Embed Size (px)
Citation preview
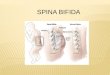
Spina BifidaAmaan Mohiuddin
Gary Oh
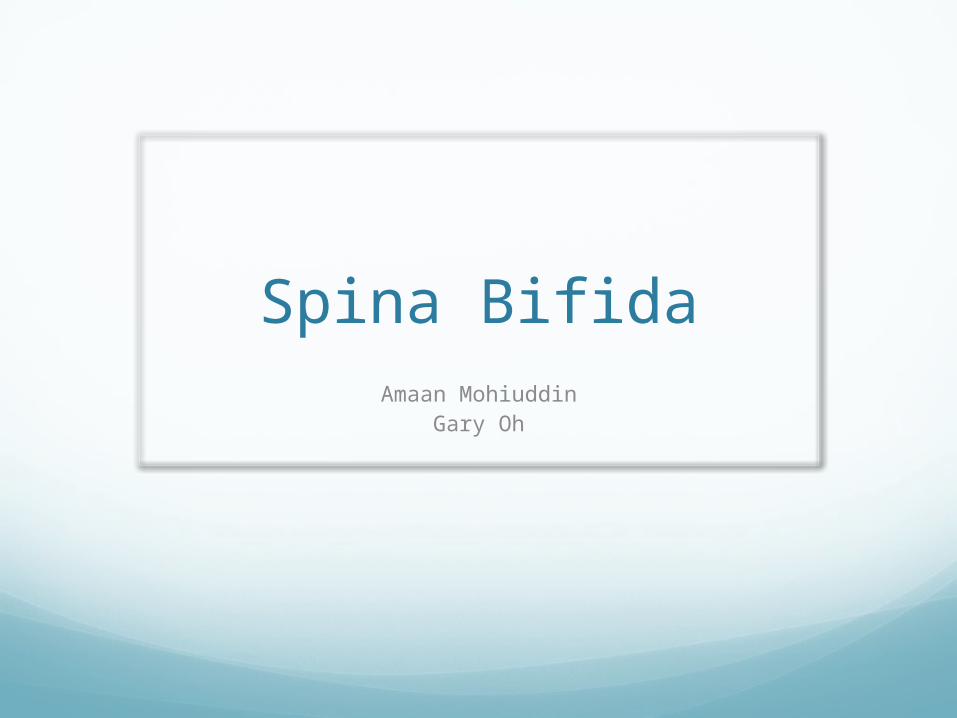
CaseNewborn infant in the
labor and delivery room
Physical examVital signs normalAppearance
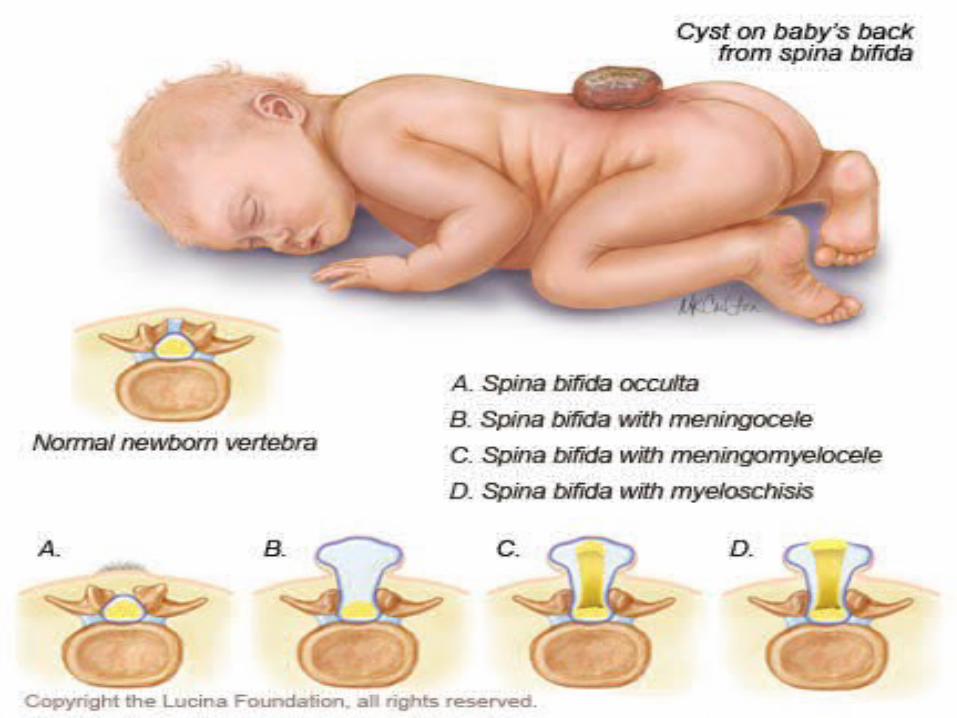
Bulging cyst-like structure approximately 4 cm in diameter protruding from his back.
