Embed Size (px)
Citation preview

Spine involvement in Crystal diseases
JFIM Hanoï 2015
Pr Jean Denis LAREDO Hôpital Lariboisière -‐ Paris

Spinal Crystal diseases
§ Urate monosodium : Gout § Calcium crystals
– Calcium phosphate « Apatite disease » – Calcium pyrophosphates « CPPD disease » – Calcium oxalate

Spinal Crystal diseases
§ Urate monosodium : Gout § Calcium crystals
– Calcium phosphate « Apatite disease » – Calcium pyrophosphates « CPPD disease » – Calcium oxalate

Gout

Gout



Spine Gout
§ Very uncommon
§ Severe tophaceous gout
§ Symptoms Asymptomatic at an early stage Acute and chronic back pain Nerve compression +++
§ Diagnosis: urate crystals Aspiration or biopsy DECT ? Kersley, 1950

J Radiol 2008;89
S Semlali et al. Tophus goutteux du rachis lombaire simulant unespondylodiscite : aspect en imagerie
905
chis lombaire a été retenu. Le patient aété mis sous colchicine pendant un moispuis sous allopurinol. L’évolution a étémarquée par une stabilisation de l’étatdu patient, avec disparition des lombal-gies.
DiscussionEn 1947, Bauer et Klemperer (1) font lapremière description radiologique d’uneatteinte goutteuse du rachis. Mais c’est en1950 que Kersley et al. (2) ont établi la pa-
Fig. 2 : Tomodensitométrie lombaire.a Coupe axiale passant par L2, fenêtre osseuse.b Reconstructions sagittales, en fenêtre osseuse, montrant les lésions lytiques des pla-
teaux vertébraux de L1 et L2. Noter les érosions des apophyses articulaires posté-rieures de L1 (flèche).
c Reconstruction sagittale en fenêtre parties molles, après injection de produit de contraste, montrant la prise de contraste de l’épidurite antérieure et l’épaississement des parties molles prévertébrales.
ac b
Fig. 3 : Imagerie par résonance magnétique lombaire, coupes sagittales.a Spin écho T1 : hyposignal des corps vertébraux de L1 et L2.b Spin écho T2 : les corps vertébraux L1 et L2 et le disque sont en hypersignal hétéro-
gène. Les tophus épiduraux sont en hyposignal et compriment le fourreau dural (flèches).
c STIR : le tophus épidural est en hypersignal modéré et hétérogène (flèches).
a b c
thogénie de cette atteinte, à travers les ré-sultats de l’autopsie d’un patient décédé àla suite d’une compression médullaire pardestruction du corps de la première vertè-bre cervicale par un tophus goutteux avecsub-luxation axo-atloïdienne.Le dépôt de cristal d’urate de sodium sefait le plus souvent au niveau des articula-tions et les structures péri-articulaires pé-riphériques. L’atteinte intéresse rarementle squelette axial. Quand elle existe, elleest due à un dépôt d’urate de sodium dansle disque intervertébral, le corps verté-bral, le ligament jaune ou le ligament in-tervertébral postérieur. Les phénomènesdégénératifs du rachis ont été proposéscomme facteurs prédisposant aux dépôtsd’urate, étant donnée la prédominance del’atteinte du rachis lombo-sacré (3). Cetteatteinte vertébrale est probablement sous-estimée, puisque le bilan radiologiquen’est effectué que chez les patients symp-tomatiques (3). Il n’existe pas de prédomi-nance de sexe. Les patients ont souventune longue histoire d’hyperuricémie etd’arthropathie goutteuse chronique. Lessignes cliniques sont variables, faits dedouleurs rachidiennes associées ou non àdes signes de compression médullaire ouradiculaire (4). Tous les segments rachi-diens peuvent être intéressés, avec unefréquence égale (3).Les radiographies standard mettent enévidence une discopathie érosive ainsiqu’une atteinte articulaire postérieurepouvant provoquer des subluxations oudes troubles de la statique. La TDM pré-cise les lésions lytiques du corps et desapophyses articulaires postérieures.L’IRM est réalisée quand il existe des si-gnes de compression médullaire, à la re-cherche de lésion intracanalaire. Un to-phus épidural apparaît comme une massede taille variable en avant du ligamentlongitudinal postérieur ou des ligamentsjaunes, dont le signal T1 est hypointenseou intermédiaire en T1. En pondérationT2, il est le plus souvent hypointense, se-lon le degré de calcification. Après injec-tion de gadolinium, un rehaussement ho-mogène du tophus est fréquent. Parfois lerehaussement concerne seulement la pé-riphérie du tophus (5) qui peut alors si-muler un abcès épidural tuberculeux ou àgermes banals, ou encore un processus tu-moral intracanalaire (3, 6).D’autres diagnostics différentiels peuventégalement être évoqués : une arthropa-thie à microcristaux de pyrophosphate decalcium se traduit par des calcificationsJ Radiol 2008;89
S Semlali et al. Tophus goutteux du rachis lombaire simulant unespondylodiscite : aspect en imagerie
905
chis lombaire a été retenu. Le patient aété mis sous colchicine pendant un moispuis sous allopurinol. L’évolution a étémarquée par une stabilisation de l’étatdu patient, avec disparition des lombal-gies.
DiscussionEn 1947, Bauer et Klemperer (1) font lapremière description radiologique d’uneatteinte goutteuse du rachis. Mais c’est en1950 que Kersley et al. (2) ont établi la pa-
Fig. 2 : Tomodensitométrie lombaire.a Coupe axiale passant par L2, fenêtre osseuse.b Reconstructions sagittales, en fenêtre osseuse, montrant les lésions lytiques des pla-
teaux vertébraux de L1 et L2. Noter les érosions des apophyses articulaires posté-rieures de L1 (flèche).
c Reconstruction sagittale en fenêtre parties molles, après injection de produit de contraste, montrant la prise de contraste de l’épidurite antérieure et l’épaississement des parties molles prévertébrales.
ac b
Fig. 3 : Imagerie par résonance magnétique lombaire, coupes sagittales.a Spin écho T1 : hyposignal des corps vertébraux de L1 et L2.b Spin écho T2 : les corps vertébraux L1 et L2 et le disque sont en hypersignal hétéro-
gène. Les tophus épiduraux sont en hyposignal et compriment le fourreau dural (flèches).
c STIR : le tophus épidural est en hypersignal modéré et hétérogène (flèches).
a b c
thogénie de cette atteinte, à travers les ré-sultats de l’autopsie d’un patient décédé àla suite d’une compression médullaire pardestruction du corps de la première vertè-bre cervicale par un tophus goutteux avecsub-luxation axo-atloïdienne.Le dépôt de cristal d’urate de sodium sefait le plus souvent au niveau des articula-tions et les structures péri-articulaires pé-riphériques. L’atteinte intéresse rarementle squelette axial. Quand elle existe, elleest due à un dépôt d’urate de sodium dansle disque intervertébral, le corps verté-bral, le ligament jaune ou le ligament in-tervertébral postérieur. Les phénomènesdégénératifs du rachis ont été proposéscomme facteurs prédisposant aux dépôtsd’urate, étant donnée la prédominance del’atteinte du rachis lombo-sacré (3). Cetteatteinte vertébrale est probablement sous-estimée, puisque le bilan radiologiquen’est effectué que chez les patients symp-tomatiques (3). Il n’existe pas de prédomi-nance de sexe. Les patients ont souventune longue histoire d’hyperuricémie etd’arthropathie goutteuse chronique. Lessignes cliniques sont variables, faits dedouleurs rachidiennes associées ou non àdes signes de compression médullaire ouradiculaire (4). Tous les segments rachi-diens peuvent être intéressés, avec unefréquence égale (3).Les radiographies standard mettent enévidence une discopathie érosive ainsiqu’une atteinte articulaire postérieurepouvant provoquer des subluxations oudes troubles de la statique. La TDM pré-cise les lésions lytiques du corps et desapophyses articulaires postérieures.L’IRM est réalisée quand il existe des si-gnes de compression médullaire, à la re-cherche de lésion intracanalaire. Un to-phus épidural apparaît comme une massede taille variable en avant du ligamentlongitudinal postérieur ou des ligamentsjaunes, dont le signal T1 est hypointenseou intermédiaire en T1. En pondérationT2, il est le plus souvent hypointense, se-lon le degré de calcification. Après injec-tion de gadolinium, un rehaussement ho-mogène du tophus est fréquent. Parfois lerehaussement concerne seulement la pé-riphérie du tophus (5) qui peut alors si-muler un abcès épidural tuberculeux ou àgermes banals, ou encore un processus tu-moral intracanalaire (3, 6).D’autres diagnostics différentiels peuventégalement être évoqués : une arthropa-thie à microcristaux de pyrophosphate decalcium se traduit par des calcifications
Semlali J Radiol 2008;89:904-‐6
Fig 1. A, Lateral-view radiograph of the cervical spine shows atypical diskovertebral changes from C-3 to C-6. Deep erosions ofseveral end plates (black arrow) are associated with hyperostosis (star) and prominent marginal osteophytosis (white arrows).
B, Unenhanced sagittal T1-weighted spin-echo MR image (450/20) shows large hypointense areas within the vertebral bodies of C-4,C-5, and C-6 without changes in the adjacent epidural and prevertebral spaces.
C, Postcontrast T1-weighted MR image in the same plane. Enhanced foci involve both the C-4 to C-6 disk spaces and the contiguousvertebral erosions. The ventral segment of C5-6 is spared despite dorsal involvement. Note the continuum between the diskal andvertebral lesions.
D, T2-weighted fast spin-echo MR image (3200/120, echo train length 16) in the same plane. The enhanced foci in C appear aslow-signal-intensity areas. Cord compression is obvious at the C5-6 level.
E, Histologic section of a surgically resected specimen. Two tophaceous deposits (thick black arrows) surrounded by histiocytes andmultinucleated giant cells (open arrows) are embedded in a chronic inflammatory stroma. Vascular channels (stars) and cancellous bonefragments (curved arrow) without lamellar organization are present. Note pseudopalissadic disposition of histiocytes surrounding tophi(small double arrowhead).
152 DUPREZ AJNR: 17, January 1996
Fig 1. A, Lateral-view radiograph of the cervical spine shows atypical diskovertebral changes from C-3 to C-6. Deep erosions ofseveral end plates (black arrow) are associated with hyperostosis (star) and prominent marginal osteophytosis (white arrows).
B, Unenhanced sagittal T1-weighted spin-echo MR image (450/20) shows large hypointense areas within the vertebral bodies of C-4,C-5, and C-6 without changes in the adjacent epidural and prevertebral spaces.
C, Postcontrast T1-weighted MR image in the same plane. Enhanced foci involve both the C-4 to C-6 disk spaces and the contiguousvertebral erosions. The ventral segment of C5-6 is spared despite dorsal involvement. Note the continuum between the diskal andvertebral lesions.
D, T2-weighted fast spin-echo MR image (3200/120, echo train length 16) in the same plane. The enhanced foci in C appear aslow-signal-intensity areas. Cord compression is obvious at the C5-6 level.
E, Histologic section of a surgically resected specimen. Two tophaceous deposits (thick black arrows) surrounded by histiocytes andmultinucleated giant cells (open arrows) are embedded in a chronic inflammatory stroma. Vascular channels (stars) and cancellous bonefragments (curved arrow) without lamellar organization are present. Note pseudopalissadic disposition of histiocytes surrounding tophi(small double arrowhead).
152 DUPREZ AJNR: 17, January 1996
Duprez et al. AJNR 1996;17:151-‐3
Haush et al. J Clin Rheumatol 1999;6:335-‐41
• Gout : joint deposits ü Intervertebral disc

