges in th e c e ntra l n e rvous system, a n d d e ath u s u a l ly o c c u rs before th e a g e of 4 yea rs .
2. A h a l l m a rk of Hur ler syndrome i s that g lycosam i nog lyc a n s ( GAGs ) and p roteog lyc ans a c c u m u l ate i n t h e h e a rt, b ra i n , l iver, a n d oth e r o rg a ns . Th is rare i n h e rited d i sease i s c a used b y a d efi c i e n cy in a ny 1 of 1 0 lysoso m a l e nzymes involved in the sequenti a l d e g r a datio n of GAGs . C l i n i c a l fe atu res of H u r l e r synd rome i n c l u d e s ke l eta l d eform iti es, e n l a rg e d o rg a n s, prog ress ive m e nta l d eter io ration , d e afness, a n d d e ath before th e a g e of 10 yea rs.
3. G lycogen storage d iseases a re c a used by a he red ita ry d efect i n an enzyme involved i n e ith e r th e synth es is o r t h e deg r adati o n o f g lyc ogen . As a resu lt, g lycogen a c c u m u l ates most ofte n i n th e l iver, ske leta l musc l e , a n d t he h e a rt, b u t th e ma jo r o rg a n invo lvement d e pends on t he p a rt ic u l a r enzymat ic d efe ct. The re a re at l e ast 1 0 d isti n ct g lycogen sto ra g e d i seases .
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which of the following organelles divides by fission?
(A) Golgi complex (B ) RER (C ) Peroxisome (D ) SER (E ) Centriole
2. A 30-year-old man with very high blood cholesterol levels (290 mg/dL) has been diagnosed with premature atherosclerosis. His father died of a heart attack at age 45, and his mother, aged 44, has coronary artery disease. Which of the following is the most likely explanation of his condition?
(A) He has a lysosomal storage disease and cannot digest cholesterol.
(B ) He has a peroxisomal disorder and produces low levels of hydrogen peroxide.
(C) The SER in his hepatocytes has proliferated and produced excessive amounts of cholesterol.
(D ) He has a genetic disorder and synthesizes defective LDL receptors.
(E) He is unable to manufacture endosomes.
3. Movement of protein from the RER to the VTC takes place in which of the following cell components?
(A) A caveolin-coated vesicle (B ) A clathrin-coated vesicle (C) A coatomer !-coated vesicle (D ) A coatomer II-coated vesicle (E ) An early endosome
4. The retrieval of secretion granule membrane immediately after exocytosis occurs in which of the following cell components?
(A) A caveolin-coated vesicle (B ) A clathrin-coated vesicle (C) A coatomer !-coated vesicle (D ) A coatomer II-coated vesicle (E ) An early endosome
58
5. Movement of protein from trans to cis-Golgi cisternae occurs in which of the following cell components?
(A) A caveolin-coated vesicle (B ) A clathrin-coated vesicle (C ) A coatomer !-coated vesicle (D ) A coatomer II-coated vesicle (E) An early endosome
6. Uncoupling of endocytosed ligands from receptors takes place in which of the following cell components?
(A) A caveolin-coated vesicle (B ) A clathrin-coated vesicle (C) A coatomer !-coated vesicle (D ) A coatomer II-coated vesicle (E) An early endosome
7. Movement of acid hydrolases from the TGN to a late endosome takes place in which of the following cell components?
(A) A caveolin-coated vesicle (B ) A clathrin-coated vesicle (C) A coatomer !-coated vesicle (D ) A coatomer II-coated vesicle (E) An early endosome
8. Which of the following cytoskeletal components is associated with kinesin?
(A) Keratin (B ) Lamin A (C ) Micro filament (D ) Microtubule (E ) Neurofilament
9. Which of the following consists of globular actin monomers linked into a double helix?
(A) Keratin (B ) Lamin A (C ) Microfilament (D ) Microtubule (E ) Neurofilament
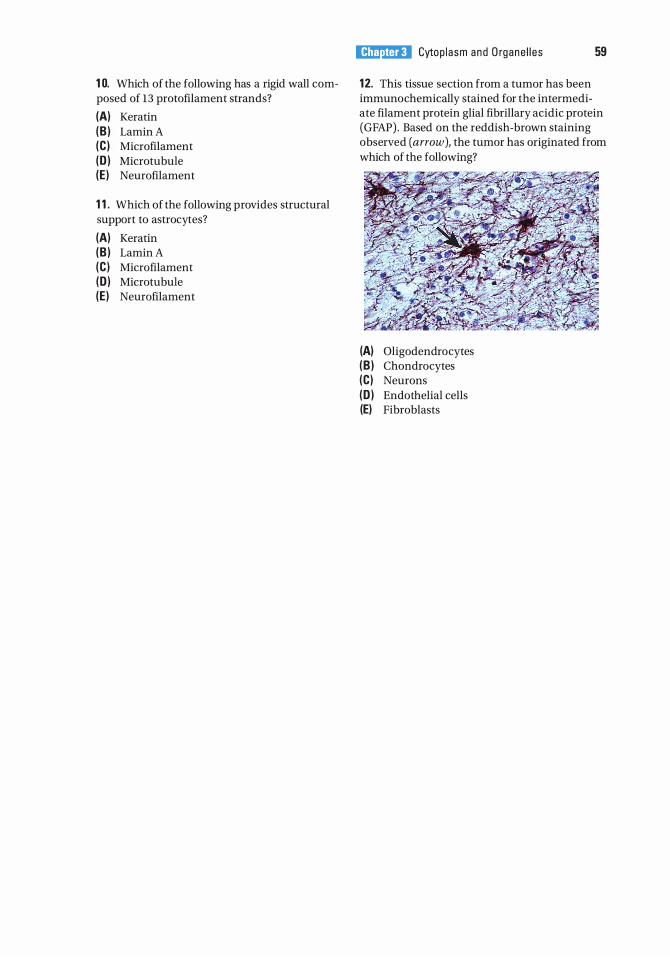
1 0. Which of the following has a rigid wall composed of 13 protofilament strands?
(A) Keratin (B ) Lamin A (C ) Microfilament (D ) Microtubule (E ) Neurofilament
1 1 . Which of the following provides structural support to astrocytes?
(A) Keratin (B ) Lamin A (C ) Micro filament (D ) Microtubule (E ) Neurofilament
l!1i!tttttiil Cytop l a sm a n d O rgane l l e s 59
1 2. This tissue section from a tumor has been immunochemically stained for the intermediate filament protein glial fibrillary acidic protein (GFAP) . Based on the reddish-brown staining observed (arrow), the tumor has originated from which of the following?
(A) Oligodendrocytes (B ) Chondrocytes (C) Neurons (D ) Endothelial cells (E) Fibroblasts
Answers and Explanations
1 . C. A peroxisome originates from preexisting peroxisomes. It imports specific cytosolic proteins and then undergoes fission. The other organelle that divides by fission is the mitochondrion (see receptor-mediated Chapter 3 II A 10) .
2. D . Cells import cholesterol by the receptor-mediated uptake of LDLs in coated vesicles. Certain individuals inherit defective genes and cannot make LDL receptors, or they make defective receptors that cannot bind to clathrin-coated pits. The result is an inability to internalize LDLs, which leads to high levels of LDLs in the bloodstream. High LDL levels predispose a person to premature atherosclerosis and increase the risk of heart attacks (see Chapter 3 III A 1 Clinical Considerations) .
3. D . Transport of protein from the RER to the VTC occurs via (COP-II) coatomer-coated vesicles (see Chapter 3 III B c) .
4. B. Membrane recycling after exocytosis of the contents of a secretion granule occurs via clathrin-coated vesicles (see Chapter 3 III A 3) .
5. C. Transfer of material among the cisternae of the Golgi complex in a retrograde direction takes place via (COP-I} coatomer-coated vesicles (see Chapter 3 III B e) .
6. E . The uncoupling of ligands and receptors internalized by receptor-mediated endocytosis occurs in the early endosome (see Chapter 3 II A 9 b) .
7 . B . Proteins targeted for lysosomes (via late endosomes) leave the TGN in clathrin-coated vesicles (see Chapter 3 II A 8 a).
8. D . Kinesin is a force-generating protein associated with microtubules. It serves as a molecular motor for the transport of organelles and vesicles outward, away from the centrosome (see Chapter 3 II C 1 ) .
9. C. Globular actin monomers (G actin} polymerize into a double helix of filamentous actin (F actin}, also called a microfilament, in response to the regulatory influence of a number of actinbinding proteins (see Chapter 3 II C 2} .
1 0. D . A microtubule consists of a- and �-tubulin dimers polymerized into a spiral around a hollow lumen to form a fairly rigid tubule. When cross-sectioned, the microtubule reveals l3 protofilament strands, which represent the tubulin dimers present in one complete turn of the spiral (see Chapter 3 II C 1 ) .
1 1 . E . Glial filaments are a type of intermediate filament composed of GFAP and present in fibrous astrocytes. These filaments are supportive, but they may play additional roles in both normal and pathologic processes in the central nervous system (see Chapter 3 II C 3} .
1 2. A. The intermediate filament protein GFAP is present in glial cells, including microglia, oligodendrocytes, fibrous astrocytes, and Schwann cells. Vim en tin is found in cells of connective tissue origin, which include fibroblasts, chondrocytes, and endothelial cells. Neurons contain intermediate neurofilaments, which would not stain for either GFAP or vimentin (Chapter 3 II C 3 Clinical Considerations).
60
Extracellular Matrix
A. Structure. The extracellular matrix (ECM) is an organ ized meshwork of macromolecules surrounding and underlying cells. Although it varies in composition, in general it consists of an amorphous ground substance (containing primarily glycosaminoglycans [GAGs], proteoglycans, and glycoproteins [multiadhesive glycoproteins] ) and f ibers (Figure 4 . 1 ) .
B . Functions. The ECM, along with water and other small molecules (e.g., nutrients, ions), constitutes the extracel lu lar environment . By affecting the metabolic activities of cells in contact with it, the ECM may alter the cells and influence their shape, migration, cell-cell interactions, cell division, and their differentiation. Additionally, the ECM provides physical support against compressive as well as tensile forces.
A. G lycosaminoglycans (GAGs), are long, unbranched polysaccharides composed of repeating identical disaccharide un its. 1. An amino sugar, either N-acetylglucosamine or N-acetylgalactosamine, is always one of the
repeating disaccharides. 2. Because GAGs are commonly su lfated and usually possess a uron ic ac id sugar, which has a
carboxyl group in the repeating disaccharide unit, they have a strong negative charge . 3. GAGs are generally linked to a core protei n . 4 . The attraction of osmotically active cations (e.g., Na+) to GAGs results in a heavily hydrated
matrix that strongly resists compress ion . 5 . Their extended random coils occupy large volumes of space because they do not fold
compactly. 6. GAGs may be classified into four main groups on the basis of their chemical structure
(Table 4 . 1 ) . a. Hya luron ic acid (hyaluronan) i s a very large unsulfated molecule up to 20 1-!m in length and
as much as 10,000 kDa in weight; but it is not attached to a core protein. b. The other three GAG groups are chondro it in su lfate and dermatan su lfate, hepar in and
heparan su lfate, and keratan su lfate .
61
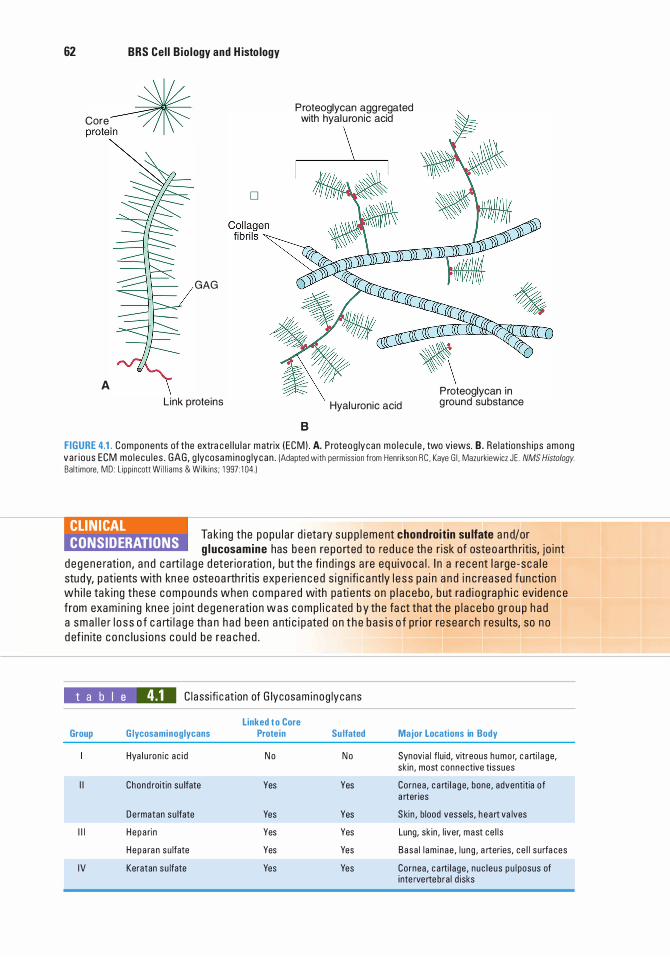
62 BRS Cel l B io logy and H isto logy
C"e � prole�
D
GAG
A Link proteins
P roteoglycan agg regated with hyal u ronic acid
\
Hyal u ronic acid
B
P roteoglycan in g round substance
FIGURE 4.1 . Components of the extra ce l l u l a r m atrix I ECM) . A. P roteog lycan mo l ecu l e , two vi ews. B. Re lationsh i ps among va r i ous ECM mo l ecu l es . GAG, g lycosa m i nog lycan . (Adapted with permiss ion from Henr ikson RC . Kaye G l . Mazurkiewicz J E . NMS Histology.
Ba lt imore , MD : L ipp incott Wi l l i ams & Wilk ins ; 1 997 : 1 04. )
CLIN ICAL CONSIDERATIONS
Ta k ing the popu l a r d i eta ry s upp l ement chondroit in su lfate a n d/or g lucosamine has been re po rted to red u c e th e r isk of osteo a rth ritis, j o i nt
d e gene rati on , a n d c a rti l a g e d eter io rati on , but th e fi n d i n gs a re eq u ivo c a l . I n a re c e nt l a rge -sc a l e study, p at ie nts with kn ee osteoa rth ritis exp e rie n c e d s i gn ifi c a ntly l e s s p a i n a n d i n c reased fun cti on wh i l e ta k ing these com pounds when c o m p a red with pati e nts on p l a c e bo, b ut ra d i o g ra p h i c evid e n c e from exam i n i n g kn ee j o i nt d e gene rati on w a s c omp l i c ated b y the fa ct that th e p l a c e bo g r o u p h a d a sma l l e r l o s s o f c a rti l a g e tha n h a d been a nti c i p ated on t h e b a s i s o f pr io r resea rch resu lts, so n o d ef in ite c o n c l us i ons c ou l d be rea ched .
t a b I e 4.1 C l a ssifi c at ion of G lycosam i nog lycans
Linked t o Core Group G lycosaminoglycans Protein Su lfated
Hya l u ron i c a c i d N o N o
I I Chond roitin su lfate Yes Yes
De rmatan su lfate Yes Yes
I l l H e pa ri n Yes Yes
Hepa ra n su lfate Yes Yes
IV Keratan su lfate Yes Yes
Major Locations in Body
Synovi a l f lu id, vitreous humo r, c a rti l a ge, sk in , most connective tissues
Cornea , c a rti l a ge, bone , adventitia of a rter ies
S kin , b lood vesse ls , h e a rt va lves
Lung, sk in , l iver, mast ce l l s
Basa l l am i nae , l u ng , a rteries, c e l l su rfa ces
Cornea , c a rti l age , nuc l eus p u l posus of inte rvertebra l d isks
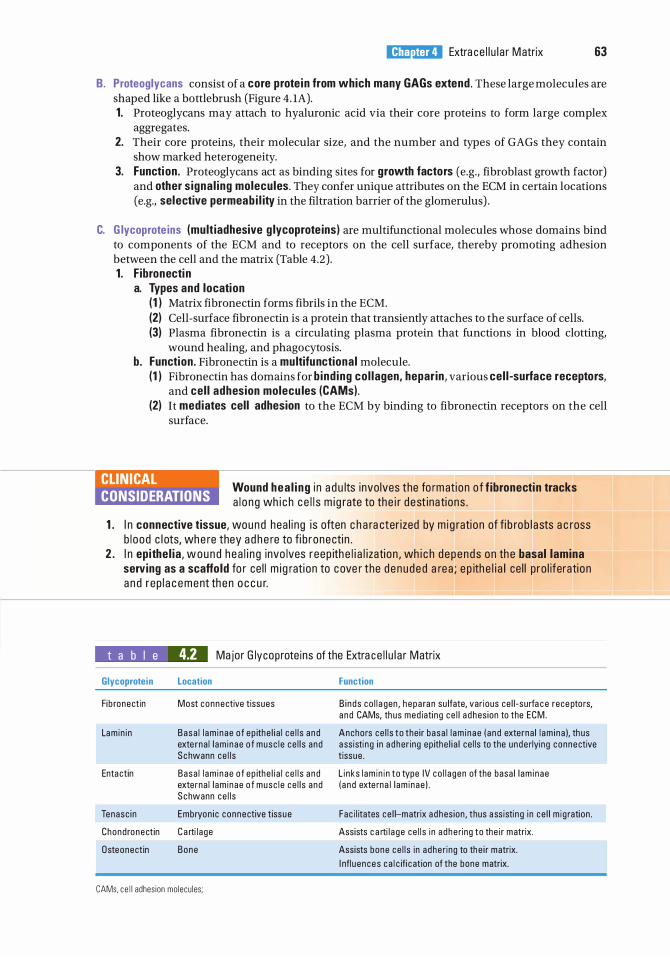
l!il!lJ'dQij Extra ce l l u l a r Matrix 63
B. Proteoglycans consist of a core prote in from which many GAGs extend . These large molecules are shaped like a bottlebrush (Figure 4. 1A). 1. Proteoglycans may attach to hyaluronic acid via their core proteins to form large complex
aggregates. 2. Their core proteins, their molecular size, and the number and types of GAGs they contain
show marked heterogeneity. 3. Function. Proteoglycans act as binding sites for growth factors (e.g., fibroblast growth factor)
and other s igna l ing molecules. They confer unique attributes on the ECM in certain locations (e.g., selective permeab i l ity in the filtration barrier of the glomerulus) .
C. G lycoprote ins (mult iadhesive g lycoprote ins) are multifunctional molecules whose domains bind to components of the ECM and to receptors on the cell surface, thereby promoting adhesion between the cell and the matrix (Table 4.2) . 1 . F ibronecti n
a. Types and location ( 1 ) Matrix fibronectin forms fibrils in the ECM. (2) Cell-surface fibronectin is a protein that transiently attaches to the surface of cells. (3) Plasma fibronectin is a circulating plasma protein that functions in blood clotting,
wound healing, and phagocytosis. b. Function . Fibronectin is a multifunctional molecule.
(1 ) Fibronectin has domains for b ind ing co l lagen, hepar in , various cel l -surface receptors, and cel l adhesion molecu les (CAMs).
(2) It mediates cell adhesion to the ECM by binding to fibronectin receptors on the cell surface.
CLINICAL CONSIDERATIONS
Wound hea l i ng i n a d u lts invo lves the fo rmati on o f f ibronecti n tracks a l o n g wh i c h c e l l s m i g rate to the i r d est inations .
1 . I n connective tissue, wound hea l i ng i s often c h a ra cter ized by m i g rati on of fi b rob l a sts a c ross b l ood c l ots, whe re they a d h e re to fi b ronecti n .
2 . I n epithe l ia , wound hea l i n g invo lves reep ith e l i a l i zati on , wh i c h d epends on th e basal lamina serving as a scaffold fo r ce l l m i g rati on to cove r the d e n uded a rea ; e p ith e l i a l ce l l p ro l iferati on a n d rep l a c e ment th en o c c u r.
t a b I e 4.2 Major G lycoprote ins of the Extra ce l l u l a r Matrix
Glycoprotein
Fib ronectin
Lam in i n
Enta ctin
Tenasc i n
Chondronectin
Osteonectin
Location
Most connective tissues
Basa l l am i nae of ep ithe l i a l c e l l s a nd exte rna l l am inae o f musc l e ce l l s and Schwann ce l l s
Basa l l am i nae o f ep ithe l i a l c e l l s a nd externa l l am inae o f musc l e ce l l s and Schwann ce l l s
Embryon i c connective tissue
C a rti l a ge
Bone
CAMs. c e l l adhes ion mo lecu les;
Function
B i nds co l l a gen , h epa ra n su lfate, var ious ce l l - su rfa c e rece ptors, a nd CAMs, th us med iati ng ce l l a d hes ion to the ECM.
Anchors ce l l s to the i r basa l l am i nae ( a nd externa l l am i na ), th us a ss isti ng i n a d her ing ep ithe l i a l ce l l s to the unde rlyi ng connective tissue .
L i nks l am i n i n to type IV co l l a gen of the basa l l am i nae ( a nd exte rna l l am i nae ) .
Fac i l itates ce l l-matrix a dhes ion , thus a ss isti n g i n ce l l m i g ration .
Assists c a rti l a ge ce l l s i n a dhe ring to the i r matrix.
Assists bone ce l l s in a dhe ring to th e i r matrix.
I nfl u ences c a l c ifi c at ion of the bone matrix.
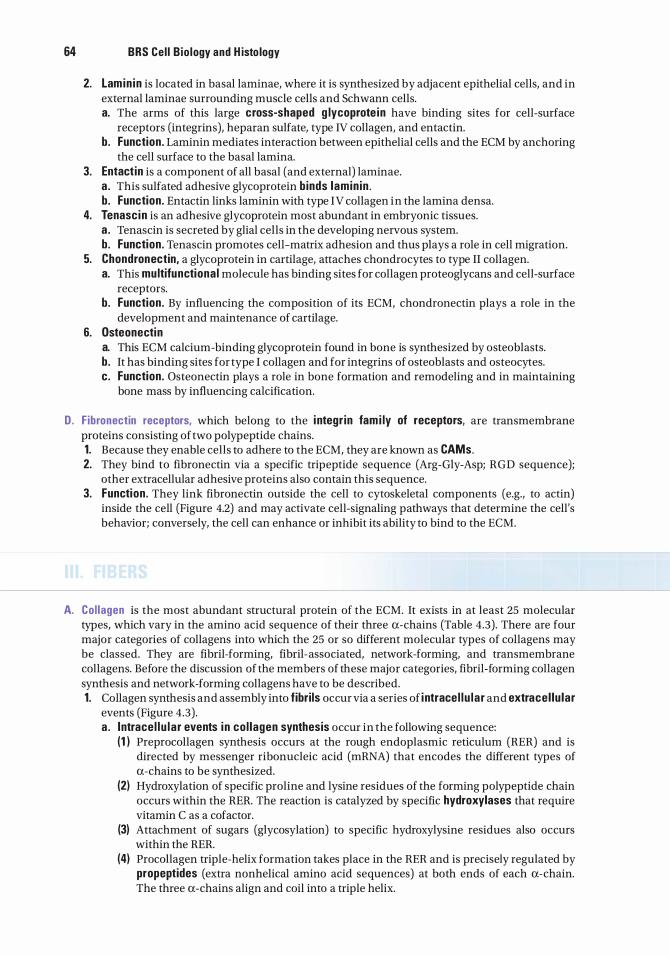
64 BRS Cel l B io logy and H isto logy
2. Lamin in is located in basal laminae, where it is synthesized by adjacent epithelial cells, and in external laminae surrounding muscle cells and Schwann cells. a. The arms of this large cross-shaped g lycoprote in have binding sites for cell-surface
receptors (integrins), heparan sulfate, type IV collagen, and entactin. b. Function . Laminin mediates interaction between epithelial cells and the ECM by anchoring
the cell surface to the basal lamina. 3. Entact in is a component of all basal (and external) laminae.
a . This sulfated adhesive glycoprotein binds lamin in . b . Function . Entactin links laminin with type IV collagen in the lamina densa.
4. Tenasc in is an adhesive glycoprotein most abundant in embryonic tissues. a . Tenascin is secreted by glial cells in the developing nervous system. b. Function . Tenascin promotes cell-matrix adhesion and thus plays a role in cell migration.
5. Chondronectin, a glycoprotein in cartilage, attaches chondrocytes to type II collagen. a. This multifunctiona l molecule has binding sites for collagen proteoglycans and cell-surface
receptors. b. Function . By influencing the composition of its ECM, chondronectin plays a role in the
development and maintenance of cartilage. 6. Osteonectin
a. This ECM calcium-binding glycoprotein found in bone is synthesized by osteoblasts. b. It has binding sites for type I collagen and for integrins of osteoblasts and osteocytes. c. Function . Osteonectin plays a role in bone formation and remodeling and in maintaining
bone mass by influencing calcification.
D. F ibronectin receptors, which belong to the i ntegr in fam i ly of receptors, are transmembrane proteins consisting of two polypeptide chains. 1. Because they enable cells to adhere to the ECM, they are known as CAMs. 2. They bind to fibronectin via a specific tripeptide sequence (Arg-Gly-Asp; RGD sequence);
other extracellular adhesive proteins also contain this sequence. 3. Function . They link fibronectin outside the cell to cytoskeletal components (e.g., to actin)
inside the cell (Figure 4.2) and may activate cell-signaling pathways that determine the cell's behavior; conversely, the cell can enhance or inhibit its ability to bind to the ECM.
A. Col lagen is the most abundant structural protein of the ECM. It exists in at least 25 molecular types, which vary in the amino acid sequence of their three a-chains (Table 4.3). There are four major categories of collagens into which the 25 or so different molecular types of collagens may be classed. They are fibril-forming, fibril-associated, network-forming, and transmembrane collagens. Before the discussion of the members of these major categories, fibril-forming collagen synthesis and network-forming collagens have to be described. 1. Collagen synthesis and assembly into fibri ls occur via a series of i ntrace l l u la r and extracel lu lar
events (Figure 4.3) . a . Intrace l l u la r events i n co l lagen synthesis occur in the following sequence:
(1 ) Preprocollagen synthesis occurs at the rough endoplasmic reticulum (RER) and is directed by messenger ribonucleic acid (mRNA) that encodes the different types of a-chains to be synthesized.
(2) Hydroxylation of specific proline and lysine residues of the forming polypeptide chain occurs within the RER. The reaction is catalyzed by specific hydroxylases that require vitamin C as a cofactor.
(3) Attachment of sugars (glycosylation) to specific hydroxylysine residues also occurs within the RER.
(4) Procollagen triple-helix formation takes place in the RER and is precisely regulated by propeptides (extra nonhelical amino acid sequences) at both ends of each a-chain. The three a-chains align and coil into a triple helix.
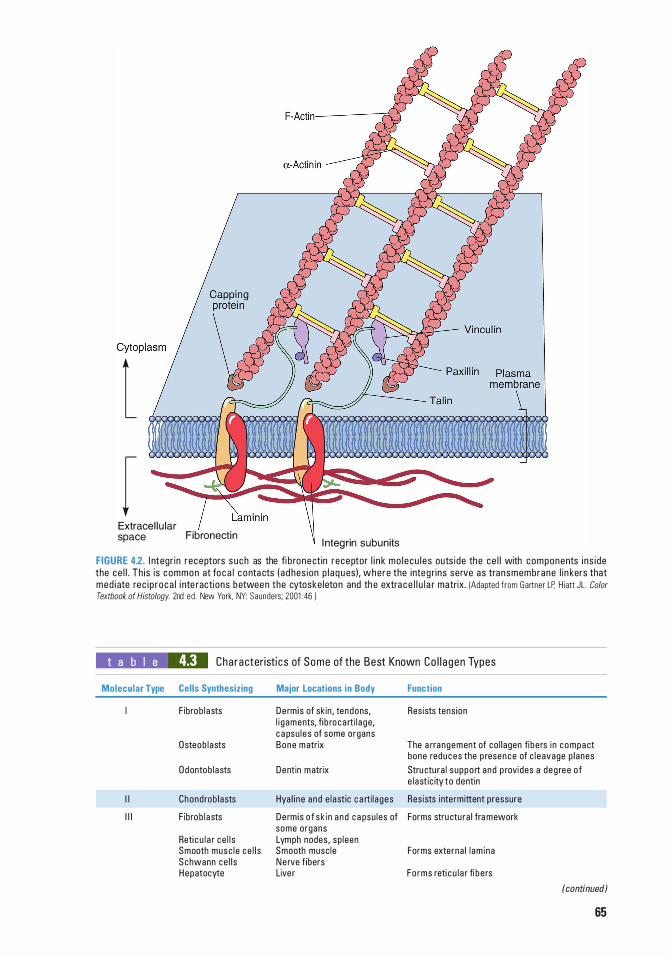
l r
Extracel lu lar space Fibronectin l nteg rin subunits
FIGURE 4.2. l ntegr in r eceptors s uch as the fi b ronect in r eceptor l i n k mo l ecu l e s outs ide the ce l l with components i ns i de the ce l l . Th is is common at foc a l c o nta cts ( ad hes ion p l a q u es) , where the i nteg rins serve as transmembrane l i n kers that med i ate rec i p r oca l i nte ractions b etwee n the cytoske leton and th e extra c e l l u l a r matr ix. IAdapted f rom Gartner LP, H iatt JL . Color
Textbook of Histology. 2nd ed . New York, NY: Saunders; 2001 :46 )
t a b I e 4.3 Cha racter isti cs of Some of the Best Known Co l l a gen Types
Molecular Type Cel ls Synthesizing
F ibrob l asts
Dsteob l asts
D dontob l asts
I I Chond rob lasts
I l l F ibrob l asts
Reti c u l a r c e l l s Smooth musc l e ce l l s S chwann ce l l s Hepatocyte
Major Locations in Body
De rm is of sk in , tendons, l i g aments, fi b ro ca rti l a ge, c a psu l es of some organs Bone m atrix
Dentin m atrix
Hya l i ne a nd e l a st ic c a rti l a ges
De rm is o f sk i n a nd c a psu les of some organs Lymph nodes , sp leen Smooth musc le Ne rve f ibers Live r
Function
Resists tens ion
The a rra ngement of co l l agen fi be rs i n compact bone reduces the p resence of c l e avage p l anes
Stru ctu ra l s uppo rt and p rovides a deg ree of e l astic ity to dentin
Res ists i nte rmittent pressure
Forms stru ctu ra l fra mework
Forms externa l l am i na
Fo rms reti c u l a r fi be rs
(continued)
65
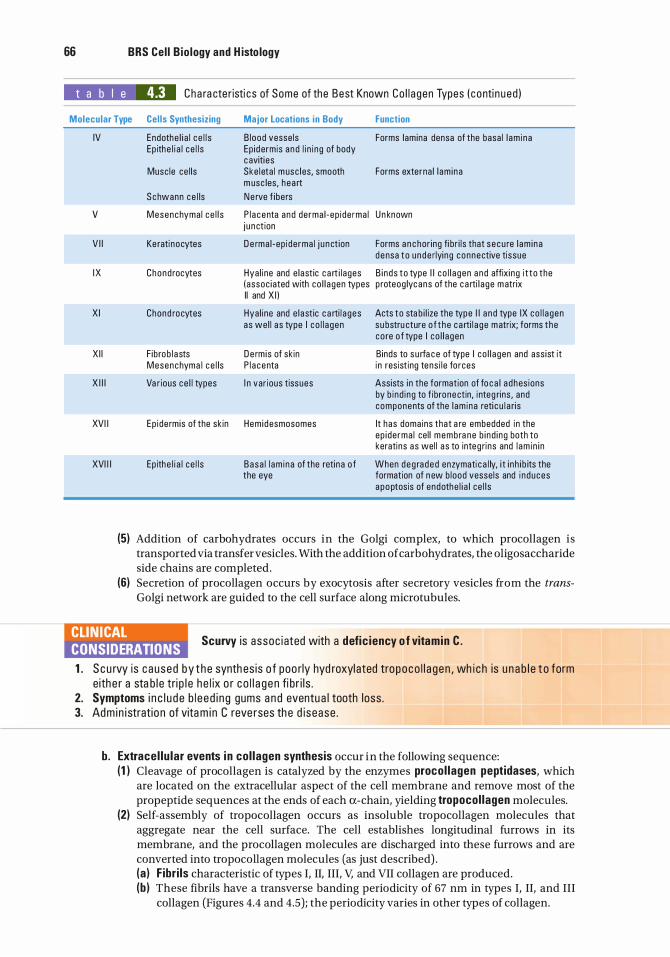
66 BRS Cel l B io logy and H isto logy
t a b I e 4.3 Cha ra cte r isti cs of Some of the Best Known Co l l a gen Types ( c onti n ued )
Molecular Type Cel ls Synthesizing Major Locations in Body Function
IV
v
V I I
I X
X I
X I I
X I I I
XVI I
XVI I I
Endothe l i a l c e l l s B lood vesse ls Forms lamina densa of the basa l l am i na Ep ithe l i a l ce l l s Ep id ermis a nd l i n i ng of body
c aviti es Musc le ce l l s Ske leta l m usc l es, smooth Forms externa l l am i na
m usc les, hea rt
Schwann ce l ls Ne rve f ibers
Mesenchyma l ce l l s P l a centa and derma l -ep i de rma l Un known j u nct ion
Ke rati nocytes D e rma l -ep i de rma l j u n ct ion Forms a n c hor ing fi br i l s that s e cu re l am i na d en sa to u nde rlyi ng connective ti ssue
Chond rocytes Hya l ine and e lastic c a rt i l ages B i nds to type I I co l l a gen a nd affixi ng i t to the (assoc iated with co l l agen types p roteog lyc ans of the c a rti l a ge m atrix II and X I )
Chond rocytes Hya l ine and e l astic c a rti l a ges Acts to sta b i l ize the type I I a n d type IX co l l a gen as we l l a s type I co l l a gen su bstru cture o f t he c a rti l a ge m atrix; forms the
co re o f type I co l l a gen
F ibrob l a sts De rm is of sk in B inds to s u rfa c e of type I co l l a gen and ass ist it Mesenchyma l c e l ls P l a centa i n resist ing te ns i l e fo rces
Va r ious ce l l types I n var ious tissues Assists i n the formation of fo c a l a d hes ions by b i nd i ng to f ibronectin, i nteg rins , and components of the l am ina reti c u l a ris
Ep i de rmis of the sk in Hem idesmosomes It has doma ins that a re embedded i n the ep i de rma l ce l l membra ne b i nd i ng both to keratins as wel l a s to integ rins and l am i n i n
Ep ithe l i a l ce l l s Basa l l am i na of the reti na o f When d eg raded enzymati c a l ly, i t i n h i b its the the eye formation of n ew b lood vesse ls and i n duces
a poptosis of endothe l i a l ce l l s
(5) Addition of carbohydrates occurs in the Golgi complex, to which procollagen is transported via transfer vesicles. With the addition of carbohydrates, the oligosaccharide side chains are completed.
(6) Secretion of procollagen occurs by exocytosis after secretory vesicles from the transGolgi network are guided to the cell surface along microtubules.
CLIN ICAL CONSIDERATIONS
Scurvy i s assoc i ated with a defic iency o f vitamin C .
1 . S c u rvy is c aused by t he synth es is o f poo rly hyd roxyl ated tropoco l l a gen , wh i c h is u n a b l e t o form eith e r a sta b l e tri p l e h e l ix o r c o l l a g e n fi b r i l s .
2. Symptoms i n c l u d e b l e ed i n g gums a n d eventu a l tooth loss . 3. Adm in i stratio n of vita m i n C reve rses th e d isease .
b. Extracel lu lar events i n col lagen synthesis occur in the following sequence: (1 ) Cleavage of pro collagen is catalyzed by the enzymes procol lagen peptidases, which
are located on the extracellular aspect of the cell membrane and remove most of the propeptide sequences at the ends of each a-chain, yielding tropocol lagen molecules.
(2) Self-assembly of tropocollagen occurs as insoluble tropocollagen molecules that aggregate near the cell surface. The cell establishes longitudinal furrows in its membrane, and the procollagen molecules are discharged into these furrows and are converted into tropocollagen molecules (as just described) . (a ) F ibr i ls characteristic of types I, II, III, V, and VII collagen are produced. (b ) These fibrils have a transverse banding periodicity of 67 nm in types I, II, and III
collagen (Figures 4.4 and 4.5); the periodicity varies in other types of collagen.
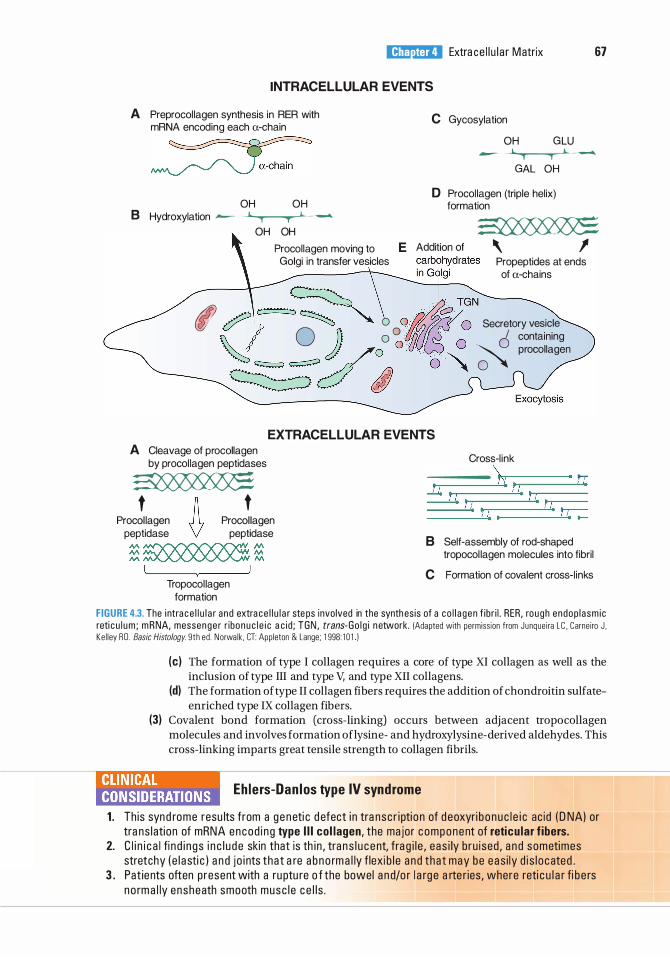
l!il!lJ'dQij Extra ce l l u l a r Matrix 67
INTRACELLULAR EVENTS
A Preprocol lagen synthesis in RER with mRNA encoding each a-chain
� OH OH
8 Hydroxylation �
OH OH
Procollagen moving to Golgi in transfer vesicles
C Gycosylation
OH GLU
� GAL OH
D Procol lagen (triple helix) formation �
E A�moo � \ 1 Propeptides at ends of a-chains
rl ��=� 0 o/..1�>·.2?· T�N Secretory vesicle
� A 0 ) o 0 l/ff/r . · · I containing �d/�ou' o � � ,_,,,'"
EXTRACELLULAR EVENTS A Cleavage of procollagen
by procol lagen peptidases � Proc!lagen A Proc!agen
peptidase V peptidase
� � � N\ � M
Tropocol lagen formation
Cross-l ink ----- ..,,....------- 1-r
8 Self-assembly of rod-shaped tropocol lagen molecules into fibril
C Formation of covalent cross-l inks
FIGURE 4.3. The i ntra c e l l u l a r a nd extra ce l l u l a r ste ps invo lved in the synth es is of a co l l a gen f ib r i l . RER, rough endop l asm i c reti c u l um ; m RNA, messenge r r ibo n u c l e i c a c i d ; TGN , trans-Go l g i n etwork. !Adapted with permiss ion from Junque i ra L C . Carneiro J , Ke l l ey RD . Basic Histology. 9th ed. Norwa lk . CT: Appleton & Lange; 1 998: 1 0 1 1
(c) The formation of type I collagen requires a core of type XI collagen as well as the inclusion of type III and type V, and type XII collagens.
(d) The formation of type II collagen fibers requires the addition of chondroitin sulfateenriched type IX collagen fibers.
(3) Covalent bond formation (cross-linking) occurs between adjacent tropocollagen molecules and involves formation oflysine- and hydroxylysine-derived aldehydes. This cross-linking imparts great tensile strength to collagen fibrils.
liHnla!B Eh lers-Dan los type IV syndrome
1 . This synd rome resu lts from a g e neti c d efect i n tra nsc r i pti o n of d eoxyri b o n u c l e i c ac id ( D NA) or tra ns l ation of mRNA encod i n g type I l l col lagen, the major c omponent of reticu lar f ibers.
2. C l i n i c a l fi n d i n g s i n c l u d e skin that is th i n , tra n s l u c ent, fra g i l e , eas i ly b ru i sed , a n d sometimes stretchy ( e l a sti c ) a n d j o i nts that a re a b no rm a l ly f lexi b l e a n d that may be e a s i ly d i s l o cated .
3 . Pat ients often p resent with a ru ptu re o f the bowel a n d/o r l a rg e a rte r ies, where reti c u l a r fi b e rs no rm a l ly ensheath smooth musc l e c e l l s .
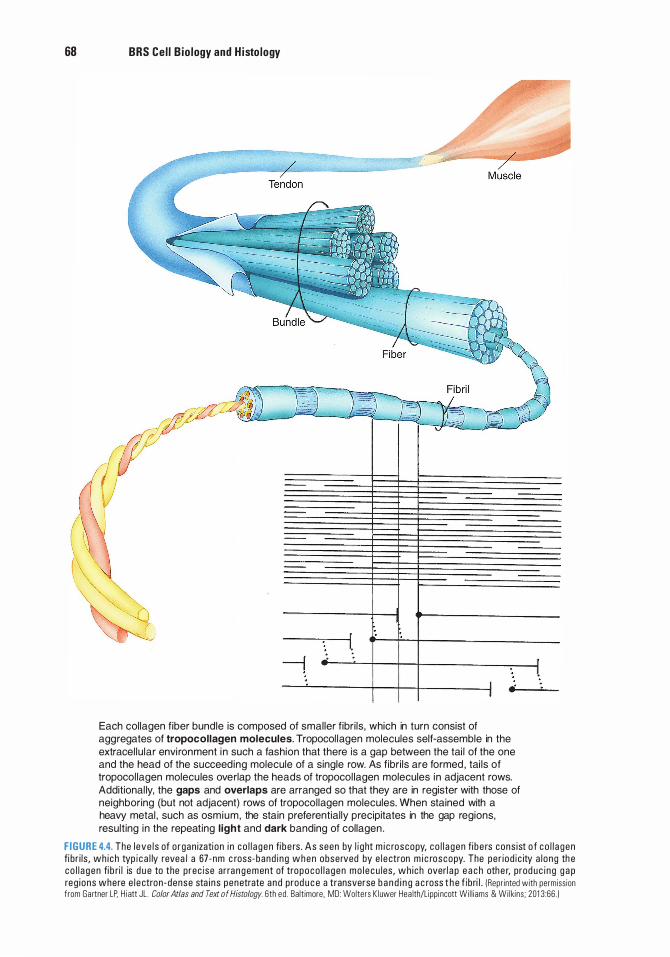
68 BRS Ce l l B io logy and H isto logy
Each collagen f iber bundle is composed of smal ler f ibr i ls , which in turn consist of aggregates of tropocollagen molecules. Tropocol lagen molecules self-assemble in the extracel lu lar envi ronment i n such a fashion that there is a gap between the tai l of the one and the head of the succeeding molecule of a single row. As f ibr i ls are formed , tai ls of tropocol lagen molecu les overlap the heads of tropocol lagen molecules in adjacent rows. Additional ly, the gaps and overlaps are arranged so that they are in register with those of neighboring (but not adjacent) rows of tropocol lagen molecules. When stained with a heavy metal , such as osmium, the stain preferential ly precipitates in the gap regions, result ing in the repeating l ight and dark banding of collagen .
F I G U R E 4.4. The l eve l s of o rgan izati on i n c o l l a gen fi b e rs . As seen by l i g ht m i c roscopy, c o l l a gen fi b e rs cons ist o f c o l l a gen fi br i l s , wh i ch typ i c a l ly revea l a 67-nm c ross-band i ng when observed by e l e ctron m i c roscopy. The pe r i od i c ity a l ong th e co l l a gen fi b ri l is d u e to the p rec ise ar ra n g e ment of tropoco l l a gen mo l e cu les , wh ich overl a p e a c h othe r, prod uc i n g g a p reg i ons where e l e ctron -dense sta i n s penetrate and prod u c e a transverse b a n d i n g a c ross t h e f ib ri l . (Repr inted with permiss ion from Gartner LP. H i att JL . Color Atlas and Text of Histology. 6th ed . Ba lt imore. MD: Wolters K luwer Hea lth/Lippi ncott Wi l l iams & Wi lkins ; 201 3 :66 . )
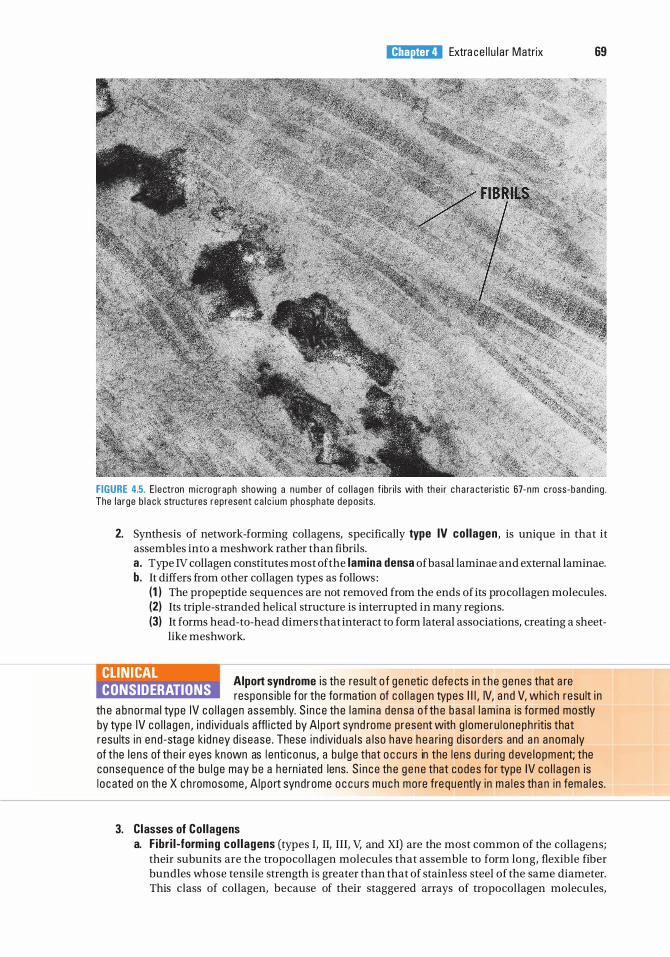
l!il!lJ'dQij Extra ce l l u l a r Matrix 69
FIGURE 4.5. E l ectron m i c rog raph showing a n umbe r of co l l a gen f ibr i l s with th e i r c h a ra cteristi c 67- nm c ross- band i n g . The l a rge b l a c k stru ctu res represent c a l c i um phosphate deposits.
2. Synthesis of network-forming collagens, specifically type IV col lagen, is unique in that it assembles into a meshwork rather than fibrils. a. Type IV collagen constitutes most of the lamina densa of basal laminae and external laminae. b. It differs from other collagen types as follows :
(1 ) The propeptide sequences are not removed from the ends of its pro collagen molecules. (2) Its triple-stranded helical structure is interrupted in many regions. (3) It forms head-to-head dimers that interact to form lateral associations, creating a sheet
like meshwork.
CLIN ICAL CONSIDERATIONS
Alport syndrome i s the resu lt o f geneti c d efe cts i n t he genes that a re respons ib l e for the fo rmation of co l l a gen types I l l , IV, a nd V, whi c h resu lt i n
th e a bnorma l type IV co l l a gen assem b ly. S i n ce th e l am i na den sa o f th e basa l l am i na is fo rmed mostly by type IV co l l a gen , i nd ivi d ua l s affl i cted by AI po rt synd rome present with g l omeru l oneph ritis that resu lts in end -sta ge kid ney d isease . These i nd ivid ua l s a lso have h ea ri ng d i sorders and an anoma ly of the l ens of the i r eyes known as l enti conus, a bu l ge that o c c u rs in the l ens d u ri ng d eve l opment; the consequence of the bu l g e may be a h e rn i ated lens. S i n ce th e gene that codes fo r type IV co l l a gen is l o cated on th e X c h romosome, A I po rt syndrome o c c u rs m u c h more frequently i n ma l es tha n in fema l es.
3. Classes of Col lagens a. F ibr i l -form ing co l lagens (types I, II, III, V, and XI) are the most common of the collagens;
their subunits are the tropocollagen molecules that assemble to form long, flexible fiber bundles whose tensile strength is greater than that of stainless steel of the same diameter. This class of collagen, because of their staggered arrays of tropocollagen molecules,
70 BRS Ce l l Bio logy and H isto logy
display a 67-nm cross-band ing . Each tropocollagen molecule, as mentioned above, is composed of three a-chains wrapped around each other, where each a-chain is about 1 ,000 amino acids long. Because every third amino acid in each a-chain is a g lycine, the smallest of the amino acids, the three chains can form a very tight helix by bending around these amino acids. Moreover, hydroxypro l i ne and hydroxylys ine molecules also abound in all three a-chains; the hydroxyprolines of each a-chain form tight bonds with each other, assisting in the maintenance of the tight helix. The hydroxylysines bind to each other across neighboring tropocollagen molecules, thus assisting in the formation of collagen fiber bundles.
b. F ib r i l -assoc iated co l l agens (types IX and XII) are bound to the surfaces of fibrilforming collagens and thereby they stabilize the collagen framework of the tissues in which they reside by adhering not only to the collagen fibers but also to the molecules of the ground substance. Type IX co l l agens are associated with type II collagens of cartilage, and type XII co l l agens are localized on the surface of type I collagens of the dermis and placenta.
c. Network-fo rm i ng co l l agens (types IV and VII) , unlike the other types of collagen, have procollagen as their subunits. As described above, procollagen possesses the pro peptide sequences at both ends of the molecule, which, in fibril -forming collagens, are removed by procollagen peptidase in the extracellular environment. Procollagen molecules are unable to assemble in the style of tropocollagen molecules; hence, they do not form fibers. Instead, the pro collagen molecules form head-to-head dimers that interact forming lateral associations, creating a sheet- l i ke meshwork. Type IV co l l agen forms the lamina densa of the basal lamina, and type V I I collagens form the anchoring fibrils that secure the lamina densa to the lamina reticularis of the underlying connective tissue.
d . Transmembrane co l lagens (types XIII, XVII, and XVIII) are associated with focal adhesions, hemidesmosomes, and the basal laminae, respectively.
CLINICAL CONSIDERATIONS
Knobloch syndrome (type I ) i s a n i n h e rited d i sease resu lti n g from the m a lfo rmati on o f type XVI I I c o l l a gen . The sym ptoms i n c l u de e n cepha l o
ce l e , the fo rmati on o f l a rg e b ra i n ves i c l e s that j u t o ut th rou g h a d efect o f t h e bony s ku l l d u e t o i n comp l ete fus ion o f t he n e u ra l tu be d u ri n g e m b ryon i c d eve l o pment, a s we l l as spo ra d i c d eta c h m e nt o f th e reti na , a n d n e a rs i g hted n ess that may become evi d ent by the tim e the ch i l d is a yea r o l d .
B. E lastic f ibers 1 . Components
a. E lastin, an amorphous structural protein, imparts remarkable elasticity to the ECM; 90% of elastic fibers or elastic sheets are composed of elastin. (1 ) Elastin is unusual in that its lysine molecules form unique linkages with one another. (2) Lysine residues of four different chains form covalent bonds called desmosine cross-
l i nks to create an extensive elastic network. (3) Like a rubber band, after being stretched, the elastin returns to its original shape once
the tensile force is released. b. F ibri l l i n-1 , a glycoprotein, organizes elastin into fibers and is the main component of the
peripheral microfi br i ls of elastic fibers. (1 ) The amino terminus of one fibrillin -1 interacts with the carboxyl terminus of another
fibrilin- 1 molecule to form pencil-like head-to-tail assembly of fibrilin- 1 molecules to form microfibrils.
(2) Fibrillin- 1 possesses binding sites for tropoelastin, which form cross-links with each other. (3) Heparin competes with tropoelastin for binding sites on fibrillin- 1 , which probably has
a regulatory effect on elastic fiber formation.
l!il!lJ'dQij Extra ce l l u l a r Matrix 71
c. Fibul in-5, a protein, forms bonds with integrin molecules of cells such as vascular smooth muscle cells and endothelial cells of blood vessels, and also facilitates the formation of elastic fibers. (1 ) Fibulin-5 also binds to microfibrils and tropoelastin. (2) It has been shown that during wound healing fibulin-5 is present in an increased
concentration than in undamaged blood vessels. d . Type V I I I co l l agen is often associated with elastic fibers, most probably to limit the
extent of elastic fiber stretching, protecting the elastic fibers from being damaged by overstretching.
2. Synthesis of e lastic f ibers is carried out by f ibroblasts in elastic ligaments, smooth muscle ce l ls in large arteries, and chondrocytes and chondroblasts in elastic cartilage. a. Synthesis begins with the elaboration off ibri l l i n microfi bri l templates that are arranged in
a parallel array near regions of the cell surface. b. These cells manufacture and exocytose a soluble form of elastin, known as tropoelastin,
and fibulin-5 which bind not only to each other but also to fibrillin- 1 . c. Tropoelastin molecules cross-link with each other t o form insoluble, mature elastin. d. Additional factors, such as heparan sulfate, microfibril-associated glycoproteins, and
fibrillin-2, have been implicated in the assembly of elastic fibers.
CLIN ICAL CONSIDERATIONS
Marfan syndrome resu lts from m utati ons i n the genes e n cod i n g f ibri l l in , a c riti c a l c omponent of e l a sti c fi b e rs .
1 . Pat ients with th is c ond itio n h ave u nusua l ly long , s l e nde r l imbs and long fi n g e rs . 2. The l e ns of th e eye ofte n d i s l o cates; c a rd iova s c u l a r p rob l ems a re common ; a n d th e a o rta may
ru ptu re, c a us i ng d e ath . 3. Treatme nt i n c l u d es drugs that d e c rease b lood p ressu re, and i n severe cases su rge ry re p l a c i n g
t h e a o rta .
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which one of the following statements about the fibronectin receptor is true?
(A) It is located exclusively in the basal lamina.
(B ) It is a cross-shaped glycoprotein. (C) It mediates the linkage of molecules out
side the cell with cytoskeletal elements inside the cell.
(D ) It belongs to the entactin family of receptors.
(E) Its absence is associated with scurvy.
2. Which one of the following events in collagen synthesis occurs outside of the cell?
(A) Synthesis of preprocollagen (B ) Hydroxylation of lysine residues (C) Triple-helix formation (D ) Carbohydrate addition to procollagen (E) Cleavage of pro collagen by procollagen
peptidases
3. A medical student goes to the emergency department and is diagnosed with a ruptured bowel, the result of a genetic condition called Ehlers-Danlos type IV syndrome. Which one of the following statements about this patient's condition is true?
(A) He has a defect in the synthesis of mRNA encoding type I collagen.
(B ) He has a defect in the genes encoding type IV collagen.
(C) He has defective type II collagen. (D ) He has an increased risk of breaking his
bones. (E ) He has a defect in the translation of mRNA
for type III collagen.
72
4. Which one of the following statements about hyaluronic acid is true?
(A) It is a component of elastic fibers. (B) It is a glycosaminoglycan. (C ) It is a proteoglycan with a shape resem
bling a bottlebrush. (D ) It is sulfated. (E) It is a small molecule.
5. Which one of the following statements about osteonectin is true?
(A) It is present in the lacunae of bone. (B) It is a proteoglycan. (C ) It binds to type II collagen. (D ) It influences calcification of bone. (E) It is synthesized by osteoclasts.
6. Which of the following statements about scurvy is true?
(A) One of its symptoms is bowlegs. (B ) It is caused by excessive glycosylation of
tropocollagen. (C) It is caused by a deficiency of vitamin A. (D) It is associated with structurally defective
elastic fibers. (E) It is alleviated by eating citrus fruits.
7. Which one of the following is a glycoprotein across which fibroblasts migrate during wound healing?
(A) Fibrillin (B ) Fibronectin (C ) Elastin (D ) Entactin (E ) Laminin
8. Which of the following is an adhesive glycoprotein that links type IV collagen with laminin in the lamina densa?
(A) Fibrillin (B ) Fibronectin (C ) Elastin (D ) Entactin (E ) Tenascin
9. Which one of the following is a main component of peripheral microfibrils in an elastic fiber?
(A) Fibrillin (B ) Fibronectin (C ) Elastin (D ) Entactin (E ) Laminin
l!i1fftlllil Extra ce l l u l a r Matrix 73
1 0. Which one of the following is present in the basement membrane and is manufactured by connective tissue cells?
(A) Fibrillin (B ) Fibronectin (C) Elastin (D ) Entactin (E ) Laminin
Answers and Explanations
1 . C. The fibronectin receptor is a transmembrane protein that enables cells to adhere to the ECM. Laminin is a cross-shaped glycoprotein in the basal lamina, where entactin is also present (see Chapter 4 II D) .
2. E. In the extracellular space, peptidases cleave off end sequences of pro collagen to yield tropocollagen, which self-assembles to form collagen fibrils (see Chapter 4 III A 1 ) .
3. E . Ehlers-Danlos type IV syndrome is associated with a defect in the synthesis and translation of mRNA for type III reticular collagen (see Chapter 4 III A 1 Clinical Considerations).
4. B . Hyaluronic acid is a glycosaminoglycan, not a pro teo glycan. The core protein of proteoglycans can attach to hyaluronic acid forming large aggregates (see Chapter 4 II A).
5. D . Osteonectin synthesized by osteoblasts influences the calcification of bone and binds to type I collagen in the bone matrix. Type II collagen is found in cartilage (see Chapter 4 II C) .
6. E . Scurvy is caused by a deficiency of vitamin C, a necessary cofactor in the hydroxylation of preprocollagen. Citrus fruits are rich in vitamin C (see Chapter 4 III A 1 Clinical Considerations).
7. B . Fibronectin forms tracks along which cells migrate. During wound healing in connective tissue, fibroblasts adhere to fibronectin in blood clots, facilitating the healing process (see Chapter 4 II C 1 Clinical Considerations) .
8. D. Entactin is a sulfated adhesive glycoprotein in basal and external laminae that binds both type IV collagen and laminin (see Chapter 4 II C) .
9. A. Fibrillin is the major component of the peripheral micro fibrils of elastic fibers (see Chapter 4 III B) .
1 0. B . Fibronectin is synthesized by cells of the connective tissue, usually fibroblasts, and is located in the lamina reticularis near the lamina densa (see Chapter 4 II C 1 ) .
74
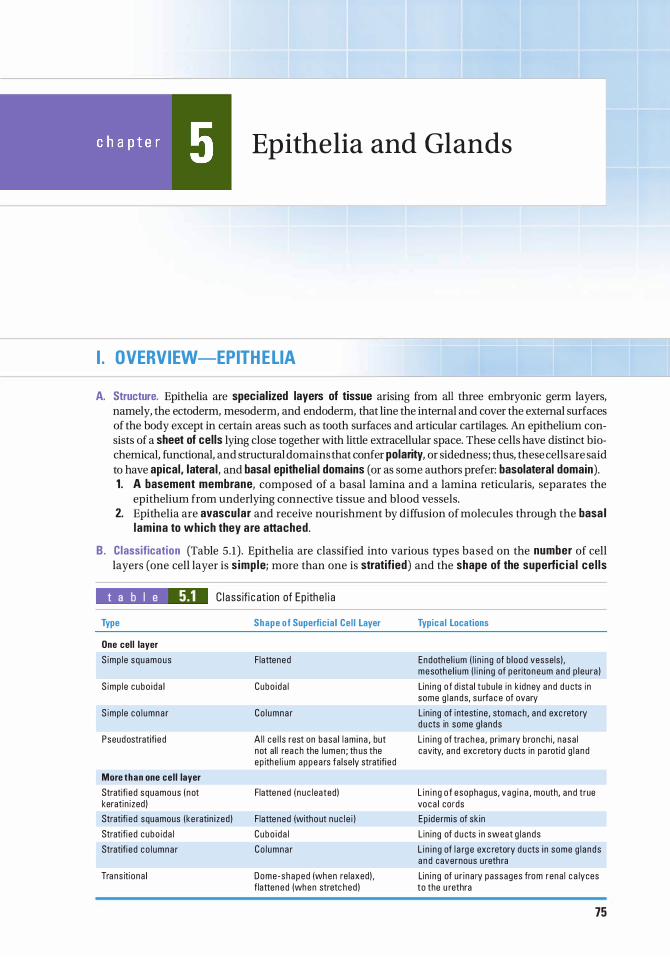
Epithelia and Glands
I. OVERVIEW-EPITHELIA
A. Structure. Epithelia are special ized layers of tissue arising from all three embryonic germ layers, namely, the ectoderm, mesoderm, and endoderm, that line the internal and cover the external surfaces of the body except in certain areas such as tooth surfaces and articular cartilages. An epithelium consists of a sheet of cells lying close together with little extracellular space. These cells have distinct biochemical, functional, and structural domains that confer polarity, or sidedness; thus, these cells are said to have apical, lateral, and basal epithel ia l domains (or as some authors prefer: basolateral domain). 1 . A basement membrane, composed of a basal lamina and a lamina reticularis, separates the
epithelium from underlying connective tissue and blood vessels. 2. Epithelia are avascular and receive nourishment by diffusion of molecules through the basa l
lamina to which they are attached.
B . Classification (Table 5 .1) . Epithelia are classified into various types based on the number of cell layers (one cell layer is s imple; more than one is stratified) and the shape of the superfic ia l ce l ls
t a b I e 5.1 C l a ss ifi c at ion of Ep ithe l i a
Type
One cell layer
S imp l e squamous
S imp l e cubo i da l
S imp l e co l umna r
Pseudostratifi e d
More than one cel l layer
Stratifi e d squamous ( not keratin i zed !
Stratifi e d squamous (ke ratin i zed )
Stratifi e d cubo i da l
Stratifi e d co l umna r
Tra ns iti ona l
Shape of Superfic ia l Cel l Layer
Flattened
Cubo i da l
Co l umna r
A l l c e l l s rest on basa l l am i na , but not al l rea c h the l umen ; th us the ep ithe l i um appea rs fa lse ly stratifi e d
Flatte ned ( n u c leated)
Flatte ned (without n uc l e i )
C ubo i d a l
Co l umna r
Dome-shaped (when re laxed) . f lattened (when stretc hed )
Typical Locations
Endothe l i um ( l i n i ng of b lood vesse ls ) . mesothe l i um ( l i n i ng of peritoneum and p l eu ra )
Lin i ng o f d i sta l tubu le i n k idney a nd d u cts i n some g l a nds, s u rfa c e of ovary
L in ing of i ntesti ne , stomach, a nd exc reto ry d u cts in some g l ands
L i n i ng of tra c h ea , pr ima ry b ronch i, nasa l cavity, and exc retory d u cts in pa roti d g l a nd
L i n i n g o f esophagus, v ag i n a , mouth, a nd true voca l cords
Ep i de rmis of sk in
L in ing of d u cts in sweat g l a nds
L i n i n g of l a rg e exc retory d u cts i n some g l a nds a n d cavernous u reth ra
Lin i ng of u r i na ry passages from rena l c a lyces to the u rethra
75
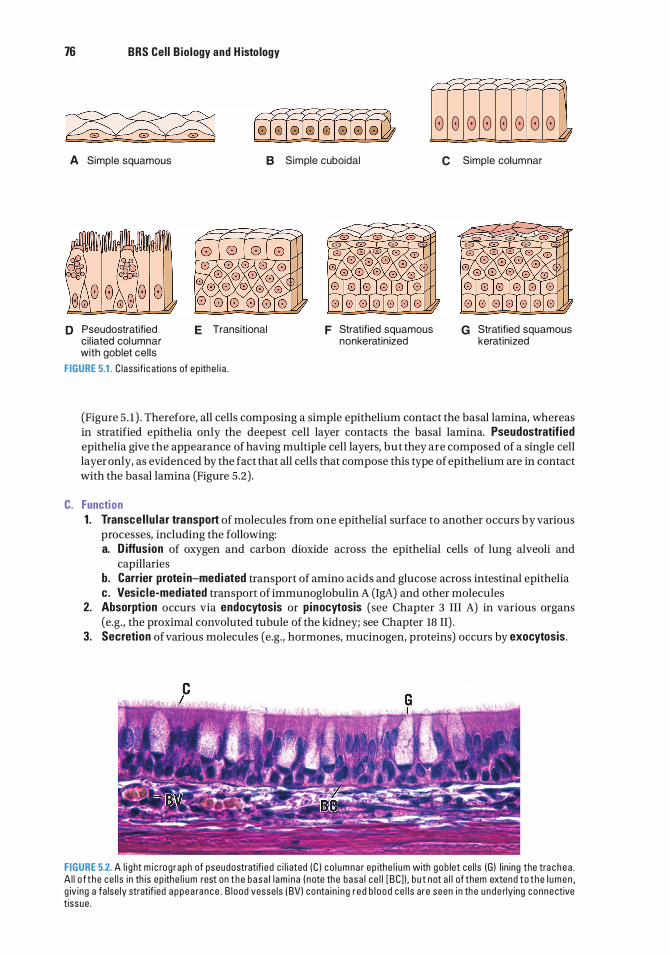
76 BRS Cel l Bio logy and H isto logy
A Simple squamous B Simple cuboidal
D Pseudostratified ci l iated columnar with goblet cel ls
E Transitional
FIGURE 5.1 . C l a ssif i c ations of e p ith e l i a .
F Stratified squamous nonkeratin ized
8 8 8 8 8 8 8 8 ? C Simple columnar
G Stratified squamous kerat in ized
(Figure 5 . 1 ) . Therefore, all cells composing a simple epithelium contact the basal lamina, whereas in stratified epithelia only the deepest cell layer contacts the basal lamina. Pseudostratif ied epithelia give the appearance of having multiple cell layers, but they are composed of a single cell layer only, as evidenced by the fact that all cells that compose this type of epithelium are in contact with the basal lamina (Figure 5.2) .
C. Function 1 . Transce l lu lar transport of molecules from one epithelial surface to another occurs by various
processes, including the following: a. D iffusion of oxygen and carbon dioxide across the epithelial cells of lung alveoli and
capillaries b. Carrier prote in-med iated transport of amino acids and glucose across intestinal epithelia c. Vesic le-med iated transport of immunoglobulin A (IgA) and other molecules
2. Absorption occurs via endocytosis or p inocytosis (see Chapter 3 III A) in various organs (e.g., the proximal convoluted tubule of the kidney; see Chapter 18 II) .
3. Secretion of various molecules (e.g., hormones, mucinogen, proteins) occurs by exocytosis.
FIGURE 5.2. A l i g ht m i c rog raph of pseudostratifi ed c i l i ated (C ) c o l umna r ep ithe l i um with g o b let ce l ls (G ) l i n ing the tra c h e a . A l l o f t h e ce l l s i n th is ep ith e l i um rest on t h e b a s a l l am i na ( n ote the basa l c e l l [ B C] ) , b u t not a l l of them extend t o t h e l u m e n , g iv ing a fa lse ly stratif ied a p p e a ra n c e . B l ood vesse ls ( BV) conta i n i ng r e d b l o o d ce l l s a re seen i n th e u n d e rly ing connective tissue .
l!illlJttQij Ep ithe l i a and G l ands 77
4. Selective permeab i l ity results from the presence of tight junctions between epithelial cells and permits fluids with different compositions and concentrations to exist on separate sides of an epithelial layer (e.g., intestinal epithelium) .
5 . Protection from abrasion and injury i s provided by the epidermis, the epithelial layer of the skin.
CLIN ICAL CONSIDERATIONS
Fi rst-degree burns a re les ions c a used by he at, fr icti on , o r oth e r a g e nts .
1 . D a m a g e is l im ited to the s u pe rfi c i a l l ayers of the epithe l ium � u s ua l ly th e e p i d e rm is of th e sk in ) . 2. Redness a n d edema o c c u r, b ut b l i sters d o not fo rm .
a . M itoti c a l ly a ctive c e l ls rem a i n v ia b l e i n the deeper l ayers of the e p i d e rm is . b. They d ivi d e a n d re p l a c e th e d a m a g e d o r destroyed c e l l s .
These surfaces contain specialized molecules that form junctions that permit cells to adhere to each other and restrict movement of materials between adjacent cells (paracellular route) into and out of the lumen lined by the epithelium.
A. The junctiona l complex is an intricate arrangement of membrane-associated ce l l adhesion molecules that function in cell-to-cell attachment of columnar epithelial cells. It corresponds to the terminal bar observed in epithelia by light microscopy and consists of three distinct components that are visible by electron microscopy. 1 . The t ight junction (zonu la occludens; plural: zonulae occludentes) is a zone that surrounds
the entire apical perimeter of adjacent cells and is formed by fusion of the outer leaflets of the cells' plasma membranes (Figure 5.3) . a. In freeze-fracture preparations of this zone, the tight junction is visible as a branching
anastomosing network of intramembrane strands �r idges) on the plasma membrane inner leaflet next to the cytoplasm (P-face) and grooves on the corresponding external E-face, the inner aspect of the outer leaflet (Figure 5 .3) . The strands consist of transmembrane prote ins of each cell attached d i rectly to one another, thus sealing off the extracellular space.
b. The intramembrane strands that close off the paracellular route possess four groups of transmembrane proteins : claudins, occludins, nectins, and junctional adhesive molecules (JAMs). � 1 ) Claud ins are believed to bear the greatest responsibility in closing off the paracellular
route by creating a physical barrier that prevents the movement of material between the cells. However, claudins do form small aqueous pores that allow water and small ions to penetrate this barrier.
�2) Occlud ins are also present in most, but not all, epithelial cell tight junctions. Their role is not understood as yet.
�3) Nectins are also present in the zonula occludens, and their extracellular domains form a part of the physical barrier.
�4) JAMs are similar to nectins in that their extracellular domains probably impede the movement of molecules in the extracellular space of the tight junction.
These four proteins have to be reinforced so that they maintain their proper position, and this reinforcement is due to the presence of actin f i laments (F-acti n ) of the cytoskeleton. However, there are intermediary proteins that are capable of binding both to F-actin as well as to the four proteins just described. These are the three zonu la occludens prote ins, Z0-1 , Z0-2, and Z0-3, as well as a fourth protein, known as afad in . These four intermediary proteins are located on the cytoplasmic aspect of the region of the cell membrane involved in the formation of the tight junction and, in that fashion, are interposed between the F-actin and the claudins, occludins, nectins, and JAMs, forming a strong bond that maintains the integrity of the tight junction.
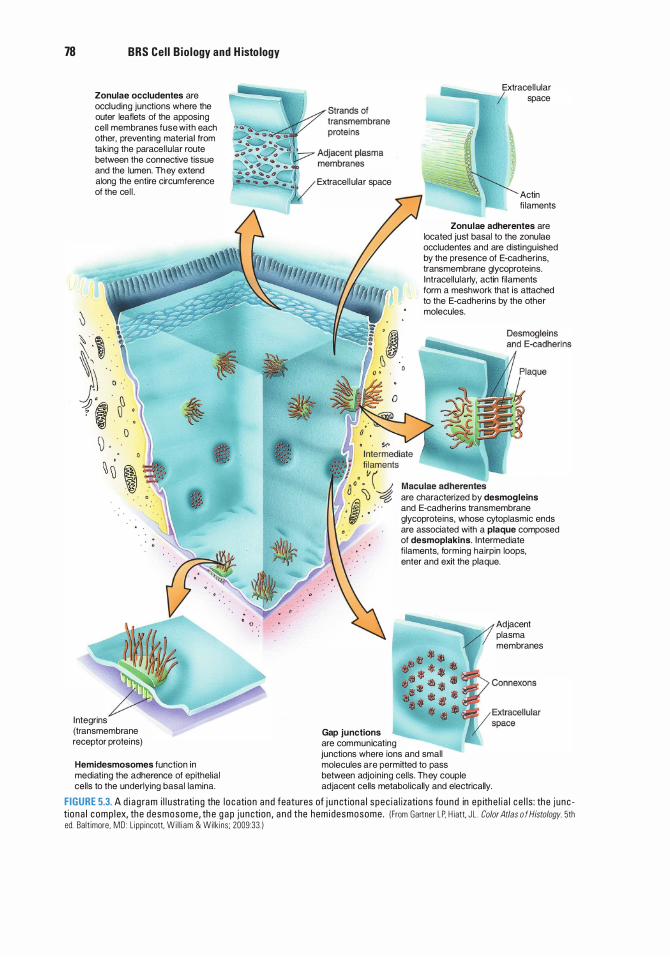
78 BRS Cel l B io logy and H isto logy
0
Zonulae occludentes are occluding junctions where the outer leaflets of the apposing cel l membranes fuse with each other, preventing material from taking the paracel lu lar route between the connective tissue and the lumen. Th ey extend along the entire circumference of the cel l .
� ' � ·
l �J -:1) ' ? i � ·
� ·
� � '
l ntegrins (transmembrane receptor protei ns)
� I
• '
Extracel l ular space
Gap junctions are communicating
Extracel l ular --.....:;�-� space
Actin fi laments
Zonulae adherentes are located just basal to the zonulae occludentes and are distingu ished by the presence of E-cadherins, transmembrane glycoproteins. lntracel lularly, actin fi laments form a meshwork that is attached to the E-cadherins by the other molecules.
are characterized by desmogleins and E-cadherins transmembrane glycoproteins, whose cytoplasmic ends are associated with a plaque composed of desmoplakins. I ntermediate fi laments, forming hairpin loops, enter and exit the plaque.
Adjacent plasma membranes
junctions where ions and small Hemidesmosomes function in molecules are permitted to pass mediating the adherence of epithelial between adjoin ing cells. Th ey couple cells to the underlying basal lamina. adjacent cells metabol ically and electrically.
FIGURE 5.3. A d i a g ra m i l l u strati n g the l o cation and features of j u n ction a l spec i a l izati ons found in e p ithe l i a l c e l l s : the j unc tio na l c omp l ex, the desmosome , th e g a p j unction , a n d the hem idesmosome . I From Gartner L P, H iatt. J L . Color Atlas o f Histology. 5th ed. Ba lt imore, MD : L ipp incott, Wi l l i am & Wilk ins ; 2009:33. )
l!illlJttQij Ep ith e l i a a nd G l a n d s 79
c. The tight junction prevents not only the movement of substances into the extracel lu lar space from the lumen but also intermingling of the transmembrane proteins of the apical with those of the lateral domains. This ability (its tightness) is directly related to the number and complexity of the intramembrane strands and to the function of the epithelia housing the particular tight junction.
d . The fasc ia occludens, a ribbon-like area of fusion between transmembrane proteins on adjacent endothe l ia l ce l ls lining capillaries, is analogous to the zonula occludens but does not encircle the perimeter of the entire cell.
2. Anchoring junctions of epithelial cells consist of four types, two on the cell's lateral domain, zonu la adherens (plural: zonulae adherentes) and desmosome (macula adherens; plural: maculae adherentes) and two, discussed in the section below, on the cell's basal domain, namely hemidesmosomes and focal adhesions. a . The adhering junction, zonu la adherens, surrounds the entire perimeter of epithelial cell,
and is located just basal to and reinforcing the zonula occludens (Figure 5 .3) . (1 ) It is characterized by a 10-to 20-nm separation between the adjoining cell membranes
where the extracellular portions of the transmembrane glycoprotein E-cadherin molecules occupy the intercellular space.
(2) A mat of actin f i laments is located on each of the cytoplasmic surfaces of the zonulae adherentes. The actin filaments are linked to each other via the actin-binding proteins a-actin in, and are linked, via another actin-binding protein vincu l in, to the protein caten in , which also binds to the intracellular portion of the E-cadherin molecules. It is in this fashion that the E-cadherin molecules are reinforced by the a-actinin filaments of the cytoskeleton. The extracellular moieties of E-cadherins of adjacent cells face each other in the extracellular space and, in the presence of Ca2+ ions, bind to each other, promoting adhesion of adjacent cells to each other.
(3) Fasc iae adherentes, ribbon-like adhesion zones in the i ntercalated d isks of cardiac muscle, are analogous to zonulae adherentes, but they do not surround the entire perimeter of the cardiac muscle cells.
b. Desmosomes (maculae adherentes) are small, discrete, disk-shaped adhesive sites. Desmosomes are commonly found at sites other than the junctional complex, where they join epithelial cells to each other. (1 ) Desmosomes are characterized by having five regions, two intracellular regions in
each cell, namely the outer dense p laque and inner dense p laque, and an extracellular region, known as the extracel lu la r core, in the space between the two cells.
(2) The extracellular moieties of the transmembrane glycoproteins, desmogle ins and desmocol l ins, members of the E-cadherin superfamily, of one cell contact desmogleins and desmocollins of the other cell in the extracellular space. In order for these glycoproteins to form strong adhesive bonds with their counterparts, Ca2+ ions must be present. These extracellular moieties of desmogleins and desmocollins of each cell form the extracellular core and hold the two cells to each other.
(3) The intracellular moieties of desmogleins and desmocollins form bonds with the desmosomal plaque proteins plakoglob ins and p lakoph i l ins . Additional large proteins, known as desmoplakins, contact both plakoglobins and plakophilins, and together they form the outer dense p laque that presses against the cytoplasmic aspect of each cell membrane.
(4) The desmoplakins are large molecules, and their tails extend farther into the cytoplasm where they contact and form bonds with the keratin intermediate f i laments of the epithelial cell. This region of bonding between the desmoplakins and the intermediate filaments forms the inner dense p laque, and it is here that the cytoskeleton is affixed to the site of adhesion.
B. Gap junctions (communicating junctions; nexus) are not part of the junctional complex and are frequent components of certain tissues other than epithelia (e.g., central nervous system, cardiac muscle, and smooth muscle) . 1 . Gap junctions are small aqueous pores that are inserted into the plasma membranes that
couple adjacent ce l ls metabolically and electrically (see Figure 5 .3) .
80 BRS Cel l B io logy and H isto logy
2. A gap junction is composed of subunits, called connexons (hemichanne ls), which extend beyond the cell surface into the gap (a 2-nm-wide intercellular space) (Figure 5.3) . Two connexons, one in the plasma membrane of each adjacent cell contacting each other in the intercellular space, form a single gap junction. a . Connexons consist of six subunits (composed of proteins called connexins), which are
arranged radially around a central channel with a diameter of 1 . 5 nm (see Figure 5 .3) . b. Precise a l ignment of connexons on adjacent cells produces a junction where they form
cel l -to-ce l l channels permitting the passage of ions and small molecules with a molecular weight of less than 1 kDa (kilodaltons) but preventing these molecules from escaping into the extracellular space.
c. Since there are different connexons, depending on the amino acid sequence of their connexins, gap junctions may be homotypic or heterotypic.
d . Connexins may alter their conformation to shut off communication between cells, especially if one of the cells is dying.
e. Usually, a large number of gap junction channels are clustered together to form a gap junction p laque where exchange of ions and small second messenger molecules may occur.
f. Connexons are in abundant supply where intercellular communication and coordination is essential such as in smooth and cardiac muscles, nerves, and certain epithelia.
Deafness M utati ons of c e rta i n c onnex ins g e nes, wh i c h a re a b u n d a nt i n the c o c h l ea , a re respons i b l e fo r d e afness .
Bone deve lopment and m ineral izat ion Ce rta i n genes code fo r c onnex ins l o c ated in gap j u n cti ons betwee n osteob l a sts a n d osteo cytes i n deve l o p i n g bone . When a p a rti c u l a r g e ne ( Cx43) is d e l eted, ske l eta l d efe cts d eve lop and bone m i n e ra l izati on i s d e layed .
Darier d isease ( a lso known as keratosis fo l l icu laris) i s re cogn iza b l e d u e t o th e pus-fi l l e d , d ry, d a rk reg ions on the sk in ( a lth o ugh th e pus may be a bsent) . It is a n i n he rited , a utosom a l d om i n ant, n onconta g i ous c o nd itio n . H i sto l o g i c a l ly, the ke rati no cytes of the sk in ( e spec i a l ly those of the stratu m sp i nosum a n d stratu m g ra n u l o sum ) a re rou n d ed , a n d b e c a use the desmosoma l conta cts a re comprom ised , th e i nte rc e l l u l a r c onnect ions a re weakened a n d i n effe ctive, l e a d i n g t o a c a ntho lys is . The d i sti n g u is h i ng c h a ra cter isti c s of the d isease a re a s pec ifi c s c ent of the affe cted sk i n a n d t he fra g i l ity of the fi n g e rna i l s . O n the ave rage , 1 i n 1 00,000 peop l e is affl i cted by D a ri e r d i sease wor ldwi de . The cond iti on a p p e a rs to be due to a p rob l em of i ntrace l lu lar trafficking of desmop lakin to th e late ra l c e l l m e m b ra n e d u ri n g desmoso m a l assem b ly.
C. Lateral i nterd ig itations (p l icae) are irregular finger like projections that inter lock adjacent epithelial cells. These lateral interdigitations are most frequently present in cells that function in fluid and/ or electrolyte transport (e.g., epithelial lining of the intestines, proximal tubules of the kidney) .
A. The basement membrane is a narrow, flexible, PAS-positive (i .e. , it stains purplish with periodic acid-Schiff reagent) acellular supportive structure that is consistently interposed between the epithelium and the underlying connective tissue. The thickness of the basement membrane depends on its location, so that it is much thicker in thick skin than in the lining of the trachea, but on the average it is usually 0.3 Jlm wide. When viewed with the electron microscope, the basement membrane is resolved to be composed of two layers, the basal lamina , approximately 100 nm in thickness, and the lamina reticu laris, which is at least 200 nm in thickness (Figure 5.4) . 1 . The basa l lamina is manufactured by the ep ithe l ia l layer and is composed of two regions, the
electron-lucent lamina Iucida, which is in direct contact with the basal plasma membrane of
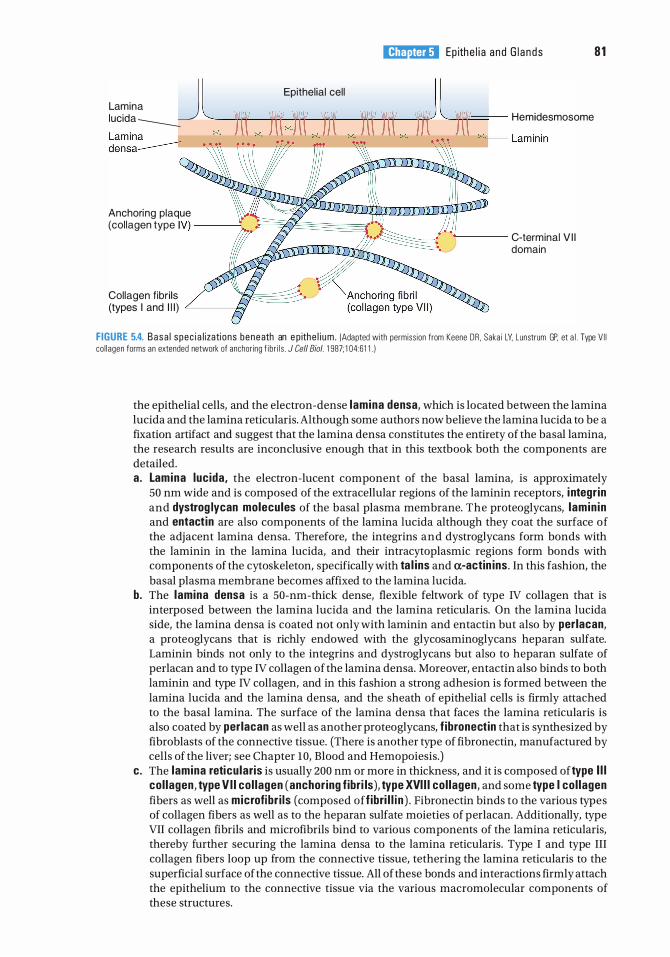
l!illlJttQij Ep ith e l i a a nd G l a n d s 81
Lamina J Epithel ial cel l � Iucida --------...::: '----rni'--'iTr---nn--..-IT-----rrr--'i'ni--..T""r' - Hemidesmosome
� Lamin in -- ��� -+ H+-- ��-��-- ��-------¥�--�
Anchoring plaque (col lagen type IV) ----=_
'----- C-terminal V I I domain
Collagen fibri ls (types I and I l l ) L__ __ ---i"V
FIGURE 5.4. Basa l spec i a l izati ons beneath an e p ithe l i um . (Adapted with permiss ion from Keene DR . Sakai LV. Lunstrum GP. et a l . Type V I I co l l agen forms an extended network of anchor ing f i b r i l s . J Cell Bioi. 1 987; 1 04:61 1 . )
the epithelial cells, and the electron-dense lamina densa, which is located between the lamina lucida and the lamina reticularis. Although some authors now believe the lamina lucida to be a fixation artifact and suggest that the lamina densa constitutes the entirety of the basal lamina, the research results are inconclusive enough that in this textbook both the components are detailed. a. Lamina Iucida, the electron-lucent component of the basal lamina, is approximately
50 nm wide and is composed of the extracellular regions of the laminin receptors, i ntegr in and dystrog lycan molecules of the basal plasma membrane. The proteoglycans, lamin in and entact in are also components of the lamina lucida although they coat the surface of the adjacent lamina densa. Therefore, the integrins and dystroglycans form bonds with the laminin in the lamina lucida, and their intracytoplasmic regions form bonds with components of the cytoskeleton, specifically with ta l ins and a-actin ins . In this fashion, the basal plasma membrane becomes affixed to the lamina lucida.
b. The lamina densa is a 50-nm-thick dense, flexible feltwork of type IV collagen that is interposed between the lamina lucida and the lamina reticularis. On the lamina lucida side, the lamina densa is coated not only with laminin and entactin but also by perlacan, a proteoglycans that is richly endowed with the glycosaminoglycans heparan sulfate. Laminin binds not only to the integrins and dystroglycans but also to heparan sulfate of perlacan and to type IV collagen of the lamina densa. Moreover, entactin also binds to both laminin and type IV collagen, and in this fashion a strong adhesion is formed between the lamina lucida and the lamina densa, and the sheath of epithelial cells is firmly attached to the basal lamina. The surface of the lamina densa that faces the lamina reticularis is also coated by perlacan as well as another proteoglycans, f ibronectin that is synthesized by fibroblasts of the connective tissue. (There is another type of fibronectin, manufactured by cells of the liver; see Chapter 10, Blood and Hemopoiesis.)
c. The lamina reticu laris is usually 200 nm or more in thickness, and it is composed of type I l l col lagen, type V I I col lagen (anchor ing fibri ls), type XVI I I col lagen, and some type I col lagen fibers as well as microfibr i ls (composed offibri l l i n ) . Fibronectin binds to the various types of collagen fibers as well as to the heparan sulfate moieties of perlacan. Additionally, type VII collagen fibrils and microfibrils bind to various components of the lamina reticularis, thereby further securing the lamina densa to the lamina reticularis. Type I and type III collagen fibers loop up from the connective tissue, tethering the lamina reticularis to the superficial surface of the connective tissue. All of these bonds and interactions firmly attach the epithelium to the connective tissue via the various macromolecular components of these structures.