Child has limited movement of the lower extremities
Both feet are plantarflexed and inverted at the ankle
What is it?“Cleft spine,” is characterized
by the incomplete development of the brain, spinal cord, and/or meninges.
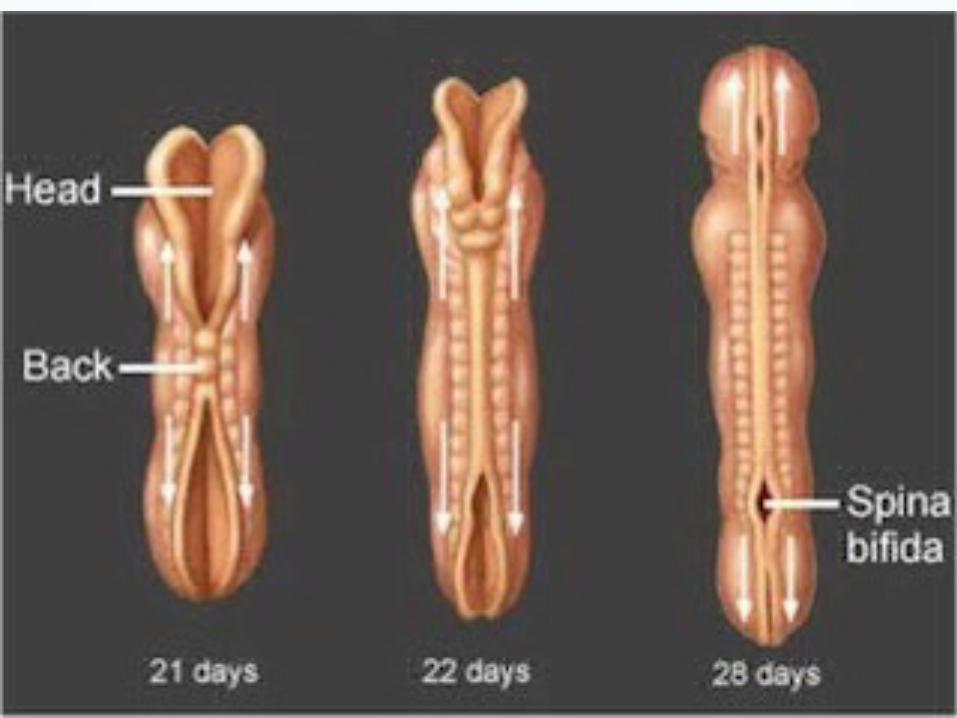
Neural Tube DefectFailure to close during 4th
week embryogenesis
SymptomsLeg paralysis
Incontinence
Anaesthesia
Hip, knee, feet abnormalities
Hydrocephalus
Arnold-Chiari Type II
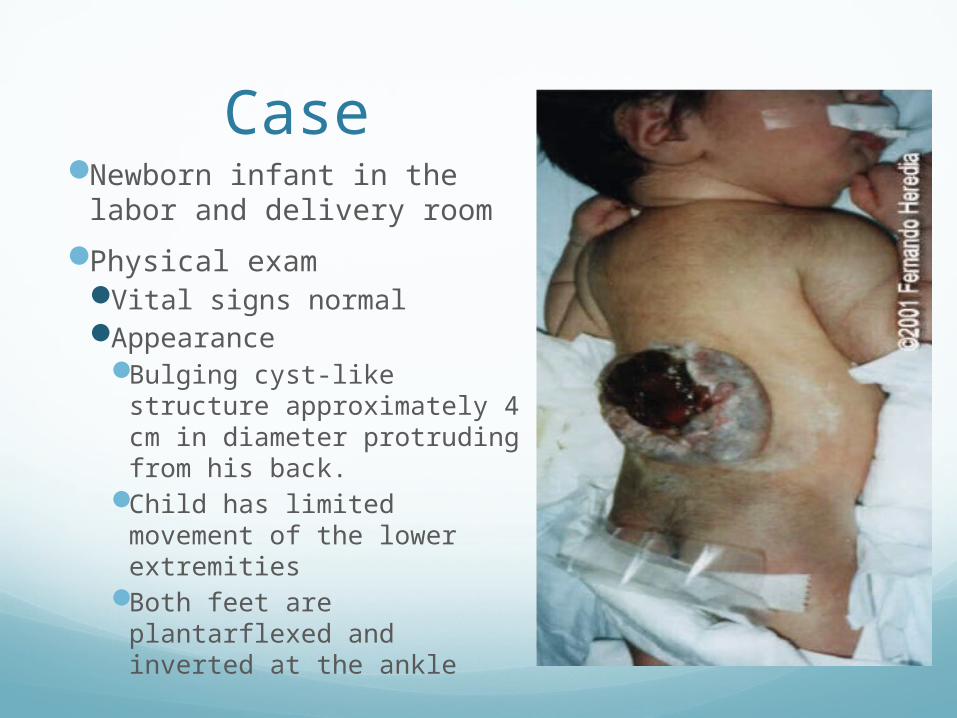
Physical ExamInspection (Back):
Tuft of hair, subcutaneous lipoma or dimple may be observed in occulta
Localised sac in cystic type, increased head size
Deformity of lower limb as flexion: Abduction and internal rotation of hipFlexion or hyper extension kneeEquinous or calcanous deformity of foot,Scoliosis or lordosis of spine
Skin ulceration and soft tissue injury due to pressure
Physical Exam(Cont)Palpation:
Bony defectSubcutaneous lipomaLoss of sensation and muscle bulk
ScreeningMyelomeningocele can be diagnosed in second
trimester of pregnancy
Increased maternal serum alpha-fetoprotein (MSAFP) Check at 15-20 weeks if maternal age > 35
yearsPrior child with open neural tube defect
Amniocentesis at 14-18 weeksRoutine second-trimester ultrasound might be
more sensitive than MSAFP alone for detecting neural tube defects
Screening (Cont)Imaging
Spinal X-rayUSMRI
