Embed Size (px)
Citation preview

Radiation Pneumonitis
大里仁愛醫院核子醫學科 林文玉醫師

Effects of Radiation Therapy on the Lung: Radiologic Appearance
§ Radiation-induced lung disease ( RILD )§ Confined to the lung tissues within radiation
port§ Acute phase: ground-glass opacity or
attenuation or consolidation § Late phase: traction bronchiectasis, volume
loss, and scarring§ Unusual distribution: newer irradiation
technique such as 3D comformal RT/oblique beam angles

60 y/o F with stage IIIb non-small cell lung cancer
Before 2 months after completion of R/T
9 months after completion of R/T

Differentiation diagnosis
Local recurrence of malignancy Infection such as bacterial pneumonia, TB
pneumonia. Radiation induced tumor Lymphangitis carcinomatosis

HRCT findings in Lymphangitic Carcinomatosis
Interlobular septal thickening, thickening of fissures and thickening of the peribronchovascular interstitium (bronchial cuffing).Depending on filling with fluid or with tumor cells, septal thickening is irregular or smooth.

Subacute hypersensitivity pneumonitisThe key findings in the subacute hypersensitivity pneumonitis are:ill-defined centrilobular nodules of ground-glass opacity (80% of cases) or mosaic pattern of a combination of patchy ground-glass opacity due to lung infiltration and patchy lucency due to bronchiolitis with air trapping

Histopathologic Features of RP
Reference point: the day of completion of RT Early RP: within 4-12 weeks after RT Radiation fibrosis develops within 6-12 months
after RT and can progress for up to 2 years before stability.
Radiation fibrosis: well-defined area of volume loss, linear scarring, consolidation, and traction bronchiectasis. consolidation usually coalesces and typically has a relatively sharp border that conforms to the treatment portals rather than anatomic boundaries.

LLL lung mass

Various Factors Influence the Degree of Lung Injury
Patient age Prior or concomitant chemotherapy:
actinomycin D, adrimycin, Bleomycin and busulfan.
Irradiation technique factors: The volume of lung irradiated: V13, V20, V30 The total dose of radiation delivered: rarely 20 Gy,
always present while doses greater than 40 Gy. The fractionation of the dose
Abrupt termination of steroid

Factors predicting radiation pneumonitis in lung cancer patientsa retrospective study
Radiotherapy and Oncology 67 (2003) 275–283
Tiziana Rancatia, Giovanni Luca Ceresolib, Giovanna Gagliardic, Stefano Schipanib, Giovanni Mauro Cattaneod,* Physics Department, University of Milano, Via Celoria 16, 20133, Milan, Italy; Radiochemotherapy Department, Scientific Institute H.S. Raffaele, Via Olgettina 60, 20132 Milan, Italy; Department of Hospital Physics, Karolinska Hospital, Stockholm, Sweden ; Medical Physics Department, Scientific Institute H.S. Raffaele, Via Olgettina 60, 20132 Milan, Italy
Purpose: To evaluate clinical and lung dose–volume histogram based factors as predictors of radiation pneumonitis (RP) in lung cancer patients (PTs) treated with thoracic irradiation

Methods and Material
1. 84 PTs with small or non-small-cell lung cancer, irradiated at > 40 Gy, with full 3D dosimetry data and a follow-up time of 6 months from start of treatment, were
analysed for RP. 2. Pneumonitis was scored on the basis of SWOG toxicity criteria and was considered a complication when grade > II. 3. The following clinical parameters were considered: gender, age, surgery,
chemotherapy agents, presence of chronic obstructive pulmonary disease (COPD), performance
status. 4. Dosimetric factors including prescribed dose (Diso), presence of final conformal
boost, mean lung dose (Dmean), % of lung receiving > 20, 25, 30, 35, 40, and 45 Gy (respectively V20 to V45), and normal tissue complication probability (NTCP) values were analysed.

The goal of radiotherapy
To deliver a sufficient dose to the tumor to provide a high probability of cure while inducing minimal damage in the surrounding normal tissues, leaving them architecturally intact and functionally competent
Establishing the NTCP Evaluation System for Radiotherapy is mandatory.

Probit model (Lyman)
n
ref
t
vTDvTD
vTDmvTDDt
VVv
dttNTCP
)1()(
))(/())((
/
)2/exp(2/1
5050
5050
2
TD50(1) : the tolerance dose
for reference volume
irradiation
m : the steepness slope of the dose response curve
Vref : the reference volume
n : tissue-specific parameter




Radiation therapy technique
Limited radiation portals Tangential beams 3 D Conformal irradiation
Multiple radiation beams to generate dose distributions that conform tightly to target volume.
Entire target volume is adequately treated while minimizing dose to normal structure.
IMRT Delivering intesity-modulated radiation to irregularly
shaped target volume by using dynamic multileaf collimators in 3DCRT.