658 D. Wendling et al. / Joint Bone Spine 80 (2013) 656–659
Fig. 1. Patient #1: discovertebral involvement with a C5-C6 tophus. T1-weightedpostgadolinium magnetic resonance imaging on the left and computed tomographyon the right.
Fig. 2. Patient #4: magnetic resonance imaging of the lumbar spine, sagittal sec-tion, T1-weighted sequence (left) and postgadolinium T1-weighted sequence (right)showing L2-L3 discitis.
elevation was noted in only two patients. In addition, only twopatients had laboratory markers for systemic inflammation.
Magnetic resonance imaging (MRI) and computed tomography(CT) showed discovertebral lesions in three patients (at the cer-vical spine in two [Fig. 1] and lumbar spine in one [Fig. 2]) andlumbar facet joint lesions in two patients (Fig. 3). Specimens of thespinal lesions were obtained in three patients: in each of the twopatients with facet joint involvement, the surgical biopsy recov-ered a tophus and the needle aspirate contained monosodium uratecrystals; and in the patient with lumbar discitis, the biopsy con-tained an inflammatory granuloma and the needle aspirate waspositive for monosodium urate crystals. In the two patients withcervical lesions, the diagnosis relied on a history of gout attacksand a rapid response to colchicine with resolution of the clinicalmanifestations and decreases in the serum uric acid and/or CRPlevels. The outcome was rapidly favorable with colchicine therapyalone in four of the five patients. Surgical resection of the affectedfacet joint was performed in the remaining patient.
Fig. 3. Patient #5: computed tomography of the lumbar spine showing a destructivelesion in the right L4-L5 facet joint.
4. Discussion
Spinal involvement with gout has chiefly been described asanecdotal case reports. Our case-series of five patients illustratesvarious types of spinal lesions due to gout: discitis, discovertebraltophus, and facet joint deposits.
4.1. Frequency
The prevalence of spinal gout is unclear since most of theavailable information comes from anecdotal case-reports. A ret-rospective study of 64 patients with documented peripheral goutwho underwent CT of the spine for various reasons showed sugges-tive changes (discovertebral erosions or tophi) in 14% of cases [5]. Arecent study involved routine CT of the spine in 45 patients with anat least 3-year history of inadequately controlled peripheral gout[6]. Spinal lesions were seen in 17 (35%) patients. The symptomswere often minimal: one or more spinal tophi were visualized in41% of these 17 patients but only half the patients reported backpain and only one patient received diagnosis of spinal gout basedon the clinical findings. Factors associated with CT abnormalitiessuggestive of spinal gout were diabetes and presence of peripheralradiographic erosions [6]. Patients with and without spinal lesionswere not significantly different for age, gout duration, body massindex, renal function, presence of hypertension, or presence of backpain. None of the patients underwent spinal biopsy, and the diag-nosis of spinal gout relied only on the CT abnormalities and historyof peripheral gout. This fact contributes to validate the diagnosis ofspinal gout in our patients #1 and #3.
4.2. Sites of involvement
No spinal segment is exempt. In the study of 45 patients withpoorly controlled gout [6], the abnormalities evidenced by routineCT of the cervical and lumbar segments were located in the lumbarspine in 94% of cases and in the cervical spine in 42% of cases; inaddition, 6% of patients had lesions of the sacroiliac joints. CT of thethoracic spine was not performed, although this segment can beinvolved [4,7,8]. As shown in two of our five patients, lesions of thecervical spine are fairly common [9]. Development of a tophus in thedens [10–12] and atlantoaxial subluxation [13] have been reported.Involvement of the cervical spine may seem counterintuitive, asperipheral gouty arthritis predominantly affects the distal lowerlimbs.
4.3. Presenting symptoms
The presentation of spinal gout varies considerably. Somepatients have little or no symptoms, and the diagnosis is establishedonly when an imaging study shows abnormalities, particularlya spinal tophus [6] (as in our patient #2). Others present withsevere symptoms such as inflammatory pain suggesting discitis[14–16] (as in our patients #3 and #4), epidural infection [17], or aparaspinal abscess [18]. Spinal instability due to gouty lesions hasbeen reported more rarely [13,19].
4.4. Neurological complications
Spinal gout may cause neurological complications dependingon the spinal segment involved (cervical, thoracic, or lumbar) andon the location of the tophi (bone, epidural space, or filum ter-minale). Thus, patients may present with nerve root symptoms,spinal cord compression, or symptoms of lumbar spinal stenosis[20–26]. Only one of our five patients had neurological symptoms

M 42, Gout for 15 years. Tophus of the extremiQes for 1 year. IntermiRent back pain



T1-‐WI Gad-‐enhanced T1-‐WI

ARTICLE IN PRESSG Model
Revue du rhumatisme xxx (2013) xxx–xxx
Disponible en ligne sur
www.sciencedirect.com
Lettre à la rédaction
Goutte rachidienne chez un jeune patient comportant uneatteinte des régions thoraciques, lombaires et des sacro-iliaques!
i n f o a r t i c l e
Mots clés :GoutteGoutte rachidienneSacroiliite
Un homme âgé de 25 ans consulta pour une atteinte polyarti-culaire comportant des douleurs, un gonflement et une raideur. Ilexistait des douleurs modérées du flanc gauche, de la fièvre, dessueurs nocturnes, et une anorexie évoluant depuis une semaine.Dans les antécédents, il était noté, deux ans auparavant, une aug-mentation de la créatininémie, mais le patient avait été perdu devue. Cet homme jeune était originaire d’Amérique du Sud et tra-vaillait dans une ferme laitière.
À l’examen physique, le patient était apyrétique et ses fonc-tions vitales étaient normales. La seule anomalie consistait en unerougeur et une chaleur de nombreuses articulations. Les examensbiologiques initiaux montraient une créatininémie à 700 !mol/L,une uricémie à 462 !mol/L et une leucocytose à 13 500/mm3. Larecherche de l’antigène HLA B27 était négative. L’analyse du liquidearticulaire obtenu par ponction du genou droit révélait des cristauxd’urate de sodium. Les sérologies infectieuses étaient négatives, demême que le test tuberculinique, les hémocultures, les cultures desurines et du liquide articulaire. L’échographie rénale était en faveurd’une néphropathie chronique.
La tomodensitométrie (TDM) abdominopelvienne mettait enévidence des lésions articulaires érosives, bien limitées, sansostéolyse, et des nodules tissulaires siégeant aux articulationscostovertébrales droites de T9 et T10, à l’articulation costoverté-brale gauche de T12 (Fig. 1), aux articulation interapophysairespostérieures, à droite en L3-L4 et L4-L5, et à gauche en L5-S1. Il exis-tait également une atteinte érosive de l’articulation sacro-iliaquegauche évocatrice de sacroiliite (Fig. 2). Les diagnostics envisagésétaient les suivants : goutte, brucellose, tuberculose, amylose, ainsiqu’une spondyloarthrite sous-jacente.
À l’IRM rachidienne, on observait de nombreuses lésions biencirconscrites, centrées sur les articulations, en hyposignal T1 etayant un signal discrètement hétérogène en T2. Il existait des éro-sions de la sacro-iliaque gauche.
On réalisait alors, sous contrôle TDM, une biopsie percutanéed’une lésion de l’arc postérieur de L5 à gauche. L’analyse mettait
DOI de l’article original : http://dx.doi.org/10.1016/j.jbspin.2013.02.012.! Ne pas utiliser, pour citation, la référence franc aise de cet article, mais la réfé-
rence anglaise de Joint Bone Spine avec le DOI ci-dessus.
en évidence des dépôts de cristaux d’urate de sodium accompa-gnés d’une réaction à corps étrangers compatible avec un tophusgoutteux.
Le patient était traité par prednisone, initialement à la posologiede 50 mg/j, posologie ensuite décroissante. Un traitement par allo-purinol était débuté à la posologie de 100 mg/j. Malgré cela, sontsurvenues plusieurs crises de goutte qui ont pu être dues à unefaible observance thérapeutique ou à l’aggravation de la fonctionrénale qui nécessita la mise en dialyse péritonéale.
La goutte rachidienne était auparavant considérée comme rare,mais des études récentes ont montré une prévalence allant jusqu’à35 % chez des patients ayant une goutte articulaire [1–3]. Dansune étude récente, l’âge moyen des patients ayant une goutterachidienne était de 65 ans [2]. La goutte rachidienne atteint pré-férentiellement le rachis lombaire et l’atteinte des sacro-iliaquesest inhabituelle [1–4]. Les signes cliniques de la goutte rachidiennepeuvent être très variables [1,4]. Il est très rare qu’elle atteigne despatients âgés de moins de 45 ans. Dans la littérature, il en a étérapporté trois cas atteignant le rachis lombaire (âge des patients :17, 27 et 29 ans), un cas atteignant le rachis thoracique (28 ans) etun cas atteignant le rachis cervical (29 ans) [4–8]. Les mécanismesphysiopathologiques incriminés sont une longue évolution de lamaladie goutteuse, une atteinte rachidienne dégénérative associéeet une transplantation rénale.
Dans les cas de goutte rachidienne, la TDM peut mon-trer des érosions intra-articulaires et juxta-articulaires avec
Fig. 1. Érosion articulaire de la costovertébrale gauche de T12. La coupe axiale TDMmontre des érosions articulaires bien limitées, sans ostéolyse, sur la costovertébralegauche de T12. Il existe un aspect nodulaire des parties molles autour des érosionssous-chondrales.
1169-8330/$ – see front matter © 2013 Publie par Elsevier Masson SAS pour la Société Française de Rhumatologie.http://dx.doi.org/10.1016/j.rhum.2013.03.013
REVRHU-4210; No. of Pages 2
• Gout : joint deposits ü Intervertebral disc ü Costo-‐vertebral joint ü Facet joint

Interspinous gout bursi2s

Tophus in ligaments

Spinal cord compression due to tophus
Dharmadhikari et al., A rare cause of spinal cord compression, Skeletal Radiol(2006)35: 942–945

Dharmadhikari et al., A rare cause of spinal cord compression, Skeletal Radiol(2006)35: 942–945

On CT imaging, gouty tophi have been noted to measurearound 160 HU because of the monosodium urate crystal dep-osition.3 The attenuation of the lesions in our patient was inthe range of 130 –170 HU, which is consistent with previouslyreported findings.
FDG-PET fusion images with both MR and CT wereacquired because of the differential diagnostic consider-ations, including metastatic disease. To the best of ourknowledge, no published reports have discussed the meta-bolic characteristics of gout on PET. FDG-PET imagingdemonstrates hypermetabolism within the lytic bone le-sions and paraspinal masses.
The pathophysiology of prolonged hyperuricemia resultsin crystals precipitating in joint cavities. The crystals provokean acute inflammatory response (acute gouty arthritis), whichin severe cases progresses to form chalky white tophi (chronictophaceous gout). By routine light microscopy the tophi ap-pear as extracellular gray material surrounded by fibrous tis-sue and histiocytes/multinulceated giant cells. Polarized light
can be confirmatory by demonstrating the needle-shapedcrystals with strong negative birefringence characteristic ofgout.
Macrophages and growth factors have been shown to play aprotective role in the pathophysiology of gout and in the res-olution of acute gout with removal of urate crystals.4,5 Highuptake of FDG has been related to macrophage activity and thepresence of growth factors, which accounts for the intenseradiotracer accumulation on FDG-PET.6-8 PET imaging alsodemonstrates excellent correlation between the regions of hy-permetabolism and gadolinium enhancement.
The location of the hypermetabolic activity, within the pos-terior elements, with relative sparing of the vertebral bodies,should have broadened the differential diagnostic consider-ations initially entertained to include hypermetabolic spinallesions such as gout, in addition to infection and neoplasticetiologies. Retrospectively, the patient’s history was crucial tothe diagnosis, as many of the other articles published on spinalgouty tophi state.2,9-18
Fig 2. A, T2-weighted sagittal image (TR/TE, 4550/110) shows predominantly hypointense mass lesions replacing the posterior elements of T4 through T7. B, T1-weighted sagittal image(516/12) demonstrates hypointensity of the same lesions. C, T1-weighted fat saturation images with gadolinium (816/12) with avid enhancement of the lesions.
Fig 3. A, T1-weighted axial image (TR/TE, 617/10); B, T1-weighted axial image with 20 mL gadolinium (550/12) and C, T2-weighted axial image (6350/80) demonstrate extradural lesionswith mass effect on the thecal sac resulting in spinal stenosis.
1202 Popovich ! AJNR 27 ! Jun-Jul 2006 ! www.ajnr.org
On CT imaging, gouty tophi have been noted to measurearound 160 HU because of the monosodium urate crystal dep-osition.3 The attenuation of the lesions in our patient was inthe range of 130 –170 HU, which is consistent with previouslyreported findings.
FDG-PET fusion images with both MR and CT wereacquired because of the differential diagnostic consider-ations, including metastatic disease. To the best of ourknowledge, no published reports have discussed the meta-bolic characteristics of gout on PET. FDG-PET imagingdemonstrates hypermetabolism within the lytic bone le-sions and paraspinal masses.
The pathophysiology of prolonged hyperuricemia resultsin crystals precipitating in joint cavities. The crystals provokean acute inflammatory response (acute gouty arthritis), whichin severe cases progresses to form chalky white tophi (chronictophaceous gout). By routine light microscopy the tophi ap-pear as extracellular gray material surrounded by fibrous tis-sue and histiocytes/multinulceated giant cells. Polarized light
can be confirmatory by demonstrating the needle-shapedcrystals with strong negative birefringence characteristic ofgout.
Macrophages and growth factors have been shown to play aprotective role in the pathophysiology of gout and in the res-olution of acute gout with removal of urate crystals.4,5 Highuptake of FDG has been related to macrophage activity and thepresence of growth factors, which accounts for the intenseradiotracer accumulation on FDG-PET.6-8 PET imaging alsodemonstrates excellent correlation between the regions of hy-permetabolism and gadolinium enhancement.
The location of the hypermetabolic activity, within the pos-terior elements, with relative sparing of the vertebral bodies,should have broadened the differential diagnostic consider-ations initially entertained to include hypermetabolic spinallesions such as gout, in addition to infection and neoplasticetiologies. Retrospectively, the patient’s history was crucial tothe diagnosis, as many of the other articles published on spinalgouty tophi state.2,9-18
Fig 2. A, T2-weighted sagittal image (TR/TE, 4550/110) shows predominantly hypointense mass lesions replacing the posterior elements of T4 through T7. B, T1-weighted sagittal image(516/12) demonstrates hypointensity of the same lesions. C, T1-weighted fat saturation images with gadolinium (816/12) with avid enhancement of the lesions.
Fig 3. A, T1-weighted axial image (TR/TE, 617/10); B, T1-weighted axial image with 20 mL gadolinium (550/12) and C, T2-weighted axial image (6350/80) demonstrate extradural lesionswith mass effect on the thecal sac resulting in spinal stenosis.
1202 Popovich ! AJNR 27 ! Jun-Jul 2006 ! www.ajnr.org
Spinal cord compression due to tophus
Popovitch et al AJNR 2006 27:1201-‐3