Dysraphism – incomplete closure of bony ring or vertebrae surround neural tube (spinal cord)
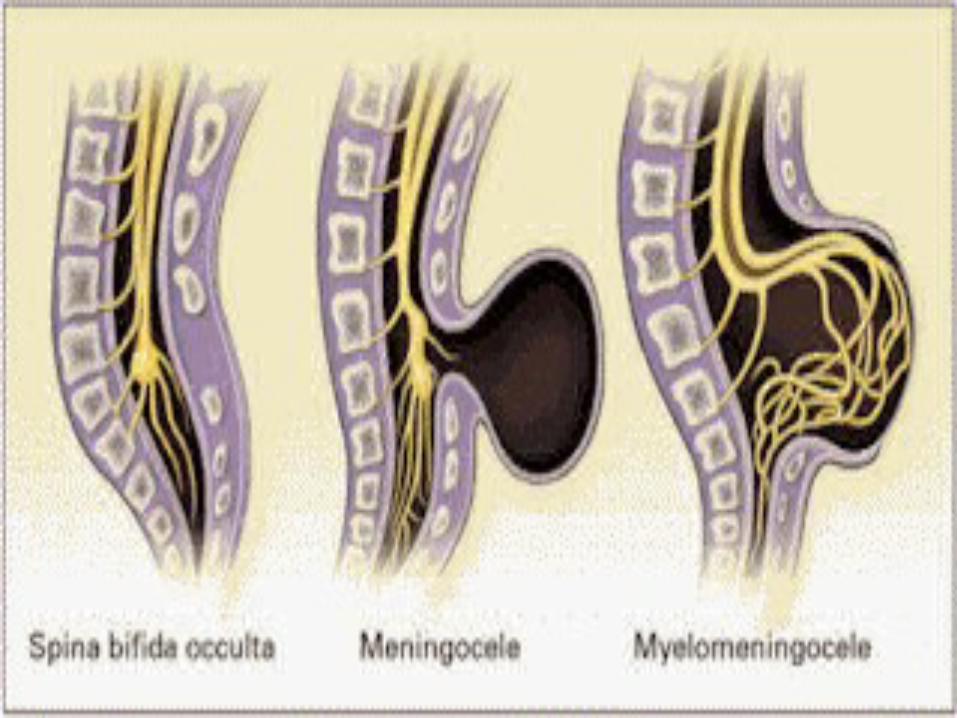
Spina bifida occulta Mildest form of spina bifida Abnormal opening of spine, may have dimple on skin,
tuft of hair or nothing Small defect in one or more vertebrae, usually no
complications Outer part of some vertebrae not completely closed The split in the vertebrae is so small that the spinal
cord does not protrude The condition is asymptomatic Bony abnormality seen by X–ray
Classification
Classification (Cont)Meningocele
Spinal defect with cyst of membranes protruding through spine
Vertebral arches are unfusedHerniation of the meningesCorrective surgery can be done
MyelomeningoceleSpinal defect with cyst including membranes,
nerve roots and possibly spinal cord protruding through spinal opening.
The spinal cord fails to develop properly and nerves are damaged
CauseScientists suspect genetic, nutritional,
and environmental factors play a role
Folic acid deficiencies from lack of intake before and during pregnancy have shown to be a cause
The Folate Metabolism Pathway is suspected to be a major contributor
IncidenceMost common severe birth defects in the
United States
1,500 to 2,000 babies (one in every 2,000 live births) each year
1970 to 1977: In US, incidence of spina bifida decreased 6.7%/year, before folic acidsupplementation was prevalent