82 BRS Cel l Bio logy and H isto logy
B . Two additional components of the basal domain of the cell membrane, the anchoring junctions focal adhesions and hemidesmosomes, also participate in the adhesion mechanism between the epithelium and the connective tissue. 1 . Focal adhesions are regions of relatively weak anchoring junctions that assist in the attachment
of the epithelium to the basal lamina. The principal components are clusters of transmembrane proteins, a lpha and beta integri ns, whose cytoplasmic moieties are attached to actin fi laments of the cytoskeleton via the intracellular anchorage proteins a lpha acti n in, ta l in, paxi l l i n , and vincul in , and their extracellular regions are attached to lamin in and fi bronecti n of the basal lamina. Focal adhesions may be attachments of long duration, but mostly they are formed as cells that migrate along the basal lamina surface and continuously detach and reattach during their movement. Both the attachment and the detachment are dynamic processes that occur due to intracellular and/or extracellular signals that alter the three-dimensional conformation of the integrin molecules, causing them to form or break bonds with the intracellular anchorage proteins and with the proteoglycans of the basal lamina.
2. Hemidesmosomes are specialized anchoring junctions whose morphology resembles that of a half of a desmosome. However, instead of attaching cells to each other, hemidesmosomes mediate strong adhes ion of epithelial cells to the underlying extracellular matrix (see Figure 5 .3) . Unlike focal adhesions, hemidesmosomes are mostly of longer duration and provide a firmer attachment of the cell to the basal lamina. Moreover, instead of binding to actin filaments of the cytoskeleton, they are bound to the more robust intermediate filaments. a. There are two types of hemidesmosomes : the classica l type (type I) located in the stratum
basale of skin, in the lining of the esophagus, in the masticatory and lining mucosae of the oral cavity, as well as in the cells of pseudostratified epithelia of structures such as the trachea, and type II hemidesmosomes are present mostly in the simple columnar epithelia of the intestinal lining. Type I hemidesmosomes are more complex, whereas type II hemidesmosomes have much fewer components. (1 ) Type I hemidesmosomes have several components, namely the dense cluster of
transmembrane proteins a6�4 integrin, whose intracytoplasmic moieties bind to the protein erbin and the plakin proteins plectin and bul lous pemphigoid antigen 230 (BP230) . It is these two plakin proteins that connect a6�4 integrins to the intermediate filaments (keratin-5 and keratin-1 4, also known as tonofi laments) . Erbin assists in the binding of the integrin molecule to BP230. Two additional proteins are associated with the a6 component of the integrin, namely bul lous pemphigoid antigen 180 (BP 1 80, also known as type XVI I col lagen) and cluster of d ifferentiation protein 1 51 (CD151 ) . BP 180 binds intracellularly to both the a6 component of the integrin and to plectin, and extracellularlyto the a6 component of the integrin and to laminin of the basal lamina. The extracellular moieties of a6�4 integrins also bind to the lamin ins and type IV col lagens of the basal lamina. CD1 51 functions to ensure that enough integrin molecules are recruited to the area so that hemidesmosome formation can occur. The intracytoplasmic components of the hemidesmosome form an electron-dense, plaque-like structure that resembles but is different from the outer dense plaque of a desmosome.
(2) Type II hemidesmosomes are much simpler than the classical hemidesmosomes, in that they are composed only of the dense cluster of transmembrane proteins a6�4 integr in whose intracytoplasmic moieties bind to the plak in protein p lectin, which in turn binds to the intermediate filaments keratin-S and keratin-18 (tonofi laments) . As in type I hemidesmosomes, the intracytoplasmic components form an electron-dense, plaque-like structure that resembles but is different from the outer dense plaque of a desmosome.
b. Because of the large number of a6�4 integrins and their connection to the tougher intermediate filaments rather than to the less sturdy actin filaments, hemidesmosomes form much stronger anchoring junctions than focal adhesions. However, similar to focal adhesions, the presence of Ca2+ ions are necessary for the formation and maintenance of these anchoring junctions, and the cell is able to form and disassemble hemidesmosomes as required. Both the formation and disassembly are regulated by a series of intracellular and extracellular signaling events, many of which act during the formation of new cells that
l!illlJttQij Ep ithe l i a and G l a nds 83
either become anchored to the basal lamina or are moving toward the free surface of the epithelium.
c. Keratin filaments (tonofilaments) in the cell terminate in the hemidesmosome plaque, allowing these junctions to l i nk the cytoskeleton with the components of the extracellular matrix.
CLIN ICAL CONSIDERATIONS
Bul lous pemphigo id i s a n autoimmune d isease i n wh i c h a nti bod i e s a g a i nst h em i d esmosomes a re prod u c e d .
1 . T h i s d i sease is c h a ra cte r ized b y c h ron i c g e n e ra l i zed b l i ste rs i n t h e sk i n . 2. These b l i sters cause the e p ith e l i um to sepa rate f rom the u n d e rlyi ng su bstratu m .
C . Basal p lasma membrane info ld ings are common in ion-transporting epithe l ia (e.g., distal convoluted tubule of the kidney, striated ducts in salivary glands) . 1 . They form deep invaginations that compartmentalize mitochondria. 2. Function . They increase the surface area and bring ion pumps (Na+ -K+ adenosine
triphosphatase [ATPase] ) in the plasma membrane close to their energy supply (ATP produced in mitochondria).
These surfaces may possess specialized structures such as microvilli, stereocilia, and cilia. Flagella, modified cilia that are present only in spermatozoa, are discussed in Chapter 20, The Male Reproductive System.
A. Microvi l l i are fingerlike projections of epithelia approximately l J..lm long that extend i nto a lumen and increase the cell's surface area. 1 . A g lycoca lyx (sugar coat) is present on their surfaces (see Chapter I II C) . 2. A bundle of approximately 25 to 30 actin f i laments runs longitudinally through the core of
each microvillus, extending from the tip of the microvillus into the termina l web, a zone of intersecting filaments in the apical cytoplasm. a. The actin filaments within the microvillus are bound to each other by the actin-binding
proteins vi l l in , f imbrin, esp in , and fasc in, and the actin filaments at the perimeter of the actin bundle are affixed to the plasmalemma ofthe microvillus by calmodu l i n and myosin I .
b . The actin filaments are arranged in a specific orientation within the microvillus, so that their plus ends (barbed ends) extend to the tip ofthe microvillus, where they are embedded in an amorphous material known as vi i i in. The minus ends (po inted ends) of the bundle of actin filaments extend into the terminal web of the epithelial cell, where they are affixed to the spectrin and actin filaments of the terminal web.
3. The myosin II and tropomyosin molecules located at the terminal web can interact to contract the apical region of the cell, thereby causing the microvilli to diverge from each other, increasing the intermicrovillar spaces. These enlarged intermicrovillar spaces facilitate the increased transport of materials into the cell.
4. Microvilli constitute the brush border of kidney proximal tubule cells and the striated border of intestinal absorptive cells.
B. Stereoci l ia are very long ( 15-20 J..lm in length) microvi l l i (they are not cilia) in the hair cells of the inner ear, in the epididymis, and in the vas deferens of the male reproductive tract. The core of the stereocilia is composed of actin filaments that are attached to each other by f imbrin and to the plasmalemma of the stereocilia by vi l l in-2 and ezri n (but not in the hair cells of the inner ear) . As in microvilli, the barbed ends of the actin filament bundle extend to the tip of the stereocilia, where villin is absent, and their pointed ends reach and are anchored in the cell web.
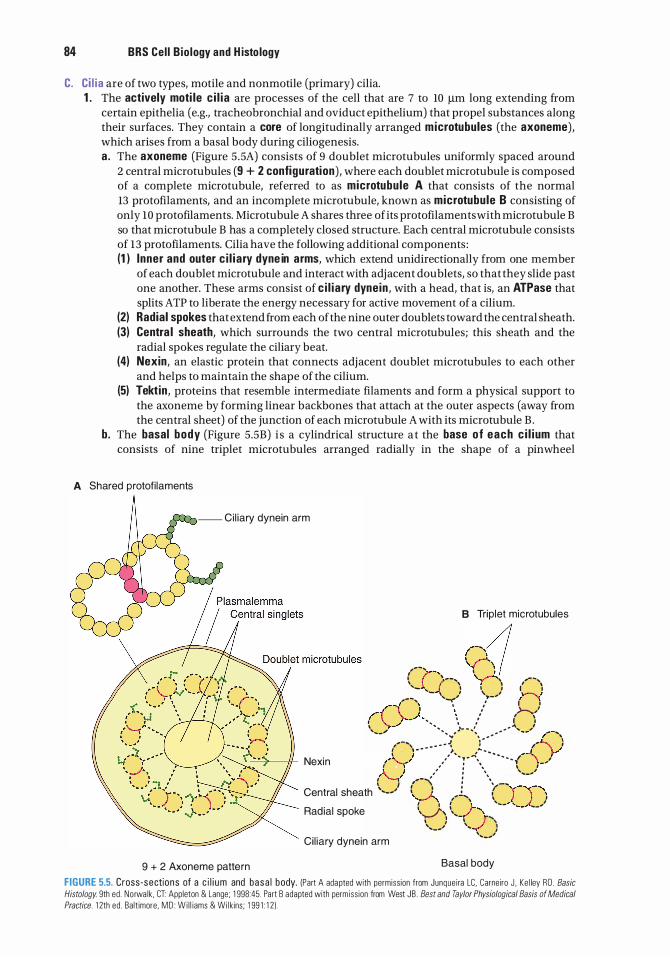
84 BRS Cel l B io logy and H isto logy
C. C i l i a are of two types, motile and nonmotile (primary) cilia. 1 . The actively moti le c i l i a are processes of the cell that are 7 to 10 J.lm long extending from
certain epithelia (e.g., tracheobronchial and oviduct epithelium) that propel substances along their surfaces. They contain a core of longitudinally arranged microtubules (the axoneme), which arises from a basal body during ciliogenesis. a . The axoneme (Figure 5 .5A) consists of 9 doublet microtubules uniformly spaced around
2 central microtubules (9 + 2 configuration) , where each doublet microtubule is composed of a complete microtubule, referred to as microtubu le A that consists of the normal l3 protofilaments, and an incomplete microtubule, known as microtubule B consisting of only 10 protofilaments. Microtubule A shares three of its protofilaments with microtubule B so that microtubule B has a completely closed structure. Each central microtubule consists of 13 proto filaments. Cilia have the following additional components : (1 ) Inner and outer c i l i a ry dyne in arms, which extend unidirectionally from one member
of each doublet microtubule and interact with adjacent doublets, so that they slide past one another. These arms consist of c i l i a ry dynein , with a head, that is, an ATPase that splits ATP to liberate the energy necessary for active movement of a cilium.
(2) Radial spokes that extend from each of the nine outer doublets toward the central sheath. (3) Centra l sheath, which surrounds the two central microtubules; this sheath and the
radial spokes regulate the ciliary beat. (4) Nexin, an elastic protein that connects adjacent doublet microtubules to each other
and helps to maintain the shape of the cilium. (5) Tektin , proteins that resemble intermediate filaments and form a physical support to
the axoneme by forming linear backbones that attach at the outer aspects (away from the central sheet) of the junction of each microtubule A with its microtubule B .
b. The basal body (Figure 5.5B) i s a cylindrical structure a t the base of each c i l i um that consists of nine triplet microtubules arranged radially in the shape of a pinwheel
A Shared protofi laments
-- Ci l iary dynein arm
9 + 2 Axoneme pattern
B Triplet microtubules
/- CA/1 1 r-, I �� I \ .,. ... , ,_,......-... , ...... ' I ' 7 ' •'' '\, '- ' .{ I I I
, ...... , - '-r/ �.,_,, ,�' ,--(--\._) . . . / ,'>--.../ ' \,.-""' ...... , , l J '
, ..... .. )· .. .. ' # ... ... ,
,_ , ... -.. , .. .. .. ........ :;' ",: .. ... .. .. .. , ... (-... '} : , .. .. ,1, ,""' .. .. .. .. ......t... }''
=-:,._-----n1- Nexin ,,....._ j ' · . - �. · · · { \ ' I \ ,' : \ \ , -' 1'--,1' # # I \
\ ,,_,1
{ I , .... -'\ ! \ -... Central sheath '•--' I 1 1 ( y--J.--\ ,,...,...,...., t' "''\ \ _} I
Radial spoke :,_;, \, _f-., , _ _ , '-- ---'
, J -,, T'\ \,,,_ ... , ... -./ J \.,._,,
Cil iary dynein arm
Basal body
FIGURE 5.5. Cross-sections of a c i l i um and basa l body. (Part A adapted with permiss ion from Junque i ra LC. Carneiro J , Ke l ley RD . Basic
Histology 9th ed . No rwa lk , CT: Appleton & Lange; 1 998:45. Part B adapted with perm iss ion from West JB . Best and Taylor Physiological Basis of Medical
Practice. 1 2th ed . Ba lt imore. MD : Wi l l iams & Wil k ins; 1 99 1 : 1 2) .
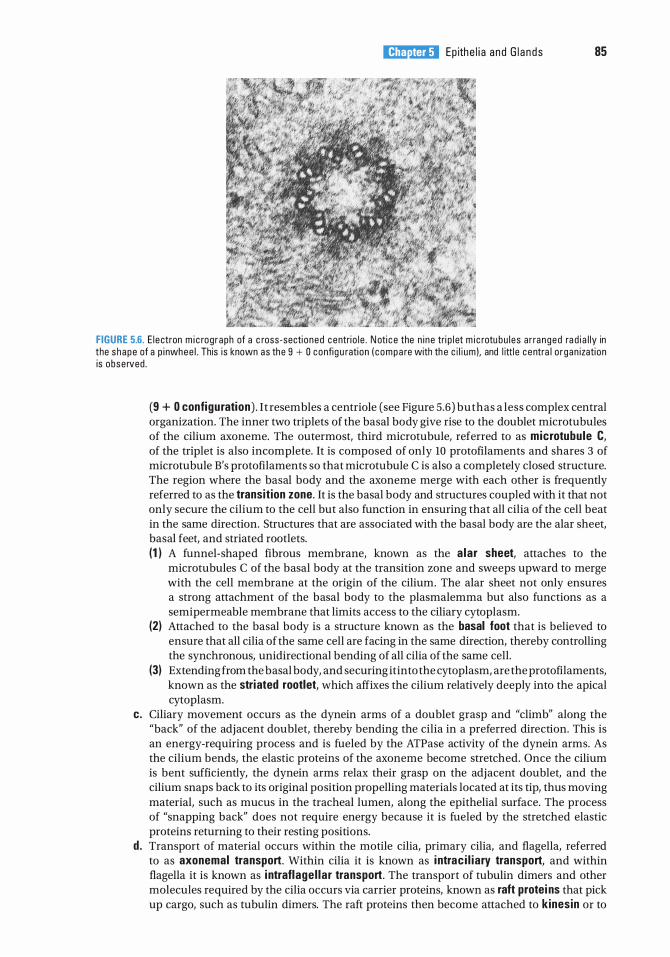
l!illlJttQij Ep ith e l i a a nd G l a n d s 85
FIGURE 5.6. E l ectron m i c rog raph of a c ross-secti oned centri o l e . N oti c e the n i ne tri p l et m i c rotu bu l es a r ra nged ra d i a l ly in the shape of a p i nwhee l . This i s known as the 9 + 0 config u rati on ( c o m p a re with th e c i l i um ). and l ittl e c entra l o rgan izati on is obse rved .
(9 + 0 configuration) . It resembles a centriole (see Figure 5.6) but has a less complex central organization. The inner two triplets of the basal body give rise to the doublet microtubules of the cilium axoneme. The outermost, third microtubule, referred to as microtubule C, of the triplet is also incomplete. It is composed of only 10 protofilaments and shares 3 of microtubule B's protofilaments so that microtubule C is also a completely closed structure. The region where the basal body and the axoneme merge with each other is frequently referred to as the transition zone. It is the basal body and structures coupled with it that not only secure the cilium to the cell but also function in ensuring that all cilia of the cell beat in the same direction. Structures that are associated with the basal body are the alar sheet, basal feet, and striated rootlets. (1 ) A funnel-shaped fibrous membrane, known as the a lar sheet, attaches to the
microtubules C of the basal body at the transition zone and sweeps upward to merge with the cell membrane at the origin of the cilium. The alar sheet not only ensures a strong attachment of the basal body to the plasmalemma but also functions as a semipermeable membrane that limits access to the ciliary cytoplasm.
(2) Attached to the basal body is a structure known as the basal foot that is believed to ensure that all cilia of the same cell are facing in the same direction, thereby controlling the synchronous, unidirectional bending of all cilia of the same cell.
(3) Extending from the basal body, and securing it into the cytoplasm, are the protofilaments, known as the striated rootlet, which affixes the cilium relatively deeply into the apical cytoplasm.
c. Ciliary movement occurs as the dynein arms of a doublet grasp and "climb" along the "back" of the adjacent doublet, thereby bending the cilia in a preferred direction. This is an energy-requiring process and is fueled by the ATPase activity of the dynein arms. As the cilium bends, the elastic proteins of the axoneme become stretched. Once the cilium is bent sufficiently, the dynein arms relax their grasp on the adjacent doublet, and the cilium snaps back to its original position propelling materials located at its tip, thus moving material, such as mucus in the tracheal lumen, along the epithelial surface. The process of "snapping back" does not require energy because it is fueled by the stretched elastic proteins returning to their resting positions.
d . Transport of material occurs within the motile cilia, primary cilia, and flagella, referred to as axonemal transport. Within cilia it is known as i ntrac i l iary transport, and within flagella it is known as i ntraflage l lar transport. The transport of tubulin dimers and other molecules required by the cilia occurs via carrier proteins, known as raft protei ns that pick up cargo, such as tubulin dimers. The raft proteins then become attached to kinesin or to
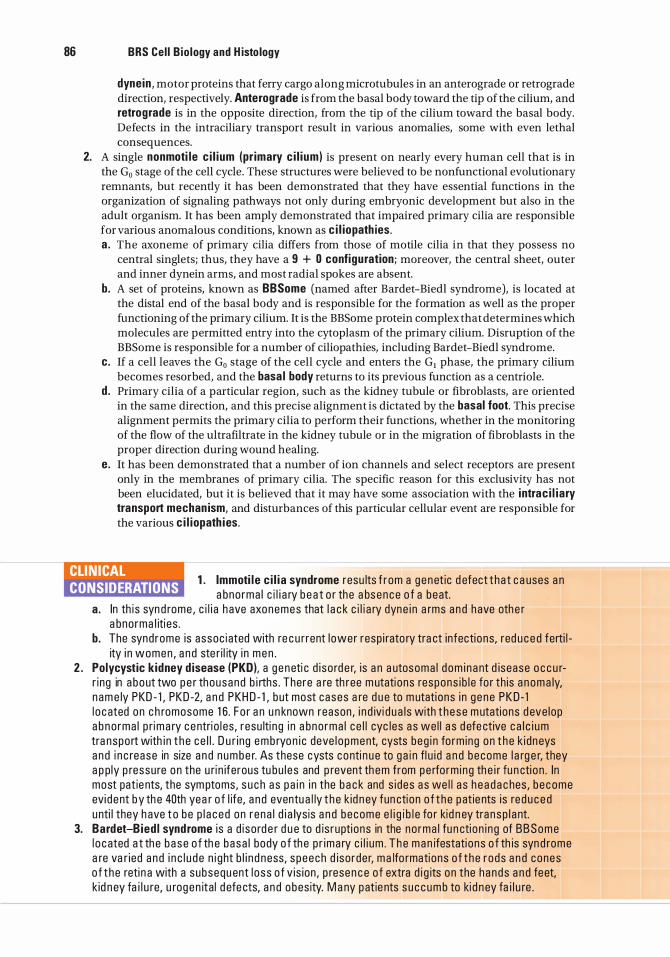
86 BRS Cel l B io logy and H isto logy
dynein , motor proteins that ferry cargo along microtubules in an anterograde or retrograde direction, respectively. Anterograde is from the basal body toward the tip of the cilium, and retrograde is in the opposite direction, from the tip of the cilium toward the basal body. Defects in the intraciliary transport result in various anomalies, some with even lethal consequences.
2. A single nonmoti le c i l i um (pr imary c i l ium) is present on nearly every human cell that is in the G0 stage of the cell cycle. These structures were believed to be nonfunctional evolutionary remnants, but recently it has been demonstrated that they have essential functions in the organization of signaling pathways not only during embryonic development but also in the adult organism. It has been amply demonstrated that impaired primary cilia are responsible for various anomalous conditions, known as c i l iopath ies. a . The axoneme of primary cilia differs from those of motile cilia in that they possess no
central singlets; thus, they have a 9 + 0 configuration; moreover, the central sheet, outer and inner dynein arms, and most radial spokes are absent.
b. A set of proteins, known as BBSome (named after Bardet-Biedl syndrome), is located at the distal end of the basal body and is responsible for the formation as well as the proper functioning of the primary cilium. It is the BBSome protein complex that determines which molecules are permitted entry into the cytoplasm of the primary cilium. Disruption of the BBSome is responsible for a number of ciliopathies, including Bardet-Biedl syndrome.
c. If a cell leaves the G0 stage of the cell cycle and enters the G1 phase, the primary cilium becomes resorbed, and the basa l body returns to its previous function as a centriole.
d . Primary cilia of a particular region, such as the kidney tubule or fibroblasts, are oriented in the same direction, and this precise alignment is dictated by the basal foot. This precise alignment permits the primary cilia to perform their functions, whether in the monitoring of the flow of the ultrafiltrate in the kidney tubule or in the migration of fibroblasts in the proper direction during wound healing.
e. It has been demonstrated that a number of ion channels and select receptors are present only in the membranes of primary cilia. The specific reason for this exclusivity has not been elucidated, but it is believed that it may have some association with the i ntrac i l iary transport mechan ism, and disturbances of this particular cellular event are responsible for the various c i l iopath ies.
CLINICAL CONSIDERATIONS
1 . lmmoti l e c i l i a syndrome resu lts f r om a g e net ic d efect t ha t c a uses a n a bno rma l c i l i a ry b e a t o r the a bsence o f a beat.
a. In th i s syn d rome , c i l i a h ave axonemes that l a c k c i l i a ry dyne i n a rms a n d have oth e r a bno rma l iti es .
b. The synd rome is assoc i ated with re c u rrent l ower resp i rato ry tra ct infecti ons, red u c e d ferti l ity i n women , a n d ste r i l ity i n m e n .
2 . Polycystic k idney d isease (PKD), a g e neti c d i so rd e r, is a n a utosoma l d om i n ant d isease o c c u rr i ng in a bout two p e r thousand b irths . There a re th ree m utati ons respons i b l e fo r th is a n oma ly, n am e ly PKD - 1 , PKD -2, a n d PKH D - 1 , b ut most cases a re d u e to m utati ons i n g e ne PKD - 1 l o c ated on c h romosome 1 6 . F o r a n u n known reason , i n d ivi d u a ls with t h ese m utations d eve lop a b no rma l p r ima ry c e ntri o l es , resu lti ng i n a bno rma l c e l l cyc l es a s we l l a s d efe ctive c a l c i um tra nspo rt with i n t h e c e l l . D u r i ng e m b ryon i c deve l o pment, cysts beg i n fo rm ing on t h e k i dn eys a n d i n c rease in size a n d n u m b e r. As these cysts conti n u e to g a i n fl u i d a n d become l a rg e r, they a p p ly p ressu re on the u r i n iferous tu bu l e s and p revent th em from pe rfo rm ing th e i r fu n cti o n . In most pat ie nts, the sym ptoms, s u c h a s p a i n i n the b a c k and s i des a s we l l a s h e a d a c hes , b e come evi d ent by th e 40th yea r o f l ife, a n d eventu a l ly t h e k id n ey fun cti on o f t h e pat ie nts i s red u c e d unti l they h ave t o be p l a c ed on r ena l d i a lys is a n d become e l i g i b l e fo r kid n ey tra nsp l a nt.
3. Bardet-B ied l syndrome i s a d i so rd e r d u e to d is rupti ons in the no rma l fu n cti on i n g of B B S o m e l o c ated a t th e b a s e o f th e basa l body o f th e p r ima ry c i l i um . T h e m a n ifestati ons o f th is syn d rome a re va r ied a n d i n c l u d e n i g ht b l i n d ness, s peech d iso rde r, ma lfo rmations o f t he r ods a n d cones o f t he reti n a with a subsequ ent l o ss o f v is ion , p resen c e o f extra d i g its on the h ands a n d feet, k id n ey fa i l u re, u rog en ita l d efe cts, a n d o bes ity. M a ny pat ie nts s u c c u m b to ki d n ey fa i l u re .
l!illlJttQij Ep ith e l i a a nd G l a n d s 87
They originate from an epithelium that penetrates the connective tissue and forms secretory units.
A. Structure. A gland consists of a functional portion (parenchyma) of secretory and ductal epithelial cells, which is separated by a basal lamina from supporting connective tissue elements (stroma) .
B. Classification. Glands are classified into three types based on the site of secretion. Exocrine g lands secrete into a duct or onto a surface. Endocrine g lands secrete into the bloodstream. Paracrine g lands secrete into the local extracellular space. 1. Exocrine g lands
a . Unicel lu lar g lands are composed of a single cell (e.g., goblet cells in tracheal epithelium). b. Multice l lu lar g lands (Figure 5.7)
(1 ) Classification is based on two criteria. (a ) Multicellular glands are classified according to duct branch ing as simple g lands
(duct does not branch) or compound g lands (duct branches) . (b ) They are further classified according to the shape of the secretory un it as acinar or
a lveolar (saclike or flasklike) or tubu lar (straight, coiled, or branched).
, , -� ' -----·
FIGURE 5.7. L ight m i c rog raph showing stratifi ed squamous non ke ratin i zed ep ithe l i um ( arrow) l i n i n g the l umen of the esophag us . Th is e p ith e l i um is th i c k, and ce l ls i n i ts u p p e r laye rs a re f lattened o r s quamous , whereas th e basa l ce l ls that u nde rg o m itosis and g ive r ise to ce l l s of the u p p e r layer a re c u bo i da l . Eso p h a g e a l c a rd i a c g l a n ds ( E G ) a re present in the connective ti ssue (CT) layer ( l am i na p rop r i a ) d eep to the e p ithe l i um . These g l a nds a re l o c ated i n the v i c i n ity of the eso p h a g e o c a rd i a c j u n cti on , a nd they a re l ined by s imp le c o l u m n a r ep ithe l i a l ce l ls that sec rete m u cus .
88 BRS Cel l Bio logy and H isto logy
(2) A connective tissue capsule may surround the gland, or septa of connective tissue may divide the gland into lobes and smaller lobu les.
(3) Glands may have ducts between lobes ( i nter lobar) , within lobes ( i ntra lobar), between lobules ( i nter lobu lar) , or within lobules ( intra lobular), such as striated and intercalated ducts.
(4) Multicellular glands secrete various substances. (a ) Mucus is a viscous material that usually protects or lubricates cell surfaces. (b) Serous secretions are watery and often rich in enzymes. (c) Mixed secretions contain both mucous and serous components.
(5) Mechanisms of secretion vary. (a ) In merocrine glands (e.g., parotid gland), the secretory cells release their contents
by exocytosis. (b) In apocrine glands (e.g., lactating mammary gland), part of the apical cytoplasm of
the secretory cell is released along with the contents. (c) In holocr ine glands (e.g., sebaceous gland), the entire secretory cell along with its
contents is released. 2. Endocrine g lands may be un ice l lu lar (e.g., individual endocrine cells in gastrointestinal and
respiratory epithelia) or multice l l u la r (e.g., adrenal gland), and they lack a duct system. In multicellular glands, secretory material is released into fenestrated capillaries, which are abundant just outside the basal lamina of the glandular epithelium.
1 . Ep ithe l i a sometimes u n de rgo metaplasia i n response to pe rs iste nt i n CLIN ICAL CONSIDERATIONS j u ry. M eta p l as i a i s the convers ion o f o ne type o f d iffe re nti ated e p ith e
l i um i nto a n oth e r. M ost c ommon ly, a g l a n d u l a r e p ith e l i um is tra nsfo rmed i nto a s quamous e p ith e l i um . H oweve r, i n cases o f c h ro n i c a c i d refl ux from th e sto m a c h i nto th e lower e sopha g us, the stratifi e d s quamous non ke rati n ized e p ith e l i um is re p l a c ed by a g l a n du l a r m u cuss e c reti ng e p ith e l i um (Barrett epithe l ium) s im i l a r to that fo und l i n i n g the c a rd i a of th e sto m a c h . T h i s h e l ps t o p rote ct th e e s o p h a g u s a g a inst t h e i n j u r i ous effects o f t h e a c i d a n d p e ps i n , b ut i s a l so a we l l - known p re c u rso r o f eso ph agea l a d e n o c a rc i n oma .
2 . Epithe l ia l ce l l tumors o c c u r when ce l l s fa i l t o respond t o no rm a l g rowth reg u l ato ry m e c h a n isms . a. These tumo rs a re benign when they rema i n l oca l . b . They a re mal ignant when they i nvade ne ighbor ing tissues. Then they may ( o r m ay not)
metastasize to oth e r p a rts of th e body. i. Carc inomas a re m a l i g n a nt tu mo rs that a ri se from surface ep ithe l ia .
i i . Adenocarcinomas a re ma l i g n a nt tumo rs that a rise from g lands.
Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which one of the following statements about the desmosome is true?
(A) It is sometimes called a nexus. (B ) It permits the passage of large proteins
from one cell to an adjacent cell. (C) It has a plaque made up of many
connexons. (D ) It facilitates metabolic coupling between
adjacent cells. (E) It is a disk-shaped adhesion site between
epithelial cells.
2. A medical student who has chronic lower respiratory infections seeks the advice of an ear, nose, and throat specialist. A biopsy of the student's respiratory epithelium reveals alterations in certain epithelial structures. This patient is most likely to have abnormal
(A) microvilli. (B ) desmosomes. (C) cilia. (D ) hemidesmosomes. (E) basal plasmalemma infoldings.
3. Which one of the following statements about the gap junction is true?
(A) It extends as a zone around the apical perimeter of adjacent cells.
(B ) It possesses dense plaques composed in part of desmoplakins.
(C ) It permits the passage of ions from one cell to an adjacent cell.
(D ) Its adhesion is dependent upon calcium ions.
(E) It possesses transmembrane linker glycoproteins.
4. Which one of the following statements about glands is true?
(A) Exocrine glands lack ducts. (B ) Simple glands have ducts that branch. (C) Endocrine glands secrete into ducts. (D ) Serous secretions are watery. (E ) Holocrine glands release their contents by
exocytosis.
5. Which one of the following statements about epithelia is true?
(A) They are polarized. (B) They are vascular. (C) They are completely surrounded by a basal
lamina. (D ) They contain wide intercellular spaces. (E) They are not part of the wall of blood
vessels.
6. Which one of the following statements about cilia is true?
(A) They possess a 9 + 0 configuration of microtubules.
(B) They do not contain an axoneme. (C) They contain ciliary dynein arms. (D) They are nearly identical to centrioles. (E) They play a major function in absorption.
7. Which one of the following statements about stratified squamous epithelium is true?
(A) The surface layer of cells is always keratinized.
(B) The cells in its most superficial layer are flattened.
(C) Its basal cells rest on an elastic lamina. (D ) Its cells lack desmosomes. (E) It lines the ducts of sweat glands.
8. Which one of the following is an autoimmune disease?
(A) Adenocarcinoma (B) Bullous pemphigoid (C) Carcinoma (D ) First-degree burn (E) Immotile cilia syndrome
9. Which one of the following is a hereditary disease that may be associated with infertility?
(A) Adenocarcinoma (B) Bullous pemphigoid (C) Carcinoma (D ) Edema (E) Immotile cilia syndrome
89
90 BRS Cel l B io logy and H isto logy
1 0. Which one of the following is a tumor arising from glandular epithelium?
(A) Adenocarcinoma (B ) Bullous pemphigoid (C) Carcinoma (D ) Edema (E ) Immotile cilia syndrome
1 1 . Which of the following is a condition affecting the epidermis of the skin in which blisters do not form?
(A) Adenocarcinoma (B ) Bullous pemphigoid (C ) Carcinoma (D ) First-degree burn (E ) Immotile cilia syndrome
Answers and Explanations
1 . E. Desmosomes are sites of adhesion characterized by dense cytoplasmic plaques and associated keratin filaments. Only gap junctions permit cell-to-cell communication of small molecules via their connexon channels (see Chapter 5 II A) .
2. C. Individuals with abnormal respiratory cilia commonly have recurrent respiratory infections if the cilia are unable to clear the respiratory epithelium of microorganisms, debris, and so forth. The student may have immotile cilia syndrome, which is caused by a genetic defect, resulting in cilia with axonemes that lack ciliary dynein arms and thus are unable to beat (see Chapter 5 IV C 2 Clinical Considerations) .
3. C. The gap junction channel regulates the passage of ions and small molecules from cell to cell, excluding those having a molecular weight greater than 1200 Da. The tight junction is the zone of adhesion around the apical perimeter of adjacent cells. The other statements are characteristics of desmosomes (see Chapter 5 II B).
4. D . Serous secretions produced by glands are often rich in enzymes and watery in consistency. Exocrine glands secrete into ducts, and endocrine glands lack ducts. Merocrine glands use exocytosis to release their products (see Chapter 5 V B) .
5. A . Epithelia are polarized, meaning they show sidedness and have apical and basolateral surfaces with specific functions (see Chapter 5 I A) .
6. C. Cilia contain an axoneme with ciliary dynein arms extending unidirectionally from one member of each doublet. Ciliary dynein has ATPase activity, and when it splits ATP, the adjacent doublets slide past one another and the cilium moves. Microvilli, not cilia, function in absorption (see Chapter 5 IV C) .
7. B . Stratified squamous epithelium is characterized by flattened cells with or without nuclei in its superficial layer. It may or may not be keratinized, and it rests on a basal lamina produced by the epithelium. Stratified cuboidal epithelium lines the ducts in sweat glands (see Chapter 5 I B) .
8. B . Bullous pemphigoid is an autoimmune disease. Affected individuals form antibodies against their own hemidesmosomes (see Chapter 5 III B Clinical Considerations).
9. E . Immotile cilia syndrome results from a genetic defect that prevents synthesis of ciliary dynein ATPase, resulting in cilia that cannot actively move. Men are sterile because their sperm are not motile (the flagella in their tails lack this enzyme). Women may be infertile because cilia along their oviducts may fail to move oocytes toward the uterus (see Chapter 5 IV C 2 Clinical Considerations) .
10 . A. Adenocarcinomas are epithelial tumors that originate in glandular epithelia. Carcinomas originate from surface epithelia (see Chapter 5 V B 2 Clinical Considerations).
1 1 . D . First-degree burns damage the upper layers of the epidermis only, and blisters do not form in the skin (see Chapter 5 I C Clinical Considerations) .
91
Connective Tissue
I. OVERVIEW-CONNECTIVE TISSUE
A. Structure. Connective tissue is formed primarily of extrace l lu lar matrix (ECM), consisting of ground substance and f ibers, in which various connective tissue cel ls are embedded.
B. Function. Connective tissue supports organs and cells, acts as a medium for exchange of nutrients and wastes between the blood and tissues, protects against microorganisms, repa i rs damaged tissues, and stores fat.
The ECM provides a medium for the transfer of nutrients and waste materials between connective tissue cells and the bloodstream.
A. G round substance is a colorless, transparent, gel-like material in which the cells and fibers of connective tissue are embedded. 1. It is a complex mixture of g lycosaminog lycans, proteog lycans, and g lycoprote ins (see
Chapter 4). 2. Ground substance serves as a lubricant, helps to prevent invasion of tissues by foreign agents,
and resists forces of compression.
B. Fibers (collagen, reticular, and elastic) are long, slender protein polymers present in different proportions in different types of connective tissue.
92
1 . Col lagen f ibers. Although there are at least 25 different types of collagen, the most common collagen types in connective tissue proper are types I and I l l co l lagen (see Chapter 4, Table 4.3), both consisting of many closely packed tropocol lagen fibrils. The diameter of individual type I collagen fibrils varies greatly ( 10-300 nm). These fibrils may aggregate and form cable-like structures up to several centimeters in length and display 67-nm periodicity (see Chapter 4 and Figure 4.4) . a. Collagen fibers are produced in a two-stage process, involving both intracellular and
extracellular events (see Chapter 4 and Figure 4.3) . b. Collagen fibers have great tensile strength, which imparts both flexibility and strength to
tissues containing them.
l!ii!!J1lliij Connective Tissue 93
c. Bone, skin, cartilage, tendon, and many other structures of the body contain collagen fibers.
2. Reticu lar f ibers are extremely th in (0.5-2.0 J.Lm) in diameter and are composed primarily of type I l l co l lagen; they have higher carbohydrate content than other collagen fibers. a. Type III collagen fibers constitute the architectural framework of certain organs and glands. b. Because of their high carbohydrate content, they stain black with silver salts.
3. E lastic f ibers are coiled branching fibers 0.2 to 1 . 0 J.Lm in diameter that sometimes form loose networks. a. These fibers may be stretched up to 150% of their resting length. b. They consist of a central amorphous substance known as elastin that is surrounded by thin
microfi br i ls . The latter are composed of fibri l l i n-1 , which is bound to elastin by the protein fibu l in-5 (see Chapter 4 III B) .
c. Elastic fibers require special staining to be observed by light microscopy.
Connective tissue cells include many types with different functions. Some originate locally and remain in the connective tissue (fixed ce l ls), whereas others originate elsewhere and remain only temporarily in connective tissue (transient cel ls) (Figure 6 . 1 ) . Fixed connective tissue ce l ls include fibroblasts, pericytes, adipose cells, mast cells, and fixed macrophages. Transient connective tissue ce l ls include certain macrophages, lymphocytes, plasma cells, neutrophils, eosinophils, and basophils.
A. Fixed cel ls of connective tissue 1. Fibroblasts arise from mesenchymal cells and are the predominant cells in connective tissue
proper (Figure 6.2) . They often possess an oval nucleus with two or more nucleoli. Fibroblasts seldom undergo mitosis except in wound healing. They may differentiate into other cell types under certain conditions (see Clinical Considerations).
Active fibroblasts are spindle shaped (fusiform) and contain well-developed rough endoplasmic reticulum (RER) and many Golgi complexes. Myosin is located throughout the cytoplasm, and actin and a-actinin are located at the cell periphery. Synthetica l ly active, they produce procollagen, collagen, and elastic fibers and most of the ground substance as well as other components of the ECM.
CLIN ICAL CONSIDERATIONS
Fibroblasts u n d e rgo m itosis o n ly d u ri n g wound hea l i n g . H owever, unde r c e rta i n c o nd iti ons , fi b ro b l a sts m ay d iffere ntiate i nto a d i pose c e l ls, o r d u r
i ng fi b ro c a rti l a g e fo rmation , they may d iffe rentiate i nto c hond ro cytes . I n a d d iti on , u n de r patho l o g i c a l c ond itions , fi b rob l a sts may d i ffe re ntiate i nto osteob l a sts .
2. Pericytes (adventitia l cel ls; perivascu lar cel ls) are derived from embryonic mesenchymal cells and may retain a p luri potentia l ro le . a . They possess characteristics of endothelial cells as well as smooth muscle cells because they
contain actin, myosin, and tropomyosin, suggesting that they may function in contraction where they assist to modify blood flow through capillaries.
b. They are smaller than fibroblasts, are located mostly along capillaries, and are completely enveloped by their own basal lamina, which is continuous with the basal lamina of the capillary endothelium.
c. During blood vessel formation and repair, they may differentiate into fibroblasts, smooth muscle cells, as well as endothelial cells of blood vessel walls.
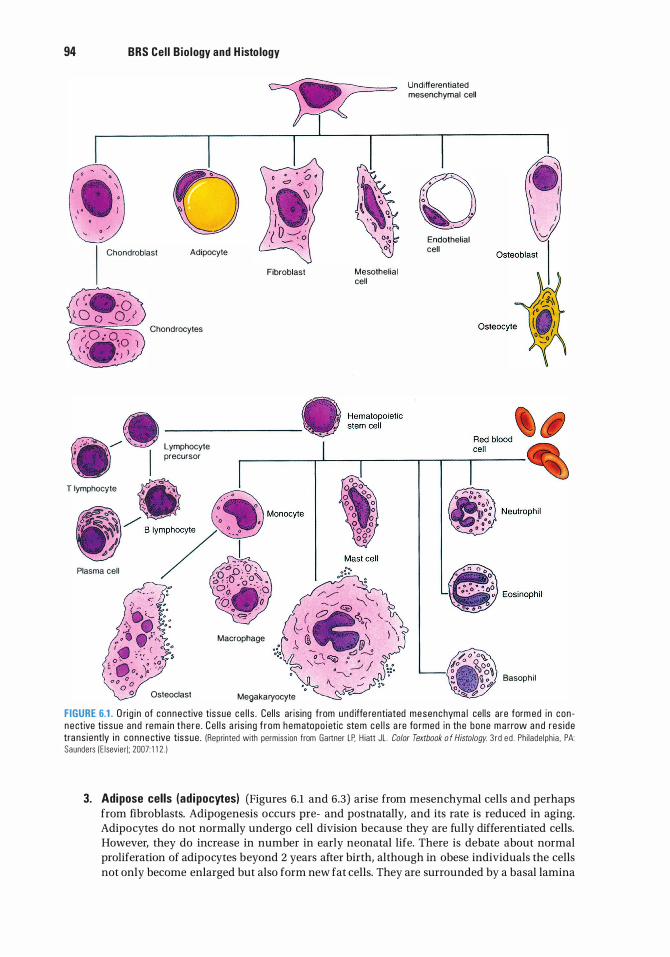
94 BRS Cel l B io logy and H isto logy
0 I Chondroblast Adipocyte
Chondrocytes
Lymphocyte precursor
Fibroblast Mesothelial cell
Undifferentiated mesenchymal cell
0 Endothelial cell
T lymphocyte
Plasma cell
Macrophage
Osteoclast Megakaryocyte
Basophi l
FIGURE 6.1 . O ri g i n of connective tissue ce l l s . Cel ls ar is ing from und iffe rentiated mesenchyma l ce l ls a re form ed in con n ective ti ssue and rem a i n the re . Ce l l s a ri s i ng f rom hematopo ietic stem ce l l s a re fo rmed in the bone m a rrow a n d res i de tra ns iently i n c onnective tissue . (Reprinted with permiss ion from Gartner LP. H iatt JL . Color Textbook o f Histology. 3 r d e d . Ph i l ade lph ia . PA: Saunders ( E l sevie r); 2007: 1 1 2 . )
3. Adipose cells (ad ipocytes) (Figures 6.1 and 6.3) arise from mesenchymal cells and perhaps from fibroblasts. Adipogenesis occurs pre- and postnatally, and its rate is reduced in aging. Adipocytes do not normally undergo cell division because they are fully differentiated cells. However, they do increase in number in early neonatal life. There is debate about normal proliferation of adipocytes beyond 2 years after birth, although in obese individuals the cells not only become enlarged but also form new fat cells. They are surrounded by a basal lamina
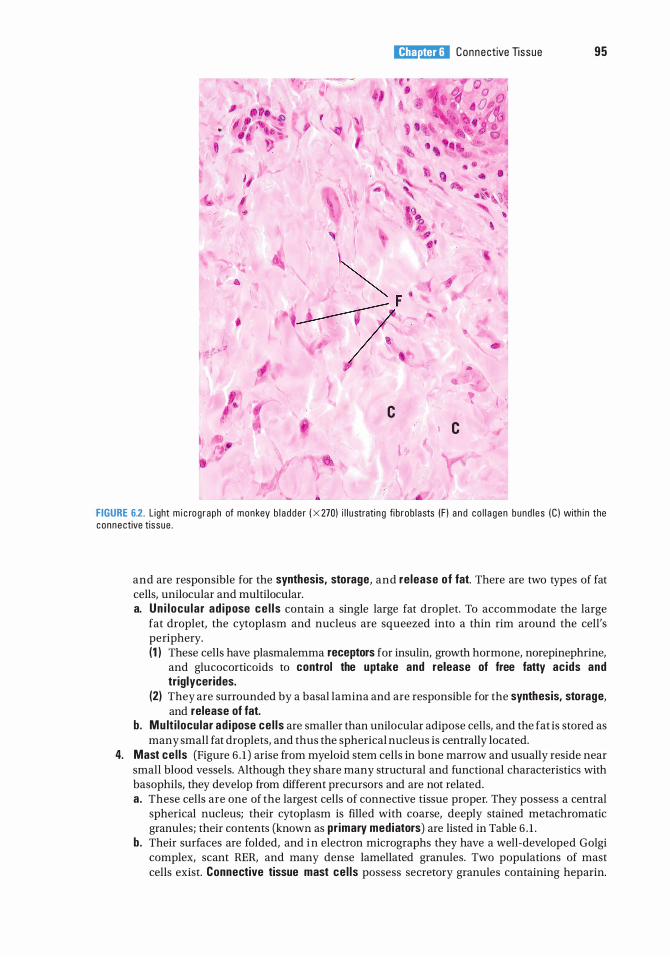
•
l!ii!!J1lliij Connective Tissue 95
� F � ..
• ' c
c I
F IGURE 6.2. L ight m i c rog raph of monkey b l a dde r ( X 270) i l l u strati n g fi b rob l asts (F ) a n d co l l a gen bund l es (C ) with i n the connective tissue .
and are responsible for the synthesis, storage, and re lease of fat. There are two types of fat cells, unilocular and multilocular. a. Un i locu lar ad ipose ce l l s contain a single large fat droplet. To accommodate the large
fat droplet, the cytoplasm and nucleus are squeezed into a thin rim around the cell's periphery. (1 ) These cells have plasmalemma receptors for insulin, growth hormone, norepinephrine,
and glucocorticoids to control the uptake and release of free fatty acids and triglycerides.
(2) They are surrounded by a basal lamina and are responsible for the synthesis, storage, and release of fat.
b . Mu lt i locular ad ipose ce l ls are smaller than unilocular adipose cells, and the fat is stored as many small fat droplets, and thus the spherical nucleus is centrally located.
4. Mast ce l ls (Figure 6 . 1 ) arise from myeloid stem cells in bone marrow and usually reside near small blood vessels. Although they share many structural and functional characteristics with basophils, they develop from different precursors and are not related. a. These cells are one of the largest cells of connective tissue proper. They possess a central
spherical nucleus; their cytoplasm is filled with coarse, deeply stained metachromatic granules; their contents (known as pr imary mediators) are listed in Table 6 . 1 .
b. Their surfaces are folded, and in electron micrographs they have a well-developed Golgi complex, scant RER, and many dense lamellated granules. Two populations of mast cells exist. Connective tissue mast ce l ls possess secretory granules containing heparin.
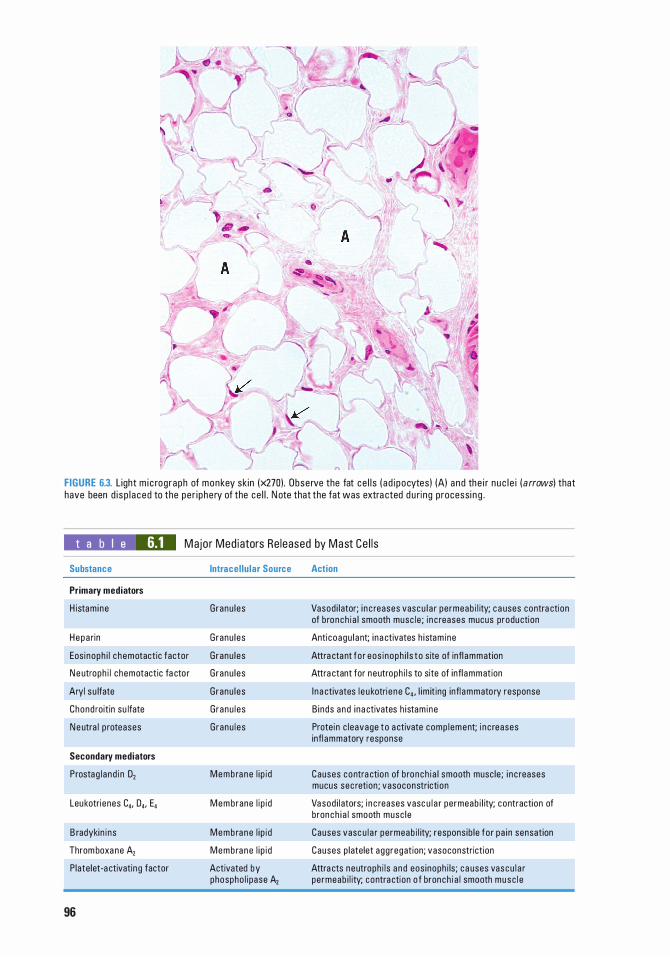
FIGURE 6.3. Light m i c rog raph of monkey sk in (x270) . Obse rve the fat ce l l s ( a d i pocytes) (A) a nd the i r n u c l e i ( arrows) that have been d i s p l a ced to the pe r i phe ry of the ce l l . N ote that the fat was extra cted d u ri ng p rocessi n g .
t a b I e 6.1 Major Med iators Re leased by Mast Ce l l s
Substance
Primary mediators
H istam ine
Hepa rin
Eos i noph i l c hemotactic factor
N e utroph i l chemotactic fa cto r
Aryl su lfate
Chond roitin su lfate
N e utra l p roteases
Secondary mediators
Prostag l a nd i n D,
Leukotri enes C4, 04, E4
B radyki n i ns
Throm boxa ne A,
P late let-a ctivatin g factor
96
Intracel lu lar Source
Granu l es
Granu l es
Granu l es
Granu l es
Granu l es
G ranu l es
G ranu l es
Memb ra ne l i p i d
Mem brane l i p i d
Memb ra ne l i p i d
Memb ra ne l i p i d
Activated by phospho l i pase A2
Action
Vasod i l ator; i n c reases vascu l a r pe rmeab i l ity; c a uses contra ction of b ronch i a l smooth musc le ; i n c reases mucus production
Anti coagu l ant; i na ctivates h i stam ine
Attra ctant fo r eos i noph i l s to s ite of infl ammation
Attra ctant for neutroph i l s to site of infl ammation
I n a ctivates l e u kotri e ne C4, l im it ing infl ammato ry response
B i nds a nd i na ctivates h i stam ine
Prote in c l eavage to a ctivate comp l ement; i n c reases infl ammatory response
Causes contra ction of b ronch i a l smooth musc le ; i n c reases mucus sec retion ; vasoconstricti on
Vasod i l ators; i n c reases vasc u l a r permeab i l ity; contraction of bronch i a l smooth musc l e
Causes vasc u l a r permeab i l ity; respons ib le fo r pa i n sensation
Causes p latelet agg regation; vasoconstriction
Attra cts neutroph i l s a nd eos inoph i ls ; c a uses vascu l a r permeab i l ity; contra ction o f bronch i a l smooth musc l e
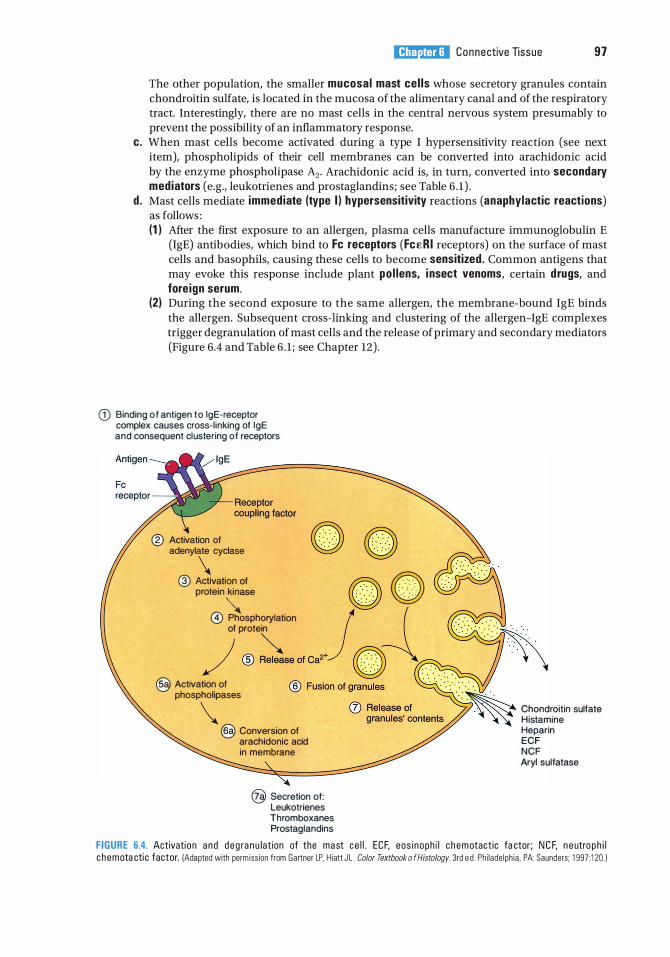
l!ii!!J1lliij Connective Tissue 97
The other population, the smaller mucosal mast cel ls whose secretory granules contain chondroitin sulfate, is located in the mucosa of the alimentary canal and of the respiratory tract. Interestingly, there are no mast cells in the central nervous system presumably to prevent the possibility of an inflammatory response.
c. When mast cells become activated during a type I hypersensitivity reaction (see next item), phospholipids of their cell membranes can be converted into arachidonic acid by the enzyme phospholipase A2• Arachidonic acid is, in turn, converted into secondary mediators (e.g., leukotrienes and prostaglandins; see Table 6 . 1 ) .
d . Mast cells mediate immediate (type I ) hypersensitivity reactions (anaphylactic reactions) as follows : (1 ) After the first exposure to an allergen, plasma cells manufacture immunoglobulin E
(IgE) antibodies, which bind to Fe receptors (FcER I receptors) on the surface of mast cells and basophils, causing these cells to become sensitized . Common antigens that may evoke this response include plant po l lens, i nsect venoms, certain drugs, and fore ign serum.
(2) During the second exposure to the same allergen, the membrane-bound IgE binds the allergen. Subsequent cross-linking and clustering of the allergen-IgE complexes trigger degranulation of mast cells and the release of primary and secondary mediators (Figure 6.4 and Table 6 . 1 ; see Chapter 12) .
CD Binding o f antigen t o lgE·receptor complex causes cross-l inking of lgE and consequent clustering of receptors
® Activation of adenylate cyclase \ ® =::�::. e � @) Phosphorylation j
of protein
/ ® ��c.� @ Activation of
phospholipases \ @ Conversion of arachidonic acid in membrane
@ Secretion of: Leukotrienes Thromboxanes Prostaglandins
Chondroitin sulfate Histamine Heparin ECF NCF Aryl sulfatase
FIGURE 6.4. Activati on a n d d e g ra n u lat ion of the mast c e l l . ECF, eos i noph i l c h e m otact ic fa ctor; N C F, n e utro p h i l c h emota cti c factor. (Adapted with perm iss ion from Gartner LP, H iatt J L . Color Textbook o f Histology. 3rd e d . Ph i l ade lph ia , PA: Saunders; 1 997: 1 20 . )
98 BRS Cel l B io logy and H isto logy
Hay fever and asthma Hay fever i s c h a ra cter ized by nasa l c ongesti on c a used by l o c a l ized
edema i n the nasa l m u c osa . Th is edema resu lts f rom the i n c reased pe rmeab i l ity of sma l l b lood vesse l s b e c a use of excess ive re l ease of histamine f rom mast ce l l s i n the nasa l m u c osa .
Peop l e with asthma have d iffi c u lty b re ath i ng d u e to b ronchospasms resu lti n g from leukotrienes re l eased i n the l u ngs .
Anaphylactic shock resu lts from the effe cts o f powerfu l med i ators re l eased d u ri n g a n immediate hypersensitivity reaction fo l l owi n g a s e c o n d exposu re t o a n a l l e rg e n .
1 . Th i s rea cti on c a n o c c u r with i n s e conds o r m i n utes afte r conta ct with a n a l l e rg e n . 2 . S i gns a n d sym ptoms i n c l u d e sho rtn ess o f b re ath, d e c reas i ng b l o o d p ressu re , a n d oth e r s i gns
a n d sym ptoms o f s hock. 3. Ana p hy la cti c s hock may be l i fe-th reaten i n g if u ntreated .
B. Transient ce l ls o f connective tissue 1. Macrophages (Figure 6 . 1 ) are the principal phagocytosing cells of connective tissue. They
are responsible for removing large particulate matter and assisting in the immune response. They also secrete substances that function in wound healing. a. Macro phages originate in the bone marrow as monocytes, circulate in the bloodstream, and
then migrate into the connective tissue, where they mature into functional macro phages (see Chapter 10 VI E). Macrophages increase in number because of the activity of the macrophage colony-stimulating factor (M-CSF). In addition, the colony-forming unit monocyte (CFU-M) facilitates the mitosis and differentiation of monocytes to form macrophages.
b. Macrophages are members of the mononuclear phagocyte system. They are anti gen presenti ng ce l ls, in that they phagocytose antigens, break them down into epitopes, and, using MHC I or MHC II molecules, place the epitopes on their cell surface to present it to immunocompetent T cells (see Chapter 12 Section III) . For historical reasons, macrophages have different names in various regions of the body (e.g., Kupffer cells in the liver, dust cells in the lungs, osteoclasts in bone, Langer hans cells in skin, microglia in the central nervous system). Macro phages display Fc£RI receptors as well as receptors for complement.
c. When activated, they display filopodia, an eccentric kidney-shaped nucleus, phagocytic vacuoles, lysosomes, and residual bodies.
d . When stimulated, they may fuse to form fore ign body g iant cel ls. These multinuc leated cel ls surround and phagocytose large foreign bodies.
2. Lymphoid cel ls (Figure 6 . 1 ) arise from lymphoid stem cells during hemopoiesis (see Chapter 10 VI G). They are located throughout the body in the subepithelial connective tissue and accumulate in the respiratory system, gastrointestinal tract, and elsewhere in areas of chronic inflammation. (For more information concerning lymphoid cells, see Chapter 12 II.) a . T lymphocytes (T cells) initiate the cel l -mediated immune response . b. B lymphocytes (B cells), following activation by an antigen, differentiate into plasma cells,
which function in the humoral immune response. c . Natura l k i l ler (NK) cells lack the surface determinants characteristic of T and B lympho
cytes but may display cytotoxic activity against tumor cells. 3. Plasma cel ls (Figure 6 . 1 ) are antibody-manufactur ing cel ls that arise from activated
B lymphocytes and are responsible for humoral immun ity. a . These ovoid cells contain an eccentric nucleus possessing c lumps of heterochromati n,
which appear to be arranged in a wheel-spoke fashion. b. Their cytoplasm is deeply basophilic because of an abundance of RER. c. A prominent area adjacent to the nucleus appears pale and contains the Golgi complex
(negative Golgi image). d . They are most abundant at wound entry sites or in areas of chronic inflammation.
4. Granulocytes (Figure 6 . 1 ) are white blood cells that possess cytoplasmic granules and arise from myeloid stem cells during hemopoiesis. At sites of inflammation, they leave the
l!ii!!J1lliij Connective Tissue 99
bloodstream and enter the loose connective tissue, where they perform their specific functions (see Chapter 10 II B 2 a). a. Neutrophi ls phagocytose, k i l l , and d igest bacteria at sites of acute inflammation. Pus is an
accumulation of dead neutrophils, bacteria, extracellular fluid, and additional debris at an inflammatory site.
b. Eosinophi ls bind to antigen-antibody complexes on the surface of parasites (e.g., helminthes) and then release cytotoxins that damage the parasites. (1 ) They are most prevalent at sites of chronic or allergic inflammation. (2) Eosinophils are attracted by eosinophil chemotactic factor (ECF), which is secreted by
mast cells and basophils, to sites of allergic inflammation. There, eosinophils release enzymes that cleave histamine and leukotriene C, thus moderating the a l lergic reaction .
(3 ) These cells also phagocytose antibody-antigen complexes. c. Basophi ls are similar to mast cells in that they possess FceRI receptors; their granules
house the same primary mediators; and the same secondary mediators are manufactured de novo from the phospholipids of their plasmalemma. They differ, however, in that they circulate via the bloodstream, whereas mast cells do not.
Classification is based on the proportion of cells to fibers and on the arrangement and type of fibers (embryonic connective tissue, connective tissue proper, or specialized connective tissue).
A. Embryonic connective tissue 1. Mucous tissue (Wharton je l ly) is a loose connective tissue that is the main constituent of the
umbilical cord. It consists of a jellylike matrix with some collagen fibers in which large stellate fibroblasts are embedded.
2. Mesenchymal tissue is found only in embryos. It consists of a gel-like amorphous matrix containing only a few scattered reticular fibers, in which star-shaped, pale-staining mesenchymal cells are embedded. Mitotic figures are often observed in these pluripotential cells.
B. Connective tissue proper 1. Loose connective tissue (areolar tissue) possesses fewer fibers but more cells than dense
connective tissue. a. This tissue is well vascularized, f lexible, and not very resistant to stress. b. It is more abundant than dense connective tissue and is the connective tissue that fills in the
spaces just deep to the skin.
CLIN ICAL CONSIDERATIONS
Edema i s a patho l og i c p rocess resu lti n g i n a n increased volume o f tissue f lu id .
Edema may be c a used by venous obstructi on o r d e c reased venous b lood f low ( a s i n congestive h e art fa i l u re ) , i n c reased c a p i l l a ry p e rmeab i l ity ( d u e to i nj u ry), sta rvati on , excess ive re l ease of h i stamine, and obstru cti on of lymphati c vesse ls .
Edema that is respons ive to l o c a l ized p ressure ( i . e . , d e p ress ions pe rs ist afte r re lease of p ressure) i s c a l l e d pitting edema.
2. Dense connective t issue contains more fibers but fewer cells than loose connective tissue. It is classified by the orientation of its fiber bundles into two types : a. Dense, i rregular connective t issue (most common), which contains fiber bundles that
have no definite orientation. This tissue is characteristic of the dermis and capsules of many organs.
b . Dense, regu lar connective tissue, which contains fiber bundles and attenuated fibroblasts that are arranged in a uniform parallel fashion. (1 ) It is present only in tendons and l igaments. (2) This tissue may be collagenous or elastic.
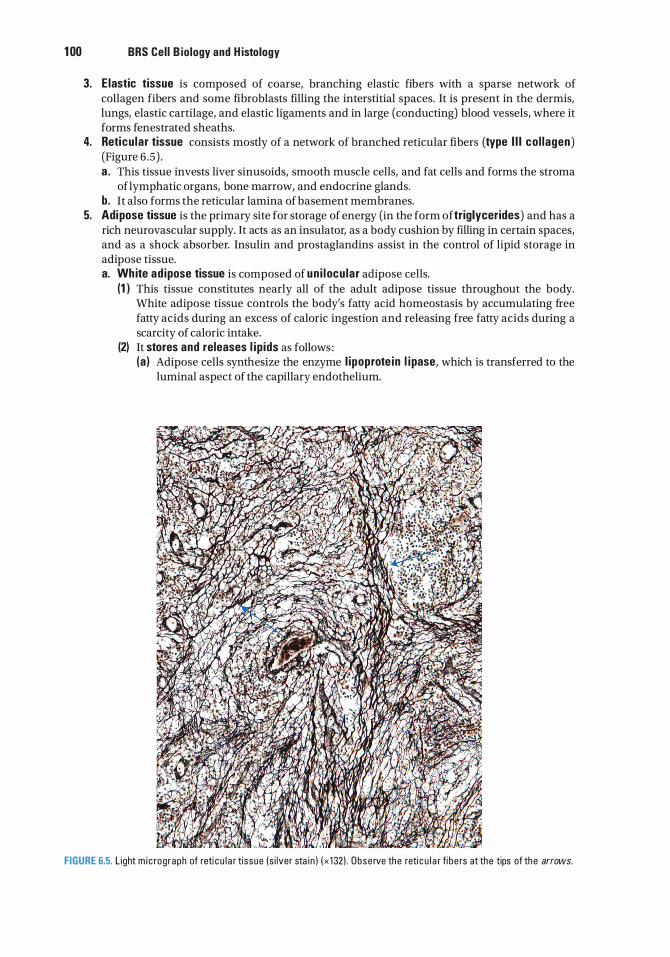
1 00 BRS Cel l B iology and H istology
3. E lastic tissue is composed of coarse, branching elastic fibers with a sparse network of collagen fibers and some fibroblasts filling the interstitial spaces. It is present in the dermis, lungs, elastic cartilage, and elastic ligaments and in large (conducting) blood vessels, where it forms fenestrated sheaths.
4. Reticu lar tissue consists mostly of a network of branched reticular fibers (type I l l co l lagen) (Figure 6 .5) . a . This tissue invests liver sinusoids, smooth muscle cells, and fat cells and forms the stroma
of lymphatic organs, bone marrow, and endocrine glands. b. It also forms the reticular lamina of basement membranes.
5. Adipose tissue is the primary site for storage of energy (in the form oftriglycerides) and has a rich neurovascular supply. It acts as an insulator, as a body cushion by filling in certain spaces, and as a shock absorber. Insulin and prostaglandins assist in the control of lipid storage in adipose tissue. a. Wh ite ad ipose tissue is composed of un i locu lar adipose cells.
(1 ) This tissue constitutes nearly all of the adult adipose tissue throughout the body. White adipose tissue controls the body's fatty acid homeostasis by accumulating free fatty acids during an excess of caloric ingestion and releasing free fatty acids during a scarcity of caloric intake.
(2) It stores and releases l ip ids as follows : (a ) Adipose cells synthesize the enzyme l ipoprote in l i pase, which is transferred to the
luminal aspect of the capillary endothelium.
FIGURE 6.5. L ight m i c rog raph of reti c u l a r tissue (s i lver sta i n ) ( x 1 32) . Obse rve the reti c u l a r fi b e rs at the tips of the arrows.
l!ii!!J1lliij Connective Tissue 1 01
(b ) Dietary fat is transported to adipose tissue as very- low-density l ipoprote ins and chylomicrons. Lipoprotein lipase then hydrolyzes these substances into fatty acids and glycerol.
(c) The free fatty acids enter the adipose cells, where they are re-esterified and stored as triglycerides (in fat droplets) . Adipose cells also synthesize fatty acids from glucose.
(d) Lipid storage is stimulated by insu l in , which increases the rate of synthesis of lipoprotein lipase and the uptake of glucose by adipose cells.
(e) Release of lipids is affected by neural impulses and/or adrenaline. Stored triglycerides are hydrolyzed by hormone-sensitive l ipase, which is activated by cyclic adenosine monophosphate. The free fatty acids are released into the ECM and then enter the capillary lumen.
(3) Wh ite ad ipose tissue is also an endocrine organ that produces a number of hormones known as ad ipokines . Some of these hormones, leptin, ad iponectin, resisti n, and retino l b ind ing prote in-4, are manufactured by adipocytes, whereas other hormones/factors, namely tumor necrosis factor-a and i nter leukin-6, are produced by the macrophages that reside in adipose tissue of obese individuals. It has been reported that obesity is always accompanied by chronic i nflammation, and inflammatory agents released in response to inflammation-damaged tissue elicit a recruitment of macrophages into the connective tissue stroma among the enlarged adipocytes. (a) Leptin is a protein hormone, produced primarily by adipocytes, which inhibits
appetite for extended periods of time by binding to the appetite increasing neuropeptide Y, thus suppressing the area of the hypothalamus that control feeding, and induces the regions of the hypothalamus that controls the disbursement of energy. Additionally, leptin also induces the synthesis and release of the appetiterepressing neuropeptide a-melanocyte-stimulating hormone. Individuals who have mutations in the leptin gene or in the receptors for leptin exhibit uncontrollable hunger and become obese as a result. The volume of each adipocyte and the number of adipocytes are greater in obese than in thin individuals; therefore, the blood leptin levels of obese individuals may be as much as seven times greater than those of thin individuals.
(b ) Ad iponectin is also a protein hormone produced only by unilocular adipocytes. This hormone increases insulin sensitivity, therefore, facilitates the uptake of glucose and the oxidation of fatty acids in skeletal muscle cells, and decreases gluconeogenesis and glucose release by hepatocytes. Thus, adiponectin regulates the body's energy metabolism and facilitates weight loss. The blood levels of this hormone are greater in thin than in obese individuals.
(c) Resistin is a peptide hormone that is manufactured by adipocytes in rodents but by macrophages in humans. It is suggested that this hormone induces insu l i n resistance, resulting in hyperglycemia and type I I diabetes mellitus in obese patients. Additionally, resistin contributes to the inflammatory response, a common finding in insulin resistance, obesity, and type II diabetes mellitus.
(d ) Retino l -b ind ing protein-4 is also produced by unilocular adipocytes, and it has been demonstrated to elevate insulin resistance, inflammation, and fatty liver disease with a concomitant increase in glucose output by hepatocytes.
(e ) Tumor necrosis factor-a (TNF-a) is manufactured by macrophages that reside in adipose tissues of obese individuals and is believed to be the principal cause of insulin resistance. Additionally, TNF-a also depresses liver cell's ability to oxidize fatty acids.
(f) l nter leukin-6 (l l-6) is also manufactured and released by macrophages in the connective tissue interstices of unilocular adipose tissue of obese individuals. Similar to tumor necrosis factor-a interleukin-6 increases insulin resistance but also enhances skeletal muscle cells' ability to take up glucose and oxidize fatty acids.
1 02 BRS Cel l B iology and H istology
CLIN ICAL CONSIDERATIONS
OBESITY has been re c ently re c l a ss ifi e d a s a d i sease . I n d iv id ua l s a re sa i d to be obese i f th e i r a d i pose ti ssue b u i l d u p is g re at enough that th e i r body
mass i ndex is g reater th a n 30 kg/m2 with a resu ltant d e c rease i n l ife s p an a n d a n i n c rease i n the pos s i b i l ity of a c q u i r i ng a g roup o f h e a lth p rob l ems refe rred to a s metabo l ic syndrome. I n su l i n res ista nce , type I I d i a b etes me l l itus, fatty l i v e r d i sease , a n d c a rd i ova s c u l a r d isease a re common ly i n c l u d e d u n d e r t h e r u b r i c o f metabo l i c syn d rome .
Obesity o c c u rs a s e ith e r hypertroph ic obesity, c h a ra cter ized by a n i n c rease i n a d i pose c e l l size resu lti ng from i n c reased fat sto rage ( adu lt onset), o r hyperce l lu lar (hyperplast ic) obesity, c h a ra cte rized by a n i n c rease in th e number of a d i p ose ce l l s that beg i n s in c h i l d hood a n d is usua l ly l i fe l o ng .
A genetic basis fo r obesity is t h e resu lt of m utati ons i n th e g e ne f o r t he ho rmone l e pti n o r i n th e genes for l e pt in re c e pto rs, th us p reventi ng the p ro d u ctio n of l e pt in o r p rod uc i n g a n i n a ctive form of th e ho rmone o r prod uc i n g i n a ctive l e pt in re c e ptors. S i n c e l e pti n fun cti ons in th e reg u l atio n of a ppe tite , p e rsons affe cted by e ith e r o f t h ese two cond it ions possess a n i n sati a b l e a p p etite , b r i n g i n g a b o ut u n restra i n ed we ight g a i n . The vo l u m e of e a c h a d i p o cyte a n d the n u m b e r of a d i p o cytes a re g re ater i n o b e se th a n i n t h i n i n d iv id u a ls; the refo re, t h e b l o o d l e pt in l eve ls o f o b e se i n d ivi d u a l s may be a s m u c h as seven times g re ater th a n i n th i n i n d iv id u a ls .
b. Brown ad ipose tissue is composed of multi locu lar adipose cells, which contain many large mitochondria. (1 ) This tissue is capable of generati ng heat by uncoup l ing oxidative phosphorylation .
Thermogenin, a transmembrane protein in mitochondria, causes the release of protons away from adenosine triphosphate synthesis, resulting in heat production.
(2) This tissue is found in infants (also in hibernating animals) and is much reduced in adults.
CLINICAL CONSIDERATIONS
1 . Ad ipose tumors may be e ith e r ben i g n o r m a l i g n a nt. Lipomas a re b en i g n fatty ti ssue tumo rs usua l ly fo u n d in s u b c uta neous c onnective
t issues of th e n e c k, b a c k, a n d p roxima l re g i ons of the l imbs of m i d d l e - a ged a n d e l d e r ly pe rsons . 2. Liposarcomas a re th e most common ma l i g n a nt a d i pose tu mo rs . Alth ough l i posa rcomas a re
most fre q uently l o c ated in the l e g a n d/o r the retrope rito nea l tissues , they a re not restri cted to th ese sites . L iposa rcomas a re d iffi c u lt to d i a g nose s i n c e they resemb l e l i p omas . Ad i po cytes of the m a l i g n a nt tissue resem b l e e ith e r u n i l o c u l a r o r m u lti l o c u l a r a d i p o cytes . P resently, c h romosome ma rke rs a re used to d iffe renti a l ly d i a g nose l i posa rcomas .
CLINICAL CONSIDERATIONS
I r is in . When a n i n d ivi d u a l i s do i n g physi c a l exe rc ises , h i s/h e r ske leta l musc l e c e l l s re l ease the ho rmone i r is in that not o n ly converts c e rta i n
u n i l o c u l a r a d i p o cytes i nto mu lti l o c u l a r a d i p o cytes b ut a l so e n h a n c es the m a i nte n a n c e of n e u romus cu l a r syna pses .
C. Specia l ized connective tissue 1. Cartilage and bone are discussed in Chapter 7. 2. Blood is discussed in Chapter 10.
Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which one of the following statements regarding collagen is true?
(A) It is composed of tropocollagen. (B ) Reticular fibers are composed of type II
collagen. (C) It is synthesized mostly by mast cells. (D ) Elastic fibers are composed of type IV
collagen. (E) Type II collagen is most common in
connective tissue proper.
2. Dense regular connective tissue is present in
(A) capsules of organs. (B ) basement membrane. (C) tendons. (D ) skin. (E ) dermis.
3. Of the following cell types found in connective tissue, which is most often present along capillaries and resembles fibroblasts?
(A) Plasma cell (B ) Lymphocyte (C ) Macrophage (D ) Mast cell (E) Pericyte
4. Synovial fluids of normal joints are usually devoid of collagen. Patients with rheumatoid diseases have various types of collagen in their synovial fluid, depending on the tissue being damaged. If a patient has type II collagen in the synovial joint, which of the following tissues is being eroded?
(A) Vascular endothelium (B ) Compact bone (C) Vascular smooth muscle (D ) Articular cartilage (E ) Synovial membrane
5. Which one of the following cell types arises from monocytes?
(A) Plasma cells (B ) Fibroblasts (C) Lymphocytes (D ) Macrophages (E) Mast cells
6. Foreign body giant cells are formed by the coalescence of
(A) macrophages. (B) lymphocytes. (C) fibroblasts. (D ) adipose cells. (E) plasma cells.
7. Which one of the following cell types in the connective tissue arises from myeloid stem cells?
(A) Pericytes (B ) Eosinophils (C) Fibroblasts (D ) Osteoblasts (E) Adipocytes
8. Which of the following cell types is responsible for anaphylactic shock?
(A) Fibroblasts (B ) Eosinophils (C) Pericytes (D) Mast cells (E) Macrophages
1 03
1 04 BRS Cel l B iology and H istology
9. Which one of the following statements regarding proteoglycans is true?
(A) They consist of a core of fibrous protein covalently bound to glycoproteins.
(B ) They are attached to ribonucleic acid. (C) They are binding sites for deoxyribonucleic
acid. (D ) They are composed of a protein core to
which glycosaminoglycans are attached. (E ) They are the exclusive substance of the
ECM along with collagen.
1 0. Which one of the following statements concerning loose connective tissue is true?
(A) It is less abundant than dense connective tissue.
(B ) It has a lower proportion of cells to fibers than does dense connective tissue.
(C ) It acts as a medium for exchange of nutrients and wastes between the blood and tissues.
(D) It provides structural support for organs. (E) It consists of many fibers in which various
types of cells are embedded.
Answers and Explanations
1 . A. Collagen is composed of closely packed tropocollagen molecules. Reticular fibers are composed of type III collagen, whereas elastic fibers are composed of elastin micro fibrils rather than collagen. Fibrocytes are inactive nonsecreting fibroblasts that synthesize the pro collagen molecules (see Chapter 6 II B 1 ) .
2. C. Tendons are composed of dense regular connective tissue containing collagen fibers arranged in a uniform parallel fashion (see Chapter 6 IV B 2) .
3. E. Pericytes are pluripotential cells that resemble fibroblasts, although they are smaller, and are adjacent to capillaries (see Chapter 6 III B) .
4. D . Type II collagen is present only in hyaline and elastic cartilages; therefore, finding type II collagen in the synovial fluid of a joint indicates erosion of the articular cartilage (see Chapter 6 II B 1 ) .
5. D . Monocytes leave the bloodstream and migrate into the connective tissue, where they mature into functional macrophages (see Chapter 6 III E) .
6. A. Foreign body giant cells result when macro phages coalesce (see Chapter 6 III E 3 ) .
7. B . Eosinophils arise from myeloid stem cells during hemopoiesis and migrate to sites of inflammation within the connective tissue. Pericytes, fibroblasts, osteoblasts, and adipocytes arise from undifferentiated mesenchymal cells (see Chapter 6 III H 2) .
8. D . After first exposure to an allergen, plasma cells make IgE antibodies that bind to FceRI receptors on mast cells (and basophils), sensitizing them. At the second exposure, the allergen binds to IgE, initiating degranulation of mast cells and releasing several mediators that give rise to type I hypersensitivity reaction (see Chapter 6 III D 4).
9. D . Proteoglycans consist of a protein core to which glycosaminoglycans are attached (see Chapter 6 II A).
1 0. C. Both loose and dense connective tissues are composed of three elements : an amorphous ground substance, fibers, and various types of cells. The amorphous ground substance of loose connective tissue is the medium of exchange between the connective tissue cells and the bloodstream (see Chapter 6 IV B 1 ) .
1 05
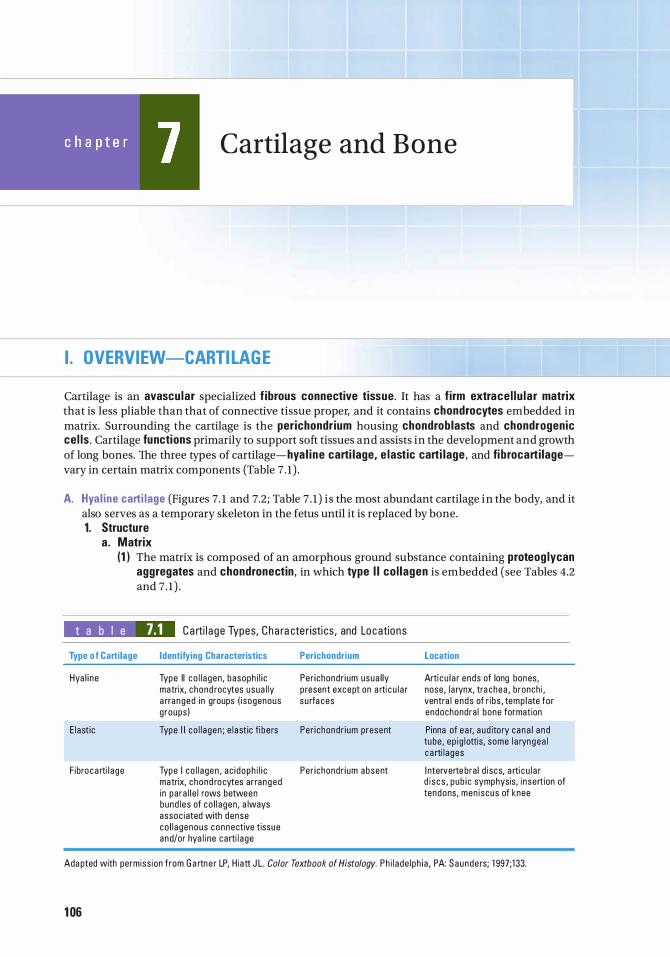
Cartilage and B one
I. OVERVIEW-CARTILAGE
Cartilage is an avascu lar specialized f ibrous connective tissue. It has a f irm extrace l lu lar matrix that is less pliable than that of connective tissue proper, and it contains chondrocytes embedded in matrix. Surrounding the cartilage is the perichondrium housing chondrob lasts and chondrogenic cel ls . Cartilage functions primarily to support soft tissues and assists in the development and growth of long bones. The three types of cartilage- hya l ine carti lage, e lastic carti lage, and fi brocartilagevary in certain matrix components (Table 7 . 1 ) .
A. Hya l ine carti lage (Figures 7. 1 and 7.2; Table 7 . 1 ) i s the most abundant cartilage in the body, and it also serves as a temporary skeleton in the fetus until it is replaced by bone. 1. Structure
a . Matrix (1 ) The matrix is composed of an amorphous ground substance containing proteog lycan
aggregates and chondronectin, in which type I I co l lagen is embedded (see Tables 4.2 and 7 . 1 ) .
t a b I e 7.1 Ca rti l a ge Types, C ha ra cte r isti cs, and Locations
Type o f Cartilage
Hya l i ne
E l ast ic
F ibro c a rti l a ge
Identifying Characteristics
Type II c o l l a gen, basoph i l i c matrix, chond rocytes usua l ly a rra nged i n groups ( i sogenous g roups )
Type I I co l l a gen ; e l a st ic fi be rs
Type I co l l a gen , ac i doph i l i c matrix, chond ro cytes ar ra nged i n pa ra l l e l rows between bund l es of co l l a gen, a lways assoc iated with dense co l l a genous connective tissue and/or hya l i ne c a rti l a ge
Perichondrium
Per i chondr i um usua l ly p resent except on a rti c u l a r s u rfa ces
Per i chondr i um present
Per i chondr i um absent
Location
Arti c u l a r ends of long bones, nose, l a rynx, tra chea , bronch i , ventra l ends of r ibs , temp l ate for endochondra l bone formation
Pinna of e a r, a ud ito ry c ana l a n d tu be, ep i g l ottis, some l a ryngea l c a rti l a ges
I nterverte bra l d i scs, a rti c u l a r d i s c s , pub i c symphysis, i nsert ion of tendons, men i scus of knee
Ada pted with permiss ion f rom G a rtne r LP, H iatt J L. Color Textbook of Histology. Ph i l ade l ph i a , PA: Saunde rs; 1 997;1 33.
1 06
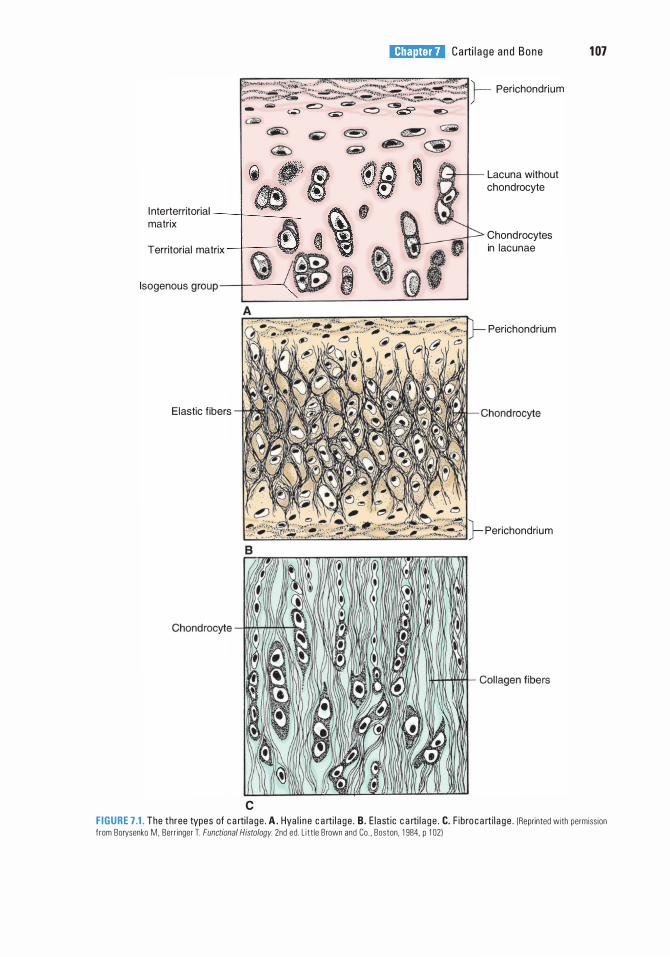
l!ilDttm Carti l a g e and Bone 1 07
;��;����;:��;§�$,?;ift!�;f���� }- Perichondrium
- = � = c:::> G.5" @::> aiil>
<iiW �
ieiJfr m f10 1 s · (!] l nterterritorial ---r---___,_ . f matrix � ,� -+--- � ... • Territorial matrix �
lsogenous group--+-i __ --z 13 �
Elastic f ibers
c
Lacuna without chondrocyte
Chondrocytes in lacunae
Perichondrium
Perichondrium
F IGURE 7.1. The three types of c a rti l a ge . A. Hya l i n e c a rti l a ge . B. E l astic c a rti l a ge . C. F ibro c a rti l a g e . (Reprinted with permiss ion from Borysenko M. Berr inger l Functional Histology. 2nd ed . L itt le Brown and Co . . Boston, 1 984, p 1 02)
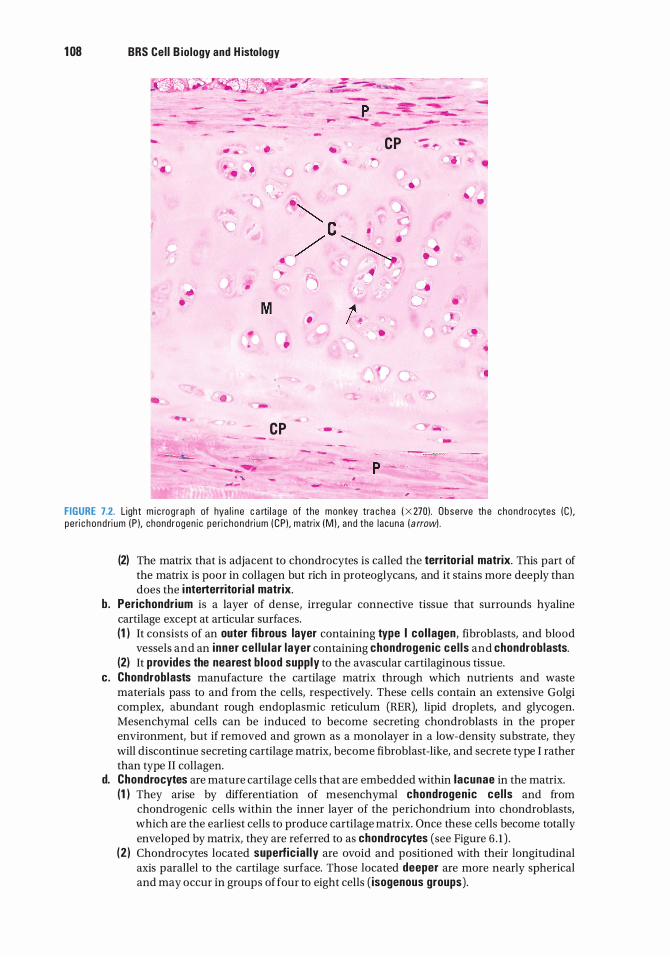
1 08 BRS Cel l B iology and H istology
� - - -
... . . •
-
• ..
-•
•
•
•
•
� c / M
•
•
CP - -
"':"-· -
1 .
- - -
CP - '=" . ,.
•
•
•
• •
• •
• •
•
-
p �
FIGURE 7.2. L ight m i c rog raph of hya l i n e c a rti l a g e of the monkey tra chea ( X 270) . Obse rve th e chond rocytes (C ) , pe ri c hond ri um ( P ), chondrogen ic pe ri c hond ri um ( CP) , m atrix (M ) , a nd the l acuna ( a rrow) .
(2) The matrix that is adjacent to chondrocytes is called the territor ia l matrix. This part of the matrix is poor in collagen but rich in proteoglycans, and it stains more deeply than does the i nterterritor ia l matrix.
b . Perichondrium is a layer of dense, irregular connective tissue that surrounds hyaline cartilage except at articular surfaces. (1 ) It consists of an outer fi brous layer containing type I co l lagen, fibroblasts, and blood
vessels and an inner ce l lu lar layer containing chondrogenic ce l ls and chondroblasts. (2) It provides the nearest b lood supply to the avascular cartilaginous tissue.
c. Chondroblasts manufacture the cartilage matrix through which nutrients and waste materials pass to and from the cells, respectively. These cells contain an extensive Golgi complex, abundant rough endoplasmic reticulum (RER), lipid droplets, and glycogen. Mesenchymal cells can be induced to become secreting chondroblasts in the proper environment, but if removed and grown as a monolayer in a low-density substrate, they will discontinue secreting cartilage matrix, become fibroblast-like, and secrete type I rather than type II collagen.
d. Chondrocytes are mature cartilage cells that are embedded within lacunae in the matrix. (1 ) They arise by differentiation of mesenchymal chondrogen ic ce l ls and from
chondrogenic cells within the inner layer of the perichondrium into chondroblasts, which are the earliest cells to produce cartilage matrix. Once these cells become totally enveloped by matrix, they are referred to as chondrocytes (see Figure 6 . 1 ) .
(2 ) Chondrocytes located superfic ia l ly are ovoid and positioned with their longitudinal axis parallel to the cartilage surface. Those located deeper are more nearly spherical and may occur in groups of four to eight cells ( isogenous groups).
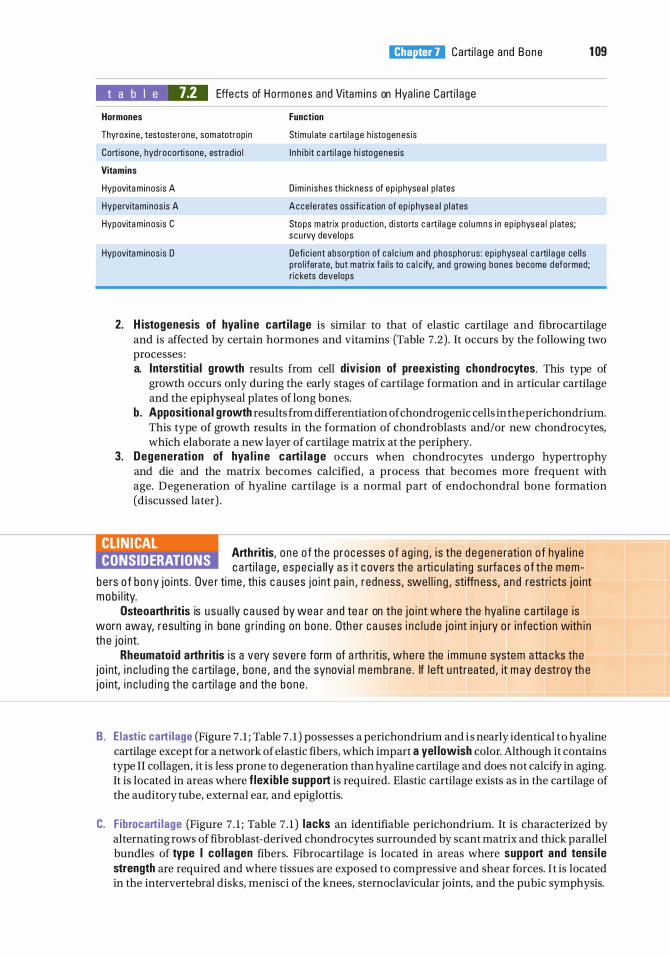
l!iitJ'!1tiii Carti l a ge and Bone 1 09
t a b I e 7.2 Effe cts of Ho rmones and Vitam i n s on Hya l i ne Carti l age
Hormones
Thyroxine , testoste rone, somatotrop in
Cortisone , hyd rocortisone , estra d io l
Vitamins
Hypovita m inosis A
Hypervitaminos is A
Hypovita m inosis C
Hypovita m inos is D
Function
Stimu l ate c a rti l a g e h istogenesis
I n h i b it c a rti l a ge h i stogenes is
D im in i shes th ickness of ep i physea l p l ates
Acce l e rates ossif ic ation of ep i physea l p l ates
Stops matrix production , d i sto rts c a rti l a g e co l umns i n ep i physea l p l ates; s cu rvy deve lops
Defi c i ent abso rption of c a l c i um and phosphorus : ep i physea l c a rti l a ge ce l l s p ro l iferate, but matrix fa i l s to c a l c ify, and g rowing bones become d eformed; r ic kets develops
2. H istogenesis of hya l i ne carti lage is similar to that of elastic cartilage and fibrocartilage and is affected by certain hormones and vitamins (Table 7.2) . It occurs by the following two processes : a. Interstit ia l growth results from cell divis ion of preexisting chondrocytes. This type of
growth occurs only during the early stages of cartilage formation and in articular cartilage and the epiphyseal plates of long bones.
b. Appositiona I growth results from differentiation of chondrogenic cells in the perichondrium. This type of growth results in the formation of chondroblasts and/or new chondrocytes, which elaborate a new layer of cartilage matrix at the periphery.
3. Degenerati on of hya l i ne carti l age occurs when chondrocytes undergo hypertrophy and die and the matrix becomes calcified, a process that becomes more frequent with age. Degeneration of hyaline cartilage is a normal part of endochondral bone formation (discussed later) .
CLIN ICAL CONSIDERATIONS
Arthritis, one o f th e p roc esses o f a g i n g , i s the d e gene rati on o f hya l i n e c a rti l a g e, e spec i a l ly a s i t c overs th e a rti c u lati ng s u rfa ces o f t he mem
be rs o f b ony jo i nts . Ove r time , th is c a uses j o int pa i n , redn ess, swe l l i n g , stiffness, a n d restri cts j o i nt mob i l ity.
Osteoarthritis is u s ua l ly c a used by wea r a n d te a r on the j o i nt where the hya l i n e c a rti l a g e is worn away, resu lti ng i n bone g ri n d i n g on bone . Oth e r c a uses i n c l u d e j o i nt i n j u ry o r i nfecti on with i n th e j o i nt.
Rheumatoid arthritis i s a very severe form of a rth rit is, where the immune system atta c ks the j o i nt, i n c l u d i n g the c a rti l a ge , bone , a n d th e synovi a l mem b ra n e . If l eft u ntreated , it m ay destroy th e j o i nt, i n c l u d i n g the c a rti l a g e a n d th e bone .
B. E lastic carti lage (Figure 7 . 1 ; Table 7 . 1 ) possesses a perichondrium and i s nearly identical to hyaline cartilage except for a network of elastic fibers, which impart a yel lowish color. Although it contains type II collagen, it is less prone to degeneration than hyaline cartilage and does not calcify in aging. It is located in areas where f lex ib le support is required. Elastic cartilage exists as in the cartilage of the auditory tube, external ear, and epiglottis.
C. Fibrocarti lage (Figure 7 . 1 ; Table 7 . 1 ) lacks an identifiable perichondrium. It is characterized by alternating rows of fibroblast-derived chondrocytes surrounded by scant matrix and thick parallel bundles of type I co l lagen fibers. Fibrocartilage is located in areas where support and tens i le strength are required and where tissues are exposed to compressive and shear forces. I t is located in the intervertebral disks, menisci of the knees, sternoclavicular joints, and the pubic symphysis.
1 1 0 BRS Cel l B iology and H istology
Bone is the primary constituent of the adult skeleton. It is a specialized type of connective tissue with a calcified extracellular matrix in which characteristic cells are embedded. Bone functions to support and protect vital organs, and fleshy structures, as a hemopoiesis organ, and provides a storage site for phosphate and calcium (bone contains about 99% of the body's calcium). Secondarily, it functions to regulate blood calcium levels via input from two separate non bony tissues. Parathyroid hormone (PTH) from the parathyroid gland acts to increase calcium levels in the blood, whereas calcitonin secreted by the parafollicular cells (C cells) of the thyroid gland decreases calcium levels in the blood. Thus, the activities of these two substances on the calcium levels in bone are responsible for maintaining the proper blood calcium level. Bone is also a dynamic tissue that constantly undergoes changes in shape, such that applied pressure results in bone resorption, whereas applied tension results in bone formation.
A. Structure 1 . Bone matrix
a . The inorganic (calc ified) portion of the bone matrix (about 65% of the dry weight) is composed of calcium, phosphate, bicarbonate, citrate, magnesium, potassium, and sodium. It consists primarily of hydroxyapatite crysta ls, which have the composition Ca10(P04)s(OH)2•
b. The organ ic portion of the bone matrix (about 35% of the dry weight) consists primarily of type I co l lagen (95%) and a minor contribution of type V col lagen . It has a ground substance that contains chondroitin su lfate, keratan su lfate, and hya luron ic ac id . (1 ) Osteocalcin, stimulated by vitamin D, inhibits osteoblast function, and osteopontin,
both glycoproteins, binds to hydroxyapatite and to integrins on osteoblasts and osteoclasts. Osteonectin, produced mostly by osteoblasts, is located in bone undergoing remodeling. Cytokines, growth hormones, and bone morphogenic proteins (BMPs), among others contribute to the bone matrix.
(2) Bone sialoprotein is a matrix protein that also binds to integrins of the osteoblasts and osteocytes and is thus related to adherence of bone cells to bone matrix.
2. The periosteum is a layer of noncalc if ied connective tissue covering bone on its external surfaces, except at synovial articulations and muscle attachments. a. It is composed of an outer dense f ibrous collagenous layer and an inner cellular
osteoprogenitor (osteogenic) layer. b. Sharpey f ibers (type I collagen) attach the periosteum to the bone surface. c. The periosteum functions to distribute blood vessels to bone.
3. The endosteum is a thin specialized connective tissue that lines the marrow cavities and supplies osteoprogenitor cel ls and osteoblasts for bone growth and repair.
B. Bone ce l ls 1 . Osteoprogen itor ce l ls
a . These spindle-shaped cells are derived from embryonic mesenchyme and are located in the periosteum and the endosteum, and persist throughout l ife as stem ce l ls that l i ne bone . They can be activated later for bone repair of fractures or other repair .
b . They are capable of differentiating into osteoblasts. However, at low oxygen tensions, they may change i nto chondrogenic cel ls .
2. Osteoblasts a. Osteoblasts are derived from osteoprogenitor cells under the influence of members of
the BMP fami ly and also transforming growth factor-�. They possess receptors for PTH (see Chapter 13 V). Osteoblasts are responsible for the synthesis of organic protein components of bone matrix, including type I collagen, proteoglycans, and glycoproteins, which they secrete as osteoid (uncalcified bone matrix), which is mineralized under the influence and control by the osteoblasts. Additionally, they produce macrophage colonystimulating factor (M-CSF), a receptor for the activation of nuclear factor kappa B (RANKL),
l!iitJ'!1tiii Carti l a g e and Bone 1 1 1
osteoprotegerin, osteocalc in (for bone mineralization), osteopontin (for formation of sealing zone between osteoclasts and the subosteoclastic compartment), osteonectin (related to bone mineralization), and bone s ia loprote in (binding osteoblasts to extracellular matrix) .
b. On bony surfaces, they resemble a layer of cuboidal, basophilic cells as they secrete organic matrix (see Figure 6 . 1 ) .
c. They possess cytoplasmic processes with which they contact the processes of other osteoblasts and osteocytes and form gap junctions.
d . When synthetical ly active, they have a well-developed RER and Golgi complex. e. These cells become entrapped in lacunae, but maintain contact with other cells via their
cytoplasmic processes. Entrapped osteoblasts are known as osteocytes. 3. Osteocytes (Figure 7.3)
a. Osteocytes are mature bone cel ls housed in their own lacunae. b. They have narrow cytoplasmic processes that extend through canal icu l i in the calcified
matrix (see Figures 6 . 1 and 7.3) . c. They maintain communication with each other via gap junctions between their processes. d . They are nourished and maintained by nutrients, metabolites, and signal molecules carried
by the extracellular fluid that flows through the lacunae and canaliculi. In addition, calcium released from bone enters the extracellular fluid located within these spaces.
e. They contain abundant heterochromatin, a paucity of RER, and a small Golgi complex. 4. Osteoclasts
a. Overview. Osteoclasts are large, motile, multinucleated cells (up to 50 nuclei) that resorb bone. They are derived from cells of the mononuclear-phagocyte system, comprising blood-borne monocytes that enter the connective tissue spaces where they differentiate into various types of macrophages and osteoclasts (see Section (3)) . (1 ) Osteoclasts possess cell surface receptors : colony-stimulating factor- 1 receptor,
calcitonin receptor, and RANK (nuclear factor kappa B) . (2) Osteoblasts that have been stimulated by PTH promote osteoclast formation, whereas
osteoblasts that have been stimulated by calcitonin inhibit osteoclast formation by stimulating osteoid synthesis and calcium deposition.
(3) Via a series of three osteoblast signals, osteoclast precursors (macrophages) are stimulated by M-CSF to undergo mitosis. Another signaling molecule, RANKL, binds to the precursor, inducing it to differentiate into the multinucleated osteoclast, thus activating it to commence bone resorption. A third signal, osteoproteger in (OPG), a member of the tumor necrosis factor receptor (TNFR) family produced by osteoblasts and other cells, can prohibit RANKL from binding to the macrophage, thus prohibiting osteoclast formation.
b. Osteoclast cytoplasm is acidoph i l ic . Osteoclasts function in the resorption of bone (osteolysis). They form and reside in depressions known as Howship lacunae, which represent areas of bone resorption.
c. Morphology. Osteoclasts activated by osteoclast-stimulat ing factor produced and released by osteoblasts display four regions in electron micrographs. (1 ) Basal zone is that part of the osteoclast housing most of the organelles and is the
farthest from the subosteoclastic compartment. (2) The ruffled border is the site of active bone resorption. It is composed of irregular
fingerlike cytoplasmic projections extending into the subosteoclastic compartment, a slight depression that deepens as the osteoclast resorbs bone and then that depression is referred to as Howship lacuna . The ruffled border of an inactive osteoclast is collapsed as the cell is in a resting stage.
(3) The clear zone surrounds the ruffled border. It contains actin filaments at the periphery that help osteoclasts maintain contact with the bony surface. This isolates and seals the region of osteolytic activity. Further, osteopontin, secreted by osteoblasts, is used to seal the zone between osteoclasts and the subosteoclastic compartment.
(4) The vesicular zone contains exocytotic vesicles that transfer lysosomal enzymes to Howship lacunae and endocytotic vesicles that transfer degraded bone products from Howship lacunae to the interior of the cell.
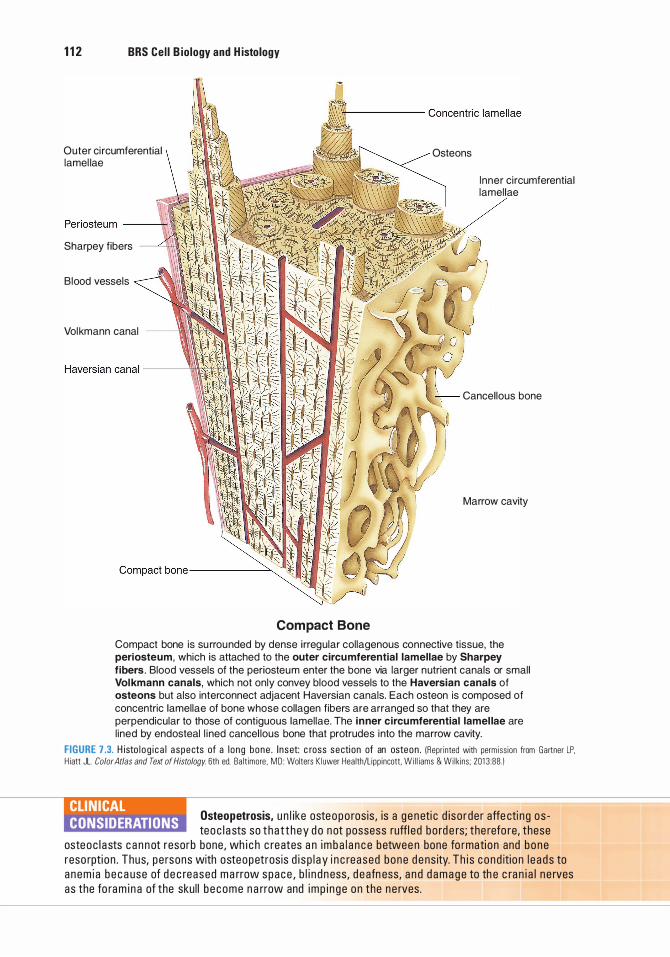
1 1 2 BRS Cel l B iology and H istology
Outer ci rcumferential lamel lae
Sharpey fibers
Blood vessels
Volkmann canal
Compact Bone
Osteons
Inner ci rcumferential lamellae
Cancel lous bone
Marrow cavity
Compact bone is su rrounded by dense i rregular collagenous connective tissue, the periosteum, which is attached to the outer circumferential lamellae by Sharpey
fibers . Blood vessels of the periosteum enter the bone via larger nutrient canals or small Volkmann canals, which not only convey blood vessels to the Haversian canals of osteons but also interconnect adjacent Haversian canals. Each osteon is composed of concentric lamellae of bone whose collagen fibers are arranged so that they are perpendicular to those of contiguous lamellae. The inner circumferential lamel lae are l ined by endosteal l i ned cancel lous bone that protrudes into the marrow cavity.
FIGURE 7.3. H isto l o g i c a l aspects of a l ong bone . I n set: c ross secti on of an osteon . (Repr inted with perm iss ion from Gartner LP. H iatt JL. Color Atlas and Text of Histology. 6th ed. Ba lt imore , MD: Wolters K luwer Hea lth/L ipp incott, Wi l l iams & Wi lkins ; 201 3 :88 . 1
CLINICAL CONSIDERATIONS
Osteopetrosis, un l ike osteopo ros is , is a g e neti c d i so rde r affe cti n g os teoc l a sts so t ha t t hey d o not possess ruffl ed bo rd e rs; the refo re, these
osteoc l a sts c a n n ot resorb bone , wh i c h c reates a n i m b a l a n c e betwee n bone fo rmati on and bone reso rpti on . Thus, pe rsons with osteopetrosis d i s p l ay i n c reased bone d e ns ity. Th i s c ond itio n l e a ds to a nem i a b e c a use of d e c reased ma rrow space , b l i n d n ess, d e afn ess, a n d d a m a g e to th e c ra n i a l n e rves as the fo ram i n a of the sku l l b e come n a rrow and imp i n ge on the n e rves .
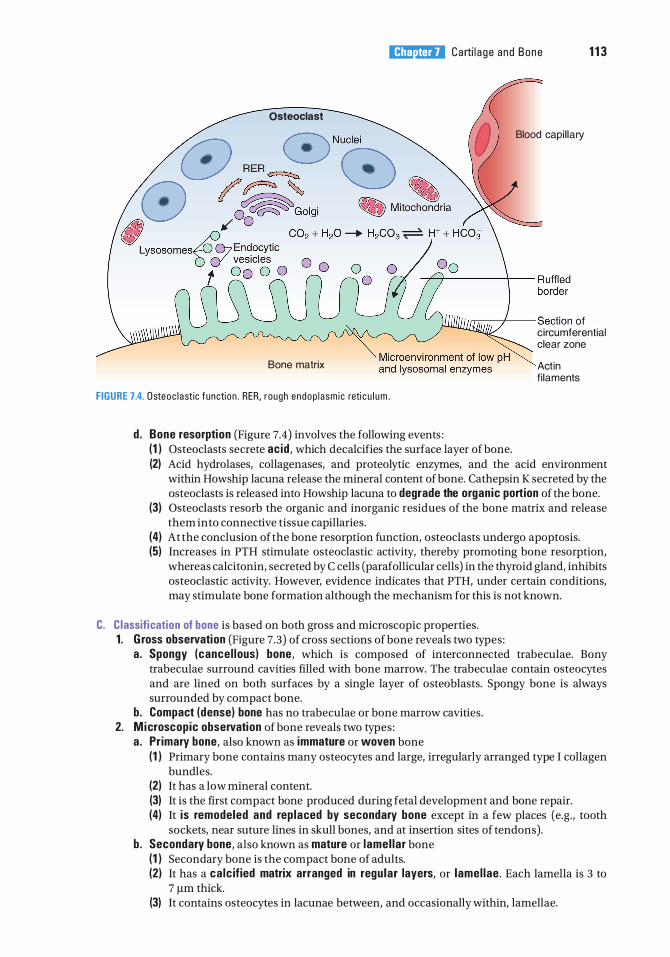
l!iitJ'!1tiii Carti l a g e and Bone 1 1 3
Osteoclast
Blood capi l lary
J,..,-;;-:----1-- Section of
Bone matrix
FIGURE 7.4. Osteoc l a stic function . RER, rough endop l a sm ic reti c u l u m .
d . Bone resorption (Figure 7.4) involves the following events : (1 ) Osteoclasts secrete acid , which decalcifies the surface layer of bone.
circumferential clear zone
Actin f i laments
(2) Acid hydrolases, collagenases, and proteolytic enzymes, and the acid environment within Howship lacuna release the mineral content of bone. Cathepsin K secreted by the osteoclasts is released into Howship lacuna to degrade the organic portion of the bone.
(3) Osteoclasts resorb the organic and inorganic residues of the bone matrix and release them into connective tissue capillaries.
(4) At the conclusion of the bone resorption function, osteoclasts undergo apoptosis. (5) Increases in PTH stimulate osteoclastic activity, thereby promoting bone resorption,
whereas calcitonin, secreted by C cells (parafollicular cells) in the thyroid gland, inhibits osteoclastic activity. However, evidence indicates that PTH, under certain conditions, may stimulate bone formation although the mechanism for this is not known.
C. Classification of bone is based on both gross and microscopic properties. 1. G ross observation (Figure 7.3) of cross sections of bone reveals two types :
a. Spongy (cancel lous) bone, which is composed of interconnected trabeculae. Bony trabeculae surround cavities filled with bone marrow. The trabeculae contain osteocytes and are lined on both surfaces by a single layer of osteoblasts. Spongy bone is always surrounded by compact bone.
b. Compact (dense) bone has no trabeculae or bone marrow cavities. 2. Microscopic observation of bone reveals two types :
a. Primary bone, also known as immature or woven bone (1 ) Primary bone contains many osteocytes and large, irregularly arranged type I collagen
bundles. (2) It has a low mineral content. (3) It is the first compact bone produced during fetal development and bone repair. (4) It is remodeled and rep laced by secondary bone except in a few places (e.g., tooth
sockets, near suture lines in skull bones, and at insertion sites of tendons). b . Secondary bone, also known as mature or lamel lar bone
(1 ) Secondary bone is the compact bone of adults. (2) It has a calc ified matrix arranged in regu lar layers, or lamel lae . Each lamella is 3 to
7 IJ,m thick. (3) It contains osteocytes in lacunae between, and occasionally within, lamellae.
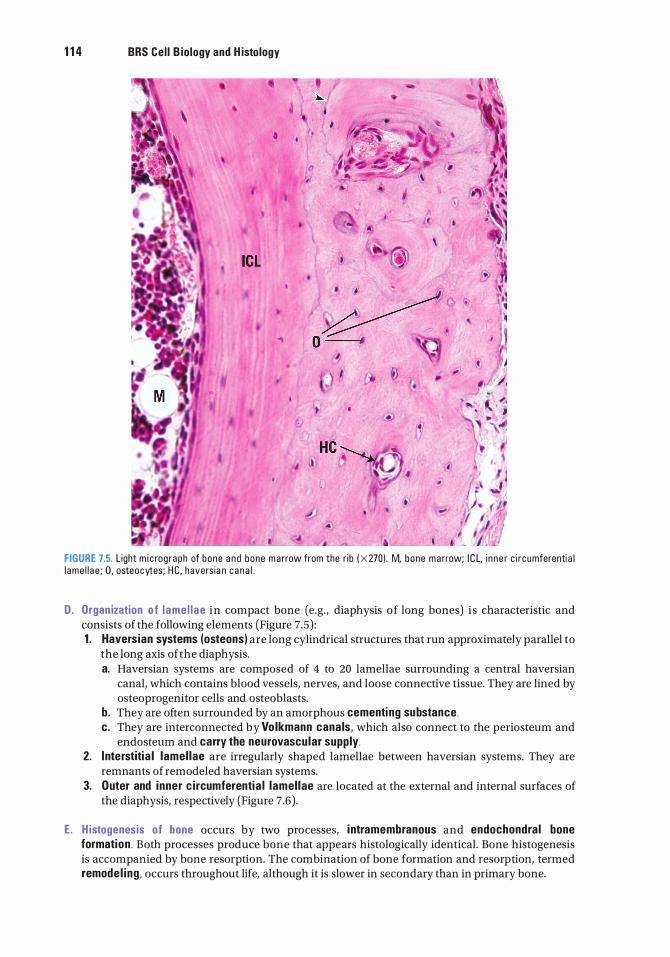
1 1 4 BRS Cel l B iology and H istology
�. Q --1
I I
I
• •
HC
...
•
FIGURE 7.5. L ight m i c rog raph of bone a n d bone m a rrow from the r ib ( X 270) . M, bone m a rrow; I C L, i n n e r c i r cumferenti a l l ame l l a e ; 0, osteocytes; H C, havers ia n c a n a l .
D. Organ ization o f l ame l l ae in compact bone (e.g., diaphysis of long bones) i s characteristic and consists of the following elements (Figure 7 .5) : 1 . Haversian systems (osteons) are long cylindrical structures that run approximately parallel to
the long axis of the diaphysis. a. Haversian systems are composed of 4 to 20 lamellae surrounding a central haversian
canal, which contains blood vessels, nerves, and loose connective tissue. They are lined by osteoprogenitor cells and osteoblasts.
b. They are often surrounded by an amorphous cementi ng substance . c . They are interconnected by Vo lkmann canals, which also connect to the periosteum and
endosteum and carry the neurovascular supply. 2. I nterstitia l lamel lae are irregularly shaped lamellae between haversian systems. They are
remnants of remodeled haversian systems. 3. Outer and inner c i rcumferentia l lamel lae are located at the external and internal surfaces of
the diaphysis, respectively (Figure 7.6) .
E. H istogenesis of bone occurs by two processes, i ntramembranous and endochondral bone formation . Both processes produce bone that appears histologically identical. Bone histogenesis is accompanied by bone resorption. The combination of bone formation and resorption, termed remode l ing , occurs throughout life, although it is slower in secondary than in primary bone.
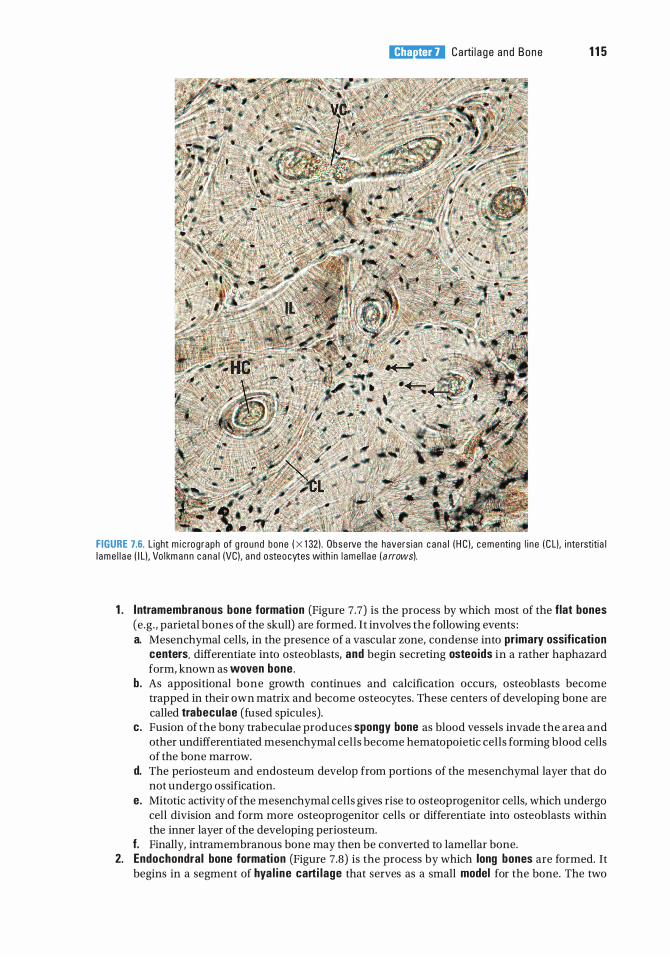
l!iitJ'!1tiii Carti l a g e and Bone 1 1 5
FIGURE 7.6. L ight m i c rog raph of g round bone ( x 1 32) . Obse rve the havers ian c a n a l ( H C) , c ementi ng l i n e ( C L). i nte rstiti a l l ame l l a e ( I L) , Vo l km a n n c a n a l (VC). a n d osteocytes with in l ame l l a e ( a rrows).
1 . I ntramembranous bone formation (Figure 7.7) is the process by which most of the flat bones (e .g . , parietal bones of the skull) are formed. It involves the following events : a. Mesenchymal cells, in the presence of a vascular zone, condense into primary ossification
centers, differentiate into osteoblasts, and begin secreting osteoids in a rather haphazard form, known as woven bone .
b . As appositional bone growth continues and calcification occurs, osteoblasts become trapped in their own matrix and become osteocytes. These centers of developing bone are called trabeculae (fused spicules).
c. Fusion of the bony trabeculae produces spongy bone as blood vessels invade the area and other undifferentiated mesenchymal cells become hematopoietic cells forming blood cells of the bone marrow.
d. The periosteum and endosteum develop from portions of the mesenchymal layer that do not undergo ossification.
e. Mitotic activity of the mesenchymal cells gives rise to osteoprogenitor cells, which undergo cell division and form more osteoprogenitor cells or differentiate into osteoblasts within the inner layer of the developing periosteum.
f. Finally, intramembranous bone may then be converted to lamellar bone. 2. Endochondral bone formation (Figure 7.8) is the process by which long bones are formed. It
begins in a segment of hya l ine carti lage that serves as a small model for the bone. The two
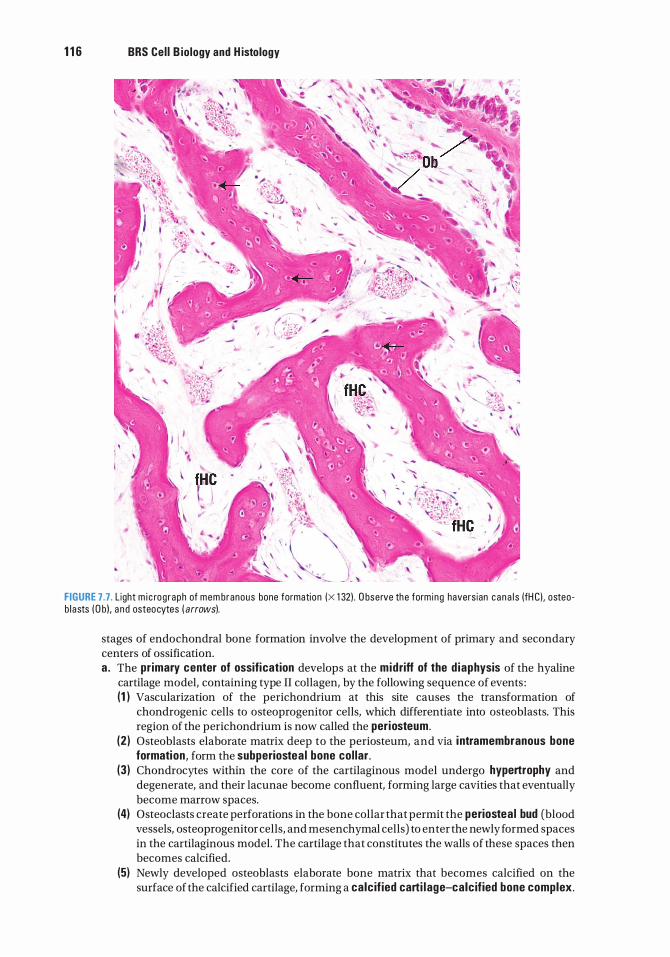
1 1 6 BRS Cel l B iology and H istology
FIGURE 7.7 . L ight m i c rog raph of mem branous bone formati on (X 1 321 . O bserve the form ing havers ian c ana l s (fH Cl . osteob l asts ( O bi . a n d osteocytes ( arrows).
stages of endochondral bone formation involve the development of primary and secondary centers of ossification. a . The primary center of ossification develops at the midriff of the d iaphysis of the hyaline
cartilage model, containing type II collagen, by the following sequence of events : (1 ) Vascularization of the perichondrium at this site causes the transformation of
chondrogenic cells to osteoprogenitor cells, which differentiate into osteoblasts. This region of the perichondrium is now called the periosteum.
(2) Osteoblasts elaborate matrix deep to the periosteum, and via i ntramembranous bone formation, form the subperiostea l bone col lar .
(3) Chondrocytes within the core of the cartilaginous model undergo hypertrophy and degenerate, and their lacunae become confluent, forming large cavities that eventually become marrow spaces.
(4) Osteoclasts create perforations in the bone collar that permit the periostea l bud (blood vessels, osteoprogenitor cells, and mesenchymal cells) to enter the newly formed spaces in the cartilaginous model. The cartilage that constitutes the walls of these spaces then becomes calcified.
(5) Newly developed osteoblasts elaborate bone matrix that becomes calcified on the surface of the calcified cartilage, forming a calc if ied carti lage-calc ified bone complex.
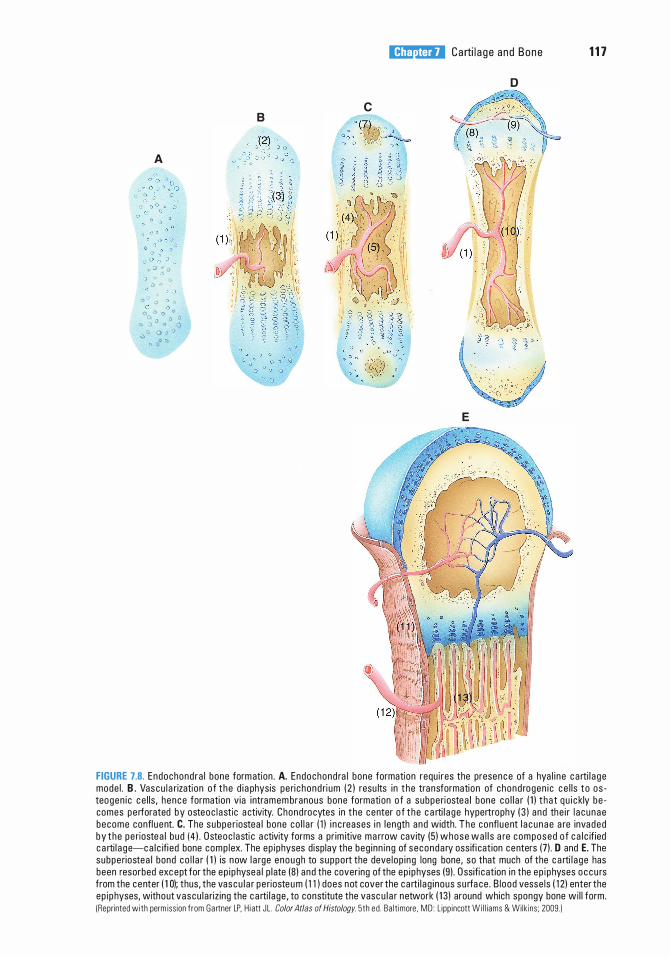
A
"' 0 � 0 0 ° 0 0 0 0
_, cJ � � " 0 0 0 0 0 °
0 0 0 0 1:) ') 0 0 vv o o O
() 00 {')
B
l!iitJ'!1tiii Carti l a g e and Bone 1 1 7
D
c
. Yi - · ., :a � ·� ·; ./�
E
FIGURE 7.8. Endochondra l bone formation . A. Endochond ra l bone formation requ i res the presence of a hya l i ne c a rti l a ge mode l . B. Vascu l a rization o f t he d i a physis peri c hond ri um ( 2 ) resu lts i n t he transformati on of chond rogen i c c e l ls t o os teogen i c c e l ls , hence formation v ia i ntramem branous bone formation o f a subperiostea l bone co l l a r ( 1 ) t ha t q u i c kly be comes pe rforated by osteoc l astic a ctivity. Chond rocytes in t he center o f t he c a rti l a ge hypertrophy ( 3 ) and the i r l a cunae become confl uent. C. The subpe r iostea l bone co l l a r ( 1 ) i n c reases i n l ength and width. The confl uent l a c unae a re invaded by t he pe riostea l bud ( 4 ) . Osteoc l asti c a ctivity forms a pr im itive ma rrow cavity (5 ) whose wa l l s a re composed o f c a l c if ied c a rti l a ge-ca l c ifi ed bone comp lex. The ep iphyses disp lay the beg inn ing of seconda ry oss ifi cat ion centers (7) . D and E. The subperiostea l bond co l l a r ( 1 ) is now l a rge enough to suppo rt the deve lop i ng long bone, so that much of the c a rti l a ge has been resorbed exc ept for the ep i physea l p l ate (8) and the cover ing of the ep i physes (9) . Ossifi cat ion i n the ep i physes o ccu rs from the center ( 1 0); thus, the vascu l a r pe riosteu m ( 1 1 ) does not cover the ca rti l ag i nous su rfa ce . B lood vesse ls ( 1 2) enter the ep ip hyses, without vascu l a riz ing the c a rti l age , to constitute the vasc u l a r network ( 1 3) around which spongy bone wi l l form. !Reprinted with perm iss ion f rom Gartner LP. H i att JL . Color Atlas of Histology. 5th ed . Ba lt imore . MD : L ipp incott Wi l l iams & Wilk ins ; 2009.)
1 1 8 BRS Cel l B iology and H istology
In histological sections, the calcified cartilage stains basoph i l ic, whereas the calcified bone stains ac idoph i l ic .
(6 ) The subperiosteal bone collar becomes thicker and elongates toward the epiphysis. (7) Osteoclasts begin to resorb the calcified cartilage-calcified bone complex, thus
enlarging the primitive marrow cavity. (B) Repetition of this sequence of events results in bone formation spreading toward the
epiphyses. b . Secondary centers of ossification develop at the ep iphyses in a sequence of events similar
to that described for the primary center, except a bone collar is not formed. (1 ) Development of these centers begins when osteoprogenitor cells invade the
epiphysis and differentiate into osteoblasts, which elaborate bone matrix to replace the disintegrating cartilage. When the epiphyses are filled with bone tissue, cartilage remains in two areas, the articular surfaces and the epiphyseal plates.
(2) Articular cartilage persists and does not contribute to bone formation. (3) Epiphyseal plates continue to grow by adding new cartilage at the epiphyseal end while
it is being replaced with bone at the diaphyseal end (lengthening the bone). (4) Ossification of the epiphyseal plates and cessation of growth occur at about 20 years
of age. 3. Zones of the ep iphyseal p lates are histologically distinctive and arranged in the following
order: a . The zone of reserve cartilage is at the epiphyseal side of the plate. It possesses small,
randomly arranged inactive chondrocytes. b. The zone of prol iferation (of chondrocytes) is a region of rapid mitotic divisions giving rise
to rows of isogenous cell groups. c. The zone of cell hypertrophy and maturation is the region where the chondrocytes are
greatly enlarged. d . The zone of calc ification is the region where hypertrophied chondrocytes die and the
cartilage becomes calcified. e. The zone of ossification is the area where newly formed osteoblasts elaborate bone matrix
on the calcified cartilage, forming a calcified cartilage-calcified bone complex, which is resorbed and replaced by bone.
4. Calc ification of bone is not clearly understood, however. a. Osteonectin, proteog lycans, and bone s ia loprote in are known to stimulate calcification. b. Bone matrix contains high concentrations of calcium Ca2+ along with several other organic
compounds and enzymes. Osteocalcin and sialoproteins further concentrate the calcium, resulting in osteoblasts secreting alkaline phosphatase, thus concentrating P04
3- ions, which further concentrates the calcium ions. Small matrix vesicles are released into the bone matrix from the osteoblasts, resulting in crystallization of calcium phosphate within the matrix vesicles.
c. Calcium pumps in the matrix vesicle membranes bring in more calcium, concentrating it and forming calcium hydroxyapatite crystals that grow and eventually puncture the matrix vesicle expelling its contents.
d. Calcium hydroxyapatite crystals that become free in the matrix become n id i of crysta l l ization .
e . Released enzymes free phosphate ions that unite with the calcium forming calcium phosphate.
f. Calcium phosphate then begins to calcify the matrix around the nidi of crystallization. g. Water is removed from the matrix, permitting hydroxyapatite crystals to be deposited into
gaps within the collagen fibrils. h. Nidi of mineralization enlarge and fuse with neighboring nidi, eventually calcifying the
entire matrix.
F. Bone remodel ing . Bone is constantly being remodeled as necessary for growth and to alter its structural makeup to adapt to changing stresses in the environment throughout life. 1 . Early on, bone development outpaces bone resorption as new haversian systems are added
and fewer are resorbed.
l!iitJ'!1tiii Carti l a ge and Bone 1 1 9
2 . Later, when the epiphyseal plates are closed, ending bone growth, bone development and resorption are balanced.
Several factors, including calc iton in and PTH, are responsible for this phenomenon regarding compact bone (see Section II J) . Remodeling of cancellous bone is under the control of many factors within the bone marrow.
G. Repair of a bone fracture. A bone fracture damages the matrix, bone cells, and blood vessels in the region and is accompanied by localized hemorrhaging and blood clot formation. 1 . Prol iferation of osteoprogenitor ce l ls occurs in the periosteum and endosteum in the vicinity
of the fracture. As a result of this proliferation, cellular tissue surrounds the fracture and penetrates between the ends of the damaged bone.
2. Formation of a bony ca l l us occurs both internally and externally at a fracture site. a. Fibrous connective tissue and hyaline cartilage are formed in the fracture zone. b. Endochondral bone formation replaces the cartilage with primary bone. c. Intramembranous bone formation also produces primary bone in the area. d . The irregularly arranged trabeculae of primary bone join the ends of the fractured bone,
forming a bony ca l lus. e . The primary bone is resorbed and replaced with secondary bone as the fracture heals.
CLIN ICAL CONSIDERATIONS
Bone Repair. Afte r severe i n j u ry whe re segments o f bone h ave been lost o r must be removed, the rema i n i n g bone is p revented from form ing a bony
un ion fo l l owed by a bony c a l l u s that over time wou l d resu lt i n c omp l eted bone re p a i r. When the bony un ion is not poss i b l e , a bone g raft is req u i r ed . For th is p u rpose , bone fra g m e nts that a re sto red frozen t o m a i nta i n osteogen i c potenti a l m ay th en may b e uti l i zed i n bone g rafts .
Autographs a re most s u c cessfu l s i n ce the bone dono r is the re c i p i e nt. Homographs a re of bone donated from a d iffe rent i n d iv id u a l . Heterographs a re t h e l e a st s u c c essfu l b e c a use t h e dono r bone c o m e s from a n oth e r s pec ies .
H oweve r, c a lf bone that h a s been froze n can se rve a s a vi a b l e bone g raft when n e c essa ry.
H. Role of vitamins in bone formation 1 . Vitamin D is necessary for absorption of ca lc ium from the small intestine. Vitamin D
deficiency results in poorly calcified (soft) bone, a condition known as r ickets in children and osteomalacia in adults. Vitamin D is also necessary for bone formation (ossification), whereas an excess of vitamin D causes bone resorption.
2. Vitamin A deficiency inhibits proper bone formation and growth, whereas an excess accelerates ossification of the epiphyseal plates. Deficiency or excess of vitamin A results in small stature.
3. Vitamin C is necessary for col lagen formation . Deficiency results in scurvy, characterized by poor bone growth and inadequate fracture repair.
CLIN ICAL CONSIDERATIONS
Rickets o c c u rs i n c h i l d ren d efi c i e nt i n vitam i n D , wh i c h resu lts i n c a l c i u m defi c i e n cy. I t is c h a r a cte r ized b y d efi c i e nt c a l c ifi c ati o n i n n ewly fo rmed
bone and is g ene r a l ly a c compa n i ed by d eformati o n of the bone sp i cu l es i n e p i p hyse a l p l ates; a s a resu lt, bones g row mo re s l owly th a n no rm a l a n d a re d efo rmed by the stress of we ight b e a ri n g . Osteomalacia ( ri c kets o f a d u lts) resu lts from ca l c i um d efi c i e n cy.
1 . It is c h a ra cter ized by d efi c i e nt c a l c if ic ati on in n ewly fo rmed bone a n d d e c a l c ifi c ation of a l ready c a l c if ied bone .
2 . Th i s d i sease may be severe d u ri ng p re g n a n cy b eca use th e ca l c i um req u i rements o f the fetus may l e a d to c a l c i um loss from th e mothe r.
1 20 BRS Cel l B iology and H istology
I . Ro le of hormones in bone formation 1. PTH activates osteoblasts to secrete osteoclast-stimulat ing factor, which then
activates osteoclasts to resorb bone, thus e levating blood ca lc ium levels . Excess PTH (hyperparathyroidism) renders bone more suscepti b le to fracture and subsequent deposition of calcium in arterial walls and certain organs, such as the kidney.
2. Calciton in is produced by parafollicular cells ( C cells) of the thyroid gland. It eliminates the ruffled border of osteoclasts and inh ib its bone matrix resorption, preventing the release of calcium.
3. Pitu itary g rowth hormone (somatotrop in ) is produced in the pars distalis of the pituitary gland. It stimulates overall growth, especially that of epiphyseal plates, and influences bone development via insulin-like growth factors (somatomedins), especially stimulating growth of the epiphyseal plates. Children deficient in this hormone exhibit dwarfism, whereas adults with an excess of somatotropin in their growing years display pitu itary g igantism and acromegaly.
CLINICAL CONSIDERATIONS
Osteoporosis i s a d i sease c h a ra cte r ized by l ow bone mass ( low bone minera l density) and stru ctu ra l d eter iorati on of bone ti ssue , m a ki ng the
bone fra g i l e and suscepti b l e to fra ctu re . Osteopo ros is is assoc i ated with a n a b no rma l rati o of m i n e ra l t o m atrix.
1. It resu lts from i n c reased bone reso rpti on , d e c reased bone fo rmation , o r both. 2. Estrogen a ctivates bone fo rmation by osteob l a sts, and i n its a bsence a n imba l a n c e c a uses
osteoc l a sti c a ctivity to ren d e r bones fra g i l e a n d suscepti b l e to fra ctu re . a . Osteoporos is is most c ommon i n postmenopausa l wom e n b e c a use of d im i n i shed estrogen
sec retion , a n d i n immob i l e pat ie nts b eca use o f l a c k o f physi c a l stress on t he bone . b . Estrogen the ra py was e m p loyed f o r d e c a des t o m i n im ize the onset o f osteopo ros is .
R e cently, it was d eterm i ned that estrogen re p l a c ement th e ra py i n c reases th e r isk of h e a rt d isease , stro ke, b reast c a n c e r, a n d b l ood c l ots . N ow, i nste a d of estrogen , a r ecent new g ro u p of d rugs , the b i sphosphonates, h as been d eve l o ped that red u c es the i n c i d e n ce of osteopo ros is .
c. Preve ntive measu res i n c l u d e a b a l a n c e d d i et ri c h i n c a l c i um and vita m i n D and we ig htb e a ri n g exe rc i se .
Acromegaly Acromega ly resu lts f rom a n excess of p itu itary g rowth hormone i n a d u lts. It is c h a ra cte rized by very th ick bones in the extrem iti es a n d in p o rtions of the fa c i a l ske leton .
A . Synarthroses are immovable jo ints composed of connective tissue, cartilage, or bone. These joints unite the first rib to the sternum and connect the skull bones to each other.
B. D iarthroses (synovia l jo ints) permit maximum movement and generally unite long bones. These joints are surrounded by a two-layered capsule, enclosing and sealing the articular cavity. The articular cavity contains synovial f lu id , a colorless, viscous fluid that is rich in hyaluronic acid and proteins. 1 . The externa l (fibrous) capsu lar layer is a tough, fibrous layer of dense connective tissue. 2. The i nterna l (synovia l ) capsu lar layer is also called the synovia l membrane. It is lined by a layer
of squamous to cuboidal epithelial cells on its internal surface. Two cell types are displayed in electron micrographs of this epithelium. a. Type A ce l ls are intensely phagocytic and have a well-developed Golgi complex, many
lysosomes, and sparse RER. b. Type B ce l ls resemble fibroblasts and have a well-developed RER; these cells probably
secrete synovial fluid.
Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which of the following statements characterizes osteoclasts?
(A) They are enucleated cells. (B ) They produce collagen. (C) They secrete osteoid. (D ) They are derived from osteoprogenitor
cells. (E ) They occupy Howship lacunae.
2. Which one of the following statements is correct concerning the periosteum?
(A) It is devoid of a blood supply. (B ) It produces osteoclasts. (C) It is responsible for interstitial bone
growth. (D ) Its inner layer contains osteoprogenitor
cells. (E ) Its outer layer is devoid of fibers.
3. Which one of the following statements is characteristic of osteocytes?
(A) They communicate via gap junctions between their processes.
(B) They contain large amounts of RER. (C) They are immature bone cells. (D ) They are housed as isogenous groups in
lacunae. (E) They give rise to osteoclasts.
4. Which one of the following statements concerning hyaline cartilage is correct?
(A) It is vascular. (B ) It contains type IV collagen. (C) It undergoes appositional growth only. (D ) It is located at the articular ends of long
bones. (E) Its chondrocytes are aligned in rows.
5. A 7-year-old boy is seen by his pediatrician because the child broke his humerus as he tripped and fell while walking. The pediatrician asked about the child's diet and learned that he might have a dietary deficiency. Which of the following may be lacking in his diet?
(A) Potassium (B ) Calcium (C) Iron (D ) Carbohydrates (E ) Protein
6. A 22-year-old woman is seen for the first time by her new physician, who notes that she has very thick bones in her extremities and face. The physician suspects acromegaly, caused by which of the following?
(A) Hypervitaminosis A (B ) Excess growth hormone (C) Hypovitaminosis A (D ) Hypervitaminosis D (E) Hypovitaminosis D
7. Which of the following statements is characteristic of bone?
(A) Bone matrix contains primarily type II collagen.
(B ) About 65% of the dry weight of bone is organic.
(C) Haversian canals are interconnected via Volkmann canals.
(D ) Bone growth occurs via interstitial growth only.
(E ) Bone growth occurs via appositional growth only.
1 21
1 22 BRS Cel l B iology and H istology
8. Which one of the following inhibits histogenesis of cartilage?
(A) Thyroxine (B ) Hypervitaminosis A (C) Hypovitaminosis D (D ) Hydrocortisone (E) Hypovitaminosis C
9. Which one of the following stimulates cartilage histogenesis?
(A) Thyroxine (B ) Hypervitaminosis A (C) Hypovitaminosis D (D ) Hydrocortisone (E) Hypovitaminosis C
1 0. Which one of the following accelerates epiphyseal ossification?
(A) Thyroxine (B ) Hypervitaminosis A (C) Absence of vitamin D (D ) Hydrocortisone (E) Hypovitaminosis C
1 1 . Which one of the following makes epiphyseal cartilage matrix fail to calcify?
(A) Thyroxine (B ) Hypervitaminosis A (C ) Hypovitaminosis D (D ) Hydrocortisone (E) Hypovitaminosis C
1 2. A 25-year-old patient, anemic for several years, complains of failing eyesight and hearing loss. During a physical examination, it is determined that the patient has lost function of some of the cranial nerves. The diagnosis could be which one of the following?
(A) Osteoporosis (B ) Osteomalacia (C) Rickets (D ) Acromegaly (E ) Osteopetrosis
Answers and Explanations
1 . E. Osteoclasts are multinucleated cells that produce proteolytic enzymes and occupy Howship lacunae. They are not derived from osteoprogenitor cells but from monocyte precursors (see Chapter 7 II C 4).
2. D . The inner layer of the periosteum possesses osteoprogenitor cells, whereas the outer layer of the periosteum is fibrous. The periosteum functions to distribute blood vessels to the bone; thus, appositional bone growth takes place here (see Chapter 7 II B 2).
3. A. Osteocytes communicate with each other via gap junctions on narrow cytoplasmic processes that extend through canaliculi. They are mature bone cells that occupy individual lacunae as mature resting bone cells (see Chapter 7 II C 3) .
4. D . Hyaline cartilage is avascular, contains type II collagen, and grows both interstitially and appositionally. It is located at the articulating ends of long bones (see Chapter 7 I A) .
5. B. Because calcium must be maintained at a constant level in the blood and the tissues, a diet deficient in calcium leads to calcium loss from the bones. As a result, the bones become fragile (see Chapter 7 II C 4 Clinical Considerations).
6. B . Excessive growth hormone causes acromegaly. Excessive vitamin D causes bone resorption. Both an excess and a deficiency of vitamin A result in short stature (see Chapter 7 II J Clinical Considerations).
7 . C. Haversian canals run longitudinally, parallel to the long axis of bone. They are connected to one another by Volkmann canals that run perpendicular (or obliquely) to them (see Chapter 7 II E 1 ) .
8. D . Hydrocortisone inhibits cartilage growth and matrix formation (see Chapter 7 I A 2).
9. A. Thyroxine, testosterone, and somatotropin stimulate cartilage growth and matrix formation (see Chapter 7 I A 2) .
1 0. B . Hypervitaminosis A accelerates ossification of epiphyseal plates, whereas hypovitaminosis A reduces the width of the epiphyseal plates (see Chapter 7 II I) .
1 1 . C. In the absence of vitamin D, epiphyseal chondrocytes continue to proliferate, but their matrix does not calcify, which leads to rickets (see Chapter 7 II I Clinical Considerations) .
1 2. E. Osteopetrosis is a genetic defect involving the osteoclasts. Persons with this defect possess osteoclasts without ruffled borders, which prohibit them from resorbing bone. Therefore, bone forms but is not resorbed. This leads to increased bone density, anemia, blindness, deafness, and cranial nerve involvement because the nerves are impinged upon as they exit the cranium via their foramina (see Chapter 7 II B Clinical Considerations).
1 23
Muscle
I. OVERVIEW-MUSCLE
A. Muscle is classified into two types : striated and smooth, and striated muscle has two subdivisions : skeleta l and cardiac muscles.
B. Muscle cells possess contracti le f i laments whose major components are actin and myosin .
C. Contraction may be vo luntary (skeletal muscles) or i nvoluntary (cardiac and smooth muscles) .
A. Connective tissue investments convey neural and vascular elements to muscle cells and provide a vehicle that harnesses the forces of muscle contraction. 1. Ep imysium surrounds an entire muscle and forms aponeuroses, which connect skeletal
muscle to muscle, and tendons, which connect skeletal muscle to bone. 2. Perimysium surrounds fasc icles (small bundles) of muscle cells. 3. Endomysium surrounds individual muscle cells and is composed of reticu lar f ibers and an
external lamina .
B. Types of skeletal muscle ce l ls 1 . Types of skeletal muscle cells (also known as musc le f ibers) include red (slow contraction but
does not fatigue easily), white (fast contraction but fatigues easily), and i ntermed iate. All three types may be present in a given muscle.
2. These three types differ from each other in their content of myoglob in (a protein that is similar to hemoglobin in that it binds 02), number of mitochondria, concentration of various enzymes, and rate of contraction (Table 8 . 1 ) .
3 . A change in innervation can change a fiber's type. I f a red fiber i s denervated and its innervation replaced with that of a white fiber, the red fiber will change its characteristics and will become a white fiber.
C. Skeleta l muscle cel ls (Figures 8 . 1 and 8.2) are long, cylindrical, multi nuc leated and are enveloped by an external lamina and reticular fibers. Their cytoplasm is called sarcop lasm, and their plasmalemma is called the sarco lemma and forms deep tubular invaginations, or T (transverse )
1 24
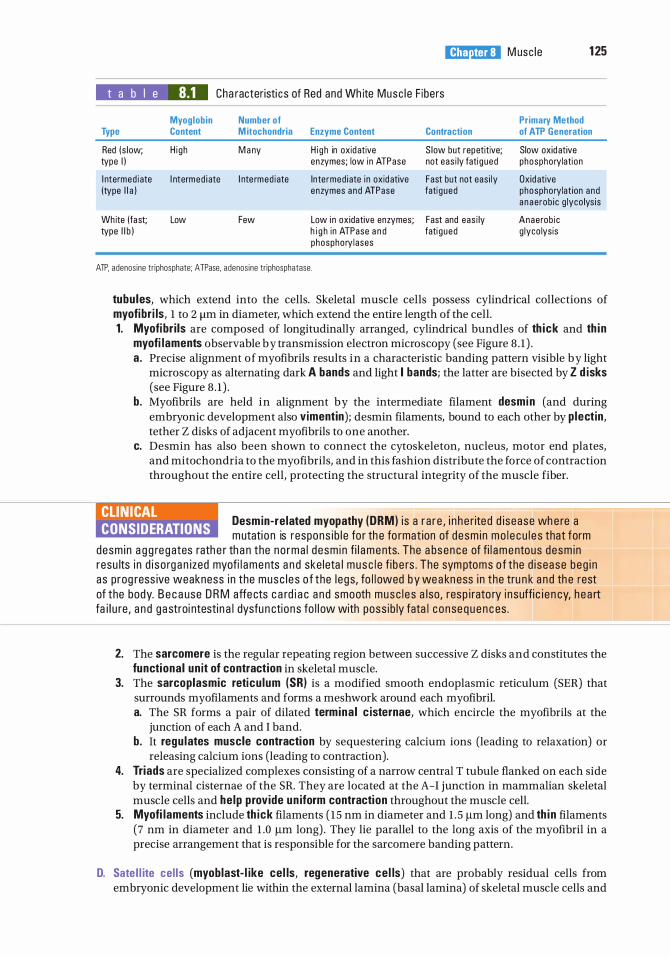
l!1lllJ1llllj M usc le 1 25
t a b I e 8.1 Cha racter isti cs of Red and Wh ite Musc l e F ibers
Myoglobin Number of Primary Method Type Content M itochondria Enzyme Content Contraction of ATP Generation
Red (s low; H i gh M a ny H i gh in oxid ative S low but repetitive; Slow oxid ative type I ) enzymes; low in ATPase not eas i ly fati gued phosphorylation
I ntermed iate I ntermed i ate I nte rmed iate Inte rmed iate i n oxid ative Fast but not eas i ly Oxid ative (type l l a ) enzymes and ATPase fati gued phosphorylat ion and
a n aerob ic g lyco lys is
Wh ite (fast; Low Few Low i n oxidative enzymes; Fast and eas i ly Anaerob ic type l i b ) h i g h in ATPase a n d fati gued g lyco lysis
phosphory lases
ATP, adenos ine tr iphosphate; ATPase. adenos ine tr iphosphatase.
tubu les, which extend into the cells. Skeletal muscle cells possess cylindrical collections of myofibr i ls, 1 to 2 11m in diameter, which extend the entire length of the cell. 1. Myofibr i ls are composed of longitudinally arranged, cylindrical bundles of th ick and th i n
myofi laments observable by transmission electron microscopy (see Figure 8 . 1 ) . a. Precise alignment of myofibrils results in a characteristic banding pattern visible by light
microscopy as alternating dark A bands and light I bands; the latter are bisected by Z d isks (see Figure 8 . 1 ) .
b. Myofibrils are held in alignment by the intermediate filament desmin (and during embryonic development also vimentin); desmin filaments, bound to each other by p lectin, tether Z disks of adjacent myofibrils to one another.
c. Desmin has also been shown to connect the cytoskeleton, nucleus, motor end plates, and mitochondria to the myofibrils, and in this fashion distribute the force of contraction throughout the entire cell, protecting the structural integrity of the muscle fiber.
CLIN ICAL CONSIDERATIONS
Desmin-related myopathy (DRM) i s a r a r e , i n h e rited d isease wh e re a mutati o n is respons i b l e fo r th e fo rmat ion of desm i n mo l e c u l e s that form
desm in a g g regates rath e r th a n the no rma l desm in fi l aments. The a bsence of fi l amentous desm i n resu lts i n d i so rg a n ized myofi l aments a n d ske leta l musc l e fi b e rs . The sym ptoms o f the d i sease beg i n as prog ress ive weakness i n the musc l e s o f the l egs, fo l l owed by wea kn ess i n the tru n k a n d th e rest of the body. B e c a use D R M affe cts c a rd i a c a n d smooth musc l e s a l so, resp i rato ry i n suffi c i e n cy, h e a rt fa i l u re , a n d gastroi ntesti n a l dysfu n ctions fo l l ow with poss ib ly fata l c onse q u e n c es .
2. The sarcomere is the regular repeating region between successive Z disks and constitutes the functional un it of contraction in skeletal muscle.
3. The sarcoplasmic reticu lum (SRI is a modified smooth endoplasmic reticulum (SER) that surrounds myofilaments and forms a meshwork around each myofibril. a. The SR forms a pair of dilated termina l c isternae, which encircle the myofibrils at the
junction of each A and I band. b. It regu lates muscle contraction by sequestering calcium ions (leading to relaxation) or
releasing calcium ions (leading to contraction). 4. Triads are specialized complexes consisting of a narrow central T tubule flanked on each side
by terminal cisternae of the SR. They are located at the A-I junction in mammalian skeletal muscle cells and he lp provide un iform contraction throughout the muscle cell.
5. Myofi laments include th ick filaments ( 15 nm in diameter and l . 5 Jlm long) and th i n filaments (7 nm in diameter and 1 .0 Jlm long) . They lie parallel to the long axis of the myofibril in a precise arrangement that is responsible for the sarcomere banding pattern.
D. Sate l l ite cel ls (myoblast- l ike cel ls, regenerative ce l ls) that are probably residual cells from embryonic development lie within the external lamina (basal lamina) of skeletal muscle cells and
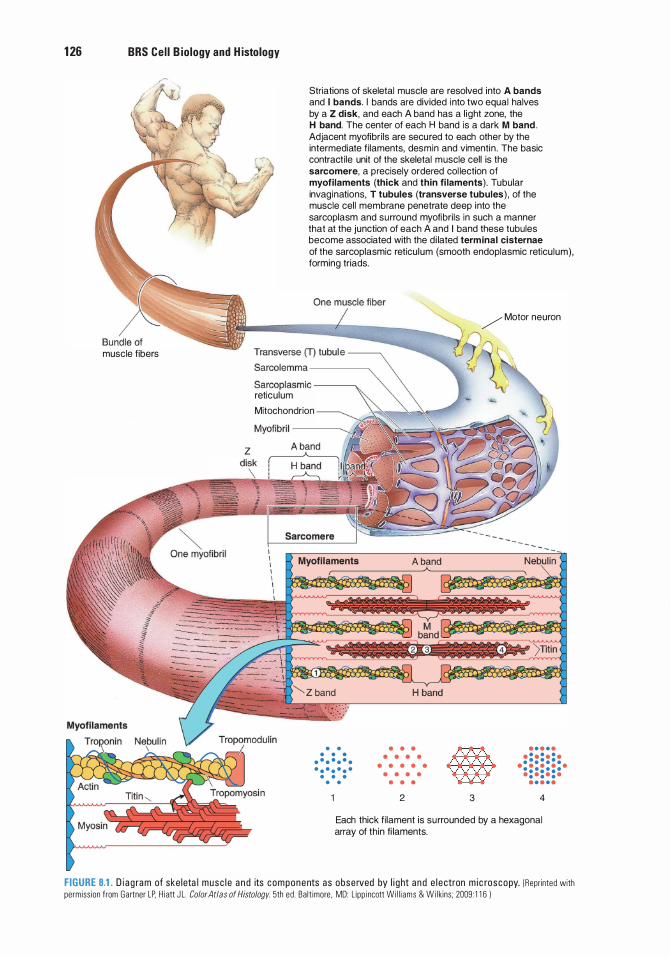
1 26 BRS Cel l B iology and H istology
muscle fibers
z
Striations of skeletal muscle are resolved into A bands and I bands. I bands are divided into two equal halves by a Z disk, and each A band has a l ight zone, the H band. The center of each H band is a dark M band .
Adjacent myofibri ls are secured to each other by the intermediate f i laments, desmin and vimentin . The basic contracti le unit of the skeletal muscle cell is the sarcomere, a precisely ordered col lection of myofilaments (thick and thin fi laments) . Tubular invaginations, T tubules (transverse tubules ) , of the muscle cell membrane penetrate deep into the sarcoplasm and surround myofibri ls in such a manner that at the junction of each A and I band these tubules become associated with the d i lated term inal cisternae
of the sarcoplasmic reticulum (smooth endoplasmic reticu lum) , forming triads.
/ Motor neuron
Sarcolemma -----,
Sarcoplasmic --------. reticulum
Mitochondrion
Myofibri l ----�
• • • • •
• • • • • • • • • • • • • •
• • • • •
• • •
• • • •
•
• •
• • • • • •
• • · : · : · : · • • • • • • • • • • • • • • • • • • • • • • • • • • • •
• • • • • • •
2 3 4
Each thick fi lament is surrounded by a hexagonal array of thin fi laments.
FIGURE 8.1. D i a g ra m of ske leta l musc l e a n d its components as obse rved by l i g ht a nd e l e ctron m i c roscopy. (Reprinted with permiss ion from Gartner LP. H i att J L. Color Atlas of Histology. 5th ed . Ba lt imore . MD: L ipp i ncott Wi l l i ams & Wi lkins ; 2009 : 1 1 6 )
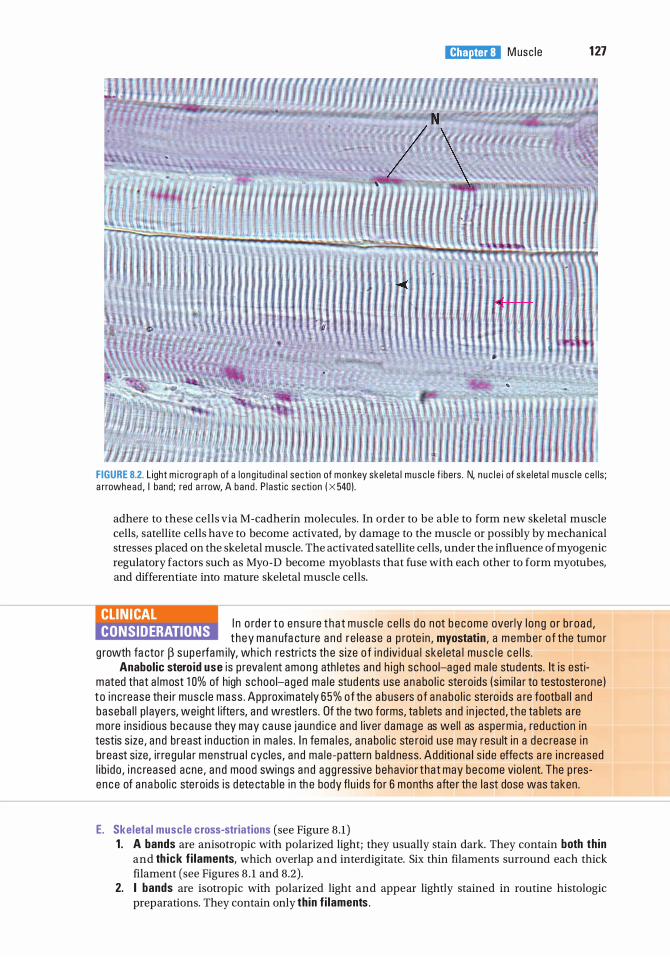
l!1lllJ1llllj M usc le 1 27
FIGURE 8.2. L ight m i c rog raph of a l ong itud i n a l sect ion of monkey ske leta l musc l e f ibers . N, n u c l e i of ske leta l musc l e c e l ls ; a rrowhead , I band; red a rrow, A band . P l ast ic se ction ( X 540) .
adhere to these cells via M-cadherin molecules. In order to be able to form new skeletal muscle cells, satellite cells have to become activated, by damage to the muscle or possibly by mechanical stresses placed on the skeletal muscle. The activated satellite cells, under the influence of myogenic regulatory factors such as Myo-D become myoblasts that fuse with each other to form myotubes, and differentiate into mature skeletal muscle cells.
CLIN ICAL CONSIDERATIONS
I n o rd e r t o ensu re t ha t m usc l e c e l l s d o not b e come over ly l o ng o r b road , t hey m a n ufa ctu re a n d re l ease a p rote i n , myostatin , a membe r o f the tu mo r
g rowth fa cto r � s upe rfa m i ly, wh i c h restri cts th e s ize o f i n d iv i d u a l ske l eta l musc l e c e l l s . Anabolic stero id use is p reva lent among ath l etes and h i gh sc hoo l-aged ma l e students. It is esti
mated that a lmost 1 0% of high sc hoo l-aged ma l e stud ents use a nabo l i c ste ro ids ( s im i l a r to testoste rone ) to i nc rease the i r musc l e mass . App roximately 65% of the a busers o f a nabo l i c ste ro ids a re footba l l and baseba l l p l aye rs, we ight l ifte rs, and wrestle rs . Of the two forms, ta b lets and in jected , t he ta b l ets a re more ins id ious because they may ca use j aund i ce and l iver d amage as we l l as aspermia , red u ction in testis s ize , and breast i nduction in ma les . I n fema l es, a n abo l i c ste roid use may resu lt i n a d ec rease i n breast size, i r regu l a r menstrua l cycles, and ma le -patte rn ba l d ness . Add iti ona l s i de effects a re i n c reased l i b i do , i n c reased acne , a nd mood swings and agg ressive behavior that may become vio l ent. The p resence of ana bo l i c ste ro ids is d ete cta b l e i n th e body fl u i ds fo r 6 months afte r the l ast dose was taken .
E. Skeletal muscle cross-striations (see Figure 8 .1) 1 . A bands are anisotropic with polarized light; they usually stain dark. They contain both th in
and th ick f i laments, which overlap and interdigitate. Six thin filaments surround each thick filament (see Figures 8 . 1 and 8.2) .
2. I bands are isotropic with polarized light and appear lightly stained in routine histologic preparations. They contain only th in f i laments .
1 28 BRS Cel l B iology and H istology
3. H bands are light regions transecting A bands; they consist of thick f i laments only. 4. M l ines are narrow, dark regions at the center of H bands formed by several cross-connections
(M-bridges) at the centers of adjacent thick filaments. 5. Z d isks ( l i nes) are dense regions bisecting each I band.
a . Z disks contain a-acti n i n and Cap Z, two proteins that bind to thin filaments and anchor them to Z disks with the assistance of nebul i n .
b . Desmin, aided by p lectin, anchors Z disks to each other. Peripherally located Z disks are anchored to regions of the sarcolemma, known as costameres, dystroph in-associated g lycoprote in complexes. (1 ) Costa meres are specialized areas of the sarcolemma located at regions that correspond
to the Z-lines of myofibrils that are situated just beneath the striated muscle cell membrane. Costameres are defined by the presence of peripheral and transmembrane protein complexes whose principal moieties are localized on the sarcoplasmic aspect of the striated muscle cell membrane.
(2) Dystroph in-associated g lycoprote in complexes are composed of several protein groups, including dystrophin, sarcoglycan complex, dystroglycan complex, syntrophins, and dystrobrevin. (a ) Dystrophin is a pencil-shaped molecule that is the lynchpin between the extracellular
matrix and the cytoskeleton attached to the peripheral-most myofibril of the striated muscle fiber. It is dystrophin that plays the greatest role in strengthening and maintaining the integrity of the sarcolemma during the process of contraction.
(b ) Sarcog lycan complex is composed of several transmembrane proteins localized at the costameres of the sarcolemma. They form attachments to and reinforce the dystroglycan complex.
(c) Dystrog lycan complex is a complex of two transmembrane proteins whose extracellular domains bind to l amin in of the external lamina of the muscle cells. Intracellularly dystroglycan binds to dystrophin as well as to syntroph ins.
(d ) Syntrophins are relatively small proteins, approximately 60 kDa, that form bonds not only with dystrophins but also with desmin and dystrobrevin.
(e) The protein dystrobrevin has binding sites with syntrophins and desmin. Therefore, the dystrophin-associated glycoprotein complex forms a series of
bonds centered around dystrophin. These function to affix the desmin intermediate filaments to laminin of the extracellular matrix, allowing them to maintain the precise orientation and arrangement of the Z-lines of adjacent myofibrils throughout the entire skeletal muscle cell. These attachments to the glycoprotein laminin of the extracellular matrix occur in the costamere regions of the sarcolemma.
CLINICAL CONSIDERATIONS
Duchenne muscular dystrophy (DMD) i s c a used by a sex- l i nked, recess ive g e net ic d efect that resu lts i n th e i n a b i l ity to synth es ize dystroph in , an
a cti n - b i n d i n g p rote i n no rma l ly p resent i n sma l l a m o u nts i n the sa r cop l a sm . Dystro ph i n a l so sta b i l i zes the sa r co l emma and a cts as a l i nk between the cytoske leton and the extra c e l l u l a r matrix.
1. This c ommon, se r i ous d e gene rative d i so rde r o c c u rs in yo ung m e n a n d resu lts i n d e ath u sua l ly before 20 yea rs of a ge .
2 . DMD i s c h a ra cter ized by t h e r e p l a cement o f d e gene rati n g ske leta l musc l e c e l l s by fatty a n d fi b rous c onnective tissue , b ut i t m ay a l so affe ct c a rd i a c musc l e .
Facioscapulohumeral muscular dystrophy ( FSHMD or Landouzy-Dejerine syndrome) i s not sexl i n ked , b ut is an autosomal dominant g e n et ic d efect that resu lts i n "wasti n g " of the ske leta l musc l e s o f th e fa ce , those a round the s c apu l a , a n d those o f t he u p pe r a rm , i n iti a l ly, b ut a s t he d isease p rog resses i t affe cts s ke l eta l musc les of oth e r a reas of th e body. I t is o ne of th e most common fo rms of muscu l a r dystro p hy a n d m a n ifests itse lf i n the l ate teens a n d ea r ly twenti es .
1 . M a ny affe cted pat ients s uffe r h e a ri n g l oss, a b no rma l h e a rt rhythm, and d i l ations of th e b lood vesse ls i n th e reti n a of the eye ( reti n a l te l a n g i e ctas i a ) .
2. The d isease does not imp i n ge on l ife expectan cy, a n d 85% of affe cted i n d iv id ua l s d o not b e come whee l c h a i r bound .
F. Molecular organ ization of myofi laments
l!1lllJ1llllj M usc l e 1 29
1 . Th in f i laments are composed of F-actin, tropomyosin, troponin, and associated proteins. a. F-actin (see Figure 8 . 1 ) is a polymer of G-actin monomers arranged in a double helix.
(1 ) Each monomer possesses an active site that can interact with myosin. (2) F-actin is present as filaments (with a diameter of 5-7 nm) that exhibit polarity, having
a plus ( + ) and a minus (-) end, where the plus end is tethered to Cap Z ofthe Z disk and the minus end, capped bytropomodu l i n, is located at the H band and is the growing end of the F-actin.
(3) F-actin loses and gains back G-actin molecules at both its plus and minus ends, but this turnover rate is very slow, occurring over a period of several days, whereas in other cells this turnover occurs every few minutes.
b. Tropomyosin molecules are about 40 nm in length. They bind head to tail, forming filaments that are located in the grooves of the F-actin helix.
c. Troponin is associated with each tropomyosin molecule and is composed of the following: (1 ) Troponin T (TnT), which forms the tail of the molecule and functions in binding the
troponin complex to tropomyosin. (2) Troponin C (TnC), which possesses four binding sites for calcium. It may be related to
calmodulin. (3) Troponin I (Tn l) , which binds to actin, inhibiting interaction of myosin and actin.
d. Nebu l in is a long, inelastic protein. Two nebulin molecules wrap around each thin filament and assist in anchoring it to the Z disk (see Figure 8 . 1 ) . ( 1 ) Each nebulin molecule i s embedded in the Z disk by its carboxy terminal but does not
span the entire Z disk. (2) The amino terminal of each nebulin molecule ends in the A band, at or near the free
end of its thin filament. (3) Nebulin in skeletal muscle is thought to determine the length of its associated thin
filament, although in cardiac muscle it extends only one-quarter of the length of the thin filament.
e. Tropomodu l i n caps the minus end of each thin filament and prevents the addition of more G-actin molecules to the growing end; thus, it limits the length of the F-actin filament.
2. Each th ick f i lament contains approximately 250 myosin II molecules arranged in an antiparallel fashion and associated proteins-myomesin, titin, and C protein and the enzyme creatine kinase. a. Myosin II (see Figure 8 . 1 ) is composed of two identical heavy chains and two pairs of light
chains. There are at least 18 different subtypes of myosin, and the one present in skeletal muscle is myosin II. This particular type of myosin molecule resembles a double-headed golf club, and from this point on it will be referred to as "myosin" without its numerical appellation in this textbook. (1 ) Myosin heavy chains consist of a long rod-like "tail" and a globular "head:' The tails of
the heavy chains wind around each other in an a-helical configuration. (a) Tails function in the self-assembly of myosin molecules into bipolar thick filaments. (b) Actin-binding sites of the heads function in contraction.
(2) Myosin l i ght chains are of two types; one molecule of each type is associated with the globular head of each heavy chain.
(3) D igestion of myosin (a ) The enzyme tryps in cleaves myosin into l i ght meromyosin (part of the tail
portion) and heavy meromyosin (the two heads and the remainder of the tail) (see Figure 8 . 1 ) .
(b ) The enzyme papa in cleaves the heavy meromyosin, releasing the short tail (S2 fragment) and the two globular heads (51 fragments) . These S1 fragments have adenosine triphosphatase (ATPase) activity but require interaction with actin to release the non covalently bound adenosine diphosphate (ADP) and Pi.
b. Myomesin and creati ne kinase are located at the M line. The former is a protein that crosslinks adjacent thick filaments to one another to maintain their spatial relations, whereas the latter is an enzyme that is responsible for removing a phosphate group from creatine phosphate and phosphorylating ADP converting it to the energy-rich compound adenosine triphosphate (ATP).
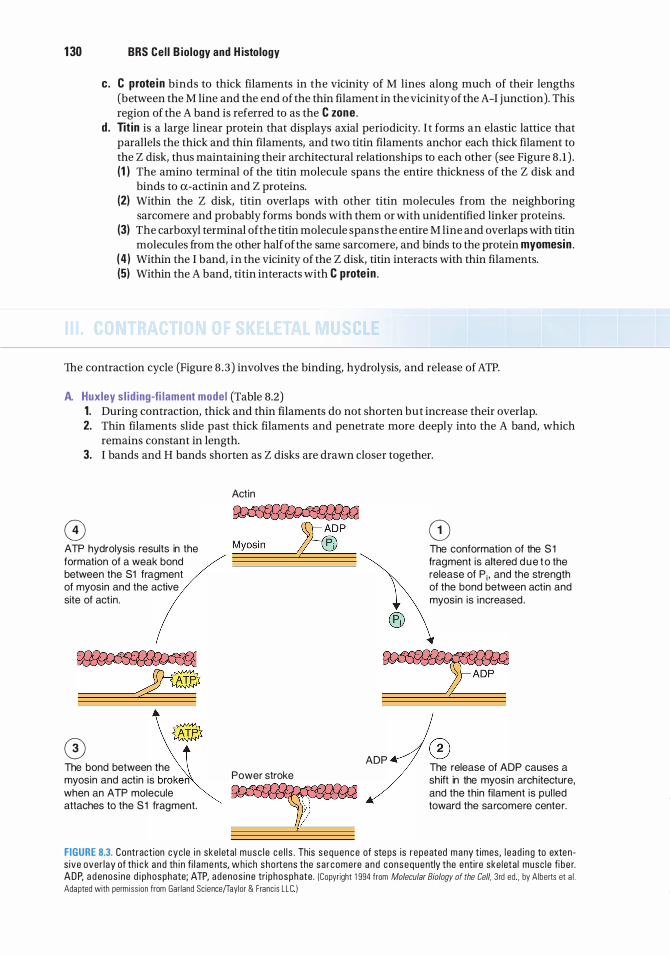
1 30 BRS Cel l B iology and H istology
c. C prote in binds to thick filaments in the vicinity of M lines along much of their lengths (between the M line and the end of the thin filament in the vicinity of the A-I junction). This region of the A band is referred to as the C zone .
d . Tit in is a large linear protein that displays axial periodicity. I t forms an elastic lattice that parallels the thick and thin filaments, and two titin filaments anchor each thick filament to the Z disk, thus maintaining their architectural relationships to each other (see Figure 8 . 1 ) . (1 ) The amino terminal of the titin molecule spans the entire thickness of the Z disk and
binds to a-actinin and Z proteins. (2) Within the Z disk, titin overlaps with other titin molecules from the neighboring
sarcomere and probably forms bonds with them or with unidentified linker proteins. (3) The carboxyl terminal of the titin molecule spans the entire M line and overlaps with titin
molecules from the other half of the same sarcomere, and binds to the protein myomesin . ( 4 ) Within the I band, in the vicinity of the Z disk, titin interacts with thin filaments. (5) Within the A band, titin interacts with C prote in .
The contraction cycle (Figure 8 .3 ) involves the binding, hydrolysis, and release of ATP.
A. Huxley s l id ing-fi lament model (Table 8.2) 1. During contraction, thick and thin filaments do not shorten but increase their overlap. 2. Thin filaments slide past thick filaments and penetrate more deeply into the A band, which
remains constant in length. 3. I bands and H bands shorten as Z disks are drawn closer together.
0 ATP hydrolysis results in the formation of a weak bond between the S1 fragment of myosin and the active site of act in .
0 The bond between the myosin and actin is broken when an ATP molecule attaches to the S 1 fragment.
Actin
Power stroke
�
®
ADP
CD The conformation of the S 1 fragment is altered d u e t o the release of P; , and the strength of the bond between actin and myosin is increased .
® The release of ADP causes a sh ift in the myosin arch itecture, and the thin fi lament is pul led toward the sarcomere center.
FIGURE 8.3. Contraction cyc le i n ske leta l musc l e ce l l s . This sequence of steps is repeated many t imes, l e ad i ng to extens ive over lay of th i c k a nd th i n fi l ame nts, wh ich sho rtens the sa rcomere and consequently the entire ske leta l musc le fi be r. ADP, a d enos ine d i phosphate; ATP, adenos i ne tri phosphate . (Copyright 1 994 from Molecular Biology of the Cell, 3rd ed , by Alberts et a l . Adapted with permiss ion from Gar land Sc ience(Taylor & Franc is L LC I
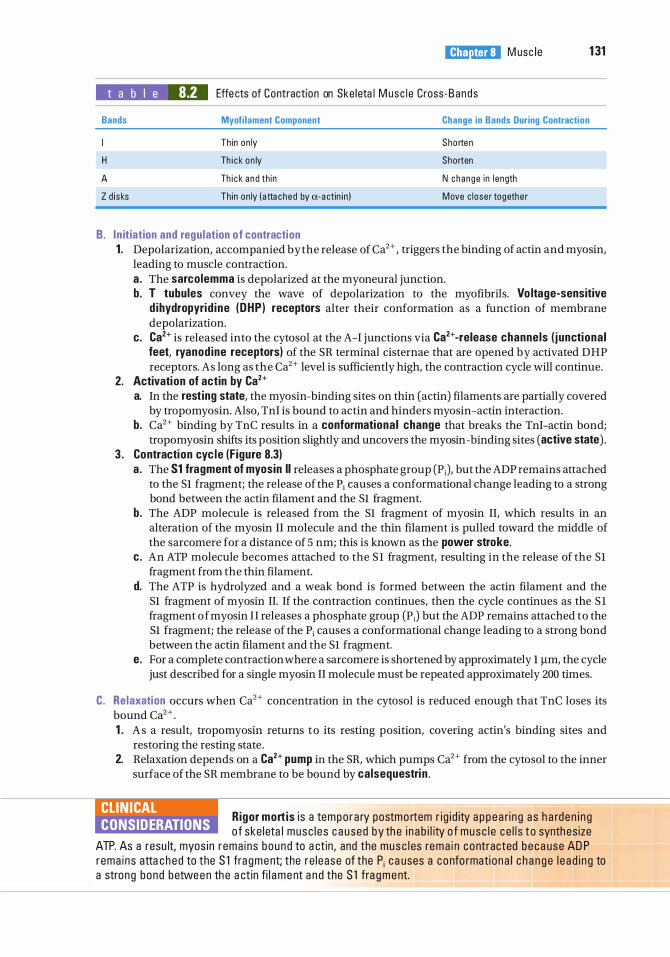
t a b I e 8.2
l!1lllJ1llllj M usc I e 1 31
Effe cts of Contraction on Ske leta l M usc l e Cross-Bands
Bands Myofi lament Component Change in Bands During Contraction
H
A
Th in on ly
Th i c k on ly
Th i c k a nd th in
Sho rten
Shorten
Z d i sks Th in on ly ( a tta ched by a-a ctin i n )
N change in l ength
Move c loser togethe r
B. I n itiation and regu lation of contraction 1 . Depolarization, accompanied by the release of Ca2+ , triggers the binding of actin and myosin,
leading to muscle contraction. a . The sarcolemma is depolarized at the myoneural junction. b. T tubules convey the wave of depolarization to the myofibrils. Vo ltage-sensitive
d ihydropyrid ine (DHP) receptors alter their conformation as a function of membrane depolarization.
c. Ca2+ is released into the cytosol at the A-I junctions via Ca2+-release channels ( j unctional feet, ryanodine receptors) of the SR terminal cisternae that are opened by activated DHP receptors. As long as the Ca2+ level is sufficiently high, the contraction cycle will continue.
2. Activation of actin by Ca2+ a. In the rest ing state, the myosin-binding sites on thin (actin) filaments are partially covered
by tropomyosin. Also, Tnl is bound to actin and hinders myosin-actin interaction. b. Ca2+ binding by TnC results in a conformational change that breaks the Tnl-actin bond;
tropomyosin shifts its position slightly and uncovers the myosin -binding sites (active state) . 3 . Contraction cyc le (F igure 8.3)
a . The S1 fragment of myosin II releases a phosphate group (PJ, but the ADP remains attached to the Sl fragment; the release of the Pi causes a conformational change leading to a strong bond between the actin filament and the Sl fragment.
b. The ADP molecule is released from the Sl fragment of myosin II, which results in an alteration of the myosin II molecule and the thin filament is pulled toward the middle of the sarcomere for a distance of 5 nm; this is known as the power stroke.
c . An ATP molecule becomes attached to the S l fragment, resulting in the release of the Sl fragment from the thin filament.
d. The ATP is hydrolyzed and a weak bond is formed between the actin filament and the Sl fragment of myosin II. If the contraction continues, then the cycle continues as the S l fragment of myosin I I releases a phosphate group (PJ but the ADP remains attached to the Sl fragment; the release of the Pi causes a conformational change leading to a strong bond between the actin filament and the Sl fragment.
e. For a complete contraction where a sarcomere is shortened by approximately 1 f!m, the cycle just described for a single myosin II molecule must be repeated approximately 200 times.
C. Re laxation occurs when Ca2+ concentration in the cytosol is reduced enough that TnC loses its bound Ca2+ . 1 . A s a result, tropomyosin returns t o its resting position, covering actin's binding sites and
restoring the resting state . 2. Relaxation depends on a Ca2+ pump in the SR, which pumps Ca2+ from the cytosol to the inner
surface of the SR membrane to be bound by calsequestri n .
R igor mortis i s a tempo ra ry postmo rtem r i g i d ity a p p e a ri n g a s h a rden i n g CLIN ICAL CONSIDERATIONS o f ske leta l musc l e s c a u sed by th e i n a b i l ity o f musc l e ce l l s t o synth es ize
ATP. As a resu lt, myos in rema ins bound to a ct in , and the musc l es rema i n contracted b e c a use AD P rema ins atta ched to the S l fra gment; the re l ease of the P; c a uses a co nfo rmati o na l c h a n g e l e a d i n g to a strong bond between th e a ct in fi l a m e nt a n d the S l fra g m e nt.
1 32 BRS Cel l B iology and H istology
D . A motor un it consists of a neuron and every muscle cell it innervates. A muscle may contract with varying degrees of strength because only some of the muscle cells contract, but an individual muscle cell obeys the "a l l or none law" (i .e. , it either contracts or does not contract) . All muscle cells of a single motor unit contract in unison, and a large muscle such as the trapezius may have thousands of muscle cells in a motor unit, whereas a muscle such as the superior oblique muscle of the eye may have as few as 10 to 15 muscle cells in a motor unit.
CLIN ICAL CONSIDERATIONS
Norma l ly, a s a musc l e contra cts the sa r comeres sho rten a nd , conse q u ently, th e ent ire musc l e b e comes sho rte r. Th is type of contra cti on i s
refe rred to as concentric contraction, as i n p i c ki ng u p a d u m b be l l and do ing c u r ls . Anoth e r type of contracti o n i s isometric contraction, where the sa r comeres do not sho rten; th us, the ent ire musc l e r ema i n s th e s ame l e ngth, as i n s q ueez ing a h a rd ob ject s u c h a s a so l i d meta l b a l l .
Innervation consists o f motor nerve endings (myoneural junctions) and two types o f sensory nerve endings (muscle spindles and Golgi tendon organs) . Both types of sensory nerve endings function in proprioception .
A. The myoneural junction (neuromuscular junction) is a synapse between a branch of a motor nerve axon and a skeletal muscle cell. 1 . Structural components
a. The axon termina l lacks myelin but has a Schwann ce l l on its nonsynaptic surface. (1 ) The membrane on the synaptic surface of the axon terminal is called the presynaptic
membrane . (2) The axon terminal contains mitochondria, synaptic vesicles (containing the neurot
ransmitter acetylcho l i ne), and SER elements. b. The synaptic c left is a narrow space between the presynaptic membrane of the axon
terminal and the postsynaptic membrane (also known as the motor end p late) of the muscle cell. The synaptic cleft contains an amorphous external lamina, a basal lamina-like material, derived from the muscle cell.
c. Muscle ce l l near the myoneural junction (1 ) Sarcolemmal invaginations (of the postsynaptic membrane), called junctiona l folds,
are lined by an external lamina and extend inward from the synaptic cleft. (2) Acetylcho l ine receptors are located in the postsynaptic membrane at the peaks of the
junctional folds. (3) The sarcoplasm is rich in mitochondria, ribosomes, and rough endoplasmic reticulum
(RER) . 2. Conduction of a nerve impu lse across a myoneural junction
a . The presynaptic membrane (i .e . , the axon's end foot membrane) is depolarized and voltagegated Ca2+ channels open, permitting the entry of extracellular Ca2+ into the axon terminal.
b. The rise in cytosolic Ca2+ triggers the synaptic vesicles to release acetylcholine in multimolecular quantities (quanta) into the synaptic cleft. A quantum is approximately equivalent to 20,000 acetylcholine molecules.
c . The released acetylcholine binds to acetylcholine receptors located on the peaks of the postsynaptic membrane.
d. These acetylcholine receptors are transmitter-gated Na+ ion channels, and the binding of acetylcholine results in a conformational change of the gate, permitting the influx of Na + ions, resulting in depolarization of the sarcolemma and generation of an action potentia l .
e . The enzyme acetylcho l inesterase, located in the external lamina lining the junctional folds of the motor end plate, degrades acetylcholine, thus ending the depolarizing signal to the muscle cell.
l!1lllJ1llllj M usc le 1 33
f. Acetylcholine is recycled as chol ine and is returned to the axon terminal to be recombined with acetyl coenzyme A (CoA) (from mitochondria) under the influence of the enzyme cho l ine acetyl transferase to form acetylcholine, which is then stored in synaptic vesicles.
g . Membranes of the emptied synaptic vesicles are recycled via c lathrin-coated endocytic vesic les (see Figure 3.5 in Chapter 3, Cytoplasm and Organelles).
CLIN ICAL CONSIDERATIONS
Amyotrophic latera l sclerosis ( o r Lou Gehrig d isease) i s m a rked by de g e n e rati on o f moto r n e u rons of th e s p i n a l c o rd , resu lti n g i n musc l e atro
phy. D e ath i s u sua l ly d u e to resp i rato ry musc l e fa i l u re . Myasthen ia gravis i s a n autoimmune d isease i n wh i c h antibodies b lock acetylcho l ine recep
tors of myoneu ra l j u n cti ons , red u c i n g th e n u m b e r of s ites ava i l a b l e fo r i n it iati on of sa r co l emma d epo l a rizati on .
1 . Myasthen i a g ravis is c h a ra cte r ized by g r a dua l weaken i ng o f ske l eta l musc l es, e spec i a l ly t he most a ctive ones ( e . g . , m usc l e s o f th e eyes, ton g u e, fa ce , a n d extrem iti es ) . D e ath may resu lt from resp i rato ry com promise a n d p u lmona ry infecti ons .
2. C l i n i ca l s i gns i nc l ude thym i c hyp e rp l as i a (thymo m a ) a n d the presen c e of c i rc u l ati ng a nti bod i e s to a c etyl c ho l i n e rece pto rs.
Botu l ism i s a form of food poison ing c a used by i n g esti on of Clostridium botulinum toxi n , wh i c h i n h i b its a c etyl c ho l i n e re l ease a t myo n e u ra l j u n ctions . B otu l i sm is ma rked b y musc l e p a ra lys is , vomiti ng , n a usea , and vis u a l d i so rde rs and i s fata l if u ntreated .
B. The muscle sp ind le (neuromuscu lar sp ind le ) i s an elongated, fusiform sensory organ within skeletal muscle that functions primarily as a stretch receptor. 1 . Structure
a . It is bounded by a connective tissue capsule enclosing the fluid-filled periaxia l space and 8 to 10 modified skeletal muscle fibers ( i ntrafusal f ibers) .
b . Normal skeletal muscle fibers (extrafusa l f ibers) surround it. c. It is anchored via the capsule to the perimysium and endomysium of the extrafusal fibers.
2. Function a . Stretch ing of a muscle also stretches the muscle spindle and thus stimulates the afferent
nerve endings to send impulses to the central nervous system. The response is to both the rate (phasic response) and the duration (ton ic response) of stretching.
b. Depolarization of y-efferent neurons also stimulates the intrafusal nerve endings; the rate and duration of the stimulation are monitored in the same way as stretching.
c. Muscle overst imulation results from stretching at too great a frequency or for too long a time. Overstimulation causes stimulation of a-efferent neurons to the muscle, initiating contraction and thus counteracting the stretching.
C. The Golg i tendon organ, located in tendons, counteracts the effects of muscle spindles. 1 . Structure. It is composed of encapsulated col lagen f ibers that are surrounded by terminal
branches of type lb sensory nerves. 2. It is stimulated when the muscle contracts too strenuously, increasing tension on the tendon.
Impulses from type Ib neurons i nh ib it a-efferent (motor) neurons to the muscle, preventing further contraction.
A. Genera l features-card iac muscle cel ls (Table 8.3). Cardiac muscle cells have the following features : 1 . Contract spontaneously and d isp lay a rhythmic beat, which is modified by hormonal and
neural (sympathetic and parasympathetic) stimuli. 2. May branch at their ends to form connections with adjacent cells.
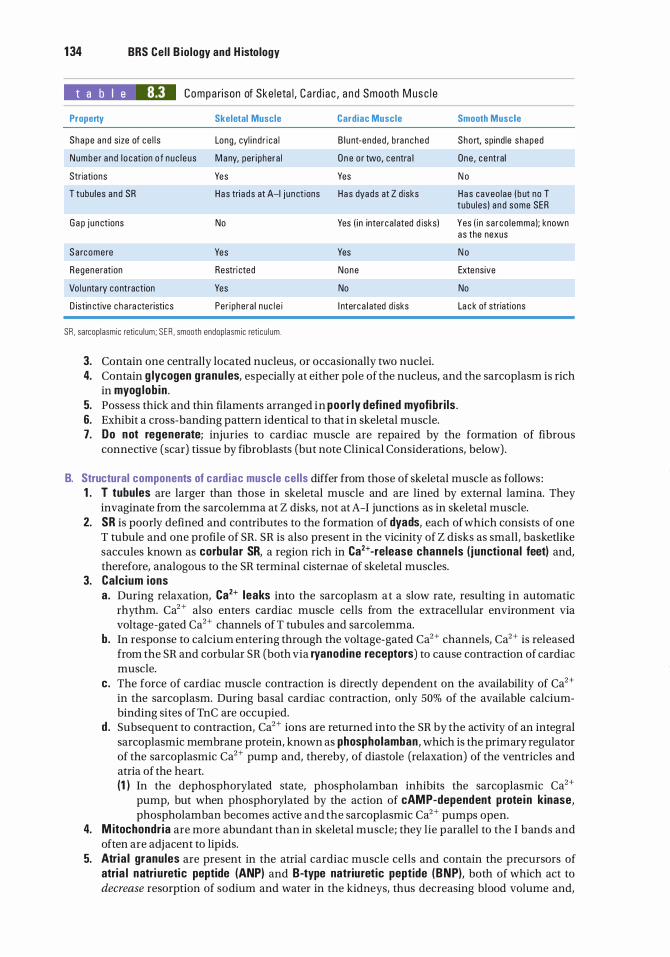
1 34 BRS Cel l B iology and H istology
t a b I e 8.3 Compa ri son of Ske l eta l , C a rd i a c , a n d Smooth M usc l e
Property
Shape a nd size of ce l l s
Numbe r a nd l o cat ion o f nuc l eus
Striations
T tubu les a nd SR
G a p j u nct ions
S a rcomere
Regeneration
Vo l u nta ry contraction
D istin ctive c h a ra cte risti cs
Skeletal Muscle
Long , cyl i nd r i ca l
M any, per i phera l
Yes
Has tri a d s at A-1 j u n ct ions
No
Yes
Restri cted
Yes
Per iphera l n u c l e i
SA , sarcop lasmic reti cu l um ; S E A , smooth endop lasmic reti cu l um .
Cardiac Muscle
B l u nt-ended , b ra n ched
O n e o r two, c entra l
Yes
Has dyads at Z d isks
Smooth Muscle
Short, sp ind le shaped
One , c entral
N o
H a s caveo lae ( b ut no T tubu les ) a nd some SER
Yes ( i n inte rca l ated d isks) Yes ( i n sa rco l emma ); known as the nexus
Yes N o
None Extensive
No No
I nterc a l ated d isks La c k of striations
3. Contain one centrally located nucleus, or occasionally two nuclei. 4. Contain g lycogen g ranu les, especially at either pole of the nucleus, and the sarcoplasm is rich
in myog lob in . 5. Possess thick and thin filaments arranged in poor ly defi ned myofibr i ls . 6. Exhibit a cross-banding pattern identical to that in skeletal muscle. 7. Do not regenerate; injuries to cardiac muscle are repaired by the formation of fibrous
connective (scar) tissue by fibroblasts (but note Clinical Considerations, below) .
B. Structural components of card iac muscle cel ls differ from those of skeletal muscle as follows : 1 . T tubules are larger than those in skeletal muscle and are lined by external lamina. They
invaginate from the sarcolemma at Z disks, not at A-I junctions as in skeletal muscle. 2. SR is poorly defined and contributes to the formation of dyads, each of which consists of one
T tubule and one profile of SR. SR is also present in the vicinity of Z disks as small, baskedike saccules known as corbu lar SR, a region rich in Ca2+·release channels ( j unctional feet) and, therefore, analogous to the SR terminal cisternae of skeletal muscles.
3. Calc ium ions a . During relaxation, Ca2+ leaks into the sarcoplasm at a slow rate, resulting in automatic
rhythm. Ca2+ also enters cardiac muscle cells from the extracellular environment via voltage-gated Ca2+ channels of T tubules and sarcolemma.
b. In response to calcium entering through the voltage-gated Ca2+ channels, Ca2+ is released from the SR and corbular SR (both via ryanodine receptors) to cause contraction of cardiac muscle.
c. The force of cardiac muscle contraction is directly dependent on the availability of Ca2+ in the sarcoplasm. During basal cardiac contraction, only 50% of the available calciumbinding sites of TnC are occupied.
d . Subsequent to contraction, Ca2+ ions are returned into the SR by the activity of an integral sarcoplasmic membrane protein, known as phospholamban, which is the primary regulator of the sarcoplasmic Ca2+ pump and, thereby, of diastole (relaxation) of the ventricles and atria of the heart. (1 ) In the dephosphorylated state, phospholamban inhibits the sarcoplasmic Ca2+
pump, but when phosphorylated by the action of cAMP-dependent prote in kinase, phospholamban becomes active and the sarcoplasmic Ca2+ pumps open.
4. M itochondr ia are more abundant than in skeletal muscle; they lie parallel to the I bands and often are adjacent to lipids.
5. Atria l granules are present in the atrial cardiac muscle cells and contain the precursors of atria l natri uretic peptide (ANP) and B-type natriuretic peptide (BNP), both of which act to decrease resorption of sodium and water in the kidneys, thus decreasing blood volume and,
l!1lllJ1llllj M usc le 1 35
thereby, reducing blood pressure. ANP and BNP act by inhibiting the release of renin from the juxtaglomerular cells of the kidney and aldosterone from the suprarenal cortex. Additionally, both ANP and BNP hinder vascular smooth muscle contraction, further reducing blood pressure. Ventricular cardiac muscle cells, if stretched much greater than under normal conditions, release both peptides.
6. Interca lated d isks (Figures 8.4a, 8.4b, and 8.5) are complex step-like junctions forming endto-end attachments between adjacent cardiac muscle cells. a. The transverse portion of interca lated d isks runs across muscle fibers at right angles and
possesses three specializations : fasc iae adherentes (analogous to zonula adherentes) to which actin filaments attach, desmosomes (macula adherentes), and gap junctions (see Chapter 5 II) .
b. The l atera l portion of intercalated d isks has desmosomes and numerous large gap junctions, which facilitate ion ic coup l i ng between cells and aid in coordinating contraction; thus, cardiac muscle behaves as a functiona l syncytium.
7. Their thin filaments are secured to the Z disk by a-actinin as well as by nebulette, a nebulinlike molecule that, unlike nebulin in skeletal muscle, extends only as far as the proximal 25% of the length of the thin filament.
8. Connective tissue e lements support a rich capillary bed that supplies sufficient nutrients and oxygen to maintain the high metabolic rate of cardiac muscle. At least 90% of the energy production of cardiac muscle cells is generated by aerobic respiration.
9. Purkinje f ibers are mod ified cardiac muscle cells located in the bund le of H is . They are specialized for conduction and contain a few peripheral myofibrils. a. These large, pale cells are rich in glycogen and mitochondria. b. They form gap junctions, fasciae adherentes, and desmosomes with cardiac muscle cells
(but not through typical intercalated disks) .
Alth ough it was mentioned ea r l i e r that no new ca r d i a c m usc l e c e l l s CLIN ICAL CONSIDERATIONS c a n be g e n e rated i n the a d u lt h u m a n, re c e nt stud i e s p e rfo rmed on t is
sue sou rces p ro c u red from the Karo l i nska I n stitute i n Sweden and from th e UK H u m a n Tissue B a n k i n G reat B rita i n , b a s e d on t h e 1 4C leve ls i n t h e D NA o f h e a rt m u s c l e s o f i n d ivi d u a ls w h o were bo rn before the n u c l e a r bomb testi ng began , showed oth e rwise . It a p p e a rs that a p p roximately 1 % of the h e a rt musc l e fi b e rs of 20-yea r-o l d i n d ivi d u a ls a n d a l most 50% of the c a rd i a c musc l e ce l l s of 50-yea r-o l d i n d iv id u a l s were form ed afte r these i n d iv id ua l s were bo rn .
Myocard ia l i nfarct i s a n i rreve rs i b l e n e c ros is of c a rd i a c musc l e ce l l s d u e to p ro l onged i schem ia ( i s chem ia l a sti ng fo r mo re th a n a p p roximately 20 m i n utes) . Dyi n g a n d d e ad ca rd i ac musc l e ce l l s re l ease c re ati n e phosphoki n ase , c reati ne phosphoki nase MB i soenzyme, a n d c a rd i o cyte s pec ifi c tropon i n I , a n d th ese th ree substa n ces-espec i a l ly th e l a st-a re i n d i c ative of a myo c a rd i a l i nfa rct, a c ond itio n that may res u lt in d eath if the c a rd i a c musc l e d a m a g e is extens ive .
A. Structure-smooth muscle ce l ls (see Table 8.3; Figures 8.6 and 8.7) . Smooth muscle cells are nonstriated , fusiform cells that range in length from 20 J..Lm in small blood vessels to 500 J..Lm in the uterus of pregnant women. They contain a single nucleus and actively divide and regenerate. They are surrounded by an external lamina and a reticular fiber network and may be arranged in layers, small bundles, or helices (in arteries) . 1 . Nucleus
a. The centrally located nucleus may not be visible in each cell in cross sections of smooth muscle because some nuclei lie outside the plane of section.
b. The nucleus in longitudinal sections of contracted smooth muscle has a corkscrew shape and is deeply indented .
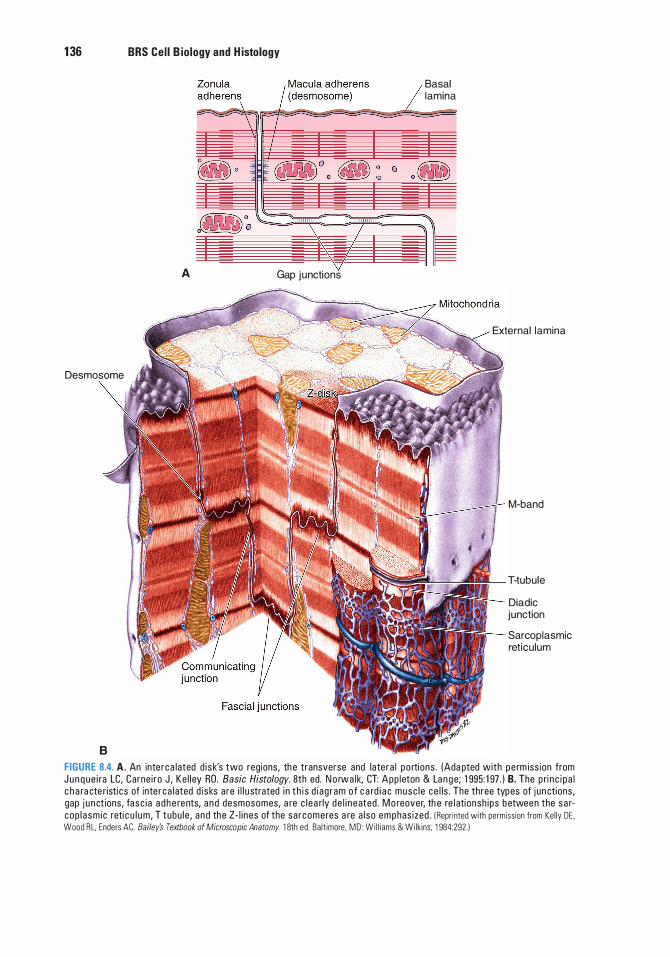
1 36 BRS Cel l B iology and H istology
A Gap junctions
Desmosome
8
Basal lamina
External lamina
M-band
T-tubule
Diadic junction
Sarcoplasmic reticulum
FIGURE 8.4. A. An inte rca lated d i sk's two reg ions, th e transverse and late ra l po rti ons . (Ada pted with pe rm iss ion from J u n q ue i ra LC, Carne i ro J , Ke l l ey RO. Basic Histology. 8th ed. N o rwa lk, CT: App l eton & La n g e; 1 995: 1 97 . ) B. The p ri n c i p a l c h a ra cte r isti cs of inte r ca l ated d i sks are i l l u strated i n t h i s d i ag ram o f c a rd i a c musc l e ce l ls . The three types of j un ctions , gap j u n ct ions, fa sc i a a d h e re nts, a nd desmosomes, a re c l e a rly de l i n eated . M o reover, th e re l ati onsh i ps b etwee n the s a rcop l a sm i c reti c u l u m, T tubu le , a nd the Z - l i nes of the sa rcomeres a re a l so emphas ized . I Repri nted with permiss ion from Ke l ly DE . Wood R L. Enders AC. Bailey's Textbook of Microscopic Anatomy. 1 8th ed . Ba lt imore . MD : Wi l l iams & Wi lk ins ; 1 984:292.)
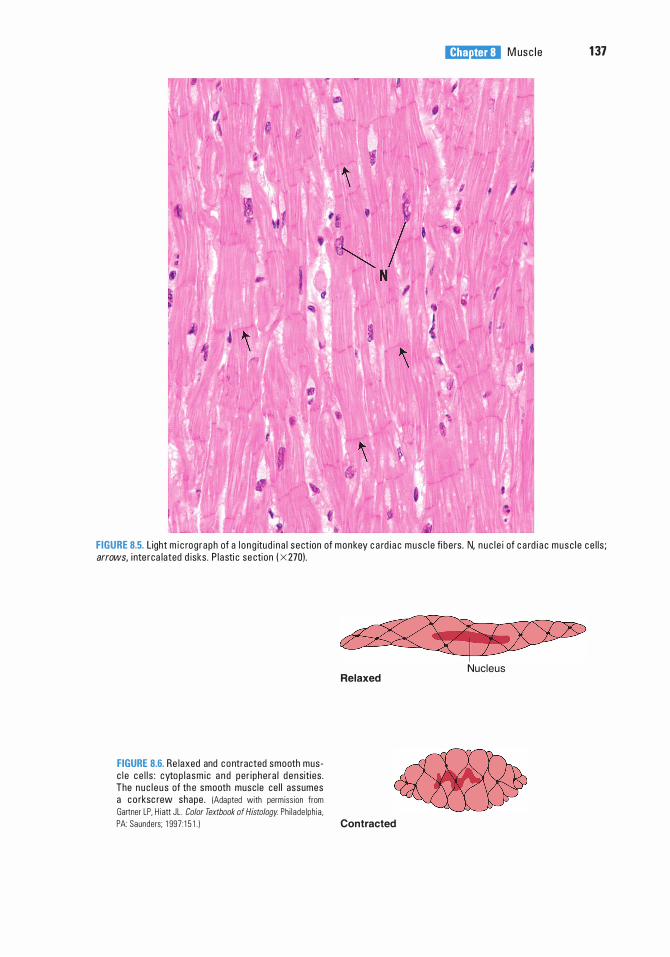
l!1lllJ1llllj M usc l e 1 37
FIGURE 8.5. L ight m i c rog raph of a l o n g itud i n a l sect ion of monkey c a rd i a c musc l e fi be rs . N, n u c l e i of c a rd i a c musc l e c e l l s ; arrows, i nte rca lated d isks . P l asti c se ction ( X 270).
FIGURE 8.6. Re laxed and c o ntracted smooth musc l e ce l l s : cytop l a sm i c a n d per i phera l d ensiti es . The nuc l e us of th e smooth musc le ce l l assumes a c o rksc rew shape . !Adapted with perm iss ion from Gartner LP. H i att JL . Color Textbook of Histology Ph i lade lph ia .
Relaxed
PA: Saunders; 1 997 : 1 5 1 . ) Contracted
Nucleus
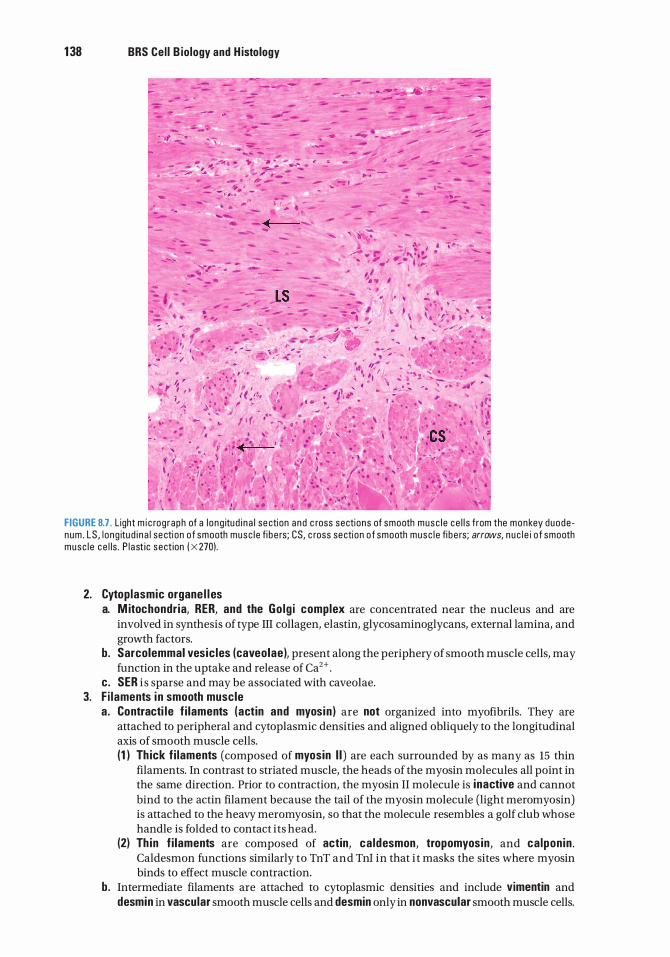
1 38 BRS Cel l B iology and H istology
. , •,
,•
�
.·
. �
' J
' ' .
FIGURE 8.7. Light m i c rog raph of a l o ng itu d i n a l se ction and c ross sections of smooth musc l e ce l l s from the monkey duode num . LS , l o ng itu d i n a l se cti on o f smooth musc l e fi b e rs; CS, c ross secti on o f smooth musc l e fi b e rs; arrows, n u c l e i o f smooth musc l e c e l ls . P l a st ic sect ion ( X 270).
2. Cytoplasmic organe l l es a. M itochondr ia, RER, and the Go lg i complex are concentrated near the nucleus and are
involved in synthesis of type III collagen, elastin, glycosaminoglycans, external lamina, and growth factors.
b. Sarcolemmal vesic les (caveolae), present along the periphery of smooth muscle cells, may function in the uptake and release of Ca2+ .
c. SER i s sparse and may be associated with caveolae. 3. F i laments i n smooth muscle
a . Contracti le f i laments (actin and myosin ) are not organized into myofibrils. They are attached to peripheral and cytoplasmic densities and aligned obliquely to the longitudinal axis of smooth muscle cells. (1 ) Th ick f i laments (composed of myosin I I ) are each surrounded by as many as 15 thin
filaments. In contrast to striated muscle, the heads of the myosin molecules all point in the same direction. Prior to contraction, the myosin II molecule is inactive and cannot bind to the actin filament because the tail of the myosin molecule (light meromyosin) is attached to the heavy meromyosin, so that the molecule resembles a golf club whose handle is folded to contact its head.
(2) Th in f i laments are composed of actin, ca ldesmon, tropomyosin , and ca lpon in . Caldesmon functions similarly to TnT and Tni in that i t masks the sites where myosin binds to effect muscle contraction.
b. Intermediate filaments are attached to cytoplasmic densities and include vimentin and desmin in vascular smooth muscle cells and desmin only in nonvascular smooth muscle cells.
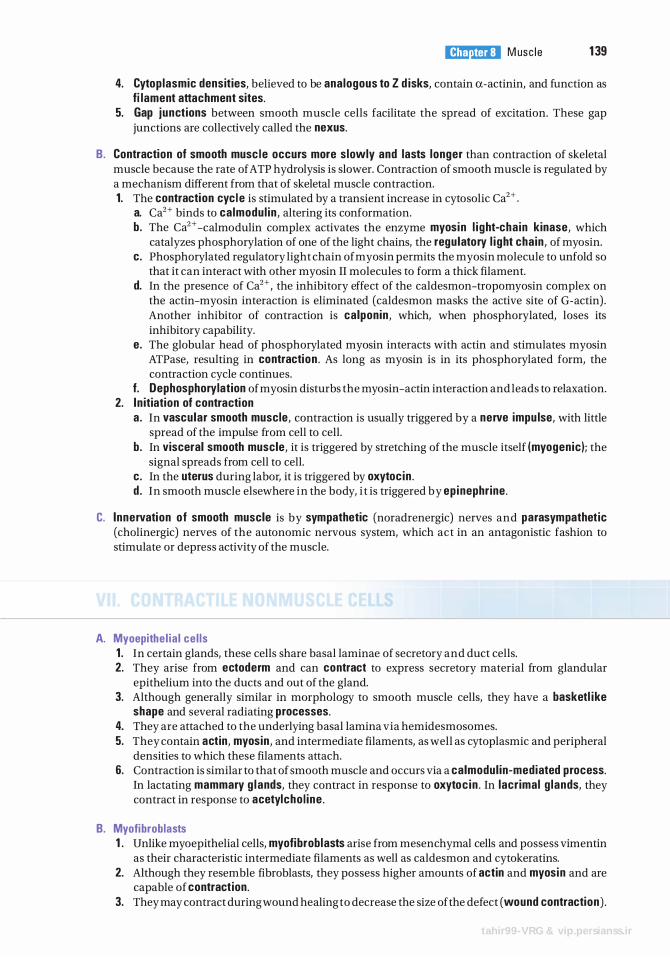
l!1lllJ1llllj M usc l e 1 39
4. Cytop lasmic densities, believed to be analogous to Z d isks, contain a-actinin, and function as fi lament attachment sites.
5. Gap junctions between smooth muscle cells facilitate the spread of excitation. These gap junctions are collectively called the nexus.
B. Contraction of smooth musc le occurs more slowly and lasts longer than contraction of skeletal muscle because the rate of ATP hydrolysis is slower. Contraction of smooth muscle is regulated by a mechanism different from that of skeletal muscle contraction. 1. The contraction cyc l e is stimulated by a transient increase in cytosolic Ca2+ .
a. Ca2+ binds to calmodul in , altering its conformation. b. The Ca2+ -calmodulin complex activates the enzyme myosin l i ght-cha in kinase, which
catalyzes phosphorylation of one of the light chains, the regulatory l i ght chain , of myosin. c. Phosphorylated regulatory light chain of myosin permits the myosin molecule to unfold so
that it can interact with other myosin II molecules to form a thick filament. d. In the presence of Ca2+ , the inhibitory effect of the caldesmon-tropomyosin complex on
the actin-myosin interaction is eliminated (caldesmon masks the active site of G-actin) . Another inhibitor of contraction is calponin , which, when phosphorylated, loses its inhibitory capability.
e. The globular head of phosphorylated myosin interacts with actin and stimulates myosin ATPase, resulting in contraction . As long as myosin is in its phosphorylated form, the contraction cycle continues.
f. Dephosphorylation of myosin disturbs the myosin-actin interaction and leads to relaxation. 2. In itiation of contraction
a . In vascular smooth muscle, contraction is usually triggered by a nerve impu lse, with little spread of the impulse from cell to cell.
b. In visceral smooth muscle, it is triggered by stretching of the muscle itself (myogenic ); the signal spreads from cell to cell.
c. In the uterus during labor, it is triggered by oxytoc in . d . In smooth muscle elsewhere in the body, i t is triggered by ep inephr ine .
C. I nnervation of smooth muscle is by sympathetic (noradrenergic) nerves and parasympathetic (cholinergic) nerves of the autonomic nervous system, which act in an antagonistic fashion to stimulate or depress activity of the muscle.
A. Myoepithe l ia l ce l ls 1 . In certain glands, these cells share basal laminae of secretory and duct cells. 2. They arise from ectoderm and can contract to express secretory material from glandular
epithelium into the ducts and out of the gland. 3. Although generally similar in morphology to smooth muscle cells, they have a basketl ike
shape and several radiating processes. 4. They are attached to the underlying basal lamina via hemidesmosomes. 5. They contain actin, myosin , and intermediate filaments, as well as cytoplasmic and peripheral
densities to which these filaments attach. 6. Contraction is similar to that of smooth muscle and occurs via a calmodul in-mediated process.
In lactating mammary g l ands, they contract in response to oxytoc in . In lacr imal g lands, they contract in response to acetylcho l ine .
B. Myofibroblasts 1 . Unlike myoepithelial cells, myofibroblasts arise from mesenchymal cells and possess vim en tin
as their characteristic intermediate filaments as well as caldesmon and cytokeratins. 2. Although they resemble fibroblasts, they possess higher amounts of actin and myosin and are
capable of contraction. 3. They may contract during wound healing to decrease the size of the defect (wound contraction) .
tahir99-VRG & vip.persianss.ir
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which of the following is true for mammalian skeletal muscle?
(A) T tubules are located at the Z disk. (B ) T tubules are absent. (C) Troponin is absent. (D ) It possesses triads. (E) It possesses caveolae.
2. Which of the following is true for cardiac muscle?
(A) T tubules are located at the Z disk. (B ) T tubules have a smaller diameter than
those of skeletal muscle. (C) Troponin is absent. (D ) It possesses triads. (E) Oxytocin triggers contraction.
3. Which of the following is true for smooth muscle?
(A) T tubules are located at the Z disk. (B ) It possesses dyads. (C) Caveolae store and release calcium ions. (D ) It possesses triads. (E) T tubules are located at the A-I interface.
4. Contraction in all types of muscle requires calcium ions. Which of the following muscle components can bind or sequester calcium ions?
(A) Rough endoplasmic reticulum (B ) Tropomyosin (C) Troponin (D ) Active sites on actin (E ) Titin
1 40
5. Each smooth muscle cell
(A) has triads associated with its contraction. (B) has dyads associated with its contraction. (C) possesses a single central nucleus. (D ) is characterized by the absence of sarco
lemmal vesicles. (E) contains troponin.
6. Thick filaments are anchored to Z disks by
(A) C protein. (B ) nebulin. (C ) titin. (D ) myomesin. (E) a-actinin.
7. The endomysium is a connective tissue investment that surrounds
(A) individual muscle fibers. (B ) muscle fascicles. (C) individual myofibrils. (D) an entire muscle. (E) small bundles of muscle cells.
8. Which of the following statements concerning triads in mammalian skeletal muscle is true?
(A) They are located in the Z disk. (B ) They consist of two terminal cisternae of
the SR separated by a T tubule. (C) They can be observed with the light
microscope. (D) They are characterized by a T tubule that
sequesters calcium ions. (E) They consist of two T tubules separated by
a central terminal cisterna.
tahir99-VRG & vip.persianss.ir