T1 T2 T1 G
Cauda equina compression due to tophus

Odontoid fractures
550 Letters to the editor / Joint Bone Spine 38 (2013) 541–555
Spontaneous odontoid fracture on a tophus responsible forspinal cord compression: A case report
a r t i c l e i n f o
Keywords:Tophaceous goutOdontoid processFractureCervical spineCord compression
We report the case of a 60-year-old man with a 6-month his-tory of walking disorders recently complicated by urinary andbowel incontinence. For more than 15 years, he had large tophi,severe deformities and repeated articular gout crisis treated withcolchicine.
Clinical examination disclosed hypoesthesia, spasticity andincreased deep tendons reflexes of the lower limbs. He hadhigh C-reactive protein (323 mg/l) and serum uric acid (SUA)(11.4 mg/dL) levels without renal failure. Rheumatoid factor andanti-citrullinated protein antibodies were negative. Blood culturesremained sterile.
Fig. 1. Cervical spine imaging. Magnetic resonance imaging of the cervical spineshowing C1-C2 anterior arthritis. Sagittal T2-weighed sequence with fat satura-tion (A) revealed bone oedema, erosions and destruction of the anterior C1-C2joint. Synovial hypertrophy was in high T2 signal. Unenhanced sagittal T1-weightedsequence (B) showed joint destruction and suspected odontoid peg fracture.Enhanced sagital T1-weighed sequence with fat saturation (C) highlights anteriorsynovial hypertrophy C1-C2 enhanced by gadolinium, confirmed large erosionsincluding clivus. Computed tomography scan in sagittal (D) and axial planes (E) atthe upper cervical spine. It displayed the erosive lesions of C1-C2 anterior joint witha fracture of the odontoid peg responsible for the posterior subluxation of the odon-toid process. Cord compression resulted from the synovial hypertrophy of C1-C2worsened by the posterior subluxation of odontoid process.
Fig. 2. Multimodal fusion using a post-treatment software (General Electric®)between CT scan and enhanced T1-weighted sequence images showing the pro-jection of inflammatory synovial hypertrophy C1-C2 (in green) on erosive bonelesions.
Cervical spine magnetic resonance imaging (MRI) showed syno-vial hypertrophy of the anterior C1-C2 joint with large erosions(Fig. 1). Computed tomography scan (CT) depicted a fracture at thebase of the odontoid dens associated with posterior C1-C2 sub-luxation (Fig. 1D and E). Multimodal fusion between CT and MRIviews highlighted the projection of inflammatory synovial hyper-trophy at C1-C2 level on bone erosions (Fig. 2). Because of fractureinstability and medullar compression signs, surgical procedure wasperformed using posterior cervical C1-C2 arthrodesis. In additionto colchicine, febuxostat 80 mg/d was initiated. Two weeks later,CRP and SUA have sharply decreased (15 mg/l [−95%] and 7.7 mg/dl[−33%], respectively). Three months after surgery, under activephysical therapy, the patient was able to walk on his own withtwo crutches and has partially recovered continence.
1. Discussion
This exceptional case of tophus eroding the odontoid processleading to spontaneous fracture and medullar compression high-lights the potential aggressiveness of chronic hyperuricemia anduntreated gout. Nevertheless, gout tophus was not formally provenin spite of surgical procedure. This approach to treat spinal cordcompression was chosen since it provided better biomechanicalstability and, based on imaging data, there was no argument for aninfection or a tumor. This technique reduces the neurological riskof an anterior approach of the cervical spine, but biopsy could notbe performed.
Nearly 120 cases of spinal tophaceous gout have been describedsince 1950 [1,2]. Spine involvement can lead to neurological com-plications such as root, spinal cord compression or intermittentclaudication [1]. Spinal location may be underestimated. Indeed,spine radiological changes were found in 14% of patients withperipheral gout [3] and in 35% of the one with history of goutyarthritis for at least 3 years [4]. By contrast, gout leading to odon-toid process spontaneous fracture is extremely rare. Three cases arereported in literature: two cases had only neck pain [5,6] and onehad cranial nerve palsies [7]. Spontaneous tophaceous fractures arerare but can be found at various locations [8].
550 Letters to the editor / Joint Bone Spine 38 (2013) 541–555
Spontaneous odontoid fracture on a tophus responsible forspinal cord compression: A case report
a r t i c l e i n f o
Keywords:Tophaceous goutOdontoid processFractureCervical spineCord compression
We report the case of a 60-year-old man with a 6-month his-tory of walking disorders recently complicated by urinary andbowel incontinence. For more than 15 years, he had large tophi,severe deformities and repeated articular gout crisis treated withcolchicine.
Clinical examination disclosed hypoesthesia, spasticity andincreased deep tendons reflexes of the lower limbs. He hadhigh C-reactive protein (323 mg/l) and serum uric acid (SUA)(11.4 mg/dL) levels without renal failure. Rheumatoid factor andanti-citrullinated protein antibodies were negative. Blood culturesremained sterile.
Fig. 1. Cervical spine imaging. Magnetic resonance imaging of the cervical spineshowing C1-C2 anterior arthritis. Sagittal T2-weighed sequence with fat satura-tion (A) revealed bone oedema, erosions and destruction of the anterior C1-C2joint. Synovial hypertrophy was in high T2 signal. Unenhanced sagittal T1-weightedsequence (B) showed joint destruction and suspected odontoid peg fracture.Enhanced sagital T1-weighed sequence with fat saturation (C) highlights anteriorsynovial hypertrophy C1-C2 enhanced by gadolinium, confirmed large erosionsincluding clivus. Computed tomography scan in sagittal (D) and axial planes (E) atthe upper cervical spine. It displayed the erosive lesions of C1-C2 anterior joint witha fracture of the odontoid peg responsible for the posterior subluxation of the odon-toid process. Cord compression resulted from the synovial hypertrophy of C1-C2worsened by the posterior subluxation of odontoid process.
Fig. 2. Multimodal fusion using a post-treatment software (General Electric®)between CT scan and enhanced T1-weighted sequence images showing the pro-jection of inflammatory synovial hypertrophy C1-C2 (in green) on erosive bonelesions.
Cervical spine magnetic resonance imaging (MRI) showed syno-vial hypertrophy of the anterior C1-C2 joint with large erosions(Fig. 1). Computed tomography scan (CT) depicted a fracture at thebase of the odontoid dens associated with posterior C1-C2 sub-luxation (Fig. 1D and E). Multimodal fusion between CT and MRIviews highlighted the projection of inflammatory synovial hyper-trophy at C1-C2 level on bone erosions (Fig. 2). Because of fractureinstability and medullar compression signs, surgical procedure wasperformed using posterior cervical C1-C2 arthrodesis. In additionto colchicine, febuxostat 80 mg/d was initiated. Two weeks later,CRP and SUA have sharply decreased (15 mg/l [−95%] and 7.7 mg/dl[−33%], respectively). Three months after surgery, under activephysical therapy, the patient was able to walk on his own withtwo crutches and has partially recovered continence.
1. Discussion
This exceptional case of tophus eroding the odontoid processleading to spontaneous fracture and medullar compression high-lights the potential aggressiveness of chronic hyperuricemia anduntreated gout. Nevertheless, gout tophus was not formally provenin spite of surgical procedure. This approach to treat spinal cordcompression was chosen since it provided better biomechanicalstability and, based on imaging data, there was no argument for aninfection or a tumor. This technique reduces the neurological riskof an anterior approach of the cervical spine, but biopsy could notbe performed.
Nearly 120 cases of spinal tophaceous gout have been describedsince 1950 [1,2]. Spine involvement can lead to neurological com-plications such as root, spinal cord compression or intermittentclaudication [1]. Spinal location may be underestimated. Indeed,spine radiological changes were found in 14% of patients withperipheral gout [3] and in 35% of the one with history of goutyarthritis for at least 3 years [4]. By contrast, gout leading to odon-toid process spontaneous fracture is extremely rare. Three cases arereported in literature: two cases had only neck pain [5,6] and onehad cranial nerve palsies [7]. Spontaneous tophaceous fractures arerare but can be found at various locations [8].
De Parisot et al Joint Bone Spine. 2013;38:550-‐1
550 Letters to the editor / Joint Bone Spine 38 (2013) 541–555
Spontaneous odontoid fracture on a tophus responsible forspinal cord compression: A case report
a r t i c l e i n f o
Keywords:Tophaceous goutOdontoid processFractureCervical spineCord compression
We report the case of a 60-year-old man with a 6-month his-tory of walking disorders recently complicated by urinary andbowel incontinence. For more than 15 years, he had large tophi,severe deformities and repeated articular gout crisis treated withcolchicine.
Clinical examination disclosed hypoesthesia, spasticity andincreased deep tendons reflexes of the lower limbs. He hadhigh C-reactive protein (323 mg/l) and serum uric acid (SUA)(11.4 mg/dL) levels without renal failure. Rheumatoid factor andanti-citrullinated protein antibodies were negative. Blood culturesremained sterile.
Fig. 1. Cervical spine imaging. Magnetic resonance imaging of the cervical spineshowing C1-C2 anterior arthritis. Sagittal T2-weighed sequence with fat satura-tion (A) revealed bone oedema, erosions and destruction of the anterior C1-C2joint. Synovial hypertrophy was in high T2 signal. Unenhanced sagittal T1-weightedsequence (B) showed joint destruction and suspected odontoid peg fracture.Enhanced sagital T1-weighed sequence with fat saturation (C) highlights anteriorsynovial hypertrophy C1-C2 enhanced by gadolinium, confirmed large erosionsincluding clivus. Computed tomography scan in sagittal (D) and axial planes (E) atthe upper cervical spine. It displayed the erosive lesions of C1-C2 anterior joint witha fracture of the odontoid peg responsible for the posterior subluxation of the odon-toid process. Cord compression resulted from the synovial hypertrophy of C1-C2worsened by the posterior subluxation of odontoid process.
Fig. 2. Multimodal fusion using a post-treatment software (General Electric®)between CT scan and enhanced T1-weighted sequence images showing the pro-jection of inflammatory synovial hypertrophy C1-C2 (in green) on erosive bonelesions.
Cervical spine magnetic resonance imaging (MRI) showed syno-vial hypertrophy of the anterior C1-C2 joint with large erosions(Fig. 1). Computed tomography scan (CT) depicted a fracture at thebase of the odontoid dens associated with posterior C1-C2 sub-luxation (Fig. 1D and E). Multimodal fusion between CT and MRIviews highlighted the projection of inflammatory synovial hyper-trophy at C1-C2 level on bone erosions (Fig. 2). Because of fractureinstability and medullar compression signs, surgical procedure wasperformed using posterior cervical C1-C2 arthrodesis. In additionto colchicine, febuxostat 80 mg/d was initiated. Two weeks later,CRP and SUA have sharply decreased (15 mg/l [−95%] and 7.7 mg/dl[−33%], respectively). Three months after surgery, under activephysical therapy, the patient was able to walk on his own withtwo crutches and has partially recovered continence.
1. Discussion
This exceptional case of tophus eroding the odontoid processleading to spontaneous fracture and medullar compression high-lights the potential aggressiveness of chronic hyperuricemia anduntreated gout. Nevertheless, gout tophus was not formally provenin spite of surgical procedure. This approach to treat spinal cordcompression was chosen since it provided better biomechanicalstability and, based on imaging data, there was no argument for aninfection or a tumor. This technique reduces the neurological riskof an anterior approach of the cervical spine, but biopsy could notbe performed.
Nearly 120 cases of spinal tophaceous gout have been describedsince 1950 [1,2]. Spine involvement can lead to neurological com-plications such as root, spinal cord compression or intermittentclaudication [1]. Spinal location may be underestimated. Indeed,spine radiological changes were found in 14% of patients withperipheral gout [3] and in 35% of the one with history of goutyarthritis for at least 3 years [4]. By contrast, gout leading to odon-toid process spontaneous fracture is extremely rare. Three cases arereported in literature: two cases had only neck pain [5,6] and onehad cranial nerve palsies [7]. Spontaneous tophaceous fractures arerare but can be found at various locations [8].