洋紅 , 藍寶石

53 y/0 woman, adeno. LLL,(a) before RT, (b) 1mon after RT and(c) 5mon after RT




Mantle field: all the major lymph node regions above the diaphragm

Epidemiology
Clinical pneumonitis
Radiographic abnormalities
Breast ca. 0 ~ 10 % 27 ~ 40 %
Lung ca. 5 ~ 15 % 66%
Ref.: UpToDate: Radiation-induced lung injury

Radiation Pneumonitis vs Radiation Fibrosis
Atypia of type II pneumocytes Alveolar wall edema Infiltration of inflammatory cells
in the interstitium Aggregation of alveolar
macrophage Hyaline membranes lining
alveolar ducts and alveoli
Accumulation of fibrin Atypical fibroblasts in the
interstitium
Ref.: Semin Oncol 32(Suppl 3): S42-S54.

Capillary lumen
Type I pneumocyte Type I
pneumocyte
Type IIpneumocyte
Endothelium
Alveolar space
Type II pneumocyte secreting surfactant: lower surface tension

Histopathologic grading Acute phase (1-2 months post-RT )
Exudative: vascular congestion, edema, inflammatory response Clinically silent
Intermediate phase (2-9 months) Hyaline membrane formation Type II pneumocyte proliferation Macrophages fill air sacs Continued edema
Reparative phase (6-9 months) Type I & II cells depleted Thickened basement membrane Capillary regeneration
Late/Chronic (9+ months) Pulmonary fibrosis Type I pneumocytes (nondividing) replaced with scar tissue

Role of type II pneumocytes : dose response of radiation-induced lung changes in the transient high vascular permeability period
Wistar rats were given a single dose of 1–25 Gy irradiation to the thorax. Group one was treated with saline only, while group two was administered subcutaneously a combination of pentoxifylline (35 mg/kg) and dexamethasone (1 mg/kg) twice per week. Lungs were examined histochemically and number of neutrophile granulocytes, alveolar septal thickness, air/tissue ratio, number of alveoli per field, number of type II pneumocytes per alveolus, and occludin 1 expression were measured.
A significant dose-dependent depletion of type II pneumocytes was found after irradiation with a dose of 1 Gy and higher. Alveolar neutrophils increased after 1 Gy with a dose dependency noted after 10–25 Gy, and alveolar septa thickening followed 5–25 Gy. Anti-inflammatory therapy partially inhibited the increase of neutrophils at all radiation doses and the depletion of type II pneumocytes after doses of 1, 10, and 15 Gy.
Experimental and Toxicologic PathologyVolume 56, Issue 3, 3 December 2004, Pages 181-187

Radiation pneumonitis in mice:A severe injury model for pneumocyte engraftment from bone
marrow
The lung responds to irradiation with breakdown of alveolar capillaries, focal hemorrhage, and pneumocyte loss with maximal damage apparent 3 days postirradiation [8–10]. By day 5, healing is apparent and day 5 was the first time point at which cytokeratin, marrow-derived pneumocytes made their appearance as isolated cells, usually at the corners of alveoli, typical of type II pneumocytes. The percentage of marrow derived type II pneumocytes increased over time from an average of 0.9% at day 5 to 11–14% at month 6, demonstrating either progressive expansion of the engrafted population or continuous engraftment of circulating marrow derived cells. In animals sacrificed at months 2, 4, and 6,engraftment yielded isolated clusters of pneumocytes, which sometimes comprised entire alveolar surfaces. This pattern of engraftment supports the concept that type I pneumocytes derive from cells that had initially engrafted as type II pneumocytes.
Experimental Hematology 30 (2002) 1333–1338

Clinical manifestation Nonproductive cough Dyspnea Fever, low grade Chest pain Malaise and weight loss Skin erythema, outline the radiation port
Crackles or pleural rub; normal Dullness percussion due to pleural effusion cyanosis, pulmonary hypertension
Ref.: UpToDate: Radiation-induced lung injury. Semin Oncol 32(Suppl 3): S42-S54.

Grading of Acute Pneumonitis
Ref.: Semin Oncol 32(Suppl 3): S42-S54. Int j Radiation Oncology biol Phys 63(1):5-24.
ADL: activities of daily living
Radiation Therapy Oncology Group
South-West Oncology Group
National Cancer Institute

Grading of Late Lung Toxicity
Ref.: Semin Oncol 32(Suppl 3): S42-S54.