9. Which one of the following statements concerning cardiac muscle cells is true?
(A) They are spindle shaped. (B) They require an external stimulus to
undergo contraction. (C) They are multinuclear cells. (D ) They are joined together end to end by
intercalated disks. (E) They possess numerous caveolae.
l!1lllJ1llllj M usc I e 1 41
1 0. A 19-year-old male patient and his mother arrive in the emergency department, both with nausea, vomiting, and visual disorders. The physician taking their history notes that they both had canned green beans that tasted funny. Which of the following possibilities should the physician consider?
(A) Duchenne muscular dystrophy (B ) Amyotrophic lateral sclerosis (C) Botulism (D ) Myasthenia gravis (E ) Myocardial infarct
tahir99-VRG & vip.persianss.ir
Answers and Explanations
1 . D . The T tubules of skeletal muscle cells are positioned so that they form triads with the terminal cisternae of the SR at the interface of the A and I bands (see Chapter 8 II C) .
2. A. The T tubules of cardiac muscle cells are wider than those of skeletal muscle cells and are lined by external lamina (a basal lamina-like material) . In contrast to skeletal muscle, the T tubules are located at the Z disk, where they often form dyads, not triads (see Chapter 8 V B 6).
3. C. Smooth muscle cells do not have T tubules. Contraction may be initiated by stretching, neural impulses, the intercellular passage of small molecules via gap junctions, or the action of hormones such as oxytocin. Contraction is not dependent on troponin, which is absent from the thin filament of smooth muscle. Instead, Ca2+ controlled by sarcolemmal vesicles known as caveolae is released into the cytosol, where it binds with calmodulin. The calcium-calmodulin complex activates myosin light-chain kinase, which participates in the contraction process (see Chapter 8 VI A 2) .
4. C. Binding of Ca2+ to the TnC subunit of troponin leads to the uncovering of myosin -binding sites on actin (thin filaments) (see Chapter 8 II F l c) .
5. C. Smooth muscle cells contain one centrally located nucleus (see Chapter 8 VI A l ) .
6. C. Titin forms an elastic lattice that anchors thick filaments to Z disks (see Chapter 8 II F 2 c) .
7. A. The endomysium is a thin connective tissue layer composed of reticular fibers and an external lamina that invests individual muscle fibers (cells). The epimysium surrounds the entire muscle, and the perimysium surrounds bundles (fascicles) of muscle fibers (see Chapter 8 II A 3) .
8. B . A triad in skeletal muscle is composed of three components : a T tubule and two terminal cisternae of the SR that flank it. The SR, not the T tubules, sequesters Ca2+ (see Chapter 8 II C 4).
9. D . Cardiac muscle cells are joined together end to end by a unique junctional specialization called the intercalated disk (see Chapter 8 V B 6).
1 0. C. Botulism is the only possible consideration, especially since they both had canned food.
1 42
Duchenne muscular dystrophy is most common in young men but very rare in older women. It would be highly unlikely that both mother and son would show symptoms of amyotrophic lateral sclerosis or myasthenia gravis or have myocardial infarct at the same time (see Chapter 8 II E Clinical Considerations) .
tahir99-VRG & vip.persianss.ir
Nervous System
I. OVERVIEW-NERVOUS SYSTEM
The nervous system can be organized by anatomical or functional divisions.
A. Nervous system is divided anatomical ly into the centra l nervous system (CNS), which includes the brain and spinal cord encased in the skull and vertebral column, and the peripheral nervous system (PNS), which includes the nerves outside the CNS and their associated ganglia as well as connections to the CNS, including the receptors and motor components of the peripheral nerves of the body.
B. Nervous system is divided functional ly into a sensory component, which transmits electrical impulses (signals) to the CNS, and a motor component, which transmits impulses from the CNS to various structures of the body. The motor component is further divided into the somatic and autonomic systems. The somatic nervous system (SNS), located within both the CNS and PNS, controls sensory and motor functions of all conscious voluntary actions. However, it does not control functions related to smooth or cardiac muscles, reflex arcs, or glands.
The autonomic nervous system (ANS) functions to regulate the internal organs. It is further subdivided into the sympathetic, parasympathetic, and enteric systems. The sympathetic nervous system readies the body for action against hostile situations, resulting in "flight or fight or freeze;' whereas the parasympathetic nervous system is "calming" and supplies secretomotor innervation to most exocrine glands. The enteric nervous system, a very large component of the autonomic system, serves the digestive system. Although it operates independently, both the sympathetic and the parasympathetic components are utilized in modulating the functions of the enteric system.
C. Nervous tissue contains two types of cells : nerve cel ls (neurons), which conduct electrical impulses, and supporting cells, which support, nurture, and protect the neurons within the CNS ( g l i a l [neurog l ia l ] cel ls), as well as cells located in the PNS (sate l l ite cel ls, capsule cel ls, and Schwann cel ls ) .
A. The neuroepithel ium thickens and differentiates to form the neural plate.
B. The neural p late invaginates and thickens to form the neural g roove .
C. The neural tube, a cylindrical structure that results from fusion of the edges of the neural groove, enlarges at its cranial end to form the brain . The remaining portion gives rise to the spina l cord .
1 43
tahir99-VRG & vip.persianss.ir
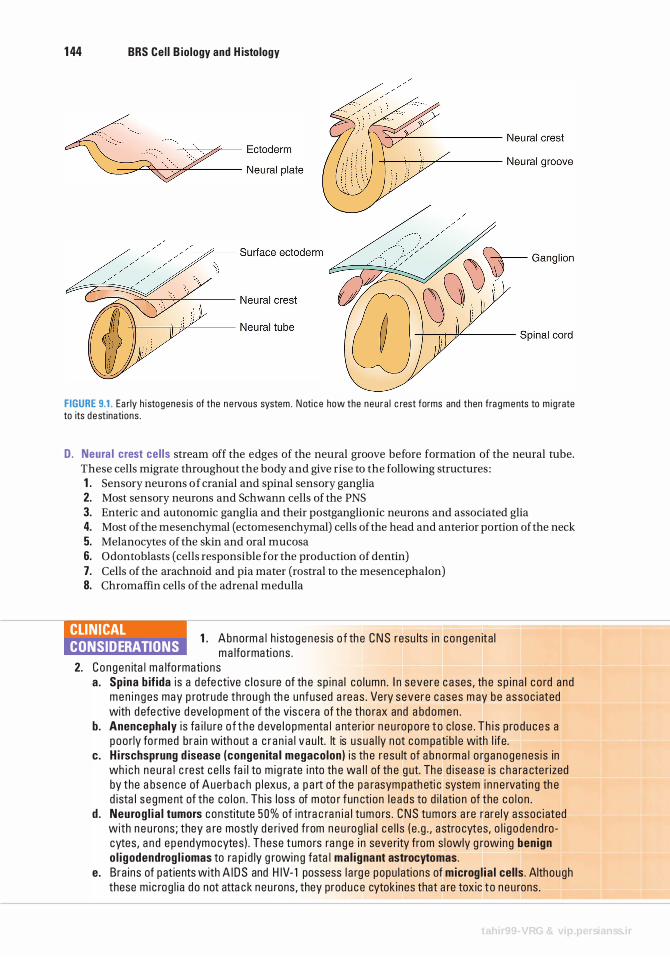
1 44 BRS Cel l B iology and H istology
FIGURE 9.1. Ea rly h i stogenes i s of the n e rvous system . N oti c e how the neu ra l c rest forms and then fra g m e nts to m i g rate to its dest inations .
D. Neura l crest cel ls stream off the edges of the neural groove before formation of the neural tube. These cells migrate throughout the body and give rise to the following structures : 1 . Sensory neurons of cranial and spinal sensory ganglia 2. Most sensory neurons and Schwann cells of the PNS 3. Enteric and autonomic ganglia and their postganglionic neurons and associated glia 4. Most of the mesenchymal ( ectomesenchymal) cells of the head and anterior portion of the neck 5. Melanocytes of the skin and oral mucosa 6. Odontoblasts (cells responsible for the production of dentin) 7. Cells of the arachnoid and pia mater (rostral to the mesencephalon) 8. Chromaffin cells of the adrenal medulla
CLIN ICAL CONSIDERATIONS
1 . Abnorm a l h i stogenes is o f th e C N S resu lts i n c o ngen ita l m a lfo rmati ons .
2. Congen ita l ma lfo rmations a. Sp ina b if ida i s a d efe ctive c l o su re of th e sp i na l co l umn . I n severe c ases , th e sp i n a l c o rd and
men i n g es may p rotrude thro u gh th e unfused a reas . Ve ry severe cases m ay be assoc i ated with d efe ctive d eve l o pment of th e vis c e ra of the tho rax and a bdomen .
b. Anencephaly i s fa i l u re o f t h e d eve l o pmenta l a nter io r n e u ropo re t o c l ose . Th i s p ro d u ces a poo rly fo rmed b ra i n with out a c r a n i a l vau lt. It is u sua l ly not com pati b l e with l ife .
c. H i rschsprung d isease (congenita l megacolon) i s th e resu lt of a b no rm a l o rg anogen es is in wh i c h n e u ra l c rest ce l l s fa i l to m i g rate i nto th e wa l l of th e g ut. The d i sease is c h a ra cte r ized by the a bsence of Aue rb a c h p l exus, a p a rt of th e pa rasym path eti c system i n ne rvati n g th e d ista l s egment of the co l o n . Th is loss of moto r fun cti on l e ads to d i l atio n of the co l o n .
d . Neurog l ia l tumors constitute 50% of i ntra c ra n i a l tumo rs . CNS tumo rs a re rare ly assoc i ated with n e u rons ; they a re mostly d e rived from n e u rog l i a l c e l l s ( e . g . , a stro cytes, o l i g o dend rocytes, a n d e p endymocytes ) . These tumors ra n ge i n seve rity from s l owly g rowing benign o l igodendrog l i omas to ra p i d ly g rowin g fata l mal ignant astrocytomas.
e . Bra ins of patients with A I D S and H IV- 1 possess l a rg e popu l ations of microg l ia l cel ls . Although these m i c rog l i a do not atta ck neu rons, they prod uce cytok ines that a re toxic to neu rons .
tahir99-VRG & vip.persianss.ir
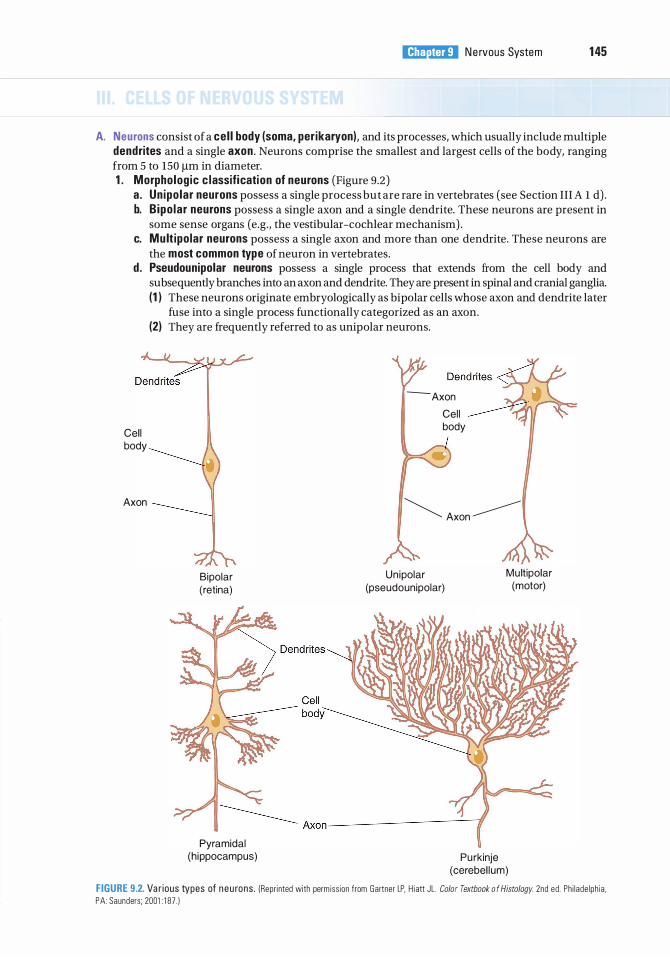
i!1llll'1ttDll N e rvous System 1 45
A. Neurons consist of a cel l body (soma, perikaryon), and its processes, which usually include multiple dendrites and a single axon . Neurons comprise the smallest and largest cells of the body, ranging from 5 to 150 J.!m in diameter. 1 . Morpholog ic c lassification of neurons (Figure 9.2)
a. Un ipo lar neurons possess a single process but are rare in vertebrates (see Section III A l d) . b. B ipo lar neurons possess a single axon and a single dendrite. These neurons are present in
some sense organs (e.g., the vestibular-cochlear mechanism) . c. Mult ipo lar neurons possess a single axon and more than one dendrite. These neurons are
the most common type of neuron in vertebrates. d . Pseudounipolar neurons possess a single process that extends from the cell body and
subsequently branches into an axon and dendrite. They are present in spinal and cranial ganglia. (1 ) These neurons originate embryologically as bipolar cells whose axon and dendrite later
fuse into a single process functionally categorized as an axon.
Cell body
Axon
(2) They are frequently referred to as unipolar neurons.
Bipolar (retina)
Pyramidal (h ippocampus)
- Axon
Cel l body
� Axon ----------
Unipolar (pseudounipolar)
Mu ltipolar (motor)
Purkinje (cerebel lum)
FIGURE 9.2. Va r ious types of n eu rons . (Repri nted with perm iss ion from Gartner LP, H i att JL . Color Textbook o f Histology. 2nd ed . Ph i l ade lph ia , PA: Saunders; 2001 : 1 87 . )
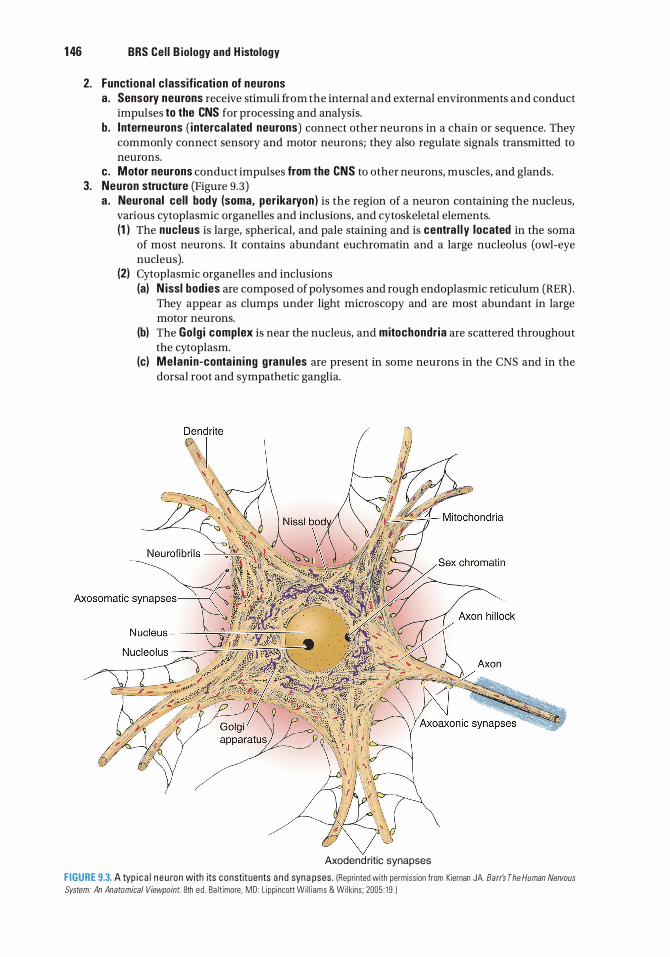
1 46 BRS Cel l B iology and H istology
2. Functiona l c lassification of neurons a . Sensory neurons receive stimuli from the internal and external environments and conduct
impulses to the CNS for processing and analysis. b. lnterneurons ( interca lated neurons) connect other neurons in a chain or sequence. They
commonly connect sensory and motor neurons; they also regulate signals transmitted to neurons.
c. Motor neurons conduct impulses from the CNS to other neurons, muscles, and glands. 3. Neuron structure (Figure 9.3)
a . Neuronal cell body (soma, per ikaryon ) is the region of a neuron containing the nucleus, various cytoplasmic organelles and inclusions, and cytoskeletal elements. (1 ) The nucleus is large, spherical, and pale staining and is centra l ly located in the soma
of most neurons. It contains abundant euchromatin and a large nucleolus (owl-eye nucleus).
(2) Cytoplasmic organelles and inclusions (a) N issl bodies are composed of polysomes and rough endoplasmic reticulum (RER) .
They appear as clumps under light microscopy and are most abundant in large motor neurons.
(b) The Golg i complex is near the nucleus, and mitochondr ia are scattered throughout the cytoplasm.
(c) Melan in-conta in ing g ranu les are present in some neurons in the CNS and in the dorsal root and sympathetic ganglia.
Axodendritic synapses
FIGURE 9.3. A typ i c a l n e u ron with its constituents a n d syna pses . (Repri nted with permiss ion from Kiernan JA. Barr's The Human Nervous
System: An Anatomical Viewpoint. 8th ed . Ba lt imore , MD : L ipp incott Wi l l i ams & Wi lkins ; 2005 : 1 9 . )
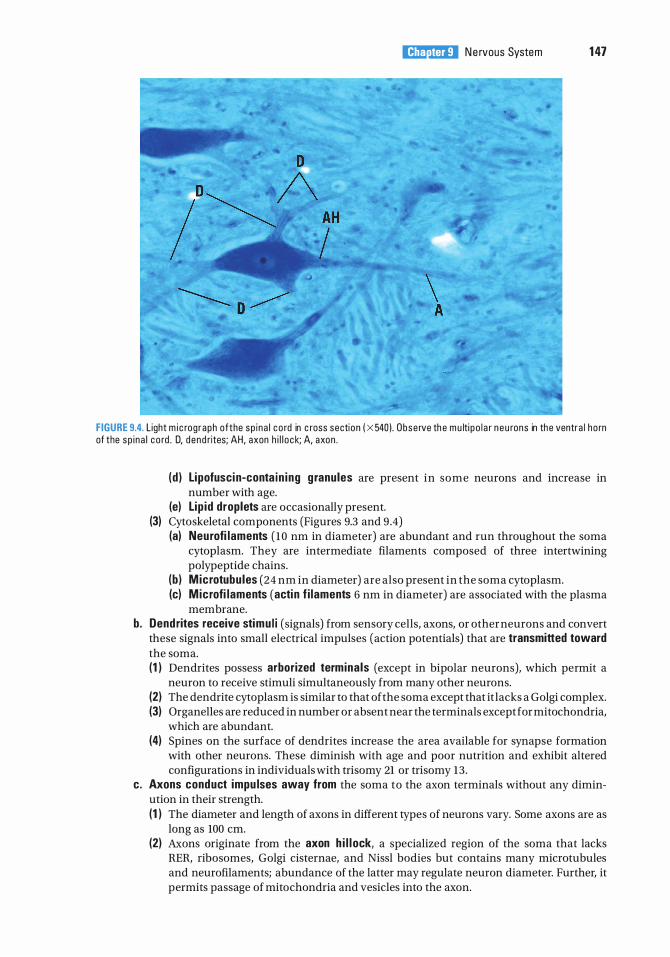
i!1llll'1ttDll N e rvous System 1 47
FIGURE 9.4. L ight m i c rog raph ofthe sp i na l c o rd in c ross section ( X 540 l . Obse rve th e m u lti p o l a r n e u rons in the ventra l ho rn of the sp i na l c o rd . D, d end rites; AH, axon h i l l o ck; A, axon .
(d ) Lipofuscin-conta in ing g ranules are present in some neurons and increase in number with age.
(e) Lip id droplets are occasionally present. (3) Cytoskeletal components (Figures 9.3 and 9 .4)
(a) Neurofi laments ( 10 nm in diameter) are abundant and run throughout the soma cytoplasm. They are intermediate filaments composed of three intertwining polypeptide chains.
(b ) Microtubu les (24 nm in diameter) are also present in the soma cytoplasm. (c) Microfi laments (acti n f i laments 6 nm in diameter) are associated with the plasma
membrane. b. Dendrites receive stimu l i (signals) from sensory cells, axons, or other neurons and convert
these signals into small electrical impulses (action potentials) that are transmitted toward the soma. (1 ) Dendrites possess arborized termina ls (except in bipolar neurons), which permit a
neuron to receive stimuli simultaneously from many other neurons. (2) The dendrite cytoplasm is similar to that of the soma except that it lacks a Golgi complex. (3) Organelles are reduced in number or absent near the terminals except for mitochondria,
which are abundant. (4) Spines on the surface of dendrites increase the area available for synapse formation
with other neurons. These diminish with age and poor nutrition and exhibit altered configurations in individuals with trisomy 21 or trisomy 13 .
c. Axons conduct impu lses away from the soma to the axon terminals without any diminution in their strength. (1 ) The diameter and length of axons in different types of neurons vary. Some axons are as
long as 100 em. (2) Axons originate from the axon h i l l ock, a specialized region of the soma that lacks
RER, ribosomes, Golgi cisternae, and Nissl bodies but contains many microtubules and neurofilaments; abundance of the latter may regulate neuron diameter. Further, it permits passage of mitochondria and vesicles into the axon.
1 48 BRS Cel l B iology and H istology
(3) Axons may have co l latera ls, branching at right angles from the main trunk. (4) Axon cytoplasm (axoplasm) lacks a Golgi complex but contains smooth endoplasmic
reticulum (SER), RER, and elongated mitochondria. (5) A plasma membrane surrounding the axon is called the axolemma. (6) Axons terminate in many small branches (axon terminals) from which impulses are
passed to another neuron or other types of cells.
CLIN ICAL CONSIDERATIONS
Alzheimer d isease i s the most common c a use o f d ementi a . I t i s the s ixth l e a d i n g c ause of d eath in the U n ited States a n d is cons i de red to be a
d i sease of the a g ed . Cu rrently, a bout 5 .2 m i l l i o n p e rsons i n the U n ited States have been d i a g nosed with Alzh e ime r d isease , of whom five m i l l i on a re a g ed 65 a n d o l de r a n d 200,000 a re yo unge r tha n 6 5 yea rs o f a g e . I t is estimated that i n 20 1 3 Alzh e ime r d isease i s expe cted t o cost the U n ited States $203 b i l l i o n , wh i ch i s expe cted to rise to $1 .2 tri l l i o n by 2050. Alzh e ime r d i sease sta rts with memo ry loss a n d confus ion , loss of fi n d i n g words, loss of a bstra ct th i nk i ng , d i sor i entati on , a n d d e p ress ion , fo l l owed by i rr ita b i l ity a n d mood swings with a g g ress i on . Fi n a l ly, th e re i s with d rawa l a n d d e c l i n e of senses a n d th e loss of bod i ly fu n cti ons . I t a p p e a rs that a c omb i n ati o n of g e neti cs , l ifestyl e , and th e env i ro nment p l ays a ro l e in tri g g e ri n g th e onset. The d isease is c h a ra cte r ized by th e loss of n e u rons a n d syna pses ma i n ly with i n the c e re b ra l c o rtex fo l l owed by atro phy o f the i n d iv id u a l c e re b ra l l obes . Pat ients with Alzh e ime r d isease deve l o p � -amy lo i d p l aques a n d n e u rofi b ri l l a ry ta ng l e s that ren d e r t h e n e u rons nonfu n ction a l . R ecent stud i es h ave shown that �-amy lo id p rote i n c a n a ct as a p r i on a n d be tra nsfe rred f rom infected n e u rons to non i nfected n e u rons by trave l i n g d own the axon of th e i nfe cted c e l l a n d ente r i ng the un i nfected c e l l v ia syna pses . Sti l l oth e r c u rrent investi g ati ons s ugg est that Alz he ime r d isease is a n e u roendoc ri n e d iso rde r, s pec ifi c a l ly type Ill d iabetes me l l itus, resu lti n g from spec ifi c d efi c i e n c i e s in i n su l i n , i n su l i n - l i ke g rowth fa cto r- 1 , a n d i n su l i n - l i ke g rowth fa ctor-2 p ro d u ction , as we l l as i n th e s c a rc ity of rec e pto rs fo r these three mo l e c u l es c o nfi n ed to c e rta i n reg ions of the b ra i n .
B. The neurog l ia l cel ls, astrocytes and oligodendroglia (as well as microglia and ependymal cells) are located only in the CNS. Schwann cells and capsule cells are their PNS equivalent cells. 1 . General characteristics. Neuroglial cells comprise several cell types and outnumber neurons
by approximately a factor of 10. These cells are embedded in a web of tissue composed of modified ectodermal elements; the entire supporting structure is termed the neurog l i a . They function to support and protect neurons, but they do not conduct impulses or form synapses with other cells; however, they do appear to provide some regulation of neurons in the process of neural transmissions. Neuroglia do that by actively monitoring synapses, removing neurotransmitter molecules from synapses, and delivering molecules known as g l iotransmitter substances, such as glutamate and ATP into the synaptic vicinity. These gliotransmitters appear to suppress synaptic transmission in cultured hippocampal neurons. Additionally, neuroglial cells possess the capacity to undergo cell division. Neuroglia are revealed in histologic sections of the CNS only with special gold and silver stains.
2. Types of neurog l ia l cel ls (Figure 9 .5) . Note that Schwann cells are also discussed in this section, but they are present only in the PNS. a. Astrocytes
( 1 ) Astrocytes are the largest of the neuroglial cells that reside in the CNS. They have many processes, some of which possess expanded pedicles (vascu lar feet) that surround blood vessels, whereas others exhibit processes that contact the pia mater.
(2) Function (a) Astrocytes scavenge ions and debris from neuron metabolism and supply energy
for metabolism. (b) Along with other components of the neuroglia, astroglia form a protective sea led
barr ier between the pia mater and the nervous tissue of the brain and the spinal cord. (c) They provide structura l support for nervous tissue. (d) They proliferate to form scar tissue (g l ia l scar) after injury to the CNS.
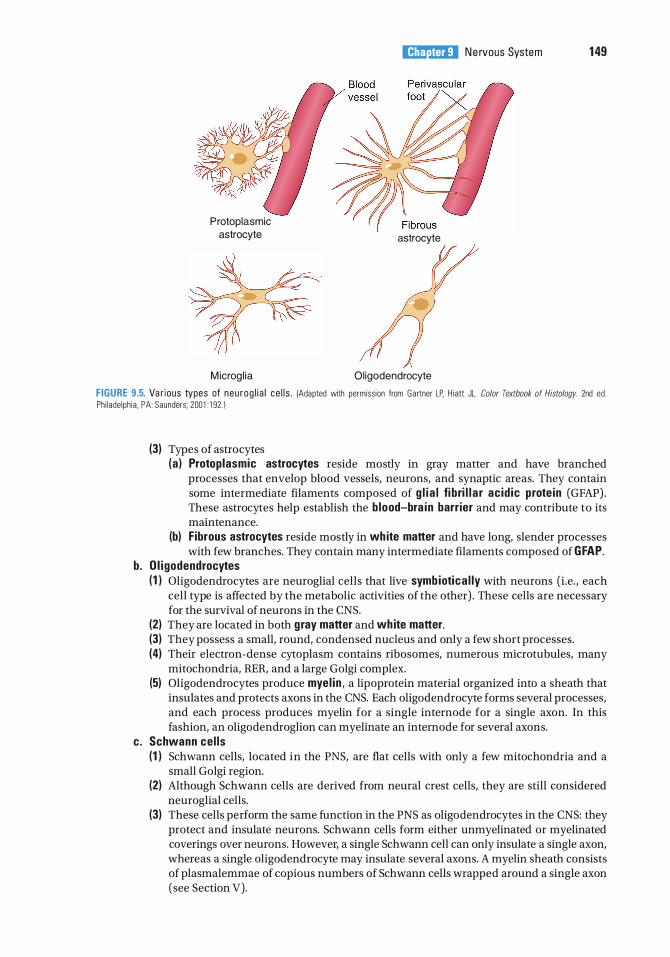
Protoplasmic astrocyte
M icrog l ia
i!1llll'1ttDll N e rvous System 1 49
astrocyte
Oligodendrocyte
FIGURE 9.5. Va r ious types of neu rog l i a l ce l l s . !Adapted with permiss ion from Ga rtner LP. H i att JL. Color Textbook of Histology. 2nd ed . Ph i lade lph ia . PA: Saunders; 200 1 : 1 92 . 1
(3) Types of astrocytes (a ) Protoplasmic astrocytes reside mostly in gray matter and have branched
processes that envelop blood vessels, neurons, and synaptic areas. They contain some intermediate filaments composed of g l i a l fi bri l l a r ac id ic prote in (GFAP) . These astrocytes help establish the b lood-bra in barrier and may contribute to its maintenance.
(b) Fibrous astrocytes reside mostly in white matter and have long, slender processes with few branches. They contain many intermediate filaments composed of GFAP.
b . O l i godendrocytes ( 1 ) Oligodendrocytes are neuroglial cells that live symb iotica l ly with neurons (i .e. , each
cell type is affected by the metabolic activities of the other) . These cells are necessary for the survival of neurons in the CNS.
(2) They are located in both gray matter and white matter. (3) They possess a small, round, condensed nucleus and only a few short processes. (4) Their electron-dense cytoplasm contains ribosomes, numerous microtubules, many
mitochondria, RER, and a large Golgi complex. (5) Oligodendrocytes produce myel in , a lipoprotein material organized into a sheath that
insulates and protects axons in the CNS. Each oligodendrocyte forms several processes, and each process produces myelin for a single internode for a single axon. In this fashion, an oligodendroglion can myelinate an internode for several axons.
c. Schwann ce l ls (1 ) Schwann cells, located in the PNS, are flat cells with only a few mitochondria and a
small Golgi region. (2) Although Schwann cells are derived from neural crest cells, they are still considered
neuroglial cells. (3) These cells perform the same function in the PNS as oligodendrocytes in the CNS: they
protect and insulate neurons. Schwann cells form either unmyelinated or myelinated coverings over neurons. However, a single Schwann cell can only insulate a single axon, whereas a single oligodendrocyte may insulate several axons. A myelin sheath consists of plasmalemmae of copious numbers of Schwann cells wrapped around a single axon (see Section V).
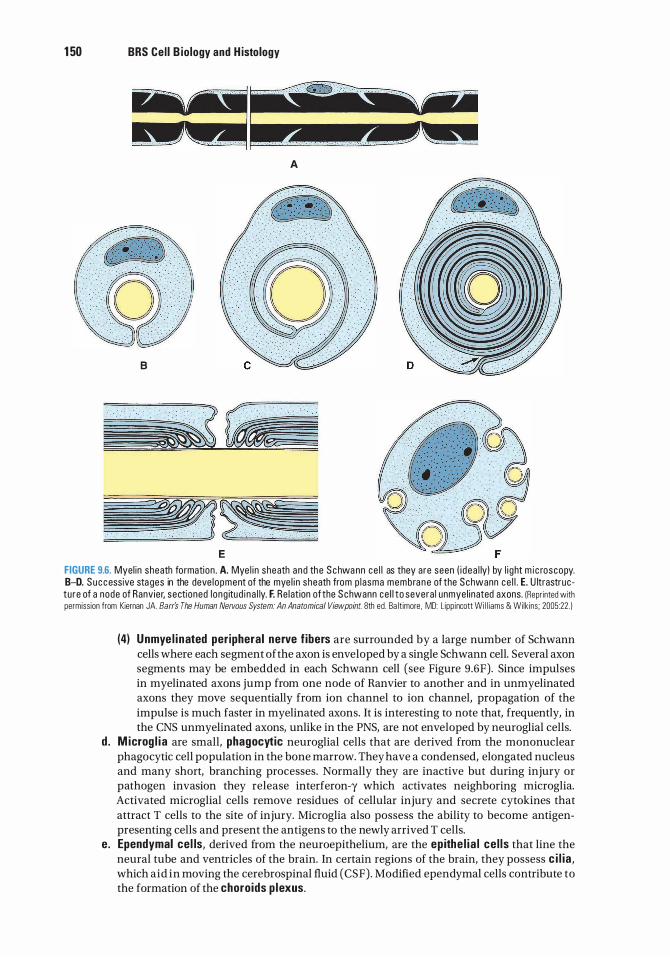
1 50 BRS Cel l B iology and H istology
8
E
A
FIGURE 9.6. Myel in sheath formation . A. Mye l i n sheath and the Schwa nn ce l l as they are seen ( i dea l ly) by l i ght m i c roscopy. B-D. Successive stages in the deve lopment of the mye l i n sheath from p lasma membra n e of the Schwann ce l l . E. U ltrastructure of a node of Ranv ier, sectioned l ong itud i na l ly. F. Re lat ion of the Schwann ce l l to severa l unmye l inated axons. IReprinted with permission from Kiernan JA. Barr's The Human Nervous System: An Anatomical Viewpoint. 8th ed. Ba lt imore, MD: L ippincott Wi l l iams & Wilk ins; 2005:22. )
(4) Unmye l inated peripheral nerve f ibers are surrounded by a large number of Schwann cells where each segment of the axon is enveloped by a single Schwann cell. Several axon segments may be embedded in each Schwann cell (see Figure 9.6F). Since impulses in myelinated axons jump from one node of Ranvier to another and in unmyelinated axons they move sequentially from ion channel to ion channel, propagation of the impulse is much faster in myelinated axons. It is interesting to note that, frequently, in the CNS unmyelinated axons, unlike in the PNS, are not enveloped by neuroglial cells.
d . M icrog l i a are small, phagocytic neuroglial cells that are derived from the mononuclear phagocytic cell population in the bone marrow. They have a condensed, elongated nucleus and many short, branching processes. Normally they are inactive but during injury or pathogen invasion they release interferon-y which activates neighboring microglia. Activated microglial cells remove residues of cellular injury and secrete cytokines that attract T cells to the site of injury. Microglia also possess the ability to become antigenpresenting cells and present the antigens to the newly arrived T cells.
e. Ependymal cel ls, derived from the neuroepithelium, are the epithe l ia l ce l ls that line the neural tube and ventricles of the brain. In certain regions of the brain, they possess c i l ia , which aid in moving the cerebrospinal fluid (CSF) . Modified ependymal cells contribute to the formation of the choroids p lexus.
IV. SYNAPSES
i!1llll'1ttDll Nervous System 1 51
Synapses are sites offunctiona l apposition where signals are transmitted from one neuron to another or from a neuron to another type of cell (e.g., muscle cell).
A. C lassification . Synapses are classified according to the site of synaptic contact and the method of signal transmission (Figure 9.3) . 1 . S ite of synaptic contact
a . Axodendritic synapses are located between an axon and a dendrite. b. Axosomatic synapses are located between an axon and a soma. The CNS primarily contains
axodendritic and axosomatic synapses. c. Axoaxonic synapses are located between axons. d . Dendrodendritic synapses are located between dendrites.
2. Method of signal transmission a . Chemical synapses
( 1 ) These synapses involve the release of a chemical substance (neurotransmitter or neuromodu lator) by the presynaptic cell, which acts on the postsynaptic cell to generate an action potential.
(2) Chemical synapses are the most common neuron-neuron synapse and the only neuron-muscle synapse.
(3) Signal transmission across these synapses is delayed by about 0 .5 ms, the time required for secretion and diffusion of neurotransmitter from the presynaptic membrane of the first cell into the synaptic cleft and then to the postsynaptic membrane of the receiving cell.
(4) Neurotransmitters do not effect the change; they only activate a response in the receiving cell.
Parkinson D isease Pa rki nson d i sease i s a p rog ressive d e gene rative d isease c h a ra cte r ized by
tremo rs, m u s c u l a r ri g i d ity, d iffi c u lty i n i n it iati n g movements, s l ow vo lu nta ry sh uffl i n g movement, a n d maskl i ke fa c i a l express i on . T h e c a use is th e loss o f d opam ine rg i c n e u rons from th e substant ia n i g ra of the b ra i n . Alth o ugh the c ause of the loss of these ce l l s is u n c l e a r, it is kn own that c e rta i n i n d ustri a l toxi ns , s u c h a s those t o whi c h m a n g a nese m i n e rs a re exposed , a n d t h e po i sonous m ethyl - p heny l tetra hyd ropyri d i n e , a s u bsta n c e p resent i n i l l e g a l ly m a n ufactured h e ro i n , c a u se Pa rki nson d i sease . Treatment moda l iti es i n c l ude a dm i n iste r i ng levodopa , wh i ch g ives some re l i ef, a lth ough the ce l l s conti n u e to d i e . Tra nsp l a nti ng feta l a d re n a l g l a n d ti ssue has p rovi d ed o n ly tra ns i ent re l i ef. Adva nces i n stem c e l l rese a r ch may be a p p l i ed some d ay t o c u ri ng t h i s d e a d ly d i sease .
Deep bra in stimu lation i s a te c h n i q u e that does not c u re Pa rki nson d i sea se, b ut c a n ease the symptoms a n d imp rove the pat ie nt's q u a l ity of l i f e . Presently, i t i s used when ro uti n e med i c ations e i th e r fa i l o r p rod u c e severe s i de effe cts.
Hunt ington Chorea H u nt ington c ho rea is a fata l h e re d ita ry d i sease that becomes evi d e nt d u ri n g th e th i rd and fo u rth d e c a des o f l ife, fi rst p resent ing a s pa i nfu l j o i nts a n d prog ress i ng t o u n c o ntro l l e d fl i c ki n g o f j o i nts, m oto r dysfu n cti on , d ement ia , a n d d e ath . The c a use is tho ught to be the loss of n e u rons that prod u c e th e n e u rotransm itte r y-am i nobutyri c a c i d ( GABA) . The sym ptoms of d e m ent ia a re th o ught to b e re l ate d to the loss of the ce l l s sec reti ng a c etyl c ho l i n e .
b. E lectrica l synapses (1 ) These synapses involve movement of ions from one neuron to another via gap
junctions, which transmit the action potential of the presynaptic cell directly to the postsynaptic cell.
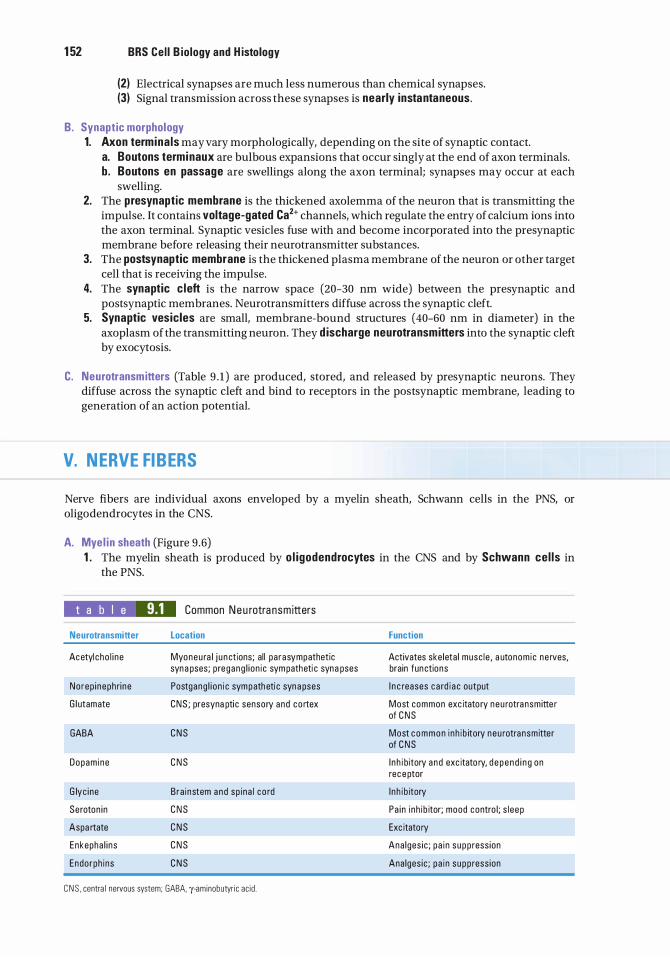
1 52 BRS Cel l B iology and H istology
(2) Electrical synapses are much less numerous than chemical synapses. (3) Signal transmission across these synapses is nearly instantaneous.
B. Synaptic morphology 1. Axon termina ls may vary morphologically, depending on the site of synaptic contact.
a. Boutons terminaux are bulbous expansions that occur singly at the end of axon terminals. b. Boutons en passage are swellings along the axon terminal; synapses may occur at each
swelling. 2. The presynaptic membrane is the thickened axolemma of the neuron that is transmitting the
impulse. It contains voltage-gated Ca2+ channels, which regulate the entry of calcium ions into the axon terminal. Synaptic vesicles fuse with and become incorporated into the presynaptic membrane before releasing their neurotransmitter substances.
3. The postsynaptic membrane is the thickened plasma membrane of the neuron or other target cell that is receiving the impulse.
4. The synaptic c left is the narrow space (20-30 nm wide) between the presynaptic and postsynaptic membranes. Neurotransmitters diffuse across the synaptic cleft.
5. Synaptic vesicles are small, membrane-bound structures (40-60 nm in diameter) in the axoplasm of the transmitting neuron. They d ischarge neurotransmitters into the synaptic cleft by exocytosis.
C. Neurotransmitters (Table 9 . 1 ) are produced, stored, and released by presynaptic neurons. They diffuse across the synaptic cleft and bind to receptors in the postsynaptic membrane, leading to generation of an action potential.
V. NERVE FIBERS
Nerve fibers are individual axons enveloped by a myelin sheath, Schwann cells in the PNS, or oligodendrocytes in the CNS.
A. Mye l in sheath (Figure 9 .6) 1 . The myelin sheath is produced by o l igodendrocytes in the CNS and by Schwann ce l ls in
the PNS.
t a b I e 9.1 Neurotransmitter
Acetyl cho l i ne
Norep i neph ri ne
G l utamate
GABA
Dopam ine
G lyc i ne
Seroton in
Aspa rtate
Enkepha l i ns
Endorph ins
Common Ne u rotra nsm itters
Location
Myoneu ra l j u n ctions; al l pa rasympathetic syna pses; p regang l i on i c sym patheti c syna pses
Postgang l i on i c sympatheti c syna pses
CNS ; presyna pti c sensory and co rtex
C N S
C N S
Bra instem and sp i na l co rd
C N S
C N S
C N S
C N S
C N S . centra l nervous system; GABA. y-aminobutyr ic ac id .
Function
Activates ske leta l musc l e , a utonom ic ne rves, brain fun ctions
I n c reases c a rd i a c output
Most common exc itatory neu rotra nsm itte r of C N S
Most c o m m o n i nh i b itory neu rotra nsm itter of C N S
I n h i bitory a nd exc itato ry, d e p e n d i n g on rec e ptor
I n h i b itory
Pa i n i nh i b itor; mood contro l ; s l eep
Exc itatory
Ana lges ic ; pa i n supp ress ion
Ana lges ic ; pa i n supp ress ion
i!1llll'1ttDll Nervous System 1 53
2. It consists of several spiral layers of the plasma membrane of an oligodendrocyte or Schwann cell wrapping around the axon.
3. It is not continuous along the length of the axon but is interrupted by gaps called nodes of Ranvier.
4. Its thickness is constant along the length of an axon; however, thickness usually increases as the axonal diameter increases.
5. The myelin sheath can be extracted by standard histological techniques. Methods using osmium tetroxide preserve the myelin sheath and stain it black.
6. Under electron microscopy, the myelin sheath displays the following features : a. Major dense l ines represent fusions between the cytoplasmic surfaces o f the plasma
membranes of Schwann cells (or oligodendrocytes) . b. lntraperiod l i nes represent c lose contact, but not fusion, of the extracellular surfaces of
adjacent Schwann cell (or oligodendrocyte) plasma membranes. c. C lefts ( inc isures) of Schmidt-Lanterman (observed in both electron and light microscopy)
are cone-shaped oblique d isconti nu ities of the myelin sheath due to the presence of Schwann cell (or oligodendrocyte) cytoplasm within the myelin.
B. Nodes of Ranvier are regions along the axon that lack mye l in and represent discontinuities between adjacent Schwann cells or adjacent oligodendrocytes. 1 . In the PNS, the axon at the nodes of Ran vier is covered by interdigitated cytoplasmic processes
of adjacent Schwann cells that protect the myelin-free surface of the axon. In the CNS, however, the axon is not covered by cytoplasmic processes of oligodendrocytes. Instead, the myelin-free surface of the axon at the node of Ran vier is covered by a foot plate of an astrocyte.
2. The axolemma at the nodes contains many Na + pumps, and in electron micrographs, it displays a characteristic electron density.
C. I nternodes are the segments of a nerve fiber between adjacent nodes of Ranvier . They vary in length from 0.08 to 1 mm, depending on the size of the Schwann cells or oligodendrocytes associated with the fiber.
Mu ltip le Sclerosis M u lti p l e s c l e ros is ( M S ) is a n immune -med i ated d isease c h a ra cte r ized by
c h ron i c a n d prog ressive dysfu n cti on of th e n e rvous system d u e to d emye l i n atio n of the C N S, espe c i a l ly i n the b ra i n , sp i na l c o rd , a n d o pt ic n e rves . M S affl i cts a b o ut 1 i n 700 i n th is c ou ntry, most common ly i n the 20 - to 40-yea r a ge g ro u p, affe cti ng 2 fema l e s to 1 ma l e . There a re ra ndom ep i sodes o f infl a m m ation , e dema , a n d d emye l i n atio n of axons fo l l owed by p e ri ods of rem iss ion t ha t may l a st fo r months to ye a rs . E a c h ep i sode may red u c e the vita l ity of the pati ent a n d be suffi c i e nt to c a use d e ath with i n months . I t i s b e l ieved that, in the C N S, T lym pho cytes mount an atta c k on mye l i n s heaths, d e mye l i n ate axons, a n d i nterfere with no rm a l p ro p a g ati on o f a ctio n potenti a l s . H oweve r, re c e nt stu d i es h ave suggested tha t the t r ue c a usative fa cto r of M S is o l i g o dend rog l i o pathy a n d the T-c e l l response is me re ly a s e conda ry rea cti on . Present tre atments i n c l u d e immunosupp ress ion with c o rti coste ro ids .
VI. NERVES
Nerves are cordlike bundles of nerve fibers surrounded by connective tissue sheaths (Figure 9.7) . They are visib le to the unaided eye and usually appear wh itish because of the presence of myelin.
A. Connective tissue investments 1 . Epineurium is the layer of dense fibrous connective tissue (fasc ia) that forms the external coat
of nerve bundles and is often embedded in adipose tissue.
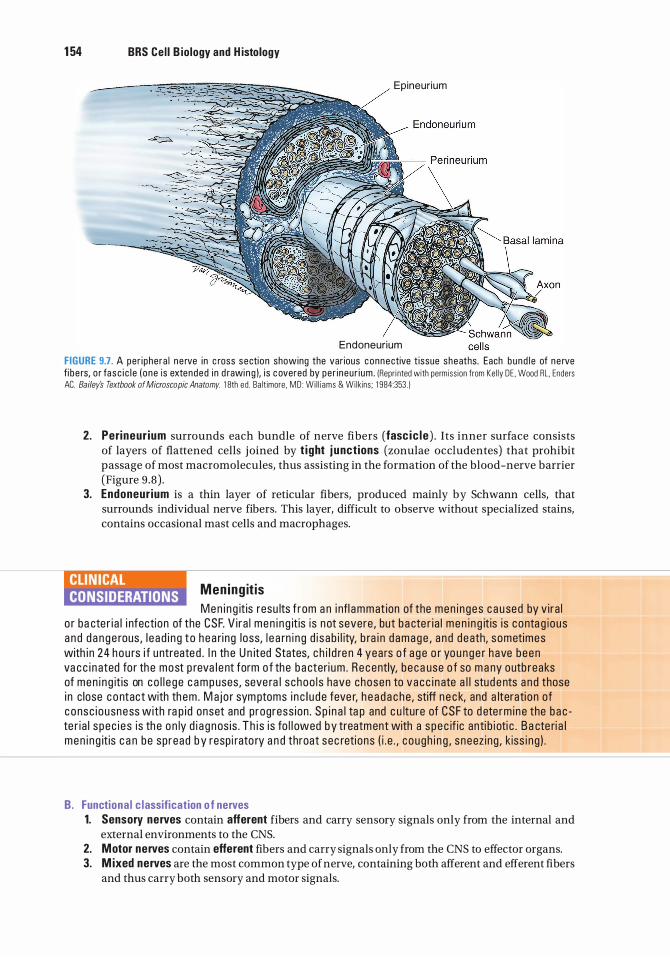
1 54 BRS Cel l B iology and H istology
Epineur ium
Endoneurium
FIGURE 9.7. A per i phe ra l n e rve in c ross section showing the var ious connective t issue sheaths. Each b und l e of ne rve fi b e rs, o r fasc i c l e ( one is extended i n d rawi n g ), i s c overed by pe r i neu r i um . (Repr i nted with permiss ion from Ke l ly DE . Wood RL. Enders AC. Bailey's Textbook of Microscopic Anatomy. 1 8th ed . Ba lt imore. MD : Wi l l i ams & Wi lkins ; 1 984:353 . )
2. Perineur ium surrounds each bundle of nerve fibers (fasc ic le ) . Its inner surface consists of layers of flattened cells joined by t ight j unct ions (zonulae occludentes) that prohibit passage of most macromolecules, thus assisting in the formation of the blood-nerve barrier (Figure 9 .8) .
3. Endoneur ium is a thin layer of reticular fibers, produced mainly by Schwann cells, that surrounds individual nerve fibers. This layer, difficult to observe without specialized stains, contains occasional mast cells and macro phages.
Mening it is Men i n g it is resu lts f rom a n i nfl ammat ion of the men i n ges c a u sed by v i ra l
o r ba cte r i a l i nfecti on of the CSF. V i ra l men i n g it is is not severe , but b a cte r i a l men i n g it is i s conta g ious a n d d a n g e rous , l e a d i n g to h e a ri ng l oss, l e a rn i n g d i s ab i l ity, b ra i n d amage , a n d d eath, sometimes with i n 24 hou rs i f u ntreated . I n th e U n ited States, c h i l d re n 4 yea rs o f a g e o r yo u n g e r h ave been va c c i n ated fo r th e most p reva l e nt form o f the b a cteri um . R e cently, b e ca use o f so m a ny outb reaks of men i n g it is on co l l e ge c a m p uses, seve ra l s choo l s have chosen to vacc i n ate a l l stud e nts a n d those i n c lose c o ntact with th em . M aj o r sym ptoms i n c l u d e feve r, h e a d a c he, stiff n e c k, and a lterati on of c o nsc i ousness with ra p i d onset and p rogress ion . S p i n a l ta p and c u lture of CSF to d ete rm i ne the b a c te r i a l s pec i e s is th e o n ly d i a g nos is . T h i s i s fo l l owed by treatm ent with a s pec if ic anti b i oti c . B a cte ri a l men i n g it is c a n be sp read b y resp i rato ry a n d throat sec reti ons ( i . e . , c o ugh i n g , s neez ing , k iss i ng ) .
B. Functiona l c lassification o f nerves 1. Sensory nerves contain afferent fibers and carry sensory signals only from the internal and
external environments to the CNS. 2. Motor nerves contain efferent fibers and carry signals only from the CNS to effector organs. 3. M ixed nerves are the most common type of nerve, containing both afferent and efferent fibers
and thus carry both sensory and motor signals.
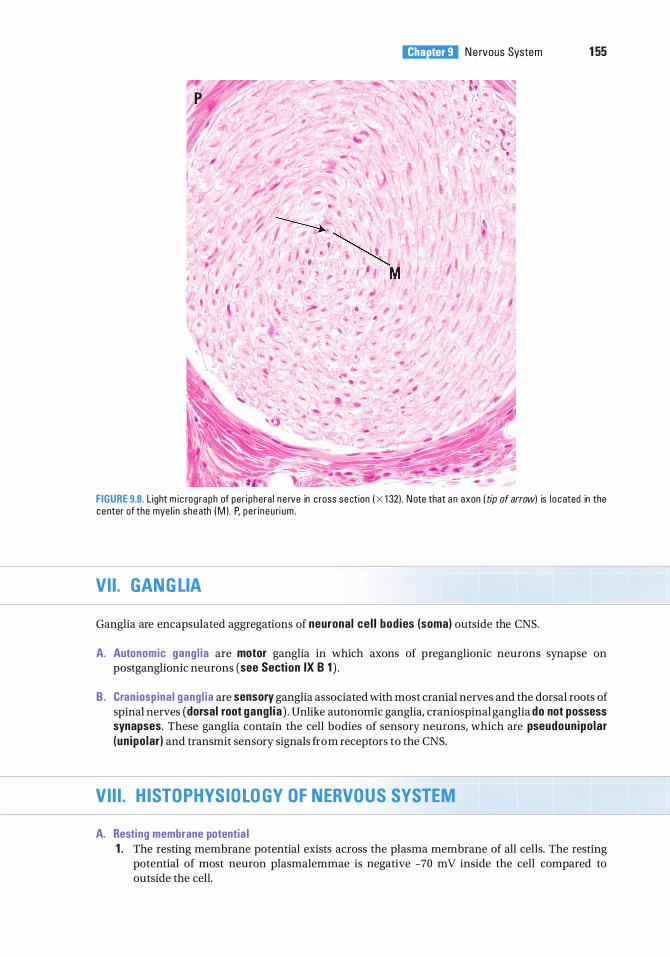
i!1llll'1ttDll N e rvous System 1 55
FIGURE 9.8. L ight m i c rog raph of per i phera l n e rve in c ross sect ion I x 1 32) . N ote that a n axon (tip of arrow) is l o c ated in the center of the mye l i n she ath I M ) . P, pe r i neu ri um .
VII. GANGLIA
Ganglia are encapsulated aggregations of neuronal ce l l bod ies (soma) outside the CNS.
A. Autonomic gang l ia are motor ganglia in which axons of preganglionic neurons synapse on postganglionic neurons (see Section IX B 1 ) .
B. Cran iospinal gang l ia are sensory ganglia associated with most cranial nerves and the dorsal roots of spinal nerves (dorsal root gang l ia ) . Unlike autonomic ganglia, craniospinal ganglia do not possess synapses. These ganglia contain the cell bodies of sensory neurons, which are pseudounipo lar (un ipo lar) and transmit sensory signals from receptors to the CNS.
VIII. HISTOPHYSIOLOGY OF NERVOUS SYSTEM
A. Resting membrane potentia l 1 . The resting membrane potential exists across the plasma membrane of all cells. The resting
potential of most neuron plasmalemmae is negative -70 mV inside the cell compared to outside the cell.
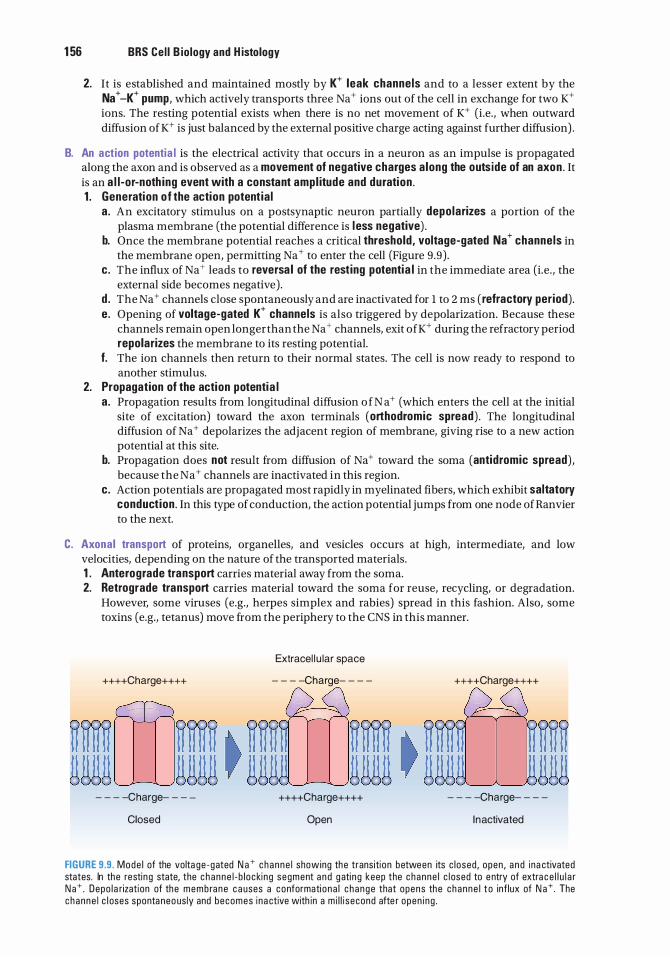
1 56 BRS Cel l B iology and H istology
2. It is established and maintained mostly by K+ leak channels and to a lesser extent by the Na + -K+ pump, which actively transports three Na + ions out of the cell in exchange for two K+ ions. The resting potential exists when there is no net movement of K+ (i.e. , when outward diffusion ofK+ is just balanced by the external positive charge acting against further diffusion) .
B. An action potentia l is the electrical activity that occurs in a neuron as an impulse is propagated along the axon and is observed as a movement of negative charges a long the outs ide of an axon . It is an a l l-or-noth ing event with a constant ampl itude and duration . 1 . Generation of the action potent ia l
a . An excitatory stimulus on a postsynaptic neuron partially depolarizes a portion of the plasma membrane (the potential difference is l ess negative) .
b. Once the membrane potential reaches a critical threshold, voltage-gated Na+ channels in the membrane open, permitting Na+ to enter the cell (Figure 9 .9) .
c. The influx of Na + leads to reversa l of the resting potentia l in the immediate area (i.e . , the external side becomes negative) .
d . The Na + channels close spontaneously and are inactivated for l to 2 ms ( refractory period) . e . Opening of voltage-gated K+ channels is also triggered by depolarization. Because these
channels remain open longer than the Na + channels, exit ofK+ during the refractory period repolarizes the membrane to its resting potential.
f. The ion channels then return to their normal states. The cell is now ready to respond to another stimulus.
2. Propagation of the action potentia l a . Propagation results from longitudinal diffusion o f N a + (which enters the cell at the initial
site of excitation) toward the axon terminals (orthodromic spread) . The longitudinal diffusion of Na + depolarizes the adjacent region of membrane, giving rise to a new action potential at this site.
b. Propagation does not result from diffusion of Na+ toward the soma (antidromic spread) , because the Na+ channels are inactivated in this region.
c. Action potentials are propagated most rapidly in myelinated fibers, which exhibit saltatory conduct ion . In this type of conduction, the action potential jumps from one node ofRanvier to the next.
C. Axonal transport of proteins, organelles, and vesicles occurs at high, intermediate, and low velocities, depending on the nature of the transported materials. 1 . Anterograde transport carries material away from the soma. 2. Retrograde transport carries material toward the soma for reuse, recycling, or degradation.
However, some viruses (e.g., herpes simplex and rabies) spread in this fashion. Also, some toxins (e.g., tetanus) move from the periphery to the CNS in this manner.
++++Charge++++
- - - -Charge- - -
Closed
Extracel l u lar space
- - - -Charge- - - -
++++Charge++++
Open
++++Charge++++
- - - -Charge- - - -
Inactivated
FIGURE 9.9. Mode l of the volta ge -gated N a + c hanne l showing the transiti on between its c l osed , open , a n d i na ctivated states. In the resting state, the c hanne l - b l ocki ng segment a n d g ati n g keep the c hanne l c l osed to e ntry of extra c e l l u l a r N a + . Depo l a rization of the memb ra n e c a uses a conformati ona l c h ange that opens the c h a n n e l t o inf lux of N a + The c hanne l c l oses sponta neo us ly and becomes i na ctive with in a m i l l i second afte r open i ng .
D. Troph ic function of nervous tissue 1. Denervation of a muscle or gland leads to its atrophy.
i!1llll'1ttDll N e rvous System 1 57
2. Reinnervation of a muscle or gland restores its structure and function.
IX. SOMATIC NERVOUS SYSTEM AND AUTONOMIC NERVOUS SYSTEM
Somatic and autonomic are functional concepts relating to all the neural elements involved in the transmission of impulses from the CNS to the somatic and visceral components of the body, respectively. Neural crest cells give rise to neurons of both the parasympathetic and sympathetic divisions of the ANS whose pregang l ion ic ce l l bodies are located in the CNS and postgang l ion ic ce l l bodies are located in autonomic gangl ia located outside the CNS.
A. The somatic nervous system (SNS) contains sensory fibers that bring information to the CNS and the motor fibers that originate in the CNS that innervate voluntary skeletal muscles.
B. The autonomic nervous system (ANS) is generally considered to be purely motor in function as it contains motor fibers that control and regulate smooth muscle, card iac muscle, and some g lands. It establishes and maintains homeostasis of the body's visceral functions. Anatomically and functionally, the ANS is divided into three parts : the sympathetic, parasympathetic, and enteric nervous systems. The sympathetic and parasympathetic nervous systems generally function antagonistica l ly in a given organ (i .e . , when the sympathetic system stimulates an organ, the parasympathetic inhibits it, and vice versa) . The enteric nervous system is confined to the digestive system, where it controls digestive processes; however, it is modulated by the sympathetic and parasympathetic nervous systems. 1. Autonomic nerve chains
a. Cell bodies of pregang l ion ic neurons are located in the CNS and extend their pregang l ion ic f ibers (axons) to an autonomic gangl ion located outside of the CNS.
b. In the ganglion, the preganglionic fibers synapse with postganglionic neurons, which typically are multipolar and are surrounded by satellite cells.
c. Postgang l ion ic f ibers leave the ganglion and terminate in the effector organ (smooth muscle, cardiac muscle, and glands).
2. Sympathetic system (thoracolumbar outflow) a . Preganglionic cell bodies of the sympathetic nervous system are located in the thoracic and
the first two lumbar segments of the spinal cord. b. Function . The sympathetic system effects vasoconstriction . In general, it functions to
prepare the body for flight -or-fight-or-freeze responses by increasing heart rate, respiration, blood pressure, and blood flow to skeletal muscles; dilating pupils; and decreasing visceral function.
3. Parasympathetic system (cran iosacral outflow) a . Preganglionic cell bodies of the parasympathetic nervous system are located in certain
cranial nerve nuclei within the brain and in some sacral segments of the spinal cord. b. Function . The parasympathetic system stimulates secretion (secretomotor function) . In
general, it functions to prepare the body for rest-or-digest functions by decreasing heart rate, respiration, and blood pressure; constricting pupils; and increasing visceral function.
4. Enteric nervous system a. Enter ic nervous system consists of two divisions of neurons located in the wall of the
digestive tract : the myenter ic p l exus of Auerbach and the submucosal p l exus of Me issner .
b . Function . The enteric nervous system is a stand-alone system that is generally responsible for the proper course of digestion, including the control of digestive secretions and blood flow to and from the gut. Although the enteric system is considered to be an independent system, its functions are modulated by the sympathetic and parasympathetic components of the ANS.
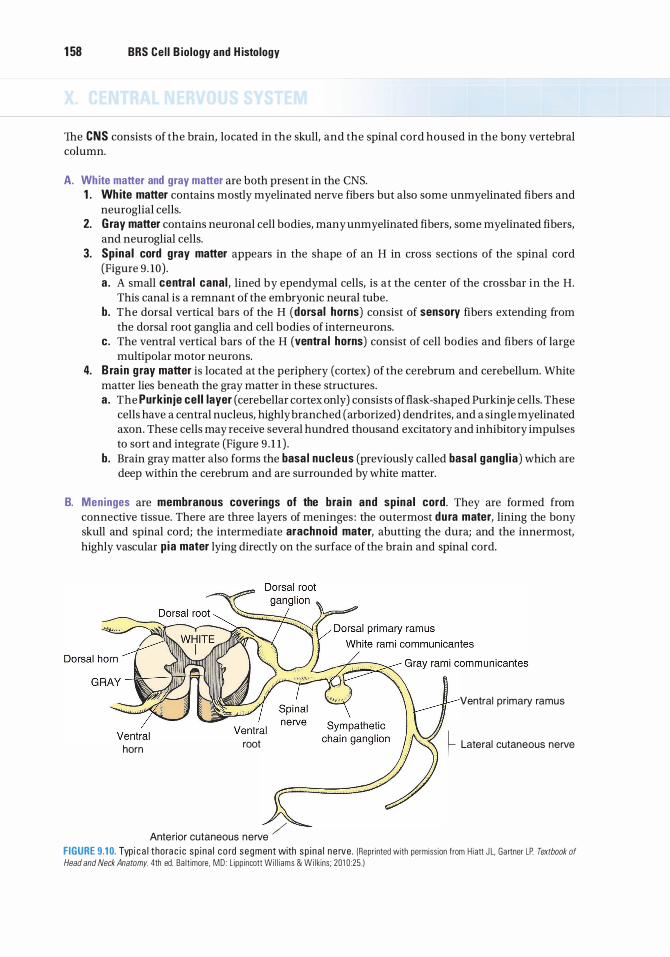
1 58 BRS Cel l B iology and H istology
The CNS consists of the brain, located in the skull, and the spinal cord housed in the bony vertebral column.
A. White matter and gray matter are both present in the CNS. 1 . Wh ite matter contains mostly myelinated nerve fibers but also some unmyelinated fibers and
neuroglial cells. 2. G ray matter contains neuronal cell bodies, many unmyelinated fibers, some myelinated fibers,
and neuroglial cells. 3. Spina l cord gray matter appears in the shape of an H in cross sections of the spinal cord
(Figure 9. 10) . a . A small centra l canal , lined by ependymal cells, is at the center of the crossbar in the H.
This canal is a remnant of the embryonic neural tube. b. The dorsal vertical bars of the H (dorsal horns) consist of sensory fibers extending from
the dorsal root ganglia and cell bodies of interneurons. c. The ventral vertical bars of the H (ventra l horns) consist of cell bodies and fibers of large
multipolar motor neurons. 4. B ra i n g ray matter is located at the periphery (cortex) of the cerebrum and cerebellum. White
matter lies beneath the gray matter in these structures. a . The Purkinje cel l layer (cerebellar cortex only) consists offlask-shaped Purkinje cells. These
cells have a central nucleus, highly branched (arborized) dendrites, and a single myelinated axon. These cells may receive several hundred thousand excitatory and inhibitory impulses to sort and integrate (Figure 9 . 1 1 ) .
b. Brain gray matter also forms the basa l nuc leus (previously called basa l gang l ia) which are deep within the cerebrum and are surrounded by white matter.
B. Meninges are membranous coverings of the bra in and spina l cord. They are formed from connective tissue. There are three layers of meninges : the outermost dura mater, lining the bony skull and spinal cord; the intermediate arachnoid mater, abutting the dura; and the innermost, highly vascular p ia mater lying directly on the surface of the brain and spinal cord.
Ventral pr imary ramus
horn root � Lateral cutaneous nerve
Anterior cutaneous nerve / FIGURE 9.1 0. Typ i c a l thora c i c sp i na l c o rd segment with sp i n a l n e rve . (Repri nted with permiss ion from H iatt J L. Gartner LP Textbook of
Head and Neck Anatomy. 4th ed. Ba lt imore, MD : L ipp incott Wi l l i ams & Wi lkins ; 201 0 :25 . )
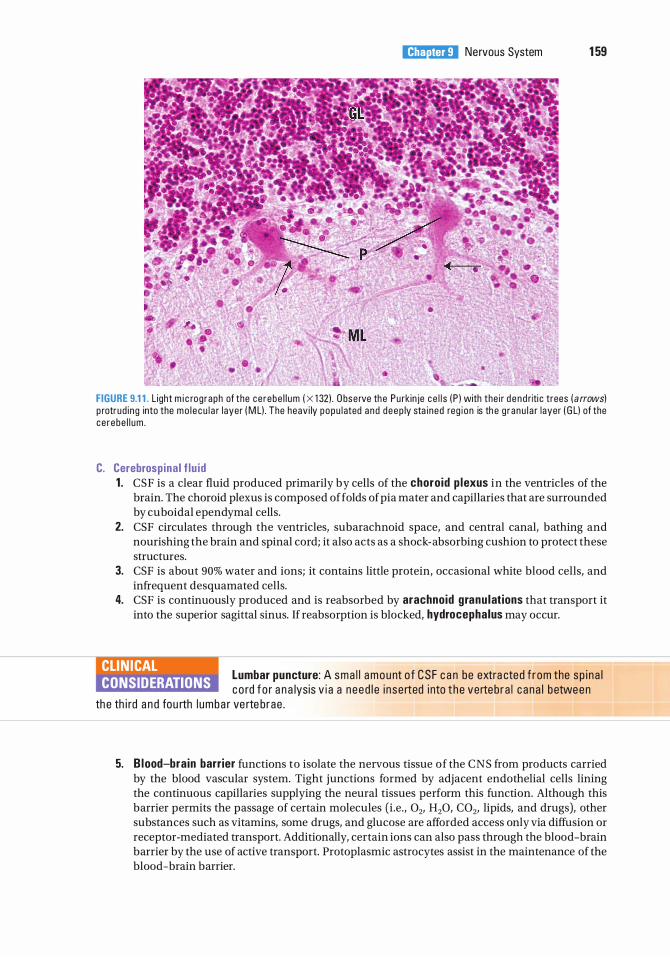
i!1llll'1ttDll Nervous System 1 59
FIGURE 9.1 1 . L ight m i c rog raph of the ce rebe l l um ( X 1 32) . O bse rve the Pu rk in je ce l l s ( P ) with the i r d e n d riti c trees ( a rrows) p rotrud i ng into the mo l e cu l a r l ayer ( M L) . The heav i ly popu l ated and deep ly sta i ned reg i on is th e g r anu l a r layer ( G L) of the ce rebe l l um .
C. Cerebrospina l f lu id 1 . CSF is a clear fluid produced primarily by cells of the choro id p lexus in the ventricles of the
brain. The choroid plexus is composed of folds of pia mater and capillaries that are surrounded by cuboidal ependymal cells.
2. CSF circulates through the ventricles, subarachnoid space, and central canal, bathing and nourishing the brain and spinal cord; it also acts as a shock-absorbing cushion to protect these structures.
3. CSF is about 90% water and ions; it contains little protein, occasional white blood cells, and infrequent desquamated cells.
4. CSF is continuously produced and is reabsorbed by arachnoid granu lations that transport it into the superior sagittal sinus. If reabsorption is blocked, hydrocephalus may occur.
CLIN ICAL CONSIDERATIONS
Lumbar puncture: A sma l l a m o u nt o f CSF c a n be extra cted f r om the s p i n a l c o rd f o r a n a lysis v i a a n eed l e i n se rted i nto t he verteb ra l c ana l b etween
th e th i rd a n d fou rth l umba r ve rte b rae .
5. B lood-brain barrier functions to isolate the nervous tissue of the CNS from products carried by the blood vascular system. Tight junctions formed by adjacent endothelial cells lining the continuous capillaries supplying the neural tissues perform this function. Although this barrier permits the passage of certain molecules (i.e. , 02, H20, C02, lipids, and drugs), other substances such as vitamins, some drugs, and glucose are afforded access only via diffusion or receptor-mediated transport. Additionally, certain ions can also pass through the blood-brain barrier by the use of active transport. Protoplasmic astrocytes assist in the maintenance of the blood-brain barrier.
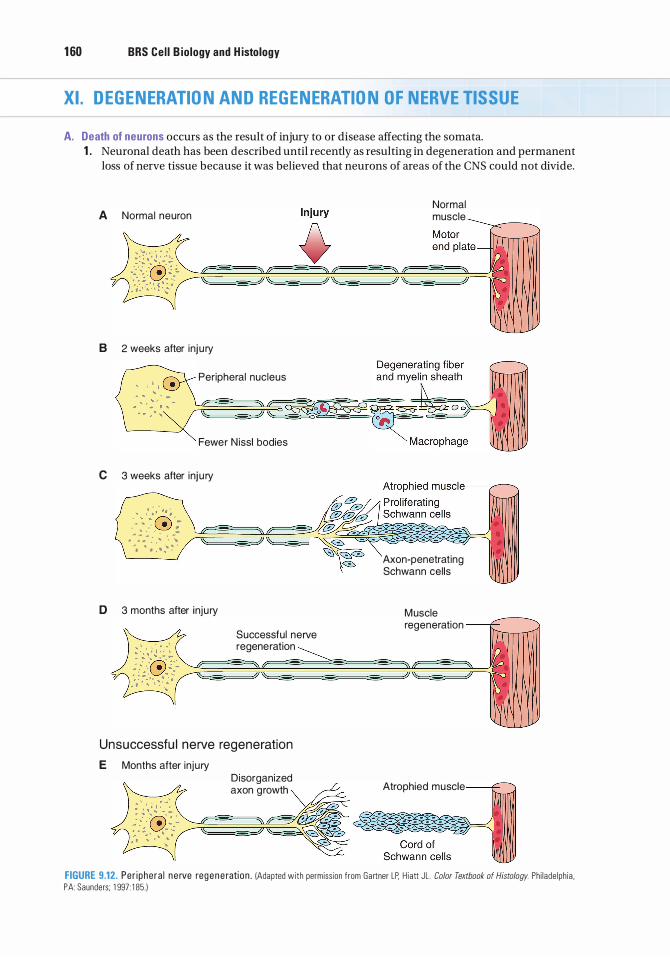
1 60 BRS Cel l B iology and H istology
XI. DEGENERATION AND REGENERATION OF NERVE TISSUE
A. Death of neurons occurs as the result of injury to or disease affecting the somata. 1 . Neuronal death has been described until recently as resulting in degeneration and permanent
loss of nerve tissue because it was believed that neurons of areas of the CNS could not divide.
A Normal neuron
B 2 weeks after inj u ry
Peripheral nucleus
Fewer N issl bodies
C 3 weeks after inj u ry
, · · . .
, "" , ' .:� . - - . . � : .. - : .. : .
. .
. � ·. -: ,. ... -... .. .
. . .. .
D 3 months after inju ry
Successful nerve regeneration
Unsuccessfu l nerve regeneration E Months after inju ry
Disorganized axon growth
Normal muscle
Axon-penetrating Schwann cel ls
Muscle regeneration
Atrophied muscle
FIGURE 9.12. Per i phera l n e rve reg e n e rati on . IAdapted with permiss ion from Gartner LP. H i att JL . Color Textbook of Histology. Ph i lade lph ia . PA : Saunders; 1 997 : 1 85. )
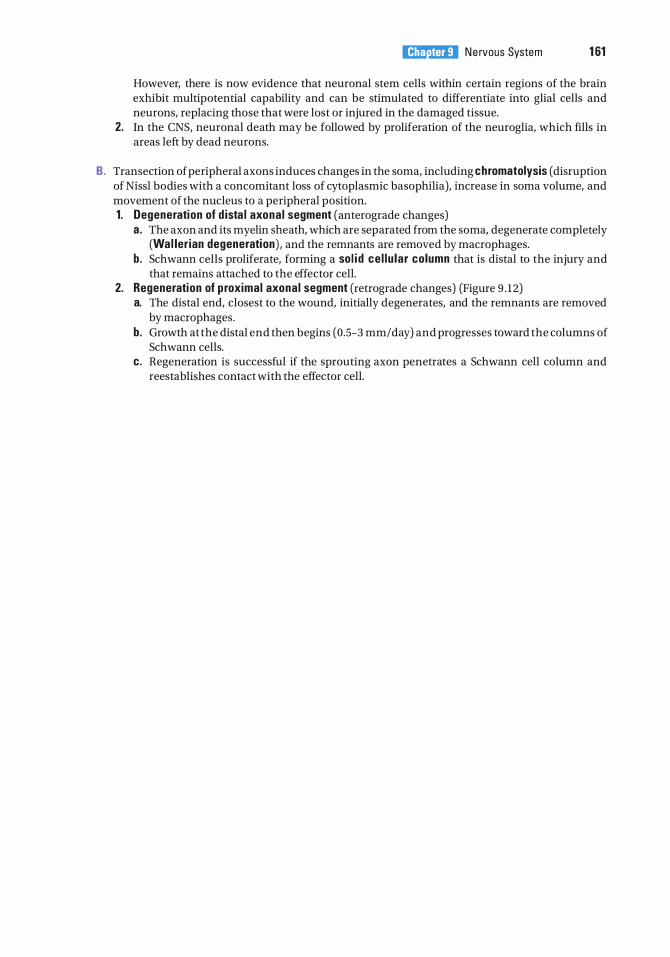
i!1llll'1ttDll N e rvous System 1 61
However, there is now evidence that neuronal stem cells within certain regions of the brain exhibit multipotential capability and can be stimulated to differentiate into glial cells and neurons, replacing those that were lost or injured in the damaged tissue.
2. In the CNS, neuronal death may be followed by proliferation of the neuroglia, which fills in areas left by dead neurons.
B. Transection of peripheral axons induces changes in the soma, including chromatolysis (disruption of Nissl bodies with a concomitant loss of cytoplasmic basophilia), increase in soma volume, and movement of the nucleus to a peripheral position. 1. Degeneration of d ista l axona l segment (anterograde changes)
a. The axon and its myelin sheath, which are separated from the soma, degenerate completely (Wal ler ian degeneration) , and the remnants are removed by macrophages.
b. Schwann cells proliferate, forming a so l i d ce l lu lar column that is distal to the injury and that remains attached to the effector cell.
2. Regeneration of p roximal axona l segment (retrograde changes) (Figure 9 . 12) a. The distal end, closest to the wound, initially degenerates, and the remnants are removed
by macrophages. b. Growth at the distal end then begins (0.5-3 mm/day) and progresses toward the columns of
Schwann cells. c. Regeneration is successful if the sprouting axon penetrates a Schwann cell column and
reestablishes contact with the effector cell.
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Neural crest cells give rise to which of the following?
(A) Dorsal horns of the spinal cord (B ) Adrenal cortex (C ) Sympathetic ganglia (D ) Preganglionic autonomic nerves (E) Somatic motor neurons
2. Which one of the following neurotransmitters functions to increase cardiac output?
(A) Dopamine (B ) Serotonin (C) Norepinephrine (D ) Glutamate (E ) GABA
3. Which of the following statements regarding nerve cell membrane potentials is true?
(A) Membrane potentials are maintained at rest by Na + entering the cell.
(B ) Entrance of K+ causes the membrane to return to its resting potential.
(C) Depolarization triggers the opening of voltage-gated K+ channels.
(D ) Voltage-gated Na + channels become activated during the refractory period.
(E ) The influx of K+ reverses the resting potential.
4. Which of the following statements is characteristic of the perineurium?
(A) It is a fascia surrounding many bundles of nerve fibers.
(B ) It is the fascia surrounding a single nerve fiber.
(C) It is a thin layer of reticular fibers covering individual nerve fibers.
(D ) It is a fascia that excludes macromolecules and forms the external coat of nerves.
(E ) It consists in part of epithelioid cells that surround a bundle (fascicle) of nerve fibers.
1 62
5. Acetylcholine is the only neurotransmitter in which of the following regions of the nervous system?
(A) Central nervous system (B ) Presynaptic sensory cortex (C ) Myoneural junctions (D ) Postganglionic sympathetic synapses (E) Motor cortex
6. Nissl bodies are composed of
(A) synaptic vesicles and acetylcholine. (B) polyribosomes and rough endoplasmic
reticulum. (C ) lipoprotein and melanin. (D ) neurofilaments and microtubules. (E) SER and mitochondria.
7. The axon hillock contains
(A) rough endoplasmic reticulum. (B ) ribosomes. (C) microtubules. (D) Golgi complex. (E) synaptic vesicles.
8. Synaptic vesicles possess which of the following characteristics?
(A) Manufacture neurotransmitter (B ) Enter the synaptic cleft (C ) Become incorporated into the presynaptic
membrane (D ) Become incorporated into the postsynap
tic membrane (E) Release neurotransmitter via endocytosis
9. A patient with Hirschsprung presents with which of the following symptoms?
(A) Absent cranial vault (B ) Exposed spinal cord (C) Headache (D ) Large, dilated colon (E) Absent small intestine
10 . Myelination of peripheral nerves is accomplished by
(A) astrocytes. (B) oligodendrocytes. (C) Schwann cells. (D ) neural crest cells. (E) basket cells.
1 1 . Episodes of demyelination are associated with
(A) meningitis . (B) Huntington chorea. (C) spina bifida. (D ) Parkinson disease. (E ) multiple sclerosis.
1 2. Tremors, shuffling gate, and masklike facial expressions are associated with
(A) meningitis. (B) Huntington chorea. (C) spina bifida. (D ) Parkinson disease. (E) multiple sclerosis.
13. Loss of neurotransmitter GABA is associated with
(A) meningitis. (B) Huntington chorea.
l!1llll'1ttDll N e rvous System 1 63
(C) spina bifida. (D ) Parkinson disease. (E) multiple sclerosis.
1 4. Rapid onset of fever, stiff neck, headache, and an altered state of consciousness are associated with
(A) meningitis. (B) Huntington chorea. (C) spina bifida. (D ) Parkinson disease. (E ) multiple sclerosis.
1 5. Deterioration and death of the dopaminergic neurons within the substantia nigra of the brain are associated with
(A) meningitis . (B ) Huntington chorea. (C) spina bifida. (D ) Parkinson disease. (E ) multiple sclerosis.
Answers and Explanations
1 . C. Neural crest cells migrate throughout the body and give rise to ganglia and other structures, including portions of the adrenal medulla, but they do not contribute to the development of preganglionic autonomic nerves, adrenal cortex, or the dorsal horns of the spinal cord (see Chapter 9 II D).
2. C. Norepinephrine increases cardiac output, whereas dopamine and GABA are CNS inhibitors. Glutamate is the most common excitatory neurotransmitter of the CNS. Serotonin functions as a pain inhibitor in mood control and in sleep (see Chapter 9 IV C) .
3. C. Once the critical threshold is reached, voltage-gated Na + channels open and Na + enters the cell, which depolarizes the cell. Depolarization triggers the opening of voltage-gated K+ channels, and K+ then exits the cell (see Chapter 9 VIII A) .
4. E. Each bundle of nerve fibers is surrounded by the perineurium, which consists primarily of several layers of epithelioid cells. Tight junctions between these cells exclude most macromolecules. The external coat of nerves, the epineurium, surrounds many fascicles but does not exclude macromolecules. The layer of reticular fibers that covers individual nerve fibers is the endoneurium; it also does not exclude macromolecules (see Chapter 9 VI A).
5. C. Acetylcholine is the neurotransmitter for myoneural junctions as well as for preganglionic sympathetic and preganglionic and postganglionic parasympathetic synapses (Table 9 . 1 ) .
6. B . Nissl bodies are large, granular basophilic bodies composed of polysomes and RER. They are found only in neurons (in the soma cytoplasm) (see Chapter 9 III A 3) .
7. C. The axon hillock is devoid of large organelles, such as Nissl bodies and Golgi cisternae, but it does contain microtubules arranged in bundles and permits passage of neurofilaments, mitochondria, and vesicles into the axon (see Chapter 9 III A 3 c) .
8. C. Synaptic vesicles release neurotransmitter into the synaptic cleft by exocytosis. In this process, the vesicle membrane is incorporated into the presynaptic membrane. Although these vesicles contain neurotransmitter, they do not manufacture it (see Chapter 9 IV B 2) .
9. D . Hirschsprung disease is characterized by a dilated colon caused by the absence of the parasympathetic myenteric ganglia known as Auerbach plexus (see Chapter 9 II D Clinical Considerations) .
1 0. C. Schwann cells produce myelin in the PNS, whereas oligodendrocytes produce myelin in the CNS. Astrocytes, neural crest cells, and basket cells do not produce myelin (see Chapter 9 V A B) .
1 1 . E. Mu lt ip le sclerosis is an immune-mediated disease exhibiting chronic and progressive dysfunction of the nervous system due to demyelination of the CNS and optic nerves, striking the 20- to 40-year age group affecting 1 .5 times more women than men. There are random episodes of inflammation, edema, and demyelination of axons followed by periods of remission. Each episode may reduce the vitality of the patient and be sufficient to cause death within months (see Chapter 9 V B Clinical Considerations).
1 2. D . Parkinson d isease is a progressive degenerative disease characterized by tremors, muscular rigidity, difficulty in initiating movements, slow voluntary shuffling movement, and masklike face. The cause is the loss of dopaminergic neurons from the substantia nigra of the brain. Although the cause of the loss of these cells is unclear, it is known that certain poisons and environmental factors cause Parkinson disease (see Chapter 9 IV A Clinical Considerations).
1 3. B . Huntington chorea is a fatal heredity disease that becomes evident during the third and fourth decades of life. It progresses to uncontrolled flicking of joints, motor dysfunction,
1 64

i!1llll'1ttDll Ne rvous System 1 65
dementia, and death. The cause is apparently the loss of neurons that produce the neurotransmitter GABA. Dementia symptoms are thought to be related to the loss of cells secreting acetylcholine (see Chapter 9 IV A Clinical Considerations).
1 4. A. Men ing itis results from an inflammation of the meninges caused by viral or bacterial infection in the CSF. Although viral meningitis is not severe, bacterial meningitis is contagious and dangerous, leading to hearing loss, learning disability, brain damage, and death if untreated, sometimes within 24 hours. Major symptoms include fever, headache, stiff neck, and alteration of consciousness with rapid onset and progression. Spinal tap and culture of CPS to determine the bacterial species is the only diagnosis. Treatment is by species-specific antibiotic. Bacterial meningitis can be spread by respiratory and throat secretions (i .e. , coughing, sneezing, kissing) (see Chapter 9 VI A Clinical Considerations) .
1 5. D . Parkinson d isease i s a progressive degenerative disease characterized by tremors, muscular rigidity, difficulty in initiating movements, slow voluntary shuffling movement, and masklike face. It is caused by the loss of dopaminergic neurons from the substantia nigra of the brain (see Chapter 9 IV A Clinical Considerations) .
Blo o d and Hemopoiesis
I. OVERVIEW-BLOOD
A. Blood is a specialized connective tissue that consists of formed elements (erythrocytes, leukocytes, and p late lets) and a fluid component called plasma.
B. The volume of blood in an average human adult is approximately 5 L.
C. Blood circulates in a closed system of vessels and transports nutrients, waste products, hormones, proteins, ions, oxygen (02), carbon dioxide (C02), and formed elements.
D. It also regu lates body temperature and assists in regulation of osmotic and acid-base ba lance .
E. Blood cells have short life spans and are continuously replaced by a process called hemopoiesis.
A. P lasma consists of 90% water; 9% organ ic compounds (such as proteins, amino acids, and hormones); and 1% inorganic sa lts, dissolved gases, and nutr ients.
1 66
1 . Main p lasma prote ins a . A lbumin, a small protein (60,000 molecular weight), preserves the colloid osmotic
pressure in the vascular system and helps transport some metabolites. Colloid osmotic pressure assists in maintaining proper blood volume by resisting the exit of plasma from the bloodstream. Recall that p lasma that leaves blood vessels to enter the connective tissue spaces is known as extrace l lu lar f lu id (tissue f lu id) .
b . y-G iobu l ins are antibod ies ( immunoglobu l i ns) (see Chapter 1 2) . c . a-G lobu l ins and �-g lobu l ins transport metal ions (e.g., iron and copper) and lipids (in the
form of lipoproteins). d . Clotting proteins, including f ibr inogen, a soluble protein that is converted into fibrin during
blood clotting. e. Complement prote ins (Cl-C9) are part of the innate immune system, and they function in
nonspecific host defense and initiate the inflammatory process. 2. Serum is the yel l owish f lu id that remains after blood has clotted. It is similar to plasma but
lacks fibrinogen and clotting factors.
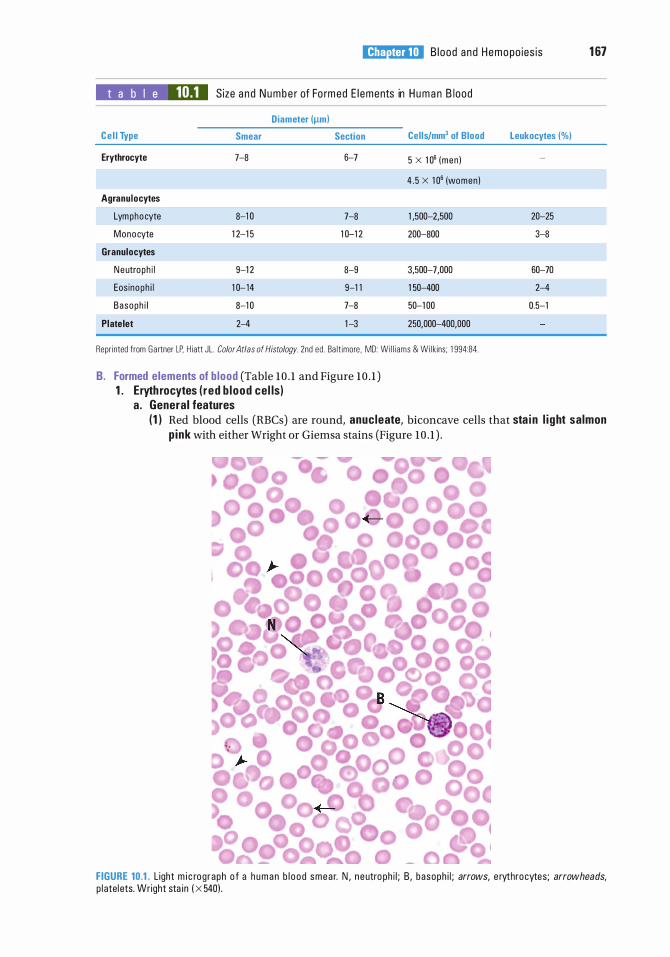
I!1JEtt!Dl!l B lood and Hemopo ies is 1 67
t a b I e 10.1 Size a n d Numbe r of Fo rmed E l ements in H uman B lood
C e l l Type
Erythrocyte
Agranulocytes
Lymphocyte
Monocyte
Granulocytes
Neutroph i l
Eos inoph i l
Basoph i l
Platelet
Diameter (!lml
Smear
7-8
8-1 0
1 2-1 5
9-1 2
1 0-- 14
8-1 0
2-4
Section Cel ls/mm3 of Blood
6-7 5 x 1 06 (men )
4 . 5 x 1 06 (women )
7-8 1 ,500--2,500
1 0--1 2 200-800
8-9 3,500--7,000
9-1 1 1 50-400
7-8 50-1 00
1 -3 250,000-400,000
Repr inted from Ga rtner LP. H iatt JL . Color Atlas of Histology. 2nd ed . Ba lt imore, MD: Wi l l i ams & Wi lk ins; 1 994:84.
B. Formed elements of b lood (Table 10 . 1 and Figure 10 . 1 ) 1 . Eryth rocytes ( red b lood cel ls)
a . General features
Leukocytes (%)
20-25
3-8
60-70
2-4
0.5-1
( 1 ) Red blood cells (RBCs) are round, anucleate, biconcave cells that sta i n l i ght salmon p ink with either Wright or Giemsa stains (Figure 10 . 1 ) .
FIGURE 10.1. Light m i c rog raph o f a h u m a n b l o o d smea r. N , n e utro ph i l ; B , basoph i l ; arrows, e rythrocytes; arrowheads, p l atel ets. Wright sta in ( X 540) .
1 68 BRS Cel l B iology and H istology
(2) The average life span of an RBC is 120 days. Aged RBCs are fragile and express membrane surface oligosaccharides that are recognized by splenic, hepatic, and bone marrow macrophages, which destroy those erythrocytes.
(3) Carbohydrate determinants for the A, B, and 0 blood groups are located on the external surface of the erythrocyte's plasmalemma. A, B, and 0 antigens are short sequences of carbohydrate molecules that are almost identical to each other. All three are attached to the extracellular moiety of transmembrane proteins (g lycophorins), and the only difference is that in types A and B there is an additional terminal sugar molecule attached to the carbohydrate chain of type 0 antigens. The addition of the terminal carbohydrate molecule requires enzymes whose presence is genetically determined. (a ) In type A, the enzyme N-acetylgalactosamine transferase adds a terminal
N-acetylga lactosamine to the type 0 antigen. (b) In type B, the enzyme galactose transferase adds a terminal ga lactose to the type
0 antigen. (c) In type AB, both enzymes are present; therefore, RBCs possess both A and B
antigens on their cell membranes. (d) In type 0, neither enzyme is present; therefore, only type 0 antigens are located on
the RBC cell membrane. Blood type AB is the un iversal acceptor, that is, an individual with AB blood type
can receive a transfusion from individuals whose blood type is A or B or AB or 0. Blood type 0 is the un iversa l donor, so that an individual with blood type 0 can
give blood to individuals whose blood type is A or B or AB or 0. (4) Although there are more than 45 Rh blood type antigens, the most important one is
the D antigen because it is prone to result in the greatest immunogenic response and is the one which is responsible for erythroblastosis feta l is in the newborn ("Rh" is for Rhesus monkey whose blood cells were used in the original work on this antigen) . A particular individual's RBC either expresses (Rh positive, Rh+) or does not express (Rh negative, Rh-) the D antigen (Rh factor). If a mother who is Rh negative carries an Rhpositive fetus, it is quite possible that the fetus' erythrocytes may come in contact with the mother's blood either during the third trimester or during the birth process.
CLIN ICAL CONSIDERATIONS
Erythroblastosis feta l is, as d e s c ri b ed i n th e text, may o c c u r i n p re g n an c i e s whe r e t h e mothe r's b l o o d s up p ly is exposed t o D a nti g en (th e Rh fac
tor) . I f the mothe r i s Rh negative, her immune system wil l p rod u c e l g M a nti bod i es a g a i nst D a nti gen , b ut t hese a nti bod i es a re too l a r ge to g o thro u gh the p l a c e nta l b a rr i e r. D u ri ng a s ubsequent p reg n a n cy with a n oth e r Rh -pos itive fetus, th e moth e r wi l l a g a i n p ro d u c e a nti bod ies , b ut th i s tim e l gG a ntibod i es and these a re sma l l e nough to pen etrate the p l a c enta l b a rr i e r a n d mount an immune response a g a i nst the fetus . Th is c ond itio n i s kn own as e ryth ro b l a stosis feta l is and may be l eth a l to the fetus . I n o r de r to p rote ct futu re fetuses , the Rh - negative moth e r who has a n Rh -pos itive ch i l d i s g iven a nt i -D g l o b u l i n (RhoGAM) afte r th e b a by is bo rn . The a nti - D g l o b u l i n atta ches to the a nti g e n i c s i tes of the D a nti g en so that the moth e r's immune system does not recogn ize it a n d does not p rod u c e a nti bod i es a g a i nst the D a nti g e ns, p rote cti n g futu re Rh -pos itive fetuses f rom the moth e r's immune system .
(5) Several cytoskeleta l prote ins (ankyrin, band 4 . 1 and band 3 proteins, spectrin, and actin) maintain the shape of RBCs (see Chapter 1, Plasma Membrane, Section V A) .
(6 ) Mature erythrocytes possess no organelles but are filled with hemog lob in (Hb ) . ( 7 ) Erythrocytes also contain solub le enzymes that are responsible for glycolysis, the hexose
monophosphate pathway, and the production of adenosine triphosphate (ATP). b. The hematocrit is an estimation of the volume of packed erythrocytes per un it vo lume of
blood. (1 ) The hematocrit is expressed as a percentage. (2) Normal values are 40% to 50% in adult men, 35% to 45% in adult women, 35% in children
up to 10 years of age, and 45% to 60% in newborns.
I!1JEtt!Dl!l B lood and Hemopo ies is 1 69
c. Hb is a protein composed of four polypeptide chains, each covalently linked to a heme group. The four chains that normally occur in humans are a, �. y, and 8. Each chain differs in its amino acid sequence. (1 ) Hb occurs in several normal forms that differ in their chain composition .
(a ) The predominant form of adult Hb is HbA1 ( Uz�2) . (b ) A minor form is HbA2 (azo2) . (c ) Fetal Hb is designated HbF ( <X.zY2) .
d . Transport of C02 and 02 to and from the tissues of the body i s carried out by erythrocytes and plasma. (1 ) Every minute approximately 200 mL of C02 is formed by cells of the body. Since the
partial pressure of C02 is higher in the tissue than in the capillaries, the C02 enters the capillaries via simple diffusion. (a) Twenty milliliters of the C02 is transported in the plasma, 40 mL binds to the
globin moiety ofHb (forming carbaminohemoglob in ) , and 140 mL enters the RBC cytosol.
(b ) Within the cytosol, the enzyme carbonic anhydrase forms H2C03 by combining C02 with H20. H2C03 dissociates and the HC03- leaves the RBC to enter the plasma, and cr from the plasma enters the erythrocyte cytosol to maintain electrical equilibrium. This exchange of ions between the RBC cytosol and the plasma is referred to as the ch lor ide sh ift.
(c) Meanwhile, since the partial pressure of 02 is greater in the RBC than in the tissue, the 02 is released from the Hb, forming deoxyhemoglobin , and the place of 02 is taken up by the binding of 2,3-d iphosphog lycerate .
(2) The partial pressure of 02 is greater in the alveolar airspace than in the alveoli of the lung than in the capillaries; therefore, 02 enters the capillaries via simple diffusion. (a) 02 enters the erythrocyte cytosol and binds to the heme moiety of the Hb molecule
to form oxyhemog lob in . (b ) Bicarbonate ions of the plasma reenter the RBC cytosol, and in exchange c r ions
leave the RBC to enter the plasma (a reversal of the chloride shift) . The bicarbonate ion is combined with H+ ions to form H2C03, which is cleaved by carbonic anhydrase to form C02 and H20. The C02 enters the plasma, and from there the alveolar airspace via simple diffusion to be exhaled.
(3) Because carbon monoxide binds avidly to Hb, it can block binding of 02 and cause carbon monoxide asphyxiation if it is inhaled in sufficient amounts.
(4) Nitric oxide is a neurotransmitter substance that binds to Hb; in areas that are poor in 02, it facilitates dilation of blood vessels and a more efficacious exchange of 02 for C02.
CLIN ICAL CONSIDERATIONS
1 . S i ck le ce l l anemia i s c a used by a po i nt m utatio n i n th e d eoxyri bonu c l e i c a c i d ( D NA) e ncod i n g th e H b mo l e c u l e , l e a d i n g t o th e p ro d u cti o n
o f a n abnormal Hb ( H bS ) . I n t he �- c h a i n o f H bS, th e am i no a c i d val i ne i s s ubstituted fo r g lutamate. a . Although th is d isease o c c u rs a l most exc l us ive ly among peop l e of Afr i c a n desc ent (1 i n
5 00 is affected i n the U n ited States) , among t he U S H is pan i c popu l ation , 1 i n 1 ,000 t o 1 ,400 peop l e i s affected with s i c kl e c e l l a n em i a .
b . C rysta l l izati on o f H b u n d e r l ow 02 te ns ion g ives R B Cs t h e c h a ra cte r isti c s i c kl e s h ape . Sickle RBCs a re fra g i l e and have a h igher rate of destruction th a n no rma l c e l l s .
c. S i gns i n c l u d e hypoxi a , i n c reased b i l i r ub in l eve ls , low RBC count, and c a p i l l a ry stas is . 2. Pernic ious anemia i s c a used by a severe defic iency of vitamin 8 1 2, resu lti n g from impa i re d
p ro d u ctio n o f gastric i ntri nsic factor by t he pa ri eta l c e l l s o f th e sto m a c h . Th i s fa cto r i s req u i red for the p ro pe r abso rpti o n of vita m i n 8 1 2.
3. N ewborns a re fre q u ently d efi c i e nt in vitamin K, a n essenti a l c ofactor fo r th e c l otti n g p roc ess, and if they d o not re c e ive exog enous a dm i n istrati o n of th is vita m in , they may die of h emo rrh a g i c d i sease of the newborn . Ad u lts who a re u n a b l e to a bsorb l i p i d s may a lso suffe r from excess ive b l eed i ng , but th e s u pp l ementa l i n jectio n of vita m i n K imp roves th is c ond itio n .
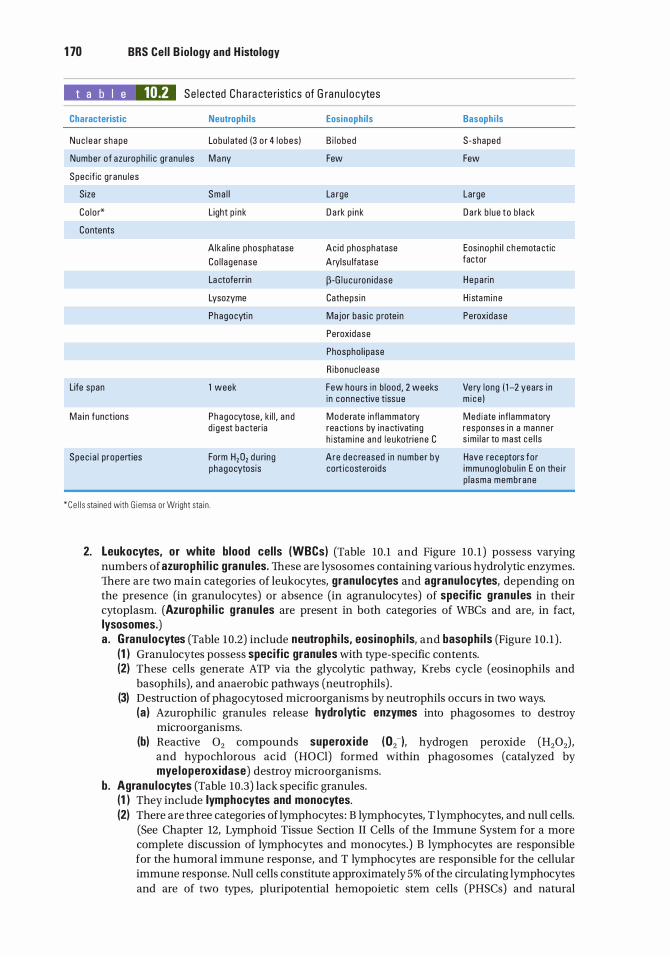
1 70 BRS Cel l B iology and H istology
t a b I e 10.2 Se l e cted Cha ra cte r isti cs of G ra nu l o cytes
Characteristic Neutrophi ls Eosinophi ls Basoph i ls
Nuc l e a r shape Lobu l ated (3 o r 4 l obes ) B i l o bed S-shaped
Number of azu roph i l i c g ranu les M a ny Few Few
Spec if ic g ranu l es
Size Sma l l La rge Large
Co lo r* L ight p i nk D a rk p i nk D a rk b l ue to b l ack
Contents
A lka l i ne phosphatase Ac id phosphatase Eosinoph i l c h emota ctic
Co l l agenase Arylsu lfatase factor
La ctoferr in �-G l u c u ron i dase Hepa ri n
Lysozyme Catheps in H i stam i ne
Phagocytin Major bas ic p rote i n Peroxidase
Peroxi dase
Phospho l i pase
R ibonuc lease
Life span 1 week Few hou rs i n b lood , 2 weeks Ve ry l ong ( 1 -2 years i n i n connective tissue m i ce )
Ma i n funct ions Phagocytose, k i l l , a n d Mode rate infl ammatory Med i ate infl ammatory d i gest ba cter ia rea ctions by i na ctivati ng responses i n a manne r
h i stam i ne a nd l e u kotri e ne C s im i l a r to mast ce l l s
Spec i a l p ropert ies Form H2D2 d u ri ng Are d e c reased i n number by Have receptors fo r phagocytosis corticostero ids immunog l obu l i n E on the i r
p l asma membrane
*Ce l l s sta ined with G i emsa or Wright sta i n .
2. Leukocytes, or wh ite blood cel ls (WBCs) (Table 10.1 and Figure 10 . 1 ) possess varying numbers of azuroph i l i c granu les. These are lysosomes containing various hydrolytic enzymes. There are two main categories of leukocytes, granulocytes and agranulocytes, depending on the presence (in granulocytes) or absence (in agranulocytes) of specific granu les in their cytoplasm. (Azuroph i l ic g ranu les are present in both categories of WBCs and are, in fact, lysosomes.) a . G ranu locytes (Table 10.2) include neutroph i ls, eosinoph i ls, and basoph i ls (Figure 10 . 1 ) .
(1 ) Granulocytes possess specific granules with type-specific contents. (2) These cells generate ATP via the glycolytic pathway, Krebs cycle (eosinophils and
basophils), and anaerobic pathways (neutrophils) . (3) Destruction of phagocytosed microorganisms by neutrophils occurs in two ways.
(a ) Azurophilic granules release hydro lyt ic enzymes into phagosomes to destroy microorganisms.
(b) Reactive 02 compounds superoxide ( 02-), hydrogen peroxide (H202), and hypochlorous acid (HOCl) formed within phagosomes (catalyzed by mye loperoxidase) destroy microorganisms.
b. Agranu locytes (Table 10.3) lack specific granules. (1 ) They include lymphocytes and monocytes. (2) There are three categories of lymphocytes : B lymphocytes, T lymphocytes, and null cells.
(See Chapter 12, Lymphoid Tissue Section II Cells of the Immune System for a more complete discussion of lymphocytes and monocytes.) B lymphocytes are responsible for the humoral immune response, and T lymphocytes are responsible for the cellular immune response. Null cells constitute approximately 5% of the circulating lymphocytes and are of two types, pluripotential hemopoietic stem cells (PHSCs) and natural
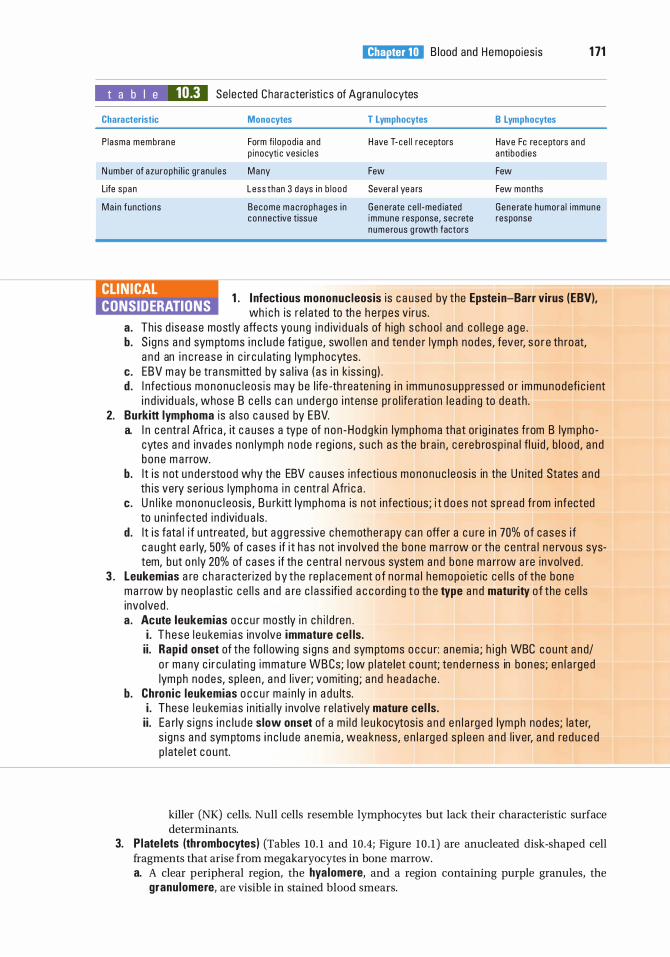
I!1JEtt!Dl!l B lood and Hemopo ies is 1 71
t a b I e 10.3 Se lected Cha ra cteristi cs of Agranu l ocytes
Characteristic Monocytes T Lymphocytes
P lasma membra ne Form fi l opod ia a nd H ave T- ce l l r eceptors p inocyti c ves i c l es
N umber of azu roph i l i c g ranu l es M a ny Few
Life span Less than 3 days i n b l ood Severa l yea rs
Ma i n functions Become m a c rophages i n Generate ce l l -med iated connective tissue immune response, sec rete
n ume rous g rowth factors
B Lymphocytes
Have Fe re ceptors a nd a nti bod ies
Few
Few months
Gene rate humora l immune response
CLINICAL CONSIDERATIONS
1 . I nfectious mononucleosis i s c a used by the Epste in-Barr virus (EBV), wh i c h is re l ated to th e h e rpes v i rus .
a. Th is d i sease mostly affe cts yo ung i n d ivi d u a ls of h igh s choo l and co l l e g e a g e . b. S i gns a n d sym ptoms i n c l u d e fati g u e, swo l l e n a n d ten d e r lym ph nod es, fever, s o r e th roat,
a n d an i n c rease in c i r c u l ati n g lym phocytes . c. EBV m ay be tra nsm itted by s a l iva ( a s i n k iss i ng ) . d . I nfecti ous mononuc l eos is may be l ife -th reaten i n g i n i m m unosupp ressed o r immunodefi c i e nt
i n d iv id u a ls , whose B ce l l s c a n u n d e rgo i ntense p ro l ife rati on l e a d i n g to d e ath . 2. Burkitt lymphoma i s a l so c a used by EBV.
a. I n c entra l Afri c a , it c a uses a type of n on -Hodgkin lym phoma that or ig i n ates from B lym pho cytes a n d invades non lym ph node reg ions, s u ch a s the b ra i n , c e re b rosp i na l fl u i d , b l ood , a n d bone m a rrow.
b. I t i s not u n de rstood why the EBV c a uses i nfecti o us mononuc l eos is in the U n ited States a n d th is very ser i ous lymphoma i n c e ntra l Afri c a .
c. U n l i ke monon u c l eos is , B u rkitt lymphoma is not i nfectious ; i t d o e s not sp read from i nfected to u n i nfe cted i n d ivid u a ls .
d. I t i s fata l i f u ntreated , b ut a g g ressive c h emothe r apy c a n offer a c u re i n 70% of cases i f c a u g ht ea rly, 50% of cases if i t h as not invo lved the bone m a rrow o r the c e ntra l n e rvous system, b ut o n ly 20% of cases if th e c e ntra l n e rvous system a nd bone m a rrow a re invo lved .
3 . Leukemias a re c h a ra cter ized by the re p l a c e me nt o f no rma l h emopo i et ic c e l l s of the bone ma rrow by neop l a st ic ce l l s a n d a re c l a ss ifi e d a c co rd i n g t o th e type and maturity o f the ce l l s invo lve d . a . Acute leukemias o c c u r mostly i n c h i l d re n .
i . These l e u kem i as invo lve immature ce l ls. i i . Rap id onset of the fo l l owing s i gns a n d symptoms o c c u r: a nem i a ; h i g h WBC count a n d/
o r m a ny c i r c u l ati n g immature WB Cs; l ow p l ate let c ou nt; ten d e rness in bon es; e n l a rged lym ph nodes, sp l een , a n d l iver; vom iti n g ; a n d h e a d a c h e .
b. Chron ic leukemias o c c u r ma i n ly i n a d u lts. i . These l e u kem i a s i n iti a l ly i nvolve re l at ively mature cel ls. i i . Ea rly s i gns i n c l u d e slow onset of a m i l d l e u kocytos is a n d e n l a rg e d lym ph nod es; later,
s i g ns a n d sym ptoms i n c l u d e a n e m ia , wea kness, e n l a rg e d sp l e en a n d l iver, a n d red u c e d p l ate l et c o u nt.
killer (NK) cells. Null cells resemble lymphocytes but lack their characteristic surface determinants.
3. P late lets (thrombocytes) (Tables 10 . 1 and 10 .4; Figure 10 . 1 ) are anucleated disk-shaped cell fragments that arise from megakaryocytes in bone marrow. a. A clear peripheral region, the hya lomere, and a region containing purple granules, the
granulomere, are visible in stained blood smears.
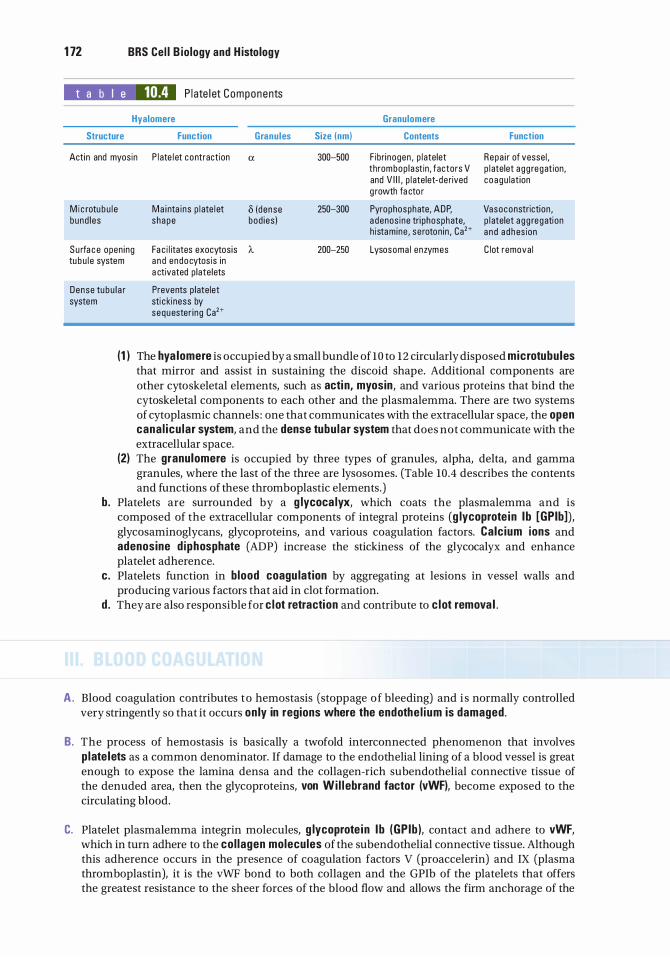
1 72 BRS Cel l B iology and H istology
t a b I e 10.4 P l ate l et Components
Hyalomere Granulomere
Structure Function Granules Size (nm) Contents Function
Actin and myosin P l ate l et contraction a 300--500 F ibri nogen , p l atelet Repa i r of vesse l , thrombop lastin, factors V p l atelet a gg regation, and V I I I , p l atelet-derived coagu lat ion g rowth fa cto r
M i c rotubu l e Ma i nta ins p l ate l et i5 (dense 250--300 Pyrophosphate, ADP, Vasoconstriction , bund l es shape bod ies ) a denos ine tri phosphate, p l atelet a g g regation
h istam ine , se roton in , Ca2+ a nd a dhes ion
Su rfa c e open ing Fa c i l itates exocytos is A. 200-250 Lysosoma l enzymes C lot remova l tu bu l e system and endocytos is in
a ctivated p late lets
Dense tu bu l a r Prevents p late let system sti c kiness by
sequester ing Ca2+
(1 ) The hya lomere is occupied by a small bundle of lO to 12 circularly disposed microtubu les that mirror and assist in sustaining the discoid shape. Additional components are other cytoskeletal elements, such as acti n, myosin, and various proteins that bind the cytoskeletal components to each other and the plasmalemma. There are two systems of cytoplasmic channels : one that communicates with the extracellular space, the open cana l icu lar system, and the dense tubu lar system that does not communicate with the extracellular space.
(2) The granulomere is occupied by three types of granules, alpha, delta, and gamma granules, where the last of the three are lysosomes. (Table 10.4 describes the contents and functions of these thromboplastic elements.)
b. Platelets are surrounded by a g lycoca lyx, which coats the plasmalemma and is composed of the extracellular components of integral proteins (g lycoprote in l b [GPib]), glycosaminoglycans, glycoproteins, and various coagulation factors. Calc ium ions and adenosine d iphosphate (ADP) increase the stickiness of the glycocalyx and enhance platelet adherence.
c. Platelets function in blood coagu lation by aggregating at lesions in vessel walls and producing various factors that aid in clot formation.
d . They are also responsible for c lot retraction and contribute to c lot remova l .
A . Blood coagulation contributes to hemostasis (stoppage of bleeding) and i s normally controlled very stringently so that it occurs on ly in regions where the endothe l ium is damaged.
B. The process of hemostasis is basically a twofold interconnected phenomenon that involves p late lets as a common denominator. If damage to the endothelial lining of a blood vessel is great enough to expose the lamina densa and the collagen-rich subendothelial connective tissue of the denuded area, then the glycoproteins, von Wi l l ebrand factor (vWF), become exposed to the circulating blood.
C. Platelet plasmalemma integrin molecules, g lycoprote in l b (GP ib ), contact and adhere to vWF, which in turn adhere to the col lagen molecules of the subendothelial connective tissue. Although this adherence occurs in the presence of coagulation factors V (proaccelerin) and IX (plasma thromboplastin), it is the vWF bond to both collagen and the GPib of the platelets that offers the greatest resistance to the sheer forces of the blood flow and allows the firm anchorage of the
I!1JEtt!Dl!l B lood and Hemopo ies is 1 73
platelets to the denuded area. The contact between the GPib and the vWF initiates the p late let reaction, and platelets that adhere to the vWF are said to be activated .
D. Activated p latelets become flattened (to cover a greater surface area of the denuded region) and degranulate, releasing ADP and calc ium ions, and in the platelet membrane the enzyme thromboxane-A synthase converts membrane arachidonic acid to synthesize thromboxane A2, an avid vasoconstrictor and platelet activator. Moreover, regions of the platelet plasma membrane become modified to display phospho l ip id complexes that facilitate the progression of the coagulation cascade. ADP and thromboxane A2 attract additional platelets to the injury site and cause the platelets to be present, resulting in the aggregation of the platelets. The platelets are held together by unmasking another set of their integrin molecules, g lycoprote in l i b/l i la (GP I Ib/l l la ), that bind to fibrinogen, which then binds platelets to each other. As the platelet numbers adhering to each other increase in number and size, they block the injury site by the formation of a primary hemostatic p lug .
E. The primary hemostatic plug i s not a very strong barrier and i s reinforced by the process of platelet contraction, which is initiated by its contact with fibrinogen, a protein present in circulating blood, and the primary hemostatic plug becomes a very dense, firm, and well-anchored secondary hemostatic p lug . Since this process of contraction is completed in about 15 to 20 minutes after its initiation, this time lag provides ample opportunity for the coagulation cascade to reinforce the clot and anchor it in place, preventing further blood loss.
F. Once the secondary hemostatic plug is large enough to stop blood loss, it must not increase in size. This is controlled by the release of NO and prostacycl i ns by the endothelial cells, two substances that inhibit platelet aggregation. Additionally, the anticoagu lant pathways inhibit the coagulation cascade. One anticoagulant pathway involves Prote in C complex (a combination of thrombomodulin and thrombin) and Prote in S, which inhibit factors Va and VIlla. Another pathway involves antithrombin III, which not only inactivates thrombin but also acts as an enzyme, degrading factors IXa, Xa, XIa, and Xlla. A third pathway, tissue factor pathway inh ib itor, secreted mostly by endothelial cells, binds to factor Xa and to tissue factor-VIIa complex, inactivating them and thereby inhibiting the coagulation cascade.
G . Phospho l i p i d complexes of activated p late let membranes and Ca2+ ions (also known as factor IV) are also required for blood coagulation.
H. Blood coagulation occurs via two interrelated pathways, the extrinsic and i ntri nsic pathways. The final steps in both pathways, referred to as the common pathway, involve the transformation of prothrombin to thrombin , an enzyme that catalyzes the conversion of fibrinogen (factor I) to f ibr in monomers, which, under the influence of Ca2+ ions and factor XI I I a, coalesce to form a reticu lum of c lot. 1. The extri nsic pathway occurs in response to damaged blood vessels where the insult involves
not only the endothelium but also the wall of the vessel. It is initiated within seconds (rap id onset) after trauma that releases tissue thromboplasti n (factor III).
2. The i ntri nsic pathway is initiated within several minutes (slow onset) after trauma to the endothe l i a l ce l ls, per se, of the blood vessels or when platelets or factor XII are exposed to collagen in the vessel wall. This pathway depends on von Wil lebrand factor and factor VI I I .
3 . The common pathway involves the conversion o f prothrombin to thrombin and that of fibrinogen to fibrin and, finally, the cross-linking of f ibr in monomers to form the f ibr in reticu lum, which is deposited within and around the contracted platelet plug.
I . Once the blood vessel is repaired, the clot is no longer necessary and has to be removed. This process is initiated by tissue plasminogen activator (tPA) and by urokinase-type plasminogen activator (u-PA), enzymes localized on the luminal cell membranes of endothelial cells and in blood plasma. Both enzymes activate p lasminogen, an enzyme precursor synthesized by liver cells and released into the bloodstream, by converting it to the active enzyme plasmin . It is plasmin that in concert with macro phages dissolves the secondary hemostatic plug.
1 74 BRS Cel l B iology and H istology
CLIN ICAL CONSIDERATIONS
Coagu lation disorders fre q uently resu lt f r om i n h e rited o r a c q u i re d d efe cts of c o a g u l ati o n factors.
1 . Factor VII I defic iency (hemoph i l i a A) i s an X- l i nked d iso rd e r that affe cts mostly men . a. Seve rity va r ies with th e extent o f red u ctio n i n t h e leve l o f fa cto r VI I I ( p rod u ced by
h e pato cytes ) . b. H emoph i l i a A resu lts i n excess ive b l eed i ng ( i nto j o i nts, i n severe c ases ) . c. Affected i n d ivi d u a l s h ave a norma l p l ate l et c ou nt, norma l b l e ed i n g time , and no pete c h i a e,
but th rombop l a stin time is i n c reased . 2. von Wi l l ebrand d isease i s a n a utosom a l d om i n ant g e net ic d efe ct, resu lti n g i n a decrease i n the
amount of von Wi l lebrand factor, wh i c h is req u i re d i n the i ntri ns i c p athway of c o a g u l atio n . a. M ost cases a re m i l d a n d d o not invo lve b l e ed i n g into the j o i nts. b. Seve re cases a re c h a ra cter ized by excessive a n d/o r sponta n eous b l e ed i n g from mucous
mem branes a n d wounds . 3. Bernard-Soul ier syndrome i s a n u n c ommon , a utosoma l d i sease that i s d i sti n g u is hed by very
l a rg e p late l ets ( a s l a rg e as 1 11m in d i a m eter ) that d o not possess e nough G P i b i nte g ri n mo l e c u l es i n th e i r p l a sma m e m brane . B e c a use of th is d efe ct, the p late l ets c a n not fo rm bonds with von Wi l l e b rand factor a nd , the refo re, c a n not form a p ri m a ry hemostati c p l u g , res u lti n g in exc e pti o n a l ly severe b l e ed i n g .
4 . G lanzmann's thrombasthenia i s a lso a n u n common b l e ed i n g d iso rd e r, a n a utosom a l rec ess ive tra it, where the p late l ets of affe cted i n d ivi d u a ls possess d efe ctive g lycoprote in l i b/l i la (Gp l l b/ l i l a ) . S i n c e th is p l ate l et p l a sma l emma i nte g ri n mo l e c u l e is respons i b l e fo r b i n d i n g to fi b ri n ogen a n d th ereby ensu ri ng that p l ate l ets o f a p r ima ry hemostati c p l u g a d h e re t o e a c h othe r, a d efect i n the inte g ri n mo l e c u l e p revents the fo rmat ion of a primary hemostatic plug. S i n c e h em ostas is is n ot contro l l e d p rope rly, severe b l eed i ng m ay o c c u r with consequent d e ath of th e affe cted i n d iv id u a l .
A . Ye l low marrow i s located in the long bones o f adults and i s highly infiltrated with fat. I t i s not hemopoietic, but it has the potential to become so if necessary.
B. In adults, red ma rrow is located in the epiphyses of long bones and in flat, irregular, and short bones (Figure 1 0 .2) . It is highly vascular and composed of a stroma, irregular s inuso ids, and islands of hemopo iet ic ce l ls . Red marrow is the site of blood cell d iffe rentiati on and maturati o n . The largest cells of bone marrow are the megakaryocytes (Figure 10 .2) , precursors of platelets. 1. S inusoids are large venous vessels with highly attenuated (very thin) endothelia. They are
associated on their extravascular surfaces with reticular fibers and adventitia l reticu lar cel ls, which manufacture these fibers.
2. Stromal ce l ls include macrophages, adventitial reticular cells, fibroblasts, and endothelial cells. These cells produce and release various hemopoietic g rowth factors (see Table 10 .7) . a . Macrophages are located in extravascular areas near sinusoids and extend processes
between endothelial cells into sinusoidal lumina. These cells phagocytose cast off cytoplasm and extruded nuclei and also transfer iron to differentiating cells of the red blood cell lineage.
b. Adventitia l reticu lar ce l ls (Figure 10 .2) are believed to subdivide the bone marrow cavity into smaller compartments, which are occupied by is lands of hemopoietic cel ls . Adventitial reticular cells may accumulate fat (instead of fat cells), thus transforming red marrow into yellow marrow.
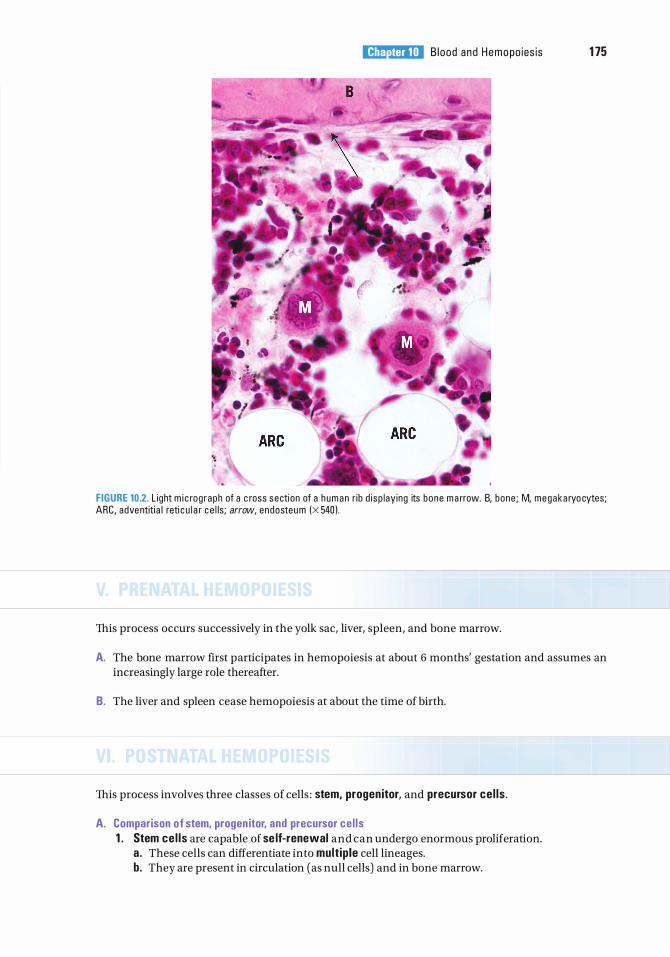
I!1JEtt!Dl!l B lood and Hemopo ies is 1 75
FIGURE 10.2. L ight m i c rog raph of a c ross secti on of a h uman r ib d i sp lay ing its bone m a rrow. B, bone ; M, megaka ryo cytes; ARC, adve ntiti a l reti c u l a r c e l ls ; arrow, endosteu m (X 540 ) .
This process occurs successively in the yolk sac, liver, spleen, and bone marrow.
A. The bone marrow first participates in hemopoiesis at about 6 months' gestation and assumes an increasingly large role thereafter.
B. The liver and spleen cease hemopoiesis at about the time of birth.
This process involves three classes of cells : stem, progen itor, and precursor ce l ls .
A. Comparison of stem, progen itor, and precursor ce l ls 1 . Stem ce l ls are capable of se lf-renewal and can undergo enormous proliferation.
a. These cells can differentiate into mult ip le cell lineages. b. They are present in circulation (as null cells) and in bone marrow.
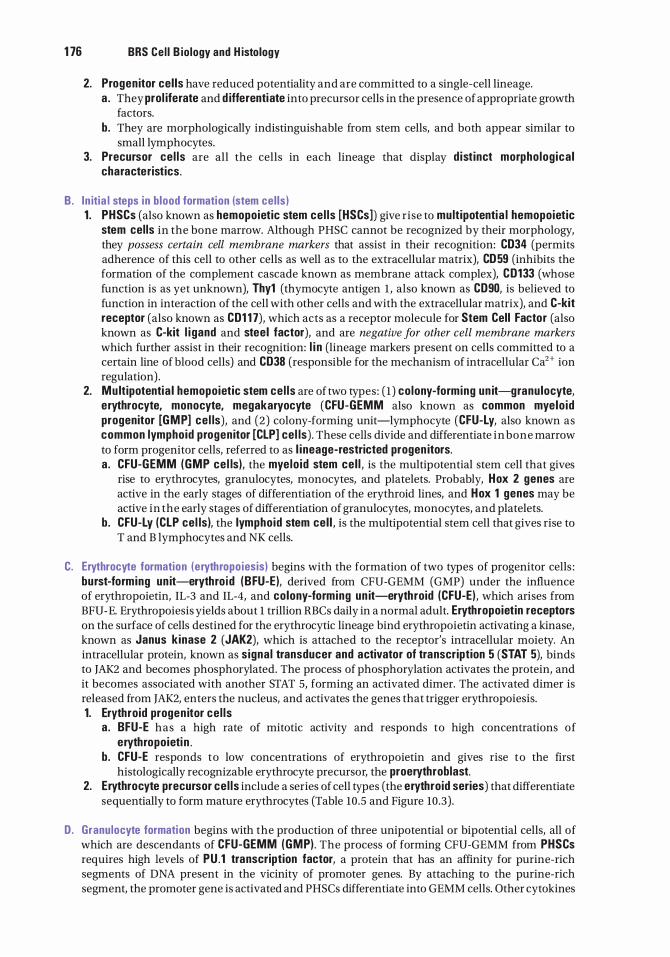
1 76 BRS Cel l B iology and H istology
2. Progenitor cel ls have reduced potentiality and are committed to a single-cell lineage. a . They prol iferate and d ifferentiate into precursor cells in the presence of appropriate growth
factors. b. They are morphologically indistinguishable from stem cells, and both appear similar to
small lymphocytes. 3. Precursor ce l ls are all the cells in each lineage that display d ist inct morpholog ica l
characteristics.
B. In itia l steps in blood formation (stem cel ls) 1 . PHSCs (also known as hemopoietic stem cel ls [HSCs]) give rise to multipotentia l hemopoietic
stem cel ls in the bone marrow. Although PHSC cannot be recognized by their morphology, they possess certain cell membrane markers that assist in their recognition: CD34 (permits adherence of this cell to other cells as well as to the extracellular matrix), CD 59 (inhibits the formation of the complement cascade known as membrane attack complex), CD133 (whose function is as yet unknown), Thy1 (thymocyte antigen 1 , also known as CD90, is believed to function in interaction of the cell with other cells and with the extracellular matrix), and C-kit receptor (also known as CD1 1 7), which acts as a receptor molecule for Stem Cell Factor (also known as C-kit l i gand and steel factor), and are negative for other cell membrane markers which further assist in their recognition: l i n (lineage markers present on cells committed to a certain line of blood cells) and CD38 (responsible for the mechanism of intracellular Ca2+ ion regulation) .
2. Multipotentia l hemopoietic stem cel ls are of two types : ( 1 ) colony-forming un it-granulocyte, erythrocyte, monocyte, megakaryocyte (CFU-GEMM also known as common myelo id progenitor [GMP] ce l ls), and (2) colony-forming unit-lymphocyte (CFU-Ly, also known as common lymphoid progenitor [CLP] cel ls) . These cells divide and differentiate in bone marrow to form progenitor cells, referred to as l i neage-restricted progen itors. a . CFU-GEMM (GMP ce l ls), the myelo id stem cel l , is the multipotential stem cell that gives
rise to erythrocytes, granulocytes, monocytes, and platelets. Probably, Hox 2 genes are active in the early stages of differentiation of the erythroid lines, and Hox 1 genes may be active in the early stages of differentiation of granulocytes, monocytes, and platelets.
b. CFU-Ly (CLP cel ls), the lymphoid stem cel l , is the multipotential stem cell that gives rise to T and B lymphocytes and NK cells.
C. Erythrocyte formation (erythropoiesis) begins with the formation of two types of progenitor cells : burst-forming un it-erythro id (BFU-E), derived from CFU-GEMM (GMP) under the influence of erythropoietin, IL-3 and IL-4, and colony-forming un it-eryth roid (CFU-E) , which arises from BFU-E. Erythropoiesis yields about 1 trillion RBCs daily in a normal adult. Erythropoietin receptors on the surface of cells destined for the erythrocytic lineage bind erythropoietin activating a kinase, known as Janus kinase 2 (JAK2), which is attached to the receptor's intracellular moiety. An intracellular protein, known as signa l transducer and activator of transcription 5 (STAT 5), binds to JAK2 and becomes phosphorylated. The process of phosphorylation activates the protein, and it becomes associated with another STAT 5, forming an activated dimer. The activated dimer is released from JAK2, enters the nucleus, and activates the genes that trigger erythropoiesis. 1. Erythroid progen itor ce l ls
a . BFU-E has a high rate of mitotic activity and responds to high concentrations of erythropoieti n .
b . CFU-E responds to low concentrations of erythropoietin and gives rise to the first histologically recognizable erythrocyte precursor, the proerythroblast.
2. Erythrocyte precursor ce l ls include a series of cell types (the erythroid series) that differentiate sequentially to form mature erythrocytes (Table 10 .5 and Figure 10.3) .
D. Granulocyte formation begins with the production of three unipotential or bipotential cells, all of which are descendants of CFU-GEMM (GMP) . The process of forming CFU-GEMM from PHSCs requires high levels of PU . 1 transcription factor, a protein that has an affinity for purine-rich segments of DNA present in the vicinity of promoter genes. By attaching to the purine-rich segment, the promoter gene is activated and PHSCs differentiate into GEMM cells. Other cytokines
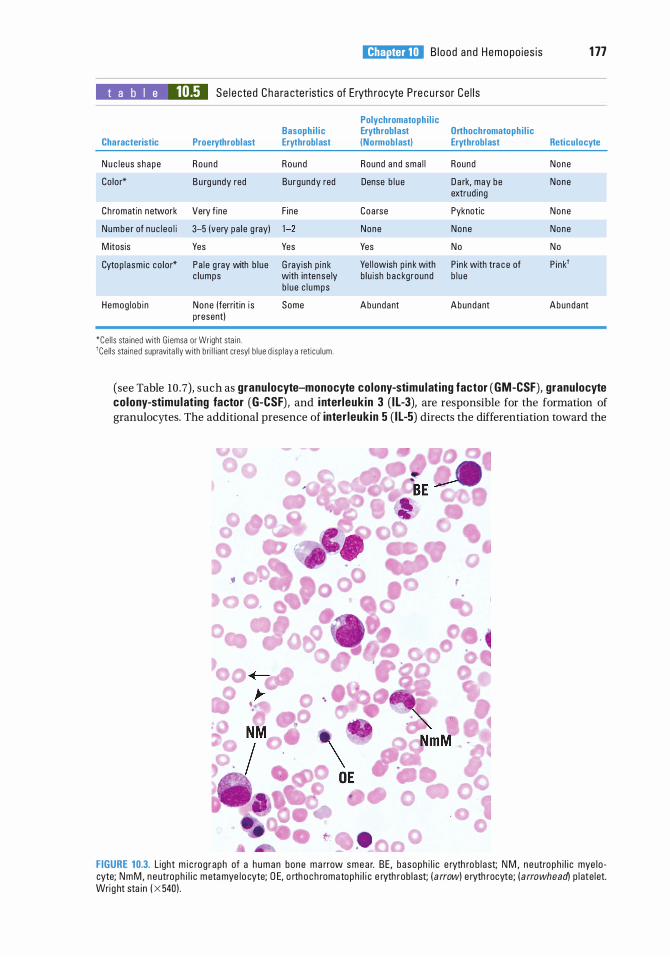
I!1JEtt!Dl!l B lood and Hemopo ies is 1 77
t a b I e 10.5 Se l e cted Cha ra cte risti cs of Eryth rocyte P re c u rsor Ce l l s
Polychromatophi l ic Basophi l ic Erythroblast Orthochromatoph i l ic
Characteristic Proerythroblast Erythroblast (Normoblast) Erythroblast Reticulocyte
N u c leus shape Round Round Round a nd sma l l Round None
Co lor* B u rg undy red Burgundy red Dense b l u e D a rk, may be None extrud ing
Ch romatin network Very f ine F ine Coa rse Pyknotic None
Numbe r of nuc l eo l i 3-5 (very pa l e g ray) 1 -2 None None None
M itosis Yes Yes Yes No No
Cytop l asm i c co lo r* Pa l e g ray with b l ue G rayish p i nk Ye l l owish p i n k with P i nk with tra c e of P i nk1 c l umps with intense ly b lu i sh b a c kground b l u e
b l u e c l umps
Hemog lob i n None (ferritin i s Some Abundant Abundant Abundant present)
*Ce l l s sta ined with G iemsa or Wright sta i n . 1Ce l l s sta ined supravita l l y with bri l l iant cresyl b l ue d i sp l ay a reti cu l um .
(see Table 10 .7), such as granulocyte-monocyte colony-stimulat ing factor (GM-CSF), granulocyte colony-stimulating factor (G-CSF), and i nterleukin 3 (I L-3), are responsible for the formation of granulocytes. The additional presence of inter leukin 5 ( l l-5) directs the differentiation toward the
FIGURE 10.3. L ight m i c rog raph of a h u m a n bone m a rrow smea r. BE , basoph i l i c e ryth ro b l ast; N M , n e utroph i l i c mye lo cyte; NmM, n eutroph i l i c m eta mye lo cyte; D E, o rth o c h romatoph i l i c e ryth rob last; ( a rrow) e ryth rocyte; ( arrowhead) p l ate let. Wrig ht sta in ( X 540) .
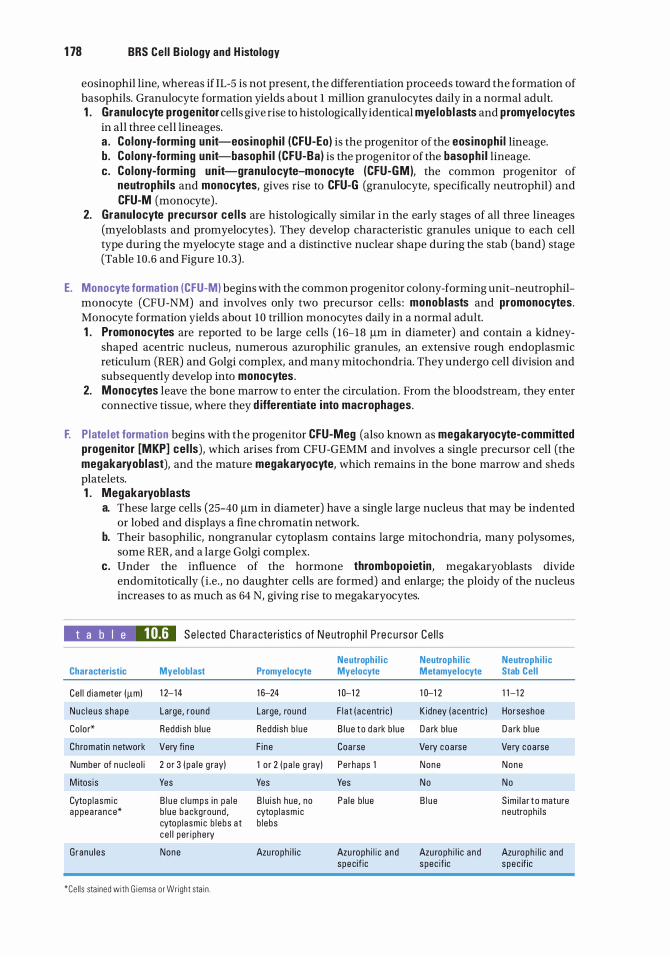
1 78 BRS Cel l B iology and H istology
eosinophil line, whereas if IL-5 is not present, the differentiation proceeds toward the formation of basophils. Granulocyte formation yields about 1 million granulocytes daily in a normal adult. 1 . Granulocyte progenitor cells give rise to histologically identical myelob lasts and promyelocytes
in all three cell lineages. a . Colony-forming un it-eosinophi l (CFU-Eo) is the progenitor of the eosinoph i l lineage. b. Colony-forming un it-basoph i l (CFU-Ba) is the progenitor of the basoph i l lineage. c. Colony-forming un it-granu locyte-monocyte (CFU-GM), the common progenitor of
neutrophi ls and monocytes, gives rise to CFU-G (granulocyte, specifically neutrophil) and CFU-M (monocyte) .
2. Granulocyte precursor ce l ls are histologically similar in the early stages of all three lineages (myeloblasts and promyelocytes) . They develop characteristic granules unique to each cell type during the myelocyte stage and a distinctive nuclear shape during the stab (band) stage (Table 10 .6 and Figure 10 .3) .
E. Monocyte formation (CFU-M) begins with the common progenitor colony-forming unit-neutrophilmonocyte (CFU-NM) and involves only two precursor cells : monoblasts and promonocytes. Monocyte formation yields about 10 trillion monocytes daily in a normal adult. 1 . Promonocytes are reported to be large cells ( 16-18 f..tm in diameter) and contain a kidney
shaped acentric nucleus, numerous azurophilic granules, an extensive rough endoplasmic reticulum (RER) and Golgi complex, and many mitochondria. They undergo cell division and subsequently develop into monocytes .
2. Monocytes leave the bone marrow to enter the circulation. From the bloodstream, they enter connective tissue, where they d ifferentiate into macrophages.
F. Plate let formation begins with the progenitor CFU-Meg (also known as megakaryocyte-committed progen itor [MKP] cel ls), which arises from CFU-GEMM and involves a single precursor cell (the megakaryoblast), and the mature megakaryocyte, which remains in the bone marrow and sheds platelets. 1 . Megakaryoblasts
a. These large cells (25-40 f..tm in diameter) have a single large nucleus that may be indented or lobed and displays a fine chromatin network.
b. Their basophilic, nongranular cytoplasm contains large mitochondria, many polysomes, some RER, and a large Golgi complex.
c. Under the influence of the hormone thrombopoietin, megakaryoblasts divide endomitotically (i .e. , no daughter cells are formed) and enlarge; the ploidy of the nucleus increases to as much as 64 N, giving rise to megakaryocytes.
t a b I e 10.6 Se l e cted Cha ra cte r isti cs of Ne utroph i l P re c u rso r Ce l l s
Neutroph i l ic Neutrophi l ic Characteristic Myeloblast Promyelocyte Myelocyte Metamyelocyte
Ce l l d i a meter ()lm) 1 2- 14 1 6-24 1 0-1 2 1 0-1 2
Nuc l e u s shape Large, r ound Large, round F l a t ( a centri c ) K idney ( a c entri c )
Co lor* Redd ish b l ue Redd ish b l u e B l u e to d a rk b l ue D a rk b l ue
Ch romatin network Very fi ne F i ne Coa rse Ve ry coa rse
Number of n u c leo l i 2 o r 3 ( p a l e g ray) 1 o r 2 ( p a l e g ray) Perhaps 1 None
M itos is Yes Yes Yes No
Cytop l asm ic B l u e c l umps i n p a l e B l u ish hue , no Pa le b lue B l u e a ppea ra n c e* b l u e background , cytop l asm ic
cytop l asm ic b l ebs a t b lebs ce l l pe r i phery
G ranu l es None Azu roph i l i c Azu roph i l i c a nd Azu roph i l i c a nd specif ic spec if ic
*Ce l l s sta ined with G i emsa o r Wright sta i n .
Neutrophi l ic Stab Cel l
1 1 -1 2
Horseshoe
D a rk b l ue
Ve ry coa rse
None
No
S im i l a r t o mature neutroph i l s
Azu roph i l i c and spec if ic
2. Megakaryocytes
I!1JEtt!Dl!l B lood and Hemopo ies is 1 79
a. These extremely large cells (40- 100 J.Lm in diameter) have a single large polypoid nucleus that is highly indented (Figure 10 .2) .
b. They possess a well-developed Golgi complex associated with the formation of a-granules, lysosomes, and dense bodies Co-granules); they also contain many mitochondria and an extensive RER.
c. Megakaryocytes lie just outside the sinusoids in the bone marrow and form p latelet demarcation channels, which fragment into proplatelets (clusters of adhering platelets) or single platelets that are released into the sinusoidal lumen.
G. Lymphocyte formation ( lymphopo iesis) begins with differentiation of CFU-Ly (CLP), the lymphoid stem cell, into the immunoincompetent progenitor cells CFU-LyB and CFU-LyT. This step requires the presence of medium concentrations of transcription factor PU . t as well as intranuclear zinc finger transcription factors such as the lkaros fami ly of transcription factors. These zinc finger proteins have protruding hairpin-like extensions, maintained by zinc and iron ions that fit into grooves in the promoter or other regulatory regions of the DNA molecule and, thereby, activate or inhibit a particular gene. (It should be noted that zinc finger proteins bind not only to DNA but also to RNA, proteins, as well as to lipids.)
These pre lymphocytes are processed and become mature immunocompetent cells. 1 . B lymphocyte (B-ce l l ) maturation
a . Requires the presence of Pax5 transcription factor. b. Pre-B lymphocytes acquire cell surface markers, including membrane-bound antibodies,
which confer immunocompetence. c . In mammals, B-cell maturation occurs in the bone marrow, whereas in birds it occurs in the
bursa of Fabricius (hence, B lymphocytes) . 2. T- lymphocyte (T-ce l l ) maturati on
a . Requires the presence of GATA-3 transcription factor. b. Progenitor T lymphocytes migrate to the thymic cortex, where they acquire cell surface
markers, including T-ce l l receptors, which confer immunocompetence . c . Most of the newly formed T lymphocytes are destroyed in the cortex of the thymus and do
not enter into circulation. 3. Mature B and T lymphocytes leave the bone marrow and thymus, respectively, and circulate to
peripheral organs (e.g., the lymph nodes and spleen) to establish clones of immunocompetent lymphocytes (see Chapter 12} .
A. Hemopoiesis is modulated by several growth factors and cytokines, including CSFs, stem cell factor (steel factor}, interleukins, and macrophage-inhibiting protein-a (Table 10 .7) . Stem ce l l factor is probably the most important of the CSFs because it must be present to maintain a large enough population of PHSCs as well as multipotential hemopoietic stem cells and progenitor cells.
B. These factors may circulate in the bloodstream, acting as hormones, or they may act as local factors produced in the bone marrow that facilitate and stimulate formation of blood cells in their vicinity.
C. They act at low concentrations and bind to specific membrane receptors on single target cells.
D. Their various effects on target cells include control of mitotic rate, enhancement of cell survival, control of the number of times the cells divide before they differentiate, and promotion of cell differentiation.
E. Hemopoietic stem cel ls that do not contact growth factors, especially Stem Cell Factor, usually enter apoptosis and are eliminated by macrophages.
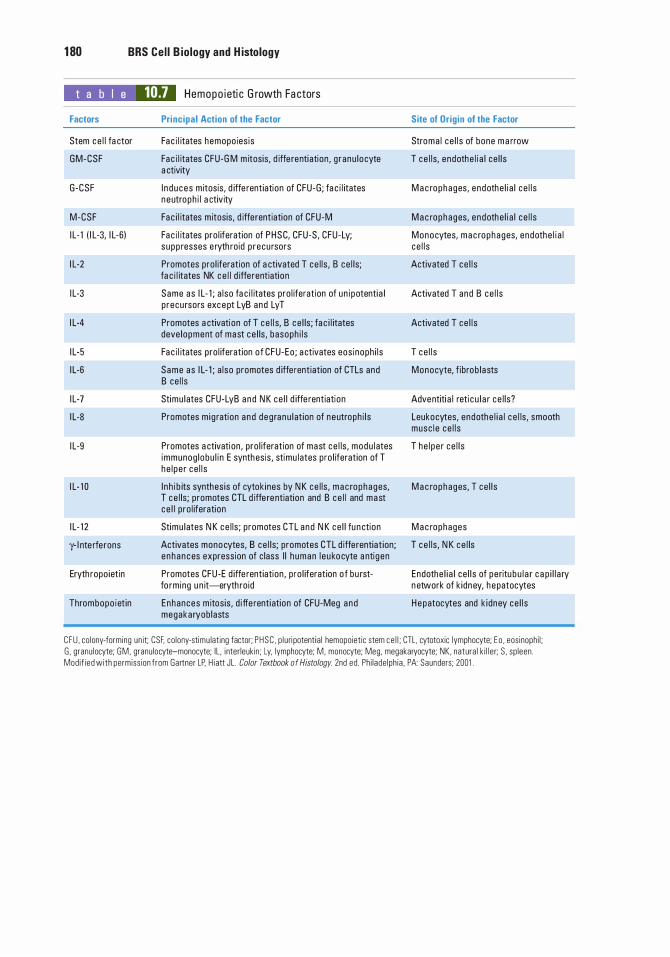
1 80 BRS Cel l B iology and H istology
t a b I e 10.7 Hemopo i eti c G rowth Fa ctors
Factors
Stem ce l l fa ctor
GM-CSF
G-CSF
M-CSF
I L- 1 ( I L-3, I L-6)
I L-2
I L-3
I L-4
I L-5
I L-6
I L-7
I L-8
I L-9
I L- 1 0
I L- 1 2
y- l nte rfe rons
Eryth ropo ietin
Thrombopo iet in
Principal Action of the Factor
Fac i l itates hemopo ies is
Fa c i l itates CFU-G M m itosis, d iffe renti ation , g ranu l ocyte a ctivity
I n d u ces m itosis, d iffe rentiation of CFU-G ; fa c i l itates neutroph i l a ctivity
Fa c i l itates m itosis, d iffe rentiation of CFU-M
Fac i l itates pro l iferation of PHSC, CFU-S, CFU-Ly; s upp resses e ryth roid p recu rsors
Promotes pro l iferation of a ctivated T ce l ls , B ce l ls; fa c i l itates NK c e l l d iffe rentiation
Same as I L- 1 ; a l so fa c i l itates pro l iferation of un i potenti a l p recu rsors exce pt LyB and LyT
Promotes a ctivation of T ce l l s, B ce l ls ; fa c i l itates deve lopment of mast ce l ls, basoph i l s
Fa c i l itates pro l iferation of CFU-Eo ; a ctivates eos inoph i l s
Same as I L- 1 ; a l so promotes d iffe rentiat ion of CTLs and B ce l l s
Stimu l ates CFU-LyB and N K ce l l d iffe rentiation
Promotes m i g ration a nd deg ranu l at ion of neutroph i l s
Promotes a ctivation , pro l iferation of mast ce l ls , modu l ates immunog lobu l i n E synthesis , stimu lates pro l iferation of T he l pe r ce l l s
I n h i b its synthes is of cytok ines by N K ce l ls , mac rophages, T ce l ls; promotes CTL d iffe re ntiation and B c e l l and mast ce l l p ro l iferation
Stimu l ates N K ce l ls ; p romotes CTL and N K ce l l fu n ction
Activates monocytes, B ce l ls; promotes CTL d iffe rentiat ion; e nhances expression of c lass I I h uman l e ukocyte a nti gen
Promotes CFU-E d iffe rentiation , p ro l iferation o f bu rstfo rming u n it-eryth roid
Enhances m itos is , d i ffe renti ation of CFU-Meg and megakaryob lasts
Site of Origin of the Factor
Stroma l ce l l s of bone m a rrow
T ce l ls, endothe l i a l ce l l s
M a c rophages, endothe l i a l ce l l s
M a c rophages, endothe l i a l ce l l s
Monocytes, mac rophages, endothe l i a l ce l l s
Activated T ce l l s
Activated T and B ce l l s
Activated T ce l l s
T ce l l s
Monocyte, f ibrob l asts
Adventiti a l reti c u l a r ce l ls?
Leukocytes, endothe l i a l c e l ls , smooth musc l e ce l l s
T he l pe r ce l l s
M a c rophages, T ce l l s
M a c rophages
T ce l ls , N K ce l ls
Endothe l i a l ce l l s of peritu bu l a r c a p i l l a ry n etwork of k idney, h epatocytes
H e patocytes and k i dney ce l l s
CFU , co lony-forming un it CSF, co lony-stimu lat ing factor; PHSC , p l u ri potent ia l hemopoiet ic stem c e l l ; CTL, cytotoxic lymphocyte; E o , eos inoph i l ; G , granu locyte; GM , granu locyte-monocyte; IL , i nter leukin ; Ly, lymphocyte; M , monocyte; Meg, megakaryocyte; NK , natura l k i l l e r; S , sp leen . Mod i f ied with permiss ion f rom Gartner LP. H i att JL . Color Textbook of Histology. 2nd ed . Ph i l ade lph ia , PA: Saunders; 2001 .
Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1 . Which of the following proteins associated with the erythrocyte plasma membrane is responsible for maintaining the cell's biconcave disk shape?
(A) HbA1 (B ) HbA2 (C ) Porphyrin (D ) Spectrin (E ) a-Actinin
2. Which of the following is an immunocompetent cell?
(A) Red blood cell (B ) Lymphocyte (C ) Platelet (D ) Neutrophil (E ) Basophil
3. Which of the following is derived from CPU-Meg (MKP cells)?
(A) Red blood cell (B ) Lymphocyte (C ) Platelet (D ) Neutrophil (E ) Basophil
4. Which of the following is derived from CFU-E?
(A) Red blood cell (B) Lymphocyte (C ) Platelet (D ) Neutrophil (E ) Basophil
5. Which of the following is derived from CFU-GM?
(A) Red blood cell (B ) Lymphocyte (C) Platelet (D ) Neutrophil (E ) Basophil
6. Which of the following is associated with demarcation channels?
(A) Red blood cell (B) Lymphocyte (C) Platelet (D ) Neutrophil (E) Basophil
7. Which of the following is derived from myeloblasts?
(A) Red blood cell (B ) Lymphocyte (C) Platelet (D ) Monocyte (E ) Basophil
8. Which one of the following cells is associated with antibody production?
(A) Red blood cell (B ) Lymphocyte (C) Monocyte (D ) Neutrophil (E) Basophil
1 81
1 82 BRS Cel l B iology and H istology
9. Which of the following possesses specific and azurophilic granules?
(A) Red blood cell (B ) Lymphocyte (C) Platelet (D ) Neutrophil (E ) Monocyte
1 0. Which of the following is derived from reticulocytes?
(A) Red blood cell (B ) Lymphocyte (C) Platelet (D ) Neutrophil (E ) Basophil
1 1 . A 4-year-old boy is taken by his parents to the pediatrician because of vomiting, headaches, and tenderness in the bones of his arms and legs. On palpation, the physician notes that many lymph nodes are enlarged, as is the liver. The pediatrician should order a complete blood count in order to determine whether or not the child may have
(A) chronic leukemia. (B ) infectious mononucleosis. (C) von Willebrand disease. (D) acute leukemia. (E ) pernicious anemia.
Answers and Explanations
1 . D. Spectrin is associated with the erythrocyte cell membrane and assists in maintaining its biconcave disk shape (see Chapter 10 II B) .
2. B . Lymphocytes are immunocompetent cells (see Chapter 10 VI G) .
3. C. Platelets are derived from CFU-Meg (MKP cells) (see Chapter 10 VI F) .
4. A. Red blood cells are derived from CFU-E (see Chapter 10 VI C) .
5. D . Neutrophils are derived from CFU-GM (see Chapter 10 VI D).
6. C. Platelets are derived from megakaryocytes, and those cells possess demarcation channels (see Chapter 10 VI F) .
7. E. Basophils are derived from myeloblasts (see Chapter 10 VI D) .
8. C. Lymphocytes and plasma cells manufacture antibodies (see Chapter 10 VI G) .
9. D . Neutrophils possess both azurophilic and specific granules (see Chapter 10 II B 2) .
1 0. A. Red blood cells are derived from reticulocytes (see Table 10.5) .
1 1 . D . Acute leukemia is a disease of children with symptoms that include headaches; vomiting; swollen lymph nodes, liver, and spleen; and the sensation of tenderness in bones. Chronic leukemia is a disease that usually affects adults. von Wille brand disease is a coagulation disorder and does not have the same symptoms as acute leukemia. Infectious mononucleosis affects mostly young adults of high school and college age. Pernicious anemia is caused by vitamin B deficiency, and its symptoms do not resemble those of acute leukemia (see Chapter 10 II B 2 Clinical Considerations).
1 83
Circulatory System
I. OVERVIEW-BLOOD VASCULAR SYSTEM
The blood vascular system consists of the heart, arteries, veins, and capillaries. This system transports oxygen and nutrients to tissues, carries carbon d ioxide and waste products from the tissues, and circulates hormones from the site of synthesis to their target cells.
A. The heart is a four-chambered pump composed of two atria and two ventric les and is surrounded by a fibroserous sac called the pericard ium.
Tetra logy of Fa l l ot Tetra logy of Fa l l ot is a congenital ma lformation cons isti n g of a defe c
tive i nte rve ntri c u l a r s eptum, hype rtro phy o f th e ri g ht ve ntri c l e ( d u e t o a n a rrow pu lmona ry a rte ry o r va lve) , a n d tra nsposed ( d extro posed ) a o rta . I t s hou l d be repa i red surg ica l ly ea rly i n l ife, b efore the p u lmona ry constr icti on becomes exa c e rbated .
B. Atria are receiving chambers, whereas ventricles are discharging chambers. Moreover, the heart is divided functionally into the right heart (pu lmonary system) and the left heart (systemic system) . The right atrium receives venous blood from the body and discharges i t into the right ventricle. From here the blood is pumped into the pulmonary trunk to be distributed to the lungs. Venous blood from the pulmonary system is received in the left atrium and then discharged into the left ventricle to be pumped out through the aorta into the systemic circulation.
The heart receives sympathetic innervation via upper thoracic levels of the spinal cord and parasympathetic innervation via vagus nerves, which modulate the rate of the heartbeat but do not initiate it. The heart (mostly the atria) also produces atria l natri uretic peptide, and B-type natriuretic peptide, hormones that increases secretion of sodium and water by the kidneys, inhibits renin release, and decreases blood pressure. • Sympathetic innervation accelerates the heart rate, increases the force of the heartbeat, and
dilates the coronary vessels. • Parasympathetic innervation slows the heart rate, reduces the force of the heartbeat, and con
stricts the coronary vessels.
1 84
1 . Card iac layers (from internal to external) a. Endocardium lines the lumen of the heart and is composed of simple squamous epithelium
(endothe l ium) and a thin layer of loose connective tissue. Subendocardium, a connective tissue layer that contains veins, nerves, and Purkinje fibers, underlies it.
l!1lEJ1l!Dij C i rcu l ato ry System 1 85
b. Myocard ium consists of layers of striated card iac muscle cel ls arranged in a spiral fashion about the heart's chambers and inserted into the fibrous skeleton. The myocardium contracts to propel blood into the arteries for distribution to the body.
c. Epicardium, the outermost layer of the heart, constitutes the visceral layer of the pericard ium. It is composed of simple squamous epithelium (mesothe l ium) on the external surface. Beneath the mesothelium lies fibroelastic connective tissue, containing nerves, the coronary vessels, and adipose tissue.
2. The f ibrous skeleton of the heart consists of thick bundles of col lagen f ibers oriented in various directions and especially oriented to support the four valve rings of the heart valves. It also contains occasional foci of fibrocartilage.
3. Heart va lves a . Atrioventricu lar (AV) valves are composed of a skeleton of fibrous connective tissue,
arranged like an aponeurosis, and lined on both sides by endothelium. They are attached to the annu l i fi brosi of the fibrous skeleton. The right AV valve is formed of three interlocking cusps (tri cusp id valve), whereas the left AV valve is formed of two interlocking cusps (bicuspid or mitra l valve) . These valves prevent regurgitation of ventricular blood into the atria.
b. Semi lunar va lves in the pulmonary and aortic trunks are each composed of three cusps that approximate each other as they fill with arterial blood. They are lined with endothelium on both sides separated by sparse strands of connective tissue. These valves prevent regurgitation of pulmonary and aortic blood into the respective ventricles.
CLIN ICAL CONSIDERATIONS
Rheumatic heart valve d isease is a sequel to chi ldhood rheumatic fever (subsequent to streptococca l infection ), which causes sca rring of the heart valves.
1. The d i sease i s c h a ra cte r ized by red u c e d e l asti c ity of the h e a rt va lves, m a ki n g th em u n ab l e to c l ose ( i ncompetence) or u n a b l e o pen (stenosis) p rope rly.
2. It most common ly affe cts th e mitra l va lve, fo l l owed by the a o rti c va lve .
4. The impu lse-generati ng and impu lse-conducting system of the heart comprises several specialized structures with coordinated functions that act to i n itiate and regu late the heartbeat. a . The sinoatr ia l (SA) node, the pacemaker of the heart, is composed of specialized cardiac
cells located within the wall of the right atrium adjacent to the entry of the superior vena cava into the heart. It generates impu lses that initiate contraction of atrial muscle cells; which are then conducted to the AV node.
b. The AV node is located in the wall of the right atrium, adjacent to the tricuspid valve. c. The AV bund le of H is is a band of conducting tissue radiating from the AV node into the
interventricular septum, where it divides into two branches and continues as Purkinje fibers.
d . Purkinje f ibers are large, modified cardiac muscle cells (see Chapter 8 V B 9) that make contact with cardiac muscle cells at the apex of the heart via gap junctions, desmosomes, and fasciae adherentes.
e. As indicated (in Section I B of the current chapter), the autonomic nervous system modulates the heart rate and stroke volume.
CLIN ICAL CONSIDERATIONS
Card iac arrest o c c u rs when the h e a rt ceases to beat, resu lti n g i n c essation of b l ood f l ow i n the e nt ire c i rc u l ato ry system . Card i ac d eath
i s imm i nenet u n l ess c a rd io p u lmona ry resusc itati on a n d d efi b r i l l ati o n a re c o ndu cted s u c cessfu l ly and th e e l e ctri c a l system of th e h e a rt is revived . H e a lth c ond it ions that may lead to c a rd i a c a rrest i n c l u d e, b ut a re n ot l im ited to, ta c hyca rd i a , fi b r i l l ation , a n d b radyca rd i a .
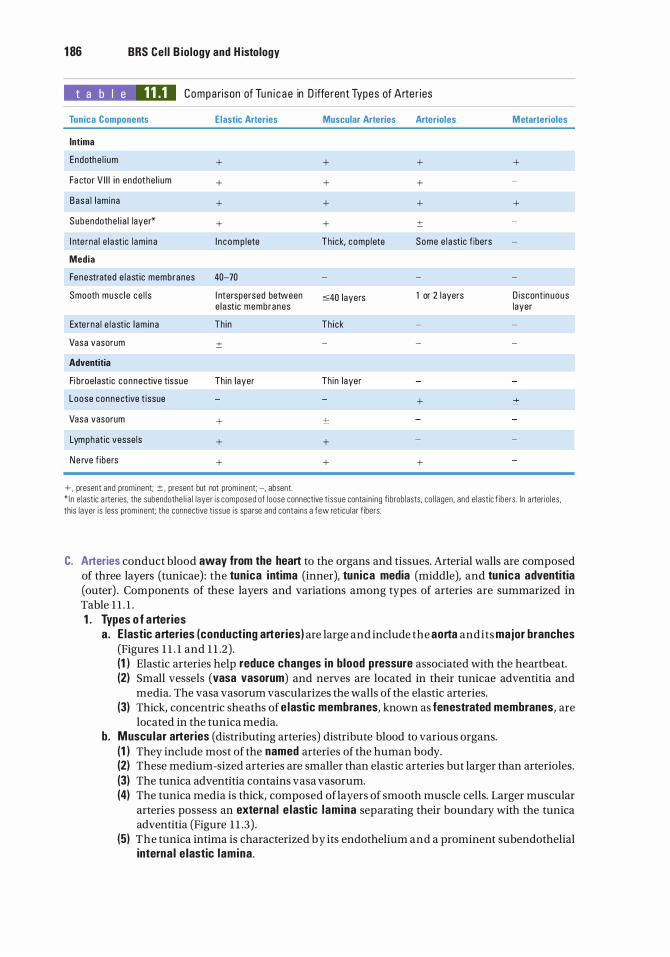
1 86 BRS Cel l B iology and H istology
t a b l e 11.1 Compa rison of Tu n i c a e in D iffe rent Types of Arte r ies
Tunica Components
Intima
Endothe l i um
Fa ctor V I I I i n endothe l i um
Basa l l am ina
Subendothe l i a l layer*
I nte rna l e l astic l am i na
Media
Fenestrated e l a st ic membranes
Smooth musc l e ce l l s
Exte rna l e l a st ic l am i na
Vasa vasorum
Adventitia
Fi broe lastic connective tissue
Loose connective t issue
Vasa vasorum
Lymphatic vesse ls
N e rve f ibers
Elastic Arteries
+
+
+
+
I n com p lete
40-70
I nterspersed between e last ic membranes
Th in
±
Thin layer
+
+
+
+ , present and prominent; ± , present but not prominent; -, absent.
Muscular Arteries Arterioles
+ +
+ +
+ +
+ ±
Th i ck, comp l ete Some e l a st ic f ibers
:s:40 layers 1 or 2 1 ayers
Th i ck
Th in layer
+
+
+ +
Metarterioles
+
+
D iscontin uous layer
* I n e lastic a rteries. the subendothe l i a l l ayer is composed of loose connective t i ssue conta i n i ng f ibroblasts. co l lagen . and e lastic f ibers . I n a rteri o les . th is layer is less prominent; the connective t issue is sparse and conta ins a few ret icu lar f ibers.
C. Arteries conduct blood away from the heart to the organs and tissues. Arterial walls are composed of three layers (tunicae) : the tunica intima (inner), tunica media (middle), and tunica adventitia (outer) . Components of these layers and variations among types of arteries are summarized in Table 1 1 . 1 . 1 . Types o f arteries
a . E lastic arteries (conducting arteries) are large and include the aorta and its major branches (Figures 1 1 . 1 and 1 1 .2) . (1 I Elastic arteries help reduce changes in blood pressure associated with the heartbeat. (2) Small vessels (vasa vasorum) and nerves are located in their tunicae adventitia and
media. The vasa vasorum vascularizes the walls of the elastic arteries. (3) Thick, concentric sheaths of e lastic membranes, known as fenestrated membranes, are
located in the tunica media. b. Muscu lar arteries (distributing arteries) distribute blood to various organs.
(1 I They include most of the named arteries of the human body. (2) These medium -sized arteries are smaller than elastic arteries but larger than arterioles. (3) The tunica adventitia contains vasa vasorum. (4) The tunica media is thick, composed of layers of smooth muscle cells. Larger muscular
arteries possess an external e lastic lamina separating their boundary with the tunica adventitia (Figure 1 1 .3) .
(51 The tunica intima is characterized by its endothelium and a prominent subendothelial interna l e lastic lamina .
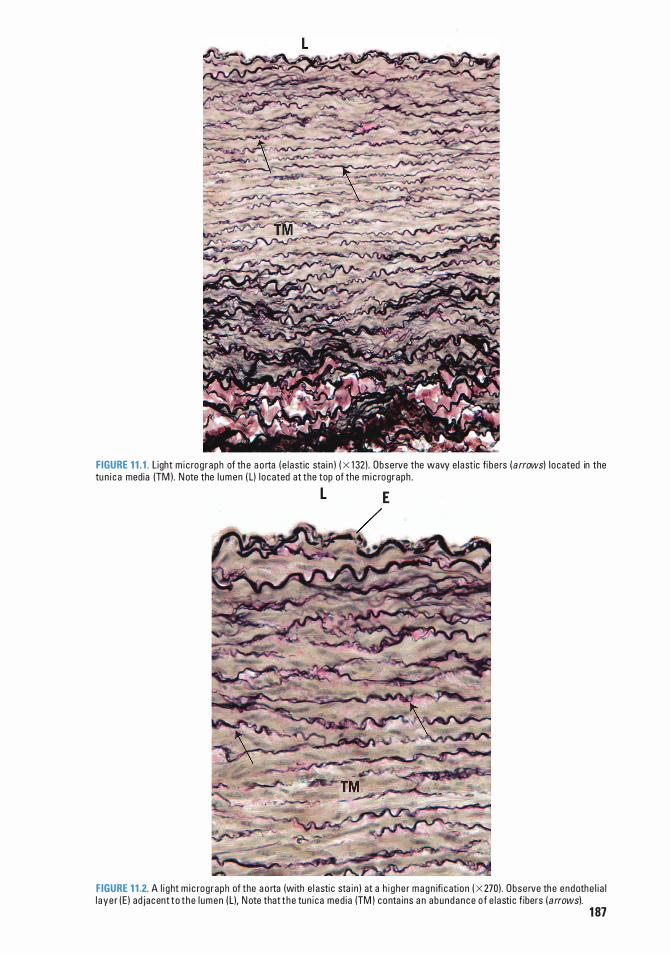
FIGURE 1 1 . 1 . L ight m i c rog raph of th e a o rta ( e l a st ic sta i n ) ( X 1 32) . Obse rve the wavy e l astic fi be rs ( a rrows) l o cated in the tu n i c a media (TM ) . N ote the l umen ( L) I o cated at the top of the m i c rog raph . L E
FIGURE 1 1 .2. A l i ght m i c rog raph of the a o rta (with e l asti c sta i n ) at a h i g he r m a g n ifi c ation ( X 270) . Obse rve the endothe l i a l l a ye r ( E ) ad jacent t o t he l umen ( L), N ote that t he tun i ca med i a (TM ) conta ins a n a bundance o f e l a sti c f ibers ( arrows).
1 87