to confirm the diagnosis of axial gout. Dual-energy CT isincreasingly recognized as a very sensitive tool for identifi-cation of monosodium urate deposits in the appendicularskeleton, but has not been systematically applied to the diag-nosis of axial gout7.
We hypothesized that axial gout will be seen more com-monly in patients with prolonged duration of proven appen-dicular gout and in patients with radiological evidence ofgouty erosions or tophi in the hands or feet. To test thishypothesis, we performed a cross-sectional study in subjectswith definite gouty arthritis whose condition was not underoptimal control.
MATERIALS AND METHODSPatients. Patients who satisfied the American College of Rheumatology(ACR) criteria for gout were included in the study from January 2008 toMay 20108. All the study-related procedures were performed at WashingtonHospital Center and were approved by the institutional review board.Subjects with a history of gout for 3 or more years were recruited if theyhad at least 1 attack of acute gouty arthritis in the prior year or had persist-ent hyperuricemia (serum uric acid > 7.0 mg/dl) on a minimum of 3 occa-sions for 3 years prior to enrollment.
Clinical and laboratory data included duration of peripheral gouty arthri-tis; past or present back pain; presence of joint deformities from gouty arthri-tis; presence of clinical tophi; urate crystal demonstration from synovial fluidor tophi; body mass index (BMI); comorbid conditions, namely DM andHTN; current allopurinol therapy; serum uric acid (SUA); and creatinineclearance calculated by the modification of diet in renal disease method.
Imaging studies included radiographs of the hands and feet andlow-dose non-contrast CT of the cervical spine, lumbar spine, and sacroil-iac joints (SIJ). If prior radiographs of the hands and feet that were avail-able showed erosions or tophi characteristic of gouty change, then no further radiographs were performed. Radiographs were read by an experi-enced rheumatologist (AW) blinded to CT results. CT were read by 2 mus-culoskeletal radiologists blinded to clinical data and appendicular radio -graphy results. These radiography and CT results were used in the study.However, the same images (radiographs and CT) were also read by the clin-ical radiologist in the radiology department assigned to a given patient; thereading was not part of the study but became part of the respective patient’ssource document. Primary and other analyses. Primary analyses included an estimation of theprevalence of axial gout in this population and correlation of axial goutwith the duration of peripheral gouty arthritis. Other analyses includedspinal location of axial gout and correlation of axial gout with the clinical,laboratory, and radiologic features described above.Statistical methods. Sample size calculations were based on a frequency ofaxial gout of 20% in our study population and a mean duration of gout insubjects with axial disease of 13.5 years compared to 9.0 years in thosewithout axial gout. Depending on the estimates of the standard deviationsof the duration of gout, sample size estimates for 80% power varied from40 to 120 patients for nonparametric analyses. We recorded the estimatedduration of gout in 5-year increments to > 15 years. Demographic and clin-ical features were summarized as mean (SD) values for continuous vari-ables and proportions for categorical variables for all subjects and by axialgout status. Fisher’s exact test and Wilcoxon rank-sum test were used tocompare the proportion and distribution between the axial groups, respec-tively. Two-tailed p values < 0.05 were considered statistically significant.Data were analyzed using SAS version 9.1 (SAS Institute, Cary, NC, USA).
RESULTSForty-eight subjects were studied. The characteristics of the
population are shown in Table 1 and the comparison of thosesubjects with and without axial gout is shown in Table 2.The gout control was less than optimal, with 96% ofresearch subjects having experienced at least 1 attack ofarthritis within the year prior to enrollment. Seventeen of the48 subjects (35%) had CT evidence of spinal gout with ero-sions and/or tophi and 7 (15%) had spinal tophi (Figures 1and 2). The locations of the characteristic CT changes ofaxial gout were lumbar in 16 (94%), cervical in 7 (42%), andSIJ in 1 (6%). Of the 17 patients with axial gout, 14 (82%)had more than 1 vertebral level involved.
Men comprised 73% of cases of axial gout compared towomen at 27%, but these proportions were similar to theentire gout population studied. The majority (87%) of ourstudy population was black and all the patients with axialgout were black (p = 0.08).
Twenty-six (54%) subjects had gout for more than 10years and 18 (38%) for more than 15 years. Only 7 subjects(15%) had gout for less than 5 years. While 65% of the sub-jects with axial gout had clinical gouty arthritis for morethan 10 years (compared to 48% of those without axialgout), this was not statistically significant (p = 0.37). Therewas also no correlation of axial gout with duration of gout
1446 The Journal of Rheumatology 2012; 39:7; doi:10.3899/jrheum.111517
Personal non-commercial use only. The Journal of Rheumatology Copyright © 2012. All rights reserved.
Table 1. Features of the gout population studied (n = 48 patients).
Characteristic Number or %
Mean age (SD)/range, yrs 61 (12.8)/35–85Male, % 73Black, % 88Mean serum uric acid level (SD)/range, mg/dl 7.7 (2.5)/2.8–13.6Duration of gout > 10 yrs, % 54Clinical tophi present, % 46Back pain present, % 50Peripheral radiographic erosions, n (%) 21/47 (45)Axial gout erosions and/or tophi, n (%) 17/48 (35)Axial tophi, n (%) 7/48 (15)
Table 2. Features of subjects with and without axial gout.
Characteristic Axial Gout, No Axial Gout, pn = 17 n = 31
Mean age (SD), yrs 65 (10.8) 59 (13.5) 0.16Duration of gout > 10 years,
n (%) 11 (65) 15 (48) 0.37Mean serum uric acid level (SD),
mg/dl 7.5 (2.7) 7.9 (2.5) 0.39Back pain, n (%) 10 (59) 14 (45) 0.55Peripheral clinical tophi, n (%) 11 (65) 11 (35) 0.07Hypertension, % 94 81 0.40Body mass index > 25, % 62 67 0.10Creatinine clearance < 60 ml/min, % 93 62 0.07Current allopurinol therapy, % 41 42 1.0Diabetes mellitus, % 65 32 0.04Peripheral radiographic erosions,
n (%) 13 (81) 8 (26) < 0.001
of RheumatologyThe Journal on January 3, 2014 - Published by www.jrheum.orgDownloaded from
1445Konatalapalli, et al: Axial gout
Personal non-commercial use only. The Journal of Rheumatology Copyright © 2012. All rights reserved.
Correlates of Axial Gout: A Cross-sectional Study RUKMINI M. KONATALAPALLI, ELENA LUMEZANU, JAMES S. JELINEK, MARK D. MURPHEY, HONG WANG,and ARTHUR WEINSTEIN
ABSTRACT. Objective. A cross-sectional study was undertaken to determine the prevalence of axial gout inpatients with established gouty arthritis and to analyze clinical, laboratory, and radiological correlations.Methods. Forty-eight subjects with a history of gouty arthritis (American College of Rheumatologycriteria) for ≥ 3 years under poor control were included. Subjects underwent history, physical exam-ination, laboratory testing, and imaging studies, including radiographs of the hands and feet andcomputerized tomography (CT) of the cervical and lumbar spines and sacroiliac joints (SIJ). Patientswith characteristic erosions and/or tophi in the spine or SIJ were considered to have axial or spinalgout.Results. Seventeen patients (35%) had CT evidence of spinal erosions and/or tophi, with tophi iden-tified in 7 of the 48 subjects (15%). The spinal location of axial gout was cervical in 7 patients(15%), lumbar in 16 (94%), SIJ in 1 (6%), and more than 1 location in 14 (82%). Duration of gout,presence of back pain, and serum uric acid levels did not correlate with axial gout. Extremity radio -graphs characteristic of gouty arthropathy found in 21 patients (45%) were strongly correlated withCT evidence of axial gout (p < 0.001). All patients with tophi in the spine had abnormal hand or feetradiographs (p = 0.005).Conclusion.Axial gout may be a common feature of chronic gouty arthritis. The lack of correlationwith back pain, the infrequent use of CT imaging in patients with back pain, and the lack of recog-nition of the problem of spinal involvement in gouty arthritis suggest that this diagnosis is oftenmissed. (First Release April 15 2012; J Rheumatol 2012;39:1445–9; doi:10.3899/rheum.111517)
Key Indexing Terms:
GOUT SPINE TOPHI EROSIONS COMPUTERIZED TOMOGRAPHY BACK PAIN
From the Division of Rheumatology, Department of Medicine, and
Department of Radiology, Washington Hospital Center, Washington, DC;
and Department of Biostatistics and Epidemiology, MedStar Health
Research Institute, Hyattsville, Maryland, USA.
Supported in part by a research grant from Savient Pharmaceuticals, Inc.
and by a Fellowship Training Award from the Research and Education
Foundation, American College of Rheumatology.
R.M. Konatalapalli, MD, Former Fellow; E. Lumezanu, MD, Fellow,
Division of Rheumatology; J.S. Jelinek, MD, FACR, Chair, Department of
Radiology, Washington Hospital Center; M.D. Murphey, MD, FACR,
Physician-in-Chief, American Institute for Radiologic Pathology, Silver
Spring, Maryland, and Professor of Radiology, Uniformed Services
University of the Health Sciences, Bethesda, Maryland; H. Wang, MD,
MS, Statistician, Department of Biostatistics and Epidemiology, MedStar
Health Research Institute, the Georgetown and Howard Universities
Center for Clinical and Translational Sciences, Georgetown; A. Weinstein,
MD, FACP, FRCP, MACR, Professor of Medicine, Georgetown University
Medical Center; Chief, Division of Rheumatology, Washington Hospital
Center.
Address correspondence to Dr. A. Weinstein, Division of Rheumatology,
Suite 2A-66, Washington Hospital Center, 110 Irving Street, NW,
Washington, DC 20010, USA. E-mail: [email protected]
Accepted for publication February 12, 2012.
Axial gout is recognized as a known feature of chronicgout1. With the increasing prevalence of hyperuricemia andgout, it is likely that axial gout would be recognized morefrequently2. Although literature reviews have describedmany cases3,4, its prevalence and clinical correlations remainuncertain, as no large, prospective studies have been pub-lished. In an earlier analysis of patients with gout who had
spinal computerized tomography (CT) available for evalua-tion, the prevalence of axial gout was 14%1. However,because of its retrospective design, we were not able toderive definitive data on the possible association of axialgout with important clinical and laboratory features includ-ing duration of peripheral gouty arthritis; serum urate levels;and presence of clinical or radiological tophi, symptomaticback pain, and comorbidities such as hypertension (HTN),diabetes mellitus (DM), and chronic renal insufficiency.
This cross-sectional study was undertaken to obtain amore accurate estimation of the prevalence of axial gout andto explore its clinical, laboratory, and radiologic correlates.
Similarly to our prior study, CT was utilized as the imag-ing modality to identify axial gout5. CT reveals characteris-tic changes of axial gout: intraarticular and juxtaarticularerosions with sclerotic margins and an attenuation or densi-ty greater than the surrounding muscle due to deposition ofsodium urate crystals. Multiple anatomic sites within thevertebral column can be involved, including the epiduralspace, intradural space, ligamentum flavum, discovertebraljunction, the pedicles, facet joints, spinous processes, filumterminale, and neural foramina5. Other reports have shownbiopsy-proven urate crystals in the spine in the presence ofcharacteristic imaging appearance6. Therefore for this study,in the presence of typical CT findings of axial gout inpatients with proven clinical gout, biopsy was not obtained
of RheumatologyThe Journal on January 3, 2014 - Published by www.jrheum.orgDownloaded from
1445Konatalapalli, et al: Axial gout
Personal non-commercial use only. The Journal of Rheumatology Copyright © 2012. All rights reserved.
Correlates of Axial Gout: A Cross-sectional Study RUKMINI M. KONATALAPALLI, ELENA LUMEZANU, JAMES S. JELINEK, MARK D. MURPHEY, HONG WANG,and ARTHUR WEINSTEIN
ABSTRACT. Objective. A cross-sectional study was undertaken to determine the prevalence of axial gout inpatients with established gouty arthritis and to analyze clinical, laboratory, and radiological correlations.Methods. Forty-eight subjects with a history of gouty arthritis (American College of Rheumatologycriteria) for ≥ 3 years under poor control were included. Subjects underwent history, physical exam-ination, laboratory testing, and imaging studies, including radiographs of the hands and feet andcomputerized tomography (CT) of the cervical and lumbar spines and sacroiliac joints (SIJ). Patientswith characteristic erosions and/or tophi in the spine or SIJ were considered to have axial or spinalgout.Results. Seventeen patients (35%) had CT evidence of spinal erosions and/or tophi, with tophi iden-tified in 7 of the 48 subjects (15%). The spinal location of axial gout was cervical in 7 patients(15%), lumbar in 16 (94%), SIJ in 1 (6%), and more than 1 location in 14 (82%). Duration of gout,presence of back pain, and serum uric acid levels did not correlate with axial gout. Extremity radio -graphs characteristic of gouty arthropathy found in 21 patients (45%) were strongly correlated withCT evidence of axial gout (p < 0.001). All patients with tophi in the spine had abnormal hand or feetradiographs (p = 0.005).Conclusion.Axial gout may be a common feature of chronic gouty arthritis. The lack of correlationwith back pain, the infrequent use of CT imaging in patients with back pain, and the lack of recog-nition of the problem of spinal involvement in gouty arthritis suggest that this diagnosis is oftenmissed. (First Release April 15 2012; J Rheumatol 2012;39:1445–9; doi:10.3899/rheum.111517)
Key Indexing Terms:
GOUT SPINE TOPHI EROSIONS COMPUTERIZED TOMOGRAPHY BACK PAIN
From the Division of Rheumatology, Department of Medicine, and
Department of Radiology, Washington Hospital Center, Washington, DC;
and Department of Biostatistics and Epidemiology, MedStar Health
Research Institute, Hyattsville, Maryland, USA.
Supported in part by a research grant from Savient Pharmaceuticals, Inc.
and by a Fellowship Training Award from the Research and Education
Foundation, American College of Rheumatology.
R.M. Konatalapalli, MD, Former Fellow; E. Lumezanu, MD, Fellow,
Division of Rheumatology; J.S. Jelinek, MD, FACR, Chair, Department of
Radiology, Washington Hospital Center; M.D. Murphey, MD, FACR,
Physician-in-Chief, American Institute for Radiologic Pathology, Silver
Spring, Maryland, and Professor of Radiology, Uniformed Services
University of the Health Sciences, Bethesda, Maryland; H. Wang, MD,
MS, Statistician, Department of Biostatistics and Epidemiology, MedStar
Health Research Institute, the Georgetown and Howard Universities
Center for Clinical and Translational Sciences, Georgetown; A. Weinstein,
MD, FACP, FRCP, MACR, Professor of Medicine, Georgetown University
Medical Center; Chief, Division of Rheumatology, Washington Hospital
Center.
Address correspondence to Dr. A. Weinstein, Division of Rheumatology,
Suite 2A-66, Washington Hospital Center, 110 Irving Street, NW,
Washington, DC 20010, USA. E-mail: [email protected]
Accepted for publication February 12, 2012.
Axial gout is recognized as a known feature of chronicgout1. With the increasing prevalence of hyperuricemia andgout, it is likely that axial gout would be recognized morefrequently2. Although literature reviews have describedmany cases3,4, its prevalence and clinical correlations remainuncertain, as no large, prospective studies have been pub-lished. In an earlier analysis of patients with gout who had
spinal computerized tomography (CT) available for evalua-tion, the prevalence of axial gout was 14%1. However,because of its retrospective design, we were not able toderive definitive data on the possible association of axialgout with important clinical and laboratory features includ-ing duration of peripheral gouty arthritis; serum urate levels;and presence of clinical or radiological tophi, symptomaticback pain, and comorbidities such as hypertension (HTN),diabetes mellitus (DM), and chronic renal insufficiency.
This cross-sectional study was undertaken to obtain amore accurate estimation of the prevalence of axial gout andto explore its clinical, laboratory, and radiologic correlates.
Similarly to our prior study, CT was utilized as the imag-ing modality to identify axial gout5. CT reveals characteris-tic changes of axial gout: intraarticular and juxtaarticularerosions with sclerotic margins and an attenuation or densi-ty greater than the surrounding muscle due to deposition ofsodium urate crystals. Multiple anatomic sites within thevertebral column can be involved, including the epiduralspace, intradural space, ligamentum flavum, discovertebraljunction, the pedicles, facet joints, spinous processes, filumterminale, and neural foramina5. Other reports have shownbiopsy-proven urate crystals in the spine in the presence ofcharacteristic imaging appearance6. Therefore for this study,in the presence of typical CT findings of axial gout inpatients with proven clinical gout, biopsy was not obtained
of RheumatologyThe Journal on January 3, 2014 - Published by www.jrheum.orgDownloaded from
1445Konatalapalli, et al: Axial gout
Personal non-commercial use only. The Journal of Rheumatology Copyright © 2012. All rights reserved.
Correlates of Axial Gout: A Cross-sectional Study RUKMINI M. KONATALAPALLI, ELENA LUMEZANU, JAMES S. JELINEK, MARK D. MURPHEY, HONG WANG,and ARTHUR WEINSTEIN
ABSTRACT. Objective. A cross-sectional study was undertaken to determine the prevalence of axial gout inpatients with established gouty arthritis and to analyze clinical, laboratory, and radiological correlations.Methods. Forty-eight subjects with a history of gouty arthritis (American College of Rheumatologycriteria) for ≥ 3 years under poor control were included. Subjects underwent history, physical exam-ination, laboratory testing, and imaging studies, including radiographs of the hands and feet andcomputerized tomography (CT) of the cervical and lumbar spines and sacroiliac joints (SIJ). Patientswith characteristic erosions and/or tophi in the spine or SIJ were considered to have axial or spinalgout.Results. Seventeen patients (35%) had CT evidence of spinal erosions and/or tophi, with tophi iden-tified in 7 of the 48 subjects (15%). The spinal location of axial gout was cervical in 7 patients(15%), lumbar in 16 (94%), SIJ in 1 (6%), and more than 1 location in 14 (82%). Duration of gout,presence of back pain, and serum uric acid levels did not correlate with axial gout. Extremity radio -graphs characteristic of gouty arthropathy found in 21 patients (45%) were strongly correlated withCT evidence of axial gout (p < 0.001). All patients with tophi in the spine had abnormal hand or feetradiographs (p = 0.005).Conclusion.Axial gout may be a common feature of chronic gouty arthritis. The lack of correlationwith back pain, the infrequent use of CT imaging in patients with back pain, and the lack of recog-nition of the problem of spinal involvement in gouty arthritis suggest that this diagnosis is oftenmissed. (First Release April 15 2012; J Rheumatol 2012;39:1445–9; doi:10.3899/rheum.111517)
Key Indexing Terms:
GOUT SPINE TOPHI EROSIONS COMPUTERIZED TOMOGRAPHY BACK PAIN
From the Division of Rheumatology, Department of Medicine, and
Department of Radiology, Washington Hospital Center, Washington, DC;
and Department of Biostatistics and Epidemiology, MedStar Health
Research Institute, Hyattsville, Maryland, USA.
Supported in part by a research grant from Savient Pharmaceuticals, Inc.
and by a Fellowship Training Award from the Research and Education
Foundation, American College of Rheumatology.
R.M. Konatalapalli, MD, Former Fellow; E. Lumezanu, MD, Fellow,
Division of Rheumatology; J.S. Jelinek, MD, FACR, Chair, Department of
Radiology, Washington Hospital Center; M.D. Murphey, MD, FACR,
Physician-in-Chief, American Institute for Radiologic Pathology, Silver
Spring, Maryland, and Professor of Radiology, Uniformed Services
University of the Health Sciences, Bethesda, Maryland; H. Wang, MD,
MS, Statistician, Department of Biostatistics and Epidemiology, MedStar
Health Research Institute, the Georgetown and Howard Universities
Center for Clinical and Translational Sciences, Georgetown; A. Weinstein,
MD, FACP, FRCP, MACR, Professor of Medicine, Georgetown University
Medical Center; Chief, Division of Rheumatology, Washington Hospital
Center.
Address correspondence to Dr. A. Weinstein, Division of Rheumatology,
Suite 2A-66, Washington Hospital Center, 110 Irving Street, NW,
Washington, DC 20010, USA. E-mail: [email protected]
Accepted for publication February 12, 2012.
Axial gout is recognized as a known feature of chronicgout1. With the increasing prevalence of hyperuricemia andgout, it is likely that axial gout would be recognized morefrequently2. Although literature reviews have describedmany cases3,4, its prevalence and clinical correlations remainuncertain, as no large, prospective studies have been pub-lished. In an earlier analysis of patients with gout who had
spinal computerized tomography (CT) available for evalua-tion, the prevalence of axial gout was 14%1. However,because of its retrospective design, we were not able toderive definitive data on the possible association of axialgout with important clinical and laboratory features includ-ing duration of peripheral gouty arthritis; serum urate levels;and presence of clinical or radiological tophi, symptomaticback pain, and comorbidities such as hypertension (HTN),diabetes mellitus (DM), and chronic renal insufficiency.
This cross-sectional study was undertaken to obtain amore accurate estimation of the prevalence of axial gout andto explore its clinical, laboratory, and radiologic correlates.
Similarly to our prior study, CT was utilized as the imag-ing modality to identify axial gout5. CT reveals characteris-tic changes of axial gout: intraarticular and juxtaarticularerosions with sclerotic margins and an attenuation or densi-ty greater than the surrounding muscle due to deposition ofsodium urate crystals. Multiple anatomic sites within thevertebral column can be involved, including the epiduralspace, intradural space, ligamentum flavum, discovertebraljunction, the pedicles, facet joints, spinous processes, filumterminale, and neural foramina5. Other reports have shownbiopsy-proven urate crystals in the spine in the presence ofcharacteristic imaging appearance6. Therefore for this study,in the presence of typical CT findings of axial gout inpatients with proven clinical gout, biopsy was not obtained
of RheumatologyThe Journal on January 3, 2014 - Published by www.jrheum.orgDownloaded from
48 paQents, gout > 3y; lumbar & cervical CT-‐scan; hands and feet radiographs