1996: The US FDA authorized all enriched grain products be fortified with folic acid
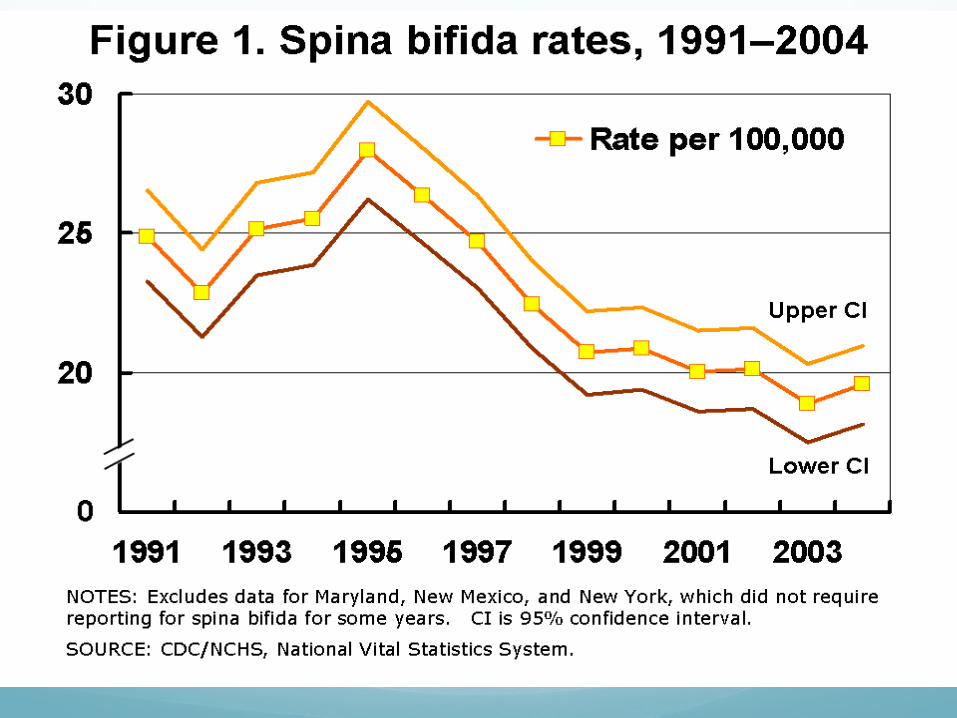
PrevalenceDecreased prevalence of spina
bifida and anencephaly from 1995 to 2002 in United States (during period of transition to mandatory folic acid fortification)
Risk FactorsPROBABLE:
History of prior delivery of offspring with neural tube defect
Prenatal exposure to valproic acidMaternal diabetesMaternal obesity
POSSIBLE:Maternal peri-conceptional opioid useLower vitamin B12 levels during pregnancyAntimalarial drugs during first trimesterChronic low-dose radiation exposure
Associated ConditionsDermal sinus tract
Diastematomyelia (splitting of cord into half)
TreatmentPrenatal surgery for myelomeningocele
reduces need for shunt placement compared to postnatal repair
Primary surgical closure of defect to prevent infection in more severe casesOften hydrocephalus develops due to
associated Arnold-Chiari malformation, shunting may be necessary
ComplicationsMental retardation and seizures with
hydrocephalus
Neurologic deficits below lesion
Absent bladder control, recurrent urinary tract infections
Urinary diversion severe chronic constipation
Club foot
PrognosisImproved 1-year survival from 1979 to
2003
Worsening cerebellar herniation on MRI associated with increased risk of poor functional outcomes in fetuses with spina bifida