1 88 BRS Cel l B iology and H istology
FIGURE 1 1 .3. L ight m i c rog raph of a n a rtery (X 1 32) . Obse rve the lumen ( L) , e ndothe l i a l l ayer (E ) , inte rna l e l ast ic l am i na ( single arrow), tu n i c a intima ( T I ) , tun i c a med i a (TM), externa l e l a sti c l am i na ( double arrows), a n d tun i c a a dventitia (TA) .
llfi'n�M��� Atherosc lerosis Athe ros c l e ros is i s the most fre q u ent c a use of morb i d ity of the vasc u l a r
d i seases . I t is c h a ra cter ized b y d e pos its o f ye l l owish p l a q u e s (atheromas) i n t h e intima o f l a rg e a n d med i um -s ized a rte r ies . T he p l a q ues m ay b l o c k b l o o d f low t o th e r e g i o n supp l i e d by th e affe cted a rte ry. Conti n u ed d e pos its form p l a ques that red u c e the l um i n a of the vesse ls , a n d th e pati e nt m ay fe e l refe rred pa i n a n d pressure . Susta i n e d na rrowin g res u lts i n i s chem i a o r c omp l ete b l o c kage , wh i ch may be fata l if u ntre ate d . Ma jo r vesse ls affected by ath e rosc l e ros is i n c l u d e term i n a ls o f t he c o ro n a ry a rter ies , l a rg e r b ra n c he s of the c a rotid a rte r ies , c e re b ra l a rter ies, l a rg e a rter ies of the lower extrem i t ies, ren a l a rter ies , a n d mesente r ic a rteri es . Athe ros c l e ros is o f t he c e re b ra l a rte r ies is th e ma j o r c a use o f stro ke ( b ra i n i nfa rct) . Oth e r athe ros c l e roses affect t he h e a rt ( see th e sectio n on i s chem i c h e a rt d i sease ), i s chem i c bowel d i sease , a n d rena l a rte r i a l i s c hem i a .
Ischemic (coronary) heart d isease I s c hem i c h e a rt d i sease is usua l ly c a used by coronary atherosc lerosis, which resu lts i n d e c reased b lood f l ow to th e myo c a rd i um . It may resu lt ( depend ing on its seve rity) i n ang i na pecto ris, myo c a rd i a l i nfarction , c h ron i c i s c hem i c c a rd i opathy, o r sudden c a rd i a c d eath. Ang iop l asty i s the c u rrent mode of treatment fo r p a rti a l ly c l ogged arte ries, a nd bypass su rge ry is n ec essary fo r severe ly c l ogged a rte r ies .
c. Arterio les ( 10-100 f-lm in diameter) regulate blood pressure and are the terminal arterial vessels. They are the sma l lest arteries, with diameters of less than 0 . 1 mm and a narrow lumen; their luminal diameter usually equals the wall thickness. (1 ) The tunica adventitia is scant, whereas the tunica media consists of up to two layers of
smooth muscle. (2) The tunica intima consists of an endothelium, basal lamina, and scant connective tissue.
l!1lEJ1l!Dij C i rcu l ato ry System 1 89
d. Metarter io les ( �8 11-m in diameter) are narrow vessels arising from arterioles that give rise to capi l laries. (1 ) They are surrounded by incomplete rings of smooth muscle cells and possess individual
smooth muscle cells (precap i l l a ry sphincters) that surround capillaries at their origin. (2) Constriction of precapillary sphincters prevents blood from entering the capillary bed.
lin'l(lfll Arteriosc lerosis Arte r ios c l e ros is i s c h a racter ized by ri g i d ity and hya l i n e th i c ken i n g of
th e b lood vesse l wa l l s . It may i nvolve th e med i a of med i um -s ized a rter ies and eve ntu a l c a l c ifi c at ion i n the med i a . Hya l i n e th i c ken i n g u sua l ly atta c ks sma l l a rte r ies and a rte r io les i n the k i dn eys and i s u sua l ly assoc i ated with hyp e rtens i on a n d d i a b etes me l l itus .
2. Vasoconstriction primarily involves arterioles and reduces blood flow to a local region. Vasoconstriction is stimulated by sympathetic nerve f ibers (see Chapter 9 IX B) via vasomotor nerves. These nerves do not synapse on the muscle cells of the tunica media; rather they discharge the neurotransmitter norepinephrine that diffuses throughout the muscle layer and induces contraction of cells via gap junctions that reduce luminal diameter.
3. Vasod i lat ion is accomplished by parasympathetic nerve f ibers as follows : a. Acetylcholine released from these nerve terminals stimulates the endothelium to release
n itric oxide, previously known as endothelial-derived relaxing factor (EDRF). b. N itric oxide diffuses to smooth muscle cells in the vessel wall and activates their cyclic
guanosine monophosphate ( cGMP) system, resulting in relaxation, which dilates the lumen.
Aneurysm i s a bal loon ing out of an artery. CLIN ICAL CONSIDERATIONS
1 . An a n e u rysm o c c u rs b e c a use o f a wea kness i n t h e a rte r i a l o r venous wa l l , wh i c h may resu lt i n r upture . Arte ri a l a n e u rysms m ay resu lt f rom a ge - re l ated d i s p l a c ement of e l a sti c fi b e rs by co l l a g en .
2 . Aneu rysms may b e assoc i ated with atherosc lerosis and syph i l is . Atherosc l e ros is , e spec i a l ly of the a b dom i n a l a o rta, may be d u e to g e net ic c o nne ctive t issue d i so rde rs s u ch as M a rfa n syn d rome o r Eh l e rs-D an l o s synd rome ( see C h a pter 4, I l l A C l i n i c a l Cons i de rati ons ) .
3. D issecti n g a n e u rysms a re most often l o cated i n the a scend i n g a o rta a n d a re re presented by a l o ng itu d i n a l tea r i n the wa l l c h a ra cte r ized by tea ri n g of th e e l a sti c a n d muscu l a r t issues, resu lti n g i n ru ptu re i nto th e pe r i c a r d i a ! s a c .
4 . These c ond iti ons c a n be l ife -th reaten i n g b eca use a weakness i n a n a rte r i a l wa l l may c a use the a rte ry to bu rst.
D. Capi l la ries are small vessels (about 8-10 11-m in diameter and usually less than l mm long) . Capillaries exhibit selective permeabi l ity, permitting the exchange of oxygen, carbon dioxide, metabolites, nutrients, metabolic wastes, signaling molecules, hormones, and other substances between the blood and tissues. They form cap i l la ry beds interposed between arterioles and venules. 1. Cap i l la ry endothe l ia l cel ls-General features. Capillaries consist of a s ing le layer of
endothe l ia l cel ls arranged as a continuum to form a cylinder, which is surrounded by a basal lamina and occasional pericytes (see Chapter 6 III A.2) . Endothelial cells a. are nucleated, polygonal cells with an attenuated cytoplasm. b. possess a Golgi complex, ribosomes, mitochondria, and some rough endoplasmic
reticulum (RER) . c. contain intermediate filaments of desmin , vimentin , or both in the perinuclear zone; these
filaments have a supportive function. d. are generally joined by fasc iae occludentes (tight junctions); some desmosomes and gap
junctions also are present. Characteristically, they contain pinocytotic vesicles. e. luminal diameter sometimes accommodates only one red blood cell at a time.
2. C lassification of cap i l l a ries. There are three types of capillaries, depending on the structure of their endothelial cells and the continuity of the basal lamina (Figure 1 1 .4).
tahir99-VRG & vip.persianss.ir
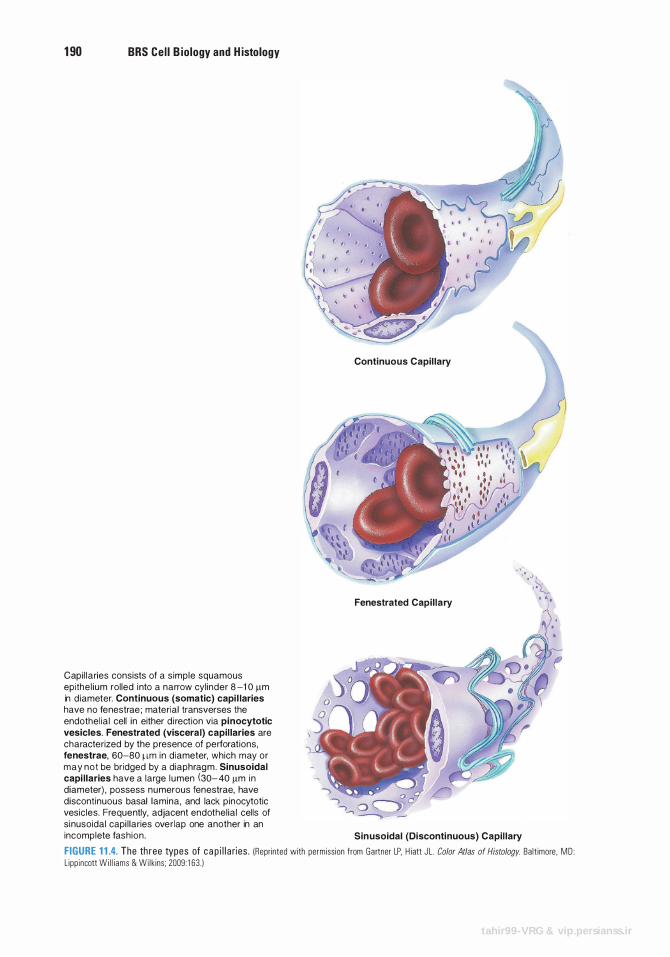
1 90 BRS Cel l B iology and H istology
Capi l laries consists of a s imple squamous epithe l ium rol led i nto a narrow cyl inder 8 -1 0 11m in d iameter. Continuous (somatic) capi l laries have no fenestrae ; material transverses the endothel ia l cell in either d i rection via pinocytotic vesicles. Fenestrated (visceral) capil laries are characterized by the presence of perforat ions, fenestrae, 60-80 11m i n d iameter, which may or may not be bridged by a d iaphrag m . Sinusoidal capi l laries have a large l u men (30- 40 11m i n diameter) , possess nu merous fenestrae, have disconti nuous basal lamina, and lack p inocytotic vesicles. Frequently, adjacent endothel ia l cells of s i nusoidal capi l laries ove rlap one another in an
Continuous Capil lary
Fenestrated Capi l lary
incomplete fash ion . Sin usoidal (Discontinuous) Capil lary
FIGURE 1 1 .4. The th ree types of c a p i l l a ries . !Reprinted with permiss ion from Gartner LP. H iatt J L. Color Atlas of Histology. Ba lt imore . MD : L ipp incott Wi l l i ams & Wi l k ins ; 2009 : 1 63 . )
tahir99-VRG & vip.persianss.ir
l!1lEJ1l!Dij C i rc u l ato ry System 1 91
a. Conti nuous (somatic ) cap i l laries contain numerous pinocytotic ves ic les except in the central nervous system (CNS), where they contain only a limited number of pinocytotic vesicles (a property that is partly responsible for the blood-brain barrier) . (1 ) Continuous capillaries lack fenestrae and have a continuous basal lamina. (2) They are located in nervous tissue, muscle, connective tissue, exocrine glands, and the
lungs. b. Fenestrated (viscera l ) capi l l a ries are formed from endothelial cells that are perforated
with fenestrae . These openings are 60 to 80 nm in diameter and are bridged by a d iaphragm thinner than a cell membrane; in the renal glomerulus, the fenestrae are larger and lack a diaphragm. (1 ) Fenestrated capillaries have a conti nuous basal lamina and few pinocytotic vesicles. (2) They are located in endocrine glands, the intestine, the pancreas, and the glomeruli of
kidneys. c. S inusoidal cap i l l a ries (sinusoids) possess many large fenestrae that lack d iaphragms.
(1 ) Sinusoidal capillaries are 30 to 40 IJ,m in diameter, much larger than continuous and fenestrated capillaries.
(2) Sinusoidal capillaries have a d isconti nuous basal lamina and lack pinocytotic vesicles. (3) Gaps may be present at the cell junctions, permitting leakage between endothelial cells. (4) They are located in the liver, spleen, bone marrow, lymph nodes, and adrenal cortex.
3. Permeabi l ity of cap i l l a ries is dependent on the morphology of their endothelial cells and on the size, charge, and shape of the traversing molecules. Permeability is altered during the inflammatory response by histamine and bradyk in in . a . Some substances d iffuse, whereas others are actively transported across the plasma
membrane of capillary endothelial cells. b. Other substances move across capillary walls via sma l l pores (intercellular junctions) or
large pores (fenestrae and pinocytotic vesicles) . c. Leukocytes leave the bloodstream to enter the tissue spaces by penetrating intercellular
junctions. This process is called d iapedesis. 4. Metabol ic functions of cap i l la ries are carried out by the endothe l ia l cel ls, and include the
following (see Table 1 1 .2) : a. Conversion of inactive angiotensin I to active angiotensin II (especially in the lung) .
This powerful vasoconstrictor also stimulates secretion of aldosterone, a hormone that promotes water retention.
b. Deactivation of various pharmacologically active substances (e.g., bradykinin, serotonin, thrombin, norepinephrine, prostaglandins).
c. B reakdown of l ipoproteins to yield triglycerides and cholesterol. d . Release of prostacycl in , a potent vasodilator and inhibitor of intravascular platelet
aggregation. e. Release of the relaxing factor NO (n itric oxide) and contraction factor ( endothe l i n 1 ) . f . Regulat ion of transendothelial migration o f inflammatory cells (neutroph i ls ) . g . Release of tissue factors responsible for blood coagulation.
5. B lood flow to cap i l lary beds occurs either from metarterioles (with precapillary sphincters) or from termina l arterioles (Figure 1 1 .5) . a. Centra l channels are vessels that traverse a capillary bed and connect arterioles to small
venules. Their proximal portion is the metarterio le (possessing precapillary sphincters), and their distal portion is the thoroughfare channel (with no precapillary sphincter) (see Figure 1 1 .5) .
b. Metarterioles supply blood to the capillary bed, whereas thoroughfare channels receive blood from capillary beds.
6. Arteriovenous shunt (bypassing a cap i l la ry bed) a . Contraction of precap i l l a ry sph incters forces the blood flow from the metarterio le directly
into the thoroughfare channel , thus bypassing the capillary bed and draining into a postcapillary venule.
b. AV anastomoses are small vessels that directly connect arterioles to venules, bypassing the capillary bed. They function in thermoregu lation, especially in the skin where they are abundant. These anastomoses also control blood pressure and flow.
tahir99-VRG & vip.persianss.ir
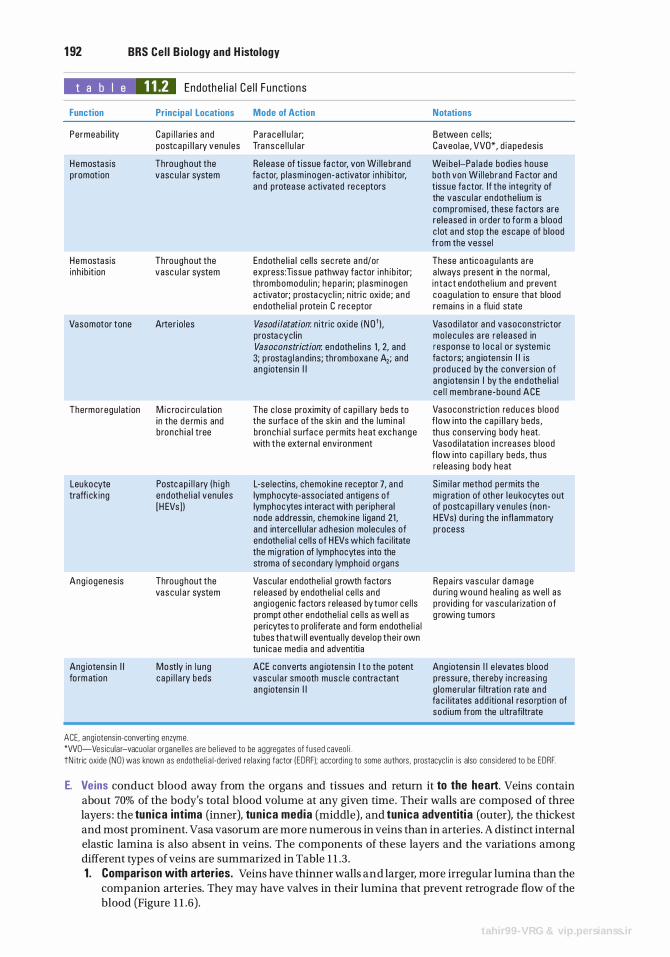
1 92 BRS Cel l B iology and H istology
t a b I e 11.2 Endothe l i a l Ce l l Functions
Function Principal Locations Mode of Action
Permeab i l ity Cap i l l a ri es and Pa ra ce l l u l a r; postcap i l l a ry venu les Transce l l u l a r
Hemostasis Throughout the Re lease of t issue fa ctor, von Wi l l e brand promotion vasc u l a r system fa ctor, p l asm inogen -activator i nh i bitor,
a n d p rotease a ctivated re ceptors
Hemostasis Throughout the Endothe l i a l ce l ls sec rete a nd/or i nh i b it ion vasc u l a r system express: Tissue pathway factor i nh ib itor;
thrombomodu l i n ; h epa rin ; p l asm inogen a ctivator; p rosta cyc l i n ; n itri c oxide ; a nd endothe l i a l p rote in C re ceptor
Vasomotor tone Arte r io les Vasodilatation: n itr ic oxi de ( N O' ) . prosta cyc l in Vasoconstriction: endothe l i ns 1 , 2, and 3; p rostag l a nd ins ; thromboxane A2; and a ng iotens in I I
Thermoregu l at ion M i c roc i r cu lat ion The c lose proxim ity of c ap i l l a ry beds to in the d e rm is and the su rfa c e of the sk in and the l um i na l b ronch i a l tree bronch i a l s u rfa c e perm its heat exc hange
with t he externa l env i ronment
Leukocyte Postc ap i l l a ry ( h i g h L-se lectins, chemokine receptor 7, and traffi ck ing endothe l i a l venu les lymphocyte-assoc iated antigens of
[H EVs ] ) lymphocytes i nteract with per iphera l node add ressin, chemokine l igand 21 , and interce l l u l a r adhesion molecu les of endothe l i a l ce l l s of H EVs which fa c i l itate the mig ration of lymphocytes into the stroma of secondary lymphoid organs
Ang iogenes is Throughout the Vascu la r endothe l i a l g rowth fa ctors vas c u l a r system re leased by endothe l i a l ce l l s and
ang iogen ic factors re leased by tumor ce l l s prompt othe r endothe l i a l ce l l s as we l l as peri cytes to prol ife rate and form endothe l i a l tu bes that wi l l eventua l ly deve lop the i r own tun i cae med ia and adventitia
Ang iotens in I I Mostly in l u ng ACE converts ang iotens in I t o the potent fo rmation c ap i l l a ry beds vasc u l a r smooth musc l e contra ctant
a ng iotens in I I
ACE. ang iotensin-converti ng enzyme. *WO-Vesicu lar-vacuo la r organe l l es a re be l ieved to be aggregates of fused caveo l i .
Notations
B etween ce l ls; Caveo lae , VVO*, d i apedes is
We ibe i-Pa l a de bod ies house both von Wi l l eb rand Fa ctor and tissue fa ctor. I f the integ rity of the vasc u l a r endothe l i um is com promised , these fa ctors are re leased in order to form a b lood c l ot a nd stop the escape of b lood from the vesse l
These anti c oagu l a nts a re a lways p resent in the norma l , i n tact endothe l i um and prevent coagu l at ion to ensure that blood rema ins in a f lu id state
Vasod i l ator a nd vasoconstrictor mo l e cu l e s a re re leased in response to l o c a l o r system i c fa cto rs; a n g iotens i n I I i s prod uced by the convers ion of a ng iotens i n I by the e ndothe l i a l c e l l memb rane -bound ACE
Vasoconstriction reduces b lood f low i nto the cap i l l a ry beds , th us conserv ing body heat. Vasod i l atation i n c reases b lood f low i nto c a p i l l a ry beds , th us re leas ing body heat
S im i l a r method perm its the m ig ration of othe r l e ukocytes out of postc ap i l l a ry venu les ( non -H EVs) d u ri ng the infl ammato ry process
Repa i rs vascu l a r d amage d u ring wound hea l i n g as we l l as p rovid i ng for vascu l a rization of g rowing tumors
Ang iotens in I I e l evates b lood p ressure, thereby i n c reas ing g l omeru l a r fi ltration rate a nd fa c i l itates add iti ona l reso rption of sod i um from the u ltra filtrate
tN itric oxide (NO ) was known as endothe l i a l -derived relaxing factor (EORF); accord ing to some authors, prostacyc l i n is also cons idered to be EDRF.
E. Veins conduct blood away from the organs and tissues and return it to the heart. Veins contain about 70% of the body's total blood volume at any given time. Their walls are composed of three layers : the tun ica intima (inner), tun ica media (middle), and tunica adventitia (outer), the thickest and most prominent. Vasa vasorum are more numerous in veins than in arteries. A distinct internal elastic lamina is also absent in veins. The components of these layers and the variations among different types of veins are summarized in Table 1 1 .3 . 1 . Comparison with arteries. Veins have thinner walls and larger, more irregular lumina than the
companion arteries. They may have valves in their lumina that prevent retrograde flow of the blood (Figure 1 1 .6) .
tahir99-VRG & vip.persianss.ir
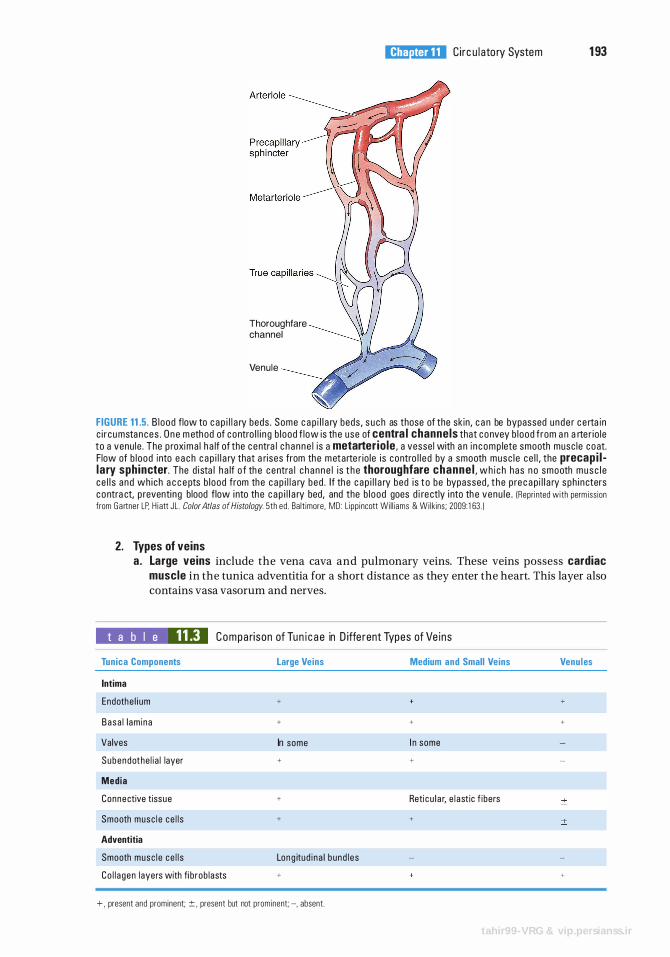
Thoroughfare channel
Venule
l!1lEJ1l!Dij C i rc u l ato ry System 1 93
FIGURE 11.5. B lood flow to c a p i l l a ry beds . Some c a p i l l a ry beds , s u c h as those of the sk in , c a n be bypassed unde r c e rta in c i r cu mstances . O n e m ethod of contro l l i n g b l ood f low is the use of centra l channels that convey b l ood f rom a n a rte r io le to a venu le . The p roxima l h a lf of the centra l c h anne l i s a metarterio le , a vesse l with a n i n comp lete smooth musc le coat. F low of b l ood into e a c h c a p i l l a ry that a rises from the m etarte r io le i s contro l l e d by a smooth musc l e ce l l , the precap i l lary sphincter. The d i sta l h a lf o f th e centra l c h a n n e l i s t h e thoroughfare channe l . w h i c h has n o smooth m u s c l e c e l l s a nd wh ich a c c e pts b l ood from the c a p i l l a ry bed . If the c a p i l l a ry bed i s t o be bypassed , t h e p re c a p i l l a ry sph i n cters c o ntra ct, p reventi ng blood f low i nto the c a p i l l a ry bed, and the b l ood goes d i re ctly i nto th e venu l e . (Repri nted with perm iss ion from Ga rtner LP, H i att JL . Color Atlas of Histology. 5th ed . Ba lt imore. MD: L ipp i ncott Wi l l iams & Wi lkins ; 2009: 1 63 . )
2. Types of veins a . Large veins include the vena cava and pulmonary veins. These veins possess cardiac
muscle in the tunica adventitia for a short distance as they enter the heart. This layer also contains vasa vasorum and nerves.
t a b I e 11.3 Compa ri son of Tun i c a e in D iffe rent Types of Ve ins
Tunica Components
Intima
Endothe l i um
Basa l l am ina
Valves
Subendothe l i a l layer
Media
Connective tissue
Smooth musc l e ce l l s
Adventitia
Smooth musc l e ce l l s
Co l l a gen layers with fi b rob lasts
Large Veins
+
+
In some
+
+
+
Long itud i na l bund l e s
+
+ . present and prominent; ± , present but not prominent; -, absent.
Medium and Small Veins
+
I n some
+
Reti c u l a r, e l astic f ibers
+
Venules
+
+
+
tahir99-VRG & vip.persianss.ir
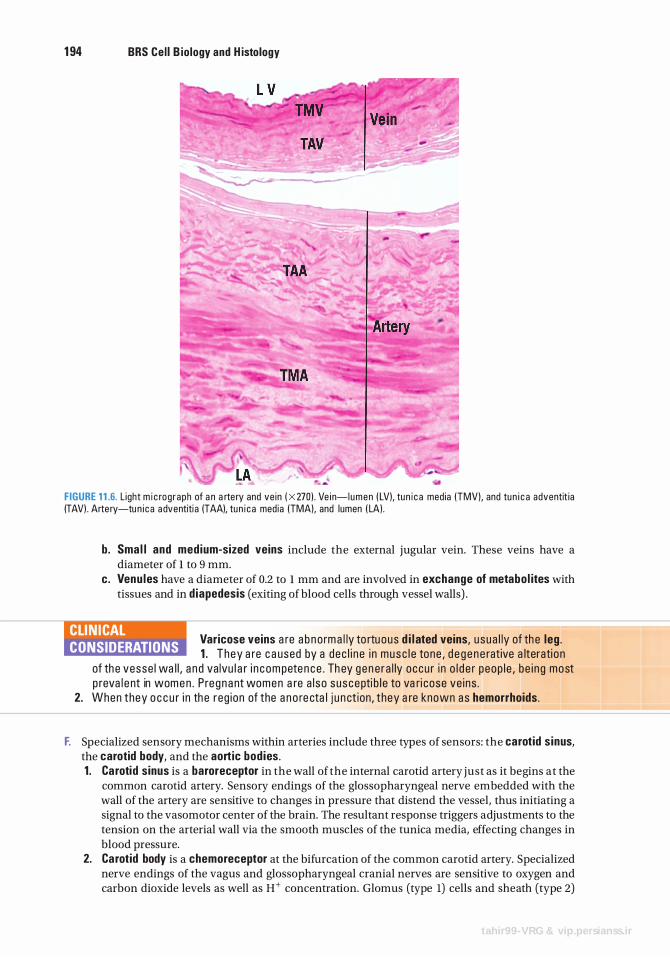
1 94 BRS Cel l B iology and H istology
FIGURE 1 1 .6. L ight m i c rog raph of a n a rte ry and ve in ( X 270l . Ve i n-lumen ( LVI, tun i c a media (TMVI, and tun i c a adventit ia (TAVI . Arte ry-tu n i c a a dventiti a (TAAI, tun i c a media (TMAI. and lumen ( LAI .
b. Sma l l and medium-sized veins include the external jugular vein. These veins have a diameter of l to 9 mm.
c. Venu les have a diameter of 0.2 to l mm and are involved in exchange of metabol ites with tissues and in d iapedesis (exiting of blood cells through vessel walls) .
Varicose veins a re a b no rm a l ly to rtu ous d i l ated veins, usua l ly of th e leg . CLIN ICAL CONSIDERATIONS 1 . They a re c a used by a dec l i n e i n musc l e tone , d e g e n e rative a lterati on
of th e vesse l wa l l , a n d va lvu l a r i n c om peten ce . Th ey g e n e ra l ly occu r i n o l d e r peop l e , be i ng most p reva l e nt in wome n . P re gnant women a re a l so suscepti b l e to va ri cose ve ins .
2. When they o c c u r i n th e reg ion of the a n o re cta l j u n ct ion , they a re known as hemorrhoids.
F. Specialized sensory mechanisms within arteries include three types of sensors: the carotid s inus, the carotid body, and the aortic bodies. 1 . Carotid sinus is a baroreceptor in the wall of the internal carotid artery just as it begins at the
common carotid artery. Sensory endings of the glossopharyngeal nerve embedded with the wall of the artery are sensitive to changes in pressure that distend the vessel, thus initiating a signal to the vasomotor center of the brain. The resultant response triggers adjustments to the tension on the arterial wall via the smooth muscles of the tunica media, effecting changes in blood pressure.
2. Carotid body is a chemoreceptor at the bifurcation of the common carotid artery. Specialized nerve endings of the vagus and glossopharyngeal cranial nerves are sensitive to oxygen and carbon dioxide levels as well as H+ concentration. Glomus (type l) cells and sheath (type 2)
tahir99-VRG & vip.persianss.ir
l!1lEJ1l!Dij Circu l ato ry System 1 95
cells, which envelop the glomus cells, constitute the parenchyma. Nerve endings lose their Schwann cells upon entering the parenchyma, becoming covered instead by sheath cells. Impulses are shuttled to the brain by these two cranial nerves for processing.
3. Aortic bod ies are located in the wall of the arch of the aorta at the junction of the common carotid and subclavian arteries. Their structure and function are similar to those of the carotid body.
4. Hormonal contro l of l ow blood pressure starts with the kidney: a . K idney produces ren in b. Renin cleaves angiotensinogen circulating in the blood, forming angiotensin I , a mild
vasoconstrictor. c. Angiotensin I is converted into ang iotensin II by angiotensin-converting enzyme (ACE),
located on the luminal plasmalemmas of capillary endothelia (especially capillaries of the lungs) .
d . Angiotensin II , a potent vasoconstrictor, causes the walls of arterioles to contract, which raises blood pressure.
e. Antidiuretic hormone, or vasopressin, secreted by the pituitary gland, is another potent vasoconstrictor employed after severe hemorrhage.
This system consists of peripheral lymphatic capillaries, lymphatic vessels of gradually increasing size, and lymphatic ducts. The lymphatic vascular system col lects excess tissue f lu id ( lymph) and returns it to the venous portion of the card iovascular system. I t drains most tissues with the exception of the nervous system and bone marrow.
A. Lymphatic capi l laries are thin-walled vessels that begin as b l ind-ended channels (e.g., lacteals) adjacent to capillary beds where they collect lymph. 1. They are composed of a single layer of attenuated endothe l ia l cel ls that lack fenestrae and
fasciae occludentes. They possess a sparse basal lamina. 2. Lymph enters these leaky capillaries via spaces between overlapping endothelial cells. 3. Small lymphatic anchoring filaments between the surrounding connective tissue and the
abluminal plasma membrane assist in maintaining luminal patency in these delicate vessels.
B. Large lymphatic vesse ls possess valves and are similar in structure to small veins, except that they have larger lumina and thinner walls . 1 . Lymph nodes that filter the lymph are interposed along their routes. 2. These vessels converge to form the thoracic duct and r ight lymphatic duct. The thoracic
duct empties into the venous system at the junction of the left internal jugular vein with the subclavian vein, whereas the right lymphatic duct empties into the venous system at a similar location on the right side of the neck.
CLIN ICAL CONSIDERATIONS
Edema is a patho l og i c p rocess resu lti ng i n a n i ncreased volume o f tissue f lu id .
Edema may be caused by venous obstructi on o r d e c reased venous b lood f low ( a s i n c o ngestive h e a rt fa i l u re ) , i n c reased c a p i l l a ry p e rm e a b i l ity ( d u e to i nj u ry), sta rvati on , excess ive re l ease of h i sta m ine , a n d obstruction of lym ph ati c vesse ls . It i s c ommon d u ri ng p re g n a n cy a n d in o l d e r p e rsons . Edema that is responsive to l o c a l i zed pressure ( i . e . , d e p ress ions p e rs ist afte r re l ease of p ressure ) i s ca l l ed p itt ing edema . Edema can be a sym ptom of a ser ious u n d e rlyi n g d iso rd e r, i n c l u d i n g h e a rt d i sease ; l i ver d isease ; o r d i seases of th e thyro i d , lym phati c system, o r th e k i dn eys, with se r i ous consequen ces .
tahir99-VRG & vip.persianss.ir
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1 . The epicardium is one of the three layers of the heart. It is
(A) continuous with the endocardium. (B ) also known as the visceral pericardium. (C) composed of modified cardiac muscle
cells. (D ) capable of increasing intraventricular
pressure. (E) capable of decreasing the rate of
contraction.
2. The atrial muscle of the heart produces a hormone that
(A) decreases blood pressure. (B ) increases blood pressure. (C) causes vasoconstriction. (D) facilitates the release of renin. (E) facilitates sodium resorption in the
kidneys.
3. The generation of impulses in the normal heart is the responsibility of which of the following structures?
(A) Atrioventricular (AV) node (B) AV bundle of His (C) Sympathetic nerves (D ) Sinoatrial (SA) node (E) Purkinje fibers
4. Metarterioles, vessels interposed between arterioles and capillary beds,
(A) function to control blood flow into arterioles.
(B ) possess a complete layer of smooth muscle cells in their tunica media.
(C) possess precapillary sphincters. (D ) receive blood from thoroughfare channels. (E) possess valves to regulate the direction of
blood flow.
1 96
5. Which of the following statements concerning innervation of blood vessels is true?
(A) Vasoconstriction is controlled by parasympathetic nerve fibers.
(B ) Acetylcholine acts directly on smooth muscle cells.
(C) Acetylcholine acts directly on endothelial cells.
(D ) Vasodilation is controlled by sympathetic nerve fibers.
(E) Nitric oxide acts as a vasoconstrictor.
6. Which of the following characteristics distinguishes somatic capillaries from visceral capillaries?
(A) Presence or absence of fenestrae (B ) Size of the lumen (C ) Thickness of the vessel wall (D ) Presence or absence ofpericytes (E ) Thickness of the basal lamina
7. The blood-brain barrier is thought to exist because capillaries in the central nervous system have which of the following characteristics?
(A) Discontinuous basal lamina (B ) Fenestrae with diaphragms (C ) Fenestrae without diaphragms (D ) A few pinocytic vesicles (E) No basement membrane
8. Which of the following statements about healthy, intact capillaries is true?
(A) They control blood pressure. (B ) They are lined by a simple columnar
epithelium. (C ) They have a smooth muscle coat. (D ) They inhibit clot formation. (E) Satellite cells share their basal lamina.
tahir99-VRG & vip.persianss.ir
9. A patient complains of shortness of breath even after only mild exercise. She states that she has had this condition for 2 years but recently has noticed that it has become more pronounced. Her medical history indicates that she had rheumatic fever when she was a child. Auscultation indicates an enlarged heart. What may the physician expect to find with other diagnostic tests?
(A) Mitral valve stenosis (B ) Tetralogy of Fallot (C ) Pulmonary artery aneurysm (D ) Coronary heart disease (E) Ischemic heart disease
1 0. Diagnostic tests for ischemic heart disease usually reveal
(A) malformed heart valves. (B) atherosclerosis of coronary arteries. (C) irregular heartbeat. (D ) faulty SA valve. (E ) arteriosclerosis of coronary arteries.
l!iltl'115II C i rc u l ato ry System 1 97
1 1 . Vasa vasorum function in a way that is similar to
(A) AV valves. (B ) semilunar valves. (C) coronary arteries. (D) elastic arteries. (E ) metarterioles.
1 2. Which one of the following possesses a distinct internal elastic lamina?
(A) Capillary (B ) Metarteriole (C) Arteriole (D ) Muscular artery (E ) Vein
1 3. Ischemic heart disease is the usual sequel to
(A) arteriosclerosis. (B ) abdominal aortic aneurysm. (C) rheumatic fever. (D ) varicose veins. (E) atherosclerosis.
tahir99-VRG & vip.persianss.ir
Answers and Explanations
1 . B . The pericardium is a fibroserous sac that encloses the heart. The innermost layer of the pericardium, the epicardium, is also known as the visceral pericardium (see Chapter 1 1 I A 1 ) .
2. A. Atrial natriuretic peptide, which decreases blood pressure, i s produced mainly by cardiac muscle cells of the right atrium. It inhibits the release of renin and causes the kidneys to decrease the resorption of sodium and water (see Chapter 1 1 I A 1 b) .
3. D . Impulses are generated in the sinoatrial node, which is the pacemaker of the heart. They are then conducted to the AV node. The bundle of His and Purkinje fibers conduct impulses from the AV node to the cardiac muscle cells of the ventricles. Sympathetic nerves can increase the rate of the heartbeat but do not originate it (see Chapter 1 1 I A 4 a).
4. C. The proximal portion of a central channel is known as a metarteriole, whereas its distal portion is the thoroughfare channel. Blood from metarterioles may enter the capillary bed if their precapillary sphincters are relaxed. If the precapillary sphincters of metarterioles are constricted, blood bypasses the capillary bed and flows directly into thoroughfare channels and from there into a venule (see Chapter 11 I B 1 d).
5. C. Acetylcholine stimulates the endothelial cells of a vessel to release nitric oxide (EDRF), which causes relaxation of smooth muscle cells. Thus, acetylcholine does not act directly on smooth muscle cells (see Chapter 1 1 I B 2) .
6. A. Somatic (continuous) capillaries lack fenestrae, whereas visceral (fenestrated) capillaries are characterized by their presence. Both types of capillary possess a continuous basal lamina and are surrounded by occasional pericytes (see Chapter 1 1 I C 2) .
7 . D . Capillaries in the CNS are of the continuous type and thus lack fenestrae but have a continuous basal lamina. In contrast to continuous capillaries in other parts of the body, they contain only a few pinocytic vesicles; this characteristic is thought to be partly responsible for the blood-brain barrier (see Chapter 1 1 I C 2) .
8. D. The smooth endothelial lining of intact, healthy capillaries inhibits clot formation. Capillaries do not control blood pressure (see Chapter 11 I C 2).
9. A. A person who has had rheumatic fever as a child may develop heart valve disease later in life. Although the mitral valve is the one most commonly affected, the other valves may also be involved. The mitral valve becomes inflamed, fibrotic, and eventually incompetent or stenotic. This condition leads to respiratory hypertension and edema, which restricts respiratory function. The key is a history of rheumatic fever, because those individuals are predisposed to developing heart valve diseases (see Chapter 1 1 I A 3 Clinical Considerations).
1 0. B . Diagnostic tests for ischemic heart disease reveal atherosclerosis of the coronary vessels. Over time, excessive plaque composed of cholesterol and fats is layered beneath the intima of these vessels, thus restricting blood flow to the myocardium of the heart, leading to angina pectoris, an infarction, or perhaps sudden death (see Chapter 1 1 I B 1 Clinical Considerations).
1 1 . C. Vasa vasorum are the small blood vessels that serve the walls of elastic and muscular arteries with oxygen and nutrients just as the coronary arteries provide for the walls of the heart (see Chapter 11 I B 1).
1 2. D . The muscular artery possesses a distinct internal elastic lamina. Elastic arteries possess an incomplete internal elastic lamina, whereas capillaries, arterioles, metarterioles, and veins do not possess an internal elastic lamina (see Table 1 1 . 1 and Chapter 1 1 I D) .
1 3. E. Ischemic heart disease is usually caused by coronary atherosclerosis, resulting in decreased blood flow to the myocardium. It may develop into angina pectoris, myocardial infarction, chronic ischemic cardiopathy, or sudden cardiac death. On the other hand, arteriosclerosis (hardening ofthe arteries) usually attacks renal arteries and is related to hypertension and diabetes mellitus (see Chapter 1 1 I B Clinical Considerations) .
1 98
tahir99-VRG & vip.persianss.ir
Lymphoid Tissue
I. OVERVIEW-THE LYMPHOID (IMMUNE) SYSTEM
A. The lymphoid system consists of capsulated lymphoid tissues (thymus, spleen, tonsils, and lymph nodes); diffuse lymphoid tissue; and lymphoid cells, primarily T lymphocytes (T cells), B lymphocytes (B cells), and macrophages. Capsulated lymphoid organs are of two types, primary lymphoid organs that "educate" lymphocytes so that they become immunocompetent cells; these are the bone marrow (discussed in Chapter 10 Section IV) and the thymus (discussed in this chapter, Section VI B). Secondary lymphoid organs sequester immunogens and allow immunocompetent cells and antigenpresenting cells (APCs) to interact with the immunogens and with each other to initiate an immune reaction and eliminate the antigenic attack. The d iffuse lymphoid tissue, lymph nodes, spleen, and tonsils are the secondary lymphoid organs and are discussed in Section VI of this chapter.
B. The immune system has two components : the innate immune system (nonspecific) and the adaptive immune system (specific) . 1 . The i nnate immune system has no immunological memory; it acts rapidly, but in a nonspecific
manner. Its chief constituents are complement proteins, toll-like receptors (TLRs), mast cells (see Chapter 6 III A 4), eosinophils (see Chapter 10 Table 10 .2), neutrophils (see Chapter 10 Table 10 .2), macro phages (see Chapter 6 III B 1) , and natural killer (NK) cells (see Section I I D) . a. Complement prote ins are blood-borne proteins (C1-C9) that function in nonspecific host
defense and initiate the inflammatory process. b. TLRs in humans are a family of 10 receptors that are integral proteins located either in the cell
membranes or in the membranes of endosomes of specific cells of the innate immune system. (1 ) It is believed that in order to perform their function, they have to pair up with their
counterpart, usually the same TLR (forming homodimers); however, TLR2 can form dimers with TLR1 and TLR6 (forming heterodimers) .
(2) TLRs have key functions in the recognition of repeating molecular patterns that exist in pathogens, known as pathogen-associated molecular patterns (PAMPs).
(3) Each TLR, or TLR pair, recognizes PAMPs that are specific to them (Table 12 . 1 ) . ( 4 ) TLRs 1 , 2 , 4 , 5, 6 , and 10 are integral proteins of the cell membrane and recognize
molecular patterns belonging to bacteria, protozoa, and fungi, whereas TLRs 3, 7, 8, and 9 are integral proteins of endosomal membranes and recognize molecular patterns belonging to nucleic acids of viruses (and some other microorganisms) .
(5) For instance, TLR4 recognizes lipopolysaccharides of gram-negative bacteria, and TLR2 recognizes peptidoglycan of gram-positive bacteria. Once these receptors bind to their ligand, they cause the release of tumor necrosis factor a (TNF-a), inter leukins 1 and 1 2 ( I L-1 and IL-12), and other systemic inflammation-inducing cytokines.
1 99
tahir99-VRG & vip.persianss.ir
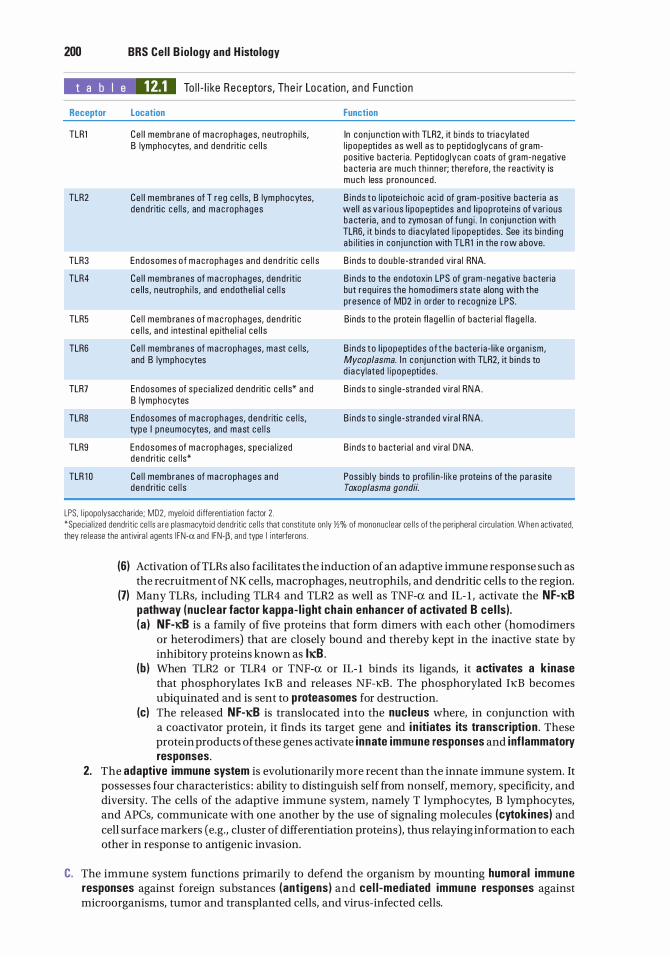
200 BRS Cel l B iology and H istology
t a b I e 12.1 To l l - l i ke Receptors, The i r Loc at ion, a n d Fun cti on
Receptor
TLRl
TLR2
TLR3
TLR4
TLR5
TLR6
TLR7
TLR8
TLR9
TLR 1 0
Location
Ce l l membrane of m a c rophages, neutro ph i ls , B lymphocytes, and dend ritic ce l l s
Ce l l membranes of T reg ce l ls, B lym phocytes, dend riti c c e l l s , and m a c rophages
Endosomes o f m a c rophages a nd dend ritic ce l l s
Ce l l membra nes of m a c rophages, dend ritic c e l ls , ne utroph i ls , and endothe l i a l c e l l s
Ce l l membranes o f m a c rophages, dend riti c c e l ls, and intesti n a l ep ithe l i a l ce l l s
Ce l l membranes of mac rophages, mast c e l ls , and B lymphocytes
Endosomes of spec i a l i zed dend riti c ce l l s* a nd B lymphocytes
Endosomes of m a c rophages, d e nd riti c c e l ls , type I pneumocytes, and mast ce l l s
Endosomes of m a c rophages, spec i a l ized d end ritic c e l ls*
Ce l l membranes of mac rophages a nd dend riti c ce l l s
Function
In conj u n ction with TLR2, it b inds to tri a cylated l i popepti des as we l l a s to pepti dog lycans of g rampos itive bacter ia . Peptidog lycan coats of g ram-negative ba cter ia a re much th inner; the refo re, the rea ctivity is much less p ronounced .
B i nds to l i pote i cho i c ac i d of g ram-pos itive ba cter ia as we l l as va r i ous l i popeptides a nd l i pop rote i ns of var ious ba cter ia , a n d to zymosan of fung i . I n conj u n ct ion with TLR6, it b inds to d i a cylated l i popepti des . See its b i nd i ng ab i l it ies in conj unction with TLRl i n the row above.
B i nds to doub l e -stra nded v i ra l RNA.
B i nds to the endotoxin LPS of g ram-negative ba cteria but requ i res the homod ime rs state along with the presence of MD2 i n order to recognize LPS.
B inds to the p rote in fl age l l i n of bacte r ia l fl a ge l l a .
B i nds to l i popeptides o f t he bacter ia- l ike organ ism, Mycoplasma. I n conj u n ction with TLR2, it b i nds to d i a cylated l i popeptides .
B i nds to s i ng l e -stra nded v i ra l RNA.
B i nds to s i ng l e -stra nded v i ra l RNA.
B i nds to bacteri a l a n d v i ra l D NA.
Possib ly b inds to p rofi l i n - l i ke p rote ins of the pa ras ite Toxoplasma gondii.
LPS. l i popo lysaccharide; MD2 . mye lo id d ifferentiation factor 2 . *Spec ia l ized dendrit ic ce l l s a r e p lasmacyto id dendritic ce l l s that constitute on ly Yl% of mononuc lear ce l l s of t he per iphera l c i rcu lat ion . When activated, they re l ease the antivira l agents I FN-a and IFN-P. and type I i nterferons .
(6) Activation ofTLRs also facilitates the induction of an adaptive immune response such as the recruitment of NK cells, macrophages, neutrophils, and dendritic cells to the region.
(7) Many TLRs, including TLR4 and TLR2 as well as TNF-a and IL- l , activate the Nf-JCB pathway (nuc lear factor kappa- l ight cha in enhancer of activated B cel ls) . (a ) Nf-KB is a family of five proteins that form dimers with each other (homodimers
or heterodimers) that are closely bound and thereby kept in the inactive state by inhibitory proteins known as IJCB .
(b ) When TLR2 or TLR4 or TNF-a or IL- l binds its ligands, it activates a k inase that phosphorylates IKB and releases NF-KB . The phosphorylated IKB becomes ubiquinated and is sent to proteasomes for destruction.
(c) The released Nf-JCB is translocated into the nucleus where, in conjunction with a coactivator protein, it finds its target gene and i n itiates its transcription . These protein products of these genes activate innate immune responses and i nflammatory responses.
2. The adaptive immune system is evolutionarily more recent than the innate immune system. It possesses four characteristics : ability to distinguish self from nonself, memory, specificity, and diversity. The cells of the adaptive immune system, namely T lymphocytes, B lymphocytes, and APCs, communicate with one another by the use of signaling molecules (cytokines) and cell surface markers (e.g., cluster of differentiation proteins), thus relaying information to each other in response to antigenic invasion.
C. The immune system functions primarily to defend the organism by mounting humoral immune responses against foreign substances (ant igens) and cel l -mediated immune responses against microorganisms, tumor and transplanted cells, and virus-infected cells.
I!1Jllt!llllij Lympho id Tissue 201
CLIN ICAL CONSIDERATIONS
I n d iv id ua l s may suffe r from congenita l immunodefic iency d isorders, usua l ly a rec ess ive X- l i nked g e n eti c d efect that affe cts ma l e s to a m u c h
g reater extent tha n fe ma les . T h e most c o m m o n sym ptoms a re re c u rrent resp i rato ry infecti ons that h ave a te n den cy to p rog ress to p neumon i a . Add iti o n a l i n d i c ators a re m u lti p l e sk in and ora l i nfecti ons, s u c h a s yeast i nfecti ons of the mouth (th rush ) o r of the va g i n a . I n some c ases, s u c h a s X-l i nked agammag lobu l i nemia, B lymphocytes do not d eve lop , resu lti n g i n s c a rc ity of p l a sma ce l l s a n d consequently l a c k o f immunog l o bu l i n p ro d u cti on .
A. Overview-Cel ls o f the immune system: T lymphocytes, B lymphocytes, and APCs 1. Cells of the immune system include c lones of T lymphocytes (T cel ls) and B lymphocytes
(B cel ls) . A clone is a small number of ident ical cells that can recognize and respond to a single or a small group of related antigenic determinants known as epitopes. a. An epitope is that small portion of an antigen to which an antibody ( immunog lobu l in ) binds.
A single antigen may have a number of epitopes, each different, recognized by different antibodies each of which is specific to each of those epitopes.
b. The region of the antibody that binds to an epitope is known as a paratope . c . I t is important to realize that, instead of recognizing antigens, antibodies recognize those
portions of antigens that act as epitopes. Exposure to antigen and one or more cytokines induce activation of rest ing T and B cel ls, leading to their proliferation and differentiation into effector ce l ls (Figure 12 . 1 ) . Both B cells and T cells arise in the bone marrow, T cells leave the bone marrow to mature in the thymus, whereas B cells remain in and mature in the bone marrow.
2. APCs (e.g., macrophages, lymphoid dendritic cells, Langerhans cells, follicular dendritic cells, M cells, and B cells), mast cel ls, and granu locytes are also cells of the immune system (see Chapter 6 III A and B) _ i
B. T lymphocytes 1 . Overview-T lymphocytes
a . T lymphocytes include several functionally distinct subtypes and are responsible for cel l -med iated immune responses. They assist B cells in developing humoral responses to thymic-dependent antigens.
b . T-ce l l receptors (TCRs) are heterodimers, that is, they are composed of two dissimilar protein chains: a and � or y and o. TCRs are present only on the surfaces of T lymphocytes and are always associated with a CD3 molecule; although they belong to the Ig (immunoglobulin) superfamily unlike Igs, they are not secreted. TCRs recognize only protein antigens. (1 ) y/o T ce l ls are more uniform, are much fewer in number, do not form memory T cells,
and are usually located in the intestinal mucosa; they react to antigens that are indicative of microbial assault.
(2) a/� T cel ls constitute the bulk of the T-cell population, form memory T cells, and, although they react slower than y/o T cells, they are responsible for most T-cell responses.
c. It is important to realize that T cells do not recognize antigens; instead they recognize only ep itopes that are bound to major h istocompatib i l ity complex (MHC) molecules on the surface of APCs. Since T cells require that the epitopes be presented in conjunction with MHC molecules, they are said to be MHC restricted (see Section III of this chapter) .
2. Maturati on of a/� T ce l ls, y/o T ce l ls, and NKT ce l ls occurs in the thymus. Only a/� T ce l l s spend a considerable time in the thymus and they go through a series of steps in their "education" to become immunocompetent cells. Although y/o T ce l ls and NKT ce l ls also
1 Although B cells can presents epitopes to T cells and are thus antigen-presenting cells, their role in this function
is probably limited to the secondary (anamnestic) immune response rather than the primary immune response.
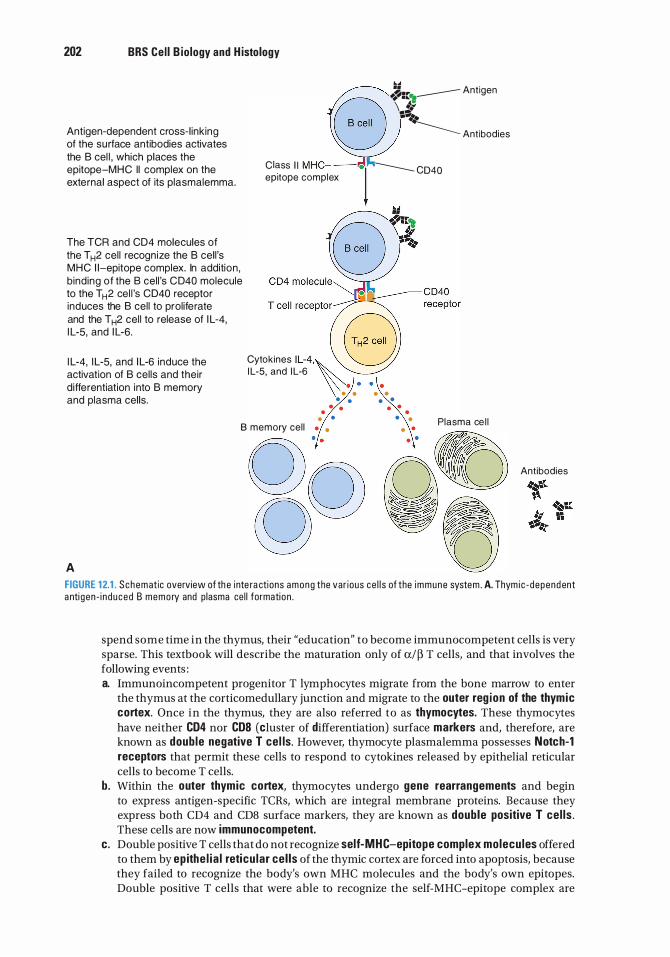
202 BRS Cel l B iology and H istology
Antigen-dependent cross- l ink ing of the surface antibodies activates the B cel l , which places the epitope-MHC II complex on the external aspect of its plasmalemma.
The TCR and CD4 molecules of the T H2 cel l recognize the B cel l 's MHC 1 1-epitope complex. In addition , b ind ing of the B cel l 's CD40 molecule to the T H2 cel l 's CD40 receptor induces the B cel l to prol iferate and the TH2 cel l to release of I L-4, I L-5, and I L-6.
I L-4, I L-5, and I L-6 induce the activation of B cel ls and their d ifferentiation into B memory and plasma cells.
••
B •l':::�--- Antigen
\ J.-�� . ....
--------- Antibodies
Class I I M HC- -- .1 ---... C040 ep1tope complex
Cytokines I L-4,\';8 I L-5, and I L-6
• • • • • • • •
• • • • . . . . • •
• • • • PI I I B memory cel l • • • •
asma ce
Q(y OftJ g0 we A
Antibodies
FIGURE 12.1 . S chematic overview of th e inte ra ctions among the var ious ce l l s of the immune system . A. Thym ic - depend ent a nti gen - i n duced B memory and p lasma ce l l formati on .
spend some time in the thymus, their "education" to become immunocompetent cells is very sparse. This textbook will describe the maturation only of a/� T cells, and that involves the following events : a. Immunoincompetent progenitor T lymphocytes migrate from the bone marrow to enter
the thymus at the corticomedullary junction and migrate to the outer reg ion of the thymic cortex. Once in the thymus, they are also referred to as thymocytes. These thymocytes have neither CD4 nor COB (cluster of differentiation) surface markers and, therefore, are known as double negative T cel ls. However, thymocyte plasmalemma possesses Notch-1 receptors that permit these cells to respond to cytokines released by epithelial reticular cells to become T cells.
b. Within the outer thymic cortex, thymocytes undergo gene rearrangements and begin to express antigen-specific TCRs, which are integral membrane proteins. Because they express both CD4 and CDS surface markers, they are known as double positive T ce l ls . These cells are now immunocompetent.
c . Double positive T cells that do not recognize self-MHC-epitope complex molecu les offered to them by ep ithe l ia l reticu lar cel ls of the thymic cortex are forced into apoptosis, because they failed to recognize the body's own MHC molecules and the body's own epitopes. Double positive T cells that were able to recognize the self-MHC-epitope complex are
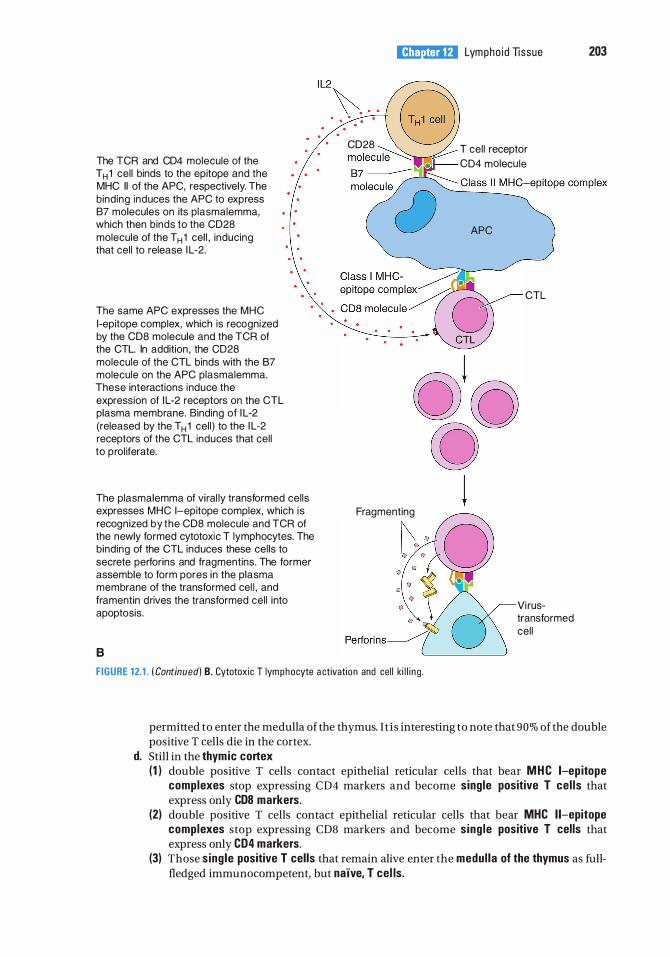
The TCR and CD4 molecule of the T H 1 cel l binds to the epitope and the MHC II of the APC, respectively. The binding induces the APC to express 87 molecules on its plasmalemma, which then binds to the CD2S molecule of the T H 1 cel l , inducing that cel l to release I L-2.
The same APC expresses the MHC 1 -epitope complex, which is recognized by the CDS molecule and the TCR of the CTL. In addition , the CD2S molecule of the CTL binds with the 87 molecule on the APC plasmalemma. These interactions i nduce the expression of I L-2 receptors on the CTL plasma membrane. Binding of I L-2 (released by the T H 1 cel l) to the I L-2 receptors of the CTL induces that cel l to prol iferate.
The plasmalemma of vi ral ly transformed cel ls expresses MHC 1-epitope complex, which is recognized by the CDS molecule and TCR of the newly formed cytotoxic T lymphocytes. The binding of the CTL induces these cel ls to secrete perforins and fragmentins. The former assemble to form pores in the plasma membrane of the transformed cel l , and framentin drives the transformed cel l into apoptosis.
8
I!1Jllt!llllij Lympho i d Tissue 203
8 CD2S � T cel l receptor molecu le .� CD4 molecu le
APC
Fragmenting
CTL
Vi rustransformed cel l
FIGURE 12.1 . ( Continued) B. Cytotox ic T lym p h ocyte a ctivation and ce l l ki l l i n g .
permitted to enter the medulla of the thymus. I t is interesting to note that 90% of the double positive T cells die in the cortex.
d. Still in the thymic cortex (1 ) double positive T cells contact epithelial reticular cells that bear MHC 1-ep itope
complexes stop expressing CD4 markers and become single positive T ce l ls that express only CDS markers.
(2) double positive T cells contact epithelial reticular cells that bear MHC 1 1-epitope complexes stop expressing CD8 markers and become s ing le positive T cells that express only CD4 markers.
(3) Those s ing le positive T cells that remain alive enter the medul la of the thymus as fullfledged immunocompetent, but na"ive, T cel ls.
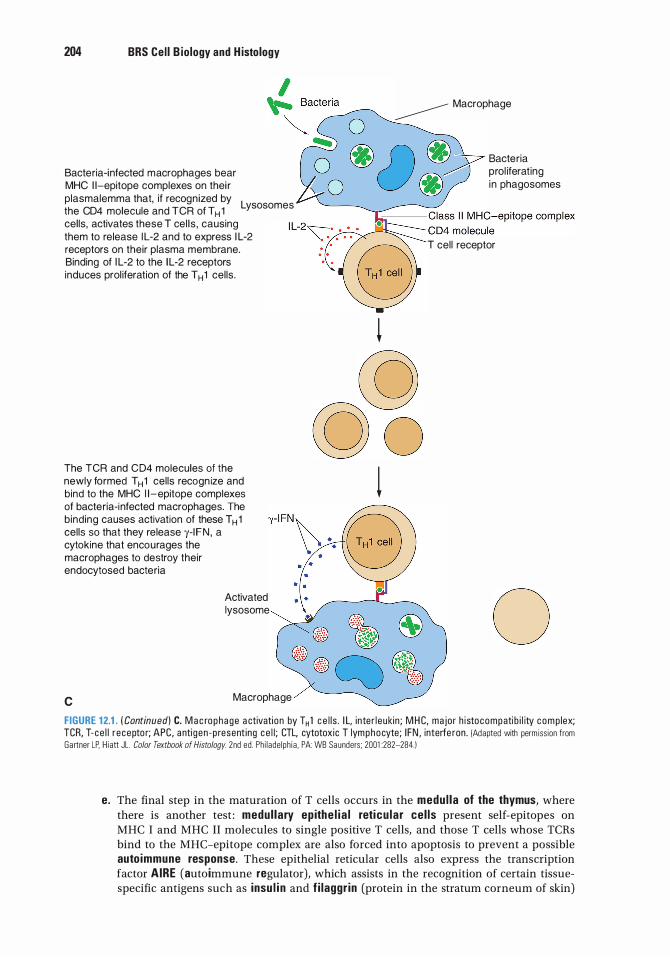
204 BRS Cel l B iology and H istology
Bacteria-infected macrophages bear MHC 1 1-epitope complexes on thei r plasmalemma that, if recognized by
L the CD4 molecule and TCR of T H 1
ysosomes
cel ls, activates these T cel ls , causing them to release I L-2 and to express I L-2 receptors on their plasma membrane. Binding of I L-2 to the I L-2 receptors induces prol iferation of the T H 1 cel ls.
The TCR and CD4 molecules of the newly formed T H 1 cel ls recogn ize and bind to the MHC 1 1-epitope complexes of bacteria-i nfected macrophages. The b ind ing causes activation of these T H 1 cel ls so that they release y- I FN , a cytokine that encourages the macrophages to destroy their endocytosed bacteria
c
Activated lysosome
Macrophage
� Macrophage
� cg © o
l
Bacteria prol iferat ing i n phagosomes
T cel l receptor
0 FIGURE 12.1 . ( Continued) C. M a c ro p h a g e a ctivation by T H 1 c e l l s . I L, i nte r l eukin ; M H C, ma jor h istocompati b i l ity c o m p lex; TCR, T- ce l l r ecepto r; APC, a nti gen -p resent ing c e l l ; CTL, cytotoxic T lymphocyte; I FN , interfe ron . (Adapted with perm iss ion from Gartner LP. Hiatt JL. Color Textbook of Histology. 2nd ed . Ph i lade lph ia , PA: WB Saunders ; 2001 :282-284.1
e. The final step in the maturation of T cells occurs in the medu l la of the thymus, where there is another test : medul lary ep ithe l i a l reticu lar ce l ls present self-epitopes on MHC I and MHC II molecules to single positive T cells, and those T cells whose TCRs bind to the MHC-epitope complex are also forced into apoptosis to prevent a possible auto immune response. These epithelial reticular cells also express the transcription factor AIRE (auto immune regulator) , which assists in the recognition of certain tissuespecific antigens such as insu l i n and f i laggr in (protein in the stratum corneum of skin)
I!1Jllt!llllij Lympho id Tissue 205
(see Chapter 14 Section II B 2 c), and force T cells that would be triggered by these proteins to initiate an immune response into apoptosis.
f. The T cells that survive this final test are permitted to leave the thymic medulla to be distributed by the circulatory system to various regions of the body.
g. The entire process of T cell development is directed by a variety of growth factors and signa l i ng molecules released by the various types of epithe l ia l reticu lar ce l ls of the thymus.
3. T lymphocyte subtypes. There are three types of T cells : na'ive, memory, and effector T cells. Some have a number of subtypes. a. Naive T cells are immunologically competent cells that have not as yet been activated (i .e. ,
they have not come into contact with their designated antigen outside the thymic cortex), but possess CD45RA surface markers. Once activated, they undergo cell division and form both memory T cells and effector T cells.
b. Memory T cel ls, derived from naive T cells, possess CD45RO surface molecules. There are two classes of these cells, central memory T cells (CR7 + ) and effector memory T cells (CR7-). (1 ) Central memory T cells (TCMs) reside in the para cortex of lymph nodes. If they interact
with an epitope that they recognize when APCs present it to them, they cause the APC to release IL- 12, which induces TCMs to undergo cell division, and the newly formed cells differentiate into effector T memory cells.
(2) Effector T memory cells migrate to inflammatory sites, where they undergo cell division and form effector T cel ls.
c . Effector T ce l ls are derived from effector T memory cells and are capable of initiating an immune response. The subtypes of effector T cells are T helper cells, cytotoxic T lymphocytes (CTLs, T killer cells), and regulatory T cells (T reg cells) . (1 ) T he lper cel ls (THO, TH1 , T H2, Tl7, and THa�) are CD4+ cells. After activation, these cells
synthesize and release numerous growth factors known as cytokines ( lymphokines). THO ce l ls differentiate into the other four types of T helper cells. (a) T H 1 ce l ls regulate responses against viral or bacterial invasions and instruct
macro phages in killing bacteria. (b ) T H2 ce l ls regulate humoral responses against parasitic or mucosal attacks by
stimulating B cells to produce antibodies. (c) T1 7 cel ls manufacture and release IL- 17, which recruits neutrophils and enhances
their bactericidal activities. (d) T Ha� ce l ls are activated by IL- 10 as well as interferon a or � (INF-a or INF-�) to act
against viruses. (e) The cytokines I L-4, I L-5, and I L-6 released by T H2 cells induce B cells to proliferate
and mature and thus respond to an antigenic stimulus, whereas I L- 10 inhibits the formation ofT H 1 cells, I L-9 enhances the proliferation ofT H2 cells as well as mast cell responses, and IL- 13 retards TH1 cell development and induces the development of B cells.
(f) Other cytokines produced by TH1 cells, such as IL-2, IFN-y, and others, modulate the immune response in diverse ways (Table 12.2) . Macrophages synthesize and release IL- 12, which restricts the development of TH2 cells and encourages the formation ofTH1 cells.
CLIN ICAL CONSIDERATIONS
Acqu i red immunodefic iency syndrome (AIDS) i s c a used by i nfecti on with human immunodeficiency vi rus, wh i c h p refe renti a l ly invades TH c e l ls ,
c a us i ng a severe d e press ion i n th e i r n u m b e r and th us suppressing both cel l-mediated and humoral immune responses.
1. A I D S is c h a ra cte r ized by secondary infections by oppo rtun isti c m i c roo rg a n isms that c ause p neumon i a , toxo p l asmosis , c a n d i d i a s is, a n d oth e r d iseases .
2 . It is a l so c h a ra cte r ized by the deve l o pment of c e rta i n ma l i g n a n c i es, such a s Kaposi sarcoma and non-Hodgkin lymphoma.
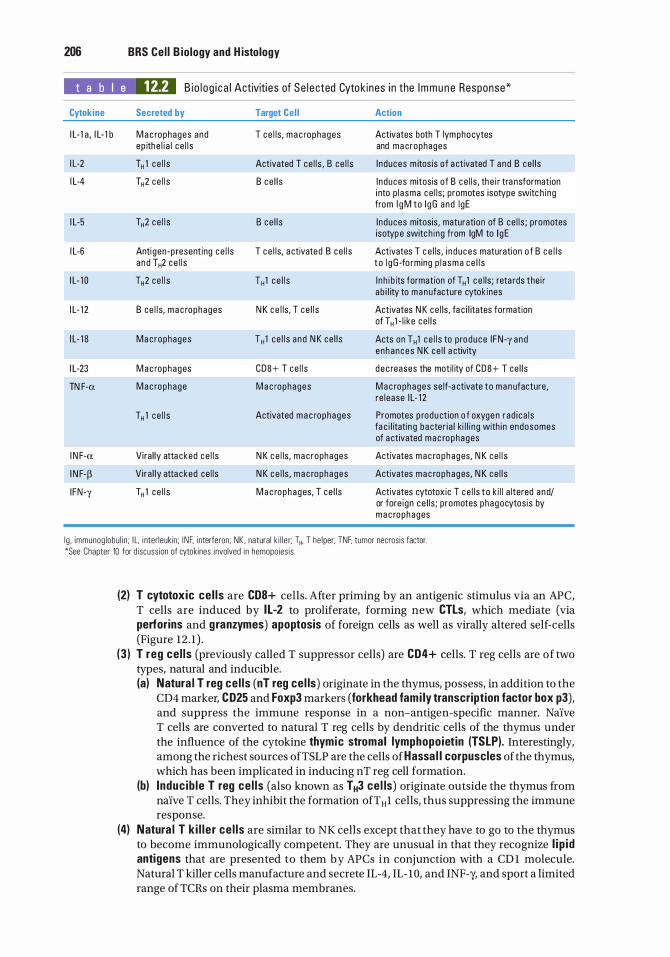
206 BRS Cel l B iology and H istology
t a b I e 12.2 B i o l o g i c a l Activiti es of Se l e cted Cytok ines i n the Immune Response*
Cytokine Secreted by
I L- 1 a , I L- 1 b M a c rophages and ep ithe l i a l ce l l s
I L-2 T" 1 ce l l s
I L-4 T"2 ce l l s
I L-5 T"2 ce l l s
I L-6 Anti gen -p resent ing ce l l s a nd T"2 ce l l s
I L- 1 0 T"2 ce l l s
I L- 1 2 B ce l l s, m a c rophages
I L- 1 S Ma crophages
I L-23 M a c rophages
TN F-a Mac rophage
T" 1 ce l l s
I N F-a Vira l ly atta cked ce l l s
I N F-p V i ra l ly atta cked ce l l s
I FN-y T" 1 ce l l s
Target Cel l
T ce l ls , m a c rophages
Activated T ce l l s , B ce l l s
B ce l l s
B ce l l s
T ce l ls, a ctivated B ce l l s
T" 1 ce l l s
N K c e l ls , T ce l l s
T" 1 ce l l s a nd N K ce l l s
CDS+ T ce l l s
M a c rophages
Activated m a c rophages
N K c e l ls , ma crophages
N K c e l ls , m a c rophages
M a c rophages, T ce l l s
Action
Activates both T lymphocytes and ma crophages
I nduces m itos is o f a ctivated T a nd B ce l l s
I nduces mitosis of B c e l ls , th e i r tra nsformation i nto p l asma ce l ls ; promotes isotype switc h ing from l g M to l gG a nd l gE
I nduces mitosis, maturation of B ce l l s ; promotes isotyp e switc h ing from lgM to l g E
Activates T c e l ls , i n duces maturation o f B c e l l s t o l g G -fo rming p l a sma c e l l s
I n h i b its formation of T" 1 c e l ls ; reta rds the i r ab i l ity to manufacture cytok ines
Activates N K ce l ls, fa c i l itates formation of T" 1 - l i ke ce l l s
Acts on T" 1 ce l l s to p roduce I FN-y and enhances N K ce l l a ctivity
d e c reases the moti l ity of CDS+ T ce l l s
Mac rophages se lf-a ctivate to manufacture, re lease I L- 1 2
Promotes p rodu ct ion o f oxyge n rad i ca l s fa c i l itatin g ba cter i a l ki l l i ng with i n endosomes of a ctivated m a c rophages
Activates mac rophages, N K ce l l s
Activates m a c rophages, N K ce l l s
Activates cytotoxic T ce l l s to k i l l a ltered a nd/ or fore i gn ce l ls ; promotes phagocytosis by m a c rophages
l g , immunog lobu l i n ; I L. i nter leukin ; I N F. i nterferon; NK . natural k i l l e r; T", T he lper; TNF, tumor necrosis factor. *See Chapter 10 for d iscuss ion of cytokines i nvolved in hemopoies is .
(2) T cytotoxic ce l ls are CDS+ cells. After priming by an antigenic stimulus via an APC, T cells are induced by IL-2 to proliferate, forming new CTLs, which mediate (via perforins and granzymes) apoptosis of foreign cells as well as virally altered self-cells (Figure 12 . 1 ) .
(3 ) T reg ce l ls (previously called T suppressor cells) are CD4+ cells. T reg cells are of two types, natural and inducible. (a) Natura l T reg ce l ls (nT reg cel ls) originate in the thymus, possess, in addition to the
CD4 marker, CD25 and Foxp3 markers (forkhead fami ly transcription factor box p3), and suppress the immune response in a non-antigen-specific manner. Naive T cells are converted to natural T reg cells by dendritic cells of the thymus under the influence of the cytokine thymic stromal lymphopoietin (TSLP). Interestingly, among the richest sources ofTSLP are the cells of Hassa l l corpuscles of the thymus, which has been implicated in inducing nT reg cell formation.
(b) Induc ib le T reg ce l ls (also known as T H3 ce l ls) originate outside the thymus from naive T cells. They inhibit the formation ofTH1 cells, thus suppressing the immune response.
(4) Natura l T k i l l e r ce l ls are similar to NK cells except that they have to go to the thymus to become immunologically competent. They are unusual in that they recognize l i p id antigens that are presented to them by APCs in conjunction with a CD 1 molecule. Natural T killer cells manufacture and secrete IL-4, IL- 10, and INF-y, and sport a limited range of TCRs on their plasma membranes.
C. B lymphocytes 1 . Overview-B lymphocytes
I!1Jllt!llllij Lympho i d Tissue 207
a. B lymphocytes originate and mature into immunocompetent cells within the bone marrow. They are responsible for the humoral immune response. These cells go through a series of developmental steps going from pre-B cells through immature and finally transitional B cel ls, where they express different light and heavy chains of immunoglobulins on their cell membranes. Transitional B cells travel to the spleen where they either d ie or undergo f ina l maturation and become mature B cells.
b. Mature B ce l ls express immunoglobulins IgD and the monomeric form of IgM on the external aspect of their plasma membranes (known as surface immunog lobul ins [slgs]); all of the immunoglobulin molecules on a particular B cell recognize and bind to the same antigenic determ inant (epitope) . There are several types ofB cells, but B-2 B cells and B - 1 B cells are the most predominant forms. (1 ) B-2 B cel ls are the "conventional" B cells and will be referred to as "B cells" in this
textbook; they are the most numerous and are present throughout the body; they must interact with T cells to propagate (in the bone marrow) and to become activated; they recognize an immense number of ep itopes; and they are able to switch isotypes (i.e. , switch in the synthesis of antibody types) and establish memory B ce l ls . They are considered to be firmly related to the adaptive immune system.
(2) B-1 B ce l ls are much fewer in number than B cells and are usually limited to the gastrointestinal and respiratory systems; they very seldom require T-cell interaction; they do not have to regenerate in the bone marrow but proliferate peripherally; they target carbohydrates rather than proteins; they very seldom switch isotypes; and they do not establish memory B - 1 B cells. They cross over between the innate and adaptive immune systems.
c. CD40 molecules are present on the plasmalemmae of B cells. They interact with CD40 receptors on TH2 cells, causing release of cytokines that (1 ) facilitate proliferation and transformation of B cells into B memory and plasma
cells and (2) inhibit TH 1 cell proliferation.
d . The specific cytokines that are released by T helper cells depend on the invad ing pathogen . (1 ) IL-4 and IL-5 are released by T helper cells in response to parasitic worms causing
B cells to switch to IgE formation. (2) IL-6 and IFN-y are released by T helper cells in response to bacteria and viruses in the
connective tissue, causing B cells to switch to IgG formation. (3) Transforming growth factor � (TGF-�) is released by T helper cells in response to the
presence of bacteria and viruses on mucosal surfaces causing B cells to switch to IgA formation.
e. B lymphocytes can present epitopes complexed with class II human leukocyte antigen (HLA) to TH1 cells; therefore, they are considered to be APCs.
f. When activated, B lymphocytes release I L-1 2 to induce TH1 cell formation and NK cell activation.
g. During a humoral immune response to an antigenic challenge, B lymphocytes proliferate and differentiate to form plasma cells and B memory cells (Figure 12 . 1A).
2. Plasma ce l ls lack surface antibody and actively synthesize and secrete antibody specific aga inst the cha l leng ing ant igen.
3. B memory ce l ls are long- l ived committed immunocompetent ce l ls that are formed during proliferation in response to an antigenic challenge. They do not react against the antigen but remain in the circulation or in specific regions of the lymphoid system. Since they increase the size of the original clone, they provide a faster and g reater secondary response (anamnestic response) against a future challenge by the same antigen.
4. There are also two groups of B cells in the spleen: the more populous follicular B cells and fewer marginal zone B cells. a. Fo l l icu lar B ce l ls are more populous and are located in the primary and secondary follicles
of the spleen (see VI C 3 ofthis chapter); they sport IgM, IgD, and CD21 surface markers; and
208 BRS Cel l B iology and H istology
they are T cell dependent for immune function. They are believed to be in the final stage of their maturation into fully functioning mature B cells.
b. Marg ina l zone B ce l ls are fewer in number than follicular B cells; are located in the marginal zone of the spleen (see VI C 3 of this chapter); they sport IgM, CD 1, CD9, and CD21 on their plasmalemmae; they are T cell independent for their immune functions. They react primarily to self-antigens and bacterial invasion.
CLIN ICAL CONSIDERATIONS
Common var iab le immunodefic iency i s a d i sease of the young , deve l op i n g i n pat ie nts who a re between 1 0 a n d 20 yea rs o f a g e . Alth ough
th ese patie nts have no rm a l B - c e l l p o p u l ati on , they d o not m a n ufacture e nough immunog l obu l i ns , with th e conseq u e n c e of be ing p rone to re c u rrent resp i rato ry i nfecti ons and the deve l o pment of a uto immune d iso rd e rs such a s rh e umato id a rth ritis, thyro i d it is, and Add ison d isease . Affected i n d iv id u a l s fre q u ently suffe r from g a stroi ntesti n a l d i so rde rs, s u c h a s d i a rrhea and i nsuffi c i e nt abso rpti on of n utr ients from th e a l imenta ry c a n a l .
Hodgkin d isease i s a ma l i g n a nt neoplastic transformation o f lymphocytes.
1 . It o c c u rs mostly in yo ung men . It i s c h a ra cte r ized by the presen c e of Reed Sternberg cel ls, wh ich a re g i a nt c e l l s with two l a rge , va c u o lated n u c l e i , e a c h with a dense n u c l eo l u s .
2. S i gns a n d sym ptoms i n c l ude pa i n l ess prog ressive en largement o f the lymph nodes, spleen, and l iver; anem i a ; fever ; wea kness; a n o rexi a ; and we ight loss .
D. NK cel ls belong to a category of nul l cel ls, a small group of peripheral-blood lymphocytes that l ack the surface determinants that are characteristic of T and B lymphocytes. However, they do possess two specific receptors : k i l le r activat ion receptors that respond to stress molecules and k i l l e r i nh ib it ion receptors that respond to MHC Class I molecules. It is these receptors that aid them in the recognition of virally altered cells and tumor cells that have to be forced into apoptosis. 1. As soon as they are formed, NK cells are immunocompetent. They do not have to enter the
thymic environment. 2. Not only are NK cells not MHC restricted but they also exhibit an apparently nonspecific
cytotoxic ity against tumor cells and virus-infected cells. The mechanism by which NK cells recognize these target cells is not yet understood.
3. NK cells can also kill specific target cells that have antibodies bound to their surface antigens in a process known as antibody-dependent cel l -med iated cytotoxic ity (ADCC); macrophages, neutrophils, and eosinophils also exhibit ADCC.
4. NK cells use perforins and granzymes to drive the virally altered cells or tumor cells into apoptosis.
E. Macrophages function both as APCs and as cytotoxic effector ce l ls in ADCC. 1 . When acting as APCs, macro phages phagocytose antigens, fragment them into small antigenic
components, known as ep itopes, and present them to T cells. 2. Macrophages produce and release I L- 1 , which helps activate TH cells and self-activate
macrophages. Moreover, they produce TNF-a, which also self-activates macrophages and induces the release of IL- 12; in conjunction with IFN-y facilitates killing of endocytosed bacteria (Table 12.2). In addition, macrophages secrete prostag land in E2 (PGE2), which decreases certain immune responses, I L-6, which activates T cells and stimulates B cells to differentiate into plasma cells, I L- 12, which activates TH1 cells to proliferate and activates NK cells, I L-1 8, which acts on TH1 cells to produce IFN-y and also enhances NK cell activity, and I L-23, which decreases the motility of CDS + T cells. It should be noted that I L- 1 , I L-6, and TN F-a act together to induce an inf lammatory process.
A. MHC
I!1Jllt!llllij Lympho i d Tissue 209
1 . The MHC (major histocompatibility complex) is a large genetic complex with many loci that encode two main classes of integral membrane molecules: class I molecules (MHC 1 ), which are expressed by nearly all nucleated cel ls, and c lass II molecules (MHC I I ) , which are expressed by the various cells that function as APCs.
2. In humans, the MHC is referred to as the HLA complex (human lymphocyte antigen) . Therefore, MHC I is class I HLA, and MHC II is class II HLA. As described below, MHC I molecules bind epitopes derived from endogenous prote ins, whereas MHC II molecules bind epitopes derived from exogenous prote ins. Both types of MHC molecules present their epitopes to T cells.
B. lmmunogens are molecules that are capable of i nduc ing an immune response. All immunogens are antigens, that is, molecules whose epitopes can react with an antibody or a TCR (T ce l l receptor). Most, but not all, antigens are immunogens. 1. Exogenous immunogens are derived from proteins that were endocytosed or phagocytosed
by APCs and degraded intracellularly, yielding antigenic peptides containing an epitope that enter the trans-Golgi network (TGN) .
2. In the TGN, the complex is sorted into specialized antigenic peptides (containing an epitope) that associate with class II H LA molecules (MHC II molecules) . a. These epitopes are relatively long, composed of 13 to 25 amino acids. b. Class II HLA molecules are synthesized on the rough endoplasmic reticulum (RER) and are
loaded within the RER cisternae with a protein known as CLIP (c lass II-associated invariant protein).
c. The class II HLA-CLIP complex enters the Golgi apparatus, where it is delivered to MIIC vesicles (MHC c lass II compartment vesicles that already contain epitopes derived from exogenous immunogens), where the CLIP is exchanged for the epitope.
d . The epitope-class II HLA complexes are transported to and displayed on the cell surface, where they are presented to T cells.
3. Endogenous immunogens are derived from proteins that were produced with i n host cells (these may be viral prote ins synthesized in virus-infected cells or tumor prote ins synthesized in cancerous cells). a. C lass I H LA molecules (MHC I molecules), synthesized on the RER surface, enter the RER
cisternae. b. Endogenous immunogens are degraded by organelles of the host cells, known as
proteasomes, into short polypeptide fragments. These fragments are antigenic peptides (8- 12 amino acids in length) known as ep itopes.
c. The epitopes are transported by TAP1 and TAP2 (transporter proteins l and 2) into the RER cisternae.
d. Within the RER cisternae, the epitopes derived from endogenous immunogens are loaded on the c lass I HLA.
e. The peptide-class I HLA complexes are transported to the Golgi complex for sorting and eventual delivery within clathrin-coated vesicles to the cell surface, where they are presented to T cells.
C. MHC (HLA) restriction-T lymphocytes. Each subtype of T lymphocytes (except T memory cells) recognizes only epitopes that are associated with either MHC I or MHC II (class I or class II HLA) molecules as follows: 1 . THl and TH2 cells (CD4+ cells) recognize MHC II (class II HLA) molecules. 2. Cytotoxic T cells (CDS+ cells) recognize MHC I (class I HLA) molecules. 3. T memory cells (CD45RO cells) recognize both MHC I and MHC II (class I and class II HLA)
molecules.
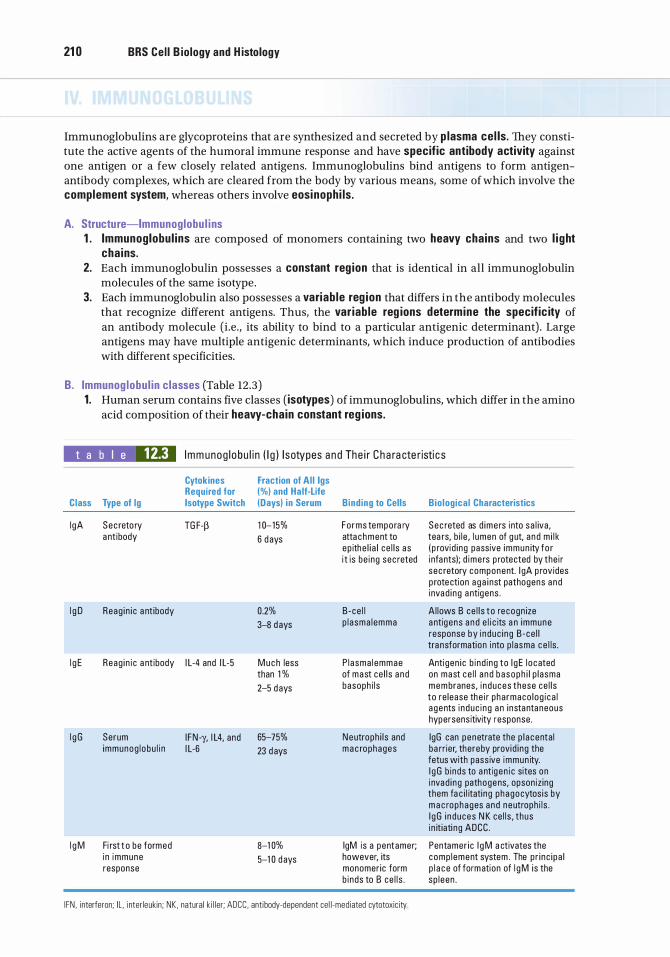
21 0 BRS Cel l B iology and H istology
Immunoglobulins are glycoproteins that are synthesized and secreted by p lasma cel ls. They constitute the active agents of the humoral immune response and have specific antibody activity against one antigen or a few closely related antigens. Immunoglobulins bind antigens to form antigenantibody complexes, which are cleared from the body by various means, some of which involve the complement system, whereas others involve eosinophi ls .
A. Structure-Immunoglobu l i ns 1 . Immunoglobul ins are composed of monomers containing two heavy chains and two l i ght
cha ins. 2. Each immunoglobulin possesses a constant reg ion that is identical in all immunoglobulin
molecules of the same isotype. 3. Each immunoglobulin also possesses a variab le reg ion that differs in the antibody molecules
that recognize different antigens. Thus, the var iab le reg ions determine the specific ity of an antibody molecule (i .e. , its ability to bind to a particular antigenic determinant) . Large antigens may have multiple antigenic determinants, which induce production of antibodies with different specificities.
B. Immunog lobu l in classes (Table 12.3) 1 . Human serum contains five classes (isotypes) of immunoglobulins, which differ in the amino
acid composition of their heavy-chain constant reg ions.
t a b I e 12.3 I mm unog l obu l i n ( l g ) l sotypes a n d The i r C h a ra cte r isti c s
Cytokines Fraction of Al l lgs Required for (%) and Ha lf-Life
C lass Type of lg lsotype Switch (Days) i n Serum Bind ing to Cells Bio log ical Characteristics
l gA Sec reto ry TG F-� 1 0- 15% Forms tempora ry Sec reted as d ime rs i nto sa l iva, a nt ibody 6 d ays atta c hment to tea rs, b i l e , l umen of g ut, a n d m i l k
ep ithe l i a l ce l l s as ( p rovid i ng passive immun ity fo r i t is be ing sec reted i nfa nts); d ime rs p rotected by the i r
sec retory component. l gA p rovides p rote ction a g a i nst pathogens a nd i nvad i ng a ntig ens .
l g D Reag i n i c a nt ibody 0.2% B -ce l l A l lows B ce l l s t o re cogn ize 3-8 d ays p l a sma l emma a ntig ens a n d e l i c its a n immune
response by i nduc i ng B -ce l l tra nsformation i nto p l asma c e l ls .
l g E Reag i n i c a nt ibody I L-4 and I L-5 M u c h less P l a sma l emmae Anti gen i c b i nd i ng to l g E l o cated than 1 % of mast ce l l s a nd on mast ce l l a n d b a soph i l p l asma
2-5 d ays basoph i l s membranes, i n duces these ce l l s to re lease the i r pha rmaco log i ca l a gents i nduc i ng a n i nstantaneous hypersens itivity response .
l g G Serum I FN -y, I L4, and 65-75% Neutroph i l s and lgG can penetrate the p l a centa l immunog l obu l i n I L-6 23 d ays m a c rophages ba rr ier, thereby provid i ng the
fetus with pass ive immun ity. l g G b inds to a ntig en i c sites on i nvad i ng pathogens, opson iz ing them fa c i l itati ng phagocytos is by m a c rophages a nd neutroph i l s . l g G i n duces N K ce l l s , thus i n it iati ng ADCC .
l g M Fi rst t o be formed 8-1 0% lgM is a pentamer; Pentamer i c l g M a ctivates the i n immune 5-1 0 d ays however, its comp l ement system . The p r i nc i pa l response monomer ic form p l a c e of formation of l g M is the
b i nds to B ce l l s . sp l een .
I FN , i nterferon; IL . i nter leukin ; NK , natural k i l l er; ADCC, antibody-dependent ce l l -mediated cytotoxic ity
2. The different isotypes exhibit functional differences.
I!1Jllt!llllij Lympho i d Tissue 21 1
a. lgA is secretory immunoglobulin that is released, in the form of dimers, into tears, bile, saliva, milk, and as part of the nasal discharge to protect the body (and the nursing infant) from pathogenic microorganisms and invading antigens. It is protected from digestive enzymes by its secretory component synthesized by epithelial cells and hepatocytes.
b. I gO and lgE are reaginic antibodies; IgE binds to IgE receptors of mast cells and basophils and prompts the release of pharmacologic agents from these cells to initiate an immediate hypersensitivity response. IgD binds to B-cell plasma membranes and permits these cells to recognize antigens and thus initiate a response against antigenic challenges by prompting B cells to differentiate into antibody-secreting p lasma cel ls.
c . l gG , the most abundant serum immunoglobulin, crosses the placental barrier to shield the fetus-a process known as passive immun ity. It attaches to antigenic sites on invading microorganisms, thus opsonizing these pathogens, making them available for phagocytosis by macrophages and neutrophils. These antibodies activate NK cells, thus initiating ADCC.
d . l gM forms pen tamers and is the first isotype to be formed in an immune response. It activates the complement system. Its monomeric form binds to the B-cell plasma membrane.
Diffuse lymphoid tissue is considered to be a secondary lymphoid tissue. It is especially prominent in the mucosae of the gastrointestinal and respiratory systems. It is organized as nonencapsulated clusters of lymphoid cells or as lymphoid (lymphatic) nodules. Diffuse lymphoid tissue is collectively called mucosa-associated lymphoid tissue (MALT).
A. MALT consists of two major types : bronchus-associated lymphoid tissue (BALl) and gut-associated lymphoid tissue (GALT). Both types possess lymphoid nodules that are isolated from one another, except in the case of Peyer patches.
B . Peyer patches are aggregates of lymphoid nodules found in the i l eum. They are components of the GALT.
C. Lymphoid ( lymphatic) nodules are transitory dense spherical accumulations of lymphocytes (mostly B cells) . The dark, peripheral region of nodules (corona) is composed mainly of small, newly formed lymphocytes. Lymphoid nodules of the GALT are isolated from the lumina of their respective tracts by microfo ld (M) ce l ls, which transfer antigens from the lumen and present them (without processing them into epitopes) to lymphocytes and macrophages lying in deep invaginations of their basal cell surfaces. From here, an appropriate immune response is mounted by lymphoid tissue in the underlying lamina propria. 1 . Secondary nodules, formed in response to an antigenic challenge, have a lightly staining
central area called the germina l center, which is composed of B lymphocytes ( lymphoblasts [centroblasts] as well as centrocytes). A darker region, known as the mantle (corona) , is composed of resting B cells that are being displaced from the germinal center by the newly formed B cells. In addition to centroblasts and centrocytes, the germinal center houses B memory cells, plasma cells, migrating dendritic cells, follicular dendritic cells, macrophages, and reticular cells. a. Centroblasts do not display surface immunoglobulins (sigs), whereas centrocytes have
expressed sigs. b. Centrocytes that express sigs against self are forced into apoptosis. c. Surviving centrocytes become B memory ce l ls or plasma cel ls. d . M igrating dendritic cel ls, derived from the bone marrow, are located in various regions of
the body, and when they encounter an antigen, they travel to a nearby lymphoid nodule or lymph node to precipitate an immune reaction.
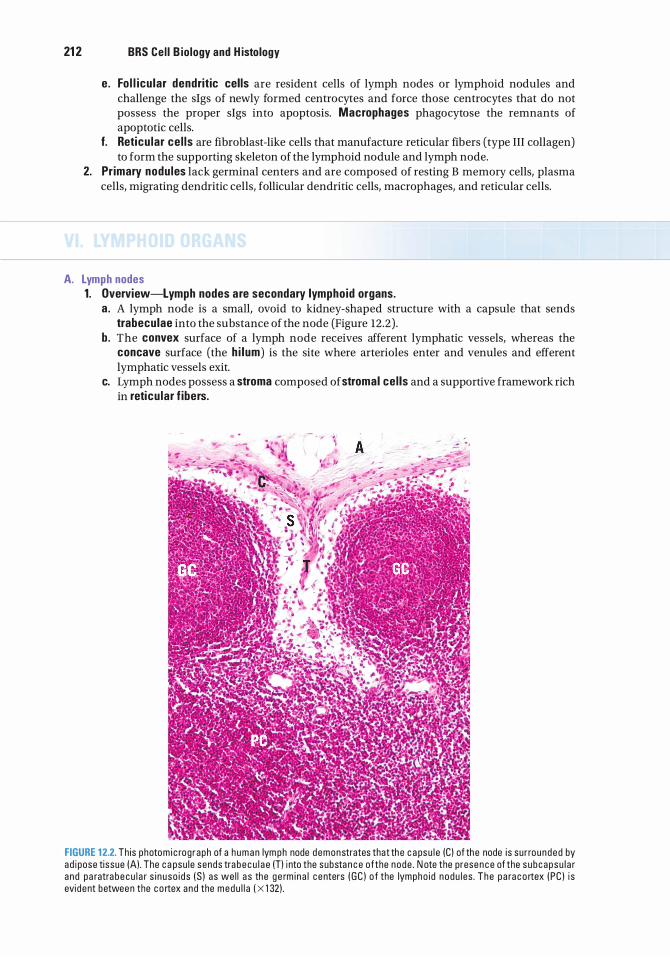
21 2 BRS Cel l B iology and H istology
e. Fo l l icu lar dendritic cells are resident cells of lymph nodes or lymphoid nodules and challenge the slgs of newly formed centrocytes and force those centrocytes that do not possess the proper slgs into apoptosis. Macrophages phagocytose the remnants of apoptotic cells.
f. Reticu lar ce l ls are fibroblast-like cells that manufacture reticular fibers (type III collagen) to form the supporting skeleton of the lymphoid nodule and lymph node.
2. Primary nodu les lack germinal centers and are composed of resting B memory cells, plasma cells, migrating dendritic cells, follicular dendritic cells, macro phages, and reticular cells.
A. Lymph nodes 1. Overview-Lymph nodes are secondary lymphoid organs.
a . A lymph node is a small, ovoid to kidney-shaped structure with a capsule that sends trabeculae into the substance of the node (Figure 12.2) .
b. The convex surface of a lymph node receives afferent lymphatic vessels, whereas the concave surface (the h i lum) is the site where arterioles enter and venules and efferent lymphatic vessels exit.
c. Lymph nodes possess a stroma composed of stromal ce l ls and a supportive framework rich in reticu lar f ibers.
FIGURE 12.2. Th is photo m i c rog raph of a h u m a n lym ph node demonstrates that the c a psu l e (C) of the node i s sur rounded by ad i pose ti ssue (A) . The c a psu le sends tra b e c u l a e (T) i nto the substa n c e ofthe node . N ote the prese n c e of the s ubcapsu l a r a nd pa ratra b e c u l a r s i n u so i d s (S ) as we l l a s the g e rm i n a l c enters ( G C ) o f the lympho i d nodu l es . The pa ra c o rtex ( PC ) i s evi dent betwee n the c o rtex and the medu l l a ( X 1 32) .
I!1Jllt!llllij Lympho i d Tissue 213
d . Function. Lymph nodes filter lymph, maintain and produce T and B cells, and possess memory cells (especially T memory cells). Antigens delivered to lymph nodes by APCs are recognized by T cells, and an immune response is initiated. Additionally, some of the stromal ce l ls and some of the dendritic cel ls of lymph nodes express the transcription factor AIRE (auto immune regulator), which selectively induces anti-self-T cells that escaped destruction in the thymus to go into apoptosis.
2. Structure-Lymph nodes. Lymph nodes are divided into three regions : the outermost cortex, the middle para cortex, and the innermost medul la (Figure 12.2). Stromal cells of these regions release a variety of chemotactic chemokines lymphocytes (CCLs) that attract lymphocytes. Depending on the CCL released, B cells or T cells are attracted to a particular region of the lymph node. In order to attract both B cells and T cells, CCLs are conveyed to the luminal endothelial cell membranes of postcapillary venules, the region where lymphocytes leave the circulatory system to enter the substance of the lymph node. Once in the lymph node stroma, both B cells and T cells are segregated within the cortex of the lymph node by those CCLs to which each responds. a. The cortex of lymph nodes
(1 ) lies deep to the capsule, from which it is separated by a subcapsular sinus. (2) is incompletely subdivided into compartments by connective tissue septa derived from
the capsule. (3) contains lymphoid nodules and sinusoids.
(a) Lymphoid nodules are composed mainly ofB cells but also of some T cells, follicular dendritic cells, macrophages, and reticular cells. They may possess a germinal center and then they are known as secondary lymphatic nodules.
(b) Sinusoids are endothelium-lined lymphatic spaces that extend along the capsule and trabeculae and are known as subcapsu lar and cortical sinusoids, respectively.
b. The para cortex of the lymph node is located between the cortex and the medulla. (1 ) It is composed of a non-nodular arrangement of mostly T lymphocytes (the thymus
dependent area of the lymph node) and dendritic ce l ls . (2 ) The paracortex is the region where circulating lymphocytes gain access to lymph nodes
via postcap i l la ry (h igh endothe l ia l ) venules (HEVs). c . The medul la of a lymph node lies deep to the paracortex and cortex, except at the region of
the hilum. It is composed of medullary sinusoids and medullary cords. (1 ) Medullary sinusoids are endothelium-lined spaces supported by reticular fibers and
reticular cells. They frequently contain macrophages and receive lymph from the cortical sinuses.
(2) Medullary cords are composed of lymphocytes and plasma cells.
B. The thymus is a pr imary lymphoid organ. 1 . Overview-Thymus
a . The thymus is a bilobed structure located in the neck. It is derived from both endoderm (epithe l ia l reticu lar cel ls), derived from the third pharyngeal pouch of the embryo, and mesoderm (lymphocytes [thymocytes]) . The development of the epithelial reticular cells of the thymus (especially in the medulla) is dependent on the formation and release of lymphotoxins, members of the tumor necrosis factor family of cytokines. In the absence of these proteins the thymus does not develop or function properly. The thymus begins to involute near the time of puberty.
b. A connective tissue capsule surrounds the thymus. The septa of this capsule divide the parenchyma into incomplete lobules, each of which contains a cortical and medul lary reg ion (Figure 12 .3) . The thymus does not possess lymphoid nodules.
2. Structure-Thymus a . The thymic cortex is supplied by arterioles in the septa; these arterioles provide capillary
loops that enter the substance of the cortex. The cortex is the region in which T-ce l l maturation occurs. (1 ) Ep ithe l ia l reticu lar ce l ls (Figure 12.3)
(a ) There are six types of epithelial reticular cells (see Table 12.4) . They are pale cells (derived, during embryogenesis, from the third and perhaps fourth pharyngeal pouches) and have a large ovoid lightly staining nucleus that often displays a nucleolus.
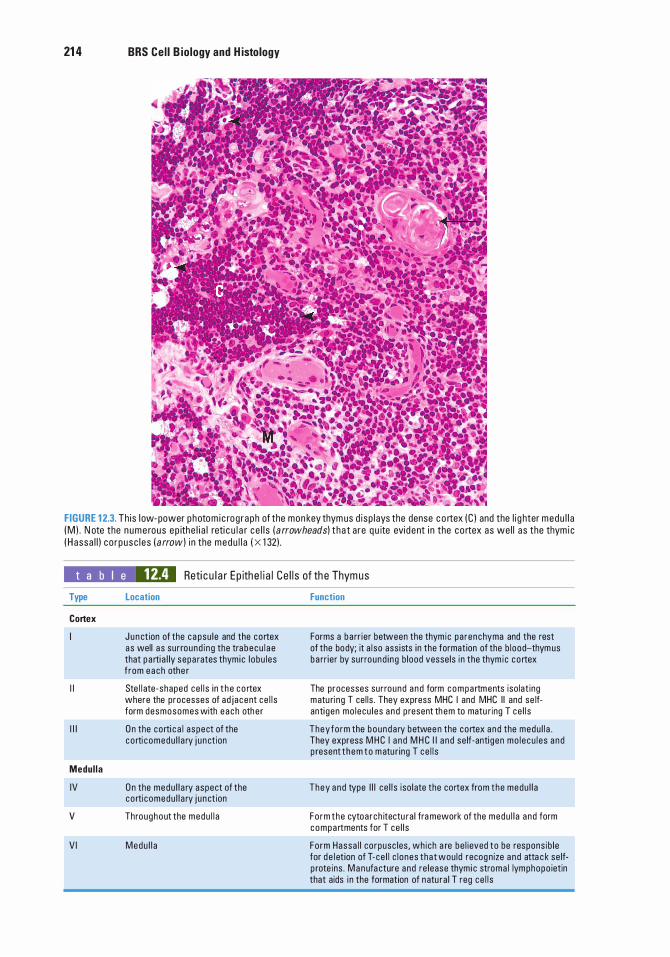
21 4 BRS Cel l B iology and H istology
FIGURE 1 2.3. Th is l ow- power photo m i c rog raph of the mon key thym us d i sp l ays the dense c o rtex (C ) and the l i g hter medu l l a (M ) . N ote the n u m e rous ep ithe l i a l reti c u l a r ce l l s ( a rrowheads) t ha t are q u ite evi dent i n the co rtex as we l l as the thym i c ( H assa l l ) c o r pusc l e s ( arrow) i n the medu l l a ( x 1 32) .
t a b I e 12.4 Reti c u l a r Ep ithe l i a l Ce l l s of th e Thymus
Type
Cortex
I I
I l l
Medul la
IV
v
VI
Location
Jun ction of the ca psu le and the cortex as well a s sur round i ng the tra becu l a e that partia l ly sepa rates thym ic l obu l es f rom each othe r
Ste l l ate-shaped ce l l s i n t h e c o rtex where the processes of ad jacent ce l l s form desmosomes with e a ch othe r
O n the corti c a l aspect of the co rti comedu l l a ry j u n ct ion
O n the medu l l a ry aspect of the co rti comedu l l a ry j u n ct ion
Throughout the medu l l a
Medu l l a
Function
Forms a ba rr ier between the thym ic pa renchyma and the rest of the body; it a l so ass ists in the formation of the b lood-thym us ba rr ier by surround i ng b lood vesse ls i n the thym ic cortex
The processes surround a nd form compa rtments iso lat ing matu ri ng T ce l ls . They express MHC I and MHC I I and se lfanti gen mo lecu l es a nd p resent th em to matu r ing T ce l l s
They fo rm the bounda ry betwee n the cortex and the medu l l a . They express M H C I a n d M H C I I a n d se lf-anti gen mo l ecu l e s a nd p resent t hem to m atu r ing T ce l l s
They and type I l l ce l l s iso l ate the cortex from the medu l l a
Fo rm the cytoa rch itectu ra l fra mework of the medu l l a and form compa rtments for T ce l l s
Form Hassa l l co rpusc les, wh ich a re be l ieved to be respons ib le for d e l et ion of T-ce l l c l ones that wou ld recog nize a nd atta c k se lfp rote ins . M a nufa cture and re lease thym i c stroma l lymphopo ietin that aids i n the formation of natu ra l T reg ce l l s
I!1Jllt!llllij Lympho id Tissue 21 5
(b ) They possess long processes that surround the thymic cortex, isolating it from both the connective tissue septa and the medulla. These processes, which are filled with bundles oftonofi laments, form desmosomal contacts with each other.
(c ) They manufacture thymosin, serum thymic factor, thymopoietin, and thymic stromal lymphopoietin, hormones that function in the transformation of immature T lymphocytes into immunocompetent T cells.
(2) Thymocytes (a ) Thymocyte plasmalemma possesses Notch-1 receptors that permit these cells to
respond to cytokines released by epithelial reticular cells to become T cells. Once committed to the T-cell lineage, they are known as immature T lymphocytes and are noted to be present within the thymic cortex in different stages of differentiation.
(b) Thymocytes are surrounded by processes of epithelial reticular cells, which help segregate thymocytes from antigens during their maturation.
(c) They migrate toward the medulla as they mature. Most T cells die in the cortex, and the dead cells are phagocytosed by macrophages.
(d) Surviving T cells are naive. They leave the thymus and are distributed to secondary lymphoid organs by the vascular system.
(3) B lood-thymus barrier (a ) This barrier exists in the cortex on ly, making it an immunologically protected region. (b) It ensures that antigens escaping from the bloodstream do not reach developing
T cells in the thymic cortex. (c) It consists of the following layers : endothe l ium of the thymic capillaries and the
associated basal lamina, perivascu lar connective tissue and ce l ls (e.g., pericytes and macrophages), and type I ep ithe l ia l reticu lar cel ls and their basal laminae.
b. Thymic medu l l a (1 ) The thymic medulla i s continuous between adjacent lobules and contains large
numbers of epithe l ia l reticu lar ce l ls and mature T cel ls, which are loosely packed, causing the medulla to stain lighter than the cortex (Figure 12 .3) .
(2) It also contains whorl-like accretions of type VI epithelial reticular cells called Hassa l l corpuscles (thymic corpuscles). These structures display various stages of keratinization and increase in number with age. It has been shown that these epithelial reticular cells manufacture TSLP (thymic stromal lymphopoietin), a cytokine that facilitates dendritic cell maturation which, in turn, elicit the transformation of naive T cells into natural T reg cells.
(3) Mature T cells exit the thymus via venules and efferent lymphatic vessels from the thymic medulla. The T cells then migrate to secondary lymphoid structures.
(4) Hormones acting on the thymus (a ) Thymosin, thymopoietin, thymulin (thymic factor), somatotropin, thymic
stromal lymphopoietin, and thymic humoral factor promote the formation of immunocompetent T cells.
(b) Thyroxin encourages thymulin production by epithelial reticular cells. (c) Adrenocorticostero ids depress T-cell formation in the thymus.
CLIN ICAL CONSIDERATIONS
DiGeorge syndrome, a l so c a l l e d congenita l thymic ap lasia , i s c h a ra cte rized by the congen ita l a b sence of the thym us a n d pa rathyro i d g l a nds ,
resu lti n g from a b no rma l d eve l o pment of the th i rd and fo u rth p h a ryn g e a l p o u ches .
1 . Th is syn d rome is assoc i ated with abnormal ce l l -med iated immun ity but re l ative ly norma l h u m o ra l i m m u n ity.
2. It u sua l ly resu lts i n death from tetany or u n contro l l a b l e i nfection.
C. Sp leen 1 . Overview-Spleen
a . A simple squamous epithelium (peritoneum) covers the dense irregular collagenous connective tissue capsu le of the spleen, which sends trabeculae into the substance of the spleen to form a supportive framework (Figure 12 .4).
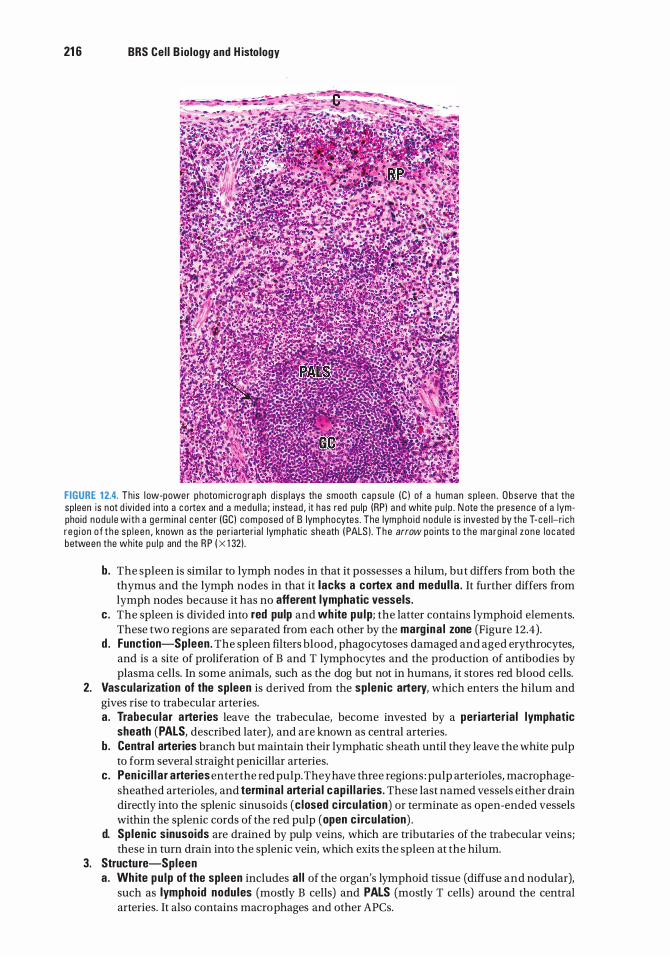
21 6 BRS Cel l B iology and H istology
FIGURE 12.4. Th is l ow-power photo m i c rog raph d i sp l ays the smooth capsu l e IC ) of a h uman sp l een . Obse rve that the sp leen is not d iv i ded i nto a c o rtex and a medu l l a ; i nstead , it has red pu lp IRP) a nd wh ite p u l p . N ote the p resence of a lympho id nodu l e with a g e rm i n a l c enter IGC) com posed of B lym phocytes . The lym pho i d nodu l e i s invested by the T- ce l l-ri c h r e g i o n o f t h e s p l e e n , known a s the pe r i a rte r i a l lym phati c she ath I PALS ) . T h e arrow po ints t o t h e ma rg i n a l z o n e l oc ated between the white p u l p and the R P I X 1 32) .
b. The spleen is similar to lymph nodes in that it possesses a hilum, but differs from both the thymus and the lymph nodes in that it lacks a cortex and medul la . It further differs from lymph nodes because it has no afferent lymphatic vessels.
c . The spleen is divided into red pulp and white pu lp; the latter contains lymphoid elements. These two regions are separated from each other by the marg ina l zone (Figure 12.4) .
d . Function-Spleen. The spleen filters blood, phagocytoses damaged and aged erythrocytes, and is a site of proliferation of B and T lymphocytes and the production of antibodies by plasma cells. In some animals, such as the dog but not in humans, it stores red blood cells.
2. Vascularization of the spleen is derived from the splen ic artery, which enters the hilum and gives rise to trabecular arteries. a. Trabecular arteries leave the trabeculae, become invested by a periarter ia l lymphatic
sheath (PALS, described later), and are known as central arteries. b. Centra l arteries branch but maintain their lymphatic sheath until they leave the white pulp
to form several straight penicillar arteries. c. Pen ic i l l a r arteries enter the red pulp. They have three regions : pulp arterioles, macrophage
sheathed arterioles, and termina l arteria l cap i l l a ries. These last named vessels either drain directly into the splenic sinusoids (c losed c i rcu lation) or terminate as open-ended vessels within the splenic cords of the red pulp (open c i rcu lation) .
d. Sp len ic sinusoids are drained by pulp veins, which are tributaries of the trabecular veins; these in turn drain into the splenic vein, which exits the spleen at the hilum.
3. Structure-Spleen a . Wh ite pu lp of the spleen includes al l of the organ's lymphoid tissue (diffuse and nodular),
such as lymphoid nodules (mostly B cells) and PALS (mostly T cells) around the central arteries. It also contains macro phages and other APCs.
b. The marg ina l zone (MZ) of the spleen
I!1Jllt!llllij Lympho i d Tissue 21 7
(1 ) is a sinusoidal reg ion between the red and white pulps at the periphery of the PALS (Figure 12.4) .
(2) receives blood from capillary loops derived from the central artery and is thus the fi rst site where b lood contacts the splen ic parenchyma.
(3) is richly supplied by avidly phagocytic macrophages and other APCs. There are two types of macrophages in the marginal zone: the MZ macrophages and the MZ meta l loph i l i c macrophages. (a ) MZ macrophages express molecules on their surface that recognize pathogens
such as bacteria, viruses, and yeasts. (b) MZ meta l loph i l i c macrophages express molecules that bind to cell-bound
oligosaccharide ligands; these macrophages also interact with marg ina l zone B cells (see Section II C 4 b in this chapter), promoting them to migrate to the white pulp of the spleen and present blood-borne antigens to T cells.
(4) The MZ is the region where circulating T and B lymphocytes enter the spleen before becoming segregated to their specific locations within the organ and where interd ig itati ng dendritic cel ls are able to display their MHC-epitope complex for recognition by T cells.
(5) Stromal cells of the MZ release a variety ofCCLs (chemotactic chemokines lymphocytes) that attract lymphocytes. Depending on the CCL released, B cells or T cells are attracted to a particular region of the spleen. In order to attract both B cells and T cells to the MZ, CCLs are conveyed to the luminal endothelial cell membranes of MZ sinusoids. Once in the spleen parenchyma, both B cells and T cells are segregated within the white pulp of the spleen by those CCLs to which each responds.
c. Red pu lp of the spleen (Figure 12 .4) is composed of an interconnected network of sinusoids supported by a loose type of reticular tissue (sp len ic cords). (1 ) Sinusoids
(a) are lined by long fusiform endothelial cells separated by relatively large bloodcontaining intercellular spaces.
(b) have a discontinuous basal lamina underlying the endothelium and circumferentially arranged ribs of reticular fibrils.
(2) Sp len ic cords (cords of B i l l roth ) contain plasma cells, stellate reticular cells, blood cells, and macro phages enmeshed within the spaces of the reticular fiber network. Processes of the macro phages enter the lumina of the sinusoids through the spaces between the endothelial cells.
D. Tonsi ls are aggregates of lymphoid tissue, which sometimes lack a capsule. All tonsils are in the upper section of the digestive tract, lying beneath but in contact with the epithelium. B and T cells in the three sets of tonsils are localized in different regions of any particular tonsil. The mechanism of distribution is similar to that which occurs in lymph nodes and the spleen, and depends on the various chemotactic chemokines for lymphocytes (CCLs) secreted by stromal cells. Tonsils assist in combating antigens entering via the nasal and oral epithelia. 1 . Palat ine tonsi ls
a . possess crypts, deep invaginations of the stratified squamous epithelium covering of the tonsils, frequently containing debris;
b. possess primary and secondary (with germinal centers) lymphoid nodules; c. are separated from subjacent structures by a connective tissue capsu le .
2. The pharyngeal tonsi l is a sing le tonsil in the posterior wall of the nasopharynx. a. It is covered by a pseudostratified ciliated columnar epithelium. b. Instead of crypts, it has longitudinal pleats (infoldings) . c. Possesses primary and secondary (with germinal centers) lymphoid nodules.
3. Li ngual tonsi l a . is on the dorsum of the posterior third of the tongue and is covered by a stratified squamous
nonkeratinized epithelium. b. possesses deep crypts, which frequently contain debris. Ducts of the posterior mucous
glands of the tongue often open into the base of these crypts. c. possesses primary and secondary (with germinal centers) lymphoid nodules.
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1. Which of the following statements concerning T helper cells is true?
(A) They possess membrane-bound antibodies.
(B) They can recognize and interact with antigens in the blood.
(C) They produce numerous cytokines. (D) They function only in cell-mediated
immunity. (E ) Their activation depends on interferon-y.
2. Which of the following statements concerning T cytotoxic (T c) cells is true?
(A) They assist macro phages in killing microorganisms.
(B ) They possess antibodies on their surfaces. (C) They possess CD8 surface markers. (D ) They possess CD28 surface markers. (E) They secrete interferon-y.
3. Which of the following cell types is thought to function in suppressing the immune response?
(A) Inducible T reg cells (B ) B cells (C) T memory cells (D ) TH cells (E) Mast cells
4. Which of the following statements concerning interferon-y is true?
(A) It is produced by T memory cells. (B) It is produced by T reg cells. (C) It activates macrophages. (D) It inhibits macrophages. (E) It induces viral proliferation.
21 8
5. A patient who was given penicillin had an adverse reaction to the antibiotic. Although the reaction was due to the actions of mast cells, the response occurred because mast cells have IgE receptors in their cell membranes. Which of the following cells produced the IgE decorating the plasma cell's surface?
(A) T memory cells (B ) B memory cells (C ) T helper cells (D ) Plasma cells (E) T cytotoxic cells
6. Which of the following statements concerning the thymus is true?
(A) Lymphoid nodules form much of the thymic cortex.
(B ) Epithelial reticular cells form Hassall corpuscles.
(C) T cells migrate into the medulla, where they become immunologically competent.
(D ) Most T cells that enter the thymus are killed in the medulla.
(E ) Macrophages are essential components of the blood-thymus barrier.
7. Which of the following statements concerning Hassan corpuscles is true?
(A) They are located in the thymic cortex of young individuals.
(B ) They are located in the thymic cortex of old individuals.
(C) They are derived from mesoderm. (D ) They are located in the thymic medulla. (E ) They are derived from T memory cells.
8. After their maturation in the thymus and release into the circulation, T lymphocytes migrate preferentially to which of the following sites?
(A) Para cortex of lymph nodes (B) Cortical lymphoid nodules of lymph nodes (C ) Hilum of lymph nodes (D) Lymphoid nodules of the tonsils (E) Lymphoid nodules of the spleen
9. In which of the following sites do lymphocytes become immunocompetent?
(A) Germinal center of secondary lymphoid nodules
(B ) White pulp of the spleen (C) Thymic cortex (D ) Red pulp of the spleen (E) Paracortex of lymph nodes
I!1Jllt!llllij Lympho i d Tissue 21 9
1 0. Which of the following statements about IgG is true?
(A) It is located in the serum and on the membrane of B cells.
(B ) It can cross the placental barrier. (C) It is involved in allergic reactions. (D) It exists as a pentamer. (E ) It binds to antigens on the body surface
and in the lumen of the gastrointestinal tract.
Answers and Explanations
1 . C. T helper cells produce a number of cytokines that affect other cells involved in both the cellmediated and humoral immune responses. T helper cells possess antigen-specific TCRs (not antibodies) on their membranes. These cells recognize and interact with antigenic determinants that are associated with class II HLA molecules on the surface of APCs. IL- l is necessary for activation of T helper cells (see Chapter 12 II B 3 c) .
2. C. T cytotoxic cells are CDS+ cells. CD28 molecules are present on THl cells. IFN-y is released by THl cells, which also assist macrophages in killing microorganisms (see Chapter 12 II B 3 c) .
3. A. The immune response is decreased by inducible T reg cells. They suppress the formation of THl cells, thereby suppressing the immune response (see Chapter 12 II B 3 c) .
4. C. Interferon-y activates macrophages, NK cells, and T cytotoxic cells, enhancing their phagocytic or cytotoxic activity or both (see Chapter 12 II E 2) .
5. D . Individuals allergic to penicillin produce IgE antibodies. The cells that manufacture IgE are plasma cells. After an antigenic challenge, proliferation and differentiation of B cells give rise to plasma cells and B memory cells (see Chapter 12 II C 2) .
6. B . Epithelial reticular cells of the medulla congregate to form Hassan (thymic) corpuscles (see Chapter 12 VI B 2 b) .
7. D . Hassall corpuscles are concentric accretions of epithelial reticular cells (derived from endoderm) found only in the medulla of the thymus (see Chapter 12 VI B 2 b) .
8. A. T lymphocytes are preferentially located in the paracortex of lymph nodes, whereas B lymphocytes are found in lymphoid nodules located in lymph nodes, tonsils, and the spleen (see Chapter 12 VI A 2 a) .
9. C. T lymphocytes mature and become immunocompetent in the cortex of the thymus, whereas B lymphocytes do so in the bone marrow. After an antigenic challenge, lymphocytes proliferate and differentiate in various lymphoid tissues (see Chapter 12 II B 2 and II C 1 ) .
1 0. B . IgG is the most abundant immunoglobulin isotype in the serum. I t can cross the placental barrier but does not bind to the B-cell plasma membrane. It exists as a monomer, functions to activate complement, and acts as an opsonin (see Chapter 12 IV B 2).
220
Endocrine System
I. OVERVIEW-THE ENDOCRINE SYSTEM
A. The endocrine system is composed of several ductless g lands, c l usters of cel ls within certain organs, and isolated single endocrine cel ls, known as the diffuse neuroendocrine system (DNES) cells, located in the epithelial lining of the respiratory and gastrointestinal systems (discussed in chapters 15 and 16, respectively) .
B. Glands of the endocrine system include the p itu itary g land (and a region of the brain known as the hypotha lamus), as well as the thyro id, parathyro id, adrenal , and pinea l glands. Additional components of the endocrine system, such as the Islets of Langerhans, adipose tissue, female gonads, and male gonads, are discussed in the pertinent chapters.
C. Function. The endocrine system secretes hormones into nearby capillaries and interacts with the nervous system to modulate and control the body's metabolic activities.
Hormones are chemical messengers that are carried via the bloodstream to distant target cel ls . They include low-molecular-weight water-so lub le proteins, polypeptides, and amino acids (e.g., insulin, glucagon, follicle-stimulating hormone [FSH]) and l i p id-so lub le substances, principally the steroid hormones (e.g., progesterone, estradiol, and testosterone).
A. Water-so lub le hormones interact with specific cell surface receptors on target cells, which communicate a message that generates a biological response by the cell. 1. G prote in-l i nked receptors are used by some hormones (e.g., epinephrine, thyroid-stimulating
hormone [TSH] , serotonin). Binding of the hormone to the G protein-linked receptor leads to the production of a second messenger that evokes a target-cell response.
2. Cata lytic receptors are used by insulin and growth hormone. Binding of the hormone to the catalytic receptor activates protein kinases that phosphorylate target proteins.
B. Lip id-solub le hormones diffuse across the plasma membrane of target cells and bind to specific receptors in the cytosol or in the nucleus, forming hormone-receptor complexes that regulate transcription of deoxyribonucleic acid (DNA) .
221
222 BRS Cel l B iology and H istology
The p itu itary gland lies below the hypothalamus in a bony housing known as the hypophyseal fossa, a depression in the se l l a turc ica of the sphenoid bone located in the base of the middle cranial fossa of the skull.
The hypothalamus is a region of the diencephalon of the brain; it possesses nuclei that are structurally and functionally linked to the pituitary gland. The structural link is via a series of axons whose cell bodies are located in the supraoptic and paraventricu lar nuclei of the hypothalamus. These axons form the hypotha lamo-hypophysea l tract and terminate in the pars nervosa of the pituitary gland, where they store and, when needed, release their hormones. The functional connection is via releasing hormones that are synthesized in the arcuate, pa raventri cu lar (and media l paraventricu lar), periventricu lar, ventromedia l , and dorsal nuc le i of the hypothalamus. These hormones are released by the neurons located in these nuclei, enter a capillary bed, and make their way, via the hypophysea l porta l system to a second capillary bed in the anterior lobe of the pituitary gland, leave the capillary bed, and bind to their respective target cells in the anterior pituitary.
The p ituitary g land is a relatively small gland, weighing only about 0.6 g in men and 1 .2 g in women who are pregnant or who have given birth to two or more children. The pituitary is divided into two major subdivisions, the adenohypophysis and the neurohypophysis (Figure 13 . 1 ) . Each subdivision is derived from a distinct embryonic analog, which is reflected in its unique cellular constituents and functions.
A. The adenohypophysis is also called the anterior p ituitary g land (Figures 13 . 1 and 13.2) . It originates from an ectodermal diverticulum of the stomodeum (Rathke pouch) . The adenohypophysis is subdivided into the pars d ista l is, pars i ntermedia , and pars tubera l is .
1 . The pars d ista l is i s supported by a connective tissue capsule and framework. I t consists of irregular cords composed of two types of parenchymal cells, chromoph i ls and chromophobes, lying adjacent to fenestrated capillaries. a . Chromophi ls (Figures 13 . 1 and 13 .3)
(1 ) Overview. Chromophi ls are parenchymal cells that stain intensely because of their hormone-containing secretory granules. They synthesize, store, and release several hormones. They are regulated by specific stimu latory and i nh ib itory hormones produced by neurons, referred to as neurosecretory cel ls, in the hypotha lamus. These hormones are conveyed to the pars distalis via a system of portal blood vessels originating in the median eminence .
(2 ) Types. Chromophils are classified into two types, acidophils and basophils, depending on the dyes they bind using special histological stains. With hematoxylin-eosin stain, the distinction between the two cell types is much less obvious. (a) Acidophi ls (Tables 13 . 1 and 13 .2) bind acidic dyes and often stain orange or red.
They are small cells of two subtypes: somatotrophs and mammotrophs. 1 . Somatotrophs constitute about 50% of the chromophils and produce
somatotrop in (g rowth hormone) . They are stimulated by somatotrop in-releasing hormone and are inhibited by somatostatin .
2. Mammotrophs ( lactotrophs) constitute about 10% of the chromophil population, except in multiparous women, where they may be as high as 30%. Mammotrophs produce pro lactin, which is stored in small secretory granules. They are stimulated by prolacti n-re leasing hormone and thyrotrop in-re leasing hormone (TRH ) and are inhibited by dopamine (until re-identified that it was designated as pro lacti n - inh ib it ing hormone) .
(b ) Basoph i ls (Tables 13.1 and 13 .2) bind basic dyes and typically stain blue. They include three subtypes: corticotrophs, thyrotrophs, and gonadotrophs. 1 . Corticotrophs constitute about 10% of the chromophil population. They produce
pro-opiomelanocortin (POMC) whose by-products are adrenocorticotrop ic hormone (ACTH), melanocyte-stimulating hormone (MSH), and l i potropic
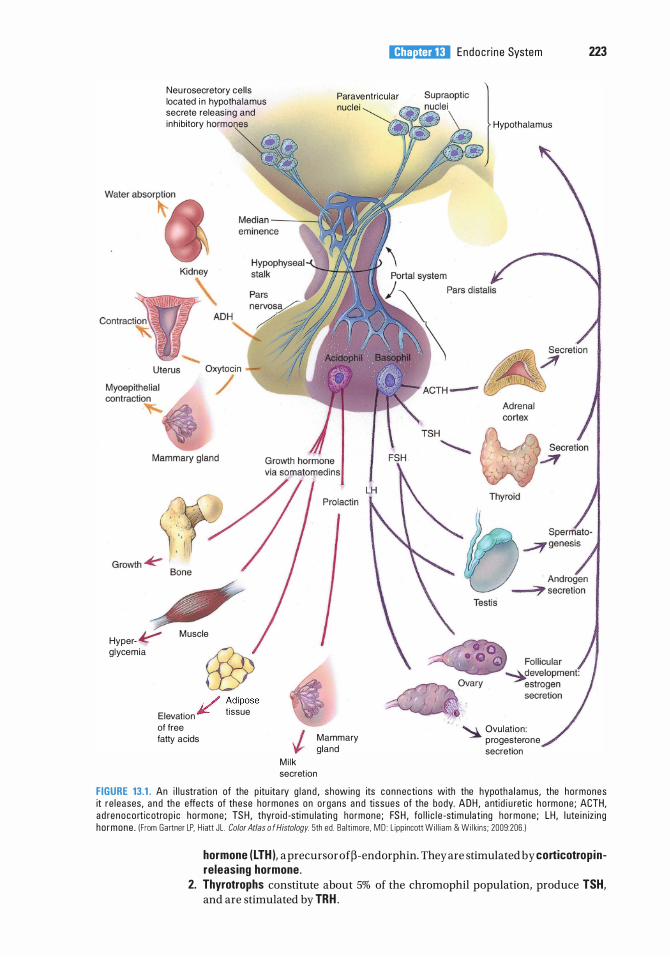
Hyper- � glycemia
Neu rosecretory cel ls located i n hypothalamus secrete releas ing and inh ibitory hnnmnr''"'
M uscle
, / Adipose
Elevation JC t issue
of free fatty acids
l!iitJ'!1tilU Endoc ri n e System 223
Parave ntricular nuclei
Mammary gland
M i l k secretion
Hypothalamus
· � Ovulat ion : progesterone secretion
FIGURE 13.1 . An i l l u stration of the p itu ita ry g l a nd , showing its connecti ons with the hypotha l amus, the hormones it re leases, a n d the effects of these hormones on o rgans a n d tissues of the body. ADH , a ntid i u reti c h o rmone ; ACTH, a d renoco rtic otrop i c hormone ; TS H , thyro i d -sti m u lati n g hormone ; FS H , fo l l i c l e -sti m u lat ing hormone ; LH , l ute i n iz i ng ho rmone . I From Gartner LP. H iatt JL . Color Atlas o f Histology. 5th ed . Ba lt imore . MD : L ipp i ncott Wi l l i am & Wi l kins ; 2009:206. )
hormone (LTH ), a precursor of�-endorphin. They are stimulated by corticotrop inreleasing hormone .
2. Thyrotrophs constitute about 5% of the chromophil population, produce TSH, and are stimulated by TRH .
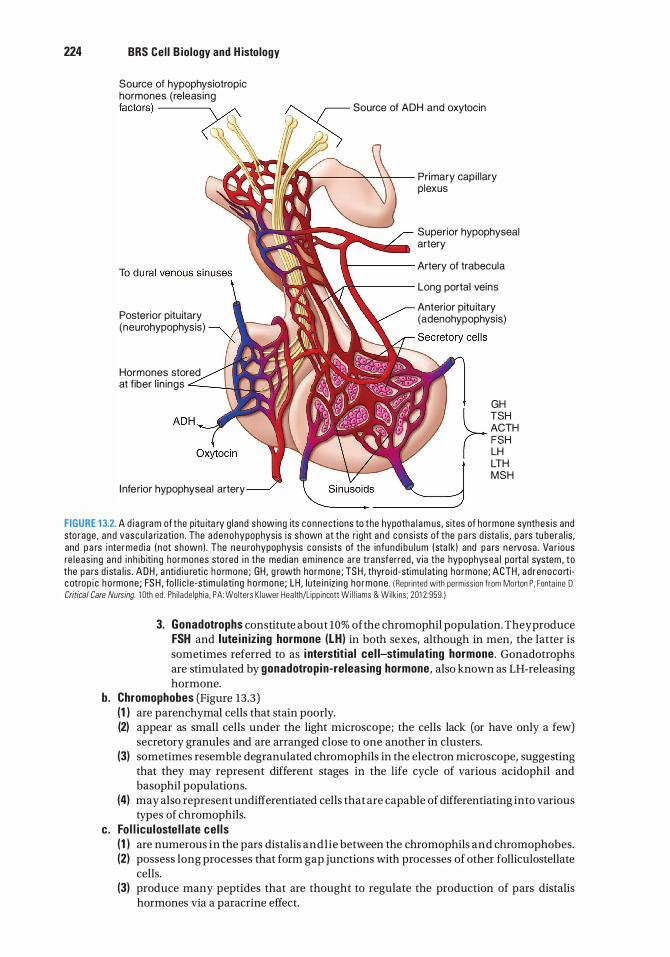
224 BRS Cel l B iology and H istology
Source of hypophysiotropic hormones (releasing factors) --------,. Source of ADH and oxytocin
-�·�� Wit.li?..----�--'<-T-- Primary capi l lary
Posterior pitu itary (neurohypophysis)
Hormones stored at f iber l in ings ---4-....__�-•n•
I nferior hypophyseal artery
plexus
Superior hypophyseal artery
a------ Artery of trabecula
....,...k----- Long portal veins
Anterior pitu itary (adenohypophysis)
GH TSH ACTH FSH LH LTH MSH
FIGURE 1 3.2. A d i a g ra m of the p itu ita ry g land showing its connect ions to the hypoth a l a m us, sites of ho rmone synthes is and sto rage , a nd vasc u l a rizati o n . The aden ohypophysis i s shown at the r ight a nd consists of the p a rs d ista l is , p a rs tu bera l is , and p a rs i nte rmed ia ( n ot shown) . The n e u rohypophysis cons ists of the infund i b u l um (sta lk ) and pa rs n e rvosa . Va r ious re l eas i ng a nd i n h i b iti n g ho rmones sto red i n the med ian em i nence are tra nsferred , v ia the hypophysea l po rta l system, to the pa rs d i sta l i s . ADH , a nti d i u reti c h o rmone ; GH , g rowth hormone ; TS H , thyro id -stimu l at ing ho rmone; ACTH, ad renoco rtic otrop i c h o rmone ; FS H , fo l l i c l e-stimu lati ng h o rmone ; LH , lute i n iz i ng ho rmone . IRepr inted with permiss ion from Morton P. Fonta ine D. Critical Care Nursing. 1 0th ed . Ph i l ade lph ia . PA: Wolters K l uwer Hea lth/L ipp incott Wi l l iams & Wilk ins ; 201 2 :959. )
3. Gonadotrophs constitute about 10% ofthe chromophil population. They produce FSH and lute in iz ing hormone (LH) in both sexes, although in men, the latter is sometimes referred to as i nterstit ia l cel l-stimulating hormone. Gonadotrophs are stimulated by gonadotrop in-releasing hormone, also known as LH-releasing hormone.
b. Chromophobes (Figure 13.3) (1 ) are parenchymal cells that stain poorly. (2) appear as small cells under the light microscope; the cells lack (or have only a few)
secretory granules and are arranged close to one another in clusters. (3) sometimes resemble de granulated chromophils in the electron microscope, suggesting
that they may represent different stages in the life cycle of various acidophil and basophil populations.
(4) may also represent undifferentiated cells that are capable of differentiating into various types of chromophils.
c. Fo l l icu loste l l ate cel ls (1 ) are numerous in the pars distalis and l ie between the chromophils and chromophobes. (2) possess long processes that form gap junctions with processes of other folliculostellate
cells. (3) produce many peptides that are thought to regulate the production of pars distalis
hormones via a paracrine effect.
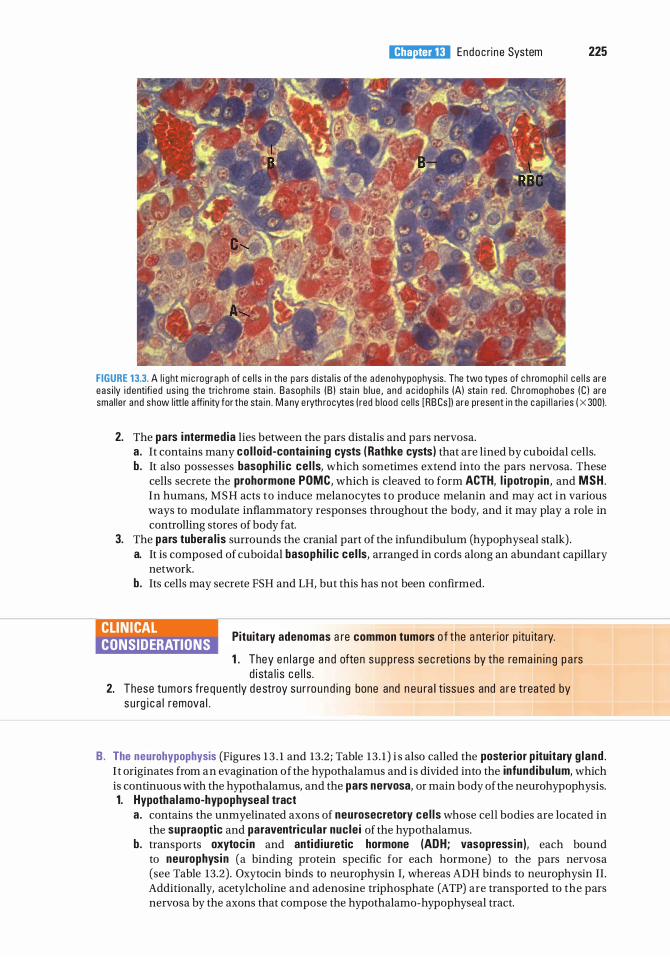
l!iitJ'!1tilU Endoc ri n e System 225
FIGURE 13.3. A l i ght m i c rog raph of ce l l s i n the p a rs d ista l i s of the adenohypophysis . The two types of c h romoph i l ce l l s a re eas i ly i dentifi ed us ing the tri c h rome sta i n . Basoph i l s (B ) sta i n b l ue , a nd a c idoph i l s (A) sta in red . Chromophobes (C ) are sma l ler and show l ittle affin ity for the sta i n . M a ny e ryth rocytes ( red b l ood ce l ls [RB Cs]) a re present i n the c ap i l l a ries ( X 300).
2. The pars intermedia lies between the pars distalis and pars nervosa. a. It contains many co l lo id-conta in ing cysts ( Rathke cysts) that are lined by cuboidal cells. b. It also possesses basoph i l i c ce l ls, which sometimes extend into the pars nervosa. These
cells secrete the prohormone POMC, which is cleaved to form ACTH, l i potrop in , and MSH. In humans, MSH acts to induce melanocytes to produce melanin and may act in various ways to modulate inflammatory responses throughout the body, and it may play a role in controlling stores of body fat.
3. The pars tubera l is surrounds the cranial part of the infundibulum (hypophyseal stalk) . a. It is composed of cuboidal basoph i l i c cel ls, arranged in cords along an abundant capillary
network. b. Its cells may secrete FSH and LH, but this has not been confirmed.
CLIN ICAL CONSIDERATIONS
Pituitary adenomas a re common tumors o f the a nte r ior p itu ita ry.
1 . They e n l a rg e a n d often s u p p ress sec reti ons by the rema i n i n g p a rs d i sta l i s c e l l s .
2. These tumo rs fre q uently destroy su r ro und i n g bone and n e u ra l t issues and a re treated by s u rg i c a l remova l .
B. The neurohypophysis (Figures 1 3 . 1 and 13.2; Table 13 . 1 ) i s also called the poster ior p ituitary g land . I t originates from an evagination of the hypothalamus and i s divided into the infund ibu lum, which is continuous with the hypothalamus, and the pars nervosa, or main body of the neurohypophysis. 1. Hypotha lamo-hypophyseal tract
a . contains the unmyelinated axons of neurosecretory ce l ls whose cell bodies are located in the supraoptic and paraventricu lar nucle i of the hypothalamus.
b. transports oxytoc in and antid iuretic hormone (ADH; vasopress in ), each bound to neurophysin (a binding protein specific for each hormone) to the pars nervosa (see Table 13.2) . Oxytocin binds to neurophysin I, whereas ADH binds to neurophysin II . Additionally, acetylcholine and adenosine triphosphate (ATP) are transported to the pars nervosa by the axons that compose the hypothalamo-hypophyseal tract.
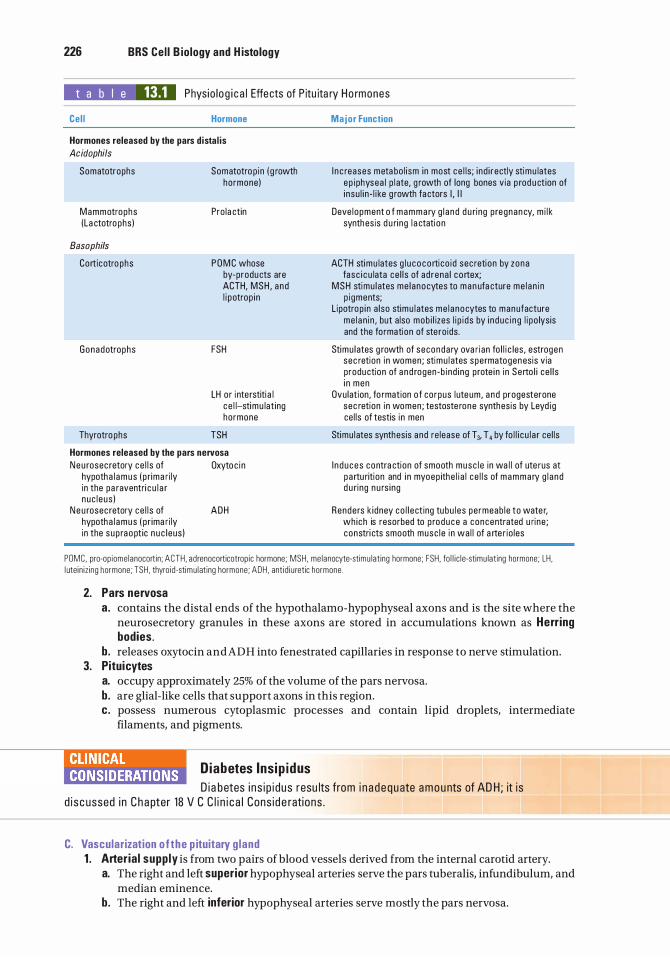
226 BRS Cel l B iology and H istology
t a b I e 13.1 Phys io lo g i c a l Effects of P itu ita ry Ho rmones
Cel l Hormone
Hormones released by the pars d istal is Acidophils
Somatotrophs
Mammotrophs (La ctotrophs )
Basophi/s
Corticotrophs
Gonadotrophs
Thyrotrophs
Somatotrop in ( g rowth hormone )
Pro la ctin
P O M C whose by-products are ACTH, MSH , a nd l i potrop in
FSH
LH or i nte rstiti a l c e l l-stimu lat ing hormone
TSH
Hormones released by the pars nervosa Neu rosec retory ce l l s of Oxytoc i n
hypotha l amus ( p rima r i ly in the pa raventri c u l a r nuc l eus )
Ne u rosec retory ce l l s of AOH hypotha l amus ( p r ima r i ly in the sup raopt ic n u c leus )
Major Function
I n c reases meta bo l i sm in most ce l ls ; i nd i rectly stimu lates ep iphysea l p l ate, g rowth of long bones via p rod u ct ion of i nsu l i n - l i ke g rowth fa ctors I , I I
Deve lopment o f mammary g l a nd d u ring p regnan cy, m i l k synthes is d u ri ng l a ctation
ACTH stimu lates g l u coco rti co id sec retion by zona fasc i c u lata ce l l s of ad rena l c o rtex;
MSH stimu l ates me l anocytes to man ufa cture me l an i n p i gments;
L ipotrop in a lso stimu l ates me l a nocytes to manufacture me l a n in , but a lso mob i l izes l i p i ds by i n duc i n g l i po lysis and the fo rmation of ste ro ids .
Stimu l ates g rowth of seconda ry ova r ian fo l l i c les , estrogen sec retion i n women ; stimu l ates spermatogenesis via production of a n d rogen -b i nd i ng p rote i n i n Serto l i ce l l s i n men
Ovu lat ion, fo rmation o f corpus l ute um, a nd progesterone sec retion i n women ; testoste rone synthesis by Leyd ig ce l ls of testis i n men
Stimu l ates synthesis and re lease of T3, T4 by fo l l i c u l a r ce l ls
I n d u ces contra ction of smooth musc l e in wa l l of ute rus at p a rtu rition and i n myoep ithe l i a l ce l l s of mammary g l a nd d u ring n u rs ing
Renders k idney co l l e ct ing tu bu l es pe rmeab l e to wate r, wh ich is resorbed to p roduce a concentrated u rine ; constri cts smooth musc l e i n wa l l of a rte r io les
POMC. pro-op iome lanocort in ; ACTH . adrenocorticotrop ic hormone; MSH . me lanocyte-stimu lat ing hormone; FSH. fo l l i c l e-stimu lat ing hormone; LH . l utein i z ing hormone ; TSH, thyro id-stimu lat ing hormone ; ADH . ant i d i u retic hormone .
2. Pars nervosa a . contains the distal ends of the hypothalamo-hypophyseal axons and is the site where the
neurosecretory granules in these axons are stored in accumulations known as Herring bodies.
b . releases oxytocin and ADH into fenestrated capillaries in response to nerve stimulation. 3. Pituicytes
a. occupy approximately 25% of the volume of the pars nervosa. b. are glial-like cells that support axons in this region. c. possess numerous cytoplasmic processes and contain lipid droplets, intermediate
filaments, and pigments.
Diabetes Insip i dus D i a betes i n s i p i dus resu lts from i n a dequate a m o u nts of AD H ; it is
d i s c ussed i n C h apter 18 V C C l i n i c a l Cons id e rati ons .
C. Vascularization o f the p ituitary g land 1 . Arteria l supp ly is from two pairs of blood vessels derived from the internal carotid artery.
a. The right and left superior hypophyseal arteries serve the pars tuberalis, infundibulum, and median eminence.
b. The right and left inferior hypophyseal arteries serve mostly the pars nervosa.
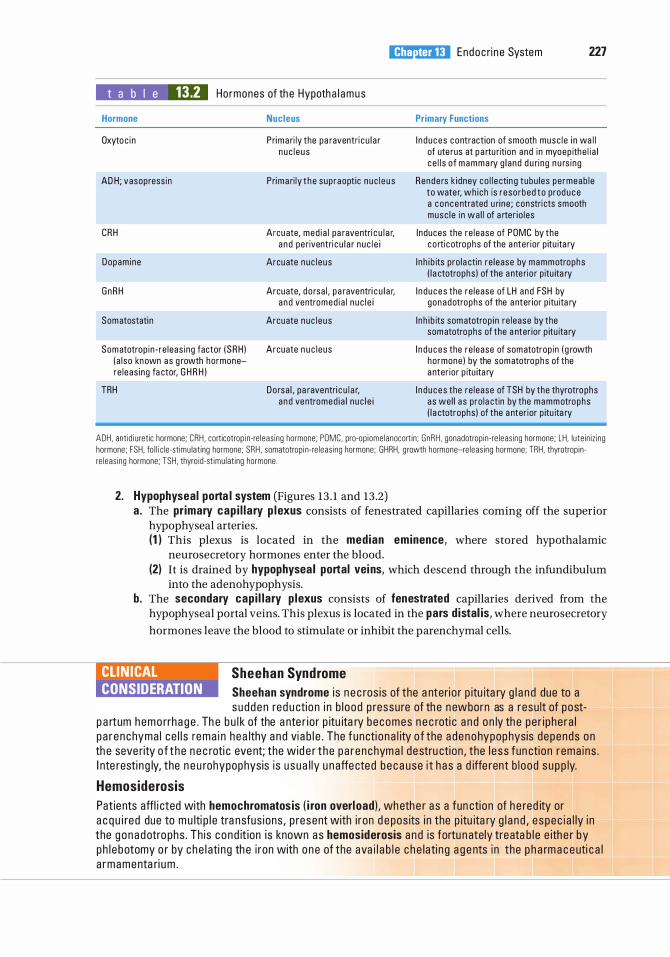
l!iitJ'!1tilU Endoc ri n e System 227
t a b I e 13.2 Hormones of th e Hypoth a l amus
Hormone
Oxytoc i n
AD H ; vasopress in
CRH
Dopamine
GnRH
Somatostati n
Somatotrop in - re leas ing factor ( SRH ) ( a l so known as g rowth hormonere leas ing fa ctor, G H R H )
TRH
Nucleus
Prima ri ly the pa raventri c u l a r n u c l e u s
Prima ri ly t he sup raopt ic n u c l e u s
Arcuate, med i a l pa raventri c u l a r, a n d pe riventri c u l a r n u c l e i
Arcuate nuc l e us
Arcuate, d o rsa l , p a raventri c u l a r, a n d ventromed i a l n u c l e i
Arcuate nuc l e us
Arcuate n u c leus
Do rsa l , pa raventri c u l a r, a n d ventromed i a l n u c l e i
Primary Functions
I n d uces contraction of smooth musc l e i n wa l l of ute rus at p a rtu riti on and i n myoep ithe l i a l c e l l s o f mamma ry g l a nd d u ring n u rs i ng
Rende rs k idney co l l e cti n g tubu les pe rmeab l e to wate r, wh ich is reso rbed to prod u ce a concentrated u ri ne ; constri cts smooth musc l e i n wa l l of a rter io les
I nduces the re lease of POMC by the co rti c otro phs of the a nter ior p itu ita ry
I nh i b its pro la ctin re lease by mammotrophs ( l a ctotrophs ) of the a nte ri o r p itu ita ry
I n duces the re lease of LH and FSH by gonadotrophs of the a nter ior p itu ita ry
I nh i b its somatotrop in re lease by the somatotrophs of the a nter ior p itu ita ry
I n d u ces the re lease of somatotrop in ( g rowth hormone ) by the somatotrophs of the a nter ior p itu ita ry
I n d u ces the re lease of TSH by the thyrotro phs as wel l a s pro la ctin by the mammotrophs ( l a ctotrophs ) of the a nter ior p itu ita ry
ADH, anti d i u retic hormone; CRH , corticotrop i n-re leas ing hormone; PDMC, pro-op iome lanocortin; GnRH , gonadotrop in-re leas ing hormone; LH, lute in iz ing hormone; FSH, fo l l i c le-stimu lat ing hormone; SRH , somatotrop i n-re leas ing hormone; GHRH, g rowth hormone-re leas ing hormone; TRH, thyrotrop inre leas ing hormone; TSH, thyro id-st imu lat ing hormone.
2. Hypophyseal porta l system (Figures 13 . 1 and 13 .2) a. The primary cap i l l a ry p lexus consists of fenestrated capillaries coming off the superior
hypophyseal arteries. (1 ) This plexus is located in the median eminence, where stored hypothalamic
neurosecretory hormones enter the blood. (2) It is drained by hypophysea l portal veins, which descend through the infundibulum
into the adenohypophysis. b. The secondary cap i l lary p lexus consists of fenestrated capillaries derived from the
hypophyseal portal veins. This plexus is located in the pars d istal is, where neurosecretory
hormones leave the blood to stimulate or inhibit the parenchymal cells.
CLIN ICAL CONSIDERATION
Sheehan Syndrome Sheehan syndrome i s n e c ros is of the a nteri o r p itu ita ry g l a n d due to a s u d den red u ctio n i n b l ood p ressure of th e n ewborn as a resu lt of post
p a rtum hemo rrha g e . Th e b u l k of the a nte r io r p itu ita ry becomes n e c roti c a n d on ly th e pe r i phe ra l p a r enchyma l ce l l s rema i n hea lthy a n d vi a b l e . The functi o na l ity o f the a denohypophysis depends on th e seve rity o f t he n e c roti c eve nt; the wid e r t he pa r enchyma l d estru ction , the l e s s fun ction rema i ns . I nte resti n g ly, the n e u rohypophysis is u sua l ly u n affe cted b e c a use i t h as a d iffe rent b l ood s u p p ly.
Hemosiderosis Patients affl i cted with hemochromatos is ( i ron overload) , whethe r a s a fun cti on of h e red ity or a c q u i re d due to m u lti p l e tra nsfus ions , p resent with i ron d e pos its i n the p itu ita ry g l a n d , e spec i a l ly i n the g onadotro phs . Th is cond it ion i s known as hemosiderosis and is fortu n ately treata b l e e ith e r by ph l e botomy o r by c he l ati ng th e i ron with o ne of the ava i l a b l e c h e lati n g a g e nts i n the p h a rm a c e uti c a l a rmamenta ri u m .
228 BRS Cel l B iology and H istology
D . Regulation of the pars d ista l is (Figures 13.1 and 13 .2) 1. Neurosecretory cells in the hypothalamus synthesize specific hormones that enter the
hypophyseal portal system and stimulate or inhibit the parenchymal cells of the pars distalis (see Table 13 .2) .
2. The hypothalamic neurosecretory cells in turn are regulated by the level of hormones in the blood (negative feedback) or by other physiological (or psychological) factors.
3. Some hormones (e.g., thyroid hormones, cortisol) exert negative feedback on the pars distalis directly.
The thyroid gland is composed of two lobes connected by an isthmus. It is surrounded by a dense irregular collagenous connective tissue capsule, in which (posteriorly) the parathyro id g lands are embedded. The thyroid gland is subdivided by capsular septa into lobules containing fo l l i c les . These septa also serve as conduits for blood vessels, lymphatic vessels, and nerves.
A. Thyroid fol l i c les are spherical structures filled with col lo id , a viscous gel consisting mostly of iod inated thyrog lobu l in (Figure 13.5) 1 . Surrounding the colloid within each follicle is a single layer of epithelial cells, called fo l l icu lar
cel ls . In addition, one or more parafo l l icu lar ce l ls occasionally lie sandwiched between the follicular cells. Both of these parenchymal cell types rest upon the basal lamina surrounding the follicle, which separates them from the abundant network offenestrated cap i l l a ries in the connective tissue.
2. Function . Thyroid follicles synthesize, store, and release thyroid hormones.
B. Fo l l icu lar cells (Figure 13 .6) 1. Structure
a . Follicular cells are normally cuboidal, but they become columnar when stimulated and squamous when inactive.
b. They possess a distended rough endoplasmic reticulum (RER) with many ribosomefree regions, a supranuclear Golgi complex, many lysosomes, and rod-shaped mitochondria.
c. Follicular cells also contain many small ap ica l vesic les, which are involved in the transport and release of thyroglobulin and enzymes into the colloid.
d . They possess short, blunt microvilli that extend into the colloid. 2. Synthesis and release of the thyro id hormones thyroxine (T4) and tri iodothyron ine (T3) occur
by the sequence of events illustrated in Figure 13 .7 . These processes are evoked by TSH, which binds to G protein-linked receptors on the basal surface of follicular cells.
CLIN ICAL CONSIDERATIONS
Graves d isease i s c h a ra cter ized by a d iffuse en largement o f the thyro id gland and protrusion of the eyebal ls ( exophth a lm i c go iter ) .
1 . Th is d i sease is assoc iated with th e prese n c e of c o l umna r-sh a ped thyro i d fo l l i c u l a r c e l l s, exc essive p rod u ct ion of thyro i d ho rmones, a n d d e c reased amounts of fo l l i c u l a r co l l o i d .
2. I t is c a used by th e b i nd i ng o f a uto immune immunog l obu l i n G ( l gG ) a nti bod i es to TS H re c e pto rs, wh ich stimu l ates th e thyro id fo l l i c u l a r c e l l s . Add iti o na l ly, infl ammato ry c e l ls , s u c h as T c e l ls, n e utro ph i ls, and m a c rophages, inva d e the connective tissues of the retro-orb ita l reg ion a n d re l ease cytoki nes that a ctivate fi b rob l a sts not on ly t o i n c rease th e i r prod u ctio n o f p roteog lycans but a l so to d iffe re ntiate i nto fat ce l l s . S i nce p roteog lycans read i ly attra ct N a+ i ons wh i c h attra ct wate r mo l e c u l es, th e connective tissue vo l ume i n c reases; mo reover, th e a d d itio n a l n umbe r of fat ce l l s a l so a cts to i n c rease th e vo l ume of the retro-o rb ita l c onnective tissue , putting i n c reased pressu re on the b a c k o f the eyeba l l , push i ng i t fo rwa rd, resu lti ng i n p rotrus ion of the eye.
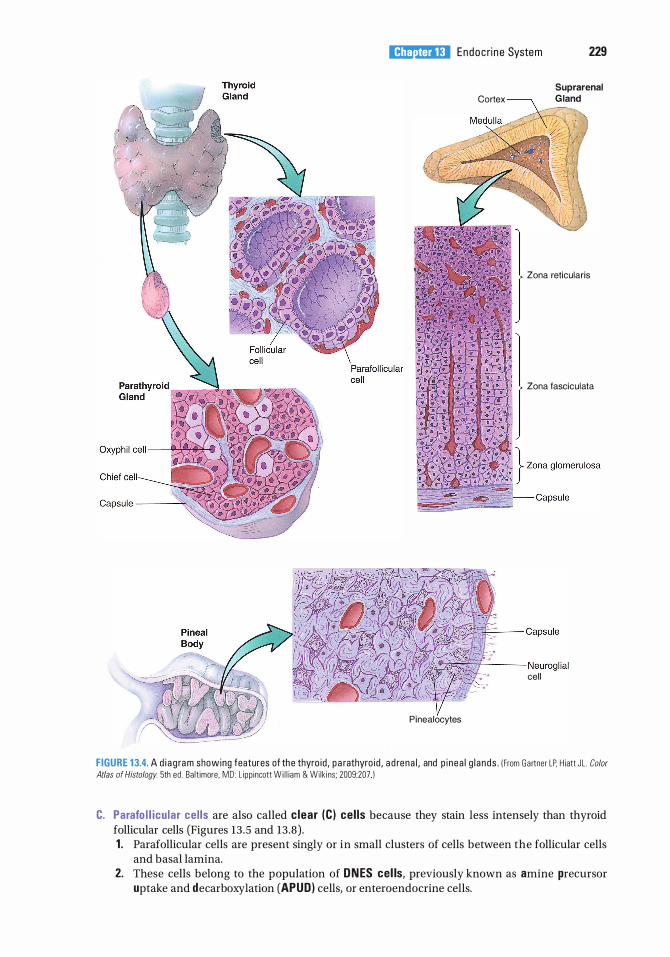
l!iitJ'!1tilU Endoc ri n e System 229
Pinealocytes
Suprarenal
Cortex G land
Zona reticularis
Zona fasciculata
:---'i'----- Neurogl ial cell
FIGURE 1 3.4. A d i a g ra m showing features of the thyro id , p a rathyro id , a d rena l , and p i nea l g l a nds . ( From Gartner LP, H iatt JL . Color
Atlas of Histology. 5th ed . Ba lt imore. MD : L ipp incott W i l l iam & Wilk i ns; 2009:207 )
C. Parafo l l icu lar ce l ls are also called clear (C) cel ls because they stain less intensely than thyroid follicular cells (Figures 13 .5 and 13.8) . 1 . Parafollicular cells are present singly or in small clusters of cells between the follicular cells
and basal lamina. 2. These cells belong to the population of ONES cel ls, previously known as amine precursor
uptake and decarboxylation (APUD) cells, or enteroendocrine cells.
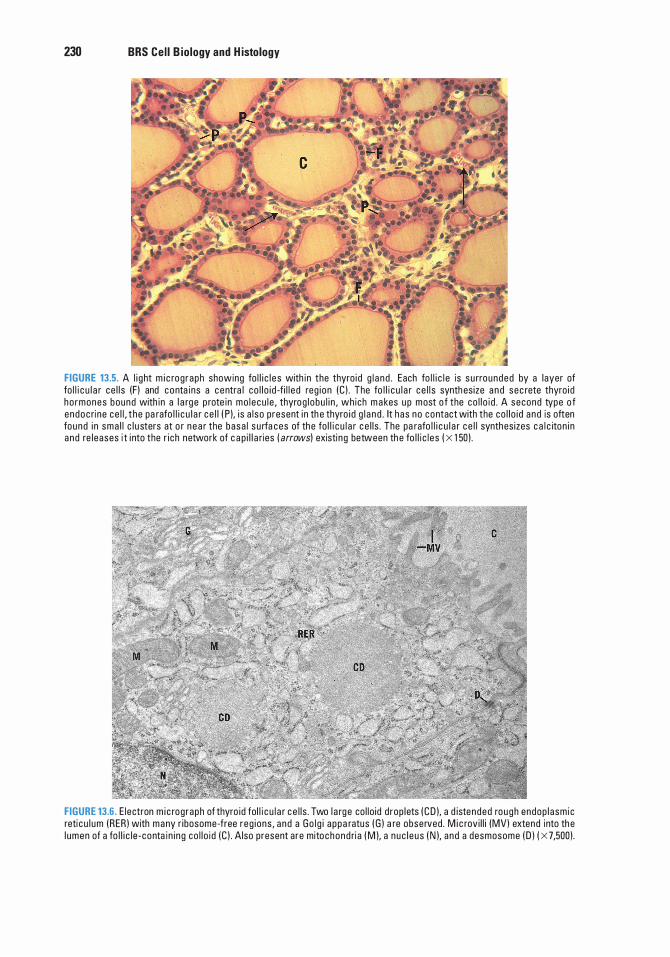
230 BRS Cel l B iology and H istology
FIGURE 13.5. A l i g ht m i c rog raph showing fo l l i c l e s with in the thyro i d g l a n d . Each fo l l i c l e is s u rrounded by a layer of fo l l i c u l a r ce l l s (F ) and c o nta ins a c entra l co l l o i d -fi l l e d reg i on (C ) . The fo l l i c u l a r ce l l s synth es ize a n d sec rete thyro i d ho rmones bound with in a l a rg e p rote in mo l ecu l e , thyrog l obu l i n , wh ich m a kes u p most o f the co l l o i d . A second type o f e ndoc ri ne ce l l , t he pa rafo l l i c u l a r c e l l ( P ). i s a l so present i n th e thyro i d g l a n d . It h as no contact with the co l l o i d a nd is often found i n sma l l c l u sters at o r n e a r the basa l s u rfa ces of the fo l l i c u l a r c e l l s . The pa rafo l l i c u l a r c e l l synthes izes c a l c iton i n a nd re l eases i t i nto the r i ch network of c a p i l l a ries ( arrows) existi ng between th e fo l l i c l es ( X 1 50) .
FIGURE 13.6. E lectron m i c rog raph of thyro id fol l i c u l a r c e l l s . Two l a rg e co l lo id d rop lets ( C D ), a d istended rough endop l asm ic reti c u l um (RER ) with many r ibosome-free reg i ons , a nd a Go l g i a ppa ratus ( G ) a re observed . M i c rov i l l i (MV) extend into th e l umen of a fo l l i c l e - conta i n i ng co l l o i d (C ) . Also present are mitochond ri a ( M ), a nuc l e us ( N ), a nd a desmosome ( D ) ( X 7,500) .
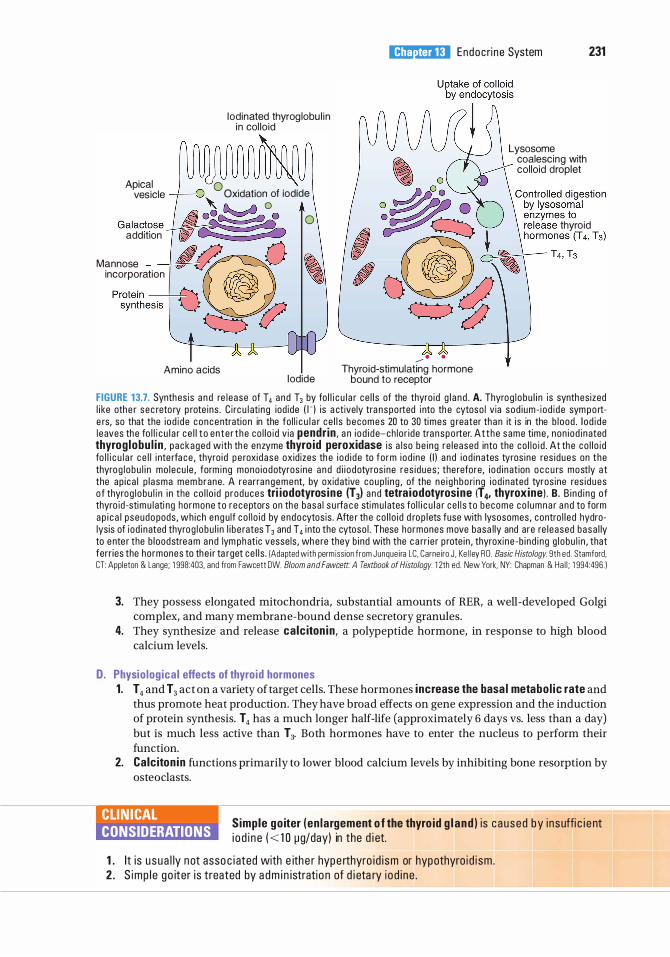
Iodinated thyrog lobu l in in col lo id
Apical 0 . . . . vesicle -� 0 Ox1dat1on of 10d1de
' &... � 0 � -·� · 0 Galactose �#
add1t1on I � Mannose ��0 incorporation I �
Protein ---�- � synthesis V � t;?
l!iitJ'!1tilU Endoc ri n e System 231
� 0 Lysosome
coalescing with .-------'\ col loid droplet
o :::!�t• • •� release thyroid
C:? (;J -- · .
Amino acids Thyroid-stimulating hormone Iodide bound to receptor
FIGURE 13.7. Synthes is a n d re l ease of T4 a nd T3 by fo l l i c u l a r ce l l s of the thyro i d g l a n d . A. Thyrog l obu l i n is synthes ized l i ke othe r sec reto ry p rote ins . C i rc u l atin g iod ide o-l i s a ctively tra nspo rted i nto th e cytoso l via sod i um- i od i de sym p o rte rs, so that the i od i de concentration in the fo l l i c u l a r ce l l s becomes 20 to 30 times g reater tha n it i s in the b l ood . I o d i de l eaves the fo l l i c u l a r c e l l t o en te r t he co l l o i d v ia pendr in , a n i o d i d e-ch lo r i de tra nspo rter. At t he same time , non i od i nated thyrog lobu l in , packaged with th e enzyme thyro id peroxidase i s a l so be i ng re leased into the co l l o i d . At the co l l o i d fo l l i c u l a r c e l l i nte rfa ce , thyro i d pe roxi dase ox id izes th e i od i de to fo rm i od i ne ( I ) and i od i nates tyros i ne res i dues on the thyrog l o bu l i n mo lecu l e , form ing mono i odotyros ine a n d d i i o dotyros ine res i dues ; the refore, i o d i nat ion o c c u rs mostly a t the ap i ca l p l asma mem brane . A rearrangement, by oxid ative coup l i n g , of the ne i g hbo ri ng i od i nated tyros ine res i dues o f thyrog l obu l i n i n the co l l o i d p roduces tri iodotyrosine (T3) and tetra iodotyrosine (14, thyroxine) . B. B i nd i ng o f thyro id -stimu l ati ng hormone to receptors on the basa l s u rfa c e stimu l ates fo l l i c u l a r ce l l s to become co l umna r a nd to form a p i c a l pseudo pods , wh ich eng u lf co l l o i d by endocytos is . Afte r the co l l o i d d rop l ets fuse with lysosomes , contro l l ed hydrolysis of i od i nated thyrog l obu l i n l i b e rates T3 and T4 i nto the cytoso l . These hormones move basa l ly and are re l eased basa l ly to e nte r the b l oodstrea m and lym phatic vesse ls , wh ere they b i nd with the c a rr i e r p rote i n , thyroxi ne -b i nd i ng g l obu l i n , that ferr ies the hormones to the i r ta rget ce l l s . (Adapted with perm iss ion from Junque i ra LC. Carne i ro J . Ke l l ey RO . Basic Histology. 9th ed . Stamford. CT: Appleton & Lange; 1 998:403, and from Fawcett OW. Bloom and Fawcett. A Textbook of Histology. 1 2th ed . New York, NY: Chapman & Ha l l ; 1 994:496 . )
3. They possess elongated mitochondria, substantial amounts of RER, a well-developed Golgi complex, and many membrane-bound dense secretory granules.
4. They synthesize and release calc iton in, a polypeptide hormone, in response to high blood calcium levels.
D. Physio log ica l effects of thyroid hormones 1. T4 and T3 act on a variety of target cells. These hormones increase the basa l metabo l ic rate and
thus promote heat production. They have broad effects on gene expression and the induction of protein synthesis. T 4 has a much longer half-life (approximately 6 days vs. less than a day) but is much less active than T3. Both hormones have to enter the nucleus to perform their function.
2. Calc iton in functions primarily to lower blood calcium levels by inhibiting bone resorption by osteoclasts.
CLIN ICAL CONSIDERATIONS
Simple go iter (en largement o f the thyro id g l and ) i s c aused by i nsuffi c i e nt i o d i n e ( < 1 0 �g/day) in the d i et.
1 . It is u sua l ly not assoc i ated with e ith e r hype rthyro i d i sm or hypothyro i d i sm . 2 . S imp l e go iter i s treated by a d m i n istratio n of d i eta ry i od i ne .
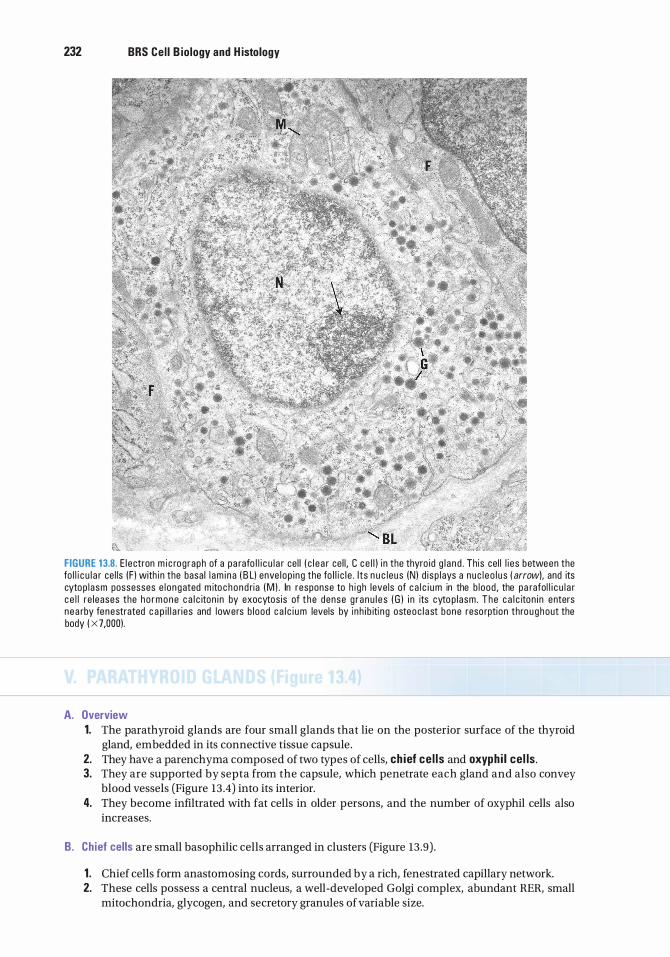
232 BRS Cel l B iology and H istology
FIGURE 13.8. E l ectron m i c rog raph of a pa rafo l l i c u l a r ce l l ( c l e a r ce l l , C c e l l ) i n the thyro id g l a nd . Th is ce l l l i es between the fo l l i c u l a r ce l ls (F ) with in the basa l l am i n a ( B L) enve l op i ng the fo l l i c l e . I ts n u c leus (N) d i sp l ays a n uc l e o l u s ( arrow) , and its cytop l asm possesses e l o ngated m ito c h o n d ria (M ) . In response to h i g h leve ls of c a l c i u m in the b l ood , the pa rafol l i c u l a r c e l l re leases the h o r m o n e c a l c iton i n by exocytos is of t h e dense g r a n u l e s ( G ) i n its cyto p l asm . T h e c a l c iton i n enters nea rby fenestrated c a p i l l a r i es and l owers b l ood c a l c i u m levels by i n h i b iti n g osteoc l a st bone reso rption thro u g h out the body ( X 7,000).
A. Overview 1. The parathyroid glands are four small glands that lie on the posterior surface of the thyroid
gland, embedded in its connective tissue capsule. 2. They have a parenchyma composed of two types of cells, ch ief ce l ls and oxyph i l ce l ls . 3. They are supported by septa from the capsule, which penetrate each gland and also convey
blood vessels (Figure 13 .4) into its interior. 4. They become infiltrated with fat cells in older persons, and the number of oxyphil cells also
increases.
B. Chief cells are small basophilic cells arranged in clusters (Figure 13 .9) .
1 . Chief cells form anastomosing cords, surrounded by a rich, fenestrated capillary network. 2. These cells possess a central nucleus, a well-developed Golgi complex, abundant RER, small
mitochondria, glycogen, and secretory granules of variable size.
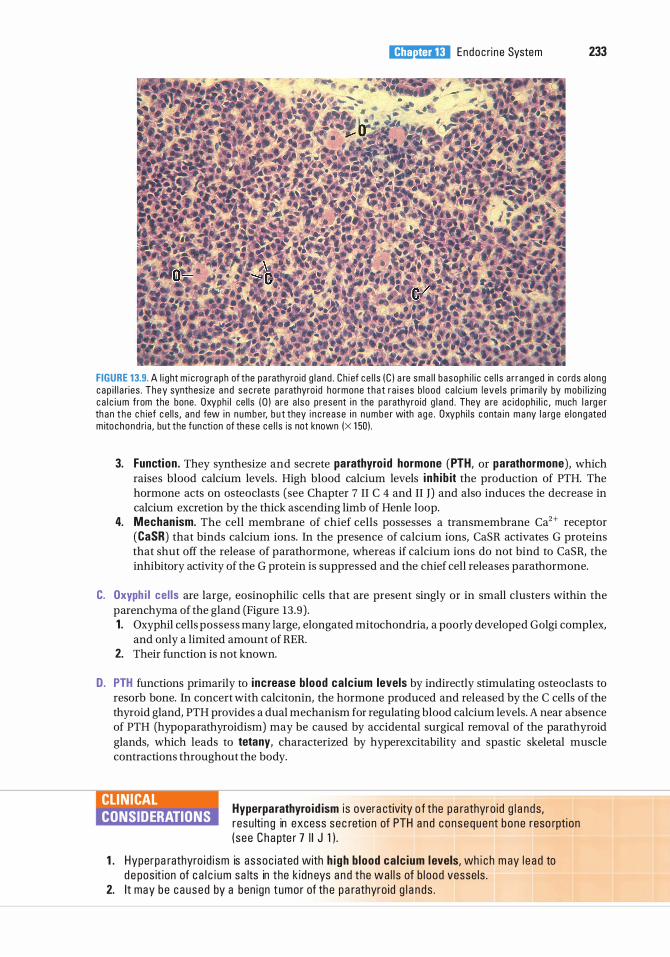
l!iitJ'!1tilU Endoc ri n e System 233
FIGURE 13.9. A l i ght m i c rog raph of the pa rathyroid g l a n d . Ch i ef ce l l s ( C ) a re sma l l basoph i l i c ce l l s a r ranged in c o rds a l ong c ap i l l a r i es . They synthesize a n d sec rete pa rathyro id ho rmone tha t r a i ses b l ood ca l c i um l eve l s pr ima r i ly by mob i l iz ing c a l c i u m from the bone . Oxyph i l ce l l s ( 0 ) are a l so present i n the pa rathyro id g l a nd . They a re a c i d oph i l i c , much l a rg e r th a n t h e c h ief c e l l s , a nd few i n n umbe r, b u t they i n c rease i n n umbe r with a g e . Oxyph i l s c onta i n m a ny l a rg e e l ongated m ito chond ri a , but the fun ction of these ce l l s is not known (X 1 50) .
3. Function . They synthesize and secrete parathyro id hormone (PTH, or parathormone), which raises blood calcium levels. High blood calcium levels i nh ib it the production of PTH. The hormone acts on osteoclasts (see Chapter 7 II C 4 and II J) and also induces the decrease in calcium excretion by the thick ascending limb of Henle loop.
4. Mechan ism. The cell membrane of chief cells possesses a transmembrane Ca2+ receptor (CaSR) that binds calcium ions. In the presence of calcium ions, CaSR activates G proteins that shut off the release of parathormone, whereas if calcium ions do not bind to CaSR, the inhibitory activity of the G protein is suppressed and the chief cell releases parathormone.
C. Oxyph i l ce l ls are large, eosinophilic cells that are present singly or in small clusters within the parenchyma of the gland (Figure 13 .9) . 1 . Oxyphil cells possess many large, elongated mitochondria, a poorly developed Golgi complex,
and only a limited amount of RER. 2. Their function is not known.
D. PTH functions primarily to increase b lood ca lc ium levels by indirectly stimulating osteoclasts to resorb bone. In concert with calcitonin, the hormone produced and released by the C cells of the thyroid gland, PTH provides a dual mechanism for regulating blood calcium levels. A near absence of PTH (hypoparathyroidism) may be caused by accidental surgical removal of the parathyroid glands, which leads to tetany, characterized by hyperexcitability and spastic skeletal muscle contractions throughout the body.
CLIN ICAL CONSIDERATIONS
Hyperparathyro id ism i s overa ctivity o f the pa rathyro id g l a nds, resu lti n g in excess sec retio n of PTH a n d consequent bone reso rpti on ( see Chapte r 7 I I J 1 ) .
1 . Hyperpa rathyro i d i sm is assoc i ated with h igh b lood ca lc ium levels, wh i c h m ay l e a d to d e pos it ion of c a l c i u m sa lts in the k i dn eys a n d the wa l l s of b l ood vesse ls .
2. It may be caused by a ben ign tumor of th e pa rathyro id g l a n ds .
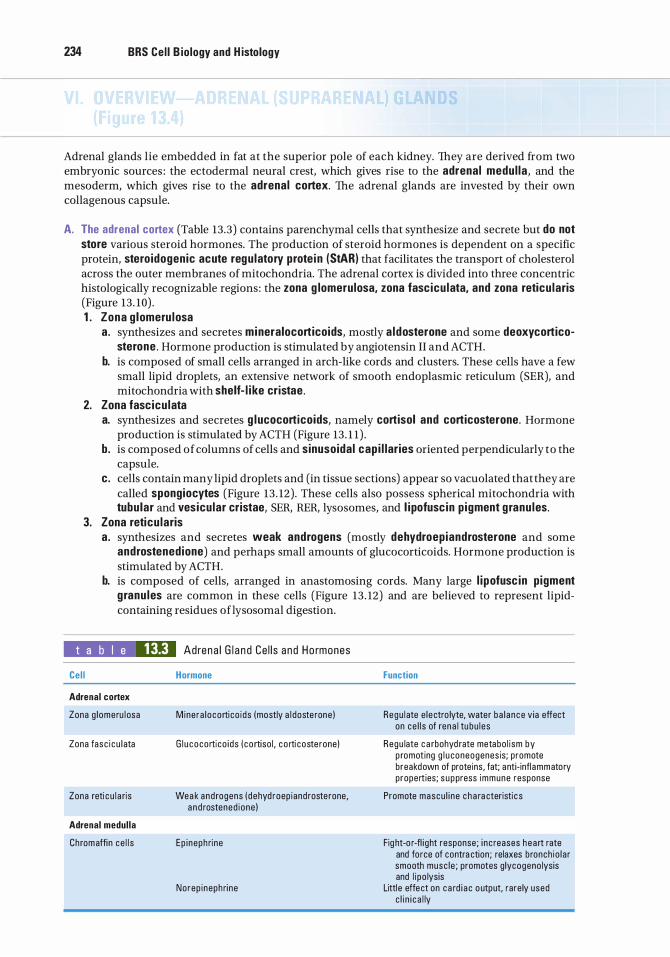
234 BRS Cel l B iology and H istology
Adrenal glands lie embedded in fat at the superior pole of each kidney. They are derived from two embryonic sources : the ectodermal neural crest, which gives rise to the adrenal medul la , and the mesoderm, which gives rise to the adrenal cortex. The adrenal glands are invested by their own collagenous capsule.
A. The adrenal cortex (Table 13.3) contains parenchymal cells that synthesize and secrete but do not store various steroid hormones. The production of steroid hormones is dependent on a specific protein, stero idogenic acute regu latory prote i n (StAR) that facilitates the transport of cholesterol across the outer membranes of mitochondria. The adrenal cortex is divided into three concentric histologically recognizable regions : the zona g lomerulosa, zona fasc icu lata, and zona reticu laris (Figure 13 . 10) . 1 . Zona g lomeru losa
a . synthesizes and secretes mineralocorticoids, mostly a ldosterone and some deoxycorticosterone . Hormone production is stimulated by angiotensin II and ACTH.
b. is composed of small cells arranged in arch-like cords and clusters. These cells have a few small lipid droplets, an extensive network of smooth endoplasmic reticulum (SER), and mitochondria with shelf- l i ke cristae .
2. Zona fasc icu lata a. synthesizes and secretes g lucocorticoids, namely cortisol and corticosterone. Hormone
production is stimulated by ACTH (Figure 13 . 1 1 ) . b. is composed of columns of cells and sinusoidal cap i l lar ies oriented perpendicularly to the
capsule. c. cells contain many lipid droplets and (in tissue sections) appear so vacuolated that they are
called spongiocytes (Figure 13 . 12) . These cells also possess spherical mitochondria with tubu lar and vesicu lar cristae, SER, RER, lysosomes, and l ipofusc in p igment g ranu les.
3. Zona reticu laris a . synthesizes and secretes weak androgens (mostly dehydroepiandrosterone and some
androstenedione) and perhaps small amounts of glucocorticoids. Hormone production is stimulated by ACTH.
b. is composed of cells, arranged in anastomosing cords. Many large l i pofusc in p igment g ranu les are common in these cells (Figure 13 . 12) and are believed to represent lipidcontaining residues oflysosomal digestion.
t a b I e 13.3 Cel l
Adrenal cortex
Zona g l omeru l osa
Zona fasc i c u l ata
Zona reti c u l a ris
Adrenal medul la
Chromaffi n ce l l s
Adrena l G l a n d Ce l l s a nd Ho rmones
Hormone
Mine ra l oco rti co i ds (mostly a l doste rone )
G l u cocorti co i ds ( co rtiso l , c o rti coste rone )
Wea k and rogens ( dehyd roep iand roste rone, a n d rostened i one )
Ep i neph ri ne
Norep i neph ri ne
Function
Regu l ate e l e ctro lyte, water b a l a nce v ia effect on ce l l s of ren a l tu bu l es
Regu late c a rbohyd rate metabo l i sm by p romoting g l u coneogenes is; promote breakdown of proteins, fat; anti· infl ammatory properties; s u ppress immune response
Promote mascu l i n e c h a ra cteristi c s
Fig ht·o r·fl i ght response; i n c reases hea rt rate and fo rce of contra ction; relaxes b ronch io l a r smooth musc l e ; promotes g lycogeno lysis and l i po lysis
Littl e effe ct on c a rd i a c o utput, rare ly used c l i n i c a l ly
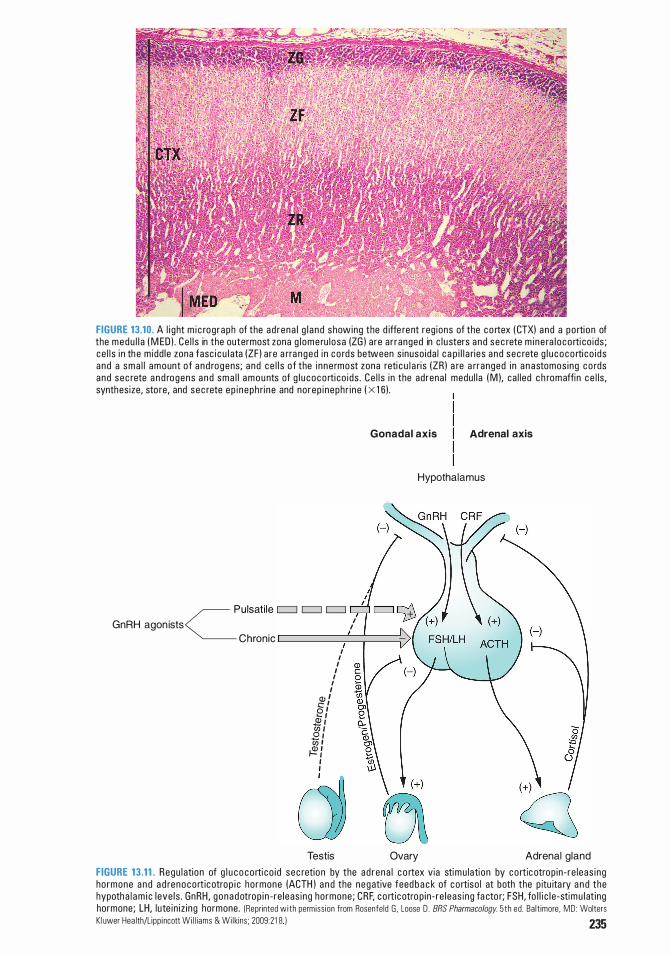
FIGURE 13.10. A l i g ht m i c rog raph of the ad rena l g l a n d showing the d iffe rent reg ions of the c o rtex ( CTX) a nd a po rti on of the medu l l a ( M ED ) . Ce l l s in the outermost zona g l ome ru l osa (ZG ) a re a r ranged in c l u sters a nd sec rete m i n e ra l o co rti co ids ; ce l l s i n th e m idd le zona fasc i c u l ata (ZF ) a re a rra nged i n c o rds between s inuso ida l c a p i l l a ri es a nd sec rete g l u c o c o rti co i ds a nd a sma l l amount o f a n d rogens; a nd ce l l s o f the i n ne rmost zona reti c u l a ri s (ZR ) a re a rranged i n a n astomos ing c o rds and sec rete a n d rogens a n d sma l l a m o u nts of g l u coco rti co ids . Ce l l s i n the adrena l medu l l a ( M ), ca l l ed c h romaffin c e l ls , synthesize, sto re, and sec rete ep i neph ri n e and no rep i neph r i ne ( X 1 6) .
Gonadal axis Adrenal axis
Hypothalamus
GnRH agon ists / CPulsat i le c:::::J c:::::J c:::::J
Chronic c:=====:-�==� I
I I
I I I I I
� � e : 2 1 (/J f 0 1 '/ii i
� : I I
(] � Testis Ovary Adrenal gland
FIGURE 13.11. Regu l ation of g l u c o co rti co i d sec retion by the ad rena l c o rtex via stimu lati on by co rtic otrop in - re l eas ing ho rmone a n d a d renoco rt ic otrop i c ho rmone (ACTH ) a n d the negative feed b a c k of co rtiso l at both the p itu ita ry a n d the hypoth a l a m i c l eve l s . GnRH , gonadotrop i n - re leas ing hormone ; CRF, co rt icotro p in - re l eas ing fa cto r; FSH, fo l l i c l e -stimu l at ing hormone; LH, lute in i z i ng hormone . (Reprinted w i th permiss ion from Rosenfeld G . Loose D . BRS Pharmacology. 5th ed . Ba lt imore . MD : Wolters Kl uwer Hea lth/L ipp i ncott W i l l i ams & Wi l kins; 2009:2 1 8 ) 235
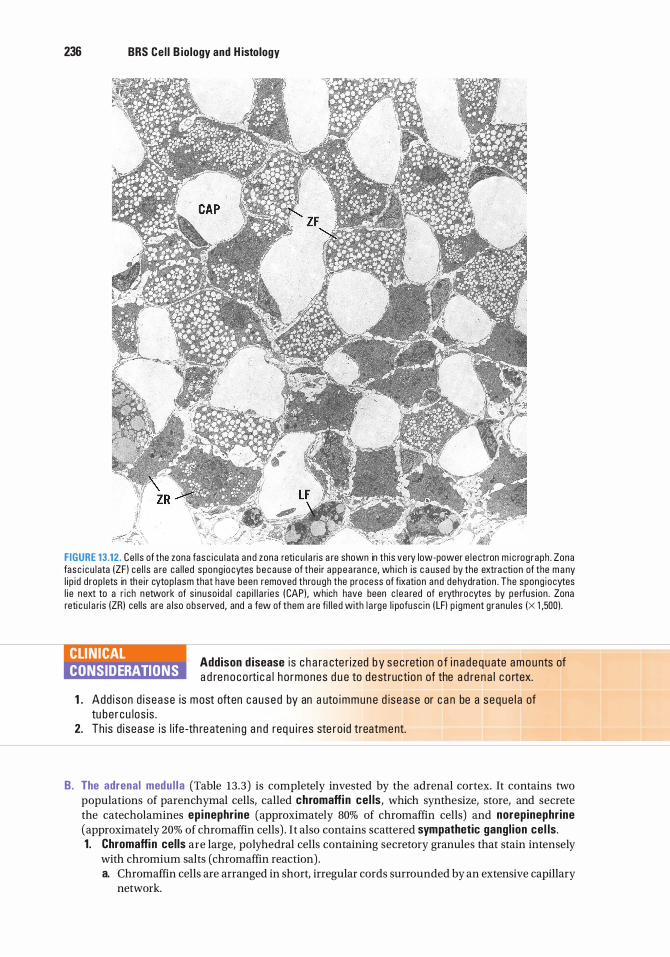
236 BRS Cel l B iology and H istology
!' . . F.Z::.\ FIGURE 13.12. Ce l l s of the zona fasc i cu l ata a nd zona reti c u l a ri s a re shown in th is very low-power e l ectron m i c rog raph . Zona fasc i cu l ata (ZF ) ce l l s a re ca l led spong io cytes because of the i r a ppea ra n c e, wh i c h is c a used by the extra cti on of the m a ny l i p i d d rop lets in the i r cytop lasm that have been removed through the process of fixation and dehydrati on . The spong iocytes l i e next to a r i ch n etwork of s i nuso ida l c ap i l l a ries ( CAP) , which have been c l e a red of e rythrocytes by pe rfus ion . Zona reti c u l a ris (ZR) cel ls are a lso observed, and a few of them a re fi l l ed with l a rge l i pofusc in ( LF) p i gment g ranu les (X 1 ,500) .
CLINICAL CONSIDERATIONS
Addison d isease i s c h a ra cte r ized by sec reti on o f i n a d equate a m o u nts of a d re noco rti c a l ho rmones d u e to destructi on of the a d re n a l c o rtex.
1 . Add ison d i sease is most often c aused by an a uto immune d isease or c a n be a seque l a of tu be r cu los is .
2. Th is d isease is l ife -th re aten i n g a n d req u i res ste ro id treatm ent.
B. The adrenal medu l la (Table 13.3) is completely invested by the adrenal cortex. It contains two populations of parenchymal cells, called chromaffin cel ls, which synthesize, store, and secrete the catecholamines ep inephr ine (approximately 80% of chromaffin cells) and norepinephr ine (approximately 20% of chromaffin cells) . I t also contains scattered sympathetic gangl ion cel ls . 1 . Chromaffin cel ls are large, polyhedral cells containing secretory granules that stain intensely
with chromium salts (chromaffin reaction) . a. Chromaffin cells are arranged in short, irregular cords surrounded by an extensive capillary
network.
l!iitJ'!1tilU Endoc ri n e System 237
b. They are innervated by pregang l ion ic sympathetic (cho l inergic) f ibers, making these cells analogous in function to postganglionic sympathetic neurons.
c. They possess a well-developed Golgi complex, isolated regions of RER, and numerous mitochondria.
d. They also contain large numbers of membrane-bound granules containing one of the catecholamines, ATP, enkephalins, and chromogran ins, which may function as binding proteins for epinephrine and norepinephrine.
2. Catecholamine release occurs in response to intense emotional stimuli and is mediated by the preganglionic sympathetic fibers that innervate the chromaffin cells.
CLIN ICAL CONSIDERATIONS
A pheochromocytoma i s a tumo r a ri s i ng i n cate c ho l am i ne -se c reti ng c h romaffi n ce l l s of the a d re n a l medu l l a . The tu mo r is r a re ; i t is fo und i n
both sexes, a n d 90% of the tim e i t is ben i gn . H oweve r, its s e c retio n of excessive a m o u nts of ep i n e p h ri n e a n d no re p i n e ph ri n e l e ads to hypertension ( ep i sod i c o r susta i n e d ) , a lth o ugh the pati e nt may rema i n a sym ptomati c . I n c reased leve ls of c ate cho l a m i nes a n d th e i r m eta bo l ites in the u ri n e a re d i a g n osti c o f p heoch romocytoma . If the tumo r i s d etected e a rly a n d is su rg i ca l ly removed, t he hype rtens i on i s c o rrecta b le , b ut i f n ot, p ro l o nged a n d susta i n ed hype rtens ion may p rove fata l .
C . B lood supply to the adrenal g lands i s derived from the superior, middle, and inferior adrenal arteries, which form three groups of vessels : to the capsule, to parenchymal cells of the cortex, and directly to the medulla. 1 . Cortical b lood supply
a . A fenestrated capillary network bathes cells of the zona glomerulosa. b. Stra ight, disconti nuous, fenestrated capillaries supply the zona fasciculata and zona
reticularis . 2. Medu l lary b lood supply
a . Venous b lood rich in hormones reaches the medulla via the discontinuous fenestrated capillaries that pass through the cortex.
b. Arteria l b lood from direct branches of capsular arteries forms an extensive fenestrated capillary network among the chromaffin cells of the medulla.
c. Medul lary veins join to form the suprarenal vein, which exits the gland.
A. Overview (Figure 13 .4) 1. The pineal gland projects from the roof of the d iencephalon . 2. Its secretions vary with the light and dark cycles of the day, thereby regulating the individual's
circadian rhythm. Although the pineal gland is buried deep within the head, it receives information about the light and dark conditions from special ganglion cells in the retina of the eye. These ganglion cells send their information about the presence of daylight via the retinohypothalamic tract that projects to the suprachiasmatic nucleus of the hypothalamus, from where information reaches the superior cervical sympathetic ganglion whose postganglionic sympathetic fibers reach the pineal gland by riding on the tunica adventitia of blood vessels that supply the pineal.
3. This gland has a capsule formed of the pia mater, from which septa (containing blood vessels and unmyelinated nerve fibers) extend to subdivide it into incomplete lobules.
4. It is composed primarily of pinealocytes, which constitute approximately 95% of the cells, and neuroglial cells (interstitial cells), which constitute about 5% of the cells.
5. It also contains calcified concretions (b ra i n sand) in its interstitium. The function of these concretions is unknown, but they increase during short light cycles and decrease during periods of darkness.
238 BRS Cel l B iology and H istology
B. P inealocytes are pale-staining cells with numerous long processes that end in dilations near capillaries. 1. Pinealocytes contain many secretory granules, microtubules, microfilaments, and unusual
structures called synaptic r ibbons. 2. These cells synthesize and immediately secrete melaton in but almost only at night. During the
day, melatonin synthesis is mostly inhibited. 3. Pinealocytes may also produce arg in ine vasotocin, a peptide that appears to be an antagonist
ofLH and FSH; they also secrete small quantities of serotonin, histamine, and dopamine. Most of the serotonin manufactured by the pinealocytes is converted to melatonin in a two-step reaction, the first of which is catalyzed by the enzyme N-acetyltransferase. It is the activity of this particular enzyme that is inhibited during daylight conditions, thus preventing the formation of melatonin during daylight.
C. Neurog l ia l ( i nterstitia l ) ce l ls resemble astrocytes, with elongated processes and a small, dense nucleus. They contain micro tubules and many microfilaments and intermediate filaments.
CLINICAL CONSIDERATIONS
Me l aton i n is used t o treat j et l a g a n d seasona l affe ctive d iso rd e r (SAD) , a n emoti o na l response to shorte r day l i ght h ou rs d u ri ng the winte r.
Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1. Protein hormones act initially on target cells by
(A) attaching to receptors on the nuclear membrane.
(B ) attaching to receptors in the nucleolus. (C) diffusing through the plasma membrane. (D) attaching to receptors on the plasma
membrane. (E) attaching to receptors on the rough
endoplasmic reticulum membrane.
2. Which of the following statements concerning adrenal parenchymal cells is true?
(A) Those of the zona fasciculata produce androgens.
(B ) Those of the adrenal medulla produce epinephrine and norepinephrine.
(C) Those of the zona glomerulosa produce glucocorticoids.
(D ) Those of the cortex contain numerous secretory granules.
(E) Those of the zona reticularis produce mineralocorticoids.
3. Characteristics of pinealocytes include which one of the following?
(A) They produce melatonin. (B ) They resemble astrocytes. (C) They contain calcified concretions of
unknown function. (D) They act as postganglionic sympathetic cells. (E ) They are unaffected by dark and light cycles.
4. Prolactin is synthesized and secreted by which of the following cells?
(A) Acidophils in the pars distalis (B ) Basophils in the pars tuberalis (C ) Somatotrophs in the pars distalis (D ) Basophils in the pars intermedia (E) Gonadotrophs in the pars distalis
5. ACTH is produced by which of the following cells?
(A) Chromophobes in the pars distalis (B ) Neurosecretory cells in the median
eminence (C) Basophils in the pars distalis (D ) Neurons of the paraventricular nucleus
in the hypothalamus (E ) Basophils in the pars intermedia
6. The histological appearance of a thyroid gland being stimulated by TSH would show which of the following?
(A) Decreased numbers of follicular cells (B ) Increased numbers of parafollicular cells (C) Column-shaped follicular cells (D ) An abundance of colloid in the lumen of
the follicle (E ) Decreased numbers of parafollicular
capillaries
7. A 40-year-old woman is diagnosed with Graves disease. Which of the following characteristics would be associated with her condition?
(A) Inadequate levels of iodine in her diet (B ) Weight gain (C) Flattened thyroid follicular cells (D ) Excessive production of thyroid hormones (E) Increased amounts of follicular colloid
8. Which one of the following hormones lowers blood calcium levels by inhibiting bone resorption?
(A) Calcitonin (B ) Epinephrine (C) Parathyroid hormone (D ) Prolactin (E ) T3
239
240 BRS Cel l B iology and H istology
9. A 5 1 -year-old man underwent surgery for removal of a carcinoma on his trachea. After surgery, he suffered excessive nervousness, muscle cramps, and spasmodic skeletal muscle contractions in his arms, legs, and feet. Laboratory tests revealed markedly low levels of calcium in his blood. Treatment with intravenous calcium and vitamin D led to recovery in a few weeks. Which one of the following conditions is responsible for these symptoms in this patient following surgery?
(A) Hypothyroidism (B ) Hyperthyroidism (C) Hypoparathyroidism (D ) Graves disease (E) Hyperparathyroidism
10 . Which one of the following hormones plays a role in regulating body temperature by promoting heat production?
(A) Calcitonin (B ) Epinephrine (C ) Parathyroid hormone (D ) Prolactin (E ) Triiodothyronine (T3)
Answers and Explanations
1 . D. Protein hormones initiate their action by binding externally to transmembrane receptor proteins in the target-cell plasma membrane. Receptors for some hormones (e.g., TSH, serotonin, epinephrine) are linked to G proteins; other receptors, including those for insulin and growth hormone, have protein kinase activity (see Chapter 13 II A).
2. B . Chromaffin cells in the adrenal medulla synthesize and store epinephrine and norepinephrine in secretory granules, which also contain ATP, chromogranins, and enkephalins. The cortical parenchymal cells of the zona fasciculata produce glucocorticoids, and those of the zona glomerulosa produce mineralocorticoids. The cortical parenchymal cells do not store their secretory products and thus do not contain secretory granules (see Chapter 13 VI) .
3. A. Pinealocytes, the parenchymal cells of the pineal gland, produce melatonin at night and serotonin during the day. The pineal gland also contains neuroglial cells that resemble astrocytes, and its interstitium has calcified concretions called brain sand (see Chapter 13 VII) .
4. A. Prolactin is produced by mammotrophs, one of the two types of acidophils located in the pars distalis of the pituitary gland. As their name implies, these cells produce a hormone that regulates the development of the mammary gland during pregnancy and lactation (see Chapter 13 III A).
5. C. ACTH is produced by corticotrophs, a type of basophil, present in the pars distalis of the pituitary gland (see Chapter 13 III A) .
6. C. Stimulation of the thyroid gland by TSH causes the follicular cells to become more active and column shaped. They form apical pseudopods and engulf colloid, which is removed from the lumen of the follicle by endocytosis and broken down by controlled lysosomal hydrolysis to yield the thyroid hormones T 3 and T 4• Parafollicular cells and capillaries do not contain receptors for TSH (see Chapter 13 IV) .
7. D. Graves disease (exophthalmic goiter) results in an enlarged thyroid gland due to stimulation of the follicular cells to produce an excessive amount of thyroid hormones by binding of autoimmune antibodies to TSH receptors. Follicular cells actively remove colloid from the lumen of the follicles. Heat intolerance and weight loss are common, but the disease is not caused by iodine deficiency (see Chapter 13 IV B Clinical Considerations) .
8 . A . Calcitonin lowers blood calcium levels and thus has an effect antagonistic to that of parathyroid hormone. It is produced by parafollicular cells of the thyroid gland (see Chapter 13 IV D).
9. C. Upon removal of the carcinoma from his neck, the parathyroid glands were also removed or damaged, causing hypoparathyroidism (a lack of parathyroid hormone that increases blood calcium). Treatment with calcium (and vitamin D, which aids in its absorption) corrected these symptoms. The marked neuromuscular irritability in the absence of calcium reveals its importance in regulating skeletal muscle contraction (see Chapter 13 V D) .
1 0. E. Triiodothyronine (T 3) and thyroxine (T 4) both increase the basal metabolic rate, which affects heat production and body temperature. These thyroid hormones also have many other effects (see Chapter 13 IV D).
241
Skin
A. The skin is the heaviest organ, about 16% of the total body weight.
B. It is composed of two layers, the epidermis and the dermis, which interdigitate to form an irregular contour.
C. A deeper superficial fascial layer, the hypodermis, lies under the skin. This layer, which is not considered part of the skin, consists of loose connective tissue that binds skin loosely to the subjacent tissue.
D. The skin contains several epidermal derivatives (sweat glands, hair follicles, sebaceous glands, nails, and the mammary glands, discussed in Chapter 19) . The skin along with its derivatives is called the i ntegument.
E. Function . The skin protects the body against injury, desiccation, and infection; regulates body temperature; absorbs ultraviolet (UV) radiation, which is necessary for synthesis of vitamin D; and contains receptors for touch, temperature, and pain stimuli from the external environment. Additionally, skin acts as an excretory organ via sebaceous, sweat, and apocrine glands.
A. Overview-Epidermis
242
1 . The epidermis is the superfic ia l layer of the skin. Primarily of ectodermal or ig in , it is classified as stratified squamous kerati n ized epithe l ium. The epidermis is composed predominantly of kerati nocytes and three other types of cells : melanocytes, Langerhans ce l ls, and Merkel cel ls .
2. The epidermis is constantly being regenerated. Regeneration, which occurs approximately every 30 days, is carried out by the mitotic activity of keratinocytes, which normally divide at night.
3. The epidermis has deep downgrowths called epiderma l r idges that i nterd ig itate with projections of the dermis (dermal r idges), resulting in a highly irregular interface. Each dermal ridge is often further subdivided into two secondary dermal ridges by a narrow downgrowth ofthe epidermis, called an i nterpap i l la ry peg. Where the epidermis overlies the dermal ridges,
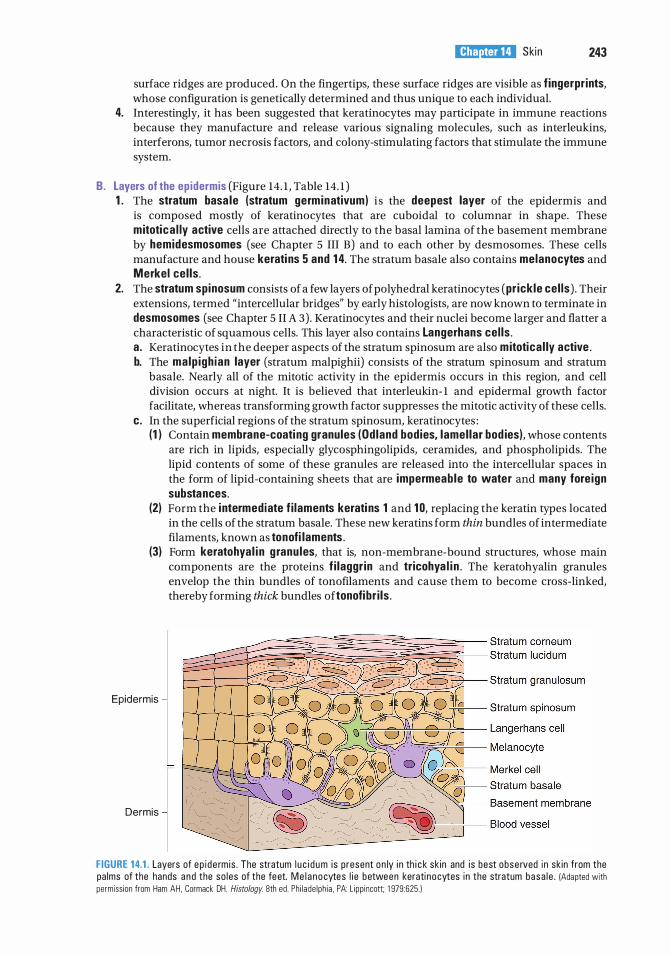
l!1lEl'1lttllJ Ski n 243
surface ridges are produced. On the fingertips, these surface ridges are visible as f ingerprints, whose configuration is genetically determined and thus unique to each individual.
4. Interestingly, it has been suggested that keratinocytes may participate in immune reactions because they manufacture and release various signaling molecules, such as interleukins, interferons, tumor necrosis factors, and colony-stimulating factors that stimulate the immune system.
B. Layers of the ep idermis (Figure 14. 1 , Table 14. 1 ) 1 . The stratum basa le (stratum germinativum) i s the deepest layer of the epidermis and
is composed mostly of keratinocytes that are cuboidal to columnar in shape. These mitotica l ly active cells are attached directly to the basal lamina of the basement membrane by hemidesmosomes (see Chapter 5 III B) and to each other by desmosomes. These cells manufacture and house kerati ns 5 and 1 4. The stratum basale also contains melanocytes and Merkel cel ls .
2. The stratum spinosum consists of a few layers of polyhedral keratinocytes (pr ickle cel ls) . Their extensions, termed "intercellular bridges" by early histologists, are now known to terminate in desmosomes (see Chapter 5 II A 3) . Keratinocytes and their nuclei become larger and flatter a characteristic of squamous cells. This layer also contains Langerhans cel ls . a . Keratinocytes in the deeper aspects of the stratum spinosum are also mitotica l ly active . b. The malp igh ian layer (stratum malpighii) consists of the stratum spinosum and stratum
basale. Nearly all of the mitotic activity in the epidermis occurs in this region, and cell division occurs at night. It is believed that interleukin- 1 and epidermal growth factor facilitate, whereas transforming growth factor suppresses the mitotic activity of these cells.
c. In the superficial regions of the stratum spinosum, keratinocytes : (1 ) Contain membrane-coati ng granules (Od land bodies, lamel lar bod ies), whose contents
are rich in lipids, especially glycosphingolipids, ceramides, and phospholipids. The lipid contents of some of these granules are released into the intercellular spaces in the form of lipid-containing sheets that are impermeable to water and many fore ign substances.
(2) Form the i ntermediate f i laments kerati ns 1 and 10, replacing the keratin types located in the cells of the stratum basale. These new keratins form thin bundles of intermediate filaments, known as tonofi laments .
(3) Form keratohya l i n g ranu les, that is, non-membrane-bound structures, whose main components are the proteins f i laggr in and tricohya l i n . The keratohyalin granules envelop the thin bundles of tonofilaments and cause them to become cross-linked, thereby forming thick bundles oftonofibr i ls .
Epidermis
Dermis
FIGURE 1 4.1 . Layers of ep i de rm is . The stratum l u c i d um is present on ly i n th i c k sk in and i s best obse rved in sk in from the pa lms of the hands and the so les of the feet. Me l a nocytes l i e between kerati nocytes in the stratum basa l e . (Adapted with permiss ion from Ham AH. Cormack DH. Histology. 8th ed . Ph i l ade lph ia . PA: L ipp i ncott; 1 979:625. )
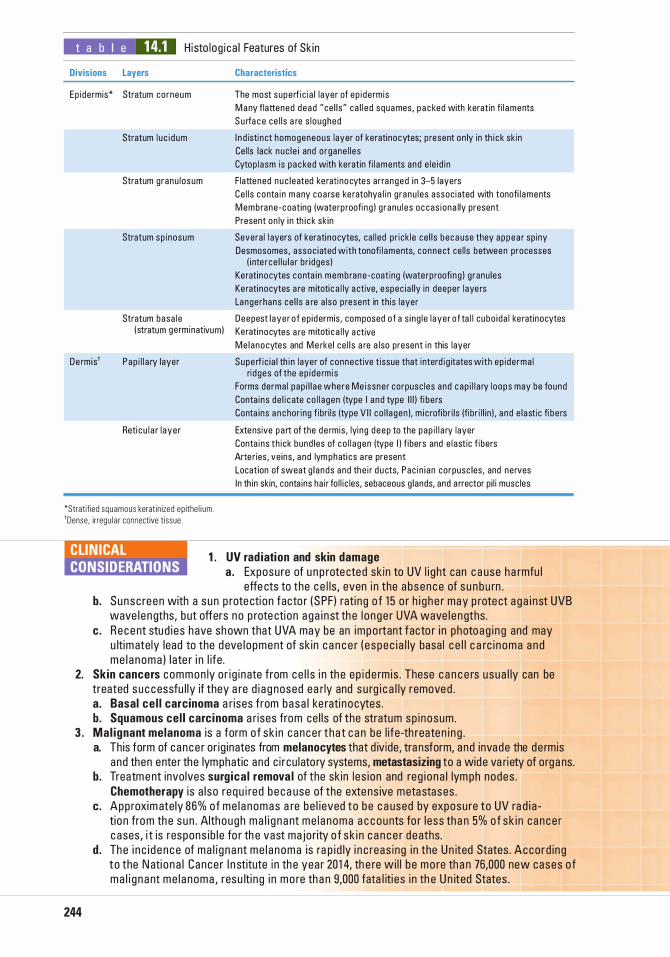
t a b I e 14.1 H isto l og i ca l Features of Sk in
Divisions Layers Characteristics
Ep idermis* Stratum corneum The most supe rf i c i a l l ayer of ep i de rmis
Stratum l u c i d um
Stratum g ranu l osum
Stratum sp i nosum
M a ny f lattened dead "ce l l s" ca l l e d squa mes, p a c ked with keratin f i l aments Su rfa c e ce l l s a re s l oughed
I n d isti nct homogeneous layer of keratinocytes; p resent on ly in th i c k sk in Ce l ls lack nuc l e i and o rgane l l es Cytop l asm is p a c ked with keratin f i l aments and e l e i d i n
F latte ned n u c leated ke rati no cytes a r ra nged i n 3-5 1ayers Ce l l s conta in m a ny coa rse ke ratohya l i n g ranu l es assoc iated with tonofi l aments Membrane -coat ing (waterp roofi n g ) g ranu l es oc cas iona l ly present Present on ly i n th i c k sk in
Severa l l ayers of kerati nocytes, ca l led pr ick le ce l l s beca use they a ppea r sp iny Desmosomes, assoc iated with tonofi l aments, connect ce l ls between processes
( i nte r ce l l u l a r b r i dges ) Kerati nocytes conta i n membrane -coat ing (wate rp roofi n g ) g ranu les Kerati nocytes a re m itoti c a l ly a ctive, espec i a l ly in deeper l aye rs Langerhans ce l l s a re a l so p resent in th is layer
Stratum basa l e Deepest l aye r o f ep id ermis, composed of a s i ng l e l ayer o f ta l l cubo i da l ke ratinocytes (stratum ge rminativum) Kerati nocytes a re m itoti c a l ly a ctive
Me l anocytes and M e rke l ce l l s a re a lso present i n this layer
De rm is' Pap i l l a ry layer Supe rf i c i a l th i n layer of connective t issue that i nterd i g itates with ep i de rma l
Reti c u l a r l aye r
ri d ges of the ep i de rm is Forms derma l pap i l l ae where Me issne r corpusc les and cap i l l a ry l oops may be found Conta i ns de l i c ate co l l a gen (type I a n d type I l l ) fi be rs Conta ins a n chor ing f ibr i ls (type V I I co l l a gen ), m i c rofi br i ls (fib r i l l i n ) , a nd e l astic fi be rs
Extensive part of the d e rmis , lyi ng d eep to the pap i l l a ry layer Conta i ns th ick bund les of co l l a gen (type I ) f ibers and e l astic f ibers Arte r ies, ve ins , a n d lym phati cs a re present Location of sweat g l a nds and the i r d u cts, Pac i n i an corpusc les, and ne rves In th in skin, conta ins ha i r fo l l i c les, sebaceous g lands, and a rrector p i l i musc les
*Stratified squamous kerat in ized ep ithe l i um . 'Dense. irregu l a r connective t issue.
1 . UV rad iation and skin damage a . Exposu re of u n p rote cted sk in to UV l i g ht can c a use ha rmfu l
effe cts to the c e l ls , even i n the a bsence of s u n b u rn . b. Sunsc reen with a s un p rote cti on facto r ( S PF ) rati ng o f 1 5 o r h i g h e r may p rote ct a g a i nst UVB
wave l e ngths, b ut offers no p rote cti on a g a i n st th e l o n ge r UVA wave l e ngths . c. Recent stu d i es h ave shown that UVA may be an impo rtant facto r i n photoag i n g and may
u ltimate ly lead to the d eve l opment of sk in c a n c e r ( e s pec i a l ly basa l c e l l c a rc i n oma a n d me l a noma ) l ate r i n l ife .
2. Skin cancers common ly o r i g i nate from ce l l s i n th e e p i d e rm is . These c a n c e rs u sua l ly can be treated s u c cessfu l ly if they a re d i a g nosed ea rly and s u rg i c a l ly removed . a. Basal ce l l carcinoma a rises from basa l ke rati no cytes . b. Squamous ce l l carc inoma a rises from ce l l s of the stratum sp i nosum .
3 . Mal ignant melanoma i s a form o f sk i n cance r t ha t c a n be l i fe-th reate n i n g .
244
a. This form of cance r or ig inates from melanocytes that d iv ide, tra nsform, and invade the de rmis and then ente r the lymphatic and c i rcu lato ry systems, metastasizing to a wide va riety of orga ns.
b. Treatm e nt invo lves surg ica l remova l of the sk in l es i on and reg i o n a l lym ph nodes . Chemotherapy i s a l so req u i re d b e c a use of the exte ns ive metastases .
c. Approxim ately 86% of me l a nomas a re be l ieved to be c a used by exposu re to UV ra d i a tio n from th e s un . Although m a l i g n a nt me l a noma a c counts fo r l ess tha n 5% o f s k i n c ance r c ases, i t is respons i b l e fo r th e vast ma jo rity o f s k i n c a n c e r d eaths .
d . The i n c i d e n c e of ma l i g n ant me l a noma is ra p i d ly i n c reas i ng i n the U n ited States . Acco rd i ng to the N ati o n a l Cance r I n stitute i n th e yea r 20 1 4, th e re wi l l b e mo re th a n 76,000 new cases o f ma l i g n a nt me l a noma , resu lti n g i n mo re th a n 9,000 fata l iti es i n th e U n ited States .
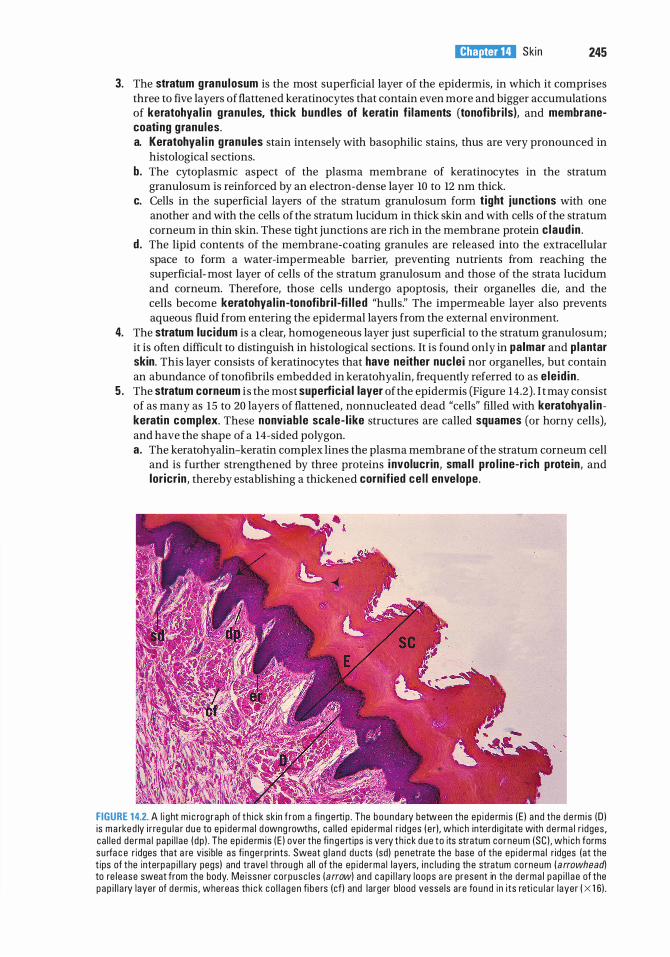
l!1lEl'1lttllJ Ski n 245
3. The stratum granu losum is the most superficial layer of the epidermis, in which it comprises three to five layers of flattened keratinocytes that contain even more and bigger accumulations of keratohya l i n g ranu les, thick bund les of kerat in f i laments (tonofi br i ls), and membranecoating granules. a. Keratohya l i n g ranu les stain intensely with basophilic stains, thus are very pronounced in
histological sections. b. The cytoplasmic aspect of the plasma membrane of keratinocytes in the stratum
granulosum is reinforced by an electron-dense layer 10 to 12 nm thick. c. Cells in the superficial layers of the stratum granulosum form t ight junctions with one
another and with the cells of the stratum lucidum in thick skin and with cells of the stratum corneum in thin skin. These tight junctions are rich in the membrane protein c laud in .
d . The lipid contents of the membrane-coating granules are released into the extracellular space to form a water-impermeable barrier, preventing nutrients from reaching the superficial- most layer of cells of the stratum granulosum and those of the strata lucidum and corneum. Therefore, those cells undergo apoptosis, their organelles die, and the cells become keratohya l in -tonofi br i l -fi l l ed "hulls:' The impermeable layer also prevents aqueous fluid from entering the epidermal layers from the external environment.
4. The stratum luc idum is a clear, homogeneous layer just superficial to the stratum granulosum; it is often difficult to distinguish in histological sections. It is found only in palmar and p lantar skin. This layer consists of keratinocytes that have neither nuc le i nor organelles, but contain an abundance of tonofibrils embedded in keratohyalin, frequently referred to as e le id in .
5 . The stratum corneum i s the most superfic ia l layer ofthe epidermis (Figure 14.2) . I t may consist of as many as 15 to 20 layers of flattened, nonnucleated dead "cells" filled with keratohya l i n kerati n complex. These nonviab le sca le- l ike structures are called squames (or horny cells), and have the shape of a 14-sided polygon. a. The keratohyalin-keratin complex lines the plasma membrane of the stratum corneum cell
and is further strengthened by three proteins i nvolucrin, sma l l pro l ine-r ich prote in, and lor icr in , thereby establishing a thickened cornified ce l l envelope.
FIGURE 1 4.2. A l i g ht m i c rog raph of th i ck sk in f rom a fi n gertip . The bounda ry between the ep i de rm is ! E l a nd the d e rm i s !D l is m a rke d ly i r re g u l a r d u e to ep i de rma l d owng rowths, ca l l ed ep ide rma l r i dges ( e rl , wh i ch interd ig itate with d e rm a l r i dges , ca l l ed de rma l pap i l l ae ( dp l . The ep i de rm is ! E l over the fi n g e rt ips is very th i ck d u e to its stratum co rneum (SC I . wh ich forms su rfa c e r idges that a re v is ib le as fi nge rp rints. Sweat g l a nd d u cts (sdl penetrate the base of the ep i de rma l r idges (at the t ips of the interpap i l l a ry pegsl and trave l thro u g h a l l of the ep i de rma l layers, i n c l u d i n g the stratum co rneum ( a rrowheadl to re l ease sweat from the body. Me issner co rpusc l es ( arrowl and c a p i l l a ry l oops a re present in the de rma l p ap i l l a e of the pap i l l a ry layer of de rmis , whereas th i c k co l l a gen fi b e rs (cfl and larger b lood vesse ls a re fo und in i ts reti c u l a r layer ( X 1 6l .
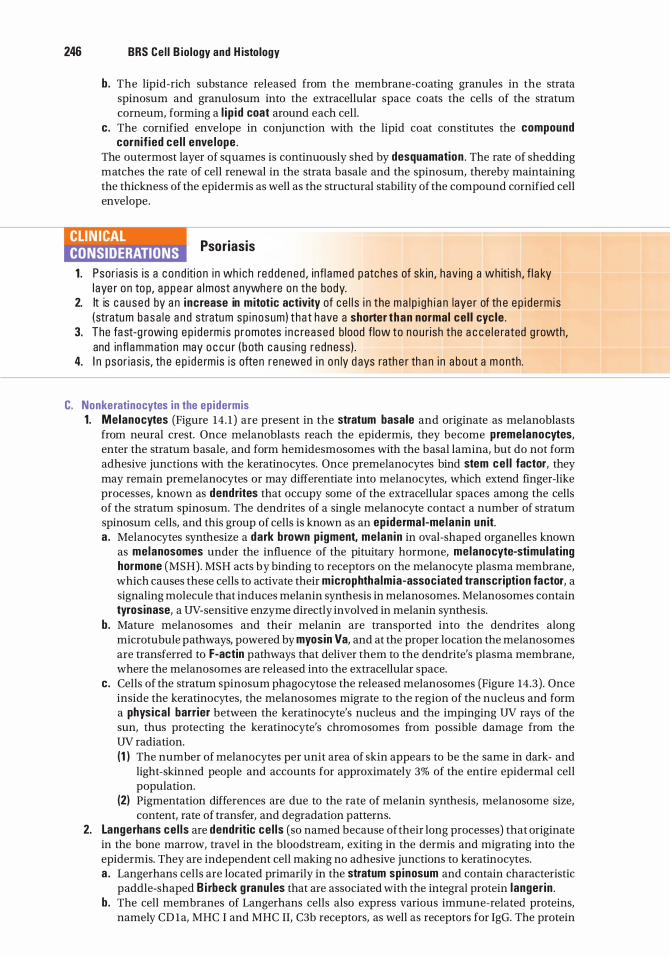
246 BRS Cel l B iology and H istology
b. The lipid-rich substance released from the membrane-coating granules in the strata spinosum and granulosum into the extracellular space coats the cells of the stratum corneum, forming a l i p id coat around each cell.
c. The cornified envelope in conjunction with the lipid coat constitutes the compound cornif ied ce l l enve lope .
The outermost layer of squames is continuously shed by desquamation . The rate of shedding matches the rate of cell renewal in the strata basale and the spinosum, thereby maintaining the thickness of the epidermis as well as the structural stability of the compound cornified cell envelope.
llfi'n�MIII Psoriasis
1 . Psor ias is is a c ond iti o n i n wh i c h red d e n ed , infl amed patc hes of sk in , hav ing a wh iti sh , f l a ky l aye r on to p, a p p e a r a lmost a nywhe re on the body.
2. It is c aused by a n increase in mitotic activity of ce l l s i n the ma l p i g h i a n laye r of th e e p i d e rm is (stratum basa l e a n d stratum sp i nosum ) that h ave a shorter than normal cel l cyc le .
3. The fa st-g rowing e p i d e rm i s p romotes i n c reased b lood f low to nou rish the a c c e l e rated g rowth, and infl ammatio n may o c c u r ( b oth c a us i ng redness ) .
4. I n psor i as is, th e e p i d e rm i s is often renewed i n on ly d ays rath e r th a n i n a bout a m onth.
C. Nonkeratinocytes in the ep idermis 1. Melanocytes (Figure 14 . 1 ) are present in the stratum basale and originate as melanoblasts
from neural crest. Once melanoblasts reach the epidermis, they become premelanocytes, enter the stratum basale, and form hemidesmosomes with the basal lamina, but do not form adhesive junctions with the keratinocytes. Once premelanocytes bind stem ce l l factor, they may remain premelanocytes or may differentiate into melanocytes, which extend finger-like processes, known as dendrites that occupy some of the extracellular spaces among the cells of the stratum spinosum. The dendrites of a single melanocyte contact a number of stratum spinosum cells, and this group of cells is known as an epiderma l-me lan in un it. a . Melanocytes synthesize a dark brown p igment, melan in in oval-shaped organelles known
as melanosomes under the influence of the pituitary hormone, melanocyte-stimulating hormone (MSH). MSH acts by binding to receptors on the melanocyte plasma membrane, which causes these cells to activate their microphtha lmia-associated transcription factor, a signaling molecule that induces melanin synthesis in melanosomes. Melanosomes contain tyrosinase, a UV-sensitive enzyme directly involved in melanin synthesis.
b. Mature melanosomes and their melanin are transported into the dendrites along microtubule pathways, powered by myosin Va, and at the proper location the melanosomes are transferred to F-actin pathways that deliver them to the dendrite's plasma membrane, where the melanosomes are released into the extracellular space.
c. Cells of the stratum spinosum phagocytose the released melanosomes (Figure 14.3) . Once inside the keratinocytes, the melanosomes migrate to the region of the nucleus and form a physical barrier between the keratinocyte's nucleus and the impinging UV rays of the sun, thus protecting the keratinocyte's chromosomes from possible damage from the UV radiation. (1 ) The number of melanocytes per unit area of skin appears to be the same in dark- and
light-skinned people and accounts for approximately 3% of the entire epidermal cell population.
(2) Pigmentation differences are due to the rate of melanin synthesis, melanosome size, content, rate of transfer, and degradation patterns.
2. Langerhans ce l ls are dendritic ce l ls (so named because of their long processes) that originate in the bone marrow, travel in the bloodstream, exiting in the dermis and migrating into the epidermis. They are independent cell making no adhesive junctions to keratinocytes. a . Langerhans cells are located primarily in the stratum spinosum and contain characteristic
paddle-shaped B i rbeck g ranu les that are associated with the integral protein langer in . b . The cell membranes of Langerhans cells also express various immune-related proteins,
namely CD 1a, MHC I and MHC II, C3b receptors, as well as receptors for IgG. The protein
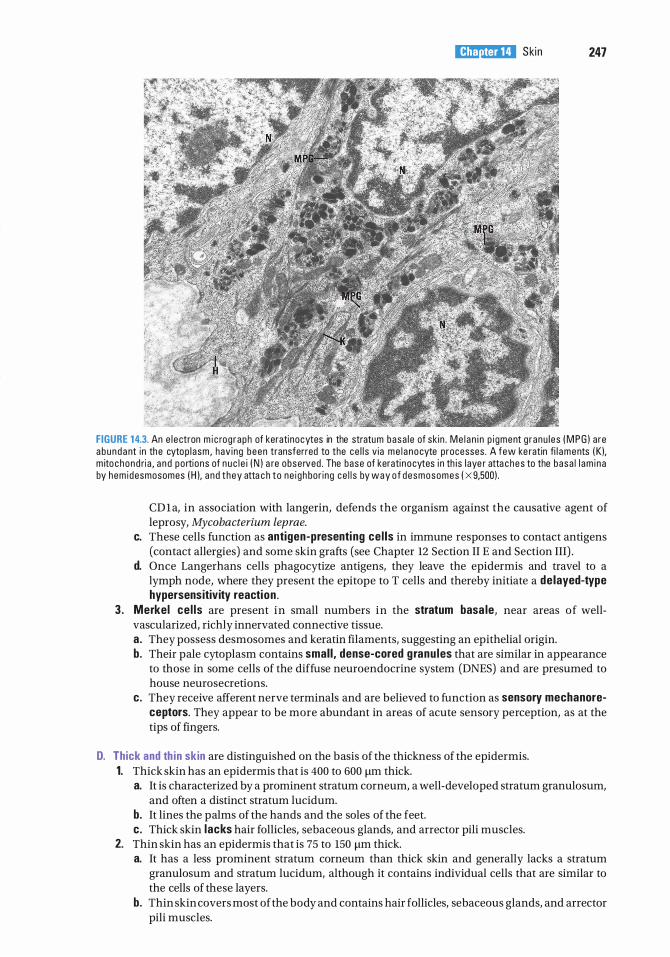
l!1lEl'1lttllJ Ski n 247
FIGURE 1 4.3. An e l e ctron m i c rog raph of keratinocytes in the stratum basa l e of sk in . M e l a n i n p i gment g ranu l es ( M P G ) a re a b u n d a nt i n the cytop l asm , hav ing been transferred to the ce l l s v ia me l a nocyte processes . A few ke ratin fi l aments ( K), m ito chond ri a , a n d po rtions of n u c l e i ( N ) a re obse rved . The base of kerati nocytes i n th is l aye r atta ches to the basa l l am i na by hem idesmosomes ( H ), a nd t hey atta c h to ne i gh bor ing ce l l s by way o f desmosomes ( X 9,500) .
CD1 a, in association with langerin, defends the organism against the causative agent of leprosy, Mycobacterium leprae.
c. These cells function as antigen-presenti ng cel ls in immune responses to contact antigens (contact allergies) and some skin grafts (see Chapter 12 Section II E and Section III) .
d. Once Langerhans cells phagocytize antigens, they leave the epidermis and travel to a lymph node, where they present the epitope to T cells and thereby initiate a delayed-type hypersensitivity reaction .
3 . Merkel ce l ls are present in small numbers in the stratum basa le, near areas of wellvascularized, richly innervated connective tissue. a. They possess desmosomes and keratin filaments, suggesting an epithelial origin. b. Their pale cytoplasm contains smal l , dense-cored g ranu les that are similar in appearance
to those in some cells of the diffuse neuroendocrine system (DNES) and are presumed to house neurosecretions.
c. They receive afferent nerve terminals and are believed to function as sensory mechanoreceptors. They appear to be more abundant in areas of acute sensory perception, as at the tips of fingers.
D. Thick and th in skin are distinguished on the basis of the thickness of the epidermis. 1. Thick skin has an epidermis that is 400 to 600 11m thick.
a. It is characterized by a prominent stratum corneum, a well-developed stratum granulosum, and often a distinct stratum lucidum.
b. It lines the palms of the hands and the soles of the feet. c. Thick skin lacks hair follicles, sebaceous glands, and arrector pili muscles.
2. Thin skin has an epidermis that is 75 to 150 11m thick. a. It has a less prominent stratum corneum than thick skin and generally lacks a stratum
granulosum and stratum lucidum, although it contains individual cells that are similar to the cells of these layers.
b. Thin skin covers most of the body and contains hair follicles, sebaceous glands, and arrector pili muscles.
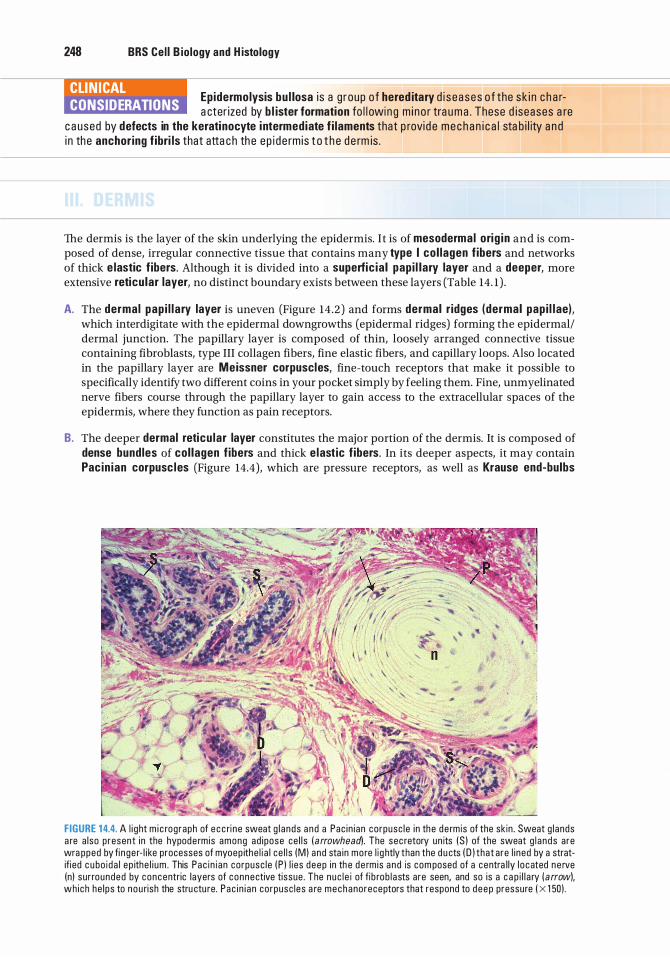
248 BRS Cel l B iology and H istology
CLIN ICAL CONSIDERATIONS
Epidermolysis bu l losa i s a g roup o f hered itary d i s e ases o f the s k i n c h a ra cter ized by b l ister formation fo l l owin g m i no r tra u m a . These d iseases a re
c a used by defects in the keratinocyte intermediate f i laments that p rovi d e m e c h a n i c a l sta b i l ity a n d i n the anchor ing fibri ls that atta ch th e ep i d e rm is t o t h e d e rm is .
The dermis is the layer of the skin underlying the epidermis. It is of mesodermal orig in and is composed of dense, irregular connective tissue that contains many type I co l lagen fibers and networks of thick e lastic f ibers. Although it is divided into a superfic ia l pap i l lary layer and a deeper, more extensive reticu lar layer, no distinct boundary exists between these layers (Table 14. 1 ) .
A. The dermal pap i l l a ry layer is uneven (Figure 14 .2) and forms dermal r idges (dermal pap i l l ae), which interdigitate with the epidermal downgrowths (epidermal ridges) forming the epidermal/ dermal junction. The papillary layer is composed of thin, loosely arranged connective tissue containing fibroblasts, type III collagen fibers, fine elastic fibers, and capillary loops. Also located in the papillary layer are Meissner corpuscles, fine-touch receptors that make it possible to specifically identify two different coins in your pocket simply by feeling them. Fine, unmyelinated nerve fibers course through the papillary layer to gain access to the extracellular spaces of the epidermis, where they function as pain receptors.
B. The deeper dermal reticu lar layer constitutes the major portion of the dermis. It is composed of dense bundles of col lagen f ibers and thick elastic f ibers. In its deeper aspects, it may contain Pac in ian corpusc les (Figure 14.4), which are pressure receptors, as well as Krause end-bulbs
FIGURE 1 4.4. A l i g ht m i c rograph of e c c ri ne sweat g l ands and a Pac in i an corpusc le i n the de rmis of the sk in . Sweat g l ands a re a lso p resent i n the hypode rm is among ad ipose ce l l s ( arrowhead). The sec retory un its (S ) of the sweat g l a nds are wra pped by fi nge r- l i ke processes of myoep ithe l i a l ce l l s (M) and sta in mo re l i g htly than the d u cts ( D ) that are l i ned by a stratifi ed c u bo i da l ep ithe l i um . This Pac i n i an corpusc le ( P ) l i es deep in th e de rm is a nd is com posed of a centra l ly l o cated ne rve (n) sur rounded by concentric layers of connective tissue . The nuc l e i of fi b rob l asts are seen, and so is a c a p i l l a ry ( arrow), which he l ps to nou rish the stru ctu re. Pac i n i a n corpusc les a re mechanoreceptors that respond to deep pressure ( X 1 50) .
l!1lEl'1lttllJ Skin 249
(formerly thought to be cold receptors, but their actual function is uncertain). Specialized diffuse receptors are discussed in Chapter 21 II.
C. Located at various levels in the dermis are the appendages of skin. These include the two types of sweat glands (eccrine and apocrine), sebaceous glands, hair follicles, and nails.
CLIN ICAL CONSIDERATIONS
Kelo ids a re swe l l i n g s i n the sk i n t ha t resu lt f r om i n c reased co l l a gen fo rmat ion i n hype rp l a st ic s c a r t issu e . They a re most p reva l ent i n Afri c a n Ameri c ans .
A. The 3 to 4 million eccrine sweat g lands (Figure 14.4) are s imp le coi led tubu lar g lands consisting of a secretory unit and a single duct. These glands are present in skin throughout most of the body but not in the lips and certain regions of the external genitalia. Eccrine sweat glands function in controlling body temperature, conserving electrolytes, and excreting urea and lactic acid. 1 . The secretory un it of eccrine sweat g lands is approximately 0.4 mm in diameter, and is
embedded in the dermis, and composed of three cell types. a. Dark cells line the lumen of the gland and contain many mucinogen-rich secretory
granules. b. C lear ce l ls underlie the dark cells, are rich in mitochondria and glycogen, and contain
intercellular canaliculi that extend to the lumen of the gland. These cells secrete a watery, electrolyte-rich material.
c. Myoepithe l i a l ce l ls lie scattered in an incomplete layer beneath the clear cells. They stain deeply with eosin and are easily identified in histological sections. Their contractions aid in expressing the gland's secretions into the duct.
2. The duct (Figure 14.4) of eccrine sweat g lands is narrow and lined by stratified cuboidal ep ithe l ia l cel ls, which contain many keratin filaments and have a prominent terminal web. The cells forming the external (basal) layer of the duct have many mitochondria and a prominent nucleus. a. The duct leads from the secretory unit through the superficial portions of the dermis to
penetrate an i nterpap i l l a ry peg of the epidermis, where the duct cells end. Beginning from this point, the walls of the duct are formed by epidermal cells as the duct forms a tight spiral through the layers of the epidermis to open at the surface of the skin at a sweat pore to deliver sweat to the sweat pore on the skin surface (Figure 14.2) .
b. As the secreted material passes through the dermal region of the duct, its cells reabsorb some electrolytes and excrete other substances (such as urea, lactic acid, ions, and certain drugs).
c. Eccrine glands are stimulated by parasympathetic innervation as a result of fluctuations in body temperature.
CLIN ICAL CONSIDERATIONS
Hyperh idrosis i s a d iso rde r o f excess ive sweati n g c a used by ove rpe rsp i rati on from s e c retio n by e c c ri ne sweat g l a n d s i n th e sk in .
Treatment with d r ugs has been unsatisfa cto ry i n a l l ev iati ng the sym ptoms of th is c o nd iti on , b ut i n ject ing a h i g h ly d i l uted form of Botox d i re ctly i nto th e sk in on the pa lms of the h a nds, so l es of th e fe et, o r of the axi l l a e offe rs re l i ef. The tox in b l o c ks sym path eti c n e rve impu lses to th e ce l l s of the e c c ri n e sweat g l a n d s and d e c reases th e i r a b i l ity to sec rete . A s i n g l e i n j ect ion of Botox may p rovi d e months o f re l i ef, a n d t h e i n j ecti ons c a n be re peated when exc essive sweati ng resumes .
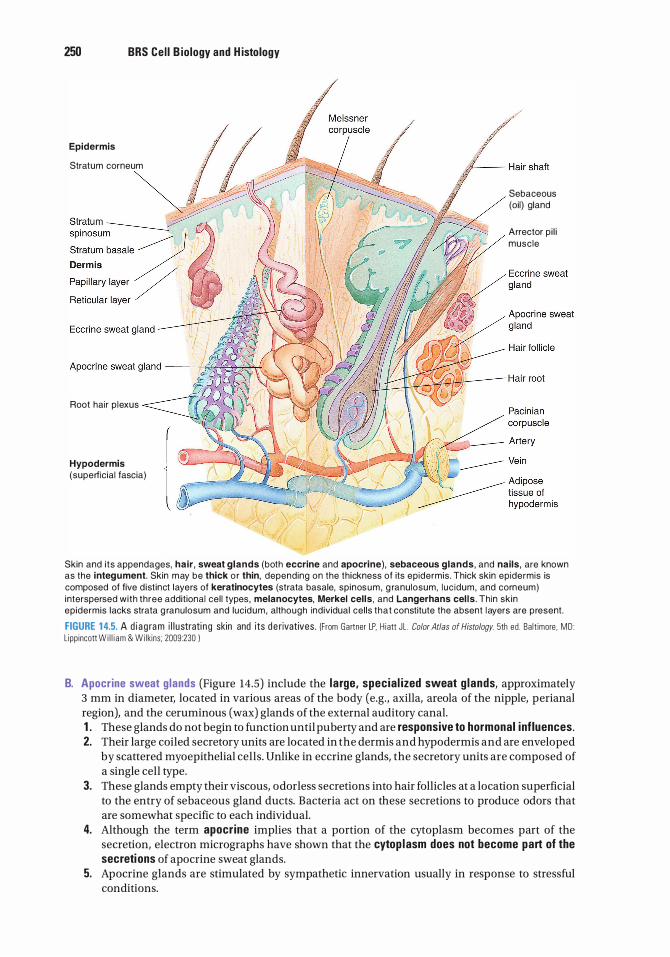
250 BRS Cel l B iology and H istology
Epidermis
Stratum corneum
Root hair p l exus
Hypodermis (superficial fascia)
Sebaceous (oi l} gland
Arrector p i l i musc le
Skin and i ts appendages, hair , sweat glands (both eccrine and apocrine), sebaceous glands, and nails, are known as the integu ment. Skin m ay be thick o r thin, depending on the thickness of its ep idermis . Thick skin ep idermis is composed of five d ist inct layers of keratinocytes (strata basale, sp inos u m , g ranu losum, luc idum, and corneum) interspersed with three additional cel l types , melanocytes, Merkel cel ls , and Langerhans cel l s . Thin sk in epidermis lacks strata g ranulosum and lucid u m , although ind ividual cel ls that constitute the absent l ayers are p resent.
FIGURE 1 4.5. A d i a g ra m i l l u strati n g skin and its d e rivatives . (From Gartner LP, H i att JL . Color Atlas of Histology. 5th ed . Ba lt imore , MD : L ipp incott W i l l i am & Wi lkins ; 2009:230 I
B. Apocrine sweat g lands (Figure 14.5) include the l a rge, specia l ized sweat g lands, approximately 3 mm in diameter, located in various areas of the body (e.g., axilla, areola of the nipple, perianal region), and the ceruminous (wax) glands of the external auditory canal. 1 . These glands do not begin to function until puberty and are responsive to hormonal inf luences. 2. Their large coiled secretory units are located in the dermis and hypodermis and are enveloped
by scattered myoepithelial cells. Unlike in eccrine glands, the secretory units are composed of a single cell type.
3. These glands empty their viscous, odorless secretions into hair follicles at a location superficial to the entry of sebaceous gland ducts. Bacteria act on these secretions to produce odors that are somewhat specific to each individual.
4. Although the term apocrine implies that a portion of the cytoplasm becomes part of the secretion, electron micrographs have shown that the cytop lasm does not become part of the secretions of apocrine sweat glands.
5. Apocrine glands are stimulated by sympathetic innervation usually in response to stressful conditions.
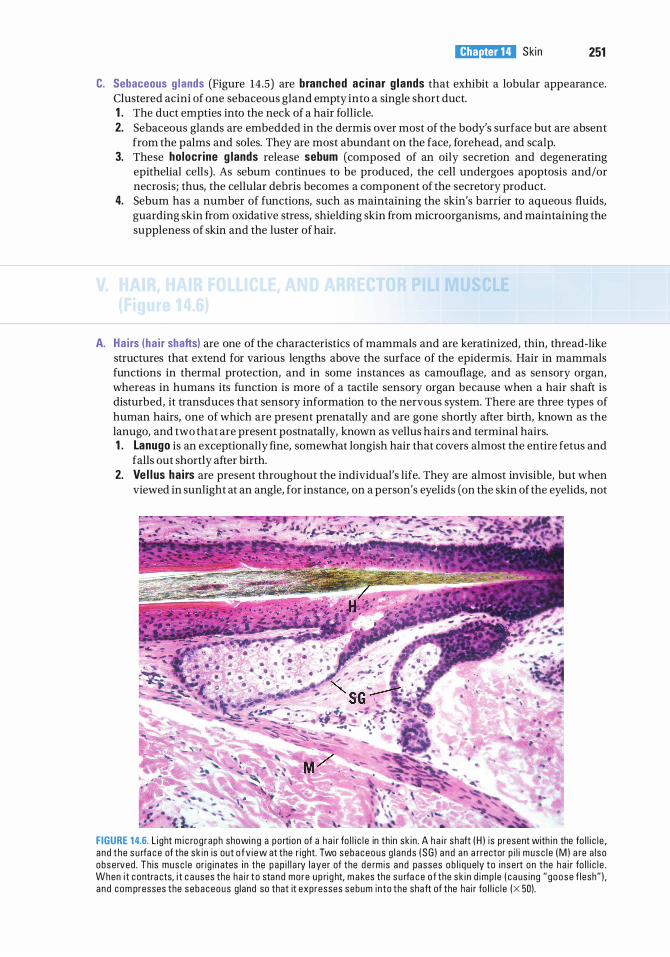
l!1lEl'1lttllJ Ski n 251
C. Sebaceous g lands (Figure 14.5) are branched acinar g lands that exhibit a lobular appearance. Clustered acini of one sebaceous gland empty into a single short duct. 1 . The duct empties into the neck of a hair follicle. 2. Sebaceous glands are embedded in the dermis over most of the body's surface but are absent
from the palms and soles. They are most abundant on the face, forehead, and scalp. 3. These holocr ine g lands release sebum (composed of an oily secretion and degenerating
epithelial cells). As sebum continues to be produced, the cell undergoes apoptosis and/or necrosis; thus, the cellular debris becomes a component of the secretory product.
4. Sebum has a number of functions, such as maintaining the skin's barrier to aqueous fluids, guarding skin from oxidative stress, shielding skin from microorganisms, and maintaining the suppleness of skin and the luster of hair.
A. Ha i rs (ha i r shafts) are one of the characteristics of mammals and are keratinized, thin, thread-like structures that extend for various lengths above the surface of the epidermis. Hair in mammals functions in thermal protection, and in some instances as camouflage, and as sensory organ, whereas in humans its function is more of a tactile sensory organ because when a hair shaft is disturbed, it transduces that sensory information to the nervous system. There are three types of human hairs, one of which are present prenatally and are gone shortly after birth, known as the lanugo, and two that are present postnatally, known as vellus hairs and terminal hairs. 1 . Lanugo is an exceptionally fine, somewhat longish hair that covers almost the entire fetus and
falls out shortly after birth. 2. Ve i l us ha i rs are present throughout the individual's life. They are almost invisible, but when
viewed in sunlight at an angle, for instance, on a person's eyelids (on the skin of the eyelids, not
FIGURE 1 4.6. l i ght m i c rog raph showi n g a po rtion of a h a i r fo l l i c l e in th in sk in . A h a i r shaft ( H ) is present with i n the fo l l i c l e , a nd t he s u rfa c e of the sk i n is out o f v i ew at the r i ght. Two sebaceous g l a nds ( SG ) a n d a n a rrector p i l i musc l e ( M ) a re a l so obse rved . Th is musc l e or ig i n ates i n the p ap i l l a ry l ayer of the d e rmis a nd passes ob l i q ue ly to i nse rt on the h a i r fo l l i c l e . When i t contra cts, i t c a uses the ha i r t o stan d more u p rig ht, m a kes the s u rfa c e o f the sk i n d imp l e ( c a us i ng " goose f lesh" ) , a nd com presses the sebaceous g land so that it expresses sebum into the shaft of the ha i r fo l l i c l e (X 50).
252 BRS Cel l B iology and H istology
the eyelashes), they are evident as short, very fine, soft, and pale structures. Most of the human body is covered by vellus hairs.
3. Termina l ha i rs are the coarse, long, highly keratinized, dark hairs that one associates with the word "hair:' These are present on the head, eyebrows, eyelashes, pubic hairs, etc. Most of the primate body is covered by terminal hair.
B. A ha i r fo l l ic le is an invag ination of the ep idermis, extending deep into the dermis. 1 . The hai r shaft is a long, slender filament in the center of the follicle that extends above the
surface of the epidermis. It consists of an inner medu l l a, cortex, and cutic le of the ha i r. At its deep end, it is continuous with the hai r root. The cuticle of the hair is surrounded by the internal root sheath (see below) .
2. The ha i r root is the terminal expanded region of the hair follicle, located deep within the dermis where the hair is rooted. The hair root is deeply indented by a dermal pap i l la , which contains a capillary network necessary for sustaining the follicle. The hair root is separated from the dermal papilla by a basement membrane, and the two together constitute the ha i r bu lb . a . The ha i r root contains keratinocytes that function as stem cel ls for hair shaft regeneration.
Interestingly, these stem cells are present even in bald individuals, but the signaling molecules that induce them to form new hair are absent.
b. The majority of the cells of the hair root comprise the matrix, whose cells form the medu l la (the core of thick hairs) and the internal root sheath. (1 ) The i nterna l root sheath lies deep to the entrance ofthe sebaceous gland. It is composed
of the Hen le layer, the Huxley layer, and the cutic le of the interna l root sheath (not to be confused with the cuticle of the hair) .
(2) The external root sheath is a direct continuation of the stratum malpighii of the epidermis.
(3) The g lassy membrane is a nonce l l u la r layer, a thickening of the basement membrane. It separates the hair follicle from the surrounding dermal sheath.
c. Melanocytes are located in the matrix, lying on the basement membrane. The long dendrites of these cells penetrate the extracellular space among cells of the cortex and deliver their melanosomes into these spaces. Cells of the cortex phagocytose the melanosomes, and it is in this fashion that hair acquires its color. As the individual ages, the tyrosinase synthesis by the melanocytes of the hair follicles diminishes and eventually ceases, resulting in the absence of melanin production, and hair loses its color and turns gray.
3. The average human head has approximately 150,000 hairs, which grow at a rate of 2 mm per day. Hair growth occurs in three phases; a growing phase, known as the anagen phase; a short respite from active growth, known as the catagen phase; and the terminal resting phase, known as the te logen phase when the hair falls out; that shed hair is known as a club hair because the removed hair possesses a club-shaped root. On a daily basis, approximately 50 to 100 hairs are lost from the head. Hairs in some regions of the body last longer than others. Hair on the head stays in place for as long as seven years, whereas hairs in the armpit fall out in less than half a year.
C. The arrector p i l i musc le attaches at an obl ique angle to the dermal sheath surrounding a hair follicle. 1 . It extends superficially to underlie sebaceous glands, passing through the reticular layer of the
dermis and i nserting i nto the pap i l la ry layer of the dermis. 2. The contraction of this smooth musc le elevates the hair and is responsible for formation of
goose bumps, caused by depressions of the skin where the muscle attaches to the papillary layer of the dermis.
Nails are located on the distal phalanx of each finger and toe.
A. Nails are hard keratinized plates that rest on the na i l bed composed of the epidermis and underlying dermis of the skin.
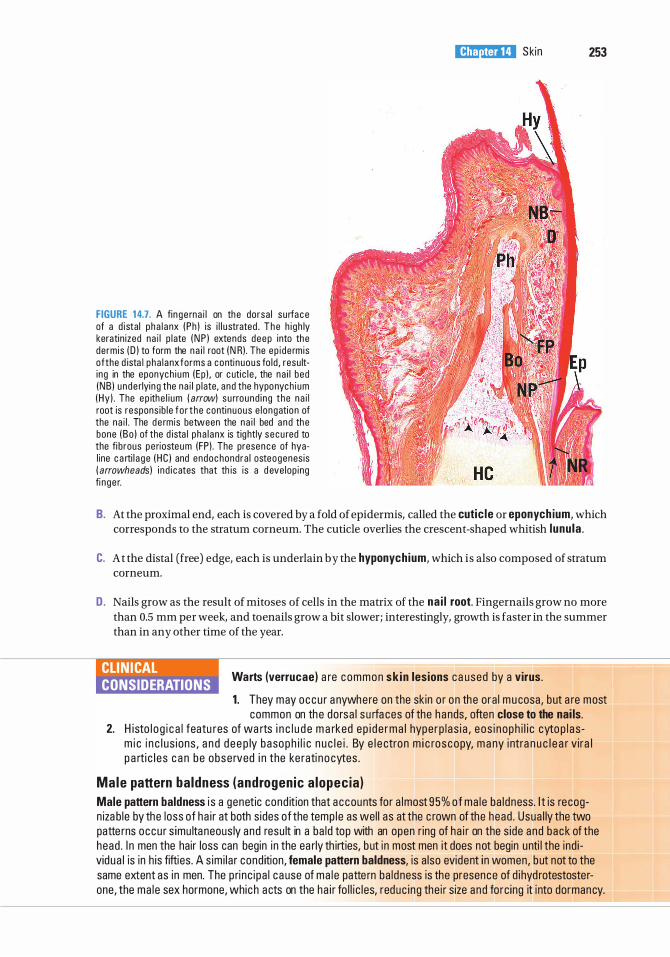
FIGURE 1 4.7. A fin ge rna i l on the dorsa l su rfac e of a d istal p ha l a nx (Ph ) is i l l u strated . T h e h i gh ly keratin ized na i l p l ate ( N P l extends deep into the derm is ( D ) to form the n a i l root ( N R) . The ep i de rm is ofthe d ista l pha l anx forms a conti nuous fo ld , resu lti ng in the eponych i um (Ep ) , or c uti c l e , the na i l bed (NB l unde rlyin g the na i l p l ate, and the hyponych i um (Hy l . The ep ithe l i um ( arrow) su rround i ng the na i l root is respons ib le f o r t he continuous e l ongation of the na i l . The de rmis between the na i l bed and the bone (Bo l of the d ista l pha l anx is tig htly secu red to the fi brous pe riosteum (FP) . The presence of hyal ine c a rti l a ge ( HC l and endoc hondra l osteogenes is ( arrowheads ) i n d i c ates that th is is a d eve lop ing fi nge r.
l!1lEl'1lttllJ Skin 253
B. At the proximal end, each is covered by a fold of epidermis, called the cutic le or eponych ium, which corresponds to the stratum corneum. The cuticle overlies the crescent-shaped whitish l unu la .
C. At the distal (free) edge, each is underlain by the hyponychium, which is also composed of stratum corneum.
D. Nails grow as the result of mitoses of cells in the matrix of the na i l root. Fingernails grow no more than 0.5 mm per week, and toenails grow a bit slower; interestingly, growth is faster in the summer than in any other time of the year.
CLIN ICAL CONSIDERATIONS
Warts (verrucae) a re common sk in lesions ca used by a virus.
1 . They may occu r a nywhere on the skin o r on the ora l mu cosa, but a re most common on the dorsa l s u rfa ces of the hands, often close to the nai ls.
2. H isto l o g i c a l featu res of wa rts i n c l u d e m a rked ep i d e rma l hype rp l as i a , eos i noph i l i c cyto p l a sm i c i n c l us ions , a n d d ee p ly basoph i l i c n u c l e i . By e l e ctron m i c roscopy, m a ny i ntra n u c l e a r v ira l p a rti c l e s c a n be obse rved i n the ke rati no cytes .
Male pattern ba ldness (androgenic a lopec ia ) Male pattern baldness i s a genetic cond ition that accounts for a lmost 95% o f ma le ba ldness. I t is recogn iza b le by the loss of ha i r at both s ides of the temp le as wel l as at the c rown of the head . Usua l ly the two patte rns occu r s imu ltaneous ly and resu lt in a ba ld top with an open r ing of ha i r on the s ide and back of the head . I n men the hair loss can begin in the ea rly th irties, b ut in most men it does not begin unti l the ind i vidua l is in h is fifties. A s im i lar cond ition, female pattern baldness, is a lso evident in women, b ut not to the same extent as in men. The p rinc ipa l ca use of ma l e patte rn ba ldness is the presence of d ihyd rotestosterone, the ma le sex hormone, which acts on the ha i r fo l l i c les, reduc ing the i r size and forc ing it into dormancy.
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1. Intercellular bridges are characteristic of which of the following layers of the epidermis?
(A) Stratum granulosum (B ) Stratum lucidum (C) Stratum corneum (D ) Stratum spinosum (E) Stratum basale
2. Which of the following statements concerning the stratum granulosum is true?
(A) It contains melanosomes. (B) It lies superficial to the stratum lucidum. (C) It is the thickest layer of the epidermis in
thick skin. (D ) It contains keratohyalin granules. (E ) It contains large numbers of dividing cells.
3. Which of the following statements about Langerhans cells is true?
(A) They are commonly found in the dermis. (B ) They function as sensory
mechanoreceptors. (C) They function as receptors for cold. (D ) They play an immunological role in the skin. (E ) They are of epithelial origin.
4. Meissner corpuscles are present in which of the following regions of the skin?
(A) Dermal reticular layer (B ) Dermal papillary layer (C) Hypodermis (D ) Stratum basale (E) Epidermal ridges
5. Which of the following statements concerning thin skin is true?
(A) It does not contain sweat glands. (B ) It lacks a stratum corneum. (C) It is less abundant than thick skin. (D ) It contains hair follicles. (E ) Its epidermis does not rest on a basement
membrane.
254
6. Which of the following statements about eccrine sweat glands is true?
(A) They are absent in thick skin. (B ) They are holocrine glands. (C) They have a narrow duct lined by a
stratified cuboidal epithelium. (D ) They secrete an oily material called
sebum. (E) They empty into hair follicles.
7. Which of the following statements about hair follicles is true?
(A) They are always associated with an eccrine sweat gland.
(B ) They are present in thin skin but not in thick skin.
(C) Their associated arrector pili muscle is composed of striated fibers.
(D ) Their hair shaft inserts into the papillary layer of the epidermis.
(E) They do not extend into the dermis.
8. Which of the following statements concerning skin melanocytes is true?
(A) They synthesize a pigment that protects against damage caused by UV radiation.
(B) They are located only in the dermis. (C) They produce keratohyalin granules. (D) They may give rise to basal cell
carcinoma. (E) They originate from the mesoderm.
9. Which of the following statements concerning sebaceous glands is true?
(A) They do not begin to function until puberty.
(B ) They employ the mechanism of holocrine secretion.
(C) They are present in thick skin. (D ) They secrete only in response to
hormones. (E) They produce a watery enzyme-rich
secretion.
l!1lEl'1lttllJ Ski n 255
1 0. Which of the following is an appendage of skin?
(A) Meissner corpuscle (B ) Langerhans cell (C) Krause end-bulb (D ) Pacinian corpuscle (E) Nail
Answers and Explanations
1 . D . Observations with an electron microscope show that intercellular bridges are associated with desmosomes (maculae adherentes), linking the processes of adjacent cells in the stratum spinosum. Desmosomes also link cells within the other epidermal layers, but these cells do not form processes characteristic of bridges. The keratinocytes of the stratum basale also contain hemidesmosomes, which attach the cells to the underlying basal lamina (see Chapter 14 II B) .
2. D . The stratum granulosum contains a number of dense keratohyalin granules, but not melanosomes. It lies just deep to the stratum lucidum and is a relatively thin layer in the epidermis of thick skin. Only rarely would a cell undergo mitosis in this layer of the skin (see Chapter 14 II B) .
3. D . Langerhans cells in the epidermis function as antigen-presenting cells by trapping antigens that penetrate the epidermis and transporting them to regional lymph nodes, where they are presented to T lymphocytes. In this way, these cells assist in the immune defense of the body. They originate in the bone marrow and do not arise from epithelium (see Chapter 14 II C) .
4. B . Meissner corpuscles are encapsulated nerve endings present in dermal papillae, which are part of the papillary layer of the dermis. These corpuscles function as receptors for fine touch (see Chapter 14 III A).
5. D. In contrast to thick skin, which lacks hair follicles, thin skin contains many of them (see Chapter 14 II D) .
6. C. Eccrine sweat glands are simple, coiled tubular glands that have a duct lined by a stratified cuboidal epithelium. They are found in both thick and thin skin and are classified as merocrine glands, meaning they release only their secretory product, which does not include cells or portions of cells (see Chapter 14 IV A).
7. B . Hair follicles are present only in thin skin. They are associated with sebaceous glands and arrector pili smooth muscle bundles (see Chapter 14 V) .
8. A. Melanocytes are present in the stratum basale of the epidermis. They synthesize melanin pigment and transfer it to keratinocytes to protect against damage caused by UV radiation. Melanocytes sometimes give rise to a form of skin cancer called malignant melanoma. They derive from neural crest and migrate into the epidermis early during embryonic development (see Chapter 14 II C) .
9. B . Sebaceous glands produce sebum, an oily material, and release it into the upper shaft of the hair follicle by a mechanism called holocrine secretion (which means the product and cellular debris are both released from the gland) (see Chapter 14 IV C) .
1 0. E. The nail is one appendage of the skin. Other skin appendages are hair follicles, sweat glands, and sebaceous glands (see Chapter 14 VI) .
256
Respiratory System
A. The respiratory system includes the lungs and a series of a i rways that connect the lungs to the external environment.
B. The respiratory system can be functionally classified into two major subdivisions : a conducting portion, consisting of airways that deliver air to the lungs, and a respi ratory portion, consisting of structures within the lungs in which oxygen in the inspired air is exchanged for carbon dioxide in the blood.
C. The components of the respiratory system possess characteristic lining epithelia, supporting structures, glands, and other features, which are summarized in Table 1 5 . 1 .
This portion o f the respiratory system includes the nose, nasopharynx, larynx, trachea, bronchi, and bronchioles of decreasing diameters, including and ending at the terminal bronchioles. These structures warm, moisten, and fi lter the air before it reaches the respiratory components, where gas exchange occurs.
A. Nasal cavity. The nasal cavity is subdivided by the median nasal septum into right and left nasal cavities, each leading to the paranasal sinuses, thus providing a large surface area for filtering, moistening, and warming the inspired air. 1 . The nares are the nostrils ; their outer portions are lined by th in skin . They open into the
vestibule. 2. The vestibu le is the first portion of the nasal cavity, where the epithelial lining becomes
nonkeratin ized. Posteriorly, the lining changes to respi ratory ep ithe l ium (pseudostratified ciliated columnar epithelium with goblet cells). a. The vestibule contains vibrissae (thick, short hairs), which filter large particles from the
inspired air. b. It has a richly vascularized lamina propria (many venous plexuses) and contains
seromucous g lands. c . Each nasal cavity contains bony shelves that originate from the lateral nasal wall and
project into the nasal cavity. These are the superior, midd le , and i nferior conchae
257
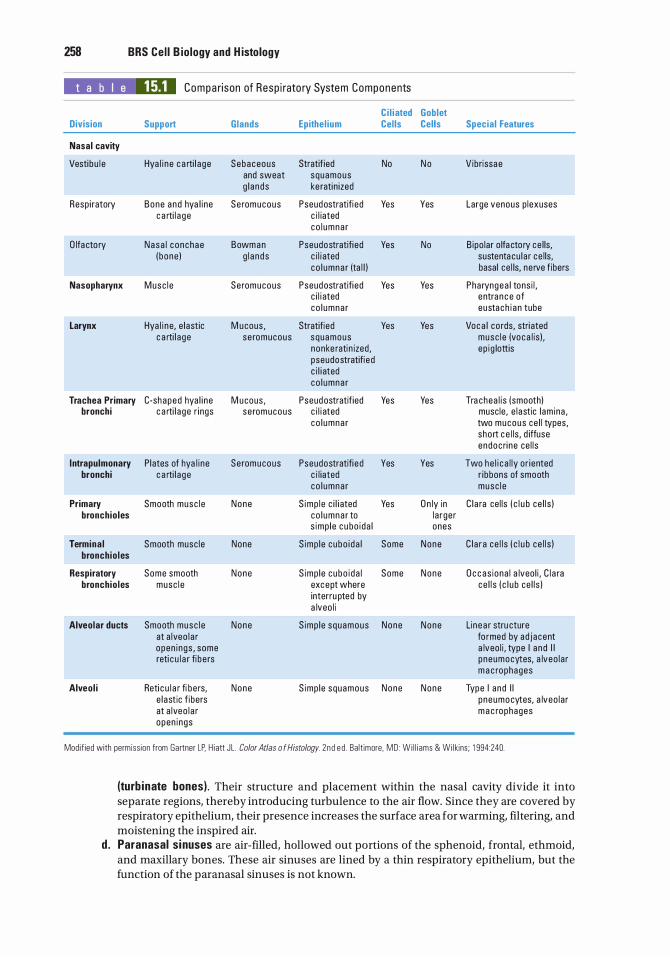
258 BRS Cel l B iology and H istology
t a b I e 15.1 Compa rison of Resp i rato ry System Components
Ci l iated Division Support Glands Epithel ium Cel ls
Nasal cavity
Vestibu l e Hya l i n e c a rti l a ge Sebaceous Stratif ied No and sweat squamous g l ands ke rati n ized
Resp i ratory Bone a nd hya l i ne Se romucous Pseudostratifi ed Yes c a rti l a ge c i l iated
co l umna r
O lfa cto ry Nasa l c onchae Bowman Pseudostratifi ed Yes ( bone ) g l a nds c i l i ated
co l umna r (ta l l )
Nasopharynx Musc l e Se romucous Pseudostratifi ed Yes c i l i ated co l umna r
Larynx Hya l i n e, e l astic M ucous , Stratified Yes c a rti l a ge se romucous squamous
nonke rati n ized , pseudostratifi e d c i l i ated co l umna r
Trachea Primary C-shaped hya l i ne M ucous , Pseudostratif ied Yes bronchi c a rti l a ge r i ngs se romucous c i l i ated
co l umna r
I ntrapulmonary Plates of hya l i ne Seromucous Pseudostratifi e d Yes bronchi c a rti l a ge c i l iated
co l umna r
Primary Smooth musc l e None S imp l e c i l i ated Yes bronchioles co l umna r to
s imp le c u bo i da l
Termina l Smooth musc le None S imp le cubo i da l Some bronchioles
Respiratory Some smooth None S imp le cubo i da l Some bronchioles musc l e except where
interru pted by a lveo l i
Alveolar ducts Smooth musc l e None S imp le squamous None at a lveo l a r open i ngs , some reti c u l a r fi be rs
Alveol i Reti c u l a r fi be rs, None S imp le squamous None e l ast ic f ibers at a lveo l a r open i ngs
Goblet Cells Special Features
N o Vibrissae
Yes Large venous p lexuses
No B ipo lar o lfa cto ry ce l ls, sustenta cu l a r ce l ls, basal ce l ls, ne rve f ibers
Yes Pha ryngea l tons i l , entra n c e of eustach i a n tube
Yes Voca l cords, stri ated musc l e (voca l is ) . ep i g lottis
Yes Tra chea l i s (smooth) musc le , e l astic l am ina , two mucous ce l l types, short c e l ls , d iffuse endoc ri ne ce l l s
Yes Two he l i c a l ly or iented r ibbons of smooth musc l e
O n ly in C l a ra ce l ls ( c l u b ce l l s ) l a rge r ones
None C l a r a ce l l s ( c l u b ce l l s )
None O c c as iona l a lveo l i , C l a ra ce l l s ( c l u b ce l l s )
None Lin e a r stru cture fo rmed by ad j acent a lveo l i , type I a n d I I p neumocytes, a lveo l a r m a c rophages
None Type I and I I p neumocytes, a lveo l a r m a c rophages
Modif ied with permiss ion from Gartner LP. H i att JL . Color Atlas o f Histology. 2nd e d . Ba lt imore, MD : W i l l i ams & Wi lkins ; 1 994:240.
(turb inate bones) . Their structure and placement within the nasal cavity divide it into separate regions, thereby introducing turbulence to the air flow. Since they are covered by respiratory epithelium, their presence increases the surface area for warming, filtering, and moistening the inspired air.
d . Paranasal sinuses are air-filled, hollowed out portions of the sphenoid, frontal, ethmoid, and maxillary bones. These air sinuses are lined by a thin respiratory epithelium, but the function of the paranasal sinuses is not known.
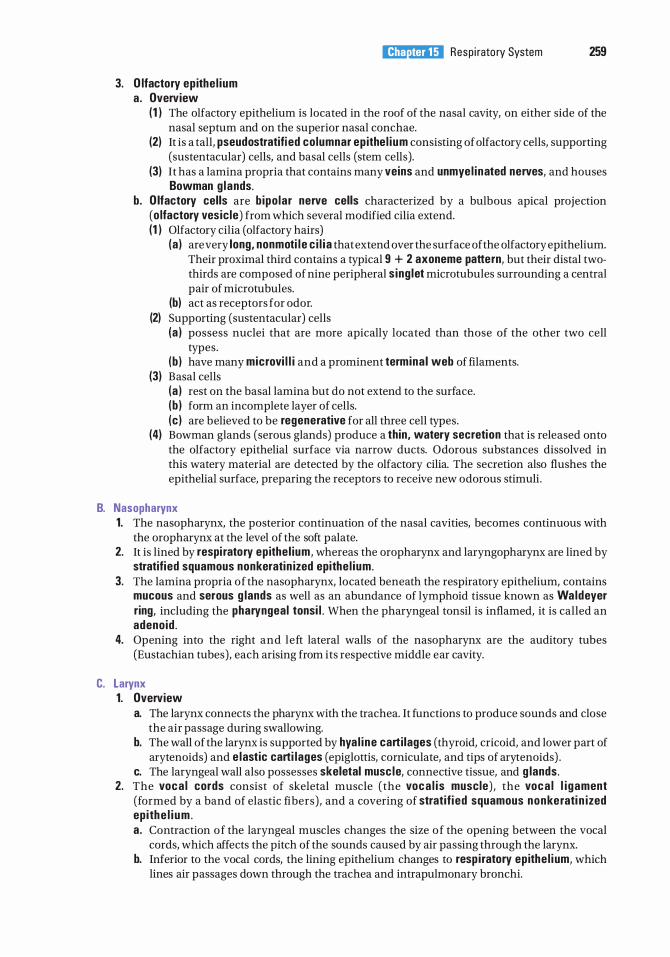
I!1JtJttQi1ij Resp i rato ry System 259
3. O lfactory ep ithe l ium a . Overview
(1 ) The olfactory epithelium is located in the roof of the nasal cavity, on either side of the nasal septum and on the superior nasal conchae.
(2) It is a tall, pseudostratifi ed columnar ep ithe l i um consisting of olfactory cells, supporting (sustentacular) cells, and basal cells (stem cells).
(3) It has a lamina propria that contains many veins and unmyel inated nerves, and houses Bowman g lands.
b . O lfactory cells are b ipo lar nerve cells characterized by a bulbous apical projection (o lfactory vesic le) from which several modified cilia extend. (1 ) Olfactory cilia (olfactory hairs)
(a ) are very long, nonmoti l e c i l i a that extend over the surface of the olfactory epithelium. Their proximal third contains a typical 9 + 2 axoneme pattern, but their distal twothirds are composed of nine peripheral s ing let microtubules surrounding a central pair of microtubules.
(b) act as receptors for odor. (2) Supporting (sustentacular) cells
(a ) possess nuclei that are more apically located than those of the other two cell types.
(b ) have many microvi l l i and a prominent termina l web of filaments. (3) Basal cells
(a ) rest on the basal lamina but do not extend to the surface. (b ) form an incomplete layer of cells. (c ) are believed to be regenerative for all three cell types.
(4) Bowman glands (serous glands) produce a thin, watery secretion that is released onto the olfactory epithelial surface via narrow ducts. Odorous substances dissolved in this watery material are detected by the olfactory cilia. The secretion also flushes the epithelial surface, preparing the receptors to receive new odorous stimuli.
B. Nasopharynx 1. The nasopharynx, the posterior continuation of the nasal cavities, becomes continuous with
the oropharynx at the level of the soft palate. 2. It is lined by respi ratory ep ithe l ium, whereas the oropharynx and laryngopharynx are lined by
stratified squamous nonkeratin ized epithe l ium. 3. The lamina propria of the nasopharynx, located beneath the respiratory epithelium, contains
mucous and serous g lands as well as an abundance of lymphoid tissue known as Waldeyer ring, including the pharyngeal tonsi l . When the pharyngeal tonsil is inflamed, it is called an adenoid .
4. Opening into the right and left lateral walls of the nasopharynx are the auditory tubes (Eustachian tubes), each arising from its respective middle ear cavity.
C. Larynx 1. Overview
a. The larynx connects the pharynx with the trachea. It functions to produce sounds and close the air passage during swallowing.
b. The wall of the larynx is supported by hya l i ne cartilages (thyroid, cricoid, and lower part of arytenoids) and e lastic carti lages (epiglottis, corniculate, and tips of arytenoids) .
c. The laryngeal wall also possesses skeletal musc le, connective tissue, and g lands. 2. The voca l cords consist of skeletal muscle (the voca l i s muscle) , the voca l l i gament
(formed by a band of elastic fibers) , and a covering of stratifi ed squamous nonkerati n ized ep ithe l i um . a . Contraction o f the laryngeal muscles changes the size o f the opening between the vocal
cords, which affects the pitch of the sounds caused by air passing through the larynx. b. Inferior to the vocal cords, the lining epithelium changes to resp i ratory ep ithe l i um, which
lines air passages down through the trachea and intrapulmonary bronchi.
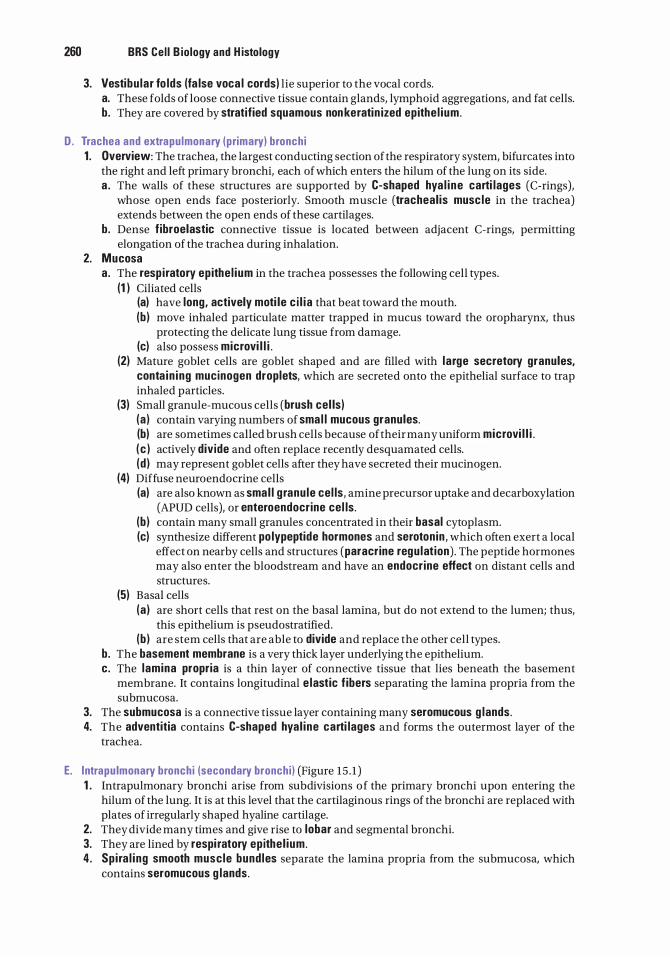
260 BRS Cel l B iology and H istology
3. Vestibu lar fo lds (fa lse voca l cords) lie superior to the vocal cords. a. These folds of loose connective tissue contain glands, lymphoid aggregations, and fat cells. b. They are covered by stratified squamous non keratin ized ep ithe l ium.
D . Trachea and extra pu lmonary (primary) bronchi 1 . Overview: The trachea, the largest conducting section of the respiratory system, bifurcates into
the right and left primary bronchi, each of which enters the hilum of the lung on its side. a . The walls of these structures are supported by C-shaped hya l i ne carti lages (C-rings),
whose open ends face posteriorly. Smooth muscle (tracheal is musc le in the trachea) extends between the open ends of these cartilages.
b. Dense f ibroelastic connective tissue is located between adjacent C-rings, permitting elongation of the trachea during inhalation.
2. Mucosa a . The resp i ratory ep ithe l ium in the trachea possesses the following cell types.
(1 ) Ciliated cells (a) have long, actively moti le c i l i a that beat toward the mouth. (b ) move inhaled particulate matter trapped in mucus toward the oropharynx, thus
protecting the delicate lung tissue from damage. (c) also possess microvi l l i .
(2) Mature goblet cells are goblet shaped and are filled with l a rge secretory granules, conta in ing mucinogen droplets, which are secreted onto the epithelial surface to trap inhaled particles.
(3) Small granule-mucous cells (brush cel ls) (a ) contain varying numbers of sma l l mucous granules. (b) are sometimes called brush cells because of their many uniform microvi l l i . ( c ) actively divide and often replace recently desquamated cells. (d ) may represent goblet cells after they have secreted their mucinogen.
(4) Diffuse neuroendocrine cells (a) are also known as sma l l g ranu le cel ls, amine precursor uptake and decarboxylation
(APUD cells), or enteroendocrine cel ls . (b ) contain many small granules concentrated in their basal cytoplasm. (c) synthesize different po lypeptide hormones and serotonin , which often exert a local
effect on nearby cells and structures (paracrine regu lat ion) . The peptide hormones may also enter the bloodstream and have an endocrine effect on distant cells and structures.
(5) Basal cells (a ) are short cells that rest on the basal lamina, but do not extend to the lumen; thus,
this epithelium is pseudo stratified. (b ) are stem cells that are able to divide and replace the other cell types.
b. The basement membrane is a very thick layer underlying the epithelium. c. The l amina propria is a thin layer of connective tissue that lies beneath the basement
membrane. It contains longitudinal e lastic f ibers separating the lamina propria from the submucosa.
3. The submucosa is a connective tissue layer containing many seromucous g lands. 4. The adventitia contains C-shaped hya l ine carti lages and forms the outermost layer of the
trachea.
E. Intrapu lmonary bronchi (secondary bronchi ) (Figure 15 . 1 ) 1 . Intrapulmonary bronchi arise from subdivisions of the primary bronchi upon entering the
hilum of the lung. It is at this level that the cartilaginous rings of the bronchi are replaced with plates of irregularly shaped hyaline cartilage.
2. They divide many times and give rise to lobar and segmental bronchi. 3. They are lined by respi ratory ep ithe l ium. 4 . Sp i ra l i ng smooth musc le bund les separate the lamina propria from the submucosa, which
contains seromucous g lands.
I!1JtJttQi1ij Resp i rato ry System 261
FIGURE 1 5.1 . A l i ght m i c rog raph of an intra pu lmona ry b ronchus c ut i n c ross sectio n . Lin i n g its l umen is a pseud ostratifi ed c i l iated co l umna r ep ithe l i um with g o b let ce l l s ( E l . Beneath the ep ithe l i um i n the l am i na p rop ria of loose , fi b roe l ast ic connective t issu e are bund l es of smooth musc l e ce l l s (SMl wrapped in a sp i ra l i n g a r ra ngement a round the l umen . I n the submucosa l connective ti ssue o uts i de of the smooth musc l e a re i r re gu l a r p l ates of c a rti l a g e ( C l, se romucous g l a nds ( G l, a nd lym pho i d t issu e ( Ll . Alveo l i (Al a re ev ident in the nea rby resp i rato ry tissue ( x 75l .
llYniJII Lung cancer
1 . Lu ng c a n c e r is the l e a d i n g c a use of d e ath from c a n c e r i n men a n d women ; most of it (90% ) is a conseq uence of c i g a rette smok i ng .
2 . Two types o f l u n g cance r tha t a re i n c reased i n smoke rs i n c l u d e squamous c e l l c a rc i noma and sma l l c e l l ( oat ce l l ) c a rc i n oma .
3 . Squamous ce l l carcinoma typ i c a l ly a rises i n t h e bron c h i , whe r e c i g a rette smok i n g c a uses the resp i rato ry ep ith e l i um to c h a n g e to a stratif ied s quamous e p ith e l i um ( a meta p l a st ic c h a nge ) . T hen , a d isord e rly p ro l iferati on o f c e l ls showing g re at va ri a b i l ity i n n u c l e a r s ize a n d s hape o c c u rs i n t h e e p ith e l i um (dysp l a s i a ) , fo l l owed by atyp i c a l c h a nges that resu lt i n a c a r c i n oma ( a ma l i g n a nt neop l a sm ) .
4 . Sma l l ce l l (oat ce l l ) carcinoma i s a h i g h ly a g g ress ive c a rc i n oma o f b ro n c h i a l o r i g i n whose i n c i d e n c e i s g re atly i n c reased i n smoke rs . It h as a poo r p rognos is .
F. Primary and termina l bronchio les lack g lands in their submucosa. Their walls contain smooth muscle rather than cartilage plates (Figure 15 .2). 1. Primary bronch io les
a. Primary bronchioles have a diameter of 1 mm or less. b. They are lined by epithelium that varies from c i l iated columnar with gob let ce l ls in the
larger airways to c i l i ated cuboida l with C lara cel ls in the smaller passages. c. They divide to form several terminal bronchioles after entering the pulmonary lobu les.
2. Termina l bronchio les a. Terminal bronchioles are the most d ista l part of the conducting portion of the respiratory
system.
262 BRS Cel l B iology and H istology
FIGURE 1 5.2. A l i g ht m i c rog raph of a b ronch i o l e i n c ross se cti on . A s imple c o l umna r e p ithe l i um ( E ) l ines its l umen , a nd smooth musc l e ce l l s (S M ) s uppo rt its wa l l . S u rround i ng the b r onch i o l e is l u ng t issu e with a lveo l i , a nd n o c a rti l a g e o r g l a nds a re present. N e a rby, a m u s c u l a r a rtery (MAl i s evi d ent ( x 75) .
b. They have a diameter of less than 0.5 mm. c. They are lined by a simple cuboida l ep ithe l ium that contains mostly club cells (formerly
known as Clara cel ls), some ciliated cells, and no goblet cells. d . Function . C lub ce l ls have the following functions :
(1 ) Club cells d ivide, and some of them differentiate to form ciliated and nonciliated cells. (2) They secrete a surfactant- l ike material that reduces a lveo lar surface tension,
preventing the collapse of alveoli. They also produce club cel l secretory prote in whose function is assumed to be the protection of the respiratory epithelium.
(3) They metabol ize a i rborne toxins, a process that is carried out by cytochrome P450 enzymes in their abundant smooth endoplasmic reticulum (SER) .
lin'n����� Asthma
1 . Asthm a is m a rked by wid esp read constriction of smooth musc le i n the bronch io les, c a us i ng a d e c rease in th e i r d i a m eter.
2. It is assoc i ated with extremely d ifficult exp i ration of a i r, accumulation of mucus in th e passageways, a n d i nfi ltrat ion of inflammatory cel ls .
3. It is often treated with d r ugs, s u ch a s a l b utero l , that a ct to re lax th e b ron ch i o l a r smooth musc l e ce l l s a n d d i l ate th e passageways a n d/o r with c o rti coste ro ids , wh i c h a re a nti - i n fl a m mato ry.
4. Rec ent stud i es h ave demonstrated that th e re a re taste receptors on th e smooth musc l e c e l l s of b ro n c h i o l es of the l u n g s that respond to b itter tastes, a n d when stimu l ated by a b i tte r tasta nt, they c a use b ron ch i o l a r smooth musc l es to re lax a n d the b ro n c h io l es to open to 90% of th e i r n o rm a l vo l ume . Cu rrent work is p ro ceed i n g t o d eve l o p a e roso l i zed s u bsta n ce s t ha t c a n be u sed t o stimu l ate t hese re c e ptors.
This portion of the respiratory system includes the respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli, all in the lung. The exchange of gases takes place in this portion of the respiratory system.
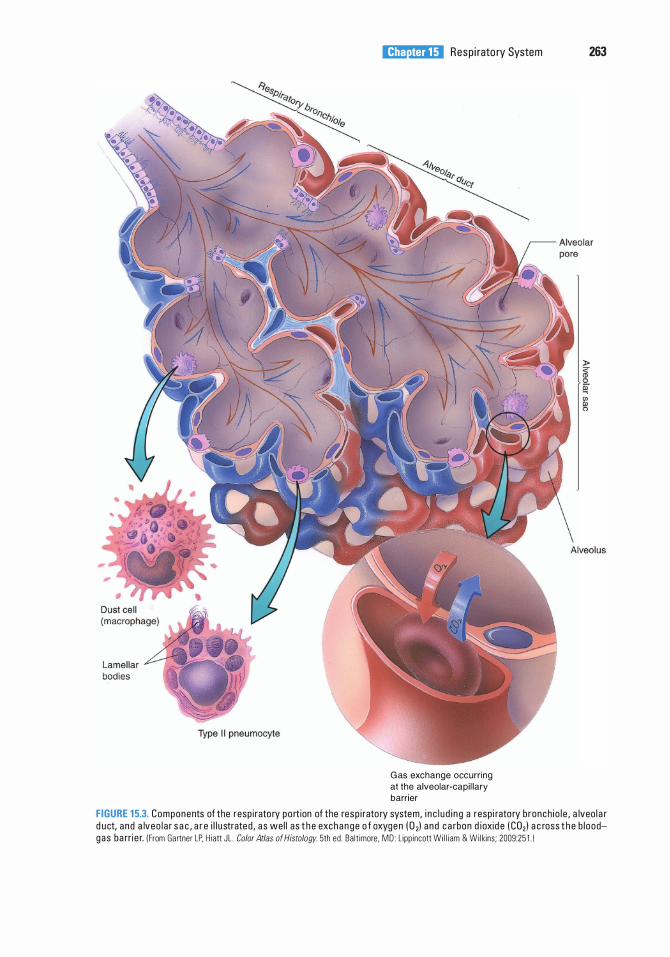
I!1JtJttQi1ij Resp i rato ry System 263
G as exchange occurr ing at the alveolar-capi l lary barrier
FIGURE 1 5.3. Components of the resp i rato ry po rt ion of the resp i rato ry system, i n c l u d i n g a resp i rato ry b ronch i o l e , a lveo l a r d uct, a nd a lveo l a r s a c , a r e i l l u strated , a s wel l as t h e exc h a n g e o f oxyge n ( 0 1) a nd c a rbon d ioxid e ( C02) a c ross t h e b l oodgas ba rri e r. ( From Gartner LP. H i att JL . Color Atlas of Histology. 5th ed . Ba lt imore, MD : L ipp incott Wi l l i am & Wi l kins ; 2009:25 1 . 1
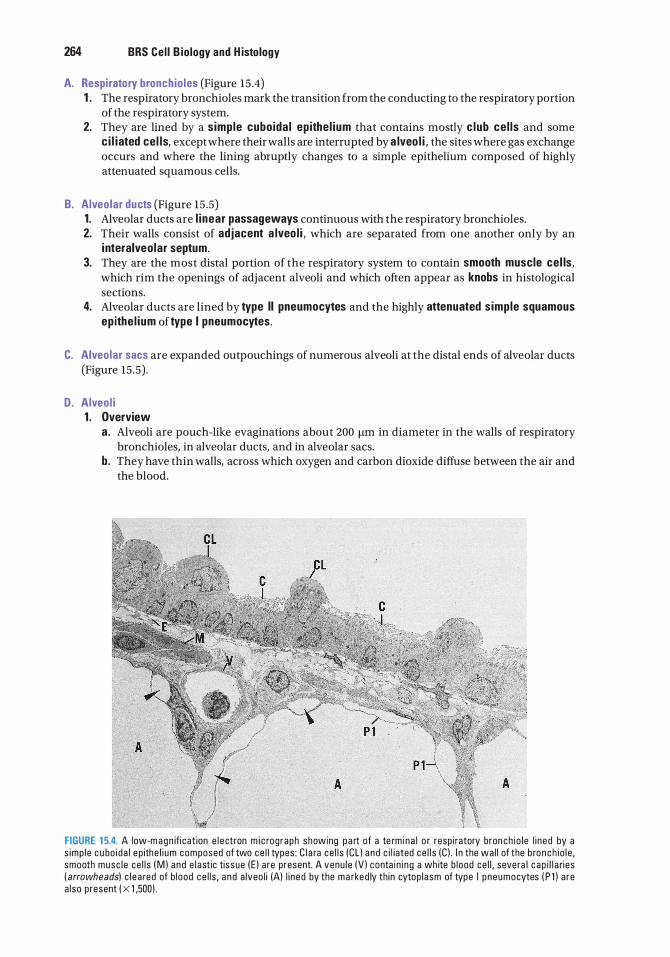
264 BRS Cel l B iology and H istology
A. Respi ratory bronchio les (Figure 15 .4) 1 . The respiratory bronchioles mark the transition from the conducting to the respiratory portion
of the respiratory system. 2. They are lined by a simple cuboida l ep ithe l ium that contains mostly c lub ce l ls and some
c i l iated cel ls, except where their walls are interrupted by a lveo l i , the sites where gas exchange occurs and where the lining abruptly changes to a simple epithelium composed of highly attenuated squamous cells.
B. Alveolar ducts (Figure 15 .5) 1. Alveolar ducts are l i near passageways continuous with the respiratory bronchioles. 2. Their walls consist of adjacent a lveo l i , which are separated from one another only by an
i nteralveolar septum. 3. They are the most distal portion of the respiratory system to contain smooth muscle cel ls,
which rim the openings of adjacent alveoli and which often appear as knobs in histological sections.
4. Alveolar ducts are lined by type II pneumocytes and the highly attenuated s imple squamous ep ithe l ium of type I pneumocytes.
C. Alveolar sacs are expanded outpouchings of numerous alveoli at the distal ends of alveolar ducts (Figure 15 .5) .
D. Alveo l i 1 . Overview
a. Alveoli are pouch-like evaginations about 200 f.Lm in diameter in the walls of respiratory bronchioles, in alveolar ducts, and in alveolar sacs.
b. They have thin walls, across which oxygen and carbon dioxide diffuse between the air and the blood.
FIGURE 1 5.4. A low-m a g n ifi cat ion e l e ctron m i c rog raph showing p a rt of a te rm i na l o r resp i ratory bron ch i o l e l i n ed by a s imp l e c u bo i d a l e p ithe l i um composed of two ce l l types : C l a ra ce l l s (CL ) a n d c i l iated ce l l s (C ) . I n the wa l l of the b ro n c h io l e , smooth musc l e ce l l s ( M ) a nd e l a st ic tissue ( E ) a re present. A venu l e (V ) conta i n i ng a wh ite b l ood ce l l , seve ra l c a p i l l a ri es ( arrowheads) c l e a red of b l ood c e l l s , a n d a lveo l i (A) l i n ed by the m a rked ly th in cytop l asm of type I p neumocytes ( P l ) a re a l so present ( X 1 ,500) .
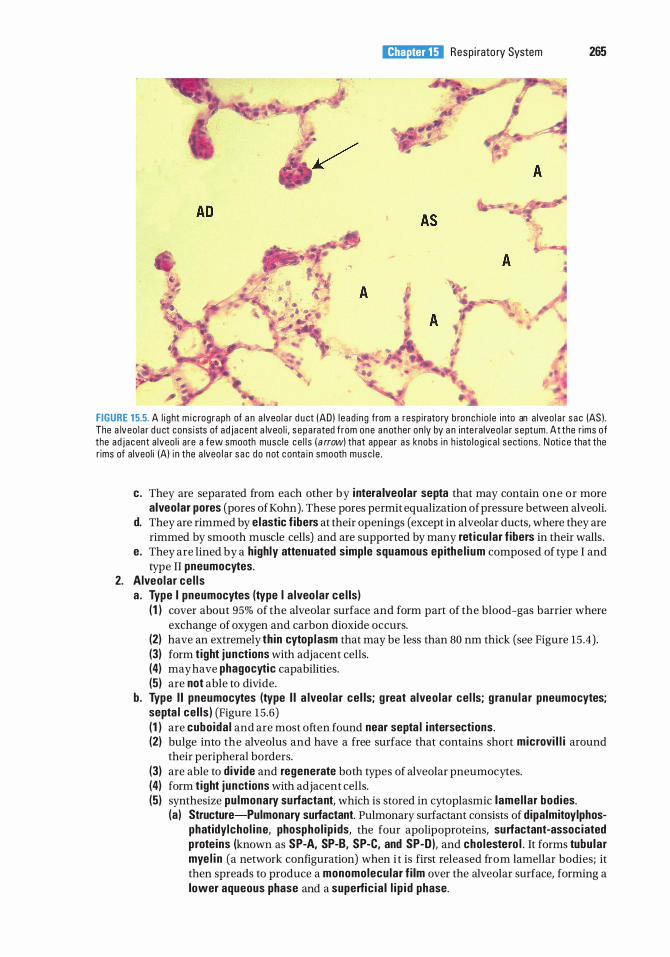
•
I!1JtJttQi1ij Resp i rato ry System 265
A
FIGURE 1 5.5. A l i g ht m i c rog raph of a n a lveo l a r d u ct (AD) l e ad i ng from a resp i rato ry b ronch i o l e i nto an a lveo l a r s ac (AS ) . The a lveo l a r d u ct cons ists of ad j acent a lveo l i , s epa rated f rom one a n other on ly by a n i nte ra lveo l a r septum. At the r ims of the ad j ac ent a lveo l i a re a few smooth musc le ce l l s ( a rrow) that appear as knobs in h isto l o g i c a l sections . N oti c e that the r ims of a lveo l i (A) i n the a lveo l a r s ac do not c onta i n smooth musc l e .
c. They are separated from each other by intera lveolar septa that may contain one or more alveolar pores (pores ofKohn). These pores permit equalization of pressure between alveoli.
d. They are rimmed by elastic f ibers at their openings (except in alveolar ducts, where they are rimmed by smooth muscle cells) and are supported by many ret icu lar fibers in their walls .
e. They are lined by a highly attenuated simple squamous epithe l ium composed of type I and type II pneumocytes.
2. Alveo lar ce l ls a . Type I pneumocytes (type I a lveo lar ce l ls)
( 1 ) cover about 95% of the alveolar surface and form part of the blood-gas barrier where exchange of oxygen and carbon dioxide occurs.
(2) have an extremely thin cytop lasm that may be less than 80 nm thick (see Figure 15 .4). (3) form t ight junctions with adjacent cells. (4) may have phagocytic capabilities. (5) are not able to divide.
b. Type I I pneumocytes (type I I a lveo lar cel ls; g reat a lveo lar cel ls; g ranu lar pneumocytes; septa l cel ls ) (Figure 1 5 .6) (1 ) are cuboida l and are most often found near septa l i ntersections. (2) bulge into the alveolus and have a free surface that contains short microvi l l i around
their peripheral borders. (3) are able to divide and regenerate both types of alveolar pneumocytes. (4) form t ight junctions with adjacent cells. (5) synthesize pulmonary surfactant, which is stored in cytoplasmic lamel lar bodies.
(a) Structure-Pulmonary surfactant. Pulmonary surfactant consists of dipalmitoylphosphatidylcho l ine, phospho l ip ids, the four apolipoproteins, surfactant-associated proteins (known as SP-A, SP-8, SP-C, and SP-D), and cholestero l . It forms tubu lar mye l i n (a network configuration) when it is first released from lamellar bodies; it then spreads to produce a monomolecular f i lm over the alveolar surface, forming a lower aqueous phase and a superfic ia l l i p id phase.