Incidence and RT protocol
2DRT 2 ~ 31 % for RTOG
grade 3 or SWOG grade 2,
NCI-CTC v3.0 grade 2 Medical help ( oxygen,
steroid )
3DRT
Ref.: Semin Oncol 32(Suppl 3): S42-S54.

Radiation Pneumonitis
Ref.: Semin Oncol 32(Suppl 3): S42-S54.

FDG PET Demonstrates Radiation-Induced Changes to Nonirradiated Lungs ..
Symptomatic pnuemonitis because of irradiation does not predict fibrosis, and tolerance of irradiation early in therapy does not predict development of symptomatic pneumonitis.
FDG PET was conducted before and after RT was localized to the tumor bed with shielding of the uninvolved areas.
PET scanning of lungs in irradiated patients may provide an early demonstrable barometer of pulmonary toxicity.
CHEST 2005; 128:1448–1452
To determine whether acute changes in shielded lungs can be detected by PET after RT.. ( single center from 1995 to 1999, C/T + R/T + op/ biopsy, 3/16 small cell, 13/16 NSCLC )

Results
13/16 showed increased FDG uptake in the shielded nonirradiated lung.
Pleural uptake seen in the patients exceeding the surrounding lung “ background” activity by20-30%:
Contralateral peripheral pleural uptake in 5/16 ( 31.2% ).
Ipsilateral peripheral pleural uptake in 5/16 ( 31.2% ). Bilateral peripheral pleural uptake in 1/16 ( 6.2% ) Bilateral background uptake in 1/16 ( 6.2% ) Three patient: no increased uptake in nonirradiated
lung ( 18.8% ) Clinically evident radiation pneumonitis: only one ( bil. )

Most RP occurs in RT tx fieldbut why bilateral ? Gibson et al: increased total number of cells recovered from
lavage fluid in both the irradiated and unirradiated lungs with mechanisms similar to hypersensitivity pneumonitis. Ann Intern Med 1998
Robert et al: breast cancer patients s/p RT, p’t with clinical pneumonitis: bilateral severe lymphocytic alveolitis and bilateral increased Ga-67 uptake ( even in p’t without symptom). Ann Intern Med 1993
Arbetter et al: radiation induced organizing pneumonitis outside the direct RT field in breast cancer patients. 2 patients with lymphocytes found on BAL sample, 5 with bronchiolitis obliertans-organizing pneumonia on lung biopsy samples. Attributed to lymphocytic alveolitis. Mayo Clin Proc 1999
Fujita et al: two case with bilateral RP with unilateral thoracic RT for lung cancer. Histologically: diffuse alveolar damage, and antibodies against cytokertin 8,18, and 19. Respir Med 2000

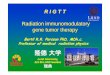
Radiation Pneumonitis: Pulmonary Metabolic Response to Radiation ( PMRR) in Lung Cancer Patients
BACKGROUND: Radiation pneumonitis is a potentially fatal complication of thoracic radiotherapy. Its prediction, detection, and prevention are important in allowing better tumor control in certain patients. [(18)F]2-fluoro-2-deoxyglucose positron emission tomography (FDG-PET) detects tissue metabolic activity, including inflammatory response, and can quantify the normal tissue response to radiation.
Matthew McCurdy1,2, Josue Martinez3, Rick Castillo4, Nicolas Zouain2, and Thomas Guerrero41.Baylor College of Medicine, Houston, TX, 2. University of North Dakota School of Medicine & Health Sciences, Fargo and Grand Forks, ND 3. Texas A&M University, College Station, TX, 4. The University of Texas M.D. Anderson Cancer Center, Houston, TX

Purpose
To quantify the relationship between the local radiation dose received and the posttreatment PET/computed tomography (PET/CT) FDG uptake in the lung in patients with lung cancer.
The overall objective was to validate FDG-PET imaging as an imaging biomarker of radiation .


RESULTS: The median time between radiotherapy completion and FDG-PET imaging was 47 days (range, 34-71 days). The removal of the tumor volume from analysis was possible using a threshold planning dose. The median of the mean standard uptake value in the lung that received 0-5 Gy was 0.51 (range, 0.35-1.15), 5-10 Gy was 0.77 (range, 0.40-1.36), 10-20 Gy was 0.80 (range, 0.40-1.69), and >20 Gy was 1.08 (range, 0.55-2.70). A hierarchical linear regression model of the radiation dose and normalized FDG uptake per case found an adequate fit with the linear model. The 18 cases had a posterior mean of slopes range of 0.0011-0.064. The slope of this relationship varied over an order of magnitude, reflecting the range of the underlying pulmonary biological response to radiation among the study population.