Oxalate de calcium et rachis
Oxalose primitive Condensation osseuse Fragilité osseuse, tassements vertébraux

Spinal Crystal diseases
§ Urate monosodium : Gout § Calcium crystals
– Calcium phosphate « Apatite disease » – Calcium pyrophosphates « CPPD disease » – Calcium oxalate

Intervertebral disc apatite (phosphocalcic bruschite) deposits
« ApaQte rheumaQsm » § Hydroxyapatite deposition disease § Children intervertebral disc calcification § Intradiscal steroid injections § Disc ankylosis (Forestier, SPA, spine
arthrodeses…) § Chronic hemodialysis for renal failure § Ochronosis

« ApaQte rheumaQsm »
Amor et al Rev Rhum 1977 : 45 paQents § Acute back pain: 33% § CalcificaQons : 53%

Spine apaQte deposits and clinical findings
§ Acute back pain and sometimes fever § Tensor longus capitae tendinitis § Crowned dens syndrome § Calcifyed herniated discs ü Thoracic spine : spinal cord
compression ü Lumbar spine : inflammatory painful
nerve root pain

Rev Rhum 1982; 49: 549-‐551

§ 4 paQentes avec cervicalgie haute aiguë § 2 femmes âgées de 59 et 63 ans, porteuses de mulQples calcificaQons péri-‐arQculaires évocatrices de rhumaQsme apaQQque
§ 2 femmes âgées de 69 de 75 ans, porteuses d’une CCA typique
§ Dépôts calciques péri-‐odontoïdiens § Bonne réponse aux AINS
Ziza et al, Rev Rhum 1982; 49: 549-‐551

Crowned dens syndrome
§ Occipital pain § + Arnold pain, ear pain, mandibular or temporo-‐mandibular pain
§ Abrupt onset, intense pain § SomeQmes subacute or even chronic pain § Fever, increased CRP/blood sedimentaQon rate
§ Cervical moQon limitaQon

WU et al ArthriOs Care Res 2005; 53: 133-‐7

Mai 1981 Septembre 1981

§ W 69y § Past history : shoulder calcific tendiniQs § Acute cervical and ear pain § Impossibility to turn the head on the len § Free other cervical moQon
§ Bone scinQgraphy increased uptake § Increased sedimenQon rate § Radiographs: calcific deposits around the dens
§ Complete recovery within 4 days with diclofenac (200mg/j)

Crowned dens syndrome

Crown dens syndrome due to apaQte deposits
El Mahou et al Presse Méd 2006; 35:803-‐4

Tensor longus capitae tendinitis

Intervertebral disc apaQte deposits


ApaQte disc space inflammaQon mimicking infecQon
*
*
*
*

Intervertebral disc apaQte deposits
• Intraspinal migraQon of dense calcificaQons of the nucleus pulposus (arrows) through a rupture of the annulus fibrosus (black arrow).
• Interspinous dense and round calcificaQon (arrowhead).

• Intraspinal migraQon of disc calcificaQon. • Note the less dense calcificaQon in L1-‐L2 compared to T12-‐L1, probably due to parQal migraQon of the
calcificaQon.
Intervertebral disc apaQte deposits migraQon

ArthriOs Rheum 1985; 28: 1417-‐1420

Syndrome de la dent couronnée § DiagnosQc = imagerie
§ Cliché bouche ouverte de la charnière cervico-‐occipitale de face
§ ScinQgraphie osseuse
§ Scanner : opacités entourant le sommet et les côtés de l’odontoïde en couronne ou halo

Dépôts coccygeal deposits
RicheSe P, Maigne JY, Bardin T. Spine 2008

Spinal Crystal diseases
§ Urate monosodium : Gout § Calcium crystals
– Calcium phosphate « Apatite disease » – Calcium PyroPhosphates « CPPD disease » – Calcium oxalate

Intervertebral disc CPPD : Frequency in the general populaQon
§ Autopsic studies (Pritzker.Orthop Clin North Am 1977;8:65-‐77, Feinberg Clin Orthop1990;254:303-‐10)
ü 6 à 20 % ü Increases with age
§ Discectomy samples (Andres Arch Pathol Lab Med 1980;104:269-‐71; Lagefoged Ann Rheum Dis 1986 Ann Rheum Dis 1986;45:239-‐43; Markiewitz Spine;21:506-‐11)
ü 10-‐26 % ü AsymptomaQc

Intervertebral disc CPPD: Radiologic appearance
§ Lines or minispots, someQmes aggregates § Annulus fibrosis > nucleus pulposus : verQcal lines § CarQlage endplate : horizontal lines parallel to the endplate


Resnick & Niwayama
CPPD Intervertebral disc



CPPD: Disc deposits


Resnik & Niwayama
Facet joints and posterior ligaments CPPD deposits

Facet joint Ligamentum flava
CPPD

Resnik & Niwayama

CPPD Transverse ligament
§ Frequent at CT-‐scan: • ConstanQn et al: 14/21 (Ann
Rheum Dis 1996; 55: 137-‐9) • Finkh et al : 24/35 vs 4/11
chez les contrôles (J Rheumatol 2004;31:544-‐51)
§ Usually asymptomaQc
Kakitsubata. Radiology 2000; 216: 213-‐219

CPPD Transverse ligament calcificaQon

CPPD Crowned dens syndrome
Acute cervical and occipital pain, fever, loss of motion (rotations +++) Traitement:
pain killers oral steroids immobilisation C1-C2 lateral joint steroid injection (Frey et al PM&R 2009;1:379-82)