Perineal sensation in infancy predicts better prognosis in patients with open spina bifida
PreventionFolic acid fortification associated with reduction
in incidence of neural tube defects
Folic acid 0.4 mg/day around time of conception
4 mg/day if previous infant with neural tube defects
Peri-conceptional folate supplements associated with reduced frequency of neural tube defects in women with and without previously affected pregnancy
ReferencesDynamed: Spina BifidaObstet Gynecol 2005 Oct;106(4):747MMWR Morb Mortal Wkly Rep 1997 Dec 12;46(49):1171 full-text in Pediatric
Notes 1998 Jan 1;22(1):1Pediatrics 2005 Sep;116(3):580, editorial can be found in Pediatrics 2005
Sep;116(3):753, commentary can be found in Pediatrics 2006 Apr;117(4):1394
Cerebrospinal Fluid Res 2006 Aug 1;3:10 full-textObstet Gynecol 2013 Oct;122(4):838Pediatrics 2009 Mar;123(3):917Pediatr Neurosurg 2011;47(3):194 in J Neonat Surg 2012 Jul-Sep;1(3):43 PDFPediatrics 2010 Apr;125(4):e836Birth Defects Res A Clin Mol Teratol 2012 Oct;94(10):756Pediatric Surgery Update 2008 Jan;30(1):2Pediatric Surgery Update 1998 Apr;10(4):3Pediatrics 1998 Sep;102(3):e34BMC Pediatrics 2005 Aug 25;5:32J Pediatr 2012 Dec;161(6):1132Obstet Gynecol 2010 Aug;116(2 Pt 1):323Arch Dis Child 2007 Jan;92(1):67Cochrane Database Syst Rev 2010 Oct 6;(10):CD007950