Embed Size (px)
DESCRIPTION
Twins pregnancy and delivery in Obstetrics
Citation preview

Multiple pregnancy
Assist.prof. Andrii Berbets

Multiple pregnancy
Multiple pregnancy involves more than one embryo (fetus) in any one gestation.
Two independent mechanisms may lead to multiple gestation:
• segmentation of a single fertile ovum (identical, monovular, or monozygotic)
• or fertilization of separate ova by different spermatozoa (fraternal or dizygotic)

BENSON & PERNOLL’SHANDBOOK OF OBSTETRICS AND GYNECOLOGY

Maternal complications
• anemia; • urinary tract infection; • preeclampsia-eclampsia, • hydramnios, • uterine inertia (overdistention);• hemorrhage (before, during, and after
delivery).

Fetal complications
• prematurity• fetal growth retardation• congenital anomalies (18% higher)• abnormal presentations• cord prolapse (5 times increased)• collision of twins• fetus-fetus tranfusion syndrome


Clinical findings
• A uterus larger than expected for the duration of pregnancy (4 cm than anticipated);
• Excessive maternal weight gain not explained by eating or edema;
• Hydramnios;• Iron deficiency anemia;• Maternal reports of increased fetal activity;

Clinical findings
• Uterus containing 3 large parts or multiple small parts;
• Simultaneous auscultation or recording of two fetal hearts varying 8 beats per min and asychronous to the maternal heart
• Ultrasound confirmation

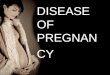
Two-vertex twins presentation

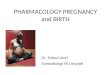
One vertex and one breech presentation

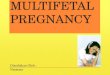
Locked twins

Feto-fetal transfusion syndrome
• This condition affects approximately 1 in 5 (20%) of all twins that share the same placental mass (monochorionic).
• This is a highly pathological condition, which if untreated will lead to fetal or newborn death in excess of 95% of cases.

Feto-fetal transfusion syndrome
• The underlying abnormality is that the placenta contains vascular connections that connect the twins, in effect, making them connected together by a continuous blood supply.

Feto-fetal transfusion syndrome
• The vascular (blood supply) connection between twins within the placenta leads to a haemodynamic (blood flow) imbalance between the twins, with one, the recipient, having a relative high perfusion of blood and the other, the donor, being under perfused with blood.

Feto-fetal transfusion syndrome

Severity classification
• Stage 1. There is a difference in the amounts of amniotic fluid surrounding the twins. The recipient often is complicated by polyhydramnios (excess amniotic fluid with a maximum pool depth of around 8cms) and the donor is complicated by oligohydramnios (reduced amniotic fluid with a maximum pool depth of around 2cms).

Severity classification
• Stage 2. In addition to the discrepancy of amniotic fluid volumes, there is a difference in size between the two babies (the recipient is often larger than the donor).

Severity classification
• Stage 3. There are haemodynamic differences between the twins. The recipient has evidence of abnormal blood flow and right-sided heart strain. The donor often demonstrates absent or reversed blood flow in the umbilical arterial (cord) circulation.
• Stage 4. One twin shows signs of severe right-sided heart failure.
• Stage 5. One of twin has already died.

Feto-fetal transfusion syndrome

TreatmentFetoscopy and placenta laser ablation

Delivery
• Cesarean section is recommended for monoamniotic twins because of the 10% delivery loss from cord entanglement.
• Other standard indications for cesarean include: any birth number exceeding twins (e.g., triplets), or if the first twin is nonvertex.
• The first twin may be delivered vaginally if it presents by the vertex.

Delivery
• A vaginal examination immediately after the first delivery is performed to identify a possible forelying or prolapsed cord

Delivery
• If 2nd fetus has continued as a vertex, a second vaginal delivery may be performed.

Delivery
If the second fetus is anything but vertex there are three alternatives.
● Bringing the head into the inlet by external guidance (version); if successful, allows labor to proceed for another vertex vaginal delivery.
● Perform cesarean section● Complete a vaginal breech delivery

Delivery
• Rupture of the second sac (if present) is accomplished as late as possible to avoid prolapse of the cord.

Thank You!