266 BRS Cel l B iology and H istology
FIGURE 1 5.6. E l ectron m ic rog raph of a typ e I I p neumocyte that synthes izes su rfa ctant and sto res it i n l ame l l a r bod ies ! LB ) i n its cyto p l asm . Type I I p neumocytes are present m a in ly n ea r the septa l i ntersecti ons a n d l i n e on ly sma l l p o rtions of the a l veo l i (A ) . They possess m i c rovi l l i ( a rrowhead) a n d a re c u bo i d a l i n s hape ( X 7,000) .
(b ) Function-Pu lmonary surfactant. Pulmonary surfactant reduces the surface tension at the a i r-l iqu id interface of the alveolar surface, permitting the alveoli to expand easily during inspiration and preventing alveolar collapse during expiration. Additionally, surfactant reduces fluid accumulation in the alveoli. Moreover, SP-A and SP-D, apolipoproteins of the surfactant, participate in innate immunity by binding to bacterial and viral surfaces, and in that fashion opsonizing them. The opsonized microorganisms are recognized and phagocytosed by macrophages (dust cel ls) of the lung.
CLIN ICAL CONSIDERATIONS Hya l ine membrane d isease; infant respi ratory d istress
syndrome 1 . Hya l i n e m e m b ra n e d i sease is fre q uently obse rved i n premature i nfants (<28 weeks' gesta
t ional age) who lack adequate amounts of pu lmonary surfactant. 2. I t is c h a ra cte r ized by l abored breath ing , which resu lts from d iffi c u lty expand i n g the a lveo l i be
cause of a h i g h a lveo l a r s u rfa c e tens i on . 3 . I f d etected before b i rth, hya l i n e m e m b ra n e d i sease c a n ofte n be p revented by p ro l o ng i n g p reg
n a n cy a n d sometimes by a d m i n iste r i ng g lucocorticoids to the expe cta nt mothe r a few d ays p r i o r to d e l ivery to h e l p i n d u c e the synth es is of su rfa cta nt.
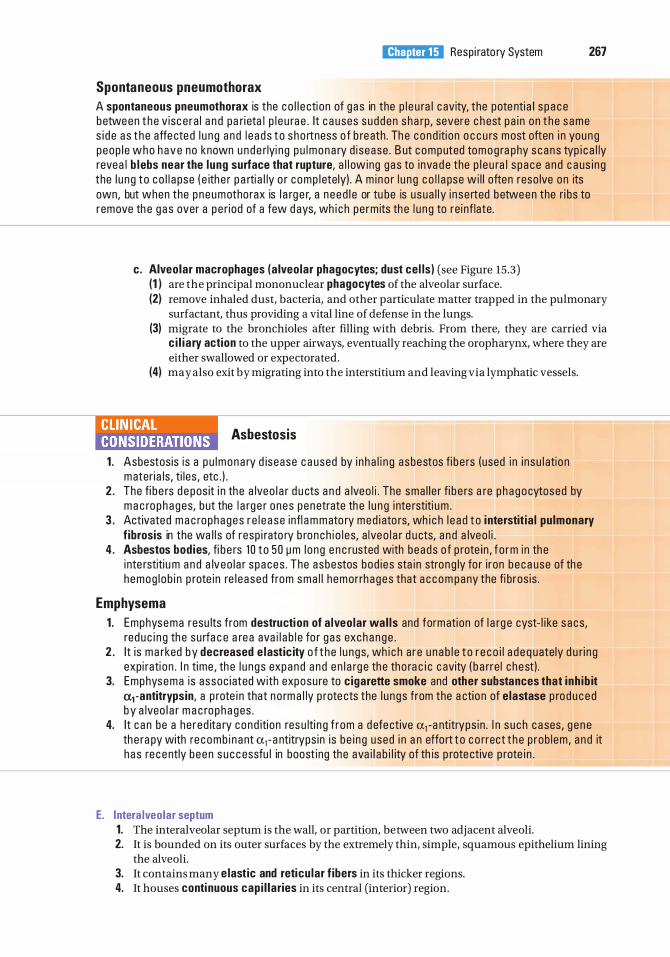
Spontaneous pneumothorax
I!1JtJttQi1ij Resp i rato ry System 267
A spontaneous pneumothorax is the c o l l e cti on of g as in the p l e u ra l c avity, the pote nti a l s p a c e between t h e v isc e ra l a n d pa ri eta l p l e u ra e . It c a uses s udden sha rp, severe c h est p a i n on t h e s ame s i d e a s t h e affe cte d l u n g a n d l e a ds t o s ho rtness o f b re ath . Th e c ond iti on o c c u rs most often i n young peop l e who h ave no known u n d e rlyi ng p u lmona ry d i sease . B ut c omputed tom o g ra phy s cans typ i c a l ly revea l b lebs near the lung surface that rupture, a l l owing gas to inva d e the p l e u ra l s p a ce a n d c a us i n g the l u n g to c o l l a pse ( e ith e r p a rti a l ly o r c omp l etely) . A m i no r l u n g c o l l a pse wi l l often reso lve on its own, but when the p neumotho rax is l a rg e r, a n e ed l e or tu be is usua l l y i n se rted between the ri bs to remove th e g a s over a p e riod of a few d ays, wh i c h pe rm its th e l u n g to re i nf late.
c. Alveolar macrophages (a lveo lar phagocytes; dust cel ls) (see Figure 15 .3) (1 ) are the principal mononuclear phagocytes of the alveolar surface. (2) remove inhaled dust, bacteria, and other particulate matter trapped in the pulmonary
surfactant, thus providing a vital line of defense in the lungs. (3) migrate to the bronchioles after filling with debris. From there, they are carried via
c i l i a ry action to the upper airways, eventually reaching the oropharynx, where they are either swallowed or expectorated.
(4) may also exit by migrating into the interstitium and leaving via lymphatic vessels.
l!n'l(�NIII Asbestosis
1 . Asbestos is is a p u lmona ry d isease c a used by i n h a l i n g asbestos fi b e rs (used i n i nsu l atio n materi a ls , ti l es , etc . ) .
2 . The fi b e rs d e pos it i n th e a lveo l a r d u cts a n d a lveo l i . The sma l l e r fi b e rs a re p h ago cytosed by m a c ro p h a ges, b ut the l a rg e r ones pen etrate th e l u n g i nte rstiti um .
3 . Activated m a c rophages r e l e a s e infl a m mato ry med i ato rs, wh i c h l e a d t o i nterstit ia l pulmonary f ibrosis in the wa l l s of resp i rato ry b ronch i o l es, a lve o l a r d u cts, a n d a lveo l i .
4 . Asbestos bodies, fi b e rs 1 0 to 50 � m l ong e n c rusted with beads o f p rote in , f o rm i n th e i nte rstiti u m a n d a lveo l a r s paces . The asbestos bod i es sta i n stron g ly fo r i ron b e c a use of th e hemog l ob i n p rote i n re l e ased from sma l l h em orrh ages that a c c o m pany the fi b ros is .
Emphysema 1 . Emphysema resu lts from destruction of a lveo lar wal ls and formati on of l a rg e cyst- l i ke s acs,
red u c i n g th e su rfa c e a re a ava i l a b l e fo r g as exchange . 2 . It is ma rked by decreased e lastic ity o f t h e l u n gs, wh i c h a re u n a b l e t o r e co i l a d e q uately d u ri n g
expi rati on . I n time , th e l u n gs expand a n d e n l a rg e th e tho ra c i c c avity ( b a rre l c hest) . 3. Emphysema is assoc i ated with exposu re to cigarette smoke and other substances that inh ib it
a1 -antitrypsin, a p rote i n that no rm a l ly p rote cts the l u n gs from the a ctio n of elastase p ro d u ced by a lveo l a r m a c ro p h a ges .
4. It c a n be a he red ita ry cond iti on res u lti n g f rom a d efe ctive a1 -a ntitryps in . I n s u ch c a ses, g e ne th e ra py with re comb i n a nt a1 - a ntitryps in i s b e i n g used i n a n effo rt t o c o rrect t h e p rob l em , a n d it h as re c ently b een s u c c essfu l in boost ing the ava i l a b i l ity of th is p rote ctive p rote i n .
E. l ntera lveolar septum 1. The interalveolar septum is the wall, or partition, between two adjacent alveoli. 2. It is bounded on its outer surfaces by the extremely thin, simple, squamous epithelium lining
the alveoli. 3. It contains many e lastic and reticu lar f ibers in its thicker regions. 4. It houses conti nuous cap i l laries in its central (interior) region.
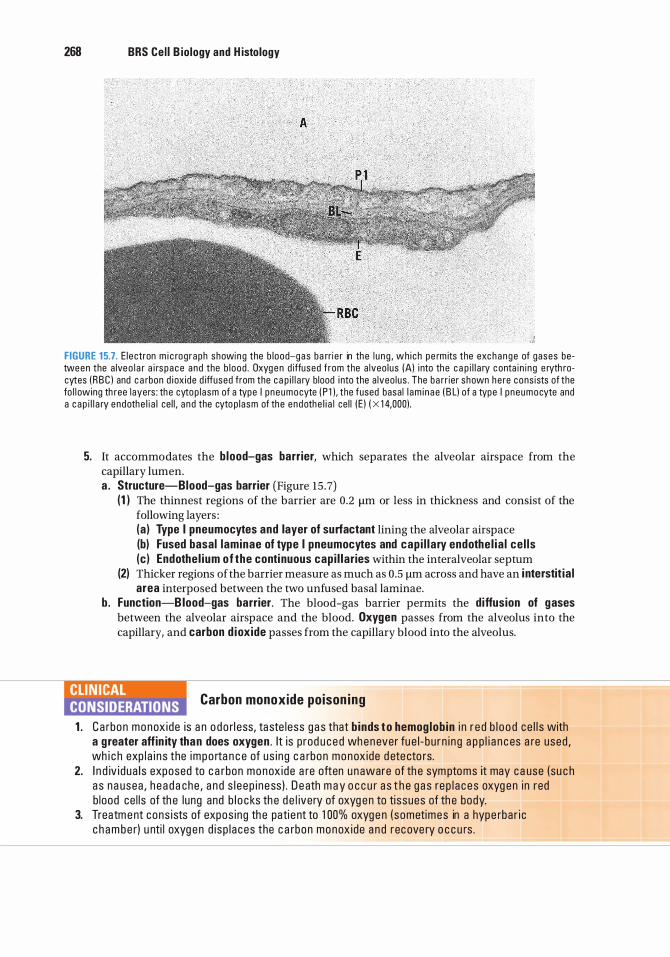
268 BRS Cel l B iology and H istology
; . ) A
FIGURE 1 5.7. E le ctron m i c rog raph showing the b lood-gas ba rri e r in the l u ng , wh i ch pe rm its the exchange of gases between the a lve o l a r a i rs pace and the b l ood . Oxyg e n d iffused f rom the a lveo lus IAl i nto the c a p i l l a ry c onta i n i ng e ryth rocytes ( RBC ) and c a rbon d i ox ide d iffused from the c a p i l l a ry b lood i nto the a lveo lus . The ba rr ier shown he re cons ists of the fo l l owing th ree layers : the cytop l asm of a type I p neumocyte ( P l ) . the fused basa l l am i n ae ( B L) of a type I p neumocyte and a c ap i l l a ry endothe l i a l ce l l , a nd the cyto p l asm of the endothe l i a l ce l l ( E ) ( X 1 4,000).
5. It accommodates the b lood-gas barrier, which separates the alveolar airspace from the capillary lumen. a . Structure-Blood-gas barrier (Figure 15 .7)
(1 ) The thinnest regions of the barrier are 0.2 11m or less in thickness and consist of the following layers : (a ) Type I pneumocytes and layer of surfactant lining the alveolar airspace (b) Fused basal laminae of type I pneumocytes and cap i l la ry endothe l ia l ce l ls (c) Endothe l ium of the conti nuous cap i l laries within the interalveolar septum
(2) Thicker regions of the barrier measure as much as 0.5 1-!m across and have an i nterstit ia l area interposed between the two unfused basal laminae.
b. Function-Blood-gas barrier. The blood-gas barrier permits the diffusion of gases between the alveolar airspace and the blood. Oxygen passes from the alveolus into the capillary, and carbon d ioxide passes from the capillary blood into the alveolus.
llYftiJB Carbon monoxide poison ing
1 . Ca rbon monox ide is a n o do rl ess, taste less g a s that b inds t o hemog lob in i n r e d b l o o d ce l l s with a g reater affin ity than does oxygen . It is p rod u ced whenever fu e l - b u r n i ng a p p l i a n c es a re used , wh i c h exp l a i n s the impo rta n c e of us i ng c a rbon monox ide d ete cto rs.
2. I n d iv i dua l s exposed to c a rbon monox ide a re often u naware of th e sym ptoms it may ca use (su c h a s na usea , h e a d a che , a n d s l e ep i n ess ) . D e ath m a y o c c u r a s t h e g a s re p l a c es oxyg en i n red b lood ce l l s of th e lung and b l o c ks th e d e l ivery of oxyg en to ti ssues of th e body.
3. Treatm e nt cons i sts of expos ing th e pati e nt to 1 00% oxyge n ( sometimes in a hype rba r i c c h a m be r) u nti l oxyg en d i sp l aces the c a rbon monox ide a n d recove ry o c c u rs .
I!1JtJttQi1ij Resp i rato ry System 269
A. Lung lobules vary greatly in size and shape, but each has an apex directed toward the pulmonary hilum and a wider base directed outward.
B. Each lobule contains a s ing le pr imary bronchio le , which enters at the apex and branches to form five to seven terminal bronchioles. The terminal bronchioles in turn divide, ultimately giving rise to alveoli at the base of the lobule.
A. Pulmonary artery 1. The pulmonary artery carries blood to the lungs to be oxygenated . 2. I t enters the root of each lung and extends branches along the divisions of the bronchial tree. 3. It enters lung lobules, where its branches fo l l ow the bronch io les (see Figure 15 .2).
B. Pulmonary veins 1. In lung lobules, pulmonary veins run in the intersegmental connective tissue, separated from
the arteries. 2. After leaving the lobules, the pulmonary veins come close to divisions of the bronchial tree
and run para l le l to branches of the pulmonary artery as they accompany bronchi to the root of the lung.
C. Bronchial arteries and veins 1. Bronchial arteries and veins provide nutrients to and remove wastes from the nonrespiratory
portions of the lung (bronchi, bronchioles, interstitium, and pleura) . 2. They follow the branching pattern of the bronchial tree and form anastomoses with the
pulmonary vessels near capillary beds.
The pulmonary nerve supply consists primarily of autonomic f ibers to the smooth musc le of bronchi and bronchio les. Axons are also present in the thicker parts of the interalveolar septa.
A. Parasympathetic stimulation causes contraction of pulmonary smooth muscle.
B. Sympathetic stimu lation causes relaxation of pulmonary smooth muscle and can be mimicked by certain drugs that cause dilation of bronchi and bronchioles.
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1. Characteristics of olfactory epithelium include which one of the following?
(A) It is located in the inferior region of the nasal cavity.
(B ) It is classified as simple columnar. (C) It has an underlying lamina propria
containing mucous glands. (D) It has modified cilia, which act as receptors
for odor. (E ) It is unable to regenerate.
2. Which of the following statements concerning terminal bronchioles is true?
(A) They are part of the conducting portion of the respiratory system.
(B ) They function in gas exchange. (C) They do not contain ciliated cells. (D ) They have cartilage plates present in their
walls. (E) They do not contain secretory cells.
3. The trachea possesses which one of the following components?
(A) Irregular cartilage plates in its wall (B ) Skeletal muscle in its wall (C) An epithelium containing only two cell types (D ) A thick basement membrane underlying
its epithelium (E ) Bowman glands in its lamina propria
4. Which of the following statements concerning respiratory bronchioles is true?
(A) No gas exchange occurs in them. (B ) They do not have alveoli forming part of
their wall. (C) They contain goblet cells in their lining
epithelium. (D ) They are included in the conducting
portion of the respiratory system. (E) Ciliated cells comprise a portion of their
lining epithelium.
270
5. True statements about asthma include which one of the following?
(A) It is due to a loss of lung elasticity. (B ) It eventually causes the lungs to expand
and leads to a barrel chest. (C) It is associated with difficulty expiring air
from the lungs. (D ) It may be helped by gene therapy using
recombinant <Xi -antitrypsin. (E) It is usually not associated with
inflammation.
6. Which of the following statements concerning alveolar macrophages is true?
(A) They secrete <Xi -antitrypsin. (B ) They secrete elastase. (C ) They originate from blood neutrophils. (D ) They may play a role in causing hyaline
membrane disease. (E) They secrete small amounts of
surfactant.
7. Which one of the following disorders may in some cases be successfully treated with antielastase (<Xi -antitrypsin}?
(A) Asbestosis (B ) Asthma (C ) Carbon monoxide poisoning (D ) Emphysema (E) Hyaline membrane disease
8. Which one of the following is characterized by interstitial pulmonary fibrosis?
(A) Asbestosis (B ) Asthma (C ) Carbon monoxide poisoning (D ) Emphysema (E) Hyaline membrane disease