CPPD vs apaQte deposits around the dens Differences in distribuQon and appearance
Round and dense calcificaQons bone erosions
Concentric, linear calcificaQons «crowned dens »
CPPD ApaQteE
Periodontoid deposits

CPPD Frequency of atlanto-axial deposits at CT-scan
Radiology: Volume 269: Number 2—November 2013 n radiology.rsna.org 523
MUSCULOSKELETAL IMAGING: Frequency of Atlantoaxial Calcium Pyrophosphate Dihydrate Deposition Chang et al
This is highlighted by the fact that we had many more men (354 patients) than women (159 patients) and that there were disproportionately higher numbers of men aged 20–30 years and elderly women. However, ethical concerns with the delivery of ionizing radiation pre-clude the evaluation of consecutive pa-tients in the general population. In addi-tion, although CT is generally regarded as sensitive for the detection of small calcifications, it is certainly less sensitive than histologic examination (17), which may result in underestimation of the true prevalence. Furthermore, not all CT-evident calcifications relate to CPPD crystal deposition at histologic examina-tion, although histologic analysis is gen-erally not performed in the clinical set-ting and characteristic calcifications are generally assumed to be due to CPPD crystal deposition (22,28). With regard to retro-odontoid soft-tissue thickness, we did not evaluate any potential causes other than CPPD crystal deposition that could be diagnosed at imaging, such as osteoarthrosis or an inflammatory ar-thropathy. Another limitation of this
There are several limitations to our study. Our sample included patients with acute trauma and is not necessarily representative of the general population.
CPPD crystal deposition should alert the interpreting radiologist to pay par-ticular attention to the retro-odontoid soft-tissue thickness.
Figure 4
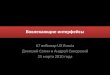
Figure 4: Bar chart shows prevalence of atlantoaxial CPPD deposition ac-cording to age group. Prevalence increases with advancing age for both male (blue) and female (red) patients (P , .0001, logistic regression coefficient).
Figure 5
Figure 5: Scatter plot of age versus retro-odontoid soft-tissue thickness in (a) male (blue) and female (red) patients and (b) patients without CPPD crystal depo-sition (blue) and those with CPPD crystal deposition (red). There is significant positive correlation (r = 0.48, P , .0001) between age and retro-odontoid soft-tissue thickness in entire population.
Chang et al. Radiology 2013; 269:519-24
522 radiology.rsna.org n Radiology: Volume 269: Number 2—November 2013
MUSCULOSKELETAL IMAGING: Frequency of Atlantoaxial Calcium Pyrophosphate Dihydrate Deposition Chang et al
CPPD crystal deposition = 0.0067, P = .004, multiple R2 = 0.35). There was no significant difference between the retro-odontoid soft-tissue thickness in men ver-sus that in women (mean, 2.4 mm vs 2.3 mm, respectively; P = .2574, t test). The mean retro-odontoid soft-tissue thickness in patients with CPPD crystal deposition was greater than that in patients without CPPD crystal deposition (3.4 mm vs 2.2 mm, respectively; P , .0001; Fig 5b).
Discussion
In this study, we demonstrated that atlantoaxial CPPD crystal deposition is more common than previously rec-ognized. In fact, nearly half of our patients aged 80 years and older had atlantoaxial CPPD crystal deposition at CT. We have confirmed that there is an increasing prevalence of such deposi-tion with advancing age (4–7,24,25). In addition, the presence of CPPD crystal deposition was associated with thicker retro-odontoid soft tissues.
The true prevalence of CPPD crystal deposition is unknown. Previous stud-ies have primarily used conventional radiography as a diagnostic tool and have found CPPD crystal deposition to be highest in the peripheral articula-tions, particularly the knee, with rates reported to be as high as 8.1% in those older than 63 years (1425 patients) (7), 17.5% in those aged 80–84 years (1727 patients) (4), and 44% in those older than 84 years (100 patients) (24).
To date, there have been relatively few reports of CPPD crystal deposi-tion in the cervical spine, in part be-cause clinical radiography is much less
Figure 3
Figure 3: Bar charts show age distribution of (a) male and (b) female patients. There were 354 male patients and 159 female patients (P , .0001, x2 test). Of note, female patients were disproportionately older than male patients (mean age, 62 years vs 48 years, respectively; P , .0001, t test).
Summary of Demographic Characteristics
Age (y) No. of Male Patients No. of Female Patients No. of Patients with Calcification*
,20 (n = 14) 10 4 0 (0)20–29 (n = 85) 68 17 0 (0)30–39 (n = 62) 45 17 0 (0)40–49 (n = 83) 65 18 2 (2.4)50–59 (n = 99) 83 16 4 (4.0)60–69 (n = 42) 31 11 4 (9.5)70–79 (n = 53) 28 25 17 (32)80–89 (n = 54) 19 35 21 (39)90–99 (n = 21) 5 16 16 (76)
* Numbers in parentheses are percentages.
sensitive to soft-tissue calcifications re-lated to the superimposition of adjacent structures (17). To our knowledge, the only study to date in which CT was used to determine the prevalence of CPPD crystal deposition in the cervical spine was performed in 1995 by Zapletal et al (25), who evaluated 700 consecutive patients undergoing CT of the brain or paranasal sinuses and found a preva-lence of 8.8% in those aged 60 years and older and an overall prevalence of 5.7%. The prevalence data in our study were much higher than those obtained by Zapletal et al (25): We found a prev-alence of 34% in patients aged 60 years and older and an overall prevalence of 12.5%. This is likely related to the increased sensitivity of current-gener-ation CT scanners, which use thinner collimation than the scanners used by Zapletal et al (5.0-mm collimation).
The importance of noting the high prevalence of incidental atlantoaxial CPPD crystal deposition is demonstrated
in the diagnosis of crowned dens syndrome, which is seen in patients who present with severe neck pain due to calcium deposits about the odontoid process (22). As expected, a major di-agnostic criterion is the finding of peri-odontoid calcific deposits. Our study demonstrated that this finding is very common and often incidental, highlight-ing the importance of using other cri-teria such as fever or positive biologic inflammatory markers to make the di-agnosis (10), particularly in the elderly.
We have demonstrated that atlan-toaxial CPPD crystal deposition is asso-ciated with greater retro-odontoid soft-tissue thickness in older subjects, even after separately adjusting for age. This finding supports the few case reports in the literature of CPPD crystal de-posits causing enlarged retro-odontoid masses (15,16), although other causes have also been demonstrated, including osteoarthrosis and rheumatoid arthritis (25–27). The presence of atlantoaxial
513 consecutive patients CT-scan for trauma Overall prevalence :12,5 % Increase with age

Calcium pyrophosphate deposits (CPPD) involving the spine
§ Intervertebral discs, facet joints, ligaments § Cervical and lumbar spine § Clinical findings
– Asymptomatic – Acute pain and fever – Subacute pain – Disc inflammation mimicking infection – Nerve compression

Acute arthriQs
F 70. T12 fracture aner a fall. Inflammatory low back pain





Rachis cervical haut et dépôts de CPP
§ Dépôts péri-‐odontoïdiens
Syndrome de la dent couronnée Arthrites aiguës C1-‐C2 latérales Érosions de l’odontoïde; fractures de type 2 Compressions bulbo-‐médullaires (foramen magnum)
§ Arthropathies C1-‐C2 latérales

CPPD Erosive changes

CPP atlanto-axial deposits erosions of the dens

CPP atlanto-axial deposits Fractures of the dens
Kakitsubata. Radiology 2000;216:213-9 : 9 cas de fractures de l’odontoïde (type 2)
14). Destruct ive an d h ypertroph ic ar-th ropath y of th e cervical sp in e with asso-ciated ossific fragm en tation also h as beenreported (15). In our study, CT scan n in gsh owed osseous abn orm alit ies of th eodon toid process, such as subch on dralcysts or erosion s, in all cases. Amon g th ebon e ch an ges, subch on dral cyst form a-tion was especially prom in en t. Th is fea-ture is in terestin g, because con spicuoussubch on dral cyst form ation in th e periph -eral join ts is typical of CPPD crystal depo-sit ion even wh en calcification is n ot pres-en t (10).Massive CPPD crystal deposits with
bon e erosion in volvin g th e cervical verte-brae h ave been reported previously (16–18). In our six cases with a soft-t issue
m ass, th e odon toid process also was m ark-ed ly eroded . In th ese cases, a ret ro-odon toid m ass con tain in g CPPD crystalsm ay h ave resu lted in erosion or destruc-t ion of th e odon toid process. Bon e ero-sion h as n ot been reported as a dom in an tfeature of CPPD crystal deposit ion diseasein th e periph eral join ts an d is gen erallycon sidered a fin din g th at suggests analtern ative diagn osis (eg, rh eum atoid ar-th rit is) (14,19). Our study fin din gs, h ow-ever, suggest th at CPPD crystal deposi-t ion in th e tran sverse ligam en t can beassociated with erosion of th e odon toidprocess.To our kn owledge, a relat ion sh ip be-
tween th e CPPD deposition in an d aroun dth e C1-C2 articu lation an d odon toid frac-
ture h as n ot been reported previously.Radiograph s of oth er art icu lation s weren ot available for review, wh ich wouldh ave allowed assessm en t of wh eth er th eCPPD crystal deposit ion was prim aryrath er th an secon dary in relation to th eodon toid fracture. In our series of pa-t ien ts, a type 2 odon toid fracture wasseen in patien ts with h istories of m ajortraum a (n ! 2), m in or traum a (n ! 3), orn o traum a at all (n ! 4). We recogn izeth at CPPD crystal deposit ion m ay occuras a complication of traum a (20) butbelieve th at CPPD crystal deposit ion sec-on dary to in jury is un likely because CPPDcrystals were eviden t with in 1 week of th etraum atic episode in our patien ts. Al-th ough th e exact relation sh ip of th e odon -
a. b. c.
d. e. f.
Figure 4. Im ages obtain ed in a 56-year-old m an with CPPD crystal deposit ion disease, traum atic type 2 odon toid fracture, an d retro-odon toid m ass.(a) Tran sverse CT scan sh ows calcification s (straigh t arrow) aroun d th e odon toid process. Atlan toaxial join t space n arrowin g an d destructive ch an gesin volvin g th e atlas (curved arrow) are observed. (b) CT scan reform atted in th e sagit tal p lan e dem on strates periodon toid calcification (sh ort straigh tarrow), cystic ch an ges in th e den s (curved arrow), an d a type 2 odon toid fracture (lon g straigh t arrow). (c) Sagit tal T1-weigh ted SEMR im age (705/15)sh ows a retro-odon toid m ass (arrow) compressin g th e cervical sp in al cord. Th e sign al in ten sity of th e retro-odon toid m ass is low compared with th atof th e spin al cord an d bon e m arrow. (d) On th e T2-weigh ted fast SE MR im age (4,282/94), th e sign al in ten sity of th e retro-odon toid m ass (arrow) islow compared with th at of th e spin al cord an d bon e m arrow. (e) Ph otom icrograph sh ows a large crystal deposit (lon g arrows) as pale n odules withh yalin ization bordered by in flammatory cells (sh ort arrow). (Hem atoxylin -eosin stain ; origin al m agn ification , "16.) (f) Ph otom icrograph obtain edby usin g a polarizin g len s dem on strates crystal deposits (arrow) in th e lesion . (Hem atoxylin -eosin stain ; origin al m agn ification , "40.)
Volume 216 • Number 1 Calcium Pyrophosphate Dihydrate Crystal Deposit ion in the At lantoaxial Joint • 217

CPPD Atlanto-axial lateral joint acute arthritis
Tobyashi et al. The Spine Journal 2014 § 27 paQents, 56 to 90y (mean 76) § Acute (VAS>7) upper cervical pain for 2-‐3 days § Head rotaQon < 20° § Increased CRP
§ Radiographs: normal or mild erosive changes § CT-‐Scan: Transverse ligament calcificaQon: 81 %,
§ PoncQon C1-‐C2 latéral joint aspiraQon: 5,000-‐14,000 WBC/mm3
PPC crystals : 10 pts Pain improvement with aspiraQon: VAS decreasing from 82 to 35,5 within 30 mn
��������� ������
����� ������� ���������������������������������� �����������
��������������������������� �������������������������� �����!���� ����������"�����������������#���� ����$�����%�����������#������&��'�����������
�$$( &)*+,�,-./0).1/)2+-�*
�3$( )/4)/)56�4��� ��4+/).4)/4/*-
7����� ��( &�$ ""�**5*8
����������� ( The Spine Journal
7����9�����( +/� �9�'����+/)+
7�9�������( ++�3������+/).
����������( +,�3������+/).
������������������������(������������������������ ���� �� ������"��$�����%��#��&��'���#������ ������� ���������������������������������� ����������� ��The Spine Journal�0+/).1����(�)/4)/)56�4��� ��4+/).4)/4/*-4
������������:���������� �� ����'� ����������������� ��������������������� 4���������9�������������'����%���������9�� ;�����������9����� �������'� ������4�����'� �������%����� ��;�������� ;�������� ;��� ���9��%������������� ;����������������������������� ������ ������'4������� ��������� ;����������� ����������������'����������9����%��������������������� � ��� ������;���������'���������������������� �������� 4
MANUSCRIPT
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED MANUSCRIPT