1. A linear relationship was found between the local radiation dose and the voxel-averaged post-treatment FDG uptake.
2. The slope of that relationship varied across the patients and was independent of the interval between radiotherapy completion and PET imaging (within 1–3 months) and of the percentage of volume of lung irradiated.
3. We propose this response slope is a measure of the underlying individual intensity of radiation pneumonitis
Conclusion:

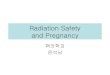
Local dose vs. FDG uptake response in irradiated lung
Purpose: To quantify the relationship between local radiation dose received and posttreatment FDG uptake in the lung.
Methods and Materials: 36 p’t with esophageal cancer s/p RT, underwent restaging PET/CT between 4-12 weeks after completion of RT. Using histiogram analysis, the voxel average FDG-PET uptake vs. radiation dose was obtained for each case.
Thomas Guerrero, et alDivision of Radiation Oncology, and Department of Biostatistics and Applied Mathematics
I.J. Radiation Oncology Bio. Phys. Vol. 68 No.4 pp.1030-35

The Slope
I.J. Radiation Oncology Bio. Phys. Vol. 68 No.4 pp.1030-35

FDG uptake not related to time and volume
I.J. Radiation Oncology Bio. Phys. Vol. 68 No.4 pp.1030-35

I.J. Radiation Oncology Bio. Phys. Vol. 68 No.4 pp.1030-35

FDG PET in predicting RP SONG Hao, YU Jin-ming, Feng-ming Kong, LU Jie, BAI Tong, MA Li and FU ZhengDepartment of Radiation Oncology, Tianjin Medical University Cancer Institute and Hospital, Tianjin 360060, China (Song H); Department of Radiation Oncology (Yu JM).
Methods:1.41 patients with lung cancer underwent FDG-PET/CT before and after radiotherapy. The mean standardized uptake value (SUV) was measured for the isodose regions of 0–9 Gy, 10–19 Gy, 20–29 Gy, 30–39 Gy, 40–49 Gy. The mean SUV of these regions after radiotherapy was compared with baseline. The mean SUV in patients who developed RP was also compared with that in those who did not. 2. The Radiation Therapy Oncology Group (RTOG) criteria were used for diagnosis and grading of RP.

Conclusion
The data supported a linear relation between the radiation dose and the normalized FDG uptake in the lung.
The slope of this relationship varied over an order of magnitude, reflecting the range of the underling biologic response to radiation.



Conclusion
Compared with their counterparts, the elevation of SUV was significantly greater in those patients who developed acute RP subsequently. Unexpectedly elevated SUV levels probably carry high risk of RP.
FDG-PET/CT may play a new role as a bio-barometer of the radiation damage of the lung.

Radiation Pneumonitis: correlation of Toxicity with PMRR
Purpose: to charactierize the relationship between RP clinical symptoms and PMRR
Patients and Methods: Retrospective, 101 esophageal cancer 3-12 weeks after completion of RT with restaging PET/CT. NIH-CTCAE v.3. (by definition a 5-point scale, mild, moderate, severe, life-threatening and death ) to score RP symptoms. Linear regression for normalized FDG uptake vs. radiation dose. PMRR was quantified as this slope. Modeling was performed to determine the interaction of PMRR, MLD and the percentage of lung receving > 20 Gy with RP outcome.
I. J. Radiation Oncology Biology Physics Volume 71, Number 4, 2008
Justin P. Hart, MD., PH.D., Mathew R. McCurDy, PH.D. et al.Department of Radiation Oncology, Quantitative Sciences, and Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, TX..



Take home messages (1) Early RP develops within 4-12 weeks after RT, and radiation
fibrosis develops within 6-12 months after RT and can progress for up to 2 years before stability.
CXR: consolidation usually coalesces and typically has a relatively sharp ( geographic ) border that conforms to the treatment portals rather than anatomic boundaries.
Incidence of pneumonitis curve linear correlation with mean lung dose.
Autoimmune process may play a role in the development of RP.
FDG PET response has linear correlation with radiation dose delivery although some cancers might have threshold ( no response for the first 15 Gy ).
FDG uptake not well related to time and volume after RT.

Take home messages (2) Pulmonary metabolic response to radiation (
PMRR) in lung cancer patients, associated with mean lung dose, best predicts of radiation pneumonitis, in comparsion with PMRR only, MLD only, V20 only, PMRR+V20, and MLD+V20.