9. Which one of the following is associated with a barrel chest?
(A) Asbestosis (B ) Asthma (C ) Carbon monoxide poisoning (D ) Emphysema (E) Hyaline membrane disease
I!1JtJttQi1ij Resp i rato ry System 271
1 0. Which one of the following is frequently treated successfully with glucocorticoids?
(A) Asbestosis (B) Asthma (C) Carbon monoxide poisoning (D ) Emphysema (E) Hyaline membrane disease
Answers and Explanations
1 . D . The olfactory epithelium possesses nonmotile cilia, which act as receptors for odor. They are extensions of the bipolar nerve cells that form part of this tall, pseudostratified epithelium located in the roof of the nasal cavity. Bowman glands, which lie in the lamina propria beneath this epithelium, produce a watery secretion, which moistens the olfactory surface (see Chapter 1 5 II A).
2. A. Terminal bronchioles are the most distal components of the conducting portion of the respiratory system. They lack alveoli and thus do not function in gas exchange. They are lined by an epithelium composed of two cell types : secretory (Clara) cells and ciliated cells. Cartilage is not present in bronchioles (see Chapter 15 II F) .
3. D . The pseudostratified ciliated columnar epithelium lining the trachea rests on a thick basement membrane and contains five cell types. The trachea possesses C-shaped cartilages with smooth muscle (the trachealis) extending between their ends. Bowman glands are found only in the nasal cavity and produce a thin watery secretion (see Chapter 15 II D) .
4. E . Respiratory bronchioles have alveoli interrupting their walls, so some gas exchange takes place at this level. Their remaining walls are lined by a simple cuboidal epithelium consisting of Clara cells and ciliated cells. Respiratory bronchioles are categorized as part of the respiratory portion of the system (see Chapter 15 III A) .
5. C. Asthma results from the constriction of smooth muscle in the bronchioles, which decreases their diameter and makes the expiration of air very difficult. Mucus accumulates in the airways, and inflammatory cells invade the bronchiolar walls (see Chapter 15 II F Clinical Considerations) .
6. B . Alveolar macrophages secrete elastase. Normally, «:xi -antitrypsin, a serum protein, interacts with elastase, thereby protecting the lung against damage that may lead to emphysema. Alveolar macro phages, like all macro phages, arise from blood monocytes; they do not secrete surfactant; and they are unrelated to the pathogenesis of hyaline membrane disease (see Chapter 15 III D Clinical Considerations) .
7. D. Hereditary forms of emphysema are now being treated with recombinant «:xi -antitrypsin, which has antielastase activity (see Chapter 15 III D Clinical Considerations) .
8. A. Inhaling asbestos fibers causes interstitial pulmonary fibrosis in the walls of respiratory bronchioles, alveolar ducts, and alveoli. Asbestos bodies are a classic feature of asbestosis. After prolonged heavy exposure to asbestos, this disease may progress to mesothelioma (a malignant tumor) (see Chapter 15 III D Clinical Considerations) .
9. D. A loss of lung elasticity in emphysema makes it difficult for the lungs to recoil normally during expiration. The lungs and thoracic cavity enlarge, producing a barrel chest (see Chapter 15 III D Clinical Considerations) .
1 0. E. Glucocorticoids, which stimulate synthesis of pulmonary surfactant, are often administered to the expectant mother a few days prior to delivery to prevent or alleviate hyaline membrane disease in the premature infant (see Chapter 15 III D Clinical Considerations) .
272
Digestive System : Oral Cavity and Alimentary Tract
I. OVERVIEW-THE DIGESTIVE SYSTEM
A. The digestive system comprises the ora l region and a l imentary canal (esophagus, stomach, and sma l l and large intestines) and several extrinsic g lands .
B. I t consists of a hollow tube (highly modified in the oral cavity) of varying diameter, composed of a mucosa, submucosa, muscularis externa, and serosa ( or adventitia ) .
C. Function. The digestive system secretes enzymes and hormones that function in ingestion, digestion, and absorption of nutrients and in the elimination of indigestible materials.
The oral region includes the l i ps; pa late; teeth and associated structures; tongue; major salivary glands; and lingual, palatine, tubal, and pharyngeal tonsils, where the tonsils (collections of lymphoid nodules) form Waldeyer tonsilar ring, to protect the entryways into the alimentary canal and the respiratory system. The oral region is lined in most places by a stratified squamous epithe l ium whose ep ithe l i a l r idges interdigitate with tall connective tissue pap i l l ae (connective tissue ridges) of the subjacent connective tissue. The epithelial ridges and the connective tissue ridges are collectively known as the rete apparatus. The epithelium and connective tissue together form the mucosa. The oral cavity has three types of mucosae: l i n ing mucosa, whose epithelium is nonkeratinized; masticatory mucosa, whose epithelium is keratinized; and spec ia l ized mucosa, whose nonkeratinized stratified squamous epithelium possesses taste buds. The dorsal surface of the tongue, hard palate, and gingivae are the only regions that possess masticatory mucosa; the dorsum of the tongue, soft palate, and regions of the pharynx possess specialized mucosa; the remainder of the oral cavity is lined by lining mucosa. The histology of the tongue is described at the end of Section II of this chapter.
A. The l i ps are divided into the external (skin) reg ion, the vermi l ion zone, and the internal (mucosa l ) reg ion . The first two regions are covered by stratified squamous keratinized epithelium, whereas the internal region is lined by a wet stratified squamous nonkeratinized epithelium. 1 . A dense irregular collagenous connective tissue core envelops skeletal muscle. 2. Sebaceous g lands, sweat g lands, and ha i r fo l l ic les are present in the external region; minor
sal ivary g lands in the internal region; and occasional, nonfunctional sebaceous glands (known as Fordyce g ranu les) in the internal region and vermilion zone.
273
274 BRS Cel l B iology and H istology
B. The palate separates the nasal cavity from the oral cavity and is divided into an anterior hard pa late (possessing a bony shelf in its core) and a posterior soft pa late (possessing skeletal muscle in its core) . At the posterior terminus of the soft palate is the uvu la . Therefore, the palate has a nasal aspect and an oral aspect. The entire nasal aspect of the palate (with the exception of the uvula) is lined by pseudostratified c i l iated columnar ep ithe l ium (respiratory epithelium) . 1 . The hard pa late is lined on its oral aspect by stratified squamous parakerati n ized to stratified
squamous kerati n ized epithelium. It contains adipose tissue anteriorly and minor mucous salivary glands posteriorly in the oral aspect of its connective tissue, also known as the mucoperiosteum.
2. The soft pa late is lined on its oral aspect by stratified squamous non keratin ized epithelium. It contains minor mucous salivary glands in the oral aspect of its connective tissue.
1. Herpetic stomatitis i s c aused by h e rpes s imp lex v i rus ( H SV) type 1 . I n CLIN ICAL CONSIDERATIONS the do rmant state, t h i s v i r u s r es i des i n the tr ig em i n a l g ang l i a . H SV type
1 i nfecti on i s very common a n d is tra nsm itted by kiss i ng . Th i s i nfecti on is c h a ra cte r ized by pa i n fu l feve r b l iste rs on t he l i p s o r i n t he v i c i n ity o f th e nostri l s . These b l i ste rs exud e a c l e a r fl u i d o r a re c overed by a scab .
2. Angu lar che i l itis (per leche) is a pa infu l c o nd iti on , u sua l ly i n p at ie nts o l d e r th a n 50 yea rs o f a g e , i n wh i ch the co rne rs of th e mouth h ave sho rt e ryth ematous f issu res a n d c ra c ks that a re infl amed and may become i nfected with Candida albicans o r with o c c as i ona l s e conda ry ba cte r i a l c o l o n izati on by Staphylococcus au reus. Li c ki n g th e co rne r of the mouth exa c e rbates and p ro l ongs th e cond itio n . Treatment is u s u a l ly with an a ntifu n g a l o i ntm e nt, a n d i n case of a s e conda ry b a cteri a l infection , a n a nti b i oti c reg imen a n d behav iora l mod if ic ati on , that is , hav ing th e pati e nt res ist the u rge to l i ck the co rne rs of the mouth .
3. Cancers of the oral reg ion most c ommon ly affect th e l i ps, to n g ue , a n d fl oo r of the mouth . These c a n c e rs i n iti a l ly resemb l e l e u ko p l a ki a and a re a sym ptomati c . S u rviva l rate is h i gh if these c a n c e rs a re re cogn ized and t reated i n the ea rly sta g es .
C. Teeth 1 . Overview-Teeth
a. Teeth are composed of an internal soft tissue, the pu lp, and three calcified tissues : enamel and cementum, which form the surface layer, and dentin , which lies between the surface layer and the pulp. As in bone, calc ium hydroxyapatite is the mineral material in the calcified dental tissues.
b. Teeth have an enamel-covered crown, a cementum-covered root, and a cervix, the region where the two surface materials meet.
2. Components-Teeth a . Enamel
(1 ) has a highly calcified matrix with an organic component that is composed mostly of the fibrous keratin-like protein, enamel in , a substance that is elaborated by ameloblasts during formation of the crown and becomes calcified by the deposition of calc iumhydroxyapatite c rysta ls . I t consists of only 4% organic material and 96% inorganic material and, thus, is the most calcified tissue in the body.
(2) is ace l lu lar after tooth eruption and therefore cannot repair itself.
CLIN ICAL CONSIDERATIONS
The bacte r ia l f lora of the o ra l c avity a cts on food remnants l odged between teeth and in th e g i n g iva l su l c us, the no rma l ly t iny c revi c e between t he g u m
and t h e e n a m e l o f th e tooth . A s t h e ba cte r ia meta bo l ize t h e s u ga rs i n th e food deb ris, they prod uce l a c t i c a c id th at c a n d isso lve e n o u g h o f t h e ca l c i um-hyd roxya patite c rysta ls t o form c a rious l es ions (tooth d e c ay), u n less th e i nd iv id u a l p ra cti ces good ora l hyg i ene . The use of fl uor ide in the wate r supp ly (system i c a pp l i c atio n ), as we l l as the a dd it ion of f l uor ide in tooth paste (top i c a l a p p l i c ation ) , m a kes ename l more res ista nt t o b acteri a l a c i d s by a lte r ing th e hyd roxyapatite c rysta l s (fl uo r i de re p l aces hyd roxyl mo l e cu les ) . Mo reove r, the prese nce of f l uor ide on th e ename l s u rfa c e cata lyzes its rem i ne ra l izati on .
l!1ltJ'!1tJiij D i g estive System : O ra l Cavity a n d A l imenta ry Tra ct 275
b. Denti n (1 ) surrounds the central pu lp chamber of the crown and pu lp (root) cana l . (2) has a calcified matrix containing mostly type I co l lagen f ibers. (3) is manufactured by odontoblasts, which persist and continue to elaborate dentin for
the life of the tooth. c. Cementum
(1 ) has a mostly type I co l lagen-conta in ing calcified matrix, which is produced by cementob lasts.
(2) is conti nuously e laborated even after tooth eruption, since it compensates for the decrease in tooth length resulting from abrasion of the enamel.
d . Dental pu lp (1 ) i s a gelatinous, richly vascularized connective tissue containing odontob lasts in its
peripheral layer (closest to the dentin), fibroblasts and mesenchymal cells, and thin types I and III collagen fibers.
(2) contains afferent nerve f ibers. All sensations from the pulp are interpreted as pain in the central nervous system.
3. Crown formation a . The crown begins to form 6 to 7 weeks after conception as a horseshoe-shaped band, the
dental lamina, which is derived from the oral ep ithe l ium. A dental lamina develops in each jaw and projects into the underlying ectomesenchyme. The development of teeth, known as tooth germs, depends on the interaction, known as ep ithe l ia l-mesenchymal i nteraction, between the epithelium and the ectomesenchyme (neural crest-derived mesenchymal tissue). This interaction is dependent on various signaling molecules produced by both the epithelium and the ectomesenchyme. A tooth germ has two components : the epithelially derived enamel organ and the ectomesenchymally derived denta l pap i l l a surrounded by the ectomesenchymally derived denta l sac. The enamel organ is responsible for the formation of the enamel and j unctional ep ithe l ium; the dental papilla will give rise to dentin and the pu lp; and the dental sac will form the attachment apparatus, namely cementum, periodontal l igament, bony a lveolus, and the connective tissue of the g ing iva .
b. The crown forms before the root formation begins. c. The sequential stages of crown formation of the tooth germ are bud, cap, be l l , and
appositiona l stages. d . The ectomesenchyme releases Activin �A and bone morphogenic prote in 4 (BMP 4),
stimulating the epithelium to form epithelial downgrowths, known as the bud, 10 buds along the maxillary and l 0 buds along the mandibular dental laminae.
e. Each bud, in tum releases fibroblast growth factor 4 as well as BMP 2, BMP 4, and BMP 7, which instruct the tooth germ to assume a specific shape (incisor, canine, premolar, or molar) .
4. Root formation follows completion of the crown and is accompanied by tooth eruption.
D. Denta l-supporting structures (Attachment apparatus) 1. The periodontal l igament is composed of a dense irregular collagenous connective tissue
whose type I collagen fibers are arranged in five pr inc ipa l f iber bund les, which extend from cementum to bone (alveolar crest, horizontal, oblique, apical, and interradicular fiber groups), suspending the tooth in its a lveo lus.
2. G ing ivae (gums) are covered by stratified squamous kerati n ized (or parakerati n ized) epithelium; their collagen fibers are also arranged in five princ ipa l fiber bund les (alveologingival, dentogingival, circular, dentoperiosteal, and transseptal fiber groups) .
3. Alveolar bone consists of an inner layer of compact bone (cribriform p late, or alveolar bone proper). There is also an outer layer (cortical p late) of compact bone with an intervening layer of cancellous bone (spongiosa ) .
E. Tongue 1 . Overview-Tongue
a . The tongue is divided into an anterior two-thirds and a posterior one-third by the V-shaped sulcus termina l is, whose posteriorly pointing apex ends in the foramen cecum.
b . Its dorsal surface is covered by stratified squamous parakerati n ized to keratin ized epithelium, whereas its ventral surface is covered by stratified squamous nonkerati n ized
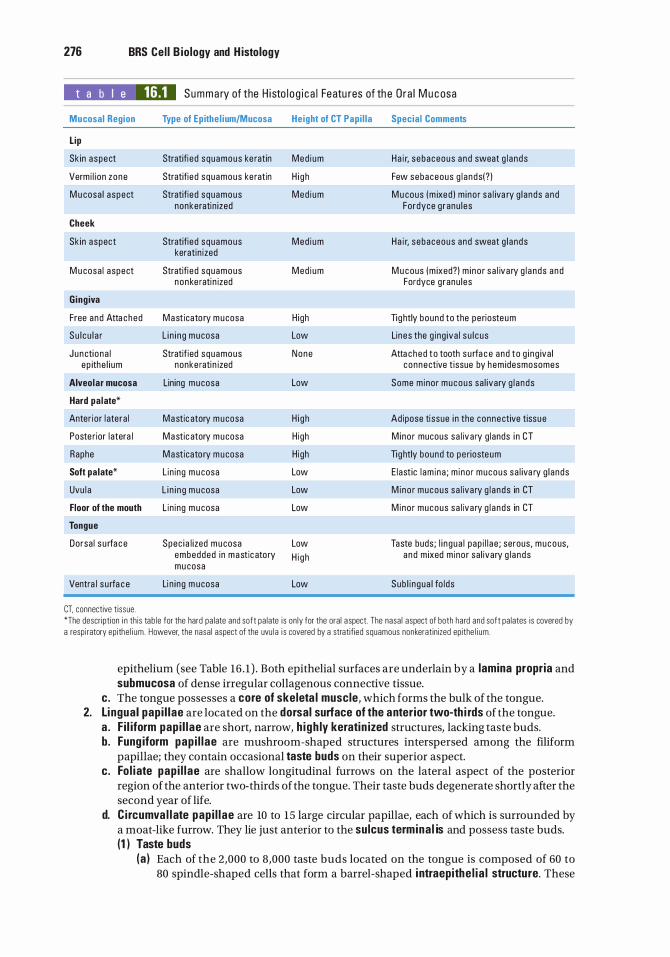
276 BRS Cel l B iology and H istology
t a b I e 16.1 Summa ry of the H i sto l o g i c a l Featu res of th e Ora l Mu c osa
Mucosal Region Type of Epithe l ium/Mucosa Height of CT Papi l la Special Comments
Lip
Sk in aspect Stratifi e d squamous ke ratin Med i um Ha i r, sebaceous a nd sweat g l a nds
Verm i l i on zone Stratifie d squamous ke ratin H i g h Few sebaceous g l a nds( ? )
M u cosa l aspect Stratifie d squamous Med i um M u cous (m ixed ) m ino r sa l iva ry g l ands a nd nonkeratin i zed Fordyce g ranu l es
Cheek
Sk in aspect Stratifie d squamous Med i um Ha i r, sebaceous and sweat g l a nds keratin ized
M u cosa l aspect Stratifi e d squamous Med i um M u cous (m ixed? ) m i no r sa l iva ry g l a nds a nd nonke rati n ized Fordyce g ranu les
Ging iva
Free and Atta ched Mast icato ry m ucosa H igh Tig htly bound to the pe riosteum
Su l c u l a r L i n i n g m ucosa Low Lines the g ing iva l s u l c us
J unctiona l Stratif ied squamous None Atta ched to tooth surfa c e and to g i n g iva l e p ithe l i um nonke rati n ized connective t issue by hem idesmosomes
Alveolar mucosa Lining m ucosa Low Some m inor mucous sa l ivary g l a nds
Hard palate*
Anter ior l ate ra l Mastic atory m ucosa H i g h Ad ipose ti ssue i n the connective tissue
Poste r ior l atera l Mastic atory m ucosa H igh M ino r mucous sa l iva ry g lands i n CT
Raphe Masticato ry m ucosa H igh Tightly bound to pe riosteum
Soft palate* L in ing m u cosa Low E last ic l am i na ; m i no r mucous sa l iva ry g l ands
Uvu l a L i n i n g m u cosa Low M ino r mucous sa l iva ry g l a nds in CT
Floor of the mouth L in ing m u cosa Low Mino r mucous sa l iva ry g l a nds in CT
Tongue
Dorsa l s u rfa c e Spec i a l i zed m ucosa Low Taste buds ; l i n gua l pap i l l a e ; serous, mucous, embedded in mastic atory H i gh a nd m ixed m inor sa l ivary g l a nds mu cosa
Ventra l s u rfa c e Li n i ng m ucosa Low Sub l i n gua l fo l ds
CT. connective t issue . *The descr ipt ion i n th is tab le for the hard pa late and soft pa late i s on ly for the ora l aspect The nasa l aspect of both hard and soft pa lates is covered by a respi ratory ep ithe l i um . However, the nasa l aspect of the uvu la i s covered by a stratif ied squamous nonkeratin ized epithe l i um .
epithelium (see Table 16 . 1 ) . Both epithelial surfaces are underlain by a lamina propria and submucosa of dense irregular collagenous connective tissue.
c. The tongue possesses a core of skeleta l muscle, which forms the bulk of the tongue. 2. Li ngual pap i l lae are located on the dorsal surface of the anterior two-th i rds of the tongue.
a . Fi l iform pap i l lae are short, narrow, h igh ly keratin ized structures, lacking taste buds. b. Fung iform pap i l l ae are mushroom-shaped structures interspersed among the filiform
papillae; they contain occasional taste buds on their superior aspect. c. Fo l iate pap i l l ae are shallow longitudinal furrows on the lateral aspect of the posterior
region of the anterior two-thirds of the tongue. Their taste buds degenerate shortly after the second year of life.
d. C i rcumva l l ate pap i l l ae are 10 to 15 large circular papillae, each of which is surrounded by a moat-like furrow. They lie just anterior to the sulcus termina l is and possess taste buds. (1 ) Taste buds
(a ) Each of the 2,000 to 8,000 taste buds located on the tongue is composed of 60 to 80 spindle-shaped cells that form a barrel-shaped i ntraepithe l ia l structure. These
l!1ltJ'!1tJiij D i g estive System: O ra l Cavity and A l imenta ry Tra ct 277
structures are located on the superior surface of fungiform papillae, on the lateral surfaces of circumvallate papillae, and in the wal ls of the surrounding moatlike furrows. Each taste bud has a small opening, the taste pore, from which microvilli (taste ha i rs) project into the oral cavity (or into the moat surrounding the circumvallate papilla).
(b) Four different cells may be recognized, three of which are spindle shaped: dark cells (type I cells), light cells (type II cells), and intermediate cells (type III cells) have short life spans; the fourth type are the short, regenerative, basal cells. Types I, II, and III cells form synapses with afferent nerve f ibers that deliver the taste information to the central nervous system.
(c) When basal cells divide, they give rise to a basal cell and a dark cell. As the dark cell matures, it becomes a light cell, and as it degenerates, it becomes an intermediate cell . These three cell types are neuroep ithe l i a l cells whose microvilli, the taste hairs, recognize one specific tastant. The process of going from a newly formed dark cell to a dead intermediate cell takes about 10 days. A particular taste bud contains a variety of neuroepithelial cells that recognize all tastants, but each taste bud appears to be specialized to respond to only one or two of the tastants.
(d) Function . Taste buds perceive salty, sour, bitter, sweet, and umami (glutamate receptor that senses delicious flavors) taste sensations, and some, in individuals who have the genetic capability, may specialize in tasting fats. The chemical moieties of the food substances that are recognized by taste buds are known as tastants .
(e ) Salt and sour tastants stimulate sodium and hydrogen ion channels, respectively; sweet, bitter, and umami tastants stimulate G protein-linked receptors; and fatty tastants stimulate fatty acid transporters.
CLIN ICAL CONSIDERATIONS
I t a p p e a rs t ha t the mo re mo l e c u l es o f a p a rti c u l a r tasta nt b i n d to a n e u roep ithe l i a l ce l l , the stron ge r th e taste sensati on . Recently, it h as been
shown th at t he ta ste re c e ptors a l so h ave b i n d i n g s ites f o r nontasta nt mo l e c u l es that a ct a s enhancer molecules. Th e refo re, when e n h a n c e r mo l e c u l e s b ind a l o n g with tasta nts, th e ta sta nts a re l o c ked i n th e re c e pto r for a l onger pe ri od of time . Thus, the tasta nt-e n h a n c e r mo l e c u l e c omb i n atio n a u g m e nts th e taste sensat ion so that the b i n d i n g of o n ly a few tasta nt mo l e c u l es is i nterp reted as if m a ny s u c h tasta nt mo l e c u l es were present.
The sense of ta ste i s a com p lex i nte ra cti on between th e i nfo rmati on that th e b ra i n re c e ives from the taste bu ds; from senso ry c e l l s that d ete rm i ne the tem p e ratu re, s p i c i n ess, and texture of th e food ; a s we l l as from retronasal o lfaction . The process of retronasa l o lfacti on depends on o lfa cto ry ce l l s l o c ated i n the poste r io r a spect o f th e n asa l cavity, a n d t he odo r that they pe r ce ive a r i ses from th e b a c k of the mouth rath e r tha n th e mo re common ly tho ught of orthonasa l o lfaction, where the odo r i s pe rce ived v i a a i r e nte r i ng the n asa l c avity. An a d d iti o n a l c omponent o f t he pe r ceptio n o f taste i s th e vis u a l informati on that th e b ra i n g l e a n s v ia the sense of s ig ht. An unusua l ly c o l o red vers ion of a p a rti c u l a r food mo rse l may e l i c it a sense of d i sgust, a pe rce ived a lte red taste, a n d th e i n a b i l ity to consume th e food su bsta n c e .
(2) G lands o f von Ebner are minor salivary glands that deliver their serous secretion into the furrow surrounding each papilla, assisting the taste buds in perceiving stimuli. These glands also deliver their saliva into the furrows of the foliate papillae.
3. The muscu lar core of the tongue is composed of bundles of skeleta l muscle f ibers arranged in three planes with minor sal iva ry g lands interspersed among them.
4. A l ingua l tonsi l is located on the dorsal surface of the poster ior one-th i rd of the tongue.
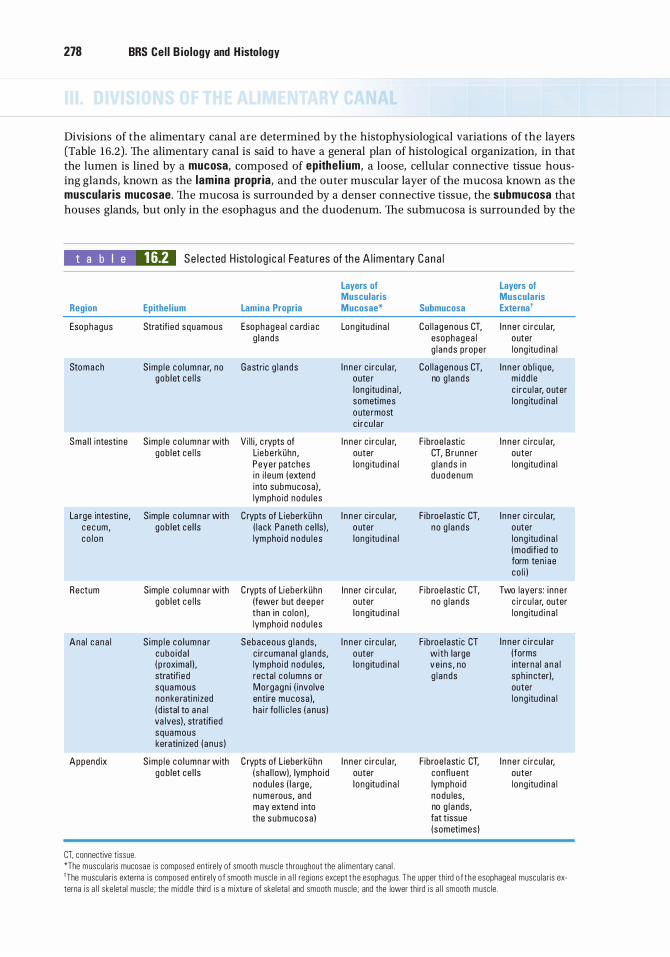
278 BRS Cel l B iology and H istology
Divisions of the alimentary canal are determined by the histophysiological variations of the layers (Table 16.2) . The alimentary canal is said to have a general plan of histological organization, in that the lumen is lined by a mucosa, composed of epithe l i um, a loose, cellular connective tissue housing glands, known as the lamina propria, and the outer muscular layer of the mucosa known as the muscularis mucosae. The mucosa is surrounded by a denser connective tissue, the submucosa that houses glands, but only in the esophagus and the duodenum. The submucosa is surrounded by the
t a b I e 16.2 Se l e cted H isto l o g i c a l Featu res of th e A l imenta ry Cana l
Layers of Muscularis
Region Epithel ium Lamina Propria Mucosae* Submucosa
Esophagus Stratifi ed squamous Esophagea l c a rd i a c Long itud i n a l Co l l a genous CT, g l ands esophagea l
g l a nds proper
Stomach S imp l e co l umna r, no Ga stric g l a nds I n ne r c i r cu l a r, Co l l a genous CT, gob let ce l l s oute r no g l a nds
long itud i na l , sometimes oute rmost c i r cu l a r
Sma l l i ntesti ne S imp l e co l umna r with V i l l i , c rypts of I n n e r c i r cu l a r, F ibroe l astic gob let ce l l s Liebe rkiihn , outer CT, B runner
Peyer patc hes long itu d i n a l g l a nds i n i n i l e um ( extend d uodenum into submucosa ) , lym pho id nodu l es
La rge intestine , S imp le co l umna r with Crypts of L ieberkiihn I n n e r c i r cu l a r, F ibroe l astic CT, c e c um, gob let ce l l s ( l ack Paneth ce l ls ) . o uter no g l a nds co l o n lym pho id nodu l e s l ong itu d i n a l
Rectum Simp le co l umna r with C rypts of Li eberkiihn Inner c i r cu l a r, F ibroe l astic CT, gob let c e l ls (fewer but deepe r outer no g l a nds
than in co lon ) , l ong itud i n a l lym pho id nodu l e s
Ana l c ana l S imp l e co l umna r Sebaceous g l a n ds, I n n e r c i r c u l a r, F ibroe l astic CT cubo i da l c i r c umana l g l a n ds, o uter with large ( p roxima l ) . lym pho id nodu l es, l ong itud i n a l ve i n s , no stratifi e d recta l co l umns or g l a nds squamous Morgagn i ( involve nonke rati n ized entire m ucosa ), ( d istal to a n a l h a i r fo l l i c l es ( a n us ) va lves) . stratifi ed squamous keratin ized ( anus )
Append ix S imp l e co l umna r with C rypts of L ieberkii hn I n ne r c i r c u l a r, F ibroe l astic CT. gob let ce l l s ( sha l l ow). lympho id outer confl u ent
nodu l es ( l a rge , l ong itud i n a l lym pho id n ume rous, and nodu les, may extend i nto no g l a nds, the submucosa ) fat t issue
(sometimes )
CT. connective t issue. *The muscu laris mucosae is composed entirely of smooth musc le throughout the a l imentary cana l .
Layers of Muscularis Externa'
I n n e r c i r c u l a r, outer l ong itu d i n a l
I n n e r ob l i q ue, m i dd l e c i r c u l a r, o uter l ong itud i n a l
I n n e r c i rc u l a r, outer l ong itu d i n a l
I n n e r c i r c u l a r, outer l ong itu d i n a l (modif ied to form ten i ae co l i )
Two layers : i n ne r c i r c u l a r, outer l ong itu d i n a l
I n n e r c i r c u l a r (forms inte rna l a n a l sph i ncter). outer l ong itud i n a l
I n n e r c i r cu l a r, outer l ong itud i n a l
'The muscu lar is externa is composed entirely o f smooth musc le i n a l l regions except t h e esophagus . T h e upper th i rd o f t h e esophageal muscu lar is ex-terna is a l l ske letal musc le ; the midd le third is a m ixture of skeleta l and smooth musc le ; and the lower th i rd is a l l smooth musc le .
l!1ltJ'!1tJiij D i g estive System : O ra l Cavity a n d A l imenta ry Tra ct 279
muscularis extern a, which, in turn, is covered by either a serosa or an adventitia . Variations of the components of these layers permit regional structural and functional specialization of the alimentary canal. Innervation of the alimentary canal is accomplished by the enteric nervous system (whose neurons are located in Meissner [submucosal] and Auerbach [myenteric] p lexuses) . The function of the enteric nervous system is modified by the sympathetic and parasympathetic components of the autonomic nervous system (See Chapter 9 IX) .
A. Esophagus 1 . The esophagus is lined by a stratified squamous nonkeratinized ep ithe l ium. 2 . The lamina propria contains mucus-secreting esophageal cardiac g lands. 3. The muscu laris mucosae varies in thickness and, in the esophagus, it is composed of a single
longitudinal layer of smooth muscle. 4. The submucosa houses mucus-secreting esophageal g lands proper. 5. The upper third of the muscularis extern a is composed only of skeleta l muscle; the middle third
is composed of a combination of smooth and skeleta l muscle; and the lower third is composed only of smooth muscle . The striated muscles are controlled by the vagus nerve (CN X), whereas the smooth muscles are controlled by nerve fibers derived from the enteric nervous system.
6. The muscularis extern a of the esophagus conveys a bolus of food from the pharynx into the stomach by perista ltic activity. Two physiological sphincters (the pharyngoesophageal and the gastroesophageal) in the muscularis externa ensure that the bo lus is transported in only one direction, toward the stomach.
B. Stomach. The stomach ac id ifies and converts the bolus into a thick, viscous fluid known as chyme. It also produces d igestive enzymes and hormones. 1 . General structure-Stomach
a . The stomach exhibits longitudinal folds of the mucosa and submucosa (called rugae) , which disappear in the distended stomach. The gross anatomy of the stomach is divided into four regions (cardiac, fundic, body, and pyloric), but histologically, the stomach is said to have only three regions : the cardiac reg ion (card ia ), where the esophagus joins the stomach; the bulk of the stomach, composed of the fundus and body, which are histologically identical and therefore referred to by histologists as the fund ic reg ion (fundus); and the pyloric reg ion (pylorus), where the stomach joins the small intestine.
b. The lining of the stomach has many well-like openings, known as gastric p its (foveolae), which are shallowest in the cardia and deepest in the pylorus (Figure 16 . 1 ) . The gastric glands of the stomach mucosa deliver their secretions into the bases of the gastric pits. (1 ) Gastric mucosa
(a) The simple columnar epithelium of the gastric mucosa is composed of mucinogenproducing surface l i n ing ce l ls (Figure 16 . 1) , which are not goblet cells but produce a thick, viscous mucus, known as vis ib le mucus, that lines the epithelial lining of the stomach and protects it from the highly acidic chyme and, therefore, from autodigestion. It also houses a very small number of taste cells that, similarly to the taste buds of the tongue, are capable of recognizing the taste sensations, especially bitter, umami, and sweet. These cells are described more fully in the section on the small intestine.
(b) The lamina propria is a loose connective tissue housing smooth muscle cells, lymphocytes, plasma cells, mast cells, and fibroblasts. It contains gastric g lands.
(c ) The muscu laris mucosae is composed of a poorly defined inner circular layer, an outer longitudinal layer, and occasionally an outermost circular layer of smooth muscle.
(2) Gastric submucosa (a) is composed of dense, irregular co l lagenous connective tissue. (b) contains fibroblasts, mast cells, and lymphoid elements embedded in the
connective tissue. (c) houses Meissner (submucosa l ) p lexus. (d ) possesses arterial and venous plexuses that respectively supply and drain the
vessels of the mucosa.
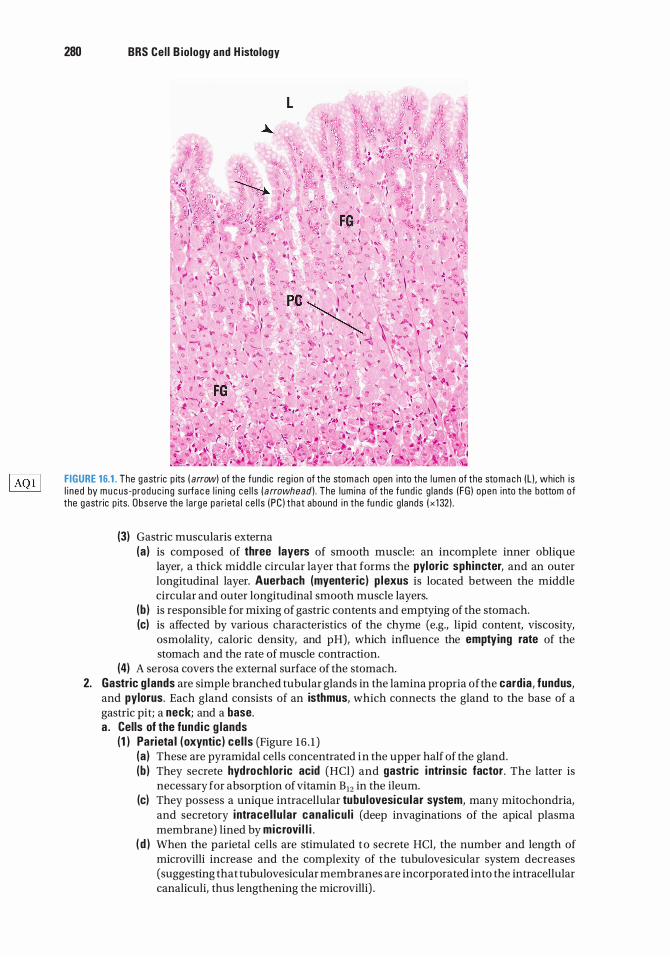
280 BRS Cel l B iology and H istology
FIGURE 16.1 . The gastr ic p its ( arrow) of the fund ic reg i on of the stomach open into the l umen of the sto m a c h (L ) , which i s l i ned by m u c us-prod uc i n g su rfa c e l i n i ng ce l l s ( arrowhead) . The lum ina of the fund i c g lands ( FG ) open into the bottom of the gastr ic p its. Obse rve the l a rge pa ri eta l ce l l s ( PC ) that abound i n the fu nd i c g lands ( x 1 32) .
(3) Gastric muscularis externa (a ) is composed of three layers of smooth muscle: an incomplete inner oblique
layer, a thick middle circular layer that forms the pyloric sph incter, and an outer longitudinal layer. Auerbach (myenteric) p lexus is located between the middle circular and outer longitudinal smooth muscle layers.
(b ) is responsible for mixing of gastric contents and emptying of the stomach. (c) is affected by various characteristics of the chyme (e.g., lipid content, viscosity,
osmolality, caloric density, and pH), which influence the emptying rate of the stomach and the rate of muscle contraction.
(4) A serosa covers the external surface of the stomach. 2. Gastric g lands are simple branched tubular glands in the lamina propria ofthe cardia, fundus,
and pylorus. Each gland consists of an isthmus, which connects the gland to the base of a gastric pit; a neck; and a base. a . Cells of the fund ic g lands
(1 ) Parieta l (oxyntic) cel ls (Figure 16 . 1 ) (a ) These are pyramidal cells concentrated in the upper half of the gland. (b ) They secrete hydroch loric acid (HCl) and gastric i ntrinsic factor. The latter is
necessary for absorption of vitamin B12 in the ileum. (c) They possess a unique intracellular tubu lovesicu lar system, many mitochondria,
and secretory i ntrace l lu lar cana l icu l i (deep invaginations of the apical plasma membrane) lined by microvi l l i .
( d ) When the parietal cells are stimulated t o secrete HCl, the number and length of microvilli increase and the complexity of the tubulovesicular system decreases (suggesting that tubulovesicular membranes are incorporated into the intracellular canaliculi, thus lengthening the microvilli) .
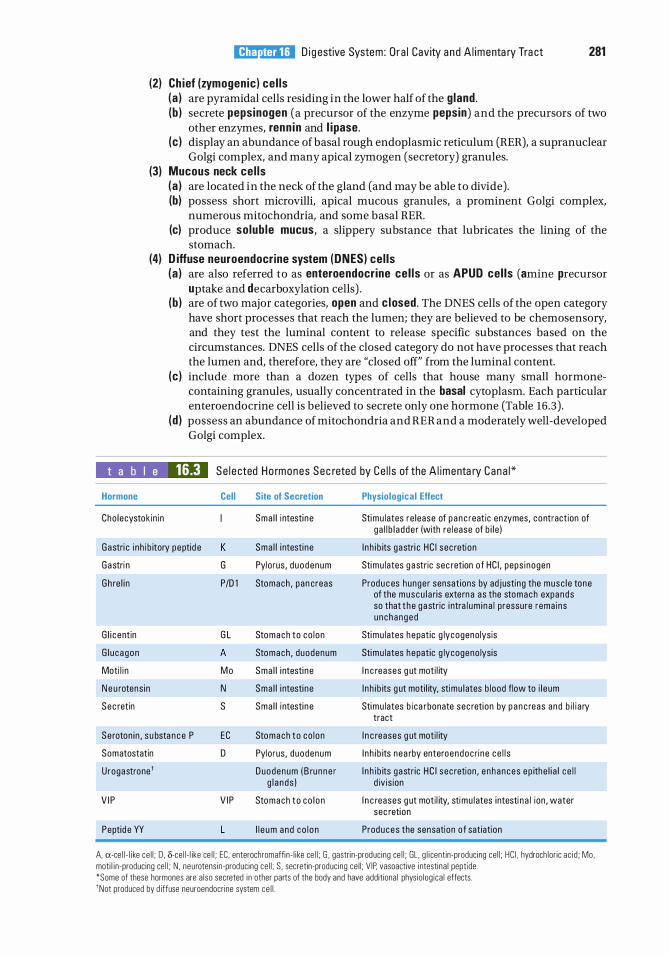
l!1ltJ'!1tJiij D i g estive System : O ra l Cavity a n d A l imenta ry Tra ct 281
(2) Ch ief (zymogenic) cel ls (a ) are pyramidal cells residing in the lower half of the gland . (b ) secrete pepsinogen (a precursor of the enzyme pepsin) and the precursors of two
other enzymes, renn in and l i pase. (c ) display an abundance of basal rough endoplasmic reticulum (RER), a supranuclear
Golgi complex, and many apical zymogen (secretory) granules. (3) Mucous neck ce l ls
(a ) are located in the neck of the gland (and may be able to divide). (b) possess short microvilli, apical mucous granules, a prominent Golgi complex,
numerous mitochondria, and some basal RER. (c) produce solub le mucus, a slippery substance that lubricates the lining of the
stomach. (4) D iffuse neuroendocrine system (ONES) cel ls
(a ) are also referred to as enteroendocrine ce l ls or as APUD cel ls (amine precursor uptake and decarboxylation cells) .
(b ) are of two major categories, open and c losed. The DNES cells of the open category have short processes that reach the lumen; they are believed to be chemosensory, and they test the luminal content to release specific substances based on the circumstances. DNES cells of the closed category do not have processes that reach the lumen and, therefore, they are "closed off" from the luminal content.
(c ) include more than a dozen types of cells that house many small hormonecontaining granules, usually concentrated in the basal cytoplasm. Each particular enteroendocrine cell is believed to secrete only one hormone (Table 16 .3) .
(d ) possess an abundance of mitochondria and RER and a moderately well-developed Golgi complex.
t a b I e 16.3 Se l e cted Ho rmones Sec reted by Ce l l s of the A l imenta ry Cana l *
Hormone Cell
Cho lecystok in in
Gastri c i nh i b itory peptid e K
Gastri n G
Gh re l i n P/0 1
G l i c entin G L
G l u cagon A
Moti l i n M o
N e u rotens in N
Sec retin s
Seroton in , su bsta n c e P EC
Somatostatin D
Urogastrone'
V I P V I P
Peptid e YY L
Site of Secretion
Sma l l i ntesti ne
Sma l l i ntesti ne
Pylorus, d uodenum
Stomach , pan creas
Stomach to co l on
Stomach , duodenum
Sma l l i ntesti ne
Sma l l i ntesti ne
Sma l l i ntesti ne
Stomach to co l on
Pylorus, duodenum
Duodenum ( B ru nne r g l a n ds )
Stomach t o co l o n
I l e um and co l o n
Physiological Effect
Stimu lates re lease of p a n c reatic enzymes, contract ion of ga l l b l a dde r (with re lease of b i l e )
I n h i b its gastri c HC I sec retion
Stimu lates g a stric sec retion of HC I , peps inogen
Produ c es hunger sensat ions by adjusting the musc l e tone of the muscu l a ris extern a as the stomach expands so that t he g a stric i ntra l um i n a l pressure rema ins u nchanged
Stimu lates hepatic g lycogenolysis
Stimu lates hepatic g lycogeno lysis
I n c reases g ut moti l ity
I n h i b its g ut moti l ity, stimu l ates b lood flow to i l eum
Stimu lates b i ca rbonate sec retion by p a n c reas and b i l i a ry tract
I n c reases g ut moti l ity
I n h i b its nea rby enteroendoc ri ne ce l l s
I n h i b its gastr ic HC I sec retion , e nhances ep ithe l i a l c e l l d iv is ion
I n c reases g ut moti l ity, stimu l ates intesti n a l ion , water sec retion
Produces the sensation of satiation
A, a-ce l l - l i ke ce l l ; 0 , o-ce l l - I ike ce l l ; EC, enterochromaffi n - l i ke ce l l ; G , gastri n-produc ing ce l l ; GL, g l i cent in-producing ce l l ; HC I , hydroch lor ic ac i d ; Mo, moti l i n-producing ce l l ; N , neurotens in-produc ing ce l l ; S , secretin-produc ing ce l l ; V IP. vasoactive i ntesti na l peptide. *Some of these hormones are a lso secreted i n other parts of the body and have addit ional phys io log ica l effects. 1Not produced by d iffuse neuroendocr ine system ce l l .
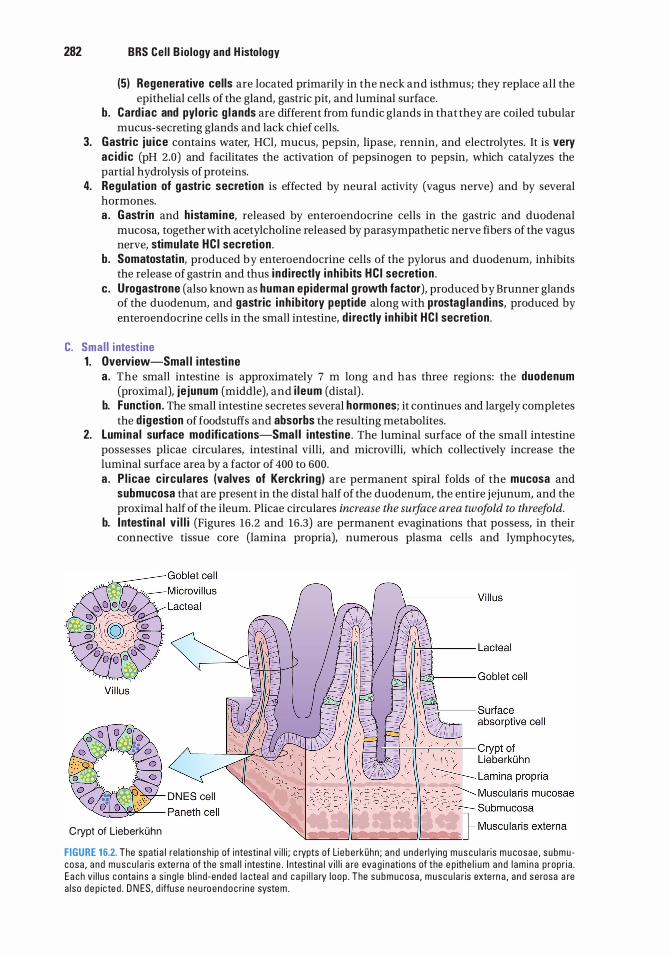
282 BRS Cel l B iology and H istology
(5) Regenerative cells are located primarily in the neck and isthmus; they replace all the epithelial cells of the gland, gastric pit, and luminal surface.
b. Card iac and pyloric g lands are different from fundic glands in that they are coiled tubular mucus-secreting glands and lack chief cells.
3. Gastric ju ice contains water, HCl, mucus, pepsin, lipase, rennin, and electrolytes. It is very ac id ic (pH 2.0) and facilitates the activation of pepsinogen to pepsin, which catalyzes the partial hydrolysis of proteins.
4. Regulation of gastric secretion is effected by neural activity (vagus nerve) and by several hormones. a . Gastr in and histamine, released by enteroendocrine cells in the gastric and duodenal
mucosa, together with acetylcholine released by parasympathetic nerve fibers of the vagus nerve, stimu late HC I secretion .
b . Somatostati n, produced by enteroendocrine cells of the pylorus and duodenum, inhibits the release of gastrin and thus i nd i rectly inh ib its HC I secretion .
c . Urogastrone (also known as human epidermal g rowth factor), produced by Brunner glands of the duodenum, and gastric inh ib itory peptide along with prostag land ins, produced by enteroendocrine cells in the small intestine, d i rectly inh ib it HC I secretion .
C. Smal l i ntestine 1 . Overview-Smal l i ntesti ne
a . The small intestine is approximately 7 m long and has three regions: the duodenum (proximal), je junum (middle), and i leum (distal) .
b. Function . The small intestine secretes several hormones; it continues and largely completes the d igestion of foodstuffs and absorbs the resulting metabolites.
2. Lumina l surface mod ifications-Smal l intesti ne . The luminal surface of the small intestine possesses plicae circulares, intestinal villi, and microvilli, which collectively increase the luminal surface area by a factor of 400 to 600. a . P l icae c ircu lares (valves of Kerckri ng ) are permanent spiral folds of the mucosa and
submucosa that are present in the distal half of the duodenum, the entire jejunum, and the proximal half of the ileum. Plicae circulares increase the surface area twofold to threefold.
b. Intestina l v i l l i (Figures 16 .2 and 16.3) are permanent evaginations that possess, in their connective tissue core (lamina propria), numerous plasma cells and lymphocytes,
Crypt of Lieberkuhn
FIGURE 16.2. The spati a l re lati onsh i p of i ntestin a l v i l l i ; c rypts of Li e be rkOhn ; a nd unde rly ing muscu l a ris m u cosae , s ubmu cosa , a nd muscu l a ris exte rna of the sma l l i ntestin e . I ntesti n a l v i l l i a re eva g i nations of the e p ithe l i um and l am i na p ropr i a . E a ch v i l l u s c onta i n s a s i ng l e b l i nd -ended l a ctea l a nd c a p i l l a ry l oop . The s ubmucosa , muscu l a ris exte rn a , a nd se rosa a re a l so d e p icte d . O N ES, d iffuse n e u roendoc ri ne system .
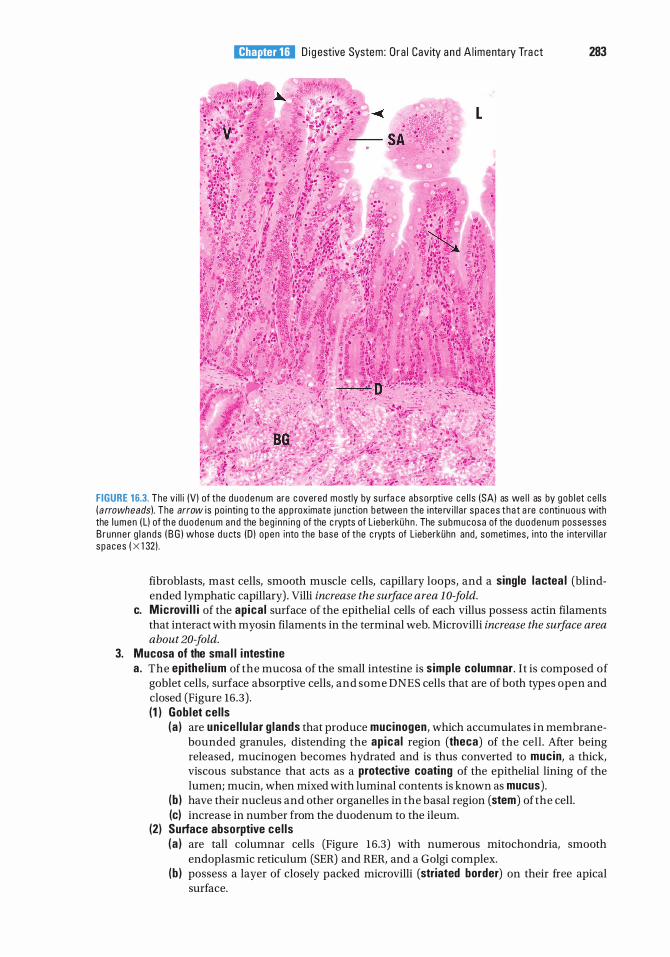
l!1ltJ'!1tJiij D i g estive System : O ra l Cavity a n d A l imenta ry Tra ct 283
FIGURE 16.3. The v i l l i (V) of the d uodenum are c overed mostly by su rfa c e abso rptive ce l l s (SA) as we l l as by gob l et ce l l s ( arrowheads). The arrow i s po i nti n g to the a p p roximate j u n ct ion b etwee n the i nte rv i l l a r spaces tha t a re conti n uous with the l umen ( L) of th e d uodenum a n d the beg i nn i ng of the c rypts of L ieberkiih n . The s ubmucosa of the duodenum possesses B runne r g l a nds ( B G ) whose d u cts (D ) open into the base of the c rypts of L ieberkiihn and , sometimes , i nto the i nte rvi l l a r spaces ( X 1 32) .
fibroblasts, mast cells, smooth muscle cells, capillary loops, and a single lactea l (blindended lymphatic capillary) . Villi increase the surface area 1 0-fold.
c. Microvi l l i of the apica l surface of the epithelial cells of each villus possess actin filaments that interact with myosin filaments in the terminal web. Microvilli increase the surface area about 20-fold.
3. Mucosa of the sma l l i ntesti ne a . The epithe l ium of the mucosa of the small intestine is s imple columnar . It is composed of
goblet cells, surface absorptive cells, and some DNES cells that are of both types open and closed (Figure 16 .3) . (1 ) Gob let cel ls
(a ) are un ice l lu lar g lands that produce mucinogen, which accumulates in membranebounded granules, distending the apica l region (theca) of the cell . After being released, mucinogen becomes hydrated and is thus converted to mucin, a thick, viscous substance that acts as a protective coating of the epithelial lining of the lumen; mucin, when mixed with luminal contents is known as mucus) .
(b ) have their nucleus and other organelles in the basal region (stem) of the cell. (c) increase in number from the duodenum to the ileum.
(2) Surface absorptive ce l ls (a ) are tall columnar cells (Figure 16.3) with numerous mitochondria, smooth
endoplasmic reticulum (SER) and RER, and a Golgi complex. (b ) possess a layer of closely packed microvilli (striated border) on their free apical
surface.
284 BRS Cel l B iology and H istology
(c) have a g lycoca lyx, which overlies the microvilli and binds various enzymes, including disaccharidases and dipeptidases.
(d) have well-developed t ight junctions and zonu la adherens. (3) DNES cells produce and secrete gastrin, cho lecystokin in , gastric inh ib itory peptide,
and several other hormones (Table 16.3) . Some ofthe open DNES cells possess the three genes for G protein-linked taste receptors similar to those of the taste buds located on the tongue. As in taste buds, sweet taste is coded for by TlR2 and TlR3, bitter by two copies of T2R subtypes, umami by TlR1 and TlR3. It is important to note that the taste cells of the gastrointestinal tract communicate with the islets of Langer hans, signaling the beta cells to release insulin once sweet taste is detected in the lumen.
b. Lamina propria (1 ) occupies the cores of the villi and the interstices between the numerous g lands (crypts)
of Lieberkiihn (Figure 16.3) . (2) consists of loose connective tissue with lymphoid cells, fibroblasts, mast cells, smooth
muscle cells, nerve endings, and lymphoid nodu les. (3) also contains lactea ls (blind-ended lymphatic vessels) and capi l lary loops.
(a) Crypts of Lieberkiihn are simple tubular glands that extend from the intervillous spaces to the muscularis mucosae of the intestine. They are composed of goblet and oligomucous cells, columnar cells (similar to surface absorptive cells), DNES cells, regenerative cells, Paneth cells, intermediate cells, and M cells (M cells, the last of this group, are discussed under the category of lymphoid nodules). 1. Paneth cel ls, located at the base of the crypts of Lieberkiihn, are pyramidal cells
that secrete the antibacterial enzyme lysozyme stored in large, apical, membranebounded secretory granules. These cells also release other antibacterial agents, defensins and tumor necrosis factor a and display extensive RER (basally), a large supranuclear Golgi complex, and many mitochondria. These agents have the capability of killing bacteria as well as certain protozoa.
2. Regenerative cel ls, located in the basal half of the crypts ofLieberkiihn, are thin, tall, columnar stem cel ls that divide to replace themselves and the other types of epithelial cells.
3. I ntermed iate ce l ls make up the bulk of the epithelial lining of the crypts of Lieberkiihn. These cells have regenerative properties; they are derived from regenerative cells, but have not as yet committed themselves to a certain cell line.
(b ) Lymphoid nodu les are usually small and solitary and are located in the lamina propria of the duodenum and jejunum. They increase in size and number in the ileum, where they form large contiguous aggregates, known as Peyer patches, which frequently extend through the muscularis mucosae into the submucosa. 1. M (microfo ld ) ce l ls are highly specialized, have an unusual shape, and lie in the
epithelium over lymphoid nodules and Peyer patches. They are derived from undifferentiated cells of the crypts of Lieberkiihn. They sample antigens as well as bacteria, viruses, and parasitic microorganisms. The endocytosed particles are conveyed via transcytosis to macrophages and lymphocytes that lie in the infoldings of the basal plasmalemma of M cells. These macrophages and the B and T lymphocytes are actually located in the lamina propria.
2. Activated B lymphocytes respond to antigenic challenge by forming more B cells, which enter the lymph and blood circulation, then home back to their original locations, where they populate the lamina propria and differentiate into immunoglobulin A (IgA) producing plasma cells.
3. Plasma cel ls manufacture monomeric immunoglobulin A (lgA). Two lgAs are bound to each other within the plasma cell by a protein, prote in J, another product of the plasma cell, forming a dimeric variety of IgA. The IgA dimer then enters the lamina propria of the small intestine and binds to dimeric IgA receptors at the basal membrane of the surface absorptive cells. The lgAreceptor complex is endocytosed into the cell and is transported to an early endosome to be transported across the intestinal epithelium (transcytosis) to
l!1ltJ'!1tJiij D i g estive System: O ra l Cavity and A l imenta ry Tra ct 285
the glycocalyx. Here a portion of the dim eric IgA receptor is cleaved from the complex, whereas the remainder of the receptor remains bound to the dim eric IgA as its secretory component, and the molecule is known as secretory lgA (slgA). Some of the slgA remains as an immunological defense against bacteria and antigens in the lumen of the intestine. Much of the slgA is reabsorbed by the surface absorptive cells and is transported into the lamina propria, where it enters blood vessels and goes to the liver, where it is internalized by hepatocytes to be secreted as part of bile. From the liver, slgA enters the gallbladder to be released into the lumen of the duodenum to join the slgA already present there to contribute to the immunological defense of the gastrointestinal tract. This process is referred to as the enterohepatic c i rcu lat ion.
c . The muscularis mucosae is composed of an inner circular and an outer longitudinal layer of smooth muscle.
CLIN ICAL CONSIDERATIONS
1 . I t i s i nte resti n g to note t ha t th e immune system o f the a l im enta ry c a n a l , u n d e r no rma l c ond iti o ns, is to l e ra nt of th e no rma l b a cteri a l fl o ra
a n d of e p ith e l i a l c e l l s l i n i n g the g ut that a re in c l ose conta ct with b a cteri a . It h a s b een shown that th is to l e r ance i s d u e to d e n d riti c c e l l s that i n h i b it T ce l l s from i n it iati n g an immune response . H oweve r, if the cond it ions b e come i n im i c a l to h e a lth, a s i n a n infl amm ato ry rea ction , th e d e n d riti c ce l l s i nstruct th e T ce l l s to respond and e l i c it a n immune rea cti on . I n o rd e r to ass i st the dend riti c c e l l s in th e i r fun cti on of d i ctati ng to l e r ance , strom a l ce l l s of lym ph nodes p resent p rote i n s p ro d u ced by ce l l s of th e a l imenta ry cana l t o n a'ive T c e l ls, i n stru cti ng th em to be to l e rant of th ose p rote i ns u n l ess i n structed oth e rwise by d e n d riti c ce l l s .
2 . Tou rists who have contracted th e Sh i g atoxi g en i c g roup o f Escherichia coli a re at r i s k when they med i c ate th emse lves with a nti b ioti cs, such as C i p rofloxa c i n , that they ta ke on th e i r tr i p s a s a p rotective measu re t o c u re th e i r d i a rrh e a . U nfortu nate ly, when th ese E. coli d i e , they re l ease e no rmous q u a ntiti es o f th e Sh i g a tox in that c a n k i l l the pati e nt. I t is a dvisa b l e fo r p ati ents not to ta ke C i p rofl oxa c i n in case they have b loody d i a rrhea but seek c ompetent m e d i c a l advi c e .
4 . Submucosa o f t he sma l l intestine a . consists of fibroelastic connective tissue containing blood and lymphatic vessels, nerve
fibers, and Meissner p lexus. b . also houses Brunner g lands (Figure 16.3), which are present only in the duodenum. These
glands produce an a lka l ine fl u id and urogastrone . The former protects the duodenal epithelium from the acidic chyme; the latter is a polypeptide hormone (human ep idermal g rowth factor) that enhances epithelial cell division and inhibits gastric HCl production.
5. The muscularis extern a of the sma l l i ntesti ne is composed oftwo layers of smooth muscle: an inner circular and an outer longitudinal layer. The inner layer participates in the formation of the i l eocecal sphincter. Auerbach (myenteric) p lexus is housed between the two layers.
6. External layer of the sma l l intesti ne a . Serosa covers all of the jejunum and ileum and part of the duodenum. b. Adventitia covers the remainder of the duodenum.
D. Large intestine 1 . Overview-Large intesti ne
a . The large intestine consists of the cecum, colon (ascending, transverse, descending, and sigmoid colon), rectum, ana l canal , and appendix.
b . The large intestine contains some digestive enzymes received from the small intestine. c. It houses bacteria that produce vitamin 812 and vitamin K; the former is necessary for
hemopoiesis and the latter for coagulation. d . The large intestine produces abundant mucus, which lubricates its lining and facilitates the
passage and elimination of feces.
286 BRS Cel l B iology and H istology
e. Function . The large intestine functions primarily in the absorption of electrolytes, fl u ids, and gases. Dead bacteria and indigestible remnants of the ingested material are compacted into feces.
2. Cecum and colon a . The mucosa of the cecum and colon lacks v i l l i and possesses no specialized folds.
(1 ) The epithe l ium of the mucosa of the cecum and colon is simple columnar with numerous goblet cells, surface absorptive cells, and occasional DNES cells.
(2) The lamina propria is similar to that of the small intestine, possessing lymphoid nodules, blood and lymph vessels, and closely packed crypts ofLieberkiihn, which lack Paneth cells. (a) Fibroblasts at the base of the crypts of Lieberkiihn of the lamina propria undergo
mitotic division and travel alongside of the epithelial components of the intestinal crypt, and as they reach the vicinity of the opening of the crypt, differentiate into cells with characteristics of macrophages. It is believed that these newly differentiated cells assist the monocyte-derived macro phages in their protective functions.
(b) Lymphoid e lements, members of the gut-associated lymphoid tissues (GALT), composed oflymphoid nodules and cells, are richly represented in the lamina propria.
(c) Interestingly, lymphoid dra inage occurs rarely, if ever, from the lamina propria; thereby, the absence of lymphatic vessels greatly limits the capability of metastasis of malignant tumors from the mucosa of the colon.
(3) The muscular is mucosae consists of an inner circular and outer longitudinal layer of smooth muscle cells.
b. The submucosa of the cecum and colon is composed of f ibroelastic connective tissue. It contains blood and lymphatic vessels, nerves, and Meissner (submucosa l ) p lexus.
c . The muscu laris externa of the cecum and colon is composed of an inner circular and a modified outer longitudinal layer of smooth muscle. The outer layer is gathered into three flat, longitudinal ribbons of smooth muscle that form the ten iae co l i . When continuously contracted, the teniae coli form sacculations of the wall known as haustra co l i . Auerbach (myenteric) p lexus is housed between the two layers of smooth muscle.
d . External layer of the cecum and colon (1 ) Adventitia covers the ascending and descending portions of the colon. (2) Serosa covers the cecum and the remainder ofthe colon. Fat-filled outpocketings of the
serosa (appendices ep ip loicae) are characteristic of the transverse and sigmoid colon. e. The l umen of the large intesti ne houses trillions of microbes, approximately lO times
the number of cells in the entire human body. These microorganisms form a part of the body's microbiome, whose physiological balance has shown to reflect the health of the individual harboring them. It appears that there are three groups of intestinal flora, known as enterotypes that predominate in the human population, and each individual possesses a predominance of one of these enterotypes. How these enterotypes develop and what their significance is are not as yet understood.
CLIN ICAL CONSIDERATIONS
1 . Malabsorption d isorders may l e a d to m a l n utriti on , resu lti ng i n wasti ng d i sea ses, i f ma jo r n utr ie nts ( c a rbohyd rates, am i no a c ids , i ons ) c a nnot be ass im i l ated .
a. G luten enteropathy ( n ontro p i c a l s p r u e ) resu lts from th e destru ctive effe cts o f c e rta i n g l u te ns ( p a rti c u l a r ly o f rye a n d wheat) o n t h e i ntesti n a l vi l l i , wh i c h red u c e th e s u rfa c e a rea ava i l a b l e fo r a bso rpti o n . It is treated by e l im i n ati ng wheat a n d rye p ro d u cts f rom the d i et.
b. Malabsorption of vitamin 812 may ca use pe rn i c i ous a n em i a . It u s ua l ly resu lts from i n ad e q u ate p ro d u ct ion o f g a str ic i ntri ns i c fa cto r by th e pa ri eta l c e l l s o f t he g a stri c m u c osa .
2 . Cholera- induced d iarrhea i s c a used by the a ctio n of c ho l e ra toxi n , wh i ch b l o c ks i ntesti n a l a bso rpti on o f sod i um i ons a n d p romotes exc reti on o f wate r a n d e l e ctro lytes . It c a uses d eath sho rtly afte r onset u n l ess th e l ost e l e ctro lytes a n d wate r a re re p l a c e d .
3 . D iverticu l itis i s a d i sease o f t h e a g i n g i n d ivi d u a l . As th e p e rson ente rs t h e f ifth d e c a d e o f l ife, the musc u l a r l ayers of the l a rge i ntesti n e beg i n to wea ken, p e rm itti n g th e eventu a l fo rmati on of outpo c keti n gs ( d iv e rti c u l a ) of the m u cosa a n d s u bmucosa of th e d ista l co l on , m a i n ly
l!1ltJ'!1tJiij D i g estive System: O ra l Cavity and A l imenta ry Tra ct 287
in the lowe r descend i n g co l on a n d th e s i gmo i d c o l o n . As materi a l s b e come tra pped in th ese d ive rti c u l a , infl a m m ati on o c c u rs i n a bo ut 1 5% to 25% of i n d ivi d ua l s with d ive rti c u l os is , and i t is th is i nfl ammati o n that i s kn own a s d iverti c u l it is . I n d iv id ua l s suffe r i ng from d ive rti c u l it is exh i b it a b dom i n a l p a i n ( u s u a l ly in th e l eft l owe r q u a d ra nt of the a bdomen) , a n d if the i nfl a mmati o n is severe, feve r, n a usea , d i a r rhea , and c r amps m ay a l so be expe ri e n c ed .
4 . Feca l transp lant i s a re l at ively re c e nt p ro c e d u re used i n pat ie nts whose no rm a l b a cte ri a l fl o ra h as been d e c imated a n d usu rped by p athogen i c b a cter ia , s u c h as Clostridium difficile. These i n d iv id u a l s suffe r from C. difficile co l it is with a resu ltant bout of d i a rrhea that m ay l a st a s long as seve ra l months . Alth o ugh these pati ents a re p l a c e d on a l o ng -term a nti b i oti c reg imen , i n m a ny c a se s t h e co l it is rema i n s un reso lved . It has been noted that i f they re c e ive a c l e a n s i n g p repa rati on s u c h a s t h e o ne used i n p repa ration f o r a co l onoscopy a n d th en re c e ive a fe-ca l tra nsp l a nt from a h e a lthy dono r ( u sua l ly a c l ose membe r of th e househo l d ) , th e co l it is i s reso lved i n a m atter of d ays, the pati ent's i ntesti n a l f l o ra retu rns to norma l , and the d i a rrhea c eases .
5. Certain intestinal microbes have the ab i l ity to metabo l ize trimethylamine , a stru ctu re present in substances such as ca rnitine of red meat and lec ith in p resent in egg yo lk, l iver, wheat ge rm, and pork, into trimethylamine-N-oxide (TMAO), a substa n ce that i n c reases the r i sk of athe rosc le rosis and stroke. I n fa ct, it has been shown that b lood TMAO level is a re latively a ccu rate i nd i cator of impend ing hea rt atta cks and strokes in i nd iv id u a ls who othe rwise d isp lay no r isk fa cto rs for these cond itions .
3. The rectum is similar to the colon but contains fewer and deeper crypts ofLieberkiihn (Table 16.2). 4. The anal canal is the constricted continuation of the rectum.
a. The anal mucosa displays longitudinal folds called anal columns (or recta l columns of Morgagni) , which join each other to form anal valves. The regions between adjacent valves are known as ana l s inuses. (1 ) Epithelium of the anal canal
(a) is simple columnar changing to simple cuboidal proximal to the anal valves. (b ) changes to stratified squamous nonkerati nized distal to the anal valves. (c) changes to stratified squamous kerati n ized (epidermis) at the anus.
(2) The lamina propria is composed of fibroelastic connective tissue and contains sebaceous glands, circumanal glands, hair follicles, and large veins.
(3) The muscu laris mucosae consists of an inner circular and an outer longitudinal layer of smooth muscle, both of which terminate at the anal valves.
b. The anal submucosa is composed of dense, irregular fibroelastic connective tissue that houses large veins.
c. The anal muscularis externa is composed of an inner circular and an outer longitudinal layer of smooth muscle. The inner circular layer forms the internal ana l sphincter.
d . Anal adventitia attaches the anus to surrounding structures. e. The external anal sphincter is composed of skeleta l muscle, whose superficial and deep
layers invest the anal canal. It exhibits conti nuous tonus, thus maintaining a closed anal orifice. The degree of tonus is under voluntary contro l, so the retention or evacuation of feces normally can be controlled at will.
1 . Colorecta l carcinoma is th e second h i g hest c ause of c a n c e r d e ath i n CLIN ICAL CONSIDERATIONS the U n ited States . I t most common ly affects i n d ivi d u a ls who a re 55
yea rs o f a g e o r o l d e r. I t u s u a l ly a rises from adenomatous po lyps a n d may b e a sym ptom atic for m a ny yea rs . Re cta l b l e ed i n g is fre q u ently p rese nt. Co lo recta l c a rc i n oma is p ro b a b ly re l ated to d i et . D i ets h igh i n fat and refi n ed c a rbohyd rates and low i n fi b e r a p p e a r to be assoc i ated with co l o re cta l c a rc i n oma .
2 . Hemorrhoids a re very c ommon i n p eop l e o l de r tha n 50 yea rs . They present as recta l b l eed i ng d u ri ng defe cati on . Hemorrho ids a re c a used by th e breakage of d i l ated, th in -wa l l ed vesse ls of venous p l exuses e ith e r above ( i nte rna l hemorrho ids ) o r be low (exte rna l hemorrho ids ) the ano recta l l i n e .
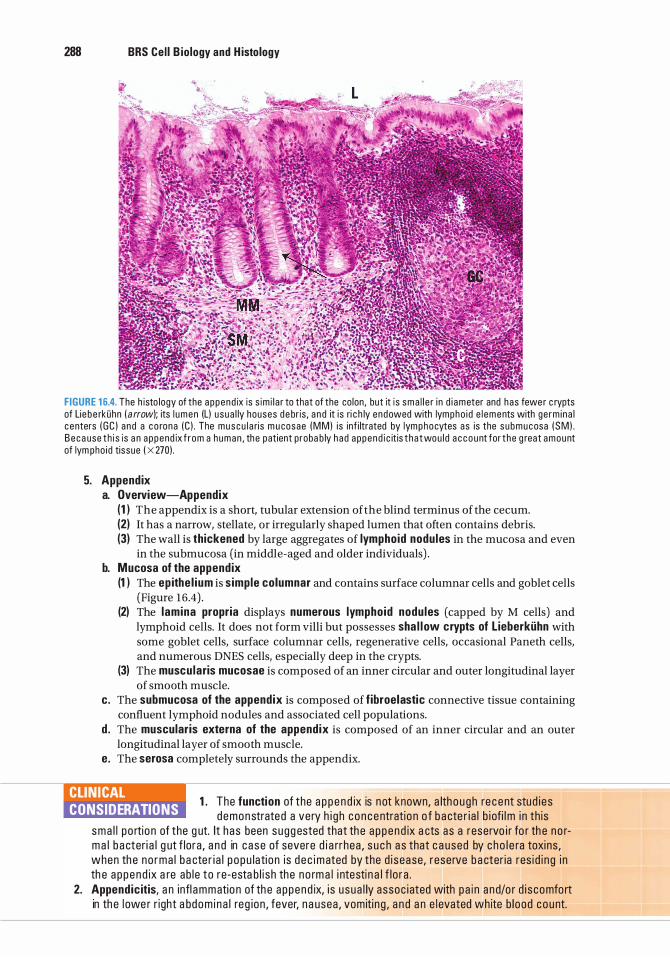
288 BRS Cel l B iology and H istology
FIGURE 1 6.4. The h isto logy of the a ppend ix is s im i l a r to that of the co lon, but it i s sma l l e r i n d i ameter and has fewe r c rypts of Lie b e rkiihn ( a rrow); its l umen (L) u sua l ly houses d e br is , a n d it i s ri c h ly endowed with lympho i d e l ements with ge rm i na l c enters ( G C ) a nd a c o rona (C ) . The muscu l a ri s m u cosae (MM) i s inf i ltrated by lym p h ocytes as is the s ubmucosa ( SM) . B e c a use t h i s is a n a p p e nd ix f r om a human , the pat ient p roba b ly h ad a ppend i c it is t ha t wou l d a c c o u nt for t he g reat amount of lym pho i d tissue ( X 270) .
5. Appendix a. Overview-Appendix
(1 I The appendix is a short, tubular extension of the blind terminus of the cecum. (21 It has a narrow, stellate, or irregularly shaped lumen that often contains debris. (31 The wall is thickened by large aggregates of lymphoid nodules in the mucosa and even
in the submucosa (in middle-aged and older individuals) . b. Mucosa of the appendix
(1 I The epithe l ium is simple columnar and contains surface columnar cells and goblet cells (Figure 16.4) .
(21 The l amina propria displays numerous lymphoid nodu les (capped by M cells) and lymphoid cells. It does not form villi but possesses sha l l ow crypts of Lieberkiihn with some goblet cells, surface columnar cells, regenerative cells, occasional Paneth cells, and numerous DNES cells, especially deep in the crypts.
(31 The muscu laris mucosae is composed of an inner circular and outer longitudinal layer of smooth muscle.
c. The submucosa of the appendix is composed of fibroelastic connective tissue containing confluent lymphoid nodules and associated cell populations.
d . The muscularis externa of the appendix is composed of an inner circular and an outer longitudinal layer of smooth muscle.
e. The serosa completely surrounds the appendix.
1 . The function of the a p p e n d ix is not known, a lth o ugh re c ent stud i es CLINICAL CONSIDERATIONS demonstrated a very h i g h c o n centratio n o f b a cte r i a l b i ofi lm i n th is
sma l l po rtio n of the g ut. It has been sugg ested that th e a p pend ix a cts as a reservo i r fo r th e no rm a l b a cteri a l g ut f lora , a n d in c ase of severe d i a rrhea , s u c h a s that c a used by c ho l e ra toxi ns , when th e no rma l b a cte r i a l p opu lati on is d e c imated by the d i sease, reserve b a cter ia res i d i ng i n th e a ppend ix a re ab l e to re-esta b l i sh the no rm a l i ntesti n a l f l o ra .
2. Appendic itis, a n infl ammatio n of th e a ppend ix, i s usua l ly assoc i ated with pa i n a nd/o r d i s comfo rt in th e l owe r r ight a bdom i na l reg ion , fever, n a usea , vomiti ng , a n d a n e l evated white b lood count.
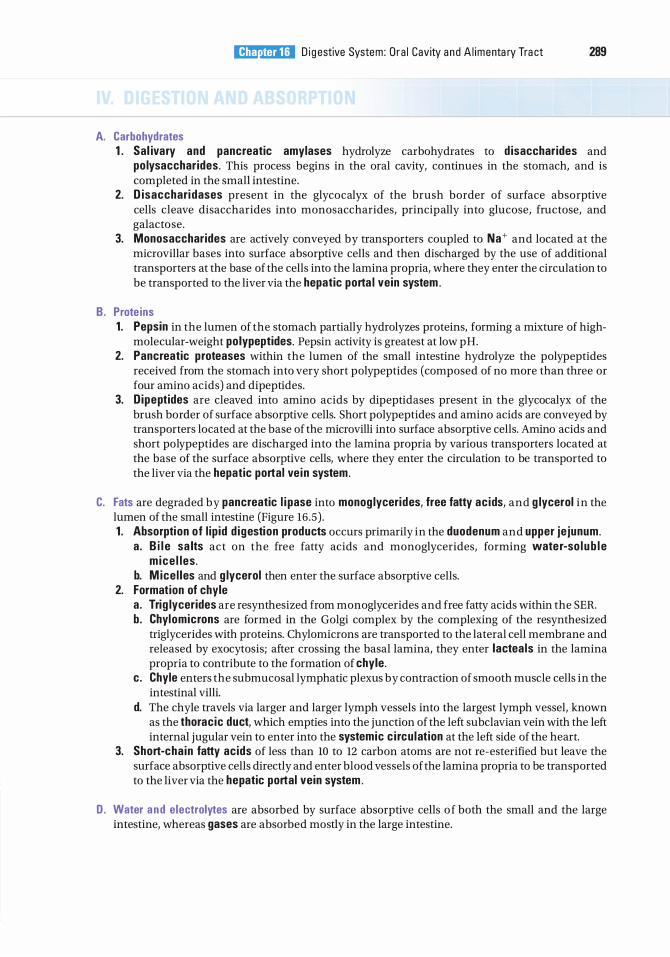
A. Carbohydrates
l!1ltJ'!1tJiij D i g estive System : O ra l Cavity a n d A l imenta ry Tra ct 289
1 . Sal ivary and pancreatic amylases hydrolyze carbohydrates to d isaccharides and po lysaccharides. This process begins in the oral cavity, continues in the stomach, and is completed in the small intestine.
2. D isacchari dases present in the glycocalyx of the brush border of surface absorptive cells cleave disaccharides into monosaccharides, principally into glucose, fructose, and galactose.
3. Monosaccharides are actively conveyed by transporters coupled to Na+ and located at the microvillar bases into surface absorptive cells and then discharged by the use of additional transporters at the base of the cells into the lamina propria, where they enter the circulation to be transported to the liver via the hepatic porta l vein system .
B . Prote ins 1 . Pepsin in the lumen of the stomach partially hydrolyzes proteins, forming a mixture of high
molecular-weight polypeptides. Pepsin activity is greatest at low pH. 2. Pancreatic proteases within the lumen of the small intestine hydrolyze the polypeptides
received from the stomach into very short polypeptides (composed of no more than three or four amino acids) and dipeptides.
3. D ipeptides are cleaved into amino acids by dipeptidases present in the glycocalyx of the brush border of surface absorptive cells. Short polypeptides and amino acids are conveyed by transporters located at the base of the microvilli into surface absorptive cells. Amino acids and short polypeptides are discharged into the lamina propria by various transporters located at the base of the surface absorptive cells, where they enter the circulation to be transported to the liver via the hepatic portal ve in system.
C. Fats are degraded by pancreatic l i pase into monog lycerides, free fatty ac ids, and g lycerol in the lumen of the small intestine (Figure 16 .5) . 1 . Absorption of l ip id d igestion products occurs primarily in the duodenum and upper je junum.
a . B i l e sa lts act on the free fatty acids and monoglycerides, forming water-so l ub l e m ice l les .
b. M ice l les and g lycerol then enter the surface absorptive cells. 2. Formation of chyle
a . Trig lycerides are resynthesized from mono glycerides and free fatty acids within the SER. b. Chylomicrons are formed in the Golgi complex by the complexing of the resynthesized
triglycerides with proteins. Chylomicrons are transported to the lateral cell membrane and released by exocytosis; after crossing the basal lamina, they enter lactea ls in the lamina propria to contribute to the formation of chyle.
c . Chyle enters the submucosal lymphatic plexus by contraction of smooth muscle cells in the intestinal villi.
d. The chyle travels via larger and larger lymph vessels into the largest lymph vessel, known as the thoracic duct, which empties into the junction of the left subclavian vein with the left internal jugular vein to enter into the systemic c i rcu lation at the left side of the heart.
3. Short-cha in fatty acids of less than 10 to 12 carbon atoms are not re-esterified but leave the surface absorptive cells directly and enter blood vessels of the lamina propria to be transported to the liver via the hepatic portal vein system .
D. Water a n d electrolytes are absorbed by surface absorptive cells o f both the small and the large intestine, whereas gases are absorbed mostly in the large intestine.

290 BRS Cel l B iology and H istology
Bi le acids � Lipids � Lipase
! Glycerol Monoglycerides
Fatty acids
v 7
GOD c> (!) (!) {;) .J!) SE�R 0 O � Trig lyceride ® �ER
synthesis (!) � .>/- Protein
Golg i
FIGURE 1 6.5. Abso rption of l i p i ds by s u rfa c e abso rptive ce l l s of the sma l l i ntesti ne and the formation of c hy lom i c rons . SER , smooth endop l a sm i c reti c u l u m; RER, rough endop lasm ic reti c u l um .
Review Test
Di rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1 . The type of epithelium associated with the vermilion zone of the lips is
(A) stratified squamous nonkeratinized. ( B ) pseudostratified ciliated columnar. (C ) stratified squamous keratinized. (D) stratified cuboidal. (E) stratified columnar.
2. Which of the following cell types is present in the gastric glands of the pyloric stomach?
(A) Goblet cells ( B ) Mucous neck cells (C) Paneth cells (D ) Basal cells (E ) Chief cells
3. Secretin and cholecystokinin are produced and secreted by cells in the lining of the alimentary tract. Which of the following statements about these two substances is true?
(A) They are produced by diffuse neuroendocrine cells (DNES cells) in the lining of the stomach and small intestine.
(B) They are digestive enzymes present within the lumen of the duodenum.
(C) They are produced by Paneth cells. (D ) They are hormones that have target cells in
the pancreas and biliary tract. (E ) They are produced by Brunner glands and
released into the lumina of the crypts of Lieberkiihn.
4. If odontoblasts malfunction because of developmental anomalies, which of the following will be affected?
(A) Cementum ( B ) Enamel (C) Dentin (D ) Tooth crown only (E ) Tooth root only
5. Which of the following statements concerning the principal fiber bundles of the periodontal ligament is true?
(A) They are composed of elastin. (B ) They extend from the cementum to the
enamel. (C) They extend from the dentin to the
cementum. (D ) They are composed of collagen. (E) They extend from one tooth to the next.
6. A patient goes to the emergency department, and the physician notes one of the classic symptoms of appendicitis. Which of the following is that symptom?
(A) Apnea (B) Vomiting of blood (C) Depressed white cell count (D ) Rectal bleeding (E ) Abdominal pain
7. Passage of a bolus through the esophagus into the stomach is facilitated by which of the following?
(A) Peristaltic activity of the esophageal muscularis externa
(B ) Peristaltic activity of the gastric muscularis mucosae
(C) Reflux through the pharyngoesophageal sphincter
(D ) Smooth muscle in the esophageal muscularis mucosae
(E) Reflux through the gastroesophageal sphincter
291
292 BRS Cel l B iology and H istology
8. The small intestine has three histologically distinct regions. Which of the following statements concerning the histological differences in the three regions is true?
(A) Peyer patches are present only in the ileum.
(B ) Goblet cells are present only in the epithelium of the duodenum.
(C) Brunner glands are located in the duodenum and jejunum but not the ileum.
(D ) Lacteals are present only in the lamina propria of the ileum.
(E) The muscularis mucosae contains three layers of smooth muscle in the ileum and two layers in the duodenum and jejunum.
9. Which of the following materials can be absorbed directly by the surface lining cells of the stomach?
(A) Vitamin B12 (B ) Polysaccharides (C) Chylomicrons (D ) Triglycerides (E) Alcohol
10. Which of the following is characteristic of angular cheilitis?
(A) Patients in the early 20s (B) Presence of herpes virus (C ) Erythematous lesions at the corners of the
mouth (D ) Apnea (E) High blood levels of secretin
Answers and Explanations
1 . C. The external aspect and vermilion zone of the lips are covered by thin skin, which contains a stratified squamous keratinized epithelium. The internal aspect of the lips is lined by a wet mucosa containing a stratified squamous nonkeratinized epithelium (see Chapter 16 II A).
2. B . Mucous neck cells are located in the neck of gastric glands in all parts of the stomach, whereas only fundic glands contain chief (zymogenic) cells (see Chapter 16 III B 2).
3. D . Secretin and cholecystokinin are hormones produced by enteroendocrine cells in the small intestine. Secretin stimulates bicarbonate secretion in the pancreas and biliary tract. Cholecystokinin stimulates the release of pancreatic enzymes and contraction of the gall bladder (see Chapter 16 III C 3) .
4. C. Dentin is manufactured by odontoblasts (see Chapter 16 II C 2).
5. D . The principal fiber bundles of the periodontal ligament are composed of collagen fibers. They suspend a tooth in its alveolus, extending from the cribriform plate of the alveolar bone to the cementum on the root of the tooth. The fibers that extend from one tooth to the next are the transseptal fibers of the gingivae (see Chapter 16 II D 1 ) .
6. E. Rectal bleeding or vomiting of blood often accompanies gastrointestinal pathologies but not appendicitis. Elevated, not depressed, white cell count and abdominal pain are classic signs of appendicitis (see Chapter 16 III D 5 Clinical Considerations).
7. A. The smooth muscle of the muscularis mucosae plays no role in the movement of a bolus through the esophagus. This movement is accomplished by peristalsis of the esophageal muscularis externa, which contains both skeletal and smooth muscle. The sphincters at the pro ximal and distal ends of the esophagus permit movement of food in only one direction, toward the stomach (see Chapter 16 III A 5) .
8. A. The primary histological differences in the three regions of the small intestine are the presence of Peyer patches in the lamina propria of the ileum and the presence of Brunner glands in the submucosa of the duodenum. The duodenum and jejunum lack Peyer patches, and the jejunum and ileum lack Brunner glands. Goblet cells are present throughout the small intestine (see Chapter 16 III C 3) .
9. E. Only a few simple substances, such as alcohol, can be absorbed by the epithelial lining of the stomach (see Chapter 16 III B 1 ) .
1 0. C. The corners of the mouth have painful erythematous lesions (see Chapter 16 I I B 2 Clinical Considerations) .
293
Digestive System : Glands
A. The extrinsic glands of the digestive system include the major sal ivary g lands, the pancreas, and the l iver (with the associated ga l l b ladder), all of which are outside the wall of the digestive tract.
B. These glands produce enzymes, buffers, emulsifiers, and lubricants that are delivered to the lumen of the digestive tract via a system of ducts.
C. They also produce hormones, blood proteins, and other products.
A. Overview
294
1. The major salivary glands consist of three pa i red exocrine glands : the parotid, submand ibu lar, and subl ingua l .
2. Function . They synthesize and secrete sal ivary amylase, lysozyme, lactoferri n, and secretory component. a . Secretory component is a portion of the lgA d imer receptor molecule located on the basal
plasma membrane of the secretory cell and facilitates the transfer of the IgA dimer into the early endosome of the secretory cell. This portion of the receptor molecule remains bound to the IgA dimers, immunoglobulins that are produced by plasma cells in the connective tissue, forming a complex that resists enzymatic digestion in the saliva but can still perform its immune function.
b. The serous secretory cells of major salivary glands also secrete histidine-rich, proline-rich, and cysteine-rich proteins. The cells of the striated ducts of these glands also release an enzyme ka l l i krein both into the lumen as well as into the connective tissue. In the lumen kallikrein begins the digestion of proline- and cysteine-rich proteins, whereas in the connective tissue kallikrein enters the bloodstream, where it converts kin i nogens into the vasodilator and bronchial smooth muscle contractant bradykin in .
c . Lysozyme and lactoferrin are antimicrobial agents that control the bacterial flora of the oral cavity.
d. Amylase begins the digestion of carbohydrates in the oral cavity.
l!il!tt'!1lliUI D ig estive System : G l a nds 295
B. Structure. The major salivary glands are compound tubuloacinar (tubuloalveolar) glands. They are further classified as serous, mucous, or mixed (both serous and mucous), depending on the type of secretory acini they contain. These glands are surrounded by a capsule of dense irregular collagenous connective tissue with septa that subdivide each gland into lobes and lobules. Neurovascular elements serving these glands are conveyed to the acinar cells within the connective tissue septa. 1. Sal ivary g land ac in i
a . Salivary gland acini consist of pyramidal serous or mucous cells arranged around a central lumen that connects with an i nterca lated duct. Mucous acini may be overlaid with a crescent-shaped collection of serous cells called serous demi l unes. Recently, it has been suggested that serous demilunes are fixation artifacts, in that a mixed acinus has both serous and mucous cells situated around a central lumen. During processing for microscopy, the mucous cells become swollen and squeeze the bulk of the serous cells to the periphery of the acinus, making them appear to form a serous cap covering the mucous cells. If the tissue is flash-frozen, so that swelling of the mucous cells is prevented, serous demilunes are not present. In spite of this finding, since in nonfrozen preparations serous demilunes are evident and since classical histology uses these artifactual structures as classifying characteristics, in this review book they will be treated as if they were actual structures.
b. Acini of salivary glands possess myoepithe l ia l ce l ls that share the basal lamina of the acinar cells. The acinus and its associated intercalated and striated ducts form the sal ivon, the functional unit of a salivary gland.
c. They release a pr imary secretion that resembles extracellular fluid. This secretion is modified in the ducts to produce the f ina l secretion .
d . Salivary glands are classified according to their types of acini. (1 ) Parotid g lands consist of serous ac in i and are classified as serous. (2) Sub l ingua l g lands consist mostly of mucous ac in i capped with serous demi l unes. They
are classified as mixed. (3) Submand ibu lar g lands consist of both serous and mucous ac in i (some also have serous
demilunes) . They are classified as mixed. 2. Sal ivary g land ducts
a. Intercalated ducts originate in the acini and join to form striated ducts. They may deliver bicarbonate ions into the primary secretion.
b. Striated ( i ntra l obu lar) ducts
C. Sa l iva
(1 ) Striated ducts are lined by ion-transporting ce l ls that remove sodium and chloride ions from the luminal fluid (via a sodium pump) and actively pump potassium and bicarbonate ions into it, thus transforming the initial saliva (pr imary sal iva) produced by the acinar cells into secondary sal iva, which leaves the striated duct and eventually enters the oral cavity.
(2) Striated ducts converge in each lobule to form i ntra lobu lar ducts that merge with each other to form i nterl obu lar (excretory) ducts, which run in the connective tissue septa. These ducts drain into the main duct of each gland, which empties into the oral cavity.
1 . Saliva is a hypoton ic solution produced at the rate of about 1 L per day. 2. Function
a . Saliva l ubricates and cleanses the oral cavity by means of its water and glycoprotein content.
b. It contro ls bacteria l flora by the action of thiocyanate, lysozyme, lactoferrin, and IgA, as well as by its cleansing action.
c. It initiates d igestion of carbohydrates by the action of salivary amylase. d . It acts as a solvent for substances that stimulate the taste buds. e. It assists in the process of deglutition (swallowing).
296 BRS Cel l B iology and H istology
1 . The f low of sa l iva is impo rtant not o n ly fo r the easy swa l lowi n g of CLIN ICAL CONSIDERATIONS masti c ated food but a l so a s a veh i c l e t ha t fa c i l itates the sensati on of
taste a n d th e i n it iati on of d i g esti on as we l l as fo r the ma i nte n a n c e of p ro pe r o ra l h e a lth . I n d ivi d u a l s who had rad i ati o n treatm ent fo r c a n c e rs of the head a n d/o r n e c k a n d those who a re be i ng treated with c h emothe rapy fre q uently h ave xe rostom i a , d ry mouth, b e c a use of red u c e d sa l iva ry g l a n d fu n cti o n . Fre q uently, these pat ie nts have t o u s e a rtifi c i a l s a l iva t o ma i nta i n a mo i st o ra l env i ro nment. U s u a l ly, s ubsequent to th e c essati on of r ad i at ion the r apy o r c hemo th e ra py, s a l iva ry g l a n d fun cti on retu rns t o no rma l .
2 . Sjogren syndrome i s be l i eved to be a n a uto immune d isease whose symptoms a re xerostom i a , d ry eyes, a n d g e n e ra l ly d ry m u cous m e m b ra n es . Alth ough the re is no c u re fo r t h i s p a i nfu l a n d potenti a l ly d eb i l itati ng d i so rd e r, eyed rops, the fre q u ent i ntake of fl u i d s, a n d/or the use of a rtifi c i a l s a l iva re l i eve some of th e sym ptoms .
3. Sa l ivary calcu lus i s a c a l c if ic ati on that is fo rmed usua l ly i n th e pa rotid g l a n d . It may b lock the f low of s a l iva th ro u gh th e pa rotid d u ct. O c c as i o na l ly, th e b l o ckage resu lts i n th e b a c kf low of s a l iva, with a c oncom itant pa infu l swe l l i n g of the pa roti d g l a n d . Fre q u ently, a s imp l e massage of th e pa roti d d u ct can d i s l o dge the stone ; oth e rwise a s u rg i c a l a p p ro a c h m ay be n e cessa ry.
4. Mumps, a vira l infection, usua l ly affects ch i l d ren 5 to 1 5 years of age but may affect adu lts as wel l . It is usua l ly re l ative ly ben ign in ch i l d ren, a lthough i t may ca use cons iderab l e pa in because of the swe l l i ng of the sa l iva ry g l ands . I n adu lt ma les the virus may a lso c a use swe l l i ng of the testes, and in add ition to the cons iderab l e pa in , i t may resu lt i n ster i l ity i f both testes a re invo lved . I n othe rs the panc reas may a lso become involved, caus ing panc reatitis with its attendant symptoms of a bdomi na l pa in and m i l d -to-severe nausea and vomiting . Fortunate ly, the symptoms subs ide with in a week and the re a re no residu a l comp l i cations . I n a few adu lts, l e ss than 1 0% of the cases, t he mumps virus may a lso ca use men ingoencepha l itis that reso lves itself i n a week o r so , but in a very sma l l number of cases, ser ious, l ife long comp l i cations may resu lt, i nc l ud i ng deafness and fa c i a l para lysis.
The pancreas has a slender connective tissue capsule. This gland produces d igestive enzymes in its exocrine portion and a number of hormones in its endocrine portion ( is lets of Langerhans) . Blood flow into the pancreas is arranged in such a fashion that the acini receive arterial blood from vessels dedicated to these structures and the islets of Langerhans also receive blood dedicated to the islets. Additionally, acini also receive venous blood drained from the islets of Langerhans, so that hormones, such as somatostatin, released by those islet cells can reach the acinar cells immediately after release.
A. The exocrine pancreas is a serous compound tubuloacinar gland. 1. Pancreatic ac inar ce l ls
a . Pancreatic acinar cells are pyramidal serous cells arranged around a central lumen. b . They possess a round basal nucleus, abundant rough endoplasmic reticulum (RER), an
extensive Golgi complex, numerous mitochondria, and many free ribosomes. c . Zymogen (secretory) g ranu les are membrane bound and densely packed in the ap ica l
region of pancreatic acinar cells. They contain enzymes and pro enzymes packaged in the Golgi complex.
d. Their basal plasmalemma has receptors for cholecystokinin and acetylcholine. 2. Pancreatic ducts
a. The initial intra-acinar portion of the intercalated ducts is formed by centroacinar cel ls, which are low cuboidal with a pale cytoplasm.
b. From the initial portion, the intercalated ducts converge into a small number of i ntra lobu lar ducts, which in turn empty into large i nterlobu lar ducts that empty into the main (or accessory) pancreatic duct.
c. The main pancreatic duct fuses with the common bile duct, forming the ampul la of Vater, which delivers secretions of the exocrine pancreas and the contents of the gallbladder into the duodenum at the major duodenal papi l l a .
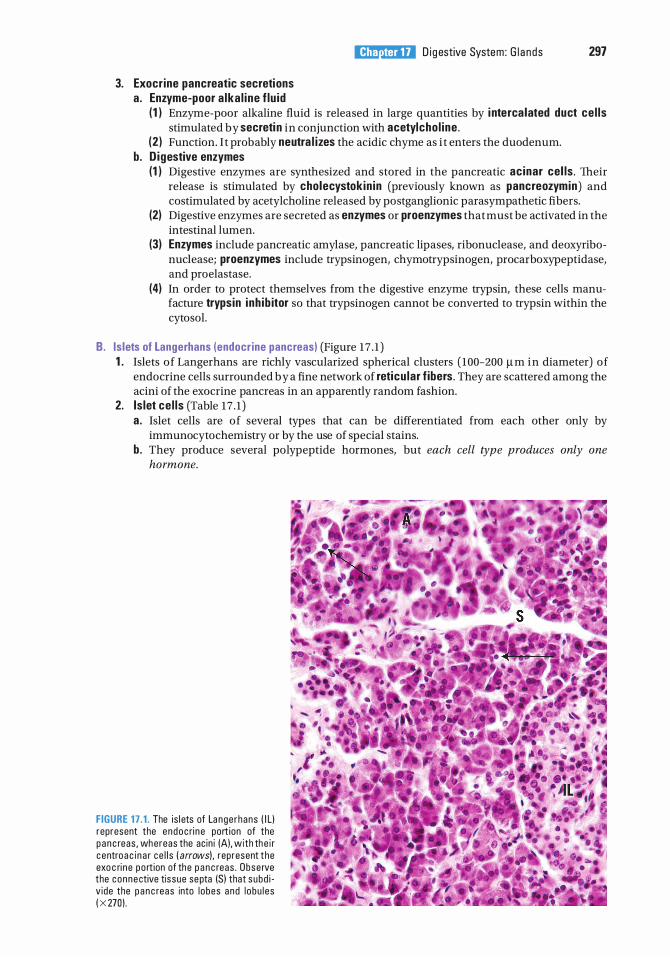
3. Exocrine pancreatic secretions a . Enzyme-poor a lka l ine f lu id
l!il!tt'!1lliUI D ig estive System : G l a nds 297
( 1 ) Enzyme-poor alkaline fluid is released in large quantities by i nterca lated duct ce l ls stimulated by secreti n in conjunction with acetylcho l ine .
(2 ) Function. I t probably neutra l izes the acidic chyme as i t enters the duodenum. b. D igestive enzymes
(1 ) Digestive enzymes are synthesized and stored in the pancreatic acinar cel ls . Their release is stimulated by cholecystok in in (previously known as pancreozymin) and costimulated by acetylcholine released by postganglionic parasympathetic fibers.
(2) Digestive enzymes are secreted as enzymes or proenzymes that must be activated in the intestinal lumen.
(3) Enzymes include pancreatic amylase, pancreatic lipases, ribonuclease, and deoxyribonuclease; proenzymes include trypsinogen, chymotrypsinogen, procarboxypeptidase, and pro elastase.
(4) In order to protect themselves from the digestive enzyme trypsin, these cells manufacture trypsin inh ib itor so that trypsinogen cannot be converted to trypsin within the cytosol.
B. Is lets of Langerhans (endocrine pancreas) (Figure 17 . 1 ) 1 . Islets of Langerhans are richly vascularized spherical clusters ( 100-200 11m in diameter) of
endocrine cells surrounded by a fine network of reticu lar f ibers . They are scattered among the acini of the exocrine pancreas in an apparently random fashion.
2. Is let ce l ls (Table 17 . 1 ) a. Islet cells are of several types that can be differentiated from each other only by
immunocytochemistry or by the use of special stains. b . They produce several polypeptide hormones, but each cell type produces only one
hormone.
FIGURE 17 . 1 . The is l ets of La nge rhans ( I ll represent the endoc ri n e port ion of the p a n c reas , wh ereas the ac in i (A), with th e i r c entro a c i n a r ce l l s ( arrows) , represent the exo c ri n e po rt ion of the p a n c reas . Obse rve the connective tissue septa (Sl that subd i v ide the p a n c reas into l obes and l obu l es ( X 270) .
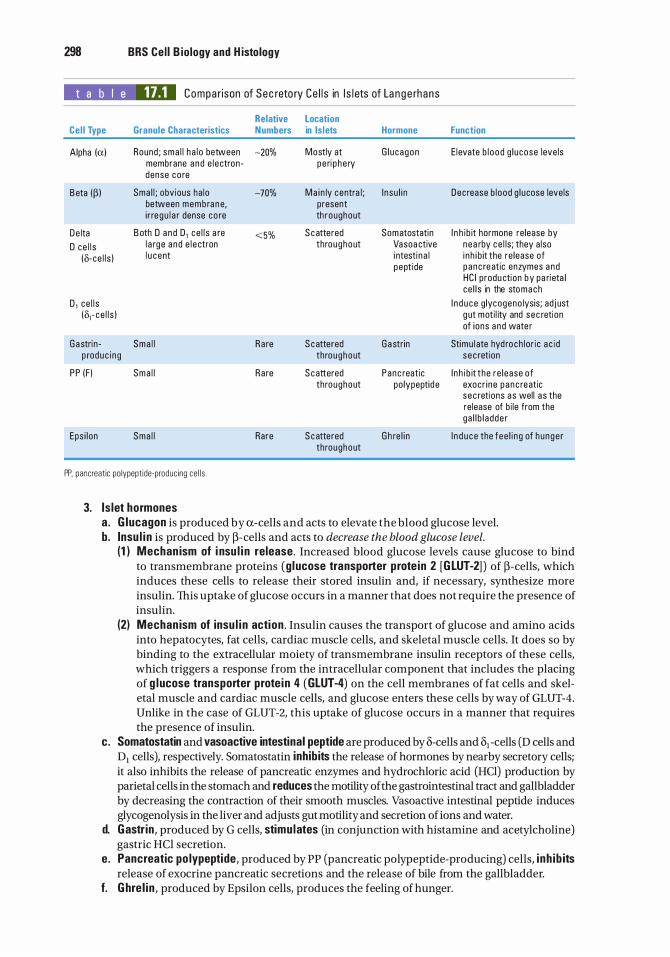
298 BRS Cel l B iology and H istology
t a b I e 17.1 Compa rison of Sec reto ry Ce l l s in I s l ets of La n g e rhans
Relative Location Cel l Type Granule Characteristics Numbers in Islets Hormone Function
Alpha (a) Round ; sma l l h a l o between -20% Mostly at G l u cagon E levate b l ood g l ucose leve ls membrane a nd e l e ctron - pe ri p he ry dense co re
B eta (� ) Sma l l ; obv ious ha lo -70% Ma i n ly centra l ; I n su l i n Dec rease b l ood g l ucose levels between membra ne, present i r re g u l a r dense co re th roughout
De lta B oth D a nd D 1 ce l l s a re <5% S cattered Somatostatin
D ce l l s l a rge a nd e l e ctron throughout Vasoa ctive
(o-ce l l s ) l u c ent i ntesti n a l pept ide
I n h ib it hormone re lease by nea rby ce l ls ; they a lso i nh i b it the re lease of p anc reatic enzymes and HC I produ ction by pa ri eta l ce l l s in the stomach
D 1 ce l l s (o, - ce l l s )
I n d u c e g lycogeno lysis; ad j ust g ut moti l ity and sec retion of ions a nd wate r
G a stri n - Sma l l Ra re S cattered Ga strin p roduc i n g throughout
Stimu l ate hyd roch lor ic a c i d s ec retion
pp (F ) Sma l l
Eps i lon Sma l l
Ra re
Rare
S c attered throughout
S cattered throughout
Panc reatic po lypeptid e
G h re l i n
I n h i b it the re l ease of exocr i ne p a n c reatic s ec retions as wel l a s the re lease of b i le from the ga l l b l a dde r
I n d u c e the fee l i n g of h unge r
PP, pancreatic po lypeptide-produc ing ce l l s .
3. Is let hormones a . G lucagon is produced by a-cells and acts to elevate the blood glucose level. b_ Insu l i n is produced by �-cells and acts to decrease the blood glucose level.
(1 ) Mechan ism of i nsu l i n release. Increased blood glucose levels cause glucose to bind to transmembrane proteins (g l ucose transporter prote in 2 [GLUT-2] ) of �-cells, which induces these cells to release their stored insulin and, if necessary, synthesize more insulin. This uptake of glucose occurs in a manner that does not require the presence of insulin.
(2) Mechan ism of insu l i n action . Insulin causes the transport of glucose and amino acids into hepatocytes, fat cells, cardiac muscle cells, and skeletal muscle cells. It does so by binding to the extracellular moiety of transmembrane insulin receptors of these cells, which triggers a response from the intracellular component that includes the placing of g lucose transporter prote in 4 (GLUT-4) on the cell membranes of fat cells and skeletal muscle and cardiac muscle cells, and glucose enters these cells by way of GLUT-4. Unlike in the case of GLUT-2, this uptake of glucose occurs in a manner that requires the presence of insulin.
c. Somatostatin and vasoactive intestinal peptide are produced by 8-cells and 81 -cells (D cells and D1 cells), respectively. Somatostatin inhibits the release of hormones by nearby secretory cells; it also inhibits the release of pancreatic enzymes and hydrochloric acid (HCl) production by parietal cells in the stomach and reduces the motility of the gastrointestinal tract and gallbladder by decreasing the contraction of their smooth muscles. Vasoactive intestinal peptide induces glycogenolysis in the liver and adjusts gut motility and secretion of ions and water.
d. Gastr in , produced by G cells, stimu lates (in conjunction with histamine and acetylcholine) gastric HCl secretion.
e. Pancreatic po lypeptide, produced by PP (pancreatic polypeptide-producing) cells, i nh ib its release of exocrine pancreatic secretions and the release of bile from the gallbladder.
f. Ghre l in , produced by Epsilon cells, produces the feeling of hunger.
l!il!tt'!1lliUI D i g estive System: G l ands 299
CLIN ICAL CONSIDERATIONS
1 . I n d iv id u a ls who h ave l ow b l ood g l u cose a n d h i g h b l ood i n su l i n l eve ls may be suffe ri ng from insu l i noma, a tu mo r of the P-ce l l s of the i s l ets of
La n g e rhans . l n s u l i n omas a re ben i g n in 90% of the c ases, a n d the cond itio n is u sua l ly reso lved by s u rg i c a l exc is ion of th e tu mo r.
2. Type 1 ( i nsu l i n-dependent) d iabetes mel l itus ( lOOM) a . I D D M resu lts from a l ow level o f p lasma insu l i n . b . I t i s c h a ra cte r ized by polyphagia ( i n sati a b l e h u n g e r) , po lyd ipsia ( u n q u e n c h a b l e th i rst), a n d
po lyuria ( excess ive u rinati o n ) . c. I t u s u a l ly h as a sudden onset before 20 yea rs o f a g e a n d i s d i sti n g u ished by damage to a n d
destructi on o f P-ce l l s o f the i s l ets o f La n g e rhans . B e c a use o f its e a rly onset, I DDM is a l s o kn own as j uven i le-onset d iabetes me l l itus.
d . I t i s treated with a comb i n ati o n of i n su l i n th e rapy a n d d i et. 3. Type 2 (non-insu l i n-dependent) d iabetes me l l itus (N IDDM)
a . N I D D M does not resu lt from low leve l s o f p l a sma i n su l i n a n d is insu l i n resistant, wh i c h is a major fa cto r i n its pathogenes is . The res ista n c e to i n su l i n is due to d e c reased b i n d i n g of i n su l i n to its p l a sma l emma re c eptors and to d efe cts i n postre c e pto r i n su l i n a cti on .
b. I t c ommon ly o c c u rs i n ove rwe i g ht i n d ivi d u a l s o l d e r th a n 40 years . c. I t i s usua l l y contro l l e d by d i et. d . O l d e r i n d iv i d u a l s with type 2 d i a b etes ofte n p resent with memo ry p rob l ems p roba b ly
b e c a use amylo id-j3-derived d iffus ib le l igands (ADDLs) b ind to the p resyna pti c m e m b ra n es of the axons of c e rta in n e u rons that a re respons i b l e fo r memo ry sto ra g e . Th is c ond iti o n p reve nts t h e rep l en i shm ent o f insu l in receptors o f th ese axons, even tho ugh t h e re c e ptors, synthes ized i n the soma , a re ava i l a b l e i n th e soma 's cytop l a sm . Appa re ntly, the re c e pto rs a re p revented from be i ng tra nsfe rred from the cytoso l of th e soma to the axop l a sm of the axo n . Th is m a kes these n e u rons i n su l i n res istant and u n a b l e to reg u l ate th e i r g l u c ose metabo l i sm, a n d in tu rn , th ese n e u rons c a n not fun cti on no rm a l ly a n d the pat ient h as memo ry l o s s a n d Alzh e ime r d isease-assoc i ated d ementi a . Some resea r che rs sugg est th is to be type 3 d iabetes.
4. Pancreatic cancer i s a ma l i g n a nt n eop l a sm , a n d most pat ients d i e with i n 6 months to 1 yea r after d i a g nos is . Most o f the cases a re adenocarcinomas i n the h e a d o f the p a n c reas . Its i n c i d e n c e is th ree to fo u r times g reater i n m a l e pat ie nts tha n i n fem a l e pat ie nts. Alth ough its sym ptoms i n c l u d e a no rexi a , f latu l e n ce , fatty stoo l if the b i l e d u ct is obstru cted , s u dden loss of we ight, wea kness, b a c k pa in , and j a u nd i ce , exp l o rato ry b i opsy is c ommon ly req u i re d fo r a d ef in itive d i a g nos is .
5. B lood g lucose level i n a fa sti ng , n o nd i a b et ic i n d ivi d u a l shou ld be between 80 and 1 1 0 mg per 1 00 ml ( 4 .4 to 6 . 1 mmol pe r L) of b l ood . I f the g l u cose leve ls r ise a bove that l eve l , the P-ce l l s r e l ease i nsu l i n . I f th e b l ood g l u cose leve ls fa l l b e low that leve l , the a- ce l l s r e l ease g l u c a g o n . Add iti o n a l c ontro l mecha n i sms i n c l u d e t h e n e u rotra nsm itte rs re l eased b y t h e ce l l s o f the a utonom i c n e rvous system, n a m e ly: sym pathet ic fi b e rs i n c rease g l u c a g o n s e c reti on and i n h i b it i n su l i n s ec reti on , whereas pa rasym pathetic fi b e rs i n c rease both i n su l i n a n d g l u c a g o n sec re t ions i n o rd e r to ma i nta i n a b a l a n c ed homeostas i s .
A. Overview 1. The liver is composed of a single type of parenchymal cell, the hepatocyte . 2. It is the largest gland in the body, weighing as much as 1 .5 kg. 3. It is surrounded by a dense, irregular collagenous connective tissue known as G l isson capsule,
which gives rise to septa that subdivide the liver into its four lobes (right, left, caudate, and quadrate lobes) and its enormous number of lobules.
4. Function . The liver produces bi le and plasma proteins and has a myriad of other functions discussed in Sections E and F.
tahir99-VRG & vip.persianss.ir
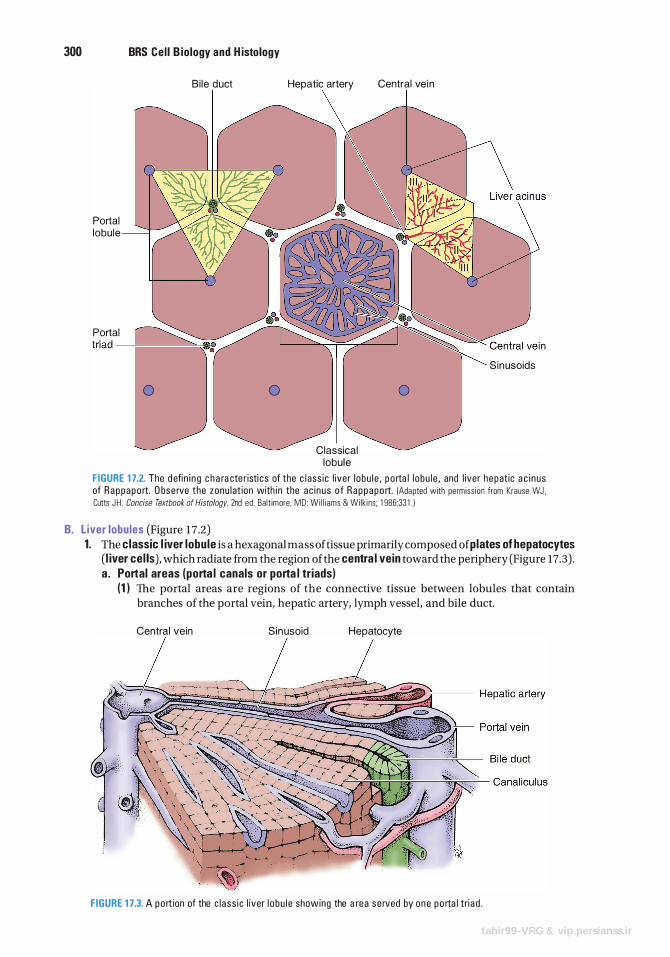
300 BRS Cel l B iology and H istology
Portal lobule
Bi le duct
Portal tr iad -�.....,.....,....,�.,
0 0
Hepatic artery Central vein
S inusoids
0
Classical lobule
FIGURE 1 7.2. The d efi n i n g c h a ra cte r isti cs of the c l ass ic l iver l obu l e , p o rta l l obu l e , and l iver hepat ic a c i nus of Rappapo rt. O bse rve the zonu l at ion with i n the ac i nus o f Rappapo rt. (Adapted with permiss ion from Krause WJ , Cutts JH . Concise Textbook of Histology. 2nd ed . Ba lt imore, MD : W i l l iams & Wilk i ns; 1 986:33 1 . )
B. L iver lobules (Figure 17.2) 1. The classic l iver lobule is a hexagonal mass of tissue primarily composed of plates of hepatocytes
( l iver cel ls), which radiate from the region of the centra l vein toward the periphery (Figure 17.3) . a. Portal areas (porta l canals or porta l triads)
(1 ) The portal areas are regions of the connective tissue between lobules that contain branches of the portal vein, hepatic artery, lymph vessel, and bile duct.
Central vein Sinusoid Hepatocyte
FIGURE 1 7.3. A p o rt ion of the c l ass i c l iver l o bu l e showing the a rea se rved by one p o rta l tri a d .
tahir99-VRG & vip.persianss.ir
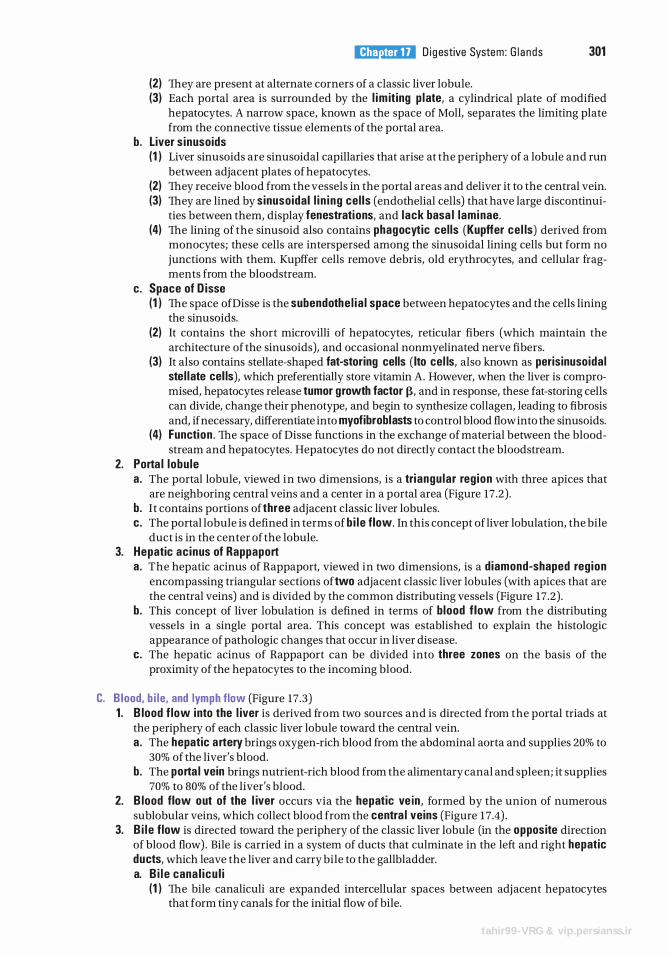
l!il!tt'!1lliUI D ig estive System : G l a nds 301
(2) They are present at alternate corners of a classic liver lobule. (3) Each portal area is surrounded by the l im it ing p late, a cylindrical plate of modified
hepatocytes. A narrow space, known as the space of Moll, separates the limiting plate from the connective tissue elements of the portal area.
b. Liver s inusoids (1 ) Liver sinusoids are sinusoidal capillaries that arise at the periphery of a lobule and run
between adjacent plates ofhepatocytes. (2) They receive blood from the vessels in the portal areas and deliver it to the central vein. (3) They are lined by sinusoidal l i n i ng cel ls (endothelial cells) that have large discontinui
ties between them, display fenestrations, and lack basa l laminae. (4) The lining of the sinusoid also contains phagocytic cel ls (Kupffer cel ls) derived from
monocytes; these cells are interspersed among the sinusoidal lining cells but form no junctions with them. Kupffer cells remove debris, old erythrocytes, and cellular fragments from the bloodstream.
c. Space of D isse (1 ) The space ofDisse is the subendothe l ia l space between hepatocytes and the cells lining
the sinusoids. (2) It contains the short microvilli of hepatocytes, reticular fibers (which maintain the
architecture of the sinusoids), and occasional nonmyelinated nerve fibers. (3) It also contains stellate-shaped fat-storing cells ( Ito cel ls, also known as perisinusoidal
stel late cel ls), which preferentially store vitamin A. However, when the liver is compromised, hepatocytes release tumor growth factor J3, and in response, these fat-storing cells can divide, change their phenotype, and begin to synthesize collagen, leading to fibrosis and, if necessary, differentiate into myofibroblasts to control blood flow into the sinusoids.
(4) Function . The space of Disse functions in the exchange of material between the bloodstream and hepatocytes. Hepatocytes do not directly contact the bloodstream.
2. Porta l lobu le a . The portal lobule, viewed in two dimensions, is a triangu lar reg ion with three apices that
are neighboring central veins and a center in a portal area (Figure 17 .2) . b. It contains portions of three adjacent classic liver lobules. c. The portal lobule is defined in terms of b i l e flow. In this concept of liver lobulation, the bile
duct is in the center of the lobule. 3. Hepatic ac inus of Rappaport
a. The hepatic acinus of Rappaport, viewed in two dimensions, is a diamond-shaped reg ion encompassing triangular sections of two adjacent classic liver lobules (with apices that are the central veins) and is divided by the common distributing vessels (Figure 17 .2) .
b. This concept of liver lobulation is defined in terms of blood f low from the distributing vessels in a single portal area. This concept was established to explain the histologic appearance of pathologic changes that occur in liver disease.
c. The hepatic acinus of Rappaport can be divided into three zones on the basis of the proximity of the hepatocytes to the incoming blood.
C. B lood, b i l e, and lymph flow (Figure 17.3) 1 . B lood f low into the l iver is derived from two sources and is directed from the portal triads at
the periphery of each classic liver lobule toward the central vein. a. The hepatic artery brings oxygen-rich blood from the abdominal aorta and supplies 20% to
30% of the liver's blood. b. The porta l vein brings nutrient-rich blood from the alimentary canal and spleen; it supplies
70% to 80% of the liver's blood. 2. B lood flow out of the l iver occurs via the hepatic ve in , formed by the union of numerous
sublobular veins, which collect blood from the centra l veins (Figure 17.4) . 3. B i l e flow is directed toward the periphery of the classic liver lobule (in the opposite direction
of blood flow) . Bile is carried in a system of ducts that culminate in the left and right hepatic ducts, which leave the liver and carry bile to the gallbladder. a. B i l e cana l icu l i
(1 ) The bile canaliculi are expanded intercellular spaces between adjacent hepatocytes that form tiny canals for the initial flow of bile.
tahir99-VRG & vip.persianss.ir
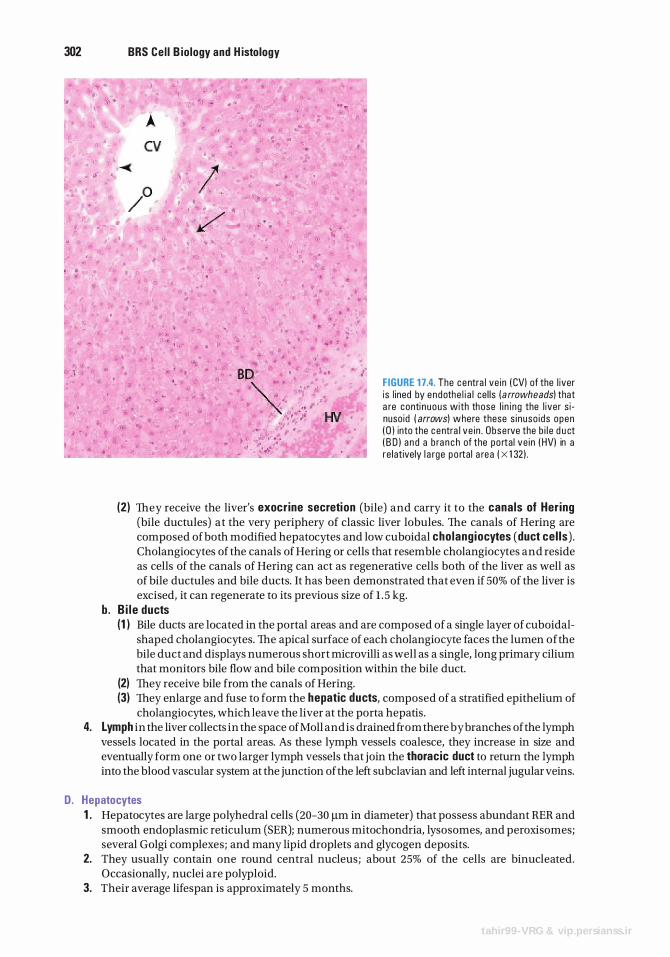
302 BRS Cel l B iology and H istology
FIGURE 1 7.4. The centra l ve in ( CVl of the l iver is l ined by endothe l i a l ce l ls ( arrowheads) that a re conti n uous with those l i n i ng the l iver s i nuso id ( arrows) where these s i nuso i ds open ( D ) into the centra l ve i n . Obse rve the b i l e d u ct ( B O l a n d a b ra n c h of the po rta l ve i n ( HVl in a re latively l a rge p o rta l a rea ( X 1 32 l .
(2) They receive the liver's exocrine secretion (bile) and carry it to the canals of Her ing (bile ductules) at the very periphery of classic liver lobules. The canals of Hering are composed of both modified hepatocytes and low cuboidal cho lang iocytes (duct cel ls) . Cholangiocytes of the canals of Hering or cells that resemble cholangiocytes and reside as cells of the canals of Hering can act as regenerative cells both of the liver as well as of bile ductules and bile ducts. It has been demonstrated that even if 50% of the liver is excised, it can regenerate to its previous size of 1 . 5 kg.
b . B i l e ducts (1 ) Bile ducts are located in the portal areas and are composed of a single layer of cuboidal
shaped cholangiocytes. The apical surface of each cholangiocyte faces the lumen ofthe bile duct and displays numerous short microvilli as well as a single, long primary cilium that monitors bile flow and bile composition within the bile duct.
(2) They receive bile from the canals of Hering. (3) They enlarge and fuse to form the hepatic ducts, composed of a stratified epithelium of
cholangiocytes, which leave the liver at the porta hepatis . 4. Lymph in the liver collects in the space of Moll and is drained from there by branches of the lymph
vessels located in the portal areas. As these lymph vessels coalesce, they increase in size and eventually form one or two larger lymph vessels that join the thoracic duct to return the lymph into the blood vascular system at the junction of the left subclavian and left internal jugular veins.
D. Hepatocytes 1 . Hepatocytes are large polyhedral cells (20-30 flm in diameter) that possess abundant RER and
smooth endoplasmic reticulum (SER); numerous mitochondria, lysosomes, and peroxisomes; several Golgi complexes; and many lipid droplets and glycogen deposits.
2. They usually contain one round central nucleus; about 25% of the cells are binucleated. Occasionally, nuclei are polyploid.
3. Their average lifespan is approximately 5 months.
tahir99-VRG & vip.persianss.ir
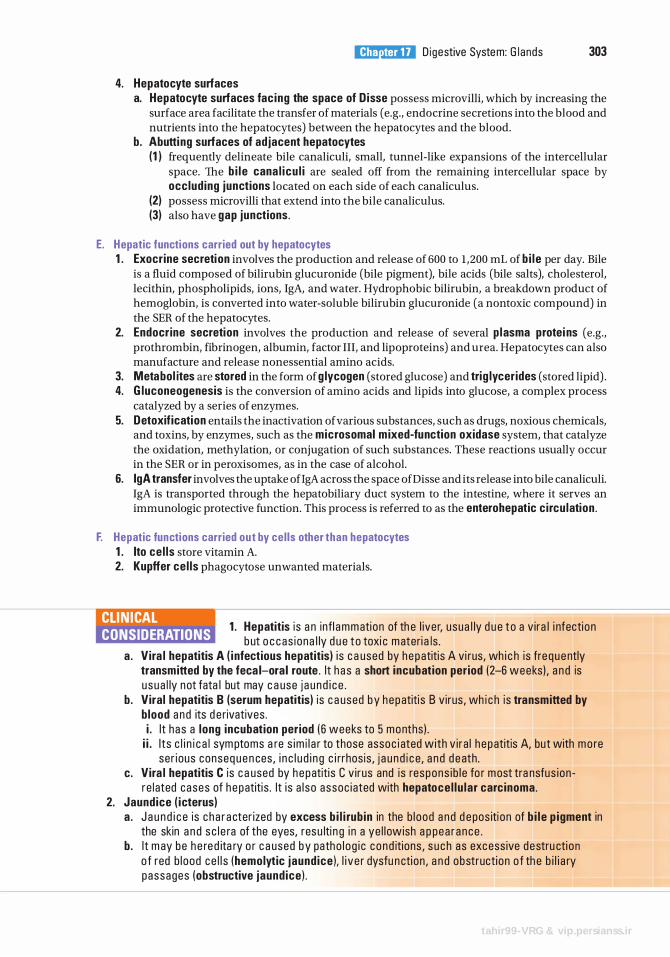
4. Hepatocyte surfaces
l!il!tt'!1lliUI Digestive System: G l ands 303
a. Hepatocyte surfaces fac ing the space of D isse possess microvilli, which by increasing the surface area facilitate the transfer of materials (e.g., endocrine secretions into the blood and nutrients into the hepatocytes) between the hepatocytes and the blood.
b. Abutting surfaces of adjacent hepatocytes (1 ) frequently delineate bile canaliculi, small, tunnel-like expansions of the intercellular
space. The b i l e cana l icu l i are sealed off from the remaining intercellular space by occlud ing junctions located on each side of each canaliculus.
(2) possess microvilli that extend into the bile canaliculus. (3) also have gap junctions.
E. Hepatic functions carried out by hepatocytes 1 . Exocrine secretion involves the production and release of 600 to 1 ,200 mL of b i l e per day. Bile
is a fluid composed of bilirubin glucuronide (bile pigment), bile acids (bile salts), cholesterol, lecithin, phospholipids, ions, IgA, and water. Hydrophobic bilirubin, a breakdown product of hemoglobin, is converted into water-soluble bilirubin glucuronide (a nontoxic compound) in the SER of the hepatocytes.
2. Endocrine secretion involves the production and release of several p lasma protei ns (e.g., prothrombin, fibrinogen, albumin, factor III, and lipoproteins) and urea. Hepatocytes can also manufacture and release nonessential amino acids.
3. Metabol ites are stored in the form of g lycogen (stored glucose) and trig lycerides (stored lipid) . 4. G luconeogenesis is the conversion of amino acids and lipids into glucose, a complex process
catalyzed by a series of enzymes. 5. Detoxif ication entails the inactivation of various substances, such as drugs, noxious chemicals,
and toxins, by enzymes, such as the microsomal m ixed-function oxidase system, that catalyze the oxidation, methylation, or conjugation of such substances. These reactions usually occur in the SER or in peroxisomes, as in the case of alcohol.
6. lgA transfer involves the uptake ofigA across the space ofDisse and its release into bile canaliculi. IgA is transported through the hepatobiliary duct system to the intestine, where it serves an immunologic protective function. This process is referred to as the enterohepatic c i rcu lation .
F. Hepatic functions carried out by cel ls other than hepatocytes 1 . Ito ce l ls store vitamin A. 2. Kupffer ce l ls phagocytose unwanted materials.
CLIN ICAL CONSIDERATIONS
1 . Hepatitis i s a n infl ammati on of th e l i ve r, usua l ly d u e to a v i ra l i nfecti on b ut o c c as i ona l ly d u e to toxi c materi a ls .
a . Vira l hepatitis A ( i nfectious hepatitis) i s c a used by hepatiti s A vi rus, wh i c h is fre q uently transmitted by the feca l-ora l route . I t h a s a short incubation period (2-6 weeks) , a n d is u sua l ly not fata l but may c a use j a u n d i c e .
b . Viral hepatitis B (serum hepatitis) i s c a used by hepatiti s B v i rus , wh i c h is transmitted by b lood and its d e rivatives . i . I t has a long incubation period ( 6 weeks to 5 months) .
i i . I ts c l i n i c a l sym ptoms a re s im i l a r to those assoc i ated with v i ra l h epatitis A, but with mo re ser ious conseq u e n ces , i n c l u d i n g c i rrhos is , j a u n d i c e, a n d d e ath .
c. Vira l hepatitis C is c a used by h e patiti s C v i rus and is respons i b l e fo r most tra nsfus i on re l ated cases of h e patiti s . It i s a l so assoc i ated with hepatoce l lu lar carcinoma.
2. Jaundice ( icterus) a . J a u n d i c e is c h a r a cter ized by excess b i l i rub in in the b l ood a n d d e pos iti on of b i l e p igment in
the skin a n d s c l e ra of the eyes, resu lti n g i n a ye l l owish a p pea r ance . b . I t m ay be h e re d ita ry o r c a used by patho l og i c c ond itions , s u ch as excess ive destru cti o n
o f red b l ood ce l l s (hemolytic jaund ice ), l i v e r dysfu n cti on , a n d obstructi on o f th e b i l i a ry passages (obstructive jaund ice ) .
tahir99-VRG & vip.persianss.ir
304 BRS Cel l B iology and H istology
A. The gallbladder communicates with the common hepatic duct via the cystic duct, which originates at the neck of the gallbladder.
B. It has a muscular wall whose contraction, stimulated by cholecystok in in (possibly in conjunction with acetylcholine), forces bile from its lumen into the duodenum. The wall has four layers : 1 . The mucosa is composed of a simple columnar epithel ium and a richly vascularized lamina
propria. When the gallbladder is empty, the mucosa displays highly convoluted folds (Figure 17 .5). 2. The musc le layer is composed of a thin, oblique layer of smooth musc le cel ls . 3. The connective tissue layer consists of dense irregular collagenous connective tissue and
houses nerves and blood vessels. 4. The serosa covers most of the gallbladder, but adventitia is present where the organ is attached
to the liver.
C. Function . The gallbladder concentrates, stores, and releases bile. It removes approximately 90% of the bile's water content by the manipulation of the subepithelial connective tissue electrolyte levels. It does so by actively removing sodium, chloride, and bicarbonate ions from the epithelial cells using energy-requiring pumps in the epithelial cell's basal plasmalemma, which, in turn, causes water to leave the cell, passively, via aquaporin l and aquaporin 8 channels. In order to equilibrate the osmotic differences between the bile in the lumen of the gallbladder and the epithelial cells lining the lumen, water moves from the bile into the epithelial cells because of the processes just described.
FIGURE 1 7.5. The m u cosa of th e em pty g a l l b l a dde r i s h i g h ly fo l ded , m a ki ng t h e l umen ( L) a p p e a r t o be e nc l osed by t he f o l d s . The co l umna r ep ithe l i um (E ) l i n i ng the l umen overl i es a ri c h ly vasc u l a rized l am i n a p ro p ri a ( LP ) that is s u rro unded by the smooth musc le ( M ) c o a t o f th e ga l l b l a dde r ( x 1 32) .
tahir99-VRG & vip.persianss.ir

l!il!tt'!1lliUI D i g estive System: G l ands 305
1 . Ga l lstones (b i l iary ca lcu l i ) CLIN ICAL CONSIDERATIONS a . G a l l stones a re c o n c retions , u s ua l ly o f f used c rysta ls o f cholesterol ,
which form i n the g a l l b l a d d e r o r b i l e d u ct. b. Accumu lation of g a l lstones may l e a d to th e b l o ckage of th e cysti c d u ct, wh i c h p revents
em pty ing of the g a l l b l a d d e r. c. G a l lstones may have to be s u rg i c a l ly removed if l ess - i nvas ive m ethods fa i l to d isso lve o r
p u lver ize th em . 2 . I nfl a m m ati o n o f t h e g a l l b l a d d e r, whethe r chron ic o r acute, usua l ly d u e t o t h e presen c e of
g a l l stones, obstructi ng the a c c ess to th e cysti c d u ct, is known as cholecystitis. Chron i c c ho l e cystitis i s fre q uently th e resu lt of m u lti p l e bouts of a c ute cystit is . The a c ute fo rm of the cond iti o n is q u ite pa i nfu l , a n d the p a i n i s expe ri e n ced in the u p p e r ri g ht q u a d ra nt of the a b domen and may be so seve re a s to i n d u c e n ausea and vomiti n g . Fre q u ently, the cond itio n is t reated by su r g i c a l remova l of the g a l l b l a d d e r.
tahir99-VRG & vip.persianss.ir
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the one lettered answer that is best in each case.
1 . An 18-year-old man feels faint. Symptoms include constant hunger, thirst, and excessive urination. The probable diagnosis is
(A) viral hepatitis A. (B ) type 1 diabetes mellitus. (C) type 2 diabetes mellitus. (D) cirrhosis. (E) mumps.
2. Which of the following statements concerning liver sinusoids is true?
(A) They are continuous with bile canaliculi. (B ) They are surrounded by a well-developed
basal lamina. (C) They are lined by nonfenestrated
endothelial cells. (D ) They deliver blood to the central vein. (E) They deliver blood to the portal vein.
3. A woman has yellow sclera and yellowish pallor. Blood test results indicate a low red blood cell count. The probable diagnosis is
(A) viral hepatitis A. (B) viral hepatitis B . (C) cirrhosis. (D) hemolytic jaundice. (E) type 2 diabetes mellitus.
4. Which of the following statements concerning the gallbladder is true?
(A) It synthesizes bile. (B) It is lined by a simple columnar
epithelium. (C) Bile leaves the gallbladder via the common
bile duct. (D ) It has no muscle cells in the walls. (E) It is affected by the hormone secretin.
306
5. A patient complains to her physician about sudden weight loss, loss of appetite, weakness, and back pain. Because the patient's sclera and skin have a yellowish pallor, the doctor suspects
(A) type 2 diabetes. (B) gallstones. (C) pancreatic cancer. (D ) viral hepatitis A. (E ) viral hepatitis B .
6. Acinar cells of the exocrine pancreas secrete
(A) glucagon. (B ) lysozyme. (C ) insulin. (D ) plasma proteins. (E ) proteases.
7. Pancreatic a-cells secrete
(A) glucagon. (B ) lysozyme. (C ) insulin. (D ) plasma proteins. (E ) proteases.
8. Pancreatic �-cells secrete
(A) glucagon. (B ) lysozyme. (C ) insulin. (D ) plasma proteins. (E ) proteases.
tahir99-VRG & vip.persianss.ir