Pseudotumoral interspinous CPP deposit and acute upper cervical pain
GEORGE LINDBECK • EXTRA-ARTICULAR CPPD 583
FIGURE 1. Cervical spine radiograph shows calcified mass between C1 and C2.
processes of C2 and C3 after C2 and C3 laminectomies. The final pathologic diagnosis was tumoral calcium pyrophosphate deposi- tion disease. Blood cultures drawn at the time of the first and second ED visits resulted in no growth; aerobic and anaerobic bacterial cultures of the cerebrospinal fluid were sterile, and viral cultures and fungal antigen assays, stains, and cultures of the cerebrospinal fluid resulted in no isolation of organisms. Gram's stains, bacterial cultures, and pathologic examination of the excised tumor mass also failed to reveal infectious organisms. The patient's postoperative course was uneventful, he developed no neurological symptoms at any time, and his fevers resolved after resection of the m a s s .
DISCUSSION Although neck pain is a relatively common complaint
seen in the ED, primary lesions of the cervical spine are unusual. The differential diagnosis of neck pain is broad and includes traumatic, infectious, malignant, and rheumato- logic etiologies. In this patient, the lack of a history of trauma and the presence of fever raised the initial concern of a deep space infection of the neck or a parameningeal focus. The question of a cervical spine tumor was suggested by abnormalities first visualized on the routine soft tissue views of the neck; after further delineation of the lesion through CT and MRI scanning, the patient was taken to the operating room with the preoperative diagnosis of primary tumor of the cervical spine. Primary tumors of the cervical spine are not common lesions; a recent series of 38 cases assembled over 34 years at a European referral center documented 23 malignant lesions, and 15 benign. 1 As with many reports of extra-articular calcium pyrophosphate deposition disease, the diagnosis in this case was not established until patho- logic examination of tissue.
Calcium pyrophosphate dihydrate deposition (CPPD) disease is characterized by the deposition of calcium pyro- phosphate crystals in tissue, most commonly articular carti- lage. Chondrocalcinosis (CC), manifest by deposition of calcium pyrophosphate crystals in hyaline and fibrocartilage and in the synovial space, is the most common form of CPPD and has been estimated to occur in 5% to 10% of the adult population? The prevalence of CPPD increases with age to as high as 30% in those older than 75 years of age, and there is probably a female preponderance with an estimated relative risk of 1.33. 2 CPPD has been noted to occur as a sporadic or idiopathic disease, related to underlying diseases that affect calcium and phosphate metabolism such as hyperthyroidism, hemochromatosis, hypomagnesemia, and in a familial pattern. 3
The mechanism of calcium pyrophosphate crystal deposi- tion is not well understood, and theories have generally focused on abnormalities of the cartilage matrix, including mechanical damage, that promote crystal deposition, or biochemical abnormalities that lead to elevated serum and synovial fluid levels of calcium or inorganic pyrophos- phate. 3 Pyrophosphate is a product of many enzymatic reactions, and conditions causing elevations in calcium (eg, hyperparathyroidism) or pyrophosphate (eg, hypophosphata- sia) concentrations could increase the ionic product and thus promote crystal formation and deposition. Crystal formation and deposition are promoted by the environment in which crystal formation occurs, and "gels" such as cartilage are recognized as such a medium. Changes in normal cartilage from trauma, disease, and metabolic disorder may enhance
FIGURE 2. CT shows expansile lesion with a bony matrix involving spinous processes of C2 with small amount of extension into spinal canal.
GEORGE LINDBECK • EXTRA-ARTICULAR CPPD 583
FIGURE 1. Cervical spine radiograph shows calcified mass between C1 and C2.
processes of C2 and C3 after C2 and C3 laminectomies. The final pathologic diagnosis was tumoral calcium pyrophosphate deposi- tion disease. Blood cultures drawn at the time of the first and second ED visits resulted in no growth; aerobic and anaerobic bacterial cultures of the cerebrospinal fluid were sterile, and viral cultures and fungal antigen assays, stains, and cultures of the cerebrospinal fluid resulted in no isolation of organisms. Gram's stains, bacterial cultures, and pathologic examination of the excised tumor mass also failed to reveal infectious organisms. The patient's postoperative course was uneventful, he developed no neurological symptoms at any time, and his fevers resolved after resection of the m a s s .
DISCUSSION Although neck pain is a relatively common complaint
seen in the ED, primary lesions of the cervical spine are unusual. The differential diagnosis of neck pain is broad and includes traumatic, infectious, malignant, and rheumato- logic etiologies. In this patient, the lack of a history of trauma and the presence of fever raised the initial concern of a deep space infection of the neck or a parameningeal focus. The question of a cervical spine tumor was suggested by abnormalities first visualized on the routine soft tissue views of the neck; after further delineation of the lesion through CT and MRI scanning, the patient was taken to the operating room with the preoperative diagnosis of primary tumor of the cervical spine. Primary tumors of the cervical spine are not common lesions; a recent series of 38 cases assembled over 34 years at a European referral center documented 23 malignant lesions, and 15 benign. 1 As with many reports of extra-articular calcium pyrophosphate deposition disease, the diagnosis in this case was not established until patho- logic examination of tissue.
Calcium pyrophosphate dihydrate deposition (CPPD) disease is characterized by the deposition of calcium pyro- phosphate crystals in tissue, most commonly articular carti- lage. Chondrocalcinosis (CC), manifest by deposition of calcium pyrophosphate crystals in hyaline and fibrocartilage and in the synovial space, is the most common form of CPPD and has been estimated to occur in 5% to 10% of the adult population? The prevalence of CPPD increases with age to as high as 30% in those older than 75 years of age, and there is probably a female preponderance with an estimated relative risk of 1.33. 2 CPPD has been noted to occur as a sporadic or idiopathic disease, related to underlying diseases that affect calcium and phosphate metabolism such as hyperthyroidism, hemochromatosis, hypomagnesemia, and in a familial pattern. 3
The mechanism of calcium pyrophosphate crystal deposi- tion is not well understood, and theories have generally focused on abnormalities of the cartilage matrix, including mechanical damage, that promote crystal deposition, or biochemical abnormalities that lead to elevated serum and synovial fluid levels of calcium or inorganic pyrophos- phate. 3 Pyrophosphate is a product of many enzymatic reactions, and conditions causing elevations in calcium (eg, hyperparathyroidism) or pyrophosphate (eg, hypophosphata- sia) concentrations could increase the ionic product and thus promote crystal formation and deposition. Crystal formation and deposition are promoted by the environment in which crystal formation occurs, and "gels" such as cartilage are recognized as such a medium. Changes in normal cartilage from trauma, disease, and metabolic disorder may enhance
FIGURE 2. CT shows expansile lesion with a bony matrix involving spinous processes of C2 with small amount of extension into spinal canal.
G Lindbeck AM J Emergency Med 1996;14:582-‐5
H de 43 ans, cervicalgie aiguë, opéré pour suspicion de tumeur: anapath dépôts de CPP

Dépôts cervico-occipitauxde PPi de Ca Arthropathies C1-C2 latérales
Gerster. Osteoarthritis Cartilage 1994;2:275-9

• Consequence of: • Facet joint damage, with secondary
spondylolisthesis • Erosive disc disease • Spinal ankylosis
CPPD DestrucQve arthropathy

Atlanto-axial CPP deposits causing spinal cord compression
Assaker. Spine, 2001;26:1396-1400

Spinal canal ligaments CPP deposits and cervical spinal cord compression
lagen fibers and cellular debris; a few were locatedwithin elastic fibers. The ultrastructural studies werehampered by the poor preservation of the specimens.
DISCUSSION
CLF at the cervical spine is exceedingly rare: only 107cases have been reported in the English-language litera-ture [6, 7], of which 104 were in Japanese patients. Asingle case has been reported in a Black patient [2] andtwo in Caucasians [8, 9]. Nevertheless, we identified sixcases in a Caribbean island with a population of400,000, suggesting a prevalence close to that reportedin an orthopedics center in Japan [10] and raising thepossibility that this condition has until now been under-
recognized in Blacks. In keeping with our findings,earlier publications show a predominance in women(91 women/16 men). Mean age at diagnosis was 65.3months (range, 30–89 years). The most common pre-sentation was subacute myelopathy due to spinal cordcompression by the calcifications in the absence ofprecipitating factors. Symptoms developed within 6.6months in our study versus 10.5 months in the study byImaï and Hukuda [7]. The most prominent presentingsymptoms (figure 5) were subjective disorders of sensa-tion in the upper limbs, clumsiness, and difficulty walk-ing, a triad that suggests cervical myelopathy. Urinarysphincter dysfunction was present in some cases. Neckpain and/or nerve root pain with low-grade fever hasbeen reported and ascribed to a flare of inflammation atthe calcified sites [7]. Objective neurological abnor-malities included motor loss, sensory loss, and pyrami-dal tract findings predominating at the upper limbs(figure 5). Examination of the spine was normal in mostcases, and radiculopathy was found in a minority ofpatients (one in our series and 20% in the literature [6,7]. A striking finding in our series is that severe motorloss was present in all five symptomatic patients. Fur-thermore, one patient had severe posterior cord syn-drome, which has rarely been reported, although thecalcifications lie on the posterior cords. Laboratory testshave been of little assistance: some patients had evi-dence of inflammation [7], one had a moderate increasein serum phosphate [11], and two had an increase inserum parathyroid hormone levels [12].
Although plain radiographs of the cervical spine pro-vided the diagnosis in some cases [3, 13-15], they wereunrewarding in others. CT is the key diagnostic inves-tigation. The calcifications are seen as high-attenuation,oval, space-occupying lesions on either side of the mid-line of the neural arch, in the interval between thelaminas of two adjacent vertebras. They are usuallyasymmetric. They never extend to the posterior facetjoints [14], a characteristic that differentiates themfrom periarticular cervical spine calcifications [16].Their location near the midline explains why nerve rootsymptoms are uncommon. Several levels can be affected,as was the case in two of our patients; however, thecalcifications consistently arise in the lower part of thecervical spine, the two most commonly affected levelsbeing C4-C5 and C5-C6 (figure 5). Sagittal CT recon-structions were obtained in three of our patients. Webelieve this technique ensures the diagnosis with 100%specificity: the location of the lesions between the lami-nas and the acute angles between each lesion and the
Figure 3. Magnetic resonance imaging of the neck (case 5):T2-weighted sequence, sagittal section. Multilevel spinal cord com-pression from C3-C4 to C5-C6, most marked at C4-C5. The highsignal from the spinal cord indicates compression. The calcificationsare visible as low-attenuation masses between the laminas.
162 P. Cabre et al.
Pathological studies
Light microscopyHistologic examination of the operative specimens fromthe two patients who had surgery showed compactcollagen-rich tissue containing roughly polycyclicdeposits of calcium crystals but no inflammatory infil-trate. In both patients, the deposits contained calciumpyrophosphate dihydrate (CPPD) with characteristicweak birefringence. In addition, multiple clusters ofalizarin red S-positive crystals suggestive of apatite wereseen.
TEMOn the semi-fine sections stained with methylene blueand azure blue, calcium crystals were seen to formcompact clusters studding the ligamentous tissue. TEMand x-ray diffraction demonstrated electron-densedeposits composed of CPPD crystals and apatite micro-crystals (figure 4), with a mean calcium over phosphateratio of 0.96 and 1.46, respectively. In the ultrathinsections (one specimen), crystals were seen amidst col-
Figure 1. Cervical computed tomography coupled with myelogra-phy (case 1): axial section through C4-C5. Compression of the spinalcord by two masses with high attenuation values similar to that ofcalcium. The masses are at the level of the laminas. Calcification orossification of the posterior longitudinal ligament (A). Computedtomography coupledwithmyelography: sagittal reconstruction show-ing a large calcific deposit at C4-C5 forming an acute angle with thesupra- and infrajacent laminas and stopping the progression of thecontrast agent (B).
A B
Figure 2. Computed tomography of the neck (case 5): axial sectioncentered on C1-C2 showing high attenuation of the transverse liga-ment posterior to the dens, consistent with an ossification orcalcification.
Cervical ligamentum flavum calcification 161
Pathological studies
Light microscopyHistologic examination of the operative specimens fromthe two patients who had surgery showed compactcollagen-rich tissue containing roughly polycyclicdeposits of calcium crystals but no inflammatory infil-trate. In both patients, the deposits contained calciumpyrophosphate dihydrate (CPPD) with characteristicweak birefringence. In addition, multiple clusters ofalizarin red S-positive crystals suggestive of apatite wereseen.
TEMOn the semi-fine sections stained with methylene blueand azure blue, calcium crystals were seen to formcompact clusters studding the ligamentous tissue. TEMand x-ray diffraction demonstrated electron-densedeposits composed of CPPD crystals and apatite micro-crystals (figure 4), with a mean calcium over phosphateratio of 0.96 and 1.46, respectively. In the ultrathinsections (one specimen), crystals were seen amidst col-
Figure 1. Cervical computed tomography coupled with myelogra-phy (case 1): axial section through C4-C5. Compression of the spinalcord by two masses with high attenuation values similar to that ofcalcium. The masses are at the level of the laminas. Calcification orossification of the posterior longitudinal ligament (A). Computedtomography coupledwithmyelography: sagittal reconstruction show-ing a large calcific deposit at C4-C5 forming an acute angle with thesupra- and infrajacent laminas and stopping the progression of thecontrast agent (B).
A B
Figure 2. Computed tomography of the neck (case 5): axial sectioncentered on C1-C2 showing high attenuation of the transverse liga-ment posterior to the dens, consistent with an ossification orcalcification.
Cervical ligamentum flavum calcification 161
supra- and infrajacent laminas differentiate CLF fromossification of the ligamentum flavum, in which theangles are obtuse. Ossification of the ligamentum fla-vum also occurs selectively in Japanese individuals. Thelesion is seen on CT sections as a V-shaped line poisedover the laminas and joining the two articular processesof the vertebra [14]. Mature lamellar bone is seen inhistological sections [14]. The lower part of the tho-racic spine is the most common target [17], althoughthe lower cervical spine can be affected [18]. Ossifica-tion of the ligamentum flavum and CLF can occur incombination with ossification of the posterior longitu-dinal ligament, which is far more common (particularlyin Japanese individuals) and may be due to geneticfactors [19]. CT demonstrated cervical spinal stenosisin our five symptomatic patients. The combination ofCLF and cervical spinal stenosis has been reported byothers [12]; in our patients, the concomitant presence
of cervical spinal stenosis probably explains the rapidsymptom onset and severe motor loss. CT coupled tomyelography can demonstrate compression of the spi-nal cord by the calcifications [13]. MRI of the neck wasperformed in two of our patients and a few previouslyreported cases [11, 19]. This investigation proved valu-able for demonstrating posterior spinal cord compres-sion as a high-intensity signal from the cervical cordopposite the calcifications on T2-weighted sequences(our cases 2 and 5). However, MRI does not demon-strate the calcifications, as both the calcified and theuncalcified ligamentum flavum generate low-intensitysignal on T1- and T2-weighted sequences. Radiographsshould be performed to look for calcific deposits else-where in the spine (intervertebral disks, posterior long-itudinal ligament, transverse ligament) or in peripheraljoints (e.g., the knees, figure 5). The natural history ofcervical myelopathy due to CLF is not well known, as
Figure 4. Transmission electron study in case 1: apatite microcrys-tals seen as electron-dense needles. Formvar, final magnification× 30,000 (A). Electron-dense calciumpyrophosphate dihydrate crys-tals exhibiting a vesicular structure under the impact of the electrons;the microanalysis diagram is shown. Ultrathin slices, final magnifi-cation × 37,500 (B). Deposit containing both calcium pyrophosphatedihydrate crystals and apatite microcrystals. Formvar, final magnifi-cation × 48,000 (C).
A B
C
Cervical ligamentum flavum calcification 163
Cabre et al. Joint Bone Spine 2001;68: 158-‐65: 6 paQents from french anQlles, 5 fast-‐onset spinal cord compression. 2 posterior decompressve surgery. PPC et BPC in ligamentum flava