9. Submandibular acinar cells secrete
(A) glucagon. ( B ) lysozyme. (C ) insulin. (D ) plasma proteins. (E) proteases.
l!il!tt'!1lliUI D ig estive System : G l a nds 307
1 0. Hepatocytes secrete
(A) glucagon. (B ) lysozyme. (C) insulin. (D ) plasma proteins. (E) proteases.
tahir99-VRG & vip.persianss.ir
Answers and Explanations
1 . B . The three classic signs of type 2 diabetes (juvenile onset) are polyphagia (excessive eating), polyuria (excessive urination), and polydipsia (excessive drinking). The condition occurs in young individuals, usually before 20 years of age (see Chapter 17 III B 3 Clinical Considerations) .
2. D . Liver sinusoids are lined by fenestrated endothelial cells, lack a basal lamina, and deliver blood directly to the central vein (see Chapter 17 IV B 1 b) .
3. D . Yellow skin and yellow sclera are indicative of jaundice. Because the patient had a low red blood cell count, the most probable diagnosis is hemolytic jaundice (see Chapter 17 IV E 6 Clinical Considerations).
4. B . The gallbladder is lined by a simple columnar epithelium (see Chapter 17 V).
5. C. Pancreatic cancer has all of the symptoms listed, namely, sudden weight loss, loss of appetite, weakness, back pain, and jaundice. Although jaundice is noted in hepatitis A and B and in the presence of obstructive jaundice caused by gallstones, sudden weight loss, loss of appetite, and weakness are not diagnostic of these diseases. Diabetes mellitus does not cause jaundice, loss of appetite, or weight loss (see Chapter 17 III B 3 Clinical Considerations).
6. E . Several pro teases are synthesized by pancreatic acinar cells and are delivered via the pancreatic duct to the duodenum (see Chapter 17 III A 3) .
7. A. Glucagon is produced by a-cells of the islets of Langerhans. They are the second most abundant secretory cells of the endocrine pancreas (see Chapter 17 III B 3) .
8. C. Insulin is produced by pancreatic f3-cells, which are the most abundant cell type of the islets of Langerhans (see Chapter 17 III B 3) .
9. B . Lysozyme, an enzyme with antibacterial activity, is produced primarily by the submandibular salivary gland acinar cells (see Chapter 17 II B 1 ) .
1 0. D . Hepatocytes synthesize several plasma proteins, including fibrinogen, prothrombin, and albumin (see Chapter 17 IV E 2) .
308
tahir99-VRG & vip.persianss.ir
The Urinary System
I. OVERVIEW-THE URINARY SYSTEM
A. Structure. The urinary system is composed of the paired kidneys and ureters and the bladder and urethra .
B. Function . The urinary system produces and excretes urine, thereby clearing the blood of waste products. The kidneys also regulate the electrolyte levels in the extracellular fluid, synthesize renin and erythropoietin, and convert the less reactive form of vitamin D3 (25-0H-vitamin D3) to its more active form known as calcitrio l [1 ,25-(0H )z vitamin 03] .
A. General structure 1. Kidneys are paired bean-shaped organs enveloped by a thin capsule of connective tissue. 2. Each kidney is divided into an outer cortex and an inner medu l la . 3. Each kidney contains about 2 million nephrons. A nephron and the collecting tubule into
which it drains form a ur in iferous tubule . Each collecting tubule drains a number of nephrons.
B . The renal h i lum is a concavity on the medial border of the kidney. It houses arteries, veins, lymphatic vessels, nerves, and the renal pelvis.
C. The rena l pelvis (Figure 18 . 1 ) is a funnel-shaped expansion of the upper end of the ureter. It is continuous with the major rena l ca lyces, each of which in turn has several small tributaries, the minor ca lyces.
D. The renal medu l la lies deep to the cortex, but sends extensions (medu l l a ry rays) into the cortex. 1 . Renal (medul lary) pyramids are conical or pyramidal-shaped structures that compose the bulk
of the renal medulla. The bases of the pyramids establish the corticomedullary junction. The apex of each pyramid forms the deepest portion of the medulla. a. Each kidney contains 10 to 18 renal pyramids. b. Each pyramid consists primarily of the thin limbs of loops of Hen le , blood vessels, and
co l lecti ng tubules. 2. The renal papi l la is located at the apex of each renal pyramid. It has a perforated tip (area
cri brosa) that projects into the lumen of a minor calyx.
309
tahir99-VRG & vip.persianss.ir
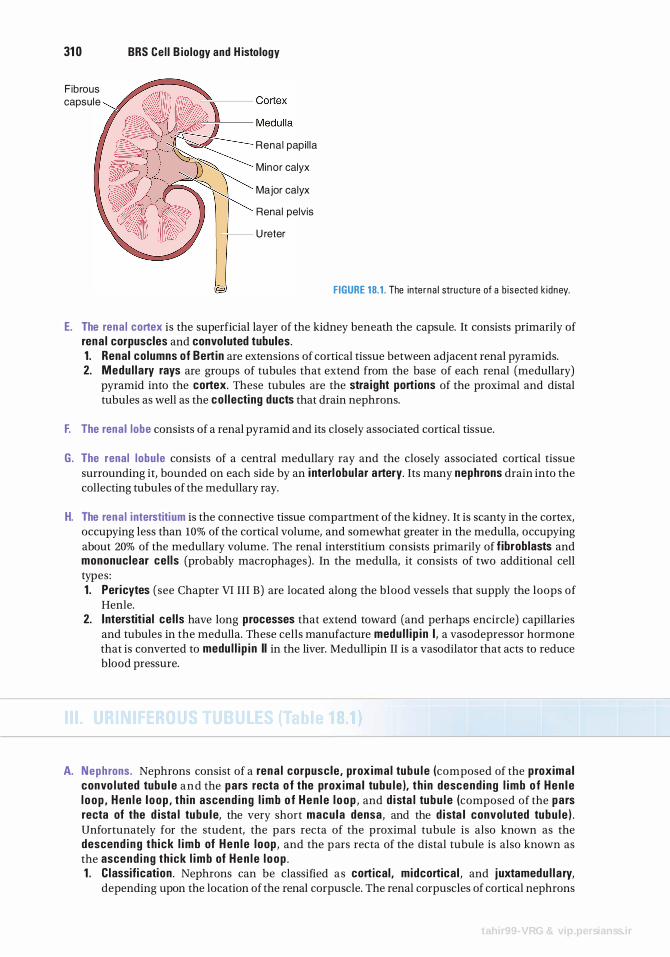
31 0 BRS Cel l B iology and H istology
Fibrous capsule
Renal papi l la
Minor calyx
Major calyx
Renal pelvis
U reter
FIGURE 18. 1 . The inte rna l stru ctu re of a b i sected k idney.
E. The rena l cortex is the superficial layer of the kidney beneath the capsule. It consists primarily of rena l corpuscles and convoluted tubules. 1 . Renal columns of Bertin are extensions of cortical tissue between adjacent renal pyramids. 2. Medu l lary rays are groups of tubules that extend from the base of each renal (medullary)
pyramid into the cortex. These tubules are the stra ight portions of the proximal and distal tubules as well as the co l lecting ducts that drain nephrons.
F. The rena l lobe consists of a renal pyramid and its closely associated cortical tissue.
G. The renal lobu le consists of a central medullary ray and the closely associated cortical tissue surrounding it, bounded on each side by an i nterl obu lar artery. Its many nephrons drain into the collecting tubules of the medullary ray.
H. The rena l interstitium is the connective tissue compartment of the kidney. It is scanty in the cortex, occupying less than 10% of the cortical volume, and somewhat greater in the medulla, occupying about 20% of the medullary volume. The renal interstitium consists primarily of f ibroblasts and mononuclear cel ls (probably macrophages). In the medulla, it consists of two additional cell types : 1 . Pericytes (see Chapter VI III B) are located along the blood vessels that supply the loops of
Henle. 2. Interstit ia l ce l ls have long processes that extend toward (and perhaps encircle) capillaries
and tubules in the medulla. These cells manufacture medu l l i p i n I , a vasodepressor hormone that is converted to medu l l i p i n II in the liver. Medullipin II is a vasodilator that acts to reduce blood pressure.
A. Nephrons. Nephrons consist of a rena l corpuscle , prox ima l tubu l e (composed of the proxima l convo l uted tubu le and the pars recta o f the prox ima l tubu le ), th in descend ing l imb of Hen le l oop , Hen l e l oop , th in ascend i ng l imb o f Hen l e l oop , and d ista l tubu le (composed of the pars recta of the d ista l tubu le, the very short macu la densa, and the d ista l convol uted tubu le ) . Unfortunately for the student, the pars recta of the proximal tubule is also known as the descend i ng th ick l imb of Hen l e loop , and the pars recta of the distal tubule is also known as the ascend i ng th ick l imb of Hen l e l oop . 1 . C lassification . Nephrons can be classified as cortical , midcortical , and j uxtamedu l l a ry,
depending upon the location of the renal corpuscle. The renal corpuscles of cortical nephrons
tahir99-VRG & vip.persianss.ir
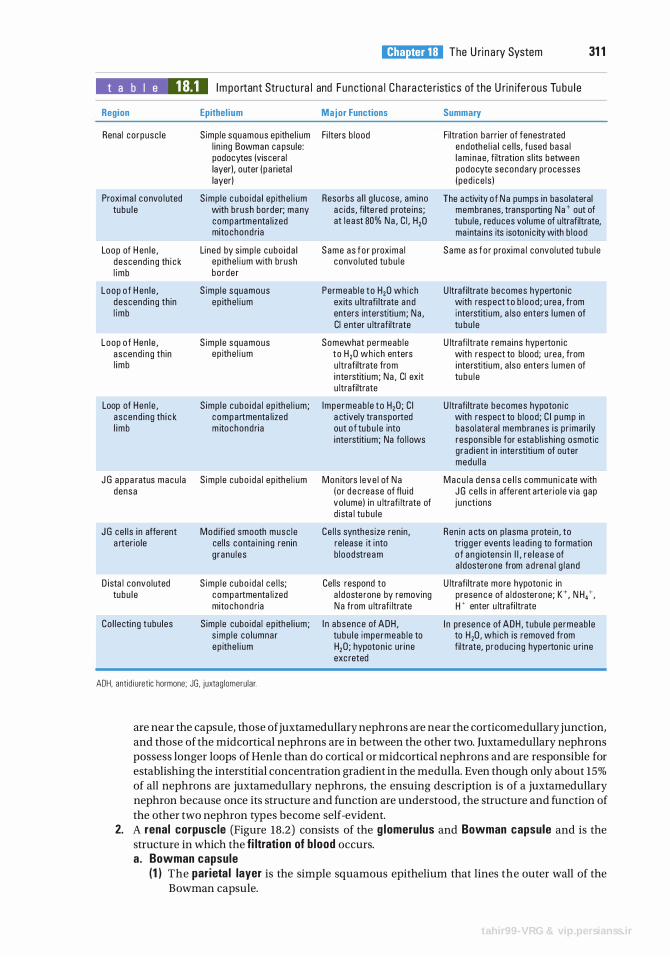
l!1llll"!ttffl The U ri n a ry System 31 1
t a b I e 18.1 I m po rtant Stru ctu ra l and Functio n a l C h a ra cte r isti c s of the U ri n ife rous Tu bu l e
Region Epithel ium Major Functions Summary
Renal co rpusc le S imp le squamous ep ithe l i um Fi lters b lood Filtration ba rr ier of fenestrated l i n ing Bowman ca psu le : e ndothe l i a l c e l ls, fused basa l podocytes (viscera l l am i nae, filtration s l its between layer), outer ( pa rieta l podocyte seconda ry processes layer) ( ped i ce l s )
Proxima l convo l uted S imp le c u bo i da l ep ithe l i um Resorbs a l l g l u cose, am ino The a ctivity of N a pumps in baso lateral tu bu l e with b rush border; many a c ids , filte red p rote ins ; membranes, transporting Na + out of
compartmenta l i zed at l e ast 80% Na , C l , H20 tubu le , reduces volume of u ltrafiltrate, mitochond ri a ma inta ins its isoton ic ity with b lood
Loop of H en le , Li ned by s imp l e cubo i da l Same as fo r p roxima l Same as fo r p roxima l convol uted tu bu l e descend i ng th i c k ep ithe l i um with brush convo l uted tu bu l e l imb bo rde r
Loop o f H en le , S imp l e squamous Permeab l e to H20 wh i ch U ltrafiltrate becomes hyperton i c descend i ng th in ep ithe l i um exits u ltrafi ltrate a nd with respect t o b l o od ; u rea , from l imb enters interstiti um ; Na , i nte rstiti um, a lso enters l umen of
Cl enter u ltrafi ltrate tu bu l e
Loop of Hen l e , S imp le squamous Somewhat pe rmeab l e U ltrafi ltrate rema ins hype rton i c ascend i ng th in ep ithe l i um to H20 wh ich enters with respect to blood; u rea , from l imb u ltrafi ltrate from i nterstiti um , a lso enters l umen of
i nte rstiti um ; Na , Cl exit tu bu l e u ltrafi ltrate
Loop of Hen l e , S imp le cubo i da l ep ithe l i um ; Impe rmeab l e to H20 ; C l U ltrafiltrate becomes hypoton i c ascend i ng th i c k compa rtmenta l i zed a ctively tra nsported with respect to b lood ; C l p ump in l imb m itochond ri a out of tu b u l e into baso latera l membranes is p r imari ly
i nte rstiti um ; Na fo l l ows respons ib le for esta b l i sh ing osmotic g rad ient in inte rstiti um of outer medu l l a
J G a ppa ratus macu l a S imp l e c ubo i d a l ep ithe l i um Mon itors l eve l of N a M a c u l a d e n s a c e l l s commun i cate with densa (o r d e c rease of fl u i d J G ce l l s in affe rent arter i o l e v ia gap
vo lume ) in u ltrafi ltrate of j u nct ions d ista l tu bu l e
J G ce l l s i n affe rent Mod if ied smooth musc l e Ce l l s synthes ize ren in , Ren in a cts on p l asma p rote in , to a rter io le ce l ls conta i n i ng ren in re lease it i nto trig ge r events l e ad i ng to formation
g ranu l es b loodstream o f a ng iotens in I I , r e l e ase of a l dosterone from a d re n a l g l a nd
D ista l convo luted S imp l e c ubo i d a l c e l ls ; Cel ls respond to U ltrafiltrate more hypoton i c in tu bu l e c ompa rtmenta l ized a l d oste rone by removing presen c e of a l d osterone; K+, N H,+,
mitochond ria N a from u ltrafi ltrate W enter u ltrafi ltrate
Co l l ecti ng tubu les S imp le cubo ida l e p ithe l i um ; I n absence of AOH , I n presence of AOH , tubu le pe rmeab le s imp l e co l umnar tu bu l e impermeab l e to to H20 , wh ich is removed from ep ithe l i um H20 ; hypoton i c u r i ne fi ltrate, p roduc i ng hype rton i c u ri ne
exc reted
ADH, ant id i u retic hormone; JG, juxtag lomeru lar.
are near the capsule, those of juxtamedullary nephrons are near the corticomedullary junction, and those of the mid cortical nephrons are in between the other two. Juxtamedullary nephrons possess longer loops of Henle than do cortical or midcortical nephrons and are responsible for establishing the interstitial concentration gradient in the medulla. Even though only about 15% of all nephrons are juxtamedullary nephrons, the ensuing description is of a juxtamedullary nephron because once its structure and function are understood, the structure and function of the other two nephron types become self-evident.
2. A renal corpuscle (Figure 18.2) consists of the g lomerulus and Bowman capsule and is the structure in which the fi ltrati on of b lood occurs. a. Bowman capsule
(1 ) The parieta l layer is the simple squamous epithelium that lines the outer wall of the Bowman capsule.
tahir99-VRG & vip.persianss.ir
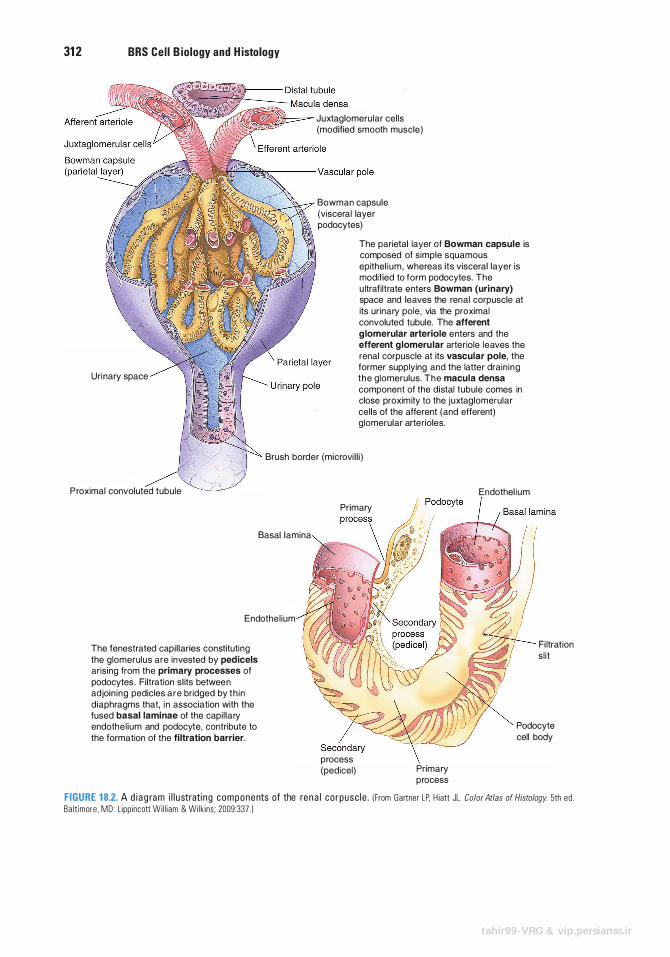
31 2 BRS Cel l B iology and H istology
Uri nary space
Juxtaglomerular cel ls (modified smooth muscle)
Bowman capsule (visceral layer podocytes)
The parietal layer of Bowman capsule is composed of s imple squamous epithel ium, whereas its visceral layer is modified to form podocytes. The u ltrafi ltrate enters Bowman (uri nary) space and leaves the renal corpuscle at its ur inary pole, via the proximal convoluted tubule. The afferent g lomerular arteriole e nters and the efferent g lomeru lar arteriole leaves the renal corpuscle at its vascular pole, the former supplying and the latter drain ing the glomerulus. The macula densa component of the distal tubule comes in close proxim ity to the juxtaglomerular cel ls of the afferent (and efferent) glomerular arterioles.
Brush border (microvi l l i )
P roximal convoluted tubule
Basal lamina
Endothel ium
The fenestrated capi l laries constituti ng the glomerulus are invested by pedicels arising from the primary processes of podocytes . Filtration sl its betwee n adjoin ing pedicles a r e bridged by t h i n diaphragms that, i n association with the fused basal laminae of the capi l lary endothel ium and podocyte, contribute to the formation of the fi ltration barrier.
Primary
process (pedicel) Primary
process
Endothel ium
Fi ltration s l i t
Podocyte cell body
FIGURE 1 8.2. A d i a g ra m i l l u strati n g components of the ren a l co rpusc l e . ! From Gartner LP. H iatt JL. Color Atlas of Histology. 5th ed . Ba l t imore . MD : L ipp incott Wi l l i am & Wilk ins ; 2009:337 . )
tahir99-VRG & vip.persianss.ir
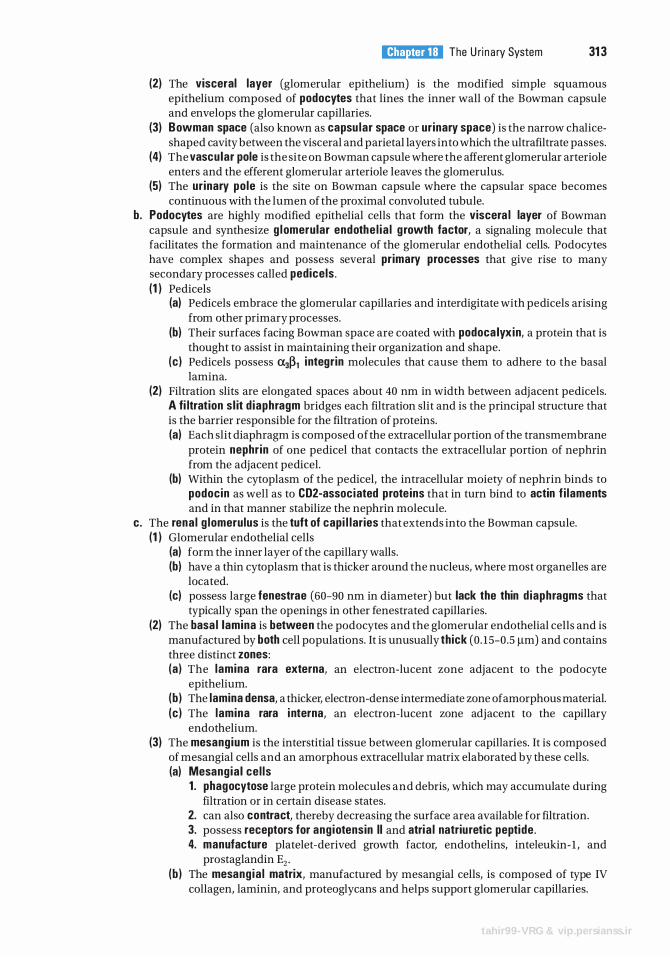
l!1llll"!ttffl The U ri n a ry System 31 3
(2) The visceral layer (glomerular epithelium) is the modified simple squamous epithelium composed of podocytes that lines the inner wall of the Bowman capsule and envelops the glomerular capillaries.
(3) Bowman space (also known as capsu lar space or urinary space) is the narrow chaliceshaped cavity between the visceral and parietal layers into which the ultrafiltrate passes.
(4) The vascular pole is the site on Bowman capsule where the afferent glomerular arteriole enters and the efferent glomerular arteriole leaves the glomerulus.
(5) The urinary pole is the site on Bowman capsule where the capsular space becomes continuous with the lumen of the proximal convoluted tubule.
b. Podocytes are highly modified epithelial cells that form the viscera l layer of Bowman capsule and synthesize g lomerular endothe l ia l g rowth factor, a signaling molecule that facilitates the formation and maintenance of the glomerular endothelial cells. Podocytes have complex shapes and possess several primary processes that give rise to many secondary processes called pedicels . (1 ) Pedicels
(a) Pedicels embrace the glomerular capillaries and interdigitate with pedicels arising from other primary processes.
(b) Their surfaces facing Bowman space are coated with podoca lyxin, a protein that is thought to assist in maintaining their organization and shape.
(c ) Pedicels possess �:XJ�1 integrin molecules that cause them to adhere to the basal lamina.
(2) Filtration slits are elongated spaces about 40 nm in width between adjacent pedicels. A fi ltration s l it d iaphragm bridges each filtration slit and is the principal structure that is the barrier responsible for the filtration of proteins. (a) Each slit diaphragm is composed ofthe extracellular portion of the transmembrane
protein nephr in of one pedicel that contacts the extracellular portion of nephrin from the adjacent pedicel.
(b) Within the cytoplasm of the pedicel, the intracellular moiety of nephrin binds to podocin as well as to CD2-associated prote ins that in turn bind to actin f i laments and in that manner stabilize the nephrin molecule.
c. The rena l g lomerulus is the tuft of capi l lar ies that extends into the Bowman capsule. (1 ) Glomerular endothelial cells
(a) form the inner layer of the capillary walls. (b) have a thin cytoplasm that is thicker around the nucleus, where most organelles are
located. (c) possess large fenestrae (60-90 nm in diameter) but lack the thin d iaphragms that
typically span the openings in other fenestrated capillaries. (2) The basa l lamina is between the podocytes and the glomerular endothelial cells and is
manufactured by both cell populations. It is unusually thick (0. 15-0.5 J..Lm) and contains three distinct zones: (a) The lamina rara externa, an electron-lucent zone adjacent to the podocyte
epithelium. (b ) The lamina densa, a thicker, electron-dense intermediate zone of amorphous material. (c ) The lamina rara i nterna, an electron-lucent zone adjacent to the capillary
endothelium. (3) The mesangium is the interstitial tissue between glomerular capillaries. It is composed
of mesangial cells and an amorphous extracellular matrix elaborated by these cells. (a) Mesang ia l ce l ls
1 . phagocytose large protein molecules and debris, which may accumulate during filtration or in certain disease states.
2. can also contract, thereby decreasing the surface area available for filtration. 3. possess receptors for ang iotensin II and atria l natriuretic peptide . 4. manufacture platelet-derived growth factor, endothelins, inteleukin- 1 , and
prostaglandin E2 • (b ) The mesang ia l matrix, manufactured by mesangial cells, is composed of type IV
collagen, laminin, and proteoglycans and helps support glomerular capillaries.
tahir99-VRG & vip.persianss.ir
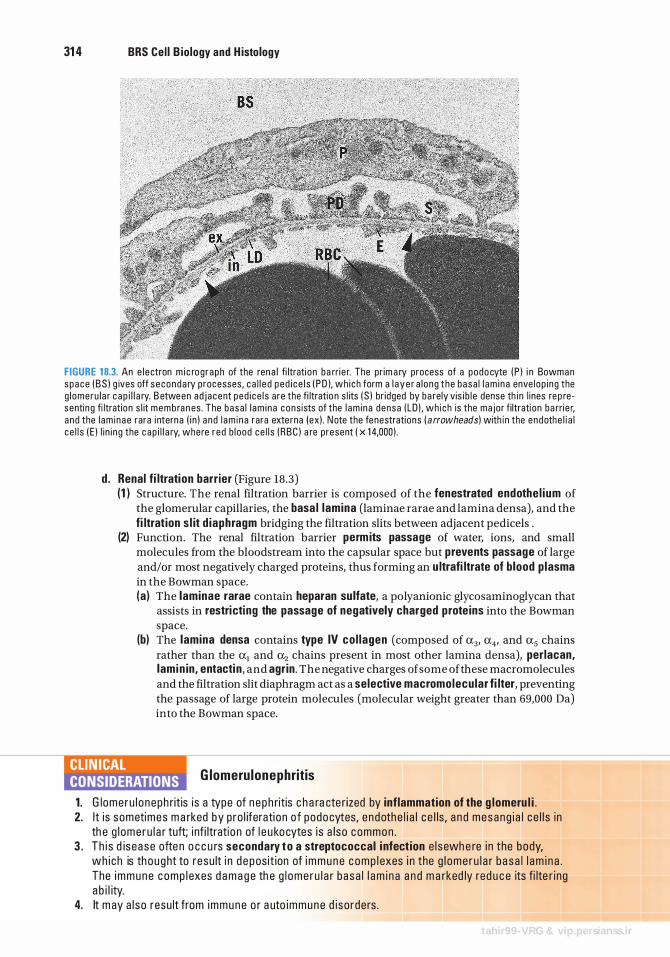
31 4 BRS Cel l B iology and H istology
FIGURE 18.3. An e l e ctron m i c rog raph of the ren a l fi ltrati on ba rri e r. The pr im a ry process of a podo cyte ( P ) i n Bowma n space ( B S ) g ives off s econda ry processes , c a l l e d p e d i c e l s ( P D ), wh i ch form a l a y e r a l ong t h e basa l l am i n a enve l op i ng the g l omeru l a r c a p i l l a ry. B etween ad j acent ped i ce l s a re the fi ltratio n s l its ( S ) br idged by ba rely vis i b l e dense th i n l ines rep re senting fi ltration s l it memb ra n es . The basa l l am i na consists of the l am i na densa (LD ) . wh i ch is the ma jor fi ltrati on ba rri e r, a nd the l am i nae rara i ntern a ( i n ) a nd l am i n a rara exte rna (ex) . N ote the fenestrati ons ( a rrowheads) with i n the endothe l i a l c e l l s ( E ) l i n i ng the c a p i l l a ry, where r ed b l ood ce l l s ( RBC ) a re present ( x 1 4,000) .
d . Renal fi ltration barr ier (Figure 18.3) (1 ) Structure. The renal filtration barrier is composed of the fenestrated endothe l ium of
the glomerular capillaries, the basa l lamina (laminae rarae and lamina densa), and the fi ltration s l it d iaphragm bridging the filtration slits between adjacent pedicels .
(2) Function. The renal filtration barrier permits passage of water, ions, and small molecules from the bloodstream into the capsular space but prevents passage of large and/or most negatively charged proteins, thus forming an u ltrafi ltrate of blood p lasma in the Bowman space. (a ) The laminae rarae contain heparan su lfate, a polyanionic glycosaminoglycan that
assists in restricting the passage of negatively charged prote ins into the Bowman space.
(b) The lamina densa contains type IV co l lagen (composed of a3, a4, and a5 chains rather than the a1 and a.z chains present in most other lamina densa), perlacan, lam i n in, entacti n, and agrin . The negative charges of some of these macromolecules and the filtration slit diaphragm act as a selective macromolecu lar fi lter, preventing the passage of large protein molecules (molecular weight greater than 69,000 Da) into the Bowman space.
lifi'n����� G lomeru lonephritis
1 . G lome ru l o neph ritis is a type of n e p h ritis c h a ra cte r ized by inflammation of the g lomeru l i . 2. I t is sometimes m a rked by p ro l iferati on o f podo cytes, e ndothe l i a l c e l ls , a n d mesang i a l c e l l s in
th e g l ome ru l a r tuft; i nf i ltratio n of l e u ko cytes i s a lso common . 3 . Th i s d is ease ofte n o c c u rs secondary to a streptococcal i nfect ion e l sewh e re i n the body,
wh i ch is th o ught to resu lt i n d e pos it ion of i m m u n e c o m p l exes i n the g l ome r u l a r b a s a l l a m i n a . The i m m u n e c omp l exes d a m a g e th e g l ome r u l a r b a sa l l a m i n a a n d m a rked ly red u c e its fi lte r i ng a b i l ity.
4. It m ay a l so resu lt from immune o r a uto immune d iso rde rs .
tahir99-VRG & vip.persianss.ir
l!1llll"!ttffl The U rinary System 315
5. It is assoc i ated with p ro d u ctio n of u r i n e - conta i n i n g b l ood (hematuria) , p rote i n ( p rote inur ia ) , o r both; i n severe c a ses, d e c reased u r i ne o utput (o l igur ia ) i s c ommon .
6 . It o c c u rs i n a c ute, s u b a c ute, a n d c h ron i c forms. The c h ron i c fo rm, i n wh i c h th e destructi on of g l ome ru l i c onti n u es, l e ads eventu a l ly to ren a l fa i l u re a n d d e ath .
Chron ic Renal Fa i l u re 1 . Ch ron i c re n a l fa i l u re c a n resu lt from a va ri ety of d i seases ( e . g . , d i a betes me l l itus, hype rte n
s ion , ath e rosc l e ros is ) i n wh i c h b l ood f l ow to the k i dn eys is red u c ed , c a us i ng a d e c rease i n g l ome r u l a r fi ltrati on a n d tu b u l a r i s c h em i a .
2 . It is assoc i ated with patho l o g i c a l c h a nges (hya l i n izati o n ) i n t h e g l ome ru l i a n d atro p hy o f the tu b u l es , wh i c h impa i r v i rtu a l ly a l l a spe cts of ren a l fu n cti on .
3 . It is ma rked by acidosis and hyperka lemia beca use the a c id-base ba l ance c a n n ot be ma i nta i n ed , a n d by uremia beca use o f th e i n a b i l ity t o e l im i n ate meta bo l i c wastes.
4. I f u ntreate d, c h ron i c ren a l fa i l u r e l e a ds to n e u ro l o g i c a l p rob l ems, coma , and d e ath .
AI port Syndrome M utation i n the a5 cha in of th e type IV co l l a g en ca uses d efective basa l l am ina fo rmati on i n th e kid n ey g l ome ru l u s ( as we l l as in othe r reg ions of the body, s uch a s the eye and i n ne r e a r) . S i n ce th e m utati on is X- l i n ked , men a re mo re se ri o us ly affe cted th a n women whose second X c h romosome may not bear the same m utati on . The effe cts on th e kid n ey resu lt i n th i cken i ng of th e basa l l am ina a n d the i n ab i l ity of the g l ome ru l a r fi ltrati on to o c c u r n o rma l ly, a n d p rote i n a nd b l ood beg i n to be present i n the u r i ne . Eventua l ly, i n m a ny pat ients, th e resu lt is k id n ey fa i l u re, a n d d i a lys is is req u i red to susta i n l ife . I n c e rta i n pat ients, k id ney transp l a nt is not v i ab l e b eca use the transp l a nted k idn ey's no rma l type IV co l l a gen may be pe rce ived as a nti g en i c by th e host a n d th e new k id ney may be rej e cted by th e immune system.
3. Proximal convo luted tubu le (Figures 18.4 and 18 .5) a. The proximal convoluted tubule is lined by a single layer of i rregu larly shaped (cuboidal
to columnar) epithelial cells that have microvilli forming a prominent brush border. These cells exhibit the following structures : (1 ) Apical canaliculi, vesicles, and vacuoles (endocytic complex), which function in prote in
absorption .
F IGURE 18.4. A l i g ht m i c rog raph of components i n the c o rtex ofthe k idney. A rena l co rpusc l e showing Bowm a n space (BS ) a nd a g l ome ru l u s ( G ); the macu l a densa (MD) of a j uxtag l ome ru l a r a p p a ratus; m a ny p roxima l tubu les ( PT) with p rom inent brush bo rde rs, a n d a few d ista l tu bu l es ( OT) a nd co l l e cti n g tu bu l es ( CT), as we l l as an a rte ry (A) a re i l l u strated ( x 1 50) .
tahir99-VRG & vip.persianss.ir
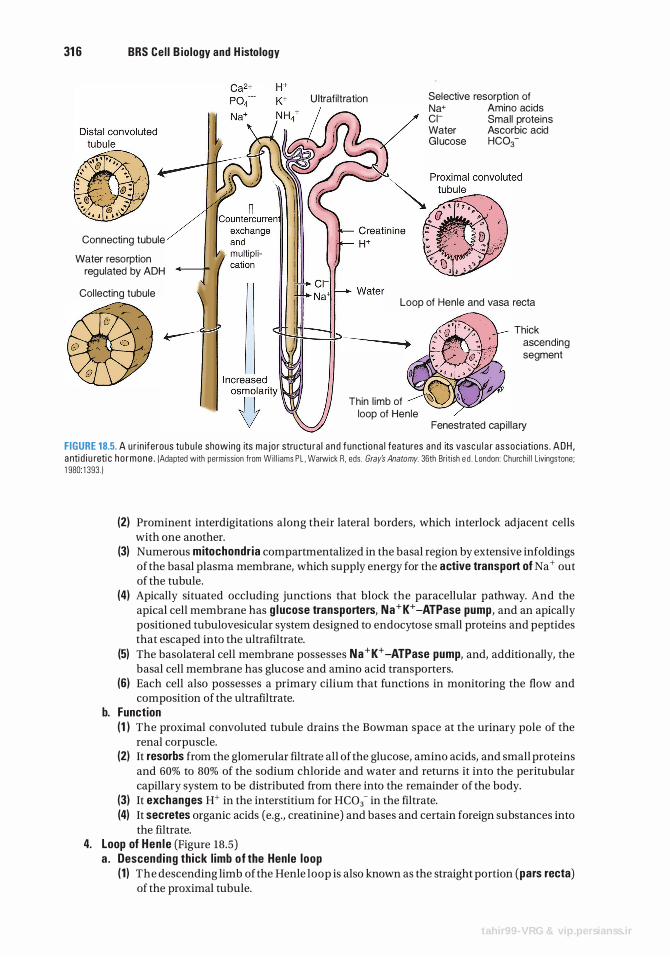
31 6 BRS Cel l B iology and H istology
Connecting tubule
Water resorption regulated by ADH
Ultrafi ltration Selective resorption of Na+ Amino acids Cl- Small proteins Water Ascorbic acid Glucose HC03-
Col lecting tubule Loop of Henle and vasa recta
Thin l imb of loop of Henle
Thick ascending segment
Fenestrated capi l lary
FIGURE 18.5. A u r i n iferous tu bu l e showing its ma jo r stru ctu ra l a n d functi o na l features and its vasc u l a r assoc i ations . ADH , a nti d i u reti c ho rmone . (Adapted with permiss ion from Wi l l iams P L . Warwick R . eds. Gray's Anatomy. 36th Br it ish e d . London : Church i l l L ivingstone; 1 980 1 393. )
(2) Prominent interdigitations along their lateral borders, which interlock adjacent cells with one another.
(3) Numerous mitochondr ia compartmentalized in the basal region by extensive infoldings of the basal plasma membrane, which supply energy for the active transport of Na + out of the tubule.
(4) Apically situated occluding junctions that block the paracellular pathway. And the apical cell membrane has g lucose transporters, Na+K+ -ATPase pump, and an apically positioned tubulovesicular system designed to endocytose small proteins and peptides that escaped into the ultrafiltrate.
(5) The basolateral cell membrane possesses Na+K+ -ATPase pump, and, additionally, the basal cell membrane has glucose and amino acid transporters.
(6) Each cell also possesses a primary cilium that functions in monitoring the flow and composition of the ultrafiltrate.
b. Function (1 ) The proximal convoluted tubule drains the Bowman space at the urinary pole of the
renal corpuscle. (2) It resorbs from the glomerular filtrate all of the glucose, amino acids, and small proteins
and 60% to 80% of the sodium chloride and water and returns it into the peri tubular capillary system to be distributed from there into the remainder of the body.
(3) It exchanges H+ in the interstitium for HC03- in the filtrate. (4) It secretes organic acids (e.g., creatinine) and bases and certain foreign substances into
the filtrate. 4. Loop of Hen le (Figure 18.5)
a . Descend ing thick l imb of the Henle loop (1 ) The descending limb of the Henle loop is also known as the straight portion (pars recta)
of the proximal tubule.
tahir99-VRG & vip.persianss.ir
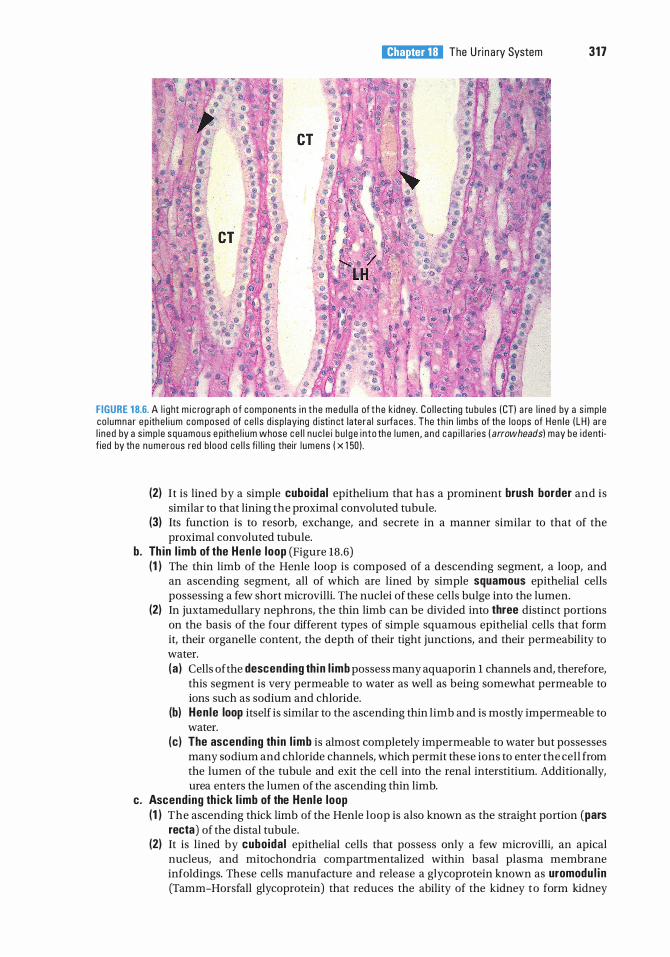
l!1llll"!ttffl The U ri n a ry System 317
FIGURE 1 8.6. A l i g ht m i c rog raph o f components i n t h e medu l l a of t h e k idney. Co l l e ct ing tu bu l es ( CTl a re l i n ed by a s imp l e co l umnar ep ithe l i um com posed of ce l l s d i sp lay ing d istin ct late ra l s u rfa ces . The th i n l imbs of the l oops of Hen l e ( LH l a re l i ned by a s imp l e squamous e p ith e l i um whose ce l l n u c l e i b u l g e i n to the l umen , a n d c a p i l l a ries ( arrowheads) may be i d entif ied by the numerous red b l ood ce l l s fi l l i n g their l umens ( x 1 50 ) .
(2) It is lined by a simple cuboidal epithelium that has a prominent brush border and is similar to that lining the proximal convoluted tubule.
(3) Its function is to resorb, exchange, and secrete in a manner similar to that of the proximal convoluted tubule.
b. Th in l imb of the Hen le loop (Figure 18 .6) (1 ) The thin limb of the Henle loop is composed of a descending segment, a loop, and
an ascending segment, all of which are lined by simple squamous epithelial cells possessing a few short microvilli. The nuclei of these cells bulge into the lumen.
(2) In juxtamedullary nephrons, the thin limb can be divided into three distinct portions on the basis of the four different types of simple squamous epithelial cells that form it, their organelle content, the depth of their tight junctions, and their permeability to water. (a ) Cells of the descending th i n l imb possess many aquaporin l channels and, therefore,
this segment is very permeable to water as well as being somewhat permeable to ions such as sodium and chloride.
(b) Hen le loop itself is similar to the ascending thin limb and is mostly impermeable to water.
(c) The ascending th in l imb is almost completely impermeable to water but possesses many sodium and chloride channels, which permit these ions to enter the cell from the lumen of the tubule and exit the cell into the renal interstitium. Additionally, urea enters the lumen of the ascending thin limb.
c. Ascending th ick l imb of the Hen le loop (1 ) The ascending thick limb of the Henle loop is also known as the straight portion (pars
recta) of the distal tubule. (2) It is lined by cuboida l epithelial cells that possess only a few microvilli, an apical
nucleus, and mitochondria compartmentalized within basal plasma membrane infoldings. These cells manufacture and release a glycoprotein known as uromodu l i n (Tamm-Horsfall glycoprotein) that reduces the ability of the kidney to form kidney
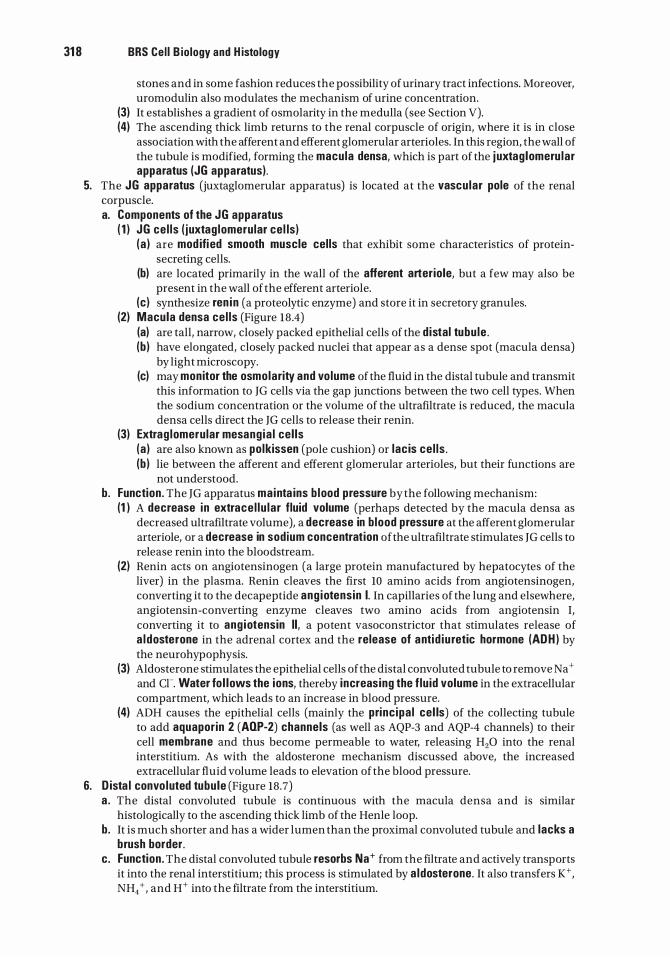
31 8 BRS Cel l B iology and H istology
stones and in some fashion reduces the possibility of urinary tract infections. Moreover, uromodulin also modulates the mechanism of urine concentration.
(3) It establishes a gradient of osmolarity in the medulla (see Section V). (4) The ascending thick limb returns to the renal corpuscle of origin, where it is in close
association with the afferent and efferent glomerular arterioles. In this region, the wall of the tubule is modified, forming the macula densa, which is part of the j uxtag lomeru lar apparatus (JG apparatus) .
5. The JG apparatus (juxtaglomerular apparatus) is located at the vascu lar pole of the renal corpuscle. a. Components of the JG apparatus
( 1 ) JG ce l ls ( juxtag lomerular cel ls) (a ) are mod ifi ed smooth muscle cel ls that exhibit some characteristics of protein
secreting cells. (b) are located primarily in the wall of the afferent arteriole, but a few may also be
present in the wall of the efferent arteriole. (c) synthesize ren in (a proteolytic enzyme) and store it in secretory granules.
(2) Macula densa ce l ls (Figure 18.4) (a) are tall, narrow, closely packed epithelial cells of the d istal tubu le . (b ) have elongated, closely packed nuclei that appear as a dense spot (macula densa)
by light microscopy. (c) may monitor the osmolarity and vo lume of the fluid in the distal tubule and transmit
this information to JG cells via the gap junctions between the two cell types. When the sodium concentration or the volume of the ultrafiltrate is reduced, the macula densa cells direct the JG cells to release their renin.
(3) Extrag lomerular mesang ia l cel ls (a ) are also known as polkissen (pole cushion) or lac is ce l ls . (b ) lie between the afferent and efferent glomerular arterioles, but their functions are
not understood. b. Function . The JG apparatus mainta ins b lood pressure by the following mechanism:
(1 ) A decrease in extrace l lu lar fluid volume (perhaps detected by the macula densa as decreased ultrafiltrate volume), a decrease in b lood pressure at the afferent glomerular arteriole, or a decrease in sodium concentration ofthe ultrafiltrate stimulates JG cells to release renin into the bloodstream.
(2) Renin acts on angiotensinogen (a large protein manufactured by hepatocytes of the liver) in the plasma. Renin cleaves the first 10 amino acids from angiotensinogen, converting it to the decapeptide ang iotensin I. In capillaries of the lung and elsewhere, angiotensin-converting enzyme cleaves two amino acids from angiotensin I, converting it to ang iotensin II, a potent vasoconstrictor that stimulates release of a ldosterone in the adrenal cortex and the release of antid iu retic hormone (ADH ) by the neurohypophysis.
(3) Aldosterone stimulates the epithelial cells of the distal convoluted tubule to remove Na + and cr. Water fo l lows the ions, thereby i ncreasing the f lu id volume in the extracellular compartment, which leads to an increase in blood pressure.
(4) ADH causes the epithelial cells (mainly the princ ipa l cel ls) of the collecting tubule to add aquaporin 2 (AOP-2) channels (as well as AQP-3 and AQP-4 channels) to their cell membrane and thus become permeable to water, releasing H20 into the renal interstitium. As with the aldosterone mechanism discussed above, the increased extracellular fluid volume leads to elevation of the blood pressure.
6. D ista l convo luted tubu le (Figure 18.7) a . The distal convoluted tubule is continuous with the macula densa and is similar
histologically to the ascending thick limb of the Henle loop. b. It is much shorter and has a wider lumen than the proximal convoluted tubule and lacks a
brush border. c . Function . The distal convoluted tubule resorbs Na+ from the filtrate and actively transports
it into the renal interstitium; this process is stimulated by a ldosterone. It also transfers K+, NH4 + , and H+ into the filtrate from the interstitium.
FIGURE 1 8.7. An e l e ctron m i c rog raph of a ce l l in the d i sta l convo luted tu bu l e of the k idney. E l ongated m ito chond ri a (M) are l o cated ( a rrowhead) with i n cytop l asm i c c o m p a rtme nts ( CC ) fo rmed by d e e p i n fo l d i ngs of the basa l p l asma mem brane where enzymes assoc iated with ion tra nsport a re l o cated . I n b etwee n these extens ive info l d i n gs is extra ce l l u l a r s pace ( a rrows). These ce l l s resorb Na+ from the fi ltrate and a ctively tra nspo rt it i nto the ren a l inte rstiti um ( a l d oste rone stimu l ates th is p rocess ) a nd a l so tra nsfer K+ , N H4 + , a nd W i nto th e fi ltrate from the i nte rstiti um . N ote the lamina densa ( LD ) and lamina Iuc ida ( LL), wh ich form the basa l l am i n a , the endothe l i a l ce l l ( E ) l i n i ng a fenestrated c a p i l l a ry, a nd the ap i ca l n u c le us ( N ) ( x 6,000).
l!1llll"!ttffl The Ur inary System 319
7. The connecti ng tubu le is a short segment between the distal convoluted tubule and the collecting tubule into which it drains. It is lined by the following two types of epithelial cells : a. Princ ipa l ce l ls have many infoldings of the basal plasma membrane. These cells remove
Na+ from the filtrate and secrete K+ into it. b. Interca lated cel ls have many apical vesicles and mitochondria. These cells remove K+
from the filtrate and secrete H+ into it.
CLIN ICAL CONSIDERATIONS
Nephrotoxic acute tubular necrosis i s the d eath o f k id n ey tu b u l e c e l l s c a used by th e i r exposu re t o a tox ic d rug o r mo l e c u le , rath e r th a n a l a c k of
oxyg en ( ischemic a c ute tu b u l a r n e c ros is ) . When a p e rson suffe rs a c rush i n j u ry c a us i ng s i g n ifi c a nt musc l e tra uma , myog l ob i n is re l eased from the musc l e a n d enters the b l oodstre a m . The myog l ob i n i s fi lte red th ro u gh the g l ome ru l i , but i t is tox ic to ce l l s of th e k id ney tu b u l es, c a us i n g n e p h rotoxi c a c ute tu b u l a r n e c ros is . I f the d a m a g e is not too severe, the ki d n ey tu b u l e c e l l s may be a b l e to re p l a c e th emse lves, b ut i n severe c a ses, they c a n n ot a n d th e k id n ey may not c o m p l ete ly recover.
B. Col lecti ng tubules (Figure 18.5) have an embryological origin different from that of nephrons. They have segments in both the cortex and the medulla and converge to form larger and larger tubules. 1. Cortica l co l lecti ng tubules are located primarily within medullary rays, although a few are
interspersed among the convoluted tubules in the cortex (cortical labyrinth). They are lined by a simple epithelium containing two types of cuboida l cells. a. Princ ipa l ( l i ght) ce l ls possess a round central nucleus and a single pr imary c i l i um. It is
these cells that are responsible for the ability of the collecting tubules to concentrate urine.
320 BRS Cel l B iology and H istology
b. I nterca lated (dark) ce l ls are less numerous than principal cells and possess microplicae (folds) on their apical surface and numerous apical cytoplasmic vesicles. There are two types of intercalated cells : a-interca lated ce l ls that have the ability to release H + ions into the tubular lumen, thus acidifying urine, and �-interca lated ce l ls that have the ability to release HC03- ions into the tubular lumen, thus causing the urine to be more alkaline. a-Intercalated cells possess hydrogen pumps, and �-intercalated cells possess HC03-pumps to fulfill their function.
2. Medul lary co l l ecti ng tubu les. In the outer medulla, medullary collecting tubules are similar in structure to cortical collecting tubules and contain both princ ipa l and i nterca lated ce l ls in their lining epithelium. In the inner medulla, the collecting tubules are lined only by princ ipa l cel ls (Figure 18.6) .
3. Pap i l l a ry co l lecting tubu les (ducts of Be l l i n i ) a . Papillary collecting tubules are large collecting tubules (200-300 Jlm in diameter) formed
from converging smaller tubules. b. They are lined by a simple epithelium composed of columnar cells that have a single
pr imary c i l i um. c . They empty at the area cr ibrosa, a region at the apex of each renal pyramid that has 10 to 25
openings through which the urine exits into a minor calyx.
The renal blood circulation is extensive, with total blood flow through both kidneys of about 1200 mL/min. At this rate, all of the circulating blood in the body passes through the kidneys every 4 to 5 minutes.
A. Arteria l supply to the kidney (Figure 18.8) 1. B ranches of the rena l artery enter each kidney at the hilum and give rise to interlobar
arteries. 2. Interlobar arteries travel between the renal pyramids and divide into several arcuate arteries,
which run along the corticomedullary junction parallel to the kidney's surface. 3. Interl obu lar arteries
a . Interlobular arteries are smaller vessels that arise from the arcuate arteries. b. They enter the cortical tissue and travel outward between adjacent medul lary rays .
Adjacent interlobular arteries delimit a renal lobule. c. They give rise to afferent (g lomeru lar) arterioles and send branches to the interstitium just
deep to the renal capsule. 4. Afferent arterioles are branches of the interlobular arteries that supply the g lomeru lar
cap i l lar ies. 5. Efferent arterio les arise from the glomerular capillaries and are associated with cortical,
midcortical, and juxtaglomerular nephrons. They leave the glomerulus of cortical and midcortical nephrons and give rise to an extensive peritubular capi l lary network that supplies the cortical labyrinth, whereas those that leave the juxtaglomerular nephrons give rise to the vasa recta .
6. Vasa recta a . The vasa recta arise from the efferent arterioles supplying j uxtamedu l la ry nephrons. b . These long, thin vessels ( arterio lae rectae) follow a straight path into the medulla and renal
papilla, where they form capillaries and then loop back and increase in diameter toward the corticomedullary boundary (venu lae rectae ) .
c . They are closely associated with the descend ing a nd ascend ing l imbs o f Hen le loops and col lecti ng ducts, to which they supply nutrients and oxygen.
d . These vessels play a critical role in countercurrent exchanges with the interstitium.
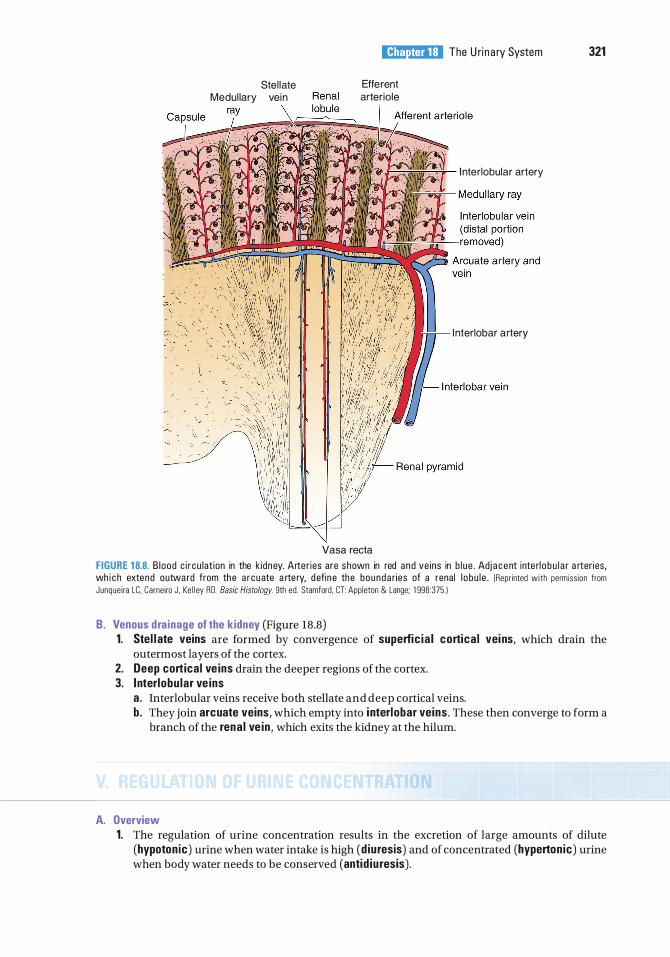
Stel late Medul lary vein
l!1llll"!ttffl The U ri n a ry System 321
Efferent arter iole
I nterlobular artery
I nterlobar artery
Vasa recta
FIGURE 1 8.8. B l ood c i r cu lat ion in the k idney. Arte r ies are shown in red and ve ins in b l u e . Adj a c e nt inte rl o b u l a r a rter ies, wh i c h extend outwa rd from the a r cuate a rte ry, d efi n e the bounda ries of a renal l o bu l e . (Repr inted with permiss ion from Junque i ra LC, Carneiro J . Ke l l ey RO. Basic Histology. 9th ed . Stamford, CT: Appleton & Lange; 1 998:375. )
B. Venous d ra inage of the kidney (Figure 18.8) 1. Stel l ate veins are formed by convergence of superfic ia l cortica l veins, which drain the
outermost layers of the cortex. 2. Deep cortical ve ins drain the deeper regions of the cortex. 3. I nterlobu lar ve ins
a . Interlobular veins receive both stellate and deep cortical veins. b. They join arcuate veins, which empty into i nterlobar veins . These then converge to form a
branch of the rena l ve in , which exits the kidney at the hilum.
A. Overview 1. The regulation of urine concentration results in the excretion of large amounts of dilute
(hypoton ic) urine when water intake is high (d iuresis) and of concentrated (hypertonic) urine when body water needs to be conserved (antid iuresis).
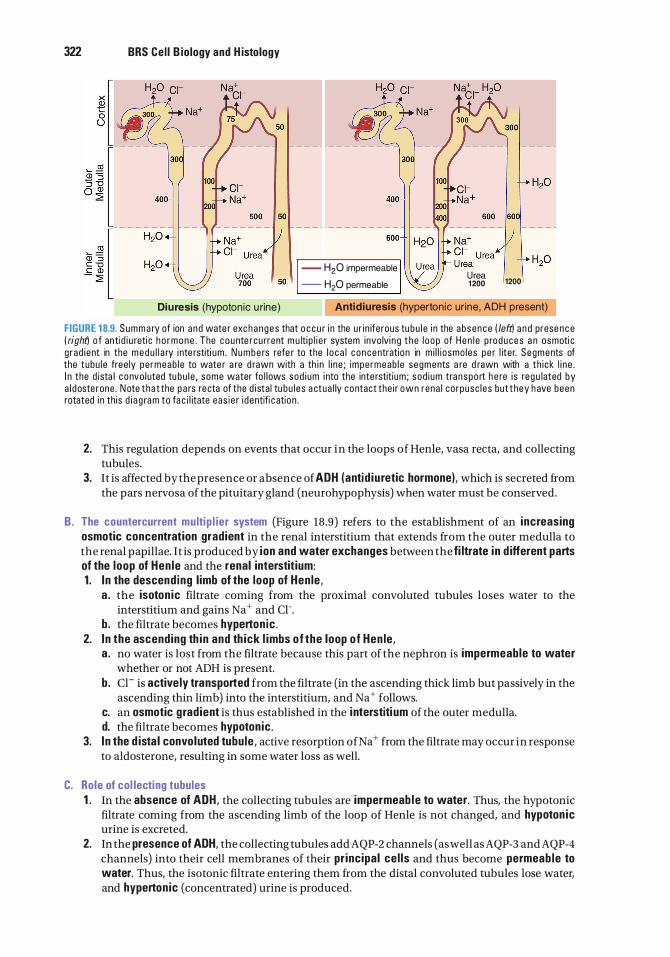
322 BRS Cel l B iology and H istology
- H20 impermeable
- H20 permeable U rea 1 200 1200
Diuresis (hypotonic u rine) Antidiuresis (hyperton ic ur ine, ADH present)
FIGURE 1 8.9. Summary of ion a nd wate r exchanges that o c c u r i n the u r i n iferous tu bu l e i n the absence ( left) a n d prese n c e ( right'l o f anti d i u reti c h o r m o n e . The c o u nte rcu rrent m u lti p l i e r system invo lvi n g t h e l oop of H e n l e p roduces a n osmoti c g rad i ent in the medu l l a ry i nte rstiti um . N u m b e rs refe r to the l o c a l c oncentration in m i l l i osmo les pe r l iter. Segments of the tubu le free ly pe rmeab l e to wate r a re d rawn with a th i n l i ne ; impe rmeab l e segments a re d rawn with a th i ck l i n e . I n the d ista l c o nvo luted tu bu l e , some water fo l l ows sod i um i nto the inte rstiti um ; sod i um transpo rt h e re i s reg u lated by a l doste rone . N ote t ha t the pa rs recta of the d i sta l tu bu l es a ctua l ly contact the i r own rena l co rpusc l es but t hey h ave been rotated i n th is d i a g ra m to fa c i l itate eas i e r i dentifi c atio n .
2. This regulation depends on events that occur in the loops of Henle, vasa recta, and collecting tubules.
3. It is affected by the presence or absence of ADH (antid iu retic hormone), which is secreted from the pars nervosa of the pituitary gland (neurohypophysis) when water must be conserved.
B . The countercurrent multi p l ier system (Figure 18.9) refers to the establishment of an increasing osmotic concentration gradient in the renal interstitium that extends from the outer medulla to the renal papillae. It is produced by ion and water exchanges between the fi ltrate in d ifferent parts of the loop of Hen le and the renal interstit ium: 1 . I n the descend ing l imb of the loop of Hen le,
a . the isoton ic filtrate coming from the proximal convoluted tubules loses water to the interstitium and gains Na+ and Cl-.
b. the filtrate becomes hyperton ic . 2. I n the ascending th in and th ick l imbs of the loop of Hen le,
a . no water is lost from the filtrate because this part of the nephron is impermeable to water whether or not ADH is present.
b. Cl- is active ly transported from the filtrate (in the ascending thick limb but passively in the ascending thin limb) into the interstitium, and Na + follows.
c. an osmotic gradient is thus established in the i nterstiti um of the outer medulla. d. the filtrate becomes hypotonic .
3. I n the d ista l convoluted tubule , active resorption ofNa + from the filtrate may occur in response to aldosterone, resulting in some water loss as well.
C. Role of col lecti ng tubules 1 . In the absence of ADH, the collecting tubules are impermeab le to water. Thus, the hypotonic
filtrate coming from the ascending limb of the loop of Henle is not changed, and hypoton ic urine is excreted.
2. In the presence of ADH, the collecting tubules add AQP-2 channels (as well as AQP-3 andAQP-4 channels) into their cell membranes of their pr incipal ce l ls and thus become permeab le to water. Thus, the isotonic filtrate entering them from the distal convoluted tubules lose water, and hypertonic (concentrated) urine is produced.
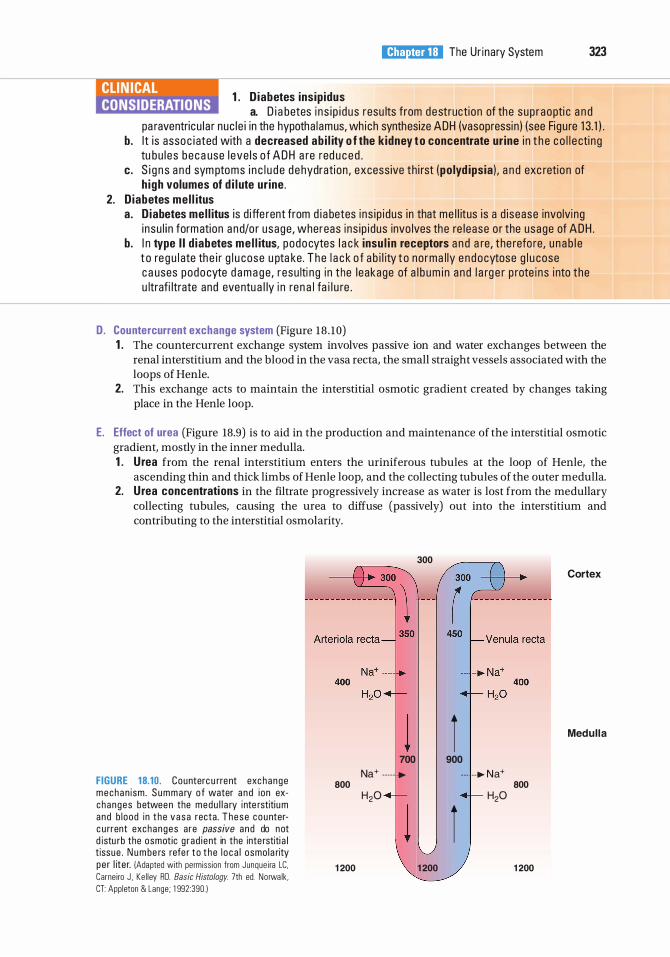
1 . D iabetes insip idus
l!1llll"!ttffl The Ur inary System 323
a. D i a betes i n s i p i d us resu lts from destructi on of the sup raopti c a n d pa raventricu l a r nuc le i in the hypotha l amus, wh ich synthesize ADH (vasopressin ) (see Figu re 1 3. 1 ) .
b. I t i s asso c i ated with a decreased ab i l ity o f the k idney t o concentrate ur ine i n t h e c o l l e cti ng tu bu l e s b eca use l eve l s o f ADH a re red u c e d .
c. S i g n s a n d sym ptoms i n c l u d e d e hydration , excess ive th i rst ( po lyd ipsia ) , a n d exc retio n of h igh volumes of d i l ute ur ine .
2. D iabetes me l l itus a . D iabetes mel l itus i s d i ffe rent from d i a betes i ns i p i dus in that me l l itus i s a d i sease involving
i nsu l i n formation and/o r usage, whereas i ns i p i dus invo lves the re l ease o r the usage of ADH . b. I n type I I d iabetes me l l itus, podocytes l a c k insu l i n receptors a n d a re, the refo re, u n a b l e
t o re g u l ate th e i r g l u cose u pta ke . T he l a c k o f a b i l ity t o no rma l ly e n docytose g l u cose c a uses podo cyte d a m a g e, resu lti ng i n the l eakage of a l b um i n and l a rg e r p rote i ns i nto the u ltrafi ltrate and eventu a l ly i n ren a l fa i l u re .
D. Countercurrent exchange system (Figure 18 . 10) 1 . The countercurrent exchange system involves passive ion and water exchanges between the
renal interstitium and the blood in the vasa recta, the small straight vessels associated with the loops of Henle.
2. This exchange acts to maintain the interstitial osmotic gradient created by changes taking place in the Henle loop.
E. Effect of urea (Figure 18.9) is to aid in the production and maintenance of the interstitial osmotic gradient, mostly in the inner medulla. 1 . Urea from the renal interstitium enters the uriniferous tubules at the loop of Henle, the
ascending thin and thick limbs of Henle loop, and the collecting tubules of the outer medulla. 2. Urea concentrations in the filtrate progressively increase as water is lost from the medullary
collecting tubules, causing the urea to diffuse (passively) out into the interstitium and contributing to the interstitial osmolarity.
FIGURE 1 8.10. Counterc u rrent exc hange mecha n ism . S u m m a ry o f water a n d i on exchanges betwee n the medu l l a ry inte rstiti u m and b l ood in t h e v a s a recta . T h e s e c o u nterc u rrent exchanges are passive and do not d istu rb the osmotic g r ad i ent in the inte rstiti a l t issue . N u m be rs refe r t o t h e l o c a l osmo la rity pe r l iter. )Adapted with permiss ion from Junque i ra LC. Carne iro J , Ke l ley RD. Basic Histology. 7th ed. No rwa lk , CT: Appleton & Lange; 1 992:390. )
800
1 200
Na+ .....
H20
300
1 700
...
1 200
Cortex
I Medul la
900
.. . ..... N a+ 800
H20
I 1 200
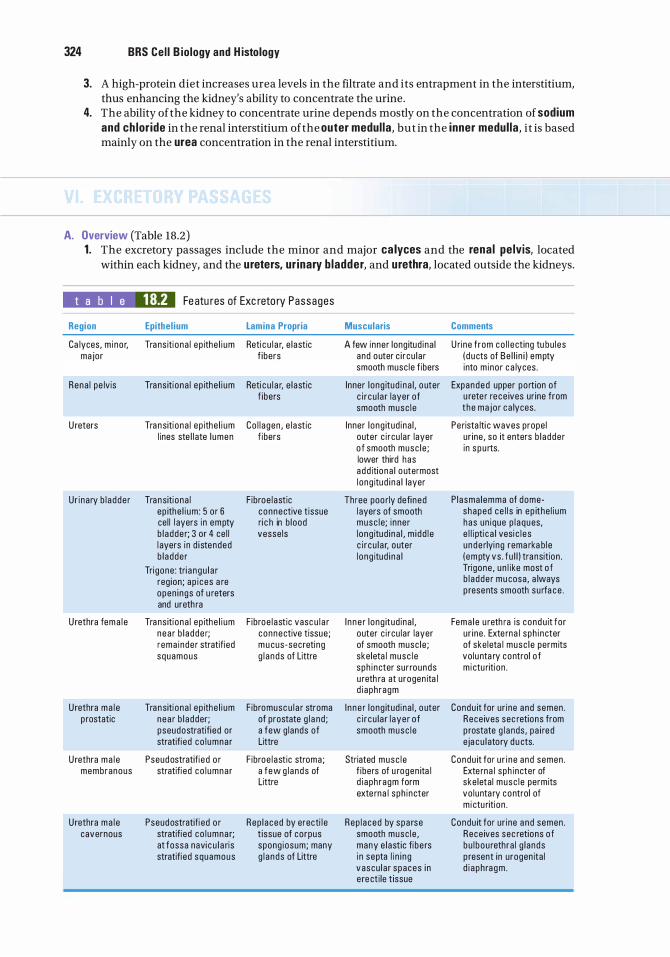
324 BRS Cel l B iology and H istology
3. A high-protein diet increases urea levels in the filtrate and its entrapment in the interstitium, thus enhancing the kidney's ability to concentrate the urine.
4. The ability of the kidney to concentrate urine depends mostly on the concentration of sodium and ch lor ide in the renal interstitium of the outer medul la , but in the inner medul la , it is based mainly on the urea concentration in the renal interstitium.
A. Overview (Table 18.2) 1 . The excretory passages include the minor and major ca lyces and the rena l pe lvis, located
within each kidney, and the ureters, ur inary b ladder, and urethra, located outside the kidneys.
t a b I e 18.2 Fe atu res of Exc reto ry Passages
Region Epithel ium Lamina Propria
Ca lyces, m i no r, Tra ns iti ona l ep ithe l i um Reti c u l a r, e l astic major f ibers
Rena l pe lvis Tra ns iti ona l ep ithe l i um Reti c u l a r, e l astic f ibers
U reters Tra nsiti ona l ep ithe l i um Co l l agen , e l a stic l ines ste l l ate l umen f ibers
Ur i na ry b l a dde r Tra nsiti ona l F ibroe l astic ep ithe l i um : 5 o r 6 connective t issue ce l l l ayers i n empty ri c h in b lood b l adde r; 3 or 4 ce l l vesse ls l ayers i n d i stended b l adde r
Tri gone : tri a ngu l a r reg ion ; ap i ces a re open i ngs of u reters and ureth ra
U rethra fema l e Tra ns iti ona l ep ithe l i um F ibroe l astic vasc u l a r n ea r b l a dde r; connective tissue ; r ema inde r stratifi ed m u cus-secreti ng squamous g l a nds of Littre
U rethra ma l e Tra nsiti ona l ep ithe l i um F ibromusc u l a r stroma p rostatic nea r b l adder; of prostate g l a nd ;
pseudostratifi ed or a few g lands of stratifi ed co l umna r Littre
U rethra ma l e Pseudostratifi e d o r F ibroe l astic stroma ; membranous stratifi ed co l umna r a f ew g l a nds of
Littre
U rethra ma l e Pseudostratifi ed o r Rep l aced by erecti l e cavernous stratifi ed co l umna r; t issue of corpus
at fossa navi c u l a ris spong iosum; many stratifi ed squamous g l a nds of Littre
Muscularis Comments
A few inner long itud ina l U ri ne f rom co l l e ct ing tu bu l es and outer c i r cu l a r ( d u cts of Be l l i n i ) empty smooth musc le f ibers into m ino r c a lyces .
Inner l ong itud i na l , o uter Expanded upper po rt ion of c i r cu l a r layer of u rete r re ce ives ur ine from smooth musc l e t he ma jo r c a lyces .
Inner l ong itud ina l , Pe rista lti c waves prope l outer c i rcu la r layer ur ine , so it enters b l adde r o f smooth musc l e ; in s p u rts. lower third has a dd iti ona l o utermost l ong itud i n a l layer
Three poo rly defi ned P l asma lemma of dome-l ayers of smooth shaped ce l l s in ep ithe l i um musc l e; i nner has un ique p l a ques, l on g itud i na l , m i dd l e e l l i pti c a l vesi c l e s c i r cu l a r, outer unde rlyi ng rema rka b le l ong itud i n a l ( em pty vs . f u l l ) tra nsition .
Tri gone , u n l ike most o f b l a dde r mu cosa , a lways p resents smooth su rfa ce .
I n n e r l ong itud ina l , Fema l e u reth ra is cond u it for outer c i rcu la r layer u r i ne . Exte rna l sph i ncter of smooth musc le ; of ske leta l musc l e permits ske leta l musc l e vo lu nta ry control o f sph i ncter sur rounds m i ctu riti on . u reth ra at u rogen ita l d i aph ragm
I n ne r l ong itud ina l , o uter Condu it for ur ine and semen . c i r cu l a r l aye r o f Rece ives sec retions from smooth musc l e p rostate g l a nds , pa i red
eja cu l ato ry d u cts.
Striated musc l e Condu it for u r i n e and semen . f ibers of u rogen ita l Exte rna l sph i ncter of d i aph ragm form ske leta l musc l e permits exte rna l sph i ncter vo lunta ry control of
m i ctu riti on .
Rep l a ced by spa rse Condu it for ur ine a nd semen . smooth musc l e , Rece ives sec retions o f many e l ast ic fi be rs bu l bou rethra l g l ands i n septa l i n i n g p resent in urogen ita l vascu l a r spaces i n d i a ph ra gm . e re cti le t issue
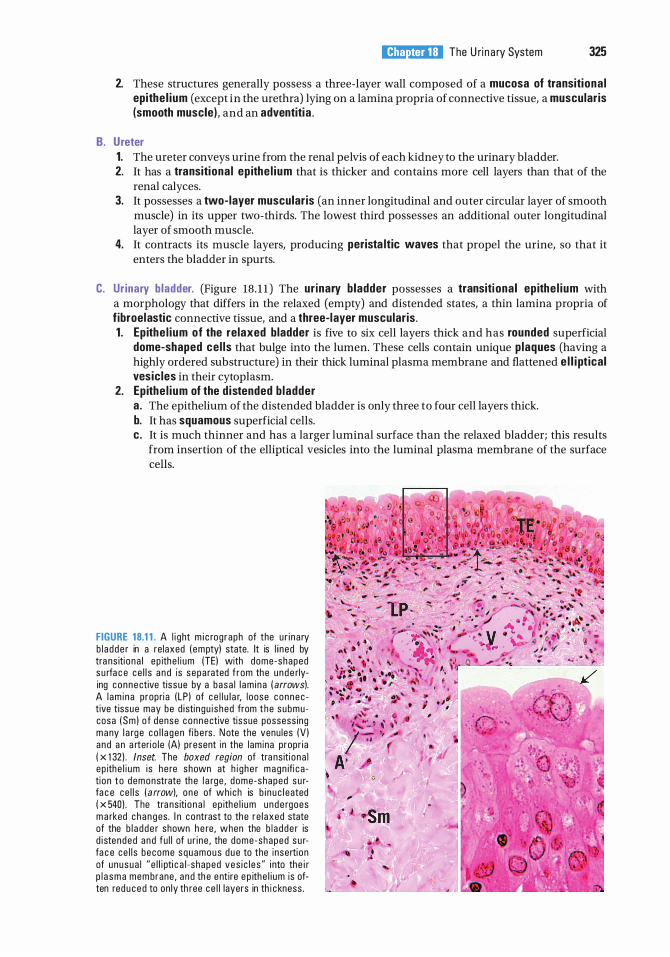
l!1llll"!ttffl The U ri n a ry System 325
2. These structures generally possess a three-layer wall composed of a mucosa of transitiona l epithe l ium (except in the urethra) lying on a lamina propria of connective tissue, a muscularis (smooth muscle) , and an adventitia .
B. Ureter 1. The ureter conveys urine from the renal pelvis of each kidney to the urinary bladder. 2. It has a transitiona l ep ithe l ium that is thicker and contains more cell layers than that of the
renal calyces. 3. It possesses a two-layer muscularis (an inner longitudinal and outer circular layer of smooth
muscle) in its upper two-thirds. The lowest third possesses an additional outer longitudinal layer of smooth muscle.
4. It contracts its muscle layers, producing perista ltic waves that propel the urine, so that it enters the bladder in spurts.
C. Ur inary bladder. (Figure 18. 1 1 ) The ur inary b ladder possesses a transiti onal ep ithe l ium with a morphology that differs in the relaxed (empty) and distended states, a thin lamina propria of f ibroelastic connective tissue, and a three-layer muscular is . 1 . Ep ithe l ium of the relaxed bladder is five to six cell layers thick and has rounded superficial
dome-shaped ce l ls that bulge into the lumen. These cells contain unique plaques (having a highly ordered substructure) in their thick luminal plasma membrane and flattened e l l i pt ical vesic les in their cytoplasm.
2. Epithe l ium of the d istended b ladder a . The epithelium of the distended bladder is only three to four cell layers thick. b. It has squamous superficial cells. c. It is much thinner and has a larger luminal surface than the relaxed bladder; this results
from insertion of the elliptical vesicles into the luminal plasma membrane of the surface cells.
FIGURE 18.1 1 . A l i ght m i c rog raph of the u r i na ry b l a dde r in a re laxed ( empty) state. It is l i ned by tra ns iti o na l ep ithe l i um (TEl with dome-shaped s u rfa c e ce l l s a n d is sepa rated f rom the u nde rlying connective tissue by a basa l l am i n a ( arrows). A l am i na p ropri a ( LP l of c e l l u l a r, l oose connec tive t issue may be d i sti ngu i shed from t he submu cosa (Sm l o f dense connective tissue possess ing many l a rg e co l l a gen fi b e rs . N ote the venu les (V l a nd a n a rteri o l e (Al present i n the lamina propr ia ( x 1 321 . Inset. The boxed region of tra ns iti o na l ep ithe l i um is h e re shown at h i g he r magn ifi c a tion to demonstrate the l a rge , dome-shaped s u rfa c e ce l l s ( a rrow). one of wh ich is b i n u c l eated ( x 5401 . The tra ns iti o n a l ep ithe l i um u n d e rgoes m a rked c h a n g es . I n contrast to the re l axed state of the b l a dde r shown h e re , when the b l a dde r is d i stended and fu l l of u r i ne , the dome-shaped s u rfa c e ce l l s become squamous d u e to the i nserti on of unusua l " e l l i pti c a l - shaped ves i c l e s " i nto the i r p l a s m a mem brane , a nd th e e ntire e p ithe l i um is often red u c e d to on ly th ree ce l l layers in th i c kness .
326 BRS Cel l B iology and H istology
CLIN ICAL CONSIDERATIONS
B ladder cancer i s two to t h ree times mo re common i n men th a n i n wom e n . M o re th a n 90% o f b l a d de r c a n c e rs or ig i n ate in the tra ns iti o n a l e p ith e l i um
l i n i n g t he o rg a n . The most common s i gn o f b l a d de r c ance r is b l ood i n t he u r i ne ( hematuria) , wh i c h m a y not be v is i b l e t o t h e n a ked eye. Fre q uent u ri n atio n a n d/o r p a i n d u ri n g u ri n ati on a re sometimes p rese nt, b ut ofte n the d isease i s sym ptom l ess . Cystoscopy i s used to exam i n e the l i n i n g o f the b l ad d e r, to ta ke t issu e samp l es i n o rd e r to c h a ra cte r ize the tumo r, a nd to d ete rm i ne the extent to wh i ch it h as penetrated i nto the b l a d de r wa l l . S u p e rfi c i a l b l a d d e r c a n c e r ( l im ited to th e e p ith e l i a l layer ) h as a 5-ye a r s u rviva l rate of a bout 85%, b ut invas ive b l a d de r c a n c e r has a l ess favo ra b l e p rognos is .
D. Urethra 1 . Overview
a. The urethra conveys urine from the bladder to outside the body. In men, the urethra also carries semen during ejaculation.
b. It has a two- layer muscularis consisting of an inner longitudinal and an outer circular layer of smooth muscle.
c. It is surrounded at some point by an external sphincter of skeleta l muscle, which permits its voluntary closure.
2. Male urethra a . The male urethra is about 20 em long and is divided into prostatic, membranous, and
cavernous portions. b. It is lined by transitiona l ep ithe l ium in the prostatic portion and by pseudostratified or
stratified columnar ep ithe l ium in the other two portions. The fossa navicu laris, located at the distal end of the cavernous urethra, is lined by stratified squamous ep ithe l ium.
c. I t contains mucus-secreting g lands of Litlre in the lamina propria. 3. Female urethra
a . The female urethra is much shorter ( 4-5 em long) than the male urethra. b. It is lined primarily by stratified squamous epithe l ium, although patches ofpseudostratified
columnar epithelium are present. c. It may contain g lands of Litlre in the lamina propria.
Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1 . Which of the following statements concerning the structure of medullary rays is true?
(A) They contain arched collecting tubules. (B) They contain proximal convoluted
tubules. (C) They do not extend into the renal cortex. (D ) They lie at the center of a renal lobule. (E) They contain thin limbs of the loops of
Henle.
2. Which one of the following structures is located in the renal cortex?
(A) Vasa recta (B ) Thin limbs of the loops of Henle (C ) Afferent arterioles (D ) Interlobar veins (E ) Area cribrosa
3. Which of the following structures is present in the male urethra but is not present in the female urethra?
(A) Stratified squamous epithelium (B ) Transitional epithelium (C ) Glands of Littre (D ) External sphincter of skeletal muscle (E) Connective tissue layer underlying
the epithelium
4. Which of the following statements concerning cortical collecting tubules is always true?
(A) They are lined by a simple epithelium containing two types of cells.
(B ) They are also known as the ducts of Bellini.
(C ) They empty on the area crib rosa. (D ) They are permeable to water. (E ) They are continuous with the ascending
thick limb of the Henle loop.
5. A 35-year-old woman had surgery to remove a cerebral tumor. A month after the procedure, she reports being excessively thirsty and drinking several liters of water per day. She must also urinate so frequently that she avoids leaving the house. Laboratory tests indicate that her urine has very low specific gravity. What is the most likely diagnosis of this woman's condition?
(A) Acute renal failure (B ) Glomerulonephritis (C) Chronic renal failure (D ) Diabetes insipidus (E) Urinary incontinence
6. The countercurrent multiplier system in the kidney involves the exchange of water and ions between the renal interstitium and
(A) the blood in the vasa recta. (B ) the blood in the peritubular capillary
network. (C) the filtrate in the proximal convoluted
tubule. (D) the filtrate in the loop of Henle. (E) the filtrate in the medullary collecting
tubule.
7. As the glomerular filtrate passes through the uriniferous tubule, ions and water are exchanged (actively or passively) with the renal interstitium, resulting in the filtrate being isotonic, hypotonic, or hypertonic relative to blood plasma. During a condition of antidiuresis, which part of the uriniferous tubule would contain a hypertonic filtrate?
(A) Ascending thick limb of the loop of Henle (B ) Bowman (capsular) space (C) Cortical collecting tubule (D ) Medullary collecting tubule (E) Proximal convoluted tubule
327
328 BRS Cel l B iology and H istology
8. As the glomerular filtrate passes through the uriniferous tubule, ions and water are exchanged (actively or passively) with the renal interstitium, resulting in the filtrate being isotonic, hypotonic, or hypertonic relative to blood plasma. During a condition of antidiuresis, which part of the uriniferous tubule would contain an isotonic filtrate?
(A) Ascending thick limb of the loop of Henle (B ) Bottom of descending thin limb of loop
of Henle (C) Bowman (capsular) space (D ) Medullary collecting tubule (E ) Papillary collecting tubule
9. As the glomerular filtrate passes through the uriniferous tubule, ions and water are exchanged (actively or passively) with the renal interstitium, resulting in the filtrate being isotonic, hypotonic, or hypertonic relative to blood plasma. During a condition of antidiuresis, which one of the following parts of the uriniferous tubule would contain a hypotonic filtrate?
(A) Bowman (capsular) space (B ) Cortical collecting tubule (C) Distal portion of the ascending thick limb
of the loop of Henle (D ) Medullary collecting tubule (E ) Proximal convoluted tubule
1 0. As the glomerular filtrate passes through the uriniferous tubule, ions and water are exchanged (actively or passively) with the renal interstitium, resulting in the filtrate being isotonic, hypotonic, or hypertonic relative to blood plasma. During a condition of antidiuresis, which part of the uriniferous tubule would contain a hypertonic filtrate?
(A) Bottom of descending thin limb of loop of Henle
(B ) Bowman (capsular) space (C) Distal portion of the ascending thick limb
of the loop of Henle (D ) Pars recta of the proximal tubule (E ) Proximal convoluted tubule
Answers and Explanations
1 . D. A medullary ray contains the straight portions of tubules projecting from the medulla into the cortex, giving the appearance of striations or rays. A renal lobule consists of a central medullary ray and its closely associated cortical tissue (see Chapter 18 II E) .
2. C. Afferent arterioles, which arise from interlobular arteries and supply the glomerular capillaries, are located in the renal cortex (see Chapter 18 III A 5) .
3. B . Only the male urethra contains transitional epithelium (in the prostatic portion) . Stratified squamous epithelium lines most of the female urethra and the distal end of the cavernous urethra in men. Mucus-secreting glands of Littre are always present in the male urethra and may be present in the female urethra (see Chapter 18 VI D) .
4. A. Cortical collecting tubules are lined by a simple epithelium containing principal (light) cells and intercalated (dark) cells. They are permeable to water only in the presence of ADH; in the absence of this hormone, they are impermeable to water. The large papillary collecting tubules, called ducts of Bellini, empty on the area cribrosa at the apex of each renal papilla (see Chapter 18 III B) .
5. D . This woman has diabetes insipidus. Surgical removal of the cerebral tumor likely damaged her hypothalamus, which in turn greatly reduced or eliminated the production of ADH. Therefore, her kidney collecting tubules and distal tubules fail to resorb water, resulting in the production of vast quantities of dilute urine and causing excessive thirst (see Chapter 18 V C Clinical Considerations) .
6. D. The countercurrent multiplier system in the loop of Henle involves ion and water exchanges between the filtrate and the interstitium. It establishes an osmotic gradient in the interstitium of the medulla, which is greatest at the papilla (see Chapter 18 V B) .
7. D . The filtrate that enters the cortical collecting tubules is nearly isotonic. When antidiuretic hormone is present (antidiuresis), water is removed from the filtrate in the collecting tubules, making the filtrate hypertonic by the time it reaches the medullary collecting tubules (see Chapter 18 V C) .
8. C. Filtration of blood in the renal corpuscle yields an isotonic ultrafiltrate that enters the Bowman (capsular) space (see Chapter 18 V B) .
9 . C. The ascending thick limb of the loop of Henle is impermeable to water even in the presence of ADH, but it actively transports cr from the filtrate into the interstitium (Na + follows passively). As a result, the filtrate becomes hypotonic as it approaches the distal convoluted tubule (see Chapter 18 V B) .
10 . A . The filtrate remains isotonic from the Bowman space throughout the proximal tubule, including the pars recta (also called the thick descending limb of the loop of Henle). As it passes through the descending thin limb of the loop of Henle, the filtrate loses water to the interstitium and gains Na+ and cr, becoming hypertonic (see Chapter 18 V B) .
329
Female Reproductive System
A. The female reproductive system consists of the paired ovaries and oviducts; the uterus, vag ina, and external genita l ia ; and the paired mammary g lands, although technically, the mammary glands are part of the integument since they are highly modified sweat glands.
B. The female reproductive system undergoes marked changes at the onset of puberty, which is initiated by menarche.
C. It exhibits monthly menstrual cycles and menses from puberty until the end of the reproductive years, which terminate at menopause.
A. Overview and embryonic development
330
1 . Overview a. Ovaries are covered by a simple cuboidal epithelium called the germina l ep ithe l ium. b . Deep to the germinal epithelium, the ovaries possess a capsule, the tun ica a lbug inea that i s
composed of a dense, irregular collagenous connective tissue. c. Each ovary is subdivided into a cortex and a medul la, which are not sharply delineated.
2. Development a. Embryonic development of the gonads is a function of the SRY gene (sex-determin ing
reg ion on the Y chromosome). I f the Y chromosome is present, the SRY gene is expressed producing the SRY prote in, which is the testis-determ in ing factor, resulting in the formation of testes. In the absence of the Y chromosome, ovaries will be developed.
b. During the sixth week of embryogenesis, primitive germ cells leave the yo lk sac to enter the gonadal ridges. Once there, they undergo cell division and increase their number. The gonadal ridges still do not have distinguishing male or female characteristics and, therefore, they are referred to as i nd ifferent gonads.
c . Approximately 6 weeks later (fourth month of development), cells, perhaps supplemented by cells of the germinal epithelium, migrate to the primitive germ cells, surrounding each germ cell, now referred to as an oogonium, to form a single layer of cells known as fo l l icu lar ce l ls around each oogonium. Only about 500,000 oogonia will be surrounded by follicular cells; oogonia that have no follicular cell sheath undergo apoptosis.
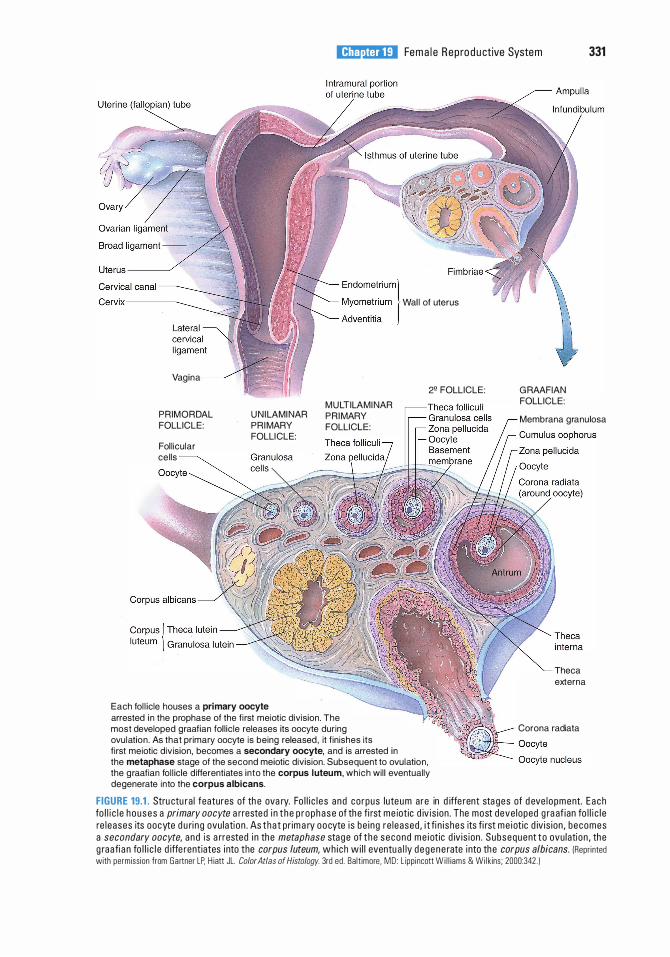
l!il!ll'tttD]j Fema l e Rep ro d u ctive System 331
Vagina
PRIMORDAL FOLLICLE:
Fol l icular cel ls
U N I LAMI NAR PRI MARY FOLLI CLE:
Each fol l icle houses a primary oocyte
M U LTILAMI NAR PRI MARY FOLLICLE:
arrested i n the prophase of the fi rst meiotic division. The most developed graafian fol l ic le releases its oocyte during ovulation . As that primary oocyte is being released , it f in ishes its f i rst meiotic division, becomes a secondary oocyte, and is arrested in
Wal l of uterus
2• FOLLICLE:
the metaphase stage of the second meiotic division. Subsequent to ovulation , the g raafian fol l icle differentiates into the corpus l uteum, which wi l l eventually degenerate into the corpus albicans.
G RAAFIAN FOLLICLE:
Membrana granulosa
Theca externa
Corona radiata
FIGURE 19.1 . Stru ctu ra l features of th e ova ry. Fo l l i c l e s a nd co rpus luteum are in d iffe rent sta ges of d eve l opment. E a ch fo l l i c l e h ouses a primary oocyte a rrested i n t he p r ophase of the fi rst me iotic d iv is ion . The most deve loped g ra af ian fo l l i c l e re l eases its oocyte d u ri n g ovu lati on . As tha t pr im a ry oocyte i s be i ng re l eased , i t fi n i shes its fi rst me i ot ic d iv is ion , becomes a secondary oocyte, and i s a rrested i n the metaphase stag e of t he second me i ot ic d iv is ion . Subsequent to ovu lation , the g raafi a n fo l l i c l e d iffe rentiates i nto the corpus /uteum, which wi l l eventu a l ly d egene rate into the corpus albicans. IRepr i nted with permiss ion from Ga rtner LP, H iatt JL. Color Atlas of Histology. 3rd ed . Ba lt imore, MD : L ipp i ncott W i l l iams & Wil k ins; 2000:342 . )
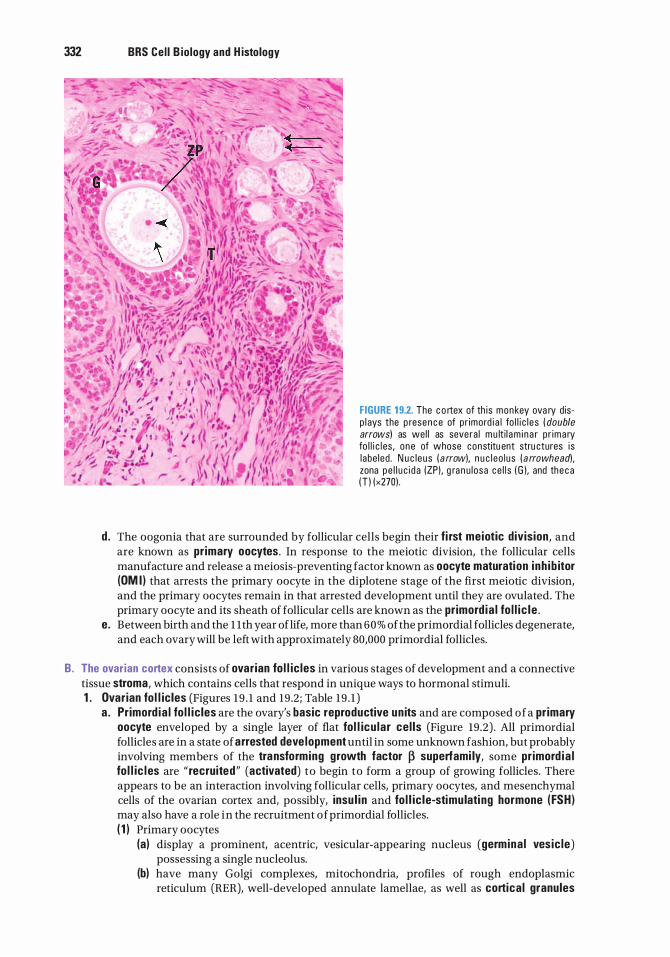
332 BRS Cel l B iology and H istology
FIGURE 1 9.2. The c o rtex of th is mon key ova ry d isp l ays the p rese n c e of p r imord i a l fo l l i c l es ( double arrows) as wel l as seve ra l m u lt i l a m i n a r p r ima ry fo l l i c l es , o ne of whose constitu ent stru ctures i s l abe led . N u c leus ( a rrow). n u c l eo l us ( a rrowhead), zona pe l l u c i d a (ZP) . g ra n u losa ce l l s ( G ). and the c a ( T ) (x270) .
d . The oogonia that are surrounded by follicular cells begin their fi rst meiotic division, and are known as primary oocy1es. In response to the meiotic division, the follicular cells manufacture and release a meiosis-preventing factor known as oocy1e maturation inh ib itor (OM I ) that arrests the primary oocyte in the diplotene stage of the first meiotic division, and the primary oocytes remain in that arrested development until they are ovulated. The primary oocyte and its sheath of follicular cells are known as the primord ia l fo l l i c le .
e . Between birth and the 1 1th year oflife, more than 60% of the primordial follicles degenerate, and each ovary will be left with approximately 80,000 primordial follicles.
B. The ovarian cortex consists of ovarian fo l l ic les in various stages of development and a connective tissue stroma, which contains cells that respond in unique ways to hormonal stimuli. 1 . Ovarian fo l l ic les (Figures 19 . 1 and 19 .2; Table 19 . 1 )
a . Primord ia l fo l l ic les are the ovary's basic reproductive un its and are composed of a primary oocy1e enveloped by a single layer of flat fol l icu lar ce l ls (Figure 19 .2) . All primordial follicles are in a state of arrested deve lopment until in some unknown fashion, but probably involving members of the transforming growth factor � superfami ly, some primord ia l fo l l ic l es are " recruited" (activated) to begin to form a group of growing follicles. There appears to be an interaction involving follicular cells, primary oocytes, and mesenchymal cells of the ovarian cortex and, possibly, insu l in and fo l l ic le-stimulati ng hormone ( FSH) may also have a role in the recruitment of primordial follicles. ( 1 ) Primary oocytes
(a) display a prominent, acentric, vesicular-appearing nucleus (germina l ves ic le) possessing a single nucleolus.
(b) have many Golgi complexes, mitochondria, profiles of rough endoplasmic reticulum (RER), well-developed annulate lamellae, as well as cortical granules
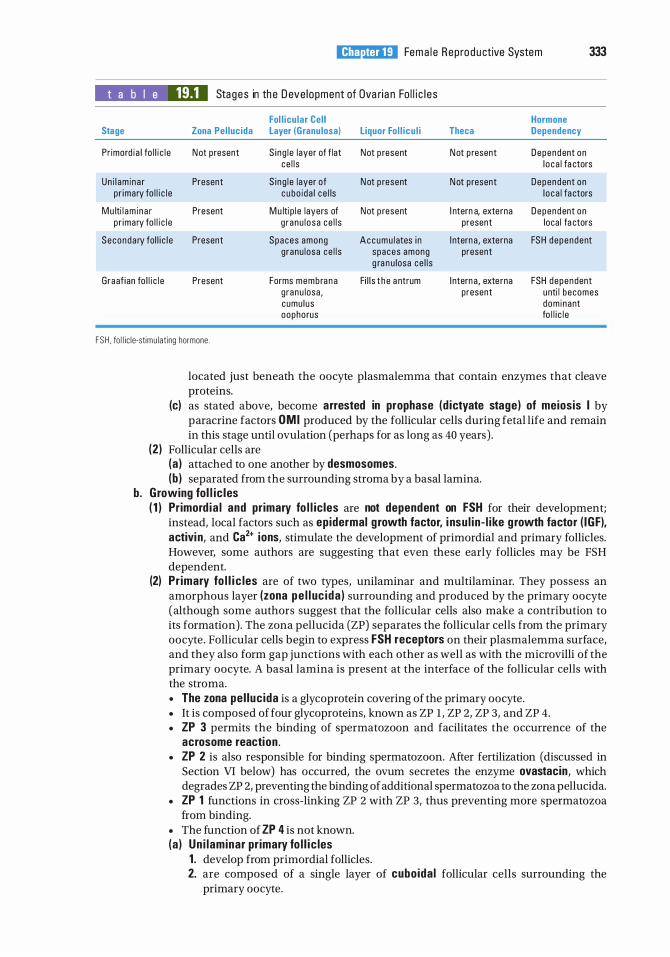
l!il!ll'tttD]j Fema l e Rep ro d u ctive System 333
t a b I e 19.1 Stages in th e D eve lopment of Ova ri a n Fo l l i c l e s
Fol l icu lar Cel l Hormone Stage Zona Pel lucida Layer (Granu losa) Liquor Fol l icu l i Theca Dependency
Pr imord i a l fo l l i c l e N ot p resent S i ng l e layer of f lat Not p resent N ot p resent Dependent on ce l l s l o ca l fa ctors
Un i l am i na r Present S i ng l e layer of N ot p resent N ot p resent Dependent on p r imary fo l l i c l e c u bo i da l c e l ls l o ca l fa ctors
Mu lti l am i na r Present M u lti p l e layers of Not p resent I ntern a, externa Dependent on p r imary fo l l i c l e g r anu l osa ce l l s present loca l fa ctors
Seconda ry fol l i c l e Present Spaces among Accumu l ates i n I ntern a , externa FSH dependent g ranu losa ce l l s spaces among present
g ra n u losa ce l l s
Graaf ian fo l l i c l e Present Forms membra n a Fi l l s t h e a ntrum I ntern a , exte rna FSH dependent g ranu losa , present unti l becomes cumu lus dom inant oophorus fo l l i c l e
FSH . fo l l ic le-stimu lat ing hormone.
located just beneath the oocyte plasmalemma that contain enzymes that cleave proteins.
(c) as stated above, become arrested in prophase (d ictyate stage) of meiosis I by paracrine factors OMI produced by the follicular cells during fetal life and remain in this stage until ovulation (perhaps for as long as 40 years) .
(2) Follicular cells are (a ) attached to one another by desmosomes. (b ) separated from the surrounding stroma by a basal lamina.
b. Growing fol l ic les ( 1 ) Primord ia l and primary fo l l ic les are not dependent on FSH for their development;
instead, local factors such as epidermal g rowth factor, i nsu l in - l ike g rowth factor ( IGF), activi n, and Ca2+ ions, stimulate the development of primordial and primary follicles. However, some authors are suggesting that even these early follicles may be FSH dependent.
(2) Pr imary fo l l i c les are of two types, unilaminar and multilaminar. They possess an amorphous layer (zona pe l l uc ida ) surrounding and produced by the primary oocyte (although some authors suggest that the follicular cells also make a contribution to its formation). The zona pellucida (ZP) separates the follicular cells from the primary oocyte. Follicular cells begin to express FSH receptors on their plasmalemma surface, and they also form gap junctions with each other as well as with the microvilli of the primary oocyte. A basal lamina is present at the interface of the follicular cells with the stroma. • The zona pe l luc ida is a glycoprotein covering of the primary oocyte. • It is composed of four glycoproteins, known as ZP 1 , ZP 2, ZP 3, and ZP 4. • ZP 3 permits the binding of spermatozoon and facilitates the occurrence of the
acrosome reaction . • ZP 2 is also responsible for binding spermatozoon. After fertilization (discussed in
Section VI below) has occurred, the ovum secretes the enzyme ovastacin, which degrades ZP 2, preventing the binding of additional spermatozoa to the zona pellucida.
• ZP 1 functions in cross-linking ZP 2 with ZP 3, thus preventing more spermatozoa from binding.
• The function of ZP 4 is not known. (a ) Un i laminar pr imary fo l l i c les
1 . develop from primordial follicles. 2. are composed of a single layer of cuboida l follicular cells surrounding the
primary oocyte.
334 BRS Cel l B iology and H istology
(b) Multilaminar primary follicles (Figure 19 .2) 1. develop from unilaminar follicles by proliferation of follicular cells. 2. proliferate because of the protein activin, a product of the primary oocyte.
Activin also promotes the release of FSH and its binding to FSH receptors. Additionally, the primary oocyte releases the growth factors bone morphogen ic prote in 1 5 (BMP-1 5) and growth d ifferentiation factor 9 (GDF-9), both of which induce granulosa cell proliferation.
3. consist of several layers of follicular cells; these follicular cells are now also known as granu losa cel ls.
4. are circumscribed by two layers of stromal cells: an inner cellular layer (theca interna) and an outer fibro-muscular layer (theca externa) . The theca interna is separated from the granulosa cells by a basal lamina.
5. Granulosa cells secrete stem ce l l factor (kit- l igand) that binds to kit ligand receptors on the surface of the pr imary oocyte plasmalemma as well as to kit ligand receptors on the surface of the theca i nterna ce l l membranes. The binding to pr imary oocyte kit ligand receptors is responsible for growth of the primary oocyte, and binding to kit ligand receptors on the theca interna cel ls facilitates their organization around the developing follicles.
6. Cells of the theca interna manufacture androstenedione (male sex hormone) and express l ute in iz ing hormone (LH) receptors on their cell membranes.
7. Androstenedione penetrates the basal lamina and enters the granulosa cells, where the enzyme aromatase converts the male hormone into estrad io l , the female hormone.
CLIN ICAL CONSIDERATIONS
M utati ons t ha t affect th e no rma l connexin synth es is res u lt i n th e a bsence o f g ra afi a n fo l l i c l e fo rmati o n as we l l as t h e i n a b i l ity o f th e oo cyte to
u n d e rgo me i oti c d iv is ion , with conse q u e nti a l fem a l e inferti l ity. The most p ro b ab l e c a use of th e d efe cts is the i n a b i l ity to exc h a n g e var ious n e c essa ry fa ctors between fo l l i c u l a r c e l l s a n d the p ri m a ry oo cyte v ia the fa u lty g a p j u n cti ons .
(3 ) Secondary (antra l ) fo l l ic les (a ) Secondary fo l l ic les are established when l i quor fo l l i cu l i , an exudate of plasma
containing various hormones, such as activin, estradiol, follistatin, inhibin, and progesterone, and oocyte maturation iunhibitor (OMI), begins to accumulate in the spaces between granulosa cells. It is the OMI, synthesized by the granulosa cells, that prevents the oocyte from becoming larger than 125 J.lm in diameter and from completing its first meiotic division. The fluid-filled spaces will begin to coalesce, eventually to form a single large cavity called an antrum.
(b ) Secondary follicles are dependent on FSH . (c) A s stated above, narrow processes extend from the granulosa cells into the zona
pellucida. (d) Granulosa cells contact each other via gap junctions and also form gap junctions
with the cell membrane of the primary oocyte. (e) Just as in the normal development of the primary follicle, the conversion from
primary to secondary follicles is greatly dependent on BMP-1 5 and GDF-9. (f) Both granulosa cells and theca interna cells express LH receptors on their plasma
membranes; additionally, granulosa cells also express FSH receptors on their cell membranes.
c. G raafian (mature) fo l l ic le (1 ) The dominant graafian follicle is the one follicle among the secondary follicles that wil l
ovu l ate. I t is FSH independent and manufactures the hormone i nh ib in that shuts off FSH release by the basophils of the anterior pituitary gland, causing atresia of the other developing follicles (secondary and nondominant graafian follicles) .
l!il!ll'tttD]j Fema le Reproductive System 335
(2) It measures approximately 2 .5 em in diameter and is evident as a large bulge on the surface of the ovary.
(3) The primary oocyte is positioned off center on a small mound of granulosa cells (cumulus oophorus) that projects into the hyaluronic acid-rich l iquor fo l l icu l i containing antrum of the follicle. Granulosa cells surround the zona pellucida. Those contacting the zona pellucida are known as the corona rad iata . Other granulosa cells line the antrum, forming the membrana granulosa.
(4) Theca interna cells, in response to luteinizing hormone (LH) binding to their LH receptors, manufacture androstenedione (androgen), which is transferred to granulosa cells. The granulosa cells, under the influence of FSH binding to their FSH receptors, transform androstenedione into testosterone and, by the use of the enzyme aromatase, convert the testosterone into estrad io l (estrogen) .
(5 ) The theca externa is composed of collagenous connective tissue enriched with a plethora of smooth muscle cells. It is also richly supplied with many blood vessels, which provide nourishment to the theca interna.
(6) Ovulation (a ) An LH surge from the pituitary gland, along with the local factor manufactured by
the primary oocyte, maturation promoting factor (a complex of cyc l in-dependent k inase and cyc l i n B ), triggers the primary oocyte to complete its first meiotic division just prior to ovu lation, forming a secondary oocyte and the fi rst po lar body. The second meiotic division is triggered by the presence of local meiosis-inducing factors but is blocked at metaphase.
(b) Ovulation also occurs in response to the LH surge. The secondary oocyte and its corona rad iata cells leave the ruptured follicle at the ovarian surface to enter the fimbriated end of the oviduct.
(c ) The remnant of the graafian follicle becomes the corpus hemorrhagicum that is transformed into the corpus l uteum of menstruation, a temporary structure that may remain functional for a couple of weeks and then degenerates into the corpus a l b icans. If the woman is pregnant, then the corpus hemorrhagicum becomes transformed into the corpus l uteum of pregnancy, which remains functional for several months, and then it also degenerates into the corpus a l b icans.
(7) Time Period of Fo l l icu logenesis . Although from the prior description offolliculogenesis it appears as if the entire process occurs within a single menstrual cycle, that is not the case. In fact, once a primordial follicle is recruited for development, almost a year is required before ovulation can occur, and it takes approximately 290 days to go from primordial to a completely developed secondary follicle and another 60 days or so for that follicle to become ovulated.
CLIN ICAL CONSIDERATIONS
Some wom e n expe ri e n c e a s u dden abdom i na l ( o r p e lvi c ) p a i n i n t he m i d d l e o f th e i r menstru a l cyc l e t ha t l asts 2 o r 3 h o u rs ( a lth o ugh i t may
l a st a s l o ng as 48-72 hou rs o r even l o n ge r), a n d they have attr ib uted that to the p ro cess of ovu l a ti o n . Alth ough th is attr i buti on was not u n iversa l ly a c c e pted, i t is now kn own tha t the s udden surge of LH i s fo l l owed by a s im i l a r su rge i n prostag land in F2a, a pha rmaco l o g i c a g ent that c a uses s udden , c r amp - l i ke c o ntra cti on of th e ova r ian , fa l l o p i a n tu be , o r ute r i ne smooth musc l e fi b e rs . It is th is v io l e nt contra cti on that is respons i b l e fo r the p a i n expe ri e n ced by some women . Oth e r c a uses, s u c h a s pa infu l d i stens ion o f the ova r i an fo l l i c l e s o r t he rupture o f t he tu n i c a a l b u g i n ea of th e ova ry, may a l so contr ib ute to the ovu l ati on pa i n .
2 . The corpus hemorrhagicum i s formed from the remnants of the graafian follicle. After the cumulus oophorus leaves the ovary, a little blood enters and forms a clot in the former antrum, and within a short period of time macrophages and connective tissue elements enter the region, and the macrophages dispose of the blood clot and other cellular debris. Once the macro phages have performed their function, the corpus hemorrhagicum, under the influence of various hormones, is converted into the corpus luteum. The hormones responsible for this
336 BRS Cel l B iology and H istology
transformation are: estrogens, prolactin, LH, human chorionic gonadotrophin (hCG), and insulin-like growth factors I and II (IGF-I and IGF-11) .
3. Corpus l uteum a. Overview
(1 1 The corpus luteum is formed from the corpus hemorrhagicum. As the corpus hemorrhagicum collapses upon itself, its cellular components become greatly modified.
(21 The corpus luteum is composed of granu losa lutein cel ls (modified granulosa cells) and theca lutein ce l ls (modified theca interna cells) .
(31 The basement membrane between the theca interna and the former membrana granulosa disintegrates, and blood and lymph vessels arising from the theca interna invade the former membrana granulosa.
(41 The formation of this richly vascularized temporary endocrine gland is dependent on LH. b. Granulosa l ute in cel ls
(1 I Granulosa lutein cells are large (30 11m in diameter), pale cells that possess an abundance of smooth endoplasmic reticulum (SER), RER, many mitochondria, a welldeveloped Golgi complex, and lipid droplets.
(21 They are derived from cells of the membrana granulosa. (31 Function. Granulosa lutein cells manufacture progesterone and convert androgens
formed by the theca lutein cells into estrogens. c . Theca l ute in cel ls
(1 I These small (15 11m in diameter) cells are concentrated mainly along the periphery of the corpus luteum.
(21 They are derived from cells of the theca interna. (31 Function. Theca lutein cells manufacture progesterone and androgens and small
amounts of estrogen. 4. The corpus a lb icans is the remnant of the degenerated corpus luteum. Its formation is due to the
hypoxic conditions present in the corpus luteum as fibroblasts manufacture an overabundance of collagen. The fibrotic event elicits the arrival of T cel ls that release interferon-y, a chemoattractant for macrophages, which release tumor necrosis factor a, a cytokine that drives both granulosa lutein and theca lutein cells into apoptosis. As the cell death and fibrosis progresses, the corpus albicans contracts and becomes a small scar on the surface of the ovary.
5. Atretic fol l ic les a. Atretic fo l l icles are follicles (in various stages of maturation) that are undergoing
degeneration. b. They are commonly present in the ovary. c. After a dominant graafian follicle ovulates, the remaining graafian and secondary follicles
degenerate because the dominant fo l l i c le releases i nh ib in that shuts off FSH production by the basophils of the anterior pituitary gland.
d . They often show pyknotic changes in the nuclei of the granulosa cells and other degenerative changes.
C. The ovarian medu l la contains large blood vessels, lymphatic vessels, and nerve fibers in a loose connective tissue stroma. They also possess a small number of estrogen -secreting i nterstitia l cel ls and a few androgen-secreting h i la r cel ls .
D. Hormonal regulation (Figure 19.3) 1 . Control of fo l l i c le maturation and ovu lation
a . The primary oocyte of unilaminar primary follicles secretes activin, which facilitates proliferation of granulosa cells. Granulosa cells secrete stem ce l l factor (kit- l igand) that binds to kit ligand receptors on the surface of the primary oocyte p lasmalemma as well as to kit ligand receptors on the surface of the theca interna cel l membranes. The binding to primary oocyte kit ligand receptors is responsible for growth of the primary oocyte, and binding to kit ligand receptors on the theca interna ce l ls facilitates their organization around the developing follicles.
b. Both the normal development of the primary follicle and the conversion from primary to secondary follicles is greatly dependent on BMP-1 5 (bone morphogenic protein 15) and GDF-9 (growth differentiation factor 9) .
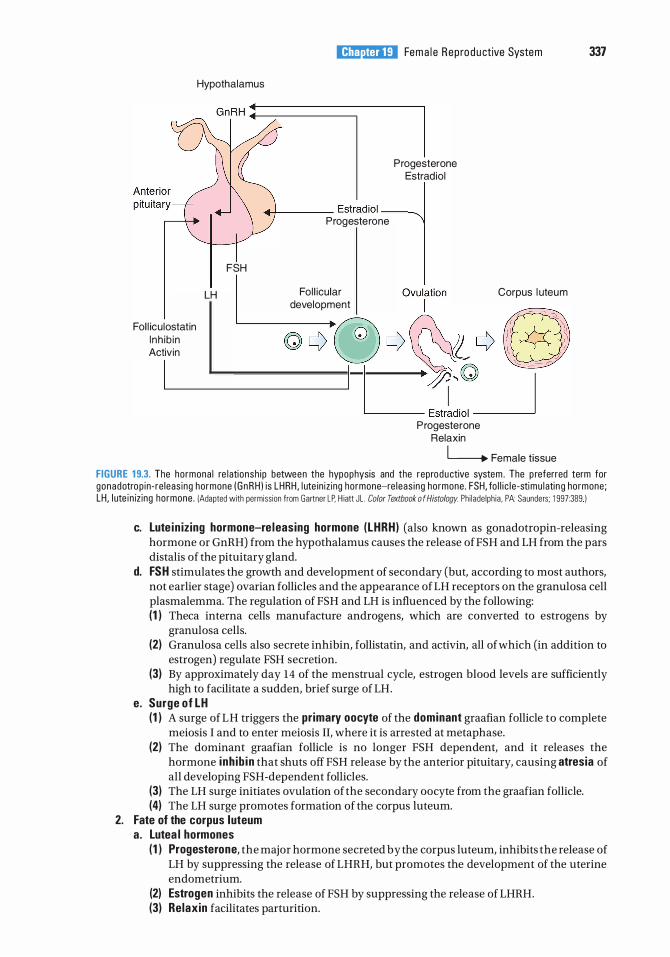
Hypothalamus
l!il!ll'tttD]j Fema l e Rep ro d u ctive System 337
Progesterone Estrad iol
.-+---- Estrad iol __ -....
Fol l icu lostatin lnh ib in Activin
I
FSH
LH
Progesterone
Fol l icular development
Progesterone Relaxin
Corpus l uteum
l______. Female tissue
FIGURE 1 9.3. The hormona l re lationsh ip between the hypophysis and the reproductive system . The p referred term for gonadotrop in-re leas ing hormone (GnRH ) is LHRH , l ute in iz ing hormone-re leas ing hormone . FSH, fo l l i c l e -stimu lati n g hormone; LH, l ute in iz ing hormone . {Adapted with permission from Gartner LP. H iatt JL . Color Textbook o f Histology. Phi lade lph ia , PA: Saunders; 1 997:389 )
c. Lute in iz ing hormone-re leasing hormone (LHRH) (also known as gonadotropin-releasing hormone or GnRH) from the hypothalamus causes the release ofFSH and LH from the pars distalis of the pituitary gland.
d. FSH stimulates the growth and development of secondary (but, according to most authors, not earlier stage) ovarian follicles and the appearance ofLH receptors on the granulosa cell plasmalemma. The regulation of FSH and LH is influenced by the following: (1 ) Theca interna cells manufacture androgens, which are converted to estrogens by
granulosa cells. (2) Granulosa cells also secrete inhibin, follistatin, and activin, all of which (in addition to
estrogen) regulate FSH secretion. (3) By approximately day 14 of the menstrual cycle, estrogen blood levels are sufficiently
high to facilitate a sudden, brief surge of LH. e. Surge of LH
(1 ) A surge of LH triggers the primary oocyte of the dominant graafian follicle to complete meiosis I and to enter meiosis II, where it is arrested at metaphase.
(2) The dominant graafian follicle is no longer FSH dependent, and it releases the hormone i nh ib in that shuts off FSH release by the anterior pituitary, causing atresia of all developing FSH-dependent follicles.
(3) The LH surge initiates ovulation of the secondary oocyte from the graafian follicle. (4) The LH surge promotes formation of the corpus luteum.
2. Fate of the corpus luteum a. Lutea l hormones
( 1 ) Progesterone, the major hormone secreted by the corpus luteum, inhibits the release of LH by suppressing the release of LHRH, but promotes the development of the uterine endometrium.
(2) Estrogen inhibits the release of FSH by suppressing the release of LHRH. (3) Relaxin facilitates parturition.
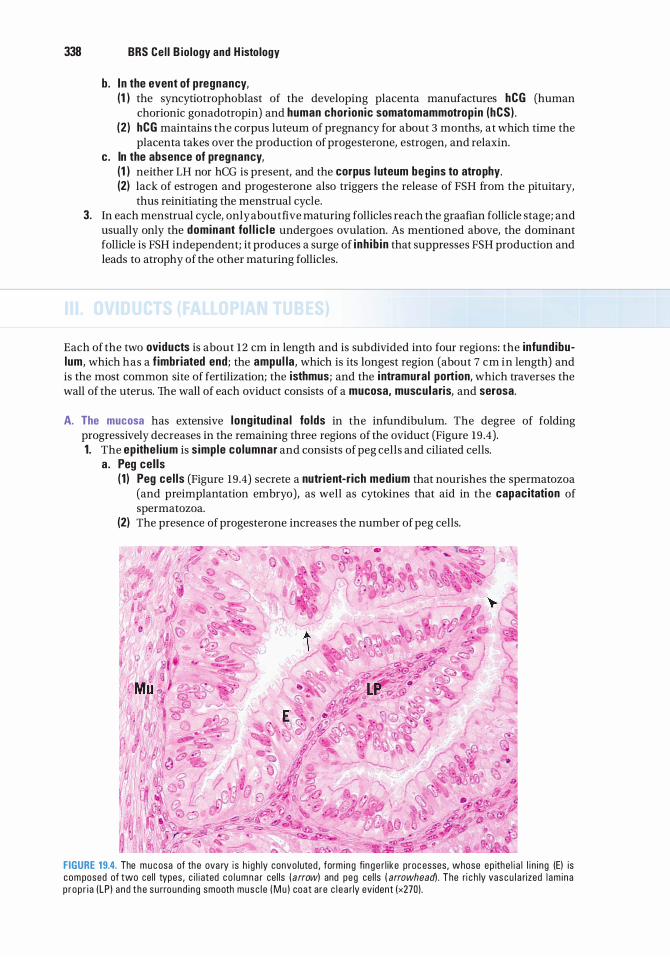
338 BRS Cel l B iology and H istology
b. In the event of pregnancy, (1 ) the syncytiotrophoblast of the developing placenta manufactures hCG (human
chorionic gonadotropin) and human chor ionic somatomammotrop in (hCS) . (2 ) hCG maintains the corpus luteum of pregnancy for about 3 months, at which time the
placenta takes over the production of progesterone, estrogen, and relaxin. c. In the absence of pregnancy,
(1 ) neither LH nor hCG is present, and the corpus l uteum begins to atrophy. (2) lack of estrogen and progesterone also triggers the release of FSH from the pituitary,
thus reinitiating the menstrual cycle. 3. In each menstrual cycle, only about five maturing follicles reach the graafian follicle stage; and
usually only the dominant fo l l i c l e undergoes ovulation. As mentioned above, the dominant follicle is FSH independent; it produces a surge of i nh ib in that suppresses FSH production and leads to atrophy of the other maturing follicles.
Each of the two oviducts is about 12 em in length and is subdivided into four regions: the infundibulum, which has a f imbriated end; the ampul la, which is its longest region (about 7 em in length) and is the most common site of fertilization; the isthmus; and the i ntramural portion, which traverses the wall of the uterus. The wall of each oviduct consists of a mucosa, muscularis, and serosa.
A. The mucosa has extensive l ong itud ina l fo lds in the infundibulum. The degree of folding progressively decreases in the remaining three regions of the oviduct (Figure 19 .4). 1. The ep ithe l ium is simple columnar and consists of peg cells and ciliated cells.
a. Peg cel ls ( 1 ) Peg ce l ls (Figure 19.4) secrete a nutr ient-r ich medium that nourishes the spermatozoa
(and preimplantation embryo), as well as cytokines that aid in the capacitation of spermatozoa.
(2) The presence of progesterone increases the number of peg cells.
FIGURE 19.4. The m u c osa of the ova ry i s h i g h ly convo luted , form i ng fi n g e r l i ke proc esses, whose ep ithe l i a l l i n i ng (E) is com posed of two ce l l types , c i l i ated c o l u m n a r ce l ls ( arrow) and peg ce l ls ( arrowhead) . The ri c h ly vas c u l a rized l am i na p rop r i a (LP ) a nd t he s u rround i n g smooth musc l e ( M u ) coat are c l e a rly ev ident (x270) .
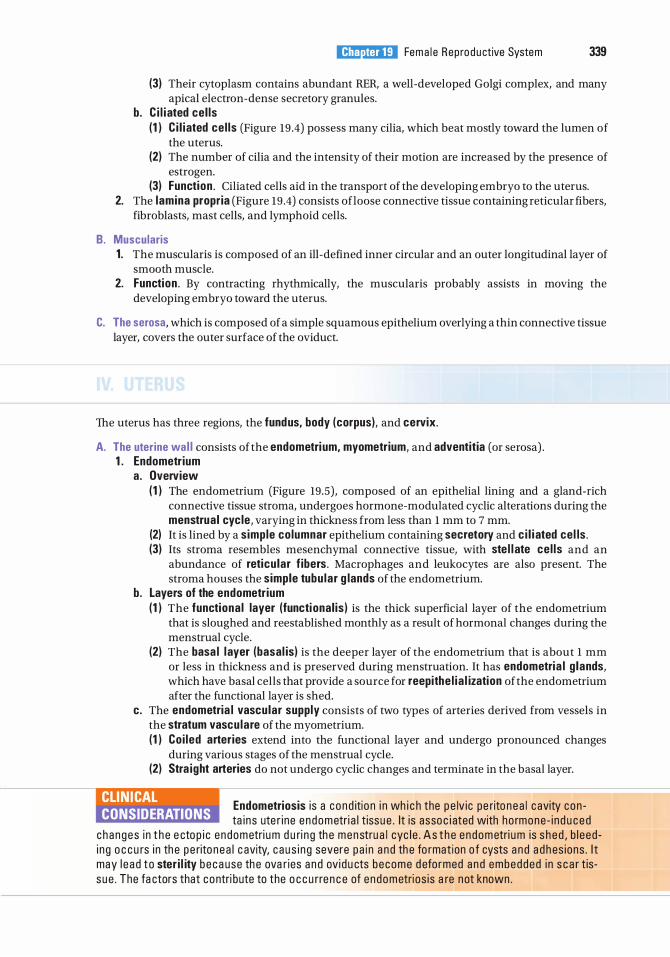
l!il!ll'tttD]j Fema l e Rep ro d u ctive System 339
(3) Their cytoplasm contains abundant RER, a well-developed Golgi complex, and many apical electron-dense secretory granules.
b. C i l i ated cel ls (1 ) C i l i ated ce l ls (Figure 19 .4) possess many cilia, which beat mostly toward the lumen of
the uterus. (2) The number of cilia and the intensity of their motion are increased by the presence of
estrogen. (3) Function . Ciliated cells aid in the transport of the developing embryo to the uterus.
2. The lamina propria (Figure 19 .4) consists ofloose connective tissue containing reticular fibers, fibroblasts, mast cells, and lymphoid cells.
B. Muscularis 1. The muscularis is composed of an ill-defined inner circular and an outer longitudinal layer of
smooth muscle. 2. Function . By contracting rhythmically, the muscularis probably assists in moving the
developing embryo toward the uterus.
C. The serosa, which is composed of a simple squamous epithelium overlying a thin connective tissue layer, covers the outer surface of the oviduct.
The uterus has three regions, the fundus, body (corpus), and cervix.
A. The uterine wa l l consists of the endometri um, myometrium, and adventitia (or serosa) . 1 . Endometrium
a. Overview (1 ) The endometrium (Figure 19.5) , composed of an epithelial lining and a gland-rich
connective tissue stroma, undergoes hormone-modulated cyclic alterations during the menstrual cyc le, varying in thickness from less than 1 mm to 7 mm.
(2) It is lined by a simple columnar epithelium containing secretory and c i l i ated cel ls . (3) Its stroma resembles mesenchymal connective tissue, with ste l l ate ce l ls and an
abundance of reticu lar f ibers. Macrophages and leukocytes are also present. The stroma houses the simple tubu lar g lands of the endometrium.
b. Layers of the endometrium (1 ) The functiona l layer (functional is ) is the thick superficial layer of the endometrium
that is sloughed and reestablished monthly as a result of hormonal changes during the menstrual cycle.
(2) The basa l layer (basal is) is the deeper layer of the endometrium that is about 1 mm or less in thickness and is preserved during menstruation. It has endometria l g lands, which have basal cells that provide a source for reepithe l ia l ization of the endometrium after the functional layer is shed.
c. The endometria l vascular supply consists of two types of arteries derived from vessels in the stratum vascu lare of the myometrium. (1 ) Co i led arteries extend into the functional layer and undergo pronounced changes
during various stages of the menstrual cycle. (2) Stra ight arteries do not undergo cyclic changes and terminate in the basal layer.
CLIN ICAL CONSIDERATIONS
Endometriosis i s a c ond itio n i n wh i c h the p e lv ic pe rito n e a l c avity con ta i ns ute r i ne e ndometri a l t issue . It is asso c i ated with ho rmone - i n d u c e d
c hanges i n t h e e ctop i c e ndometri um d u ri n g th e menstru a l cyc l e . A s t h e e ndometri um is s h e d , b l e ed i n g o c c u rs i n th e pe rito nea l c avity, c aus i n g severe pa i n a n d th e fo rmat ion o f cysts a n d a d h es ions . I t may l e a d to ster i l ity beca use th e ova r ies a n d ov i d u cts become d efo rmed a n d embedded i n s c a r t iss ue . The fa ctors that contri bute to the o c c u rre n c e of e ndometri os is a re not known .
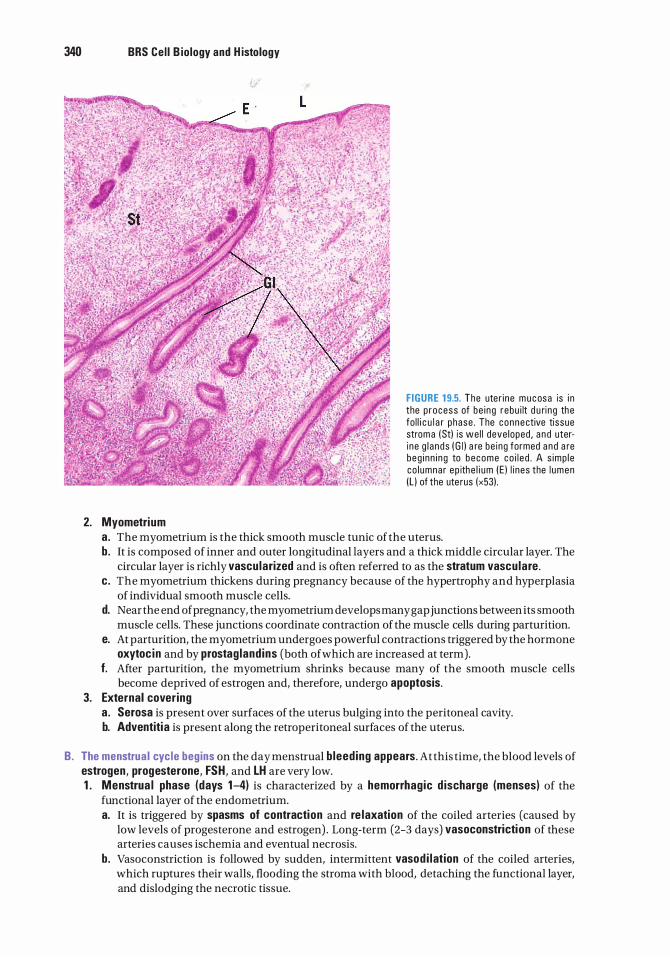
340 BRS Cel l B iology and H istology
2. Myometrium
F IGURE 1 9.5. The ute r i ne m u c osa is i n the p rocess of be i ng rebu i lt d u ri ng the fo l l i c u l a r phase . The connective tissue strom a (Stl is we l l deve loped , a n d uteri ne g l a nds ( G i l a re be ing formed a n d a re beg i nn i n g to become co i l e d . A s imp l e co l umnar ep ithe l i um ( E ) l i nes the l umen Il l of the ute rus (x53l .
a. The myometrium is the thick smooth muscle tunic of the uterus. b. It is composed of inner and outer longitudinal layers and a thick middle circular layer. The
circular layer is richly vascu larized and is often referred to as the stratum vascu lare . c . The myometrium thickens during pregnancy because of the hypertrophy and hyperplasia
of individual smooth muscle cells. d. Near the end of pregnancy, the myometrium develops many gap junctions between its smooth
muscle cells. These junctions coordinate contraction of the muscle cells during parturition. e. At parturition, the myometrium undergoes powerful contractions triggered by the hormone
oxytoc in and by prostag land ins (both of which are increased at term). f. After parturition, the myometrium shrinks because many of the smooth muscle cells
become deprived of estrogen and, therefore, undergo apoptosis. 3. External covering
a . Serosa is present over surfaces of the uterus bulging into the peritoneal cavity. b. Adventitia is present along the retroperitoneal surfaces of the uterus.
B. The menstrua l cyc le begins on the day menstrual b leed ing appears. At this time, the blood levels of estrogen, progesterone, FSH, and LH are very low. 1 . Menstrua l phase (days 1-4) is characterized by a hemorrhagic d ischarge (menses) of the
functional layer of the endometrium. a. It is triggered by spasms of contraction and re laxation of the coiled arteries (caused by
low levels of progesterone and estrogen) . Long-term (2-3 days) vasoconstriction of these arteries causes ischemia and eventual necrosis.
b. Vasoconstriction is followed by sudden, intermittent vasod i lation of the coiled arteries, which ruptures their walls, flooding the stroma with blood, detaching the functional layer, and dislodging the necrotic tissue.
l!il!ll'tttD]j Fema le Reproductive System 341
c. Because the basal layer is supplied by short straight vessels that do not undergo prolonged vasoconstriction, it is not sloughed and does not become necrotic.
d . During the menstrual phase of the menstrual cycle, blood clotting is inhibited. 2. The prol iferative (fo l l i cu lar) phase (Figure 19 .5), days 4 to 1 4, follows the menstrual phase
and involves renewa l of the entire functional layer, including the repair of glands, connective tissue, and vascular elements (specifically, the coiled arteries) . During the proliferative phase, the levels of estrogen in the blood continue to rise, and this is the principal hormone responsible for the stage of proliferation. a. The epithelium that lines the luminal surface of the uterus is renewed by mitotic activity of
cells remaining in the uterine glands of the basal layer of the endometrium. b. Glands are straight and lined by a simple columnar epithelium. c. Stromal cells divide, accumulate glycogen, and enlarge. d. Coiled arteries extend approximately two-thirds of the way into the endometrium. e. At the end of the proliferative phase, the endometrium is approximately 3 mm in thickness.
3. The secretory ( l utea l ) phase (days 1 5-28) begins shortly after ovulation and is characterized by a th ickening of the endometrium, resulting from edema and secretion by the endometrial glands. Progesterone, and to a certain degree estrogen, are the principal hormones driving the secretory phase. a. Glands become co i led; their lumina become filled with a secretion of g lycoprote in mater ia l
and g lycogen; and their cells accumulate large amounts of g lycogen, in the basal aspect of their cytoplasm.
b. Coiled arteries become not only more highly coiled but also longer, extending into the superficial aspects of the functional layer.
c. At the end of the secretory phase, the endometrium is somewhat edematous and is approximately 6 to 7 mm in thickness.
CLIN ICAL CONSIDERATIONS
Uterine prolapse i s a c o nd iti o n i n wh i c h th e ute r i ne l i g aments, n a m e ly the ro u nd l i g ament, broad l i g ament, ute ros a c ra l l i g aments, and th e l i g am ent
of the ova ry, a re no l o n ge r a b l e to ma i nta i n the no rma l a n atom i c a l pos iti o n of th is o rgan , a n d the ute rus s l i d es d own and fre q uently b u l g e s i nto the va g i n a . Th e ute rus may o c c u py on ly the u p p e r one th i rd of the va g i n a o r may s l i d e a l l th e way down to p rotru d e th ro u g h the va g i n a l o rifi c e between th e l a b i a m i no ra a n d ma jo ra . Ute r i ne p ro l a pse u s u a l ly o c c u rs i n o l d e r women , b ut may a l so be p resent in you n g e r women who h a d very l a rg e bab i e s a n d a p ro l onged , d iffi c u lt d e l ive ry. Exte ns ive p ro l a pse of the ute rus may i nte rfe re with u r i natio n as we l l a s with d efe c ati on . The usua l treatment fo r ute ri n e p ro l a pse i s s u r g i c a l reatta c hment o r, i n mo re extreme c ases, hyste re ctomy.
A. The cervix does not participate in menstruation, but its secretions change during various stages of the menstrual cycle.
B. The cervical wall is composed mainly of dense collagenous connective tissue interspersed with numerous elastic fibers and a few smooth muscle cells.
C. The cervix has a simple columnar (mucus-secreti ng ) ep ithe l ium except for the inferior portion (continuous with the lining of the vagina), which is covered by a stratified squamous nonkerati n ized ep ithe l ium.
D. Branched cervica l g lands secrete a serous fluid near the time of ovulation that facilitates the entry of spermatozoa into the uterine lumen. During pregnancy, cervical glands produce a thick, viscous secretion that hinders the entry of spermatozoa (and microorganisms) into the uterus.
E. Prior to parturition, the cervix dilates and softens as a result of the lysis of the collagen fiber bundles in response to the hormone relaxin .
342 BRS Cel l B iology and H istology
CLIN ICAL CONSIDERATIONS
1 . I n a Papan ico laou (Pap ) smear, e p ith e l i a l c e l l s a re s c ra p e d from th e l i n i n g of th e c e rvix (or v a g i n a ) a n d a re exa m i n e d to d etect
c e rv i c a l c a n c e r. A Pap s m e a r sh ows var iati on i n ce l l popu l at i ons with sta g e s of th e m e n stru a l cyc l e .
2 . Carc inoma o f the cervix o rig i n ates from stratif ied s quamous non ke rati n ized e p ith e l i a l c e l l s . It may be conta i n ed with i n th e ep ith e l i um and not inva d e the u n d e rlyi ng strom a (carcinoma in situ ) , o r it may pen etrate th e basa l l am i n a and m etastas ize to oth e r p a rts of the body ( i nvasive carcinoma) . I t o c c u rs at a re l ative ly h i g h fre q uen cy, b ut may be c u red by s u rg e ry if d i s covered ea rly ( by Pap smea r), b efore it b ecomes invas ive .
A. Ferti l ization 1. Fertilization usually takes place within the ampulla of the oviduct, and occurs when a
spermatozoon penetrates the corona radiata and the zona pellucida and pierces the plasma membrane of a secondary oocyte. a . Before a spermatozoon is capable of fertilizing, it must undergo maturation, and
capacitation, and hyperactivity. (1 ) Maturation occurs in the male reproductive tract. Prior to maturation, the spermatozoon
cannot travel in a forward direction; instead, it travels only in a circular fashion. (2) Capacitation occurs in the female reproductive tract. While the sperm is in the male
reproductive tract, it is unable to undergo capacitation because the concentration of the prostate-manufactured ferti l ization-promoting peptide (FPP) is too high. Once the sperm arrives in the female reproductive tract, the concentration of FPP is reduced to a suitable level (because it becomes diluted by the vaginal secretions), and the sperm is prompted to begin the process of capacitation. (a ) Cholestero l molecules are removed from the acrosomal plasmalemma, making the
membrane less rigid. (b) Special Ca2+ ion channels open in the plasma membrane of the spermatozoon
flagella, permitting the influx of calcium ions. (c) Elevated levels of intraflagellar calcium ions induce the formation of cAMP, which
causes the spermatozoon to become hyperactive. (3) Hyperactivity is merely the ability of the spermatozoon to swim faster and more
vigorously, making it easier for the sperm to penetrate the zona pellucida to contact the oocyte.
b. Once the spermatozoon has undergone capacitation, it is capable of fertilizing the egg, but in order to do so it must undergo the acrosome reaction, b ind to ZP3, and fuse to the p lasma membrane of the secondary oocyte . ( 1 ) The acrosome reaction and b ind ing to ZP3 occur when the spermatozoon contacts
the zona pellucida. Hydrolytic enzymes, especially acrosin, are released from the acrosome, reduce the viscosity of the zona pellucida just ahead of the spermatozoon, permitting it to reach the secondary oocyte.
(2) Fusion of the spermatozoon membrane and the secondary oocyte plasmalemma occurs due to the presence offerti l in , an integral protein in the spermatozoon membrane with CD9 molecules and integrins of the secondary oocyte's plasmalemma.
c. The secondary oocyte responds to the contact by the spermatozoon by undergoing the cortical reaction, resuming the second meiotic division, and forming the female pronucleus. (1) The cortical g ranu les of the secondary oocyte, located just deep to the cell membrane,
fuse with the cell membrane, releasing their enzymes into the zona pellucida. The ZP proteins form a complex with each other, which transforms the gelatinous nature of the zona pellucida into a highly viscous substance that stops other spermatozoa from reaching the secondary oocyte, thus preventing po lyspermy.
l!il!ll'tttD]j Fema le Reproductive System 343
(2) The contact of spermatozoon with the secondary oocyte permits the entry of the spermatozoon's nucleus (male pronucleus) and centrosome to enter the secondary oocyte's cytoplasm, triggering the oocyte to complete its second meiotic d ivision, forming the second polar body and thus transforming the secondary oocyte into the ovum.
(3) The now haploid nucleus ofthe ovum is known as the fema le pronucleus. The two haploid pronuclei travel toward each other, shed their nuclear envelopes, their chromosomes intermingle as they form a d ip lo id ce l l , known as the zygote . Immediately after the intermingling of the chromosomes, the centrosome, contributed by the spermatozoon, forms a mitotic spindle apparatus, and the zygote undergoes its fi rst mitotic division. The two newly formed daughter cells are the first two cells of the new embryo. It should be noted that all centrosomes of the new individual are derived from the father, and all of the mitochondria are derived from the mother.
B. Imp lantation 1 . The zygote undergoes mitotic cell division (known as c leavage during the early stages of
embryogenesis) and is transformed into a multicellular structure called a morula, which requires about 3 days to travel through the oviduct and enter the uterus.
2. The conceptus (the preimplantation embryo and its surrounding membranes) acquires a fluid-filled cavity and becomes a blastocyst.
3. The blastocyst implants in the endometrium of the uterus and is surrounded by an inner cellular layer, the cytotrophoblast, and an outer multinucleated layer, the syncytiotrophoblast.
4. The syncytiotrophoblast further invades the endometrium in the wall ofthe uterus by the sixth day after fertilization. Formation of the placenta then begins.
CLIN ICAL CONSIDERATIONS
1 . Ectop ic (tuba l ) pregnancy i s the implantation o f th e ea r ly embryo i n a n a bno rm a l s ite ( e . g . , wall o f the oviduct) . I t c a n be fatal without immed i ate med i c a l i nte rventi on .
2 . Teratomas a re g e rm ce l l tumo rs t ha t fa l l i nto th ree g ro u ps : mature, monode rm a l, a n d immature . a. Mature teratomas a re b en i g n ( a lth ough o c c a s i o na l ly they may become ma l i g n a nt) and a re
u s ua l ly p resent i n yo ung women . These a re cysts with wa l l s that fre q uently conta i n h a i r a n d oth e r e p i d e rm a l structures s u c h as s ebaceous g l a nds, as we l l a s b o ne , tooth, a n d c a rti l a g e fra gments.
b. Monodermal teratomas a re ra re tumo rs that a re a l so known as spec i a l i zed teratomas . The two most fre q u ent types of th ese tumors a re struma ova r i i and ova ri a n c a rc i no i d . Struma ovari i i s a n ova r i an tumo r c om posed of we l l - d eve l o ped thyro i d fo l l i c l es that prod u c e thyro i d ho rmone a n d may be respons i b l e fo r hyp e rthyro i d i sm . Ovarian carc ino id i s a tu mo r that u s ua l ly p ro d u ces se roton i n ( 5- 0 H -tryptam i ne ) .
c. Immature teratomas a re fast- g rowing m a l i g n a nt tu mo rs with a h i sto logy that resemb l e s that of feta l rath e r th a n m ature tissues . They a re usua l ly p resent i n a do l e s cents and very young women .
The placenta i s a transient structure, consisting of a materna l portion and a feta l portion .
A. Structure 1. At birth it is approximately 18 em in diameter, 2.5 em thick, and weighs about 600 g. 2. As the placenta begins its development, the cytotrophoblasts and syncytiotrophoblasts form
the chorion, and in response, the endometrium of the uterus forms the decidua . 3. The chorion develops into the chorion ic p late, which gives rise to the chor ionic vi l l i .
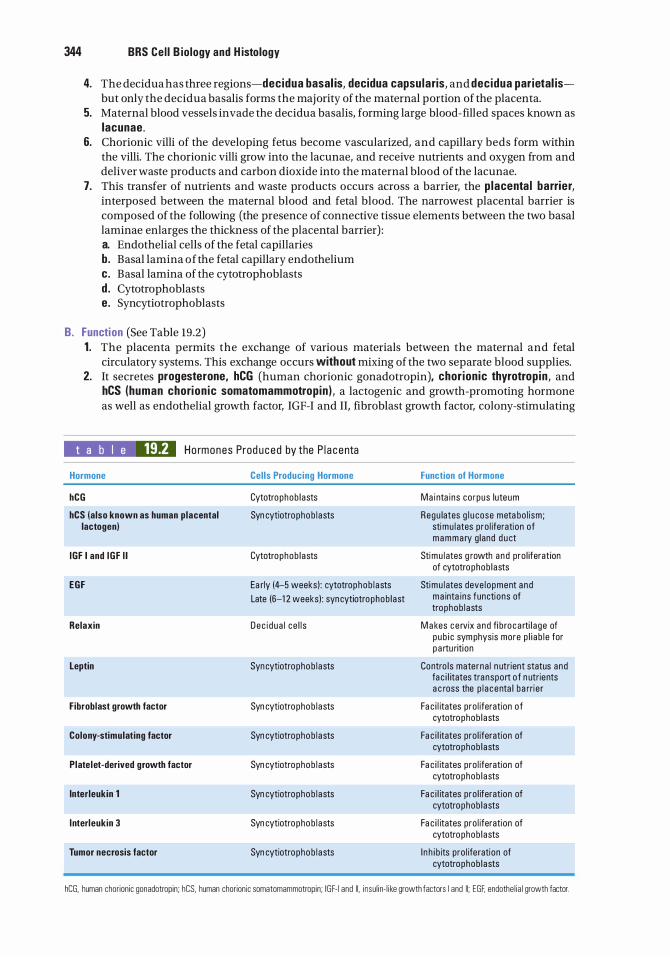
344 BRS Cel l B iology and H istology
4. The decidua has three regions-decidua basal is, decidua capsu laris, and decidua parietal isbut only the decidua basalis forms the majority of the maternal portion of the placenta.
5. Maternal blood vessels invade the decidua basalis, forming large blood-filled spaces known as lacunae.
6. Chorionic villi of the developing fetus become vascularized, and capillary beds form within the villi. The chorionic villi grow into the lacunae, and receive nutrients and oxygen from and deliver waste products and carbon dioxide into the maternal blood of the lacunae.
7. This transfer of nutrients and waste products occurs across a barrier, the p lacenta l barrier, interposed between the maternal blood and fetal blood. The narrowest placental barrier is composed of the following (the presence of connective tissue elements between the two basal laminae enlarges the thickness of the placental barrier) : a. Endothelial cells of the fetal capillaries b. Basal lamina ofthe fetal capillary endothelium c. Basal lamina of the cytotrophoblasts d . Cytotrophoblasts e. Syncytiotrophoblasts
B. Function (See Table 19.2) 1 . The placenta permits the exchange of various materials between the maternal and fetal
circulatory systems. This exchange occurs without mixing of the two separate blood supplies. 2. It secretes progesterone, hCG (human chorionic gonadotropin), chor ionic thyrotrop in , and
hCS (human chorion ic somatomammotropin ) , a lactogenic and growth-promoting hormone as well as endothelial growth factor, IGF-I and II, fibroblast growth factor, colony-stimulating
t a b I e 19.2 Ho rmones Prod uced by the P l a c e nta
Hormone
hCG
hCS (also known as human placental lactogen)
IGF I and IGF I I
EGF
Relaxin
Leptin
Fibroblast growth factor
Colony-stimulating factor
Platelet-derived growth factor
lnterleukin 1
l nterleukin 3
Tumor necrosis factor
Cel ls Producing Hormone
Cytotrophob l asts
Syn cytiotro pho b l asts
Cytotrophob l asts
Ea rly (4--5 weeks) : cytotrophob l asts
Late (6-1 2 weeks) : syncytiotrophob l ast
Dec i d ua l ce l l s
Syn cytiotro pho b l asts
Syn cytiotro pho b l asts
Syn cytiotro pho b l asts
Syn cytiotro pho b l asts
Syn cytiotro pho b l asts
Syn cytiotro pho b l asts
Syn cytiotro pho b l asts
Function of Hormone
Ma inta ins co rpus luteum
Regu lates g l u cose meta bo l i sm; stimu l ates pro l iferation of mamma ry g land d u ct
Stimu l ates g rowth a nd pro l iferation of cytotrophob l asts
Stimu l ates deve l opment a nd m a inta ins functions of trophob l asts
M a kes c e rvix a nd fi bro ca rti l a ge of pub i c sym physis more p l i a b l e for p a rtu riti on
Contro ls materna l n utrient status and fa c i l itates tra nsport o f n utrients a c ross the p l a centa l ba rri e r
Fa c i l itates pro l iferation of cytotrophob l asts
Fa c i l itates pro l iferation of cytotrophob l asts
Fa c i l itates pro l iferation of cytotrophob l asts
Fa c i l itates pro l iferation of cytotrophob l asts
Fa c i l itates pro l iferation of cytotrophob l asts
I n h i b its pro l ife ration of cytotrophob l asts
hCG, human chorionic gonadotropin; hCS, human chorionic somatomammotropin; IGF- 1 and II, insu l in- l i ke growth factors I and II; EGF, endothe l ia l growth factor.
l!il!ll'tttD]j Fema le Reproductive System 345
factor, platelet-derived growth factor, tumor necrosis growth factor, relaxin, leptin, and interleukins l and 3.
3. It also produces estrogen with the assistance of the liver and the adrenal cortex of the fetus. 4. Decidual cells of the stroma produce prostag land ins and pro lacti n .
CLIN ICAL CONSIDERATIONS
The po lyp epti d e ho rmone prolacti n, m a n ufa ctu red by basoph i l s o f th e a denohypophysis ( a nteri o r p itu ita ry), c a uses a n i n c rease i n b reast s ize
i n the preg n a nt fem a l e and i n d u ces mi lk fo rmati on a s we l l a s l a ctati o n i n the m a m m a ry g l a n d s of the postp a rtum fem a l e . I nte resti n g ly, i t a l so c a uses the fe e l i n g of sexu a l g ratifi c at ion subsequent to th e sexua l a ct. B e c a use p rogesterone has been shown to a l l evi ate th e sym ptoms of m u lti p l e s c l e ros is (MS) i n the p re g n a nt fema le , re c e nt investi g ations us i ng a mouse mode l d emonstrated that tre atment of M S -affl i cted mice with p ro l a ct in resu lted i n remye l i n ati on of n e rve fi b e rs, whose mye l i n was destroyed by the d i sease . It i s be l ieved that p ro l a cti n stimu l ates the fo rmati on of p roo l i g o dend rocytes, wh i ch d iffe renti ate i nto o l i g o dend rocytes, c e l l s that a re respons i b l e fo r mye l i n atio n of axons i n the c e ntra l n e rvous system .
A . Overview 1. The vagina is a f ibromuscu lar canal with a wall that is composed of three layers : an inner
mucosa, a middle muscularis, and an external adventitia . 2. I t is circumscribed by a skeletal musc le sphincter at its external orifice. 3. It lacks glands throughout its length and is lubricated by secretions from the cervix and by
seepage of the extracellular fluid from the vascular supply of the lamina propria.
B. The mucosa is composed of a thick, stratified squamous nonkeratin ized ep ithe l ium and a fibroelastic connective tissue, the l amina propria. 1 . The epithe l ium contains g lycogen, which is used by the vaginal bacterial flora to produce
lactic acid , an acid that lowers the pH during the follicular phase of the menstrual cycle and inhibits invasion by pathogens.
2. The l amina propria is a fibroelastic connective tissue that is h ighly vascu lar in its deeper aspect (which is possibly analogous to a submucosa) .
C. The muscularis is composed of irregularly arranged layers of smooth muscle (thin inner circular layer and a thicker outer longitudinal layer) interspersed with elastic f ibers.
D. The adventitia is composed of fibroelastic connective tissue. It attaches the vagina to the surrounding structures.
A. The lab ia majora are fat- laden fo lds of skin; hair and secretions of sebaceous g lands and sweat g lands are present on their external surfaces.
B. Labia minora 1. The labia minora are folds of skin that possess a core of h igh ly vascu lar connective tissue
containing elastic fibers. 2. They lack hair follicles, but their dermis contains numerous sebaceous g lands, which open
directly onto the epithelial surface.
346 BRS Cel l B iology and H istology
C. The vestibu le is the space between the two labia minora. Glands of Bartho l in (mucus-secret ing g lands) and numerous smaller mucus-secreting glands around the urethra and clitoris (m inor vestibu lar g lands) open into this space.
D. Cl itoris 1. The clitoris is composed of two small, cylindrical erecti le bodies, which terminate in the
prepuce-covered g lans c l itor id is . 2. It contains many sensory nerve fibers and specialized nerve endings (e.g., Meissner corpuscles
and pacinian corpuscles) .
Mammary glands of both genders are identical for the first decade or so of life, but when the female reaches puberty, the flow of estrogens and progesterone as well as lactogenic hormone induces the mammary gland to enlarge and develop a system of lobules and terminal ductules as well as an increase in the connective tissue mass and a deposit of adipose tissue. Each mammary gland of the postpubertal female is composed of numerous compound tubu loalveo lar g lands, each with its own lactiferous sinus and a duct that opens at the apex of the nipple.
CLIN ICAL CONSIDERATIONS
The use o f l ave n d e r o i l a n d tea t r ee o i l-based p ro d u cts i n p r epu bes c e nt m a l es h a s b een shown to c a use gyn e c o m a sti a , the deve l o p m e nt
of b r easts i n these i n d ivi d u a l s . The p rese n c e of the b reast ti s sue pe rsisted for seve ra l months afte r th e boys sto p p e d us ing th ese p rodu cts, and th e n s l owly reg ressed to i ts n o rma l c o n d itio n . I t a p p e a rs that th ese o i l p r odu cts a re a b l e t o im itate estro gens a n d e v e n i n h i b it th e effe cts of a n d rogens .
A . Resting (non lactati ng ) mammary g lands (in adult, nonpregnant women) 1 . Resting mammary glands are composed of lactiferous s inuses and ducts lined in most areas
by a stratified cuboidal epithelium, with a basal layer consisting of scattered myoepithe l i a l ce l ls.
2. A basal lamina separates the epithelial components from the underlying stroma.
B. Active ( lactating ) mammary g lands are enlarged during pregnancy by the development of a lveo l i . 1 . Alveolar ce l l s (secretory cells) (Figure 19.6)
a . Alveolar cells line the alveoli of active mammary glands and are surrounded by an incomplete layer of myoepithe l ia l ce l ls .
b . They are richly endowed with RER and contain several Golgi complexes, numerous mitochondria, lipid droplets, and vesicles containing milk protein (caseins) and lactose.
2. Secretion by a lveo lar ce l ls a . l ip ids are released into the lumen, perhaps, via the apocrine mode of secretion. b. Prote ins and sugars are released into the alveolar lumen via the merocrine mode of
secretion (exocytosis) .
C. N ipp le 1 . The nipple is composed of dense, irregular collagenous connective tissue interlaced with
smooth muscle fibers that act as a sphincter. 2. It contains the openings of the lactiferous ducts. 3. It is surrounded by pigmented skin (areola) that is more deeply pigmented during and
subsequent to pregnancy and contains the areo lar g lands (of Montgomery).
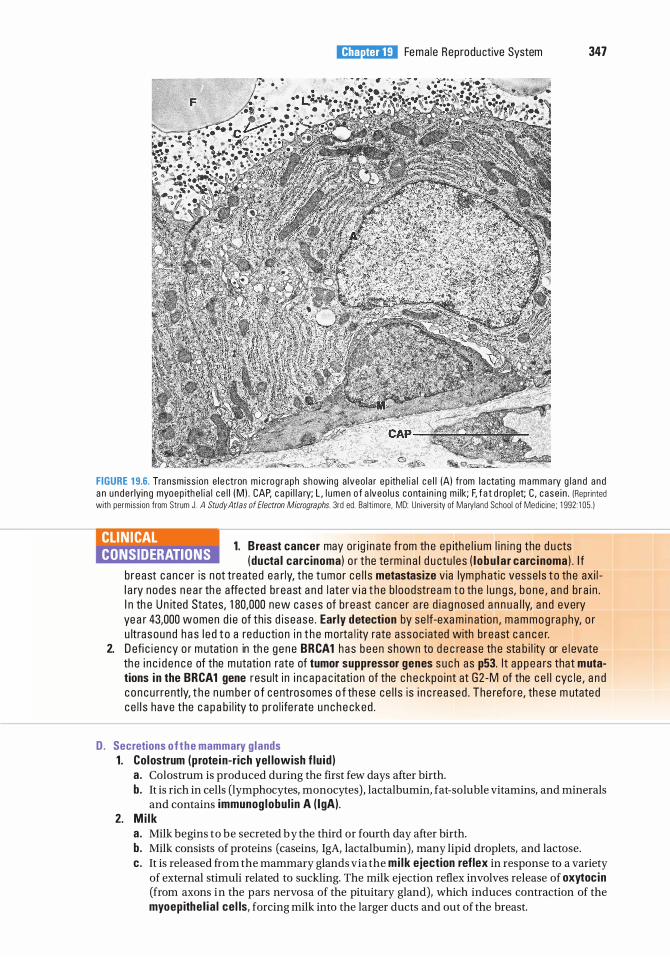
l!il!ll'tttD]j Fema le Reproductive System 347
FIGURE 1 9.6. Tra nsmiss ion e l e ctron m i c rog raph s howing a lveo la r ep ithe l i a l c e l l (A) from l a ctati ng m a m m a ry g l a n d and a n unde rlyin g myoep ith e l i a l c e l l (M ) . CAP, c a p i l l a ry; L , l umen o f a lveo l us c o nta i n i ng m i lk; F, f a t d rop l et; C , case i n . (Repr inted with permiss ion from Strum J . A Study Atlas of Electron Micrographs. 3rd ed. Ba lt imore, MD: Un ivers ity of Mary land Schoo l of Medic ine ; 1 992: 1 05 . )
1. B reast cancer may or ig i n ate from th e e p ith e l i um l i n i n g the d u cts CLIN ICAL CONSIDERATIONS ( ducta l carcinoma) o r the te rm i n a l d u ctu l es ( l obu la r carc inoma ) . I f
b reast cance r is not treated ea r ly, the tumor ce l l s metastasize via lym ph atic vesse l s t o the axi l l a ry nodes n e a r th e affe cted b reast a n d l ater v i a t h e b l oodstrea m t o th e l u n g s, b o ne , a n d b ra i n . I n th e U n ited States, 1 80,000 new cases of b reast cance r a re d i a g nosed a n n u a l ly, a n d every yea r 43,000 women d i e of th is d i sease . Early detection by se lf-exa m i n ation , mammog ra phy, o r u ltra sound h a s l e d t o a red u cti o n i n t h e mo rta l ity rate assoc i ated with b reast c a n c e r.
2. D efi c i e n cy o r m utati o n in th e g e ne BRCA1 has been shown to d e c rease th e sta b i l ity or e l evate th e i n c i d e n ce of the mutati on rate of tumor suppressor genes such as p53. I t a p p e a rs that mutations i n the BRCA1 gene resu lt i n i n c a p a c itati on of the c h e c kpo i nt at G2 -M of the c e l l cyc l e , a n d c o n c u rrently, t h e n u m b e r o f c entrosomes o f th ese ce l l s is i n c reased . The refo re, th ese m utated c e l l s have the c a p a b i l ity to p ro l ife rate u n c h e cked .
D. Secretions o f t he mammary g lands 1. Colostrum (prote in-rich yel lowish f lu id )
a . Colostrum is produced during the first few days after birth. b. It is rich in cells (lymphocytes, monocytes ) , lactalbumin, fat -soluble vitamins, and minerals
and contains immunog lobu l in A ( lgA). 2. M i lk
a . Milk begins to be secreted by the third or fourth day after birth. b. Milk consists of proteins (caseins, IgA, lactalbumin), many lipid droplets, and lactose. c. It is released from the mammary glands via the mi lk ejection reflex in response to a variety
of external stimuli related to suckling. The milk ejection reflex involves release of oxytoc in (from axons in the pars nervosa of the pituitary gland), which induces contraction of the myoepithe l ia l cel ls, forcing milk into the larger ducts and out of the breast.
Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or completions of the statement. Select the ONE lettered answer that is BEST in each case.
1. Which of the following statements concerning secondary ovarian follicles is true?
(A) They lack liquor folliculi. (B ) They contain a secondary oocyte. (C) Their continued maturation requires
follicle-stimulating hormone. (D ) They lack a theca externa. (E ) They have a single layer of cuboidal
follicular cells surrounding the oocyte.
2. Colostrum contains which of the following antibodies?
(A) IgA (B ) IgD (C) IgE (D ) IgG (E ) IgM
3. Which of the following statements concerning the corpus luteum is true?
(A) It produces LH. (B) It produces FSH. (C) It derives its granulosa luteal cells from the
theca externa. (D ) It becomes the corpus albicans. (E) It is derived from atretic follicles.
4. LH exerts which one of the following physiological effects?
(A) It triggers completion of the second meiotic division by secondary oocytes.
(B) It triggers ovulation. (C) It suppresses release of estrogens. (D ) It induces primary follicles to become
secondary follicles. (E) It induces primordial follicles to become
primary follicles.
5. The basal layer of the uterine endometrium
(A) is sloughed during menstruation. (B) has no glands. (C) is supplied by coiled arteries. (D ) is supplied by straight arteries. (E ) is avascular.
348
6. One of the recognized phases of the menstrual cycle is termed the
(A) gestational phase. (B ) active phase. (C) follicular phase. (D) resting phase. (E ) anaphase.
7. During the proliferative phase of the menstrual cycle, the functional layer of the endometrium undergoes which of the following changes?
(A) Blood vessels become ischemic. (B ) The epithelium is renewed. (C ) The stroma swells because of edema. (D ) Glands become coiled. (E ) Blood vessels break down.
8. Which of the following statements concerning the vaginal mucosa is true?
(A) It is lined by stratified columnar epithelium.
(B ) It is lined by stratified squamous keratinized epithelium.
(C ) It possesses no elastic fibers. (D ) It is lubricated by glands in the cervix. (E ) Its cells secrete lactic acid.
9. Which of the following statements concerning the oviduct is true?
(A) It is lined by a simple cuboidal epithelium. (B ) Its epithelium contains peg cells. (C) It functions in nourishing trilaminar germ
discs. (D ) Fertilization most often occurs in its
fimbriated portion. (E) Its epithelium contains goblet cells.
10. Which one of the following teratomas is a malignant, fast-growing tumor?
(A) Mature teratoma (B ) Monodermal teratoma (C) Immature teratoma (D ) Struma ovarii (E ) Ovarian carcinoid
Answers and Explanations
1 . C. Secondary follicles depend on follicle-stimulating hormone for their continued development. They are established when liquor folliculi (an ultrafiltrate of plasma and granulosa cell secretions) begins to accumulate among the granulosa cells. Secondary follicles contain a primary oocyte blocked in the prophase of meiosis I (see Chapter 19 II B 1 b) .
2. A. IgA antibodies are present in colostrum and milk. IgG antibodies are acquired by the fetus by placental transfer from the mother (see Chapter 19 X D 1 ) .
3. D . A corpus albicans i s formed from a corpus luteum that has ceased to function. LH and FSH are both produced in the anterior pituitary gland. Granulosa luteal cells are derived from the granulosa cells of an ovulated graafian follicle (see Chapter 19 II B 4) .
4. B. A sudden surge of LH near the middle of the menstrual cycle triggers ovulation (see Chapter 19 II D 1 d) .
5. D. The basal layer of the uterine endometrium is supplied by the straight arteries and contains the deeper portions of the uterine glands. Cells from these glands reepithelialize the endometrial surface after the functional layer (supplied by the coiled arteries) has been sloughed (see Chapter 19 IV A 1 b) .
6. C. The recognized phases of the menstrual cycle are the follicular (proliferative) , secretory (luteal) , and menstrual phases. The mammary glands are characterized by active (lactating) and resting phases. The term gestational phase refers to pregnancy (see Chapter 19 IV B 3) .
7. B . During the proliferative phase of the menstrual cycle, the entire functional layer of the endometrium is renewed, including the epithelium lining the surface and glands. Edema in the stroma and coiled glands is characteristic of the secretory phase of the cycle, and ischemia is responsible for the menstrual phase (see Chapter 19 IV B 2) .
8. D. The vagina lacks glands and is lubricated by secretions from cervical glands. It is lined by a stratified squamous nonkeratinized epithelium with cells that release glycogen, which is used by the normal bacterial flora of the vagina to manufacture lactic acid (see Chapter 19 VIII A 3).
9. B . The oviduct is lined by a simple columnar epithelium composed of ciliated cells and peg cells but no goblet cells. Fertilization most often occurs in the ampulla of the oviduct, not in the infundibulum, where fimbriae are located. Under normal circumstances, the trilaminar germ disk stage occurs after the blastocyst is implanted in the wall of the uterus, and is not present in the oviduct (see Chapter 19 III A l) .
10 . C. Immature teratomas are fast-growing malignant tumors. The other teratomas listed are usually benign, but even those that do become malignant are slow growing (see Chapter 19 VI B 4) .
349
Male Reproductive System
I. OVERVIEW-MALE REPRODUCTIVE SYSTEM
A. The male reproductive system consists of the testes, genita l ducts, accessory genital glands (semina l vesic les, prostate g land , and bulbourethra l g lands), and the penis .
B. Function . The male reproductive system produces spermatozoa (sperm), testosterone, and semina l fl u i d . Seminal fluid transports and nourishes the sperm as they pass through the excretory ducts. The penis delivers sperm to the exterior and also serves as the conduit for excretion of urine from the body.
The paired testes develop in the abdominal cavity and later descend into the scrotum, where they are suspended at the ends of the spermatic cords. They are the sites of spermatogenesis and production of the male sex hormones, primarily testosterone (Figure 20. 1 ) .
llYft�MfB cryptorch id ism
1 . C rypto rch i d i sm is a deve l o pmenta l d efect c h a ra cte r ized by fa i l u re of one or both testes to descend i nto th e s c rotum . The c h a n c e of th is h a ppen i n g i n fu l l -term b i rths is 1 % , whereas it r ises to a 30% c h a n c e i n p remature b i rths .
2. Th is c ond iti on resu lts i n ste ri l ity b e c a use the tem p e rature of the u ndescended testes ( i . e . , n o rm a l body tem p e ratu re ) i n h i b its spe rmatogen es is ; h oweve r, it does not affe ct testoste ron e prod u ctio n .
3. I t is associated with a m u c h h i g h e r i n c i d ence o f testicu lar mal ignancy th a n i n n o rm a l ly d e scended testes .
4. It can be surg ica l ly corrected . I n o rd e r to avo id c omp l i c ati ons l ate r on i n l ife, the u sua l re commendati o n is that t he su rge ry be p e rfo rmed p r i o r t o th e a g e o f o ne, assum ing that the ch i l d is h e a lthy enough fo r the p ro c e d u re .
350
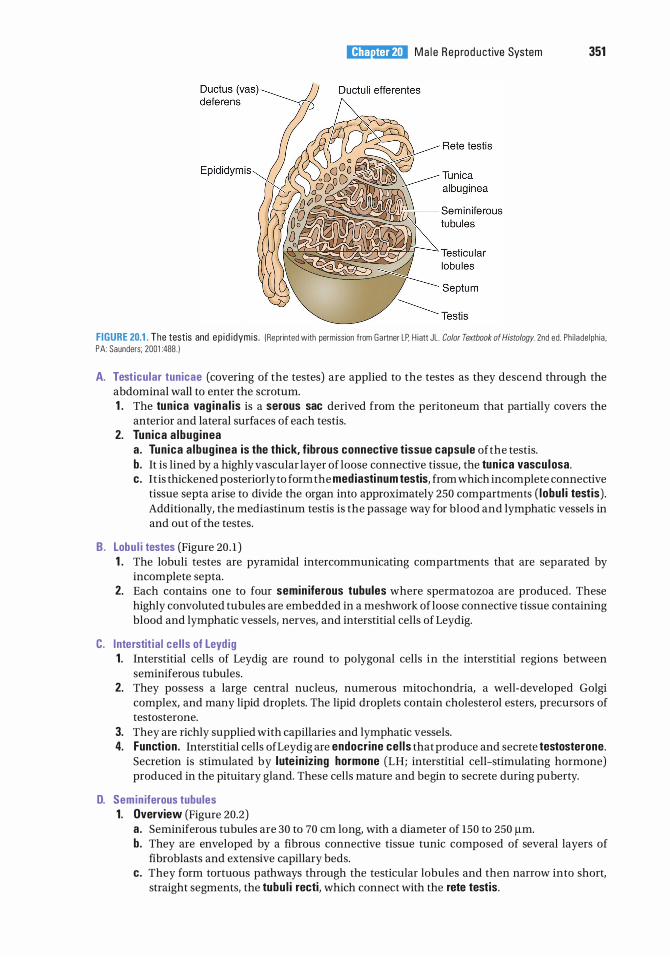
l!1lllJ1ttlfl!l Ma l e Rep rod u ctive System 351
FIGURE 20.1 . The testis and ep i d idymis . (Reprinted with permission from Ga rtner LP. H iatt JL . Color Textbook of Histology. 2nd ed . Ph i l ade lph ia . PA : Saunders; 2001 :488 . )
A. Testicular tunicae (covering of the testes) are applied to the testes as they descend through the abdominal wall to enter the scrotum. 1 . The tun ica vag ina l is is a serous sac derived from the peritoneum that partially covers the
anterior and lateral surfaces of each testis. 2. Tunica a lbug inea
a . Tun ica a lbug inea is the thick, fibrous connective tissue capsule of the testis. b. It is lined by a highly vascular layer of loose connective tissue, the tun ica vascu losa. c . It is thickened posteriorly to form the med iasti num testis, from which incomplete connective
tissue septa arise to divide the organ into approximately 250 compartments ( lobu l i testis) . Additionally, the mediastinum testis is the passage way for blood and lymphatic vessels in and out of the testes.
B. Lobu l i testes (Figure 20 . 1 ) 1 . The lobuli testes are pyramidal intercommunicating compartments that are separated by
incomplete septa. 2. Each contains one to four semin iferous tubules where spermatozoa are produced. These
highly convoluted tubules are embedded in a meshwork of loose connective tissue containing blood and lymphatic vessels, nerves, and interstitial cells of Leydig.
C. Interstit ia l cel ls of Leyd ig 1 . Interstitial cells of Leydig are round to polygonal cells in the interstitial regions between
seminiferous tubules. 2. They possess a large central nucleus, numerous mitochondria, a well-developed Golgi
complex, and many lipid droplets. The lipid droplets contain cholesterol esters, precursors of testosterone.
3. They are richly supplied with capillaries and lymphatic vessels. 4. Function . Interstitial cells of Leydig are endocrine ce l ls that produce and secrete testosterone.
Secretion is stimulated by lute in iz ing hormone (LH; interstitial cell-stimulating hormone) produced in the pituitary gland. These cells mature and begin to secrete during puberty.
D. Semin iferous tubules 1 . Overview (Figure 20.2)
a. Seminiferous tubules are 30 to 70 em long, with a diameter of 150 to 250 J.Lm. b. They are enveloped by a fibrous connective tissue tunic composed of several layers of
fibroblasts and extensive capillary beds. c. They form tortuous pathways through the testicular lobules and then narrow into short,
straight segments, the tubu l i recti, which connect with the rete testis.
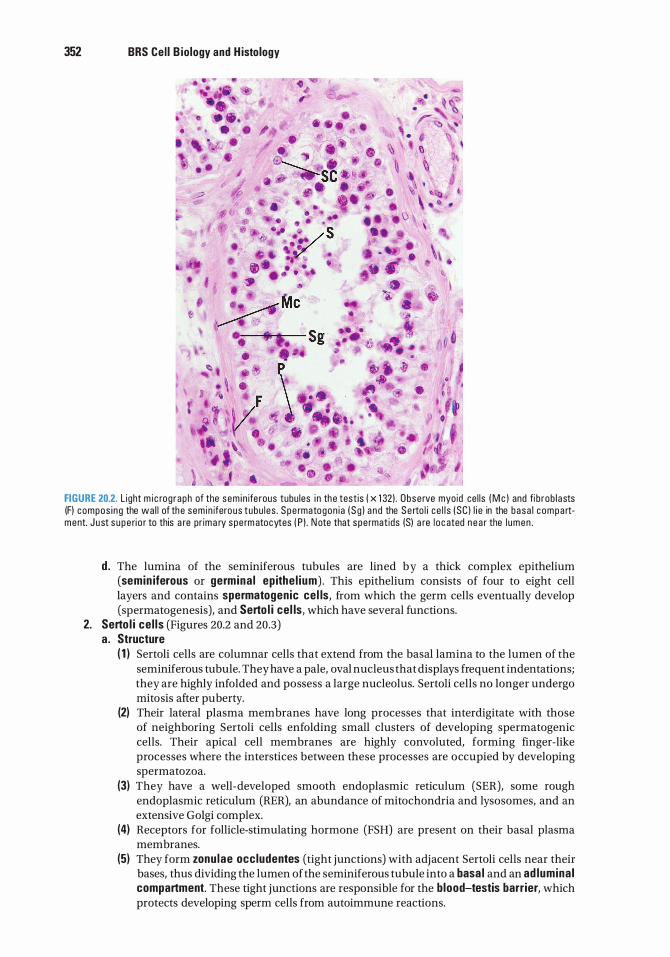
352 BRS Cel l B iology and H istology
FIGURE 20.2. L ight m i c rog raph of the sem i n ife rous tubu les i n the test is j x 1 32) . Obse rve myoid ce l ls ( M e ) and fi b rob l asts (F) compos i ng the wa l l of the sem in iferous tubu l es . Spe rmatogon i a ( Sg ) a nd the Se rto l i c e l l s (SC ) l i e in the basa l compa rtment. J ust s upe ri o r to this a re pr ima ry spe rm atocytes ( P ) . N ote that spe rmat ids (S) a re l oc ated n e a r the l umen .
d . The lumina of the seminiferous tubules are lined by a thick complex epithelium (semin iferous or germina l ep ithe l ium) . This epithelium consists of four to eight cell layers and contains spermatogenic cel ls, from which the germ cells eventually develop (spermatogenesis), and Serto l i cel ls, which have several functions.
2. Serto l i ce l ls (Figures 20.2 and 20.3) a. Structure
( 1 ) Sertoli cells are columnar cells that extend from the basal lamina to the lumen of the seminiferous tubule. They have a pale, oval nucleus that displays frequent indentations; they are highly infolded and possess a large nucleolus. Sertoli cells no longer undergo mitosis after puberty.
(2) Their lateral plasma membranes have long processes that interdigitate with those of neighboring Sertoli cells enfolding small clusters of developing spermatogenic cells. Their apical cell membranes are highly convoluted, forming finger-like processes where the interstices between these processes are occupied by developing spermatozoa.
(3) They have a well-developed smooth endoplasmic reticulum (SER), some rough endoplasmic reticulum (RER), an abundance of mitochondria and lysosomes, and an extensive Golgi complex.
(4) Receptors for follicle-stimulating hormone (FSH) are present on their basal plasma membranes.
(5) They form zonu lae occludentes (tight junctions) with adjacent Sertoli cells near their bases, thus dividing the lumen of the seminiferous tubule into a basa l and an ad lumina l compartment. These tight junctions are responsible for the blood-testis barrier, which protects developing sperm cells from autoimmune reactions.

Testis
l!1lllJ1ttlfl!l Ma l e Rep rod u ctive System 353
Semin iferous tubule
Junctional complex
Adluminal compartment
-- Junctional complex } Basal compartment
FIGURE 20.3. The sem in ifero us ( ge rm ina l ) e p ithe l i um . N ote the i nterce l l u l a r b r i dges between spe rm ato cytes and the j u nc tio na l c omp lexes n e a r the bases of ad jac ent S e rto l i c e l ls . These j u n ctio na l c omp lexes of t he Se rto l i ce l l s d i v i d e the ep ithe l i um into a n a d l u m i n a l and a basa l c o m p a rtment. !Reprinted with permiss ion f rom Krause WJ. Cutts JH . Concise Text of Histology.
2nd ed . Ba lt imore. MD : Wi l l i ams & Wi lkins; 1 986:4 1 4 )
b. Function (1 ) Sertoli cells support, protect, and nourish the spermatogenic cells. (2) They phagocytose excess cytoplasm discarded by maturing spermatids. (3) They secrete a fructose-rich fluid into the lumen that nourishes and facilitates the
transport of spermatozoa through the seminiferous tubules to the genital ducts. (4) They synthesize androgen-b ind ing prote in (ABP) under the influence of FSH. ABP
assists in maintaining the necessary concentration of testosterone in the seminiferous tubule so that spermatogenesis can progress.
(5) They secrete i nh ib in , a hormone that inhibits the synthesis and release of FSH by the anterior pituitary, as well as the hormone activin which boosts FSH release from the anterior pituitary.
(6) They establish a blood-testis barrier. (7) During fetal development they synthesize and release antimiil ler ian hormone, which
determines maleness. (8) They manufacture and release testicu lar transferrin , a protein that facilitates the
transfer of iron from serum transferrin to maturing spermatogenic cells. 3. Spermatogenesis
a . Shortly before puberty, the rise i n gonadotrophins i n itiates spermatogenesis, the process of spermatozoon (sperm) formation . It is divided into three phases : (1 ) Spermatocytogenesis-differentiation of spermatogonia into primary spermatocytes. (2) Meiosis-reduction division to reduce the diploid chromosomal complement of
primary spermatocytes to form haploid spermatids (see Chapter 2 XI) . (3) Spermiogenesis-transformation of spermatids into spermatozoa.

354 BRS Cel l B iology and H istology
b. Spermatogenesis does not occur simultaneously or synchronously in all seminiferous tubules, but rather in wavelike sequences of maturation, referred to as cycles of the semin iferous ep ithe l i um.
c. During spermatogenesis, daughter cells remain connected to each other via i nterce l l u la r br idges. The resultant syncytium may be responsible for the synchronous development of germ cells along any one seminiferous tubule.
4. Spermatogenic ce l ls (Figure 20.2) a . Spermatogonia are d ip lo id germ cells adjacent to the basal lamina of the seminiferous
epithelium. At puberty, testosterone influences them to enter the cell cycle. (1 ) Pale type A spermatogon ia possess a pale-staining nucleus, spherical mitochondria,
a small Golgi complex, and abundant, free ribosomes. They are mitotical ly active (starting at puberty) and give rise either to more cells of the same type (to maintain the supply) or to type B spermatogonia.
(2) Dark type A spermatogonia represent mitotically inactive (reserve) cells (in the G0 phase of the cell cycle, see Figure 2.6), with dark nuclei; they have the potential to resume mitosis and produce pale type A cells.
(3) Type B spermatogonia undergo mitosis and give rise to primary spermatocytes. b. Spermatocytes
(1 ) Primary spermatocytes are large d ip lo id cells with 4cDNA content. They undergo the fi rst meiotic d ivision (reductional division) to form secondary spermatocytes (see Chapter 2) .
(2) Secondary spermatocytes are haploid cells with 2cDNA that quickly undergo the second meiotic d ivision (equatorial division), without an intervening S phase, to form spermatids.
c. Spermatids ( 1 ) Spermatids are small hap lo id cells containing only 1 cDNA. (2) They are located near the lumen of the seminiferous tubule. (3) Their nuclei often display regions of condensed chromatin. (4) They possess a pair of centrioles, mitochondria, free ribosomes, SER, and a well
developed Golgi complex. 5. Spermiogenesis is a unique process of cytod ifferentiation, whereby spermatids shed much
of their cytoplasm and transform into spermatozoa, which are released into the lumen of the seminiferous tubule. Spermiogenesis is divided into four phases. a . Go lg i phase
( 1 ) The Golgi phase is characterized by the formation of an acrosoma l granu le , enclosed within an acrosomal vesic le, which becomes attached to the anterior end of the nuclear envelope of a spermatid.
(2) In this phase, centrioles migrate away from the nucleus to form the f lagel la r axoneme. Centrioles then migrate back toward the nucleus to assist in forming the connecting p iece associated with the tail.
b. The cap phase is characterized by expansion of the acrosomal vesicle over much of the nucleus, forming the acrosoma l cap.
c . Acrosomal phase is characterized by the following: ( 1 ) The nucleus becomes condensed, flattened, and located in the head region. (2) Mitochondria aggregate around the proximal portion of the flagellum, which develops
into the middle piece of the tail. (3) The spermatid elongates; this process is aided by a temporary cylinder of microtubules
called the manchette . (4) The acrosomal phase ends as the spermatid is oriented with its acrosome pointing
toward the base of the seminiferous tubule. d . Maturation phase is characterized by the fo l l owing :
( 1 ) Loss of excess cytoplasm and intercellular bridges connecting spermatids into a syncytium. The discarded cytoplasm is phagocytosed by Sertoli cells.
(2) Maturation phase ends when the nonmoti l e spermatozoa are released (tail first) into the lumen of the seminiferous tubule. Spermatozoa remain immotile until they leave the epididymis. They become capacitated (capable of fertilizing) in the female reproductive system.

l!1lllJ1ttlfl!l Ma le Reprodu ctive System 355
6. Spermatozoon a . Head of the spermatozoon (Figure 20.4)
(1 ) The spermatozoon head is flattened and contains a dense, homogeneous nucleus with 23 chromosomes: (22 plus the Y chromosome or 22 plus the X chromosome) .
(2) It also possesses the acrosome, which contains hydro lyt ic enzymes (e.g., acid phosphatase, neuraminidase, hyaluronidase, and proteases) that assist the sperm in penetrating the corona radiata and zona pellucida of the oocyte (see Chapter 19) . Release of these enzymes is termed the acrosomal reaction .
b . Ta i l of the spermatozoon includes the neck, middle piece, principal piece, and the end piece. (1 ) The neck includes the centrioles and the connecti ng p iece, which is attached to the
nine outer dense f ibers of the remainder of the tail. (2) The midd le p iece extends from the neck to the annu lus and contains the axoneme, nine
outer dense fibers, and a spirally arranged sheath of mitochondria . (3) The pr inc ipal p iece extends from the annulus to the end piece and contains the
axoneme with its surrounding dense fibers, which in turn are encircled by a fibrous sheath that has circumferential ribs.
(4) The end piece consists of the axoneme and the surrounding plasma membrane.
lin'#IBI Test icu lar cancer
1 . M ost often atta c ks m e n younge r th a n 40 yea rs of age a n d is the most common c a n c e r of men between th e ages of 20 and 34 yea rs.
2. U s u a l ly p resent a s swe l l i n g s i n the s c rotum . 3 . Those with m a l i g n a n cy typ i c a l ly h ave e l evated b l ood a-feto p rote i n a n d h u m a n c ho ri o n i c
g onadotro p i n ( h C G ) l eve ls . 4. S u rg i c a l remova l of the affe cted testis is the common tre atment. 5. Testi c u l a r c a n c e r that h a s metastas i zed n e cess itates rad iati on th era py a n d c h emothe ra py.
Head [ ] Acrosomal I • Cel l membrane cap • Acrosome
• N ucleus
J Neck
J Middle ploce - �� • Cel l membrane • M itochondrial sheath • Nine outer dense f ibers o o () • Axoneme (ci l i u m with
9 + 2 arrangement)
Tai l
� • Cel l membrane • Fibrous sheath
Principal p iece---+ • Seven outer dense f ibers • Axoneme
J Eod piece ---+ • � • • Cel l membrane • Axoneme
FIGURE 20.4. A h u m a n sperm. Reg ions of the m ature spe rm are shown on the l eft. D i a g rams of sections thro u g h the head a n d the ma jo r segments of the ta i l a re shown on t he r ig ht. IReprinted with permiss ion from Henrikson R C . Kaye G l . Mazurkiewicz J E . Histology National Medical Series for Independent Study. Ba lt imore. MD : Wi l l i ams & Wi l kins ; 1 997:399. )

356 BRS Cel l B iology and H istology
E. Regulation of spermatogenesis 1. Critica l testicu lar temperature is 35°C for spermatogenesis. Testicular arteries that arise from
the aorta accompany the testes into the scrotum, providing each testis with a vascular supply. As these convoluted arteries approach the testes, they are surrounded by a pampin iform p lexus of ve ins that dissipates the heat of the arterial blood, resulting in its temperature being reduced to 35°C. (See Section II, Cl in ica l Considerations in this chapter.)
2. Hormonal i nteractions (Figure 20.5) a . Certa in neurons i n the hypotha lamus produce luteinizing hormone-releasing hormone
(LHRH) , also known as gonadotropin-releasing hormone (GnRH) . LHRH initiates the release of LH and FSH from the adenohypophysis.
b. Stimu lation of testicu lar hormone production is effected by these two pituitary gonadotropins. (1 ) LH stimulates the interstitial cells of Leydig to secrete testosterone. (2) FSH promotes the synthesis of ABP by Sertoli cells.
c. Testosterone is necessary for the normal development of not only male germ cells but also secondary sex characteristics.
d . ABP binds testosterone and maintains it at a high concentration in the seminiferous tubule to facilitate succession of spermatogonia into spermatozoa; it can also bind estrogens, thus inhibiting spermatogenesis.
Hypothalamus ! LHRH a. The hypothalamus
� I produces LHRH r � which in it iates the
b.(2) FSH p romotes the synthesis of ABP by Serto l i cel ls.
release of LH and FSH from the adenohypophysis.
b.(1 ) LH sti m u lates the i nterstitial Leyd ig cel ls to secrete testosterone.
\ d. ABP binds
testosterone and mai ntains it at a h igh concentrat ion.
e.(2) l nh ibin, a hormone secreted by Sertol i cells, inh ibits -+-�-\\ FSH release.
e.(1 ) Excessive levels of testosterone i n h ibit LH release.
c. Testosterone is necessary for normal development.
Leyd ig cel ls
FIGURE 20.5. The hormona l contro l of testicu la r function . Note the feedback inh ibition of the p itu ita ry by testi cu l a r hormones. LH RH, luteinizing hormone-re leas ing hormone; LH, luteinizing hormone; FSH, fo l l i c le-stimu lating hormone ABP, androgen· b ind ing prote in .

l!1lllJ1ttlfl!l Ma le Reprodu ctive System 357
e. Inh ib it ion and stimulation of FSH and LH release (1 ) Excessive levels of testosterone inhibit LH release. (2) lnh ib in , a hormone secreted by Sertoli cells, inhibits GnRH, and, thereby, FSH release
from the hypophysis. (3) Activin, also secreted by Sertoli cells, stimulates the release of GnRH and, thereby, FSH
release.
CLIN ICAL CONSIDERATIONS
Hyperthermia i s a ma jo r fa cto r t h a t resu lts i n ste r i l ity i n m a l es . S p e rm p rod u ctio n is h eat sensitive . The o ptimum tem p e rature fo r s pe rm p ro d u ctio n
i s 35°C. Hen ce , t he testes a re housed i n th e sc rotum as o p posed t o be i n g housed with i n th e body, where th e tempe ratu re wou ld be a round 37°C . It h a s been repo rted that ma l e s who o pe rate l a pto p c omputers s ituated i n th e i r l a p s fo r a n h o u r a re i n c reas i ng th e i r i ntras c rota l tem p e ratu res by as much a s 2 .8°C . Although these stu d i es a re not defi n it ive, it m i g ht be wise fo r young ma les to l im it the use of l a pto p compute rs i n th e i r l aps fo r exte nded tim e pe riods .
A. l ntratesticu lar ducts 1 . The continuation of the seminiferous tubules are the tubu l i recti, short, straight tubules lined
by Sertoli cells in their proximal half and lined by a simple cuboida l ep ithe l ium in their distal half. These cuboidal cells possess microvi l l i , and some display a single flage l lum.
2. Rete testis i s a labyrinthine plexus of anastomosing channels within the mediastinum testis lined by a simple cuboidal ep ithe l i um; many of the cells possess microvilli as well as a single luminal flage l l um .
t a b I e 20.1 H isto logy and Functions of th e Ma le Gen ita l D u cts
Duct Epithel ium Connective Tissue Muscle layers
Tubu l i re cti Se rto l i c e l l s i n p roxima l ha lf; Loose No smooth musc l e s imp l e c u bo i da l ep ithe l i um i n d ista l h a lf
Rete testis S imp l e cubo i da l ep ithe l i um Vascu l a r N o smooth musc l e
D u ctu l i Reg ions of c i l i ated co l umna r Th i n , loose Th in layer of c i r cu l a rly effe rentes ce l l s a lternati ng with arra nged smooth musc l e
unc i l iated cubo i da l ce l l s ce l l s
Ep id idymis Pseudostratifi ed ep ithe l i um Th i n , l oose Layer of c i r c u l a rly composed of ta l l p r i nc i pa l a rra nged smooth musc l e ce l l s with stereoc i l i a , short ce l l s basa l ce l l s
D u ctus (vas ) Pseudostratifi ed Loose, fi b roe l ast ic Th i c k three- layer smooth d eferens stereoc i l iated co l umna r musc l e coats: i n ne r a nd
ep ithe l i um oute r l on g itud i na l ; m i dd l e c i r cu l a r
Eja cu l atory S imp l e co l umna r ep ithe l i um Subep ith e l i a l ; th rown No smooth musc l e d u ct i nto fo lds, g iv ing
lumen i r re gu l a r appea rance
Function
Conduct spe rmatozoa from sem in iferous tubu les to rete testis
Conduct spermatozoa from tu bu l i re cti to d u ctu l i effe rentes
Conduct spe rmatozoa from rete testis to ep id idymis
Conduct spe rmatozoa from d u ctu l i effe rentes to d u ctus deferens
De l iver spermatozoa from ta i l of ep i d idymis to eja c u l atory d u ct
De l iver spe rmatozoa, sem ina l fl u i d to p rostatic u rethra at co l l i c u l u s sem ina l i s

358 BRS Cel l B iology and H istology
B . Extratesticular ducts 1 . Ductu l i efferentes
a . Ductuli efferentes are a collection of 10 to 20 tubules leading from the rete testis to the ductus epididymis. Therefore, the ductuli efferentes begin as intra testicular ducts, leave the testicles, and their distal portions may be considered to be extra testicular ducts.
b. They possess a thin circular layer of smooth muscle beneath the basal lamina of the epithelium, which is responsible for peristaltic movements.
c. They are lined by a simple ep ithe l ium composed of a lternati ng c lusters of nonci l i ated cuboidal ce l ls and c i l iated columnar cel ls. The arrangement of epithelial cells of two different heights imparts a characteristic festooned appearance to the luminal outline of the ductuli efferentes.
d . Function . Ductuli efferentes reabsorb fluid from the semen and form the head of the ep id idymis.
2. Ductus ep id idymis (Figure 20.6) a. Ductus epididymis, together with the ductuli efferentes, constitutes the epid idymis. b . It is surrounded by c i rcu lar layers of smooth muscle that undergo perista ltic contractions,
which assist in conveying sperm toward the ductus deferens. c. It is lined by a pseudostratified columnar epithe l i um, which is supported by a basal lamina
and contains the following two cell types : (1 ) Basal cells are round and, morphologically, appear to be undifferentiated; they serve as
precursors of the principal cells. (2) Principal cells, which are columnar and possess nonmotile stereocilia (long, irregular
microvilli) on their luminal surfaces (a) These cells possess a large Golgi complex, RER, lysosomes, and many apical
pinocytotic and coated vesicles.
FIGURE 20.6. Light m i c rog raph of the ep i d idymis ( x 270l . Obse rve the sho rt basa l ce l l s ( B C l and the c o l u m n a r p r i n c i pa l c e l l s ( PC ) l i n i ng the l umen of the ep i d idymis . Ste reoc i l i a ( a rrows) proj e ct i nto the l umen p a c ked with spe rmatozoa (S l .

l!1lllJ1ttlfl!l Ma l e Rep rod u ctive System 359
(b ) Principal cells function, in concert with the ductuli efferentes, to absorb nearly 90% of the testicular fluid.
(c) They secrete various factors that facilitate sperm maturation; however, they also produce g lycerophosphochol i ne, which inhibits capacitation (the process whereby a sperm becomes capable of fertilizing an oocyte) . Thus, capacitation occurs only after the sperm enters the female genital tract.
3. Ductus (vas) deferens a . The ductus deferens, which begins at the tail of the epididymis, has a th ick muscu lar wa l l
with inner and outer layers o f longitudinal smooth muscle, which are separated from one another by a middle circular layer.
b. It possesses a narrow, irregular lumen lined by pseudostratified columnar ep ithe l ium similar to that of the ductus epididymis.
4. Ejacu latory duct a. The ejaculatory duct is the straight continuation of the ductus deferens beyond where it
receives the duct of the seminal vesicle. b. It lacks a muscular wall. c. It enters the prostate gland and terminates in a slit on the co l l iculus semina l is located in
the prostatic urethra.
A no rma l s pe rm count fo r a s i n g l e ej a c u l ate is a p p roxim ately 50 to CLIN ICAL CONSIDERATIONS 1 00 mi l l i o n spe rm atozoa/ml. An i n d ivi d u a l with a spe rm count o f l e s s tha n
2 0 mi l l i o n s pe rmatozoa/m l. o f ej a c u l ate i s cons i de red t o be ster i le .
Include the paired seminal vesicles, prostate gland, and the paired bulbourethral glands
A. Seminal vesic les 1. Epithelium
a. Epithelium of the seminal vesicles is pseudostratif ied columnar, with a height that varies with testosterone levels; it lines the extensively fo lded mucosa.
b . It contains many yel l ow l i pochrome p igment g ranules and secretory granules, a large Golgi complex, many mitochondria, and abundant RER.
2. The lamina propria consists of f ibroelastic connective tissue surrounded by an inner circular and outer longitudinal layer of smooth muscle.
3. The adventitia is composed of f ibroelastic connective tissue. 4. The seminal vesicles secrete a yellowish, viscous fluid containing substances that activate
sperm (e.g., fructose providing the energy source for the sperm); this fluid constitutes about 70% of the human ejaculate.
5. The duct of the seminal vesicle joins the ductus deferens at its ampulla (the enlarged terminal end), thus forming the right and left ejaculatory ducts that enter the prostate gland continuing to the urethra.
B. Prostate g land (Figure 20.7) 1. Overview
a. The prostate gland surrounds the urethra as it exits the urinary bladder. b. It consists of30 to 50 discrete branched tubu loa lveolar g lands that empty their contents via
excretory ducts into the prostatic urethra. These glands are arranged in three concentric layers (mucosa l, submucosal , and main) around the urethra.
c. The gland is covered by a f ibroelastic capsule that contains smooth muscle. Septa from the capsule penetrate the gland and divide it into lobes.

360 BRS Cel l B iology and H istology
FIGURE 20.7. L ight m i c rog raph of the p rostate g l a nd ( x 1 32) . Note the prostrate conc retion ( Pe l . smooth musc l e ( a rrow) , and th e comp ressed c o l u m n a r ce l l s ( CC ) form i ng the g l a n du l a r pa renchyma .
2 . Ep ithe l ium a . The epithelium of the prostate gland is simple or pseudostratified columnar and lines the
individual glands that constitute the prostate. b. It is composed of cells that contain abundant RER, a well-developed Golgi complex,
numerous lysosomes, and many secretory granules. 3. Corpora amylacea are prostatic concretions, composed of glycoprotein, which may become
calcified; their numbers increase with age. 4. The prostate secretes a thin whitish fluid, a part of the semen containing proteolytic enzymes,
citric acid, acid phosphatase, fibrinolysin, and lipids. The prostatic secretion serves to liquefy the coagulated semen after it is deposited in the female genital tract. Its synthesis and release are regulated by dihydrotestosterone.
CLINICAL CONSIDERATIONS Ben ign p rostatic hypertrophy (BPH )
1 . B P H most common ly invo lves on ly a n e n l a rg ement o f t h e mucosal g lands. 2. I t is fre q uently asso c i ated with an i n a b i l ity to beg i n a n d cease u r i nati o n b e c a use the u reth ra is
p a rti a l ly stra n g u l ated by th e e n l a rg e d prostate . 3. It l e a ds to nocturia ( u r i n at ion at n i g ht) a n d sensory u rg e n cy (the d es i re to u r i n ate with out
hav ing to vo i d ) . 4. Th is d i sease is c ommon in o l d e r men , o c c u rri ng in a bout 50% of m e n o l d e r th a n 50 yea rs of a g e
a n d i n 9 5% o f th ose o l d e r th a n 8 0 yea rs o f a ge . B P H c a n be c o nfi rmed b y a d i g ita l recta l exa m i n ation ; howeve r, a b i o psy is req u i red to r u l e ou t p rostati c c a n c e r.

Adenocarc inoma of the prostate g land
l!1lllJ1ttlfl!l Ma le Rep roductive System 361
1 . Adenoca r c i n oma of the p rostate g l a n d may be i n d i c ated by p a l p ati o n th ro u gh th e rectu m . H oweve r, a b io psy is req u i re d fo r pos itive i d entifi c atio n o f th e d i sease .
2 . Although th is c a n c e r g rows s l owly, i t c ommon ly metastasizes to bone v ia th e c i r c u l ato ry system .
3 . I t o c c u rs i n a b o ut one -th i rd o f m e n o l d e r tha n 75 yea rs o f a g e a n d is t h e s e c o n d most c o m m o n form o f c a n c e r i n men .
4 . It i s assoc i ated with a n e l evated prostate-specific antigen (PSA) l eve l i n b l ood . M e n with e l evated PSA va l u es a re c a n d i d ates for mo re a g g ress ive d i a g nosti c tests fo r p rostati c c a n c e r. S u rg i c a l remova l with o r witho ut ra d i atio n th e ra py is the u sua l treatment. a lth o ugh th e re may be c omp l i c ati ons o f im pote n ce a n d/o r i n c onti n e n ce . N ewer p ro c e d u res ( e . g . , b ra c hyth e ra py) i n c l u d e ra d i o a ctive seed i ng with i n the g l a n d .
C . Bulbourethra l (Cowper) g lands 1 . Bulbourethral glands are adjacent to the membranous urethra. 2. They empty their viscous, slippery secretions into the lumen of the membranous urethra to
lubricate it just prior to the emission of semen. 3. The glands are lined by a simple cuboidal or columnar ep ithe l ium. 4. They are surrounded by a fibroelastic capsu le containing smooth and skeletal muscle.
CLIN ICAL CONSIDERATIONS
Vasectomy i s t h e chosen means o f p e rm a n e nt contra c e pti o n by mo re th a n 600,000 U S m a les e a c h yea r. A phys i c i a n may p e rform the p ro c e d u re
i n the offi ce , where th e sc rotum is s l it open , a p o rti o n of the s pe rm ati c c o rd is p u l l e d o ut, c ut, c a uter ized, a n d retu rned to th e s c rotum . At the c onc l us i on of 6 weeks or so, afte r the p ro c e d u re, semen is c o l l e cted and exam i ned to assu re that no spe rmatozoa a re ej a c u l ated . Th is p ro c e d u re i s n e a rly 1 00% effe ctive. The p ro c e d u re may h ave a few comp l i c ations, but they u s u a l ly d iss i pate afte r a s hort per i od of time .
The urethra conveys urine from the bladder t o outside the body. In males, the urethra also carries semen during ejaculation. It has a two-layered muscularis consisting of an inner longitudinal and an outer circular layer of smooth muscle. It is surrounded at some point by an externa l sphincter of ske leta l muscle, which permits its voluntary closure.
A. The male urethra is about 20 em long and is divided into prostatic, membranous, and cavernous portions.
B. It is lined by transitiona l epithe l ium in the prostatic portion and by pseudostratified or stratified co lumnar epithe l ium in the other two portions. The fossa navicularis, located at the distal end of the cavernous urethra, is lined by stratified squamous ep ithe l ium.
C. I t contains mucus-secreting g lands of Littre in the lamina propria.

362 BRS Cel l B iology and H istology
A. Corpora cavernosa 1. Corpora cavernosa are pai red masses of erectile tissue that contain i rregu lar vascu lar spaces
lined by a continuous layer of endothelial cells. These spaces are separated from each other by trabeculae of connective tissue and smooth muscle.
2. The vascular spaces decrease in size toward the periphery of the corpora cavernosa. 3. During erection, the vascular spaces become engorged with blood as a resultofparasympathetic
impulses, which constrict arteriovenous shunts and dilate the helicine arteries, thus increasing flow to the vascular spaces of the two corpora cavernosa and the single corpus spongiosum.
B. Corpus spong iosum 1. The corpus spongiosum is a single mass of erecti l e tissue that contains vascular spaces of
uniform size. 2. It possesses trabeculae that contain more elastic fibers and less smooth muscle than those of
the corpora cavernosa. 3. The penile portion of the urethra passes through the length of the corpus spongiosum, opening
to the exterior at the tip of the glans penis.
C. Connective tissue and skin 1. The tun ica a lbug inea is a thick, fibrous connective sheath that surrounds the paired corpora
cavernosa and the corpus spongiosum. The arrangement of dense collagen bundles permits extension of the penis during erection.
2. G lans penis a . The glans penis is the dilated distal end of the corpus spongiosum. b. It contains dense connective tissue and longitudinal muscle fibers. c. It is covered by retractable skin, the prepuce, which is lined by stratified squamous lightly
keratinized epithelium. 3. G lands of Littre are mucus-secreting glands present throughout the length of the penile
urethra.

Review Test
D irections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which one of the following functions is attributed to the Sertoli cells?
(A) Secretion of follicle-stimulating hormone (B ) Secretion of testosterone (C) Secretion of androgen-binding protein (D ) Secretion of LH (E ) Secretion of ABP
2. Which of the following statements concerning the cells of Leydig is true?
(A) They become functional at puberty. (B ) They are within the seminiferous tubules. (C) They are stimulated by FSH. (D ) They secrete much of the fluid portion of
semen. (E) They respond to inhibin.
3. Type A spermatogonia are germ cells that
(A) develop from secondary spermatocytes. (B) undergo meiotic activity subsequent to
sexual maturity. (C ) develop through meiotic divisions. (D ) give rise to primary spermatocytes. (E) may be dark or pale.
4. Which of the following statements is related to the ductus epididymis?
(A) It begins at the rete testis. (B ) It is lined by a pseudostratified columnar
epithelium. (C ) It secretes a large volume of fluid into its
lumen. (D) It possesses motile cilia. (E) It capacitates spermatozoa.
5. Testosterone is produced by
(A) interstitial cells of Leydig. (B ) Sertoli cells. (C) spermatogonia. (D ) spermatids. (E) spermatocytes.
6. Spermatozoa are conveyed from the seminiferous tubules to the rete testis via the
(A) ductus epididymis. (B ) tubuli recti. (C) ductuli efferentes. (D) ductus deferens. (E) ejaculatory duct.
7. Manchette formation occurs during which of the following phases of spermiogenesis?
(A) Meiotic phase (B) Maturation phase (C) Golgi phase (D) Cap phase (E) Acrosomal phase
8. The structural feature that best distinguishes the ductus deferens from the other genital ducts is its
(A) smooth-bore lumen. (B) thick wall containing three muscle layers. (C) lining of transitional epithelium. (D ) flattened mucosa. (E) nonmotile stereocilia.
9. Inhibin, a hormone that inhibits synthesis and release of FSH, is secreted by
(A) prostate gland. (B) Sertoli cells. (C) seminal vesicles. (D) bulbourethral glands. (E ) interstitial cells of Leydig.
363

364 BRS Cel l B iology and H istology
1 0. A 55-year-old man has urinary complications. He complains of difficulty urinating and reduced urinary flow. He also has an elevated prostate-specific antigen (PSA) level, along with palpable hard nodules on the prostate. The possible diagnosis is
(A) benign prostatic hyperplasia. (B ) adenocarcinoma of the prostate. (C) prostatic concretions. (D ) initiation of impotence. (E) incontinence.
1 1 . A 33-year-old man detected a swelling in his scrotum. Careful palpation did not reveal whether the swelling was associated with his testis. His physician ordered blood tests, and it was determined that he had increased levels of hCG in his blood. A probable diagnosis is
(A) benign lump. (B ) hematocele. (C) cryptorchidism. (D ) testicular cancer. (E ) hydrocele.

Answers and Explanations
1 . C. Sertoli cells have many functions, including the synthesis of ABP. Testosterone is secreted by the interstitial cells of Leydig, whereas FSH and LH (also known as interstitial cell-stimulating hormone) are secreted by the pituitary gland (see Chapter 20 II D 2) .
2. A. Interstitial cells of Leydig become functional at puberty as a result of the action of LH produced in the pituitary gland (see Chapter 20 II C) .
3. E. Type A spermatogonia, which may be pale or dark, are primitive germ cells. Pale type A spermatogonia become mitotically active at puberty and give rise to type B spermatogonia, which undergo mitoses, giving rise to primary spermatocytes (see Chapter 20 II D 4).
4. B . The ductus epididymidis begins at the termination of the ductuli efferentes and is lined by a pseudostratified columnar epithelium, which has principal cells that possess nonmotile stereocilia. These cells are involved in fluid resorption and secrete glycerophosphocholine, which inhibits capacitation (see Chapter 20 III B 2) .
5. A. The hormone testosterone is produced by the interstitial cells of Leydig (see Chapter 20 II C) .
6. B . The seminiferous tubules are connected to the rete testis by the tubuli recti (see Chapter 20 II D).
7. E. Spermiogenesis is the process of cytodifferentiation by which spermatids are transformed into spermatozoa. It does not involve cell division. Manchette formation occurs during the aerosomal phase of spermiogenesis (see Chapter 20 II D 5) .
8. B . The ductus (vas) deferens possesses three layers of smooth muscle in its wall, whereas the other genital ducts do not. Like the ductus epididymidis, the ductus deferens is lined by a pseudostratified columnar epithelium with principal cells that possess nonmotile stereocilia (see Chapter 20 III B 3) .
9. B . Inhibin is secreted by Sertoli cells (see Chapter 20 II D 2) .
1 0. B . Although some of the symptoms are characteristic of benign prostatic hypertrophy, rectal palpation indicating hard nodules, along with an elevated PSA level, indicates probable prostatic adenocarcinoma (see Chapter 20 IV B Clinical Considerations) .
1 1 . D. Palpable swellings in the scrotum, especially in men younger than 40 years of age, should be seen by a physician. Elevated blood serum levels of hCG and a-fetoprotein are usually associated with testicular cancer (see Chapter 20 II D Clinical Considerations) .
365

Special Senses
I. OVERVIEW-SPECIAL SENSE RECEPTORS
A. Special sense receptors are responsible for the five special senses : taste, smel l , seeing, hearing, and fee l ing (which includes touch, pressure, temperature, pain, and proprioception). The sense of smell is described in Chapter 1 5, and the sense of taste is described in Chapter 16. The remaining special senses are described here.
B. Function. Special sense receptors transduce stimu l i from the environment into e lectrica l impu lses.
A. Overview: Sensory receptors may be categorized into three groups : 1 . Exteroceptors-access information from the outside environment. 2. Proprioceptors-access information from muscles, tendons, and joint structures. 3. Interoceptors-access information from within the internal environment.
Additionally, receptors may be categorized according to the type of stimulus perceived.
366
1 . Mechanoreceptors-are activated as the receptor or tissue in which the receptor is located physically is deformed in some manner.
2. Thermoreceptors-are activated by either heat or cold. 3. Nociceptors, also known as pain receptors, are activated by painful stimuli such as extreme
temperatures that are hot or cold enough to cause damage to the tissues, pressure or touch that are intense enough to cause damage to the tissues. a . Specialized diffuse receptors are dendritic nerve endings in the skin, fascia, muscles, joints,
and tendons. b. They respond to stimuli related to deep touch, pressure, temperature, pa in , and
proprioception. c . These receptors are specialized to receive only one type of sensory stimulus, although
they will respond to other types of stimuli provided that the stimulus is sufficiently intense.
d . They are divided morphologically into free nerve terminals and encapsulated nerve end ings, which are ensheathed in a connective tissue capsule.

A 8
E
l!1llll'ttmfiii Spec i a l Senses 367
F
H FIGURE 21 .1 . Va r ious types of spec i a l ized rec e ptors. A. M erke l d isk . B. M e issne r co rpusc l e . C. Pac i n i a n co rpusc l e . D. Free n e rve end i ngs, n oc i c eptors, and thermore c e ptors. E. Ruffi n i co rpusc l e . F. Krause end bulb ( c o l d r eceptor) . G . N e u romusc u l a r sp i nd l e . H. Go l g i tendon o rgan .
B. Touch and pressure receptors 1 . Pacin ian corpuscles
a . Pacinian corpuscles are large, ellipsoid encapsulated receptors in the dermis and hypodermis and in the connective tissue of the mesenteries and joints.
b. They are especially abundant in the digits and breasts. c. They are composed of a multi layer capsule consisting of fibroblasts and collagen and
bathed in tissue fluid. The capsule surrounds an inner unmye l inated nerve termina l . d . They often resemble a sliced onion in histological sections. e. Function. Pacinian corpuscles perceive pressure, touch, and vibration .
2. Ruffin i end ings a . Ruffini endings are encapsulated receptors in the dermis and joints. b. They are composed of groups of branched terminals from myelinated nerve fibers and are
surrounded by a thin connective tissue capsule. c. Function. Ruffini endings function in pressure, stretch ing, and touch reception.

368 BRS Cel l B iology and H istology
3. Meissner corpuscles a . Meissner corpuscles are ellipsoid, encapsulated receptors in the dermal papillae of thick
skin, eyelids, lips, and nipples. b. They possess a connective tissue capsule that envelops the nerve terminal and its associated
Schwann cell. c. Function . Meissner corpuscles function in f ine touch perception.
4. Free nerve endings a . Free nerve endings are unencapsulated, unmye l inated terminations in the skin in
longitudinal and circular arrays around most of the hair follicles. b. Function . Free nerve endings function in touch perception.
5. Krause end bu lbs a. are encapsulated receptors located in the dermis, oral cavity, peritoneum, conjunctiva,
genital regions, connective tissues, nasal cavity, and in joints. They were thought to be cold receptors, but presently their function is unknown.
C. Temperature and pa in receptors 1 . Cold receptors respond to temperatures be low 25°C to 30°C . 2 . Heat receptors respond to temperatures above 40°C to 42°C . 3. Nociceptors
a . Nociceptors are sensitive to pa i n stimu l i from mechanical stress, extremes in temperature, or the presence of certain cytokines. When a stimulus is sufficiently strong to overload the normal receptor, that stimulus may trigger pain sensations by activating the nociceptors.
b. They are delicate myelinated fibers that lose their myelin before entering the epidermis.
D. Proprioceptive receptors (see Chapter 8 IV B and C) 1 . Go lg i tendon organs are encapsulated mechanoreceptors sensitive to stretch and tension in
tendons. 2. Muscle sp ind le receptors are 3 to 12 small encapsulated intrafusal muscle fibers called
f lower spray end ings and annu lospira l end ings that sense differences in muscle length and tension.
A. Overview 1. The eyes, housed in the bony orbits, are the photosensitive organs responsible for vision. 2. Each eye is composed of three tunics : the tunica f ibrosa (outer layer), tun ica vascu losa
(middle layer), and reti na . 3. I t receives l i ght through the cornea . The light is focused by the lens on the retina, which
contains specialized cells that encode the various patterns of the image for transmission to the brain via the optic nerve.
4. The eye possesses i ntrinsic muscles that adjust the aperture of the iris and alter the lens diameter, permitting accommodation for close vision.
5. The eye also possesses extri nsic muscles, attached to the external aspect of the eyeball, which move both eyes in a coordinated manner to perceive the desired visual fields.
6. The eyeball is continually moistened on its anterior surface with lacr imal f lu id (tears) secreted by the lacr imal g land .
7. The eyebal l is covered by the upper and lower eyelids, which protect its anterior surface.
B. Tunica fibrosa (see Figure 21 .2) 1. The outermost tunica fibrosa is composed of the sclera and the cornea. The sclera (the
white of the eye) is an opaque, relatively avascular fibrous connective tissue layer that covers the posterior five-sixths of the eyeball. The sclera receives insertions of the extrinsic ocular muscles.

Posterior segment of globe
l!1llll'ttmfiii Spec i a l Senses 369
Anterior segment of g lobe
�------------��------------�� Vitreous chamber (conta in ing vitreous hu mor)
' '
' Poster ior chamber
I ris
Cornea
Canal of Schlemm
Conjunctiva
I nferior rectus muscle
FIGURE 21 .2. Anatomy of the eyeba l l . (Adapted with permiss ion f rom McConne l l TH . The Nature of Disease. Ba lt imore . MD : L ipp incott Wi l l iams & Wilk i ns; 2007 680 I
2. The cornea is the transparent, highly innervated avascu lar anterior one-sixth of the tunica fibrosa. It joins the sclera in a region called the l imbus. The cornea is composed of five layers. a. Corneal ep ithe l ium
(1 ) The corneal epithelium lines the anter ior aspect of the cornea and is continuous with the conjunctiva (a mucous membrane covering the anterior sclera and lining the internal surface of the eyelids) .
(2) It is a stratified squamous non kerati n ized ep ithe l i um . (3 ) I t possesses microvi l l i in its superficial layer that trap moisture, protecting the cornea
from dehydration. (4) The corneal epithelium is highly innervated with free nerve endings.
b. Bowman membrane is a homogeneous nonce l l u l a r layer that provides form, stability, and strength to the cornea. The basal layer of the corneal epithelium is attached to Bowman membrane via hemidesmosomes.
c. Corneal stroma ( 1 ) The corneal stroma is the thickest corneal layer. It is composed of about five layers
of both type I and V co l l agen f ibers lying parallel to each other within each row and at oblique angles to each other in adjoining layers, thus forming a lattice. These collagen fibers are embedded in a ground substance composed mostly of chondroitin sulfate and keratan sulfate . A few fibroblasts are located between the laminae of collagen fibers.

370 BRS Cel l B iology and H istology
(2) The stroma has channels in the region of the limbus that are lined by endothe l ium, forming the canal of Sch lemm (see Figure 2 1 .2) . This canal drains fluid (aqueous humor) from the anterior chamber of the eye into the venous system.
d . Descemet membrane is a thick (5- 10 J..Lm) basal lamina that is interposed between the endothelium and the connective tissue stroma of the cornea.
e. Corneal endothe l ium ( 1 ) The corneal endothelium lines the poster ior aspect of the cornea beneath Descemet
membrane, where it separates the cornea from the aqueous humor in the anterior chamber of the eye.
(2) It is a simple squamous ep ithe l i um with cells that exhibit numerous pinocytic vesic les. (3) It resorbs f lu id from the stroma, thus contributing to the transparency of the cornea,
contributory to light refraction.
Cornea B e c a use the cornea is witho ut a b lood s up p ly and lym phat ics , th e co rnea
may be tra nsp l anted with o ut e l i c iti n g a n immune response tha t wou l d resu lt i n ti ssue rej e cti o n . Thus, it i s one of the m ost fre q uently donated ti ssues .
Cornea l Reflex (b l i nk response) A wisp of cotton that h as to u c h e d th e cornea wi l l c a use th e pati e nt to b l i n k. The b l i nk is a test of th e i nteg r ity of th e ophth a lm i c d iv is ion of the tr ig em i n a l n e rve (C r an i a l n e rve V) .
C. Tunica vascu losa (uvea, the midd le tun ic ) is composed of three parts : choroid, ciliary body, and iris. (see Figure 21 .2) 1. Choroid
a . The choroid is the h ighly vascu lar, p igmented layer of the eye on the posterior wall of the eyeball; its loose connective tissue contains many melanocytes.
b . It is loosely attached to the tunica fibrosa. c. Its deepest layer, Bruch membrane extends from the ora serrata to the optic disk and
separates the choriocapillary layer from the pigment epithelium. It is composed of two thin layers of collagen fibers with an intervening layer of elastic fibers. Both layers of collagen fibers are covered by basal laminae.
d . The choriocap i l l a ry layer contains the blood capillaries derived from the choroid stroma that supply the retina.
2. C i l ia ry body a . The ciliary body is the wedge-shaped anterior expansion of the choro id . b . I t completely encircles the lens and separates the ora serrata from the iris. c. It is lined on its inner surface by two layers of cells : an outer p igmented columnar ep ithe l ium
rich in melanin and an inner nonpigmented s imple columnar epithelium. (1 ) C i l i a ry processes
(a) are radially arranged extensions (about 70) of the ciliary body. (b) have a connective tissue core containing many fenestrated cap i l lar ies. (c) are covered by two epithelial layers. The nonpigmented inner layer transports
components from the plasma filtrate in the posterior chamber and thus forms the aqueous humor, which flows to the anterior chamber via the pupillary aperture (see Figure 2 1 .2) .
(d ) possess suspensory l igaments (zonulae) that arise from the processes and insert into the capsule of the lens, serving to anchor it in place.
(2) C i l i a ry muscle (a ) is attached to the sclera and ciliary body in such a manner that its contractions
stretch the ciliary body and release tension on the suspensory ligament and lens. Ciliary muscle contraction permits the lens to become more convex, allowing the

l!1llll'ttmfiii Spec i a l Senses 371
eye to focus on nearby objects (accommodation) . With advancing age, the lens loses its elasticity, thereby gradually losing the ability to accommodate.
3. Iris
(b) The ciliary muscle is innervated via parasympathetic f ibers of the oculomotor nerve (cranial nerve III) .
a. Overview (1 ) The iris is the most anterior extension of the choroid, separating the anterior and
posterior chambers of the eyeball (see Figure 2 1 .2) . (2) It incompletely covers the anterior surface of the lens, forming an aperture called the
pup i l that is continually adjusted by intrinsic pupillary muscles. (3) The iris is covered by an incomplete layer of pigmented cells and fibroblasts on its
anterior surface. (4) It has a wall composed of loose vascular connective tissue containing melanocytes and
fibroblasts. (5) The iris is covered on its deep surface by a two-layered epithelium possessing
pigmented cells that block light from entering the interior of the eye except via the pupil.
b. Eye color is blue only if few melanocytes are present. Increasing amounts of pigment impart darker colors to the eye.
c. D i l ator pup i l l ae muscle (1 ) Dilator pupillae muscle is a smooth muscle with fibers that radiate from the periphery
of the iris toward the pupil. (2) It contracts upon stimulation by sympathetic nerve fibers, d i l at ing the pup i l .
d . Sph incter pup i l l ae muscle (1 ) Sphincter pupillae muscle is smooth muscle arranged in concentric rings around the
pupillary orifice. (2) It contracts upon stimulation by parasympathetic nerve fibers of the oculomotor nerve
(cranial nerve III), constricti ng the pup i l .
D. Refractive med ia o f the eye 1 . Aqueous humor
a . Aqueous humor is a p lasmal ike f lu id in the anterior compartment of the eye that is formed by epithe l ia l cells l i n ing the c i l i a ry processes.
b . It is constantly secreted into the posterior chamber of the eye and then flows into the anterior chamber of the eye via the pupillary aperture; from there it enters the venous system via the canal of Schlemm (Figure 2 1 .2).
lin'!!�M!B G laucoma
1 . G l a u coma is a c ond it ion of a bno rm a l ly h igh intraocular pressure. I t i s c a used by obstructi ons that p revent d ra i nage of a q ueous humor f rom the eye v ia th e cana l of S ch l emm . G l a u c oma is the l e a d i n g c a use of b l i n d ness i n Afri c a n Ameri c a n s i n the U n ited States, and wor ldwide , i t i s the second l e a d i n g c a use of b l i n d ness afte r c ata ra cts. S ince i t is a n a g e - re l ated cond it ion , a bo ut 1 i n 10 pe rsons 80 yea rs of age h ave g l a u c o m a .
2 . Chronic g laucoma, t h e most common form o f g l a u c oma , may be assoc i ated with few sym ptoms exce pt fo r a g ra d u a l loss o f pe r i phe ra l vis i on . H oweve r, u s u a l ly, t h i s c ond itio n c a n be contro l l e d with med i c ati o n i n t h e form o f eye d rops .
2 . The l ens i s a biconvex transparent flexible structure composed of the lens capsule, subcapsular epithelium, and lens fibers (Figure 2 1 .3) . a. The lens capsule is a thick basal lamina that envelops the entire lens epithelium. b. The subcapsular ep ithe l ium (on the anterior and lateral lens surfaces only) is composed
of a single layer of cuboidal cells that communicate with each other via gap junctions and interdigitate with lens fibers.

372 BRS Cel l B iology and H istology
I • '
., ,'',/\' � . '.r-� 4
E
� / SL
\
FIGURE 21 .3. L ight m i c rog raph of the l ens of the eye ( X 1 32) . Obse rve the l ens ( L) , e p ithe l i um (E ) , suspensory l i g ament (SL) of the l ens, a nd th e c i l i a ry process (CP ) .
c. Lens f ibers represent highly differentiated, elongated cells that when mature lack both nuclei and organelles. Lens fibers are filled with a group of proteins called crysta l l i ns.
d . The suspensory l i gament stretches between the lens and the ciliary body, keeping tension on the lens and enab l ing it to focus on d istant objects.
3. The vitreous body is a refracti le gel composed mainly of water, collagen, and hyaluronic acid. This gel fills the interior of the globe posterior to the lens (Figure 2 1 .2).
lln'niJa cataract
1 . A cata ra ct is an opacity of the lens resu lti n g from the a c c umu l atio n of p i gm ent or oth e r sub sta n ces i n th e l ens fi b e rs that sc atte r t he l i g ht ente ri ng the l e ns, th us p reventi n g s h a rp fo cus i ng o f the l i g ht on the reti n a .
2 . Th i s c ond itio n is often assoc i ated with ag ing . 3. I f u ntreated , it l eads to a g r a dua l l oss of vis i on . 4 . When the o p a c ity becomes severe, a n ophth a l mo log ist may remove a n d re p l a c e the affe cted
l e ns with a man -made l e ns resto r ing c l e a r vis i on .
Presbyop ia Presbyop ia i s t h e i n a b i l ity o f t h e eye t o foc u s on c l o s e ob je cts ( a c commodation ) . Th is is usua l ly asso c i ated with a g i n g , s i n c e it i s re l ated to d e c reas i ng e l a sti c ity of the l e ns, which p revents it from assum ing a sphe r i c a l s h a pe . Th is c ond it ion can u sua l ly be c o rrected with eyeg l asses .

Eye Floaters (vitreous opac ities)
l!1llll'ttmfiii Spec i a l Senses 373
Age- re l ated c h a nges with the g e l - l i ke vitreous body becom i ng mo re l i q u i d c a use d e b ris with i n it to c l u m p, a n d as l i g ht passes th ro u gh the vitreous body, the d e b ris fo rms s h a dows on the reti n a that a p p e a r as b l a c k spots, strea ks, stri n gs, s p i d e rwebs, etc . , wh i c h move a b o ut i n th e vis u a l fi e l d s . These a re c a l l e d eye floaters, which can b e come an a nnoya n ce; howeve r, m ost peop l e l e a rn to d i s re g a rd th e m . U s u a l ly, they reso lve in a few weeks o r so . When eye f lo aters a re a c compan i e d by b r i ght fl a shes of l i g ht o r fuzzy v is ion , a n o p htha lmo l o g ist shou l d be consu lted a s th is may i n d i c ate a te a r i n the reti n a .
E. Retina (Figures 2 1 .4 and 21 .5) 1 . Overview
a. The retina is the innermost of the three tunicae of the eye and is responsible for photoreception . It is interposed between the choroid and the vitreous humor. ( 1 ) It is composed of two layers-a photosensitive layer containing rods and cones and several
intemeurons, and a nonsensitive pigmented layer housing melanin producing cells. (2) The photosensitive (visual) portion of the retina ends at the ora serrata, whereas the
nonsensitive (pigmented) portion continues anteriorly to cover the ciliary body and the posterior surface of the iris.
b. The retinal layer has a shallow depression in its posterior wall that contains only cones; this is an avascular region, called the fovea centra l is , whose central region, the macula , exhibits the greatest visual acuity (Figure 2 1 .2).
rrr Direction of l ight
FIGURE 21 .4. L ight m i c rog raph of the retin a (X 1 32) . Obse rve the c ho ro ids su per io r to the p i gmented ep ithe l i a l l ayer (C ) , the rods and cones, o ute r n u c l e a r layer ( O N L), the i n ne r n u c l e a r l ayer ( I N L) , a nd the gang l i o n layer ( G ) .

374 BRS Cel l B iology and H istology
Pigmented epithe l ium
Rod ----....
Outer l im it ing membrane
Cone -----�� Y-�1'
photoreceptor
Cone pedicle
Rod spherule
Bipolar cel l
Nuclei of MO i ler cel l
Body of ------!;,..__ MOi ler cel l
Optic nerve f ibers
fl Light from lens 0 FIGURE 21 .5. The layers of the reti n a . (Adapted with permiss ion from Gartner LP. H iatt JL . Color Textbook of Histology. 2nd ed . Ph i l ade lph ia , PA: Saunders; 200 1 : 5 1 8 . )
c. The retina displays 10 d istinct layers; later in the chapter, they are discussed in order from the outermost to the innermost.
d . Only certain of these lO cell layers are composed of neurons that receive, integrate, and relay or transmit impulses to the brain for processing. These include photoreceptor rods and cones, bipolar cells, and ganglion cells. Cells of the remaining layers function in supporting the architecture of the retina.
2. The reti na l p igment ep ithe l i um is a layer of columnar cel ls firmly attached to the Bruch membrane. a . Structure
(1 ) Retinal pigment epithelial cells have j unctional complexes and basa l invaginations that contain mitochondria, suggesting the involvement of these cells in ion transport.
(2) They contain smooth endoplasmic reticulum (SER) and many melan in granu les located apically in cellular processes.
(3) They extend pigment-fi l led microvi l l us processes that invest the tips of the rods and cones.
b. Function ( 1 ) Retinal pigment epithelial cells esterify vitamin A (used in the formation of visual
pigment by rods and cones) .

l!1llll'ttmfiii Spec i a l Senses 375
(2) They phagocytize the shed tips of the outer segments of rods. (3) They synthesize melanin , which absorbs light after the rods and cones have been
stimulated. (4) serve as the blood-retinal barrier.
3. The photoreceptor layer consists of neurons (photoreceptor cells) called rods and cones. a. Rods (sensitive to l i ght of low intens ity) (Figure 2 1 .5)
(1 ) Overview (a ) Rods possess four regions-outer and inner segments, a nuclear reg ion, and a
synaptic reg ion . (b ) They may synapse with bipolar cells, giving rise to summation . (c ) They possess an incomplete c i l ium terminating in a basal body within the inner
segment. (2) Outer segments of rods
(a) consist mainly of hundreds of flattened membranous d isks that contain rhodopsin, the visual pigment located in the discs of rods and discs of cones.
(b) eventually shed their disks, which are subsequently phagocytized by the pigment epithelial cells.
(3) Inner segments of rods possess mitochondria, glycogen, polyribosomes, and proteins, which migrate to the outer segments to be incorporated into the membranous disks.
(4) Photoreception by rods is initiated by the interaction of l i ght with rhodopsin (visual purple), which is composed of the integral membrane protein opsin bound to reti nal , the aldehyde form of vitamin A. (a ) The retinal moiety of rhodopsin absorbs l i ght in the visible range. (b ) Retinal dissociates from opsin. This reaction, called b leach ing, eventually closes
the Na+ channels, thus permitting diffusion of bound Ca2+ ions into the cytoplasm of the outer segment of a rod cell.
(c) Excess Ca2+ acts to hyperpolarize the cell because Na + is prevented from entering the cell.
(d ) Ion ic a lterations in the rod generate electrical activity, which is relayed to other rods via gap junctions.
(e) Dissociated retinal and opsin reassemble by an active process in which Muller and pigment epithelial cells also participate.
(f) Ca2+ is recaptured by the membranous disks, leading to reopening of the Na + channels and reestab l ishment of the normal resting membrane potential.
b. Cones (sensitive to l i ght of h igh intens ity) (Figure 2 1 .5) (1 ) Cones are much less numerous than rods, but produce g reater visual acu ity than do
rods; thus, the macula is populated only by cones. (2) They are generally similar in structure to rods and mediate photoreception in the same
way, with the following exceptions : (a ) The membranous disks in the outer segments of cones are invaginations of the
plasma membrane, whereas in rods they are not. (b) The proteins synthesized in the inner segments of cones are passed to the entire
outer segment, whereas in rods they are added only to newly forming disks. (c) Cones possess iodopsin in their disks. The amount of this photopigment varies in
different cones, making them differentially sensitive to red, green, or blue light. (d ) Each cone synapses with a sing le bipolar neuron, whereas each rod may synapse
with several bipolar neurons.
CLIN ICAL CONSIDERATIONS
Age-re lated macular degeneration (AMD) i s a d i sease o f the reti n a l o c ated i n t h e c e ntra l r e g i o n o f t h e m a c u l a , h e n c e affe cti ng c e ntra l vis i on .
As its name imp l ies , i t i s a d i sease of a g i n g , o c c u rr i ng u s u a l ly afte r the a g e of 50 yea rs . There a re two forms: d ry a n d wet A M D . Dry macular degeneration, the most c ommon, is where th e c e ntra l v is ion i s affe cted so tha t ob je cts b e come very b l u rred . Th i s is c a used by c e l l u l a r d e b ris ( d r usen ) t ha t a p p e a rs a s ye l low spots depos ited betwee n the c ho ro i ds a n d th e reti n a . Wet macular degeneration, the most

376 BRS Cel l B iology and H istology
severe, resu lts when sma l l b l ood vesse ls , formed between the c ho ro i d and the reti n a , l e a k i nto th is s p a ce c a us i ng th e reti n a to die; a s a resu lt, a b l i n d spot fo rms i n th e c e nter of the vi s u a l fi e l d . Wet m a c u l a r d e g ene rati o n exh i b its a q u i c k onset with a sma l l b l i n d spot that may q u i c kly p rog ress to a l a rg e r b l i n d spot. Although a n AM D pati e nt may be u n a b l e to re cogn ize a fa c e in th e c e nter of v is ion , i t is i nte resti n g to note that pe r i phe ra l v is ion is u n affe cted by m a c u l a r d e g ene rati on . Whi le th e re is no c u re, c e rta i n vita m i ns a n d h i g h doses of a ntioxi d a nts a n d z i nc may be o f some ben efit fo r d ry AMD , whereas l a se r su rge ry a n d i nj e ctions o f a nti a ng i o genes is d r ugs a re used t o m a n a g e wet A M D .
4 . External l im it ing membrane a . The external limiting membrane is not a true membrane, but an area where zonu lae
adherentes (belt desmosomes) are located between the photoreceptor cells and the retinal Muller cells (glial cells).
b. This membrane also contains microvilli that project from the Muller cells. 5. The outer nuclear layer consists primarily of the nuc le i of the rods and cones. 6. Outer p lexiform layer
a . The outer plexiform layer contains axodendritic synapses between the axons of photoreceptor cells and the dendrites of bipolar and horizontal cells.
b. It displays synaptic r ibbons within the rod and cone cells at synaptic sites. 7. The inner nuc lear layer contains the ce l l bodies of b ipo lar neurons, horizontal cells, amacrine
cells, and the nuclei of Muller cells. 8. Inner p lexiform layer
a . The inner plexiform layer contains axodendritic synapses between the axons of bipolar cells and the dendrites of ganglion cells.
b. The processes of amacrine cells are located in this layer. 9. The gang l ion ce l l layer contains the somata of gang l ion cel ls, which form the final link in
the retina's neural chain. There are two types of ganglion cells: the majority (about 97% of ganglion cells) are those that function in vision and a very small minority that function in the diurnal rhythm by projecting, indirectly, to the pineal body, informing that gland whether it is daylight or night (see Chapter 13 Section VII 2) . Only the ganglion cells that function in the sensation of vision are described here. a . Structure-Gang l ion ce l ls
( 1 ) Ganglion cells are typical neurons that project their axons to a specific region of the retina called the optic disk.
(2) These cells are midget. d iffuse, and stratifi ed gangl ion cel ls . b . Function-Gang l ion ce l ls. Ganglion cells are activated by hyperpo larization of rods and
cones and generate an action potentia l , which is transmitted to horizontal and amacrine cells and carried to the visual relay system in the brain.
10. The optic nerve f iber layer consists primarily of the unmyel inated axons of ganglion cells, which form the fibers of the optic nerve. As each fiber pierces the sclera, it acquires a myelin sheath.
1 1 . The inner l im it ing membrane consists of the terminations of Muller cell processes and their basement membranes.
llt'n�MfB Detachment of the reti na
1 . Reti n a l d eta c h ment o c c u rs when th e n e u ra l a n d p i gmented layers sepa rate from e a c h oth e r, for exam p le , a s a resu lt of a s u dden h a rd j o lt.
2. This c ond iti on c a n sometimes be treated s u c c essfu l ly by l a se r su rge ry. B ut extens ive sepa ratio n req u i res c ryosu rg e ry to prod u c e s u c cessfu l a d h es ion of the two layers . If reti n a l d eta c h m e nt i s l eft u ntreated , b l i n d ness may o c c u r, a n d often even with treatm ent, t h e r o d s a n d c o n e s d i e , l eav ing b l i n d spots i n th e visu a l fi e l d .

F. Accessory structures of the eye
l!1llll'ttmfiii Spec i a l Senses 377
1. Conjunctiva (transparent mucous membrane) a . The conjunctiva lines the eyelids and is reflected onto the anterior portion of the eyeball to
the cornea, where it becomes continuous with the corneal epithelium. b. It is a stratified columnar epithe l ium possessing many gob let ce l ls . c. It is separated by a basal lamina from an underlying lamina propria ofloose connective tissue.
lin'n�%1111 conjunctivitis
1 . Con jun ctivitis is an infl a m m ati o n of the conj u n ctiva prod u c i n g red s c l e ra and a d i s c h a rg e . 2 . I t may be c a used b y b a cter ia , v i ruses, p a ras ites, a n d a l l e rgens . 3. Some fo rms a re contag i o us a n d may c a use b l i n d ness i f l e ft u ntre ated .
2 . Eye l ids a . The eyelids are lined internally by conjunctiva and externally by skin that is elastic and
covers a supportive framework of tarsa l p lates. b . Eyelids contain highly modified sebaceous g lands (meibomian glands), smaller mod ified
sebaceous g lands (glands of Zeis), and sweat g lands (glands of Moll) . 3. Lacrimal apparatus (Figure 21 .6)
a. Lacrimal g land (1 ) The lacrimal gland i s a compound tubuloa lveolar g land with secretory units that are
surrounded by an incomplete layer of myoepithe l ia l cel ls . (2) Lacrimal f lu id (tears) is mostly water, and contains lysozyme, an antibacterial enzyme.
Tears drain from the lacrimal gland via 6 to 12 ducts into the conjunctival fornix, from
Lacrimal gland
Lateral palpebral
com missure
Lower eyel id
Excretory ducts
Pupi l
Upper eyel id
Caruncula lacrimal is
Lacrimal duct
Lacrimal sac
I ris Conjunctiva Puncta Nasolacrimal lacrimal ia duct
FIGURE 21 .6. Exte rna l a n atomy of the eye. IReprinted with permiss ion from H iatt JL , Gartner LP: Textbook of Head and Neck Anatomy. 4th ed . Ba lt imore , MD: L ipp incott Wi l l iams & Wilk ins ; 201 0 : 1 64 )

378 BRS Cel l B iology and H isto logy
which the tears flow over the cornea and conjunctiva, keeping them moist. Tears then enter the lacrimal puncta, leading to the lacrimal canaliculi.
b. Lacr imal cana l i cu l i are lined by a stratified squamous ep ithe l ium and unite to form a common canaliculus, which empties into the lacrimal sac.
c. The lacr imal sac is lined by a pseudostratif ied c i l i ated co lumnar ep ithe l ium. d . The nasolacr imal duct is the inferior continuation of the lacrimal sac and is also lined by a
pseudostratified c i l iated columnar ep ithe l ium. The duct empties into the floor of the nasal cavity.
The ear consists of three parts : the external ear, which receives sound waves; the midd le ear, through which sound waves are transmitted; and the i nterna l ear, where sound waves are transduced into nerve impulses. The vestibular organ, responsible for equilibrium, is also located in the inner ear.
A. External ear (Figure 21 .7) 1. The aur ic le (p inna ) is composed of irregular plates of e lastic carti lage covered by th in skin . 2 . The externa l aud itory meatus i s lined by skin containing hair follicles, sebaceous glands, and
ceruminous g lands, which are modified sweat glands that produce earwax (cerumen) . 3. Tympan ic membrane (eardrum)
a . The tympanic membrane is covered by skin on its external surface and by a simple cuboida l ep ithe l ium on its inner surface.
b. It possesses f ibroelastic connective tissue interposed between its two epithelial coverings. c. Function . The tympanic membrane transmits sound vibrations that enter the ear to the
ossicles in the middle ear.
Facial nerve Styloid process
Opening of aud itory tube into nasopharynx
Posterior semici rcular canal
Stapes Facial nerve
FIGURE 21 .7. The exte rna l , m i dd l e , a nd i nne r e a rs . IReprinted with permiss ion from H iatt JL . Gartner LP Textbook of Head and Neck Anatomy.
2nd ed . Ba lt imore . MD : Wi l l i ams & Wi lkins ; 1 987:309. )

B. Midd le ear (tympanic cavity) (Figure 2 1 .7)
l!1llll'ttmfiii Spec i a l Senses 379
1. The tympanic cavity contains the three bony ossicles (ma l leus, incus, and stapes), which transmit movements of the tympanic membrane (eardrum) to the oval window (a membranecovered opening in the bony wall of the cochlea) . a . The bony ossicles, mal leus, incus, and stapes, are attached to each other in a chain-like
formation between the tympanic membrane and the oval window, a membrane-covered opening in the bony labyrinth. The malleus is attached to the tympanic membrane, whereas the stapes is attached to the membrane of the oval window. The middle ossicle, the incus, is interposed between the malleus and the stapes. Small ligaments interconnect the ossicles. Two separate muscles, innervated by branches of individual cranial nerves, serve to control the functioning of these ossicles. The tensor tympani muscle maintains tension on the tympanic membrane and is innervated by a branch of the trigeminal nerve (cranial nerve V) . The staped ius muscle dampens the movement of the stapes on the membrane covering the oval window. It is innervated by a branch of the facial nerve (cranial nerve VII) .
b. The bony ossicles, a s a group, function in modulating movements o f the tympanic membrane and in amplifying the sound waves by applying pressure on the membrane covering the oval window in the cochlea.
2. The middle ear is connected to the nasopharynx via the aud itory tube (eustach ian tube) . a . It is lined by a simple squamous ep ithe l ium, which changes to pseudostratified c i l iated
columnar epithe l ium near its opening to the auditory tube. b. It has a lamina propria composed of dense connective tissue tightly adherent to the bony
wall.
liHniA!III Conductive hear ing loss
1 . Con d u ctive h e a ri ng loss resu lts from a d efect i n the c o n d u cti on of sound waves in th e exte rna l o r m i d d l e e a r.
2. It may be c a used by otitis media, a common infl a m m ati o n of the m i d d l e e a r; obstruction by a fore i g n body; o r otosc lerosis of the m i d d l e e a r.
C. I nterna l ear (a bony labyrinth with in the temporal bone) (Figure 21 .7) 1. The bony labyrinth, composed of the semicircular canals, vestibule, and cochlea, is filled with
peri lymph, and houses the membranous labyrinth, which is filled with endolymph. a . Semicircular canals house the semicircular ducts of the membranous labyrinth. b. The vestibu le houses the saccule and utric le . c . Cochlea
(1 ) The cochlea winds two and a half times around a bony core (the modio lus), which contains blood vessels and the spiral ganglion.
(2) It is subdivided into three spaces : the scala vestibu l i and scala tympani , which are both filled with perilymph, and the scala media, or cochlear duct, which is filled with endolymph.
2. The membranous labyrinth is filled with endo lymph and possesses various sensory structures that are special izations of the epithe l ium. a . Saccule and utric le (within the vestibule)
(1 ) Overview (a ) The saccule and utricle are saclike bodies composed of a thin sheath of connective
tissue lined by simple squamous ep ithe l ium. (b ) Each gives rise to a duct; the two ducts join, forming the endo lymphatic sac . (c ) They possess small, specialized regions, called maculae, which contain type I and
type I I neuroepithe l ia l ha i r ce l ls, supporting cells, and a gelatinous layer (oto l ithic membrane) .
(2) Vestibular hair cells (a) These neuroepithe l ia l ce l ls contain many mitochondria and a well-developed
Golgi complex.

380 BRS Cel l B iology and H istology
(b ) They possess 50 to 100 elongated, rigid stereoci l i a (sensory microvilli) arranged in rows and a single cilium (kinoc i l ium) . These cilia extend from the apical surface of the hair cells into the otolithic membrane. They function in the detection of l i near acceleration .
(c) Types of vestibular hair cells include the following: 1 . Type I ha i r cel ls (bulbar), which are almost completely surrounded by a cup
shaped afferent nerve ending 2. Type I I ha i r ce l ls (columnar), which make contact with sma l l afferent termina ls
containing synaptic vesicles (3) Supporting ce l ls are generally columnar and possess a round basal nucleus, many
microtubules, and an extensive terminal web. (4) The oto l ith ic membrane is a gelati nous layer of glycoprotein that contains small
calcified particles called oto l iths or otoconia . b . Semic ircu lar ducts are continuous with and arise from the utricle. The three semicircular
ducts are perpendicular to each other so that they can detect angu lar acceleration of the head in three-dimensional space (see Figure 2 1 .7) . (1 ) The ampul lae are dilated regions ofthe semicircular ducts near their junctions with the
utricle. (2) Cristae ampul lares
(a) are specialized sensory regions within the ampullae of the semicircular ducts. (b) are similar to maculae but have a thicker, conical glycoprotein layer (cupula), which
does not contain otoliths. c. The endo lymphatic duct ends in the expanded endolymphatic sac. d . Endo lymphatic sac
(1 ) The endolymphatic sac has an epithelial lining containing electron-dense columnar cells, which have an irregularly shaped nucleus, and e lectron- l ucent columnar cells, which possess long microvilli, many pinocytic vesicles, and vacuoles.
(2) It contains phagocytic cel ls (macrophages, neutrophils) in its lumen. (3) Function. The endolymphatic sac may function in resorption of endolymph .
e . Coch lear duct (Figures 2 1 .8 and 2 1 .9) (1 ) Overview
(a ) The cochlear duct is a specialized diverticulum of the saccule that contains the spiral organ of Corti .
(b ) It is bordered above by the scala vestibu l i and below by the scala tympani of the bony cochlea. These scalae, which contain perilymph, communicate with each other at the hel icotrema at the apex of the cochlea.
(2) Vestibular membrane (a ) is composed of two layers of flattened squamous epithelium separated by an
intervening basement membrane. (b) helps maintain the high ionic gradients between the perilymph in the scala vestibuli
and the endolymph in the cochlear duct. (3) Stria vascularis
(a ) is a vascu larized pseudostratified epithelium that lines the lateral aspect of the cochlear duct.
(b) is composed of basal, intermediate, and marginal cells. (c) may secrete endolymph .
(4 ) Spiral prominence (a) The spiral prominence is an epithelium-covered protuberance that extends
the length of the cochlear duct. This epithelium is continuous with that of the stria vascularis and is reflected onto the basilar membrane, where it follows an indentation to form the external sp i ra l sulcus.
(b ) Its cells become cuboidal and continue onto the basilar membrane, where they are known as the ce l ls of C laud ius, which overlie the polyhedral ce l ls of Boettcher .
(5) Basi lar membrane (a ) is a thick layer of amorphous material containing kerati n- l ike f ibers. (b) extends from the spiral ligament to the tympanic lip of the limbus spiralis . (c) has two zones : the medial zona arcuata and the lateral zona pectinata .

.,. ' "-;.
sv
l!1llll'ttmfiii Spec i a l Senses
, ' , ,
, '
TM I
VM
\ "· "
CD
. . • • I . . . . .
.... �"".-� ........ - · r··· - � ··· ··.: · . � ' \ �·
BM . H \ .
,,
381
FIGURE 21 .8. L ight m i c rog raph of the coch l e a ( X 1 32) . N ote the sp i ra l g a n g l io n ( SG ), s c a l a tym pan i (ST), bas i l a r mem bra n e ( B M ), s ca l a vascu l a r is (SV), vesti b u l a r membrane (VM), tecto ria l mem brane (TM), a nd the c och l e a r d u ct ( C D ) .
F IGURE 21 .9. T h e c o c h l e a r d u ct a n d t h e s p i r a l o r g a n o f Co rt i . !Adapted with permiss ion from De l lmann HD . Textbook o f Veterinary
Histology. 4th ed . Ba lt imore . MD : Wi l l iams & Wi lk ins; 1 993:332 . )

382 BRS Cel l B iology and H istology
(6) Tector ia l membrane (a ) makes contact with the processes of the ha i r cel ls . (b ) is secreted by the interdental cells of the spiral sulcus.
(7) Sp i ra l organ of Corti (a ) lies upon both parts of the basilar membrane. (b ) displays the inner tunne l of Corti and the outer tunnel (space of Nuel ) , which
communicate with each other via intercellular spaces. (c) is composed of ha i r cel ls and various supporting cel ls .
(8 ) Hair ce l ls of the organ of Corti (a ) are neuroepithe l ia l cel ls containing a round basal nucleus surrounded by many
mitochondria. (b) possess many long, stiff stereoc i l i a (arranged in a "W" formation) on their free
surfaces, as well as a basa l body (but no kinocilium) . (c) are divided into two types : Inner ha i r ce l ls are organized in a s ing le row along the
entire length of the cochlear duct and receive numerous afferent synaptic terminals on their basal surface. Outer ha i r ce l ls are organized in three or more rows and are ensconced within a cup-shaped afferent nerve ending, where synaptic contacts are made.
(d) function in the reception of sound and can respond to different sound frequencies. (9) Inner and outer p i l l a r ce l ls of the organ of Corti
(a ) are intimately associated with each other; both types rest on the basilar membrane. (b ) enclose and support the inner tunnel of Corti, which lies between the inner and
outer pillar cells. (c) possess a wide base and have elongated processes, which contain microtubules,
intermediate filaments, and actin filaments. ( 10) Inner and outer phalangeal ce l ls of the organ of Corti
(a ) are intimately associated with the inner and outer hair cells, respectively. (b ) support the slender nerve fibers that form synapses with the hair cells.
(1 1 ) Cel ls of Hensen and border cel ls of the organ of Corti delineate the inner and outer borders of the spiral organ of Corti.
lifi'n�MJB Nerve deafness
1. N e rve deafness resu lts from a lesion i n any of the n e rves tra nsm itti ng i m p u lses from the sp i r a l o rg a n o f Co rti to the b ra i n .
2 . It may be c a used by d isease , exposu re t o d rugs, o r p ro l o nged exposu re t o l o u d no ises .
3. Aud itory function of the inner ear a . Movement of the stapes at the oval window causes disturbances in the perilymph, which
cause deflection of the basi lar membrane . Oscillations set in motion at the oval window are dissipated at the secondary tympanic membrane covering the round window of the cochlea. (At a very loud concert, the amount of energy absorbed is very high, and it may take up to 72 hours for it to be dissipated. A residual humming noise may be heard for 2-3 days.)
b. Large areas of the basilar membrane vibrate at many frequencies. However, optimal vibrations are detected at only specific areas. Sound waves of low frequency are detected farther away from the oval window.
c. The p i l lar ce l ls attached to the basilar membrane move laterally in response to this deflection, in turn causing a lateral shearing of the stereocilia of the sensory hair cells of the organ of Corti against the tectorial membrane.
d . Movement of the stereoc i l i a is transduced into electrical impulses that travel via the cochlear nerve to the brain.

4. Vestibu lar function of the inner ear
l!1llll'ttmfiii Spec i a l Senses 383
a. A change in the position of the head causes a flow of the endolymph in the semicircular ducts (c ircular movement) or in the saccules and utricles ( l inear movement) .
b. Movement of the endolymph in the semicircular ducts displaces the cupula overlying the cristae ampu l lares, causing bending of the stereocilia of the sensory hair cells.
c. Movement of the endolymph in the saccules and utricles displaces the oto l iths. This deformation is transmitted to the maculae via the overlying gelatinous layer, causing bending of the stereocilia of the sensory hair cells.
d . In both cases, movement of the stereoc i l i a is transduced into e lectrica l impulses, which are transmitted to the brain via vestibu lar nerve f ibers .
liHnl!ll Men iere d isease
1 . Mlmiere d isease i s an i n n e r ear d iso rde r c a us i ng h e a ri n g l oss, ve rti go , n a usea , ti n n itus, a n d vom iti n g . I t is re l ated t o excess fl u i d i n t h e endo lym p h at ic d u ct.
2. D rugs a re used to treat th e verti g o a n d n a usea , b ut i n severe c ases, su rge ry may be req u i re d f o r vesti b u l a r n e u re ctomy.

Review Test
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1 . Which of the following specialized receptors exhibits a large ovoid capsule consisting of many concentric lamellae, each separated by a space containing tissue fluid?
(A) Cold receptors (B ) Pacinian corpuscles (C) Ruffini endings (D ) Meissner corpuscles (E) Krause end bulb
2. Aqueous humor drains from the eye by passing
(A) into the ciliary processes. (B) from the anterior chamber into the
posterior chamber. (C) through the canal of Schlemm. (D ) into the vitreous body. (E ) through the pupil.
3. Which of the following statements is characteristic of the choroid?
(A) It is avascular. (B ) It is the posterior portion of the tunica
fibrosa. (C) It is tightly attached to the sclera. (D ) It contains many melanocytes. (E) It is not pigmented.
4. Communication of the scala vestibuli and scala tympani occurs at the
(A) round window. (B ) oval window. (C) helicotrema. (D ) endolymphatic sac. (E) inner tunnel.
384
5. The bony ossicles of the middle ear cavity are arranged in a series bridging the tympanic cavity beginning at the tympanic membrane and ending at the
(A) endolymphatic duct. (B ) round window. (C ) helicotrema. (D ) oval window. (E ) cochlear duct.
6. Which of the following cells in the inner ear are involved in detecting movements of the head?
(A) Hair cells in the maculae (B ) Outer pillar cells (C) Inner pillar cells (D ) Cells of Hensen (E) Hair cells in the organ of Corti
7. Rods and cones form synapses with which of the following cells?
(A) Amacrine (B ) Bipolar (C ) Ganglion (D ) Muller (E) Pigmented epithelium
8. Which of the following statements is characteristic of the cornea?
(A) It represents the anterior portion of the tunica vasculosa.
(B) It is composed of three layers. (C) It forms the anterior boundary of the
posterior chamber of the eye. (D ) It is devoid of nerve endings. (E) It is the anterior transparent portion of the
tunica fibrosa.

9. A patient exhibiting a high intraocular pressure in both eyes is symptomatic for
(A) cataract. (B ) detached retina. (C ) glaucoma. (D ) conjunctivitis. (E ) presbyopia.
1 0. Aqueous humor is produced by
(A) the corneal epithelium. (B ) the canal of Schlemm. (C) ciliary epithelium. (D ) conjunctiva. (E) ora serrata.
l!1llll'ttmfiii Spec i a l Senses 385
1 1 . Which one of the following is related to an overabundance of fluid in the endolymphatic duct?
(A) Glaucoma (B ) Vertigo (C) Otis media (D) Conductive hearing loss (E) Nerve deafness

Answers and Explanations
1 . B . Pacinian corpuscles are usually macroscopic. Their capsules are composed of several lamellae containing fibroblasts and collagen fibers. The lamellae are separated by sparse amounts of tissue fluid. Pacinian corpuscles respond to vibrations and pressure that distort the lamellae. Meissner corpuscles, responsible for touch, are tapered terminals at the tips of dermal papillae. Ruffini endings, which are sensitive to mechanical stresses, possess a thin connective tissue capsule that surrounds a fluid-filled space. Cold receptors are naked nerve endings that respond to temperatures below 25°C to 30°C (see Chapter 21 II B) .
2. C. Aqueous humor exits the eye by passing into the canal of Schlemm. The vitreous body is a refractile gel that fills the chamber of the globe posterior to the lens and is not related to the aqueous humor (see Chapter 2 1 III D 1 ) .
3. D . The choroid is the vascular tunic of the eye that loosely adheres to the sclera of the tunica fibrosa. It contains many melanocytes, which impart a dark pigment to the eye (see Chapter 21 III C 1 ) .
4 . C. The scala vestibuli and the scala tympani are actually one perilymphatic space separated by the cochlear duct (scala media) . The scala vestibuli and tympani communicate with each other at the helicotrema (see Chapter 21 IV C 2 e) .
5. D . The bony ossicles of the middle ear cavity articulate in a series from the tympanic membrane to the oval window (see Chapter 21 IV B) .
6. A. Neuroepithelial hair cells in the maculae of the saccule and the utricle detect linear movement of the head. These cells are connected to the vestibular portion of the acoustic nerve (see Chapter 21 IV C 2).
7 . B . Rods and cones synapse with bipolar cells and horizontal cells (see Chapter 2 1 III E 3) .
8. E. The cornea is the transparent anterior portion of the tunica fibrosa, the outer covering of the eye; thus it forms the anterior wall of the anterior chamber of the eye. It is also rich in sensory nerve endings. The sclera is the posterior portion of the tunica fibrosa. The tunica vasculosa (middle coat) is composed of the choroid and ciliary body and the iris (see Chapter 21 III B).
9. C. High intraocular pressure is a symptom of glaucoma. This condition prohibits the aqueous humor from escaping from the anterior chamber of the eye via the canal of Schlemm. If it is left untreated, a gradual loss of peripheral sight occurs; over time, blindness results. People with cataract have opacity of the lens that blurs the vision. Conjunctivitis is an inflammation of the conjunctiva of the eye with severe reddening of the sclera and the conjunctival surface of the lids, perhaps with a discharge. This condition may be contagious, and if left untreated, blindness may occur (see Chapter 21 III D Clinical Consideration) .
1 0. C. The ciliary epithelium that lines the ciliary processes secretes the aqueous humor into the posterior chamber of the eye between the iris and the lens. The aqueous humor then flows through the pupil and into the anterior chamber of the eye and finally leaves the anterior chamber by entering the venous system via the canal of Schlemm (see Chapter 21 III D 1 ) .
1 1 . B . An overabundance of endolymph in the endolymphatic duct causes vertigo, nausea, hearing loss, tinnitus, and vomiting, all symptoms of Meniere d isease (see Chapter 21 IV C 4 Clinical Consideration) .
386

Comprehensive Examination
D i rections: Each of the numbered items or incomplete statements in this section is followed by answers or by completions of the statement. Select the ONE lettered answer or completion that is BEST in each case.
1. Which of the following statements concerning ribonucleic acid (RNA) synthesis is true?
(A) RNA synthesis does not require deoxyribonucleic acid to act as a template.
(B ) Syntheses of ribosomal RNA, messenger RNA, and transfer RNA are all catalyzed by the same RNA polymerase.
(C) To yield messenger ribonucleoproteins, introns are excised, whereas exons are spliced together.
(D ) Protein moieties are removed from messenger ribonucleoproteins within the nucleolus, yielding functional messenger RNAs to exit via the nuclear pores.
(E) The start codon for RNA synthesis is UAG.
2. Which of the following factors is primarily responsible for causing osteoporosis in older women?
(A) Decreased bone formation (B ) Lack of physical exercise (C) Diminished estrogen secretion (D ) Calcium deficiency (E) Increased bone formation
3. Which of the following bases that make up deoxyribonucleic acid and ribonucleic acid (RNA) is unique to RNA?
(A) Thymine (B ) Adenine (C ) Cytosine (D ) Guanine (E ) Uracil
4. The centroacinar cells of the pancreas secrete
(A) an alkaline enzyme-poor fluid. (B ) pancreatic digestive enzymes. (C) secretin. (D ) cholecystokinin. (E ) glucagon.
5. The zona fasciculata of the adrenal cortex synthesizes and secretes
(A) mineralocorticoids. (B) glucagon. (C) epinephrine. (D ) aldosterone. (E) glucocorticoids.
6. Which of the following statements about bony joints is true?
(A) Long bones are generally united by synarthroses.
(B) Diarthroses are classified as synovial joints.
(C) Type A cells of the synovial membrane secrete synovial fluid.
(D ) Type B cells of the synovial membrane are phagocytic.
(E ) Synarthroses are usually surrounded by a two-layered capsule.
7. All of the following characteristics can be used to distinguish neutrophils and basophils histologically except one. Which one is the exception?
(A) Size of specific granules (B ) Shape of the nucleus (C) Number of azurophilic granules (D) The presence or absence of peroxidase (E) The presence of mitochondria
8. A long-time user of chewing tobacco noticed several whitish, thick, painless patches on the lining of his cheeks. The most probable diagnosis is
(A) aphthous ulcers. (B) adenocarcinoma. (C) keloids. (D) oral leukoplakia. (E) epidermolysis bullosa.
387

388 Comprehens ive Exam inati on
9. Primordial follicles of the ovary possess
(A) a layer of cuboidal follicular cells. (B ) an oocyte arrested in prophase of
meiosis I . (C) an oocyte arrested in metaphase of
meiosis II . (D ) well-defined thecae interna and externa. (E ) a thick zona pellucida.
1 0. All of the following statements regarding the membranous labyrinth of the inner ear are true except for one. Which is that exception?
(A) It contains the saccule and utricle. (B) Maculae contain neuroepithelial cells,
which possess numerous stereocilia and a single kino cilium.
(C) Cristae ampullares in the semicircular canals detect angular acceleration of the head.
(D) The otolithic membrane contains small calcified particles.
(E) It contains the vestibular membrane.
1 1 . Which of the following statements concerning euchromatin is true?
(A) It constitutes about 90% of the chromatin. (B ) It appears as basophilic clumps of nu-
cleoprotein when seen under the light microscope.
(C) It is concentrated near the periphery of the nucleus.
(D ) It is transcriptionally active. (E ) It is transcriptionally inactive.
1 2. Intercalated disks function in which one of the following?
(A) End-to-end attachments of smooth muscle cells
(B ) Intercellular movement of large proteins (C) Ionic coupling of cardiac muscle cells (D ) Storage of Ca2+ (E ) Release of neurotransmitters
1 3. Release of thyroid hormones from the follicular cells of the thyroid gland depends on thyroid-stimulating hormone (TSH). TSH stimulation involves
(A) binding of TSH to receptors on the apical plasma membrane.
(B ) formation of apical microvilli. (C) exocytosis of colloid droplets. (D ) change in cell shape from flattened to
columnar. (E ) secretion of lysosomes from the basal cell
surface.
1 4. Which one of the following statements about the development of the tooth crown is true?
(A) The enamel organ is derived from ectomesenchyme (neural crest) .
(B ) The dental papilla is derived from the epithelium.
(C ) The four-layer enamel organ appears during the cap stage.
(D ) Dentin and enamel are formed during the appositional stage.
(E ) Cementum is formed at the same time as enamel.
1 5. Which one of the following statements concerning liver sinusoids is true?
(A) Their lining includes Ito cells (fat-storing cells).
(B) They receive bile from the hepatocytes. (C) They are lined by nonfenestrated
endothelial cells. (D ) The space of Disse is located between
sinusoidal cells and hepatocytes. (E) Sinusoids convey blood from the central
vein to the portal vein.
16 . A young college student had nausea, vomiting, visual disorders, and muscular paralysis after eating canned tuna fish. The probable diagnosis is botulism, caused by ingestion of the Clostridium botulinum toxin. The physiological effect of this toxin is to
(A) inactivate acetylcholinesterase. (B) bind to and thus inactivate acetylcholine
receptors at myoneural junctions. (C) prevent release of calcium ions from the
sarcoplasmic reticulum, thus inhibiting muscle contraction.
(D) inhibit release of acetylcholine from presynaptic membranes.
(E) inhibit hydrolysis of adenosine triphosphate during the contraction cycle.
17. Which of the following statements about nucleosomes is true?
(A) Histones form the nucleosome core around which the double helix deoxyribonucleic acid is wound.
(B ) Nucleosomes without histones form the structural unit of the chromosome.
(C) Nucleosomes are composed of ribonucleic acid (RNA) molecules and two copies each of four different histones.
(D) Histone Hl forms the core of the nucleosome.
(E) Nucleosomes are linked together with RNA.

1 8. A high school student complains of fatigue and a sore throat. She has swollen, tender lymph nodes and a fever. Blood test results show an increased white blood cell count with many atypical lymphocytes; the number and appearance of the erythrocytes are normal. This student is likely to have
(A) AIDS. (B) pernicious anemia. (C) infectious mononucleosis. (D) Hodgkin disease. (E) factor VIII deficiency.
1 9. Which one of the following statements about the gallbladder is true?
(A) The gallbladder dilutes bile. (B ) Bile enters the gallbladder via the common
bile duct. (C ) Bile leaves the gallbladder via the cystic
duct. (D ) The gallbladder is lined by a simple
squamous epithelium. (E ) Secretin stimulates the wall of the gallblad
der to contract, forcing bile from its lumen.
20. Which one of the following statements concerning mitochondria is true?
(A) They change from the orthodox to the condensed form in response to the uncoupling of oxidation from phosphorylation.
(B) They are unable to divide. (C) They possess the enzymes of the Krebs
cycle in their cristae. (D ) They contain elementary particles in their
matrix. (E ) They do not contain deoxyribonucleic acid.
21 . Which one of the following components is present in muscular arteries but absent from elastic arteries?
(A) Fenestrated membranes (B) Vasa vasorum (C ) Factor VIII (D ) A thick, complete internal elastic lamina (E) Smooth muscle cells
22. Which one of the following statements concerning the pancreas is true?
(A) Islets of Langerhans secrete enzymes. (B) It possesses mucous acinar cells. (C) The endocrine pancreas has more �-cells
than 8-cells. (D ) Its a-cells secrete insulin. (E) Its 8-cells secrete amylase.
Comp rehens ive Exam i nat ion 389
23. Which one of the following stimulates the production of hydrochloric acid in the stomach?
(A) Somatostatin (B ) Gastrin (C) Secretin (D ) Cholecystokinin (E ) Urogastrone
24. A deficiency or an excess of which of the following vitamins results in short stature?
(A) Vitamin A (B ) Vitamin C (C) Vitamin D (D ) Vitamin K (E ) Vitamin B
25. The intercellular spaces in the stratum spinosum of the epidermis contain lipidcontaining sheets that are impermeable to water. This material is released from
(A) keratohyalin granules. (B) Langerhans cells. (C) membrane-coating granules. (D) sebaceous glands. (E) melanosomes.
26. Which of the following statements concerning basophilic erythroblasts is true?
(A) The nucleus has a fine chromatin network. (B ) The nucleus is in the process of being
extruded. (C) The cytoplasm contains specific granules. (D) The cytoplasm is pink and reveals a dense
reticulum. (E ) The nucleus is bilobed.
27. The ileum includes which of the following structures?
(A) Rugae (B ) Peyer patches (C) Brunner glands (D ) Parietal cells (E) Chief cells
28. A 25-year-old woman complains about a frequently recurring painful lesion on her upper lip that exudes a clear fluid. She probably has
(A) oral leukoplakia. (B ) herpetic stomatitis. (C) aphthous ulcer. (D ) bullous pemphigoid. (E) malignant melanoma.

390 Comprehens ive Exam inati on
29. Which of the following statements concerning the functions of the skin is true?
(A) Infrared radiation, necessary for synthesis of vitamin D, is absorbed by the skin.
(B ) The skin provides no protection against desiccation.
(C) The skin contains temperature receptors and plays a role in regulating body temperature.
(D ) Melanin is synthesized by melanocytes, which are located in the dermis.
(E) Sunscreen with a sun protection factor rating of 15 or higher protects the skin from harmful effects caused by ultraviolet light.
30. A person with glomerulonephritis will have which of the following signs or symptoms?
(A) Hypotonic urine (B ) Polyuria (C) Proteinuria (D ) Dehydration (E ) Polydipsia
31 . Stratified squamous keratinized epithelium is always present in the
(A) rectum. (B ) esophagus. (C) pyloric stomach. (D ) jejunum. (E ) anus.
32. Which of the following properties is exhibited in all three types of cartilage?
(A) It is involved in bone formation. (B) It possesses type II collagen. (C) It possesses type I collagen. (D ) It grows interstitially and appositionally. (E ) It has an identifiable perichondrium.
33. Which of the following is a receptor for fine touch?
(A) Pacinian corpuscle (B ) Crista ampullaris (C) Ruffini ending (D ) Krause end bulb (E ) Meissner corpuscle
34. A premature infant has labored breathing, which is eventually alleviated by administration of glucocorticoids. The most probable diagnosis is
(A) immotile cilia syndrome. (B) emphysema. (C) hyaline membrane disease. (D) asthma. (E ) chronic bronchitis.
35. Which of the following statements concerning the cribriform plate is true?
(A) It is the inner layer of the alveolar bone. (B) It lacks Sharpey fibers. (C) It is also known as the spongiosa. (D) It is composed of cancellous bone. (E) Normally, it is fused with cementum.
36. Which one of the following substances is synthesized in the pituitary gland?
(A) Oxytocin (B ) Antidiuretic hormone (C) Somatotropin (D ) Neurophysin (E ) Vasopressin
37. Which one of the following is true in breast cancer cells that involve the BRCAl gene?
(A) Mutated cells are unable to divide because of increased expression of the BRCAl gene.
(B ) Mutated cells fail to reach the Gl -S checkpoint.
(C ) Mutated cells have an abnormal number of endosomes.
(D) Mutated cells lose their G2-M cell cycle checkpoint.
(E ) Mutated cells become haploid owing to the interaction of the BRCAl and p53 genes.
Questions 38 to 40 A 42-year-old man arrives in the emergency department with a rash over much of his face, hands, and arms. He states that he was gardening and pulled out a number of weeds. On questioning the patient, the physician realized that the patient inadvertently came in contact with poison ivy.
38. Which of the following cells is responsible for the release of the pharmacological agents that caused the rash?
(A) Diffuse neuroendocrine system cells (B ) Myofibroblasts (C) Mast cells (D ) Pericytes (E ) Plasma cells
39. Which of the following is a secondary mediator produced by the cell in question 38?
(A) Histamine (B ) Chondroitin sulfate (C ) Neutral protease (D ) Bradykinin (E ) Aryl sulfatase

40. Which of the following white blood cells can also participate in the reaction of this patient to poison ivy?
(A) T cells (B ) B cells (C) Neutrophils (D ) Basophils (E ) Eosinophils
41 . A 26-year-old woman goes to the dentist because of a toothache. On examination, the dentist notes that the patient has a carious lesion that involves not only the enamel but also the dentin and the cementum of the tooth. Which of these substances cannot repair itself?
(A) Dentin (B ) Enamel (C) Cementum (D ) Dentin and cementum (E ) Dentin, cementum, and enamel
42. Lisa is small and thin in stature. She spends her days indoors and rarely eats dairy products. When she became pregnant at 25 years of age, she had severe lower back and leg pain and tenderness when pressure was applied over bony regions of her body. Radiographs revealed excessive amounts of poorly mineralized osteoid in both femurs. Beneficial treatment of her condition involved high doses of vitamin D, calcium, and phosphorus, a regimen that continued after successful delivery of her baby. Which of the following describes Lisa's disease?
(A) Osteogenesis imperfecta (B ) Osteoporosis (C) Osteomalacia (D ) Osteopetrosis (E ) Osteopenia
43. Michael had visual problems within a day after being hit in the head with a ball during a soccer game. He saw large floaters and noticed that a dark film was blocking part of the vision in his right eye. An examination by an ophthalmologist revealed that he had a detached retina, and emergency surgery was done to save the vision in that eye. Which of the following retinal layers were separated from one another to cause Michael's condition?
(A) Layer 1 from layer 2 (B ) Layer 2 from layer 3 (C ) Layer 3 from layer 4 (D ) Layer 5 from layer 6 (E ) Layer 6 from layer 7
Comp rehens ive Exam i nat ion 391
44. Blood coagulation entails a cascade of reactions that occur in two interrelated pathways, the extrinsic and intrinsic. All of the following are associated with the intrinsic pathway of blood coagulation except
(A) conversion of fibrinogen to fibrin. (B ) platelet aggregation. (C) release of tissue thromboplastin. (D ) von Wille brand factor. (E ) calcium.
45. A scientist spent a summer in a remote region of Africa, where he studied exotic plants. On returning to the United States, he developed a cough and fever that would not go away. Laboratory tests revealed that he had contracted a roundworm, Ascaris lumbricoides. Which of the following cells would be expected to be significantly elevated in a differential count of his blood?
(A) Erythrocytes (B ) Lymphocytes (C) Monocytes (D ) Eosinophils (E ) Neutrophils
46. A 45-year-old musician who played the guitar for 26 years in a rock band noticed he was having difficulty hearing. An otolaryngologist confirmed his loss of hearing and associated it with prolonged exposure to loud sounds. Which of the following structures would show degenerative changes that would account for this man's hearing loss?
(A) The epithelium lining the inner portion of the tympanic membrane
(B ) Hair cells in the ampullae of the semicircular ducts
(C) The auditory (eustachian) tube extending to the middle ear cavity
(D ) Hair cells of the organ of Corti (E ) Ossicles in the middle ear
47. Which of the following is a protein circulating in the blood that functions in wound healing?
(A) Chondronectin (B ) Plasma fibronectin (C) Osteonectin (D ) Matrix fibronectin (E ) Laminin

392 Comprehens ive Exam inati on
48. Which of the following is an adhesive glycoprotein that forms fibrils in the extracellular matrix?
(A) Chondronectin (B ) Plasma fibronectin (C) Osteonectin (D ) Matrix fibronectin (E ) Laminin
49. Which of the following is a multifunctional protein that attaches chondrocytes to type II collagen?
(A) Laminin (B ) Plasma fibronectin (C) Osteonectin (D ) Matrix fibronectin (E ) Chondronectin
50. Which of the following cells in the connective tissue is an antibody-manufacturing cell?
(A) Pericytes (B ) Macrophages (C) T lymphocytes (D ) Plasma cells (E ) Mast cells
51 . Principal phagocytes of connective tissue are the
(A) pericytes. (B) macrophages. (C) T lymphocytes. (D) plasma cells. (E) mast cells.
52. Cells in the connective tissue that can bind immunoglobulin E antibodies and mediate immediate hypersensitivity reactions are
(A) pericytes. (B ) macrophages. (C) T lymphocytes. (D ) plasma cells. (E) mast cells.
53. Connective tissue cells responsible for initiating cell-mediated immune responses are
(A) pericytes. (B) macrophages. (C) T lymphocytes. (D) plasma cells. (E) mast cells.
54. Pluripotential cells located primarily along capillaries in the connective tissue are
(A) pericytes. (B) macrophages. (C) T lymphocytes. (D) plasma cells. (E) mast cells.
55. Which of the following functions in activation of secondary messenger systems?
(A) Phospholipid (B ) Glycocalyx (C ) Carrier protein (D ) Band 3 protein (E ) G protein
56. Which of the following is primarily responsible for establishing the potential difference across the plasma membrane?
(A) K'" leak channel (B ) Glycocalyx (C ) Carrier protein (D ) Band 3 protein (E ) G protein
57. Which of the following is an amphipathic molecule?
(A) Phospholipid (B ) Glycocalyx (C ) Carrier protein (D ) Band 3 protein (E ) G protein
58. Which of the following is a carbohydratecontaining covering associated with the outer leaflet of the plasma membrane?
(A) Phospholipid (B ) Glycocalyx (C ) Carrier protein (D ) Band 3 protein (E ) G protein
59. Which of the following functions in antiport transport?
(A) Phospholipid (B ) Glycocalyx (C ) Carrier protein (D ) Band 3 protein (E ) G protein

60. Which of the following is a surface marker on T killer cells (CTL)?
(A) CD4 (B ) CDS (C) Interleukin l (D ) Interleukin 2 (E ) Perforin
61 . Which of the following is a surface marker on T helper cells?
(A) CD4 (B ) CDS (C) Interleukin l (D ) Interleukin 2 (E ) Perforin
62. Which of the following mediates lysis of tumor cells?
(A) CD4 (B ) CDS (C ) Interleukin l (D ) Interleukin 2 (E ) Perforin
63. Which of the following is released by macrophages and stimulates activated T helper cells?
(A) CD4 (B ) CDS (C ) Interleukin l (D ) Interleukin 2 (E ) Interferon-y
64. Which of the following stimulates activation of natural killer cells?
(A) CD4 (B ) Interferon-y (C ) Interleukin l (D ) Interleukin 2 (E ) Perforin
65. Identify the cells that replicate their deoxyribonucleic acid during the S phase of the cell cycle and undergo meiosis.
(A) Sertoli cells (B ) Primary spermatocytes (C ) Secondary spermatocytes (D ) Interstitial cells of Leydig (E ) Spermatids
Comp rehens ive Exam i nat ion 393
66. Identify the cells that form a temporary cylinder of microtubules called the manchette.
(A) Sertoli cells (B ) Primary spermatocytes (C) Secondary spermatocytes (D ) Interstitial cells of Leydig (E) Spermatids
67. Identify the cells that possess receptors for luteinizing hormone (LH) and produce testosterone in response to binding of LH.
(A) Sertoli cells (B ) Primary spermatocytes (C) Secondary spermatocytes (D ) Interstitial cells of Leydig (E) Spermatids
68. Identify the cells that are responsible for formation of the blood-testis barrier.
(A) Sertoli cells (B ) Primary spermatocytes (C) Secondary spermatocytes (D ) Interstitial cells of Leydig (E) Spermatids
69. Identify the cells that synthesize androgenbinding protein when stimulated by folliclestimulating hormone.
(A) Sertoli cells (B ) Primary spermatocytes (C) Secondary spermatocytes (D ) Interstitial cells of Leydig (E) Spermatids
70. Which of the following organelles possesses mixed-function oxidases that detoxify phenobarbital and other drugs?
(A) Rough endoplasmic reticulum (B ) Smooth endoplasmic reticulum (C) Mitochondrion (D ) Annulate lamella (E) Lysosome
71 . Which of the following organelles contains ribophorins?
(A) Rough endoplasmic reticulum (B ) Smooth endoplasmic reticulum (C) Mitochondrion (D ) Polyribosome (E) Lysosome

394 Comprehens ive Exam inati on
72. Which of the following is the site where degradation of foreign material ingested by the cell takes place?
(A) Rough endoplasmic reticulum (B ) Smooth endoplasmic reticulum (C) Mitochondrion (D ) Annulate lamellae (E) Lysosome
73. Which of the following organelles contains adenosine triphosphate synthase?
(A) Rough endoplasmic reticulum (B ) Smooth endoplasmic reticulum (C) Mitochondrion (D ) Annulate lamellae (E) Lysosome
74. Which of the following stimulates secretion of pepsinogen?
(A) Gastrin (B ) Somatostatin (C) Motilin (D ) Secretin (E ) Lysozyme
75. Which of the following is produced by Brunner glands and inhibits hydrochloric acid secretion by parietal cells?
(A) Gastrin (B ) Somatostatin (C) Urogastrone (D ) Pepsinogen (E) Lysozyme
76. Which of the following functions as an antibacterial agent?
(A) Gastrin (B ) Somatostatin (C) Motilin (D ) Pepsinogen (E ) Lysozyme
77. Which of the following stimulates contraction of smooth muscle in the wall of the digestive tract?
(A) Gastrin (B ) Somatostatin (C) Motilin (D ) Pepsinogen (E ) Lysozyme
78. Which of the following inhibits secretion by nearby enteroendocrine cells?
(A) Gastrin (B ) Somatostatin (C ) Motilin (D ) Pepsinogen (E ) Lysozyme
79. Which of the following is involved in forming cross-links between adjacent tropocollagen molecules?
(A) Lysine (B ) Desmosine (C) Hydroxyproline (D ) Arginine (E ) Proline
80. Which of the following cross-links elastin molecules to form an extensive network?
(A) Lysine (B ) Fibrillin (C ) Hydroxyproline (D ) Arginine (E ) Proline
81 . Inadequate amounts of iodine in the diet lead to which one of the following conditions?
(A) Simple goiter (B ) Exophthalmic goiter (C) Graves disease (D ) Addison disease (E) Hyperparathyroidism
82. Which of the following conditions is associated with the destruction of the adrenal cortex?
(A) Simple goiter (B ) Exophthalmic goiter (C) Graves disease (D ) Addison disease (E) Hyperparathyroidism
83. Which of the following hydrolyzes adenosine triphosphate?
(A) Troponin C (B ) Globular head (Sl fragment) of myosin (C ) Myoglobin (D ) Actin (E ) Tropomodulin

84. Which of the following binds oxygen?
(A) Troponin C (B ) Globular head (Sl fragment) of myosin (C ) Myoglobin (D ) Actin (E ) Tropomodulin
85. Which of the following binds Ca2+?
(A) Troponin C (B ) Globular head (Sl fragment) of myosin (C ) Myoglobin (D ) Actin (E ) Tropomodulin
86. Which of the following is a rare form of skin cancer that may be fatal?
(A) Epidermolysis bullosa (B) Basal cell carcinoma (C ) Malignant melanoma (D ) Psoriasis (E) Warts
87. Which of the following is a hereditary skin disease characterized by blister formation after minor trauma?
(A) Epidermolysis bullosa (B) Basal cell carcinoma (C ) Malignant melanoma (D ) Psoriasis (E) Warts
88. Which of the following regions of the respiratory system would concern a patient with an adenoid?
(A) Trachea (B ) Nasopharynx (C ) Terminal bronchiole (D ) Alveolar duct (E ) Intrapulmonary bronchi
89. Which of the following possesses C-shaped rings of hyaline cartilage?
(A) Trachea (B ) Nasopharynx (C ) Terminal bronchiole (D ) Alveolar duct (E ) Intrapulmonary bronchi
Comp rehens ive Exam i nat ion 395
90. Which of the following contains smooth muscle at the openings into alveoli?
(A) Trachea (B ) Nasopharynx (C) Terminal bronchiole (D ) Alveolar duct (E) Intrapulmonary bronchi
91 . Which of the following is lined by an epithelium containing ciliated cells and Clara cells?
(A) Trachea (B ) Nasopharynx (C) Terminal bronchiole (D ) Alveolar duct (E) Intrapulmonary bronchi
92. Which of the following is associated with rupture of the oviduct and hemorrhaging into the peritoneal cavity?
(A) Endometriosis (B ) Cervical cancer (C) Ectopic tubal pregnancy (D ) Breast cancer (E) Teratomas
93. Which of the following may be classified as lobular carcinoma?
(A) Endometriosis (B ) Cervical cancer (C) Ectopic tubal pregnancy (D ) Breast cancer (E) Teratomas
94. Which of the following may be detected by a Papanicolaou smear?
(A) Endometriosis (B ) Cervical cancer (C) Ectopic tubal pregnancy (D ) Breast cancer (E) Teratomas
95. Which of the following commonly results in hemorrhaging into the peritoneal cavity dependent on the stage of the menstrual cycle?
(A) Endometriosis (B ) Cervical cancer (C) Ectopic tubal pregnancy (D ) Breast cancer (E) Teratomas

396 Comprehens ive Exam inati on
96. Which of the following facilitates the absorption of vitamin B 12?
(A) Pepsin (B ) Enzyme associated with the glycocalyx
of the intestinal striated border (C) Lipase (D) Chylomicron (E ) Gastric intrinsic factor
97. Which of the following functions in the digestion of carbohydrates?
(A) Pepsin (B ) Enzyme associated with the glycocalyx of
the intestinal striated border (C) Lipase (D) Chylomicron (E ) Gastric intrinsic factor
98. Which of the following functions in the digestion of proteins?
(A) Pepsin (B ) Enzyme associated with the glycocalyx of
the intestinal striated border (C) Lipase (D) Chylomicron (E ) Gastric intrinsic factor
99. Which of the following functions in the transport of triglycerides into lacteals?
(A) Pepsin (B ) Enzyme associated with the glycocalyx of
the intestinal striated border (C) Lipase (D) Chylomicron (E ) Gastric intrinsic factor
1 00. Which of the following is manufactured and released by parietal cells?
(A) Pepsin (B ) Enzyme associated with the glycocalyx of
the intestinal striated border (C) Lipase (D) Chylomicron (E ) Gastric intrinsic factor

Answers and Explanations
1 . C. To yield messenger ribonucleoproteins (mRNPs), introns are excised, whereas exons are spliced together. Deoxyribonucleic acid does act as the template for the synthesis of ribonucleic acid (RNA) . Three RNA polymerases (I, II, and III) are needed to synthesize ribosomal RNA, messenger RNA, and transfer RNA, respectively. Protein moieties are removed from the mRNPs as they leave the nucleus to yield functional mRNAs outside the nucleus. (See Chapter 2 VIII A.)
2. C. The most common cause of osteoporosis in older women is diminished estrogen secretion. (See Chapter 7 II J Clinical Consideration.)
3. E. Although adenine, cytosine, and guanine are found in both deoxyribonucleic acid (DNA) and ribonucleic acid (RNA), uracil is found only in RNA. Uracil substitutes for the base thymine in DNA. (See Chapter 2 VIII.)
4. A. Pancreatic centroacinar cells form the initial segment of the intercalated duct and are part of the exocrine pancreas. They secrete an enzyme-poor alkaline fluid when stimulated by secretin. Pancreatic digestive enzymes are synthesized by the acinar cells of the exocrine pancreas; their release is stimulated by cholecystokinin. Glucagon is produced in the endocrine pancreas (islets of Langerhans). (See Chapter 17 III A 2.)
5. E. The zona fasciculata, the largest region of the adrenal cortex, produces glucocorticoids (cortisol and corticosterone) . The zona glomerulosa produces mineralocorticoids, primarily aldosterone. Epinephrine is produced in the adrenal medulla. Glucagon is produced in the pancreas, not in the adrenal gland. (See Chapter 13 VI A 2.)
6. B . Diarthroses, the type of joint connecting two long bones, are classified as synovial joints, which are surrounded by a two-layered capsule housing a synovial membrane. Type A cells of the synovial membrane are phagocytic, whereas type B cells secrete the synovial fluid. Synarthrosis joints are those found joining the bones of the skull, which are immovable. (See Chapter 7 III B . )
7. E. Neutrophils have a nucleus with three or four lobes, many azurophilic granules, and small specific granules that lack peroxidase. In contrast, basophils have an S-shaped nucleus, few azurophilic granules, and large specific granules that contain peroxidase. Both neutrophils and basophils possess mitochondria. (See Table 10 .2 . )
8. D . Oral leukoplakia, which results from epithelial hyperkeratosis, is usually of unknown etiology, but is often associated with the use of chewing tobacco. Although the characteristic painless lesions are benign, they may transform into squamous cell carcinoma. Aphthous ulcers are painful lesions of the oral mucosa that are surrounded by a red border. Adenocarcinoma is a form of cancer arising in glandular tissue. Keloids are swellings in the skin that arise from increased collagen formation in hyperplastic scar tissue. Epidermolysis bullosa is a group of hereditary skin diseases characterized by blister formation after minor trauma. (See Chapter 16 II.)
9. B . A primordial follicle is composed of a flattened layer of follicular cells surrounding a primary oocyte, which is arrested in prophase of meiosis I. Well-defined thecal layers and a thick zona pellucida are found in growing follicles. A graafian (mature) follicle possesses a secondary oocyte, which becomes arrested in metaphase of meiosis II just before ovulation. (See Chapter 19 II B 1 . )
397

398 Comprehens ive Exam inati on
1 0. E . The first four statements are true. Linear acceleration of the head is detected by the neuroepithelial hair cells of the maculae, which are specialized regions of the saccule and utricle. However, the vestibular membrane is a part of the organ of Corti. (See Chapter 2 1 IV C 2.)
1 1 . D . Euchromatin, the transcriptionally active form of chromatin, represents only about 10% of the chromatin. In the light microscope, it appears as a light-staining, dispersed region of the nucleus. (See Chapter 2 V 2.)
1 2. C. Large protein molecules cannot move across intercalated disks (the steplike junctional complexes present in cardiac, not smooth, muscle) . These junctional structures possess three specializations: desmosomes, which provide end-to-end attachment of cardiac muscle cells; fascia adherentes, to which the thin myofilaments attach; and gap junctions, which permit intercellular movement of small molecules and ions (ionic coupling) . (See Chapter 8 V B 6.)
1 3. D . Flattened squamous cells are characteristic of an unstimulated, inactive thyroid gland. TSH binds to G protein-linked receptors on the basal surface of follicular cells. Under TSH stimulation, thyroid follicular cells become columnar and form pseudopods, which engulf colloid. Lysosomal enzymes split thyroxine and triiodothyronine from thyroglobulin; the hormones are then released basally. (See Chapter l3 IV B 2.)
1 4. D . The enamel organ is epithelially derived, whereas the dental papilla comes from ectomesenchyme. The bell, not the cap, stage of odontogenesis is characterized by possessing a fourth layer in its enamel organ. Formation of dentin and enamel occurs during the appositional stage of tooth development. Cementum is located on the root and is formed only after the crown is complete and enamel ceases to be elaborated. (See Chapter 16 II C 3 . )
1 5. D . Liver sinusoids convey blood to the central vein. Their endothelial cells are fenestrated, and material from the sinusoids may enter the space of Disse through the fenestrae, where it may be endocytosed by hepatocytes. The space of Disse houses Ito cells (fat-storing cells) . Because bile is the exocrine secretion of hepatocytes, it does not enter the sinusoids. (See Chapter 17 IV B 2 .)
1 6. D . The toxin from Clostridium botulinum inhibits the release of acetylcholine, the neurotransmitter at myoneural junctions. As a result, motor nerve impulses cannot be transmitted across the junction, and muscle cells are not stimulated to contract. (See Chapter 8 IV 2 Clinical Considerations.)
17. A. The nucleosome, the structural unit of chromatin packing, does not contain ribonucleic acid. In extended chromatin, two copies each of histones H2A, H2B, H3, and H4 form the nucleosome core around which a deoxyribonucleic acid molecule is wound. Condensed chromatin contains additional histones (H1), which bind to nucleosomes, forming the condensed 30-nm chromatin fiber. (See Chapter 2 VI A.)
1 8. C. Only infectious mononucleosis is characterized by all of the signs and symptoms indicated. AIDS is associated with a decreased lymphocyte count, particularly of T helper cells. Pernicious anemia is associated with a decreased red blood cell count. Hodgkin disease is associated with fatigue and enlarged lymph nodes, but the nodes are not painful, and the presence of Reed-Sternberg cells is diagnostic of this disease. Factor VIII deficiency, a coagulation disorder, is not associated with any of these signs and symptoms. (See Chapter 10 II B 2 Clinical Considerations.)
1 9. C. The gallbladder, which concentrates and stores bile, is lined by a simple columnar epithelium. Cholecystokinin stimulates contraction of the gallbladder wall, forcing bile from the lumen into the cystic duct; this joins the common hepatic duct to form the common bile duct, which delivers bile to the duodenum. (See Chapter 17 III A 2.)
20. A. Uncoupling of oxidation from phosphorylation induces mitochondria to change from the orthodox to the condensed form. Condensed mitochondria are often present in brown fat cells, which produce heat rather than adenosine triphosphate. Mitochondria possess circular deoxyribonucleic acid, and they reproduce (divide) by fission. (See Chapter 3 II 6 e.)

Comp rehens ive Exam i nat ion 399
21 . D. Muscular (distributing) arteries have a thick, complete internal elastic lamina in the tunica intima, whereas elastic (conducting) arteries have an incomplete internal elastic lamina. Both types of arteries have vasa vasorum, factor VIII, and smooth muscle cells in their walls. Museular arteries possess numerous layers of muscle cells in the tunica media, but elastic arteries do not. Only elastic arteries possess fenestrated (elastic) membranes in the tunica media, in which smooth muscle cells are dispersed. (See Chapter 1 1 I B 1 b.)
22. C. In the endocrine pancreas, �-cells account for about 70% of the secretory cells; a-cells about 20%; and o-cells less than 5%. Polypeptide hormones are synthesized by and released from the islets of Langerhans (endocrine pancreas) . The exocrine pancreas possesses serous (not mucous) acinar cells. Insulin is produced by �-cells. (See Chapter 17 III B 3 .)
23. B . Somatostatin and urogastrone both inhibit the production of hydrochloric acid, whereas gastrin enhances it. Secretin and cholecystokinin act on the pancreas to facilitate secretion of buffer and pancreatic enzymes, respectively. (See Chapter 16 III B 2.)
24. A. A deficiency of vitamin A inhibits bone formation and growth, whereas an excess stimulates ossification of the epiphyseal plates, thus leading to premature closure of the plates. Both conditions result in short stature. A deficiency of vitamin D reduces calcium absorption from the small intestine and results in soft bones, whereas an excess of vitamin D stimulates bone resorption. A deficiency of vitamin C results in poor bone growth and fracture repair. Vitamin K plays no role in bone formation. (See Chapter 7 II I .)
25. C. Membrane-coating granules are present in keratinocytes in the stratum spinosum (and stratum granulosum). The contents of these granules are released into the intercellular spaces to help waterproof the skin. Keratinocytes in the stratum granulosum also possess keratohyalin granules; these contain proteins that bind keratin filaments together. (See Chapter 14 II B 2.)
26. A. The nucleus of erythroblasts is not in the process of being extruded and is round with a very fine chromatin network. The cytoplasm is blue and possesses no granules. (See Chapter 10 VI C.)
27. B . The ileum includes Peyer patches. Rugae, parietal cells, and chief cells are located in the stomach. Brunner glands are present in the submucosa of the duodenum. (See Table 16 . 1 . )
28. B . Herpetic stomatitis i s characterized by painful fever blisters on the lips or near the nostrils . These blisters exude a clear fluid. Aphthous ulcers (canker sores) do not exude fluid. Bullous pemphigoid is an autoimmune disease marked by chronic generalized blisters in the skin. (See Chapter 16 II B Clinical Considerations.)
29. C. The skin, which consists of the epidermis and dermis, is important in the regulation of body temperature and contains temperature receptors in the dermis. Ultraviolet (not infrared) radiation absorbed by the skin is necessary for the synthesis of vitamin D. Protection against desiccation is provided by the contents of the membrane-coating granules of the epidermis. Melanocytes are located in the deepest layer of the epidermis (stratum basale) . Sunscreen with sun protection factor rating of 15 or higher offers no protection against ultraviolet light of longer wavelengths, that is, in the UVA spectrum. (See Chapter 14 I E.)
30. C. Patients with glomerulonephritis excrete protein in their urine. All of the other symptoms are characteristic of patients with diabetes insipidus, who are incapable of producing adequate amounts of antidiuretic hormone and therefore have polyuria (large volume of hypotonic urine production), polydipsia, and dehydration. (See Chapter 18 III A Clinical Considerations.)
31 . E. The anus is lined by stratified squamous keratinized epithelium. The rectum, jejunum, and pyloric stomach are lined by simple columnar epithelium. The esophagus is lined by stratified squamous (nonkeratinized) epithelium. (See Chapter 16 III D 4.)
32. D . Hyaline cartilage, elastic cartilage, and fibrocartilage all exhibit both interstitial and appositional growth. Hyaline cartilage and elastic cartilage have type II collagen in their matrix and are surrounded by a perichondrium, whereas fibrocartilage has type I collagen and lacks an identifiable perichondrium. Only hyaline cartilage is involved in endochondral bone formation. (See Chapter 7 I A, B, C.)

400 Comprehens ive Exam inati on
33. E . Meissner corpuscles, in the papillary layer of the dermis, are fine touch receptors. Pacinian corpuscles perceive pressure, touch, and vibration; they are located in the dermis, hypodermis, and connective tissue of mesenteries and joints. Cristae ampullares are special regions of the semicircular canals that detect circular movements of the head. Ruffini endings, in the dermis and joints, function in pressure and touch perception. Krause end bulbs are cold and pressure receptors in the dermis. (See Chapter 14 III A.)
34. C. Hyaline membrane disease, which results from inadequate amounts of pulmonary surfactant, is characterized by labored breathing and is typically observed in premature infants. Glucocorticoids stimulate synthesis of surfactant and can correct the condition. (See Chapter 15 VIII D Clinical Considerations.)
35. A. The cribriform plate, the inner layer of the alveolar bone, is composed of compact bone. It is attached to the principal fiber groups of the periodontal ligament via Sharpey fibers. The outer layer of the alveolar bone is the cortical plate. The spongiosa is the region of cancellous (spongy) bone enclosed between the cortical and cribriform plates. (See Chapter 16 II D 3 . )
36. C. Somatotropin (growth hormone) is synthesized by cells called somatotrophs, which are acidophils located in the pars distalis of the anterior lobe of the pituitary gland. Oxytocin and antidiuretic hormone (also called vasopressin) are produced in the hypothalamus and transported to the pars nervosa of the pituitary. Neurophysin, a binding protein, aids in this transport. (See Chapter l3 III A 1 a.)
37. D . Mutations in the BRCA1 gene, a breast tumor suppressor gene, are the major cause of breast cancer. In most breast cancers involving this gene, deoxyribonucleic acid synthesis proceeds, indicating that the G 1 -S checkpoint is not affected; however, the mutated cells cannot control the transition between G2 and M. Moreover, the mutated cells had abnormal centrosome numbers, and their nuclear division did not proceed normally, leading to aneuploidy and genetic instability of the daughter cells. (See Chapter 19 X C Clinical Considerations.)
38. C. The patient has an immediate (type I) hypersensitivity reaction. The cells responsible for releasing the primary and secondary mediators are the mast cells. (See Chapter 6 III D.)
39. D . Bradykinins are the only listed pharmacological agents that are produced via the arachidonic acid pathway. All of the others are primary mediators because they are stored in the storage granules of mast cells. (See Chapter 6 III D.)
40. D . Basophils are very similar in function to mast cells. They also participate in the immediate (type I) hypersensitivity reaction. (See Chapter 6 III H 3.)
41 . B . The only hard tissue of the tooth that cannot be repaired by the body is enamel because ameloblasts, the cells that manufacture enamel, are eliminated as the tooth emerges into the oral cavity. (See Chapter 16 II C 2.)
42. C. Osteomalacia, or adult rickets, is Lisa's disorder. It is characterized by a failure of newly formed osteoid to calcify because there is a lack of calcium, vitamin D, and phosphorus. The bones gradually soften and bend, and pain accompanies the condition, which often becomes severe during pregnancy as the fetus removes calcium from the mother's body. Osteogenesis imperfecta is a genetic condition affecting the synthesis of type I collagen in the bone matrix and results in extreme bone fragility and breakage. Osteoporosis is a disease characterized by low bone mineral density and structural deterioration, making bone more susceptible to fracture, and osteopenia is reduced bone mass caused by inadequate osteoid synthesis. Osteopetrosis is the excessive formation of bone, which obliterates the marrow cavities and thus impairs the formation of blood cells. (See Chapter 7 II I Clinical Consideration.)
43. A. The pigmented epithelium (layer 1 ) was separated from the layer of rods and cones (layer 2), which make up the light-sensitive part of the neural retina. (See Chapter 2 1 III E Clinical Consideration.)

Comp rehens ive Exam i nat ion 401
44. C. The extrinsic pathway is initiated by the release of tissue thromboplastin after trauma to extravascular tissue. Platelet aggregation is promoted by von Wille brand factor, which is associated with the intrinsic pathway only. Calcium is required in both pathways, and the final reaction-the conversion of fibrinogen to fibrin-is the same in both. (See Chapter 10 III D 1 . )
45. D . Eosinophils are increased in parasitic infections and allergic reactions. Both eosinophils and basophils have receptors for immunoglobulin E, which seems to be important in the destruction of parasites. Both neutrophils and monocytes lack immunoglobulin E receptors. (See Table 10 .2 . )
46. D . The inner ear is where sound waves are transduced into nerve impulses that convey auditory information to the brain, and the hair cells of the organ of Corti play a key role in this process. Sound waves are initially received by the outer ear and transmitted via the tympanic membrane (eardrum) to the middle ear, where ossicles transmit the vibrations to the inner ear. The inner ear has an auditory system for hearing (the organ of Corti) and a vestibular system of semicircular ducts that control equilibrium and spatial orientation. (See Chapter 21 IV C e 8.)
47. B . Plasma fibronectin functions in wound healing, blood clotting, and phagocytosis of material from the blood. (See Chapter 4 II C 1 . )
48. D . Matrix fibronectin mediates cell adhesion to the extracellular matrix by binding to fibronectin receptors on the plasma membrane. (See Chapter 4 II C 1 . )
49. E. Chondronectin has binding sites for type I I collagen, proteoglycans, and chondrocyte cell-surface receptors. (See Chapter 4 II C 5 . )
50. D . Plasma cells, which arise from antigen-activated B lymphocytes, produce antibodies and are thus directly responsible for humoral-mediated immunity. (See Chapter 6 III G.)
51 . B. Macro phages, the principal phagocytes of connective tissue, remove large particulate matter and assist in the immune response by acting as antigen-presenting cells. (See Chapter 6 III E.)
52. E. Mast cells (and basophils) have receptors for immunoglobulin E antibodies on their surface. These cells release histamine, heparin, leukotriene C (slow-reacting substance of anaphylaxis), and eosinophil chemotactic factor, which have effects that constitute immediate hypersensitivity reactions. (See Chapter 6 III D.)
53. C. T lymphocytes initiate cell-mediated immune responses. (See Chapter 6 III F.)
54. A. Pericytes are smaller than fibroblasts and are located along capillaries. When necessary, they assume the pluripotential role of embryonic mesenchymal cells. (See Chapter 6 III B .)
55. E. G proteins are membrane proteins that are linked to certain cell-surface receptors. Upon binding of a signaling molecule to the receptor, the G protein functions as a signal transducer by activating a secondary messenger system that leads to a cellular response. (See Chapter 1 IV B 2 c.)
56. A. K+ leak channels are ion channels that are responsible for establishing a potential difference across the plasma membrane. (See Chapter 1 III C 1 . )
57. A . The term "amphipathic" refers to molecules, such as phospholipids, that possess both hydrophobic (nonpolar) and hydrophilic (polar) properties. The plasma membrane contains two phospholipid layers (leaflets), with the hydrophobic tails of the molecules projecting into the interior of the membrane and the hydrophilic heads facing outward. (See Chapter 1 II A 2.)
58. B . The glycocalyx (cell coat) is associated with the outer leaflet of the plasma membrane. It is composed primarily of proteoglycans, which possess polysaccharide side chains. (See Chapter 1 II C 1 . )
59. C. Membrane carrier proteins are highly folded transmembrane proteins that undergo reversible conformational alterations, resulting in transport of specific molecules across the membrane. The Na+ -K+ pump is a carrier protein that mediates anti port transport, the transport of two molecules concurrently in opposite directions. (See Chapter 1 II B 1 . )

402 Comprehens ive Exam inati on
60. B . T killer cells (cytotoxic T lymphocytes) have CDS marker molecules on their surfaces. (See Chapter 12 II B 3.)
61 . A. T helper cells have CD4 marker molecules on their surfaces. (See Chapter 12 II B 3.)
62. E . Perforin, which is released by cytotoxic T cells, mediates lysis of tumor cells and virus-infected cells. (See Chapter 12 II B 3.)
63. C. Interleukin 1 , which is produced by macrophages, stimulates activated T helper cells. In turn, activated T helper cells produce interleukin 2 and other cytokines involved in the immune response. (See Chapter 12 II E 2.)
64. B . Interferon-'{ (macrophage-activating factor) stimulates activation of natural killer cells and macro phages, thereby increasing their cytotoxic and/ or phagocytic activity. (See Chapter 12 II D 3.)
65. B . Primary spermatocytes undergo the first meiotic division following deoxyribonucleic acid replication in the S phase. The resulting secondary spermatocytes undergo the second meiotic division, without an intervening S phase, forming spermatids. (See Chapter 20 II D 4 b.)
66. E . During spermiogenesis, the manchette is formed. This temporary structure aids in elongation of the spermatid. (See Chapter 20 II D 5 c.)
67. D . Interstitial cells of Leydig produce testosterone when they are stimulated by LH. (See Chapter 20 II C 4.)
68. A. Sertoli cells are columnar cells that extend from the basal lamina to the lumen of the seminiferous tubules. Adjacent Sertoli cells form basal tight junctions, which are responsible for the blood-testis barrier, thus protecting the developing sperm cells from autoimmune reactions. (See Chapter 20 II D 2.)
69. A. Sertoli cells produce androgen-binding protein, which binds testosterone and maintains it at a high level in the seminiferous tubules. (See Chapter 20 II D 2.)
70. B . Smooth endoplasmic reticulum possesses mixed-function oxidases that detoxify phenobarbital and certain other drugs. (See Chapter 3 II 4 .)
71 . A. The membrane of the rough endoplasmic reticulum contains ribophorins, receptors that bind the large ribosome subunit. (See Chapter 3 II A 3 . )
72. E . The lysosome is the organelle where the degradation of foreign material takes place in the cell. The term "heterophagy" refers to the ingestion and degradation of foreign material, in contrast to autophagy, where parts of the cell itself are digested and degraded. (See Chapter 3 III C 2.)
73. C. The inner membrane of the mitochondrion contains adenosine triphosphate synthase, a special enzyme consisting of a head portion and a transmembrane H+ carrier; as H+ passes through adenosine triphosphate synthase, the enzyme uses the energy of the proton flow to drive the production of adenosine triphosphate. (See Chapter 3 II A 6 d.)
74. A. Gastrin, a paracrine hormone secreted in the pylorus and duodenum, stimulates pepsinogen secretion by chief cells in the gastric glands. (See Chapter 16 III B 2.)
75. C. Urogastrone, produced by Brunner glands in the duodenum, inhibits gastric hydrochloric acid secretion and enhances division of epithelial cells. (See Chapter 16 III C 4.)
76. E. Lysozyme, manufactured by Paneth cells in the crypts of Lieberkiihn, is an enzyme that has antibacterial activity. (See Chapter 16 III C 3 b (3) a.)
77. C. Motilin, a paracrine hormone secreted by cells in the small intestine, increases gut motility by stimulating smooth muscle contraction. (See Table 16 .2 .)
78. B. Somatostatin, produced by enteroendocrine cells in the pylorus and duodenum, inhibits secretion by nearby enteroendocrine cells. (See Table 16.2 .)

Comp rehens ive Exam i nat ion 403
79. A. Lysine and hydroxylysine residues within and between tropocollagen molecules form cross-links with each other or with other lysines or hydroxylysines. These covalent links add great tensile strength to the newly formed fibril. (See Chapter 4 III A 1 .)
80. A. Lysine cross-links elastin molecules, forming a network. Fibrillin is the glycoprotein that organizes elastin into fibers. (See Chapter 4 III B 1 . )
81 . A . Simple goiter is an enlargement of the thyroid gland resulting from inadequate dietary iodine ( < 1 0 fig/d) . It is common where the food supply is low in iodine. (See Chapter 13 IV D Clinical Considerations.)
82. D . Addison disease is most commonly caused by an autoimmunity that destroys the adrenal cortex. As a result, inadequate amounts of glucocorticoids and mineralocorticoids are produced. Unless these are replaced by steroid therapy, the disease is fatal. (See Chapter 13 VI A Clinical Considerations.)
83. B . The globular head of the myosin molecule has adenosine triphosphatase (ATPase) activity, but interaction with actin is required for the non-covalently bound reaction products adenosine diphosphate (ADP) and Pi to be released. This ATPase activity is retained by the S 1 fragment resulting from digestion of myosin with pro teases. (See Chapter 8 I I F 2.)
84. C. Myoglobin, a sarcoplasmic protein, like hemoglobin, can bind and store oxygen. The myoglobin content of red (slow) muscle fibers is higher than that of white (fast) muscle fibers. (See Chapter 8 II B 2.)
85. A. Troponin C is one of the three subunits of troponin that along with tropomyosin binds to actin (thin) filaments in skeletal muscle. Binding of Ca2+ by troponin C results in unmasking of the myosin-binding sites on thin filaments. (See Chapter 8 II F 2.)
86. C. Malignant melanoma, a relatively rare form of skin cancer, arises from melanocytes. It is aggressive and invasive. Surgery and chemotherapy are usually necessary for successful treatment of this cancer. (See Chapter 14 II B Clinical Considerations.)
87. A. Epidermolysis bullosa is a group of hereditary skin diseases characterized by the separation of the layers in skin with consequent blister formation. (See Chapter 14 II D Clinical Considerations.)
88. B . The nasopharynx is the site of the pharyngeal tonsil; when enlarged and infected, this tonsil is known as an adenoid. (See Chapter 15 II B . )
89. A. The trachea and extrapulmonary (primary) bronchi have walls supported by C-shaped hyaline cartilages (C-rings), whose open ends face posteriorly. (See Chapter 1 5 II D.)
90. D . The alveolar duct has alveoli with openings that are rimmed by sphincters of smooth muscle. Alveoli more distal than these have only elastic and reticular fibers in their walls. (See Chapter 15 III B . )
91 . C. Terminal bronchioles are lined by a simple cuboidal epithelium containing ciliated cells and Clara cells. Clara cells can divide and regenerate both cell types. (See Chapter 15 II F 2.)
92. C. An ectopic tubal pregnancy occurs when the embryo implants in the wall of the oviduct (rather than in the uterus). Because the oviduct cannot support the developing embryo, the duct eventually bursts, causing hemorrhaging into the peritoneal cavity. (See Chapter 19 VI B Clinical Considerations.)
93. D . Breast cancer that originates from the epithelium lining the terminal ductules of the mammary gland is classified as lobular carcinoma. (See Chapter 19 X C Clinical Considerations.)
94. B . Abnormal cells associated with cervical cancer are revealed in a Papanicolaou smear, providing a simple method for the early detection of this cancer. (See Chapter 19 V E Clinical Considerations.)

404 Comprehens ive Exam inati on
95. A. Endometriosis is a condition in which uterine endometrial tissue is located in the pelvic peritoneal cavity. The misplaced endometrial tissue undergoes cyclic hormone-induced changes, including menstrual breakdown and bleeding. (See Chapter 19 IV A 1 c Clinical Considerations.)
96. E . Gastric intrinsic factor, which is produced by parietal cells in the gastric glands, is necessary for absorption of vitamin B12 in the ileum. (See Chapter 16 III B 2.)
97. B . Disaccharidases in the glycocalyx of the striated border hydrolyze disaccharides to monosaccharides. (See Chapter 16 IV A 2.)
98. A. Digestion of proteins begins with the action of pepsin in the stomach, forming a mixture of polypeptides. Activation of pepsinogen to pepsin only occurs at a low pH. (See Chapter 16 IV B 1 .)
99. D . After free fatty acids and monoglycerides in micelles enter the surface absorptive cells of the small intestine, they are reesterified to form triglycerides. These are complexed with proteins, forming chylomicrons, which are released from the lateral cell membrane and enter lacteals in the lamina propria. (See Chapter 16 IV C 2.)
1 00. E . Parietal cells are responsible for establishing the low pH of the stomach by manufacturing hydrochloric acid. Another function of parietal cells is the synthesis and release of gastric intrinsic factor, necessary for the absorption of vitamin B12 in the ileum. (See Chapter 16 III B 2 a.)

Index
Note: Page numbers followed by f denote figure; those followed by t denote table.
A Abdominal pain, symptoms of, 291 , 293 Acetylcholine, 132- 133, 152t, 162, 164, 189
receptors, 7 Acidophils, 222 Acoustic nerve, 378f Acquired immunodeficiency syndrome
(AIDS), 144, 205, 398 Acromegaly, 120 Acrosomal reaction, 355 Actin, 10, lOf, 1 1 , 126f Actin-binding proteins, 48, 48t Actin filaments, 77, 83
function, 48 structure, 4 7
Action potential, 156 Activated platelets, 173 Active transport, 5
ATP-binding cassette transporters, 6 glucose transport, 6 Na•-K• pump, 6
Acute leukemia, 171 Acute myelogenous leukemia, 2 1 Adaptins, classes of, 38 Adaptive immune system, 200 Addison disease, 236, 394, 403 Adenine, 21 Adenocarcinoma, 88, 397
of prostate gland, 361 Adenohypophysis, 222, 224f
pars distalis, 222-223 pars tuberalis, 225
Adenoid, 259 Adenosine diphosphate (ADP), 37 Adenosine triphosphate (ATP), 131, 394, 403
-binding cassette transporters (ABC-transporters), 6
exchange proteins, 37 synthase, 36, 394, 402 synthesis, 37
Adipokines, 101 Adiponectin, 101 Adipose cells, 94 Adipose tissue, 100 Adipose tumors, 102 ADP-ribosylation factor (ARF), 40 Adrenal cortex, 234
zona fasciculata of, 387, 397 Adrenal glands, 234
adrenal cortex, 234, 235f zona fasciculata, 234, 235f zona glomerulosa, 234 zona reticularis, 234
adrenal medulla, 236-237 catecholamine release, 237 chromaffin cells, 236-237 sympathetic ganglion cells, 236
blood supply to, 237 cortical blood supply, 237 medullary blood supply, 237
cells and hormones, 234t
Adrenocorticotropic hormone (ACTH), 14, 239, 241 Adrenoleukodystrophy, 45 Adventitial reticular cells, 174 Afadin, 77 Afferent arterioles, 320 Age pigment, 46 Age-related macular degeneration (AMD), 375-376 Agranulocytes, 167t, 170-171 , 17lt Albumin, 166 Alimentary canal
esophagus, 279 histological features of, 278t hormones secreted by cells of, 28lt immune system of, 285 large intestine, 285-288 small intestine, 282-285 stomach, 279-282
a-actinin, 10f, 1 1 , 65f a-globulins, 166 A! port syndrome, 69, 315 Alveolar ducts, 264, 264f, 395, 403 Alveolar macrophages, 267 Alveolar sacs, 264, 264f Alveoli, 264-266 Alzheimer disease, 148 Amphipathic molecule, 1 , 392, 401 Ampullae, 380 Amyloid �-derived diffusible ligands (ADDLs), 299 Amyotrophic lateral sclerosis (ALS), 133 Anabolic steroid use, 127 Anagen phase, 252 Anaphase, of mitosis, 26-27, 26f, 27t Anaphylactic shock, 98 Anchoring junctions, of epithelial cells, 79 Androgen-binding protein (ABP), 353, 356, 393, 402 Androgenic alopecia. See Male pattern baldness Anencephaly, 144 Aneuploidy, 30 Aneurysm, 189 Angiotensin I, 195 Angiotensin II, 195 Angular cheilitis, 274 Ankyrin, 10, 10f Annexins, 4 Annulate lamellae, 35 Anterior chamber lateral angle, 369f Antibody-dependent cell-mediated cytotoxicity
(ADCC), 208 Anticodon, 23 Antidiuretic hormone (ADH), 195, 3 18, 322 Anus, 390, 399 Aorta, 186, 187f Aortic bodies, 195 Apocrine sweat glands, 88, 250 Apoptosis, 28 Appendicitis, 288 Aquaporins, 5 Aqueous humor, 370, 371 , 384, 386 Areolar tissue, 99 Arginine vasotocin, 238 Arteries. See Blood vascular system, arteries
405

406 I n d ex
Arterioles, 188, 193f Arteriosclerosis, 189 Arteriovenous shunt, 19 1 Arthritis, 109 Articular cartilage, 103, 105 Asbestosis, 267 Ascaris lumbricoides, 391, 401 Aspartate, 152t Asthma, 98, 262 Astrocytes, 148-149 Atherosclerosis, 50, 188 Atretic follicles, 336 Atria, 184-185 Atrial granules, 134- 135 Atrial natriuretic peptide (ANP), 134, 184 Atrioventricular (AV) bundle of His, 185 Atrioventricular node, 185 Atrioventricular valves, 185 Auditory tube, 378f, 379 Autocrine hormones, 7 Autographs, 1 1 9 Autoimmune diseases, 7 Autophagic vacuoles, 44, 45f, 56 Autophagolysosomes, 44-45 Autophagy, 56 Autosomes, 21 Axoaxonic synapses, 15 1 Axodendritic synapses, 151 Axolemma, 148, 153 Axonal transport, of materials, 156 Axoneme, 84, 84f Axon hillock, 146f, 14 7 Axons, 145f, 147- 148, 154f
peripheral, 161 Axon terminals, 132, 152 Axoplasm, 148 Axosomatic synapses, 146f, 15 1
B Bacterial flora of oral cavity, action of, 27 4 Band 3 proteins, 10 Band 4 . 1 protein, 10, 10f Bardet-Biedl syndrome (BBSome), 86 Barr body, 19 Basal body, at base of cilia, 84-85, 84f Basal lamina, 80-81, 81f, 136f, 154f Basal plasma membrane infoldings, 83 Basement membrane, 75, 80-81 Basilar membrane, 380 Basophilic erythroblasts, 177t, 389, 399 Basophils, 178, 222-223, 391 , 400
granulocytes, 99 vs. neutrophils, 387, 397
Benign prostatic hypertrophy (BPH), 360 Bernard-Soulier syndrome, 174 �-globulins, 166 Bile, 301-302 Bile ducts, 302 Bipolar neurons, 145, 145f Bladder cancer, 21, 326 Blood and hemopoiesis, 166
blood coagulation, 172 activated platelets, 173 common pathway, 173 extrinsic pathway, 173 intrinsic pathway, 173 phospholipid complexes of activated platelet
membranes, 173
bone marrow, 174, 175f erythrocytes (red blood cells)
general features of, 167-168, 167t hematocrit, 1 68 hemoglobin (Hb), 169 transport of C02 and 02 by, 169
hemopoietic growth factors, 179, 180t leukocytes (white blood cells), 167f, 167t, 170
agranulocytes, 170- 171 , 17lt granulocytes, 170, 170t
plasma, 166 platelets (thrombocytes), 167f, 167t, 171- 172, 172t postnatal hemopoiesis
blood formation, initial steps in, 176 erythrocyte formation, 176 granulocyte formation, 176-178 lymphocyte formation, 179 monocyte formation, 178 platelet formation, 178 precursor cells, 176 progenitor cells, 176 stem cells, 175
prenatal hemopoiesis, 175 review test, 181- 182
answers and explanations, 183 Blood-brain barrier, 159, 191 Blood coagulation, 172-173
intrinsic pathway of, 391 , 401 Blood-gas barrier, lung, 268 Blood-testis barrier, 393, 402 Blood vascular system, 184. See also Lymphatic
vascular system arteries, 186, 188f
arterioles, 188 elastic arteries, 186 metarterioles, 189 muscular arteries, 186 sensory mechanisms in, 194-195 vasoconstriction, 189 vasodilation, 189 and veins, comparison of, 192, 194f wall, layers of, 186, 186t
capillaries, 189, 190f arteriovenous shunt, 191 blood flow to capillary beds, 191 , 193f capillary endothelial cells, 189, 192t continuous (somatic) capillaries, 190f, 19 1 fenestrated (visceral) capillaries, 190f, 19 1 metabolic functions of, 191 permeability of, 191 sinusoidal capillaries, 190f, 191
heart, 184 atrioventricular valves, 185 cardiac layers, 184-185 fibrous skeleton of, 185 impulse-generating and impulse-conducting
system, 185 pericardium, 184 semilunar valves, 185
hormonal control of low blood pressure, 195 review test, 196-197
answers and explanations, 198 veins, 192
large veins, 193 small and medium-sized veins, 194 types of, 193t venules, 194 walls, layers of, 192, 193t

B lymphocytes (B cells), 98, 179, 207-208 Bone, llO
cells osteoblasts, ll0- ll1 osteoclasts, ll1-ll3, ll3f osteocytes, 1 l l osteoprogenitor cells, llO
classification of, ll3 compact (dense) bone, l l3 primary bone, l l3 secondary bone, ll3 spongy (cancellous) bone, ll3
development, and mineralization, 80 formation
hormones role in, 120 vitamins role in, ll9
fracture, repair of, l l9 histogenesis of, ll4
calcification of bones, ll8 endochondral bone formation, ll5-ll8 intramembranous bone
formation, ll5, ll6f zones of epiphyseal plates, 1 18
organization of lamellae in haversian systems, l l4 interstitial lamellae, l l4 outer and inner circumferential
lamellae, ll4 remodeling, l l8-ll9 repair, ll9 review test, 121-122
answers and explanations, 123 sialoprotein, l l 0 structure
bone matrix, llO endosteum, llO periosteum, llO
Bone morphogenic protein (BMP) family, llO Bony callus, formation of, ll9 Bony joints, 387, 397 Bony labyrinth, 379 Botox, 42, 249 Botulism, 133 Bowman membrane, 369 Bowman space, 3ll, 313 Bradykinin, 390, 400 Brain gray matter, 158 BRCA1 gene, mutations in, 390, 400 Breast cancer, 347, 395, 403 Brown adipose tissue, 102 Brown fat cells, 37 Bruch membrane, 370 Brunner glands, 285 B-type natriuretic peptide (BNP), 134, 184 Bulbourethral glands, 361 Bullous pemphigoid, 83 Burkitt lymphoma, 171
c Calcitonin, 120, 23 1 Calcium ions, 131 , 134 Canal of Schlemm, 369f, 370
aqueous humor and, 384, 386 Cancellous bone. See Spongy bone Cancers, oral region, 274 Capillaries. See Blood vascular
system, capillaries Capsular space. See Bowman space
Carbohydrates, 289 digestion of, 396, 404
Carbon monoxide poisoning, 268 Carcinoma, 88
of cervix, 342 Cardiac arrest, 185 Cardiac layers, 184-185 Cardiac muscle cells, 133, 134t
features of, 133-134
I n dex 407
structural components of, 134-135 Carotid body, 194- 195 Carotid sinus, 194 Carrier proteins, 5, Sf Cartilage, 106
elastic cartilage, 109 fibrocartilage, 109 hyaline cartilage, 106- 109 review test, 121-122
answers and explanations, 123 types of, 106, 106t, 107f
Caspases, 28 Catagen phase, 252 Catalytic receptors, 8 Cataract, 372 Catecholamine release, 237 Caveolin-coated vesicles, 42 Cell cycle, 25, 25f
interphase, 25 control factors, 26 G1 phase, 25 G2 phase, 26 S phase, 25
mitosis, 26, 26f anaphase, 27 metaphase, 27 prometaphase, 27 prophase, 26-27 stages of, 27t telophase, 27
Cell signaling, 5 Central memory T cells (TCMs ), 205 Central nervous system (CNS), 143
cerebrospinal fluid, 159 meninges, 158 white matter and gray matter, 158
Centriole, 9 + 0 configuration, 85f Centrosome
function, 47 polymerization of tubulin, 47f structure, 46-4 7
Cerebrospinal fluid (CSF), 159 Cervical cancer, 342, 395, 403 CPU-Meg (MKP cells), 178 Channel-linked receptors, 8 Chemiosmotic coupling mechanism,
mitochondria, 36f, 37 Chloride channel proteins, 6 Chloride shift, 169 Cholecystitis, 305 Cholera-induced diarrhea, 286 Cholera toxin, 8 Cholesterol, plasma membrane, 2 Chondroblasts, 108 Chondrocytes, 107f, 108 Chondroitin sulfate, 62 Chondronectin, 64, 392, 401 Choroid, 369f, 370
characteristic of, 384, 386

408 I n d ex
Chromaffin cells, 236-237 Chromatin, 19. See also Nucleus, chromatin
condensed, 20 extended, 20 sex, 19
Chromophobes, 224 Chromosomes. See also Nucleus, chromosomes
nondisjunction of, 30 segregation checkpoint, 26 sex, 2 1
Chronic glaucoma, 371 Chronic leukemias, 171 Chronic renal failure, 3 15 Chylomicrons, 101 , 396, 404 Chyme, 279 Cigarette smoking, and lung cancer, 261 Cilia
motile, actively, 84-86 nonmotile, 86
Ciliary body, 369f, 370-371 Ciliary dynein arms, 84, 84f Ciliated cells, 395, 403 Circulatory System. See Blood vascular system;
Lymphatic vascular system Clara cells, 262, 395, 403 Clathrin-coated vesicles, 38, 40, 40f Claudins, 77 Cleavage, 343 Clostridium botulinum toxin, 388, 398 C02 transport, by erythrocytes, 169 Coagulation disorders, 174 Coated vesicles
caveolin-coated vesicles function, 42 structure, 42
clathrin-coated vesicles, 40f function, 38, 40 structure, 38
coatomer-coated vesicles function, 41-42, 4lf structure, 40
inositol phospholipids, 42 rab proteins, 43 retromer-coated vesicles, 42
Coatomer-coated vesicles, 40-42, 4lf Cochlea, 378f, 379
micrograph of, 38lf Cochlear duct and spiral organ of Corti, 380, 38lf Codon, 2 1 Cold receptors, 367f, 368 Collagen, 64
fibers, 92-93, 107f, 369 fibril-associated collagens, 70 fibril-forming collagens, 69-70
extracellular events in synthesis, 66-67, 67f, 68-69f
intracellular events in synthesis, 64, 66 network-forming collagens, 70 synthesis, 67f transmembrane collagens, 70 types, 65-66t, 69, 71
Colorectal carcinoma, 287 Colostrum, 347 Common variable immunodeficiency, 208 Compact bone, ll2f Complement proteins, 166 Concentric contraction, 132 Concentric lamellae, 1 12f
Conductive hearing loss, 379 Cones and rods, photoreceptor layer of retina, 374f, 375 Congenital immunodeficiency disorders, 201 Congenital malformations, 144 Congenital megacolon. See Hirschsprung disease Congenital thymic aplasia. See DiGeorge syndrome Conjunctiva, 369, 369f, 377 Conjunctivitis, 377 Connective tissue, 63
classification of connective tissue proper, 99- 102 embryonic connective tissue, 99 specialized connective tissue, 102
elements, 135 extracellular matrix, 92
fibers, 92-93 ground substance, 92
fixed cells of adipose cells, 94-95 fibroblasts, 93 mast cells, 95, 97 pericytes, 93
function, 92 origin of tissue cells, 94f principal phagocytes of, 392, 401 review test, 103-104
answers and explanations, 105 structure, 92 transient cells of, 98
granulocytes, 98-99 lymphoid cells, 98 macrophages, 98 plasma cells, 98
Connexin, 80, 334 Connexons, 80 Continuous (somatic) capillaries, 190f, 191 Contractile nonmuscle cells, 139 Cornea, 369f, 370
Bowman membrane, 369 corneal endothelium, 370 corneal epithelium, 369 corneal stroma, 369-370 Descemet membrane, 370
Corneal reflex (blink response), 370 Corpora cavernosa, 362 Corpus albicans, 336 Corpus hemorrhagicum, 335-336 Corpus luteum, 336 Corpus spongiosum, 362 Corti play, hair cells of organ of, 39 1 , 401 Cortisone, 1 09t Costameres, 128 Countercurrent exchange system, 323 Cowper glands. See Bulbourethral glands C protein, 130 Creatine kinase, 129 Cribriform plate, 390, 400 Crinophagy, 56 Cristae ampullares, 380 Cryptorchidism, 350 Crypts of Lieberkiihn, 284 Crystallins, 372 Cyclin-dependent kinases (CDKs), 26 Cystic fibrosis, 6 Cystic .fibrosis transmembrane conductance
regulator (CFTR) gene, 6 Cystinuria, 6 Cytokines, in immune response, 205, 206t

Cytoplasm, 33, 65f cytoskeleton, 46
actin filaments (microfilaments), 47-48 intermediate filaments, 48, 49t microtubules, 46 plectin, 48
inclusions, 46 centrosome, 46-47 glycogen, 46 lipid droplets, 46 lipofuscin, 46
interactions among organelles, 49 intracellular digestion, 56 protein synthesis, 50-54 uptake and release of material
by cells, 49-50 organelles, 34f
annulate lamellae, 35 coated vesicles, 38, 40, 40f Golgi apparatus, 37, 38f, 39f lysosomes, 43-45 mitochondria, 36-37 peroxisomes, 45 plasma membrane, 33, 34f ribosomes, 33-34, 34f rough endoplasmic reticulum,
34-35, 34f, 35f smooth endoplasmic reticulum, 35
review test, 58-59 answers and explanations, 60
structural components, 33-49 Cytoplasmic dynein, 46 Cytoplasmic organelles, 138 Cytoskeleton, 46-48
D Darier disease, 80 Deafness, 80 Deep brain stimulation, 15 1 Defective G, proteins, 8 Demyelination, 153 Dendrites, 145, 145f, 146f, 147, 246 Dendrodendritic synapses, 15 1 Dense connective tissue, 99
irregular, 99 regular, 99
Deoxyribonucleic acid (DNA), 15, 393, 402 double helix, 2 1 structure of, 21
Dermal papillary layer, 248 Dermal reticular layer, 248-249 Dermis, 248-249 Descemet membrane, 370 Desmin, 125, 128 Desmin-related myopathy (DRM), 125 Desmoplakin, intracellular
trafficking of, 79, 80 Desmosome, 79, 136f Detached retina, 391, 400 Diabetes insipidus, 226, 323 Diabetes mellitus, 323
type III, 148 Diarthroses, 387, 397 Diffuse axonal injury, 1 1 Diffuse lymphoid tissue, 21 1-212 Diffuse neuroendocrine system (DNES) cells, 221 ,
229, 247, 281-282 DiGeorge syndrome, 215
Digestive system, 273 alimentary canal, 278-279
esophagus, 279
I n dex 409
histological features of, 278t hormones secreted by
cells of, 28lt immune system of, 285 large intestine, 285-288 small intestine, 282-285 stomach, 279-282
digestion and absorption carbohydrates, 289 fats, 289 proteins, 289 water and electrolytes, 289
function of, 273 oral region
dental-supporting structures, 275 lips, 273 palate, 274 teeth, 274-275 tongue, 275-277
review test, 291-292 answers and explanations, 293
Dilator pupillae muscle, 371 Diploid number, 2 1 Diploid zygotes, 29 Disse, space of, 301 Diverticulitis, 286-287 Dopamine, 152t, 162, 164 Double negative T cells, 202 Double positive T cells, 202 Down syndrome (trisomy 21), 30 Dry macular degeneration, 375 Duchenne muscular dystrophy
(DMD), 128 Ductuli efferentes, 358 Ductus epididymis, 358-359 Dystrobrevin, 128 Dystroglycan complex, 128 Dystrophin, 128
E Ear, sense of hearing, 378-383 E-cadherin, 79 Eccrine sweat glands, 248f, 249 Ectoderm, 144f Ectopic tubal pregnancy, 343, 395, 403 Edema, 99, 195 Effector T cells, 205 Ehlers-Danlos type IV syndrome, 67 Elastic arteries, 186 Elastic cartilage, 106t, 109, 390, 399 Elastic fibers, 93, 107f
components elastin, 70 fibrillin- 1 , 70 fibulin-5, 71 type VIII collagen, 71
synthesis of, 7 1 Elastic tissue, 100 Elastin, 70 , 93 Electrical synapses, 152-153 Embryonic connective tissue, 99 Emphysema, 267 Enamel, 391, 400 Endocardium, 184 Endocrine glands, 88
tahir99-VRG & vip.persianss.ir

41 0 I n d ex
Endocrine system, 221 adrenal glands (see Adrenal glands) function of, 221 glands of, 221 hormones, 221
lipid-soluble hormones, 221 water-soluble hormones, 221
parathyroid glands, 232-233, 233f chief cells, 232-233 oxyphil cells, 233 parathyroid hormone (PTH), 233
pineal gland, 237 neuroglial cells, 238 pinealocytes, 238
pituitary gland (see Pituitary gland) review test, 239-240
answers and explanations, 241 thyroid gland, 228, 229f
follicular cells, 228, 230f parafollicular cells, 229, 232f thyroid follicles, 228, 230f thyroid hormones, physiological
effects of, 231 Endocytic pathways, used by cells, 50, 5 lf Endocytosis, 49
phagocytosis, 50 pinocytosis, 49 receptor-mediated endocytosis, 50
Endogenous immunogens, 209 Endolymphatic duct, 380 Endolymphatic sac, 380 Endometriosis, 339, 395, 404 Endomysium, 124 Endoneurium, 154, 154f Endoplasmic reticulum, 34f Endorphins, 152t Endosomes
early, 43 late, 43-44
Endosteum, 1 1 0 Endothelium, corneal, 370 Enkephalins, 152t Entactin, 64 Enteric nervous system, 157, 279 Eosinophils, 99, 391 , 401 Ependymal cells, 150 Epicardium, 185 Epidermis
Langerhans cells, 246-247 melanocytes, 246 Merkel cells, 247 nonkeratinocytes in, 246-247 stratum basale, 246 stratum corneum, 245, 245f stratum granulosum, 245 stratum lucidum, 243 stratum spinosum, 243
Epidermolysis, 397 Epidermolysis bullosa, 248, 395, 403 Epimysium, 124 Epineurium, 153, 154f Epithelia, 63, 75
apical epithelial surfaces, 83 cilia, 84-86, 84f microvilli, 83 stereocilia, 83
basal epithelial surfaces, 80 basal plasma membrane infoldings, 83 basement membrane, 80-81
focal adhesions, 82 hemidesmosomes, 82-83
classification, 75-76, 75t, 76f function, 76-77 glands, 87
classification, 87-88 structure, 87
junctional complex, anchoring junctions, 79 lateral epithelial surfaces, 77-80
gap junction, 79-80 junctional complex, 77, 78f, 79 lateral interdigitations, 80
pseudostratified epithelia, 76, 76f review test, 89-90
answers and explanations, 9 1 structure, 75
Epithelial cell tumors, 88 Epithelial-mesenchymal interaction, 275 Epithelial reticular cells, 213, 2 14f, 215 Epitopes, 201 , 208 Epstein-Barr virus (EBV), 171 Erythroblastosis fetalis, 168 Erythrocytes (red blood cells), 167-168, 167t
formation, 176 hematocrit, 168 hemoglobin, 169 precursor cells, 176, 1 77t transport of C02 and 02 by, 169
Erythroid progenitor cells, 176 Erythropoiesis, 176 Escherichia coli, 285 Estradiol, 1 09t Estrogen, 337 Euchromatin, 16f, 19, 388, 398 Eustachian tube, 379 Examination, comprehensive, 387-396
answers and explanations, 397-404 Excessive apoptosis, 28 Exocrine glands, 87-88 Exocrine pancreas, 296-297 Exocytosis, 50 Exogenous immunogens, 209 Exons, 21, 23 Exportins, 17 External auditory meatus, 378, 378f External ear, 378 External elastic lamina, 186 External lamina, 136f Exteroceptors, 366 Extracellular matrix (ECM), 92-93
fibers collagen, 64-71 elastic fibers, 70-71
functions, 61 glycoproteins of, 63t ground substance
fibronectin receptors, 64, 65f glycoproteins, 63-64 glycosaminoglycans (GAGs), 61, 62t proteoglycans, 63
review test, 72-73 answers and explanations, 74
structure, 61, 62f Extrapulmonary bronchi, 260, 403 Eye floaters, 373 Eyelids, 377 Eyes, sense of sight
accessory structures of, 377-378 refractive media of, 371-372
tahir99-VRG & vip.persianss.ir

F
retina, 373-376 tunica fibrosa, 368-370 tunica vasculosa, 370-371
Facial nerve, 378f Facilitated diffusion of ions
gated ion channels, 6-7 ionophores, 7 K+ leak channels, 6 in passive transport, 5
Facioscapulohumeral muscular dystrophy, 128
F-actin, 65f, 77, 129 Factor VIII deficiency (hemophilia A),
174, 398 Familial hypercholesterolemia, 50 Fasciae adherents, 79 Fascial junctions, 136f Fascia occludens, 79 Fats, 289 Fatty acyl tail, plasma membrane, 1 , 2f Fecal transplant, 287 Female pattern baldness, 253 Female reproductive system, 330
cervix, 341 fertilization and implantation, 342-343 mammary glands, 346
active, 346 nipple, 346 resting, 346 secretions of, 34 7
ovaries (see Ovaries) oviducts (fallopian tubes), 338
mucosa, 338-339, 338f muscularis, 338f, 339 serosa, 339
placenta, 343-345 review test, 348
answers and explanations, 349 uterus (see Uterus) vagina, 345 vulva, 345-346
Fenestrated (visceral) capillaries, 190f, 19 1 Fertilization, 342-343 Fibers, 64-71
connective tissue, 92 collagen fibers, 92-93 elastic fibers, 93 reticular fibers, 93
Fibrillar centers, 18 Fibrillin, 71 Fibrils, 66 Fibrinogen, 166 Fibroblasts, 93 Fibrocartilage, 106t, 109, 390, 399 Fibronectin, 65f
function, 63 receptors, 64, 65f types and location, 63
Fibrous astrocytes, 149 Fibulin-5, 71 First-degree burns, 77 Fluid mosaic model, of plasma membrane, 1-4 Focal adhesions, 82 Follicle-stimulating hormone (FSH), 333, 334 Follicular cells, 228, 230f Folliculogenesis, time period of, 335 Folliculostellate cells, 224
Fordyce granules, 273 Foreign body giant cells, 98 Fovea centralis, 373 Free nerve endings, 367f, 368
G G1 DNA damage checkpoint, 26 G2 damage checkpoint, 26 Gallbladder, 304, 304f, 389, 398 Gallstones, 305
I n dex 41 1
y-aminobutyric acid (GABA), 152t, 162, 164 y-globulins, 166 Ganglia, 155 Ganglion, 144f, 376
dorsal root, 158f Gap junctions, 79-80 Gastric intrinsic factor, 396, 404 Gastric mucosa, 279 Gastric muscularis externa, 280 Gastric submucosa, 279-280 Gastrin, 282, 389, 394, 399, 402 Gated ion channels, 6-7
ligand-gated channels, 7 mechanically gated channels, 6 voltage-gated channels, 6
Gene, 2 1 Genetic apparatus, o f mitochondria, 36 Genome, 2 1 Glands, 87-88
of digestive system, 294 gallbladder, 304 liver, 299-304, 300f, 302f pancreas, 296-298, 297f, 298t review test, 306-307, 308 salivary glands, 294-295
endocrine, 88 exocrine, 87-88 structure, 87
Glans penis, 362 Glanzmann's thrombasthenia, 174 Glaucoma, 371 Glial fibrillary acidic protein, 59, 60 Glial ftlaments, 59, 60 Globular actin monomers (G actin), 58, 60 Glomerulonephritis, 314, 390, 399 Glucagon, 298 Glucocorticoids, 266, 271, 272, 387, 397 Glucosamine, 62 Glucose transport, 6 Glutamate, 152t, 162, 164 Gluten enteropathy, 286 Glycine, 70, 152t Glycocalyx (cell coat), 2, 392, 40 1
composition, 4 function, 4 of striated border, 396, 404
Glycogen, 46 storage diseases, 57
Glycolipids, plasma membrane, 2 Glycoproteins, 4, 63, 63t
chondronectin, 64 entactin, 64 fibronectin, 63 laminin, 64 osteonectin, 64 tenascin, 64
Glycosaminoglycans (GAGs), 61 , 62t Goblet cells, 283 Goiter, 231
tahir99-VRG & vip.persianss.ir

41 2 I n d ex
Golgi apparatus, 34f, 38f, 39f functions, 37 regions, 37 structure, 37
Golgi complex, 146, 146f Golgi tendon organs, 133, 367f, 368 Gonadotrophs, 224 G proteins, 8, 392, 401 G protein-linked receptors, 8
heterotrimeric G proteins, 8, 9f, 9t monomeric G proteins, 8
Graafian follicle, 334-335 Granulocytes, 98-99, 167t, 170, 170t
basophils, 99 eosinophils, 99 formation, 176-178 neutrophils, 99 precursor cells, 178 progenitor, 178
Granulomere, 172 Granulosa lutein cells, 336 Graves disease, 7, 228 Gray matter, in CNS, 158 Guanine, 21 Gynecomastia, 346
H Haploid number, 2 1 Hassall corpuscles, 215 Haversian canal, 1 12f, 1 14 Haversian systems, 1 14 Hay fever, 98 Heat receptors, 368 Hematocrit, 168 Hemoglobin (Hb), 169 Hemopoiesis. See Blood and hemopoiesis Hemopoietic growth factors, 179, 180t Hemopoietic stem cells. See Pluripotential
hemopoietic stem cells Hemorrhoids, 194, 287 Hemosiderosis, 227 Henle, loop of, 3 16-318, 3 16f Heparin, 70 Hepatic acinus of Rappaport, 301 Hepatitis, 303 Hepatocytes, 302-303
hepatic functions by, 303 Hereditary spherocytosis, 1 1 Herpetic stomatitis, 274, 389, 399 Heterochromatin, 16f, 19 Heterographs, 1 19 Heterophagy, 44f, 56, 402 Heterotrimeric G proteins, 8, 9t, 9f Hirschsprung disease, 144 Histamine, 282 hnRNP particles, 19 Hodgkin disease, 208, 398 Holocrine glands, 88 Homographs, 1 1 9 Hormones
adrenal gland cells and, 234t lipid-soluble hormones, 221 pituitary, physiological effects of, 226t water-soluble hormones, 221
Howship lacunae, 1 1 1 Human chorionic gonadotropin (hCG), 338 Human chorionic somatomammotropin (hCS), 338 Human epidermal growth factor. See Urogastrone Huntington chorea, 15 1
Hurler syndrome, 57 Huxley sliding-filament model, 130, 130f Hyaline cartilage, 106, 107f, 108f, 109t, 390, 399
degeneration of, 109 effects of hormones and vitamins on, 109t histogenesis of, 109
appositional growth, 109 interstitial growth, 109
structure of chondroblasts, 108 chondrocytes, 108 matrix, 106, 108 perichondrium, 108
Hyaline membrane disease, 266, 390, 400 Hyalomere, 171 , 172 Hyaluronic acid (hyaluronan), 61 Hydrocortisone, 109t Hydrophilic signaling molecules, 7 Hydroxylysine, 70 Hydroxyproline, 70 Hypercellular (hyperplastic) obesity, 102 Hyperhidrosis, 249 Hyperparathyroidism, 233 Hyperthermia, 357 Hypertrophic obesity, 102 Hypervitaminosis A, 109t Hypoparathyroidism, 240, 241 Hypophyseal fossa, 222 Hypophyseal portal system, 228 Hypothalamo-hypophyseal tract, 225 Hypovitaminosis A, C, D, 109t
Icterus. See Jaundice IKB, 200 Ileum, 389, 399 Immature teratomas, 343 Immature T lymphocytes, 215 Immotile cilia syndrome, 86 Immunogens, 209 Immunoglobulin E antibodies, 392, 401 Immunoglobulins, 210
classes, 210-2 1 1 IgA, 2 1 1 IgD and IgE, 2 1 1 IgG, 2 1 1 IgM, 2 1 1
structure, 2 1 0 Importins, 1 7 Incus, 378f, 379 Inducible T reg cells, 206, 218, 220 Infant respiratory distress syndrome (IRDS), 266 Infectious hepatitis. See Viral hepatitis A Infectious mononucleosis, 171 Inferior rectus muscle, 369f Inhibin, 357 Innate immune system, 199 Inner circumferential lamellae, 1 12f, 1 14 Inner ear, membranous labyrinth of, 388, 398 Inner leaflet, plasma membrane, 1 , 2f Inner nuclear membrane, 15-16 Inositol phospholipids, 42 Insufficient apoptosis, 28 Insulin, 8, 101 , 298 Insulinomas, 299 Integral proteins
freeze-fracturing and, 4f plasma membrane, 1 , 3
Integrin receptors, 64, 65f
tahir99-VRG & vip.persianss.ir

Interalveolar septum, 267-268 Intercalated disks, 135, 136f
function of, 388, 398 Intercalated neurons. See Interneurons Interchromatin granules, 19 Interferon-y, 218, 220, 393, 402 Interleukin- 1 (IL- l), 393, 402 Interleukin-6 (IL-6), 101 Intermediate filaments, 48
types of, 49t Internal acoustic meatus, 378f Internal carotid artery, 378f Internal ear, 378f, 379
auditory function of, 382 bony labyrinth, 379 membranous labyrinth, 379
cochlear duct, 380-382 endolyrnphatic duct, 380 endolyrnphatic sac, 380 saccule and utricle, 379-380 semicircular ducts, 380
vestibular function of, 383 Internal elastic lamina, 186 Interneurons, 146 Internodes segments of nerve fiber, 153 Interoceptors, 366 Interstitial cells of Leydig, 351 , 393, 402 Interstitial lamellae, 1 14 Interstitial pulmonary fibrosis, 267 Interterritorial matrix, hyaline cartilage, 107f, 108 Intestinal microbes, 287 Intracellular digestion
lysosomal digestion, 44f, 56 autophagy, 56 crinophagy, 56 heterophagy, 56
nonlysosomal digestion, 56 Intracellular second messenger system, 4 Intrapulmonary bronchi, 260 Intrinsic pathway, of blood coagulation, 391, 401 Introns, 21 Ion channel proteins, 5, Sf lonophores, 7 Iris, 369f, 371 Irisin, 102 Ischemic heart disease, 188 Islets of Langerhans, 297 Isometric contraction, 132
Jaundice, 303 Joints
diarthroses (synovial joints), 120 synarthroses, 120
Junctional adhesive molecules (JAMs), 77 Junctional complex, epithelia, 77, 78f
anchoring junctions, 79 focal adhesions, 79 hemidesmosomes, 79
tight junction, 77, 79 Juxtaglomerular {JG) apparatus, 318
K K+ leak channel, 392, 401 Kaposi sarcoma, 205 Karyotype, 21 Keloids, 249, 397 Keratosis follicularis. See Darier disease Kidneys, 309-310, 310f
arterial supply to, 320 venous drainage of, 321, 32lf
Kinesin, 46 Klinefelter syndrome, 30, 32 Knobloch syndrome {type I), 70
I n dex 41 3
Krause end bulbs (cold receptor), 367f, 368 Krebs cycle, enzymes of, 36
L Lacrimal apparatus, 377-378 Lactating mammary glands, 346 Lacunae, 107f, 108 Lamina densa, 69, 81 , 8lf, 3 13, 314 Lamina Iucida, 81 , 81f Lamina reticularis, 81 Laminin, 64, 65f Landouzy-Dejerine syndrome. See Facioscapulo-
humeral muscular dystrophy Langerhans cells, 246-247 Lanugo, 251 Large intergenic noncoding RNAs {lincRNAs), 24 Large intestine, 285
anal canal, 287 appendix, 288 cecum and colon, 286 function of, 286 lumen of, 286 rectum, 287
Larynx, 259-260 Lens, eye, 371-372, 372f Leptin, 101 , 102 Leukemias, 171 Leukocytes {white blood cells), 167f, 167t, 170
agranulocytes, 170-171 , 17lt granulocytes, 170, 170t
Leydig, interstitial cells of, 351 Ligand-gated ions channels, 7 Linker DNA, 20 Lipid bilayer, plasma membrane, 2-3f
fluidity of, 3 molecular structure
cholesterol, 2 glycolipids, 2 leaflets, 1-2 phospholipids, 1
Lipid droplets, 46 Lipid rafts, 3, 4-5 Lipid-soluble hormones, 221 Lipid-soluble signaling molecules, 7 Lipid-to-protein ratio, in plasma membranes, 4 Lipofuscin, 46 Lipomas, 102 Lipoprotein lipase, 100 Liposarcomas, 102 Lissencephaly, 46 Liver, 299
blood and bile flow, 301-302, 302f function of, 299 hepatic functions, 303 hepatocytes, 302-303 liver lobules, 300-301 , 300f sinusoids, 388, 398
Lobular carcinoma, 395, 403 Loop of Henle, 3 16-318, 3 16f Loose connective tissue (areolar tissue), 99 Lou Gehrig disease. See Amyotrophic
lateral sclerosis (ALS) Lumbar puncture, 159 Lumen, 34
tahir99-VRG & vip.persianss.ir

41 4 I n d ex
Luminal ring, of nuclear pore complex, 17, 17f Lung
cancer, 261 lobules, 269
Luteinizing hormone (LH), 334, 351 Luteinizing hormone-releasing hormone
(LHRH), 337, 356 Lymphatic capillaries, 195 Lymphatic vascular system, 195
large lymphatic vessels, 195 lymphatic capillaries, 195
Lymphatic vessels, large, 195 Lymph nodes, 212, 212f
function, 213 structure, 213
Lymphocytes, 170, 17lt formation, 179
Lymphoid cells, 98 B lymphocytes (B cells), 98 natural killer cells (NK cells), 98 T lymphocytes (T cells), 98
Lymphoid nodules, 2 1 1 -212, 284-285 primary nodules, 212 secondary nodules, 2 1 1
Lymphoid organs primary, 199 secondary, 199
Lymphoid (immune) system, 199 adaptive immune system, 200 antigen presentation and role of MHC molecules
HLA restriction, 209 immunogens, 209 MHC, 209
B lymphocytes, 207-208 cells of, 199, 202f, 203f diffuse lymphoid tissue, 2 1 1-212 immunoglobulins, 210-2 1 1 innate immune system, 199 lymphoid organs
lymph node, 213 spleen, 215-217 thymus, 213-215 tonsils, 217
macrophages, 208 NK cells, 208 review test, 218-219
answers and explanations, 220 T lymphocytes, 199
maturation of, 201-202 types and subtypes of, 205
Lymphopoiesis, 179 Lysine, 394, 403 Lysosomal storage diseases, 57 Lysosomes, 34f, 394, 402
formation, 43-44 early endosomes, 43 late endosomes, 43-44
structure, 43 types
autophagolysosomes, 44-45 multivesicular bodies, 44 phagolysosomes, 44 residual bodies, 45
Lysozyme, 377, 394, 402
M Macrophages, 50, 98, 174, 392, 40 1 Macula, 369f, 373
adherens, 136f
Maculae, neuroepithelial hair cells in, 379, 384, 386 Major histocompatibility complex (MHC), 201, 209 Malabsorption disorders, 286 Male pattern baldness, 253 Male reproductive system, 350
accessory genital glands bulbourethral glands, 361 prostate gland, 359-360, 360f seminal vesicles, 359
function of, 350 genital ducts
ductuli efferentes, 358 ductus deferens, 359 ductus epididymis, 358-359 ejaculatory duct, 359 extratesticular ducts, 358-359 histology and functions of, 357t intratesticular ducts, 357
penis connective tissue and skin, 362 corpora cavernosa, 362 corpus spongiosum, 362
review test, 363-364 answers and explanations, 365
testes, 350, 35lf interstitial cells of Leydig, 351 lobuli testes, 351 regulation of spermatogenesis, 356 seminiferous epithelium, 353f seminiferous tubules, 351 Sertoli cells, 352-353 spermatogenesis, 353-354 spermatogenic cells, 354 spermatozoon, 355 spermiogenesis, 354 testicular tunicae, 351
urethra, 361 Malignant melanoma, 244, 395, 403 Malleus, 378f, 379 Malpighian layer, 243 Manchette, 354, 393, 402 Mannose-6-phosphate (M-6-P), 44 Marfan syndrome, 71 Mast cells, 95 , 390, 392, 400, 401
activation and degranulation of, 97f mediators released by, 96t
Matrix fibronectin, 392, 401 hyaline cartilage, 106, 108
Mature teratomas, 343 Mechanoreceptors, 366 Megakaryoblasts, 178 Megakaryocytes, 179 Meiosis, 29, 29f
equatorial division (meiosis II) , 30 reductional division (meiosis I), 29
anaphase I, 30 metaphase I, 30 prophase I, 30 telophase I, 30
Meissner corpuscles, 248, 367f, 368, 390, 400 Melatonin, 238 Membrane carrier proteins, 392, 401 Membrane-coating granules, 389, 399 Membrane proteins, plasma membrane
functional characteristics of, 4 integral proteins, 3 major classes of, 9t peripheral proteins, 3-4
tahir99-VRG & vip.persianss.ir

Membrane receptors domains of, 7 functions of, 7-8 types of
catalytic receptors, 8 channel-linked receptors, 8 G protein-linked receptors, 8
Membrane recycling, 50 Membranous labyrinth, 379-382 Memory T cells, 205 Meniere disease, 383 Meninges, 158 Meningitis, 154 Menopause, 330 Merkel cells, 24 7, 367f Merocrine glands, 88 Mesenchymal tissue, 99 Messenger RNA (mRNA), 15, 22-23, 22f Metabolic syndrome, 102 Metaphase, of mitosis, 26-27, 26f, 27t Metaplasia, 88 Metarterioles, 189, 193f Microbodies. See Peroxisomes Microfilaments, 47-48, 147 Microglia, 150 Microphthalmia-associated transcription
factor, 246 MicroRNAs (miRNAs), 23, 24 Microtubule-organizing center (MTOC), of cell, 27 Microtubules, 147
associated proteins, 46 function, 46 with kinesin and cytoplasmic dynein, 46 with microtubule-associated proteins, 46 polar, 46 structure, 46
Microvilli, 83 Middle ear, 378f, 379 Milk, mammary glands, 347 Mineralization, 80 Mitochondria, 34f, 35f, 134, 136f, 146f, 389, 398
ATP synthesis, 36f, 37 condensed, 37 enzymes and genetic apparatus
elementary particles, 36 genetic apparatus, 36 Krebs cycle, enzymes of, 36
origin and proliferation, 37 structure, 36
Mitochondrion, 126f, 394, 402 Mitosis. See Cell cycle, mitosis Mixed-function oxidases, 393, 402 Mixed nerves, 154 Monocytes, 98
formation, 178 Monodermal teratomas, 343 Monomeric G proteins, 8 Mononucleosis, infectious, 389, 398 Motilin, 394, 402 Motor nerves, 154 Motor neurons, 126f, 146 Motor unit, muscle cells of, 132 Mucosa, 338-339, 338f
alimentary canal, 278 appendix, 288 gallbladder, 304, 304f oral cavity, 273 respiratory system, 260 small intestine, 283-284
I n dex 41 5
Mucosa-associated lymphoid tissue (MALT). See Diffuse lymphoid tissue
Mucous tissue (Wharton jelly), 99 Mucus, 88 Multidrug-resistant proteins (MDR proteins), 6 Multipass proteins. See Transmembrane proteins Multiple sclerosis (MS), 153 Multipolar neurons, 145, 145f Multipotential hemopoietic stem cells, 176 Multivesicular body lysosomes, 44 Mumps, 296 Muscle, 124
cardiac muscle, 133-135 contractile nonmuscle cells, 139 fibers. See Skeletal muscle review test, 140-141
answers and explanations, 142 skeletal muscle
contraction of, 130-132 innervation of, 132-133 structure of, 124
smooth muscle, 135, 137-139 spindle receptors, 133, 368
Muscular arteries, 186 Muscular (distributing) arteries, 389, 399 Muscularis mucosae, 285 Myasthenia gravis, 133 Myelin sheath, 150f, 152-153 Myeloblasts, 178 Myeloid stem cells, 98-99 Myocardial infarct, 135 Myocardium, 185 Myoepithelial cells, 139 Myofibrils, 125, 126f Myofibroblasts, 139 Myofilaments, molecular organization of
thick filaments, 129-130 thin filaments, 129
Myoglobin, 395, 403 Myomesin, 129 Myoneural junction, 132-133 Myosin, 126f
globular head of, 394, 403 Myosin II, 129, 131 Myostatin, 127
N Na+-K+ pump, 6, 392, 401 Nails, 252-253 Naive T cells, 205 Nasal cavity, 257-259 Nasopharynx, 259, 395, 403 Natural killer cells (NK cells), 98, 393, 402 Nebulin, 126f, 129 Nectins, 77 Nephrons, 310
cortical nephrons, 310 distal convoluted tubule, 318 JG apparatus, 318 juxtamedullary nephrons, 310 loop of Henle, 316-318, 316f midcortical nephrons, 310 proximal convoluted tubule, 315-316 renal corpuscle, 310, 3 12f
Bowman space, 3 1 1 , 3 13 podocytes, 313 renal filtration barrier, 3 14, 3 14f renal glomerulus, 313
Nephrotoxic acute tubular necrosis, 319
tahir99-VRG & vip.persianss.ir

41 6 I n d ex
Nerve deafness, 382 Nerve fibers, 152-153 Nervous system, 143
autonomic nervous system, 157 autonomic nerve chains, 157 enteric nervous system, 157 parasympathetic system, 157 sympathetic system, 157
cells of neuroglial cells, 148- 150 neurons, 145- 148
central nervous system, 143, 158 cerebrospinal fluid, 159 meninges, 158 white matter and gray matter, 158
degeneration and regeneration of nerve tissue neuronal death, 160- 161 peripheral nerve regeneration, 160f transection of peripheral axons, 161
ganglia, 155 autonomic ganglia, 155 craniospinal ganglia, 155
histogenesis of, 143-144, 144f histophysiology of
action potential, 156 axonal transport of materials, 156 resting membrane potential, 155-156 trophic function of nervous tissue, 157
nerve fibers, 152 internodes, 153 myelin sheath, 150f, 152-153 nodes of Ranvier, 153
nerves, 153, 154f, 155f connective tissue investments, 153-154 functional classification of, 154
peripheral nervous system, 143 review test, 162-163
answers and explanations, 164- 165 somatic nervous system, 157 synapses, 151- 152
N-ethylmaleimide-sensitive fusion (NSF) protein, 41
Neural crest cells, 144, 144f Neural groove, 143, 144f Neural plate, 143, 144f Neural tube, 143, 144f Neuroepithelium, 143 Neurofibrils, 146f Neurofilaments, 147 Neuroglial cells, 148
general characteristics of, 148 types of, 149f
astrocytes, 148- 149 ependymal cells, 150 microglial cells, 150 oligodendrocytes, 149 Schwann cells, 149-150
Neuroglial tumors, 144 Neurohypophysis, 225-226 Neuromuscular spindle, 367f Neuronal cell body, 146-147 Neurons, 145
functional classification of interneurons, 146 motor neurons, 146 sensory neurons, 146
morphologic classification of, 145f bipolar neurons, 145 multipolar neurons, 145
pseudounipolar neurons, 145 unipolar neurons, 145
structure of, 146f axons, 147- 148 dendrites, 14 7 neuronal cell body, 146- 147
Neurotransmitters, 151 , 152, 152t Neutrophils, 50, 99
precursor cells, 178t vs. basophils, 387, 397
Nexin, 84, 84f Nissl bodies, 146, 146f Nitric oxide, 169, 189 NK cells, 208 Nociceptors, 366, 367f, 368 Nondisjunction of chromosomes, 30 Nonerythroid cells, cytoskeleton of, 10f, l l Non-Hodgkin lymphoma, 205 Nonlactating mammary glands, 346 Norepinephrine, 152t, 162, 164 Nuclear basket, 17, 17f Nuclear envelope, 34f. See also Nucleus,
nuclear envelope Nuclear export sequences, 17 Nuclear localization segments (NLS), 17 Nuclear localization sequences, 17 Nuclear matrix, 18-19 Nuclear membrane
inner, 15-16 outer, 15
Nuclear pore complex (NPC) function of, 17 structure of, 16-17
cytoplasmic ring, 16-17, 17f luminal ring, 17 nucleoplasmic ring, 17
transport mechanisms, 17 Nuclear pores, 16 Nucleocytoplasmic shuttling signals, 17 Nucleolar matrix, 18 Nucleolar organizer regions (NORs), 18 Nucleolus, 16f, 18 , 34f Nucleoplasm, 18-19 Nucleoplasmic reticulum, 19 Nucleoplasmic ring, of nuclear pore complex, 17, 17f Nucleoporins, 16 Nucleosomes, 388, 398 Nucleostemin, 18 Nucleotides, 21 Nucleus, 15, 16f
chromatin, 19 euchromatin, 16f, 19 function of, 19 heterochromatin, 16f, 19
chromosomes, 20f condensed chromatin, 20 extended chromatin, 20 G-banding, 20-21 genome, 21 karyotype, 2 1 structure of, 20
DNA, 21 function of, 15 nuclear envelope
inner nuclear membrane, 15-16 nuclear pore complex, 16-17, 17f nuclear pores, 16 outer nuclear membrane, 15 perinuclear cisterna, 16
tahir99-VRG & vip.persianss.ir

0
nucleolus function of, 18 structure of, 18
nucleoplasm, 18-19 nuclear matrix, 18-19 nuclear particles, 19
review test, 31 answers and explanations, 32
RNA, 22-24 of smooth muscle cells, 135 structure of, 15
02 transport, by erythrocytes, 169 Obesity, 102 Occludins, 77 Olfactory cells, 259 Olfactory epithelium, 259 Oligodendrocytes, 149 Oncogenes, 21 Optic disk, 369f, 376 Optic nerve, 368, 369f Oral cavity, bacterial flora of, 294 Oral leukoplakia, 387, 397 Oral mucosa, histological features of, 276t Organelles. See Cytoplasm, organelles Organ of Corti
cells of Hensen and border cells of, 382 hair cells of, 382 inner and outer phalangeal cells of, 382 inner and outer pillar cells of, 382 spiral, 380, 38lf, 382
Orthochromatophilic erythroblast, 177t Osteoarthritis, 109 Osteo blasts, 1 1 0- 1 1 1 Osteocalcin, 1 10 Osteoclasts, 1 1 1 , 1 13f
bone resorption, 1 1 3 cytoplasm, 1 1 1 morphology, 1 1 1
Osteocytes, 1 1 1 Osteogenesis imperfecta, 400 Osteomalacia, 1 19, 39 1 , 400 Osteonectin, 64 Osteons. See Haversian systems Osteopetrosis, 1 1 2 Osteoporosis, 120, 400
in older women, 387, 397 Osteoprogenitor cells, 1 1 0
proliferation of, 1 19 Otitis media, 379 Otolithic membrane, 380 Outer circumferential lamellae, 1 12f, 1 1 4 Outer leaflet, plasma membrane, 1 , 2f Outer nuclear membrane, 15 Ovarian carcinoid, 343 Ovaries, 330, 33lf
germinal epithelium, 330 hormonal regulation, 336, 337f
dominant follicle, ovulation of, 338 fate of corpus luteum, 337-338 follicle maturation and ovulation,
control of, 336-337 ovarian cortex, 332, 332f
atretic follicles, 336 corpus albicans, 336 corpus hemorrhagicum, 335 corpus luteum, 336 graafian follicle, 334-335
I n dex
growing follicles, 333-334 ovarian follicles, 332-333, 333t primordial follicles, 332, 332f
ovarian medulla, 336 primordial follicles of, 388, 397
Oviducts (fallopian tubes), 338 mucosa, 338-339, 338f muscularis, 338f, 339 serosa, 339
Oxyphil cells, 233
p Pacinian corpuscles, 367, 367f Pain receptors. See Nociceptors Pancreas, 296, 389, 399
digestive enzymes by, 296 exocrine pancreas, 296-297 exocrine pancreatic secretions, 297 islet cells, 297 islet hormones, 298 islets of Langerhans, 297-298, 297f, 298t pancreatic acinar cells, 296 pancreatic ducts, 296 centroacinar cells of, 387, 397
Pancreatic acinar cells, 296 Pancreatic cancer, 299 Paneth cells, 284 Papanicolaou (Pap) smear, 342, 395, 403 Paracrine glands, 87 Paracrine hormones, 7 Parafollicular cells, 229, 231, 232f Parasympathetic system, of nerve, 157 Parathyroid glands, 232-233 Parathyroid hormone, 120 Parietal cells, 280, 396, 404 Parkinson disease, 15 1 Pars fibrosa, 18 Pars granulosa, 18 Pars nervosa, 226 Passive transport, 5, Sf
facilitated diffusion, 5 simple diffusion, 5, Sf
Pathogen-associated molecular patterns (PAMPs), 199
Paxillin, 65f Pepsin, 396, 404 Pepsinogen, 394, 402 Peptidyl transferase, 34 Perforin, 393, 402 Perichondrium, l07f, 108 Perichromatin granules, 19 Pericytes, 93, 392, 40 1 Perikaryon. See Neuronal cell body Perimysium, 124 Perineurium, 154, 154f Perinuclear cisterna, 16 Periosteum, 1 10, 1 12f Peripheral nerve fibers, unmyelinated, 150 Peripheral proteins, plasma membrane, 1 , 3-4 Permeability, of capillaries, 191 Pernicious anemia, 1 69, 398 Peroxisomal diseases, 45 Peroxisomes, 34f
function, 45 structure, 45
Pertussis toxin, 8 Peyer patches, 284, 389, 399 Phagocytosis, 50 Phagolysosomes, 44
41 7
tahir99-VRG & vip.persianss.ir

41 8 I n d ex
Phenobarbital, 35 Pheochromocytoma, 237 Phosphoinositide (PIP), 42, 42t Phospholipid, 392, 401
plasma membrane, 1 Photoreception, 375 Pineal gland, 237-238 Pinealocytes, 238 Pinocytosis, 49 Pinocytotic vesicles, 19 1 Pitting edema, 99 , 195 Pituicytes, 226 Pituitary adenomas, 225 Pituitary gland, 221, 223f, 390, 400
adenohypophysis, 222, 224f pars distalis, 222-223 pars intermedia, 225 pars tuberalis, 225
neurohypophysis, 225 hypothalamo-hypophyseal tract, 225 pars nervosa, 226 pituicytes, 226
pars distalis, regulation of, 228 pituitary hormones, physiological effects of, 226t vascularization of, 226
Pituitary growth hormone, in bone formation, 120 Placenta, 343-345, 344t Plasma cells, 98, 392, 401 Plasma fibronectin, 63, 391 , 401 Plasmalemma-cytoskeleton association, 10- 1 1 Plasmalogen deficiency, 45 Plasma membrane, 1, 33, 34f, 392, 40 1
cell-to-cell communication membrane receptors, 7-8 signaling molecules, 7, 9[
fluid mosaic model of, 1-5 glycocalyx (cell coat), 4 lipid bilayer, 1-3 lipid rafts, 4-5 membrane proteins, 3-4
function of, 1 plasmalemma-cytoskeleton association, 10- 1 1
nonerythroid cells, 1 1 red blood cells, 1 0
review test, 12-13 answers and explanations, 14
structure of, 1 transport processes, 5-7
active transport, 6 facilitated diffusion of ions, 6-7 passive transport, 5
Platelet aggregation, 401 Platelets (thrombocytes), 167f, 167t,
171-172, 172t, 178 Plectin, 48 Pluripotential cells, 392, 40 1 Pluripotential hemopoietic stem cells (PHSCs), 176 Polar head, plasma membrane, 1 , 2f Polychromatophilic erythroblast, 177t Polycystic kidney disease, 86 Polyribosome, 33 Polysome. See Polyribosome Posterior semicircular canal, 378f Postganglionic fibers, 157 Postsynaptic membrane, 152 Power stroke, 131 Precapillary sphincters, 191 , 193f Precursor cells, 176t Precursor mRNA (pre-mRNA), 19 Prenatal hemopoiesis, 175
Presbyopia, 372 Presynaptic membrane, 152 Primary bronchioles, 261 Primary lymphoid organs, 199 Primary spermatocytes, 393, 402 Primordial follicles, of ovary, 388, 397 Procollagen, cleavage of, 66 Proerythroblast, 176, 177t Progenitor cells, 176 Progesterone, 337 Programmed cell death. See Apoptosis Prolactin, 239, 241 , 345 Prometaphase, of mitosis, 26-27, 26f, 27t Promyelocytes, 178 Prophase, 26-27, 26f, 27t Prophase I, 30 Proprioceptors, 366 Prostaglandin F2rv 335 Prostate gland, 359-360, 360[
adenocarcinoma of, 361 Proteases, 306, 308 Proteasome, 56 Protein hormones, 239, 241 Proteins, 289
digestion of, 396, 404 Protein synthesis, 50, 52f
cytosolic proteins, synthesis of, 54 membrane-packaged proteins, synthesis of, 50
anterograde transport from VTC to cis-Golgi, 54
posttranslational modification in RER, 54 protein processing in Golgi complex, 54, 55f protein transport from RER to cis-Golgi, 54 sorting of proteins in TGN, 54, 55f translation of mRNAs, 52-53 transport of peptide into RER
cisterna, 53-54, 53f transmembrane proteins, synthesis of, 54
Proteinuria, 390, 399 Proteoglycans, 4, 63, 92 Proto-oncogenes, 2 1 Protoplasmic astrocytes, 149 Pseudostratified ciliated columnar with goblet cells
epithelia, 76f Pseudo unipolar neurons, 145, 145f Psoriasis, 246 Pulmonary vascular supply, 269 Pupil, 369f, 371 Purines, 21 Purkinje cell layer, 158 Purkinje fibers, 135 , 185 Pus, 99 Pyrimidines, 2 1
R Rab effector proteins, 43 Rab proteins (Rab-GTPs), 43, 43t Radial spokes, 84, 84f Ranvier, nodes of, 153 Rash, pharmacological agent for, 390, 400 Receptor-mediated endocytosis, of ligand, 39f, 50 Red blood cell, cytoskeleton of, 10, 10f Red marrow, 174 Refractive media of eye, 371-372 Regulatory RNAs, 15, 23-24 Relaxin, 337 Renal cortex, 310 Renal failure, chronic, 3 15 Renal glomerulus, 3 13 Residual body Iysosomes, 45
tahir99-VRG & vip.persianss.ir

Resistin, 101 Respiratory bronchioles, 264, 264f Respiratory system, 257
bronchial arteries and veins, 269 components of, 258t conducting portion of, 257
intrapulmonary bronchi, 260, 26lf larynx, 259-260 nasal cavity, 257-259 nasopharynx, 259 primary bronchioles, 261-262, 262f terminal bronchioles, 261-262 trachea and extra pulmonary bronchi, 260
lung lobules, 269 pulmonary artery, 269 pulmonary nerve supply, 269 pulmonary veins, 269 respiratory portion of, 262, 263f
alveolar ducts, 264, 264f alveolar macrophages, 267 alveolar sacs, 264, 264f alveoli, 264-266 blood-gas barrier in lung, 268 interalveolar septum, 267-268 respiratory bronchioles, 264, 264f type I pneumocytes, 265 type II pneumocytes, 236f, 265
review test, 270-271 answers and explanations, 272
Resting membrane potential, 155-156 Rete testis, 357 Reticular fibers, 93 Reticular tissue, 100, 100f Reticulocyte, 177t Retina, 369f, 373-374, 373f
detachment of, 376 external limiting membrane, 376 ganglion cell layer, 376 inner limiting membrane, 376 inner nuclear layer, 376 inner plexiform layer, 376 optic nerve fiber layer, 376 outer nuclear layer, 376 outer plexiform layer, 376 photoreceptor layer, 375
cones, 374f, 375 rods, 374f, 375
retinal pigment epithelium, 374-375 Retinol-binding protein-4, 101 Retromer-coated vesicles, 42 Rheumatic fever, 197 , 198 Rheumatic heart valve disease, 185 Rheumatoid arthritis, 109 Rhodopsin, 375 RhoGAM, 168 Ribonucleic acid (RNA), 22
lincRNAs, 24 miRNAs, 23 mRNA, 22-23, 22f polymerase II, 23 rRNA, 15, 23, 24f siRNAs, 24 synthesis, 387, 397 tRNA, 23
Ribophorins, 34, 393, 402 Riboses, 22 Ribosomal ribonucleic acid (rRNA), 15, 23, 24f Ribosomes, 15, 34f
composition, 34t function, 33-34
polyribosome, 33 structure, 33
Rickets, 1 19 Rigor mortis, 131
I n dex 41 9
Rods and cones, photoreceptor layer of retina, 374f, 375
Rough endoplasmic reticulum (RER), 34f, 35f, 393, 402 function, 35 structure, 34
Ruffini corpuscles, 367, 367f
s Saccule and utricle, 379-380 Saliva, 295 Salivary calculus, 296 Salivary glands, 294
acini, 295 ducts, 295 function of, 294 saliva, 295 structure of, 295
Sarcoglycan complex, 128 Sarcolemma, 124, 126f, 131 Sarcomere, 125 , 126f Sarcoplasmic reticulum (SR), 35, 125, 126f, 134, 136f Schmidt-Lanterman, clefts (incisures) of, 153 Schwann cells, 149-150, 153, 154f Sclera, 368, 369f Scurvy, 66 S DNA damage checkpoint, 26 Sebaceous glands, 251 Secondary follicles, 334 Secondary lymphoid organs, 199 Secondary messenger systems, 392, 401 Semicircular canals, 378f, 379 Semilunar valves, 185 Seminal vesicles, 359 Seminiferous tubules, 351-354, 352f Sense receptors, 366
ear, 378, 378f external, 378 internal, 379-383 middle, 379
eye, 368 accessory structures of, 377-378 anatomy of eyeball, 369f external anatomy of, 377f iris, 371 refractive media of, 371-372 retina, 373-376 tunica fibrosa, 368-370 tunica vasculosa, 370-371
function of, 366 review test, 384-385
answers and explanations, 386 specialized diffuse receptors, 366, 367f
proprioceptive receptors, 368 temperature and pain receptors, 368 touch and pressure receptors, 367-368
Sensory nerves, 154 Sensory neurons, 146 Serotonin, 152t, 162, 164, 238 Serous, 88 Serous demilunes, 295 Sertoli cells, 352-353, 393, 402 Serum, 166 Serum hepatitis, 303 Sex chromatin, 19, 146f Sex chromosomes, 21 Sheehan syndrome, 227
tahir99-VRG & vip.persianss.ir

420 I n d ex
Sickle cell anemia, 169 Signal hypothesis, 53-54, 53f Signaling molecules, 9f
example of, 7 function of, 7 hydrophilic, 7 lipid-soluble, 7
Signal recognition particle (SRP), 53 Simple columnar epithelia, 76f Simple cuboidal epithelia, 76f Simple diffusion, of plasma membrane transport, 5, Sf Simple goiter, 403 Simple squamous epithelia, 76f Sinoatrial (SA) node, 185 Sinusoidal capillaries, 190f, 191 Sinusoids, 174 Sjogren syndrome, 296 Skeletal muscle, 126f, 127f, 134t
contraction of, 130, 130f Huxley sliding-filament model, 130, 130f initiation and regulation of, 131 muscle cells of motor unit, 132 and relaxation, 131
innervation of, 132 Golgi tendon organ, 133 muscle spindles, 133 myoneural junctions, 132-133
structure of connective tissue investments, 124 cross-striations, 127-128 myofilaments, 125, 126f, 129-130 red and white muscle fibers,
characteristics of, 125t satellite cells, 125, 127 skeletal muscle cells, 124-125, 126f, 127f
Skin, 242, 248f appendages of, 249 arrector pili muscle, 25lf, 252 cancers, 244 dermis, 248-249
dermal papillary layer, 248 dermal reticular layer, 248-249
epidermis, 242-243 Langerhans cells, 246-247 layers of, 243, 243f, 244t melanocytes, 246 Merkel cells, 247 nonkeratinocytes in, 246-247 stratum basale, 246 stratum corneum, 245, 245f stratum granulosum, 245 stratum lucidum, 243 stratum spinosum, 243
functions of, 242 glands in
apocrine sweat glands, 250 eccrine sweat glands, 248f, 249 sebaceous glands, 251
hair follicle, 25lf, 252 hairs, 251-252 histological features of, 244t nails, 252-253 review test, 254-255
answers and explanations, 256 thick and thin skin, distinction between, 247 UV radiation and, 244
Small cell (oat cell) carcinoma, 261 Small interfering RNAs (siRNAs), 24 Small intestine
external layer of, 286
function of, 282 luminal surface of, 282-283
intestinal villi, 282-283, 282f microvilli, 283 plicae circulares, 282
mucosa of crypts of Lieberkiihn, 284 epithelium of, 283 lamina propria, 284-285 lymphoid nodules, 284-285 muscularis mucosae, 285
muscularis externa of, 286 regions of, 282 submucosa of, 286
Small nuclear RNPs (snRNPs), 19 Smooth endoplasmic reticulum (SER), 393, 402
function, 35 structure, 35
Smooth muscle, 134t cells, structure of
cytoplasmic densities, 139 cytoplasmic organelles, 138 filaments, 138 gap junctions, 139 nucleus, 135
contraction of, 139 innervation of, 139
SNARES, 41 v-SNARES and t-SNARES interaction, 41
Soluble NSF attachment protein (SNAP), 41 Soma. See Neuronal cell body Somatostatin, 282, 394, 402
intestinal peptide, 298 Somatotropin, 390, 400. See Pituitary
growth hormone Spectrin, 4, 10, 10f, 1 1 , 168 Spermatogenesis, 353-354
meiosis, 353 regulation of, 356, 356f spermatocytogenesis, 353 spermiogenesis, 354
Spermatogenic cells, 354 spermatids, 354, 393, 402 spermatocytes, 354 spermatogonia, 354
Spermatozoa, 363, 365 Spermatozoon, 355f
head of, 355 tail of, 355
Sperm count, normal, 359 Spermiogenesis, 354 Sphincter pupillae muscle, 371 Spina bifida, 144 Spinal cord, 144f
gray matter, 158 Spindle assembly checkpoint, 26 Spiral prominence, 380 Spleen
function of, 216 marginal zone, 2 16, 216f, 217 red pulp of, 217 smooth capsule of human spleen, 216f vascularization of, 2 16 white pulp of, 216
Spongy bone, 1 13 Spontaneous pneumothorax, 267 Squamous cell carcinoma, 261 SRY gene, 330 Stapedius muscle, 379 Stapes, 378f, 379
tahir99-VRG & vip.persianss.ir

Stem cells, 175 factor, 179
Stereocilia, 83 Stomach, 279
gastric glands, 280 cardiac and pyloric glands, 282 fundic glands, cells of, 280-282
gastric juice, 282 gastric pits, 279, 280f
gastric mucosa, 279 gastric muscularis externa, 280 gastric submucosa, 279-280 serosa, 280
gastric secretion, regulation of, 282 Stratified squamous epithelium, 89, 91, 273, 378
keratinized, 75t, 76f, 242, 275, 287, 291 , 293, 390, 399
nonkeratinized, 75t, 76f, 87f, 259-260, 275, 287, 341, 345, 369
Stratum basale, 243 Stratum corneum, 245-246 Stratum granulosum, 245 Stratum lucidum, 245 Stratum spinosum, 243 Stria vascularis, 380 Stromal cells, 17 4 Struma ovarii, 343 Subcapsular epithelium, 371 Submandibular acinar cells, 307, 308 Superior semicircular canal, 378f Surface absorptive cells, 283-284 Surface ectoderm, 144f Surface immunoglobulins, 207 Suspensory ligaments, 369f, 370 Sympathetic system, of nerve, 157 Symport, 6 Synapses, 15 1
classification on basis of method of signal transmission, 151-152 site of synaptic contact, 151
neurotransmitters, 152, 152t synaptic morphology, 152
Synapsin I, 4 Synaptic cleft, 132, 152 Synaptic ribbons, 238 Synaptic vesicles, 152 Synovial fluid, 103, 105 Syntrophins, 128
T Talin, 1 Of, 1 1 , 65f Taste sensation, 277 Tay-Sachs disease, 57 T-cell receptors (TCRs), 201 T cells
double negative, 202 double positive T cells, 202
T cytotoxic, 206, 218, 220 Tectorial membrane, 382 Teeth, 274
cementum, 275 crown formation, 275 dental pulp, 275 dental-supporting structures, 275 dentin, 275 enamel, 274 root formation, 275
Tektin, 84 Telogen phase, 252 Telophase, 26-27, 26f, 27t
Telophase I, 30
I n dex 421
Temperature and pain receptors, 368 Tenascin, 64 Tendons, dense, regular connective tissue in, 99 Tensor tympani muscle, 379 Teratomas, 343 Terminal bronchioles, 261-262, 395, 403 Terminal hairs, 252 Territorial matrix, hyaline cartilage, 107f, 108 Testicular cancer, 355 Testicular tunicae, 351 Testosterone, 109t, 351, 356, 393, 402 Tetany, 233 Tetralogy of Fallot, 184 Theca lutein cells, 336 T helper cells, 205, 218, 220, 393, 402 Thermoreceptors, 366 Thymic cortex, 203 Thymine, 2 1 Thymus, 213, 2 14f
blood-thymus barrier, 215 epithelial reticular cells, 2 13, 215
thymic cortex, 213 thymic medulla, 215 thymocytes, 215
Thyroid gland follicular cells, 228, 230f hormones, physiological effects of, 23 1 parafollicular cells, 229, 23 1 , 232f thyroid follicles, 228, 230f
Thyroid-stimulating hormone (TSH), 388, 398 Thyrotrophs, 223 Thyroxine, 1 09t Titin, 126f, 130 T killer cells, 393, 402 T lymphocytes, 98, 179, 392, 401
immature, 215 maturation of, 201-202 migration of, 219, 220 types and subtypes of, 205
Toll-like receptors (TLRs), 199, 200t Tongue, 275
lingual papillae, 276-277 lingual tonsil, 277 muscular core of, 277 taste buds, 277
Tonofilaments, 243 Tonsils, 217
lingual tonsil, 217, 277 palatine tonsils, 217 pharyngeal tonsil, 217, 259
Tooth crown, development of, 388, 398 Touch and pressure receptors, 367-368 Trachea, 395, 403 Trachea bronchi, 260 Transfer RNA (tRNA), 15, 23 Transfer vesicles, 34, 35 Transformed cells, 28 Trans-Golgi network (TGN), 37, 38f Transient cells, of connective tissue, 98-99 Transitional epithelia, 76f Translocation, of proteins, 56 Transmembrane proteins, 3 Triads, 125 Triiodothyronine, 228 Trimethylamine-N-oxide (TMAO), 287 Tropoelastin, 71 Tropomodulin, 126f, 129 Tropomyosin, 126f, 129 Troponin, 126f, 129
tahir99-VRG & vip.persianss.ir

422 I n d ex
T (transverse) tubules, 124-125, 126f, 131 , 134, 136f Tumor cells, 393, 402 Tumor diagnosis, 49 Tumor necrosis factor-u (TNF-u), 101 , 284, 336 Tunica adventitia, 186, 192 Tunica albuginea, 351 Tunica fibrosa, 368-370 Tunica intima, 186, 192 Tunica media, 186, 192 Tunica vasculosa, 370-371 Turner syndrome, 30 Tympanic membrane (eardrum), 378 Type I (insulin-dependent) diabetes
mellitus (IDDM), 299, 306, 308 Type II collagen, 103, 105 Type II (non-insulin-dependent) diabetes
mellitus (NIDDM), 299
u Unipolar neurons, 145, 145f Unreplicated DNA checkpoint, 26 Uracil, 22, 387, 397 Ureter, 325 Urethra, 326
female urethra, 326 male urethra, 326
Urinary space. See Bowman space Urinary system, 309
excretory passages, 324-325, 324t ureter, 325 urethra, 326 urinary bladder, 325, 325f
function of, 309 kidneys, 309, 310f
renal cortex, 310 renal hilum, 309 renal interstitium, 310 renal lobe and lobule, 310 renal medulla, 309 renal pelvis, 309
renal blood circulation, 320, 32lf arterial supply to kidney, 320 venous drainage of kidney, 321
review test, 327-328 answers and explanations, 329
urine concentration, regulation of, 321-322 collecting tubules, role of, 322 countercurrent exchange system, 323, 323f countercurrent multiplier system, 322, 322f effect of urea, 323-324
uriniferous tubules, 3 1 lt collecting tubules, 320 nephrons (see Nephrons)
Urogastrone, 282, 394, 402 Uromodulin, 317 Uterine endometrium, 348, 349 Uterine prolapse, 341 Uterus, 339
endometrium, 339, 340f layers of, 339 vascular supply of, 339
external covering, 340 menstrual cycle
menstrual phase, 340-341 proliferative (follicular) phase, 341 secretory (luteal) phase, 341
myometrium, 340 uterine wall, 339
v Vagina, 345 Vaginal mucosa, 348, 349 Varicose veins, 194 Vasa vasorum, 186 Vascular smooth muscle, 139 Vasectomy, 361 Vasoactive intestinal peptide, 298 Vasoconstriction, 189 Vasodilation, 189 Vasopressin. See Antidiuretic hormone Veins. See Blood vascular system, veins Vellus hairs, 251-252 Venoms, 7 Venules, 193f, 193t, 194 Verrucae. See Warts Very-low-density lipoproteins (VLDLs), 101 Vesicular-tubular clusters (VTCs), 37 , 38f, 54 Vestibular hair cells, 379-380 Vestibular membrane, 380 Vestibulocochlear apparatus, 378-383 Vinca alkaloids, 28 Vinculin, 10f, 1 1 , 65f Viral hepatitis A, 303 Viral hepatitis B, 303 Viral hepatitis C, 303 Visceral pericardium. See Epicardium Visceral smooth muscle, 139 Visible mucus, 279 Vitamin A deficiency, 389, 399 Vitamin B12 absorption, 286, 396, 404 Vitamin K, role in clotting process, 169 Vitamins
in bone formation, 1 19 effects of hormones and vitamins on, 109t effects on hyaline cartilage, 1 09t
Vitreous opacities (eye floaters), 373 Vocal cords, 260 Volkmann canal, 1 12f, 1 14 von Willebrand disease, 174
w Warts, 253 Water and electrolytes, 289 Water-soluble hormones, 221 Wet macular degeneration, 375-376 White adipose tissue, 100- 101 White matter, in CNS, 158 Wound healing, 63 Woven bone, 1 15
X Xenobiotics, 6 X-linked agammaglobulinemia, 201
y Yellow marrow, 174
z Z0- 1 , Z0-2, and Z0-3 protein, 77 Zellweger syndrome, 45 Zona fasciculata, 234 Zona glomerulosa, 234 Zona pellucida (ZP), 333 Zona reticularis, 234 Zonula adherens, 136f
junction, 79 Zygote, 343
tahir99-VRG & vip.persianss.ir