Progressive onset tetraparesia in a 90 y-‐o man
Atlanto-axial CPP deposits causing spinal cord compression

Calcium Pyrophosphate Dihydrate DeposiQon Disease Causing Thoracic Cord Compression: Case Report. Muthukumar et al. Neurosurgery. 2000; 46(1): 222

antibodies to EMA, S100, Factor 13, K-67, and collagen IV.For antigen retrieval, used with most antibodies, tissuesections were incubated in a thermoresistant chamber withReveal Decloaker (Biocare Medical, Concord CA) at 120-123°C and a pressure of 20-24 psi for 45 min. Immunohisto-chemistry was performed Dako Automated immunostainer.Hematoxylin and eosin stain (H & E) and immunohistochem-istry revealed an epithelioid mass with granular material, rarereactive chondrocytes (Fig. 3) and concentric calcificationsresembling (but not true) psammoma bodies. Lesional cells
had irregular nuclei and nucleoli. Initial stained sectionsrevealed no polarizable material. However, birefrigent rhom-boid crystals were found in sections made by one of us (H.D.)and also found in additional unstained deeper sections madeby us at URMC (Fig. 4a, b). Ki-67 labeling was seen butappeared, in part, in reactive cells. No EMA, S100, factor 13or CD68 immunostaining was seen. A final diagnosis oftophaceous pesudogout was made.
Upon further staining, the specimen (Fig. 3) appeared tobe an epithelioid mass with granular material, with rarereactive chondrocytes and concentric calcifications. Thecells themselves had irregular nuclei and nucleoli with raremitoses and scattered Ki-67 labeling. Initial stained sectionsrevealed no polarizable material. However, upon furtheranalysis of deeper sections, and in concert with another
Fig. 1 a Axial view of a T2-weighted non-contrast MRI demonstrat-ing herniation of the intervertebral disc with encroachment of the leftT10 neural foramen. b Sagittal view of a T2-weighted non-contrastMRI demonstrating herniation of the T9/10 intervertebral disc
Fig. 2 Frozen section. Yellow arrows point to three psammoma bodies;blue arrow points to leptomeningeal cells with hyalinzed blood vessels(H & E, original magnification 400×)
Fig. 3 Reactive chondrocyte (yellow arrow) seen alongside fibroblaststroma (H&E, original magnification 400×)
748 Acta Neurochir (2012) 154:747–750
antibodies to EMA, S100, Factor 13, K-67, and collagen IV.For antigen retrieval, used with most antibodies, tissuesections were incubated in a thermoresistant chamber withReveal Decloaker (Biocare Medical, Concord CA) at 120-123°C and a pressure of 20-24 psi for 45 min. Immunohisto-chemistry was performed Dako Automated immunostainer.Hematoxylin and eosin stain (H & E) and immunohistochem-istry revealed an epithelioid mass with granular material, rarereactive chondrocytes (Fig. 3) and concentric calcificationsresembling (but not true) psammoma bodies. Lesional cells
had irregular nuclei and nucleoli. Initial stained sectionsrevealed no polarizable material. However, birefrigent rhom-boid crystals were found in sections made by one of us (H.D.)and also found in additional unstained deeper sections madeby us at URMC (Fig. 4a, b). Ki-67 labeling was seen butappeared, in part, in reactive cells. No EMA, S100, factor 13or CD68 immunostaining was seen. A final diagnosis oftophaceous pesudogout was made.
Upon further staining, the specimen (Fig. 3) appeared tobe an epithelioid mass with granular material, with rarereactive chondrocytes and concentric calcifications. Thecells themselves had irregular nuclei and nucleoli with raremitoses and scattered Ki-67 labeling. Initial stained sectionsrevealed no polarizable material. However, upon furtheranalysis of deeper sections, and in concert with another
Fig. 1 a Axial view of a T2-weighted non-contrast MRI demonstrat-ing herniation of the intervertebral disc with encroachment of the leftT10 neural foramen. b Sagittal view of a T2-weighted non-contrastMRI demonstrating herniation of the T9/10 intervertebral disc
Fig. 2 Frozen section. Yellow arrows point to three psammoma bodies;blue arrow points to leptomeningeal cells with hyalinzed blood vessels(H & E, original magnification 400×)
Fig. 3 Reactive chondrocyte (yellow arrow) seen alongside fibroblaststroma (H&E, original magnification 400×)
748 Acta Neurochir (2012) 154:747–750
institution, a final diagnosis of tophaceous pesudogout wasmade.
The patient did well postoperatively and was dischargedhome 3 days later. In his postoperative visits, he describedvery minimal pain, and only with sitting or lying for longperiods of time. His pain was very well controlled with oralpain medications and anxiolytics.
Discussion
CPDD was first described by McCarty in 1962 as pseudog-out due to its similarities to gout [2, 6, 7]. Previous workwas done by Zitnan and Sitaj who described what theycalled “chondrocalcinosis polyarticularis” [2]. Abnormalpyrophosphate deposition in the joint space combines withcalcium to form dihydrate crystals on collagen fibers;
release of these crystals into the joint space results in neu-trophil and monocyte-macrophage phagocytosis and releaseof inflammatory mediators, causing joint destruction [2, 8].This becomes evident on radiological examination aschondrocalcinosis.
Calcium pyrophosphate deposition arthropathy is oftenassociated with other conditions, including hyperparathy-roidism, hemochromatosis, chronic gout, hypomagnesemiaand hypophosphatemia [3]. It may also occur on a hereditarybasis but is usually sporadic. The prevalence increases withage, with as many as 45% of those over 85 years of ageaffected in some manner [9]. The joints most commonlyaffected are the knee, shoulder, hip, elbow and metacarpo-phalangeal joints, while axial skeleton involvement is rarebut reported in the literature [1–4]. Many times, spinalcalcium pyrophosphate deposition is asymptomatic andcan be an isolated site of disease [2].
Axial calcium pyrophosphate deposition involving thespine can be lytic and create pseudospondolylistheses (i.e.,listhesis without a congenital pars defect) [3]. Some studieshave shown the incidence of symptomatic calcium pyro-phosphate deposition in the axial skeleton can be as highas 33% [9, 10]. Involvement of the ligamentum flavum oratalto-ocipital ligament can result in severe myelopathy ormimic cauda equina syndrome [3, 9, 11]. Radiologically,spinal involvement demonstrates loss of disc space height,vertebral body sclerosis, osteophyte formation and subluxation[3, 12]. Calcium pyrophosphate deposition at the craniocervicaljunction can effect the foraminal exit sites of cranial nerves,resulting in neuropathy [2, 5].
There are reports in the literature of calcium pyrophos-phate crystal deposition in the intervertebral disc itself [1, 2,4]. Previous disc surgery has been suggested as a risk factorfor the development of calcium pyrophosphate deposition[1, 2]. In one study, seven of 73 discs excised over an 18-month period revealed signs of calcium pyrophosphate de-position; all seven had previous surgery at the same or anadjacent disc space [3, 5]. Most cases appear to affect thecervical spine, while thoracic spine is the least common site[4]. Histologically, the outlines of the crystal can be visual-ized on hematoxylin and eosin stains. Under polarized light,the variable birefringent rhomboid or rod-shaped crystalscan be appreciated.
This case is unusual in that the patient presented with acommonly encountered problem (i.e., chest pain) in theoutpatient setting, which, upon further investigation, wasthe result of an uncommon etiology. Furthermore, the firstpatient’s specimen had features not associated with calciumpyrophosphate deposition (Psammoma bodies, meningealproliferation) and did not initially reveal crystals underpolarized light; further analysis demonstrated the presenceof one rhomboid crystal (Fig. 4a) and deeper sections dem-onstrated needle and rhomboid crystals (Fig. 4b).
Fig. 4 a Presence of rhomboid crystals (yellow arrow) in deepersections (H&E, original magnification 400×). b Needle and rhomboidcrystals in deeper sections under polarized light (H & E, originalmagnification 400×)
Acta Neurochir (2012) 154:747–750 749
Compression médulaire dorsale
Srinivasan Acta Neurochir 2012;154:747-‐50

CPPD and intervertebral disc destructive arthropathy § Elderly patients § Variable clinical symptoms
and signs § Cervical and lumbar spine § Multiple involvement § Mimicking disc space
infection

CPPD Chronic upper cervical pain and
Atlanto-axial lateral joint erosive arthritis

CPPD Chronic upper cervical pain and
atlanto-axial lateral joint erosive arthritis

Fig.7



81 yo woman diagnosed as vertebral infecQon

IRM T1 IRM T1 + gado IRM T2

CT-‐scan T1-‐W.MRI STIR MRI
CPPD mimicking disc space infecQon
G-‐E.T1-‐W.MRI

CPPD mimicking disc space infecQon

T1 T1+G T2 SQr CT scan

T1 T1 + Gado STIR
CPPD mimicking disc space infecQon


CPPD : microgeodes

CPPD Calcifyed facet joint cysts
Namazie. J Orthop Surg 2012;20:254-‐6

• Spondylolisthesis
CPPD

Dépôts rachidiens de CPP Lésions non-‐spécifiques
§ Discopathie dégénéraQve
§ Vide discal
§ Spondylolisthesis
§ HVA



T1 T2 SQr

CPPD and adult lumbar scoliosis
§ Scoliosis with intervertebral subluxaQon in elderly


Resnik & Niwayama

Spine involvement in crystal diseases
§ Joint and ligaments calcified deposits § Acute tendinitis § Acute arthritis (C1-2, disc space, facets, costovert. J.) § Erosive and destructive arthritis mimicking infection § Spinal cord compression § Dens fracture § Scoliosis and intervertebral subluxation § Inflammatory & erosive sacroiliitis

Erosive and destructive intervertebral disc joint
§ Infection (tuberculosis and others) § Spondyloarthritis § Crystal deposition diseases § Erosive osteoarthritis
§ Charcot joint § Amyloïdosis

Thank you

CPPD Erosive and inflammatory sacroiliac
arthriQs

Scanner T1 T1+gado T2
CPPD: sacroiliiQs

CPPD: Sacro-‐Iliac ankylosis
Scanner
IRM T1

T1
STIR
F 85. Suspicion of sepQc sacroiliiQs concomitant pyelonephriQs

Gadolinium-‐enhanced T1-‐WI



M 47, Inflammatory polyarthralgia
STIR STIR T1G T1G T1G